
Submitted:
05 November 2025
Posted:
06 November 2025
You are already at the latest version
Abstract
Background: Physical exercise has emerged as a promising intervention for depressive disorder, yet its efficacy and optimal implementation remain under investigation. Ob-jective: To thoroughly assess the effectiveness of structured physical exercise as a con-ventional treatment for adults with depressive disorder.
Methods: Adhering to PRISMA 2020 guidelines, a comprehensive literature search was conducted across PubMed/MEDLINE and institutional multi-databases. Peer-reviewed randomized controlled trials (RCTs) published between 2010 and 2025, studying adults diagnosed with depressive disorder under supervised exercise interventions, were se-lected. Methodological rigor was ensured through two independent reviewers. The in-fluence of moderating variables (workload and the instrument used to evaluate depres-sive disorder: instrument) was analyzed using meta-regression, and the pooled effect size was estimated using both frequentist and Bayesian meta-analyses. Results: From 15,542 screened records, 20 RCTs met the inclusion criteria. Workload accounts for 60% of the variance in the effect size, and instrument accounts the 15%. Supervised physical exercise significantly reduced depressive symptoms (standardized mean difference = 0.80; 95% CI: 0.57–1.03; I² = 59%). Robust Bayesian meta-analysis confirmed the consistency of these findings. Conclusion: Physical exercise serves as a valuable complement to traditional therapies for adults diagnosed with depressive disorder, resulting in clinically significant reductions in depressive symptoms.
Keywords:
depression
; major depressive disorder
; psychological disease
; Bayesian meta-analyses
; health care
; alternative therapy
; exercise intensity
; structured physical exercise
; Hamilton Depression Rating Scale
; Beck Depression Inventory
1. Introduction
Depressive disorder represents a significant challenge to global public health, affecting millions of individuals worldwide and imposing considerable societal and personal burdens [1]. With an estimated prevalence of 332 million people globally, major depressive disorder (MDD) is a primary cause of disability, with projections indicating an even greater future burden. Data from 2021 in the United States indicate that approximately 21.0 million adults (8.3%) experienced at least one episode of MDD, with a higher prevalence among females (10.3%) than among males (6.3%) [3]. Symptoms encompass persistent low mood, anhedonia, fatigue, low self-esteem, and hopelessness [1]. Moreover, comorbidities such as substance abuse, suicidal ideation, and chronic pain are also prevalent [4]. These conditions diminish quality of life and impose substantial economic costs due to decreased productivity. Depression is not merely a mental health disorder but also a major risk factor for numerous adverse health outcomes, including higher mortality rates, chronic diseases, disability, and poor prognosis in related conditions [5]. Furthermore, a complex interplay between biological, psychological, and social factors elevates the risk of depression, including sleep disturbances, trauma, low social support, and socioeconomic disadvantages [6].
The pursuit of effective, accessible, and sustainable treatments for depressive disorder is thus an urgent priority. Especially, numerous patients with MDD do not achieve remission or discontinue treatment due to various factors, including illness severity, comorbidities, high patient expectations, and adverse medication side effects [7]. Consequently, over the last decade, there has been a heightened interest in adjunctive therapies for depressive disorder. In particular, physical exercise (PE) has considerable evidence supporting its effectiveness as an adjunctive treatment for depressive disorder, serving as an alternative to traditional therapies and first-line antidepressants, while enhancing overall health and reducing relapse rates [8,9,10]. PE offers several benefits, including affordability, ease of access, self-administration, and a favorable side effect profile, which confers additional health advantages for patients afflicted with depression.
The majority of the scientific literature indicates that both aerobic and resistance training modalities are effective in reducing depressive symptoms [11,12]. Furthermore, certain mind-body practices, such as Tai Chi and yoga, have been demonstrated to provide substantial benefits for this condition [13,14], notwithstanding WHO guidelines recommending 75–150 minutes of vigorous or 150–300 minutes of moderate physical activity weekly [15]. Moreover, supervised exercise programs, compared with unsupervised ones, enhance engagement and retention, particularly among individuals with MDD, thereby leading to improved outcomes [16,17]. While several meta-analyses have clearly demonstrated that exercise is a viable and well-tolerated adjunct therapy [18,19], uncertainty persists regarding the optimal exercise dose; specifically, the appropriate duration, intensity, and frequency to achieve significant and sustained reductions in depressive symptoms. Many studies investigating short- and medium-term effects lack follow-up data [10,20,21]. Furthermore, each patient faces distinct challenges, particularly those experiencing severe symptoms of depression.
According to the PubMed database, the number of meta-analyses (147) of randomized controlled trials (RCTs) assessing the effects of exercise on depressive disorder has steadily increased since 2010. Among these, 22 studies focused on individuals without additional comorbidities; however, none conducted meta-regressions or closely monitored physical activity. Therefore, the main goal of this systematic review with meta-analysis and meta-regression is to thoroughly evaluate the effectiveness of structured physical exercise as an additional treatment for adults diagnosed with depressive disorder. It also aims to improve clinical practice and promote the integration of exercise into standard care protocols.
2. Results
2.1. Search Results
In the initial phase of our search strategy, a total of 15,542 studies were identified, comprising 2,179 from PubMed and 13,363 from institutional databases. Following automated screening, 14,384 studies were excluded, of which 288 were identified as duplicates. Of the 870 potentially pertinent articles identified, 496 were not peer-reviewed, and 32 involved animal models. Among the remaining 342 articles, 229 were not randomized controlled trials (RCTs), and 6 were protocols. During the full-text review process, 107 articles were examined, of which 91 were excluded for various reasons (Figure 1). Ultimately, 20 full texts met the predefined eligibility criteria, including four from previous reviews.
2.2. Characteristics of Participants Included in Trials
Across the selected 20 studies, a total of 1,202 adults diagnosed with depression were included: 334 males and 868 females, with ages ranging from 18 to 70 years. In three studies [38,39,40], participants exhibited low to moderate depressive symptoms (n=175), whereas the remaining subjects had MDD (n=1,027). In two studies [38,40], the participants did not report taking antidepressants (n=133); the others (n=1,069) were using antidepressant medications, including SSRIs, lithium, tricyclics, among others. The exercise interventions included aerobic training, multimodal exercise, resistance training, Yoga, and Tai Chi (Table 1). The activities in the control group included light stretching and rest during the waiting period. The duration of treatment varied from 10 days to 16 weeks. Exercise intensity levels ranged from low to vigorous, with the total number of sessions ranging from 12 to 60.
2.3. Risk of Bias
Overall, 14 studies were assessed as having good methodological rigor and a low risk of bias; 4 studies exhibited some concerns; and two studies were identified as having a high risk of bias. Three studies did not provide information regarding the intended interventions (Figure 2). The overall risk of bias was classified as follows: 70% low risk, 20% with some concerns, and 10% with high risk (Figure 2). The funnel plot, the Begg and Mazumdar test, and Egger’s regression test indicated the absence of publication bias (Figure 3).
2.4. Meta-Regression
From the 20 included studies, 52 groups (treatment and control cohorts) were analyzed. The meta-regression analysis demonstrates that the instrument employed to assess depression severity and workload accounts for 74% of the variance in the pooled effect size (Table 2).
Additionally, among the moderators (Table 3 and Figure 4), the influence of workload (F = 9.8; p = 0.005; adjusted R2 = 0.60) was larger than that of instrument type (F = 3.5; p = 0.025; adjusted R2 = 0.148). The unstandardized coefficients for BDI-II, HAM-D, and MADRS-S were positive (0.189, 1.063, 693, respectively), while DASS-21 and HADS were negative (-0.1, -0.108, respectively).
2.5. Meta-Analysis
The analysis, excluding moderating factors, indicated that the SMD ranged from -0.0389 to 2.9888, with the majority of estimates (96%) being positive (Figure 5). The estimated average SMD, as derived from the random-effects model, was 0.82 (95% CI: 0.54 to 1.11). This suggests that the average outcome significantly differed from zero (t(19) = 5.62, p < 0.0001). The Q-test results indicate heterogeneity among the true effect sizes (Q(19) = 103.61, p < 0.0001, tau² = 0.40, I² = 76%). The 95% prediction interval for the true effects ranges from -0.49 to 2.15. Given the considerable heterogeneity across studies and the influence of confounding variables—specifically, instrument and workload—these two factors were incorporated as moderators in both the classical meta-analysis and the Robust Bayesian Meta-analysis. The classical meta-analysis yielded consistent findings (SMD = 0.80, 95% CI: 0.57 to 1.03; I² = 59%) and a 95% prediction interval (PI) ranging from -0.15 to 1.74, while the Robust Bayesian Meta-analysis provided a conservative estimate of the pooled effect size (SMD = 0.61, 95% CI: -0.06 to 0.95; PI: from -0.50 to 1.53; I² = 51%) (Figure 6). Thus, although the average outcome is estimated to be positive, some studies may yield negative results. Analyzing the studentized residuals and Cook's distances, one study [41] had a value exceeding ±3.10 and could be considered a potential outlier exerting substantial influence. Then, in the sensitivity analysis, excluding this study reduced the SMD to 0.71 (95% CI: 0.49 to 0.93; PI: -0.12 to 1.53; I² = 52%). Neither the rank correlation nor the regression test indicated any asymmetry (p = 0.31 and p = 0.57, respectively (Figure 3).
