
Submitted:
10 October 2025
Posted:
14 October 2025
You are already at the latest version
Abstract
Background/Objectives: This following study explores the intricate relationship between autism, social anxiety, social cognition skills, and somatic symptoms. A review of the literature reveals that individuals with autism often face challenges in social interactions and often have heightened levels of social anxiety. Aspects of social cognition skills such as theory of mind and empathy may play a crucial role in understanding the dynamics of social anxiety in individuals with autism which may contribute to heightened levels of somatic symptoms. Methods: This study involves recruiting participants with and without a diagnosis of Autism Spectrum Disorder (ASD) for a total of 61 participants (27 with ASD, 34 without ASD) and examining the correlations between their social cognition skills, social anxiety, and somatic symptoms with a particular focus on the mediating roles of social cognition skills and social anxiety. Results: The findings suggest that individuals with self-identified ASD exhibit elevated levels of social anxiety. The study also revealed a positive correlation between higher social anxiety levels and increased somatic symptoms, with a stronger correlation between the two variables in non-ASD partici-pants. No significant correlations between social cognition skills and ASD, social anxiety, nor somatic symptoms were found. Conclusions: Findings from this study and future related studies may hopefully assist in developing more effective treatments for the treatment of somatic symptoms and social anxiety in individuals both with and without ASD. The results suggest that social anxiety levels may be a promising factor to focus on treating individuals.
Keywords:
autism
; social anxiety
; somatic symptoms
; social cognition
1. Introduction
Negative social experiences are linked to the development of social anxiety [1]. Individuals with autism, a neurodevelopmental disorder marked by impaired social communication and interaction [2], face more adverse social encounters, increasing their risk for social anxiety. Clinicians frequently report anxiety, especially social anxiety, in autistic individuals [3,4,5,6]. Due to neurobiological factors, early social deprivation, and poor social skills, these individuals may avoid social situations, reducing opportunities to practice and improve social functioning, thus creating a self-perpetuating cycle.
Theorists suggest autism’s strong genetic basis impacts brain circuits related to social interaction [7]. Prenatal stress and elevated fetal stress hormones, particularly cortisol and sex steroids, have been linked to autism and may affect social and emotional development [8]. For instance, higher fetal testosterone is associated with poorer empathy and emotion recognition [9]. Since these prenatal hormonal differences may affect the development of abilities related to social interaction, anxiety, and cognition, the combination of decreased social abilities and elevated stress response may lead autistic individuals to become more socially anxious and engage less often in meaningful and productive social interaction throughout their development.
Beyond genetics, autistic individuals often struggle with emotional identification, expression, and regulation. Alexithymia—difficulty recognizing and verbalizing emotions—is common and can understandably contribute to emotional somatization due to poor symbolic processing [10,11]. Language is also thought to aid emotion regulation and self-reflection, and without it, bodily sensations of emotion can feel overwhelming and anxiety-inducing [12]. This makes the experience of emotions more somatically negative and potentially more anxiety arousing.
Researchers and theorists have proposed that anxiety may be a central feature of autism. Singletary [7] suggests that the allostatic load, or the long-term effects of repeated and chronic stress, can lead to or increase traits often observed in autistic individuals. In fact, in response to repeated stress, the brain alters to become more sensitive to stress, strengthening the stress response. As an individual experiences more negative social interactions and has less exposure to healthy and informative interactions during development, the more they will display social differences and social anxiety [7]. Indeed, stress and anxiety seem to be prominent features in autism.
It may be because of this heightened stress response, namely related to social situations, that autistic individuals are more susceptible to social anxiety and begin withdrawing from social interaction and relationships early on. For example, autistic individuals often experience overarousal in response to eye contact, leading to gaze avoidance and thus increased social difficulties [13]. As Singletary [7] explains, “what starts as an adaptive response to perceived threat is maladaptive” (p. 35). Because of this, social skills and cognition, such as mentalization skills including empathic accuracy, are hindered.
People with Social Anxiety Disorder (SAD) tend to misinterpret certain stimuli, particularly by misinterpreting emotions as more negative or less positive than they actually are [14]. Thus, people with higher social anxiety levels may suffer from lower theory of mind abilities which could be related to these interpretation biases. Alvi et al. [14] found that higher levels of social anxiety in a non-clinical sample negatively impacted theory of mind and empathic accuracy. In another study, individuals that meet clinical criteria for social anxiety disorder performed lower on a theory of mind (ToM) task than healthy controls, but still scored higher than individuals with ASD were found to perform [15]. According to the cognitive-behavioral model, people with social anxiety disorder allocate too much attention and analysis to their own actions which may impede the acquisition of the ability to accurately analyze others’ states of minds during social interactions. Thus, as anxiety goes up, so does self-focused attention, meaning ToM accuracy goes down.
Individuals with ASD repeatedly show significant difficulty with ToM/emotion recognition and identification tasks across numerous studies [16,17]. This leaves the questions, since social cognitive differences tend to be present in autistic individuals, would social anxiety levels correlate with these differences? Indeed, autistic adults and children show higher than average levels of social anxiety. While social anxiety and ASD are repeatedly correlated in the literature, research has shown that the two conditions have unique features separate from each other; namely ASD emphasizes social difficulties as opposed to social anxiety, theory of mind differences, restricted interests, and rigid routines [18]. Some research has suggested that lack of social/emotional awareness may buffer the effects of anxiety on some individuals with ASD [3,5]. Thus, the role of mentalization abilities, or the ability to accurately perceive one’s own and other’s mental states, intentions, and affects [2] should be a point of interest when trying to determine more specifically why individuals with autism experience heightened levels of anxiety.
