1. Introduction
Tick-borne infections, such as severe fever with thrombocytopenia syndrome (SFTS) and Japanese spotted fever (JSF), are associated with specific vector species. In Japan, other tick-borne diseases such as Borrelia infection are exceedingly rare, and tularemia has not been reported for several decades. Infections caused by spotted fever group rickettsiae other than JSF are reported only once every few years. Therefore, among tick-borne diseases, the conditions of primary concern in Japan are SFTS and JSF. The principal tick vectors responsible for SFTS are
Haemaphysalis longicornis (dominant across East Asia) [
1] and, in Japan, SFTS RNA has additionally been detected in
Amblyomma testudinarium,
H.
flava,
H. hystricis,
H.
formosensis,
H.
megaspinosa,
H.
kitaokai, and occasionally
Ixodes nipponensis as a potential vector [
2]. At the same time, virus isolation has been achieved from
H.
longicornis,
Rhipicephalus microplus, and
I. nipponensis [
2]. Previous studies have isolated
R.japonica from several tick species, including
Dermacentor taiwanensis,
H.
cornigera,
H.
flava, and
H.
longicornis. Moreover, the
R. japonica gene has been identified in
H.
formosensis,
H.
megaspinosa, and
I.
ovatus [
3]. Clinical care is often initiated after symptom onset, by which time SFTS can carry substantial mortality [
4], and JSF may require prompt therapy to avoid severe complications [
5]. A key unmet need is a practical method to triage risk before symptoms appear. However, routine direct detection of causative agents from every bite site is not feasible in typical practice: severe fever with thrombocytopenia syndrome (SFTSV) requires RT-PCR [
6] and specialized reagents and facilities, whereas
R. japonica detection frequently relies on nested PCR [
7]; both approaches are resource-intensive and time-consuming, particularly when patients present with numerous lesions.
After hatching, tick larvae are mostly immobile and remain where they are, waiting to blood-feed. Eschars mark the sites of tick attachment and, when distributed in clusters of similar size and morphology, may indicate larval tick bites. Because larvae often feed in proximity and detach within a few days [
8], representative eschars can reasonably be assumed to originate from the same tick species, even if not all lesions are sampled. In endemic areas, multiple simultaneous bites significantly increase the baseline infection risk (e.g., the probability that at least one tick is infected increases with the number of bites), underscoring the need for a rapid, scalable triage strategy that does not depend on exhaustive pathogen testing. Here, we report a case in which PCR-based species identification performed on a subset of clustered eschars (and corroborated with removed ticks) yielded
A.testudinarium. Because this species is implicated in SFTSV transmission but not recognized as a vector of
