
Submitted:
24 October 2025
Posted:
27 October 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
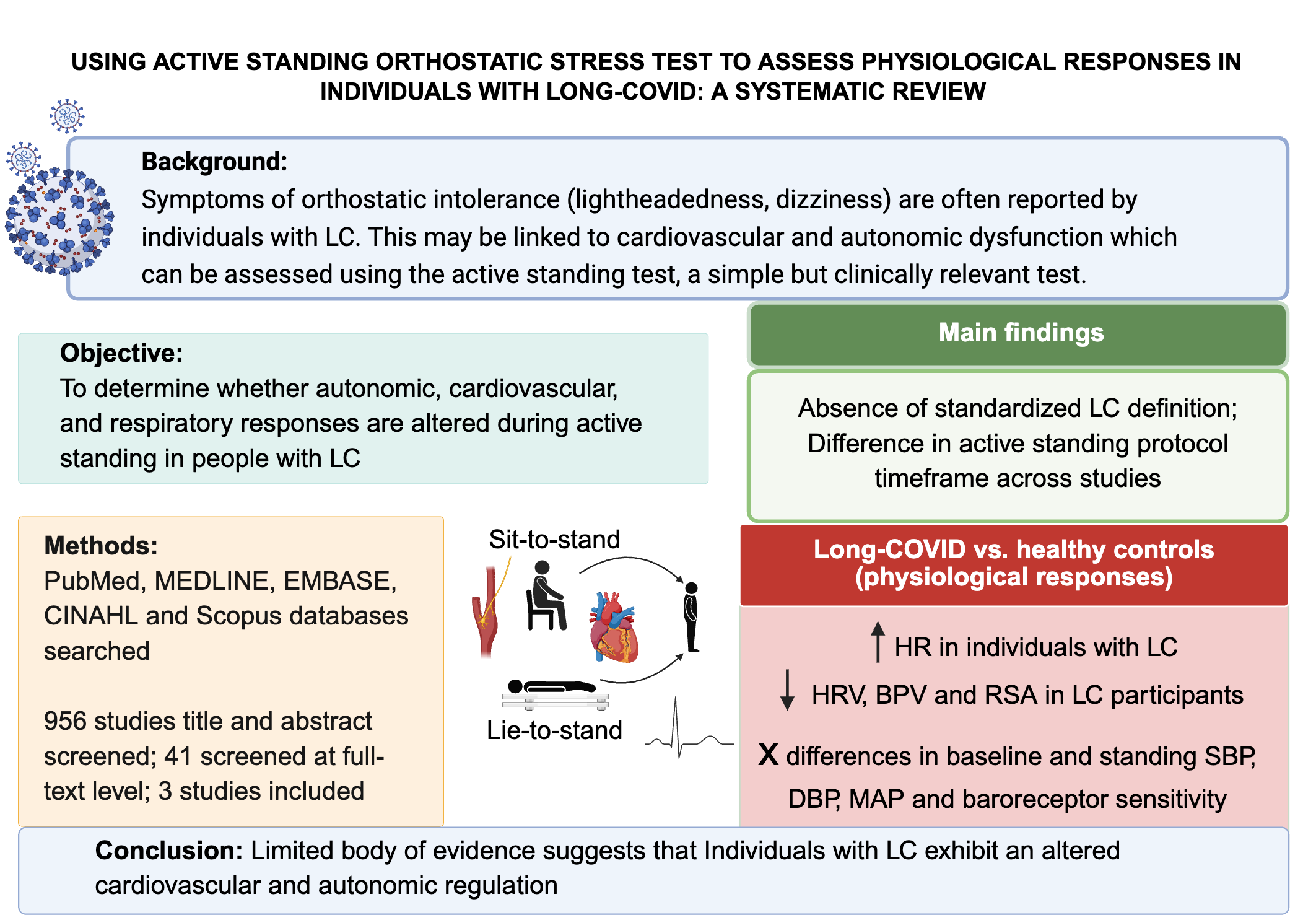
Background/Objective: Individuals experiencing long-COVID frequently report or-thostatic intolerance symptoms, which may be linked to autonomic and cardiovascular dysfunction. The active standing test provides a simple, clinically relevant means to assess these impairments. This systematic review aims to determine the use of the ac-tive standing orthostatic stress test in evaluating cardiovascular, autonomic, and res-piratory responses in people experiencing LC. Methods: A systematic search, accord-ing to PRISMA guidelines, was conducted in PubMed, MEDLINE, EMBASE, CINAHL, and Scopus for articles published between 2020 and 2025. This study was registered in PROSPERO CRD-42024615872. Studies were included if they used the active standing test, enrolled adults (≥18 years), included both Long-COVID and healthy control groups, used continuous beat-to-beat measurements, and reported physiological out-comes. Risk of bias was assessed using the nine-point Newcastle-Ottawa-Scale. Re-sults: Three studies (216 participants with Long-COVID and 186 controls) met the in-clusion criteria. Across studies, Long-COVID individuals consistently exhibited ele-vated heart rate in both supine and standing positions. However, blood pressure find-ings were more variable: only one study reported 13% of participants met orthostatic hypotension criteria, while another found significant increases in diastolic blood pres-sure during standing. Long-COVID groups also showed reduced heart rate variability compared to controls. Conclusions: Individuals experiencing Long-COVID show ele-vated heart rate and impaired autonomic function during active standing, with sub-group-specific blood pressure changes. These alterations may contribute to dizziness, fatigue, and reduced activity tolerance. Incorporating active standing into clinical as-sessment could aid early identification of autonomic dysfunction and inform rehabili-tation strategies, though more research is urgently needed.
Keywords:
long-COVID
; orthostatic stress
; active standing test
; autonomic responses
; cardiovascular responses
; orthostatic hypotension
; orthostatic intolerance
1. Introduction
Long-COVID, also called post-acute sequelae of COVID-19, post-COVID-19 condition, or chronic COVID syndrome, is when new, ongoing, or worsening symptoms last for three months or more after the severe-acute respiratory syndrome coronavirus infection and cannot be explained by other health problems [1,2]. Common issues include dizziness when standing, fatigue, breathlessness, and “brain fog,” which together can greatly affect daily activities and quality of life [3]. A systematic review reported that nearly 38% of people experienced ongoing fatigue, and more than half had reduced quality of life three to six months after infection [4].