Some research has already been done regarding the role of encoding empathy, that is the ability to empathically identify another’s feelings, and its effects on social anxiety levels in autistic adolescents. Anxiety levels in people with autism seem to rise along with empathic skills, meaning that empathy and social anxiety bear a positive correlation with each other. However, a threshold appears to pertain, such that upon attainment of a certain higher level of empathy, social anxiety lowers, creating an inverted U-shaped relationship between social anxiety and empathy [4]. This is notably different from Alvi et al.’s [14] and Hezel and McNally’s [15] findings in participants without ASD, that higher social anxiety showed lower abilities across components of the larger mentalization construct such as ToM, emotion recognition, and empathic accuracy.
White et al. [18] proposed that some autistic individuals who experience more social anxiety may do so because of particularly heightened insight and awareness of their social differences. Perhaps as mentalization skills increase, so does the ability to accurately pick up on others’ judgments, thus making a person more anxious. It can then be speculated that people without autism who present with social anxiety may think they have lower social skills than they do. Their belief that others are negatively evaluating them may hypothetically result from having lower mentalization abilities and misinterpreting others’ judgments and thoughts.
Zuckerman [19] found that, in a sample of individuals diagnosed with ASD that a larger gap between a person’s social comprehension and their actual behavior (or social skills) were positively correlated with social anxiety. The participants with higher social comprehension actually avoid social situations more, possibly because of their anxiety. This suggests that those with autism who possess greater social awareness, who would be more likely to have higher mentalization abilities, are more aware of other people’s negative judgments, leading to more social anxiety.
Social anxiety disorder has been found to be correlated with more somatic complaints and conditions [20,21]. The authors point out that the presence of anxiety itself may be a risk factor for developing somatic complaints, which aligns with the heightening of tension in the body and disruption in digestive processes that often accompany anxiety. Additionally, the heightened self and body awareness that accompanies social anxiety may be contributing to increased somatic-symptom awareness as well [20]. Given previous findings suggesting lower social cognition skills in individuals with social anxiety disorder [14,15] the role of social cognition in somatic symptoms may be important. Additionally, the findings and theories that reduced ability to recognize and process one’s own emotions can lead to higher somatization of emotions suggests a need for understanding mentalization and alexithymia’s role in somatic symptoms [10,22].
Increased neurological and immunological health issues have been observed in individuals with a diagnosis of ASD, namely neurological and immunological health issues, in a twin-study [23]. It is unknown whether social anxiety contributes to the link between a diagnosis of ASD and increased somatic health problems. However, given the established relationship between social anxiety and somatic symptoms, and previous findings suggesting these are both heightened in autistic individuals, it is worth examining.
Indeed, people with somatoform disorders, somatic symptoms with no underlying physical causes, were found to have lower emotional awareness and theory of mind [24]. The authors found a decreased ability to describe one’s own feelings and evaluate the feelings of others, suggesting social cognition skills serve as a protective factor against somatic somatology. Anxiety levels were also higher in individuals with somatoform disorders. The authors suggest a lack of understanding of emotions may lead to more somatic/physical expression and experience of the emotion rather than a conscious awareness and experience of the emotions, similar to other findings, suggestions, and theories [10,22]. A lack of theory of mind can also lead to more interpersonal and social distress, contributing to anxiety and somatic experiences related to anxiety [24]. Thus far, no studies can be found on the relationship among somatic complaints, anxiety, and social cognition in autistic people.
Understanding these relationships may improve interventions for autistic individuals experiencing social anxiety and somatic symptoms. Clinicians may benefit from assessing social cognition when addressing anxiety and physical complaints in this population, as the patterns may differ from those without ASD.
This study hypothesizes that:
- participants with ASD will display lower social perception skills, higher social anxiety levels, and higher somatic symptomology than those without ASD
- higher social anxiety levels and lower social perceptive skills will be correlated with higher somatic symptoms
- social perception skills will mediate the relationship between ASD and higher social anxiety levels
- social cognition skills and social anxiety levels will mediate the relationship between ASD and heightened somatic symptomology, with increased social cognition skills being associated with decreased somatic symptoms and increased social anxiety levels being associated with increased somatic symptoms.
Post-hoc analyses were performed when relevant regarding potential sex differences in findings.
2. Materials and Methods
2.1. Participants
Participants were recruited through a Pace University subject pool, open-access websites (e.g. Facebook, Twitter, Instagram, Reddit), and internet forums. A total of 61 participants completed all of the necessary questions to be included in the analysis (27 with ASD, 34 without). Individuals who did not complete the questionnaires related to the hypotheses of the study were not included in the analyses, nor were individuals who indicated that they were taking the questionnaires on behalf of an individual other than themselves. The participants in this study were required to confirm that they were at least 18 years of age and fluent English speakers. No compensation was offered for participation in this study. All participants completed an electronic informed-consent form prior to beginning the questionnaire. After signing the informed consent form, participants completed a demographics survey and were asked to self-report whether they have received a previous diagnosis of ASD from a healthcare professional prior to completing the measurements. All questionnaires and measurements were conducted virtually via a Qualtrics survey.
2.2. DANVA-2.
Participants were evaluated through the Diagnostic Analysis of Nonverbal Accuracy--Second Edition (DANVA-2) which measures nonverbal social perception through facial expression recognition and voice tone recognition. Participants completed the Adult Faces 2 through a virtual rendition of the original test and stimuli as created and provided by Dr. Virginia Wickline (V. Wickline, email communication, May, 2022). The facial expressions within the Adult Faces 2 subtest display a basic range of emotions including happiness, sadness, anger, and fear. Participants are shown 24 pictures one at a time for one second each; the pictures depict an adult actor portraying one of the four emotions. After each picture, participants are asked to identify out of the four emotions listed, which emotion was displayed in the picture [25]. Significant convergent validity (p=<0.5) was found between the DANVA-2 adult faces and the original DANVA scores along with high test-retest reliability in the DANVA-2 adult faces in college students (r=0.84) and third-graders (r=0.74) [25].