R. japonica, species-level identification immediately refined the differential, prioritized targeted monitoring for early SFTS, and de-emphasized JSF. We propose that selective species identification from representative eschars offers a practical, pre-symptomatic risk assessment pathway and may aid shared decision-making regarding observation versus preemptive intervention in high-risk contexts.
2. Case Presentation
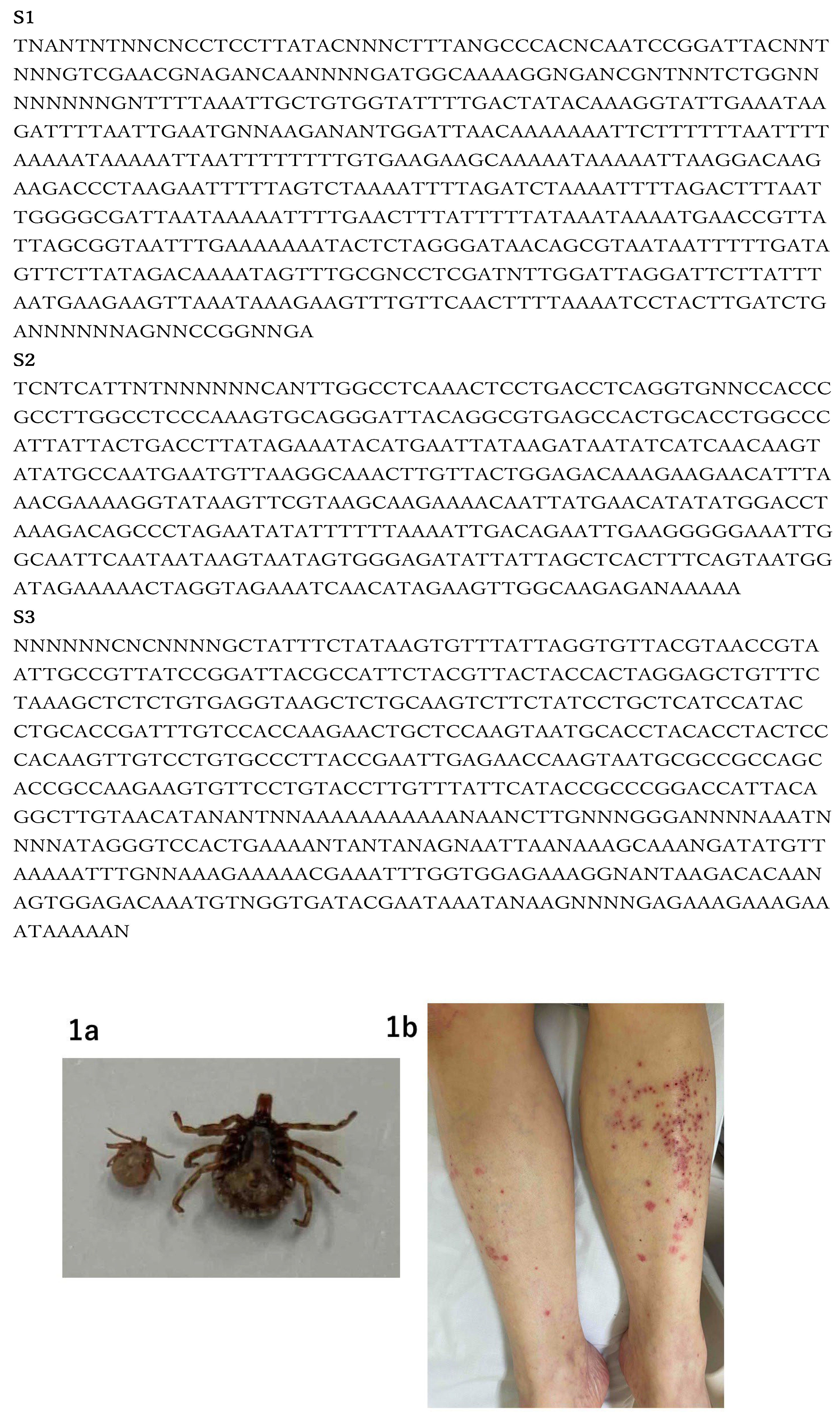
We report a case in which the tick species was successfully identified two days after a tick bite using eschar samples, prompting consideration of early countermeasures. The patient was a 78-year-old woman with a known history of dementia. When her home-care assistant visited around noon, she was not at home. She had last been seen at noon the previous day. Later that evening, she was found by police wandering in a mountainous area and was subsequently taken to the hospital. On examination, multiple abrasions and insect bite marks were observed. Two ticks were found attached to her abdomen and back and were promptly removed (
Figure 1a). Additionally, multiple eschars and erythematous lesions were noted on her lower extremities (
Figure 1b). On initial presentation, vital signs were as follows: body temperature (T) 36.4 °C; blood pressure (BP) 95/63 mmHg; heart rate (HR) 66 beats/min; and oxygen saturation (SpO₂) 97%. Laboratory tests showed: white blood cell count (WBC, /µL): 5,100; hematocrit (Ht, %): 35.7; platelet count (PLT, /µL): 98,000; D-dimer (FEU, µg/mL): 1.6; aspartate aminotransferase (AST, U/L): 46; alanine aminotransferase (ALT, U/L): 43; creatine kinase (CK, U/L): 676; blood urea nitrogen (BUN, mg/dL): 19.0; serum creatinine (Cr, mg/dL): 0.82; estimated glomerular filtration rate (eGFR, mL/min/1.73 m²): 51.0; and C-reactive protein (CRP, mg/dL): 0.5. The patient’s general condition and blood test results were largely unremarkable, aside from mild dehydration and slightly elevated inflammatory markers. Given that cases of SFTS had previously been reported in the region, we considered clustering of crusts and small erythematous macules were observed on the lower extremities, raising suspicion of bites by larval ticks. We therefore attempted to determine whether tick species identification could be achieved using material obtained from the crusts. Based on the patient’s general condition and laboratory findings, treatment consisted only of intravenous fluids, and no antibiotics were administered. However, we continued to monitor the patient closely without completely ruling out the possibility of a tick-borne infection.
3. Materials and Methods
Both the removed ticks and ten eschar samples from the lower limbs were collected for species identification. The crusted lesions were disinfected with povidone–iodine, carefully removed with forceps, and each specimen was placed individually into a sterile tube. PCR analysis was promptly performed to determine the tick species.