3. Discussion
The present systematic review and meta-analysis offer a rigorous and comprehensive evaluation of the antidepressant effects of physical exercise in individuals diagnosed with depressive disorder. The pooled analysis indicates a clinically and statistically significant reduction in depressive symptoms among participants who engage in structured physical exercise interventions (SMD = 0.82, CI: 0.54-1.25). According to Cohen’s conventions [42], this effect size is considered high, underscoring the clinical significance of exercise as a therapeutic modality for depressive disorder. Nevertheless, the analysis also identified considerable heterogeneity among the studies included (I² = 76%), reflecting substantial variability in intervention characteristics, participant populations, and study methodologies. However, when confounding variables are included in the model (depression level, workload, and the instrument used to evaluate depression), the effect size remains high (SMD = 0.80) and heterogeneity decreases considerably (I² = 59%). Additionally, using robust Bayesian meta-analysis, the pooled effect size, although moderate (SMD = 0.61), was clinically significant, as only 4% of studies favored the control group, highlighting the positive impact of exercise as an adjunct therapy to conventional treatments in reducing depression symptoms.
The comprehensive search strategy, strict adherence to PRISMA guidelines, and rigorous risk-of-bias assessment using the Cochrane Collaboration tool validate the strength and relevance of our findings. Additionally, the high pooled effect size observed is particularly meaningful given the heterogeneity of trials, exercise modalities, their intensities, and participant characteristics. This supports the role of exercise as an effective, accessible, and cost-efficient intervention for treating depression [43].
A comprehensive comparison with earlier systematic reviews and meta-analyses strengthens the consistency of the antidepressant effect of physical exercise. For example, Schuch et al. (2016) reported a high effect size (SMD = 0.99, 95% CI: 0.69–1.29) across 33 randomized clinical trials involving 1877 participants in resistance exercise protocols [44]. Cooney & Mead (2013) observed a moderate effect size (SMD = -0.62, 95% CI: -0.81 to -0.42, I2 = 63%) in their Cochrane review across 35 RCTs involving 1353 participants, but a lower effect size (SMD = 0.45, 95% CI: 0.06–0.83, I2 = 33%) in 4 methodologically robust trials [43]. Gordon et al. reported a moderate effect size (SMD = 0.66, 95% CI: 0.48 to 0.83, I2 = 76%) in 33 RCTs involving 1877 participants [45]. Kvam et al. (2016) reported a moderate effect (SMD = -0.68, 95% CI: -0.92 to -0.44, I2 = 68%) in 23 RCTs involving 977 participants [46]. Nevertheless, a meta-review reported a nonsignificant pooled effect size (SMD = 0.11, 95% CI: -0.41–0.18) in 4 high-quality trials [47], suggesting limited clinical efficacy. A recent network meta-analysis involving 14170 participants across 218 studies observed moderate to low reductions in depression. Among these, walking/jogging demonstrated the highest effect size (SMD = 0.63, 95% CI: 46-80), followed by yoga (SMD = -0.55, 95% CI: 36-73), strength training (SMD = 0.49, 95% CI: 29-69), and cycling, which exhibited the lowest effect (SMD = 0.30, 95% CI: 0.01-60), with the observed effects proportionate to the specific exercise modalities intensity [48].
Contrary to the literature, the pooled effect size in this work is relatively high, which may reflect careful control over inclusion criteria and the studied populations (without added comorbidities). In addition, the notable heterogeneity identified is not exclusive to this review; earlier meta-analyses have similarly documented substantial between-study variability, frequently ascribed to differences in exercise modality, intensity, duration, supervision, and participant characteristics [43,44,49].
This work did not identify similar studies that used rigorous Bayesian methods. Nevertheless, if the research objective were not solely to determine fixed parameters (means, standard deviations, p-values, etc.), we advocate using Bayesian analyses, owing to their greater robustness, flexibility, and extensive applicability in the health sector.
The novelty of this study lies in integrating statistically significant moderator variables into the model, alongside a comparative analysis of classical and Bayesian meta-analyses of the pooled effect sizes, methodologies that have traditionally received limited scrutiny. This amalgamation of statistical techniques enabled the isolation of moderator effects on the overall effect size and facilitated the calculation of its true value, thereby enhancing the reliability and clinical applicability of the findings. Additionally, it was observed that larger workloads are associated with larger effect sizes.
The overall effect size of the two moderators is also considered high (Adjusted R² = 0.744) [50], with workload serving as the primary moderator (Adjusted R² = 0.612), in contrast to the instrument (Adjusted R² = 0.132); effect sizes not documented in previous studies. This represents a pioneering discovery that warrants consideration in future research exploring the impact of exercise on depression. Although earlier research has established the efficacy of exercise, few studies have systematically investigated the sources of heterogeneity arising from variations in physical activity and participants' depression levels [43,44]. By addressing these gaps, this review offers a more detailed understanding of how, for whom, and under what conditions exercise is most effective.
Additionally, the ongoing global burden of MDD, the limitations of pharmacological and psychotherapeutic options, and the urgent need for affordable and sustainable intervention solutions underscore the importance of this study. In this sense, exercise, as demonstrated here, provides a compelling complement or alternative to conventional therapies, with a favorable side effect profile and additional health benefits, including reduced cardiovascular risk and improved metabolic function [51]. The evidence further supports the notion that engaging in physical exercise may help prevent depressive symptoms, irrespective of age or other health conditions [52,53].
From a clinical perspective, the incorporation of exercise into treatment protocols for depressive disorder is substantiated by the extent and consistency of numerous positive outcomes, as well as by international directives issued by the World Health Organization [1,54] and the National Institute for Health and Care Excellence [55]. Both organizations endorse physical activity as either a primary or supplementary intervention for depression. Given the accessibility and scalability of exercise interventions, they are particularly valuable in settings with limited resources, among populations with restricted access to mental health services, and for patients with different levels of depression. Moreover, unlike antidepressant medications, which may be associated with a range of adverse effects and adherence difficulties, exercise is typically well tolerated, thereby promoting overall health and improving quality of life. Nevertheless, the significant heterogeneity identified in the current analysis underscores the need for further investigation, particularly regarding the adoption of a standardized methodology for assessing depression, participants' depression levels, and, most importantly, the regulation of exercise type and workload (number of sessions and intensities).
A complex interplay of neurobiological and psychological mechanisms supports the antidepressant effects of exercise. From a neurobiological perspective, exercise enhances neurocognitive function [21], can increase brain volume [56], fosters neuroplasticity and hippocampal neurogenesis, and modulates monoaminergic neurotransmission (serotonin, dopamine, norepinephrine); all of these processes contribute to mitigating the pathology of depression [51,57,58]. Exercise also has anti-inflammatory effects, lowering levels of pro-inflammatory cytokines such as IL-6 and TNF-α, which are elevated in depression [8,58], helping to normalize hypothalamic-pituitary-adrenal axis activity and reducing hyperactivity and stress [8,12]. The social benefits are increased communication, social support, and reduced loneliness [59,60], especially when exercise occurs in natural environments (green exercise) [61]. Psychologically, physical exercise boosts energy, motivation, self-concept, self-efficacy, resilience, and social connections, and provides a sense of mastery and achievement, all of which contribute to improvements in mental health and mood, as well as a reduction in depressive symptoms [20,62,63].
A key strength of the present review is its focus on moderating factors that impact the effectiveness of exercise interventions for depression. In addition to this work, the existing literature provides substantial evidence that the following factors are crucial in influencing treatment outcomes.
- Type of Exercise: Aerobic exercise (e.g., walking, jogging, cycling) and resistance training are the most extensively studied modalities, with both demonstrating large effect sizes [48,64]. In contrast, yoga and mind-body exercises show moderate effects, especially in older adults and individuals with comorbidities [48,49].
- Intensity: The antidepressant effects of exercise are proportional to the intensity prescribed, with moderate to vigorous exercise yielding the most significant benefits [48,49,64]. However, even light physical activity confers clinically meaningful effects, especially in previously inactive individuals [48].
- Duration and Frequency: Interventions lasting 6–12 weeks, with sessions of 30–60 minutes and performed 3–4 times per week, are associated with optimal outcomes [18,64,64]. Short interventions may also produce large effects, possibly attributable to greater participant adherence to the programs and the novelty of the activities; however, sustained engagement is necessary for long-term benefits [48,49].
- Participant Characteristics: Age, sex, baseline depression severity, and comorbidities may also influence the response to exercise; however, the evidence remains inconclusive. Certain studies indicate that women might derive greater benefits from strength training, whereas older adults tend to respond favorably to yoga and walking [44,49,53].
Despite its strengths, this review possesses certain limitations. Primarily, due to the limited number of selected manuscripts, it includes only two moderators from the extensive range mentioned earlier (such as sex, age, type of exercise, and exercise supervision). Secondly, moderate to high heterogeneity (I² approximately 51-76%) limits the accuracy of the pooled effect estimate, suggesting that the antidepressant effects of exercise may differ significantly across populations and intervention protocols. Thirdly, the presence of potential outliers, as in the study by Wang & Li (2022), may further introduce bias into the outcomes [41]. Fourthly, reliance on published studies raises the possibility of publication bias, though robust statistical techniques and sensitivity analyses can mitigate this concern to some extent. Therefore, the usefulness of incorporating moderating variables into the models, performing sensitivity analysis, and using robust statistical analyses, such as Bayesian meta-analysis.
Another limitation is the variability in outcome measures and diagnostic criteria used to evaluate depression across studies, which may impact the comparability of results. The lack of long-term follow-up data in many included studies also prevents definitive conclusions about the sustainability of exercise-related improvements in depressive symptoms. The review’s emphasis on RCTs and controlled studies may reduce its relevance to real-world settings, where adherence to exercise interventions is often lower and comorbidities are more common. Future research should include pragmatic trials and implementation studies to better assess the effectiveness of exercise in routine clinical practice.
