
Submitted:
11 November 2025
Posted:
22 December 2025
You are already at the latest version
Abstract
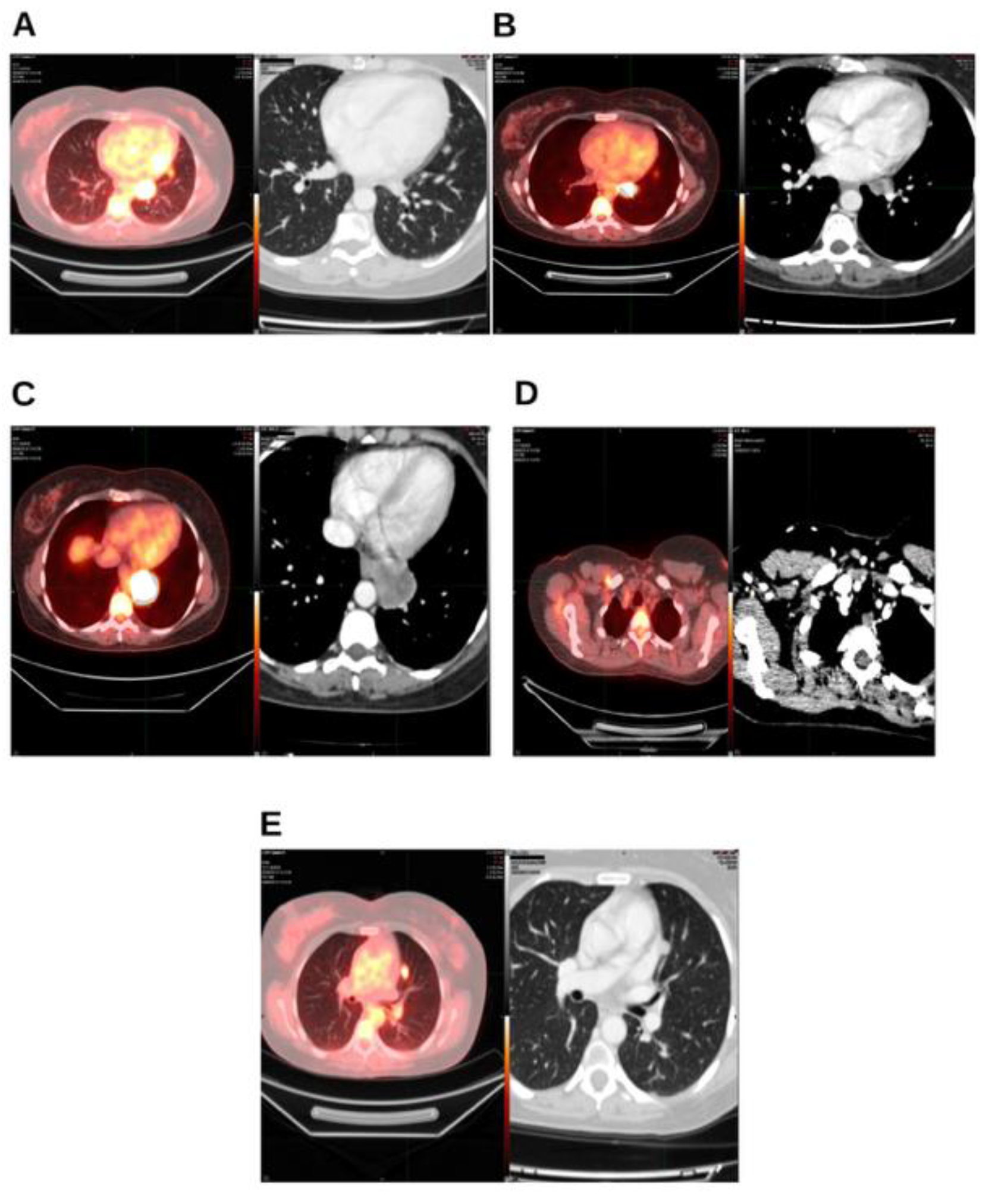
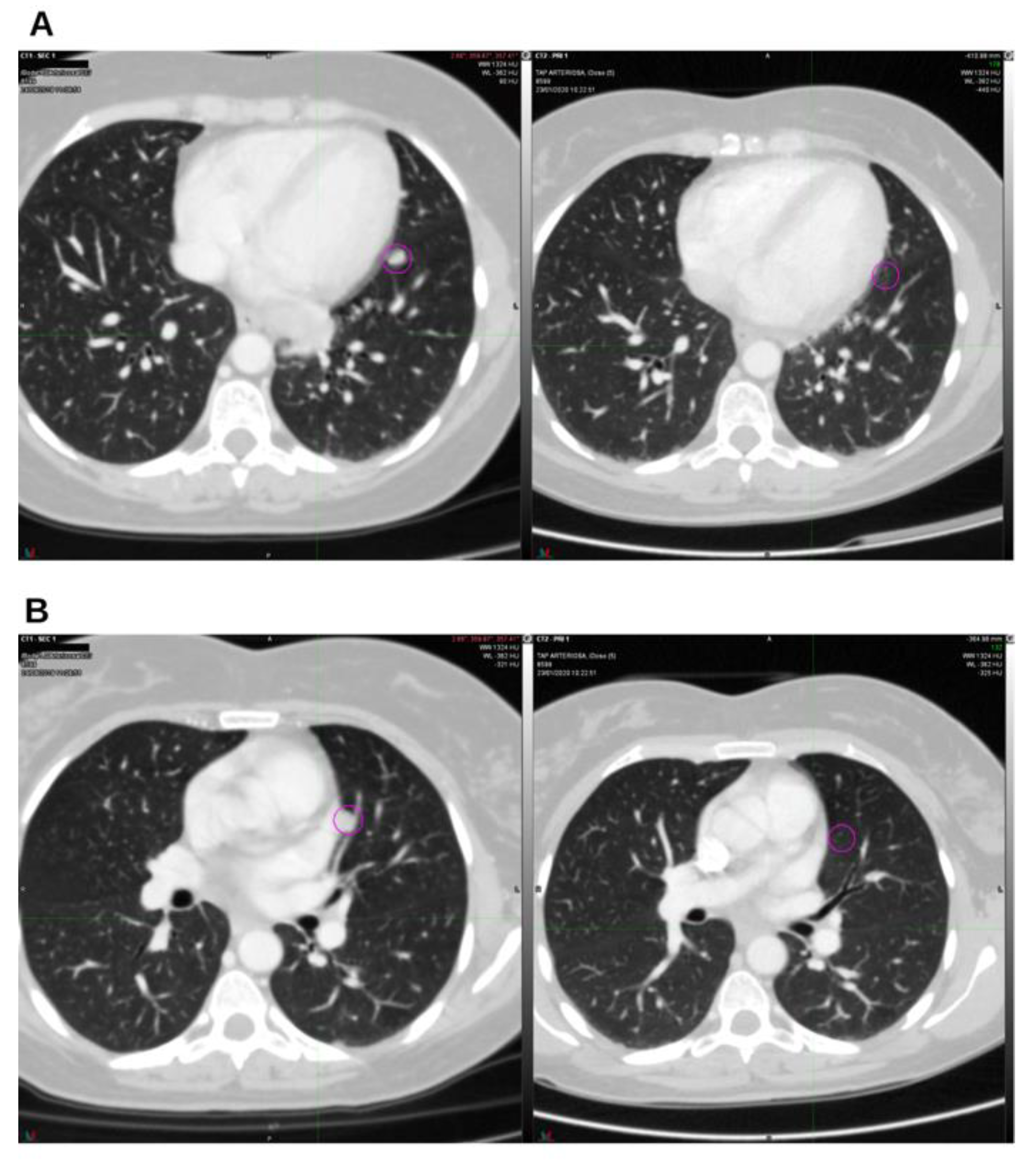
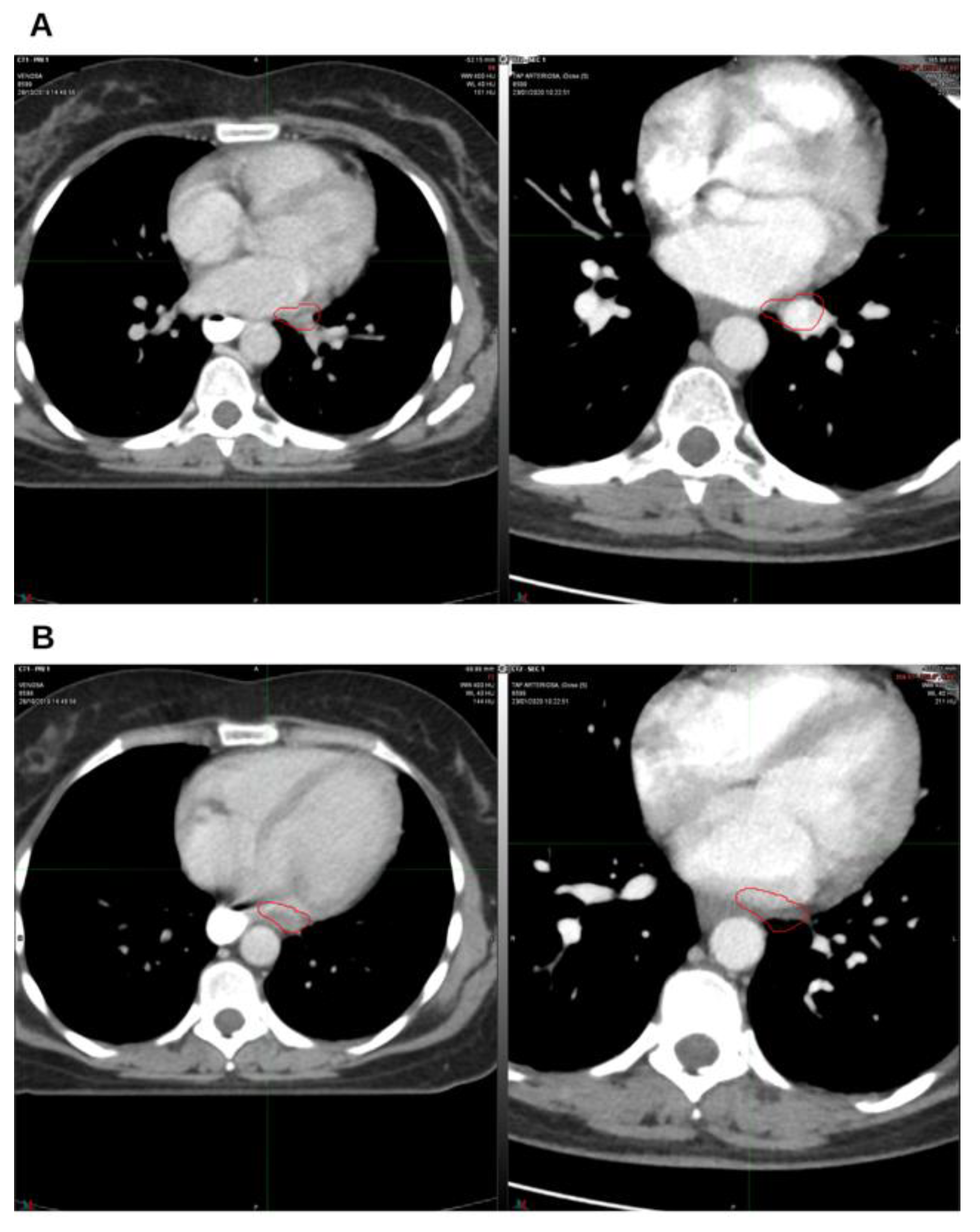
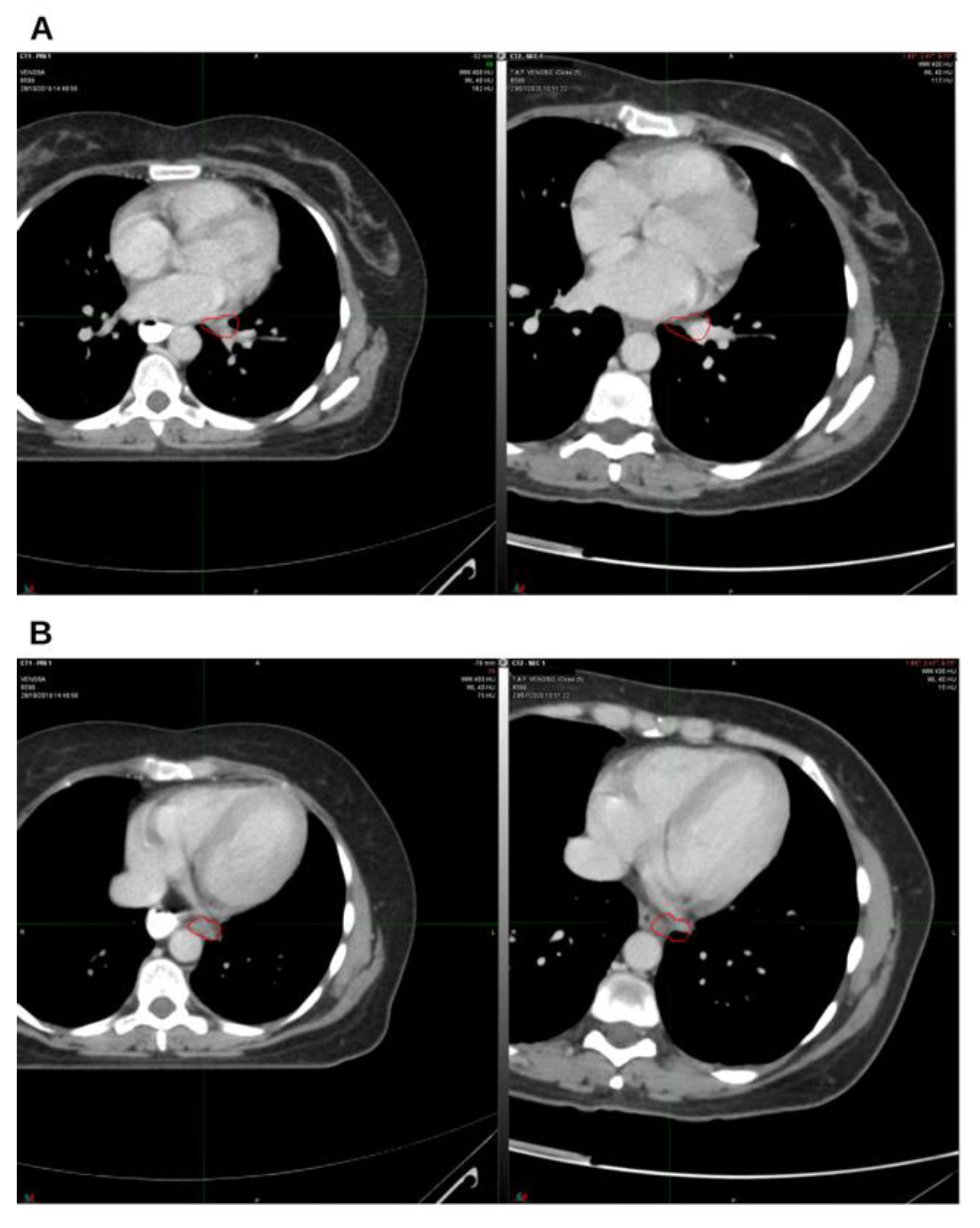
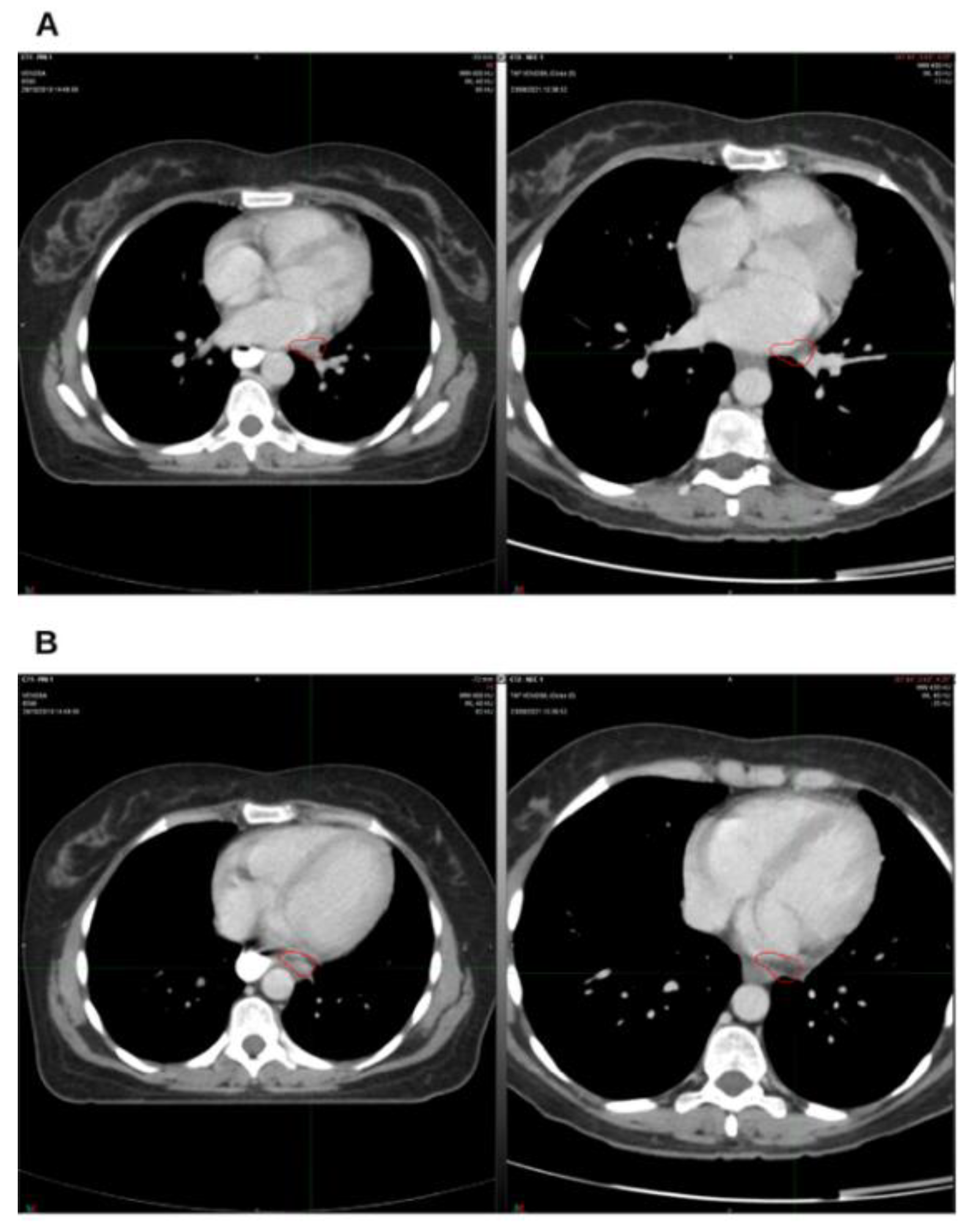
