
Submitted:
27 October 2025
Posted:
29 October 2025
You are already at the latest version
Abstract
Brazil recently implemented a national menstrual health program within its Public Health System (Sistema Único de Saúde, SUS), representing a significant policy shift toward recognizing menstrual dignity as a public health and human rights issue. The distribution of menstrual products has expanded rapidly; however, this alone is insufficient to address the structural inequalities affecting menstrual health. This article aims to analyse the implementation of the menstrual health program in Brazil, identify existing inequalities and operational barriers, and propose a research and data framework capable of strengthening monitoring, policymaking, and global collaboration. The study is part of the PLATO project (Work Package 1), integrating public health, gender equality, and implementation science. A narrative analysis was conducted using government and legal documents, demographic and WASH data, and international literature on menstrual equity. Despite strong legislation and intersectoral governance, substantial gaps remain in access, digital inclusion, infrastructure, and participation of marginalized groups. Brazil lacks standardized indicators, interoperable data systems, and monitoring strategies to assess real outcomes. A logic model and equity-centered research architecture are proposed to address these gaps by integrating product provision, WASH, data systems, community participation, and global integration. Brazil has made fundamental progress in menstrual health policy. However, achieving menstrual dignity requires moving beyond product distribution to integrated data collection, infrastructure, equity monitoring, and participatory governance. This framework offers a model applicable to Brazil and other low- and middle-income countries.
Keywords:
menstrual health
; period poverty
; health equity
; public policy
; WASH
; implementation research
; Brazil
Background
Period poverty is a complex and multidimensional condition marked by inaccessibility to resources, infrastructure, and information necessary for complete menstrual management [1]. Taboos and misconceptions regarding menstruation in society are often marked by gender inequality [2]. In Brazil, period poverty is directly related to structural inequalities, translating into socioeconomic, racial, and territorial disparities. Period poverty most heavily impacts people who menstruate from marginalised communities, such as urban peripheries and rural areas [1,3]. Among young Brazilian women aged 14 to 24, 33% declared a history of financial inability to buy sanitary pads. It is noteworthy that 33% of the women have already used toilet paper instead of sanitary pads [1].
Menstrual health awareness and equity should be part of health promotion strategies, to minimise taboos, misinformation, stigma and discrimination [4,5,6]. Brazil has made significant progress in certain aspects of menstrual health by developing the Menstrual Health Protection and Promotion Programme (Programa de Proteção e Promoção da Saúde Menstrual), underpinned by Law 14.214 in October 2021 [7] and regulated by Decree 11.432 in March 2023 [8], marking a pivotal policy shift. This programme provides free menstrual hygiene products to vulnerable populations, including low-income adolescents in public schools, women experiencing homelessness, and individuals in the prison system or complying with socio-educational measures [7,8,9]. Through the program, 40 units of disposable sanitary pads are made available every two months [9]. Other initiatives of the program involve developing menstrual training and education actions, ensuring qualified listening in health units, promoting gender equality and encouraging self-care, with attention to the physical and emotional effects of menstruation [8,9]. Implementation of the program began in January 2024, with distribution integrated into the national public health system, Sistema Único de Saúde, (SUS) through the Popular Pharmacy Program of Brazil (Programa Farmácia Popular do Brasil, PFPB). Over 31,000 accredited pharmacies across approximately 4,600 municipalities are now dispensing products to an estimated 24 million eligible people aged 10–49, identified through Brazil’s Cadastro Único (CadÚnico) social registry [9,10]. Access is facilitated via a digital authorisation system, Meu SUS Digital, with support provided through primary care units (Unidades Básicas de Saúde, UBS) for those with limited digital access [9]. Governance spans multiple ministries, including Health, Education, Justice, Women, Human Rights, and Social Development, ensuring cross-sectoral collaboration, particularly for provision to schools and prisons [8].
This article was conducted as part of the PLATO (Period Poverty and Health Outcomes Exploration) project, focusing on Work Package 1 (WP1) in Brazil. The objectives are to critically analyze the implementation of the national menstrual health program in Brazil, identify inequalities and operational challenges that still exist, and propose a research and data framework capable of strengthening evidence generation, improving public policy decision-making, and positioning Brazil in the global context of menstrual health research.
