Submitted:
15 July 2024
Posted:
16 July 2024
You are already at the latest version
Abstract
Objective To explore the endoscopic anatomical structures of lumbar surgery. Methods A total of 290 patients who underwent lumbar endoscopic surgery due to lumbar intervertebral disc (IVD) herniation from September 2020 to September 2022 were retrospectively reviewed in our hospital,179 patients had complete surgical video recordings, including 108 males and 71 females, aged from 19 to 65 years, with an average age of 41±16 years. The endoscopic structures through the intervertebral foramen and interlaminar space were independently identified by 3 doctors with more than 3 years of related surgery experience. When there were differences of opinions, the three doctors would discuss and come to a consensus. The probability, location, and neighboring structures of each specific structures were statistically analyzed. Results The anatomical structures observed through the lumbar foramen under endoscopy include muscles and ligaments attached to the superior articular process (SAP), main blood vessels inside the intervertebral foramen, blood vessels on the surface of IVD, and blood vessels on the surface of the dural sac and nerve root. The major anatomical structures observed through interlaminar space are multifidus, the conjugated ligament of ligament flavum and capsule ligament (capsule part of flavum ligaments), edges of the lamina, specific vessel bundle to facet with exit nerve root. Conclusion The anatomical structures under spinal endoscopy have certain characteristics, which are grossly different from those under open surgery. Familiarity with these anatomical structures has important clinical significance.
Keywords:
lumbar endoscopic surgery
; transforaminal
; interlaminar
; endoscopic anatomy structure
Spinal endoscopy can enlarge the structures by 3-10 times, or even higher [1]. This is significantly different from the structures seen in traditional open surgery, where submillimeter-sized structures cannot be observed by the naked eye. Although microscopic surgery also has a magnifying effect, it is far less clear than in aqueous medium. Through spinal endoscopy, one can clearly see the accompanying blood vessels of the nerve roots, blood vessels on the anulus fibrosus, ligaments attached to the facet joints, and as far as we know, some of which have not been named anatomically. In open surgery, we often ignore some microscopic structures, seemingly without affecting the completion of the surgery. However, neglecting these structures under endoscopy may result in bleeding, affecting the surgical field of view, and causing injury to nerves and blood vessels. These submillimeter-sized blood vessels, nerves, and ligaments are also part of the local anatomic microenvironment. Protecting them as much as possible can reduce invasion to the local microenvironment, and help the nerves obtain enough nutrients and recover their function [2,3]. Studying these submillimeter-sized microstructures and their characteristics can help distinguish the operative anatomic location and anatomical structures in a timely manner, and have certain clinical significance.
1. Clinical Data and Methods
1.1. General Information
The study collected data from patients who underwent full spine endoscopic surgery at our hospital from September 2020 to September 2022, including their age, gender, chief complaint, diagnosis, surgical method, surgical approach, and surgical videos.
Inclusion criteria: patients aged between 18 and 80; underwent the first lumbar spine full endoscopic surgery; have no history of lumbar intervention or surgery.
Exclusion criteria: have a history of mental illness; have lumbar spondylolisthesis; have structural abnormalities such as congenital spine cleft or segmentation anomaly; have suspected spinal infections; have primary or secondary tumors in the spine; and have no high-definition video during surgery or do not cooperate with the research protocol.
1.2. Methods
According to the surgical approach, the enrolled patients were divided into two groups: interlaminar approach and transforaminal approach. The high-definition videos of operation were reviewed by 3 members of the research group independently. The names of the microscopic structures were approved if recognized consistently by the method, or the structure with different views were assigned to all study group members for discussion.
For these microscopic anatomical structures, the probability of occurrence, variation, origin position, function and other structural characteristics were further studied, so as to clarify their spatial position and clinical significance in spinal endoscopic surgery.
1.3. Statistics
SPSS 20.0 was used to calculate the probability of occurrence of the newly discovered specific structures and the probability of variation, and the value of P≤0.05 indicates that differences are statistically significant.