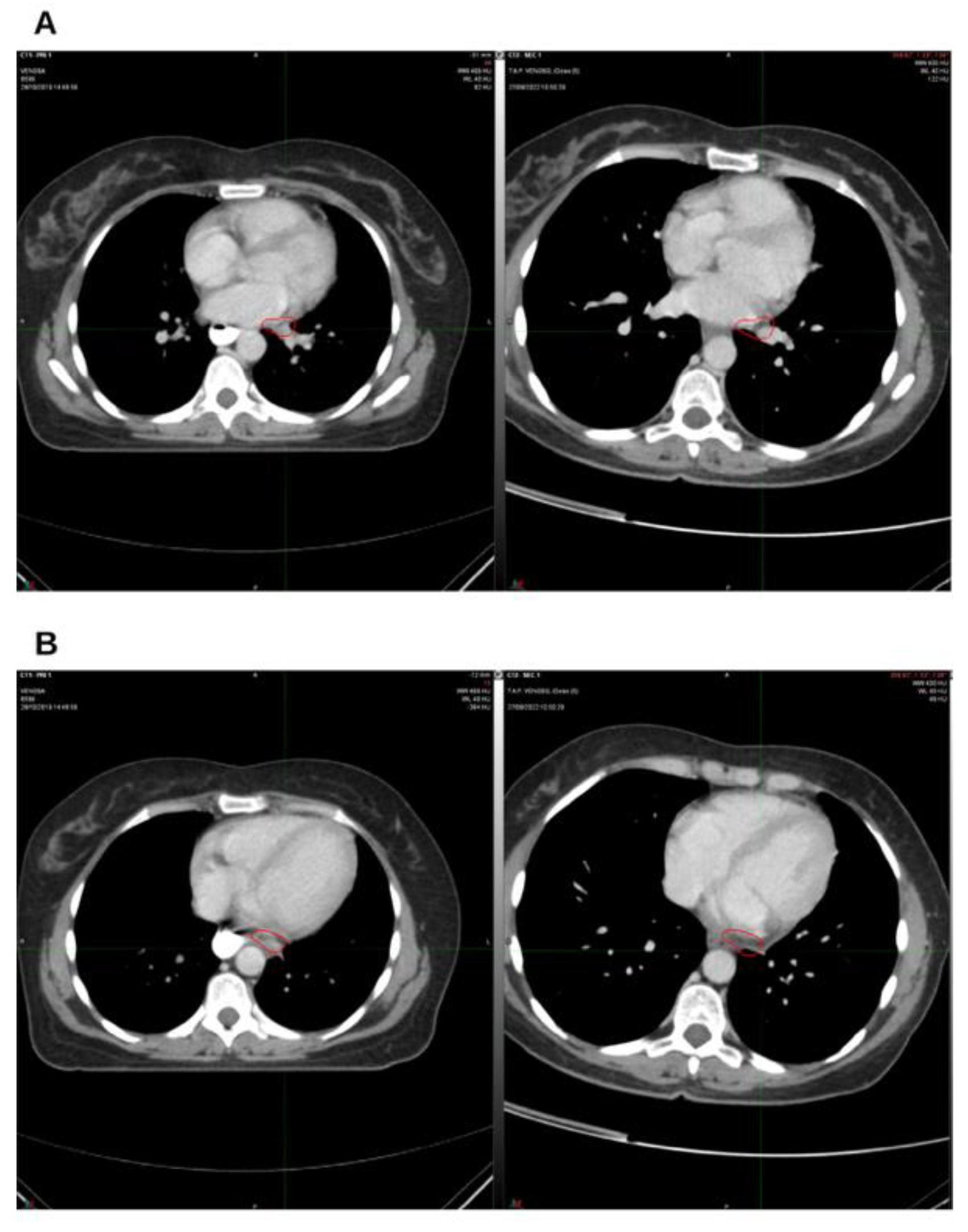
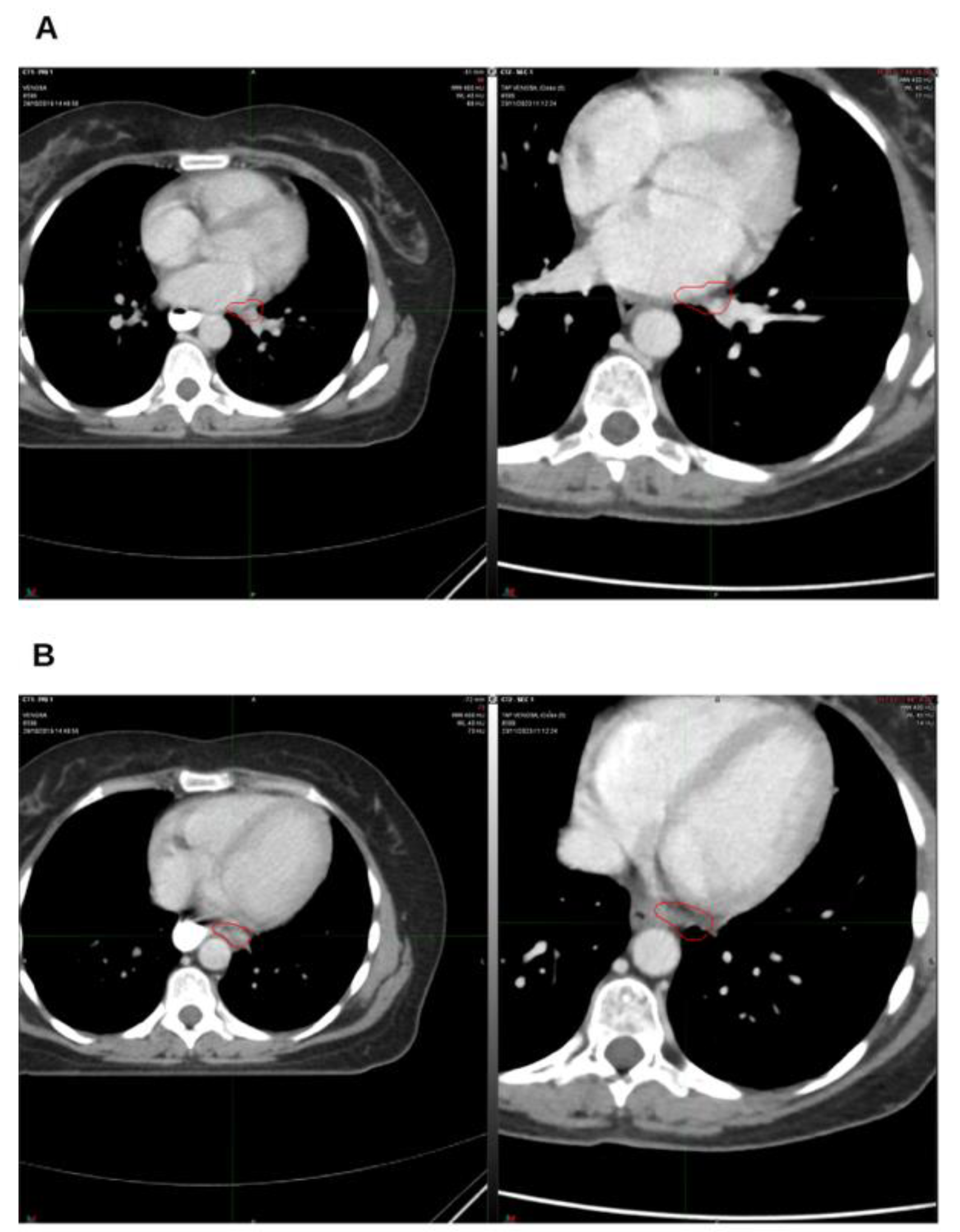
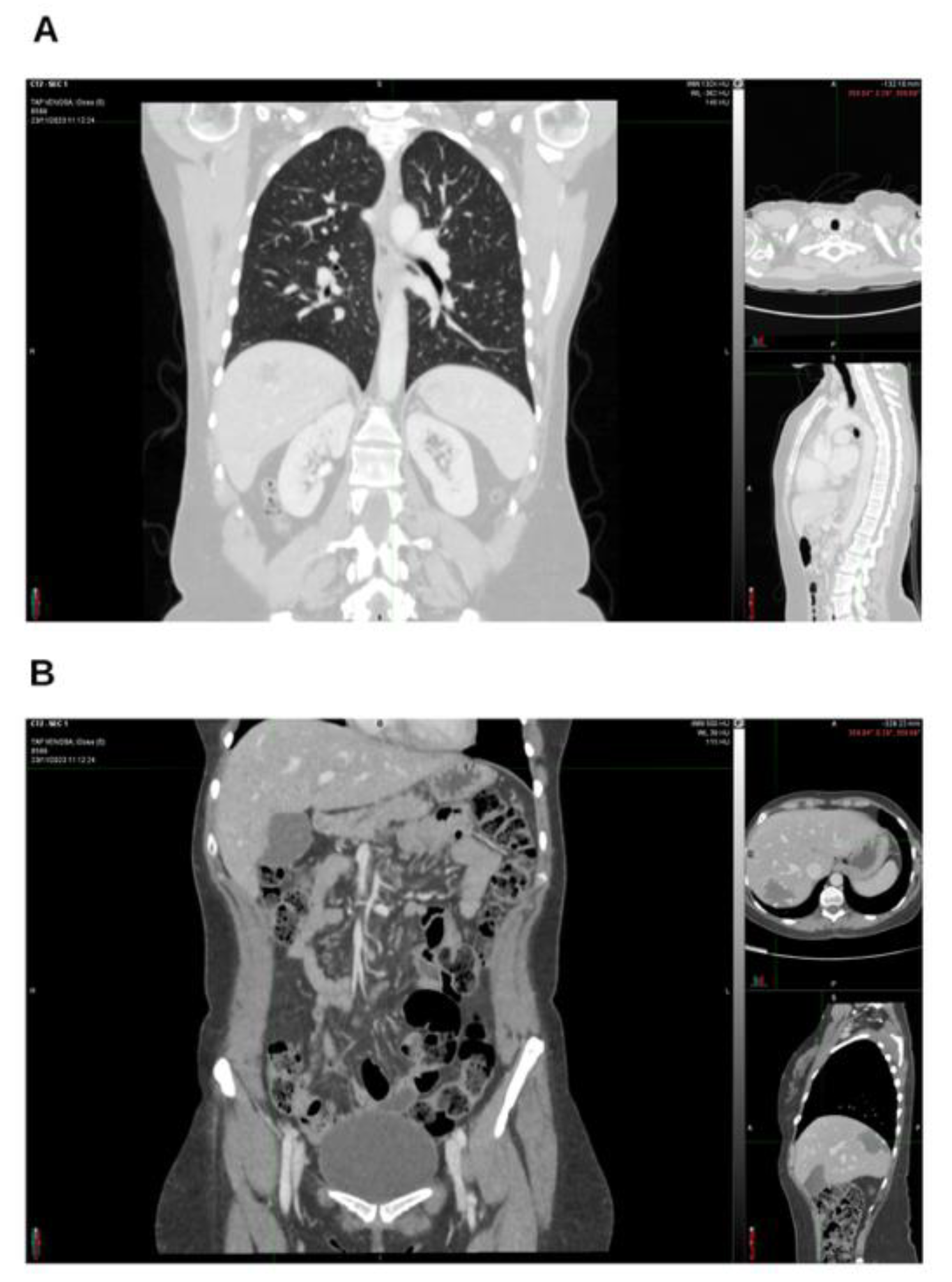
Background and Clinical Significance: Breast cancer is the most frequent malignancy in women. Advanced metastatic breast cancer is considered a treatable but incurable condition, with a median overall