
Submitted:
22 December 2025
Posted:
22 December 2025
You are already at the latest version
Abstract
Background/Objectives: Nutritional status and the gut microbiome play key roles in supporting treatment tolerance and recovery among patients with colon cancer receiving chemotherapy. This pilot study examined (1) changes in diet quality and fecal microbiome profiles during 6-month chemotherapy and (2) associations between diet quality and microbiome diversity and composition over time. Methods: A longitudinal study of 48 adults with stage II–III colon cancer receiving 5-Fluouracil (FU)–based chemotherapy assessed diet quality and the gut microbiome at baseline and 6 months post-chemotherapy initiation. Diet quality was measured using 3-day dietary recalls to compute Healthy Eating Index (HEI) scores. Stool samples collected at both timepoints underwent 16S rRNA sequencing to quantify Shannon diversity and taxonomic composition. Pre–post differences were examined using paired tests, and associations between HEI and microbiome indicators were evaluated with multivariable linear regressions adjusting for demographic and clinical covariates. Results: Diet quality declined during chemotherapy (HEI 62.4→54.2, p=0.015). Shannon diversity also decreased (1.20→1.05, p=0.011). Microbiome composition shifted, with declines in Short-Chain Fatty Acids (the result of fiber fermentation)-producing taxa (Agathobacter, Bifidobacterium, and Prevotella), and increases in Bacteroides and Proteobacteria. Higher baseline HEI was linked to greater microbial diversity, higher levels of beneficial Firmicutes, and lower Proteobacteria. Changes in HEI were significantly aligned with changes in fecal microbiome profiles. Conclusions: Chemotherapy worsens diet quality and gut microbial health. Higher baseline diet quality appeared protective against microbial disruption, supporting a bidirectional diet–microbiome relationship. Early nutritional and microbiome-supportive strategies may help preserve gut resilience during chemotherapy.
Keywords:
colon cancer
; fecal microbiome
; diet
; nutrition
; chemotherapy
1. Introduction
Colon cancer is the third most commonly diagnosed cancer and the second leading cause of cancer-related deaths in the United States (US)[1], as well as globally [2]. In the United States alone, an estimated 106,590 new cases of colon cancer and 46,220 cases of rectal cancer will be diagnosed in 2025, with over 50,000 deaths expected annually due to colon cancer-related complications [3]. The incidence of colon cancer is particularly high among individuals over 50 years old, though rates are increasing among younger adults[4]. Standard treatment for stage II and III colon cancer typically involves surgical resection followed by adjuvant chemotherapy to prevent recurrence and improve survival [5].
Nutritional health plays a pivotal role in determining both treatment efficacy and health-related quality of life (HRQOL) in patients with colon cancer undergoing chemotherapy [6]. Malnutrition is prevalent among individuals receiving cancer treatments. Specifically, with estimates suggesting that up to 80% of gastrointestinal cancer patients experience nutritional deficiencies even before chemotherapy, as well as during or after chemotherapy [7]. Poor nutritional status can exacerbate treatment-related toxicity, reduce chemotherapy tolerance, increase hospitalization rates, impair physical function and HRQOL, and contribute to emotional distress and fatigue [8]. Furthermore, diet quality has been associated with better symptom control, fewer gastrointestinal side effects (e.g., diarrhea, mucositis, nausea), reduced infection risk, and improved immune and metabolic responses to therapy [9]. Good nutrition is thought to support mucosal repair and gut barrier integrity, which are often compromised during 5-fluouracil (FU)-based chemotherapy, as the most common chemotherapy regimen in colon cancer [10]. Therefore, early identification of malnourished patients and timely nutritional intervention may improve clinical outcomes, reduce complications, and enhance adherence to the optimal chemotherapy regimens [11].
In recent years, gut microbiomes have emerged as a critical mediator of chemotherapy response, toxicity, and patient-reported outcomes [12]. Chemotherapy for colon cancer causes significant changes in gut microbial composition and function, known as gut dysbiosis.[13] This dysbiosis has been associated with worse gastrointestinal and psychological symptoms, increased risk of adverse events, systemic inflammation, and reductions in function and HRQOL [14]. Numerous studies suggest that certain microbial taxa (e.g., Lactobacillus, Bifidobacterium) may protect against chemotherapy-induced toxicity, while others (e.g., Enterobacteriaceae, Clostridium difficile) may promote inflammatory or toxic effects in other cancer types [15]. Importantly, the relationship between the gut microbiome and nutrition is dynamic and could be bidirectional, forming a complex feedback loop that has significant implications for cancer treatment and recovery [16,17,18]. On one hand, diet is a key determinant of gut microbial diversity, composition, and function [18]. Diets rich in fiber, fruits, and whole grains are associated with increased microbial diversity and enhanced production of short-chain fatty acids (SCFAs), such as butyrate, which support gut epithelial integrity, modulate immune responses, and reduce inflammation [18]. Conversely, low-quality diets—often low in fiber and high in saturated fats and processed foods—can promote microbial imbalance and pro-inflammatory metabolites, leading to dysbiosis [19]. Mechanistically, the gut microbiome plays an essential role in shaping nutritional status by influencing nutrient absorption, vitamin biosynthesis, bile acid metabolism, and even appetite regulation through gut-brain signaling pathways [20]. In the context of chemotherapy, microbial dysbiosis may exacerbate treatment-related toxicities by increasing intestinal permeability, impairing mucosal healing, and contributing to symptoms such as diarrhea, nausea, anorexia, and constipation [21,22]. These symptoms, in turn, can lead to reduced oral intake, malabsorption, and progressive nutritional decline, creating a vicious cycle of inflammation, gastrointestinal dysfunction, and undernutrition [23].
Despite the known clinical importance of both diet and the microbiome in cancer health outcomes, including gastrointestinal conditions, chemotherapy side effects, function, and HRQOL, empirical data are lacking in patients with colon cancer [24]. Specifically, little is known about how diet quality and microbiome profiles change longitudinally in colon cancer patients during chemotherapy. Furthermore, fewer studies have examined their interdependence over time; that is, whether patients with worsening gut dysbiosis also experience declining dietary quality or vice versa [25,26]. This knowledge gap is particularly critical given the increasing recognition that nutrition-microbiome interactions may influence cancer outcomes, immune competence, HRQOL, and resilience to treatment [18,19]. However, few studies have explored how these factors change over time during chemotherapy in colon cancer patients. Understanding these longitudinal trajectories and whether specific populations are more vulnerable to adverse microbiome-nutrition dynamics, is critical for informing early, personalized interventions. Identifying patients with declining microbial diversity and worsening nutritional status during chemotherapy could guide timely nutritional support, such as high-fiber or protein-dense diets, or consideration of microbiome-modulating strategies (e.g., probiotics, prebiotics, or fecal microbiota transplantation). For example, patients with persistent constipation, poor appetite, taste alterations, or gastrointestinal discomfort may benefit from microbiome-targeted approaches to improve eating conditions and nutrient absorption.
Therefore, the objective of this study is twofold: (1) to characterize longitudinal changes in dietary quality and gut microbiome diversity and composition during chemotherapy; and (2) to examine longitudinal associations between dietary quality and gut microbiome (baseline and changes over time).
2. Materials and Methods
2.1. Design
We conducted a pilot study using a longitudinal, prospective study design in 48 patients with stages II or III colon cancer. All data were collected pre- and 6-month post chemotherapy initiation. Patients were enrolled at the Oncology Clinics of the Ohio State University Comprehensive Cancer Center between March 2024 and May 2025. This study was approved by the Ohio State University’s Institutional Review Boards (IRB), and all enrolled patients provided informed consent.
2.2. Sample
We used a purposive sampling method to recruit patients with stages II or III colon cancer (N = 48). Inclusion criteria for all participants included being > 18 years old and having a histological proof of stages II-III colon cancer. In addition, patients had to be diagnosed with no distant metastasis, scheduled to receive 5-FU-based chemotherapy (5-FU alone or 5-FU combinations - FOLFOX or FOLFIRI), following colon surgeries, and had adequate organ function. Exclusion criteria for patients included chronic medical conditions involving the immune system (E.g., HIV, hepatitis B or C), regular use of immunosuppressive medications other than that routine steroids injection before the 5-FU-chemotherapy, those who cannot read and speak English, individuals with a current ostomy, chronic bowel disorders (such as irritable bowel syndrome); use of antibiotics, supplements of prebiotics, or probiotics within 1 month prior to each sample-collection time point; subjects with a significant cognitive or developmental delay; received neoadjuvant chemotherapy; and women who were pregnant.
2.3. Recruitment Strategies
Prior to participating in enrollment, the study protocol was approved by the Clinical Scientific Review Committee and the IRB of The Ohio State University Comprehensive Cancer Center. Patients with colon cancer were recruited through The Ohio State University Comprehensive Cancer Center –James Gastrointestinal Clinics and via mailings coordinated by the Ohio State University Cancer Center and College of Nursing, using purposive sampling methods. Recruitment was further supported through posters placed in the recruitment cancer center site. Patients who consented to be contacted for research received a phone call from a trained research assistant. Following completion of a screening questionnaire, eligible individuals were invited to review the study consent form, provide contact information, and schedule a follow-up phone call for enrollment and study orientation. To ensure diverse racial and ethnic representation, we purposively recruited racial and ethnic minority participants to comprise approximately half of the sample (n = 24 out of the total 48 target samples). This effort was supported through collaboration with The Ohio State University Center for Community Outreach and Engagement, which conducted targeted outreach to patients from underrepresented backgrounds.
2.4. Data Collection
Study materials and survey questionnaires were distributed either electronically via REDCap (Research Electronic Data Capture) or mailed directly to participants’ homes. Stool collection kits were also mailed, and instructions were reviewed with participants by phone. Participants were asked to return completed questionnaires either online or by mail using pre-stamped envelopes. Stool specimens were shipped overnight to the Ohio State University Biospecimen Services Shared Resource (OSU BSSR). Each participant provided diet quality data and stool samples at baseline before chemotherapy and again at 6 months, at the time of chemotherapy completion. Participants received a $25 electronic gift card for each completed time point, contingent upon receipt of both the questionnaire and stool sample.
2.5. Measures
2.5.1. Sociodemographic Data at Baseline
Demographic variables were collected via self-report survey or abstracted from electronic medical records, such as age, sex, marital status, employment status, race, education, types of insurance, and lifestyle.
2.5.2. Clinical data at baseline
Clinical data were abstracted from electronic medical records, such as cancer stage, time since diagnosis, chemotherapy regimen, history of other cancer treatments, and comorbidities.