2. Results
A total of 290 patients who underwent lumbar endoscopic surgery were included in this study. After excluding 111 patients without complete surgical videos, a total of 179 patients who underwent lumbar endoscopic surgery with IVD herniation were finally included, with 108 males and 71 females, aged 19 to 65 years old, with a mean age of 41±16 years. There were no significant differences in general information between patients with the two approaches. The intervertebral foramen approach was the most commonly used approach for lumbar endoscopic surgery, followed by the interlaminar space approach, both of which are common approaches of minimal invasive spine surgery. In addition to some well-known anatomical structures, this study also found the distribution of some blood vessels on the IVD and annulus fibrosus, ligaments and blood vessels in the intervertebral foramen area, and the distribution of blood vessels on the dura mater and nerve roots (seen in Table 1).
Figure 1.
Diagram of lumbar vessel system. (A) Diagram of lumbar artery system from sagittal view. (B) Diagram of lumbar venous system from sagittal view. (C) Diagram of lumbar artery system on the ventral side of dura sac (posterior vertebral body). (D) Diagram of lumbar venous system on the ventral side of dura sac. The use of these images has been approved by the copyright owner (https://clinicalgate.com/blood-supply-of-the-lumbar-spine/#bib3).
Figure 1.
Diagram of lumbar vessel system. (A) Diagram of lumbar artery system from sagittal view. (B) Diagram of lumbar venous system from sagittal view. (C) Diagram of lumbar artery system on the ventral side of dura sac (posterior vertebral body). (D) Diagram of lumbar venous system on the ventral side of dura sac. The use of these images has been approved by the copyright owner (https://clinicalgate.com/blood-supply-of-the-lumbar-spine/#bib3).
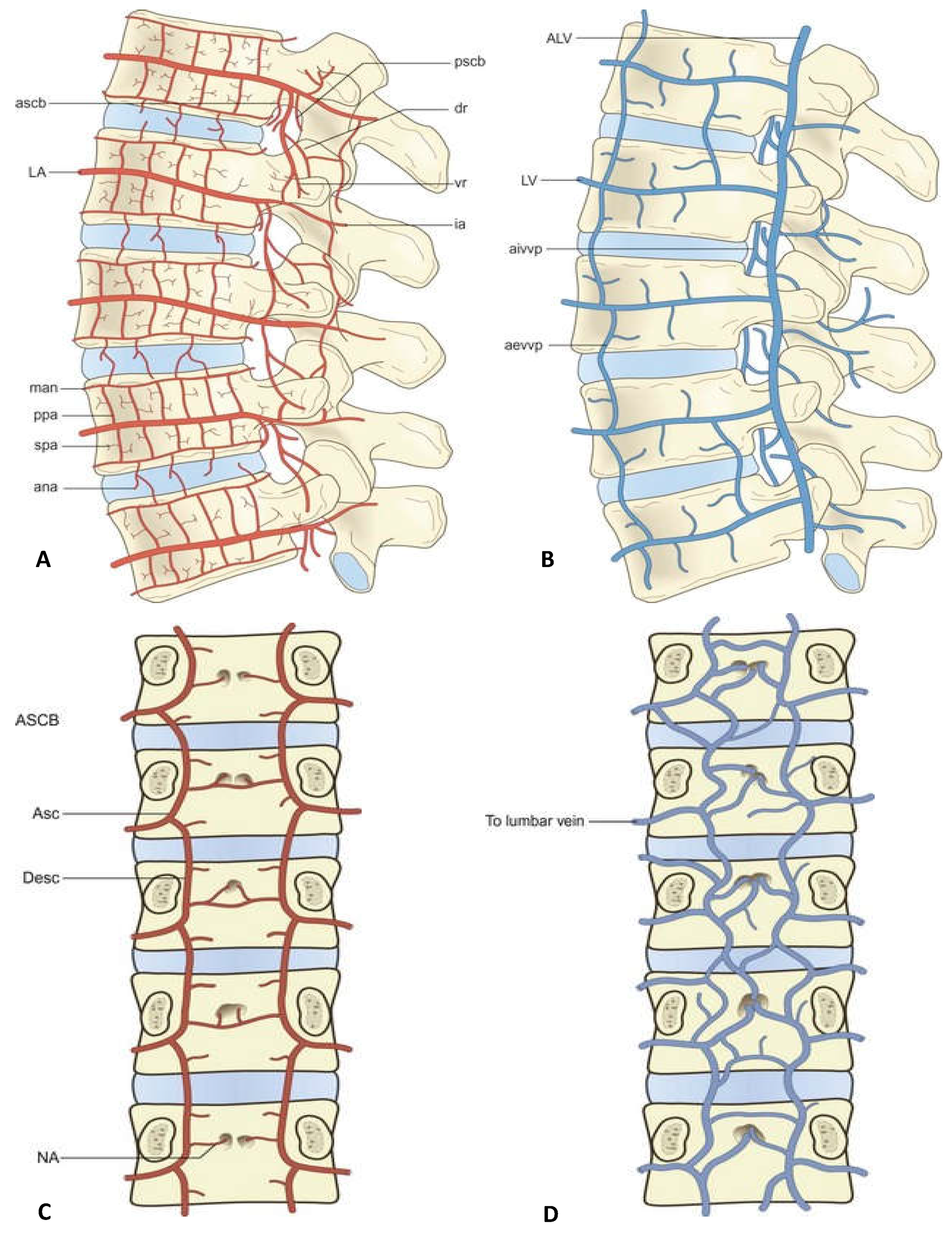
ana, anastomosis over the surface of the lumbar IVD; ascb, anterior spinal canal branch; dr, branches accompanying dorsal ramus of spinal nerve; ia, posterior branch related to the pars interarticularis of the lamina; LA, lumbar artery; man, metaphysial anastomosis; ppa, primary periosteal artery; pscb, posterior spinal canal branch; spa, secondary periosteal artery; vr, branches accompanying ventral ramus of spinal nerve; NA, nutrient arteries; lumbar ascending branch (ab.); lumbar descending branch (desc.)
aevvp, elements of the anterior external vertebral venous plexus; pevvp, posterior external vertebral venous plexus; aivvp, elements of the anterior internal vertebral venous plexus; ALV, ascending lumbar vein; LV, lumbar vein;
medial AIVV; pivvp, posterior internal vertebral venous plexus, basivertebral vein; IVV, intervertebral vein.