DNA was extracted from ten eschars and two ticks that had been attached to the patient using the QIAamp DNA Mini Kit (QIAGEN, Hilden, Germany). Tick species identification was conducted using PCR with widely adopted primers [
9]. The primers, mt-rrs1 (5'-CTG CTC AAT GAT TTT TTA AAT TGC TGT GG-3') and mt-rrs2 (5'-CCG GTC TGA ACT CAG ATC AAG TA-3'), amplify the tick mitochondrial 16S rRNA (mt-rrs) region and are utilized for species identification by sequencing. The PCR cycling conditions were as follows: initial denaturation at 95 °C for 5 min; 35 cycles of 95 °C for 30 s, annealing at 57 °C for 30 s, and 72 °C for 40 s; followed by a final extension at 72 °C for 10 min. PCR products were separated by agarose gel electrophoresis, and the positive PCR products were excised from agarose gels and purified using the FastGene® Gel/PCR Extraction Kit (NIPPON Genetics EUROPE GmbH, Düren, Germany). Sequencing was outsourced to a commercial provider (Eurofins Genomics, Tokyo, Japan). The resulting sequences were analyzed using BLAST against reference sequences in the GenBank database.
In addition, to exclude the possibility of JSF, nested PCR was performed using DNA extracted from the crusts and primers capable of detecting R. japonica as well as multiple other spotted fever group rickettsiae.
The reaction conditions were as follows: initial denaturation at 95 °C for 2 min; 35 cycles of 94 °C for 45 s, 52 °C for 30 s, and 72 °C for 45 s; followed by a final extension at 72 °C for 5 min. The primers used for the first PCR were R1 (TCAATTCACAACTTGCCATT) and R2 (TTTACAAAATTCTAAAAACC) [
10]. The primers used for the second PCR were Rr17.61p (GCTCTTGCAACTTCTATGTT) and Rr17.492n (CATTGTTCGTCAGGTTGGCG) [
11]. Both PCR assays were performed under the same reaction conditions and sequencing procedures.
4. Results
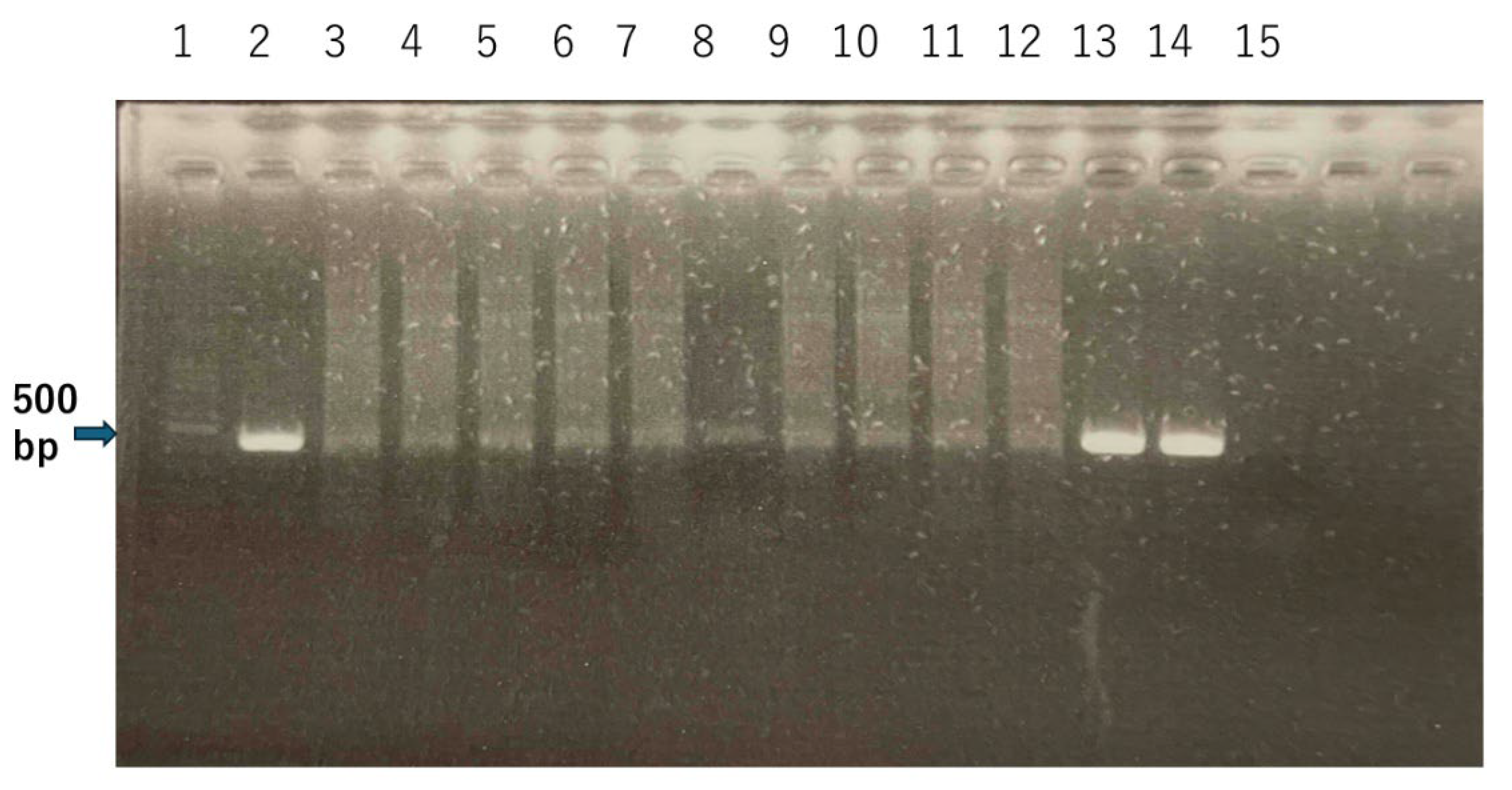
PCR using tick-identification primers yielded amplicons in all DNA samples extracted from the patient’s left lower-extremity eschars and in both ticks removed from her body. PCR results for the ten eschars and two ticks showed a positive band of about 401-416 bp (
Figure 2). Sanger sequencing identified all ten eschar-derived samples and both ticks as