2.5.3. Diet Quality (at Baseline and 6-Month Post-Chemotherapy Initiation)
We used the self-reported Short Form Food Frequency Questionnaire (SF-FFQ, 24 items, reliability = .74) and assessed this for 3 days at the time of data collection. We subsequently computed the mean values based on the 3-day dietary recalls [27]. Based on dietary intake and food groups including fruits, vegetables, grains, protein, dairy, fats and oils over the last week, we computed Healthy Eating Index (HEI) (0 “low” to 100 “high”) for use in our analysis, as a measure of diet quality (reliability = 0.91, sensitivity = 0.94) [28]. Nutritionist Pro software (version 2025) was used for data analysis [29].
2.5.4. Fecal Microbiome Profile (at Baseline and 6-Month Post-Chemotherapy Initiation)
At-Home Collection of Stool Samples. Study participants were mailed at-home stool collection kits (DNAgenotek) with written and video instructions, return packaging, and return postage, for which 500mg of stool was collected in 2mL of DNA-stabilizer solution. Defecating normally, the participant used a sterile spatula to collect an aliquot and sealed the tube by screwing on the lid. Stool samples were stored at 40C after stool collection for up to 48 hours at patients’ homes. Samples were then mailed directly to the OSU Biospecimen Services Shared Resource (OSU BSSR), and fecal samples were immediately stored at – 800C. The OSU BSSR team sent the collected stool samples to Zymo Research (Irvine, CA), where DNA extraction and sequencing were performed using 16S rRNA sequencing.
Microbiome Profiling. First, the DNA was purified with the Promega Maxwell RSC Fecal Microbiome kit (Promega, Madison, WI), sequencing libraries were generated with the Illumina DNA Prep kit (Illumina, San Diego, CA), the V3–V5 hypervariable regions of the bacterial 16S rRNA gene were amplified and 2x150bp sequencing was performed on an Illumina NextSeq2000 at Zymo Research (Irvine, CA).
Then, we assessed diversity and composition (abundance and types of bacterial taxa) of fecal microbiome bacterial profiles using 16S rRNA sequencing. Raw reads were quality filtered, trimmed, and de-noised to generate ASVs, followed by taxonomic assignment using a curated reference database. Relative abundances and alpha diversity metrics were calculated from normalized data. We excluded low-abundance bacteria with relative abundance levels < 5% at the level of phylum. We specifically assessed Shannon’s index to calculate diversity (within-sample species diversity, calculated as a function of proportional abundance). Furthermore, our study focused on phylum and genus levels in microbiome abundance data by considering clinical or translational research purposes. We used Quantitative Insights Into Microbial Ecology (QIIME) 2 to compute Shannon diversity and bacterial taxonomic compositions (types and relative abundance).
2.6. Statistical Analysis
To evaluate within-subject changes in diet quality and stool microbiome alpha diversity between pre- and post-chemotherapy timepoints, paired statistical tests were conducted. Alpha diversity indices (e.g., Shannon) and diet scores (HEI) were assessed for normality using the Shapiro–Wilk test prior to selecting the appropriate test. Given that our data was non-normally distributed, we used Wilcoxon signed-rank tests and long-transformed prior to analysis. Then, we used linear regression models to examine associations between the HEI and gut microbiome profiles. HEI was assessed at baseline and as a change score (post-chemotherapy minus pre-chemotherapy). Microbiome outcomes included alpha diversity metrics and log-transformed relative abundances, evaluated at baseline and as change scores. Separate models were fitted for each microbiome composition, with HEI as the independent variable. All models were adjusted for age, sex, body mass index (BMI), cancer stage, and chemotherapy regimen (types and doses), and baseline HEI score or microbiome measures when applicable. Based on prior research in colon cancer that observed a medium effect size (Cohen’s d = 0.5; standard deviation = 1.0) in the pre-post change of gut microbiome alpha diversity [24,25,26], a sample size of 48 participants is estimated to provide 85% power to detect a similar medium effect (i.e., a 0.5-point change in a gut microbiome alpha diversity, using a two-sided linear regressions at a 0.05 significance level [26]. Results are reported as beta coefficients (β) with 95% confidence intervals (CIs) and p-values. Analyses were conducted in R (version 4.4.0) and Python, and significance was set at p < 0.05.
3. Results
3.1. Characteristics of Participants
The study included 48 participants (mean age: 69.4 years, SD = 6.7; range: 59–86), with 54.2% male and 58.3% married (Table 1). Most were not employed (72.9%), and education levels varied: 31.3% had a high school diploma or less, 25.0% had some college, 29.2% had undergraduate degrees, and 14.6% had graduate degrees. The sample was evenly split between Black and White participants (50% each). Most had public insurance (58.3%), and 4.2% were uninsured. The majority were never smokers (62.5%), and 18.8% reported current alcohol use. About one-third reported low income (<$35,000), 37.5% middle, and 29.2% high income (≥$75,000). Healthy diet and routine physical activity were reported by 39.6% and 35.4%, respectively. Clinically, 76.9% had stage III and 23.1% stage II cancer. The mean time since diagnosis was 0.8 years (SD = 0.9). Chemotherapy included FOLFOX (50.0%), 5-FU alone (29.2%), and FOLFIRI (20.8%). All had prior colon surgery; 25.0% received radiation. Most (95.4%) had a Charlson comorbidity index > 2 (Table 1).
3.2. Nutritional Profiles Pre- and Post-Chemotherapy
Following chemotherapy, patients experienced marked reductions in several key dietary components (Table 2). Table 2 highlights substantial dietary deterioration during chemotherapy, particularly in plant-based nutrient sources and essential micronutrients. For macronutrients, the largest decline was observed in dietary fiber, which dropped by 17.1% (21.6 ± 5.4 to 17.9 ± 4.8 g/day, p = 0.009), followed by total calories (–12.7%, p = 0.012), total fat (–12.4%, p = 0.018), carbohydrates (–10.7%, p = 0.033), and protein (–10.5%, p = 0.021). For micronutrients, the greatest reduction occurred in vitamin D intake, which fell by 21.0% (310 ± 140 to 245 ± 115 IU, p = 0.041). Calcium and iron also showed notable decreases of 12.2% (p = 0.027) and 11.9% (p = 0.034), respectively. Changes in folate (–9.2%) and sodium (–0.7%) were not statistically significant. For dietary intake (food groups), the most pronounced change was in fruit and vegetable consumption, which declined by 26.5% (3.4 ± 1.2 to 2.5 ± 1.0 servings/day, p = 0.004). This was followed by whole grain intake (–23.1%, p = 0.007), added sugar (–16.2%, p = 0.026), and red meat (–18.2%, p = 0.048). The Healthy Eating Index (HEI) score significantly declined from 62.4 ± 8.5 pre-chemotherapy to 54.2 ± 9.3 post-chemotherapy (p = 0.015), reflecting a 13.1% reduction in overall dietary quality. This decrease was consistent with lower intake of fiber, fruits, vegetables, and whole grains, and reflects chemotherapy-related nutritional vulnerability.
3.3. Microbiome Profiles Pre- and Post-Chemotherapy
3.3.1. Shannon Diversity
3.3.2. Relative Abundance of Major Microbiome Phylum Pre- and Post-Chemotherapy
Fifteen phyla, excluding extremely low baseline abundances (≤0.20%), were identified as the major microbiome phyla in our dataset. Based on Wilcoxon signed-rank tests comparing relative abundance before (Pre) and after (Post) an intervention, significant changes occurred in several bacterial phyla (Table 4 and Figure 2). Actinobacteria (Pre: 6.71%, Post: 5.11%, p=0.002), Cyanobacteria (0.15% vs. 0.10%, p=0.002), and Ascomycota (0.04% vs. 0.02%, p=0.002) showed highly significant reductions over time. In contrast, Bacteroidota significantly increased (29.08% vs. 30.68%, p=0.003), as did Proteobacteria (3.62% vs. 3.95%, p=0.003), Firmicutes_C (1.35% vs. 1.44%, p=0.013), Verrucomicrobiota (1.19% vs. 1.12%, p=0.037), and Methanobacteriota (0.26% vs. 0.27%, p=0.0195). Firmicutes_A showed a marginal decrease (51.19% vs. 50.63%, p=0.0193).
3.3.3. Relative Abundance of Major Microbiome Genus Pre- and Post-Chemotherapy
25 genera were identified as the most major microbiome genus. The Wilcoxon signed-rank test revealed significant changes in several bacterial genera from pre- to post-treatment (Table 5 and Figure 3). Notably, Bacteroides showed a small but statistically significant increase in relative abundance (+1.84%, p = 0.042), while Blautia_A, Phocaeicola, and Agathobacter significantly decreased (−4.87% to −11.07%, all p < 0.05). Bifidobacterium also showed a significant reduction (−16.58%, p = 0.019), whereas Streptococcus and Prevotella had marked decreases of −22.23% and −58.04%, respectively (both p ≤ 0.031). In contrast, Faecalibacterium and Parabacteroides increased (+30.06% and +26.15%, respectively), though these changes were not statistically significant (p > 0.05). Escherichia decreased significantly by −63.39% (p = 0.012). Other genera, such as Alistipes, Ruminococcus_E, and Fusicatenibacter, showed non-significant increases, while several genera exhibited minor or non-significant changes throughout the study period.
3.4. Associations Between Diet Quality Measured with HEI and Microbiome Profiles
Linear regression analyses revealed significant associations between diet quality (HEI scores) and both microbial diversity and the relative abundances of specific phyla and genera (Table 6 and Table 7).
3.4.1. Diet quality and Shannon Diversity (Table 6)
Higher baseline HEI was positively associated with baseline Shannon diversity (adjusted B = 0.20, 95% CI: 0.06–0.34, β = +0.38, p = 0.02) and with increases in Shannon diversity over time (Δ Shannon diversity: adjusted B = 0.26, 95% CI: 0.09–0.43, β = +0.49, p = 0.01). Additionally, changes in HEI were positively associated with changes in Shannon diversity (adjusted B = 0.16, 95% CI: 0.03–0.29, β = +0.29, p = 0.02). However, baseline Shannon diversity was not associated with changes in HEI scores.
3.4.2. Diet Quality and Microbial Phyla (Table 6)
Higher baseline HEI was associated with greater baseline abundance of Firmicutes_A (adjusted B = 0.98, 95% CI: 0.02–1.94, β = +0.28, p = 0.05) and Firmicutes (adjusted B = 1.35, 95% CI: 0.15–2.55, β = +0.34, p = 0.03), and with increased Firmicutes over time (Δ Firmicutes: adjusted B = 1.02, 95% CI: 0.05–1.99, β = +0.24, p = 0.04). In contrast, higher HEI was significantly associated with lower baseline Proteobacteria (adjusted B = −1.00, 95% CI: −1.80 to −0.20, β = −0.36, p = 0.02), and reductions in Proteobacteria over time (Δ Proteobacteria: adjusted B = −0.87, 95% CI: −1.68 to −0.06, β = −0.29, p = 0.04). Baseline and changes in Proteobacteria (adjusted p < 0.05) were inversely associated with changes in HEI. No statistically significant associations were found for Bacteroidota or Actinobacteriota after adjustment.
