
Submitted:
17 November 2025
Posted:
19 November 2025
You are already at the latest version
Abstract
Full-endoscopic lumbar discectomy (FELD) has emerged over time as a minimally invasive alternative to conventional microdiscectomy. This narrative review summarizes the available evidence regarding the evolution, indications, techniques, and outcomes of FELD, with a particular focus on how different types of lumbar disc herniations influence the choice of surgical approach. The literature indicates that the transforaminal approach is most suitable for foraminal and upper lumbar disc herniations, whereas the interlaminar approach is preferred for central or migrated L5–S1 herniations due to the larger interlaminar window at this level. Unilateral biportal endoscopy (UBE) provides better flexibility, visualization, and instrument maneuverability, making it particularly useful in complex cases. Reported complication rates remain low overall but vary according to surgical technique and surgeon experience. The learning curve for FELD typically ranges from approximately 20 to over 50 cases, depending on the approach and individual proficiency. Overall, full-endoscopic techniques are redefining the management of lumbar disc herniations by offering less invasive alternatives with favorable clinical outcomes, and their role is expected to expand further as both technology and surgical expertise continue to evolve.
Keywords:
transforaminal endoscopic lumbar discectomy
; interlaminar endoscopic lumbar discectomy
; unilateral biportal endoscopic lumbar discectomy
; lumbar disc herniation
; discectomy
1. Introduction
Lumbar disc herniation (LDH) is one of the most common causes of low back pain and lumbar radiculopathy due to nerve root compression [1]. While conservative treatment options are usually sufficient, a portion of patients with persistent symptoms or progressive neurological deficit require surgical intervention [2]. For these patients, open microdiscectomy remains the current gold standard, enabling safe removal of herniated disc under surgical microscope [3]. However, despite its documented efficacy, this technique displays specific disadvantages such as the disruption of posterior musculature, osseous and ligamentous structures as well as neural tissue manipulation [3]. Hence, these factors may contribute to spinal instability, epidural fibrosis with recurrence of symptoms as well as persistent postoperative pain due to traumatization of posterior elements [3]. In addition, in cases of extensive facet joint resection, there may even be need for fusion surgery.
Over the past decades, technological advancements have eventually led to the development of full-endoscopic lumbar discectomy (FELD) as an alternative to the traditional microdiscectomy [4]. The FELD technique is based on utilization of high-definition endoscopic optics and specialized working-channel instruments to access the herniated disc through a small incision without disrupting any muscles or removing bone [4]. Additionally, it improves surgical precision by the possibility of concomitant radiofrequency ablation, which enhances hemostasis and allows for annuloplasty [4]. Depending on the pathology, the procedure can be performed by means of the three primary endoscopic approaches: the transforaminal route, the interlaminar route, or the unilateral biportal route [5].
As these techniques are growingly utilized in the field of spine surgery and the range of conditions that can be treated using ldh continues to expand, it is essential to thoroughly analyze its surgical applications, clinical outcomes and potential complications. Thus, there remains a requirement for comparison of these three full-endoscopic approaches. This review aims to collect the current available literature and to evaluate how the different types of LDH influence the selection of FELD techniques, as well as overviewing their current role and potential future applications.
2. Anatomy and Pathophysiology of Disc Herniations
The intervertebral discs (IVDs) form the main joints of the spinal column, representing fibrocartilaginous structures that lie between adjacent vertebral bodies [6,7]. IVDs hold almost one-third of the total spinal height, and their primary function is mostly mechanical [6,7,8]. They constantly absorb and transmit loads during body activity, enabling also bending, flexion, extension and torsion of the spine [7]. This provides structural integrity, contributing also to spinal flexibility. The IVD contributes approximately 30% to lumbar segmental stability [8]. In lumbar spine, IVDs are 7 to 10 mm thick and 4 cm in diameter in the anteroposterior plane [6]. They consist of three distinct components: (1) a central nucleus pulposus (NP), (2) a peripheral annulus fibrosus (AF), and (3) two cartilaginous endplates (CEPs) [6].
The IVDs are mostly avascular, with only small arteries supplying the outer AF and CEPs diffusing the inner AF and NP. Blood vessels in adjacent vertebral bodies and longitudinal ligaments transport nutrients as oxygen and glucose to IVD core passively [7,9]. Regarding innervation, the outer third of the AF is supplied by the sinuvertebral nerve, which originates from the union of the somatic root of the ventral ramus and autonomic root of the grey ramus communicans [7,10]. On the other hand, NP is not innervated at all [11]. Additionally, the posterior longitudinal ligament (PLL) and outer AF are innervated with nociceptive fibers from the ascending branch of the sinuvertebral nerve, which has been associated with chronic low back pain [6].
IVD degeneration is the most common cause of IVD herniation [1]. When the AF is compromised due to this degeneration or trauma, NP protrudes through it leading to a herniation [12]. The majority of the IVD herniations occur posterolaterally, as this area has the least amount of structural support from the longitudinal spinal ligaments and are more susceptible to compressive mechanical injury. This makes the traversing nerve root vulnerable to compression [12]. The exposure of the nerve roots to inflammatory cytokines, such as TNF-α, IL-1β and FGF, contribute to physical pain and radiculopathy [12,13,14]. In addition, FGF and midkine have been shown to recruit macrophages to the site of compression and play a role in both disc resorption and inflammatory response [12,13,14].
3. Radiological Stages of Disc Herniations
Given the clinical impact of LDH, a standardized approach to classifying disc pathology has been developed, improving decision making [15]. The morphological disc herniation types along with their definition and clinical considerations according to the North American Spine Society (NASS) nomenclature are summarized in Table 1 [16]. However, clinicians should always consider that surgical intervention is also associated to the topography of LDH, rather than radiologic morphology only.
The anatomical location of the disc material also plays a significant role in surgical planning. Therefore, LDHs can be classified based on their position relative to the spinal canal and neural elements. Table 2 describes the preferred endoscopic approaches for each herniation type based on anatomical location, an element of crucial importance in preoperative planning [17,18,19,20,21,22,23,24,25,26,27,28,29]. Additionally, Figure 1 provides schematic representations of the most common LDH types.
4. Transforaminal Endoscopic Lumbar Discectomy
General Overview
Before moving on to the specifics of each technique, it is important to note that such minimally invasive procedures are generally indicated in patients with persistent radicular symptoms who fail to respond to adequate conservative therapy. TELD is indicated in patients that present with unilateral radiculopathy, positive nerve root tension sign, foraminal, paracentral, or migrating disc herniations which, especially, are considered for this type of surgery (see Table 2) [21]. In addition, TELD approach is most appropriate in the upper lumbar levels due to larger foraminal dimensions [21]. Figure 2 provides an illustration of the TELD approach. Working corridor of TELD is schematically depicted in Figure 3.
Surgical Technique and Anatomical Landmarks
TELD is a minimally invasive procedure that is performed under local anesthesia so that the patient can be neurologically monitored intraoperatively [31]. There are two primary phases in this technique: (1) percutaneous access through the intervertebral foramen under fluoroscopic guidance, and (2) endoscopic decompression of the IVD herniation with real-time visualization [31]. Preoperative planning is of crucial importance for optimization of surgical outcome in TELD technique.
Magnetic Resonance Imaging (MRI), X-rays and Computed Tomography (CT) are used to localize IVD herniations and to determine the optimal entry point or trajectory of the disc and to underline iliac crest height in case of L5-S1 herniations [20,30,31]. Fluoroscopic guidance is used to maximize safety [20,21,31].
The patients lie prone on a radiolucent table. Alternatively, the lateral decubitus position may be adopted, with hip and knee in flexion to enlarge dimensions of the foraminal space [20,30,31]. Bending of table or using a shallow soft gel pillow at the appropriate level could help widen and open the foramen as well. However, this type of positioning is usually adopted in cases of foraminal stenosis [21]. Based on the anatomy, the entry point is usually 8-14 cm lateral to the midline [20,31]. This working corridor leads into Kambin’s triangle, a zone in the posterolateral lumbar foramen to access the herniated disc. This triangle is delineated by the exiting nerve root anteriorly, the superior CEP of the caudal vertebra inferiorly and the SAP of underlying vertebra posteriorly [4,26].
Under fluoroscopic guidance, an 18-gauge spinal needle is entered in the planned trajectory. The tip of the needle is then placed between the medial and lateral pedicular lines on anteroposterior (AP) intraoperative imaging, as well as at the posterior vertebral body line on lateral imaging [20,31]. In selected cases, the degenerated NP material can be stained and visualized to differentiate it from surrounding neural structures [31]. A guidewire is then inserted through the needle which is then followed by a stab incision so that a cannulated obturator can be introduced to gently dilate the soft tissues [30,31]. This is what ultimately establishes the working field [30,31]. In the outside-in variant of TELD, progressively larger reamers are being introduced over the guidewire to decompress the foramen before accessing the IVD, with diameters ranging from 4 mm to 9 mm [31]. Preoperative studying of the foraminal dimensions with the use of MRI and CT is extremely important when selecting the range of reamers in every patient.