Implementation and National Coverage
Using Farmácia Popular for distribution leverages a well-established infrastructure already used to deliver essential medicines such as antihypertensives and diabetes treatments. Detailed operational guidance and professional training have been rolled out nationally, alongside plans to establish a dedicated menstrual health observatory to strengthen research and monitoring [9]. While these measures lay strong foundations, gaps remain in translating national policy into equitable access [11].
Coverage varies across regions, reflecting Brazil’s socioeconomic and geographical inequalities. The North and Northeast regions face the greatest barriers, characterised by higher poverty levels, limited transport infrastructure, and fewer accredited pharmacies. While over 97% of households now have access to private toilets and sanitation, gaps in waste management persist in remote areas and informal settlements [12]. The chance of a black girl not having access to bathrooms is almost three times as likely as that of finding a white girl in the same conditions [1]. Considering only girls from Northern Brazil, which comprises one of the poorest regions of the country and with the least availability of resources, the risk of them not having an exclusive bathroom is 33 times higher than that of girls from the Southeast [1]. Approximately 2.8 million girls (18%) reside in households that rely on wells, stored rainwater, or other alternative water sources [1,6,13].
Among Brazilian students, approximately 321,000 (3% of the total) study in schools that lack adequate bathroom facilities, with 37.8% residing in the Northeast. When rural schools are analyzed separately, the value rises to 6.4%. This percentage reaches 8.4% when evaluating only schools in the North of the country. It is estimated that 1.24 million girls (11.6% of the total) do not have access to toilet paper in school bathrooms, and 66.1% of these girls are black or brown. Almost 652,000 girls (6% of the total) do not have access to sinks or washbasins for use in their schools. More than 3.5 million girls attend schools that do not provide soap to wash their hands after using the bathroom, among whom 62.6% are black or brown. Cumulatively, it is observed that more than 4 million girls (38.1% of the total) attend schools that lack at least one of these minimum hygiene requirements. Almost two hundred thousand students are totally deprived of the minimum conditions to take care of their menstruation in their schools [1,14].
Integration within SUS
Integrating menstrual health products into SUS strengthens sustainability and normalises menstrual care as part of routine health services rather than as a temporary aid initiative. The use of CadÚnico and digital platforms helps to target resources efficiently [1,15] but introduces potential barriers. Administrative delays in updating social registry data can exclude newly vulnerable households, and digital authorisation may be inaccessible to those without smartphones or reliable internet connections, or with low education [6]. In rural or remote areas, sparse pharmacy coverage increases travel distances and indirect costs, while some eligible groups, including homeless individuals, migrants, and those in undocumented situations, face additional barriers to participation [17].
Addressing Equity and Inclusion
Despite the programme’s national scope, certain populations remain at risk of exclusion. These include adolescents in remote Amazonian municipalities, Indigenous and quilombola communities (Afro-Brazilian descendants of escaped slaves), migrants at border regions, and individuals without access to identification documents. Qualitative reports suggest that stigma, school absenteeism, and unsafe coping mechanisms such as prolonged menstrual pad use or reliance on improvised materials continue to affect many, indicating that systemic change requires more than product provision [18,19]. Social norms, education, and infrastructure must evolve alongside supply chains to achieve true menstrual dignity [4,19].
Logic Model: A National–Global Research and Delivery Ecosystem for Menstrual Health
The purpose of the logic model (Table 1) is to strengthen Brazil’s ability to generate high-quality, representative evidence, inform policy, and participate in multi-country research while improving service delivery and equity.
The successful implementation and sustainability of Brazil’s national menstrual health programme rely on several key assumptions. Political continuity is crucial for maintaining momentum and ensuring that menstrual health remains a national priority beyond election cycles and changes in government leadership. Stable financing is required to guarantee uninterrupted product supply, infrastructure improvements, and workforce capacity [20,21]. Trust in data privacy is vital to encourage the sharing of sensitive health and social data, particularly as the programme expands its digital components. Finally, active community engagement, including participation by civil society and youth groups, is critical to foster local ownership, reduce stigma, and ensure that policies and services reflect the lived realities of diverse populations.
However, there are significant risks that could undermine these goals. Administrative lags in updating CadÚnico, the national social registry, may lead to the exclusion of newly vulnerable households, particularly those experiencing sudden poverty, migration, or displacement. Digital exclusion remains a significant barrier for individuals and communities that lack access to smartphones, reliable internet connections, or digital literacy skills [22]. The WASH infrastructure, especially in schools and rural areas, can prevent menstruators from fully benefiting from product provision, perpetuating absenteeism and unsafe practices [23]. High staff turnover within health and education systems can disrupt service delivery and weaken institutional memory. Finally, fragmented data systems across ministries and levels of government increase the risk of duplications, inconsistencies, and delays in monitoring and evaluation [24].
