
Submitted:
13 December 2025
Posted:
15 December 2025
You are already at the latest version
Abstract
Background/Objectives: Delirium is frequent and serious in older adults attending the emergency department (ED), but evidence on its pharmacological management in this setting is limited. This study aimed to quantify the pharmacological treatment of de-lirium in older adults in the ED and examine its association with subsequent hospital admission. Methods: An observational cross-sectional study was conducted between November 2021 and June 2022 in a Spanish ED. The sample included 153 adults aged 65 years or older with clinician-diagnosed delirium. Clinical, triage, and medication data were obtained from electronic medical records, and associations with hospital admis-sion were analysed using multivariable logistic regression. Results: Ninety-one partic-ipants (59.5%) were hospitalised. Antipsychotic, analgesic, and benzodiazepine use was associated with increased risk of hospitalisation. Absence of an underlying cause was a protective factor. The logistic regression model was significant. Conclusions: Specific drug families were associated with a higher likelihood of hospital admission in older adults with delirium in the ED. These findings support safer and more individualised pharmacological approaches and highlight the need for studies evaluating targeted interventions.
Keywords:
aged
; delirium
; drug therapy
; emergency service
; hospital
; hospitalization
1. Introduction
Delirium is an acute, prevalent, and severe neuropsychiatric syndrome characterised by rapid and fluctuating disturbances of attention, cognition, and consciousness. In older adults, its incidence in the Emergency Department (ED) ranges from 7% to 20%, reaching up to 89% in people with previous cognitive impairment or dementia [1]. The presence of delirium is associated with increased morbidity, mortality, and functional impairment, underlining the importance of early detection and management.
The ED setting presents particular challenges for the diagnosis and treatment of delirium, due to the variability of signs and symptoms, high care burden, and limited care times [2]. The Manchester Triage System (MTS) is commonly used in EDs to assess clinical features with standardised flow charts and discriminators, and to classify patients according to priority levels PI (immediate, red), PII (very urgent, orange), PIII (urgent, yellow), PIV (standard, green), and PV (non-urgent, blue) [3]. Despite its role in structuring ED workflow, the MTS lacks specific protocols for detecting delirium. This deficiency, coupled with the syndrome’s fluctuating nature, contributes to underdiagnosis rates as high as 80% [4].
The management of delirium involves a combination of pharmacological and nonpharmacological strategies. Several international clinical guidelines – including those of the American Geriatrics Society and the American Society for Enhanced Recovery and the European Society of Anaesthesiology – advise against using antipsychotics and benzodiazepines in the older population because they are associated with important adverse events and prolonged confusion [5]. Nonetheless, these drugs are still widely administered in clinical practice, despite a lack of robust evidence supporting their efficacy and safety, especially in the hospital ED setting.
Current prevention and treatment strategies for delirium are based on studies from intensive care, surgical, internal medicine, or palliative care settings. Consequently, their applicability to the ED remains uncertain, and specific data for this context are scarce [6]. Furthermore, a lack of standardised clinical criteria means drug selection and dosing for delirium is often guided by individual experience rather than structured protocols, increasing the risk of overdose, adverse events, and suboptimal clinical outcomes [7] . This situation reflects a critical knowledge gap regarding the pharmacological management of delirium in the ED [8], where over half of geriatric hospitalisations originate.
To our knowledge, no studies have specifically analysed the pharmacological treatment administered to older people with delirium in the ED. Therefore, the aim of this study was to quantify and characterise the pharmacological treatment in this population and to analyse its association with hospitalisation, in order to provide evidence to guide safer and more effective practices in this critical context.
2. Materials and Methods
Design
This was an observational, cross-sectional study conducted between November 2021 and June 2022.
Study Setting and Sampling
The study was carried out in the Emergency Department (ED) of a tertiary care university hospital in eastern Spain. The centre is a tertiary care university hospital with 256 beds, covering a population of about 188,000 inhabitants. The ED deals with an average of 60,000 episodes per year and is organised into six care areas: triage, admission, consultations, resuscitation, observation, and treatment room, as well as specific areas such as paediatrics and traumatology. The care circuit begins with triage by the nursing staff. Depending on the priority assigned, the doctor in charge carries out a clinical assessment, orders the relevant diagnostic tests, and prescribes the most appropriate treatment. The nursing staff then prepare and administer the treatment.
From November 2020 to June 2021 (i.e., one year prior to the study period), 8426 people aged 65 years or older were seen in the ED of this hospital. Based on this reference population, an estimated 1.87% prevalence of delirium, a confidence level of 95%, and a margin of error of 5%, we estimated a minimum sample size of 153 people.
Inclusion and Exclusion Criteria
The study population consisted of people aged 65 years or older who attended the ED between November 2021 and June 2022 and were diagnosed with delirium (International Classification of Diseases, tenth revision (ICD-10) code F05). The medical team made the diagnosis based on criteria set out in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). These criteria include impaired attention and alertness, acute onset and fluctuating course, additional cognitive impairment, and exclusion of causes such as pre-existing neurocognitive disorders or severely decreased level of consciousness [9]. We excluded cases where delirium was clearly due to alcohol or substance abuse.
Data Collection
We collected the following data from participants’ electronic medical records during ED care: sociodemographic variables, MTS flow charts, priority assigned according to triage, underlying pathology associated with delirium, discharge destination, place of hospitalisation (if hospitalised), and pharmacological treatment administered, including the active ingredient, administration dose, and total number of drugs per patient.
Data Analysis
All data were reviewed and verified by an independent evaluator to ensure statistical quality and reliability. We performed a descriptive analysis of the sample, expressing continuous variables as means and standard deviations (SDs), and categorical variables as absolute frequencies and percentages.
To measure the association of each variable with hospital admission, we calculated odds ratios (ORs) and their respective 95% confidence intervals (CIs) for categorical variables, and mean differences (MDs) with 95% CIs for continuous variables. Results with a p value below 0.05 were considered statistically significant.