A frequent problem in long-COVID (LC) is difficulty remaining upright, known as orthostatic intolerance [5,6]. This occurs when the body struggles to adjust to standing, leading to dizziness, light-headedness, or even fainting. These symptoms are often linked to postural tachycardia syndrome (POTS), which is defined as a rise in heart rate of ≥ 30 bpm within 10 minutes of standing without a drop in blood pressure, and orthostatic hypotension, defined as a fall in blood pressure (BP) of ≥ 20 mmHg systolic (SBP) or ≥ 10 mmHg diastolic (DBP) within three minutes of standing [7,8,9]. Both conditions increase risks such as falls and injuries.
These problems suggest that LC may disrupt multiple body systems, including the autonomic nervous, cardiovascular, and respiratory systems [3,4,10]. To investigate these changes, researchers use orthostatic stress tests such as the active standing test and the head-up tilt test [11,12]. The active standing test is especially important because it mirrors everyday life as people typically perform around 45–60 postural transitions each day [13]. Unlike the tilt test, which passively moves a person upright, active standing engages leg muscles that help blood flow return to the heart, offering a clearer picture of cardiovascular and autonomic responses [12]. The tilt test may also miss very rapid drops in blood pressure within 30 seconds of standing, known as initial orthostatic hypotension [14,15].
Despite its relevance, studies using the active standing test in people experiencing LC have reported inconsistent results [8,16,17]. For example, Monaghan et al. (2022) found that only 13% of older adults with LC met criteria for POTS, and very few reported symptoms [8]. In contrast, Blitshteyn et al. (2021) reported that 75% of participants showed this response [16]. Studies using the tilt test have also produced highly variable results as González-Hermosillo et al. (2023), for instance, found increases in BP rather than HR [17]. These inconsistencies may reflect small sample sizes, differences in participants’ age or health, timing after infection, or variations in testing methods (e.g., protocols) [18]. Therefore, this review aims to i) identify studies that used the active standing test to measure cardiovascular, autonomic, or respiratory responses in people experiencing LC; ii) describe the physiological measures reported in these studies, and iii) explore how differences in active standing protocols may explain inconsistent findings.
2. Materials and Methods
2.1. Search Strategy
The Population, Exposure, Comparison, Outcome (PECO) framework was used to guide the research question and search strategy [19]. Published literature indexed in PubMed, MEDLINE, EMBASE, CINAHL & Scopus from January 2020 to August 2024 was initially searched by FO in August 2024, and an updated search was performed in May 2025 using the University of Manitoba Libraries platform, with assistance from an experienced librarian (JW). Combinations of the following terms were used: long -covid’, OR ‘post covid’ OR ‘post-acute sequelae of SARS-CoV-2’ or ‘long-haul covid’, ‘orthostatic stress test’, ‘orthostatic hypotension’, ‘postural transition’, ‘hemodynamic responses’, ‘blood pressure’, ‘heart rate’, ‘cardiovascular’, ‘autonomic’ and ‘respiratory’. The search was limited to studies published in the English language and from 2020 – 2025. The search strategies are presented in Supplemental Material Table S1. The review was registered with PROSPERO (CRD 42024615872) and followed the Preferred Reporting Items for Systematic Review (PRISMA 2020) guidelines (Supplemental Material PRISMA 2020 Checklist).
2.2. Eligibility and Screening Criteria
Studies were included if they: (1) reported on cardiovascular, autonomic or respiratory responses during the active standing test in adults (≥18 years old) experiencing LC; (2) included a healthy control group for comparison; 3) published between 2020-2025; (4) used continuous beat-to-beat measurements of BP or HR; (5) published in the English language, and were excluded if they did not use an active standing test, only used manual measurements of BP and HR, focused on assessing immunophenotypical biomarkers of LC, used only self-reported surveys or questionnaires (e.g., DePaul symptom questionnaire, COMPASS-32), were published as systematic, scoping, narrative reviews, case studies, qualitative studies, poster or conference abstracts, letters to editors, or editorials.
Title and abstract screening criteria were independently screened by two review authors (FO and AN) using Covidence (www.covidence.org; Melbourne, Australia). Articles identified as potentially eligible by the two review authors were retrieved, and duplicates were either manually (when identified) or automatically (by Covidence) removed. Full texts of potentially eligible studies were screened independently by FO and AN, and RV resolved conflicts when necessary.
2.3. Data Extraction
A standardized extraction form was used by two authors (FO and AN) to extract relevant information pertaining to reference data (author, title, journal, year, and country), study characteristics (objective, design, testing setting), participant characteristics (age, sex, race, number of participants, and health status prior to COVID-19 infection). Study details, including the inclusion and exclusion criteria, proportion of participants who were hospitalized (severity of COVID-19 infection), current medication use, and reported symptoms, were also extracted. The instrumented (devices, active standing protocol, questionnaires), outcome measures (cardiovascular, autonomic, and respiratory variables), the definition of LC used, conclusions and limitations as identified by the study authors, and funding sources were also extracted (Supplementary Material Table S2). No automation tool was used in this process.
2.4. Quality and Risk of Bias Assessment
Two reviewers (FO and AN) independently evaluated the quality and risk of bias for each included study using the nine-point Newcastle–Ottawa Quality Assessment Scale (NOS) for case-control studies [20]. Disagreements were resolved by the supervising author (RV). The NOS was tailored to long-COVID studies. Studies were categorized based on the NOS score as follows: 0–3 points were considered low quality, 4–6 points moderate quality, and 7-9 points as high quality across the categories of (i) selection, (ii) comparability, and (iii) exposure [20].
Since the NOS was originally designed for cohort and case-control studies, we adapted the case-control scoring tool for long-COVID observational cross-sectional studies by modifying some of its domains to better assess exposure and outcome, as described in previous work in the healthcare field [21,22]. Specifically, we interpreted the domain ‘representative of long-COVID cases’ as meeting recognized definitions of long-COVID and if the sample recruited from relevant populations (e.g., community, outpatient clinics, tertiary care units, or post-COVID recovery programs), and interpreted ‘exposure’ as encompassing the process by which a study confirmed COVID-19 infection in its participants and whether the statistical test used was appropriate, fully described or incomplete. A meta-analysis could not be performed due to the small number of studies and heterogeneity across the studies. The modified scoring criteria are provided in Supplemental Material Table S3.