Mitigation strategies must be proactive and multifaceted. Offline workflows led by community health workers (CHWs) can bridge digital gaps by enabling authorisations and service delivery without requiring constant internet connectivity. Establishing on-site dispensing at primary care units (UBS) in areas with low pharmacy density can bring services closer to underserved populations and reduce travel-related barriers. Ring-fenced funding for WASH improvements ensures that resources are specifically allocated to upgrading school toilets, water supply, and waste disposal facilities, creating a supportive environment for menstrual health. The adoption of national data standards can promote interoperability, reduce duplication, and streamline reporting across ministries and sectors. Additionally, federated analytics systems offer a privacy-preserving solution by enabling collaborative analysis of datasets without the need to share raw, individual-level data, thereby improving both national and global research integration.
Conceptual Framework: Equity-Centred Data and Research Architecture
The proposed conceptual framework seeks to explain how structural, systemic, community, and individual factors shape menstrual health outcomes in Brazil. It also identifies how data systems and research methods can be strategically strengthened to close existing evidence gaps and position Brazil as a key participant in global health research. The framework adopts an equity-centred approach, recognising that menstrual health outcomes are shaped by a complex interplay of policies, service delivery, social norms, and individual circumstances.
Structural and Policy Layer
At the highest level, laws, financing arrangements, social protection policies, education standards, and infrastructure investments determine the entitlements and resources available to different populations. These structural determinants define who is eligible for menstrual health interventions and how these resources flow to municipalities and schools. Critical levers within this layer include programme rules governing product distribution, the scope and coverage of CadÚnico (Brazil’s social registry), minimum standards for WASH in schools, and procurement and disposal regulations. Public data transparency is essential to ensure accountability and to support adaptive policymaking.
Health System Layer (SUS Integration)
The Brazilian Unified Health System (Sistema Único de Saúde, SUS) plays a pivotal role in translating national policies into tangible services. This layer encompasses primary care units (Unidades Básicas de Saúde, UBS), the Farmácia Popular network, supply chain management, digital authorisation systems, and integrated information systems. Effective service delivery depends on several mechanisms: adequate pharmacy and UBS density, the ability of community health workers to conduct offline authorisations, reliable stock management systems, and strong data flows that link product dispensing to primary care and school health programmes.
Community and Service Environment Layer
Community-level factors influence whether entitlements can be accessed and used effectively. This includes the quality of school WASH infrastructure, the availability of safe disposal facilities, transport time to pharmacies or UBS, and the presence of local pharmacies or outreach services. Social norms, stigma, and the role of civil society organisations (CSOs) also have a significant impact. Community engagement, particularly through youth participation and co-production initiatives, can challenge stigma, improve programme literacy, and ensure that services are relevant and culturally appropriate.
Individual and Household Layer
At the most immediate level, individual and household characteristics shape menstrual health experiences and service uptake. These include access to identity documents, availability of phones and internet connectivity, disability status, migration background, and household income stability. Caregiver support plays a critical role for adolescents. Intersectionality is essential at this layer: age, race or colour, geography, disability, and indigeneity interact to produce unique patterns of risk and barriers to access [16]. Understanding these factors is crucial for designing equitable interventions.
Data and Research Layer (Cross-Cutting Enabler)
Data and research form a cross-cutting layer that connects all others. A national core indicator set, harmonised survey instruments, and a sentinel surveillance network are required to generate reliable and comparable evidence (Table 2). Privacy-preserving linkages and federated analytics are vital to ensure that data can be analysed collaboratively without moving sensitive, individual-level information. By aligning with global measurement standards, Brazil can participate in multi-country studies and contribute to international evidence generation without compromising data sovereignty.
This integrated framework combines evidence generation, equity-centred service delivery, and global interoperability to advance menstrual health in Brazil. The five pathways of change illustrate how products, WASH infrastructure, social support, and data systems work together to improve outcomes while reducing stigma and disparities (Figure 1). Core indicators provide a standardised measurement system to monitor coverage, equity, usability, outcomes, and data quality. Diverse study designs, including sentinel surveillance, population surveys, pragmatic trials, and qualitative research, ensure that interventions are contextually informed and representative. By linking data systems through privacy-preserving methods and promoting open science practices, Brazil can create a robust and sustainable research architecture. This approach strengthens national policy-making and positions Brazil as a key contributor to global menstrual health research, fostering both local impact and international learning.
