
Submitted:
12 June 2025
Posted:
13 June 2025
You are already at the latest version
Abstract
Introduction: Delirium is a common and debilitating clinical complication among ICU patients. Despite its prevalence, there are insufficient data to support or refute the routine use of atypical antipsychotics since the existing evidence remains sparse and inconclusive. The objective of the present study was to evaluate whether pre-ICU administration of the atypical antipsychotic olanzapine is associated with a differential time to delirium resolution relative to the control condition. Methods: In this emulated clinical trial, we utilized the MIMIC-IV v3.1 database, which contains deidentified health records from approximately 65,000 ICU patients, to derive a cohort of patients with a positive delirium screening (CAM-ICU) within 24 hours of ICU admission. We excluded patients who received any antipsychotic other than olanzapine prior to ICU admission. We performed propensity score matching using logistic regression and nearest-neighbor matching (1:1, caliper = 0.2) to balance covariates between the olanzapine and control groups. The primary outcome was time to delirium resolution, defined as the first negative CAM-ICU assessment. A Cox proportional hazards model, adjusted for multiple covariates and incorporating age as a time-dependent variable, was used to examine the association between olanzapine use and delirium resolution. Interaction terms were included to evaluate effect modification by age and gender. Results: A total of 5,070 patients with a positive delirium screening within 24 hours and no exposure to other antipsychotics met eligibility criteria; 421 olanzapine users were matched to 421 controls using propensity score matching. Covariate balance was achieved (all standardized mean differences < 0.1), and no multicollinearity was detected (all VIFs < 2). Pre-ICU olanzapine use was associated with a 27% decrease in the likelihood of delirium resolution (HR = 0.73; 95% CI: 0.63–0.86; p < 0.001). A significant interaction with age indicated that the negative impact of olanzapine on delirium resolution increased with advancing age, translating to a 2.4% increase in the risk of prolonged delirium resolution for every 10-year increase in age. There was no modification of the association according to gender. Discussion: The negative effect of olanzapine on ICU delirium resolution - in the elderly in particular - presented in this study is in line with the results of our earlier study showing a negative effect (i.e., prolonged ICU stay) in patients receiving quetiapine relative to the control condition. As both olanzapine and quetiapine have a distinctly strong anticholinergic effect relative to the other antipsychotic agents used in the ICU, their use is not advised for the treatment of delirium.
Keywords:
delirium
; olanzapine
; atypical antipsychotics
; ICU
; critical care
1. Introduction
Delirium is a disruption of attention and awareness that develops over a short period of time, typically hours to days. This debilitating condition is accompanied by at least one additional cognitive disturbance, such as memory deficit, disorientation, language impairment, or perceptual disturbance, and is not better explained by a preexisting neurocognitive disorder [1].
Though the median duration of delirium in the ICU is 4 days, the condition can last less than 24 hours and beyond 2 weeks [2,3]. Indeed, time to delirium resolution in the ICU is a robust clinical endpoint as it aligns with enhanced research rigor and patient-centered care. The measure is highly correlated with other outcomes as longer delirium duration is associated with increased length of ICU stay, higher mortality, long-term cognitive impairment and functional decline[3]. Compared to a cross-sectional, binary outcome, such as presence or absence of delirium, the measure of delirium persistence over time is more statistically robust and informative.
Current strategies for treating ICU delirium remain profoundly insufficient. In fact, the 2025 focused update [4] to the PADIS guidelines by the Society of Critical Care Medicine was not able to make a recommendation regarding routine use of antipsychotics for the prevention or treatment of delirium in adult ICU patients - of only eight randomized controlled trials evaluating the efficacy of antipsychotics for the treatment of delirium in the ICU, haloperidol was administered in six, and the overall conclusion was that it does not provide any benefit in reducing time to delirium resolution, ICU length of stay, hospital length of stay, or duration of mechanical ventilation, though there may be limited evidence (i.e., low certainty) that the treatment decreases mortality and increases the number of delirium-free days. Data on the atypical antipsychotics —such as olanzapine, quetiapine, or risperidone— were found to be sparse and heterogeneous, preventing any conclusions about their efficacy.
The sparsity of research examining the use of atypical antipsychotics for the treatment of delirium in the ICU underscores the need for more targeted research. Hence, the objective of the present study was to investigate whether pre-ICU administration of olanzapine is associated with a differential time to delirium resolution relative to the control condition (i.e., no olanzapine administration). We utilized an emulated clinical trial framework that approximates causal inference from observational data, accounting for confounding and treatment assignment.
2. Results
2.1. Participant Flow
Figure 1 outlines the cohort selection process for this emulated clinical trial evaluating olanzapine use prior to ICU admission. From an initial 94,458 ICU admissions in the MIMIC database, 65,366 first-time ICU admissions were identified. Among these, 8,951 patients had a positive delirium screening within 24 hours of ICU admission. After excluding patients who received first- or second-generation antipsychotics other than olanzapine (n = 3,881), a total of 5,070 patients met the final eligibility criteria. Of these, 427 received olanzapine prior to ICU admission and 4,643 did not. For comparative analysis that includes patients with complete datasets, a propensity score–matched sample was generated, resulting in 421 patients in both the olanzapine and control groups.
2.2. Propensity Score Matching
The variance inflation factor (VIF) values for all covariates were below 2, indicating no evidence of problematic multicollinearity. Therefore, all variables were retained for propensity score estimation. Following the propensity score matching procedure, 421 cases were matched to 421 controls, resulting in a matched sample of 842 individuals. Prior to matching, the overall distance between the groups was 0.5073. Several covariates displayed substantial imbalances, including age (SMD = 0.43), dementia (SMD = 0.33), hypertension (SMD = 0.13), and benzodiazepine use (SMD = 0.17). Following the matching procedure, the overall distance was substantially reduced to -0.0003, confirming successful alignment of the treated and control cohorts for subsequent analyses. All the covariates achieved adequate balance of absolute SMDs below 0.1. For results of the propensity matching procedure, please see Figure 2 and Table 1.
