
Submitted:
09 October 2025
Posted:
14 October 2025
You are already at the latest version
Abstract
Background Menopause, whether natural, surgical, or medically induced, represents a significant transition in women’s health, often accompanied by biological, psychological, and social challenges. Despite its global prevalence, evidence on lived experiences across diverse populations remains limited, particularly setting as Brazil. Addressing these knowledge gaps is essential for designing equitable health interventions and informing policy.Methods The MARIE-Brazil chapter conducted a qualitative study as part of work-package 2a to explore menopausal experiences. A topics guide was used to conduct interviews of participants that were purposively sampled aged 18–99 years that self-identified as experiencing perimenopause, menopause, or post-menopause. Sampling captured heterogeneity across age, menopausal stage, socio-economic position, ethnicity, and healthcare access. Data were transcribed verbatim, anonymised, and analysed thematically using Braun and Clarke’s six-phase approach. To enhance rigour, coding was conducted by multiple researchers, guided by the Delanerolle and Phiri framework, and reporting followed COREQ guidelines.Results The findings indicate intersecting biological, psychological, socio-cultural, and health system determinants shaping experiences. Participants reported vasomotor symptoms, sleep disturbance, cognitive difficulties, and urogenital changes that influenced quality of life and occupational participation. Barriers to care included limited clinical knowledge, fragmented pathways, and financial inaccessibility of treatments. Cultural stigma, gender norms, and workplace discrimination further exacerbated inequities, particularly among women with multimorbidities or marginalised identities. Conversely, peer networks, supportive clinicians, and targeted interventions improved coping and health outcomes.Conclusion Menopause is not solely a biological milestone but a multifaceted transition shaped by structural and cultural determinants. Findings highlight urgent needs for inclusive healthcare training, workplace policy reform, and accessible treatment pathways. Incorporating lived experiences into service design and policy frameworks is critical to promoting equity in menopause care across diverse global settings.
Keywords:
menopause
; brazil
; experiences
; inequities
; opportunities
; inclusive care
Background
Menopause in Brazil represents a complex intersection of biological processes, cultural perceptions, and systemic health challenges [1,2]. It is commonly defined as the permanent cessation of menstruation following 12 consecutive months without a menstrual period, and is preceded by the perimenopausal phase characterised by irregular cycles and a wide spectrum of symptoms such as vasomotor instability, sleep disturbances, mood changes, and genitourinary difficulties [3]. While the majority of Brazilian women experience natural menopause around the median age of 49–51 years, the lived experience is highly variable depending on genetics, comorbidities, socioeconomic status, and access to healthcare [4,5,6,7]. Surgical menopause, often the result of hysterectomy and bilateral oophorectomy, is also prevalent in Brazil, reflecting both the historically high rates of gynaecological surgery [8]. In addition, medical menopause induced by chemotherapy, radiotherapy, or endocrine therapies in women with cancer or other conditions introduces an abrupt and often more severe transition, with profound psychosocial consequences [9]. Together, these pathways underscore the importance of recognising not only the biological dimensions of menopause but also its broader implications across perimenopause, menopause, and post-menopause in diverse Brazilian contexts.
The epidemiological significance of menopause in Brazil is magnified by demographic transitions [10,11]. Brazil, like much of Latin America, has undergone rapid population ageing, with women constituting a majority in older age groups. Life expectancy for Brazilian women is currently above 78 years [12,13], meaning that a substantial proportion will live more than one third of their lives in post-menopause. This demographic shift carries profound implications for public health planning and national infrastructure. Women over 50 represent a growing share of the Brazilian workforce, particularly in healthcare, education, and informal caregiving sectors, and their productivity is directly influenced by menopausal wellbeing [14]. Poorly managed symptoms may contribute to absenteeism, reduced efficiency, and premature exit from employment, thereby affecting economic growth. At the same time, the burden on healthcare services is amplified, as postmenopausal women face elevated risks of osteoporosis, cardiovascular disease, diabetes, and mental health conditions. Thus, the menopause transition is not only an individual health milestone but also a pressing public health issue with wide-ranging social and economic consequences for Brazil [15,16].
Despite its epidemiological weight, the menopausal landscape in Brazil remains underdeveloped, characterised by fragmented provision, clinical guidelines not incorporated into health care, and sociocultural barriers to care. Awareness of menopause as a health issue is uneven across regions, with urban women generally reporting greater knowledge and healthcare access compared to their rural counterparts [3]. Primary care services within the Unified Health System (Sistema Único de Saúde, SUS) are not consistently equipped to address menopausal health, with significant variation in clinician training and confidence. Hormone replacement therapy (HRT) is available, but access is shaped by socioeconomic disparities, with those in the private system often benefiting from specialist care while those reliant on SUS face limited options, long waiting times, and scarce counselling about risks and benefits. Non-hormonal interventions and mental health support are even less developed, leaving many women to rely on informal coping mechanisms or complementary practices without professional oversight. Stigma and cultural silence surrounding menopause compound these systemic weaknesses, discouraging open dialogue and reinforcing inequities [17,18]. The evidence base on Brazilian menopausal experiences is sparse, with existing research concentrated in specific urban centres and predominantly quantitative, thereby missing the nuanced sociocultural and experiential dimensions of the transition.
Rationale
The Brazilian chapter of MARIE-WP2a was designed to explore gaps, recognising that menopause in Brazil is insufficiently studied through the lens of lived experience and intersectional inequality. While epidemiological surveys and clinical audits provide some insights into symptom prevalence and HRT usage, they fail to capture the everyday realities of women navigating biological, psychological, social, and systemic challenges during midlife. Qualitative exploration remains limited in Brazil, particularly across diverse regions, socioeconomic groups, and healthcare pathways. MARIE Brazil WP2a therefore seeks to fill this critical void by examining how women articulate their menopausal journeys, the barriers they encounter within the healthcare system, and the strategies they employ to cope with symptoms. By foregrounding voices that are often excluded from mainstream research including women with multimorbidities, and those dependent on public services, this study adds essential depth to the evidence base. Such insights are indispensable for shaping responsive policies, strengthening clinical training, and developing equitable interventions that can support women across all stages of menopause. In doing so, MARIE Brazil WP2a contributes both to national health priorities and to the global imperative of advancing gender-sensitive health systems.
Methods
Study Design
This qualitative study formed part of the MARIE-Brazil chapter as part of work-package (WP)2-a to investigate perimenopausal, menopausal and post-menopausal experiences. The Brazilian chapter sought to explore lived experiences of menopause, with a focus on symptom trajectories, coping practices, and health system engagement. A qualitative design was chosen to capture the depth, nuance, and contextual variation in participants’ narratives that cannot be adequately addressed through quantitative surveys alone. The study followed COREQ guidelines to ensure transparency and rigour.