2.3. Leibowitz Social Anxiety Scale
Social anxiety levels will be measured using the Liebowitz Social Anxiety Scale (LSAS) [26], a 24-item questionnaire with a 4-point Likert scale that assesses self-reported levels of fear and avoidance across a variety of social situations. Scores were found to be normally distributed with uniformly high internal consistency. The total scores were also found to have uniformly high consistency with the fear and avoidance subscales (ranging from 0.68-0.98). The Leibowitz Social Anxiety Scale also had significant convergent validity with other measures of social anxiety and avoidance (p<0.001) [27].
2.4. PHQ-15
Somatic symptoms were measured using the Patient Health Questionnaire (PHQ)-15. The PHQ-15 is a 15-item self-report questionnaire that examines somatic symptoms over the past 4 weeks on a 3-point Likert scale ranging from 1 (“not bothered at all”) to 3 (“bothered a lot”) [28]. The PHQ-15 was found to have high internal reliability (Cronbach’s alpha=0.80), convergent validity when compared to multiple other measurements including functional status, disability days, and symptom-related difficulty, discriminant validity when compared to depressive symptoms [28].
2.5. Additional Variables
To identify certain demographic characteristics that would inform variables for data analyses, participants self-reported identifying characteristics through a number of Qualtrics questions. Participants answered either “Yes” or “No” to the following question: “Have you ever been formally diagnosed with autism spectrum disorder (ASD) by a healthcare professional?”. They were also given space to provide comments to further specify the context of their diagnosis if desired. To categorize participants by biological sex, participants were prompted to select either “male”, “female”, or “other” under the prompt “biological sex”. Demographic data regarding race, ethnicity, age, and education level was also collected.
2.6. Analyses
All statistical analyses were run on IBM SPSS Statistics Version 28. Initial tests of covariance were run for the ASD vs. non-ASD groups, LSAS scores, PHQ scores, and DANVA-2 scores.
Independent samples T-tests were run to assess for significance between an ASD diagnosis as the independent variable and LSAS scores, PHQ scores, and DANVA-2 scores as the dependent variables. The DANVA-2 total score was also broken down into two scores as part of a post-hoc analysis, reflecting high-intensity scores and low-intensity scores (regarding degree of intensity of emotion displayed), for which independent samples T-tests were also run .
Bivariate Pearson correlations were run to assess for significance between LSAS scores as the independent variable and both PHQ and DANVA-2 scores set as the dependent variables. Bivariate Pearson correlations were also used to assess for significance between DANVA-2 scores as the independent variable and PHQ scores as the dependent variable.
Lastly, regression analysis using the PROCESS Procedure v4.2 package on SPSS were run to test for mediational effects of numerous variables. A test of mediation was conducted analyzing the DANVA-2 scores’ effect on the relationship between ASD and LSAS scores as well as ASD and PHQ scores. The same analyses were run with DANVA-2 low intensity and high intensity scores run separately as well. A test of mediation was also conducted again through PROCESS Procedure v4.2 package to assess for the role of LSAS scores as a mediator between an ASD diagnosis and PHQ scores. Lastly, a test of mediation was conducted to assess for the role of DANVA-2 scores on the relationship between LSAS scores and PHQ scores.
3. Results
3.1. Descriptive Statistics and Bivariate Correlations
3.1.1. ASD
A reported diagnosis of ASD was not significantly correlated with age, gender, sex, race, ethnicity, education level, or the PHQ-15.
3.1.2. LSAS
LSAS scores were not significantly correlated with age, gender, sex, race, ethnicity, education level, or the PHQ-15.
3.1.3. PHQ-15
Initial covariate analyses of PHQ-15 scores revealed a significant positive correlation with gender, with “non-binary” and “other” associated with higher somatic symptoms (p=0.047). PHQ-15 scores were also positively correlated with having at least one medical diagnosis (p=0.002), chronic pain (p<0.001), and eating difficulties (p<0.001).
3.1.3. DANVA-2
Initial covariate analyses of DANVA-2 scores revealed a significant positive correlation with a non-Hispanic ethnicity (p=0.004).
3.2. ASD, LSAS, DANVA-2, and PHQ-15
Higher LSAS scores were positively correlated with higher PHQ-15 scores (r=0.53, p<0.001) (Figure 1).
However, a diagnosis of ASD was not significantly correlated with PHQ scores (r=-0.01, p=0.972). In contrast to our hypothesis, the DANVA-2 scores did not significantly correlate with an ASD diagnosis. The DANVA-2 scores also did not correlate with LSAS scores or PHQ-15 scores nor did it mediate any relationship between an ASD diagnosis and LSAS scores nor an ASD diagnosis and PHQ-scores (Table 1).
Given social cognition’s lack of significant correspondences, as gauged by the DANVA-2, a mediation analysis between ASD and somatic symptoms (PHQ scores) was run focusing on social anxiety (LSAS scores) as a mediator. The first step of our analysis confirmed again that ASD diagnosis did not have a significant effect on PHQ scores (β=2.09, p=0.102). Mediation analysis found that social anxiety (as gauged by the LSAS) did serve as a mediator between the reported diagnosis of ASD and the measure of health quality (as per the PHQ) (95% CI = (-4.01)-(-.053)). It is noted that the relationship between no ASD diagnosis and PHQ is negative when LSAS is not considered (β =-0.50), meaning having ASD is associated with higher PHQ scores, though not significantly (Figure 2). However, once LSAS is considered, the direction of the relationship switches, resulting in a positive relationship (β=2.09), meaning a diagnosis of ASD becomes slightly negatively associated with higher PHQ scores (Figure 2). Though this relationship is still not significant, the direction of the relationship switches once LSAS is considered as a mediator .
Given these findings, we also explored whether a diagnosis of ASD changed the significance of the relationship between LSAS scores and PHQ scores; we found no significant moderating effect of an ASD diagnosis between LSAS scores and PHQ scores (β =1.49, p=0.23) (Figure 3).