2.3. Cox Proportional Hazard Analysis
In a time-varying Cox proportional hazards model evaluating predictors of time to delirium resolution among 842 matched ICU patients (600 events), pre-ICU olanzapine use was significantly associated with delayed delirium resolution, with a 27% reduction in the hazard of resolution (HR = 0.73; 95% CI: 0.63 to 0.86; p < 0.001) (Table 2). Other factors associated with significantly delayed resolution included propofol use (HR = 0.60; p < 0.001), sepsis (HR = 0.71; p = 0.0018), stroke (HR = 0.77; p = 0.009), and vasopressor use (HR = 0.76; p = 0.0039). Female gender was also associated with delayed resolution (HR = 0.81; p = 0.016), while dementia approached statistical significance (p = 0.056). Other covariates—including diabetes and baseline vital signs—were not significantly associated with time to resolution. The time-varying effect of age (modeled as age × log(time)) was also nonsignificant. Model diagnostics indicated good performance (concordance = 0.625), and global tests confirmed overall model significance (likelihood ratio test p < 0.001).
The Kaplan-Meier survival curve (Figure 3) depicts the probability of continued delirium (i.e., delirium persistence) over time among ICU patients stratified by pre-ICU olanzapine exposure. Patients who received olanzapine prior to ICU admission (orange line) had a higher probability of persistent delirium at nearly all time points compared to those who did not receive olanzapine (green line). Although the initial drop in both curves suggests that most delirium resolved relatively quickly, the slower decline and prolonged tail of the orange curve indicates that olanzapine exposure was associated with delayed resolution of delirium. The green curve continues further on the x-axis, reflecting that more patients in the non-olanzapine group remained under observation at later time points, either due to slower censoring or longer follow-up. This visual finding aligns with the Cox regression results, which showed a significantly reduced delirium resolution in the olanzapine group.
2.4. Subgroup Analysis
The effect of olanzapine varied significantly by age over time, as shown by a positive interaction between olanzapine and age modeled as a time-dependent covariate (HR = 1.0024 per unit of age × log(time), p = 0.023), suggesting that the negative impact of olanzapine on delirium resolution becomes more pronounced with increasing age (Figure 4). This translates to a 2.4% increase in the risk of prolonged delirium resolution for every 10-year increase in age. There was no evidence of effect modification by gender (olanzapine × gender interaction: HR = 1.08, p = 0.61).
3. Discussion
We report that pre-ICU administration of olanzapine results in a 27% increase in a risk of prolonged delirium in ICU patients. This finding was more pronounced in the elderly, with a 2.4% increase in the risk of prolonged delirium resolution for every 10-year increase in age. Based on these results, we emphasize the importance of careful antipsychotic selection – in the elderly in particular – and provide support for deprescribing strategies aimed at minimizing anticholinergic burden prior to ICU admission.
Olanzapine is an atypical antipsychotic with a unique mechanism of action. Its therapeutic effects are linked to the antagonism of D₂ and 5-HT₂A receptors. Though this receptor binding profile contributes to its efficacy and in parallel minimizes extrapyramidal side effects, the medication also exhibits a strong binding to the muscarinic acetylcholine M₁ through M₅ receptors which contributes to its anticholinergic side effects.
Relative to the other atypical antipsychotics (Figure 5), clozapine exhibits the strongest muscarinic binding [5,6], resulting in its well-recognized anticholinergic burden. Olanzapine and the active metabolite of quetiapine, norquetiapine, also show very strong binding to the M1, M3, and M5 receptor subtypes[7,8]. The pronounced anticholinergic effect of quetiapine is due to the moderate binding of the parent drug as well as the strong binding of norquetiapine. In contrast, paliperidone, risperidone, and ziprasidone exhibit negligible muscarinic receptor binding, resulting in a lack of anticholinergic side effects.
Antagonism of distinct muscarinic receptor subtypes results in differential therapeutic and adverse effect profiles. The function of the M1 receptor, in particular, is of critical importance in ICU delirium management. Gq/11-coupled, it is densely expressed in the cortex and hippocampus where it modulates cognitive processing, including attention, learning, and memory [9]. On the cellular level, the receptor enhances neuronal excitability via intracellular calcium signaling, thereby facilitating synaptic plasticity and long-term potentiation (LTP) [10,11]. Its blockade or knockout has detrimental effects and results in associative learning task deficits [12]. The remaining M2-M5 subtypes do not seem to contribute to the cognitive deficits - the M2 and M4 receptors regulate tachycardia and possibly extrapyramidal symptoms[13], the M3 receptor mediates peripheral anticholinergic effects such as dry mouth, constipation, urinary retention, and blurred vision[11], while the M5 receptor is implicated in reward processing, cerebral blood flow regulation, and potentially substance use behavior[14].
The antagonism of the M1 receptor is, hence, clinically relevant in the selection of antipsychotics for the treatment of delirium. In fact, we have recently applied Bayesian generalized additive modeling methodology to assess the length of ICU stay among patients with delirium treated with quetiapine, demonstrating that quetiapine administration prolongs ICU stay relative to the control (manuscript in revision). As both olanzapine and quetiapine have distinctly strong anticholinergic effects, we hypothesize that their unfavorable effects in the management of delirium are due to this particular mechanism.
In the present study the association between the risk of prolonged delirium and olanzapine administration was particularly pronounced in the elderly. This population is at a higher risk for cholinergic disruption, in large part due to diminished connectivity that affects association systems and cholinergic fibers[15]. Adding to this risk is the finding that patients in the ICU are at a higher risk for delirium, in part due to impaired mobility, and the use of opioids and benzodiazepines[16,17]. Hence, elderly patients with delirium who are administered olanzapine (or quetiapine) in the ICU essentially have three sources of increased anticholinergic burden: their age-related pathophysiology, factors related to the ICU stay, and high M1 receptor binding of olanzapine or quetiapine (for Ki values, see Figure 5).
Unfortunately, at this time, treating delirium with antipsychotics does not offer any benefit, and, depending on the specific medication, may, in fact, result in harm. For example, the MIND-USA (Modifying the Impact of ICU-Associated Neurological Dysfunction-USA) randomized controlled trial investigated whether antipsychotics improve outcomes in ICU patients with delirium. The investigators randomized 566 critically ill adults with acute delirium in the ICU (as determined by CAM-ICU) to haloperidol, ziprasidone, and placebo, reporting that neither antipsychotic resulted in a reduction of delirium or coma duration compared to placebo. Hence, while studies to date generally showed no benefit of haloperidol in delirium management [4], results presented here caution against the use of olanzapine. We concluded the same for quetiapine based on our earlier analysis (manuscript in revision).