2.5. Data Analysis and Synthesis
Descriptive characteristics were used to describe trials and participants. Means, medians, and associated measures of variability (e.g., 95% confidence intervals, interquartile ranges [IQR], were applied to continuous variables, while counts and proportions were used for dichotomous and categorical variables. Given the novelty of LC, the anticipated heterogeneity in study designs, and the scarcity of data related to the research question, conducting a meta-analysis was not feasible. Descriptions of individual studies were extracted and presented to show methodological similarities and differences. A narrative summary of results was used to summarize and interpret findings.
3. Results
3.1. Study Selection and Search Strategy
In total, 2145 references were identified and imported into Covidence for screening through database searches, with 1189 references removed as duplicates. 956 studies were screened by title and abstract following duplicate removal, and 41 studies were screened on the full-text level. Three studies were included in the review following full-text screening. The PRISMA flowchart of study selection is provided in Figure 1.
3.2. Study Characteristics
We identified 3 studies that used the active standing test to evaluate physiological responses in individuals experiencing LC [23,24,25]. These studies included assessments of cardiovascular (e.g., HR, BP), autonomic (e.g., heart rate variability, baroreflex sensitivity) and cardiorespiratory (respiratory sinus arrhythmia) variables. Sample sizes varied across studies, ranging from 30-92 LC participants and 33-120 healthy control participants.
Methodological approaches differed in terms of data collection protocols (5 mins supine and 3 mins standing vs. 10 mins supine and 10 mins standing), and the definition of LC used (WHO’s definition vs. NICE) [23,24,25]. Study design and classification was based on the descriptions provided by the original authors. Study characteristics are presented in Table 1.
Risk of bias was assessed using the nine-point Newcastle-Ottawa Quality Assessment Scale (NOS) adapted for cross-sectional long-COVID studies. All studies were classified as high quality [23,24,25]. The quality of included studies is presented in Supplementary Material Table S4.
3.3. Definitions and Diagnostic Criteria
All three studies defined POTS as an increase in HR of ≥ 30 bpm within 10 minutes of standing, in the absence of orthostatic hypotension [23,24,25]. Orthostatic hypotension (OH) was defined by Seeley et al. (2023) and Shah et al. (2022) as a ≥ 20 mmHg drop in SBP or ≥ 10 mmHg drop in DBP within 3 minutes of standing [24,25]. Hira et al. (2025) only evaluated initial orthostatic hypotension (IOH), defined as a transient SBP drop of ≥ 40 mmHg within 15 seconds of standing, with recovery within 45–60 seconds and DBP was not considered in this definition [23].
3.4. Heart Rate Responses
All three studies reported elevated HR in LC participants compared to healthy controls in both supine and upright positions [23,24,25]. Supine HR was significantly higher in LC groups, with reported averages ranging from 67 to 88 bpm, compared to 61 to 78 bpm in controls [23,24,25]. The increase in HR following standing was also significantly higher in LC participants, particularly for those meeting the POTS criteria, with standing HR ranging from 99 to 114 bpm compared to 78-83 bpm in controls. Subgroup analysis comparisons in Hira et al. (2025) study showed significant differences in supine and standing HR across LC phenotypes, with the LC-POTS group showing the highest increase after standing [23]. Detailed HR responses across studies and subgroups are presented in Table 2.
3.5. Blood Pressure Responses
Blood pressure findings were less consistent across studies. Shah et al. (2022) reported that 13% of LC participants (n = 12/92) met the criteria for OH, though absolute values and p-values were not reported [25]. Similarly, Seeley et al. (2023) reported no absolute values but found no significant group differences in supine and standing BP (p = 0.12) but observed a time-dependent increase in DBP in PASC and participants with POTS compared to controls (p = 0.03) [24]. In contrast, Hira et al. (2025) reported absolute values and found no overall BP differences between LC and controls. However, subgroup analysis showed higher SBP, DBP and mean arterial pressure (MAP) in LC participants who met the criteria of initial orthostatic hypotension (LC-IOH) compared to both LC with no abnormalities (LC-none) and LC-POTS groups (all p < 0.001). After standing, the LC-IOH showed lower SBP and MAP responses. Additionally, vascular sympathetic modulation, measured by low-frequency systolic blood pressure variability (LFSBP), was significantly reduced in LC-none compared to controls during supine and standing positions. Standing LFSBP was also significantly lower in the LC-none group compared to the LC-POTS group. Detailed responses are summarized in Table 3.
3.6. Time Domain Heart Rate Variability Responses
Shah et al. (2022) and Hira et al. (2025) reported decreases in heart rate variability (HRV) in individuals experiencing LC compared to healthy controls [23,25]. Time-domain HRV indices, such as root-mean square of successive R-R interval differences (RMSSD) and standard deviation of R-R intervals (SDNN), were consistently lower in LC participants compared to healthy controls. Shah et al. (2022) also reported a reduction in RMSSD based on COVID-19 severity, finding that the values were lowest in those with severe and moderate illness, with higher values in the mild and asymptomatic groups (p < 0.0001). Similarly, subgroup analysis by Hira et al. (2025) also showed significant reductions in heart rate variability indices in the LC-IOH and LC-POTS subgroups compared to LC-none group during standing. Standing RMSSD was lowest in LC-POTS group (9.72 [7.37-13] ms) and highest in LC-none group (19 [16-38] ms), with similar patterns observed for SDNN and pNN50 (percentage of successive R-R intervals differing by more than 50 ms). Detailed time-domain HRV across studies and subgroups are presented in Table 4 below.
3.7. Frequency Domain Heart Rate Variability Responses
Frequency-domain HRV indices, including high-frequency (HF), low-frequency (LF), total power (TP), low-frequency to high-frequency ratio (LF/HF) and vagal baroreflex sensitivity (BRSv), were reported only by Hira et al. (2025). No significant differences were found between LC and control participants during supine. However, after standing, LC participants demonstrated significantly lower HF, LF, and TP compared to controls, with no group differences found in LF/HF ratio or BRSv. Subgroup analysis revealed significant differences in HF, LF, TP, and BRSv across LC phenotypes (LC-IOH, LC-POTS, LC-none) in both supine and standing positions. During supine, the LC-IOH group showed significantly lower HF, LF, and BRSv compared to LC-POTS (all p < 0.05), and BRSv was also significantly reduced in LC-IOH compared to LC-none (p = .01). Following standing, the LC-POTS group had significantly lower HF, LF, and TP compared to LC-none (all p < 0.01). BRSv was also significantly lower in both LC-POTS and LC-IOH compared to LC-none. LF/HF ratio did not significantly differ between groups. Detailed frequency-domain HRV across studies and subgroups are presented in Table 5.