Governance and Partnership for Global Readiness
Robust governance is essential to achieve national coherence and global compatibility. An interministerial data council, including academic and civil-society representatives, should oversee standards, ethics, and data-sharing. Legal templates for data-sharing agreements and data protection impact assessments can accelerate collaborations with international partners (Table 3). A national training pipeline should focus on implementation science, advanced statistics, and research data management, with twinning arrangements established with global research centres. Brazil should also lead a Latin American node to coordinate regional studies and negotiate common indicator sets for cross-country comparability.
Data and Accountability
While the legislative and operational structures are in place, data transparency remains limited. Publicly available indicators on authorisations, redemption rates, pharmacy stock-outs, and school WASH conditions are essential for accountability and continuous improvement. Brazil has previously demonstrated strong capacity for open data in health through its vaccine and primary care reporting systems [25], and similar approaches could transform menstrual health monitoring (Table 4).
Interpretation and Way Forward
Brazil has achieved significant progress by embedding menstrual health within its universal health system and adopting a multi-ministerial approach. However, achieving equitable access requires addressing persistent inequalities in infrastructure, digital access, and social norms. Product distribution through pharmacies is a necessary foundation but cannot substitute for investments in school sanitation, safe disposal, and education.
By closing regional and demographic gaps, improving transparency, and strengthening intersectoral governance, Brazil can shift from a national programme in theory to menstrual dignity in practice. This experience has global relevance, offering lessons for countries seeking to institutionalise menstrual health as a fundamental component of public health, gender equality, and social justice.
It is essential to develop robust strategies that enable the monitoring and evaluation of implemented measures, with the establishment of standardized indicators to enhance the various interfaces of menstrual health. Additionally, the use of open data, such as OpenDataSUS, in conjunction with sentinel networks and population surveys, would enable the monitoring of the equity and coverage of implemented policies, the early and immediate identification of complications or limitations, and the perception of best practices in different regional contexts. It is essential that this continuous monitoring process include the active participation of civil representatives, including young people and historically marginalized groups, to ensure that this national program meets real local needs while sustainably preserving national cultural aspects in the short and long term.
Author Contributions
GD developed the ELEMI program and the PLATO project. This was furthered by GD and PP. GD developed the PLATO equity-centred framework. GD wrote the first draft and was furthered by all other authors. All authors critically appraised, reviewed and commented on all versions of the manuscript. All authors read and approved the final manuscript. All agree to be accountable for all aspects of the work, ensuring the accuracy and integrity of the study. All authors meet the ICMJE criteria for authorship.
Funding
NIHR Research Capability Fund
Acknowledgements
PLATO Consortium
Conflicts of interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
References
- United Nations Population Fund (UNFPA); United Nations Children's Fund (UNICEF). Menstrual poverty in Brazil: inequalities and human rights violations [in Portuguese]. Brasília: UNFPA; UNICEF; 2021.
- Perucha LM, Avciño CJ, Llobet CV, Valls RT, Pinzón D, Hernández L, et al. Menstrual health and period poverty among young people who menstruate in the Barcelona metropolitan area (Spain): protocol of a mixed-methods study. BMJ Open. 2020;10(7):e035914. [CrossRef] [PubMed] [PubMed Central]
- 3. Cobo B, Cruz C, Dick PC. Gender and racial inequalities in access to and use of Brazilian health services. Cien Saude Colet. 2021;26(9):4021–4032. [CrossRef]
- Paula MC, Monteiro BB, Ruela LO, Silva MMJ. Period poverty: a scoping review. Rev Bras Enferm. 2025;78(2):e20240567. [CrossRef]
- United Nations Population Fund (UNFPA). State of the art for menstrual dignity promotion: advances, challenges and potentialities [in Portuguese]. Brasília: UNFPA; 2022.
- Moraes MFRC, Nunes R, Duarte I. Period poverty in Brazil: a public health emergency. Healthcare (Basel). 2025;13:1944. [CrossRef]
- Brazil. Law No. 14.214 of October 6, 2021. Establishes the Program for Protection and Promotion of Menstrual Health. Diário Oficial da União. 2021 Oct 7.