Once the foraminal decompression is accomplished during this version of the technique, the obturator is introduced [21]. A beveled working cannula is placed over the obturator and positioned on the lateral aspect of the AF, which is fluoroscopically confirmed [31]. Finally, the endoscope is introduced along with continuous irrigation of the working channel. At this phase, it is crucial to first identify the anatomical landmarks: the SAP, the caudal pedicle, the exiting and traverse nerve roots, the AF and the herniated disc material [20,30]. Discectomy can be safely performed at this stage. The procedure is finished once the surgeon visualizes the dural sac and there is free mobilization of the nerve root [20,21,31].
Following the technical description of TELD, it is important to be aware of the potential complications and the learning curve that comes with it. A study by Fan et al. reported the total complication rate to be around 9.76% [32]. The most commonly reported complications included dysesthesia (1.46%), radicular pain (1.20%), dural tears (1.9%), recurrent LDH (2.3%), and persistent postoperative pain (3.79%) [32,33,34]. Patients with highly migrated herniations or foraminal stenosis featured also a higher incidence of incomplete decompression where reoperation was needed in 2-15% of cases [33]. Less common complications were infection (0.3%), epidural hematoma formation (0.04%), postoperative neurologic decline, pedicle fractures, urinary retention and intracranial hypertension [32,34]. In the systematic review by Ju et al. no major perioperative complications were found. The latter supports that TELD can be safely performed with the appropriate surgical expertise [34]. Regarding the learning curve, competency was reported after 7 to 72 cases, with a median of around 20 cases [35]. Operative time was decreased from 114 minutes to 80 minutes after the first 20 cases [35]. Another study identified a threshold of 35 cases, which also reported a 26.3% reduction in operative duration [35,36].
5. Interlaminar Endoscopic Lumbar Discectomy
General Overview
The IELD technique has initially been developed to treat central and paracentral herniations at L5-S1 level due to the wide interlaminar window [27,37,38]. Nevertheless, over time, this technique started being used more broadly in cases of large, migrated disc herniations, and even in foraminal and extraforaminal lesions via modified approaches [27,37,38]. Whenever TELD is restricted due to low intertransverse space, overlapping facet joints, or high iliac crests, the IELD technique may be effectively recruited [27,37,38]. Working corridor of IELD is schematically depicted in Figure 4.
IELD is indicated in patients who are unresponsive to conservative treatment and have large disc material that occupy more than 50% of the spinal canal with high grade caudal or cranial migration [17,37]. IELD is contraindicated when there is severe scoliosis or calcified disc herniations with adhesions to AF [17,37].
Surgical Technique and Anatomical Landmarks
IELD is a minimally invasive technique that allows posterior access to the spinal canal through the interlaminar window [17,20,27,37]. Utilized anatomical paths are similar to conventional microdiscectomy, despite being more challenging due to the use of the endoscope and limited field of view [17,20,27,37]. The patients are positioned in prone position with semi-flexed knees to flex the lumbar region and thus increase the interlaminar space, typically on a Wilson frame [27,38]. In contrast to TELD, IELD is usually done under general anesthesia [23,37].
Intraoperative fluoroscopy is used to localize the affected levels and to guide the entire surgical procedure [17,20,27,37]. The entry point on the skin in L5-S1 lesions is centered over the interlaminar window, 8-10 mm lateral to the spinous process on the symptomatic side [20,27,37]. However, in the upper levels the entry point should be directed toward the inferomedial margin of the rostral vertebra. In addition, tilting the C-arm distally allows for better and larger view of the interlaminar window. For obese patients, the surgeon should incise until the tip of the spinous process has been reached before moving laterally [38]. Then once the skin incision has been made, the thoracolumbar fascia is carefully incised without cutting through the ligamentum flavum (LF) [37].
Dilators are introduced towards the medial aspect of the facet joint, while using fluoroscopic guidance to confirm the correct position [37]. Once the position has been secured, a beveled working cannula is inserted over the dilator and after radiological verification of the position the endoscope is introduced [17,20].
In cases of severe degeneration, a high-speed drill and Kerrison rongeurs may be used to conduct a partial hemilaminotomy to widen the working area [17,20]. Additionally, the interlaminar space gets narrower at the cranial lumbar spine levels, with LF being covered by overlapped laminae [38]. In these cases, a hemilaminectomy or laminotomy is recommended [38]. At L5-S1 level, there is sufficient space for direct access without the need to resect bone [17,38]. Flavotomy and partial flavectomy is then performed to enter the epidural space. This may be facilitated hydrostatically with the use of saline pressure in the working cannula [38]. However, many techniques have been described for the opening of the LF, including direct puncture, longitudinal incision, transverse incision, and ligament detachment [29]. The recommended and most used approach in this step of the procedure is to make a longitudinal incision under tension parallel to LF fibers, so that expansion is controlled [38].
The outer layer of the LF is removed from the facet joint and interlaminar bone. The inner layer lies closer to the dural sac and has to be opened carefully using Kerrison rongeurs [20,37]. The endoscopic orientation is maintained by using the laminae, inferior articular process (IAP), SAP, LF, and facet joint capsule as anatomical landmarks [17,20,37]. Subsequently, the working cannula is utilized to enter the epidural space, whilst proper maneuvering of cannula in conjunction with dissectors and/or radiofrequency probes may also contribute at this stage. Once the epidural space is entered, cannula is appropriately rotated to protect the dural sac and nerve roots. Hence, surgeon would be able to identify these structures, subsequently utilizing the endoscopic dissectors and forceps for removal of herniated disc material.
It is recommended to intermittently derotate the working cannula during the procedure so that pressure on the neural structures is relieved. This is especially important in cases with spinal stenosis or when large disc fragments have to be removed [37]. In cases with bilateral symptoms or contralateral recess stenosis, the endoscope could be angled across the midline to decompress both sides, while preserving the contralateral bony structures that would otherwise have to be resected (over the top decompression) [17,20]. Hemostasis is achieved by bipolar coagulation and modulation of the irrigation pressure [20,37]. Additionally, epinephrine can be added to the irrigation fluid. An illustration of the intraoperative steps during IELD is shown in Figure 5. Like all surgical interventions, IELD is associated with risks and potential complications. The overall complication rate has been reported to be around 3.4%, which has been depicted to be lower than TELD in specific reports [33,39]. The most common complications included dural tears (2.19%), recurrent disc herniation (3.5%), and dysesthesia (1.3–3.1%) [33,39]. Less commonly reported complications are epidural hematoma (0.06–0.4%), infection (0.1%), and incomplete decompression (<5%) [33,39]. The competency in the IELD technique is achieved after around 50 to 60 cases, making it harder to master than the TELD approach [40,41]. Other studies suggest that proficiency is reached after around 51 cases [40,41]. The operative time has also been shown to decrease significantly, from an average of 90.2 minutes to 71.5 minutes [40,41].
6. Unilateral Biportal Endoscopic Lumbar Discectomy
General Overview
Unilateral biportal endoscopic lumbar discectomy (UBE-LD) is a minimally invasive surgical technique that makes use of two portals, one for visualization and the other for instrument manipulation [42,43,44]. Compared to the uniportal techniques that were previously mentioned, this allows for a wider range of view, as well as easier adaptation of the surgical instruments [18,42,44]. This approach has been clinically used in various types of discs herniations, including central, paracentral, foraminal, extraforaminal and even migrated pathologies [18,23,42,43,44]. In addition, it can provide bilateral decompression via a unilateral approach, while still preserving the facet joint and lamina [42,43,44]. Figure 6 illustrates the UBE-LD method.
Furthermore, this approach is particularly preferred in complex high-migrated cases, or multilevel stenosis and revision cases where the other endoscopic techniques are particularly limited [43,44]. However, this technique is also contraindicated in specific cases, like segmental instability or severe spondylolisthesis [43,44]. Additionally, even though UBE has been gaining a lot of popularity in the past years, surgeons must stay on the lookout for complications like thermal nerve injury, increased intracranial pressure, dural tears, and instability due to excessive bone resection [44].
Surgical Technique and Anatomical Landmarks
Even though it is possible for the UBE-LD technique to be performed under local or spinal anesthesia, it is generally performed under general anesthesia to make sure that the muscles are fully relaxed and patient is stable [18,23,42,43,44]. As with other posterior endoscopic approaches performed in the prone position, the patient gets place onto a radiolucent table using the Wilson frame to reduce lordosis and widen the working space [42]. Regardless of the approach used, it is important to minimize abdominal pressure during the surgery as this could lead to epidural venous bleeding, so the patients should be elevated with padded supports [42,43]. Additionally, the mean arterial pressure should be kept below 80 mmHg to reduce bleeding risk [42]. Portal placement is also guided by fluoroscopy with AP and lateral views [42].
There are three main UBE-LD surgical approaches that are used depending on the location of the herniation: (1) the interlaminar approach for central and paracentral herniations, (2) the contralateral approach for opposite lateral recess stenosis or hidden zone herniations, and (3) the paraspinal approach for foraminal and extraforaminal disc herniations by targeting the lateral facet and transverse process [42,43].