survival of only 2-3 years. Among its subtypes, triple-negative breast cancer (TNBC) accounts for a high proportion of breast cancer–related deaths. It is characterized by an aggressive clinical course, early recurrence, and a strong propensity for visceral and brain metastases. Case Presentation :We report the case of a Caucasian woman who, two years after being initially diagnosed and treated for TNBC, developed disease relapse with lung and mediastinal lymph node metastases. The patient received three months of chemotherapy combined with an adjuvant integrative protocol consisting of melatonin, cannabidiol, and oxygen–ozone therapy. This combined approach led to the complete disappearance of the lung nodules. Subsequently, stereotactic radiotherapy was performed and, in association with the ongoing integrative treatment, resulted in a significant reduction of mediastinal adenopathy. Introduction of immunotherapy, supported continuously by the same adjuvant strategy, achieved a complete and durable remission. Strikingly, the patient remained disease-free five years after the diagnosis of lung and mediastinal metastases. Conclusions: This clinical case highlights the potential benefit of using melatonin, cannabidiol, and oxygen–ozone therapy as part of an integrative approach in patients with aggressive metastatic TNBC. While it is not possible to establish causality from a single case, the sustained remission observed suggests that such unconventional adjuvant strategies could play a supportive role in enhancing the efficacy of standard oncologic therapies.