3.8. Respiratory Responses
Only Seeley et al. (2023) reported respiratory sinus arrhythmia, but no other respiratory system variables were reported. Respiratory sinus arrhythmia was significantly lower in their LC group (9.8 [7.0 – 14.5] breaths/min) compared to the group with POTS (14.0 [12.1 – 19.2] breaths/min) and healthy controls (17.4 [12.0 – 19.5] breaths/min) groups (p < 0.001) [24].
4. Discussion
This review highlights that the active standing test reveals subtle but clinically relevant cardiovascular and autonomic changes in individuals with LC. Across studies, consistent patterns included elevated HR and reduced HRV indices (RMSSD, SDNN, LF, HF, TP, BRSv), whereas BP responses were highly variable. Notably, the active standing test was able to identify subgroups with exaggerated tachycardic or hypotensive responses, suggesting its value for detecting early autonomic dysfunction. Together, these findings indicate that LC frequently involves disturbances in cardiovascular regulation, with potential implications for symptom burden, safety, and rehabilitation.
Our findings align with growing evidence that autonomic dysfunction is a core feature of long-COVID [26]. While some studies reported high prevalence of postural orthostatic tachycardia syndrome or orthostatic hypotension, others found minimal cases [8,24,25]. Such variation is in line with prior reports of heterogeneous orthostatic intolerance prevalence in post-viral syndromes [6,7]. Several mechanisms may contribute, including persistent inflammation, impaired baroreflex function, microvascular injury, and altered hemodynamics [10,27,28]. Reduced HRV indices across studies supports impaired autonomic control, consistent with prior research in long-COVID and other chronic conditions. These observations reinforce the hypothesis that long-COVID involves dysregulation of both sympathetic and parasympathetic function, which may underline symptoms such as dizziness, fatigue, and exercise intolerance [26,29].
A key challenge identified in this review is methodological heterogeneity across studies. Active standing test protocols differed in duration and timing of measurements limiting comparability [23,25]. Definitions of long-COVID also varied, with some studies relying on self-report while others required a positive polymerase chain reaction or rapid kit confirmation of infection [23,24,25]. Physiological measures were largely restricted to HR and BP, with few assessments of stroke volume, systemic vascular resistance, or cerebral blood flow, which are factors critical for understanding OI pathophysiology [30,31]. These inconsistencies likely explain much of the variability in prevalence estimates and underscore the need for standardized approaches.
This review has several limitations that need to be acknowledged. The number of eligible studies is small, restricting generalizability and precluding meta-analysis. Although our inclusion criteria strengthened rigor by requiring continuous cardiovascular monitoring and the inclusion of healthy controls, this may have excluded relevant but less detailed studies. Publication bias may also favor studies reporting positive findings. Finally, the limited representation of diverse populations reduces the ability to draw conclusions about sex, age, or comorbidity effects. Despite these limitations, this review provides important implications for both research and clinical practice.
Future studies should adopt standardized definitions of long-COVID (e.g., National Academies of Sciences, Engineering, and Medicine 2024 consensus definition), consistent active standing test protocols, and beat-to-beat monitoring to capture rapid hemodynamic changes. Expanding beyond heart rate and blood pressure to include stroke volume, systemic vascular resistance, and cerebral blood flow will clarify mechanisms of orthostatic intolerance and guide targeted interventions. Comparative research across post-viral syndromes could also help determine whether these autonomic disturbances are specific to long-COVID or reflect broader post-infectious processes.
Ultimately, the active standing test offers a simple and physiologically relevant tool to advance understanding of cardiovascular dysregulation in long-COVID, with potential to inform both diagnosis and rehabilitation strategies. Individuals with long-COVID show consistent elevations in heart rate and impaired autonomic function during active standing, with varied blood pressure abnormalities. These findings suggest altered autonomic-cardiovascular integration that may contribute to symptoms such as dizziness, fatigue, and reduced tolerance of daily activities. Incorporating active standing into clinical assessment could support earlier identification of autonomic dysfunction, guide rehabilitation strategies, and help tailor management to improve functional recovery in long-COVID. The limited evidence base also emphasizes an urgent need for further research evaluating hemodynamic and multisystem responses in this population.
5. Conclusions
This systematic review synthesized studies using the active standing test to assess cardiovascular, autonomic, or respiratory responses in long-COVID. While limited in number, findings show increased heart rate responses and reduced heart rate variability indices in individuals experiencing long-COVID, suggesting persistent autonomic dysfunction. Blood pressure responses were inconsistent, with some subgroup-level differences in systolic and mean arterial pressure. Key gaps included the absence of standardized long-COVID definitions, incomplete reporting of absolute values, and the absence of other hemodynamic variables (e.g., cardiac output, stroke volume, systemic vascular resistance) and respiratory measures, limiting comparability. Future research should consider adopting the use of standardized definitions (e.g., National Academies of Sciences, Engineering, and Medicine consensus criteria), using continuous hemodynamic measurement tools, and including broader physiological assessment of variables beyond BP and HR, and incorporate appropriate control groups. A multi-system assessment approach may better characterize dysregulation and inform targeted interventions for long-COVID.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1, Table S2, Table S3, Table S4 and PRISMA 2020 Checklist.
Author Contributions
Faith Olarinde - Conceptualization, Formal analysis, Methodology, Writing – review & editing, Writing – original draft. Albena Nunes-Silva - Formal analysis and revisions. Diana C. Sanchez-Ramirez – Validation and revisions. Yannick Molgat-Seon – Validation and revisions. Rodrigo Villar - Conceptualization, Formal analysis, Methodology, Supervision, Validation, and revisions.
Funding
FO’s research was supported by the Canadian Institute for Health Research Canada Graduate Research Scholarship-Masters and the Ruth Asper Scholarship in Kinesiology and Recreation Management. There is no associated grant number with these fundings.
Identifying Information
Faith Olarinde has moved to a new institution (affiliated as a PhD student at the Department of Kinesiology and Physical Education at McGill University, Montreal, Quebec, Canada) since completing this project.
Institutional Review Board Statement
Not applicable. This study was however registered on PROSPERO CRD-42024615872.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were generated or analyzed in support of this research. All data used are available in public databases.