In the standard interlaminar approach, there are two incisions made 1 cm caudally and cranially the medial pedicle line of the affected disc level with an additional 2-3 cm spacing between them for better triangulation [23,42,43]. The portals are aligned with the lower margin of the cranial pedicle and at the midpoint of the caudal pedicle depending on the location of the disc herniation [42]. For example, foraminal or upward migrated herniations require a more caudal placement, and downward migration requires a more upward placement [42]. On the other hand, in paraspinal approaches the skin incisions are made on the tips of the spinous processes, 1-1.5 cm lateral to the pedicle to target the foramen in the lateral view and the docking point is aligned with the lateral border of the SAP or isthmus, depending on the level [42,43]. Additionally, placement of the portals is often difficult at the L5-S1 level due to the iliac crest being in the way and the facet joints being coronally oriented [42]. For example, when operating on the left side of this level, the working portal may be required to be placed 1 cm medial to the routine portal to bypass the iliac crest [42]. Once both portals are placed, the instruments and endoscope are triangulated to check if they are correctly angled within the interlaminar or paraspinal space [42,43].
Once correct placement is confirmed, a working space has to be created between the portals with the use of serial dilators [18,23]. These are inserted gently to position the multifidus muscle away from the lamina and facet joint, so the interlaminar or paraspinal space is opened depending on the approach used [43]. The viewing portal is subsequently established, and an endoscope (zero or thirty degrees, depending on localization of pathology being treated) is inserted at set to the isthmus [42,43]. Ideally this is done with a low-pressure pump under 30mmHg or via gravity to avoid neurological complications [42,43]. A clear visual field is established by removing soft tissue and fat by using a radiofrequency probe and shaver, identifying landmarks such as the spinolaminar junction and the ligamentum flavum [42,43].
Next step is laminotomy, which starts at the lower edge of the cranial lamina by using a drill that thins the bone until the LF is visible [42]. The lateral side of the dural sac and traversing nerve root are visualized and discectomy after proper nerve root medialization may be effectively performed. In the contralateral approach, the approach to laminotomy and flavectomy is more medial than the rest, requiring a more extensive resection of bone to reach the dural sac.
The total complication rate in UBE-LD ranges from 5% to 6.7% across multiple studies [33,45]. The most reported complications are dural tears (2-4.1%), epidural hematoma (1.9%), and recurrent disc herniation (<5%) [33,45]. Less commonly reported complications include transient paresthesia (0.14%) and infection (<0.5%) [33,45]. When comparing UBE-LD to the other uniportal endoscopic techniques, a slightly higher rate of dural injuries and postoperative hematomas may be encountered. However, this procedure is related to a lower incidence of postoperative dysesthesia. Considering learning curve, competency in UBE-LD is achieved after 32 to 54 cases, which obviously depends on the surgeon’s prior experience [46,47]. Peng et al. reported proficiency after around 32.2 cases, while Xu et al. put the threshold at 54 cases [46,47]. Table 3 provides a comparing overview and the differences between TELD, IELD, and UBE-LD [37,38,42,48,49,50,51,52,53,54,55,56,57].
7. Conclusions
In this review, an overview of the most promising endoscopic lumbar discectomy techniques has been provided, which have gained attention for their ability to decompress while associated with minimal soft tissue trauma. Even though there are remarkable advantages associated with endoscopic spine surgery, limitations associated with their wide utilization should be also considered. The challenges that remain point to the need for structured training programs and careful case selection, especially for beginners in the field. Evolution of new technological advances may further widen the applications of endoscopic approaches to manage more complex conditions such as deformities, tumors and multilevel decompressions. As innovations and experience are constantly acquired, the endoscopic techniques will play a significant role in shaping the future of spine care.
Author Contributions
Concept and design: S.K. and M.C.; Data collection: M.C. and N.G.; Data interpretation: S.K., M.C., N.G., and K.P.; Writing of the manuscript: M.C. and S.K.; Critical revision: S.K., M.C., N.G., and K.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zhou, M.; Theologis, A.A.; O’Connell, G.D. Understanding the Etiopathogenesis of Lumbar Intervertebral Disc Herniation: From Clinical Evidence to Basic Scientific Research. JOR Spine 2024, 7, e1289. [Google Scholar] [CrossRef]
- Wan, Z.Y.; Shan, H.; Liu, T.F.; Zhang, Z.C.; Jiang, M.; Zhang, Y.Z. Emerging Issues Questioning the Current Treatment Strategies for Lumbar Disc Herniation. Front. Surg. 2022, 9, 814531. [Google Scholar] [CrossRef]
- Dowling, T.J.; Munakomi, S.; Dowling, T.J. Microdiscectomy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025; Available online: http://www.ncbi.nlm.nih.gov/books/NBK555984/ (accessed on 18 April 2025).
- Burkett, D.; Brooks, N. Advances and Challenges of Endoscopic Spine Surgery. J. Clin. Med. 2024, 13, 1439. [Google Scholar] [CrossRef]
- Hofstetter, C.P.; Ahn, Y.; Choi, G.; Gibson, J.N.; Ruetten, S.; Zhou, Y.; Kim, H.S.; Yeung, A.; Telfeian, A.E.; Wagner, R. AOSpine Consensus Paper on Nomenclature for Working-Channel Endoscopic Spinal Procedures. Glob. Spine J. 2020, 10 (Suppl. 2), 111S–121S. [Google Scholar] [CrossRef] [PubMed]
- Raj, P.P. Intervertebral Disc: Anatomy–Physiology–Pathophysiology–Treatment. Pain Pract. 2008, 8(1), 18–44. [Google Scholar] [CrossRef]
- De Simone, M.; Choucha, A.; Ciaglia, E.; Varrassi, G.; Pergolizzi, J.; Paladini, A. Discogenic Low Back Pain: Anatomic and Pathophysiologic Characterization, Clinical Evaluation, Biomarkers, AI, and Treatment Options. J. Clin. Med. 2024, 13(19), 5915. [Google Scholar] [CrossRef]