4. Materials and Methods
4.1. Registration
This study followed the procedures of the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 2020 statement [22]. Previously, the protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) database (registration number: CRD420251121919). The methodological criteria outlined in this work are provided in Table 4.
4.2. Search Strategy
A comprehensive, systematic, and computerized search was conducted across PubMed/MEDLINE and the institutional multi-database platforms of the National Autonomous University of Mexico and the Autonomous University of Ciudad Juárez, which included EBSCOhost, Ovid, Web of Science, and Scopus, utilizing the PICOS (population, intervention, comparison, outcome, and study design) search methodology. Literature published from January 1, 2010, to August 31, 2025, was incorporated, employing the keywords ((exercis* OR aerobic* OR running OR jogging OR walk* OR hiking OR swim* OR aquatic* OR cycling OR bicycl* OR strength*) AND (depressi*) AND ((randomized clinical trial) OR (randomized controlled trial)), adapted for each database. The following filters were applied in the databases: articles in English, Spanish, or Portuguese; availability of an abstract; publication date subsequent to 2010; and inclusion of human participants aged 18 years or older.
4.3. Eligibility Criteria
Only original, peer-reviewed randomized controlled trials (RCTs) and recent reviews that aimed to objectively study depression through any kind of physical exercise-based interventions in patients with depression were included. Exercise was defined as a planned, structured, and repetitive intervention aimed at improving or maintaining physical conditioning. Eligible reports involved (a) adult individuals (age ≥ 18) with diagnostic criteria for depression or MDD established by validated instruments, such as The Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV, DSM-IV-TR, DSM-5 [23,24], International Classification of Diseases (ICD)-10, or ICD-11 [25] and confirmed through a validated structured diagnostic interview such as the Beck Depression Inventory (BDI) [26], Hamilton Depression Rating Scale (HAM-D) [27], Patient Health Questionnaire (PHQ-9) [28], Center for Epidemiologic Studies Depression Scale (CES-D) [29], Montgomery-Åsberg Depression Rating Scale (MADRS) [27], Zung Self-Rating Depression Scale (Zung SDS) [30], The Geriatric Depression Scale (GDS) [31], Depression Anxiety Stress Scales (DASS)[32], or Hospital Anxiety and Depression Scale (HADS) [33]. (b) Peer-reviewed studies published or accepted; (c) Comparisons focused on a passive physical activity, non-exercise, or wait-list control group, with a focus on individuals with depression; (d) supervised exercise. Manuscripts with non-randomized trials, meeting abstracts, meta-analyses, reviews, case reports, as well as studies involving individuals with comorbidities such as chronic degenerative diseases associated (e.g., hypertension, cancer, diabetes, sarcopenia), severe psychiatric disorders, and those in which medication was altered during the study were excluded.
4.4. Study Selection
A compilation of potentially pertinent studies was assembled for subsequent review and screening. Two independent reviewers evaluated each article's eligibility by examining its title and abstract. The references from the reviewed articles were imported into Zotero for reference management, where duplicates were systematically eliminated. Subsequently, the two authors examined the full texts and reached a consensus regarding the inclusion of articles in the final list. A third reviewer was engaged to resolve any uncertainties concerning the inclusion or exclusion of studies. The methodology for assessing eligibility conforms to the criteria delineated in the Cochrane Handbook for Systematic Reviews of Interventions, version 6.5 [34], and adheres to the PRISMA guidelines [22] for article reporting (Figure 1). Corresponding authors were contacted when study abstracts met the inclusion criteria, but the full texts were inaccessible, or when trials lacked essential information for meta-analytical procedures.
4.5. Data Extraction
From each article included in the review, relevant data were extracted, such as sex, age, diagnostic criteria, inpatient/outpatient status, number of participants, year of publication, treatment type, duration, exercise frequency, intensity, workload, depression severity, and the instrument used to determine depression level (Table 1). For each trial, we also recorded the sample sizes, means, and standard deviations (SDs) reported for each outcome. When SDs were unavailable, we estimated them using measures of precision such as standard errors, 95% confidence intervals, or p-values.
4.6. Risk of Bias Assessment
The risk of bias assessment in the included trials was conducted independently by two reviewers, following the Cochrane Collaboration's methods [34]. A third reviewer was involved to resolve discrepancies between the initial assessments. The following criteria were evaluated: (1) bias stemming from the randomization process; (2) bias due to deviations from the intended interventions; (3) bias resulting from missing outcome data; (4) bias in the measurement of outcomes; and (5) bias in the selection of the reported results. The classification was based on the categories: “low risk,” “some concerns,” “high risk,” or “no information." To generate risk-of-bias visualizations, the Revised Cochrane Risk of Bias RoB 2 tool for randomized trials was used to assess methodological quality and internal validity [34]). The visual figures were produced using the web platform robvis (https://mcguinlu.shinyapps.io/robvis/) [35].
4.7. Statistical Analysis
The analysis was conducted employing the standardized mean difference (SMD) as the primary outcome measure. Initially, to assess the influence of moderating factors on the pooled effect, a meta-regression was performed with effect size as the dependent variable. The instruments employed to evaluate depressive disorder and workload served as the independent variables. Workload was calculated by multiplying the exercise intensity (classified as low = 1, moderate = 2, and high = 3) by the number of sessions completed by participants. Given their role as predictors and the limited number of selected randomized controlled trials (RCTs), these two independent variables were incorporated into the meta-analytic model. The severity of depression was analyzed separately. A random-effects model was fitted to the data. Heterogeneity was quantified through the estimate of tau squared (τ²), obtained via the restricted maximum likelihood estimator. Additionally, the Q-test for heterogeneity and the I-squared (I²) statistic were reported. In instances where heterogeneity was detected (i.e., τ²> 0 regardless of the Q-test outcomes), a prediction interval for the true effect sizes was provided. Statistical tests and confidence intervals were computed using the Knapp-Hartung method. Studentized residuals and Cook's distances were employed to identify potential outliers and influential studies within the model. Studies with a studentized residual exceeding the 100 × (1 - 0.05/(2 × k)) percentile of the standard normal distribution were considered potential outliers, and a Bonferroni correction was applied with a two-sided alpha level of 0.05 for k studies included in the meta-analysis. Studies with a Cook's distance exceeding the median plus six times the interquartile range of Cook's distances were deemed influential. A sensitivity analysis was conducted by removing the study with the highest Cook's distance. Publication bias was assessed using the Begg and Mazumdar rank correlation test and Egger's regression test, with the standard error of the observed outcomes as the predictor, as visualized in the asymmetry funnel plot. The meta-analysis without moderators was performed utilizing RevMan version 5.4.1 [36]. The moderator effects were incorporated into the Classical Meta-Analysis and the Robust Bayesian Meta-Analysis, utilizing the JASP software [37]
5. Conclusions
In summary, this systematic review with meta-analysis and meta-regression provides strong evidence that physical exercise has a significant and clinically meaningful antidepressant effect and should be considered as a complement or alternative to traditional therapies for individuals with depressive disorder. Additionally, we found that workload is a very important regulator of exercise efficacy, with higher workload associated with a greater antidepressant effect (R2 = 0.60). Moreover, given the diverse standardized tools for assessing depression, this factor should be considered when interpreting results. Therefore, our results indicate the need to increase both the frequency and intensity of exercise sessions.
Since exercise is usually well-tolerated and accessible, it is a valuable option in settings with limited resources, among populations with restricted access to mental health services, and useful for patients with varying levels of depression. Besides, considering the global burden of depression and the limitations inherent in current treatments, integrating exercise into standard care protocols is a vital health strategy priority.
Author Contributions
Conceptualization, A.R-J. and R.P.H-T; methodology, A.R-J. and J.A.R-H.; formal analysis, I.A.C-G.; investigation, M.T-T.; resources, J.A.R-H. and M.T-T.; data curation, I.A.C-G.; writing—original draft preparation, A.R-J.; writing—review and editing, I.A.C-G.; supervision, R.P.H-T.; project administration, A.R-J.; funding acquisition, M.T-T. All authors have read and agreed to the published version of the manuscript.
Funding
The APC was funded by PRODEP UACH and UABC.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data Availability Statements are available from the corresponding author upon request.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
The authors have reviewed and edited the output and take full responsibility for the content of this publication.
References
- WHO Depressive Disorder (Depression). Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 20 October 2025).
- Rong, J.; Wang, X.; Cheng, P.; Li, D.; Zhao, D. Global, Regional and National Burden of Depressive Disorders and Attributable Risk Factors, from 1990 to 2021: Results from the 2021 Global Burden of Disease Study. Br. J. Psychiatry 2025, 227, 688–697. [Google Scholar] [CrossRef]
- National Institute of Mental Health (NIMH) Major Depression. Available online: https://www.nimh.nih.gov/health/statistics/major-depression (accessed on 20 October 2025).