Acknowledgments
We gratefully acknowledge Janice Winkler (librarian) for her expert guidance and support during the development of this systematic review. Thank you to the FAPEMIG (APQ-04126-23), call 009/2023, for supporting Albena Nunes-Silva in the internationalization program of the ICTMGS. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| BRSv | Vagal baroreflex sensitivity |
| CI | Confidence interval |
| DBP | Diastolic blood pressure |
| HC | Health controls |
| HF | High frequency |
| HR | Heart rate |
| HR | Heart rate variability |
| IQR | Inter-quartile range |
| LC | Long-COVID |
| LC-IOH | Long-COVID and initial orthostatic hypotension |
| LC-None | Long-COVID but no abnormalities |
| LC-POTS | Long-COVID and post orthostatic tachycardia syndrome |
| LF | Lower frequency |
| LF/HF ratio | Lower to higher frequency ratio |
| LFSBP | Low-frequency systolic blood pressure |
| MAP | Mean arterial pressure |
| NASEM | National Academies of Sciences, Engineering, and Medicine |
| NICE | National Institutes for Health and Care Excellence. |
| OH | Orthostatic hypotension |
| PASC | Post-acute sequelae of SARS-CoV-2 infection |
| pNN50 | Percentage of successive R-R intervals differing by more than 50ms |
| POTS | Post orthostatic tachycardia syndrome |
| RMSSD | Root-mean square of successive R-R interval differences |
| SBP | Systolic blood pressure |
| SD | Standard deviation |
| SDNN | Standard deviation of R-R intervals |
| TP | Total Power |
| WHO | World Health Organization |
References
- National Academies of Sciences, Engineering, and Medicine. A Long COVID Definition: A Chronic, Systemic Disease State with Profound Consequences; The National Academies Press: Washington, DC, USA, 2024. [Google Scholar]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Ramirez, D.C.; Normand, K.; Zhaoyun, Y.; Torres-Castro, R. Long-Term Impact of COVID-19: A Systematic Review of the Literature and Meta-Analysis. Biomedicines 2021, 9, 900. [Google Scholar] [CrossRef]
- Ricci, F.; De Caterina, R.; Fedorowski, A. Orthostatic hypotension epidemiology, prognosis, and treatment. J. AM Coll. Cardiol. 2015, 66, 848–860. [Google Scholar] [CrossRef]
- Vernon, S.D.; Funk, S.; Bateman, L.; Stoddard, G.J.; Hammer, S.; Sullivan, K.; Bell, J.; Abbaszadeh, S.; Lipkin, W.I.; Komaroff, A.L. Orthostatic Challenge Causes Distinctive Symptomatic, Hemodynamic and Cognitive Responses in Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Med. 2022, 9, 917019. [Google Scholar] [CrossRef]
- Ormiston, C.K.; Świątkiewicz, I.; Taub, P.R. Postural orthostatic tachycardia syndrome as a sequela of COVID-19. Hear. Rhythm. 2022, 19, 1880–1889. [Google Scholar] [CrossRef]
- Monaghan, A.; Jennings, G.; Xue, F.; Byrne, L.; Duggan, E.; Romero-Ortuno, R. Orthostatic Intolerance in Adults Reporting Long COVID Symptoms Was Not Associated with Postural Orthostatic Tachycardia Syndrome. Front. Physiol. 2022, 13, 833650. [Google Scholar] [CrossRef]
- Freeman, R.; Wieling, W.; Axelrod, F.B.; Benditt, D.G.; Benarroch, E.; Biaggioni, I.; Cheshire, W.P.; Chelimsky, T.; Cortelli, P.; Gibbons, C.H.; et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin. Auton. Res. 2011, 21, 69–72. [Google Scholar] [CrossRef]
- Diab, A.M.; Carleton, B.C.; Goralski, K.B. COVID-19 pathophysiology and pharmacology: What do we know and how did Canadians respond? A review of Health Canada authorized clinical vaccine and drug trials. Can. J. Physiol. Pharmacol. 2021, 99, 577–588. [Google Scholar] [CrossRef]
- Finucane, C.; van Wijnen, V.K.; Fan, C.W.; Soraghan, C.; Byrne, L.; Westerhof, B.E.; Freeman, R.; Fedorowski, A.; Harms, M.P.M.; Wieling, W.; et al. A practical guide to active stand testing and analysis using continuous beat-to-beat non-invasive blood pressure monitoring. Clin. Auton. Res. 2019, 29, 427–441. [Google Scholar] [CrossRef]
- McJunkin, B.; Rose, B.; Amin, O.; Shah, N.; Sharma, S.; Modi, S.; Kemper, S.; Yousaf, M. Detecting initial orthostatic hypotension: a novel approach. J. Am. Soc. Hypertens. 2015, 9, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Dall, P.M.; Kerr, A. Frequency of the sit to stand task: An observational study of free-living adults. Appl. Ergon. 2010, 41, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Wieling, W.; Kaufmann, H.; E Claydon, V.; van Wijnen, V.K.; Harms, M.P.M.; Juraschek, S.P.; Thijs, R.D. Diagnosis and treatment of orthostatic hypotension. Lancet Neurol. 2022, 21, 735–746. [Google Scholar] [CrossRef]