Upon identifying LSAS as a mediator and finding that ASD overall did not serve as a significant moderator between LSAS and PHQ, a post-hoc analysis was run looking at the relationship between LSAS scores and PHQ scores within males and females with and without ASD. This revealed that LSAS and PHQ scores were significantly correlated in females with ASD (r=0.60, p=0.011), females without ASD (r=0.59, p=0.002), and males without ASD (r=0.76, p=0.017). Males with ASD did not show a significant correlation between social anxiety and somatic symptoms (r=0.37, p=0.291).
4. Discussion
The major findings from this study that align with our hypotheses include the findings that participants with ASD did have higher social anxiety levels. Higher social anxiety levels were also correlated with higher somatic symptoms, as predicted. Interestingly, social anxiety was more strongly correlated with somatic symptoms for individuals without ASD, although not significantly; regardless, social anxiety levels still contributed to the relationship for both groups overall.
Our hypotheses that individuals with ASD would have lower social cognitive skills and higher somatic symptoms were not supported, distinct from previous findings examining social cognitive skills [16, 17] and somatic health [23] in individuals with ASD. The hypothesis that social cognition would mediate the relationship between autism and both social anxiety and somatic symptoms was also not supported by our findings, once again inconsistent with previous findings [3, 5, 24]. In fact, our measurement for social cognition did not correlate with autism, social anxiety, nor somatic symptoms.
These findings suggest that the aspect of social cognition applied in this study (measured by the DANVA-2), given its limited scope in seeking visual-facial emotion recognition (matching pictured face to verbal label) does not contribute to the higher levels of social anxiety in individuals with ASD. It is important to note that the partial application of the DANVA-2 (not applying the prosodic/auditory portion), only measures one aspect of social cognition, and other aspects of social cognition, such as determining the purpose behind another’s actions or predicting the emotions or actions of others, likely do apply to the relationship between ASD and social anxiety. Since social anxiety levels were higher in individuals with ASD, this would suggest that other factors may be mediating this effect; other studies have found intolerance of uncertainty, alexithymia, and sensory hypersensitivity to be significant mediators between ASD and social anxiety [29]. The findings that the social cognitive differences assessed are not contributing to increased somatic symptoms leave other social cognitive factors in need of exploration. Additional factors contributing to the somatic health problems seen more so in individuals with ASD [23] also invite further study based upon prior findings. Alexithymia and emotion dysregulation were associated with somatoform disorders, although this was true for both individuals with and without ASD. However, researchers did find that for individuals with ASD, interoceptive sensibility was more strongly linked to somatoform disorders compared to individuals without ASD [30].
Findings also suggest that the presence of social anxiety symptoms significantly changes the relationship between a diagnosis of ASD and somatic symptoms, with the presence of social anxiety decreasing the relationship between an ASD diagnosis and somatic symptomology and increasing the relationship between having no ASD diagnosis and somatic symptomology. This suggests that additional factors not measured in this study, such as interoceptive sensibility, are contributing to the overall higher somatic symptoms in individuals with ASD more so than individuals without ASD [30], while social anxiety can be attributed to having a slightly larger effect on the presence of somatic symptoms in the non-ASD population, as supported by our moderation analysis. The finding of a notable sex difference in post-hoc analysis, indicating that the correspondence between social anxiety (LSAS) and somatic symptomatology (PHQ) was only true for females subjects, and not males with ASD also suggests that for males with ASD specifically, something other than social anxiety is contributing to somatic symptoms more so than other populations, while highlighting that social anxiety affects the somatic well-being of females with ASD more so than their male counterparts. A review on sex-differences in anxiety disorders suggests that females with generalized anxiety disorder (GAD) experience more somatic symptoms than males with GAD and describes that females tend to experience internalization of their problems more than men [31]. Both anxiety and somatization are internalization problems. It is also therefore possible that due to the distress caused by social anxiety, women with ASD tend to internalize their distress into somatic symptoms more so than men with ASD. As this was not the focus of our study, and research on these sex differences particularly within the ASD population is sparse; thus, this finding calls for more research examining sex differences between somatization of anxiety in people with ASD. Clinical/therapeutic implications would follow from understanding that the link between social anxiety and somatic health is distinct in males and females with ASD.
Regarding practical applications of the data, the results suggest that social anxiety levels could be a promising factor to focus on treating individuals, both with and without ASD, who present with somatic symptoms. An important component of Cognitive Behavioral Treatment of social anxiety focuses on teaching patients to recognize when somatic symptoms are related to or resulting from their anxiety and how to alleviate such symptoms along with relieving their anxiety [32]. There are not many papers assessing the reduction of somatic symptoms in anxiety treatments for the ASD population specifically. While Spek et al. [33] found that similar Mindfulness Based Treatments have reduced a number of co-occurring symptoms including both anxiety and somatic symptoms simultaneously, it is hard to determine the connection or causal relationship between somatic and anxiety symptoms in this study. While we hypothesized that social cognitive differences would contribute to the social anxiety levels and somatic symptoms, the facet of social cognition that was measured in this study did not appear to contribute, suggesting that focusing on compensating for or increasing visual emotion recognition will not be effective in treating social anxiety or somatic symptoms in either population. Other studies have found associations between additional social cognitive skills, namely theory of mind; most studies find stronger correlations between empathic accuracy (which pertains to predicting how a character would feel in a certain scenario), and theory of mind tasks (which pertain to inferring the mental state, desires, and intentions of another person), as opposed to purely visual emotion recognition tasks [14, 15]. The current finding also does not align with previous studies that have found social cognitive skills training helps reduce social anxiety in young people with ASD [34].
Limitations
This study had several limitations that may explain why our findings differed from previous research. Notably, neither social cognition nor somatic symptoms were significantly correlated with an ASD diagnosis. This may be due to limited sensitivity in the measures used and the sample of participants who inherently must be able to read and use a computer independently, which could have reduced detectable group differences. Prior research suggests that some social cognition measures have weaker reliability in non-clinical samples, and that face/emotion processing tasks—used here—tend to show smaller effects than mentalizing tasks, requiring larger samples to detect differences [35]. Additionally, we did not include other social cognition measures like dynamic facial emotion tasks, social relationship vignettes, or theory of mind assessments, which may have been more sensitive [35], nor did we measure identification of nonverbal emotional messaging such as prosodic sensitivity [36,37].