A. testudinarium (Accession number: PV124239-1). The forward and reverse Sanger sequencing reads (raw sequences including unresolved bases “N”) are provided in the Supplementary Material (File S1). A consensus sequence was obtained and used for BLAST analysis. Because this species is not recognized as a vector of
R. japonica—the causative agent of JSF—according to the National Institute of Infectious Diseases, we considered the likelihood of JSF to be low. Although this species is not recognized as a vector of
R. japonica, making JSF less likely, we still examined the presence of spotted fever group rickettsiae, including
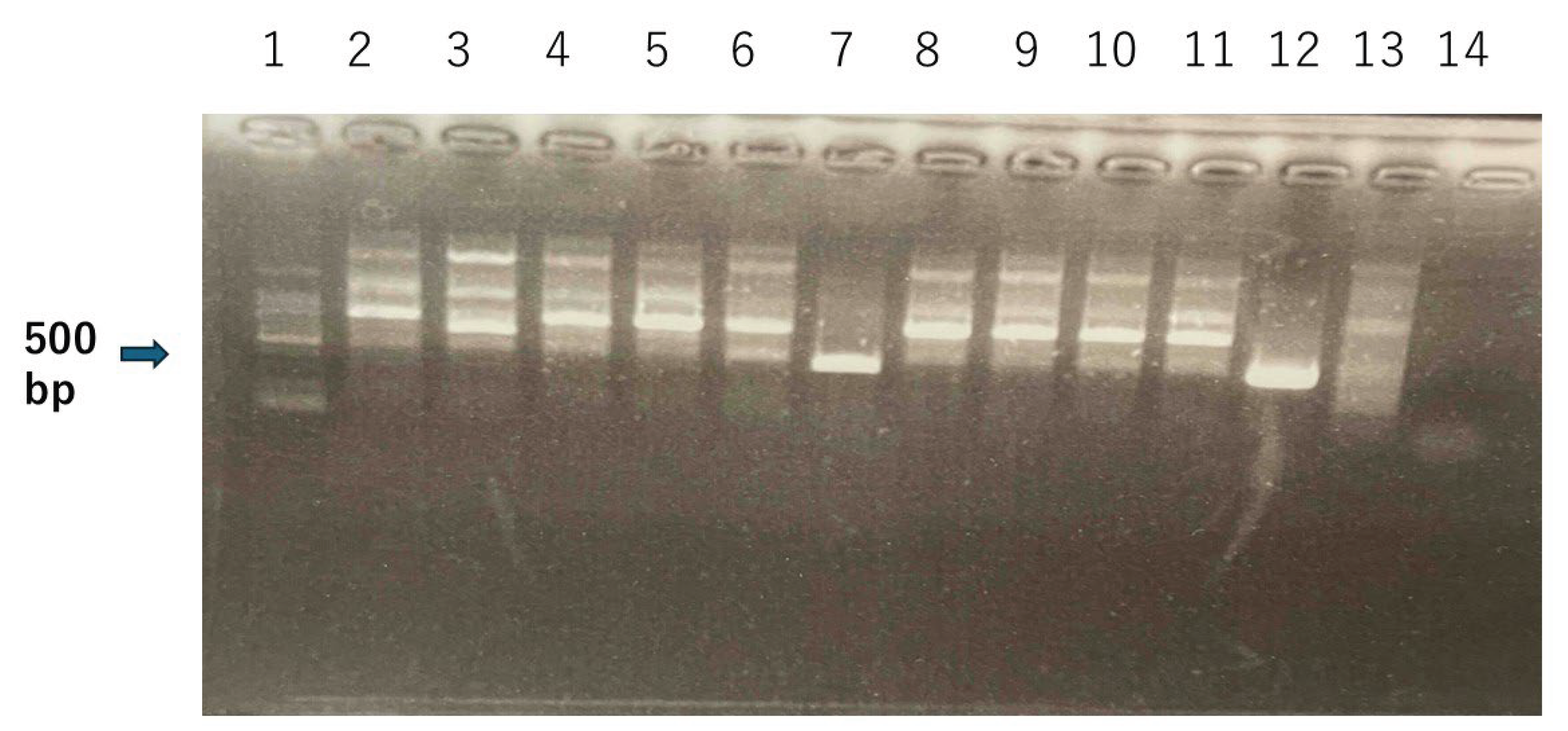
R. japonica. The results are shown in
Figure 3. A faint positive band of approximately 430 bp was observed, and because the band was considered suspicious, sequencing analysis was performed as well. The sequencing results showed that the product in lane 7 represented an erroneous human-derived artifact (File S2), whereas the product in lane 13 matched
Candidatus Rickettsia jingxinensis (Accession number: PP116496). (File S3)
Candidatus Rickettsia jingxinensis is an emerging spotted fever group rickettsia in Asia, and its pathogenicity and infectivity in humans remain uncertain [
12]. As
A. testudinarium is a known vector of SFTSV [
1], the patient was closely monitored over several days for early signs of SFTS, including leukopenia, fever, and gastrointestinal symptoms such as diarrhea [
13]. To avert contact transmission, given the possibility of SFTS infection, gown and glove use was strictly implemented. No abnormal findings or clinical deterioration were observed during the observation period. Given the stable clinical course and absence of concerning symptoms, after 9 days of admission, the patient was subsequently transferred to a long-term care facility without complications.
Sequencing Data
Sequencing revealed that the product in lane 7 was a human-derived artifact and therefore considered negative. The product in lane 12 matched the gene sequence of Candidatus Rickettsia jingxinensis.