- Wieling, W.; Krediet, C.T.P.; van Dijk, N.; Linzer, M.; Tschakovsky, M.E. Initial orthostatic hypotension: Review of a forgotten condition. Clin. Sci. 2007, 112, 157–165. [Google Scholar] [CrossRef]
- Blitshteyn, S.; Whitelaw, S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: a case series of 20 patients. Immunol. Res. 2021, 69, 205–211. [Google Scholar] [CrossRef]
- G, J.A.G.-H.; Galarza, E.J.; Fermín, O.V.; González, J.M.N.; Tostado, L.M.F.Á.; Lozano, M.A.E.; Rabasa, C.R.; Alvarado, M.d.R.M. Exaggerated blood pressure elevation in response to orthostatic challenge, a post-acute sequelae of SARS-CoV-2 infection (PASC) after hospitalization. Auton. Neurosci. 2023, 247, 103094. [Google Scholar] [CrossRef]
- Osuchowski, M.F.; Winkler, M.S.; Skirecki, T.; Cajander, S.; Shankar-Hari, M.; Lachmann, G.; Monneret, G.; Venet, F.; Bauer, M.; Brunkhorst, F.M.; et al. The COVID-19 puzzle: Deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir. Med. 2021, 9, 622–642. [Google Scholar] [CrossRef]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; Our Research; The Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLOS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef]
- Hira, R.; Baker, J.R.; Siddiqui, T.; Patel, A.; Valani, F.G.A.; Lloyd, M.G.; Floras, J.S.; Morillo, C.A.; Sheldon, R.S.; Raj, S.R.; et al. Attenuated cardiac autonomic function in patients with long-COVID with impaired orthostatic hemodynamics. Clin. Auton. Res. 2025, 35, 301–314. [Google Scholar] [CrossRef] [PubMed]
- Seeley, M.-C.; Gallagher, C.; Ong, E.; Langdon, A.; Chieng, J.; Bailey, D.; Page, A.; Lim, H.S.; Lau, D.H. High Incidence of Autonomic Dysfunction and Postural Orthostatic Tachycardia Syndrome in Patients with Long COVID: Implications for Management and Health Care Planning. Am. J. Med. 2023, 138, 354–361.e1. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.; Kunal, S.; Bansal, A.; Jain, J.; Poundrik, S.; Shetty, M.K.; Batra, V.; Chaturvedi, V.; Yusuf, J.; Mukhopadhyay, S.; et al. Heart rate variability as a marker of cardiovascular dysautonomia in post-COVID-19 syndrome using artificial intelligence. Indian Pacing Electrophysiol. J. 2022, 22, 70–76. [Google Scholar] [CrossRef]
- Novak, P.; Mukerji, S.S.; Alabsi, H.S.; Systrom, D.; Marciano, S.P.; Felsenstein, D.; Mullally, W.J.; Pilgrim, D.M. Multisystem Involvement in Post-Acute Sequelae of Coronavirus Disease 19. Ann. Neurol. 2022, 91, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Bielecka, E.; Sielatycki, P.; Pietraszko, P.; Zapora-Kurel, A.; Zbroch, E. Elevated Arterial Blood Pressure as a Delayed Complication Following COVID-19—A Narrative Review. Int. J. Mol. Sci. 2024, 25, 1837. [Google Scholar] [CrossRef]
- van Campen, C.L.M.C.; Rowe, P.C.; Visser, F.C. Two different hemodynamic responses in ME/CFS patients with postural orthostatic tachycardia syndrome during head-up tilt testing. J. Clin. Med. 2024, 13, 7726. [Google Scholar] [CrossRef]
- Fedorowski, A.; Olsén, M.F.; Nikesjö, F.; Janson, C.; Bruchfeld, J.; Lerm, M.; Hedman, K. Cardiorespiratory dysautonomia in post-COVID-19 condition: Manifestations, mechanisms and management. J. Intern. Med. 2023, 294, 548–562. [Google Scholar] [CrossRef]
- Khan, M.S.; Miller, A.J.; Ejaz, A.; Molinger, J.; Goyal, P.; MacLeod, D.B.; Swavely, A.; Wilson, E.; Pergola, M.; Tandri, H.; et al. Cerebral Blood Flow in Orthostatic Intolerance. J. Am. Hear. Assoc. 2025, 14, e036752. [Google Scholar] [CrossRef]
- de Matos, D.G.; de Santana, J.L.; Aidar, F.J.; Cornish, S.M.; Giesbrecht, G.G.; Mendelson, A.A.; Duhamel, T.A.; Villar, R. Cardiovascular regulation during active standing orthostatic stress in older adults living with frailty: A systematic review. Arch. Gerontol. Geriatr. 2025, 136, 105894. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart – study selection.
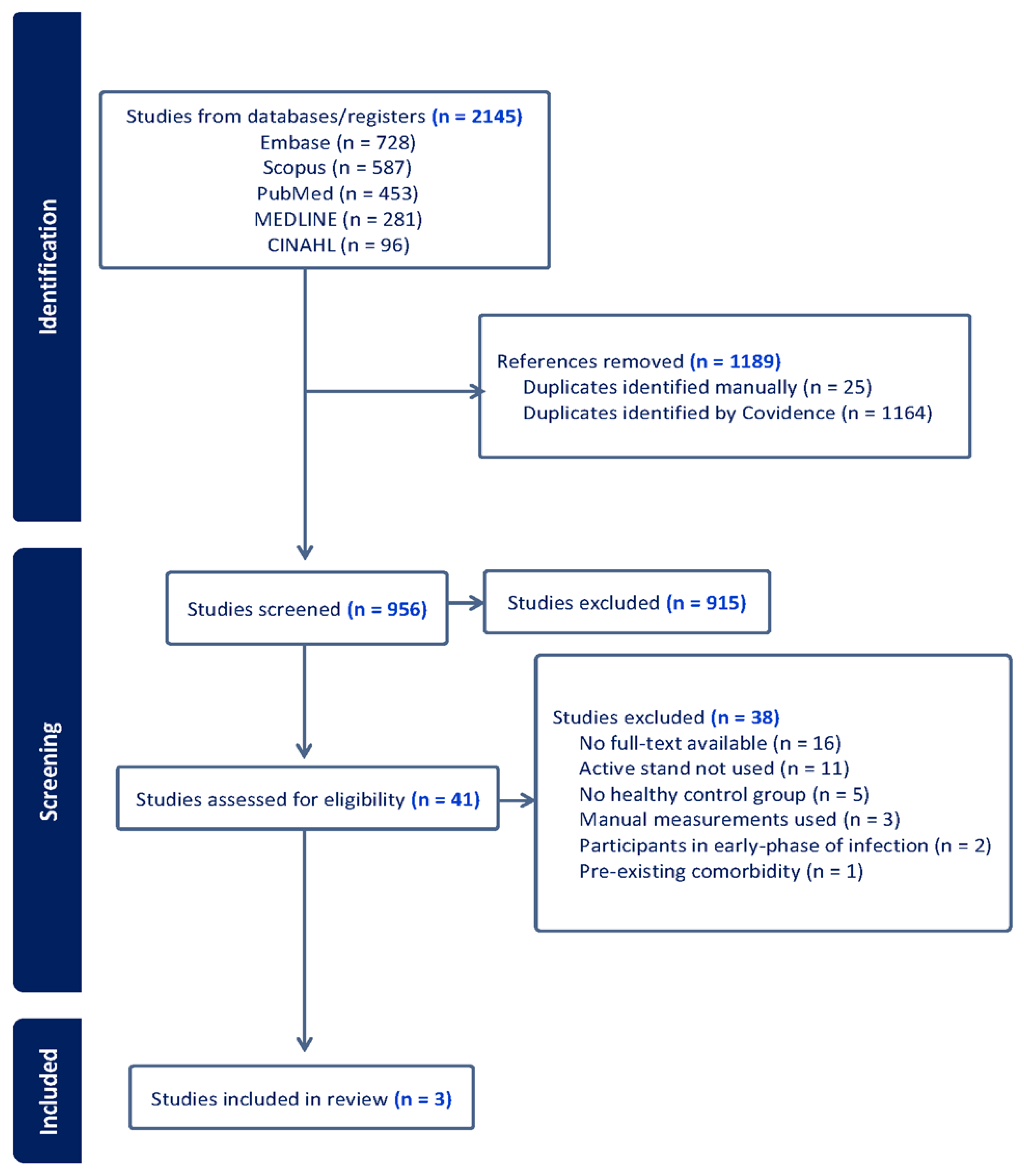

Table 1.