Keywords:
1. Introduction and Clinical Significance
2. Case Presentation
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of interest
Abbreviations
| CBD | Cannabidiol; |
| ER | estrogen receptors; |
| ER+ | ER positive; |
| HER2 | human epithelial growth factor receptor 2; |
| HER2+ | HER2 positive; |
| MLT | Melatonin; |
| O3 | Ozone; |
| O2/O3 | Oxygen-Ozone; |
| PET | Positron emission tomography; |
| PR | progesterone receptor; |
| ROS | reactive oxygen species; |
| TAC | computerized axial tomography; |
| TNBC | triple-negative breast cancers. |
References
- Siegel, RL; Miller, KD; Jemal, A. Cancer statistics, 2020. CA Cancer J Clin. 2020, 70(1), 7–30. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N; Penault-Llorca, F; Cortes, J; Gnant, M; Houssami, N; Poortmans, P; et al. Breast cancer. Nat Rev Dis Primers [Internet]. 23 Sep 2019, 5, p. 66. Available online: https://www.nature.com/articles/s41572-019-0111-2.
- Loibl, S; Poortmans, P; Morrow, M; Denkert, C; Curigliano, G. Breast cancer. The Lancet [Internet]. 2021 May [cited 2025 Feb 9], 397, pp. 1750–69. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0140673620323813.
- Nolan, E; Lindeman, GJ; Visvader, JE. Deciphering breast cancer: from biology to the clinic. Cell [Internet] 2023, 186(8), 1708–28. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0092867423000995. [CrossRef] [PubMed]
- Baeza-Noci, J; Pinto-Bonilla, R. Systemic Review: Ozone: A Potential New Chemotherapy. Int J Mol Sci. 2021, 22(21), 11796. [Google Scholar] [CrossRef] [PubMed]
- Li, Y; Pu, R. Ozone Therapy for Breast Cancer: An Integrative Literature Review. Integr Cancer Ther [Internet] Available from. 2024, 23, 15347354241226667. [Google Scholar] [CrossRef]
- Gülck, T; Møller, BL. Phytocannabinoids: Origins and Biosynthesis. Trends Plant Sci. 2020, 25(10), 985–1004. [Google Scholar] [CrossRef] [PubMed]
- Lowe, H; Toyang, N; Steele, B; Bryant, J; Ngwa, W. The Endocannabinoid System: A Potential Target for the Treatment of Various Diseases. Int J Mol Sci 2021, 22(17), 9472. [Google Scholar] [CrossRef] [PubMed]
- Twelves, C; Sabel, M; Checketts, D; Miller, S; Tayo, B; Jove, M; et al. A phase 1b randomised, placebo-controlled trial of nabiximols cannabinoid oromucosal spray with temozolomide in patients with recurrent glioblastoma. Br J Cancer 2021, 124(8), 1379–87. [Google Scholar] [CrossRef] [PubMed]
- Elbaz, M; Nasser, MW; Ravi, J; Wani, NA; Ahirwar, DK; Zhao, H; et al. Modulation of the tumor microenvironment and inhibition of EGF/EGFR pathway: novel anti-tumor mechanisms of Cannabidiol in breast cancer. Mol Oncol. 2015, 9(4), 906–19. [Google Scholar] [CrossRef] [PubMed]
- Patel, N; Kommineni, N; Surapaneni, SK; Kalvala, A; Yaun, X; Gebeyehu, A; et al. Cannabidiol loaded extracellular vesicles sensitize triple-negative breast cancer to doxorubicin in both in-vitro and in vivo models. Int J Pharm. 2021, 607, 120943. [Google Scholar] [CrossRef] [PubMed]
- Talib, WH; Alsayed, AR; Abuawad, A; Daoud, S; Mahmod, AI. Melatonin in Cancer Treatment: Current Knowledge and Future Opportunities. Molecules [Internet] cited. 2021, 26(9), 2506. [Google Scholar] [CrossRef] [PubMed]
- Zeppa, L; Aguzzi, C; Morelli, MB; Marinelli, O; Amantini, C; Giangrossi, M; et al. In Vitro and In Vivo Effects of Melatonin-Containing Combinations in Human Pancreatic Ductal Adenocarcinoma. J Pineal Res. 2024, 76(5), e12997. [Google Scholar] [CrossRef] [PubMed]
- Antonini, M; Aguzzi, C; Fanelli, A; Frassineti, A; Zeppa, L; Morelli, MB; Pastore, G; Nabissi, M; Luongo, M. The Effects of a Combination of Medical Cannabis, Melatonin, and Oxygen-Ozone Therapy on Glioblastoma Multiforme: A Case Report. Reports (MDPI) 2023, 6(2), 22. [Google Scholar] [CrossRef] [PubMed]
- Mammone, A; Zuccoli, P; Zeppa, L; Morelli, MB; Fanelli, A; Barozza, LG; Boschetti, C; Cornacchini, N; Nabissi, M; Luongo, M. Integrative Use of Medical Cannabis, Melatonin and Oxygen-Ozone Therapy in Oral Tongue Carcinoma: A Case Report. In Adv Complement Alt Med.; ACAM; Volume 8, 5.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