- Malgaroli, M.; Calderon, A.; Bonanno, G.A. Networks of Major Depressive Disorder: A Systematic Review. Clin. Psychol. Rev. 2021, 85, 102000. [Google Scholar] [CrossRef]
- Arnaud, A.M.; Brister, T.S.; Duckworth, K.; Foxworth, P.; Fulwider, T.; Suthoff, E.D.; Werneburg, B.; Aleksanderek, I.; Reinhart, M.L. Impact of Major Depressive Disorder on Comorbidities: A Systematic Literature Review. J. Clin. Psychiatry 2022, 83, 43390. [Google Scholar] [CrossRef] [PubMed]
- Maier, A.; Riedel-Heller, S.G.; Pabst, A.; Luppa, M. Risk Factors and Protective Factors of Depression in Older People 65+. A Systematic Review. PLOS ONE 2021, 16, e0251326. [Google Scholar] [CrossRef]
- De Carlo, V.; Calati, R.; Serretti, A. Socio-Demographic and Clinical Predictors of Non-Response/Non-Remission in Treatment Resistant Depressed Patients: A Systematic Review. Psychiatry Res. 2016, 240, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, B.M.; Siqueira, C.C.; Vieira, R.M.; Moreno, R.A.; Soeiro-de-Souza, M.G. Physical Activity as an Adjuvant Therapy for Depression and Influence on Peripheral Inflammatory Markers: A Randomized Clinical Trial. Ment. Health Phys. Act. 2022, 22, 100442. [Google Scholar] [CrossRef]
- Gerber, M.; Beck, J.; Brand, S.; Cody, R.; Donath, L.; Eckert, A.; Faude, O.; Fischer, X.; Hatzinger, M.; Holsboer-Trachsler, E.; et al. The Impact of Lifestyle Physical Activity Counselling in IN-PATients with Major Depressive Disorders on Physical Activity, Cardiorespiratory Fitness, Depression, and Cardiovascular Health Risk Markers: Study Protocol for a Randomized Controlled Trial. Trials 2019, 20, N.PAG-N.PAG. [Google Scholar] [CrossRef]
- Legrand, F.D.; Neff, E.M. Efficacy of Exercise as an Adjunct Treatment for Clinically Depressed Inpatients during the Initial Stages of Antidepressant Pharmacotherapy: An Open Randomized Controlled Trial. J. Affect. Disord. 2016, 191, 139–144. [Google Scholar] [CrossRef]
- Ciccolo, J.T.; Louie, M.E.; SantaBarbara, N.J.; Webster, C.T.; Whitworth, J.W.; Nosrat, S.; Chrastek, M.; Dunsiger, S.I.; Carey, M.P.; Busch, A.M. Resistance Training for Black Men with Depressive Symptoms: A Pilot Randomized Controlled Trial to Assess Acceptability, Feasibility, and Preliminary Efficacy. BMC Psychiatry 2022, 22, 283. [Google Scholar] [CrossRef]
- Gerber, M.; Imboden, C.; Beck, J.; Brand, S.; Colledge, F.; Eckert, A.; Holsboer-Trachsler, E.; Pühse, U.; Hatzinger, M. Effects of Aerobic Exercise on Cortisol Stress Reactivity in Response to the Trier Social Stress Test in Inpatients with Major Depressive Disorders: A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1419. [Google Scholar] [CrossRef]
- Cramer, H.; Anheyer, D.; Lauche, R.; Dobos, G. A Systematic Review of Yoga for Major Depressive Disorder. J. Affect. Disord. 2017, 213, 70–77. [Google Scholar] [CrossRef]
- Wu, J.; Song, J.; He, Y.; Li, Z.; Deng, H.; Huang, Z.; Xie, X.; Wong, N.M.L.; Tao, J.; Lee, T.M.C.; et al. Effect of Tai Chi on Young Adults with Subthreshold Depression via a Stress–Reward Complex: A Randomized Controlled Trial. Sports Med. - Open 2023, 9, 90. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Babyak, M.A.; Murali Doraiswamy, P.; Watkins, L.; Hoffman, B.M.; Barbour, K.A.; Herman, S.; Edward Craighead, W.; Brosse, A.L.; Waugh, R.; et al. Exercise and Pharmacotherapy in the Treatment of Major Depressive Disorder. Psychosom. Med. 2007, 69, 587–596. [Google Scholar] [CrossRef]
- Daniele de Araújo Silva, J.; Cândido Mendes Maranhão, D.; Machado Ferreira Tenório de Oliveira, L.; Luiz Torres Pirauá, A. Comparison between the Effects of Virtual Supervision and Minimal Supervision in a 12-Week Home-Based Physical Exercise Program on Mental Health and Quality of Life of Older Adults: Secondary Analysis from a Randomized Clinical Trial. Geriatr. Gerontol. Int. 2023, 23, 864–870. [Google Scholar] [CrossRef]
- Tian, S.; Liang, Z.; Qui, F.; Yu, Y.; Wang, C.; Zhang, M.; Wang, X. Optimal Exercise Modality and Dose to Improve Depressive Symptoms in Adults with Major Depressive Disorder: A Systematic Review and Bayesian Model-Based Network Meta-Analysis of RCTs. J. Psychiatr. Res. 2024, 176, 384–392. [Google Scholar] [CrossRef]
- Yang, W.; Chen, H.; Liu, W.; Qu, S.; Ge, Y.; Song, J. Efficacy of Vigorous Physical Activity as an Intervention for Mitigating Depressive Symptoms in Adolescents and Young Adults: A Comprehensive Systematic Review and Meta-Analysis. Front. Behav. Neurosci. 2025, 19. [Google Scholar] [CrossRef] [PubMed]
- Nasstasia, Y.; Baker, A.L.; Lewin, T.J.; Halpin, S.A.; Hides, L.; Kelly, B.J.; Callister, R. Differential Treatment Effects of an Integrated Motivational Interviewing and Exercise Intervention on Depressive Symptom Profiles and Associated Factors: A Randomised Controlled Cross-over Trial among Youth with Major Depression. J. Affect. Disord. 2019, 259, 413–423. [Google Scholar] [CrossRef]
- Olson, R.L.; Brush, C.J.; Ehmann, P.J.; Alderman, B.L. A Randomized Trial of Aerobic Exercise on Cognitive Control in Major Depression. Clin. Neurophysiol. 2017, 128, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Guha, M. Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th Edition). Ref. Rev. 2014, 28, 36–37. [Google Scholar] [CrossRef]
- Segal, D.L. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). In The Corsini Encyclopedia of Psychology; 2010; pp. 1–3. ISBN 978-0-470-47921-6.
- Hong, Y.; Zeng, M.L. International Classification of Diseases (ICD). Knowl. Organ. 2022, 49, 496–528. [Google Scholar] [CrossRef]
- Jackson-Koku, G. Beck Depression Inventory. Occup. Med. 2016, 66, 174–175. [Google Scholar] [CrossRef]
- Bech, P.; Allerup, P.; Larsen, E.R.; Csillag, C.; Licht, R.W. The Hamilton Depression Scale (HAM-D) and the Montgomery-Åsberg Depression Scale (MADRS). A Psychometric Re-Analysis of the European Genome-Based Therapeutic Drugs for Depression Study Using Rasch Analysis. Psychiatry Res. 2014, 217, 226–232. [Google Scholar] [CrossRef]
- Kocalevent, R.-D.; Hinz, A.; Brähler, E. Standardization of the Depression Screener Patient Health Questionnaire (PHQ-9) in the General Population. Gen. Hosp. Psychiatry 2013, 35, 551–555. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Seeley, J.R.; Roberts, R.E.; Allen, N.B. Center for Epidemiologic Studies Depression Scale (CES-D) as a Screening Instrument for Depression among Community-Residing Older Adults. Psychol. Aging 1997, 12, 277–287. [Google Scholar] [CrossRef]
- Jokelainen, J.; Timonen, M.; Keinänen-Kiukaanniemi, S.; Härkönen, P.; Jurvelin, H.; Suija, K. Validation of the Zung Self-Rating Depression Scale (SDS) in Older Adults. Scand. J. Prim. Health Care 2019, 37, 353–357. [Google Scholar] [CrossRef] [PubMed]
- reenberg, S.A. The Geriatric Depression Scale (GDS). 2012.
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Montazeri, A.; Vahdaninia, M.; Ebrahimi, M.; Jarvandi, S. The Hospital Anxiety and Depression Scale (HADS): Translation and Validation Study of the Iranian Version. Health Qual. Life Outcomes 2003, 1, 14. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.5 (Updated August 2024)[EB. OL]. Cochrane; 2024. 2025.
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- The Cochrane Collaboration RevMan: Systematic Review and Meta-Analysis Tool for Researchers Worldwide | Cochrane RevMan Available online:. Available online: https://revman.cochrane.org/info (accessed on 22 October 2025).
- JASP Team JASP (Version 0.95.3)[Computer Software] Available online:. Available online: https://jasp-stats.org/ (accessed on 21 October 2025).
- Chin, E.C.; Yu, A.P.; Leung, C.K.; Bernal, J.D.; Au, W.W.; Fong, D.Y.; Cheng, C.P.; Siu, P.M. Effects of Exercise Frequency and Intensity on Reducing Depressive Symptoms in Older Adults With Insomnia: A Pilot Randomized Controlled Trial. Front. Physiol. 2022, 13. [Google Scholar] [CrossRef]
- Danielsson, L.; Papoulias, I.; Petersson, E.-L.; Carlsson, J.; Waern, M. Exercise or Basic Body Awareness Therapy as Add-on Treatment for Major Depression: A Controlled Study. J. Affect. Disord. 2014, 168, 98–106. [Google Scholar] [CrossRef]
- Dickmeyer, A.; Smith, J.J.; Halpin, S.; McMullen, S.; Drew, R.; Morgan, P.; Valkenborghs, S.; Kay-Lambkin, F.; Young, M.D. Walk-and-Talk Therapy Versus Conventional Indoor Therapy for Men With Low Mood: A Randomised Pilot Study. Clin. Psychol. Psychother. 2025, 32, e70035. [Google Scholar] [CrossRef]
- Wang, J.; Li, Z. Effect of Physical Exercise on Medical Rehabilitation Treatment of Depression. Rev. Bras. Med. Esporte 2022, 28, 174–176. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; 2nd ed.; Routledge: New York, 2013. ISBN 978-0-203-77158-7.