The present study had limitations and strengths. Though we used a single center MIMIC database, which limits generalizability, the dataset is validated, robust and well-curated. There are important variables that are not available in the dataset, for example, baseline cognitive status and sleep quality, that may result in residual confounding despite our robust propensity score matching procedure. Though the patients were identified using the CAM-ICU routine clinical assessment, which enhances the external validity of real-world ICU practice, the measure is binary and does not assess the severity of delirium, or provide data on hypoactive and hyperactive subtypes. Finally, transparency and reproducibility of the present study is greatly enhanced due to the use of open-source packages and a public dataset.
Future studies should ideally be prospective, conducted in a multicenter fashion, with the stratification of study participants according to the delirium subtype. Based on the research findings from our group, we stress the importance of incorporating a measure of anticholinergic burden in the design of future clinical studies.
In summary, the results of this study show an significantly increased risk of delirium persistence in ICU patients receiving onlanzepine. The present study not only advances clinical practice, but also prioritizes the importance of cholinergic function preservation in ICU delirium patients; in the elderly subpopulation in particular.
4. Materials and Methods
4.1. Data Source
The data were sourced from version 3.1 of the Medical Information Mart for Intensive Care (MIMIC)-IV database, which contains health records of approximately 65,000 ICU patients treated at Beth Israel Deaconess Medical Center in Boston, Massachusetts, USA, between the years 2008 and 2022. The database was developed by the Massachusetts Institute of Technology Lab for Computational Physiology in collaboration with the Beth Israel Deaconess Medical Center. De-identified data are publicly available on PhysioNet upon completion of required training and acceptance of the Data Use Agreement. The release of the de-identified data was approved by the Beth Israel Deaconess Medical Center and the Massachusetts Institute of Technology Institutional Review Boards, with a waiver of individual patient informed consent.
4.2. Study Design
Merging data from various modules by integrating patient identifiers and hospital stay information, we formed a cohort of patients based on a positive delirium screening within 24 hours of ICU admission. The nursing staff completed the screening at least two times per day using the Confusion Assessment Method for the ICU (CAM-ICU) [18]. The assessment includes four components: (1) an acute change in mental status or fluctuating course, (2) inattention, (3) disorganized thinking, and (4) altered level of consciousness. A positive CAM-ICU assessment is made when a patient exhibits the first and second features, along with either the third or fourth feature. The assessment is recorded as “positive”, “negative”, or “unable to assess”.
Only patients’ first hospital admission data was used in the event a patient was admitted multiple times. Patients receiving an antipsychotic other than olanzapine were excluded. The cohort with a positive CAM-ICU screen within 24 hours of admission was then stratified based on the receipt of olanzapine (i.e., olanzapine==1 and control==0). The study outcome measure was the time to delirium resolution (i.e., first negative CAM-ICU screening). We collected the following factor (0==no; 1==yes) variables: antidepressant administration, benzodiazepine administration, chronic obstructive pulmonary disease, dementia, depression, diabetes, hypertension, myocardial infarction, opioid administration, propofol administration, sepsis, stroke, and vasopressor administration. Additionally, we collected baseline heart rate, respiratory rate, and temperature, as well as age, and gender. Given the low level of missingness (<2%), patients with missing data were excluded.
4.3. Statistical Analysis
The variance inflation factors (VIFs) were used to examine the presence of multicollinearity among variables. The MatchIt [19] package in R was used to propensity match the strata and achieve covariate balance between the treatment (olanzapine) and control groups. Propensity scores were assigned using a logistic regression model, with the treatment variable as the outcome and the following covariates: age, antidepressant administration, baseline heart rate, baseline respiratory rate, baseline temperature, benzodiazepine administration, chronic obstructive pulmonary disease, dementia, depression, diabetes, gender, hypertension, myocardial infarction, opioid administration, propofol administration, sepsis, stroke, and vasopressor administration. The nearest neighbor matching without replacement at a 1:1 ratio and a caliper of 0.2 standard deviations of the logit of the propensity score was implemented. Model validity was assessed by calculating standardized mean differences (SMDs), with SMD < 0.1 indicative of a balanced distribution of confounding factors between groups.
A Cox proportional hazards model was used to examine the association between time to delirium resolution and olanzapine. The model included fixed covariates for olanzapine and all the covariates included in propensity matching. Age was incorporated as a time-dependent variable using an interaction with the logarithm of time [i.e., age × log(time)] to capture changing hazard over time. Robust standard errors were estimated by clustering on the matching subclass to account for the matched design. The proportional hazards assumption was evaluated using Schoenfeld residuals and visual inspection of log(-log[survival]) curves [20]. Model fit was further assessed by examining deviance residuals and overall concordance. All analyses were conducted using the coxph function in the R survival package.
To evaluate whether the effect of pre-ICU olanzapine use on delirium resolution varied by patient age and gender, we estimated a Cox proportional hazards model incorporating interaction terms. We included interaction terms for olanzapine × gender and olanzapine × age, with age modeled as a time-varying covariate using a log(time)-dependent transformation: tt(age) = age × log(time). This allowed the age effect, and its interaction with olanzapine, to vary dynamically over time. The model was adjusted for the same set of covariates as in the original Cox model. To account for clustering due to matching, robust standard errors were estimated using the cluster() option by subclass. The coxph() function from the survival package in R was used to fit the model.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, A.H.; methodology, A.H.; software, A.H.; validation, A.H.; formal analysis, A.H.; investigation, A.H.; resources, J.D.; data curation, A.H.; writing—original draft preparation, A.H.; writing—review and editing, A.H., J.D.; visualization, A.H. All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not require Ethics Approval.
Informed Consent Statement
Deidentified data are available on PhysioNet upon signing Data Use Agreements and completing the required training. The Beth Israel Deaconess Medical Center and Massachusetts Institute of Technology approved the release of the deidentified and publicly available data without a requirement for individual patient informed consent.