- Adams, M.A.; Hutton, W.C. The Mechanical Function of the Lumbar Apophyseal Joints. Spine 1983, 8(3), 327–330. [Google Scholar] [CrossRef] [PubMed]
- Gkantsinikoudis, N.; Kapetanakis, S.; Magras, I.; Tsiridis, E.; Kritis, A. Tissue Engineering of Human Intervertebral Disc: A Concise Review. Tissue Eng. Part B Rev. 2022, 28(4), 848–860. [Google Scholar] [CrossRef]
- Bogduk, N. The Innervation of the Lumbar Spine. Spine 1983, 8, 286–293. [Google Scholar] [CrossRef]
- Freemont, A.J.; Peacock, T.E.; Goupille, P.; Hoyland, J.A.; O’Brien, J.; Jayson, M.I. Nerve Ingrowth into Diseased Intervertebral Disc in Chronic Back Pain. Lancet 1997, 350, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, G.D.; Guyre, C.A.; Vaccaro, A.R. The Epidemiology and Pathophysiology of Lumbar Disc Herniations. Semin. Spine Surg. 2016, 28(1), 2–7. [Google Scholar] [CrossRef]
- Nagashima, H.; Morio, Y.; Yamane, K.; Nanjo, Y.; Teshima, R. Tumor Necrosis Factor-Alpha, Interleukin-1Beta, and Interleukin-6 in the Cerebrospinal Fluid of Patients with Cervical Myelopathy and Lumbar Radiculopathy. Eur. Spine J. 2009, 18, 1946–1950. [Google Scholar] [CrossRef] [PubMed]
- Minamide, A.; Hashizume, H.; Yoshida, M.; Kawakami, M.; Hayashi, N.; Tamaki, T. Effects of Basic Fibroblast Growth Factor on Spontaneous Resorption of Herniated Intervertebral Discs: An Experimental Study in the Rabbit. Spine 1999, 24(10), 940–945. [Google Scholar] [CrossRef]
- Ahn, Y.; Kim, J.E.; Yoo, B.R.; Jeong, Y.M. A New Grading System for Migrated Lumbar Disc Herniation on Sagittal Magnetic Resonance Imaging: An Agreement Study. J. Clin. Med. 2022, 11(7), 1750. [Google Scholar] [CrossRef]
- Fardon, D.F.; Williams, A.L.; Dohring, E.J.; Murtagh, F.R.; Rothman, S.L.G.; Sze, G.K. Lumbar Disc Nomenclature: Version 2.0: Recommendations of the Combined Task Forces of the North American Spine Society, the American Society of Spine Radiology, and the American Society of Neuroradiology. Spine 2014, 39(24), E1448–E1465. [CrossRef]
- Wagner, R.; Haefner, M. Indications and Contraindications of Full-Endoscopic Interlaminar Lumbar Decompression. World Neurosurg. 2021, 145, 657–662. [Google Scholar] [CrossRef]
- Sun, W.; Wang, J.; Hu, Y.; Tao, J.; Yang, C. Efficacy and Safety of Unilateral Biportal Endoscopy Compared with Transforaminal Route Percutaneous Endoscopic Lumbar Decompression in the Treatment of Lumbar Spinal Stenosis: Minimum 1-Year Follow-Up. J. Pain Res. 2025, 18, 1071–1080. [Google Scholar] [CrossRef]
- Şahin, D.; Gülsever, C.İ.; Özata, M.S.; Uysal, İ.Y.; Aydoseli, A.; Aras, Y. Full Endoscopic Interlaminar Approach for Paracentral L5–S1 Disc Herniation. J. Vis. Exp. 2023, (194), 64717. [Google Scholar] [CrossRef]
- Van Isseldyk, F.; Padilla-Lichtenberger, F.; Guiroy, A.; Szmuda, T.; Gagliardi, M.; Kochanski, R.B.; López, W.; Fiani, B. Endoscopic Treatment of Lumbar Degenerative Disc Disease: A Narrative Review of Full-Endoscopic and Unilateral Biportal Endoscopic Spine Surgery. World Neurosurg. 2024, 188, e93–e107. [Google Scholar] [CrossRef]
- Kapetanakis, S.; Chaniotakis, C.; Tsioulas, P.; Gkantsinikoudis, N. Transforaminal Lumbar Endoscopic Discectomy: A Novel Alternative for Management of Lumbar Disc Herniation in Patients with Rheumatoid Arthritis? Neurospine 2024, 21(4), 1210–1218. [Google Scholar] [CrossRef]
- Gülsever, C.İ.; Şahin, D.; Ortahisar, E.; Erguven, M.; Sabancı, P.A.; Aras, Y. Full-Endoscopic Transforaminal Approach for Lumbar Discectomy. J. Vis. Exp. 2023, (199). [CrossRef]
- Jiang, H.W.; Chen, C.D.; Zhan, B.S.; Wang, Y.L.; Tang, P.; Jiang, X.S. Unilateral Biportal Endoscopic Discectomy versus Percutaneous Endoscopic Lumbar Discectomy in the Treatment of Lumbar Disc Herniation: A Retrospective Study. J. Orthop. Surg. 2022, 17(1), 30. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Lewandrowski, K.U. Five-Year Clinical Outcomes with Endoscopic Transforaminal Foraminoplasty for Symptomatic Degenerative Conditions of the Lumbar Spine: A Comparative Study of Inside-Out versus Outside-In Techniques. J. Spine Surg. 2020, 6 (Suppl. 1), S66–S83. [Google Scholar] [CrossRef]
- Bergamaschi, J.P.M.; De Oliveira Teixeira, K.; Soares, T.Q.; Almeida, J.P.; Garcia, A.C.; Linhares, M.N.; Faccioni, W.J. Extraforaminal Full-Endoscopic Approach for the Treatment of Lateral Compressive Diseases of the Lumbar Spine. J. Pers. Med. 2023, 13(3), 453. [Google Scholar] [CrossRef]
- Kapetanakis, S.; Gkantsinikoudis, N. Modified Transforaminal Lumbar Endoscopic Discectomy for Surgical Management of Extraforaminal Lumbar Disc Herniation: Case Series and Technical Note. J. Neurosurg. Spine 2025, 42(1), 49–55. [Google Scholar] [CrossRef]
- Yang, F.; Ren, L.; Ye, Q.; Wu, M.; Wang, G.; Guo, J. Endoscopic and Microscopic Interlaminar Discectomy for the Treatment of Far-Migrated Lumbar Disc Herniation: A Retrospective Study with a 24-Month Follow-Up. J. Pain Res. 2021, 14, 1593–1600. [Google Scholar] [CrossRef]
- Ahn, Y.; Jang, I.T.; Kim, W.K. Transforaminal Percutaneous Endoscopic Lumbar Discectomy for Very High-Grade Migrated Disc Herniation. Clin. Neurol. Neurosurg. 2016, 147, 11–17. [Google Scholar] [CrossRef]
- Tai, C.T.; Chen, K.T.; Jhang, S.W.; Lin, C.W.; Tsai, C.H.; Huang, K.Y.; Lin, Y.J. Transforaminal Endoscopic Lumbar Discectomy with Foraminoplasty for Down-Migrated Disc Herniation: A Single-Center Observational Study. J. Minim. Invasive Spine Surg. Tech. 2022, 7(1), 9–15. [Google Scholar] [CrossRef]
- Depauw, P.R.A.M.; Gadjradj, P.S.; Soria van Hoeve, J.S.; Harhangi, B.S. How I Do It: Percutaneous Transforaminal Endoscopic Discectomy for Lumbar Disk Herniation. Acta Neurochir. (Wien) 2018, 160(12), 2473–2477. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.G.; Ahn, Y. Transforaminal Endoscopic Lumbar Discectomy: Basic Concepts and Technical Keys to Clinical Success. Int. J. Spine Surg. 2021, 15 (Suppl. 3), S38–S46. [Google Scholar] [CrossRef] [PubMed]
- Fan, N.; Yuan, S.; Du, P.; Wei, Z.; Wu, Y.; Lu, H.; Gao, T. Complications and Risk Factors of Percutaneous Endoscopic Transforaminal Discectomy in the Treatment of Lumbar Spinal Stenosis. BMC Musculoskelet. Disord. 2021, 22(1), 1041. [Google Scholar] [CrossRef] [PubMed]
- Quillo-Olvera, J.; Quillo-Reséndiz, J.; Barrera-Arreola, M. Common Complications with Endoscopic Surgery and Management. Semin. Spine Surg. 2024, 36(1), 101087. [Google Scholar] [CrossRef]