Lane 2 shows the PCR product obtained under the same conditions from a tick that had previously been attached to the patient and was identified as A. testudinarium. Lane 3–12 represents eschars removed from the patient's left lower limb. Lanes 13 and 14 correspond to the ticks removed from the abdomen and back, respectively. Lane 15 contains the DNA-free control solution processed by PCR under the same conditions. 2-14 samples showed positive PCR bands. In the case of A. testudinarium, PCR amplification with the mt-rrs1/mt-rrs2 primers yields a mitochondrial 16S rDNA fragment of approximately 401–416 bp.
Lane 1 represents the molecular size marker. Lanes 2–11 contain PCR products amplified from DNA extracted from the crusts. Lanes 12 and 13 correspond to the ticks that had been attached to the patient. Lane 14 contains the DNA-free control solution processed by PCR under the same conditions. The expected positive band is approximately 430 bp.
5. Discussion
SFTS is a tick-borne viral disease associated with a high fatality rate of approximately 30% once clinical symptoms appear [
4]. Early symptoms include fever, gastrointestinal manifestations, malaise, and headache [
13]. Because these are non-specific, patients are often diagnosed with a common cold or gastroenteritis, resulting in delays in receiving appropriate treatment. SFTS can spread not only through tick bites but also via contact with infected individuals [
14] or animals [
15], creating the potential for rapid expansion. First reported in China in 2011 [
16], SFTS was subsequently identified in Japan in 2013 [
17]. It has now been reported in Southeast Asia as well [
18]. In contrast, JSF is transmitted solely through tick bites. It was first reported in Japan in 1984 [
19] and has spread gradually to Korea [
20] and China [
21]. In Japan, JSF remains largely confined to limited geographic areas, and there has been no sharp nationwide increase in cases; approximately 600–700 cases are reported annually. JSF requires early therapeutic intervention, as cases of disseminated intravascular coagulation (DIC) and fatal outcomes have been reported [
5,
22]. Therefore, the ability to predict these diseases before symptom onset could facilitate both prevention and early therapeutic intervention.