Data Availability Statement
Restrictions apply to the availability of these data. Data were obtained from physionet.org and are available from physionet.org with the permission of physionet.org
Acknowledgments
None
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Association AP. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); 2013. [Google Scholar]
- Desai, S.V.; Law, T.J.; Needham, D.M. Long-Term Complications of Critical Care. Crit Care Med 2011, 39, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Pandharipande, P.P.; Girard, T.D.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Pun, B.T.; Brummel, N.E.; Hughes, C.G.; Vasilevskis, E.E.; Shintani, A.K.; et al. Long-Term Cognitive Impairment after Critical Illness. N Engl J Med 2013, 369, 1306–1316. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.; Balas, M.C.; Stollings, J.L.; McNett, M.; Girard, T.D.; Chanques, G.; Kho, M.E.; Pandharipande, P.P.; Weinhouse, G.L.; Brummel, N.E.; et al. A Focused Update to the Clinical Practice Guidelines for the Prevention and Management of Pain, Anxiety, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med 2025, 53, e711–e727. [Google Scholar] [CrossRef] [PubMed]
- Richelson, E. Receptor Pharmacology of Neuroleptics: Relation to Clinical Effects. J Clin Psychiatry 1999, 60 Suppl 10, 5–14. [Google Scholar]
- Bymaster, F.P.; Calligaro, D.O.; Falcone, J.F.; Marsh, R.D.; Moore, N.A.; Tye, N.C.; Seeman, P.; Wong, D.T. Radioreceptor Binding Profile of the Atypical Antipsychotic Olanzapine. Neuropsychopharmacology 1996, 14, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Jensen, N.H.; Rodriguiz, R.M.; Caron, M.G.; Wetsel, W.C.; Rothman, R.B.; Roth, B.L. N-Desalkylquetiapine, a Potent Norepinephrine Reuptake Inhibitor and Partial 5-HT1A Agonist, as a Putative Mediator of Quetiapine’s Antidepressant Activity. Neuropsychopharmacology 2008, 33, 2303–2312. [Google Scholar] [CrossRef] [PubMed]
- Roth, Bryan L. PDSP Ki Database.
- Levey, A.I.; Edmunds, S.M.; Koliatsos, V.; Wiley, R.G.; Heilman, C.J. Expression of M1-M4 Muscarinic Acetylcholine Receptor Proteins in Rat Hippocampus and Regulation by Cholinergic Innervation. J Neurosci 1995, 15, 4077–4092. [Google Scholar] [CrossRef] [PubMed]
- Shinoe, T.; Matsui, M.; Taketo, M.M.; Manabe, T. Modulation of Synaptic Plasticity by Physiological Activation of M1 Muscarinic Acetylcholine Receptors in the Mouse Hippocampus. J Neurosci 2005, 25, 11194–11200. [Google Scholar] [CrossRef] [PubMed]
- Wess, J. Muscarinic Acetylcholine Receptor Knockout Mice: Novel Phenotypes and Clinical Implications. Annu Rev Pharmacol Toxicol 2004, 44, 423–450. [Google Scholar] [CrossRef] [PubMed]
- Anagnostaras, S.G.; Murphy, G.G.; Hamilton, S.E.; Mitchell, S.L.; Rahnama, N.P.; Nathanson, N.M.; Silva, A.J. Selective Cognitive Dysfunction in Acetylcholine M1 Muscarinic Receptor Mutant Mice. Nat Neurosci 2003, 6, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Langmead, C.J.; Watson, J.; Reavill, C. Muscarinic Acetylcholine Receptors as CNS Drug Targets. Pharmacol Ther 2008, 117, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Lamping, K.G.; Duttaroy, A.; Zhang, W.; Cui, Y.; Bymaster, F.P.; McKinzie, D.L.; Felder, C.C.; Deng, C.X.; Faraci, F.M.; et al. Cholinergic Dilation of Cerebral Blood Vessels Is Abolished in M(5) Muscarinic Acetylcholine Receptor Knockout Mice. Proc Natl Acad Sci U S A 2001, 98, 14096–14101. [Google Scholar] [CrossRef] [PubMed]
- Bugiani, O. Why Is Delirium More Frequent in the Elderly? Neurol Sci 2021, 42, 3491–3503. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.G.; Boncyk, C.S.; Fedeles, B.; Pandharipande, P.P.; Chen, W.; Patel, M.B.; Brummel, N.E.; Jackson, J.C.; Raman, R.; Ely, E.W.; et al. Association between Cholinesterase Activity and Critical Illness Brain Dysfunction. Crit Care 2022, 26, 377. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, J.R. Delirium Pathophysiology: An Updated Hypothesis of the Etiology of Acute Brain Failure. Int J Geriatr Psychiatry 2018, 33, 1428–1457. [Google Scholar] [CrossRef] [PubMed]
- Ely, E.W.; Margolin, R.; Francis, J.; May, L.; Truman, B.; Dittus, R.; Speroff, T.; Gautam, S.; Bernard, G.R.; Inouye, S.K. Evaluation of Delirium in Critically Ill Patients: Validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Crit Care Med 2001, 29, 1370–1379. [Google Scholar] [CrossRef] [PubMed]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Soft. 2011, 42. [Google Scholar] [CrossRef]
- Grambsch, P.M.; Therneau, T.M. Proportional Hazards Tests and Diagnostics Based on Weighted Residuals. Biometrika 1994, 81, 515–526. [Google Scholar] [CrossRef]
Figure 1.
Participant Flow Diagram.