- Ju, C.I.; Kim, P.; Ha, S.W.; Kim, S.W.; Lee, S.M. Contraindications and Complications of Full Endoscopic Lumbar Decompression for Lumbar Spinal Stenosis: A Systematic Review. World Neurosurg. 2022, 168, 398–410. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.P.; Olson, T.; Gabriel, B.; Rosinski, A.; Elsamadicy, A.; Mallow, G.; et al. What Is the Learning Curve for Endoscopic Spine Surgery? A Comprehensive Systematic Review. Spine J. 2025, in press. [CrossRef] [PubMed]
- Fleiderman, V.J.; Lecaros, B.J.; Cirillo, T.J.I.; Álvarez Lemos, F.; Osorio, V.P.; Wolff, B.N. Transforaminal Endoscopic Lumbar Discectomy: Learning Curve of a Single Surgeon. J. Spine Surg. 2023, 9(2), 159–165. [Google Scholar] [CrossRef]
- Won, Y.I.; Yuh, W.T.; Kwon, S.W.; Kim, C.H.; Kim, K.T.; Lee, S.G. Interlaminar Endoscopic Lumbar Discectomy: A Narrative Review. Int. J. Spine Surg. 2021, 15 (Suppl. 3), S47–S53. [Google Scholar] [CrossRef]
- González-Murillo, M.; Castro-Toral, J.; Casal-Grau, R.; Bonome-Roel, C.; Bonome-González, C.; De Mon-Montoliú, J.Á. Technical Considerations and Avoiding Complications in Interlaminar Endoscopic Lumbar Discectomy. J. Minim. Invasive Spine Surg. Tech. 2024, 9 (Suppl. 2), S136–S140. [Google Scholar] [CrossRef]
- Lee, C.H.; Choi, M.; Ryu, D.S.; Choi, I.; Kim, C.H.; Jung, S.K.; Sohn, M.J. Efficacy and Safety of Full-Endoscopic Decompression via Interlaminar Approach for Central or Lateral Recess Spinal Stenosis of the Lumbar Spine: A Meta-Analysis. Spine 2018, 43(24), 1756–1764. [Google Scholar] [CrossRef]
- Jamaleddine, Y.; Haj Hussein, A.; Honeine, M.O.; El Masri, J.; Khoury, J.; Haidar, R.; Haidar, H. Evaluating the Learning Curve and Operative Time of Interlaminar and Transforaminal Endoscopic Lumbar Discectomy. Brain Spine 2025, 5, 104225. [Google Scholar] [CrossRef]
- Koh, C.H.; Booker, J.; Choi, D.; Lin, Y.; Ahmad, F.; Smith, N.; et al. Learning Curve of Endoscopic Lumbar Discectomy: A Systematic Review and Meta-Analysis of Individual Participant and Aggregated Data. Glob. Spine J. 2025, 15(2), 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- So, J.Y.; Park, J.Y. Essential Surgical Techniques during Unilateral Biportal Endoscopic Spine Surgery. J. Minim. Invasive Spine Surg. Tech. 2023, 8(2), 186–197. [Google Scholar] [CrossRef]
- Mumcu, C. Unilateral Biportal Endoscopy for Non-Migrated Lumbar Disc Herniation. In Unilateral Biportal Endoscopy of the Spine; Quillo-Olvera, J., Quillo-Olvera, D., Quillo-Reséndiz, J., Mayer, M., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 185–204. [Google Scholar] [CrossRef]
- Choi, C.M. Biportal Endoscopic Spine Surgery (BESS): Considering Merits and Pitfalls. J. Spine Surg. 2020, 6(2), 457–465. [Google Scholar] [CrossRef]
- Pan, M.; Li, Q.; Li, S.; Ma, Y.; Yang, H.; Xu, J.; Li, X. Percutaneous Endoscopic Lumbar Discectomy: Indications and Complications. Pain Physician 2020, 23(1), 49–56. [Google Scholar] [CrossRef]
- Peng, J.; Lin, R.; Fang, D.; He, Z.; Zhao, Q.; Li, Q. Learning Curve Insights in Unilateral Biportal Endoscopic (UBE) Spinal Procedures: Proficiency Cutoffs and the Impact on Efficiency and Complications. Eur. Spine J. 2025, 34(3), 954–973. [Google Scholar] [CrossRef]
- Xu, J.; Wang, D.; Liu, J.; Zhang, H.; Chen, Y.; Huang, B.; et al. Learning Curve and Complications of Unilateral Biportal Endoscopy: Cumulative Sum and Risk-Adjusted Cumulative Sum Analysis. Neurospine 2022, 19(3), 792–804. [Google Scholar] [CrossRef]
- Lewandrowski, K.U. The Strategies behind “Inside-Out” and “Outside-In” Endoscopy of the Lumbar Spine: Treating the Pain Generator. J. Spine Surg. 2020, 6 (Suppl. 1), S35–S39. [Google Scholar] [CrossRef] [PubMed]
- Kambin, P.; Casey, K.; O’Brien, E.; Zhou, L. Transforaminal Arthroscopic Decompression of Lateral Recess Stenosis. J. Neurosurg. 1996, 84(3), 462–467. [Google Scholar] [CrossRef]
- Hijikata, S. Percutaneous Nucleotomy: A New Concept Technique and 12 Years’ Experience. Clin. Orthop. Relat. Res. 1989, (238), 9–23. [Google Scholar] [CrossRef]
- Ruetten, S.; Komp, M.; Godolias, G. A New Full-Endoscopic Technique for the Interlaminar Operation of Lumbar Disc Herniations Using 6-mm Endoscopes: Prospective 2-Year Results of 331 Patients. Minim. Invasive Neurosurg. 2006, 49(2), 80–87. [Google Scholar] [CrossRef]
- Mayer, H.M. A History of Endoscopic Lumbar Spine Surgery: What Have We Learnt? Biomed. Res. Int. 2019, 2019, 4583943. [Google Scholar] [CrossRef] [PubMed]
- Hwa Eum, J.; Hwa Heo, D.; Son, S.K.; Park, C.K. Percutaneous Biportal Endoscopic Decompression for Lumbar Spinal Stenosis: A Technical Note and Preliminary Clinical Results. J. Neurosurg. Spine 2016, 24(4), 602–607. [Google Scholar] [CrossRef]
- Choi, C.M.; Chung, J.T.; Lee, S.J.; Choi, D.J. How I Do It? Acta Neurochir. (Wien) 2016, 158(3), 459–463. [Google Scholar] [CrossRef]
- Zhong, Y.; Wang, J.; Liang, Z.; Han, T.; Lu, H.; Hou, Z. Bibliometric and Visualization Analysis of Research Hotspots and Frontiers in Endoscopic Lumbar Discectomy. J. Pain Res. 2024, 17, 2165–2190. [Google Scholar] [CrossRef] [PubMed]
- Jitpakdee, K.; Liu, Y.; Heo, D.H.; Kotheeranurak, V.; Suvithayasiri, S.; Kim, J.S. Minimally Invasive Endoscopy in Spine Surgery: Where Are We Now? Spine J. 2023, 32(8), 2755–2768. [Google Scholar] [CrossRef] [PubMed]
- De Antoni, D.J.; Claro, M.L.; Poehling, G.G.; Hughes, S.S. Translaminar Lumbar Epidural Endoscopy: Anatomy, Technique, and Indications. Arthroscopy 1996, 12(3), 330–334. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic overview of LDH types and migration patterns. (A) normal vertebra without herniation; (B) foraminal LDH; (C) cranially migrated disc herniation; (D) paracentral herniation; (E) central herniation; (F) caudally migrated disc herniation.
Figure 1.
Schematic overview of LDH types and migration patterns. (A) normal vertebra without herniation; (B) foraminal LDH; (C) cranially migrated disc herniation; (D) paracentral herniation; (E) central herniation; (F) caudally migrated disc herniation.
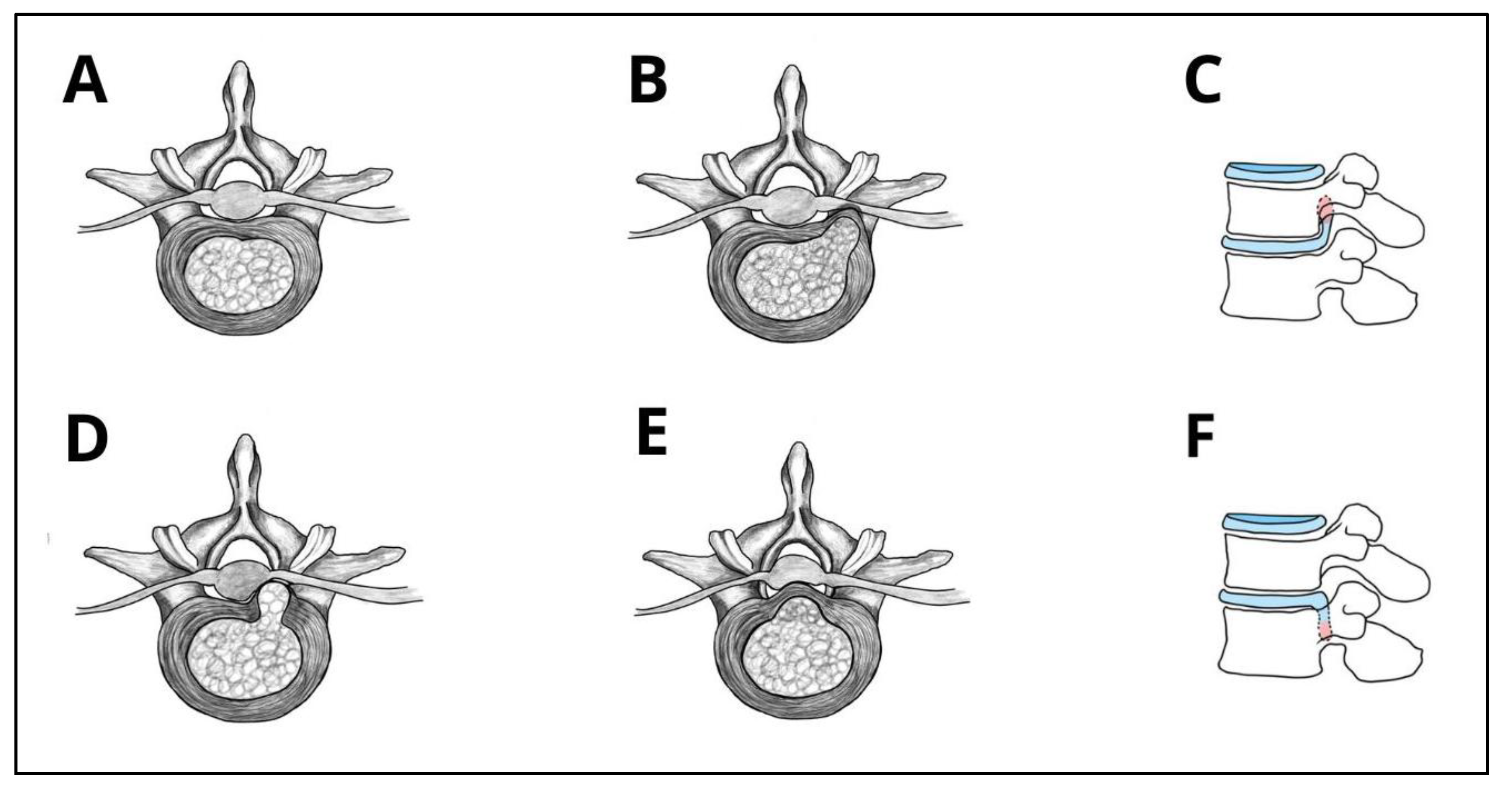
Figure 2.
Illustration of the transforaminal endoscopic lumbar discectomy (TELD) approach. The endoscope and working instruments are inserted through Kambin’s triangle.
Figure 2.
Illustration of the transforaminal endoscopic lumbar discectomy (TELD) approach. The endoscope and working instruments are inserted through Kambin’s triangle.