After removing part of the bone from the ventral side of the SAP, the ligamentum flavum in the ventral side of the articular process can be seen (Figure 2A,B), and there are cross-linked ligaments in the annulus fibrosus and the posterior longitudinal ligament of IVD, which assist in fixing the dura and nerve roots (Figure 2C). The nerve root ventral to the ligamentum flavum and the ventral IVD to the nerve root form a disc-nerve root-ligamentum flavum, sandwich structure (Figure 2D). The sandwich structure is a unique mirror image seen under the foraminal approach, especially after the removal of part of the ventral SAP, it is more clearly visible, and is an important anatomical symbol under the microscope. The dorsal is the yellow ligament, the ventral is the posterior longitudinal ligament or IVD, and the nerve root is in the middle. After the removal of the ventral bone of the SAP, the ligamentum flavum was exposed.
2.1. Ligaments Attached to the SAP
The SAP is one of the most important anatomical symbols through the foraminal approach, and many ligaments attach to it, as well as MM. There are generally three muscular ligaments attached to the SAP, namely the MM, the medial intertransverse muscle and the lateral intertransverse muscle, which connect the articular process with the spinous process and the transverse process. In addition, there are also ligaments in the transverse process and the posterior vertebral body, namely, superior corporotransverse ligaments, inferior corporotransverse ligaments, superior-transforaminal ligament, mid-transforaminal ligament and inferior-transforaminal ligament (Table 1).
2.2. IVD and AF Under Endoscopy
In patients with degenerated IVD, the annulus fibrosus is usually porcelain white (Figure 2E, 2F), accompanied by inflammatory hyperplasia, and bulge. If the outer annulus fibrosus is perforated, there will often be serious local inflammatory tissue encapsulation, and protruding nucleus pulposus and annulus fibrosus can often be found after removing the inflammatory tissue (Figure 2G). A network of blood vessels can be seen on the surface of the microscopic ring (Figure 2F), which are usually distributed transversely and have branches that are often cross-linked with each other. The annulus fibrosus of the IVD is directly connected to the posterior longitudinal ligament, which cross-link to the ligamentum flavum (Figure 2C). The annulus fibrosus and the posterior longitudinal ligament are cross-linked ligaments, which are important anatomical markers, located between the ventral dural and the IVD, starting from the IVD, oblique, about 5-10mm in diameter, and their main function is to fix the dural and nerve roots. Sometimes, in order to show the ventral dural, this ligament has to be cut (Figure 2C).