- Brazil. Decree No. 11.432 of March 8, 2023. Regulates Law No. 14.214 of October 6, 2021. Diário Oficial da União. 2023 Mar 9.
- Brazil. Ministry of Health; Ministry of Women; Ministry of Human Rights and Citizenship; Ministry of Education; Ministry of Social Development and Fight Against Hunger; Ministry of Justice and Public Security. Menstrual Dignity Program – Brazil 2024 [in Portuguese]. Brasília: Federal Government of Brazil; 2024.
- Brazil. Ministry of Health. Farmácia Popular served more than 24 million Brazilians in 2024, the highest number in history [Internet]. Brasília: Ministry of Health; 2025 Jan 14 [cited 2025 Sept 16]. Available from: https://www.gov.br/saude/pt-br/assuntos/noticias/2025/janeiro/farmacia-popular-amplia-atendimento-e-chega-a-mais-de-400-novos-municipios.
- United Nations Population Fund (UNFPA). Recommendations for implementing menstrual dignity initiatives [in Portuguese]. Brasília: UNFPA; 2023.
- Brazilian Institute of Geography and Statistics (IBGE). 2022 Demographic Census: preliminary results [in Portuguese]. Rio de Janeiro: IBGE; 2022 [cited 2025 Sept 14]. Available from: https://censo2022.ibge.gov.br.
- Brazilian Institute of Geography and Statistics (IBGE). Household Budget Survey 2017–2018: analysis of individual food consumption in Brazil [in Portuguese]. Rio de Janeiro: IBGE; 2020 [cited 2025 Sept 14].
- Brazilian Institute of Geography and Statistics (IBGE). National Health Survey 2013: perception of health status, lifestyle and chronic diseases [in Portuguese]. Rio de Janeiro: IBGE; 2014 [cited 2025 Sept 16].
- Brazil. Ministry of Social Development and Fight Against Hunger. Basic concepts: Unified Registry [in Portuguese]. Brasília: MDS; 2023 [cited 2025 Sept 19].
- Soeiro RE, Rocha L, Surita F, Bahamondes L, Costa ML. Period poverty: menstrual health and hygiene issues among adolescent and young Venezuelan migrant women at the northwestern border of Brazil. Reprod Health. 2021;18(1).
- Marques FH. Menstrual poverty among homeless women [dissertation in Portuguese]. Maringá (PR): Unicesumar; 2024.
- Gupta K, et al. Menstrual health experiences of adolescents in institutional care. SAGE Open. 2024. [CrossRef]
- Adane Y, et al. Assessment of barriers towards menstrual hygiene management: a systematic approach. Front Reprod Health. 2024.
- Machado CV, Lima LD, Andrade CLT. Political struggles for a universal health system in Brazil. Glob Health. 2019;15(1):116. [CrossRef]
- Massuda A, Hone T, Leles FAG, de Castro MC, Atun R. The Brazilian health system at crossroads: progress, crisis and resilience. BMJ Glob Health. 2018;3(4):e000829. [CrossRef]
- Ferreira SKS, Sene IJ Jr. Digital inclusion analysis for Brazil’s unified health system. J Health Inform. 2023;15(2):65–74. [CrossRef]
- Chinyama J, Chipungu J, Rudd C, Mwale M, Verstraete L, Sikamo C, et al. Menstrual hygiene management in rural schools of Zambia: a descriptive study of knowledge, experiences, and challenges faced by schoolgirls. BMC Public Health. 2019;19:16. [CrossRef]
- Jayathissa P, Hewapathirana R. Enhancing interoperability among health information systems in low- and middle-income countries: a review of challenges and strategies. arXiv [preprint]. 2023. Available from: https://arxiv.org/abs/2309.12326.
- Brazil. Ministry of Health. OpenDataSUS: Open data platform of the Unified Health System (SUS) [Internet, in Portuguese]. Brasília: Ministry of Health; [cited 2025 Sept 18]. Available from: https://opendatasus.saude.gov.br.
Figure 1.
Equity-centered conceptual framework linking structural and policy-factoring that influences a variety of environments. These should be embedded as cross-cutting data and research when developing policies. UBS: Basic Health Unit (Unidade Básica de Saúde); WASH: Water, Sanitation, and Hygiene.
Figure 1.
Equity-centered conceptual framework linking structural and policy-factoring that influences a variety of environments. These should be embedded as cross-cutting data and research when developing policies. UBS: Basic Health Unit (Unidade Básica de Saúde); WASH: Water, Sanitation, and Hygiene.