Research Team and Reflexivity
The study was conducted by a multidisciplinary team with expertise in women’s health, public health, qualitative research, and clinical practice. Interviews were conducted in Portuguese by trained interviewers experienced in sensitive health topics. Researchers maintained reflexive journals to document assumptions, positionality, and evolving interpretations. Reflexivity discussions were held during team meetings to mitigate bias and enhance interpretative depth.
Participant Selection and Recruitment
Participants were purposively recruited to capture variation across age, menopausal stage (peri-, natural post-, and surgical menopause), socioeconomic position, and healthcare access (public vs private). Recruitment strategies included outreach through community networks, women’s health organisations, and healthcare clinics. Eligibility criteria included: (i) self-identification as experiencing perimenopause, menopause, or post-menopause; (ii) age between 40 and 65 years; and (iii) residence in Brazil for ≥12 months. Exclusion criteria were inability to provide informed consent or language barriers precluding participation.
Setting and Data Collection
Interviews were conducted between October 2024 and December 2024 in urban and peri-urban settings across Brazil. Most interviews took place in private rooms within community centres or healthcare facilities, while some were conducted online using secure video platforms due to participant preference. Only the participant and interviewer were present. Interviews followed a semi-structured guide covering symptom experiences, coping strategies, healthcare encounters, workplace implications, and sociocultural meanings. Interviews were audio-recorded with consent and transcribed verbatim in Portuguese, with identifying information removed.
Translation and Transcription
Portuguese transcripts were first checked for accuracy by researchers. Transcripts were then translated into English for cross-site analysis, ensuring preservation of colloquial terms (e.g., calorão, pavio curto), which were documented in a bilingual glossary. Back-translation was applied to a subset of transcripts to confirm semantic fidelity. Where culturally specific terms lacked direct English equivalents, explanatory notes were added.
Data Analysis
Analysis followed Braun and Clarke’s six-phase thematic analysis, complemented by contextual analysis to situate experiences within biological, psychological, sociocultural, and health system dimensions. Coding was inductive and iterative, conducted using NVivo software. A codebook was developed collaboratively and refined across transcripts to ensure consistency. Themes were reviewed and defined through team consensus, with discrepancies resolved via discussion. Constant comparison across participants enabled identification of commonalities and divergences. Reflexivity notes were incorporated to maintain analytic transparency.
Trustworthiness and Rigour
Rigour was ensured through multiple strategies:
- Credibility: Triangulation across researchers and iterative coding discussions.
- Dependability: Maintenance of an audit trail including coding decisions, codebook (Table 1) evolution, and reflexivity logs.
- Confirmability: Peer debriefing within the research team to minimise individual bias.
- Transferability: Detailed description of participants, settings, and contexts to enable applicability to other health systems.
Ethical Considerations
Ethical approval was obtained from UNICAMP’s Research Ethics Committee under the reference number: CAAE 77391024.3.0000.5404 in Brazil and from the coordinating institution. All participants provided written informed consent prior to participation. Confidentiality was ensured through anonymisation of transcripts. Participants were informed of their right to withdraw at any point without penalty. Sensitive topics were approached with care, and referrals to support services were provided when needed. The study was conducted in accordance with the Declaration of Helsinki.
Results
The analysis generated a series of interrelated themes that captured the breadth of women’s menopausal experiences in Brazil. These themes encompassed symptom burdens, psychological impacts, coping strategies, healthcare encounters, and wider systemic inequities, each shaped by biological, sociocultural, and structural determinants. Table 2 presents the thematic framework, illustrating sub-themes, exposures, determinants, and participant quotations that anchor the findings in lived experience.
Thematic Analysis
Symptom Burden is Multidimensional and Mutually Reinforcing
Women described a clustered experience wherein vasomotor surges triggered night sweats and sleep fragmentation, which then intensified irritability, cognitive lapses, and daytime fatigue (Figure 1). GSM (vaginal dryness, burning and dyspareunia) was both highly prevalent and under-treated, with clear implications for intimacy and self-esteem. Cognitive symptoms slowed thinking, forgetfulness, task repetition were particularly salient for those in paid work, while musculoskeletal pain magnified the energy cost of daily functioning. Some women struggled to disentangle menopause from comorbid disability or surgical histories (attributional ambiguity).
“The hot flushes… my God! Horrible.” (PID7)
“I couldn’t sleep… I rolled in bed.” (PID16)
“Dryness in the vagina, pain in sex, libido zero.” (PID20)
“I had to redo tasks 3–4 times.” (PID20)
“I don’t know if it’s menopause or the amputation.” (PID1)
Psychological Impacts Pivot Around Irritability, Anxiety, and Lowered Mood
Irritability (“short fuse”), pervasive anxiety, and intermittent low mood were frequently reported even when vasomotor symptoms were modest often framed as loss of tolerance and emotional volatility. A distinct sub-theme concerned identity and ageing, with participants articulating a felt acceleration of ageing and diminished self-image that compounded demotivation.
“Short-fused… everything irritates me.” (PID12)
“I didn’t know I was so anxious until menopause.” (PID2)
“I felt I was ageing fast.” (PID18)
“I became more sad, cried easily.” (PID15)
Coping is Diverse: from Faith and Self-Care to Pharmacology and HRT Constrained by Access and Risk
Coping repertoires were broad. Faith-based practices and self-management such as exercise, meditation and therapy apps were common. This was often co-existing with psychotropic medications such as fluoxetine and duloxetine for mood, sleep or pain. HRT patches, gels, tablets, or vaginal preparations was effective where used, but contraindications such as thrombosis and fear of hormones, which were at times clinician-driven limited uptake. Several women pursued complementary therapies such as acupuncture and reiki with variable benefit.
“I read the Bible and prayed a lot.” (PID5)
“I used meditation apps and therapy.” (PID3)
“I use oestrogel and Duphaston.” (PID20)
“I couldn’t use hormones because of thrombosis.” (PID1)
“Doctors… are afraid to prescribe.” (PID13)
Care Pathways Bifurcate by Ability to Pay; Communication Quality is a Decisive Determinant of Outcomes
A stark private–public split emerged. Those with insurance or means secured specialist input and timely HRT, whereas SUS-reliant women faced delays, rushed consults, inconsistent clinicians, and little counselling. Communication gaps were acute after hysterectomy, where many received no anticipatory guidance on surgical menopause. Front-desk and nursing literacy also mattered; gatekeeping interactions could stigmatise hormone users. In the information vacuum, internet misinformation flourished, while several women explicitly requested group education and practical materials.