2.3. Vascular System on the Dura and Nerve Root
After removal of the ventral bone of the SAP by a lateral-posterior approach, the walking root, dural sac, and ventral disc were visible (Figure 2D). The epidural fat on the traversing roots was stripped away to expose the nerve root. It can be seen that there are mainly 2 vascular bundles on the dorsal side of the walking roots, which are distributed longitudinally paralleling to the nerve roots, and there are vascular network connections between them (Figure 1 and Figure 2H).
The key anatomic marker in the interlaminal approach is the ligamentum flavum, and the removal of part of the ligamentum flavum is a landmark step in the surgical process (Figure 2I). After breaking through the ligamentum flavum, epidural fat and dural membrane can be seen, and the surface of the dural membrane is covered by a loose layer of disintegrated tissue (Figure 2K), which is composed of epidural fat and vascular network. This membrane may be the last protective barrier of the dural membrane and should be retained unless necessary. The dorsal central fold of the dural membrane can also be found in the approach of interlaminar space (Figure 2K). The nerve root sleeve and its vessel distribution (Figure 2J) can also be clearly found. It can be seen that these blood vessels are mainly distributed longitudinally along the dural membrane and nerve roots, and there are slightly smaller communicated blood vessels distributed among them. These blood vessels are the main blood supply to the dural membrane, arachnoid membrane and the superficial part of the nerve roots, and the protection of these blood vessel networks is very important in procedures. The central bulging disc can be seen after significantly pushing of the dura and nerve root, besides that, the vascular network distributed on the dura, and the protruding nucleus pulposus can be seen in the interlaminar approach (Figure 1 and Figure 2L).
3. Discussions
Familiarity with the above anatomical structures is the basis for carrying out surgery. From this, it can be discovered which points are most prone to bleeding, such as the nutrient blood vessels of muscles at the dorsal articular processes, the accompanying blood vessels of the dorsal ramus, the venous plexus on the ventral side of the lumbar canal, the accompanying blood vessels of the exit nerve roots, the cephalad side of the vertebral pedicles, and the base of the articular processes. Hemorrhage caused by injury to the venous plexus on the ventral side of the dura sac or accompanying blood vessels of the exit nerve roots can be particularly profuse and difficult to stop, often requiring the use of gelatin sponge packing for compression hemostasis. After becoming familiar with these anatomical structures, it is possible to timely identify them during surgery and avoid damage to blood vessels and nerves.
During the procedure, the author noted some specific structures under the endoscope, such as the small ligaments (not the flavum ligament) running obliquely from the ventral and apex of the SAP to the exit root above, the ventral annulus fibrosus, and the transverse process at the caudal end. These ligaments on the SAP are important fixation structures for the contents of the intervertebral foramen. They can fix the exit nerve roots and accompanying blood vessels from different directions, combined with fatty tissues, thus reliably fixing the exit nerve roots and accompanying structures in the intervertebral foramen. The space between the ligaments contains a lot fatty tissue, which acts as a good cushion and protection for the nerve roots. There is also a flat vein (distributed longitudinally) perpendicular to the IVD, located on the outer side of the traversing roots, along the edge of the intervertebral foramen, and the position is relatively constant. Sometimes, it is necessary to coagulate it when dealing with the bulging IVD. In addition, accompanying blood vessels of the nerve roots and the dura mater, as well the protective fat tissues, they both have a protective, cushioning, and lubricating effect on the nerve roots and dura mater. These structures can be clearly displayed under the endoscope. Excessive damage to them can cause problems such as dural degeneration, scar proliferation, adhesion, etc., which may probably affect postoperative recovery. Many of these structures have a submillimeter size. The magnifying effect of the endoscope allows us to clearly distinguish and protect them.