We constructed a binary logistic regression model using backward stepwise selection, progressively eliminating variables that did not contribute significantly to the model fit, either because they did not substantially modify the estimated effect (variation < 10%) or because they did not improve the standard error. The model included variables with significance in the bivariate analysis and others considered clinically relevant according to the literature, such as MTS priority level, , older age (> 80 years), male sex, presence of an underlying disease, and pharmacological treatment administered in the ED (analgesics, antipsychotics, benzodiazepines, antibiotics, antidepressants, corticosteroids, antihypertensives, diuretics, anticonvulsants, antiarrhythmics, bronchodilators, and antidiabetics). Where several subsets of variables showed equal predictive capacity, we reached consensus through discussion for the final model selection. We determined the discriminative capacity of the model by analysing the receiver operating characteristic (ROC) curve, calculating the area under the curve (AUC) with its 95% CI as a performance indicator. All analyses were performed with IBM SPSS Statistics software for Windows, version 28.0 (IBM Corp., Armonk, NY, USA).
Ethical Considerations
The study was approved by the research ethics committee of the hospital where the data collection was conducted. All participants signed an informed consent form prior to inclusion. The research was carried out in accordance with the ethical principles of the Declaration of Helsinki and with Spanish Organic Law 3/2018, of 5 December, on Personal Data Protection and the guarantee of digital rights. Data confidentiality was ensured at all times.
3. Results
During the study recruitment period, 53,110 people were seen in the ED of Francesc de Borja Hospital, of whom 28.6% (15,197) were over 65 years of age. Within this age group, 153 people (1.01%) had a diagnosis of delirium and formed our study sample. Ninety-one participants (59.5%) required hospitalisation, mainly in Internal Medicine (94.5%, n = 86), followed by urology and surgery (2.2%, n = 2 in each department) and the intensive care unit (1.1%, n = 1).
The mean age of our sample was 84 years. There is a slight predominance of males. Most participants were classified as priority III (urgent; 62.1%, n = 95) and priority IV (standard; 31.4%, n = 48) in the MTS triage. The most commonly used MTS flow charts were ‘unwell adult’ (54.9%, n = 84), followed by ‘behaving strangely’ (15.0%, n = 23). Regarding associated clinical diagnoses, 68 participants (44.4%) had no underlying pathology associated with the delirium episode. However, 34 people (22.2%) had an infection and 16 (10.5%) had kidney disease (p = 0.012).
Regarding pharmacological treatment, participants received a mean of 2.1 drugs (SD = 1.98), and the mean difference (MD) between hospitalised versus nonhospitalised participants was 1.97 drugs (95% CI 1.41 to 2.53; p < 0.001). Of note, 73.6% (n = 67) of participants who required hospital admission were treated with more than two active ingredients during their stay in the ED, compared with 16 participants (25.8%) of nonhospitalised participants (p < 0.001).
Finally, analysis of the pharmacological groups revealed that hospitalised participants were more likely than nonhospitalised participants to have received antipsychotics (OR 9.93, 95% CI 3.32-29.73; p < 0. 001), benzodiazepines (OR 5.00, 95% CI 1.08-23.00; p = 0.024), analgesics (OR 4.97, 95% CI 2.46-10.02; p < 0.001), and antibiotics (OR 4.15, 95% CI 1.92-8.97; p < 0.001), as shown in Table 1.
Analgesics that showed a robust association with hospital admission were metamizole (OR 7.53, 95% CI 0.93-60.42; p = 0.028) and paracetamol (OR, 3.35, 95% CI 1.66-6.77; p < 0.001), while ketamine showed a weaker association (OR 3.27, 95% CI 0.89-12.02; p = 0.061). Among the antipsychotics, there were associations for haloperidol (OR 5.19, 95% CI 1.46-18.39; p = 0.006) and tiapride (OR 3.57, 95% CI 1.14-11.14; p = 0.021). Finally, although the benzodiazepine category showed an overall significant association with hospitalisation (OR 5.00, 95% CI 1.08-23.00; p = 0.024), this effect could not be confirmed for any individual drug, probably due to insufficient statistical power from a small sample size (Table 2).
An analysis of the relationship between treatment and delirium aetiology showed that people with underlying pathologies such as infections, kidney disease, or respiratory disease were more likely to receive analgesics (p = 0.028) and antibiotics (p < 0.001) compared with people who had no apparent cause of delirium. There were also relevant differences in the use of corticosteroids, diuretics, antiulcer drugs, and bronchodilators, suggesting a therapeutic adaptation according to the clinical context of the patient. These findings reflect a more targeted treatment pattern depending on the clinical origin of delirium (Table 3).
The logistic regression model constructed to predict hospitalisation in older adults with delirium was statistically significant (χ² = 49.59, p < 0.001) with a Nagelkerke R² of 0.374. It showed a sensitivity of 81.3% and a specificity of 66.1% and classified 59.5% of cases correctly. Variables included in the model were analgesics (OR 3.80, 95% CI 1.75-8.27; p < 0.001), antipsychotics (OR 9.61, 95% CI 3.02-30.56; p < 0.001), benzodiazepines (OR 3.93, 95% CI 0.75-20.5; p = 0.104), as well as the absence of an underlying cause, which behaved as a protective factor (OR 0.45, 95% CI 0.21-0.97; p = 0.043). The AUC was 0.80 (95% CI 0.72-0.86), indicating good predictive power to identify patients at increased risk of admission (Figure 1).
4. Discussion
Previous evidence suggests that delirium in older people treated in the ED is associated with longer hospital stays, increased mortality, more clinical complications, a higher probability of discharge to institutional centres, and a considerable increase in the burden of care [10]. This study aimed to define the profile of older people with delirium who required hospitalisation after an ED visit. The prevalence of hospitalisation in our sample was 59.5%. The variables associated with admission included certain drug families, particularly analgesics, antipsychotics, and benzodiazepines.
The mean age observed in our sample (84 years) suggests a possible tendency towards the presentation of delirium in older patients compared to what is reported in the literature, where averages range from 71.8 years to 77 years [11]. This difference could be related to population-specific characteristics. On the other hand, the equal distribution of men and women in our sample is consistent with previous research, reinforcing the idea that neither sex has a greater predisposition to delirium [12].
Findings related to the MTS reinforce concerns raised about the sensitivity and suitability of this tool in older adults [13]. The high proportion of cases classified as urgent (62.1%) and standard priority (31.4%), together with the frequent use of the “unwell adult” (54.9%) and “behaving strangely” (15.0%) flow charts, suggests a possible underestimation of clinical severity. These results align with previous studies in geriatric populations and suggest that the MTS may have systematic limitations in recognising the clinical complexity of older adults, particularly in conditions like delirium [14].