3.4.3. Diet Quality and Microbiome Genus (Table 7)
Several statistically significant associations were observed between HEI scores and the top 10 gut microbiota genera. Higher baseline HEI was negatively associated with baseline Blautia_A (β = −0.22, p = 0.03) and change in Blautia_A (β = −0.25, p = 0.03), as well as with change in Agathobacter (β = −0.22, p = 0.03). Higher change in HEI was also negatively associated with change in Agathobacter (β = −0.28, p = 0.01; adjusted β = −0.24, p = 0.03). Conversely, higher baseline HEI was positively associated with baseline Bifidobacterium (β = +0.19, p = 0.03) and baseline Faecalibacterium (β = +0.31, p = 0.01; adjusted β = +0.26, p = 0.03), while HEI changes were positively associated with changes in Faecalibacterium (β = +0.38, p < 0.01; adjusted β = +0.33, p = 0.01). HEI changes were also positively associated with changes in Parabacteroides (β = +0.26, p = 0.03). Higher baseline HEI was negatively associated with change in Streptococcus (β = −0.25, p = 0.01; adjusted β = −0.21, p = 0.04), and HEI changes were similarly negatively associated with change in Streptococcus (β = −0.30, p < 0.01; adjusted β = −0.26, p = 0.02). Both baseline and change in HEI were positively associated with change in Alistipes (baseline β = +0.35, p < 0.01; adjusted β = +0.31, p < 0.01; change β = +0.42, p < 0.01; adjusted β = +0.37, p < 0.01). The HEI changes were negatively associated with changes in Mediterraneibacter (β = −0.23, p = 0.04). Baseline microbiome genus levels were not associated with changes in HEI.
4. Discussion
The current pilot study is the first to longitudinally examine diet quality and fecal microbiome profiles over time in patients with colon cancer who are undergoing 5-FU-based chemotherapy regimens. The primary objective was to describe and characterize alterations in fecal microbial diversity and taxonomic distribution at both the phylum and genus levels, and their potential correlations with baseline and changes in diet quality, as assessed by the HEI. We found that significant changes in dietary patterns (worsening diet quality) and relationships with the microbiome (lower Shannon diversity) occurred during chemotherapy. This suggested that chemotherapy played a role in decreasing adherence to the recommended dietary guidelines (e.g., a plant-forward diet emphasizing fruits, vegetables, whole grains, and legumes, while limiting red and processed meats, added sugars, and ultra-processed foods), and loss of microbial richness and evenness, which has been coupled with compromised gut health, with elevated risk of gastrointestinal and systemic complications [30,31,32]. Significant microbiome composition changes were observed at the phylum and genus levels in our study. Such shifts were associated with fluctuations in beneficial taxa, such as butyrate-producing bacteria, as well as increases in potentially pathogenic or pro-inflammatory species [33], highlighting the complex and multi-directional nature of the host microbiome interactions that occur during the treatment. Relationships between HEI scores and measures of the microbiome also suggest that the quality of the diet is deeply connected with the health of the gut microbiome. The baseline diet quality and the levels of change in HEI scores over time were correlated with variations in the microbial diversity and shifts in composition, therefore, implying that patients who maintained good diet plans may have been somewhat protected against microbiome disturbances [34,35]. Our findings shed light on chemotherapy’s impact on gut microbial ecology and eating behaviors, pointing to opportunities for supportive interventions, such as microbiome-focused therapies and nutrition strategies, to help reduce treatment-related adverse effects in colon cancer patients [36,37,38].
4.1. Diet Changes
Our findings show a clear decline in HEI scores after chemotherapy begins, indicating reduced diet quality among colon cancer patients. Declines were evident not only in the overall dietary quality score but also in key components, fruits, vegetables, and whole grains, with some participants shifting toward refined foods and lower fiber and protein intake. These patterns are in line with the nutritional issues reported among oncology patients in previous literature. [39,40,41,42,43]; where diet quality commonly worsens during treatment due to physiological, psychological, and practical barriers during cancer treatments [41,42,43]. Gastrointestinal distress in patients with colon cancer is common and severe [41], including nausea, vomiting, mucositis, indigestion, diarrhea, and abdominal pain, limiting intake of nutrient-dense foods [41,42,43]. Fatigue and physical weakness further reduce the capacity to prepare balanced meals, leading many patients to rely on unhealthy processed foods [11,47]. Emotional distress may increase preference for energy-dense comfort foods [48,49], while financial strain related to cancer treatments can restrict access to fresh, high-quality options [50,51].
4.2. Microbiome Diversity (Shannon Index)
The Shannon index showed a significant reduction in alpha diversity after chemotherapy [52,53,54,55]. These findings are consistent with prior studies reporting chemotherapy-related dysbiosis and reduced alpha diversity in oncology populations [55,56,57,58,59,60], including breast cancer [58], hematopoietic stem cell transplant recipients [59] and pediatric cancer patients [60]. Mechanistically, cytotoxic therapy can damage the intestinal barrier, alter genomic integrity, and reduce ecological niches for commensal microbes [61,62,63]. Reduced diversity is linked to impaired barrier integrity, increased permeability, oxidative stress, DNA damage, and inflammation [61,62], contributing to infection risk, poor nutritional status, and delayed recovery. Evidence suggests that targeted interventions, including selective probiotics, optimized antibiotic strategies, dietary support, and other microbiome-directed therapies, may help restore diversity [64,65].
4.3. Microbiome Composition
In our study, at the phylum level, the gut microbiome was dominated by Firmicutes, Proteobacteria, Fornicata, and Verrucomicrobiota. Fornicata and Proteobacteria remained relatively stable pre- and post-treatment, suggesting resilience or rapid recovery [66]. Firmicutes increased and Verrucomicrobiota decreased, indicating shifts in community structure with potential functional implications, including reduced microbial balance and possible metabolic dysregulation [66,67,68]. Specifically, increased Firmicutes over time in our study reflects expansion of stress-tolerant and inflammation-associated taxa) [66,67,68]. Decreased Verrucomicrobiota indicates weakened mucosal barrier, impaired metabolic signaling, reduced anti-inflammatory activity, and increased susceptibility to dysbiosis [66,67,68,69]. In our study, we observed a mild increase in Faecalibacterium, a key butyrate-producing and anti-inflammatory genus [70]. In contrast, Prevotella and Roseburia (both important for fiber metabolism and SCFA production) declined [70]. These findings are consistent with prior evidence showing that chemotherapy commonly increases anti-inflammatory and reduces SCFA-associated bacteria taxa [70,71]. These treatment-related changes could be partially shaped by changes in diet, lifestyle, environmental supports, and antibiotic use during chemotherapy [70,71]. We also found that declines in fiber-utilizing taxa, and this may also reflect significantly reduced dietary fiber intake related to gastrointestinal distress, during cancer treatment in patients with colon cancer shown in our study as well as in others [72].
4.4. Associations Between Diet Quality (Measured as HEI) and Microbiome Profiles
Diet quality demonstrated a clear bidirectional relationship with the gut microbiome in this study. Reduced intake of fiber-rich plant foods limits fermentation substrates for beneficial bacteria, contributing to lower SCFA-producing taxa and diminished microbial richness [73,74,75]. Accordingly, declining HEI scores during chemotherapy appeared to drive decreases in Shannon diversity and losses of fiber-fermenting genera such as Roseburia and Prevotella [76,77]. At baseline, higher HEI scores were associated with greater alpha diversity and higher abundances of beneficial taxa, including SCFA-producing Firmicutes subgroups and Faecalibacterium, consistent with evidence that fiber-rich diets promote microbial diversity [76]. Importantly, better baseline HEI predicted smaller declines in diversity during chemotherapy, suggesting that high HEI confers microbial resilience [78,79]. A reverse pattern was also observed in our study (Table 6): participants with greater baseline microbial diversity tended to have higher baseline HEI scores and lesser worsening in HEI scores during treatment, aligning with evidence that a well-balanced microbiota supports nutrient absorption, vitamin synthesis, and reduced gastrointestinal side effects [80]. In contrast, declining HEI reflects nutritional deterioration that contributes to microbiome disruption, including reduced diversity and loss of fiber-fermenting taxa such as Roseburia and Prevotella in our study. Together, these findings support a diet–microbiome cross-talk model in which diet quality and microbial diversity mutually reinforce one another. Better baseline HEI fosters a more resilient microbial community as a protective factor, while greater microbial diversity helps sustain diet quality during treatment [81,82]. Clinically, these results underscore the importance of dietary counseling and microbiome-supportive strategies at the start of chemotherapy. Encouraging patients to maintain nutrient- and fiber-rich diets may help preserve microbial resilience, while targeted nutritional support during treatment may mitigate microbiome disruption and symptom burden [83,84,85]. Overall, our data support the hypothesis that diet quality and gut microbiome are interdependent throughout the chemotherapy experience.
4.5. Clinical Implications
The bidirectional relationship between diet quality and the gut microbiome highlights the need to integrate nutritional and microbial assessments into supportive oncology care. Because diet quality, particularly fiber intake, declined over time in our cohort in other study in breast cancer [58], and this reduction was mirrored by losses in fiber-fermenting taxa such as Roseburia and Prevotella in our study, assessing nutritional status and gut health before treatment may help identify patients at higher risk for microbiome disruption and treatment-related symptoms. Early nutritional rehabilitation, including counseling to increase fiber-rich foods and improve overall diet quality in compliance with the American Cancer Society nutritional guideline, may strengthen microbial resilience before chemotherapy begins. Given that higher baseline HEI was associated with smaller declines in microbial diversity (Table 6), nutritional interventions should be initiated prior to chemotherapy and continued throughout treatment. For patients unable to meet fiber or diet-quality targets through self-management, safe adjunctive microbiome-supportive options for cancer patients with immunodeficiency, such as probiotics, prebiotics, symbiotics, or other evidence-based formulations, may help preserve beneficial taxa and mitigate dysbiosis associated with reduced fiber intake during chemotherapy. Maintaining diet quality, especially adequate fiber consumption, during chemotherapy is essential for reducing microbiome disruption, supporting gastrointestinal function, and improving symptom management. When feasible, fecal microbiome monitoring may help detect early microbial shifts linked to toxicity and guide timely intervention [58].. Overall, integrating nutritional assessment, individualized dietary counseling, and microbiome-directed strategies into routine cancer care may enhance functional resilience, reduce treatment side effects, and improve patients’ ability to tolerate and complete chemotherapy.
4.6. Strengths and Limitations
The study shows several strengths, including its design, assessment, analysis, and statistical models. The longitudinal design within the cancer and chemotherapy background allowed for observation of changes in both the diet quality and composition of the gut microbiome throughout the whole process. Then, the integration of dietary assessments through the HEI scores with the profiling of microbiome levels provided a whole perspective of the patient’s gastrointestinal health. This analysis was not restricted, but extended to both phylum and genus levels to identify specific taxa that may lead to protective effects or draw negative results.