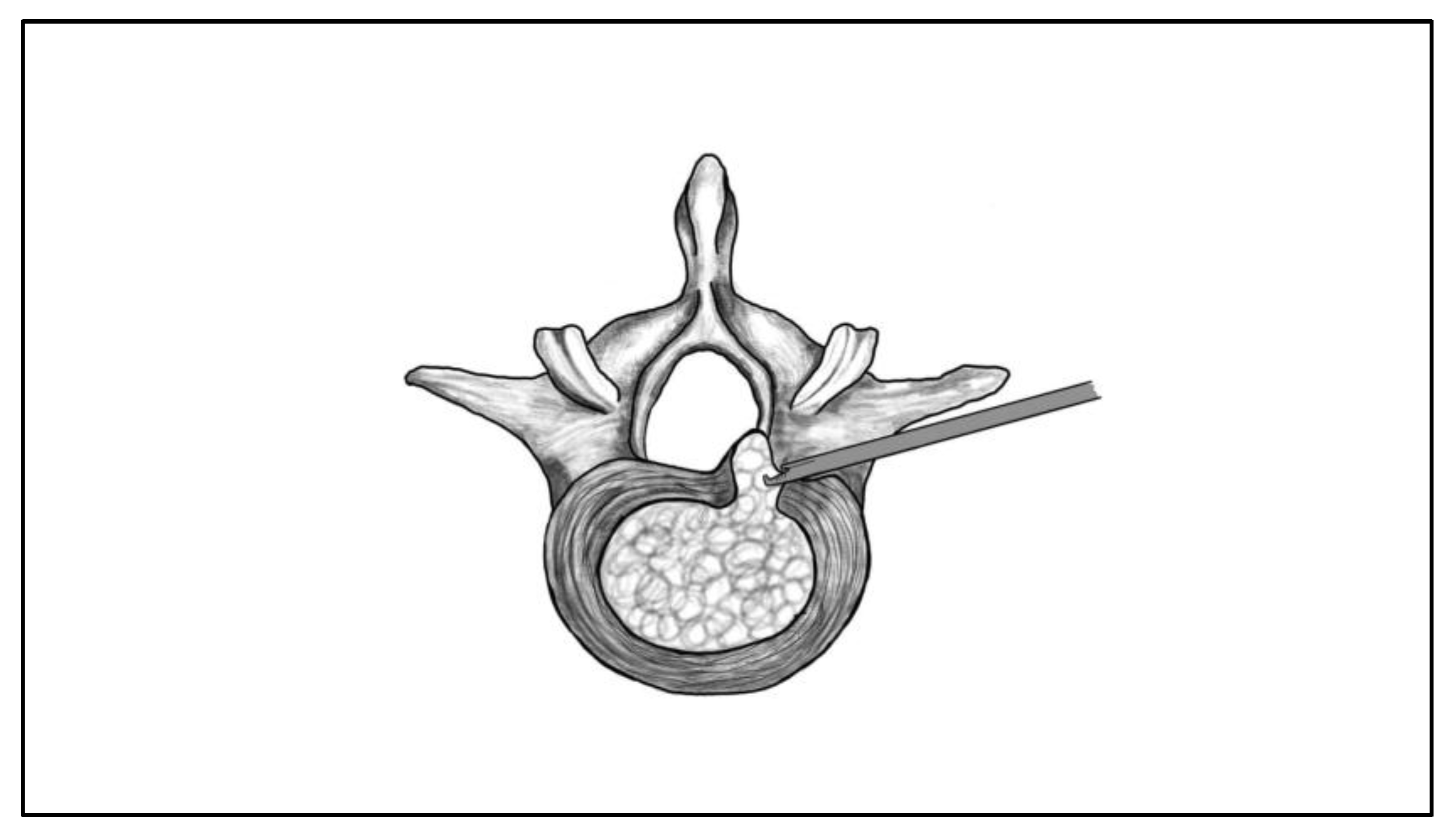
Figure 3.
Step-by-step intraoperative sequence of TELD. (a) Patient positioning and skin marking in lateral decubitus position with planned entry trajectory. (b) Insertion of the K-wire at the predetermined entry point under fluoroscopic guidance. (c) Sequential foraminal dilation using reamers to expand the working corridor. (d) Placement of the beveled working cannula through the soft tissue corridor toward the disc space. (e) Endoscopic view showing excision of herniated disc material using grasping forceps. (f) Final endoscopic view demonstrating a pulsatile traversing nerve root after successful decompression, visualized as a white band, indicating the primary endpoint of adequate neural release.
Figure 3.
Step-by-step intraoperative sequence of TELD. (a) Patient positioning and skin marking in lateral decubitus position with planned entry trajectory. (b) Insertion of the K-wire at the predetermined entry point under fluoroscopic guidance. (c) Sequential foraminal dilation using reamers to expand the working corridor. (d) Placement of the beveled working cannula through the soft tissue corridor toward the disc space. (e) Endoscopic view showing excision of herniated disc material using grasping forceps. (f) Final endoscopic view demonstrating a pulsatile traversing nerve root after successful decompression, visualized as a white band, indicating the primary endpoint of adequate neural release.
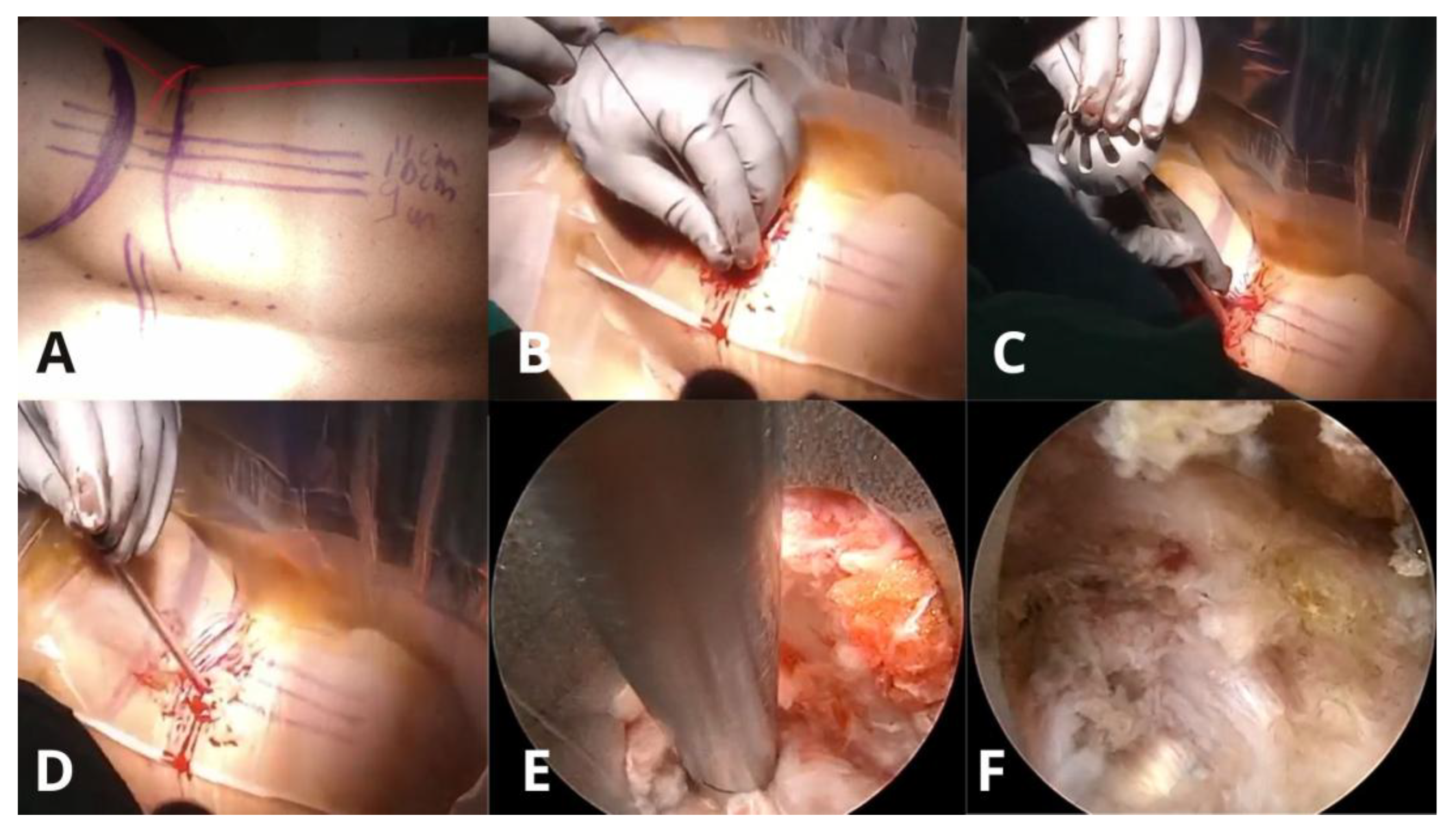
Figure 4.
Illustration of the interlaminar endoscopic lumbar discectomy (IELD) approach. The endoscope and working instruments are inserted through the interlaminar space.
Figure 4.
Illustration of the interlaminar endoscopic lumbar discectomy (IELD) approach. The endoscope and working instruments are inserted through the interlaminar space.