No underlying cause of delirium was identified in 35.2% of hospitalised people in our sample. This highlights the diagnostic difficulties of delirium in the ED setting, especially among older adults [15]. The multifactorial pathophysiology of delirium, together with precipitating factors such as pain, immobilisation, and polypharmacy, can preclude establishing a clear aetiology in the initial assessment [16]. In cases where clinicians identified a specific cause, the most frequently associated with hospitalisation was infection (30.8% in hospitalised participants vs 9.7% in nonhospitalised participants). This is likely because infections in older adults can have a substantial physiological impact and often manifest atypically, with delirium as the primary symptom. Hospital admission is necessary in these cases for proper assessment and treatment [17].
Our analysis of drug consumption showed that participants who required hospitalisation received a higher number of drugs in the ED than nonhospitalised participants (MD 1.97 drugs, 95% CI 1.41-2.53; p < 0.001), suggesting a possible association between the number of drugs administered in the ED and the clinical severity or complexity of the condition. This pattern is consistent with the literature, which reports that people with delirium are usually treated with one or two active ingredients [18]. Recent studies have described ED administration of antipsychotics (e.g., haloperidol and olanzapine), benzodiazepines (e.g., midazolam and lorazepam) [19], ketamine, opioids, and alpha-2 agonists such as dexmedetomidine [20].
Antipsychotics can be useful in treating acute mental disorders, although the evidence for their efficacy and safety in people with delirium remains limited and controversial, with some authors warning of potential risks such as increased mortality, prolonged symptoms, and serious adverse effects [21]. In our sample, antipsychotic use was significantly associated with hospitalisation, probably because these drugs are reserved for the most severe and complex cases [22]. Although several studies have evaluated the use of antipsychotics in settings with a high prevalence of delirium, such as intensive care units, general hospital wards, postoperative care, palliative care, and rehabilitation departments, there is a lack of evidence guiding their application in EDs, underscoring the need for more prospective research [23].
Given that haloperidol and tiapride were the antipsychotics that showed a significant association with hospitalisation in our study, it is pertinent to analyse them in greater depth. The prophylactic use of haloperidol in older people is not recommended due to a lack of solid evidence supporting its efficacy in preventing or managing delirium [24]. However, the coadministration of haloperidol with other drugs, such as lorazepam, has shown better response rates in specific clinical contexts [25]. Regarding tiapride, its frequent use in the ED contrasts with its scarce presence in the international scientific literature. This disparity could reflect local clinical practices or nonstandardised therapeutic decisions, highlighting the need for further research into the potential benefits of atypical antipsychotics in delirium management. To date, very few studies have specifically addressed the use of this drug, so our findings constitute a novel contribution and open a little-explored line of research [26].
In our sample, people who received benzodiazepines were more likely to need hospitalisation. This may be due to several factors: on the one hand, benzodiazepines may be administered in cases of severe hyperactive delirium, which would imply a higher clinical risk and justify admission regardless of the treatment used; and on the other hand, their effects on the sleep-wake cycle could contribute to worsening the condition, which in turn would require a longer hospital stay [27]. The evidence on the use of benzodiazepines is contradictory and depends largely on the clinical context in which it is evaluated. In intensive care units, most studies advise against their use due to an association with worsening delirium [28]. In contrast, benzodiazepines are used for delirium prevention and treatment in the perioperative setting, although the results are inconsistent. Some systematic reviews and meta-analyses have found no difference in the incidence of postoperative delirium following their use, while other studies have described an increased risk attributed to paradoxical effects such as irritability and confusion, especially with repeated doses [29]. In the ED setting, despite the potential usefulness of benzodiazepines in specific clinical situations such as agitation [30] or withdrawal syndrome [31], there is still little evidence focusing on their safety and efficacy in cases of delirium.
In this study, there was an association between analgesic use and the need for hospitalisation. Pain is not only a symptom but also a precipitating factor for delirium when poorly managed in older people. Therefore, the administration of analgesics could be interpreted as an indirect marker of greater clinical severity or an underlying cause that would justify hospitalisation [32]. Evidence on the specific impact of different analgesics on the progression of delirium remains limited and heterogeneous [33]. The analgesic most frequently associated with hospitalisation in our study was metamizole, a finding that is difficult to interpret in the absence of previous studies. It is possible that this relationship reflects the presence of pain as a symptom of clinical severity or as a precipitating factor for delirium, rather than an effect of the drug [32]. Paracetamol, widely used for mild to moderate pain, was also associated with higher admission rates in our sample, likely due to its recognised safety and frequent use in the older population. Finally, ketamine has been explored as an alternative analgesic in EDs for refractory pain. Although some studies have found no direct link between ketamine use and the development of delirium, its role remains controversial due to psychotropic effects and the limited evidence available [34].
Pharmacological treatment plays a key role in managing numerous acute conditions (e.g., pain, agitation, or withdrawal syndromes) that require rapid and effective intervention in the ED. However, a particularly careful approach is necessary when these conditions are aetiologically or symptomatically related to delirium. In this context, the inappropriate or nonindividualised use of certain drugs can have significant adverse consequences, including hospitalisation, a longer hospital stay, or an increased mortality risk [35]. Our results show that the administration of antipsychotics, analgesics, and benzodiazepines in the ED is associated with a higher probability of hospital admission in older people with delirium. This pharmacological profile could be useful for identifying more severe cases and guiding more individualised clinical decisions. Furthermore, limiting the unnecessary use of these drugs could help reduce admission rates, length of stay, and the associated economic impact.
This study has inherent limitations, as we were unable to collect confounding variables such as delirium severity, time spent in the ED, and the exact time of drug administration. Future research should focus on evaluating specific interventions in the ED and exploring the impact of nonpharmacological approaches on clinical outcomes.Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
5. Conclusions
This study quantifies the most frequent pharmacological management in the ED for older people with delirium, demonstrating a direct association between the use of antipsychotics, benzodiazepines, and analgesics and an increased risk of hospitalisation. Although further studies are needed in this area, our findings provide valuable evidence to guide safer and more personalised practices in this critical clinical setting.
Relevance for Clinical Practice
Our findings provide essential evidence to guide the pharmacological management of delirium in older adults attending hospital emergency departments. The association between the use of antipsychotics, benzodiazepines, and analgesics and higher hospitalisation risk underscores the need for safer and more personalised therapeutic strategies. These results highlight the importance of developing standardised protocols to improve decision-making, strengthen patient safety, and reduce the healthcare and economic burden associated with delirium in this vulnerable population.