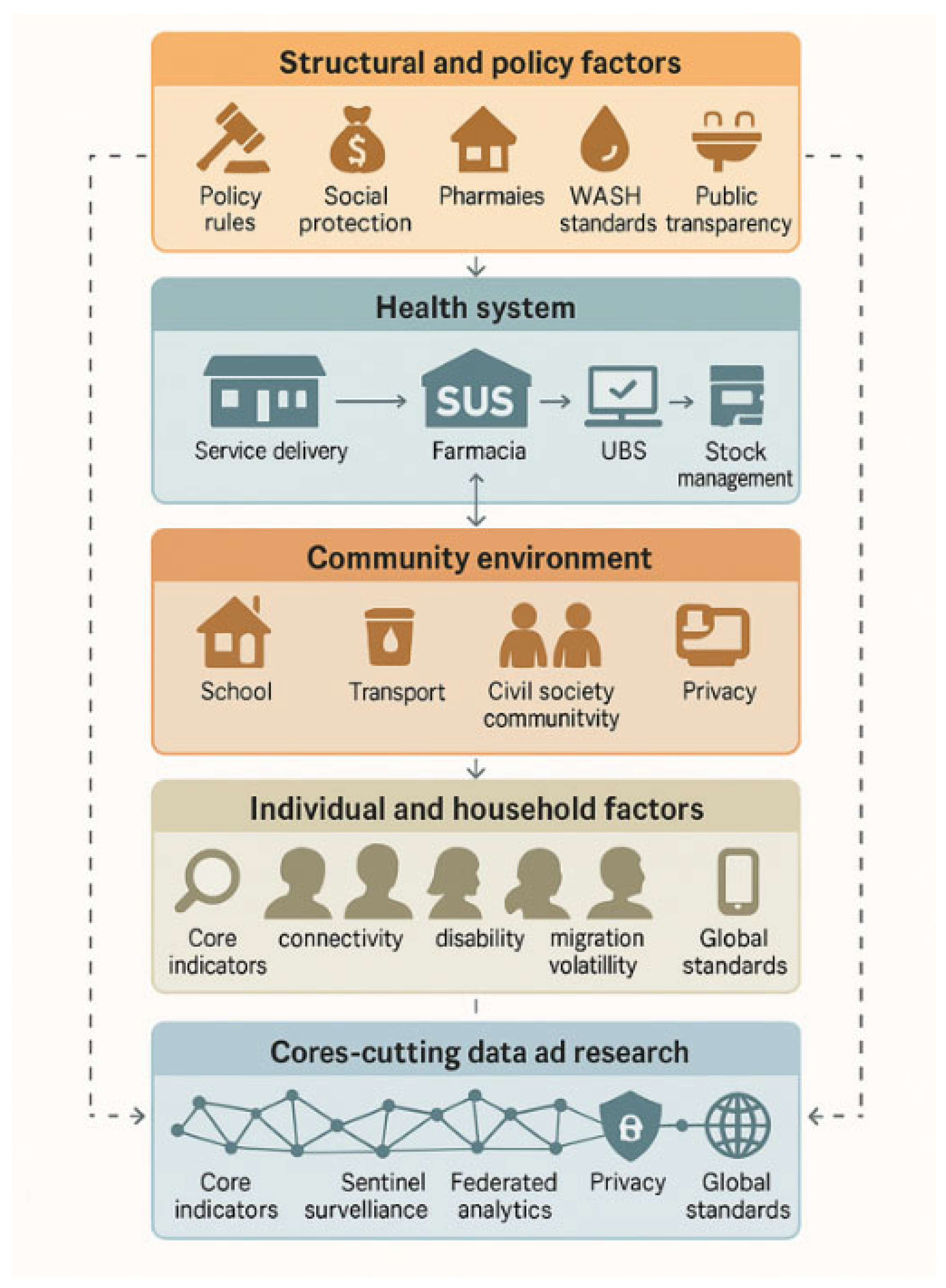

Table 1.