- Cooney, GM, Dwan, K, Greig, CA, Lawlor, DA, Rimer, J, Waugh, FR, McMurdo, M.; Mead, G. Exercise for Depression. Cochrane Database Syst. Rev. 2013. [CrossRef]
- Schuch, F.B.; Dunn, A.L.; Kanitz, A.C.; Delevatti, R.S.; Fleck, M.P. Moderators of Response in Exercise Treatment for Depression: A Systematic Review. J. Affect. Disord. 2016, 195, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B.R.; McDowell, C.P.; Hallgren, M.; Meyer, J.D.; Lyons, M.; Herring, M.P. Association of Efficacy of Resistance Exercise Training With Depressive Symptoms: Meta-Analysis and Meta-Regression Analysis of Randomized Clinical Trials. JAMA Psychiatry 2018, 75, 566–576. [Google Scholar] [CrossRef]
- Kvam, S.; Kleppe, C.L.; Nordhus, I.H.; Hovland, A. Exercise as a Treatment for Depression: A Meta-Analysis. J. Affect. Disord. 2016, 202, 67–86. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Solmi, M.; Wootton, R.E.; Vancampfort, D.; Schuch, F.B.; Hoare, E.; Gilbody, S.; Torous, J.; Teasdale, S.B.; Jackson, S.E.; et al. A Meta-Review of “Lifestyle Psychiatry”: The Role of Exercise, Smoking, Diet and Sleep in the Prevention and Treatment of Mental Disorders. World Psychiatry 2020, 19, 360–380. [Google Scholar] [CrossRef]
- Noetel, M.; Sanders, T.; Gallardo-Gómez, D.; Taylor, P.; del Pozo Cruz, B.; van den Hoek, D.; Smith, J.J.; Mahoney, J.; Spathis, J.; Moresi, M.; et al. Effect of Exercise for Depression: Systematic Review and Network Meta-Analysis of Randomised Controlled Trials. BMJ 2024, 384. [Google Scholar] [CrossRef]
- Singh, B.; Olds, T.; Curtis, R.; Dumuid, D.; Virgara, R.; Watson, A.; Szeto, K.; O’Connor, E.; Ferguson, T.; Eglitis, E.; et al. Effectiveness of Physical Activity Interventions for Improving Depression, Anxiety and Distress: An Overview of Systematic Reviews. Br. J. Sports Med. 2023, 57, 1203. [Google Scholar] [CrossRef]
- Gupta, A.; Stead, T.S.; Ganti, L. Determining a Meaningful R-Squared Value in Clinical Medicine. Acad. Med. Surg. 2024. [CrossRef]
- Ramos-Jiménez, A.; Rubio-Valles, M.; Ramos-Hernández, J.A.; González-Rodríguez, E.; Moreno-Brito, V. Adaptations in Mitochondrial Function Induced by Exercise: A Therapeutic Route for Treatment-Resistant Depression. Int. J. Mol. Sci. 2025, 26. [Google Scholar] [CrossRef]
- Mammen, G.; Faulkner, G. Physical Activity and the Prevention of Depression: A Systematic Review of Prospective Studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; Ponce De Leon, A.; Dunn, A.L.; Deslandes, A.C.; et al. Physical Activity and Incident Depression: A Meta-Analysis of Prospective Cohort Studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef]
- WHO WHO Guidelines on Physical Activity and Sedentary Behaviour; 1st ed.; Geneva: World Health Organization: Geneva, 2020. ISBN 978-92-4-001512-8.
- NICE Recommendations | Depression in Adults: Treatment and Management | Guidance | NICE Available online:. Available online: https://www.nice.org.uk/guidance/NG222/chapter/recommendations (accessed on 26 October 2025).
- Moreira-Neto, A.; Neves, L.M.; Miliatto, A.; Juday, V.; Marquesini, R.; Lafer, B.; Cardoso, E.F.; Ugrinowitsch, C.; Nucci, M.P.; Silva-Batista, C. Clinical and Neuroimaging Correlates in a Pilot Randomized Trial of Aerobic Exercise for Major Depression. J. Affect. Disord. 2024, 347, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.S.; Aghajanian, G.K.; Sanacora, G.; Krystal, J.H. Synaptic Plasticity and Depression: New Insights from Stress and Rapid-Acting Antidepressants. Nat. Med. 2016, 22, 238–249. [Google Scholar] [CrossRef]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical Activity and Depression: Towards Understanding the Antidepressant Mechanisms of Physical Activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef]
- Hou, B.; Wu, Y.; Huang, Y. Physical Exercise and Mental Health among Older Adults: The Mediating Role of Social Competence. Front. Public Health 2024, 12. [Google Scholar] [CrossRef]
- Zhang, J.; Yang, J.; Chen, S.; Feng, C.; Wang, S. Leisure Time Exercise and Depressive Symptoms in Sedentary Workers: Exploring the Effects of Exercise Volume and Social Context. Front. Psychiatry 2025, 16. [Google Scholar] [CrossRef]
- Coventry, P.A. ; Brown, JenniferV. E.; Pervin, J.; Brabyn, S.; Pateman, R.; Breedvelt, J.; Gilbody, S.; Stancliffe, R.; McEachan, R.; White, PiranC.L. Nature-Based Outdoor Activities for Mental and Physical Health: Systematic Review and Meta-Analysis. SSM - Popul. Health 2021, 16, 100934. [Google Scholar] [CrossRef]
- Peng, B.; Chen, W.; Wang, H.; Yu, T. How Does Physical Exercise Influence Self-Efficacy in Adolescents? A Study Based on the Mediating Role of Psychological Resilience. BMC Psychol. 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Tu, Y.; Su, Y.; Jin, L.; Tian, Y.; Chang, X.; Yang, K.; Xu, H.; Zheng, J.; Wu, D. The Mediating Effect of Self-Efficacy and Physical Activity with the Moderating Effect of Social Support on the Relationship between Negative Body Image and Depression among Chinese College Students: A Cross-Sectional Study. BMC Public Health 2025, 25. [Google Scholar] [CrossRef] [PubMed]
- Correia, É.M.; Monteiro, D.; Bento, T.; Rodrigues, F.; Cid, L.; Vitorino, A.; Figueiredo, N.; Teixeira, D.S.; Couto, N. Analysis of the Effect of Different Physical Exercise Protocols on Depression in Adults: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sports Health 2024, 16, 285–294. [Google Scholar] [CrossRef]
- Heissel, A.; Heinen, D.; Brokmeier, L.L.; Skarabis, N.; Kangas, M.; Vancampfort, D.; Stubbs, B.; Firth, J.; Ward, P.B.; Rosenbaum, S.; et al. Exercise as Medicine for Depressive Symptoms? A Systematic Review and Meta-Analysis with Meta-Regression. Br. J. Sports Med. 2023, 57, 1049–1057, Author 1, A.B.; Author 2, C.D. Title of the article. Abbreviated Journal Name Year, Volume, page range. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the study selection.
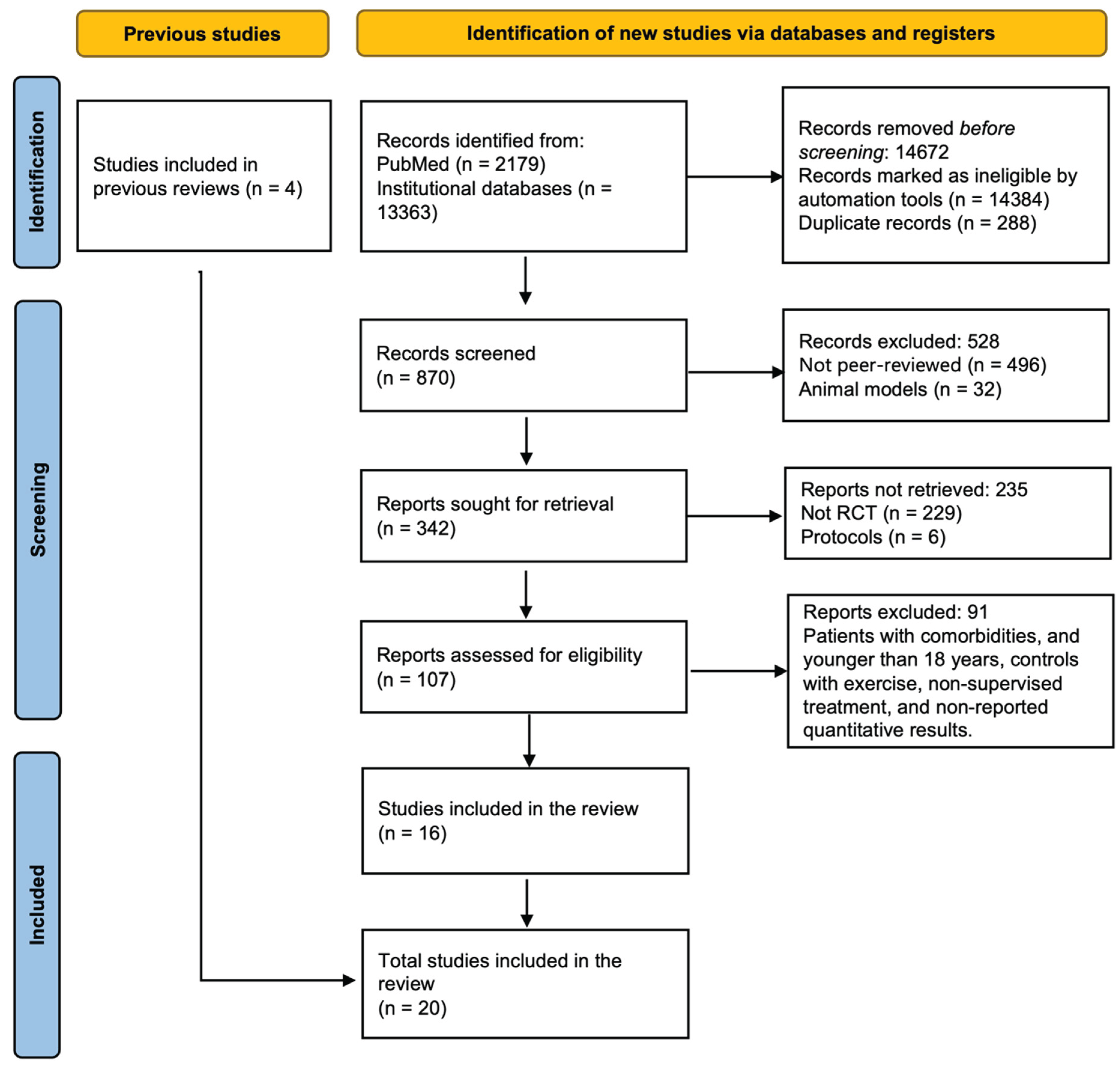
Figure 2.