It should be emphasized that the presence of ligaments in all intervertebral foramina is not always guaranteed, but if present, the probability of all ligaments being present in all intervertebral foramina is approximately 47% [5]. The most common is the superior corporotransverse ligaments (27%), and the inferior corporotransverse ligaments connect two independent bones. Many studies believe that the anatomical position of the ligaments occupies the space of the intervertebral foramen, which is the main cause of nerve root compression and radiating pain. These ligaments can reduce the cross-sectional area of the intervertebral foramen by 30% [6,7]. However, there are also different opinions. Kuofi mapped the spatial position of the ligaments [8] and believed that these ligaments are continuously present in the intervertebral foramen, and their presence not only does not cause nerve compression or radiating pain, but also has a protective effect on the blood vessels and nerves in the intervertebral foramen [5,9]. This study found that the probability of the presence of ligaments (inferior corporotransverse ligaments) was highest in the lower intervertebral foramen (89%), followed by the superior corporotransverse ligaments (84%) and the middle corporotransverse ligaments (71%). These ligaments should be preserved as much as possible and generally do not affect microscopic operations. It should be stressed that the anatomical structures discovered in this study have some anatomical differences in occurrence rates, positions, sizes, and branching situations. However, these anatomical differences have a relatively low incidence and do not affect the clinical reference value of this study.
4. Conclusion
This study successfully explored the occurrence of specific structures under lumbar endoscopy to guide precise intraoperative operations. Secondly, after the structure is confirmed, it is necessary to transition from structural research to functional research, and there is still a lot of work to be done. Thirdly, understanding these endoscopic structures and their functions will promote further development of minimally invasive spine technology.
References
- Kohoutova, D.; Banks, M.; Bures, J. Advances in the Aetiology & Endoscopic Detection and Management of Early Gastric Cancer. Cancers (Basel) 2021, 13, 6242–6250. [Google Scholar] [PubMed]
- Namba, K. Vascular Anatomy of the Cauda Equina and Its Implication on the Vascular Lesions in the Caudal Spinal Structure. Neurol Med Chir (Tokyo) 2016, 56, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Martirosyan, Nikolay; Feuerstein, Jeanne; Theodore; et al. Blood supply and vascular reactivity of the spinal cord under normal and pathological conditions A review. Journal of neurosurgery. Spine 2011, 4, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.S.; Robertson, J.T.; Frederickson, R.C.; et al. Association between peridural scar and recurrent radicular pain after lumbar discectomy: magnetic resonance evaluation. ADCON-L European Study Group. Neurosurgery 1996, 38, 855–863. [Google Scholar]
- Umeh, Randle; et al. Transforaminal Ligaments of the Lumbar Spine: A Comprehensive Review. Cureus 2016, 8, e811–e819. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhong, E.; Shi, B.; et al. The morphology and clinical significance of the intraforaminal ligaments at the L5-S1 levels. Spine J. 2016, 16, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Marić, D.L.; Krstonošić, B.; Erić, M.; et al. An anatomical study of the lumbar external foraminal ligaments: appearance at MR imaging. Surg Radiol Anat. 2015, 37, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Amonoo-Kuofi, H.S.; el-Badawi, M.G.; Fatani, J.A. Ligaments associated with lumbar intervertebral foramina. 1. L1 to L4. J Anat. 1988, 5, 177–183. [Google Scholar]
- Yuan, S.G.; Wen, Y.L.; Zhang, P.; Li, Y.K. Ligament, nerve, and blood vessel anatomy of the lateral zone of the lumbar intervertebral foramina. Int Orthop. 2015, 5, 2135–2141. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Some typical endoscopic structures of foraminal approach (A-H) and interlaminar approach (I-L). (A) the ligaments ventral to the apex of the SAP; (B) Endoscopic image of the ventral flavum ligamentum of the SAP; (C) The ligaments connecting the annulus fibrosus, dural membrane and nerve roots on the surface of the lumbar disc below the ventral ligaments of the SAP, and the soft tissues; (D) After the removal of the ventral part of the SAP, the flavum ligament and traversing root on the ventral can be seen, and the three constitute the “sandwich structure”; (E) Endoscopic view of the distribution of blood vessels on the surface of the disc on the ventral side of ligamentum flavum of the SAP; (F) The vascular distribution on the surface of the IVD below the ventral SAP and traversing root; (G) Disc herniation below the microscope, the annulus fibrosus is broken and the traversing root is compressed. (I) The “penetration of the ligament flavum” is the key procedure of the interlaminar space approach, and the epidural space can be seen after the flavum ligament is removed; (J) the location of the nerve root, and the distribution of its blood vessels; (K) epidural fat and the central folds on the dorsal dural membrane; (L) Protruding nucleus pulposus and the tensioned dura on the dorsolateral, and blood vessels surrounding the dural can be seen in the interlaminar approach.