However, some important limitations need to be acknowledged. Such constraints include the small size of the sample, which reduces the statistical power and the generalizability of study findings. Since the efforts were made to control for major variables, some confounding ones, like the use of antibiotics that were not listed, concurrent medication and changes in them, and other co-morbidities, such as depression, cannot be ruled out. Lastly, the analysis of the microbiome was limited to 16S rRNA sequencing, which excludes functional and metabolomics characterization, thereby restricting the findings and discussions. Furthermore, the dietary intake was self-reported, which might lead to the possibility of recall bias and misclassification.
5. Conclusions
Our pilot study shows that chemotherapy for colon cancer leads to parallel declines in diet quality and gut microbial health, marked by reduced HEI scores, lower microbial diversity, and losses of key fiber-fermenting and SCFA-producing taxa. Higher baseline diet quality and microbial diversity appeared protective, supporting a bidirectional diet–microbiome relationship throughout treatment. These findings suggest that early nutritional support and microbiome-focused strategies may help preserve gut resilience and reduce treatment-related disruptions. Larger studies are needed to validate these results and inform targeted dietary and microbiome-based interventions in oncology care.
Author Contributions
Conceptualization, CH, DS, DV, AN, and LP.; methodology, CH, DS, DV, and LP; validation, CH, DS, and LP; formal analysis, CH in collaboration with OSU biostatistics and Microbiome Service Center; investigation, CH; resources, CH, DS, DV, AN, and LP; data curation, CH, DS; writing—original draft preparation, CH; writing—review and editing, CH, DS, DV, AN, and LP.; supervision, CH; project administration, CH; funding acquisition, CH, DS, DV, AN, and LP. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Oncology Nursing Foundation RE03.
Acknowledgments
This manuscript incorporates analytic support from the OSU Biostatistics Consulting Service and microbiome data processing, profiling, analytic methodology, and consultation provided by the OSU Center of Microbiome Science (COMS).
Institutional Review Board Statement
All study procedures involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments. The study was approved by the Institutional Review Board (or Ethics Committee) of the Ohio State University IRB2024C0007 on 6/21/2024 for studies involving humans.
Informed Consent Statement
Written informed consent was obtained from all participants prior to enrollment. Participants were informed about the study purpose, procedures, potential risks and benefits, confidentiality protections, and their right to withdraw at any time without penalty. Only individuals who provided voluntary, written consent were included in the study.
Data Availability Statement
The data generated and analyzed during this study are not publicly available due to institutional policies and participant privacy protections, but de-identified aggregated data are available from the corresponding author upon reasonable request. Additional materials, including analytic code and study protocols, may also be shared upon request, contingent on appropriate data use agreements.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
5-FU – 5-fluorouracil
16S rRNA – 16S ribosomal ribonucleic acid
BMI – body mass index
CI – confidence interval
DNA – deoxyribonucleic acid
FOLFIRI – folinic acid, fluorouracil, and irinotecan
FOLFOX – folinic acid, fluorouracil, and oxaliplatin
GI – gastrointestinal
HEI – Healthy Eating Index
HIV – human immunodeficiency virus
HRQOL – health-related quality of life
IQR – interquartile range
IRB – Institutional Review Board
OSU BSSR – Ohio State University Biospecimen Services Shared Resource
QIIME 2 – Quantitative Insights Into Microbial Ecology 2
REDCap – Research Electronic Data Capture
SCFA(s) – short-chain fatty acid(s)
SD – standard deviation
SF-FFQ – Short Form Food Frequency Questionnaire
US – United States
References
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10–45. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.; Arnold, M.; Gini, A.; et al. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Siegel, R.L.; Laversanne, M.; et al. Colorectal cancer incidence trends in younger versus older adults. Lancet Oncol. 2025, 26, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Spaander, M.C.W.; Zauber, A.G.; Syngal, S.; et al. Young-onset colorectal cancer. Nat. Rev. Dis. Primers 2023, 9, 21. [Google Scholar] [CrossRef]
- Pu, W.; et al. A novel approach in colon cancer treatment using endoscopic rendezvous technique. Photodiagn. Photodyn. Ther. 2025, 104761. [Google Scholar] [CrossRef]
- Balderas-Peña, L.M.; et al. Body composition and nutritional status in colorectal cancer. Nutrients 2020, 12, 2110. [Google Scholar] [CrossRef]
- Gebremedhin, T.K.; et al. Malnutrition among adult cancer patients receiving chemotherapy. Heliyon 2021, 7, e07362. [Google Scholar] [CrossRef]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. ACS nutrition and physical activity guideline for cancer survivors. CA Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef]
- Xue, M.; et al. Fasting-mimicking diet in breast cancer patients receiving chemotherapy. Breast Cancer Res. Treat. 2025. [CrossRef]
- Crowder, S.L.; et al. Diet quality indices and cognition during chemotherapy. Support. Care Cancer 2022, 31, 75. [Google Scholar] [CrossRef]
- Kleckner, A.S.; et al. Mediterranean diet intervention and cancer-related fatigue. Cancers 2022, 14, 4202. [Google Scholar] [CrossRef]
- Lazar, D.C.; et al. Gastric cancer and microbiota. Life 2025, 15, 999. [Google Scholar] [CrossRef] [PubMed]
- Yan, R.; et al. Gut microbiome dysbiosis in colorectal cancer. J. Med. Microbiol. 2025, 74, 002042. [Google Scholar] [CrossRef] [PubMed]
- Asseri, A.H.; et al. Gut dysbiosis–cancer axis. Front. Pharmacol. 2023, 14, 1208044. [Google Scholar] [CrossRef]
- Artym, J.; Zimecki, M. Colostrum proteins in therapy-induced injuries. Biomedicines 2023, 11, 114. [Google Scholar] [CrossRef]
- Montassier, E.; et al. Chemotherapy-driven dysbiosis. Aliment. Pharmacol. Ther. 2015, 42, 515–528. [Google Scholar] [CrossRef]
- Goubet, A.G.; et al. Intestinal microbiota and therapeutic responses. C. R. Biol. 2018, 341, 284–289. [Google Scholar] [CrossRef]
- Zmora, N.; Suez, J.; Elinav, E. Diet and the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 35–56. [Google Scholar] [CrossRef]
- Carding, S.; Verbeke, K.; Vipond, D.T.; Corfe, B.M.; Owen, L.J. Dysbiosis of the gut microbiota. Microb. Ecol. Health Dis. 2015, 26, 26191. [Google Scholar] [CrossRef]
- Zhang, P. Influence of foods on the gut microbiome. Int. J. Mol. Sci. 2022, 23, 9588. [Google Scholar] [CrossRef]
- Aarnoutse, R.; et al. Changes in intestinal microbiota in postmenopausal oestrogen receptor-positive breast cancer patients treated with (neo)adjuvant chemotherapy. NPJ Breast Cancer 2022, 8, 89. [Google Scholar] [CrossRef]
- Maddern, A.S.; et al. The association between the gut microbiome and development and progression of cancer treatment adverse effects. Cancers 2023, 15, 4361. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.L.; et al. Prediction models for severe treatment-related toxicities in older adults with cancer: A systematic review. Age Ageing 2025, 54, afaf070. [Google Scholar] [CrossRef] [PubMed]
- Carson, T.L.; et al. Association between the gut microbiota and colorectal cancer. Gut Pathog. 2024, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- He, T.; Cheng, X.; Xing, C. Gut microbial diversity of colon cancer patients. Bioengineered 2021, 12, 7046–7060. [Google Scholar] [CrossRef]
- Colombo, F.; Illescas, O.; Noci, S.; et al. Gut microbiota composition in colorectal cancer patients. Sci. Rep. 2022, 12, 11424. [Google Scholar] [CrossRef]
- Hosein, K.; et al. Short-form food frequency questionnaire vs. 3-day food intake record. Br. J. Nutr. 2025, 1–17. [Google Scholar] [CrossRef]
- Jubayer, A.; et al. Evaluation of Bangladesh Healthy Eating Index (BD-HEI). BMC Nutr. 2025, 11, 159. [Google Scholar] [CrossRef]
- Nutritional Pro. Version 2025; Healthy Living Software Inc.: Chicago, IL, USA, 2024. DOI not available.