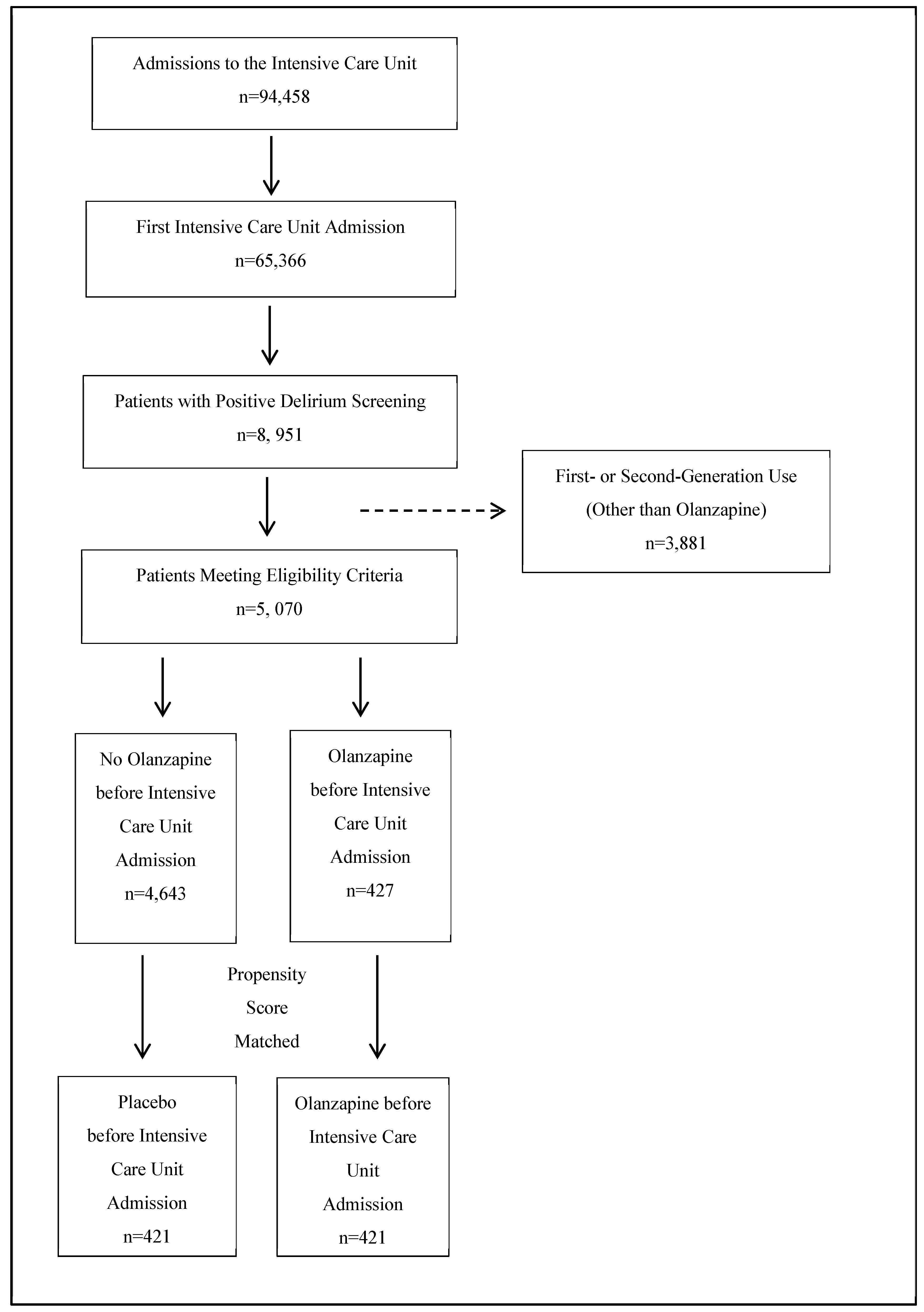
Figure 2.
Covariate balance in the unmatched and matched treatment groups.
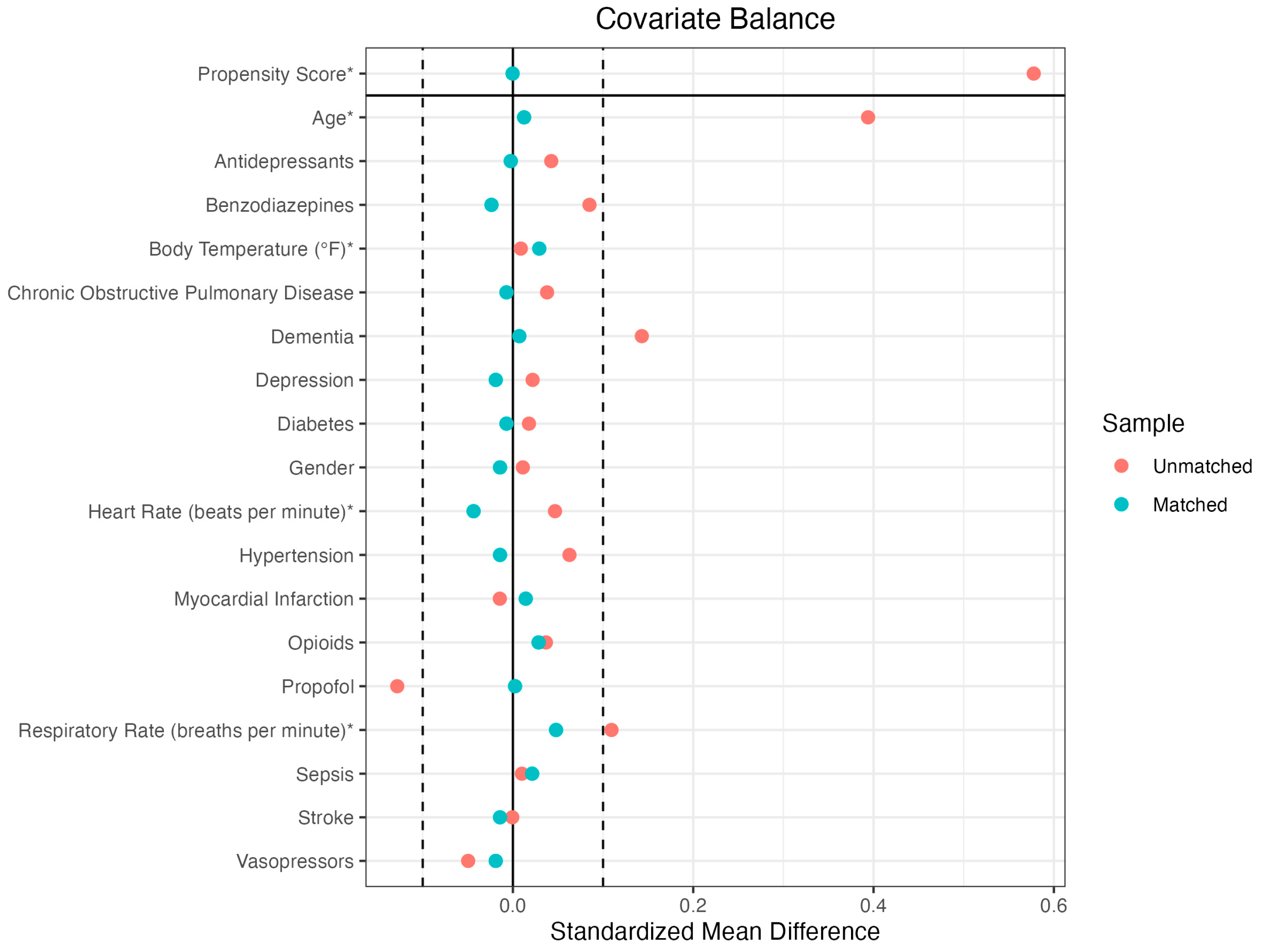
Figure 3.