Figure 2.
Some typical endoscopic structures of foraminal approach (A-H) and interlaminar approach (I-L). (A) the ligaments ventral to the apex of the SAP; (B) Endoscopic image of the ventral flavum ligamentum of the SAP; (C) The ligaments connecting the annulus fibrosus, dural membrane and nerve roots on the surface of the lumbar disc below the ventral ligaments of the SAP, and the soft tissues; (D) After the removal of the ventral part of the SAP, the flavum ligament and traversing root on the ventral can be seen, and the three constitute the “sandwich structure”; (E) Endoscopic view of the distribution of blood vessels on the surface of the disc on the ventral side of ligamentum flavum of the SAP; (F) The vascular distribution on the surface of the IVD below the ventral SAP and traversing root; (G) Disc herniation below the microscope, the annulus fibrosus is broken and the traversing root is compressed. (I) The “penetration of the ligament flavum” is the key procedure of the interlaminar space approach, and the epidural space can be seen after the flavum ligament is removed; (J) the location of the nerve root, and the distribution of its blood vessels; (K) epidural fat and the central folds on the dorsal dural membrane; (L) Protruding nucleus pulposus and the tensioned dura on the dorsolateral, and blood vessels surrounding the dural can be seen in the interlaminar approach.


Table 1.
The main structures and their functions observed under the foraminal endoscopic approach.
| Structural names | Origins | Insertions | Innervative nerve | Route | Functions | Probability of existence | Variation rate | |
| Muscles attached to SAP | Multifidus muscle (MM) | Transverse process | Spinus process, lamina | Posterior rami | fan-shaped from the down -outside to the up-inside | Dorsal extension, lateral flexion, rotating vertebral body | 100% | |
| intertransversarii mediales lumborum | Accessory process, lateral side of transverse | Accessory process of upper level, transverse process of upper level | The dorsal ramus of spinal nerve | From inferior to superior | Lateral bending, keeping spine in balance | 100% | ||
| intertransversarii lateral lumborum | Accessory process, lateral side of tranverse | Accessory process of upper level, transverse process of upper level | The dorsal ramus of spinal nerve | From inferior- lateral to superior-medial | Lateral bending, keeping spine in balance | 100% | ||
| Ligaments attached to SAP | capsule ligaments | SAP | Inferior articular process (IAP) | The medial branch of dorsal ramus of spinal nerve (same level and upper level) | Wrapped up | Keep facet joint in place | 20% | |
| Superior corporotransverse ligaments | Posterior lateral side of vertebral body | Transverse process of same level | The medial branch of dorsal ramus of spinal nerve (same level and upper level) | From inferior- lateral to superius- medial obliquely | Protects the blood vessels and nerves in the foramen | 78% | 30% | |
| inferior corporotransverse ligaments |
Posterior lateral side of vertebral body | Transverse process of inferior level | The medial branch of dorsal ramus of spinal nerve (same level and upper level) | From superius-lateral to inferior -medial obliquely | Protect the blood vessels and nerves in the foramen | 69% | ||
| superior-transforaminal ligament |
Posterior lateral side of vertebral body | Inferior pedicle notched | The medial branch of dorsal ramus of spinal nerve (same level and upper level) | From anterior to lateral posterior foramen | Protect the blood vessels and nerves in the foramen | 84% | ||
| mid-transforaminal ligament |
Posterior lateral corner of annular fibrosis (AF) | Flavum ligament of posterior facet processes and facet capsule | The medial branch of dorsal ramus of spinal nerve (same level and upper level) | From anterior to lateral posterior foramen | Protect the blood vessels and nerves in the foramen | 71% | ||
| inferior-transforaminal ligament |
Posterior inferior side of vertebral body | Pedicle notched area of vertebral body | The medial branch of dorsal ramus of spinal nerve (same level and upper level) | From anterior to lateral posterior foramen | Protect the blood vessels and nerves in the foramen | 89% | ||