- Baughman, C.; Norman, K.; Mukamal, K. Adherence to ACS nutrition and physical activity guidelines. JAMA Oncol. 2024, 10, 789–792. [Google Scholar] [CrossRef]
- Galloway-Peña, J.R.; et al. Gut microbiome signatures predict infectious risk in AML. Clin. Infect. Dis. 2020, 71, 63–71. [Google Scholar] [CrossRef]
- Rashidi, A.; et al. Gut microbiota changes and neutropenic fever. Leukemia 2020, 34, 312–316. [Google Scholar] [CrossRef]
- Al-Rashidi, H.E. Gut microbiota and immunity. Saudi J. Biol. Sci. 2022, 29, 1628–1643. [Google Scholar] [CrossRef] [PubMed]
- Anhê, F.F.; et al. Polyphenol-rich cranberry extract and Akkermansia. Gut 2015, 64, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Hills, R.D., Jr.; et al. Gut microbiome implications for diet and disease. Nutrients 2019, 11, 1613. [Google Scholar] [CrossRef] [PubMed]
- Montassier, E.; et al. Chemotherapy-induced fecal microbiota shifts. Microb. Ecol. 2014, 67, 690–699. [Google Scholar] [CrossRef]
- Kuugbee, E.D.; et al. Probiotic cocktail enhances gut barrier and reduces cancer. Dig. Dis. Sci. 2016, 61, 2908–2920. [Google Scholar] [CrossRef]
- Kober, M.M.; Bowe, W.P. Probiotics and immune regulation. Int. J. Womens Dermatol. 2015, 1, 85–89. [Google Scholar] [CrossRef]
- Rock, C.L.; et al. ACS guideline for diet and physical activity for cancer prevention. CA Cancer J. Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef]
- Guinter, M.A.; et al. Diet quality and mortality after colorectal cancer. J. Clin. Oncol. 2018, 36, JCO1800714. [Google Scholar] [CrossRef]
- Han, C.J.; Reding, K.W.; Kalady, M.F.; Yung, R.; Greenlee, H.; Paskett, E.D. GI symptoms in CRC survivors. PLoS ONE 2023, 18, e0286058. [Google Scholar] [CrossRef]
- Vandebroek, A.J.V.; Schrijvers, D. Nutritional issues in anticancer treatment. Ann. Oncol. 2008, 19, v52–v55. [Google Scholar] [CrossRef]
- Ravasco, P. Nutrition in cancer patients. J. Clin. Med. 2019, 8, 1211. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, S.; Takeda, H. Herbal medicines for chemotherapy side effects. Front. Pharmacol. 2015, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Kurt, B.; Oksuzoglu, B.O.C. Taste alterations during cisplatin therapy. Cancer Control 2025, 32, 10732748251363323. [Google Scholar] [CrossRef] [PubMed]
- Cok, O.Y.; et al. Paracetamol and postoperative nausea. Eur. J. Anaesthesiol. 2011, 28, 836–841. [Google Scholar] [CrossRef]
- Thomas, N.S.; et al. Depression, anxiety, fibromyalgia, and ME/CFS. Psychol. Med. 2025, 55, e232. [Google Scholar] [CrossRef]
- Bergerot, C.D.; et al. Distress and emotional support needs in stage IV cancer. Psychooncology 2025, 34, e70232. [Google Scholar] [CrossRef]
- Hasan, N.; et al. Dietary sugars and cancer risk. Cancer Treat. Res. Commun. 2025, 43, 100876. [Google Scholar] [CrossRef]
- Pellegrini, C.A.; et al. Healthy eating habits during COVID-19. Health Psychol. Behav. Med. 2023, 11, 2182307. [Google Scholar] [CrossRef]
- White, E. Bad eating habits of Ras-driven cancers. Genes Dev. 2013, 27, 2065–2071. [Google Scholar] [CrossRef]
- Roca-Saavedra, P.; et al. Food additives and gut microbiota. J. Physiol. Biochem. 2018, 74, 69–83. [Google Scholar] [CrossRef]
- Jiang, Y.; Li, Y. Nutrition intervention and microbiome modulation. Nutrients 2024, 16, 2621. [Google Scholar] [CrossRef] [PubMed]
- Salberg, S.; et al. Sex differences in gut microbiome and nociception. Dev. Neurobiol. 2023, 83, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Mitra, A.; et al. Microbial diversity and toxicity during chemoradiation. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Bohm, D.; et al. Gut microbiota and chemotherapy response. NPJ Precis. Oncol. 2025, 9, 265. [Google Scholar] [CrossRef]
- Yu, Z.K.; et al. Bacterial microbiome in cancer treatment. BMC Cancer 2021, 21, 934. [Google Scholar] [CrossRef]
- Otto-Dobos, L.D.; et al. Alpha diversity predicts GI symptoms. NPJ Breast Cancer 2024, 10, 99. [Google Scholar] [CrossRef]
- Rajagopala, S.V.; et al. Persistent dysbiosis in childhood ALL. Microb. Ecol. 2020, 79, 1034–1043. [Google Scholar] [CrossRef]
- Bai, J.; Behera, M.; Bruner, D.W. Gut microbiome and symptoms in pediatric cancer. Support. Care Cancer 2018, 26, 427–439. [Google Scholar]
- Di Vincenzo, F.; et al. Gut microbiota and systemic inflammation. Intern. Emerg. Med. 2024, 19, 275–293. [Google Scholar] [CrossRef]
- Ribatti, D. Comment on gut microbiota and inflammation. Intern. Emerg. Med. 2024, 19, 1515–1516. [Google Scholar] [CrossRef]
- Oh, B.; et al. Gut microbiome in chemotherapy. Front. Oncol. 2021, 11, 706331. [Google Scholar] [CrossRef] [PubMed]
- Prisciandaro, L.D.; et al. Probiotics for intestinal mucositis. Crit. Rev. Food Sci. Nutr. 2011, 51, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; et al. Postoperative probiotics in CRC. Nutrients 2023, 15, 356. [Google Scholar] [CrossRef]
- Kennedy, M.S.; Chang, E.B. Microbiome composition and locations. Prog. Mol. Biol. Transl. Sci. 2020, 176, 1–42. [Google Scholar] [CrossRef]
- Manor, O.; et al. Health and disease markers and gut microbiome. Nat. Commun. 2020, 11, 5206. [Google Scholar] [CrossRef]
- Ruan, W.; et al. Healthy human gastrointestinal microbiome. Dig. Dis. Sci. 2020, 65, 695–705. [Google Scholar] [CrossRef]
- Oliphant, K.; et al. Early-life microbiome and neurodevelopment. Gut Microbes 2021, 13, 1997560. [Google Scholar] [CrossRef]
- Portincasa, P.; et al. Gut microbiota and short-chain fatty acids. Int. J. Mol. Sci. 2022, 23, 1105. [Google Scholar] [CrossRef]
- Otto-Dobos, L.D.; et al. Chemotherapy-induced microbiome disruption and cognition. Brain Behav. Immun. 2024, 120, 208–220. [Google Scholar] [CrossRef]
- Song, M.; et al. Fiber intake and CRC survival. JAMA Oncol. 2018, 4, 71–79. [Google Scholar] [CrossRef]
- Wu, G.D.; et al. Dietary patterns and gut enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; et al. Gut microbiota and SCFAs in osteoporosis. Medicine (Baltimore) 2024, 103, e40554. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; et al. Short-chain fatty acids as antiviral mediators. Front. Immunol. 2025, 16, 1614879. [Google Scholar] [CrossRef] [PubMed]
- David, L.A.; et al. Diet rapidly alters the gut microbiome. Nature 2014, 505, 559–563. [Google Scholar] [CrossRef]
- Huang, F.; et al. Probiotics and chemotherapy-related GI complications. Nutrients 2023, 15, 356. [Google Scholar] [CrossRef]
- Shastry, R.P.; Rekha, P.D. Bacterial cross-talk with gut microbiome. Folia Microbiol. 2021, 66, 15–24. [Google Scholar] [CrossRef]
- Del Chierico, F.; et al. Mediterranean diet and gut microbiota. Int. J. Mol. Sci. 2014, 15, 11678–11699. [Google Scholar] [CrossRef]
- Bielik, V.; Kolisek, M. Minerals and gut microbiome. Int. J. Mol. Sci. 2021, 22, 6803. [Google Scholar] [CrossRef]
- Frame, L.A.; Costa, E.; Jackson, S.A. Nutrition and gut microbiome: Review of reviews. Nutr. Rev. 2020, 78, 798–812. [Google Scholar] [CrossRef]
- Velly, H.; Britton, R.A.; Preidis, G.A. Diet–microbiome–host cross-talk. Gut Microbes 2017, 8, 98–112. [Google Scholar] [CrossRef]
- Wiertsema, S.P.; et al. Gut microbiome and immune system interplay. Nutrients 2021, 13, 886. [Google Scholar] [CrossRef]
- Ross, F.C.; et al. Diet–gut microbiome interactions. Nat. Rev. Microbiol. 2024, 22, 671–686. [Google Scholar] [CrossRef]
- Zhang, P. Influence of foods and nutrition on gut microbiome. Int. J. Mol. Sci. 2022, 23, 9588. [Google Scholar] [CrossRef]
Figure 1.
Box Plot Of Shannon Diversity (Pre-Post Chemotherapy).
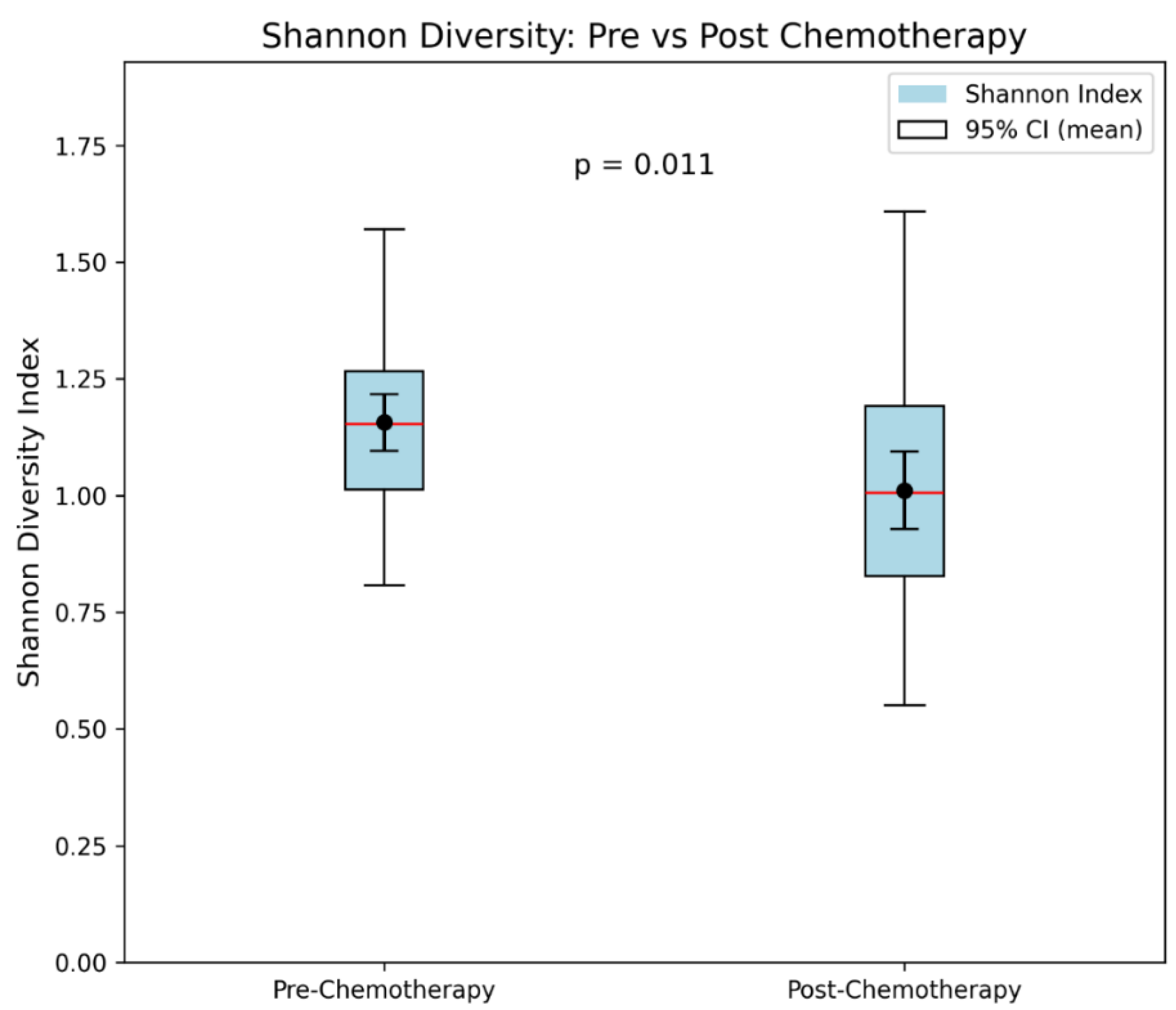
Figure 2.
Volcano Plot: Relative abundances of microbiota phyla pre- and post-chemotherapy. Points represent pre- to post-chemotherapy changes (Δ Post–Pre) and −log10 p-values from paired Wilcoxon tests. Red and blue points denote significant increases and decreases, respectively, while black points indicate non-significant changes. The dashed line marks p = 0.05.
Figure 2.