Indicates the components of the logic model and measurable indicators.
| Element | What it includes | Exemplars for Brazil | Measurable indicators |
| Inputs | Political mandate; interministerial governance; SUS primary care and Farmácia Popular networks; CadÚnico and Meu SUS Digital rails; IBGE and school WASH datasets; ethics/IRB capacity; academic consortia; civil-society and youth groups; secure data infrastructure and analytics capacity | Ministry of Health, Education, Justice, Human Rights; municipal health secretariats; universities; community health workers; UNICEF/UNFPA collaborations | Annual programme budget; number of accredited dispensing points per 10,000 girls 10–19; IRB turnaround time; number of trained field researchers; active data-sharing agreements |
| Activities | Standardise national research core set; strengthen sampling frames; integrate routine data with periodic surveys; mixed-methods studies; school-based WASH auditsa; equity-focused implementation research; capacity-building for data management and open science; translation to policy briefs; global study alignment | Annual school and UBS sentinel sites; qualitative panels with Indigenous and quilombola communities; pragmatic trials on access pathways; data stewardship training; pre-registration of protocols | Proportion of studies using the national core set; share of studies with pre-registered protocols; number of sentinel schools/UBS per region; proportion of projects with community co-production plans |
| Outputs | Curated, de-identified datasets; harmonised indicators; disaggregated dashboards; validated survey tools in Portuguese and Indigenous languages; technical reports; policy briefs; open code repositories; co-authored publications with subnational data | Menstrual-health observatory; Git-hosted codebooks and analysis scripts; bilingual instrument library | Datasets published to an open catalogue; median data release latency; number of instruments validated; number of policy briefs tabled in interministerial meetings |
| Short-term outcomes (1–2 years) | Complete, comparable coverage and equity metrics; reduced administrative exclusion; better targeting in low-pharmacy and remote municipalities; improved school WASH remediation plans | UBS dispensing added where pharmacy density is low; offline authorisation via CHWs; published WASH remediation timelines | Authorisations issued and redeemed per 1,000 eligible, by age, race/colour, disability, municipality; stock-out rate; school WASH adequacy score; absenteeism due to menstruation |
| Medium-term outcomes (3–5 years) | More representative national research portfolio; Brazil enrolled in multi-country consortia with interoperable data; routine use of findings in policy; decline in stigma and missed school/work days | Brazil leading a regional node for Latin America; pooled analyses with standard metadata | Share of studies with intersectional disaggregation; proportion of global trials including Brazilian sites; effect sizes for reduced absenteeism and improved well-being |
| Impact (5+ years) | Menstrual dignity embedded in universal health coverage; resilient, equitable systems; Brazil recognised as a global evidence leader; transferable methods adopted by other LMICs | Sustainable financing line, enduring observatory, standing global collaborations | Reduction in inequity gaps between North/Northeast and South/Southeast on key indicators; independent evaluations showing sustained coverage and quality |
aBased on adequate number of toilet stalls, lockable doors, soap, water and disposal bins. CadÚnico: Unified Registry (Cadastro Único); CHWs: Community Health Workers; IBGE: Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística); IRB: Institutional Review Board; LMICs: Low- and Middle-Income Countries; SUS: Unified Health System (Sistema Único de Saúde); UBS: Basic Health Unit (Unidade Básica de Saúde); UNFPA: United Nations Population Fund; UNICEF: United Nations International Children’s Fund; WASH: Water, Sanitation, and Hygiene.
Table 2.
Integrated approach to strengthening menstrual health research and delivery in Brazil.