Author Contributions
P.P-R and A.S-S; methodology, P.P-R and A.S-S; data acquisition, A.S-S; formal analysis, P.P-R and F.M.M-A; statistical analysis, F.M.M-A; investigation, P.P-R and A.S-S; data curation, A.S-S; writing—original draft preparation, A.S-S and P.P-R; writing—review and editing, A.S-S, P.P-R and F.M.M-A; supervision, P.P-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The APC was funded by the authors.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Research Ethics Committee of Hospital Francesc de Borja, Department of Gandia (protocol code 15/2021, approved on 11 October 2021). Informed consent was obtained from all participants involved in the study.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data from this study contain sensitive clinical information and, for ethical and privacy reasons, will not be made available in open repositories. However, they may be provided to qualified researchers upon reasonable request, as participants gave their consent for the use and transfer of their anonymized data for research purposes.
Acknowledgments
The authors thank all participants and the Emergency Department staff at Francesc de Borja Hospital for their collaboration and support.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| AUC | Area Under the Curve |
| CI | Confidence Interval |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition |
| ED | Emergency Department |
| GI | Gastrointestinal |
| ICD-10 | International Classification of Diseases, Tenth Revision |
| MD | Mean Differences |
| MTS | Manchester Triage System |
| OR | Odds Ratio |
| ROC | Receiver Operating Characteristic |
| SD | Standard Deviation |
| SPSS | Statistical Package for the Social Sciences |
References
- Morandi, A.; Inzitari, M.; Udina, C.; Gual, N.; Mota, M.; Tassistro, E.; Andreano, A.; Cherubini, A.; Gentile, S.; Mossello, E.; et al. Visual and Hearing Impairment Are Associated With Delirium in Hospitalized Patients: Results of a Multisite Prevalence Study. J Am Med Dir Assoc 2021, 22, 1162–1167.e3. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.W.; Elhadad, N.; Mattison, M.L.P.; Nentwich, L.M.; Levine, S.A.; Marcantonio, E.R.; Kennedy, M. Boarding Duration in the Emergency Department and Inpatient Delirium and Severe Agitation. JAMA Network Open 2024, 7, e2416343. [Google Scholar] [CrossRef]
- Zaboli, A.; Sibilio, S.; Massar, M.; Brigiari, G.; Magnarelli, G.; Parodi, M.; Mian, M.; Pfeifer, N.; Brigo, F.; Turcato, G. Enhancing Triage Accuracy: The Influence of Nursing Education on Risk Prediction. Int Emerg Nurs 2024, 75, 101486. [Google Scholar] [CrossRef] [PubMed]
- Chary, A.N.; Bhananker, A.R.; Brickhouse, E.; Torres, B.; Santangelo, I.; Godwin, K.M.; Naik, A.D.; Carpenter, C.R.; Liu, S.W.; Kennedy, M. Implementation of Delirium Screening in the Emergency Department: A Qualitative Study with Early Adopters. Journal of the American Geriatrics Society 2024, 72, 3753–3762. [Google Scholar] [CrossRef]
- Zarour, S.; Weiss, Y.; Kiselevich, Y.; Iacubovici, L.; Karol, D.; Shaylor, R.; Davydov, T.; Matot, I.; Cohen, B. The Association between Midazolam Premedication and Postoperative Delirium - a Retrospective Cohort Study. Journal of Clinical Anesthesia 2024, 92, 111113. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, C.R.; Hammouda, N.; Linton, E.A.; Doering, M.; Ohuabunwa, U.K.; Ko, K.J.; Hung, W.W.; Shah, M.N.; Lindquist, L.A.; Biese, K.; et al. Delirium Prevention, Detection, and Treatment in Emergency Medicine Settings: A Geriatric Emergency Care Applied Research (GEAR) Network Scoping Review and Consensus Statement. Acad Emerg Med 2021, 28, 19–35. [Google Scholar] [CrossRef]
- Skains, R.M.; Hayes, J.M.; Selman, K.; Zhang, Y.; Thatphet, P.; Toda, K.; Hayes, B.D.; Tayes, C.; Casey, M.F.; Moreton, E.; et al. Emergency Department Programs to Support Medication Safety in Older Adults: A Systematic Review and Meta-Analysis. JAMA Netw Open 2025, 8, e250814. [Google Scholar] [CrossRef]
- Zaher-Sánchez, S.; Satústegui-Dordá, P.J.; Ramón-Arbués, E.; Santos-Sánchez, J.A.; Aguilón-Leiva, J.J.; Pérez-Calahorra, S.; Juárez-Vela, R.; Sufrate-Sorzano, T.; Angulo-Nalda, B.; Garrote-Cámara, M.E.; et al. The Management and Prevention of Delirium in Elderly Patients Hospitalised in Intensive Care Units: A Systematic Review. Nursing Reports 2024, 14, 3007–3022. [Google Scholar] [CrossRef]
- European Delirium Association. American Delirium Society The DSM-5 Criteria, Level of Arousal and Delirium Diagnosis: Inclusiveness Is Safer. BMC Med 2014, 12, 141. [Google Scholar] [CrossRef]
- Al Huraizi, A.R.; Al-Maqbali, J.S.; Al Farsi, R.S.; Al Zeedy, K.; Al-Saadi, T.; Al-Hamadani, N.; Al Alawi, A.M. Delirium and Its Association with Short- and Long-Term Health Outcomes in Medically Admitted Patients: A Prospective Study. J. Clin. Med. 2023, 12. [Google Scholar] [CrossRef]
- Billig, A.E.; Lampert, M.A.; Guerra, R.R.; Steigleder, N.E. Delirium in the elderly admitted to an emergency hospital service. Rev Bras Enferm 2022, 75 Suppl 4, e20210054. [Google Scholar] [CrossRef] [PubMed]
- Soler-Sanchis, A.; Martínez-Arnau, F.M.; Sánchez-Frutos, J.; Pérez-Ros, P. Clinical Risk Group as a Predictor of Mortality in Delirious Older Adults in the Emergency Department. Exp Gerontol 2023, 174, 112129. [Google Scholar] [CrossRef]
- Li, B.; Zhang, Z.; Li, K.; Deng, Y. The Effectiveness of a Modified Manchester Triage System for Geriatric Patients: A Retrospective Quantitative Study. Nurs Open 2024, 11, e70024. [Google Scholar] [CrossRef] [PubMed]