Risk of bias of the selected manuscripts.
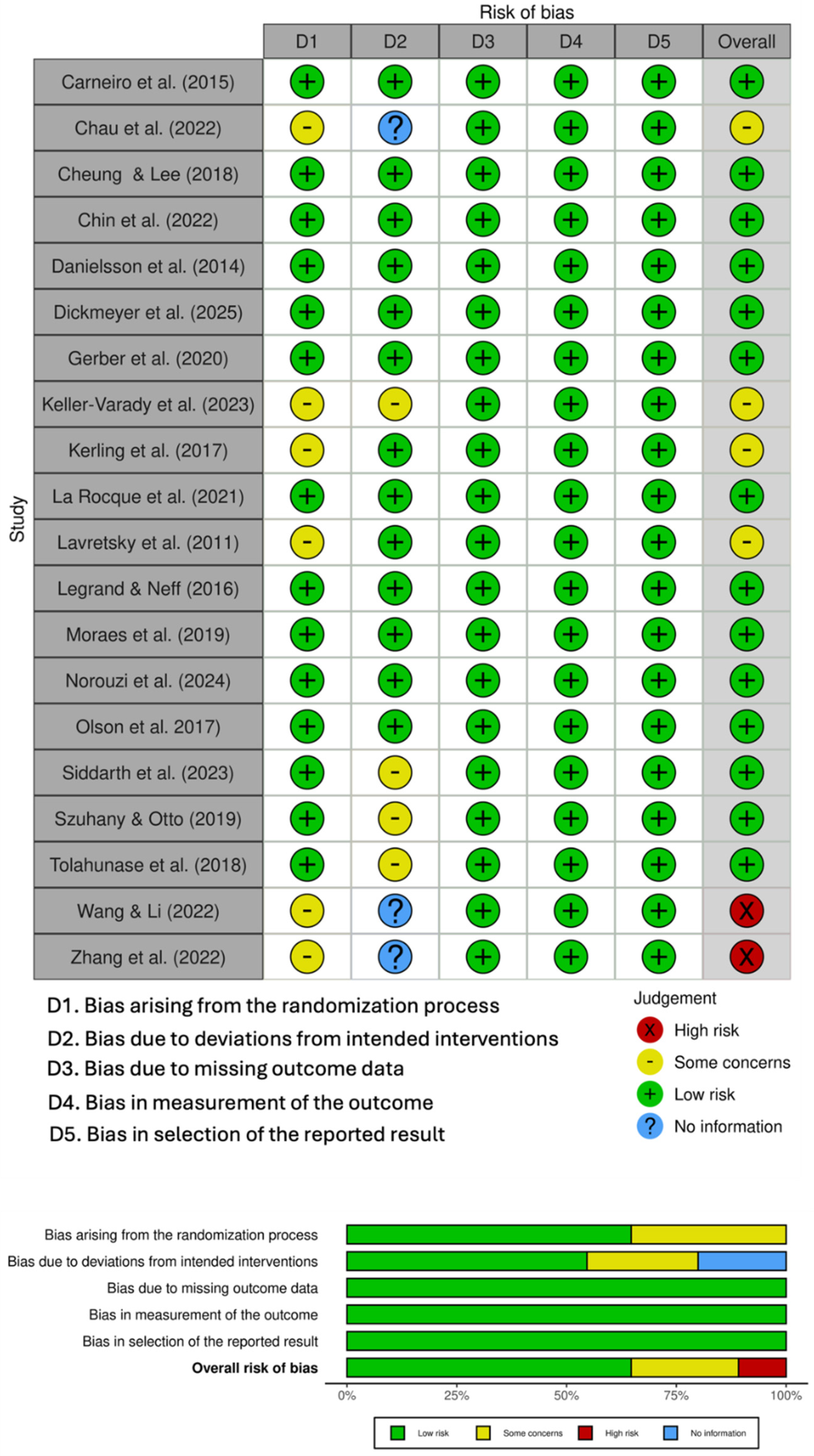
Figure 3.
Funnel plot and tests of publication bias.
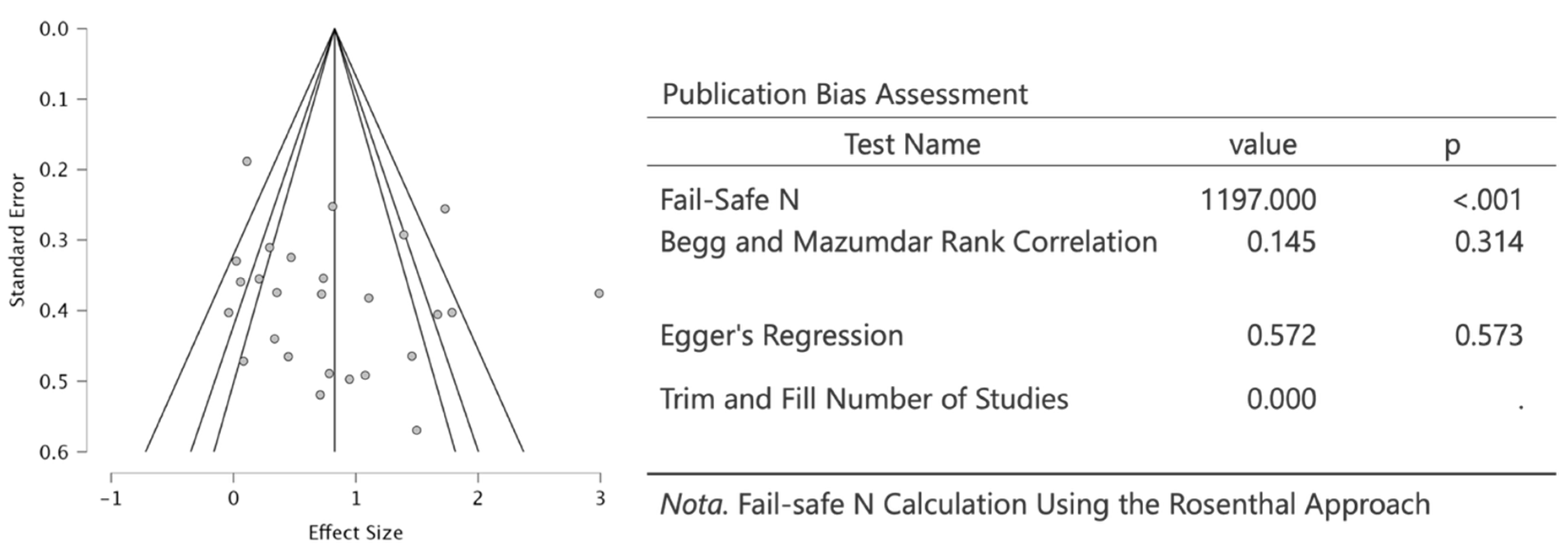
Figure 4.
Marginal Effects Plots on computed effect size.