| Domain | Components | Purpose and Expected Outcomes |
| Mechanisms of Change and Evidence Pathways | Coverage pathway – eligibility → authorisation → redemption → continuity of supply | Ensure eligible individuals receive timely, continuous access to menstrual products, minimising drop-off points. |
| Usability pathway – products + WASH + disposal + privacy | Improve safe and dignified menstrual management, reduce infections and stigma, and increase school attendance and participation. | |
| Equity pathway – intersectional identification of barriers and tailored delivery | Reduce regional and demographic disparities through targeted service delivery via UBS, schools, and community health workers. | |
| Learning pathway – routine dashboards, sentinel studies, mixed-methods research | Enable adaptive programme management through continuous, real-time feedback loops. | |
| Globalisation pathway – adoption of common data dictionaries and metadata standards | Position Brazil to participate in multi-country research and align with global menstrual health datasets. | |
| Core Indicators and Measurement Standards | Access and continuity – authorisations issued and redeemed per 1,000 eligible; median time from eligibility to first redemption; refill regularity; stock-outs per site-month | Measure programme reach, timeliness, and supply chain reliability. |
| Equity – disaggregation by age, race/colour, region, municipality, disability, school enrolment, migration status, socioeconomic deprivation | Identify inequities and monitor whether vulnerable populations are being reached. | |
| Usability and environment – school WASH adequacy index, safe disposal availability, travel time to dispensing points or UBS, digital access proxies | Assess environmental factors influencing menstrual product use and programme usability. | |
| Outcomes – menstruation-related absenteeism, self-reported stigma, infection proxies, validated quality-of-life scales in Portuguese and Indigenous languages | Track health, social, and educational outcomes linked to menstrual health. | |
| Data quality – completeness, timeliness, concordance across sources, pre-registered protocols, reproducible code availability | Ensure high-quality, transparent, and reliable data. | |
| Study Designs and Data Architecture | Sentinel surveillance – stratified schools and UBS with oversampling of remote and marginalised populations | Generate real-time, representative data across diverse geographies and communities. |
| Periodic population surveys – rotating panels with intersectional modules, using mixed modes (in-person, phone, digital) | Capture longitudinal trends and reduce exclusion through flexible data collection methods. | |
| Implementation research – pragmatic trials comparing delivery models and WASH-linked interventions | Evaluate effectiveness and cost-effectiveness of different service models, focusing on school absenteeism and participation. | |
| Qualitative inquiry – longitudinal ethnographic studies and youth advisory panels | Understand social norms, stigma, and lived experiences to refine interventions. | |
| Data linkage – privacy-preserving connections between dispensing, primary care, school health, and WASH data | Enable comprehensive analyses without moving raw, sensitive data. | |
| Open science practices – pre-registration, publicly archived analytic code, de-identified datasets | Promote transparency, reproducibility, and international collaboration. |
UBS: Basic Health Unit (Unidade Básica de Saúde); WASH: Water, Sanitation, and Hygiene.
Table 3.
Action priorities for a globally connected ecosystem.
| Priority | Concrete actions | Success indicators |
| National core indicator set | Publish a harmonised dictionary, disaggregation rules, and survey modules; mandate use in funded studies | ≥80% of new studies adopt the core set; inter-study comparability achieved |
| Sentinel network and dashboards | Establish sentinel sites in schools and UBS across all macro-regions; develop public dashboards with equity disaggregation | Dashboards refreshed monthly; measurable reductions in equity gaps |
| Inclusive delivery models | Introduce UBS on-site dispensing; enable offline authorisation by community health workers; provide transport vouchers in low-density areas | Redemption parity between remote and urban municipalities; reduced travel time |
| WASH-linked integration | Link product provision to school WASH audits and remediation funds; develop standard disposal protocols | Increase in schools meeting WASH standards; decline in menstruation-related absenteeism |
| Ethics, privacy, and open science | Develop data protection frameworks; use federated analytics; promote pre-registration and open data practices | Faster data-sharing agreements; higher proportion of pre-registered studies |
| Global interoperability | Align indicators and metadata with global research standards; contribute to international data repositories | Increase in Brazil’s participation in multi-country projects and publications |
| Workforce and community capacity | Build a national training pipeline for researchers and field teams; establish community and youth co-production panels | Trained researchers per state; proportion of projects with documented co-production plans |
UBS: Basic Health Unit (Unidade Básica de Saúde); WASH: Water, Sanitation, and Hygiene.
Table 4.
Actionable priorities to strengthen Brazil’s menstrual health programme.
| Action area | Recommended measures |
| Closing the last-mile gap | Introduce on-site dispensing at UBS facilities in areas with few pharmacies. Enable community health workers to generate authorisations offline and support initial product redemption. |
| Linking products to WASH improvements | Integrate funding for upgrading school toilets, water access, and disposal facilities. Conduct regular audits and publish remediation timelines, prioritising the North and Northeast regions. |
| Reducing administrative exclusion | Enhance outreach to register vulnerable populations, including undocumented individuals and migrants. Simplify identification requirements for those in street situations or lacking official documents. |
| Transparent monitoring and reporting | Establish a national dashboard showing coverage rates, demographic disaggregation (age, race, municipality), stock-outs, and supply continuity. Commission independent evaluations of programme impacts on school attendance, infections, and stigma. |
| Strengthening governance and cross-sectoral collaboration | Maintain interministerial coordination, including ministries of Health, Education, Justice, and Human Rights, and extend collaboration to include sanitation and infrastructure sectors. |
UBS: Basic Health Unit (Unidade Básica de Saúde); WASH: Water, Sanitation, and Hygiene.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