Kaplan Meier Curves for Delirium Persistence Probability according to Treatment Groups.
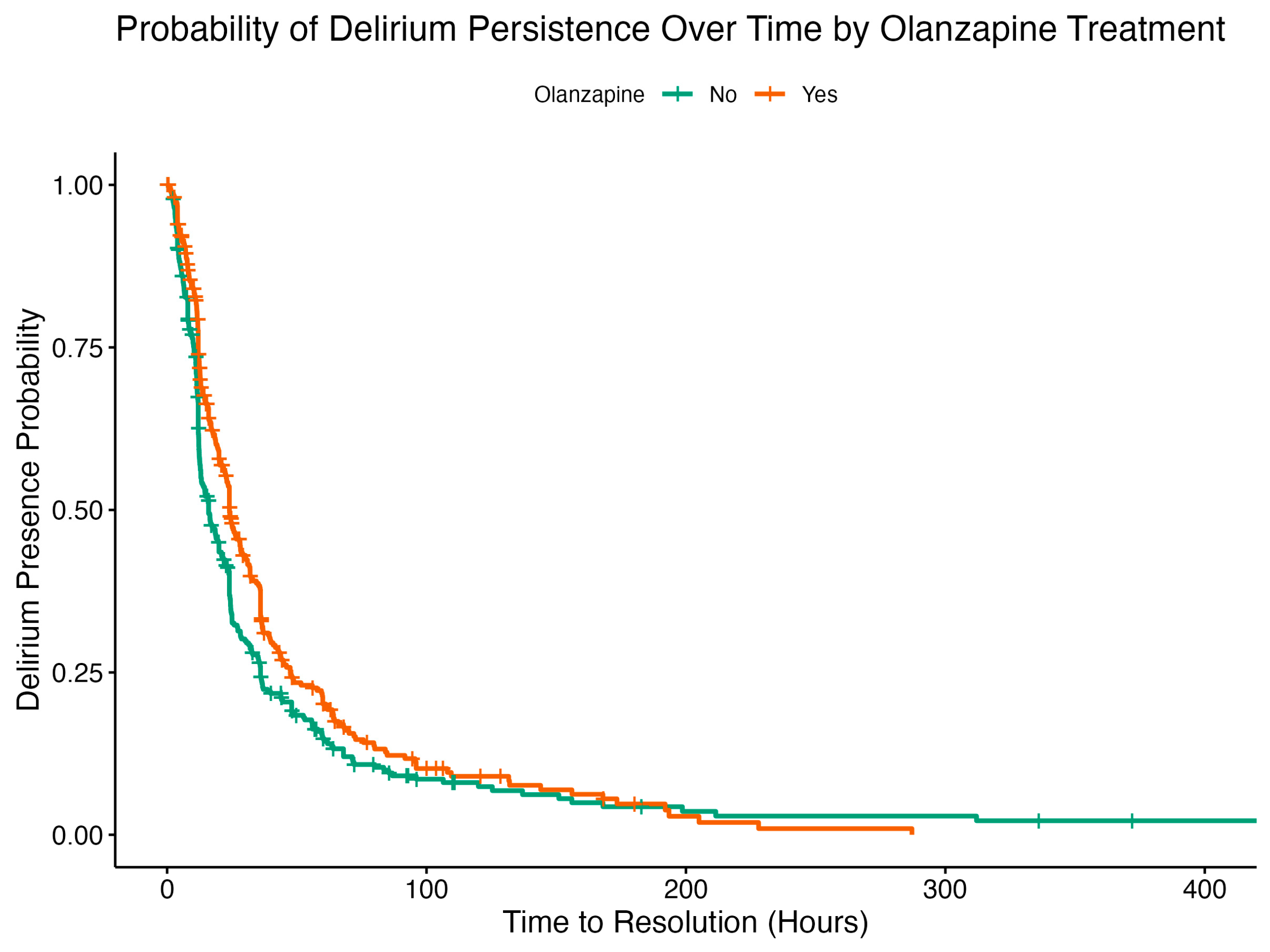
Figure 4.
Kaplan Meier Curves for Delirium Persistence Probability according to Age and Treatment Groups.
Figure 4.
Kaplan Meier Curves for Delirium Persistence Probability according to Age and Treatment Groups.