The measurement for somatic symptoms may also have been too broad; perhaps specific somatic symptoms are more common in individuals with ASD, however the measurement used for this study may have been inadequate significantly demonstrate differences between those with and without ASD, although the PHQ has been suggested as a useful measurement for assessing somatic symptoms in individuals with and without autism [38].
Another limitation was the small sample size (N = 61), which limited statistical power. Additionally, all ASD diagnoses were self-reported and not independently verified, and we did not assess for varying trait levels. Since participants needed sufficient reading and cognitive ability to complete the study, our ASD sample likely skewed toward individuals who can read and use their computer independently, limiting generalizability. It is possible that larger differences in social cognitive skills and somatic symptoms would have been found if our study had more variance in the presentation of ASD. Due to the nature of social cognition measurements and self-reported somatic symptom measurements, literature on the correlation to the severity of one’s autism with their social cognitive differences and somatic symptomology is scarce.
An additional methodological consideration involves the use of online survey data to collect responses for this study. One strength of online surveys is that they can increase accessibility and participation, especially among populations who may face challenges with in-person participation, such as individuals with ASD. Online platforms allow for flexible timing, anonymity, and reduced social pressures, which can be particularly helpful when collecting data on sensitive topics like social anxiety and somatic symptoms. Online formats can also streamline data collection across a wide sample reach, increasing generalizability [39]. However, this approach has limitations. It precludes the ability to verify ASD diagnoses through clinical records or standardized diagnostic tools, relying instead on self-report, which may reduce diagnostic accuracy. Additionally, environmental distractions, lack of researcher oversight, and potential misunderstanding of survey instructions can compromise response validity. The use of online surveys also introduces a response bias, selecting only for participants who chose to respond [39]. Response quality and attentiveness may vary, especially for longer surveys, and without a controlled setting, factors such as mood, fatigue, or external influences may bias responses. Finally, those who choose to participate in online surveys may not be representative of the broader ASD population, particularly those with more severe impairments or lower access to technology, which can introduce sampling bias.
Future research should explore whether other forms of anxiety, beyond social anxiety, contribute to somatic symptoms in ASD. It would also be useful to examine different subtypes of social anxiety and their relation to autism and specific somatic complaints. Studying distinct somatic symptoms, rather than somatic symptomology as a whole, could help identify which are most relevant to ASD and more amenable to treatment. Additionally, future work should include participants with a broader range of ASD traits to better understand how these factors interact with anxiety, social cognition, and somatic symptoms.
Author Contributions
Conceptualization, M.D.C. and K.M.S.; data curation, M.D.C. and J.G.; formal analysis, M.D.C; investigation, M.D.C. and J.G.; methodology, M.D.C. and K.M.S.; project administration, M.D.C.; resources, M.D.C., K.M.S., and J.G.; visualization, M.D.C.; writing-original draft, M.D.C.; supervision, K.M.S.; writing-review & editing, K.M.S.
Funding
This research received no external funding.
Institutional Review Board Statement
this research study was approved by the Institutional Review Board of Pace University (OHRP IRB# 0004707/FWA00023526, 08/05/2022) under the status “exempt with limited IRB review” and expired 08/04/2025.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to the necessity to discuss with the research laboratory’s principal investigator. Our consent form for participants stated “Anonymity will be broken only if necessary, within ethical parameters, and will only be accessible by the primary investigator and Advisor. Files will be stored on the investigators’ personal laptops encrypted and inaccessible to anyone other than the research team.
Acknowledgments
The authors wish to thank the members of the Mind, Movement, Interaction and Development (MMID) Lab for assisting with discussion of ideas for this research project. The authors also thank the IT department for assistance with the statistical programs utilized within the study.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ASD | Autism Spectrum Disorder |
| SAD | Social Anxiety Disorder |
| ToM | Theory of Mind |
| DANVA-2 | Diagnostic Analysis of Nonverbal Accuracy--Second Edition |
| LSAS | Liebowitz Social Anxiety Scale |
| PHQ-15 | Patient Health Questionnaire |
| GAD | Generalized Anxiety Disorder |
References
- Ginsburg, G. S.; La Greca, A. M.; Silverman, W. K. Social anxiety in children with anxiety disorders: Relation with social and emotional functioning. J. Abnorm. Child Psychol. 1998, 26(3), 175–185. [Google Scholar] [CrossRef]
- American Psychological Association. APA Dictionary of Psychology. https://dictionary.apa.org/.