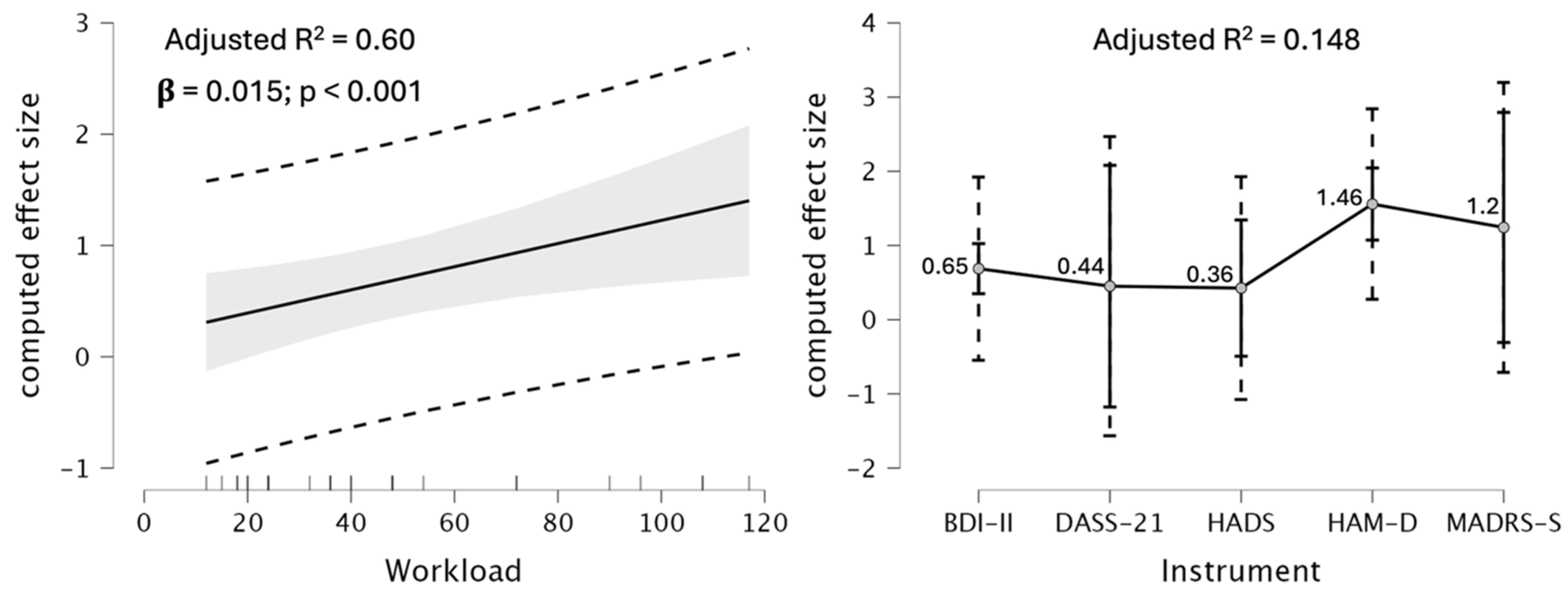
Figure 5.
Forest plot of the effect of physical exercise on depression symptoms in individuals with depressive disorder: Classical meta-analysis, without moderators.
Figure 5.
Forest plot of the effect of physical exercise on depression symptoms in individuals with depressive disorder: Classical meta-analysis, without moderators.
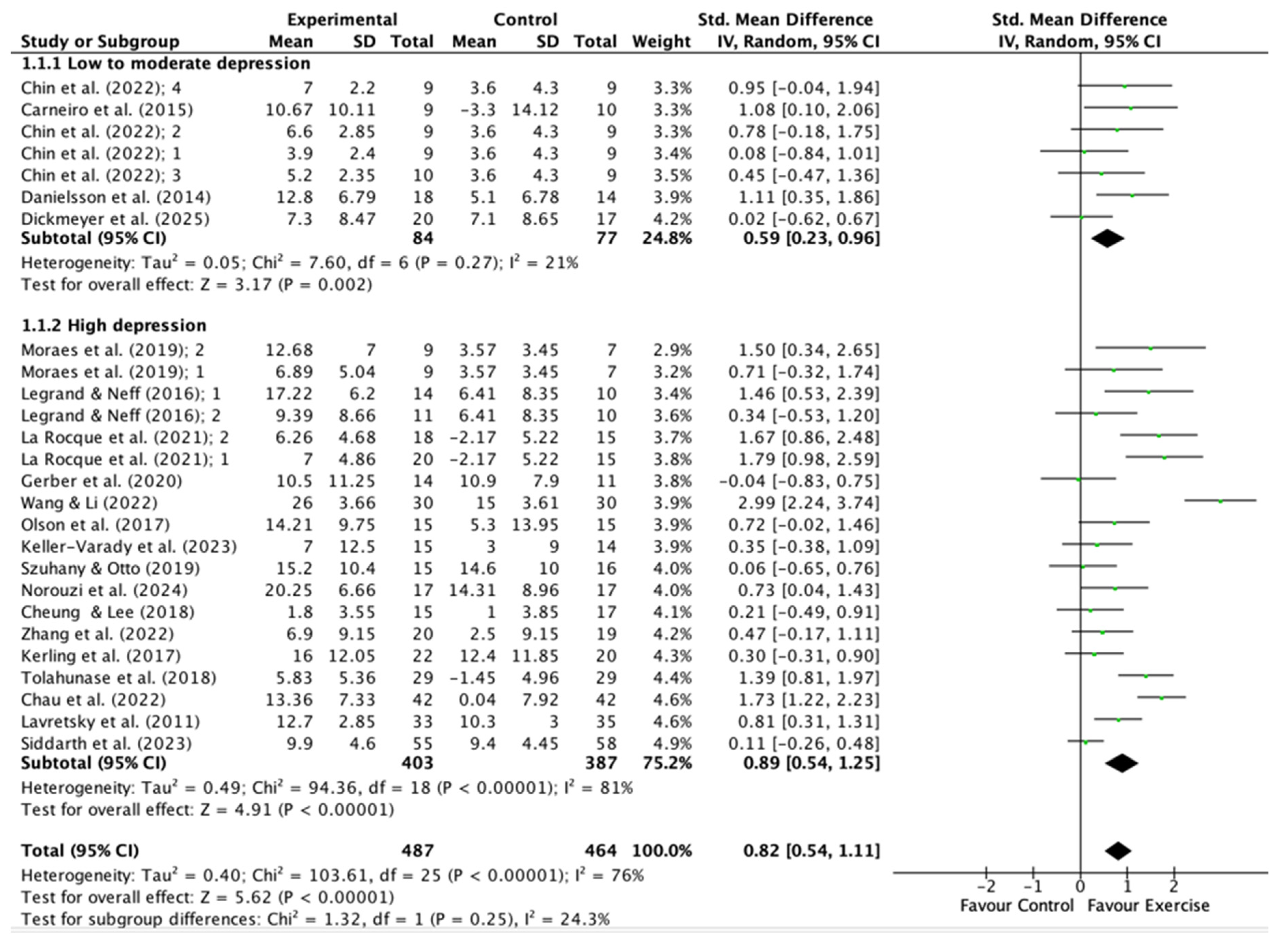
Figure 6.
Forest plot of the effect of physical exercise on depression symptoms in individuals with depressive disorder: Robust Bayesian Meta-Analysis with workload and type of instrument as moderators.
Figure 6.
Forest plot of the effect of physical exercise on depression symptoms in individuals with depressive disorder: Robust Bayesian Meta-Analysis with workload and type of instrument as moderators.
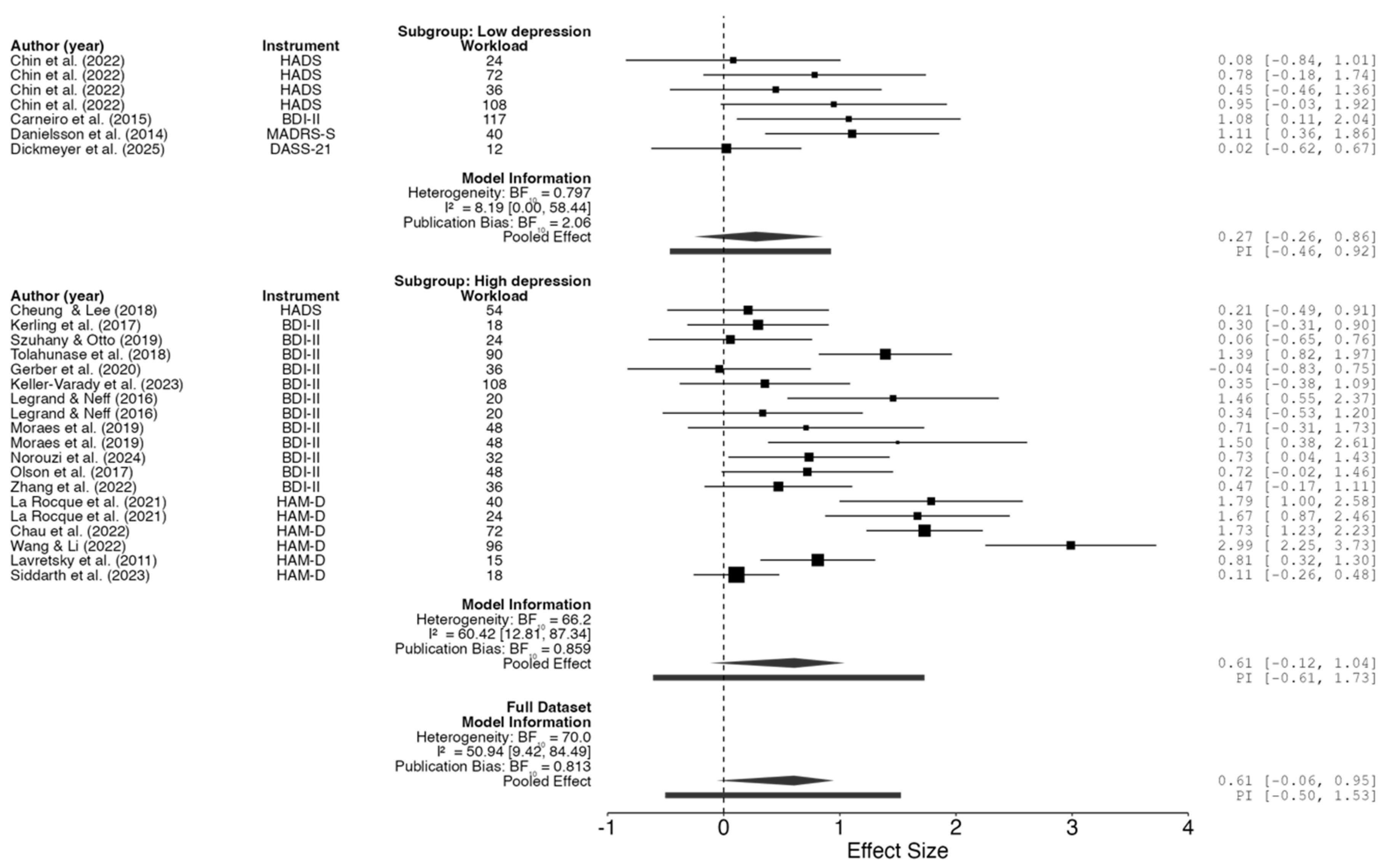

Table 1.