| Arteries in foramen (seen in the Figure 1) | anterior spinal canal branch (ascb.) | lumbar artery (la.) | running inferiorly into the foramen | Accompanying nerves of vascular sheath | From superius to inferior | Supplies the soft tissues in front of the foramen | 98% | |
| Lumbar ascending branch (ab.) | LA gives a new branch, ab. after the ascb. and lateral branch. | Foramen to posterior MM. | Modulated by accommodated nerves from the dr. | Running superiorly | Supplies the tissues in the foramen and the same level MM. | 100% | ||
| Lumbar descending branch (desc.) | Continuted ending branch of LA | Ends at the MM. and facet joints | Branch of dr. | Running inferiorly | Supplies the tissues in the facets, IVD and the inferior level MM. | 85% | ||
| posterior spinal canal branch (pscb) |
Originating from (lumbar artery, LA) | Ends at the intervertebral foramen | Modulated by accommodated nerves in vessel sheath | From superius to inferior | Supplies the tissues in the posterior foramen | 99% | ||
| branches accompanying dorsal ramus of spinal nerve (dr.) | originating from mscb of LA | ending in base of transverse process and facet | Modulated by accommodated nerves in vessel sheath | running along the dr. irregularly | Supplies the dr, facet jonts received supplies from both medially and laterally | 99% | ||
| posterior branch related to the pars interarticularis of the lamina (ia.) | Continuing of LA | crossing the joining area of pedicle and transverse, running to the posterior spinous process and facet process | Modulated by accommodated nerves in vessel sheath | Supplies the spinous process, and paraspinal muscles | 100% | |||
| veins in the foramen ( seen in the Figure 1) |
medial venous plexus of lumbar canal | joining lumbar ascending vein | descending branch of the medial branch of dorsal ramus of spinal nerve | From inferior to superior | Draining the veins in lumbar canal and foramen | 97% | ||
| Lumbar ascending vein | iliolumbar vein | left conjoining with left renal vein; right joining with inferior vena cava | From inferior to superior | Drain Vertebral body (VB) through central vein, lumbar segmental vein, and veins in foramen | 100% | |||
| Central vein | Central vein sinus | medial -anterior veinous plex of lumbar canal | from anterior to posterior | Drain VB | 100% | |||
| veins on the surface of IVD (seen in the Figure 1) | intervertebral vein (IVV) | Joining lumbar ascending vein | Underneath the pedicle, accompaied with exit nerve root, from inferior lateral to superius medial | Drain the region of foramen, lumbar canal and nerve root | 100% | |||
| lateral transverse branch | Communicated with IVV | Join the IVV | Lies in the lumbar canal anteriorly and posteriorly | Drain the lumbar canal | 91% | |||
| vein plex in the anterior of dura sac | drain the veins in the foramen and the veins lying in the anterior lumbar canal | joining segmental lumbar vein | sinuvertebral nerve (svn.) | longitudinal distribution in both ventral sides of dura sac from inferior to superior | Drain VB, foramen and annulus of IVD | 100% | ||
| arteries on the surface of IVD (seen in the Figure 1) | anastomosis over the surface of the intervertebral IVD (ana.) | metaphysial anastomosis (man.) | svn. | distributed on the surfaces of AF. | supplies the lumbar IVD | 95% | ||
| metaphysial anastomosis | communicated with ana. and primary periosteal artery (ppa.) | distributed on endplate epiphysis | supplies the endplate epiphysis and cartilage | 92% | ||||
| anterior spinal canal branch (ascb.) | Originated from segmental artery, communicated with adjacent segmental artery | distributed along the nerve root and foramen | supplies the nerve root and connective tissues in the foramen | 89% | ||||
| vessels on the dura and nerve root | generally, there are two main longitudinal veins and their communicated venous plex, while the vessels on the ventral side is hard to observe | joining the lateral transverse vein and lumbar ascending vein through aivvp. | drain connective tissues surrounding dura | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