- Kim, J. A.; Szatmari, P.; Bryson, S. E.; Streiner, D. L.; Wilson, F. J. The prevalence of anxiety and mood problems among children with autism and Asperger syndrome. Autism 2000, 4(2), 117–132. [Google Scholar] [CrossRef]
- Bellini, S. Social skill deficits and anxiety in high-functioning adolescents with autism spectrum disorders. Focus Autism Other Dev. Disabl. 2004, 19(2), 78–86. [Google Scholar] [CrossRef]
- Bejerot, S.; Eriksson, J. M.; Mörtberg, E. Social anxiety in adult autism spectrum disorder. Psychiatry Res. 2014, 220, 705–707. [Google Scholar] [CrossRef]
- Spain, D.; Sin, J.; Linder, K. B.; McMahon, J.; Happé, F. Social anxiety in autism spectrum disorder: A systematic review. Res. Autism Spectr. Disord. 2018, 52, 51–68. [Google Scholar] [CrossRef]
- Singletary, W. M. An integrative model of autism spectrum disorder: ASD as a neurobiological disorder of experienced environmental deprivation, early life stress and allostatic overload. Neuropsychoanalysis 2015, 17(2), 81–119. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Auyeung, B.; Nørgaard-Pedersen, B.; Hougaard, D. M.; Abdallah, M. W.; Melgaard, L.; Cohen, A. S.; Chakrabarti, B.; Ruta, L.; Lombardo, M. V. Elevated fetal steroidogenic activity in autism. Mol. Psychiatry 2015, 20(3), 369–376. [Google Scholar] [CrossRef] [PubMed]
- Chapman, E.; Baron-Cohen, S.; Auyeung, B.; Knickmeyer, R.; Taylor, K.; Hackett, G. Fetal testosterone and empathy: Evidence from the Empathy Quotient (EQ) and the “reading the mind in the eyes” test. Soc. Neurosci. 2006, 1(2), 135–148. [Google Scholar] [CrossRef]
- Busch, F. N.; Sandberg, L. S. Unmentalized aspects of panic and anxiety disorders. Psychodyn. Psychiatry 2014, 42(2), 175–195. [Google Scholar] [CrossRef]
- Kinnaird, E.; Stewart, C.; Tchanturia, K. Investigating alexithymia in autism: A systematic review and meta-analysis. Eur. Psychiatry 2019, 55, 80–89. [Google Scholar] [CrossRef]
- Lindquist, K. A.; MacCormack, J. K.; Shablack, H. The role of language in emotion: Predictions from psychological constructionism. Front. Psychol. 2015, 6, 444. [Google Scholar] [CrossRef]
- Sossin, K. M. A Movement-Informed Mentalization Lens Applied to Psychodynamic Psychotherapy of Children and Adolescents with High Functioning Autism Spectrum Disorder. J. Infant Child Adolesc. Psychother. 2015, 14(3), 294–310. [Google Scholar] [CrossRef]
- Alvi, T.; Kouros, C. D.; Lee, J.; Fulford, D.; Tabak, B. A. Social Anxiety Is Negatively Associated with Theory of Mind and Empathic Accuracy. J. Abnorm. Psychol. 2020, 129(1), 108–113. [Google Scholar] [CrossRef] [PubMed]
- Hezel, D. M.; McNally, R. J. Theory of Mind Impairments in Social Anxiety Disorder. Behav. Ther. 2014, 45(4), 530–540. [Google Scholar] [CrossRef] [PubMed]
- Apperly, I. Can Theory of Mind Grow Up? Mindreading in Adults, and Its Implications for the Development and Neuroscience of Mindreading. In Understanding Other Minds: Perspectives from Developmental Social Neuroscience; Oxford University Press: Oxford, U.K, 2013. [Google Scholar] [CrossRef]
- Metcalfe, D.; McKenzie, K.; McCarty, K.; Pollet, T. V. Emotion Recognition from Body Movement and Gesture in Children with Autism Spectrum Disorder Is Improved by Situational Cues. Res. Dev. Disabil. 2019, 86, 1–10. [Google Scholar] [CrossRef]
- White, S. W.; Bray, B. C.; Ollendick, T. H. Examining Shared and Unique Aspects of Social Anxiety Disorder and Autism Spectrum Disorder Using Factor Analysis. J. Autism Dev. Disord. 2012, 42(5), 874–884. [Google Scholar] [CrossRef] [PubMed]
- Zukerman, G.; Yahav, G.; Ben-Itzchak, E. The Gap between Cognition and Adaptive Behavior in Students with Autism Spectrum Disorder: Implications for Social Anxiety and the Moderating Effect of Autism Traits. J. Autism Dev. Disord. 2021, 51(5), 1466–1478. [Google Scholar] [CrossRef]
- Sackl-Pammer, P.; Özlü-Erkilic, Z.; Jahn, R.; et al. Somatic Complaints in Children and Adolescents with Social Anxiety Disorder. Neuropsychiatr. 2018, 32(4), 187–195. [Google Scholar] [CrossRef]
- Doshi-Velez, F.; Avillach, P.; Palmer, N.; et al. Prevalence of Inflammatory Bowel Disease among Patients with Autism Spectrum Disorders. Inflamm. Bowel Dis. 2015, 21(10), 2281–2288. [Google Scholar] [CrossRef]