- Soler-Sanchis, A.; Martínez-Arnau, F.M.; Sánchez-Frutos, J.; Pérez-Ros, P. Identification through the Manchester Triage System of the Older Population at Risk of Delirium: A Case-Control Study. J Clin Nurs 2022. [Google Scholar] [CrossRef]
- Lee, S.; Howard, M.A.; Han, J.H. Delirium and Delirium Prevention in the Emergency Department. Clinics in Geriatric Medicine 2023, 39, 535–551. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Angel, C.; Han, J.H. Succinct Approach to Delirium in the Emergency Department. Curr Emerg Hosp Med Rep 2021, 9, 11–18. [Google Scholar] [CrossRef]
- Anand, A.; Maclullich, A. Delirium in Older Adults. Medicine 2024, 52, 671–676. [Google Scholar] [CrossRef]
- Bonfichi, A.; Ceresa, I.F.; Piccioni, A.; Zanza, C.; Longhitano, Y.; Boudi, Z.; Esposito, C.; Savioli, G. A Lethal Combination of Delirium and Overcrowding in the Emergency Department. J Clin Med 2023, 12, 6587. [Google Scholar] [CrossRef]
- Dahlstrom, E.B.; Han, J.H.; Healy, H.; Kennedy, M.; Arendts, G.; Lee, J.; Carpenter, C.; Lee, S. Delirium Prevention and Treatment in the Emergency Department (ED): A Systematic Review Protocol. BMJ Open 2020, 10, e037915. [Google Scholar] [CrossRef]
- Sun, C.; Hirata, Y.; Kawahara, T.; Kawashima, M.; Sato, M.; Nakajima, J.; Anraku, M. Diagnosis of Respiratory Sarcopenia for Stratifying Postoperative Risk in Non-Small Cell Lung Cancer. JAMA Surg 2025, 160, 66–73. [Google Scholar] [CrossRef]
- Casey, M.F.; Elder, N.M.; Fenn, A.; Niznik, J.; Khoujah, D.; Cole, J.B.; Cardon, Z.; Ding, M.; Goukasian, N.; Moreton, E.; et al. Comparative Safety of Medications for Severe Agitation: A Geriatric Emergency Department Guidelines 2.0 Systematic Review. J Am Geriatr Soc 2025, 73, 2893–2904. [Google Scholar] [CrossRef] [PubMed]
- Carayannopoulos, K.L.; Alshamsi, F.; Chaudhuri, D.; Spatafora, L.; Piticaru, J.; Campbell, K.; Alhazzani, W.; Lewis, K. Antipsychotics in the Treatment of Delirium in Critically Ill Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit Care Med 2024, 52, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Cheng, S.-Y.; Paiva, C.E. Pharmacologic Management of End-of-Life Delirium: Translating Evidence into Practice. Cancers (Basel) 2024, 16, 2045. [Google Scholar] [CrossRef]
- Huang, J.; Zheng, H.; Zhu, X.; Zhang, K.; Ping, X. The Efficacy and Safety of Haloperidol for the Treatment of Delirium in Critically Ill Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Med (Lausanne) 2023, 10, 1200314. [Google Scholar] [CrossRef]
- Wu, Y.-C.; Tseng, P.-T.; Tu, Y.-K.; Hsu, C.-Y.; Liang, C.-S.; Yeh, T.-C.; Chen, T.-Y.; Chu, C.-S.; Matsuoka, Y.J.; Stubbs, B.; et al. Association of Delirium Response and Safety of Pharmacological Interventions for the Management and Prevention of Delirium: A Network Meta-Analysis. JAMA Psychiatry 2019, 76, 526–535. [Google Scholar] [CrossRef]
- Zangani, C.; Giordano, B.; Stein, H.-C.; Bonora, S.; Ostinelli, E.G.; D’Agostino, A. Efficacy of Tiapride in the Treatment of Psychiatric Disorders: A Systematic Review. Hum Psychopharmacol 2022, 37, e2842. [Google Scholar] [CrossRef]
- Vollmer, N.J.; Wieruszewski, E.D.; Nei, A.M.; Mara, K.C.; Rabinstein, A.A.; Brown, C.S. Impact of Continuous Infusion Ketamine Compared to Continuous Infusion Benzodiazepines on Delirium in the Intensive Care Unit. J Intensive Care Med 2024, 39, 1204–1211. [Google Scholar] [CrossRef]
- van der Hoeven, A.E.; Bijlenga, D.; van der Hoeven, E.; Schinkelshoek, M.S.; Hiemstra, F.W.; Kervezee, L.; van Westerloo, D.J.; Fronczek, R.; Lammers, G.J. Sleep in the Intensive and Intermediate Care Units: Exploring Related Factors of Delirium, Benzodiazepine Use and Mortality. Intensive Crit Care Nurs 2024, 81, 103603. [Google Scholar] [CrossRef] [PubMed]
- Xue, X.; Ma, X.; Zhao, B.; Liu, B.; Zhang, J.; Li, Z.; Li, H.; Liu, X.; Zhao, S. The Impact of Remimazolam Compared to Propofol on Postoperative Delirium: A Systematic Review and Meta-Analysis. Minerva Anestesiol 2025, 91, 70–79. [Google Scholar] [CrossRef]
- Simon, E.L.; Smalley, C.M.; Muir, M.; Mangira, C.M.; Pence, R.; Wahi-Singh, B.; Delgado, F.; Fertel, B.S. Agitation Management in the Emergency Department with Physical Restraints: Where Do These Patients End Up? West J Emerg Med 2023, 24, 454–460. [Google Scholar] [CrossRef]
- Sullivan, S.M.; Dewey, B.N.; Jarrell, D.H.; Vadiei, N.; Patanwala, A.E. Comparison of Phenobarbital-Adjunct versus Benzodiazepine-Only Approach for Alcohol Withdrawal Syndrome in the ED. Am J Emerg Med 2019, 37, 1313–1316. [Google Scholar] [CrossRef] [PubMed]
- White, N.; Bazo-Alvarez, J.C.; Koopmans, M.; West, E.; Sampson, E.L. Understanding the Association between Pain and Delirium in Older Hospital Inpatients: Systematic Review and Meta-Analysis. Age Ageing 2024, 53, afae073. [Google Scholar] [CrossRef]
- Leong, A.Y.; Edginton, S.; Lee, L.A.; Jaworska, N.; Burry, L.; Fiest, K.M.; Doig, C.J.; Niven, D.J. The Association between Pain, Analgesia, and Delirium among Critically Ill Adults: A Systematic Review and Meta-Analysis. Intensive Care Med 2025, 51, 342–352. [Google Scholar] [CrossRef]
- Riccardi, A.; Guarino, M.; Serra, S.; Spampinato, M.D.; Vanni, S.; Shiffer, D.; Voza, A.; Fabbri, A.; De Iaco, F. Study and Research Center of the Italian Society of Emergency Medicine Narrative Review: Low-Dose Ketamine for Pain Management. J Clin Med 2023, 12, 3256. [Google Scholar] [CrossRef] [PubMed]
- Jia, B.; Zhou, S.; Li, J.; Wan, L.; Zhou, Y.; Cui, Y. Risk of Drug-Induced Delirium in Older Patients- a Pharmacovigilance Study of FDA Adverse Event Reporting System Database. Expert Opin Drug Saf 2025, 24, 79–87. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
ROC curve for logistic regression model.