“I do everything private.” (PID20)
“It takes long to schedule… consults are quick.” (PID14)
“I lacked info when I had my uterus removed.” (PID8)”Receptionist asked odd questions about hormones.” (PID18)
“Why not a group for menopause?” (PID13)
Inequities are Structural, not Incidental
Participants repeatedly linked suffering to structural conditions such as resource constraints in primary care, time barriers, and the cultural invisibility of menopause at home, in clinics, and at work. Several acknowledged personal privilege, contrasting their outcomes with women who cannot pay for private care. For those in demanding jobs, the sleep–cognition–work loop produced errors, presenteeism and exhaustion, seldom buffered by formal workplace adaptations.
“If you don’t have money, it’s complicated.” (PID9)
“In my mother’s time nobody spoke [about menopause].” (PID8)
“I had to redo tasks 3–4 times.” (PID20)
Contextual Analysis
The Brazilian narratives reveal menopause as a constellation of interlocking disruptions, where vasomotor episodes, genitourinary syndrome of menopause (GSM), sleep disturbance, cognitive lapses and musculoskeletal pain converged to erode daily functioning. These symptoms did not act in isolation as night sweats fractured sleep, fragmented sleep fuelled irritability, and cumulative fatigue undermined concentration and mood, producing a cycle of depletion. Surgical menopause compounded this burden, with hysterectomised women reporting particularly severe GSM, while the presence of multimorbidity osteoporosis, diabetes, thromboembolism and disability magnified vulnerability and complexity.
Psychological strain was equally pervasive. Irritability and anxiety were intensified by disrupted sleep and workplace pressures, while demotivation and the pervasive sense of “accelerated ageing” undermined self-efficacy. Psychotropic prescriptions were common, but often addressed chronic anxiety and insomnia rather than menopause-specific drivers such as duloxetine for anxiety and pain reflecting a system that managed symptoms without recognising their hormonal origins.
Against this backdrop, cultural scripts of silence and shame restricted open discussion, curtailing help-seeking and perpetuating stigma. Faith-based coping was an important resource for some, yet sexual wellbeing was often compromised by dryness, pain, and loss of desire with misunderstandings from partners compounding distress (PID5). Women’s idiomatic language—“inferno”, “calorão”, “pavio curto”—conveyed the visceral intensity of symptoms and the subjective toll of a largely invisible condition.
The health system context further entrenched inequities. The ability to pay dictated access to specialists and HRT, leaving those reliant on SUS facing time constraints, clinician uncertainty, front-desk gatekeeping, and a conspicuous absence of post-surgical counselling. In response, participants articulated pragmatic solutions, calling for group education and genuinely multidisciplinary care models incorporating nursing, physiotherapy and mental health expertise.
The sleep–cognition–performance cascade emerged as a defining occupational hazard: women described forgetting tasks, repeating work, and struggling to maintain accuracy under fatigue. Yet formal workplace adjustments were almost entirely absent. Instead, women absorbed the burden themselves through pacing, repetition, and improvised breaks, a tacit expectation that menopause should be endured rather than supported.
Colloquial Terms Table (English- Portuguese, as Used by Participants)
Colloquial terms foreground intensity and lived salience is an important aspect to consider as indicated in Table-3: calorão and inferno convey not just heat but suffering. Emotional states are socialised through idioms—pavio curto and ficar brava por qualquer coisa—that map irritability onto everyday interactions. Sexual health language—secura, ardência, libido zero—is direct yet stigmatised, underscoring the need for sensitive counselling. Health-system slang—postinho, SUS, convênio—encodes structural pathways and classed access. Incorporating these terms into educational materials can validate experience, reduce shame, and improve message uptake.

Table 3.
Colloquialisms capture intensity, nuance and cultural meaning beyond literal translation. Below are near-equivalents used to interpret participants’ narratives and to inform culturally attuned communication materials.
Table 3.
Colloquialisms capture intensity, nuance and cultural meaning beyond literal translation. Below are near-equivalents used to interpret participants’ narratives and to inform culturally attuned communication materials.
| English | Portuguese (colloquial) |
| Hot flush / heat wave | Calorão / onda de calor |
| Night sweats | Suor noturno |
| Vaginal dryness | Secura (na vagina) / ressecamento |
| Burning (vaginal) | Ardência |
| Painful sex | Dor na relação / doía para ter relação |
| No libido | Libido zero / sem vontade |
| Short fuse / easily irritated | Pavio curto |
| Angry at anything | Ficar brava por qualquer coisa |
| Brain fog / slow thinking | Cabeça lenta |
| Forgetful | Memória falha / esquecida |
| Tiredness / fatigue | Canseira / cansaço |
| Feeling old | Me sentindo velha / envelhecendo rápido |
| Hellish experience | Inferno |
| Primary care clinic | Postinho / UBS |
| Public system | SUS |
| Private insurance | Convênio |
| Reception/front-desk | Recepção |
| Compounded cream | Remédio manipulado |
| Testosterone gel | Gel de testosterona |
| Combined pill (brand) | Ceci |
| HRT patch/gel | Adesivo/gel de hormônio |
Discussion
This study highlights that menopause in Brazil is experienced as a multifactorial transition shaped by intersecting biological, psychological, socio-cultural, and systemic determinants. Women reported the well-documented burden of vasomotor symptoms, urogenital atrophy, musculoskeletal pain, cognitive decline, and mood changes, yet these manifestations were intensified by broader inequities. Fragmented care pathways, limited health professional knowledge, and financial inaccessibility of HRT or alternatives exacerbated distress. The findings also illuminate how stigma, cultural silence around reproductive ageing, and gendered workplace dynamics contribute to concealment of symptoms and social isolation. Importantly, participants’ narratives suggest that resilience was often derived from informal networks, such as family and peer support, rather than from formal healthcare services. Collectively, the study underscores that menopause in Brazil cannot be understood through a purely biomedical lens; it is shaped by socio-economic stratification, cultural expectations, and health system limitations.