- Greenspan, S. I.; Wieder, S. The Developmental Individual-Difference, Relationship-Based (DIR/Floortime) Model Approach to Autism Spectrum Disorders. In Clinical Manual for the Treatment of Autism; Hollander, E., Anagnostou, E., Eds.; American Psychiatric Publishing: Washington, DC, 2007; pp. 179–209. [Google Scholar]
- Pan, P. Y.; Tammimies, K.; Bölte, S. The Association between Somatic Health, Autism Spectrum Disorder, and Autistic Traits. Behav. Genet. 2020, 50(4), 233–246. [Google Scholar] [CrossRef]
- Thamby, A.; Desai, G.; Mehta, U. M.; Chaturvedi, S. K. Deficits in Theory of Mind and Emotional Awareness in Somatoform Disorders. Indian J. Psychol. Med. 2019, 41(4), 368–374. [Google Scholar] [CrossRef]
- Nowicki, S.; Carton, J. The Measurement of Emotional Intensity from Facial Expressions. J. Soc. Psychol. 1993, 133(5), 749–750. [Google Scholar] [CrossRef]
- Liebowitz, M. R. Social Phobia. Mod. Probl. Pharmacopsychiatry 1987, 22, 141–173. [Google Scholar] [CrossRef]
- Heimberg, R. G.; Horner, K. J.; Juster, H. R.; et al. Psychometric Properties of the Liebowitz Social Anxiety Scale. Psychol. Med. 1999, 29(1), 199–212. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R. L.; Williams, J. B. The PHQ-15: Validity of a New Measure for Evaluating the Severity of Somatic Symptoms. Psychosom. Med. 2002, 64(2), 258–266. [Google Scholar] [CrossRef]
- Pickard, H.; Hirsch, C.; Simonoff, E.; Happé, F. Exploring the Cognitive, Emotional and Sensory Correlates of Social Anxiety in Autistic and Neurotypical Adolescents. J. Child Psychol. Psychiatry 2020, 61(12), 1317–1327. [Google Scholar] [CrossRef]
- Zdankiewicz-Ścigała, E.; Ścigała, D.; Sikora, J.; Kwaterniak, W.; Longobardi, C. Relationship between Interoceptive Sensibility and Somatoform Disorders in Adults with Autism Spectrum Traits: The Mediating Role of Alexithymia and Emotional Dysregulation. PLoS One 2021, 16(8), e0255460. [Google Scholar] [CrossRef]
- Jalnapurkar, I. Sex Differences in Anxiety Disorders: A Review. Psychiatry Depress. Anxiety 2018, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aydin, A.; Tekinsav Sütcü, S.; Sorias, O. Ergenlerde Sosyal Anksiyete Belirtilerini Azaltmaya Yönelik Bilişsel-Davranışçı Bir Grup Terapisi Programının Etkililiğinin Değerlendirilmesi. Turk. Psikiyatri Derg. 2010, 21(1), 25–36. [Google Scholar] [PubMed]
- Spek, A. A.; van Ham, N. C.; Nyklíček, I. Mindfulness-Based Therapy in Adults with an Autism Spectrum Disorder: A Randomized Controlled Trial. Res. Dev. Disabil. 2013, 34(1), 246–253. [Google Scholar] [CrossRef] [PubMed]
- Maskey, M.; Lowry, J.; Rodgers, J.; McConachie, H.; Parr, J. R. Reducing Specific Phobia/Fear in Young People with Autism Spectrum Disorders (ASDs) through a Virtual Reality Environment Intervention. PLoS One 2014, 9(7), e100374. [Google Scholar] [CrossRef]
- Morrison, K. E.; Pinkham, A. E.; Kelsven, S.; Ludwig, K.; Penn, D. L.; Sasson, N. J. Psychometric Evaluation of Social Cognitive Measures for Adults with Autism. Autism Res. 2019, 12(5), 766–778. [Google Scholar] [CrossRef]
- Charpentier, J.; Kovarski, K.; Houy-Durand, E.; et al. Emotional Prosodic Change Detection in Autism Spectrum Disorder: An Electrophysiological Investigation in Children and Adults. J. Neurodev. Disord. 2018, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Haigh, S. M.; Brosseau, P.; Eack, S. M.; Leitman, D. I.; Salisbury, D. F.; Behrmann, M. Hyper-Sensitivity to Pitch and Poorer Prosody Processing in Adults with Autism: An ERP Study. Front. Psychiatry 2022, 13, 844830. [Google Scholar] [CrossRef]
- Arnold, S. R.; Uljarević, M.; Hwang, Y. I.; Richdale, A. L.; Trollor, J. N.; Lawson, L. P. Brief Report: Psychometric Properties of the Patient Health Questionnaire-9 (PHQ-9) in Autistic Adults. J. Autism Dev. Disord. 2020, 50(6), 2217–2225. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, E.; Furnier, S. #Bias: The Opportunities and Challenges of Surveys That Recruit and Collect Data of Autistic Adults Online. Autism Adulthood 2021, 3(2), 120–128. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The significant linear correlation between social anxiety as measured by the LSAS and somatic symptoms as measured by the PHQ-15.
Figure 1.
The significant linear correlation between social anxiety as measured by the LSAS and somatic symptoms as measured by the PHQ-15.
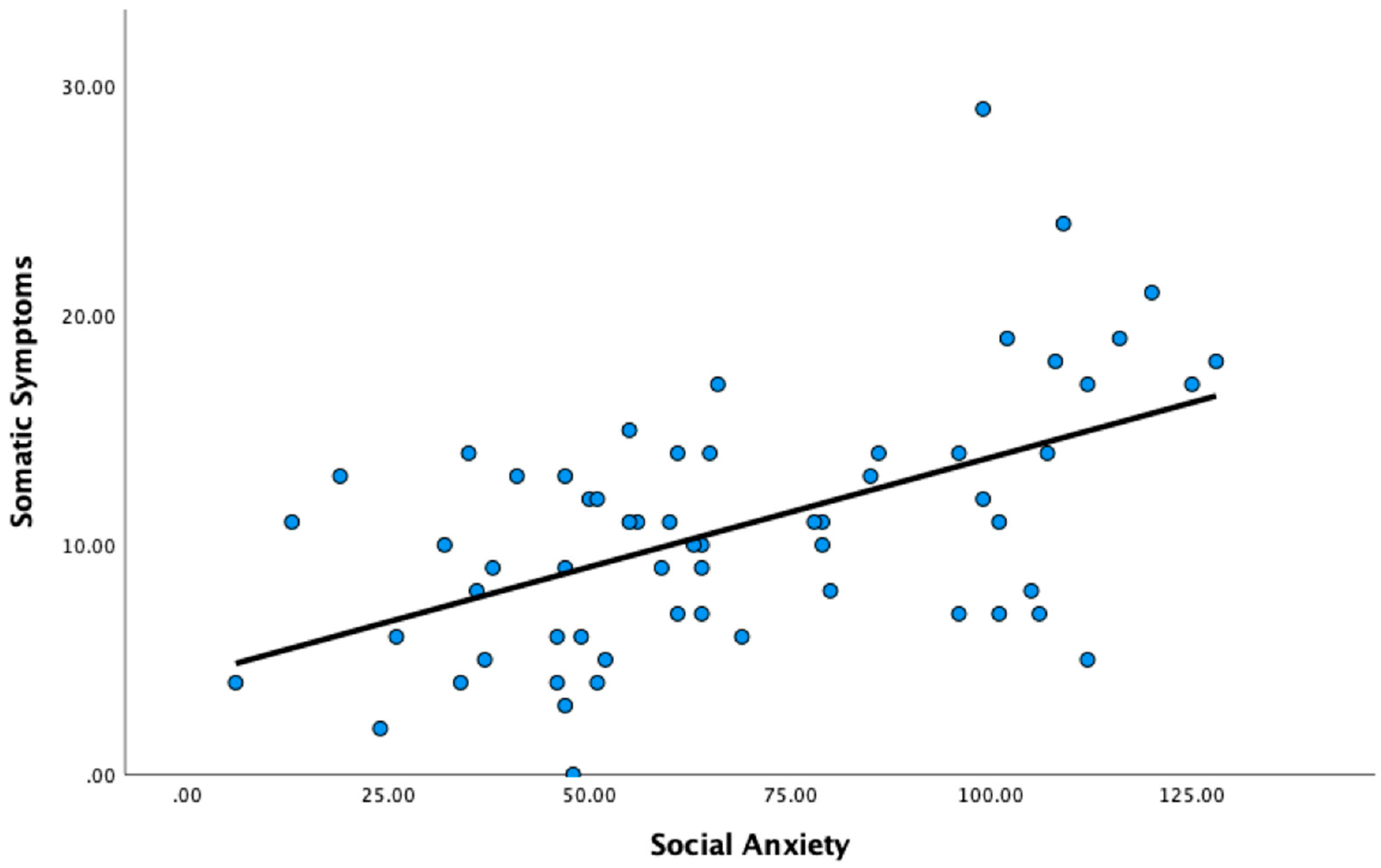
Figure 2.