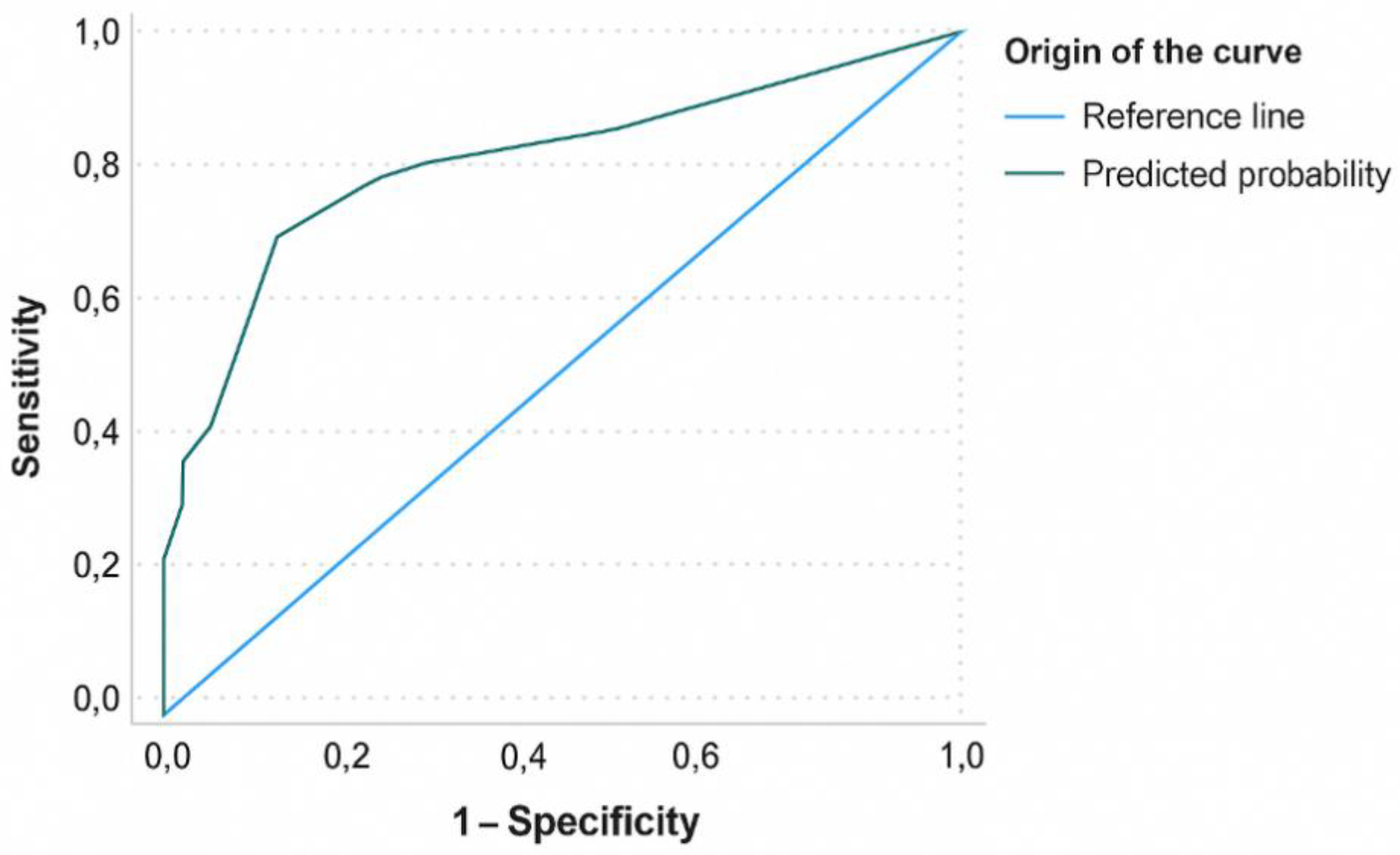

Table 1.
Participant characteristics according to hospital admission.