Population Science
The insights generated from this study hold profound implications for population health in Brazil. The country faces an epidemiological transition with rapid population ageing: by 2030, one in four Brazilian women will be over 50. The scale of menopause-related needs therefore intersects with the broader pressures on Brazil’s Unified Health System (SUS), including the rising prevalence of non-communicable diseases (NCDs) such as diabetes and cardiovascular disease. These conditions are clinically intertwined with menopausal biology and symptom burden. The qualitative evidence demonstrates that marginalised women, particularly those in low-income, rural, or racially minoritised groups experience disproportionately greater barriers to care. This reflects broader structural inequities, including regional disparities in healthcare infrastructure, limited access to gynaecological specialists outside major urban centres, and inconsistent dissemination of public health information. Stigma and cultural silence exacerbate under-recognition of symptoms, perpetuating the invisibility of menopause within population health policy. From a population science perspective, menopause must therefore be reframed as a public health priority: an issue that intersects with women’s labour force participation, mental health, and quality of life across decades. Without systemic recognition, the cumulative social and economic burden of untreated menopausal symptoms may be substantial, undermining Brazil’s progress towards gender equity and sustainable development goals.
Clinical Implications
From a clinical standpoint, the study exposes critical gaps in menopause care within Brazil, while also identifying opportunities for practice reform. Current approaches remain fragmented: while some tertiary centres and private clinics offer specialist menopause services, access is uneven and largely dependent on financial capacity. In contrast, the majority of women in the public system rely on general practitioners or gynaecologists who may lack specific training in menopausal care. This aligns with prior evidence demonstrating that SUS lacks consistent protocols for screening, counselling, and treatment of menopause, and that HRT prescribing is hindered by misconceptions about safety, inconsistent availability, and clinician hesitancy. For example, studies in São Paulo and Rio de Janeiro, report low prescription rates of HRT, often restricted to urban middle-class populations with private insurance, while women in rural North and Northeast regions face limited options altogether [19,20,21,22].
International guidelines including those from the North American Menopause Society (NAMS) and the International Menopause Society (IMS) recommend a personalised, evidence-based approach to HRT, considering risk factors, comorbidities, and patient preferences [23,24]. In Brazil, however, clinical practice often defaults to symptomatic management such as analgesics or antidepressants or fragmented gynaecological follow-up, which may not adequately address the multidimensional impact of menopause. The study’s findings demonstrate the psychological and occupational toll of untreated symptoms, pointing to the need for multidisciplinary models of care that integrate mental health, primary care, and specialist input. The socio-cultural dimension, particularly stigma and silence demands greater clinical sensitivity and training in communication, enabling clinicians to ask about symptoms proactively.
Evidence from other middle-income contexts suggests that task-shifting strategies, such as equipping community health workers to deliver basic counselling, could help bridge gaps in access [25]. Brazil’s extensive Family Health Strategy network offers a potential platform to embed menopause education, screening, and referral pathways at the community level [26]. However, such integration requires investment in training, alongside public health campaigns to normalise menopause as a legitimate health concern. Pharmacological options must also be expanded: equitable access to safe, affordable HRT through SUS is critical, alongside non-hormonal alternatives for women with contraindications.
Critically, the study illustrates that informal coping mechanisms peer networks, family support, and digital communities are compensating for formal system shortcomings. Clinical practice in Brazil must evolve to recognise and build upon these strengths, for example, by facilitating group consultations, peer support programmes, or digital health tools co-designed with women themselves. Without such reforms, the clinical management of menopause risks perpetuating inequities and failing to meet the needs of a growing segment of Brazil’s population. Based on the insights gathered, we propose the following recommendations;
| Domain | Policy Recommendations |
| Health system strengthening | • Integrate menopause into Brazil’s Unified Health System (SUS) through standardised screening, counselling, and management protocols.• Establish multidisciplinary menopause clinics in specialized public care centers and leverage the Family Health Strategy for community support. |
| Equitable access to treatment | • Guarantee the availability of affordable hormone replacement therapy (HRT) and non-hormonal alternatives through SUS, reducing urban–rural and public–private disparities.• Implement bulk procurement and subsidy mechanisms to ensure cost-effectiveness and sustainability. |
| Clinical training and education | • Introduce mandatory menopause education in medical and nursing curricula, with ongoing continuing professional development for general practitioners and gynaecologists.• Equip community health workers with training to deliver basic counselling, early recognition, and referral. |
| Public health communication | • Launch culturally tailored campaigns to reduce stigma and normalise open discussion of menopause.• Use different tools, including non-digital ones when necessary to facilitate accessibility. |
| Workplace and societal policy | • Promote workplace protections through national labour regulations, ensuring flexibility, reasonable adjustments, and anti-discrimination safeguards.• Incorporate menopause into gender equity and aging strategies to align with Brazil’s commitments to the Sustainable Development Goals, facilitating a more prolonged incorporation of women into the labor market |
Conclusion
Menopause in Brazil is shaped by complex intersections of biology, culture, socio-economic position, and health system capacity. Women’s experiences highlight persistent inequities in recognition, access, and management, with informal networks often compensating for gaps in formal care. Addressing these challenges requires health system strengthening, clinician training, equitable access to therapies, and culturally sensitive public health communication. Embedding menopause within Brazil’s broader population health and policy agendas is essential to advance equity and improve quality of life for millions of women.
Author Contributions
GD developed the ELEMI program and the MARIE project. This was furthered by GD and PP. CBP submitted and secured the ethics approval for the study in Brazil. CBP, RMN and DAY collected data. GD and JQS conducted the data analysis. GD wrote the first draft and was furthered CPB and by all other authors. All authors critically appraised, reviewed and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Funding
No funding.
Availability of data and material
The PIs and the study sponsor may consider sharing anonymous data upon reasonable a request.
Code availability
Not applicable.
Ethics approval
This research was approved by the institution’s Research Ethics Committee under the number: CAAE 77391024.3.0000.5404.
Consent to participate
Obtained.
Consent for publication
All authors consented to publish this manuscript.