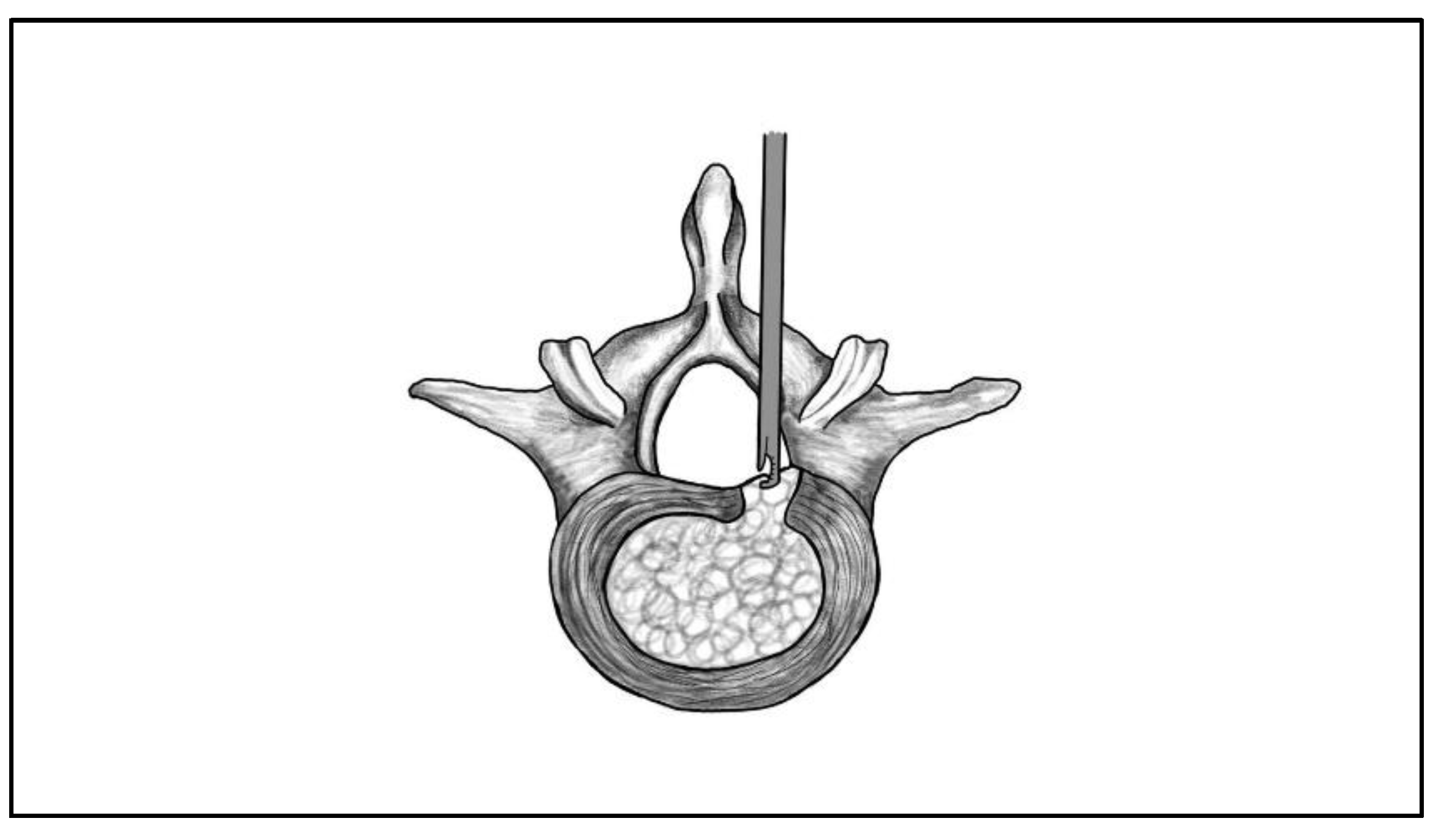
Figure 5.
Step-by-step intraoperative endoscopic views during an IELD at L5–S1 at our outpatient clinic. (A) The procedure begins with the initial flavotomy, where the outer layer of the ligamentum flavum is opened to access the deeper layers. (B) Further dissection allows entry into the epidural space, exposing the neural structures. (C) The working channel is advanced toward the epidural space. (D) The traversing nerve root is mobilized, revealing the displaced disc material beneath it. (E) A radiofrequency probe is used to safely release the LDH from the annulus. (F) Final inspection after disc removal confirms full decompression of the nerve root and restoration of the epidural space.
Figure 5.
Step-by-step intraoperative endoscopic views during an IELD at L5–S1 at our outpatient clinic. (A) The procedure begins with the initial flavotomy, where the outer layer of the ligamentum flavum is opened to access the deeper layers. (B) Further dissection allows entry into the epidural space, exposing the neural structures. (C) The working channel is advanced toward the epidural space. (D) The traversing nerve root is mobilized, revealing the displaced disc material beneath it. (E) A radiofrequency probe is used to safely release the LDH from the annulus. (F) Final inspection after disc removal confirms full decompression of the nerve root and restoration of the epidural space.
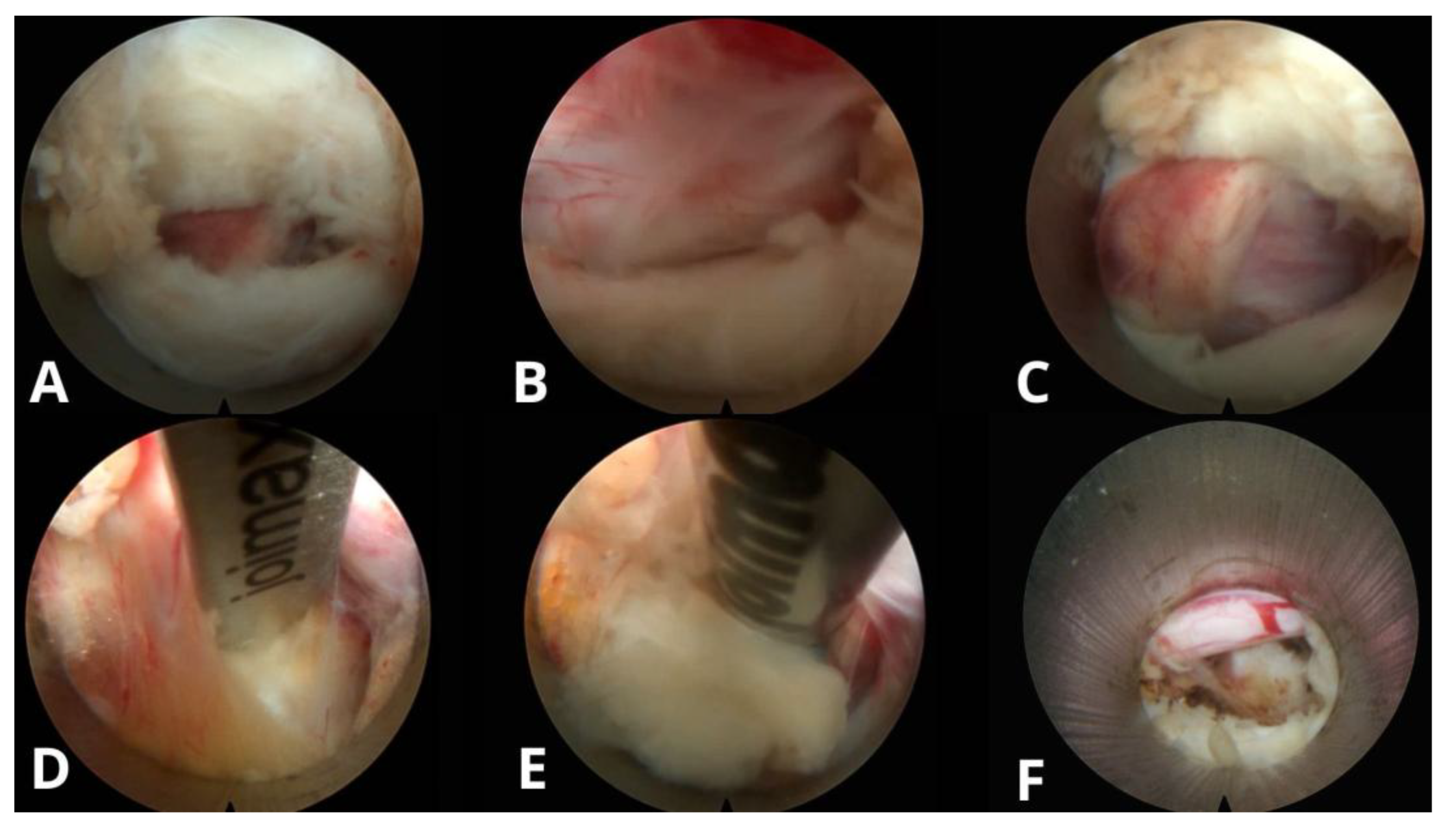
Figure 6.
Illustration of the unilateral biportal endoscopic lumbar discectomy (UBE-LD) technique. Two independent portals are used: one for endoscopic visualization and one for instrumentation.
Figure 6.
Illustration of the unilateral biportal endoscopic lumbar discectomy (UBE-LD) technique. Two independent portals are used: one for endoscopic visualization and one for instrumentation.