In this context, we focused on eschar lesions, which mark the sites of tick bites. In this PCR assay, we amplified the tick mitochondrial 16S rRNA gene, which enables species identification by sequencing followed by BLAST search and phylogenetic analysis. The eschar is composed of host-derived wound material together with tick cement substances and salivary molecules that modulate host immunity and hemostasis. Proteomic analyses of cement from
Rhipicephalus microplus have shown that, in addition to numerous tick-derived proteins, the matrix contains more than 250 host-derived proteins as well as α-Gal. Structural studies of the saliva-derived cement cone further demonstrate that the cone becomes tightly integrated with the host epidermal layers, making complete separation extremely difficult. As a result, tick-derived DNA can be recovered from eschar material [
23]. Consistent with this, previous reports have detected both
R. parkeri DNA and DNA of its vector, the Gulf Coast tick (
A. maculatum), in eschar biopsy specimens [
24]. Our assumption that these eschars resulted from tick bites was supported not only by the presence of attached ticks on the patient’s trunk but also by the clustered distribution of the eschars. After hatching, tick larvae typically remain stationary and wait for a host, rather than actively seeking one. Consequently, they tend to bite in proximity to one another, resulting in eschars that are similar in size and morphology. These characteristics suggest that the lesions were caused by bites from larval ticks. Therefore, even without analyzing all eschars, it can reasonably be inferred that they originated from the same tick species.
It is noteworthy that the presence of an attached tick at the time of disease onset is extremely rare for both SFTS and JSF [
25,
26,
27]. Larval ticks typically detach within approximately 24 hours, suggesting that asymptomatic larval tick bites may represent a plausible route of infection. Therefore, when multiple clustered eschars are present, analyzing representative lesions to identify the tick species and determining whether that species is a known vector of pathogens such as SFTSV or
R. japonica can provide valuable information for assessing the patient’s risk of tick-borne infections such as SFTS or JSF.
Direct detection of SFTSV or
R. japonica genes from eschar samples is often impractical. Routinely performing PCR on eschars in non-endemic areas is not cost-effective and therefore not advised. SFTSV is an RNA virus that requires RT-PCR, which involves costly reagents and specialized laboratory facilities [
6]. Similarly, detection of
R. japonica typically relies on nested PCR [
7], a method that is both time-consuming and expensive. Performing these assays on every eschar is not feasible. However, in endemic areas, multiple bites from different ticks substantially increase the baseline risk. If the tick infection prevalence is
p, the probability that at least one of
n bites involves an infected tick is 1 − (1 −
p)^
n. For
n = 30 bites, for example:
p = 0.5% → ~14%,
p = 1% → ~26%,
p = 2% → ~45%, and
p = 5% → ~79%. In theory, these probabilities apply; however, infection does not necessarily occur in every exposure. The previous report suggests that a substantial proportion of cases may result in subclinical infection [
28]. Prophylactic antibiotics for asymptomatic individuals are generally not recommended; however, in selected cases, pre-emptive therapy may be considered after careful risk assessment and shared decision-making. In highly endemic regions, we recommend considering the possibility of larval tick bites when partially clustered eschars are observed, particularly in asymptomatic individuals. While JSF typically shows characteristic exanthema with pronounced elevation of inflammatory markers and abnormal liver function tests, early SFTS manifestations such as fever, headache, and diarrhea are non-specific, making differentiation from common cold or gastroenteritis challenging. Selective PCR testing of representative eschars may be a useful strategy for assessing the risk of SFTS or JSF, as it enables the identification of the tick species responsible.
6. Conclusions
Selective PCR of representative clustered eschars enables the rapid pre-symptomatic triage of SFTS/JSF risk by identifying tick species. In this case, all samples were A. testudinarium, allowing us to deem JSF risk low and immediately shift to monitoring focused on early signs of SFTS. Even without pathogen testing of every lesion, this simple approach is practical for pre-symptomatic risk assessment and decision-making in endemic areas.
Author Contributions
Kondo M designed the study, treated the patient, and drafted the original manuscript. Koji H revised the manuscript. Keiichi Y granted permission to conduct the research, reviewed, and revised the manuscript. All authors have read and approved the final manuscript.
Funding
The authors did not receive any financial support for this study.