Study characteristics.
|
Study (Year) |
Country |
Study Design |
Sample size |
Proportion of females (%) | Age (mean ± SD, median [IQR])/[CI] (years) | Definition of long-COVID | Active standing protocol (Timeframe) |
Outcome Measures |
|---|---|---|---|---|---|---|---|---|
| Shah et al. (2022) | India | Prospective single center | PASC = 92 HC = 120 |
41% 46% |
PASC = 50.6 ± 12.1 HC = 51.8 ± 4.2 |
Descriptive definition; no organizational source | 5 min supine, 3 min. stand |
Heart rate variability |
| Seeley et al. (2023) | Australia | Prospective comparative | PASC = 30 POTS = 33 HC = 33 |
82% 94% 82% |
PASC = 37 [15] POTS = 28 [14] HC = 28 [23] |
WHO’s Delphi Consensus |
10 min supine, 10 min standing | Respiratory sinus arrhythmia, heart rate and blood pressure responses |
| Hira et al. (2025) | Canada | Cross-sectional | PASC = 94 HC = 33 |
81% 76% |
PASC = 42 [36, 53] HC = 49 [30, 62] |
NICE guideline |
10 min supine, 10 min standing | Heart rate variability, blood pressure variability, Baroreflex sensitivity, Blood pressure and heart rate responses |
Note: SD: standard deviation; IQR: inter-quartile range; CI: confidence interval; PASC: post-acute sequelae of SARS-CoV-2 infection; HC: healthy control; POTS: postural orthostatic tachycardia syndrome; WHO: World Health Organization; NICE: National Institutes for Health and Care Excellence.3.2. Risk of Bias Assessment.
Table 2.
Comparison of heart rate findings across studies.
| Study (Year) | Supine HR Findings | Standing HR Findings |
|---|---|---|
| Shah et al. (2022) | LC: 88 ± 15 bpm HC: 78 ± 11 bpm p = 0.0001 |
LC-OH: 99 ± 18 bpm No-OH: 86 ± 14 bpm p = 0.006 HC: not reported. |
| Seeley et al. (2023) | PASC: 72 ± 13 bpm POTS: 79 ± 12 bpm HC: 68 ± 9 bpm Group (p = 0.003) PASC > HC (p = 0.05) PASC < POTS p: not reported |
∆HR (0-10 min) PASC: 36 [30–47] bpm POTS: 46 [34–59] bpm HC: 15 [9–20] bpm Group (p = 0.001) PASC > HC (p = 0.001) PASC ~ POTS (p = 0.1) |
| Hira et al. (2025) | LC: 67 [62–75] bpm HC: 61 [56–70] bpm p = 0.01 Subgroups: LC-IOH: 67 [61–77] bpm LC-POTS: 68 [65–75] bpm LC-none: 63 [57–73] bpm HC: 61 [56–70] bpm Group (p = 0.023) LC-none ~ HC (p = 0.999) LC-none ~ LC-POTS (p = 0.283) LC-none ~ LC-IOH (p = 0.063) LC-POTS ~ LC-IOH (p = 0.999) |
LC: 89 [77–106] bpm HC: 78 [69–87] bpm p = 0.001 Subgroups: LC-IOH: 85 [77–93] bpm LC-POTS: 114 [103–131] bpm LC-none: 80 [70–88] bpm HC: 78 [69–87] bpm Group (p < 0.001) LC-none ~ HC (p = 0.999) LC-none < LC-POTS (p = 0.001) LC-none ~ LC- IOH (p = 0.279) LC-POTS > LC-IOH (p = 0.001) |
Note: Long-COVID terminology is presented as reported in each article. OH: orthostatic hypotension; LC: Long-COVID; HC: healthy controls; LC-OH: Long-COVID with orthostatic hypotension; no-OH: participants without orthostatic hypotension; PASC: post-acute sequelae of COVID-19; POTS: postural orthostatic tachycardia syndrome; HR: heart rate; LC-IOH: participants with long-COVID and initial orthostatic hypotension; LC-POTS: participants with long-COVID and postural orthostatic tachycardia syndrome; LC-none: participants with long-COVID but no abnormalities.
Table 3.
Comparison of blood pressure response findings across studies.
| Variable |
Shah et al. (2022) |
Seeley et al. (2023) |
Hira et al. (2025) |
|---|---|---|---|
| SBP-supine (mmHg) | Absolute values not reported | No significant group differences (p = 0.12). No absolute values reported |
LC: 119 [109–132] mmHg HC: 119 [114–124] mmHg p = 0.683. Subgroup: LC-IOH: 130 [123–143] mmHg LC-none: 113 [105–119] mmHg LC-POTS: 112 [103–123] mmHg LC-IOH > LC-none (p = 0.001). LC-IOH > LC-POTS (p = 0.001). |
| DBP-supine (mmHg) | Absolute values not reported | No data reported for DBP in supine | LC: 71 [64–77] mmHg HC: 67 [64–72] mmHg p = 0.065 Subgroup: LC-IOH: 76 [67–79] mmHg LC-none: 67 [63–73] mmHg LC-POTS: 66 [63–73] mmHg LC-IOH > LC-none (p = 0.001). LC-IOH > LC-POTS (p = 0.009). |
| MAP-supine (mmHg) | Not reported | Not reported | LC: 87 [80–95] mmHg HC: 85 [80–91] mmHg p = 0.268 Subgroup: LC-IOH: 94 [87–100] mmHg LC-none: 81 [78–89] mmHg LC-POTS: 81 [77–92] mmHg LC-IOH > LC-none (p = 0.001). LC-IOH > LC-POTS (p = 0.001). |
|
LFSBP supine (mmHg²) |
Not reported | Not reported | LC: 4.06 [2.69–6.62] mmHg² HC: 5.15 [3.77–9.37] mmHg² LC-none < HC (p = 0.001) |
Note: SBP: Systolic blood pressure; DBP: Diastolic blood pressure; MAP: Mean arterial pressure; LFSBP: Low-frequency systolic blood pressure; LC: long-COVID; HC: healthy control; LC-IOH: participants with long-COVID and initial orthostatic hypotension; LC-POTS: participants with long-COVID and postural orthostatic tachycardia syndrome; LC-none: participants with long-COVID but no abnormalities.