Volcano Plot: Relative abundances of microbiota phyla pre- and post-chemotherapy. Points represent pre- to post-chemotherapy changes (Δ Post–Pre) and −log10 p-values from paired Wilcoxon tests. Red and blue points denote significant increases and decreases, respectively, while black points indicate non-significant changes. The dashed line marks p = 0.05.
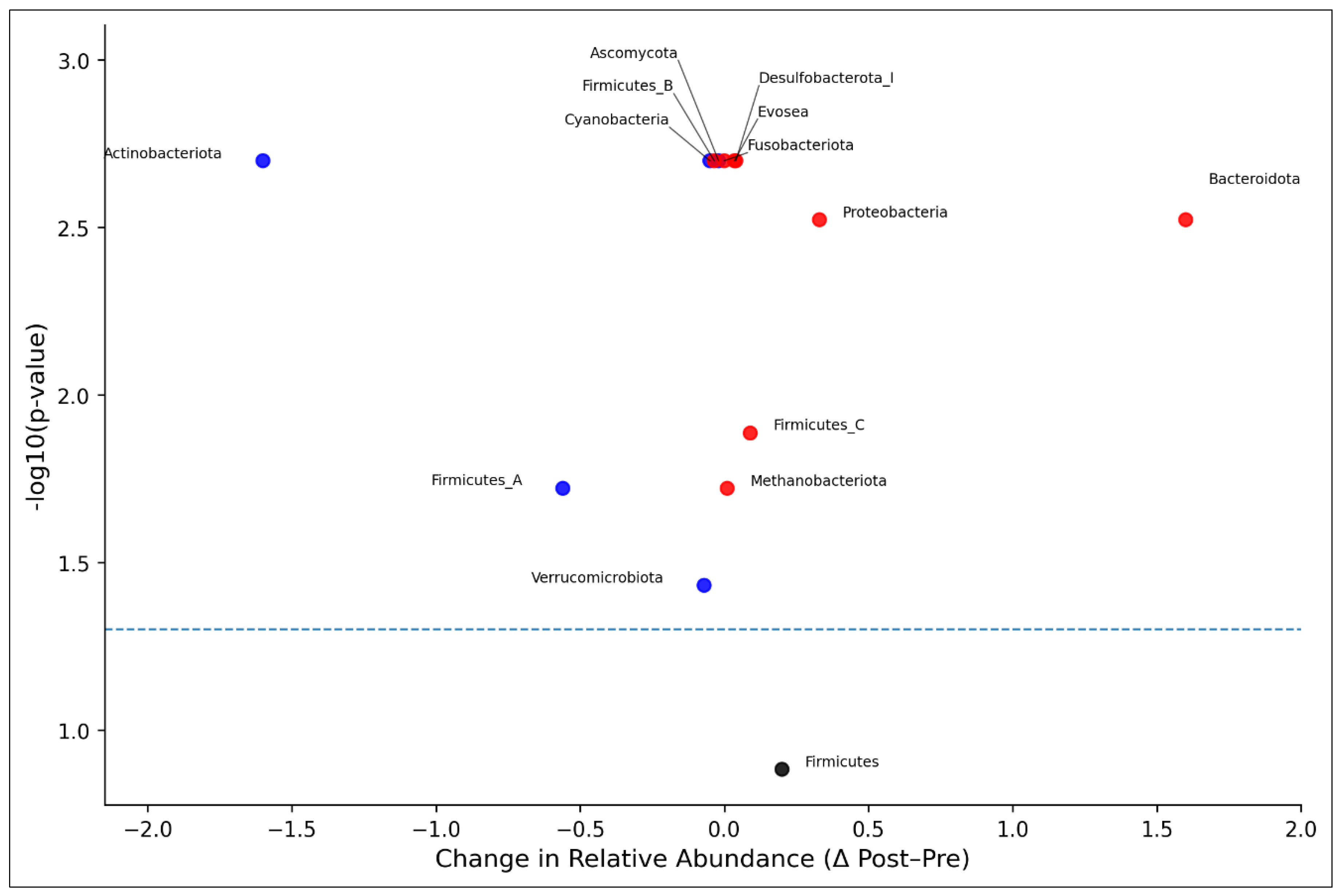
Figure 3.
Volcano Plot: Relative abundances of microbiota genus, pre- and post-chemotherapy. Points represent pre- to post-chemotherapy changes (Δ Post–Pre) and −log10 p-values from paired Wilcoxon tests. Red and blue points denote significant increases and decreases, respectively, while black points indicate non-significant changes. The dashed line marks p = 0.05.
Figure 3.
Volcano Plot: Relative abundances of microbiota genus, pre- and post-chemotherapy. Points represent pre- to post-chemotherapy changes (Δ Post–Pre) and −log10 p-values from paired Wilcoxon tests. Red and blue points denote significant increases and decreases, respectively, while black points indicate non-significant changes. The dashed line marks p = 0.05.
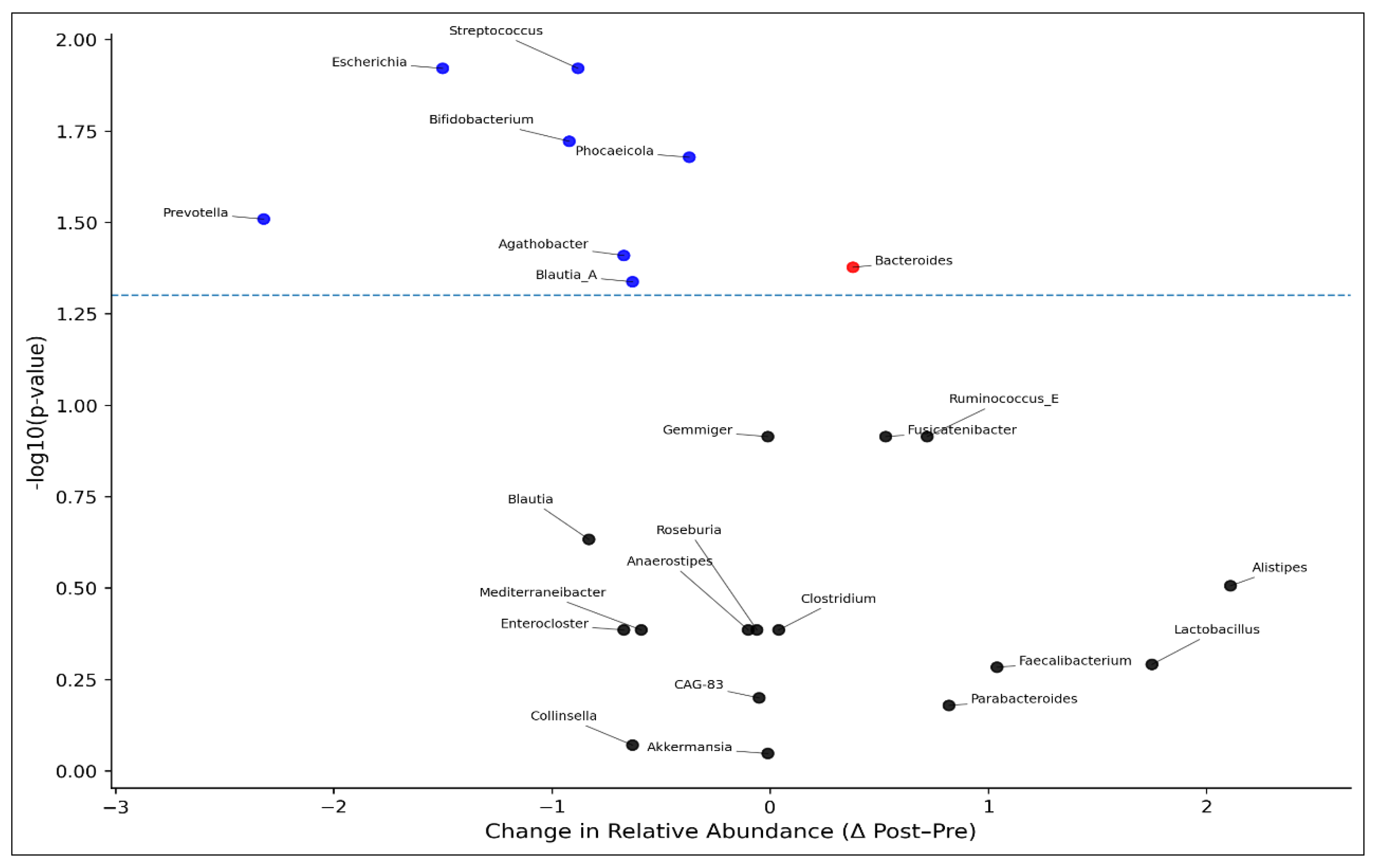

Table 1.
Sociodemographic and Clinical Characteristics of the Study Sample (N = 48).
| Characteristic | n (%) or Mean ± Standard Deviation (SD) [Range] |
| Demographic Characteristics | |
| Age (years) | 69.4 ± 6.7 [59–86] |
| Sex | |
| Male | 26 (54.2%) |
| Female | 22 (45.8%) |
| Marital Status | |
| Married | 28 (58.3%) |
| Single | 20 (41.7%) |
| Body Mass Index | 29.4 ± 3.2 [22.1-44.6] |
| Employment Status | |
| Employed | 13 (27.1%) |
| Not Employed | 35 (72.9%) |
| Education Level | |
| High School or Less | 15 (31.3%) |
| Some College | 12 (25.0%) |
| Undergraduate Degree | 14 (29.2%) |
| Graduate Degree | 7 (14.6%) |
| Race | |
| Black/White | 24 (50.0%)/ 24(50.0%) |
| Insurance Type | |
| Private | 18 (37.5%) |
| Public | 28 (58.3%) |
| None | 2 (4.2%) |
| Smoking Status | |
| Never Smoker | 30 (62.5%) |
| Former Smoker | 13 (27.1%) |
| Current Smoker | 5 (10.4%) |
| Income Levels | |
| Low income (<$35,000/year) | 16 (33.3%) |
| Middle income ($35,000–$74,999/year) | 18 (37.5%) |
| High income (≥$75,000/year) | 14 (29.2%) |
| Alcohol Use | |
| Yes/No | 9 (18.8%)/ 39(81.2%) |
| Healthy Diet Adherence | |
| Yes/No | 19 (39.6%)/ 29 (60.4%) |
| Routine Physical Activity | |
| Yes | 17 (35.4%) |
| No | 31 (64.6%) |
| Clinical Characteristics | |
| Colon Cancer Stage | |
| Stage II | 11 (23.1%) |
| Stage III | 37 (76.9%) |
| Years Since Diagnosis | 0.8 ± 0.9 [0.3–4.0] |
| Chemotherapy Regimen | |
| FOLFOX (Folinic acid, Fluorouracil, and Oxaliplatin) | 24 (50.0%) |
| 5-FU (single agent) | 14 (29.2%) |
| FOLFIRI (Folinic acid, Fluorouracil, and Irinotecan) | 10 (20.8%) |
| History of Colon Surgery, Yes | 48 (100.0%) |
| History of Radiation | |
| Yes | 12 (25.0%) |
| No | 36 (75.0%) |
| Comorbidity Index (≥2) | 46 (95.4%) |
Table 2.