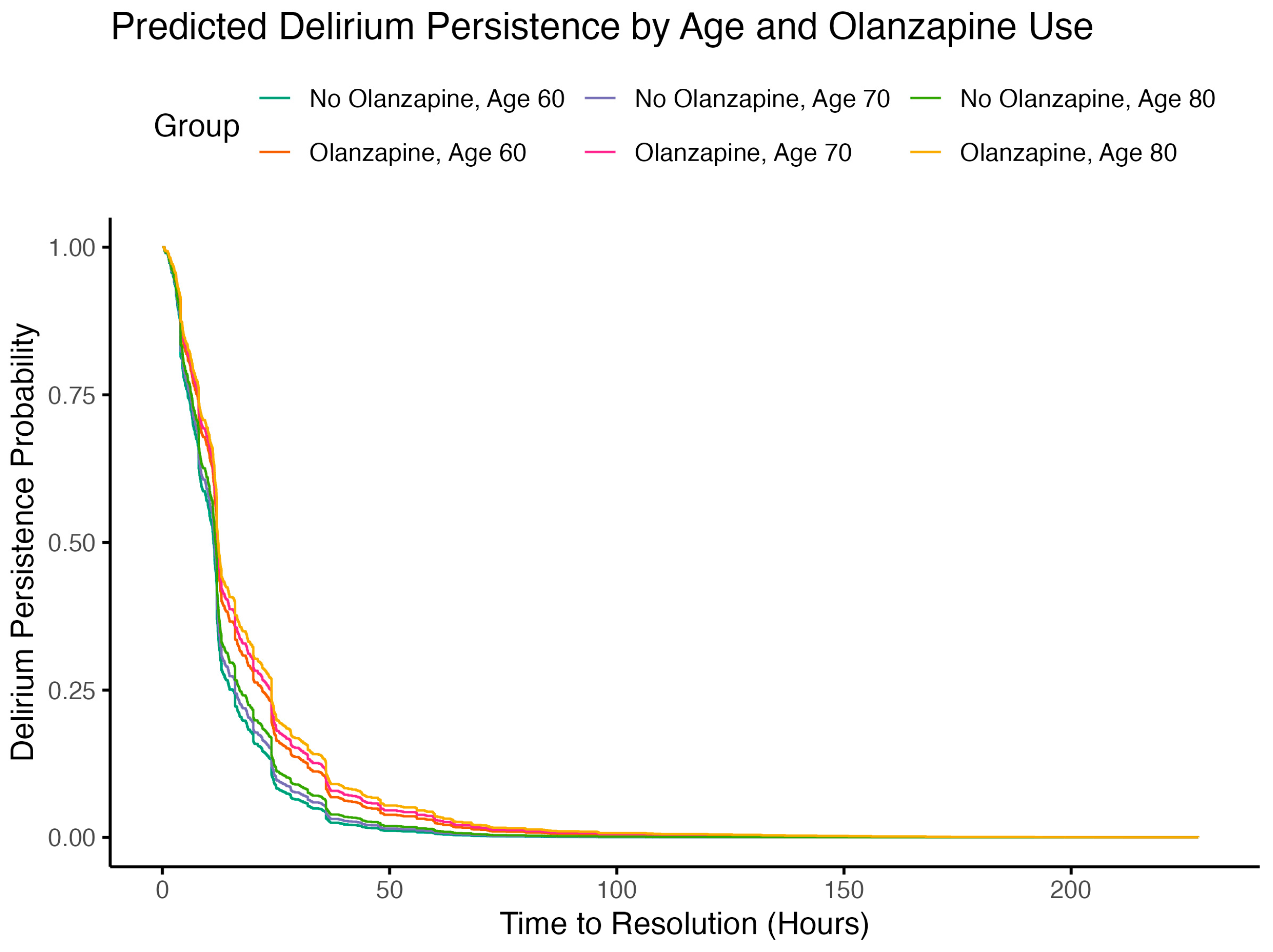
Figure 5.
Binding Affinity for Muscarinic Receptor Subtypes for seven Atypical Antipsychotic and Norquetiapine, a metabolite of Quetiapine.
Figure 5.
Binding Affinity for Muscarinic Receptor Subtypes for seven Atypical Antipsychotic and Norquetiapine, a metabolite of Quetiapine.
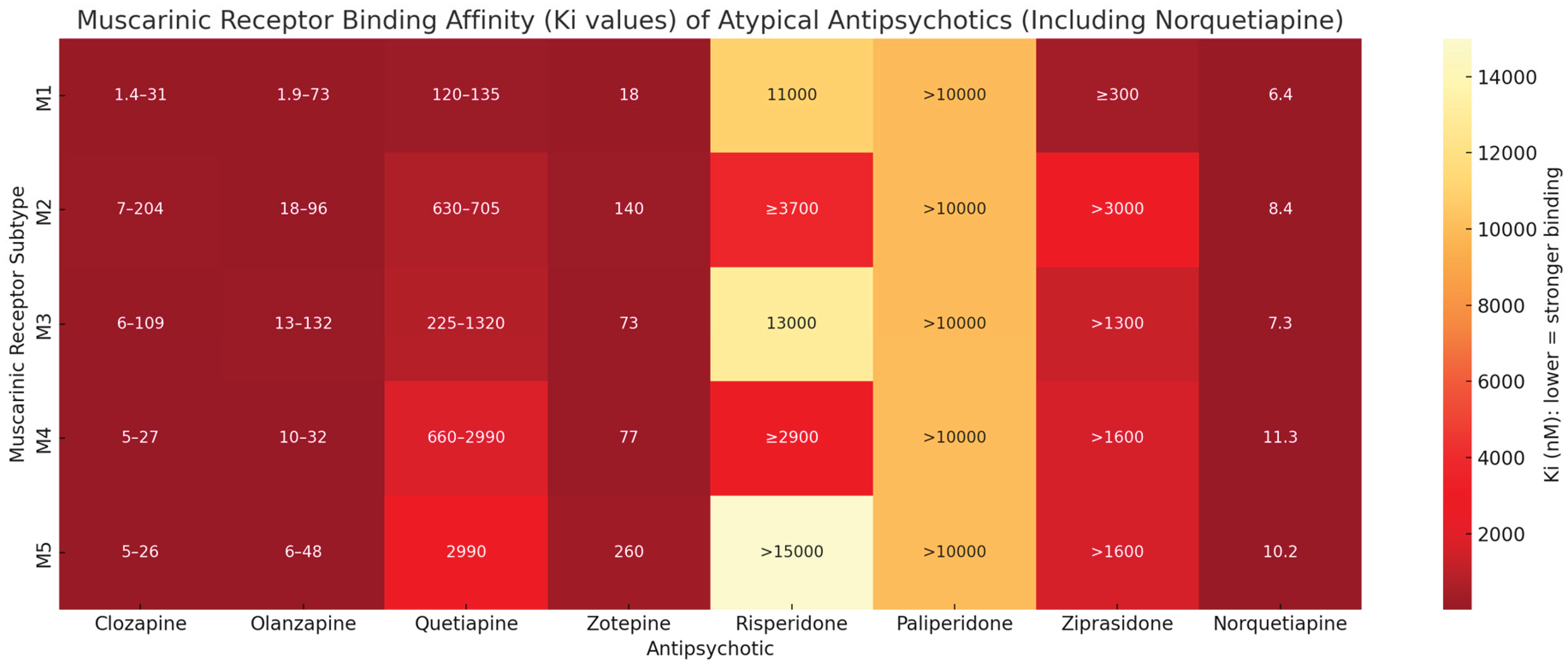

Table 1.