| Hospitalisation | Total | OR (95% CI) | P value2 | ||
|---|---|---|---|---|---|
| Yes (n = 91)1 | No (n = 62)1 | (n=153)1 | |||
| Age in years, mean (SD) | 83.82 (7.76) | 84.35 (7.60) | 84.04 (7.68) | — | 0.605 |
| Sex | |||||
| Male | 50.5 (46) | 50 (31) | 50.3 (77) | 0.97 (0.51-1.86) | 0.947 |
| Female | 49.5 (45) | 50 (31) | 49.7 (76) | ||
| MTS priority | |||||
| Priority IV (standard) | 25.3 (23) | 40.3 (25) | 31.4 (48) | 0.50 (0.25-1.00) | 0.049 |
| Priority III (urgent) | 68.1 (62) | 53.2 (33) | 62.1 (95) | 1.88 (0.96-3.65) | 0.062 |
| Priority II (very urgent) | 6.6 (6) | 6.5 (4) | 6.5 (10) | 1.02 (0.27-3.78) | 0.972 |
| MTS diagram | |||||
| Unwell adult | 51.6 (47) | 59.7 (37) | 54.9 (84) | — | 0.572 |
| Behaving strangely | 14.3 (13) | 16.1 (10) | 15.0 (23) | — | |
| Shortness of breath | 7.7 (7) | 9.7 (6) | 8.5 (13) | — | |
| Urinary problems | 3.3 (3) | 4.8 (3) | 3.9 (6) | — | |
| Mental illness | 2.2 (2) | 1.6 (1) | 2.0 (3) | — | |
| Limb problems | 13.2 (12) | 3.2 (2) | 9.2 (14) | — | |
| Abdominal pain | 4.4 (4) | 1.6 (1) | 3.3 (5) | — | |
| Infections | 1.1 (1) | 0 | 0.7 (1) | — | |
| Other | 2.2 (2) | 3.2 (2) | 2.6 (4) | — | |
| Clinical diagnosis | |||||
| No underlying disease | 35.2 (32) | 58.1 (36) | 44.4 (68) | — | 0.012 |
| Cardiac disease | 5.5 (5) | 0 (0) | 3.3 (5) | — | |
| Neurological disease | 7.7 (7) | 12.9 (8) | 9.8 (15) | — | |
| Renal disease | 11 (10) | 9.7 (6) | 10.5 (16) | — | |
| Respiratory disease | 5.5 (5) | 6.5 (4) | 5.9 (9) | — | |
| GI disease | 4.4 (4) | 3.2 (2) | 3.9 (6) | — | |
| Infection | 30.8 (28) | 9.7 (6) | 22.2 (34) | — | |
| Treatment | |||||
| ≥2 active ingredients | 73.6 (67) | 25.8 (16) | 54.2 (83) | 8.02 (3.84-16.74) | <0.001 |
| Total drugs, mean (SD) | 2.92 (2.02) | 0.95 (1.16) | 2.12 (1.98) | — | <0.001 |
| Analgesics | 67.0 (61) | 29 (18) | 51.6 (79) | 4.97 (2.46-10.02) | <0.001 |
| Antiemetics | 5.5 (5) | 0 | 3.3 (5) | 1.06 (1.00-1.11) | 0.061 |
| Antipsychotics | 40.7 (37) | 6.5 (4) | 26.8 (41) | 9.93 (3.32-29.73) | <0.001 |
| Benzodiazepines | 14.3 (13) | 3.2 (2) | 9.8 (15) | 5.00 (1.08-23.00) | 0.024 |
| Antibiotics | 47.3 (43) | 17.7 (11) | 35.3 (54) | 4.15 (1.92-8.97) | <0.001 |
| Corticosteroids | 8.8 (8) | 4.8 (3) | 7.2 (11) | 1.89 (0.48-7.44) | 0.353 |
| Antidepressants | 8.8 (8) | 0 | 5.2 (8) | 0.57 (0.49-0.65) | 0.016 |
| Antihypertensives | 2.2 (2) | 0 | 1.3 (2) | 0.58 (0.51-0.67) | 0.240 |
| Diuretics | 11.0 (10) | 3.2 (2) | 7.8 (12) | 3.07 (0.78-17.52) | 0.080 |
| Anti-ulcer drugs | 5.5 (5) | 1.6 (1) | 3.9 (6) | 3.54 (0.40-31.12) | 0.225 |
| Anticonvulsants | 4.4 (4) | 1.6 (1) | 3.3 (5) | 2.80 (0.30-25.71) | 0.342 |
| Antiarrhythmics | 2.2 (2) | 0 | 1.3 (2) | 0.58 (0.51-0.67) | 0.240 |
| Antidiabetics | 2.2 (2) | 1.6 (1) | 2.0 (3) | 1.37 (0.12-15.45) | 0.798 |
| Bronchodilators | 2.2 (2) | 3.2 (2) | 2.6 (4) | 0.67 (0.09-4.91) | 0.696 |
| Antiplatelets | 8.8 (8) | 0 | 5.2 (8) | 0.57 (0.49-0.65) | 0.016 |
| Others | 2.2 (2) | 3.2 (2) | 2.6 (4) | 0.67 (0.09-4.91) | 0.696 |
1 All data are presented as percentage (number) of participants unless otherwise specified. 2 Chi-squared p values for categorical variables and Mann-Whitney U p values for continuous variables (age and total drugs administered). Abbreviations: CI, confidence interval; GI, gastrointestinal; MTS, Manchester Triage System; OR, odds ratio.
Table 2.
Analysis of active ingredients for the most representative families of drugs related to hospital admission.
Table 2.
Analysis of active ingredients for the most representative families of drugs related to hospital admission.
| Hospitalisation | Total | OR (95% CI) | P value2 | ||
|---|---|---|---|---|---|
| Yes (n = 91)1 | No (n = 62)1 | (n=153)1 | |||
| Analgesics | 67.0 (61) | 29.0 (18) | 51.6 (79) | 4.97 (2.46-10.02) | <0.001 |
| Metamizole (≥ 2 g) | 11.0 (10) | 1.6 (1) | 7.2 (11) | 7.53 (0.93-60.42) | 0.028 |
| Paracetamol (≥ 1 g) | 53.8 (49) | 25.8 (16) | 42.5 (65) | 3.35 (1.66-6.77) | <0.001 |
| Dexketoprofen (≥ 50 mg) | 2.2 (2) | 1.6 (1) | 2.0 (3) | 1.37 (0.12-15.54) | 0.798 |
| Tramadol (≥ 100 mg) | 3.3 (3) | 1.6 (1) | 2.6 (4) | 2.08 (0.21-20.46) | 0.522 |