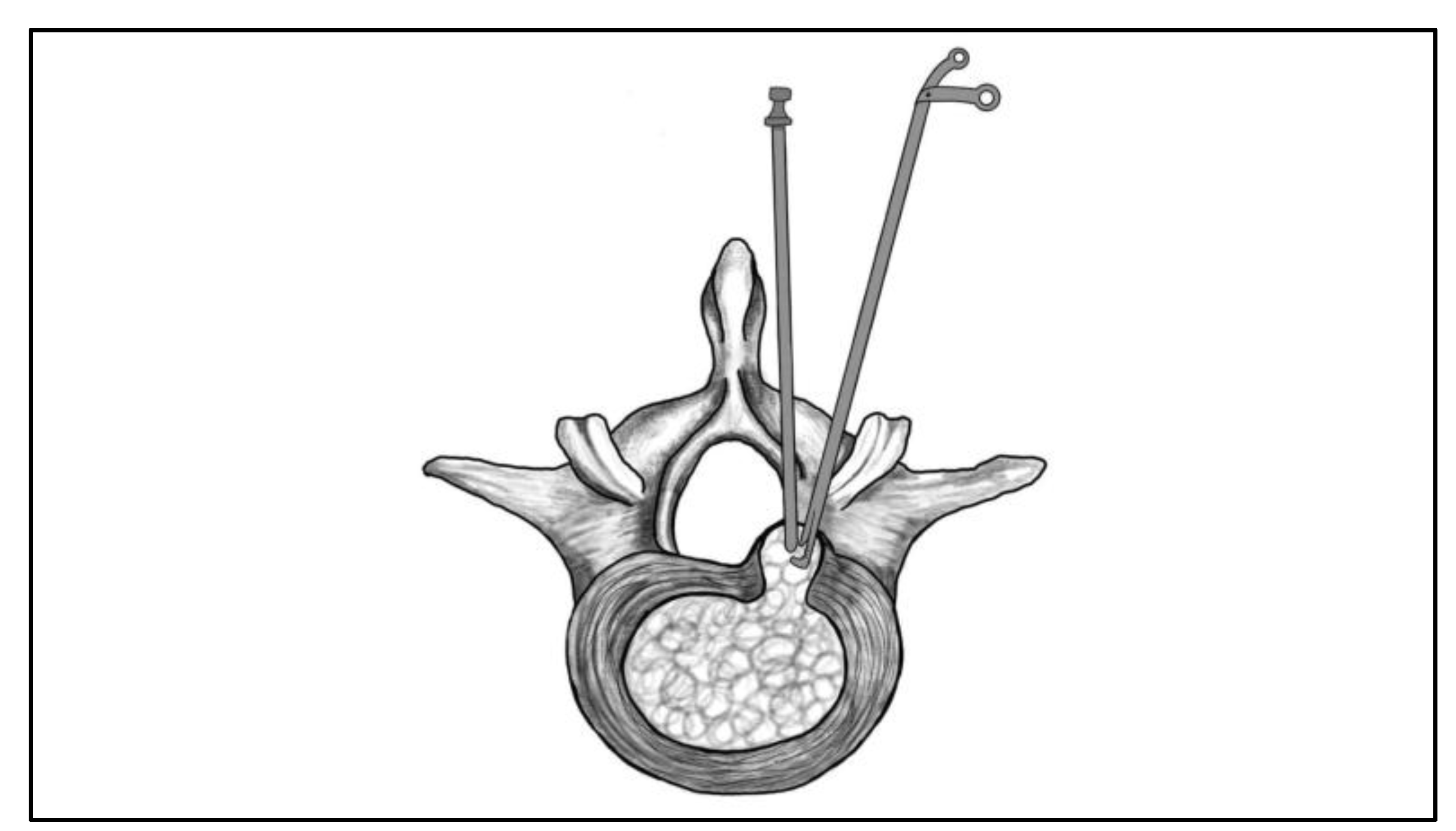

Table 1.
Summary of morphological types of LDH. Including their definitions and relevant clinical considerations, adapted from the NASS 2014 lumbar disc nomenclature version 2.0 [16].
Table 1.
Summary of morphological types of LDH. Including their definitions and relevant clinical considerations, adapted from the NASS 2014 lumbar disc nomenclature version 2.0 [16].
| Morphological Type | Definition | Clinical Considerations |
| Protrusion | Localized displacement where the width of herniation is smaller than the width of the base at the disc margin | Often asymptomatic or mildly symptomatic; usually responds well to conservative treatment; persistent bulging may lead to poorer conservative outcomes in some cases |
| Extrusion (contained) | Displaced portion of NP material with a narrower base than its displaced portion extends beyond AF, but remains covered by AF or PLL | Symptomatic cases could benefit from endoscopic decompression, as persistent bulging often leads to poor response to conservative treatment; however, if nerve compression is minimal, observation may still be appropriate. |
| Extrusion (uncontained) | Displaced portion of NP material with a narrower base than its displaced portion extends beyond AF, but remains covered by AF or PLL | Exposure causes higher inflammatory response, causing radiculopathy; usually responsive to surgical intervention. |
| Sequestration | Free NP fragment displaced from extrusion site and completely separated from disc, might migrate cranially/caudally | High surgical indication due to fragment migrations and acute symptoms; localization is important in surgical planning; spontaneous resorption typically occurs within 6–12 weeks. Follow-up MRI may show resolution, but residual pain may persist due to inflammatory response to NP exposure. |
Table 2.
Summary of LDH types based on anatomical location.
| Anatomical Location | Preferred Endoscopic Approach | Surgical Insights & Notes |
| Central | Interlaminar [17]; UBE-LD [18] | Especially effective at L4–L5 and L5–S1, due to wider interlaminar window; Allows preservation of posterior elements, such as facet joints and lamina [17]; UBE provides bigger working space and has bilateral decompression capabilities [18]. The same applies to IELD, but in experienced hands. |
| Paracentral | Interlaminar [19]; Transforaminal [20,21,22]; UBE-LD [18,23] | Interlaminar approach is often preferred at L5-S1 due to high iliac crest [19]; The traversing nerve root is usually compressed, so precise decompression is critical to avoid residual symptoms; Annular modulation or foraminoplasty is rarely required; UBE is effective for paracentral herniations, including at L5–S1, where narrow foraminal access may limit transforaminal approaches [18,23]. |
| Foraminal | Transforaminal with foraminoplasty [24]; Modified Transforaminal [25]; Paraspinal or contralateral UBE-LD [23] | The transforaminal inside-out technique allows early intradiscal access, outside-in technique is more effective for severe foraminal stenosis and allows for more extensive bone resection [24]; Foraminoplasty allows for direct visualization of the entire neuroforamen, including the “hidden zone of Macnab” [24]; extraforaminal approach used when pathology lies lateral to facet joint [25]. |
| Extraforaminal (Far-Lateral) | Modified Transforaminal [25,26]; | Allows preservation of posterior elements, such as facet joints and lamina; Technically demanding due to limited working space and proximity to dorsal root ganglion [25]. |
| Cranially Migrated | Interlaminar [27]; Transforaminal [28]; UBE-LD [23] | Performing a foraminotomy is usually indicated in transforaminal approach [28]; calcified disc could convert to bone resection or open surgery; UBE accesses cranially migrated herniations not reachable with TELD [23]. |
| Caudally Migrated | Interlaminar [27]; Transforaminal [29]; UBE-LD [23] | Performing a foraminotomy is usually indicated in transforaminal approach; calcified disc could convert to bone resection or open surgery [23]. |
Table 3.
Comparison of the three full-endoscopic discectomy techniques. Including TELD, IELD, and UBE/UBE-LD.
Table 3.
Comparison of the three full-endoscopic discectomy techniques. Including TELD, IELD, and UBE/UBE-LD.
| Approach | Technique Types | First Surgery | Geographic Trends |
| Transforaminal Endoscopic Lumbar Discectomy (TELD) | Inside-out & Outside-in [48] | Concept by Kambin (1973) [49]; first surgery by Hijikata (1975) [50] | Not specific to one approach, bibliometric analyses of FELD research show that China, South Korea, and the United States dominate the field, with over 80% of published studies [55]. |
| Interlaminar Endoscopic Lumbar Discectomy (IELD) | Single Technique with minor variations: Direct-Posterior, Translaminar&Axillary/Shoulder [37,38] | First described as open interlaminar discectomy, adapted to full-endoscopic by Ruetten et al. (2006) [51,52] | Not specific to one approach, bibliometric analyses of FELD research show that China, South Korea, and the United States dominate the field, with over 80% of published studies [55]. |
| Unilateral Biportal Endoscopic Lumbar Discectomy (UBE-LD) | Interlaminar, Contralateral&Paraspinal [42] | Concept by De Antoni et al. (1996) [57]; modern biportal technique first defined by Choi et al. & Eum et al. (2016) [53,54] | Primarily developed and studied in South Korea (82.4% of publications); top 10 most-cited UBE articles are all from South Korea [56]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