Table 4.
Time-domain heart rate variability indices.
| Variable | (Shah et al., 2022) | (Hira et al., 2025) |
|---|---|---|
| RMSSD | LC:13.9 ± 11.8 ms HC: 19.9 ± 19.5 ms LC < Controls (p = 0.01) Subgroup: Graded reduction by COVID severity (p = 0.0001) Asymptomatic: 24.2 ms Mild: 16.3 ms Moderate: 9.3 ms Severe: 7.2 ms |
Supine: No significant group-level differences. Standing: LC: 15 [8.9–22] ms HC: 18 [13–32] ms LC < HC (p = 0.011). Subgroup: LC-IOH: 15 [9.60–27] ms LC-none: 19 [16–38] ms LC-POTS: 9.72 [7.37–13] ms LC-POTS < LC-none (p = 0.001) LC-POTS < LC-IOH (p = 0.024) |
| SDNN | LC: 16.9 ± 12.9 ms HC: 22.5 ± 17.6 ms LC < Controls (p = 0.01) |
Supine: No significant group-level differences. Standing: LC: 31 [22–43] ms HC: 40 [32–55] ms; LC < HC (p = 0.001). Subgroup: LC-none: 37 [28–51] ms LC-POTS: 27 [20–33] ms LC-POTS < LC-none (p = 0.018) |
| pNN50 | Not reported |
Supine: No significant group-level differences. Standing: LC: 0.23 [0–0.87] ms HC: 0.78 [0.11–2.72] ms LC < HC (p = 0.011).Subgroup: LC-IOH: 2.46 [0.32–7.44]% LC-none: 0.83 [0–2.50]% LC-POTS: 8.12 [3.10–13]% LC-POTS > LC-none (p = 0.039) LC-POTS > LC-IOH (p = 0.026) |
Note: LC: long-COVID; HC: healthy controls; RMSSD: root-mean square of successive R-R interval differences; SDNN: standard deviation of R-R intervals; pNN50: percentage of successive R-R intervals differing by more than 50ms. LC-IOH: participants with long-COVID and initial orthostatic hypotension; LC-POTS: participants with long-COVID and postural orthostatic tachycardia syndrome; LC-none: participants with long-COVID but no abnormalities.
Table 5.
Frequency-domain heart rate variability indices from Hira et al. 2025.
| Variable | Supine Findings | Standing Findings |
|---|---|---|
| HF | No significant difference between LC and HC. Subgroup: HC: 1136 [262–3121] ms2 LC-none: 1919 [725–4921] ms2 LC-IOH: 1384 [339–2036]ms2 LC-POTS: 2166 [1112–4419] ms² Group (p = 0.026) LC-POTS > LC-IOH (p = 0.028) |
LC: 315 [95–730] ms² HC: 349 [260–1190] ms² LC < HC (p = 0.042) Subgroup: HC: 349 [260–1190] ms2 LC-none: 578 [337–1881] ms2 LC-IOH: 296 [98–871 ]ms2 LC-POTS: 100 [51–339] ms² Group (p < 0.001) LC-none > LC-POTS (p = 0.001). |
| LF | No significant differences between LC and HC. Subgroup: HC: 1484 [603–4210] ms² LC-none: 2130 [1142–4393] ms2 LC-IOH: 1429 [643–2778] ms2 LC-POTS: 2680 [1889–4938] ms² Group (p = 0.015) LC-POTS > LC-IOH (p = 0.012) |
LC: 1203 [483–2212] ms² HC: 1901 [935–4008] ms² LC < HC (p = 0.008) Subgroup: HC: 1901 [935–4008] ms² LC-none: 1806 [1106–3932] ms2 LC-IOH: 974 [428–1941] ms2 LC-POTS: 1080 [298–1671] ms² Group (p = 0.001) LC-POTS < LC-none (p = 0.020) |
| TP | No significant differences between LC and HC. Subgroup: HC: 689 [2547–17839] ms² LC-none: 7702 [4681–14480] ms2 LC-IOH: 5975 [3321–11206] ms2 LC-POTS: 9415 [5096–16398] ms² Group (p = 0.057) LC-POTS > LC-IOH (p = 0.030) |
LC: 3313 [1773–5559] ms² HC: 5342 [3410–10550] ms² LC < HC (p < 0.001) Subgroup: HC: 5342 [3410–10550] ms² LC-none: 4938 [301–9406] ms2 LC-IOH: 3269 [1757–5130] ms2 LC-POTS: 2619 [1413–3949] ms² Group (p = 0.001) LC-POTS < LC-none (p = 0.006) |
| BRSv | No significant differences between LC and HC. Subgroup: HC: 6.89 [4.94–11.4] ms/mmHg LC-none: 10.7 [5.35–17.0] ms/mmHg LC-IOH: 6.24 [4.11–10.0] ms/mmHg LC-POTS: 9.81 [8.47–16.0] ms/mmHg Group (p = 0.001) LC-POTS > LC-IOH (p = 0.010) LC-IOH > LC-none (p = 0.001) |
No significant differences between LC and controls. Subgroup: Controls: 3.97 [2.93–6.41] ms/mmHg] LC-none: 5.33 [3.34–7.06] ms/mmHg LC-IOH: 2.77 [1.76–5.11] ms/mmHg LC-POTS: 2.85 [1.44–3.93] ms/mmHg Group p = 0.001 LC-POTS < LC-none (p = 0.001) LC-IOH < LC-none (p = 0.005) |
| LF/HF ratio | No significant differences between groups or subgroups. | No significant differences between groups or subgroups. |
Note: LC: long-COVID; HC: healthy controls; HF: high-frequency; LF: low-frequency; TP: total power; BRSv: baroreflex sensitivity; LF/HF ratio: low-frequency/high-frequency ratio; LC-IOH: participants with long-COVID and initial orthostatic hypotension; LC-POTS: participants with long-COVID and postural orthostatic tachycardia syndrome; LC-none: participants with long-COVID but no abnormalities.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