Acknowledgments
MARIE Consortium: Donatella Fontana, Aini Hanan binti Azmi, Alyani binti Mohamad Mohsin, Arinze Anthony Onwuegbuna, Artini binti Abidin, Ayyuba Rabiu, Chijioke Chimbo, Chinedu Onwuka Ndukwe, Choon-Moy Ho, Chinyere Ukamaka Onubogu, Diana Chin-Lau Suk, Divinefavour Echezona Malachy, Emmanuel Chukwubuikem Egwuatu, Eunice Yien-Mei Sim, Farhawa binti Zamri, Fatin Imtithal binti Adnan, Geok-Sim Lim, Halima Bashir Muhammad, Ifeoma Bessie Enweani-Nwokelo, Ikechukwu Innocent Mbachu, Jinn-Yinn Phang, John Yen-Sing Lee, Joseph Ifeanyichukwu Ikechebelu, Juhaida binti Jaafar, Karen Christelle, Kathryn Elliot, Kim-Yen Lee, Kingsley Chidiebere Nwaogu, Lee-Leong Wong, Lydia Ijeoma Eleje, Min-Huang Ngu, Noorhazliza binti Abdul Patah, Nor Fareshah binti Mohd Nasir, Norhazura binti Hamdan, Nnanyelugo Chima Ezeora, Nnaedozie Paul Obiegbu, Nurfauzani binti Ibrahim, Nurul Amalina Jaafar, Odigonma Zinobia Ikpeze, Obinna Kenneth Nnabuchi, Pooja Lama, Puong-Rui Lau, Rakshya Parajuli, Rakesh Swarnakar, Raphael Ugochukwu Chikezie, Rosdina Abd Kahar, Safilah Binti Dahian, Sapana Amatya, Sing-Yew Ting, Siti Nurul Aiman, Sunday Onyemaechi Oriji, Susan Chen-Ling Lo, Sylvester Onuegbunam Nweze, Damayanthi Dassanayake, Nimesha Wijayamuni, Prasanna Herath, Thamudi Sundarapperuma, Vaitheswariy Rao, Xin-Sheng Wong, Xiu-Sing Wong, Yee-Theng Lau, Heitor Cavalini, Jean Pierre Gafaranga, Emmanuel Habimana, Chigozie Geoffrey Okafor, Assumpta Chiemeka Osunkwo, Gabriel Chidera Edeh, Esther Ogechi John, Kenechukwu Ezekwesili Obi, Oludolamu Oluyemesi Adedayo, Odili Aloysius Okoye, Chukwuemeka Chukwubuikem Okoro, Ugoy Sonia Ogbonna, Chinelo Onuegbuna Okoye, Babatunde Rufus Kumuyi, Onyebuchi Lynda Ngozi, Nnenna Josephine Egbonnaji, Oluwasegun Ajala Akanni, Perpetua Kelechi Enyinna, Yusuf Alfa, Theresa Nneoma Otis, Catherine Larko Narh Menka, Kwasi Eba Polley, Isaac Lartey Narh, Bernard B. Borteih, Andy Fairclough, Kingsley Emeka Ekwuazi, Michael Nnaa Otis, Jeremy Van Vlymen, Chidiebere Agbo, Francis Chibuike Anigwe, Kingsley Chukwuebuka Agu, Chiamaka Perpetua Chidozie, Chidimma Judith Anyaeche, Clementine Kanazayire, Jean Damascene Hanyurwimfura, Nwankwo Helen Chinwe, Stella Matutina Isingizwe, Jean Marie Vianney Kabutare, Dorcas Uwimpuhwe, Melanie Maombi, Ange Kantarama, Uchechukwu Kevin Nwanna, Benedict Erhite Amalimeh, Theodomir Sebazungu, Elius Tuyisenge, Yvonne Delphine Nsaba Uwera, Emmanuel Habimana, Nasiru Sani, Amarachi Pearl Nkemdirim, Rukshini Puvanendram, Manisha Mathur, Rajeswari Kathirvel, Farah Safdar, Raksha Aiyappan, Jean Pierre Gafaranga, Bertin Ngororano, Victor Archibon, Ibe Michael Usman, Baraka Godfrey Mwahi, Filbert Francis Ilaza, Zepherine Pembe, Clement Mwabenga, Mpoki Kaminyoghe, Brenda Mdoligo, Thomas Alone Saida, Nicodemus E. Mwampashi, Olisaemeka Nnaedozie Okonkwo, Bethel Chinonso Okemeziem, Bethel Nnaemeka Uwakwe, Goodnews Ozioma Igboabuchi, Ifeoma Francisca Ndubuisi.
Conflicts of interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
References
- Thurston, R. C., Thomas, H. N., Castle, A. J. & Gibson, C. J. Menopause as a biological and psychological transition. Nature Reviews Psychology, 1-14 (2025).
- Costa, C. R. N. d., Costa, N. C. V. & Manica, D. T. Menstruation as a research topic in the humanities in Brazil: a state of the art. Tapuya: Latin American Science, Technology and Society 7, 2424097 (2024).
- Delanerolle, G. et al. Menopause: a global health and wellbeing issue that needs urgent attention. The Lancet Global Health 13, e196-e198 (2025).
- Lay, A. A. R., do Nascimento, C. F., de Oliveira Duarte, Y. A. & Chiavegatto Filho, A. D. P. Age at natural menopause and mortality: a survival analysis of elderly residents of São Paulo, Brazil. Maturitas 117, 29-33 (2018).
- Lay, A. A. R., de Oliveira Duarte, Y. A. & Chiavegatto Filho, A. D. P. Factors associated with age at natural menopause among elderly women in São Paulo, Brazil. Menopause 26, 211-216 (2019).
- Ygnatios, N. T. M. et al. Age at natural menopause and its associated characteristics among Brazilian women: cross-sectional results from ELSI-Brazil. Menopause 31, 693-701 (2024).
- Pompei, L. M. et al. Profile of Brazilian climacteric women: results from the Brazilian Menopause Study. Climacteric 25, 523-529 (2022).
- Afonso, L. O. et al. Prevalence of hysterectomy and associated factors in Brazilian women aged 50 and older: findings from the Brazilian Longitudinal Study of Ageing (ELSI-Brazil). BMC Public Health 24, 1747 (2024).
- Bagga, S. S., Tayade, S., Lohiya, N., Tyagi, A. & Chauhan, A. Menopause dynamics: From symptoms to quality of life, unraveling the complexities of the hormonal shift. Multidisciplinary Reviews 8, 2025057-2025057 (2025).
- Carvalho, A. O. d., Andrade, L. B. d., Ruano, F. F. L., Wigg, C. M. D. & Marinheiro, L. P. F. Knowledge, practices and barriers to access sexual health of women in the menopausal stages: a cross-sectional study with Brazilian gynecologists. BMC Women’s Health 24, 52 (2024).
- Da Silva, A. R. & Tanaka, A. C. d. A. Factors associated with menopausal symptom severity in middle-aged Brazilian women from the Brazilian Western Amazon. Maturitas 76, 64-69 (2013).
- Bilal, U. et al. Inequalities in life expectancy in six large Latin American cities from the SALURBAL study: an ecological analysis. The lancet planetary health 3, e503-e510 (2019).