Institutional Review Board Statement
This study was conducted using ticks and eschar material removed as part of routine clinical care. All samples were fully de-identified before analysis, and no additional interventions, procedures, or human genetic analyses were performed for research purposes. Formal approval by the Institutional Review Board was not required for this study.
Informed Consent Statement
Because the patient had dementia and was unable to provide informed consent, written informed consent for publication was obtained from the patient’s family in accordance with the journal’s patient consent policy.
Data Availability Statement
All data generated or analyzed are included in this article and its Supplementary Information files.
Conflicts of Interest
Authors have declared that no competing interests exist.
Abbreviations
The following abbreviations are used in this manuscript:
| SFTS |
Severe Fever with Thrombocytopenia Syndrome |
| JSF |
Japanese Spotted Fever |
| SFTSV |
Severe Fever with Thrombocytopenia Syndrome virus |
| PCR |
Polymerase Chain Reaction |
| RT-PCR |
Real-time PCR |
| DNA |
Deoxyribonucleic Acid |
| RNA |
Ribonucleic Acid |
| BLAST |
Basic Local Alignment Search Tool |
| DIC |
Disseminated Intravascular Coagulation |
References
- Crump, A.; Tanimoto, T. Severe Fever with Thrombocytopenia Syndrome: Japan under Threat from Life-Threatening Emerging Tick-Borne Disease. JMA J. 2020, 3(4), 295–302. [Google Scholar]
- Xu, Q.; Nabeshima, T.; Hamada, K.; et al. Transmission of Severe Fever with Thrombocytopenia Syndrome Virus to Humans from Nonindigenous Tick Host, Japan. Emerg. Infect. Dis. 2024, 30(11). [Google Scholar] [CrossRef]
- Okino, T.; Ushirogawa, H.; Matoba, K.; Hatsushika, R. Bibliographical Studies on Human Cases of Hard Tick (Acarina: Ixodidae) Bites in Japan: Whole Aspect of Tick Bite Cases: 1941–2005. Kawasaki Med. J. 2012, 38, 143–150. [Google Scholar]
- Fukushima, S.; Akazawa, H.; Koyama, T.; Hagiya, H. Trends in the Incidence of Severe Fever with Thrombocytopenia Syndrome in Japan: An Observational Study from 2013 to 2022. Sci. Rep. 2025, 15, 20715. [Google Scholar] [CrossRef]
- Sakabe, S.; Sata, T.; Konishi, T.; et al. The Clinical Course of 239 Cases of Japanese Spotted Fever in Ise Red Cross Hospital, 2006–2019. J. Infect. Chemother. 2022, 28(2), 212–219. [Google Scholar] [CrossRef]
- Zeng, P.; Yang, Z.; Bakkour, S.; et al. Development and Validation of a Real-Time Reverse Transcriptase PCR Assay for Sensitive Detection of SFTSV. J. Med. Virol. 2017, 89, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Ishikura, M.; Ando, S.; Shinagawa, Y.; et al. Phylogenetic Analysis of Spotted Fever Group Rickettsiae Based on gltA, 17-kDa, and rOmpA Genes Amplified by Nested PCR from Ticks in Japan. Microbiol. Immunol. 2003, 47, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Militzer, N.; Bartel, A.; Clausen, P.H.; Hoffmann-Köhler, P.; Nijhof, A.M. Artificial Feeding of All Consecutive Life Stages of Ixodes ricinus. Vaccines 2021, 9(4), 385. [Google Scholar] [CrossRef] [PubMed]
- Ushijima, Y.; Oliver, J.H., Jr.; Keirans, J.E.; et al. Mitochondrial Sequence Variation in Carios capensis, a Parasite of Seabirds, Collected on Torishima Island in Japan. J. Parasitol. 2003, 89(1), 196–198. [Google Scholar] [CrossRef]
- Noda, H.; Munderloh, U.G.; Kurtti, T.J. Endosymbionts of Ticks and Their Relationship to Wolbachia spp. and Tick-Borne Pathogens of Humans and Animals. Appl. Environ. Microbiol. 1997, 63, 3926–3932. [Google Scholar] [CrossRef]