Standardized Mean Difference (SMD) According to Treatment Group before and after Propensity Score Matching.
Table 1.
Standardized Mean Difference (SMD) According to Treatment Group before and after Propensity Score Matching.
| BEFORE MATCHING | AFTER MATCHING | |||||
| Means Treated | Means Control | Standardized Mean Difference | Means Treated | Means Control | Standardized Mean Difference | |
| Propensity Score | 0.1145 | 0.0827 | 0.5036 | 0.1145 | 0.1144 | 0.0008 |
| Demographics | ||||||
| Age | 72.9739 | 66.5803 | 0.4264 | 72.9739 | 72.8195 | 0.0103 |
| Gender | 0.2138 | 0.1713 | 0.1037 | 0.2138 | 0.2043 | 0.0232 |
| Medical Conditions | ||||||
| Chronic Obstructive Pulmonary Disease | 0.1306 | 0.0927 | 0.1125 | 0.1306 | 0.152 | -0.0634 |
| Dementia | 0.247 | 0.104 | 0.3316 | 0.247 | 0.247 | 0 |
| Depression | 0.2067 | 0.1848 | 0.054 | 0.2067 | 0.1876 | 0.0469 |
| Diabetes | 0.3302 | 0.3123 | 0.0379 | 0.3302 | 0.3325 | -0.0051 |
| Hypertension | 0.5463 | 0.4836 | 0.126 | 0.5463 | 0.5487 | -0.0048 |
| Myocardial Infarction | 0.133 | 0.1475 | -0.0427 | 0.133 | 0.1686 | -0.1049 |
| Sepsis | 0.2518 | 0.2418 | 0.023 | 0.2518 | 0.2755 | -0.0547 |
| Stroke | 0.2043 | 0.205 | -0.0017 | 0.2043 | 0.1781 | 0.0648 |
| Medications | ||||||
| Antidepressants | 0.2138 | 0.1713 | 0.1037 | 0.2138 | 0.2043 | 0.0232 |
| Benzodiazepines | 90.304 | 89.2533 | 0.0499 | 90.304 | 92.3539 | -0.0973 |
| Propofol | 20.3183 | 19.6346 | 0.1105 | 20.3183 | 20.5701 | -0.0407 |
| Vasopressors | 98.2389 | 98.2224 | 0.011 | 98.2389 | 98.1964 | 0.0284 |
| Vitals | ||||||
| Heart Rate | 90.304 | 89.2533 | 0.0499 | 90.304 | 92.3539 | -0.0973 |
| Respiratory Rate | 20.3183 | 19.6346 | 0.1105 | 20.3183 | 20.5701 | -0.0407 |
| Body Temperature | 98.2389 | 98.2224 | 0.011 | 98.2389 | 98.1964 | 0.0284 |
Table 2.
Summary of the Cox Proportional Hazards Analysis.
| Term | Estimate | SE | Robust SE | Statistic | p.value | Confidence - Low | Confidence - High |
| Demographics | |||||||
| Age | 0.9985 | 0.0011 | 0.0011 | -1.4209 | 0.1553 | 0.9963 | 1.0006 |
| Gender (F) | 0.8086 | 0.0865 | 0.0881 | -2.4111 | 0.0159 | 0.6803 | 0.9610 |
| Medications | |||||||
| Olanzapine | 0.7342 | 0.0832 | 0.0792 | -3.9005 | 0.0001 | 0.6287 | 0.8575 |
| Antidepressants | 0.8813 | 0.1086 | 0.0934 | -1.3525 | 0.1762 | 0.7338 | 1.0584 |
| Benzodiazepines | 0.9023 | 0.0888 | 0.0871 | -1.1802 | 0.2379 | 0.7606 | 1.0703 |
| Propofol | 0.6030 | 0.0962 | 0.0909 | -5.5614 | 0.0000 | 0.5046 | 0.7207 |
| Vasopressors | 0.7571 | 0.1020 | 0.0964 | -2.8872 | 0.0039 | 0.6268 | 0.9145 |
| Vitals | |||||||
| Heart Rate | 0.9971 | 0.0021 | 0.0020 | -1.4751 | 0.1402 | 0.9933 | 1.0010 |
| Respiratory Rate | 0.9882 | 0.0075 | 0.0078 | -1.5135 | 0.1301 | 0.9732 | 1.0035 |
| Body Temperature | 0.9978 | 0.0317 | 0.0312 | -0.0693 | 0.9447 | 0.9387 | 1.0607 |
| Medical Conditions | |||||||
| Chronic Obstructive Pulmonary Disease | 0.9984 | 0.1230 | 0.1278 | -0.0122 | 0.9903 | 0.7772 | 1.2827 |
| Dementia | 0.8108 | 0.1122 | 0.1096 | -1.9137 | 0.0557 | 0.6541 | 1.0051 |
| Depression | 1.0512 | 0.1085 | 0.0949 | 0.5257 | 0.5991 | 0.8727 | 1.2662 |
| Diabetes | 0.8728 | 0.0903 | 0.0837 | -1.6259 | 0.1040 | 0.7407 | 1.0284 |
| Hypertension | 0.9752 | 0.0846 | 0.0812 | -0.3089 | 0.7574 | 0.8317 | 1.1435 |
| Myocardial Infarction | 1.0104 | 0.1379 | 0.1351 | 0.0765 | 0.9390 | 0.7754 | 1.3166 |
| Sepsis | 0.7070 | 0.1115 | 0.1112 | -3.1188 | 0.0018 | 0.5686 | 0.8791 |
| Stroke | 0.7668 | 0.1045 | 0.1015 | -2.6148 | 0.0089 | 0.6284 | 0.9357 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