- Tserotas, K. & Blumel, J. E. REDLINC: two decades of collaborative insights into menopause and women’s health in Latin America. Climacteric, 1-10 (2025).
- Connelly, R., DeGraff, D. S. & Levison, D. Women’s employment and child care in Brazil. Economic development and cultural change 44, 619-656 (1996).
- Bahiyah Abdullah, M., Moize, B., Ismail, B. A. & Zamri, M. Prevalence of menopausal symptoms, its effect to quality of life among Malaysian women and their treatment seeking behaviour. Med J Malaysia 72, 95 (2017).
- Manoharan, A. et al. Health-seeking behaviors and treatments received for menopause symptoms: a questionnaire survey among midlife women attending primary healthcare clinics in Malaysia. Journal of Menopausal Medicine 29, 119 (2023).
- Laker, B. & Rowson, T. Making the invisible visible: why menopause is a workplace issue we can’t ignore. BMJ leader (2024).
- Li, Q., Gu, J., Huang, J., Zhao, P. & Luo, C. “ They see me as mentally ill”: the stigmatization experiences of Chinese menopausal women in the family. BMC Women’s Health 23, 185 (2023).
- Pinto Neto, A. M. et al. Caracterização das usuárias de terapia de reposição hormonal do Município de Campinas, São Paulo. Cadernos de Saúde Pública 18, 121-127 (2002).
- de Arruda Amaral, I. C. et al. Factors associated with knowledge about menopause and hormone therapy in middle-aged Brazilian women: a population-based household survey. Menopause 25, 803-810 (2018).
- Augusto, R. M., Oliveira, D. C. d. & Polidoro, M. Description of drugs prescribed for hormone therapy in specialized health services for transsexual and transvestite persons in Rio Grande do Sul, Brazil, 2020. Epidemiologia e Serviços de Saúde 31, e2021502 (2022).
- Ferreira-Campos, L. et al. Hormone therapy and hypertension in postmenopausal women: results from the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Arquivos Brasileiros de Cardiologia 118, 905-913 (2022).
- Panay, N. et al. Menopause and MHT in 2024: addressing the key controversies–an International Menopause Society White Paper. South African General Practitioner 5, 119-134 (2024).
- Faubion, S. S. et al. The 2022 hormone therapy position statement of the North American Menopause Society. Menopause 29, 767-794 (2022).
- Low, T. L., Cheong, A. T., Devaraj, N. K. & Ismail, R. Prevalence of offering menopause hormone therapy among primary care doctors and its associated factors: A cross-sectional study. PLoS One 19, e0310994 (2024).
- Macinko, J. & Harris, M. J. Brazil’s family health strategy—delivering community-based primary care in a universal health system. New England Journal of Medicine 372, 2177-2181 (2015).
Figure 1.
Thematic bubble map based on identified themes and sub-themes identified from the sample.
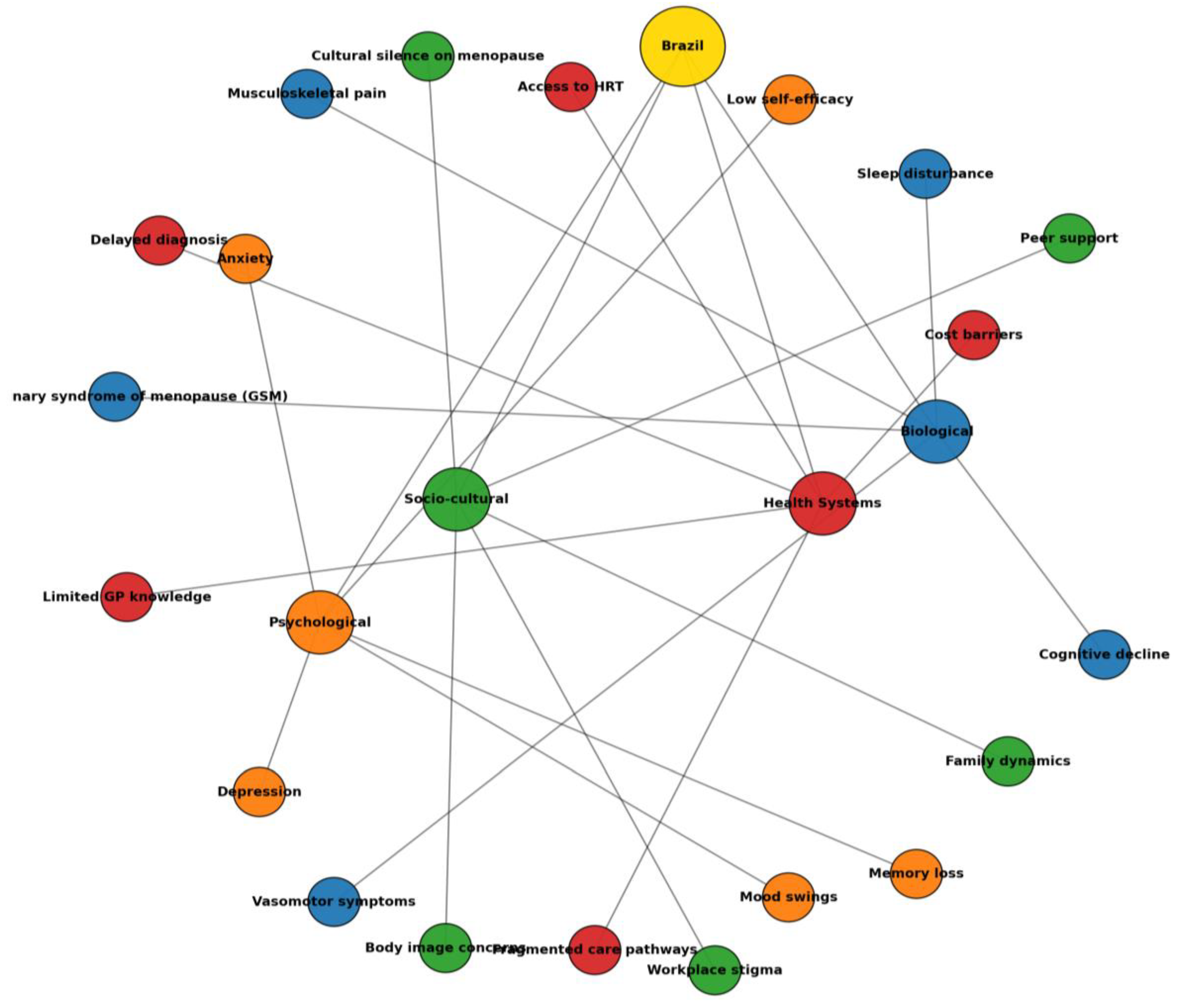
Table 1.