- Mediannikov, O.Y.; Sidelnikov, Y.; Ivanov, L.; Mokretsova, E.; Fournier, P.E.; Tarasevich, I.; et al. Acute Tick-Borne Rickettsiosis Caused by Rickettsia heilongjiangensis in Russian Far East. Emerg. Infect. Dis. 2004, 10, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Meng, C.; Zhang, B.; Wang, X.; Tian, J.; Tang, G.; et al. Prevalence of Spotted Fever Group Rickettsia and Candidatus Lariskella in Multiple Tick Species from Guizhou Province, China. Biomolecules 2022, 12(11), 1701. [Google Scholar] [CrossRef] [PubMed]
- Casel, M.A.; Park, S.J.; Choi, Y.K. Severe Fever with Thrombocytopenia Syndrome Virus: Emerging Novel Phlebovirus and Their Control Strategy. Exp. Mol. Med. 2021, 53, 713–722. [Google Scholar] [CrossRef]
- Jiang, X.-L.; Zhang, S.; Jiang, M.; et al. A Cluster of Person-to-Person Transmission Cases Caused by SFTS Virus in Penglai, China. Int. J. Infect. Dis. 2015, 33, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Mekata, H.; Umeki, K.; Yamada, K.; Umekita, K.; Okabayashi, T. Nosocomial Severe Fever with Thrombocytopenia Syndrome in Companion Animals, Japan, 2022. Emerg. Infect. Dis. 2023, 29(3), 592–595. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.-J.; Liang, M.-F.; Zhang, S.-Y.; et al. Fever with Thrombocytopenia Associated with a Novel Bunyavirus in China. N. Engl. J. Med. 2011, 364, 1523–1532. [Google Scholar] [CrossRef]
- Takahashi, T.; Maeda, K.; Suzuki, T.; et al. The First Identification and Retrospective Study of Severe Fever with Thrombocytopenia Syndrome in Japan. J. Infect. Dis. 2014, 209(6), 816–827. [Google Scholar] [CrossRef]
- Charoensakulchai, S.; Matsuno, K.; Nakayama, E.E.; Shioda, T.; Imad, H.A. Epidemiological Characteristics of Severe Fever with Thrombocytopenia Syndrome. Am. J. Trop. Med. Hyg. 2025, 112(5), 956–962. [Google Scholar] [CrossRef]
- Mahara, F. The First Report of the Rickettsial Infections of Spotted Fever Group in Japan: Three Clinical Cases. Kansenshogaku Zasshi 1985, 59(11), 1165–1172. [Google Scholar] [CrossRef]
- Chung, M.-H.; Lee, S.-H.; Kim, M.-J.; et al. Japanese Spotted Fever, South Korea. Emerg. Infect. Dis. 2006, 12(7), 1122–1124. [Google Scholar] [CrossRef]
- Teng, Z.; Zhang, X.; Zhao, N.; et al. The Increasing Prevalence of Japanese Spotted Fever in China: A Dominant Rickettsial Threat. J. Infect. 2025, 90(2), 106387. [Google Scholar] [CrossRef] [PubMed]
- Aragane, M.; Matsumoto, L.; Yasuda, H.; Nosaka, M.; Ishida, Y.; Yamamoto, H.; et al. An Autopsy Case of Fatal Japanese Spotted Fever in Wakayama. Leg. Med. 2024, 66, 102355. [Google Scholar] [CrossRef]
- Neelakanta, G.; Sultana, H. Tick Saliva and Salivary Glands: What Do We Know So Far on Their Role in Arthropod Blood Feeding and Pathogen Transmission. Front. Cell. Infect. Microbiol. 2022, 11, 816547. [Google Scholar] [CrossRef]
- Kelman, P.; Thompson, C.W.; Hynes, W.; Bergman, C.; Lenahan, C.; Brenner, J.S.; et al. Rickettsia parkeri Infections Diagnosed by Eschar Biopsy, Virginia, USA. Infection 2018, 46(4), 559–563. [Google Scholar] [CrossRef]
- Tabara, K.; Kawabata, H.; Arai, S.; et al. High Incidence of Rickettsiosis Correlated to Prevalence of Rickettsia japonica among Haemaphysalis longicornis Tick. J. Vet. Med. Sci. 2011, 73(4), 507–510. [Google Scholar] [CrossRef]
- Kondo, M.; Goto, D.; Miyazaki, M.; Yamazoe, N.; Yamanaka, K. A Case of Japanese Spotted Fever Probably Transmitted by a Tick Bite Caused by Haemaphysalis cornigera. J. Dermatol. 2024, 51, 614–616. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Wang, Q.; Fu, Y.; et al. Molecular Identification of Severe Fever with Thrombocytopenia Syndrome Viruses from Tick and Bitten Patient in Southeast China. Virol. J. 2020, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Habe, K.; Yamanaka, K. Estimating Japanese Spotted Fever Risk: Numerical Differences Between Field-Dwelling and Human-Biting Tick Species. Int. J. Dermatol. 2025. (Epub ahead of print). [Google Scholar] [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).