Nutritional Profiles Pre- and Post-Chemotherapy (Paired comparison of 3-day averages of diet recall, N = 48).
Table 2.
Nutritional Profiles Pre- and Post-Chemotherapy (Paired comparison of 3-day averages of diet recall, N = 48).
| Component | Pre-Chemo (Mean ± SD) | Post-Chemo (Mean ± SD) | Change (Post – Pre) |
% Change | P value |
|---|---|---|---|---|---|
| Macronutrients | |||||
| Total Calories (kcal) | 1925 ± 420 | 1680 ± 390 | –245 | –12.7% | 0.012 |
| Protein (g) | 72.3 ± 15.8 | 64.7 ± 14.2 | –7.6 | –10.5% | 0.021 |
| Carbohydrates (g) | 230.5 ± 50.3 | 205.8 ± 48.1 | –24.7 | –10.7% | 0.033 |
| Total Fat (g) | 78.9 ± 16.7 | 69.1 ± 15.2 | –9.8 | –12.4% | 0.018 |
| Fiber (g) | 21.6 ± 5.4 | 17.9 ± 4.8 | –3.7 | –17.1% | 0.009 |
| Micronutrients | |||||
| Vitamin D (IU) | 310 ± 140 | 245 ± 115 | –65 | –21.0% | 0.041 |
| Calcium (mg) | 925 ± 210 | 812 ± 185 | –113 | –12.2% | 0.027 |
| Folate (mcg) | 380 ± 96 | 345 ± 84 | –35 | –9.2% | 0.085 |
| Iron (mg) | 13.5 ± 3.2 | 11.9 ± 2.9 | –1.6 | –11.9% | 0.034 |
| Sodium (mg) | 2300 ± 460 | 2285 ± 450 | –15 | –0.7% | 0.770 |
| Water Intake (ml) | 1400 ± 310 | 1250 ± 285 | –150 | –10.7% | 0.045 |
| Dietary Intake (Food Groups / Serving per day) | |||||
| Added Sugar (g) | 45.6 ± 14.9 | 38.2 ± 13.2 | –7.4 | –16.2% | 0.026 |
| Red Meat (servings/day) | 1.1 ± 0.5 | 0.9 ± 0.4 | –0.2 | –18.2% | 0.048 |
| Fruit & Vegetable (serving/day) | 3.4 ± 1.2 | 2.5 ± 1.0 | –0.9 | –26.5% | 0.004 |
| Whole Grains (servings/day) | 2.6 ± 1.1 | 2.0 ± 0.9 | –0.6 | –23.1% | 0.007 |
|
HEI score (0-100), the higher the score, the better the diet quality |
62.4 ± 8.5 | 54.2 ± 9.3 | -8.2 | -13.1% | 0.015 |
Note. A Wilcoxon signed-rank test was conducted to compare the nutritional profiles between pre- and post-treatment. A p-value of < .05 was considered statistically significant.
Table 3.
Alpha Diversity Index Pre- and Post-Chemotherapy (Shannon Diversity, Paired comparison, N = 48).
Table 3.
Alpha Diversity Index Pre- and Post-Chemotherapy (Shannon Diversity, Paired comparison, N = 48).
| Metric. | Pre-Chemotherapy | Post-Chemotherapy | p-value |
|---|---|---|---|
| Mean ± SD | 1.20 ± 0.20 | 1.05 ± 0.21 | 0.011 for mean values |
| Median [IQR] | 1.19 [1.05, 1.34] | 1.03 [0.88, 1.20] | |
| 95% CI (mean) | [1.13, 1.27] | [0.97, 1.13] |
Note. A Wilcoxon signed-rank test was conducted to compare the Shannon diversity between pre- and post-treatment. A p-value of < .05 was considered statistically significant.
Table 4.
Relative Abundance of Microbiome Phylum Pre- and Post-Chemotherapy (Paired comparison, N = 48).
Table 4.
Relative Abundance of Microbiome Phylum Pre- and Post-Chemotherapy (Paired comparison, N = 48).
| Phylum | Pre | Post | Δ (Post–Pre) | % Change | Wilcoxon W | p-value |
| Firmicutes_A | 51.19 | 50.63 | -0.56 | -1.1% | 1 | 0.019 |
| Bacteroidota | 29.08 | 30.68 | 1.6 | 5.5% | 1.0 | 0.003 |
| Firmicutes | 6.14 | 6.34 | 0.2 | 3.2% | 12.0 | 0.131 |
| Actinobacteriota | 6.71 | 5.11 | -1.6 | -23.8% | 0.0 | 0.002 |
| Proteobacteria | 3.62 | 3.95 | 0.33 | 9.1% | 1.0 | 0.003 |
| Firmicutes_C | 1.35 | 1.44 | 0.09 | 6.6% | 4.0 | 0.013 |
| Verrucomicrobiota | 1.19 | 1.12 | -0.07 | -5.8% | 7.0 | 0.037 |
| Methanobacteriota | 0.26 | 0.27 | 0.01 | 3.8% | 5.0 | 0.019 |
| Desulfobacterota_I | 0.20 | 0.24 | 0.04 | 20% | 0.0 | 0.002 |
| Cyanobacteria | 0.15 | 0.10 | -0.05 | -33.3% | 0.0 | 0.002 |
| Ascomycota | 0.04 | 0.02 | -0.02 | -50% | 0.0 | 0.002 |
| Firmicutes_B | 0.02 | 0.02 | 0 | 0% | 0.0 | 0.002 |
| Fusobacteriota | 0.01 | 0.01 | 0 | 0% | 0.0 | 0.002 |
| Evosea | 0.01 | 0.01 | 0 | 0% | 0.0 | 0.002 |
Note. A Wilcoxon signed-rank test was conducted to compare the total relative abundance of the top 14 most prevalent phyla between pre- and post-treatment. A p-value of < .05 was considered statistically significant.
Table 5.
Relative Abundance of Microbiome Genus Pre- and Post-Chemotherapy (Paired comparison, N = 48).
Table 5.
Relative Abundance of Microbiome Genus Pre- and Post-Chemotherapy (Paired comparison, N = 48).
| Genus | Pre-Mean | Post Mean | Δ (Post–Pre) | % Change | Wilcoxon W | p-value |
| Bacteroides | 20.67 | 21.05 | +0.38 | +1.8% | 120 | 0.042 |
| Blautia_A | 12.94 | 12.31 | -0.63 | -4.8% | 109 | 0.046 |
| Phocaeicola | 9.62 | 9.26 | -0.37 | -3.8% | 110 | 0.021 |
| Agathobacter | 6.06 | 5.40 | -0.67 | -11.0% | 110 | 0.039 |
| Bifidobacterium | 5.55 | 4.64 | -0.92 | -16.5% | 130 | 0.019 |
| Faecalibacterium | 3.46 | 4.50 | +1.04 | +30.0% | 65 | 0.521 |
| Parabacteroides | 3.13 | 3.95 | +0.82 | +26.1% | 40 | 0.663 |
| Streptococcus | 3.95 | 3.07 | -0.88 | -22.2% | 135 | 0.012 |
| Alistipes | 2.19 | 4.30 | +2.11 | +96.5% | 138 | 0.312 |
| Mediterraneibacter | 3.41 | 2.81 | -0.59 | -17.2% | 55 | 0.412 |
| Prevotella | 4.00 | 1.68 | -2.32 | -58.0% | 125 | 0.031 |
| Enterocloster | 3.17 | 2.51 | -0.67 | -21.1% | 60 | 0.412 |
| Collinsella | 2.78 | 2.15 | -0.63 | -22.6% | 35 | 0.851 |
| Ruminococcus_E | 2.10 | 2.82 | +0.72 | +34.3% | 90 | 0.122 |
| Fusicatenibacter | 1.93 | 2.46 | +0.53 | +27.6% | 88 | 0.122 |
| Clostridium | 2.01 | 2.06 | +0.04 | +2.1% | 60 | 0.412 |
| Gemmiger | 1.82 | 1.82 | -0.01 | -0.2% | 90 | 0.122 |
| Roseburia | 1.71 | 1.65 | -0.06 | -3.5% | 60 | 0.412 |
| Akkermansia | 1.64 | 1.62 | -0.01 | -0.9% | 30 | 0.897 |
| Escherichia | 2.37 | 0.87 | -1.50 | -63.3% | 140 | 0.012 |
| Anaerostipes | 1.66 | 1.56 | -0.10 | -5.9% | 60 | 0.412 |
| CAG-83 | 1.50 | 1.45 | -0.05 | -3.5% | 50 | 0.632 |
| Blautia | 1.82 | 0.99 | -0.83 | -45.7% | 70 | 0.233 |
| Lactobacillus | 0.47 | 2.21 | +1.75 | +374.8% | 75 | 0.512 |
Table 6.
Correlations Between Diet Quality (HEI) and Microbiome Profiles at Baseline and Changes (Diversity and Microbiome Phylum).
Table 6.