Codebook developed for the purpose of the analysis. This codebook was developed inductively from qualitative interviews with participants in the MARIE Brazil study (PID1–20). It catalogues the main codes identified, with accompanying definitions, determinants, illustrative quotes, and thematic allocation. Codes reflect multiple levels of influence, including biological (e.g., vasomotor episodes, GSM, sleep disruption), psychological (e.g., irritability, anxiety, low mood), socio-cultural (e.g., faith-based coping, cultural silence, colloquial idioms), and health system determinants (e.g., private vs SUS reliance, clinician reluctance, misinformation). The structure demonstrates how symptom experiences were situated within broader contexts of comorbidity, healthcare access, and inequity. This framework provides transparency to the analytic process, ensures reproducibility, and facilitates transferability of findings across settings.
Table 1.
Codebook developed for the purpose of the analysis. This codebook was developed inductively from qualitative interviews with participants in the MARIE Brazil study (PID1–20). It catalogues the main codes identified, with accompanying definitions, determinants, illustrative quotes, and thematic allocation. Codes reflect multiple levels of influence, including biological (e.g., vasomotor episodes, GSM, sleep disruption), psychological (e.g., irritability, anxiety, low mood), socio-cultural (e.g., faith-based coping, cultural silence, colloquial idioms), and health system determinants (e.g., private vs SUS reliance, clinician reluctance, misinformation). The structure demonstrates how symptom experiences were situated within broader contexts of comorbidity, healthcare access, and inequity. This framework provides transparency to the analytic process, ensures reproducibility, and facilitates transferability of findings across settings.
| Code | Definition | Determinant(s) | Example Quote (PID) | Theme |
| Hot flushes / calorão | Sudden intense heat, often with sweating | Hormonal decline | “The hot flushes… my God! Horrible.” (PID7) | Symptom burden – vasomotor |
| Night sweats | Nocturnal sweating disrupting sleep | Vasomotor instability | “I woke up drenched, bed wet.”(PID4) | Symptom burden – vasomotor |
| Insomnia | Difficulty initiating/maintaining sleep | Vasomotor symptoms, anxiety | “I couldn’t sleep… I rolled in bed.”(PID16) | Symptom burden – sleep |
| Fragmented sleep | Multiple awakenings, unrefreshing sleep | Anxiety, night sweats | “I woke up and couldn’t sleep again.” (PID20) | Symptom burden – sleep |
| Vaginal dryness / secura | Reduced lubrication, painful sex | Oestrogen decline, hysterectomy | “Dryness in the vagina, pain in sex, libido zero.” (PID20) | Symptom burden – GSM |
| Painful sex / dor na relação | Dyspareunia linked to dryness | GSM | “Very dry… pain during sex.”(PID18) | Symptom burden – GSM |
| Recurrent UTIs | Frequent urinary infections | Oestrogen deficiency, GSM | “I get infections almost every month.” (PID8) | Symptom burden – GSM |
| Libido loss / libido zero | Diminished sexual desire | GSM, mood changes | “No desire for sex, libido gone.”(PID7, PID5) | Symptom burden – GSM |
| Memory lapses | Forgetting tasks, poor recall | Menopause, sleep loss | “I forgot many things.” (PID11) | Symptom burden – cognitive |
| Concentration difficulties | Reduced focus, task repetition | Fatigue, insomnia | “I had to redo tasks 3–4 times.”(PID20) | Symptom burden – cognitive |
| Brain fog / cabeça lenta | Slowed mental processing | Sleep loss, hormonal changes | “It seemed like my head was slow.”(PID4) | Symptom burden – cognitive |
| Back pain | Chronic lumbar pain | Osteoporosis, disability | “My back always hurts.” (PID3) | Symptom burden – musculoskeletal |
| Joint pain / knee/spine issues | Musculoskeletal complaints | Chronic illness | “Many spine problems, knee surgery.” (PID2) | Symptom burden – musculoskeletal |
| Weight gain | Noticeable post-menopause weight increase | Hormonal, lifestyle | “I gained a lot of weight after menopause.” (PID1) | Symptom burden – body image |
| Attributional ambiguity | Difficulty separating menopause from comorbidities | Disability, surgery | “I don’t know if it’s menopause or the amputation.” (PID1) | Symptom burden |
| Irritability / pavio curto | Short temper, easy frustration | Hormonal, sleep loss | “Short-fused… everything irritates me.” (PID12) | Psychological impact |
| Anxiety / nervosismo | Heightened worry, nervousness | Pre-existing or menopause-triggered | “I didn’t know I was so anxious until menopause.” (PID2) | Psychological impact |
| Low mood / sadness | Emotional downturn, crying, demotivation | Hormonal, occupational stress | “I became more sad, cried easily.”(PID15) | Psychological impact |
| Accelerated ageing | Feeling older, diminished identity | Cultural scripts | “I felt I was ageing fast.” (PID18) | Psychological impact |
| Faith-based coping | Reliance on prayer, Bible | Religious orientation | “I read the Bible and prayed a lot.”(PID5) | Coping |
| Self-care routines | Exercise, meditation, therapy apps | Individual agency | “I used meditation apps.” (PID3) | Coping |
| Psychotropic use | Antidepressants/anxiolytics | Anxiety, depression, pain | “I take fluoxetine.” (PID20); “Duloxetine for anxiety and pain.”(PID2) | Coping |
| HRT use | Hormone replacement therapy (gel, patch, tablet) | Private access, physician | “I use oestrogel and Duphaston.”(PID20) | Coping |
| HRT contraindication | Unable to use HRT | Thrombosis, risk factors | “I couldn’t use hormones because of thrombosis.” (PID1) | Coping |
| Clinician reluctance | Doctors avoid prescribing | Fear of side effects | “Doctors are afraid to prescribe.”(PID13) | Healthcare |
| Complementary therapies | Acupuncture, reiki, homeopathy | Cultural adaptation | “I tried acupuncture and reiki.”(PID2) | Coping |
| Private care reliance | Access via insurance/self-pay | Socioeconomic privilege | “I do everything private.” (PID20) | Healthcare access |
| SUS reliance | Dependence on public system | Socioeconomic constraint | “I do everything through SUS.”(PID1) | Healthcare access |
| Appointment delays | Long waits, quick consults | Under-resourcing | “It takes long to schedule, consults are quick.” (PID14) | Healthcare access |
| Doctor turnover | Lack of continuity | Workforce instability | “Hard to trust; depends on who you get.” (PID17) | Healthcare access |
| Post-surgical counselling gaps | No menopause briefing post-hysterectomy | Peri-operative care | “I lacked info when I had my uterus removed.” (PID8) | Healthcare access |
| Front-desk gatekeeping | Receptionist/nurse ignorance | System literacy gap | “Receptionist asked odd questions about hormones.” (PID18) | Healthcare access |
| Misinformation online | Confusion from internet | Information desert | “On the internet it’s worse… everyone says different.” (PID13) | Healthcare access |
| Education demand | Desire for group sessions/resources | Community-based support | “Why not a group for menopause?”(PID13) | Healthcare access |
| Equity/ability to pay | Paying vs relying on SUS determines care | Structural inequity | “If you don’t have money, it’s complicated.” (PID9) | Systemic inequity |
| Cultural silence | Generational non-discussion | Social norms | “In my mother’s time nobody spoke.” (PID8) | Systemic inequity |
| Occupational impact | Errors, fatigue, presenteeism | Sleep/cognition loop | “I had to redo tasks 3–4 times.”(PID20) | Systemic inequity |
Table 2.