| Ketamine | 14.3 (13) | 4.8 (3) | 10.5 (16) | 3.27 (0.89-12.02) | 0.061 |
| < 50 mg | 14.3 (13) | 3.2 (2) | 9.8 (15) | — | 0.040 |
| ≥ 50 mg | 0 | 1.6 (1) | 0.7 (1) | — | 0.972 |
| Morphine | 6.6 (6) | 0 | 3.9 (6) | 0.57 (0.50-0.66) | 0.039 |
| < 50 mg | 5.5 (5) | 0 | 3.3 (5) | — | 0.167 |
| ≥ 50 mg | 1.1 (1) | 0 | 0.7 (1) | — | |
| Fentanyl (< 150 mg) | 1.1 (1) | 0 | 0.7 (1) | 0.59 (0.52-0.67) | 0.408 |
| Antipsychotics | 40.7 (37) | 6.5 (4) | 26.8 (41) | 9.93 (3.32-29.73) | <0.001 |
| Haloperidol | 20.9 (19) | 4.8 (3) | 14.4 (22) | 5.19 (1.46-18.39) | 0.006 |
| < 15 mg | 19.8 (18) | 4.8 (3) | 13.7 (21) | — | 0.020 |
| ≥ 15 mg | 1.1 (1) | 0 | 0.7 (1) | — | |
| Olanzapine | 2.2 (2) | 0 | 1.3 (2) | 0.59 (0.51-0.67) | 0.240 |
| < 15 mg | 1.1 (1) | 0 | 0.7 (1) | — | 0.501 |
| ≥ 15 mg | 1.1 (1) | 0 | 0.7 (1) | — | |
| Risperidone | 2.2 (2) | 0 | 1.3 (2) | 0.58 (0.51-0.67) | 0.240 |
| < 5 mg | 1.1 (1) | 0 | 0.7 (1) | — | 0.501 |
| ≥ 5 mg | 1.1 (1) | 0 | 0.7 (1) | — | |
| Tiapride | 19.8 (18) | 6.5 (4) | 14.4 (22) | 3.57 (1.14-11.14) | 0.021 |
| < 100 mg | 3.3 (3) | 0 | 2.0 (3) | — | 0.055 |
| ≥ 100 mg | 16.5 (15) | 6.5 (4) | 12.4 (19) | — | |
| Levomepromazine (≥ 125 mg) | 1.1 (1) | 0 | 0.7 (1) | 0.59 (0.51-0.67) | 0.408 |
| Benzodiazepines | 14.3 (13) | 3.2 (2) | 9.8 (15) | 5.00 (1.08-23.00) | 0.024 |
| Diazepam (≥ 5 mg) | 3.3 (3) | 1.6 (1) | 2.6 (4) | 2.08 (0.21-20.46) | 0.522 |
| Alprazolam (≥ 1 mg) | 2.2 (2) | 0 | 1.3 (2) | 0.58 (0.51-0.67) | 0.240 |
| Lorazepam (≥ 1 mg) | 2.2 (2) | 1.6 (1) | 2.0 (3) | 1.37 (0.12-15.45) | 0.798 |
| Midazolam | 4.4 (4) | 0 | 2.6 (4) | 0.58 (0.51-0.67) | 0.094 |
| < 3 mg | 1.1 (1) | 0 | 0.7 (1) | — | 0.247 |
| ≥ 3 mg | 3.3 (3) | 0 | 2.0 (3) | — | 0.024 |
| Clorazepate (≥ 10 mg) | 1.1 (1) | 0 | 0.7 (1) | 0.59 (0.51-0.67) | 0.408 |
| Bromazepam (≥ 1.5 mg) | 1.1 (1) | 0 | 0.7 (1) | 0.59 (0.51-0.67) | 0.408 |
1 All data are presented as percentage (number) of participants unless otherwise specified. 2 Chi-squared p values. Abbreviations: CI, confidence interval; OR, odds ratio.
Table 3.
Analysis of active ingredients for the most representative families of drugs related to hospital admission.
Table 3.
Analysis of active ingredients for the most representative families of drugs related to hospital admission.
| No underlying disease (n = 68) |
Heart disease (n = 5) |
Neurological disease (n = 15) |
Kidney disease (n = 16) | Respiratory disease (n = 9) |
GI disease (n = 6) |
Infection (n = 34) |
Total (n = 153) |
P value1 | |
|---|---|---|---|---|---|---|---|---|---|
| Analgesics | 39.7 (27) | 60.0 (3) | 33.3 (5) | 62.5 (10) | 55.6 (5) | 83.3 (5) | 70.6 (24) | 51.6 (79) | 0.028 |
| Antiemetics | 10.3 (7) | 40.0 (2) | 6.7 (1) | 25.0 (4) | 22.2 (2) | 33.3 (2) | 26.5 (9) | 17.6 (27) | 0.170 |
| Antipsychotics | 22.1 (15) | 60.0 (3) | 20.0 (3) | 25.0 (4) | 22.2 (2) | 16.7 (1) | 38.2 (13) | 26.8 (41) | 0.355 |
| Antibiotics | 0 | 80.0 (4) | 13.3 (2) | 68.8 (11) | 66.7 (6) | 33.3 (2) | 58.3 (29) | 35.3 (54) | <0.001 |
| Corticosteroids | 4.4 (3) | 0 | 0 | 0 | 33.3 (3) | 0 | 14.7 (5) | 7.2 (11) | 0.013 |
| Antidepressants | 2.9 (2) | 20.0 (1) | 0 | 12.5 (2) | 0 | 0 | 8.8 (3) | 5.2 (8) | 0.306 |
| Antihypertensives | 1.5 (1) | 0 | 6.7 (1) | 0 | 0 | 0 | 0 | 1.3 (2) | 0.639 |
| Diuretics | 1.5 (1) | 60.0 (3) | 0 | 12.5 (2) | 22.2 (2) | 16.7 (1) | 8.8 (3) | 7.8 (12) | <0.001 |
| Anti-ulcer drugs | 1.5 (1) | 0 | 6.7 (1) | 0 | 11.1 (1) | 33.3 (2) | 2.9 (1) | 3.9 (6) | 0.008 |
| Benzodiazepines | 10.3 (7) | 0 | 13.3 (2) | 12.5 (2) | 0 | 0 | 11.8 (4) | 9.8 (15) | 0.847 |
| Anticonvulsants | 2.9 (2) | 0 | 6.7 (1) | 6.3 (1) | 0 | 0 | 2.9 (1) | 3.3 (5) | 0.944 |
| Antiarrhythmics | 0 | 0 | 0 | 6.3 (1) | 11.1 (1) | 0 | 0 | 1.3 (2) | 0.076 |
| Antidiabetics | 1.5 (1) | 0 | 0 | 6.3 (1) | 0 | 0 | 2.9 (1) | 2.0 (3) | 0.870 |
| Bronchodilators | 1.5 (1) | 0 | 0 | 0 | 0 | 22.2 (2) | 2.9 (1) | 2.6 (4) | 0.020 |
| Antiplatelets | 1.5 (1) | 0 | 0 | 18.8 (3) | 0 | 16.7 (1) | 8.8 (3) | 5.2 (8) | 0.064 |
| Others | 2.9 (2) | 0 | 6.7 (1) | 0 | 0 | 0 | 2.9 (1) | 2.6 (4) | 0.922 |
1 Chi-square p values. Abbreviation: GI: gastrointestinal.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