Correlations Between Diet Quality (HEI) and Microbiome Profiles at Baseline and Changes (Diversity and Microbiome Phylum).
| Diversity/ Phylum |
Outcomes | Input Variables | Unadjusted B (95% CI) | Unadjusted β (p) | Adjusted B (95% CI) |
Adjusted β (p) |
|---|---|---|---|---|---|---|
|
Shanno Diversity |
Baseline Shannon Diversity |
Baseline HEI | 0.23 (0.08,0.38) | +0.42(0.01) | 0.20(0.06,0.34) | +0.38(0.02) |
| Δ Shannon Diversity | Baseline HEI | 0.31 (0.15, 0.48) | +0.61(0.01) | 0.26 (0.09,0.43) | +0.49(0.01) | |
| Δ HEI | Baseline Shannon Diversity |
0.78 (0.07, 1.15) | +0.85(0.31) | 0.75 (0.03, 1.03) | +0.79(0.32) | |
| Δ HEI | Δ Shannon Diversity |
0.19 (0.07, 0.31) | +0.35(0.01) | 0.16 (0.03, 0.29) | +0.29(0.02) | |
| Firmicutes A | Baseline Firmicutes_A | Baseline HEI | 1.12 (0.03, 2.21) | +0.32(0.04) | 0.98 (0.02, 1.94) | +0.28(0.05) |
| Δ Firmicutes_A | Baseline HEI | 0.67(−0.40,1.75) | +0.18(0.21) | 0.81 (0.04, 1.58) | +0.22(0.04) | |
| Δ HEI | Baseline Firmicutes_A |
0.66(−0.10,1.42) | +0.27(0.09) | 0.58(−0.07,1.23) | +0.23(0.08) | |
| Δ HEI | Δ Firmicutes_A | 0.61(−0.18,1.40) | +0.22(0.13) | 0.55(−0.15,1.25) | +0.20(0.12) | |
| Bacteroidota | Baseline Bacteroidota | Baseline HEI | 0.88(−0.05,1.81) | +0.29(0.07) | 0.75(−0.12,1.62) | +0.25(0.09) |
| Δ Bacteroidota | Baseline HEI | 0.55(−0.47,1.56) | +0.14(0.29) | 0.60(−0.25,1.46) | +0.19(0.15) | |
| Δ HEI | Baseline Bacteroidota |
0.52(−0.20,1.24) | +0.21(0.15) | 0.45(−0.20,1.10) | +0.18(0.17) | |
| Δ HEI | Δ Bacteroidota | 0.48(−0.24,1.20) | +0.19(0.18) | 0.42(−0.22,1.06) | +0.17(0.19) | |
| Firmicutes | Baseline Firmicutes | Baseline HEI | 1.50 (0.30, 2.70) | +0.38(0.02) | 1.35 (0.15, 2.55) | +0.34(0.03) |
| Δ Firmicutes | Baseline HEI | 0.91(−0.27,2.08) | +0.22(0.13) | 1.02 (0.05, 1.99) | +0.24(0.04) | |
| Δ HEI | Baseline Firmicutes |
0.57(−0.11,1.25) | +0.24(0.10) | 0.50(−0.12,1.12) | +0.21(0.11) | |
| Δ HEI | Δ Firmicutes | 0.73 (0.01, 1.45) | +0.30(0.05) | 0.65 (0.01, 1.29) | +0.27(0.06) | |
| Actinobacteriota | Baseline Actinobacteriota | Baseline HEI | 0.49(−0.18,1.16) | +0.21(0.15) | 0.42(−0.23,1.07) | +0.18(0.20) |
| Δ Actinobacteriota | Baseline HEI | 0.27(−0.27,0.81) | +0.12(0.33) | 0.43(−0.06,0.91) | +0.17(0.09) | |
| Δ HEI | Baseline Actinobacteriota |
0.40(−0.25,1.06) | +0.16(0.23) | 0.35(−0.27,0.97) | +0.14(0.26) | |
| Δ HEI | Δ Actinobacteriota |
0.31(−0.32,0.94) | +0.12(0.33) | 0.25(−0.34,0.84) | +0.10(0.40) | |
| Proteobacteria | Baseline Proteobacteria | Baseline HEI | −1.11(−1.86,−0.36) | −0.40(0.01) | −1(−1.80,−0.20) | −0.36(0.02) |
| Δ Proteobacteria | Baseline HEI | −0.94(−1.67,−0.21) | −0.32(0.03) | −0.87(−1.68,−0.06) | −0.29(0.04) | |
| Δ HEI | Baseline Proteobacteria |
−0.95(−1.70,−0.20) | −0.38(0.02) | −0.85(−1.62,−0.08) | −0.34(0.03) | |
| Δ HEI | Δ Proteobacteria | −0.88(−1.60,−0.15) | −0.33(0.03) | −0.80(−1.55, −0.05) | −0.30(0.04) |
Note. Associations between baseline Healthy Eating Index (HEI) and gut microbiota diversity/composition (Shannon Diversity, Firmicutes, Bacteroidota, Actinobacteriota, Proteobacteria) at baseline and over time (Δ), including unadjusted and adjusted regression coefficients (β and B with 95% CIs). Adjusted models account for baseline microbiome or baseline HEI when appropriate, and key covariates (i.e., age, sex, BMI, cancer stage, and chemotherapy regimen) when applicable. To avoid the symmetry inherent in standardized HEI change–microbiome change models, we present only microbiome change as the input variable and HEI change as the outcome variable.
Table 7.
Correlations Between Diet Quality (HEI) and Microbiome Profiles at Baseline and Changes (Microbiome Genus).
Table 7.
Correlations Between Diet Quality (HEI) and Microbiome Profiles at Baseline and Changes (Microbiome Genus).
| Genus | Outcomes | Input Variables | Unadjusted β (95% CI) | p-value | Adjusted B (95% CI) | p-value |
|---|---|---|---|---|---|---|
| Bacteroides | Baseline | Baseline HEI | +0.15 (-0.07, 0.37) | 0.18 | +0.10 (-0.12, 0.32) | 0.37 |
| Δ | Baseline HEI | +0.12 (-0.10, 0.34) | 0.28 | +0.08 (-0.14, 0.30) | 0.47 | |
| Baseline | Δ HEI | +0.08 (-0.14, 0.30) | 0.47 | +0.05 (-0.17, 0.27) | 0.65 | |
| Δ | Δ HEI | +0.21 (-0.03, 0.45) | 0.09 | +0.18 (-0.07, 0.43) | 0.15 | |
| Blautia_A | Baseline | Baseline HEI | -0.22 (-0.42, -0.02) | 0.03 | -0.18 (-0.38, 0.02) | 0.08 |
| Δ | Baseline HEI | -0.15 (-0.35, 0.05) | 0.14 | -0.12 (-0.32, 0.08) | 0.24 | |
| Baseline | Δ HEI | -0.10 (-0.30, 0.10) | 0.33 | -0.07 (-0.27, 0.13) | 0.49 | |
| Δ | Δ HEI | -0.25 (-0.47, -0.03) | 0.03 | -0.21 (-0.43, 0.01) | 0.06 | |
| Phocaeicola | Baseline | Baseline HEI | +0.10 (-0.12, 0.32) | 0.37 | +0.07 (-0.15, 0.29) | 0.54 |
| Δ | Baseline HEI | -0.05 (-0.27, 0.17) | 0.65 | -0.03 (-0.25, 0.19) | 0.79 | |
| Baseline | Δ HEI | +0.03 (-0.19, 0.25) | 0.79 | +0.01 (-0.21, 0.23) | 0.93 | |
| Δ | Δ HEI | -0.12 (-0.34, 0.10) | 0.29 | -0.09 (-0.31, 0.13) | 0.42 | |
| Agathobacter | Baseline | Baseline HEI | -0.18 (-0.38, 0.02) | 0.08 | -0.15 (-0.35, 0.05) | 0.14 |
| Δ | Baseline HEI | -0.22 (-0.42, -0.02) | 0.03 | -0.19 (-0.39, 0.01) | 0.06 | |
| Baseline | Δ HEI | -0.07 (-0.27, 0.13) | 0.49 | -0.05 (-0.25, 0.15) | 0.63 | |
| Δ | Δ HEI | -0.28 (-0.50, -0.06) | 0.01 | -0.24 (-0.46, -0.02) | 0.03 | |
| Bifidobacterium | Baseline | Baseline HEI | +0.19 (0.02, 0.36) | 0.03 | +0.15 (-0.02, 0.32) | 0.09 |
| Δ | Baseline HEI | +0.10 (-0.07, 0.27) | 0.25 | +0.07 (-0.10, 0.24) | 0.42 | |
| Baseline | Δ HEI | +0.12 (-0.05, 0.29) | 0.17 | +0.09 (-0.08, 0.26) | 0.30 | |
| Δ | Δ HEI | -0.10 (-0.26, 0.06) | 0.22 | -0.08 (-0.24, 0.08) | 0.33 | |
| Faecalibacterium | Baseline | Baseline HEI | +0.31 (0.08, 0.54) | 0.01 | +0.26 (0.03, 0.49) | 0.03 |
| Δ | Baseline HEI | +0.25 (0.02, 0.48) | 0.04 | +0.21 (-0.02, 0.44) | 0.07 | |
| Baseline | Δ HEI | +0.18 (-0.05, 0.41) | 0.12 | +0.14 (-0.09, 0.37) | 0.23 | |
| Δ | Δ HEI | +0.38 (0.14, 0.62) | <0.01 | +0.33 (0.09, 0.57) | 0.01 | |
| Parabacteroides | Baseline | Baseline HEI | +0.13 (-0.09, 0.35) | 0.24 | +0.09 (-0.13, 0.31) | 0.41 |
| Δ | Baseline HEI | +0.22 (0.00, 0.44) | 0.05 | +0.18 (-0.04, 0.40) | 0.11 | |
| Baseline | Δ HEI | +0.15 (-0.07, 0.37) | 0.18 | +0.12 (-0.10, 0.34) | 0.28 | |
| Δ | Δ HEI | +0.26 (0.02, 0.50) | 0.03 | +0.22 (-0.02, 0.46) | 0.07 | |
| Streptococcus | Baseline | Baseline HEI | -0.20 (-0.40, 0.00) | 0.05 | -0.16 (-0.36, 0.04) | 0.12 |
| Δ | Baseline HEI | -0.25 (-0.45, -0.05) | 0.01 | -0.21 (-0.41, -0.01) | 0.04 | |
| Baseline | Δ HEI | -0.12 (-0.32, 0.08) | 0.24 | -0.09 (-0.29, 0.11) | 0.38 | |
| Δ | Δ HEI | -0.30 (-0.52, -0.08) | <0.01 | -0.26 (-0.48, -0.04) | 0.02 | |
| Alistipes | Baseline | Baseline HEI | +0.11 (-0.11, 0.33) | 0.32 | +0.07 (-0.15, 0.29) | 0.53 |
| Δ | Baseline HEI | +0.35 (0.13, 0.57) | <0.01 | +0.31 (0.09, 0.53) | <0.01 | |
| Baseline | Δ HEI | +0.14 (-0.08, 0.36) | 0.21 | +0.10 (-0.12, 0.32) | 0.37 | |
| Δ | Δ HEI | +0.42 (0.18, 0.66) | <0.01 | +0.37 (0.13, 0.61) | <0.01 | |
| Mediterraneibacter | Baseline | Baseline HEI | -0.16 (-0.36, 0.04) | 0.12 | -0.13 (-0.33, 0.07) | 0.20 |
| Δ | Baseline HEI | -0.19 (-0.39, 0.01) | 0.06 | -0.16 (-0.36, 0.04) | 0.12 | |
| Baseline | Δ HEI | -0.08 (-0.28, 0.12) | 0.43 | -0.06 (-0.26, 0.14) | 0.56 | |
| Δ | Δ HEI | -0.23 (-0.45, -0.01) | 0.04 | -0.20 (-0.42, 0.02) | 0.08 |
Note. Associations between baseline Healthy Eating Index (HEI) and gut microbiome genus at baseline and over time (Δ), including unadjusted and adjusted regression coefficients (β and B with 95% CIs). Adjusted models account for baseline microbiome or baseline HEI when appropriate, and key covariates (i.e., age, sex, BMI, cancer stage, and chemotherapy regimen) when applicable. To avoid the symmetry inherent in standardized HEI change–microbiome change models, we present only microbiome change as the input variable and HEI change as the outcome variable.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