General characteristics of the 20 chosen manuscripts.
| Author (Year) | Sample size (treatment/control) | Age, y | Gender M/F | Instrument | Grade of depression | Drugs | Intervention (treatment/control) | Time of treatment | Number of sessions | Exercise Intensity |
| Carneiro et al. (2015) | 9/10 | 18-65 | 0/19 | BDI-II | Low to moderate | Yes | Aerobic exercise/rest | 16 weeks | 39 | 65-80% MHR |
| Chau et al. (2022) | 42/42 | 18-64 | 17/67 | HAM-D | High | Yes | Multimodal exercise/rest | 12 weeks | 36 | 50-70% MHR |
| Cheung & Lee (2018) | 15/17 | 18-65 | 7/34 | HADS | High | Yes | Aerobic exercise/rest | 12 weeks | 36 | 60% MHR |
| Chin et al. (2022) | 9/9 | ≥ 60 | 3/18 | HADS | Low to moderate | NM | Aerobic exercise/light stretching | 12 weeks | 12 | ∼3.25 METs |
| Chin et al. (2022) | 9/9 | ≥ 60 | 3/18 | HADS | Low to moderate | NM | Aerobic exercise/light stretching | 12 weeks | 36 | ∼3.25 METs |
| Chin et al. (2022) | 10/9 | ≥ 60 | 4/19 | HADS | Low to moderate | NM | Aerobic exercise/light stretching | 12 weeks | 12 | ∼6.5 METs |
| Chin et al. (2022) | 9/9 | ≥ 60 | 3/18 | HADS | Low to moderate | NM | Aerobic exercise/light stretching | 12 weeks | 36 | ∼6.5 METs |
| Danielsson et al. (2014) | 18/14 | 18-65 | 10/32 | MADRS-S | Low to moderate | Yes | Aerobic exercise/rest | 10 weeks | 20 | Moderate |
| Dickmeyer et al. (2025) | 20/17 | 18-70 | 37/0 | DASS-21 | Low to moderate | NM | Aerobic exercise/rest | 6-weeks | 6 | 3.5 METs |
| Gerber et al. (2020) | 14/11 | 18-61 | 0/25 | BDI-II | High | Yes | Aerobic exercise/rest | 6 weeks | 18 | 60-75% MHR |
| Keller-Varady et al. (2023) | 15/14 | 18-60 | 4/27 | BDI-II | High | Yes | Multimodal exercise/rest | 6 weeks | 36 | Moderate-to-vigorous |
| Kerling et al. (2017) | 22/20 | 18-60 | 26/16 | BDI-II | High | Yes | Aerobic exercise/rest | 6 weeks | 18 | 50% MHR |
| La Rocque et al. (2021) | 20/15 | 18-65 | 0/35 | HAM-D | High | Yes | Multimodal exercise/rest | 8 weeks | 16 | Moderate |
| La Rocque et al. (2021) | 18/15 | 18-65 | 0/33 | HAM-D | High | Yes | Yoga/rest | 8 weeks | 16 | Low to moderate |
| Lavretsky et al. (2011) | 33/35 | ≥ 60 | 26/42 | HAM-D | High | Yes | Tai Chi/rest | 10 weeks | 10 | Low to moderate |
| Legrand & Neff (2016) | 14/10 | 27-67 | 8/16 | BDI-II | High | Yes | Aerobic exercise/rest | 10 days | 10 | 65-75% MHR |
| Legrand & Neff (2016) | 11/10 | 27-67 | 8/17 | BDI-II | High | Yes | Stretching/rest | 10 days | 10 | 65-75% MHR |
| Moraes et al. (2019) | 9/7 | ≥ 60 | 3/13 | BDI-II | High | Yes | Aerobic exercise/rest | 12 weeks | 24 | 70% MHR |
| Moraes et al. (2019) | 9/7 | ≥ 60 | 3/13 | BDI-II | High | Yes | Resistance training/rest | 12 weeks | 24 | 70% 1-MR |
| Norouzi et al. (2024) | 17/17 | 18-70 | 8/26 | BDI-II | High | Yes | Multimodal exercise/rest | 8 weeks | 16 | 70% MHR |
| Olson et al. (2017) | 15/15 | 18-30 | 6/24 | BDI-II | High | Yes | Aerobic exercise/light stretching | 8 weeks | 24 | 40–65% HR reserve |
| Siddarth et al. (2023) | 55/58 | ≥ 60 | 31/82 | HAM-D | High | Yes | Tai Chi/rest | 12 weeks | 12 | Low to moderate |
| Szuhany & Otto (2019) | 15/16 | 18-65 | 5/16 | BDI-II | High | Yes | Aerobic exercise/light stretching | 12 weeks | 12 | Moderate |
| Tolahunase et al. (2018) | 29/29 | 19-50 | 27/31 | BDI-II | High | Yes | Yoga/rest | 12 weeks | 60 | Low to moderate |
| Wang & Li (2022) | 30/30 | NM | NM | HAM-D | High | Yes | Aerobic exercise/rest | 8 weeks | 32 | 120-150 beats/min |
| Zhang et al. (2022) | 20/19 | 30-60 | 4/35 | BDI-II | High | Yes | Tai Chi/rest | 12 weeks | 24 | Low to moderate |
| Beck Depression Inventory (BDI) [26], Hamilton Depression Rating Scale (HAM-D) [27], Montgomery-Åsberg Depression Rating Scale (MADRS) [27], The Geriatric Depression Scale (GDS) [31], Depression Anxiety Stress Scales (DASS) [32], or Hospital Anxiety and Depression Scale (HADS) [33], Heart Rate (HR), Maximal Heart Rate (MHR), Maximal Repetition (MR), Metabolic Equivalent of Task (MET). | ||||||||||
Table 2.
ANOVA table of Meta-regression.
| Model | Sum of Squares | df | Mean Square | F | p-value | R2 adjusted |
|
| M₁ | Regression | 19.056 | 1 | 19.056 | 39.432 | < .001 | 0.612 |
| Residual | 12.082 | 25 | 0.483 | ||||
| Total | 31.138 | 26 | |||||
| M₂ | Regression | 25.011 | 6 | 4.169 | 13.608 | < .001 | 0.744 |
| Residual | 6.127 | 20 | 0.306 | ||||
| Total | 31.138 | 26 | |||||
| Note. M₁ includes Workload; M₂ includes Workload and Instrument | |||||||
Table 3.
Effect Size Meta-Regression Terms Tests.
| Subgroup | F | df₁ | df₂ | p-value | ||
| Workload | Full dataset | 9.759 | 1 | 20 | .005 | |
| Low depression | 15.823 | 1 | 2 | .058 | ||
| High depression | 6.582 | 1 | 15 | .022 | ||
| Instrument | Full dataset | 3.515 | 4 | 20 | .025 | |
| Low depression | 10.211 | 3 | 2 | .091 | ||
| High depression | 4.385 | 2 | 15 | .032 | ||
| Note. Fixed effects tested using Knapp and Hartung adjustment. | ||||||
Table 4.
Resume of methodological criteria covered in this work.
| Quality Characteristics | Covered in Meta-Analysis? | Details |
| Protocol pre-registration | Yes | PROSPERO (CRD420251121919) |
| Use of PRISMA | Yes | PRISMA 2020 reporting |
| Independent screening and data extraction | Yes | Two independent reviewers; third reviewer for consensus |
| Comprehensive search | Yes | Multiple databases, PICOS strategy |
| Standardized eligibility criteria | Yes | DSM/ICD diagnosis, validated instruments, exclusion of comorbidities/med changes |
| Use of validated depression assessment tools | Yes | BDI, HAM-D, PHQ-9, CES-D, MADRS, etc. |
| Risk of bias (RoB 2) assessment | Yes | All five domains, two blinded reviewers |
| Sensitivity/subgroup analyses | Yes | Performed as part of results |
| Transparent study flow and exclusion reporting | Yes | PRISMA diagram, full text review and exclusion reasons |
| Handling of missing data | Yes | SDs estimated from SEs, CIs, p-values if needed |
| Statistical rigor (heterogeneity, influence, funnel) | Yes | Tau², Q-test, I², Cook's D, studentized residuals, funnel plot asymmetry |
| Assessment of comorbidity | Yes | Included as a section in results |
| Blinding of outcome assessors | Yes (as RoB domain) | Not always feasible for exercise; assessed as risk of bias domain |
| Adverse event/safety reporting | Not explicitly | Not detailed in the provided text |
| Power analysis/sample size in included studies | Yes | In meta-analysis description |
| Long-term follow-up | Not systematically | Mentioned as a gap, not systematically analyzed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