Themes, sub-themes, determinants, exposures and example quotes of the sample.
| Theme | Sub-theme | Determinants | Exposures (what happened) | Example quote (PID) |
| Symptom burden | Vasomotor intensity & cyclicity | Oestrogen decline | Hot flushes, night sweats, daytime sweating cycles | “The hot flushes… my God! Horrible.” (PID7) |
| Sleep fragmentation & non-restorative sleep | Vasomotor activation; anxiety | Difficulty initiating sleep, multiple awakenings, unrefreshing sleep | “I couldn’t sleep… I rolled in bed.” (PID16) | |
| Genitourinary syndrome of menopause (GSM) | Oestrogen depletion; surgical menopause | Vaginal dryness, burning, dyspareunia, urinary discomfort/UTIs | “Very dry… pain during sex.” (PID18); “Frequent infections, almost every month.” (PID8) | |
| Sexual function & desire | GSM; mood; relationship context | Low libido, avoidance of sex, partner misunderstanding | “Libido zero.” (PID20); “My ex-husband didn’t understand.” (PID5) | |
| Cognitive efficiency | Menopausal transition; sleep loss | Forgetfulness; slowed processing; reduced concentration; task repetition | “I had to redo tasks 3–4 times.” (PID20); “I forgot many things.” (PID11) | |
| Musculoskeletal pain & fatigue | Osteoporosis; disability; comorbid pain | Back pain; joint pain; daytime fatigue | “My back always hurts.”(PID3) | |
| Weight & body image | Hormonal milieu; mood; activity | Weight gain; altered self-image | “I gained a lot of weight after menopause.” (PID1) | |
| Attributional ambiguity | Multimorbidity; surgical history | Difficulty separating effects of disability/surgery vs menopause | “I don’t know if it’s menopause or the amputation.” (PID1) | |
| Psychological impacts | Irritability & “short fuse” | Hormonal shifts; poor sleep | Lower tolerance, proneness to anger | “Short-fused… everything irritates me.” (PID12) |
| Anxiety amplification | Pre-existing anxiety; transition stressors | Persistent nervousness, hyper-arousal | “I didn’t know I was so anxious until menopause.”(PID2) | |
| Low mood & demotivation | Chronic symptoms; role strain | Sadness, crying, loss of drive | “I became more sad, cried easily.” (PID15) | |
| Identity/ageing sense-making | Social narratives of ageing | Feeling “old”, accelerated ageing | “I felt I was ageing fast.”(PID18) | |
| Coping & management | Faith-based coping | Religious orientation; community | Prayer, Bible reading, meaning-making | “I read the Bible and prayed a lot.” (PID5) |
| Self-care routines | Individual agency; digital access | Exercise, meditation, therapy apps; vitamins | “I used meditation apps and therapy.” (PID3) | |
| Psychotropics | Access; comorbidity | Antidepressants/anxiolytics for mood, sleep, pain | “I take fluoxetine.” (PID20); “Duloxetine for anxiety and pain.” (PID2) | |
| HRT access & effects | Private vs SUS; safety perceptions | Patches/gels/tablets; vaginal oestrogens; symptom relief | “Oestrogel and Duphaston helped.” (PID20) | |
| HRT constraints/contraindications | Thrombosis history; risk perceptions | Non-use despite need; under-prescribing | “I couldn’t use hormones because of thrombosis.”(PID1); “Doctors are afraid to prescribe.” (PID13) | |
| Complementary therapies | Cultural acceptability | Acupuncture, homeopathy, reiki | “I tried acupuncture and reiki.” (PID2) | |
| Workplace self-adaptation | Role autonomy; support | Task pacing, error checking, breaks | “I had to redo tasks several times.” (PID20) | |
| Healthcare access & communication | Private care reliance | Socioeconomic privilege | Direct gynaecology access; steady HRT | “I do everything private.”(PID20) |
| SUS reliance (UBS) pathways | Socioeconomic constraint | Family doctor triage; variable follow-up | “I do everything through SUS.” (PID1) | |
| Appointment logistics & time | Under-resourcing | Delays, rushed consults, scheduling difficulty | “It takes long to schedule… consults are quick.” (PID14) | |
| Continuity/turnover (“doctor shopping”) | Staffing; contracts | Repeating history, inconsistent advice | “It’s hard to trust; depends on who you get.” (PID17) | |
| Post-surgical counselling gaps | Peri-operative education | Hysterectomy without menopause briefing | “I lacked info when I had my uterus removed.” (PID8) | |
| Gatekeeping & staff literacy | Non-clinical staff; stigma | Receptionist/nurse questioning, embarrassment | “Receptionist asked odd questions about hormones.”(PID18) | |
| Misinformation & info deserts | Internet noise; absent materials | Conflicting guidance; fear of hormones | “On the internet it’s worse… everyone says different.”(PID13) | |
| Demand for education & groups | Community models | Desire for group classes/resources | “Why not a group for menopause?” (PID13) | |
| Systemic inequities | Ability to pay = quality of care | Income; insurance | Private/HRT vs public/limited options | “If you don’t have money, it’s complicated.” (PID9) |
| Cultural silence & stigma | Norms; generational gaps | Menopause invisible in families/work | “In my mother’s time nobody spoke.” (PID8) | |
| Occupational consequences | Sleep/cognition; supports | Errors, fatigue, presenteeism | “I had to redo tasks 3–4 times.” (PID20) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