The mediation analysis with LSAS (social anxiety) as the mediator between ASD and somatic symptoms as measured by the PHQ-15 with beta coefficient values indicated; as per Hayes, the coefficient value within parentheses indicates the value once social anxiety as measured by the LSAS is considered as the mediator. *p <.05, **p<.01.
Figure 2.
The mediation analysis with LSAS (social anxiety) as the mediator between ASD and somatic symptoms as measured by the PHQ-15 with beta coefficient values indicated; as per Hayes, the coefficient value within parentheses indicates the value once social anxiety as measured by the LSAS is considered as the mediator. *p <.05, **p<.01.
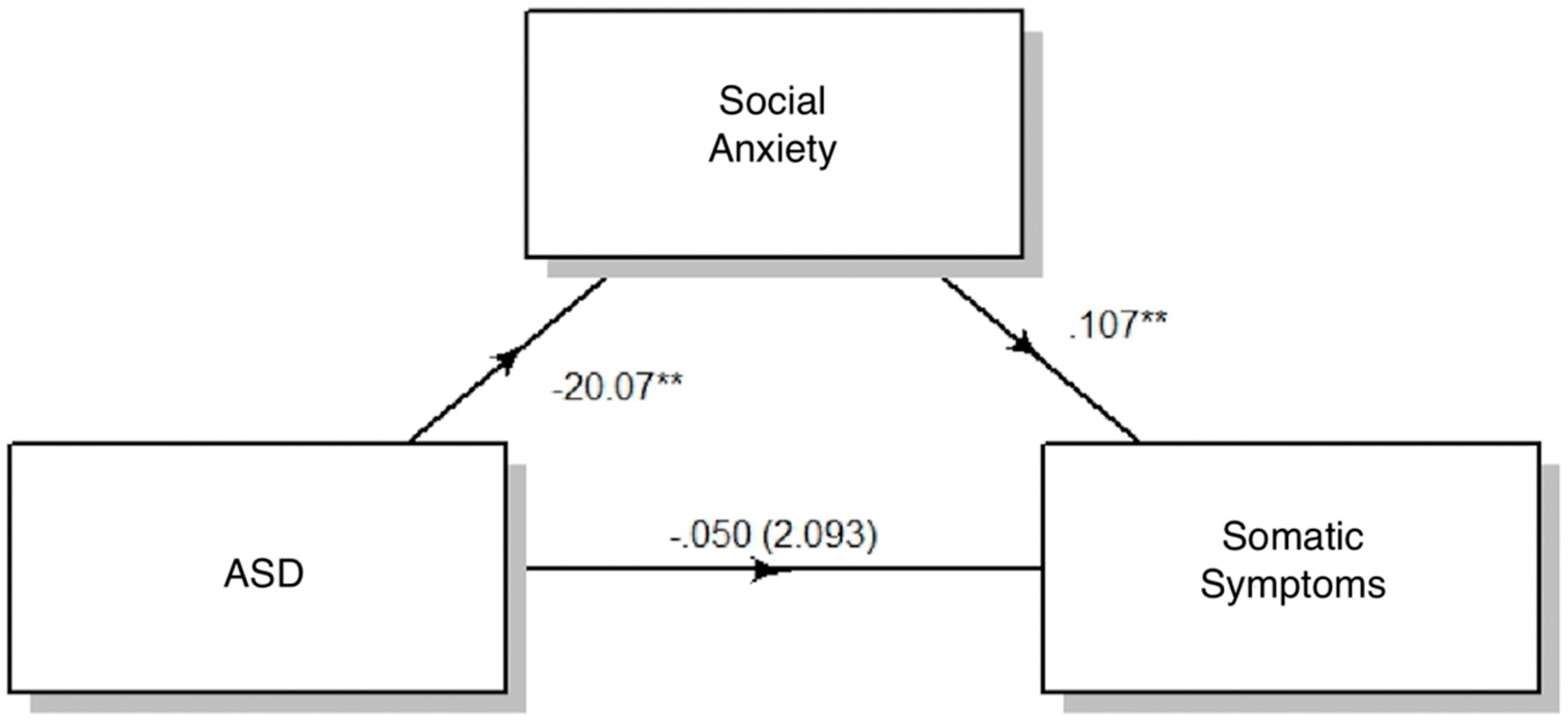
Figure 3.
ASD diagnosis as a moderator for the relationship between somatic symptoms as measured by the PHQ-15 and social anxiety as measured by the LSAS.
Figure 3.
ASD diagnosis as a moderator for the relationship between somatic symptoms as measured by the PHQ-15 and social anxiety as measured by the LSAS.
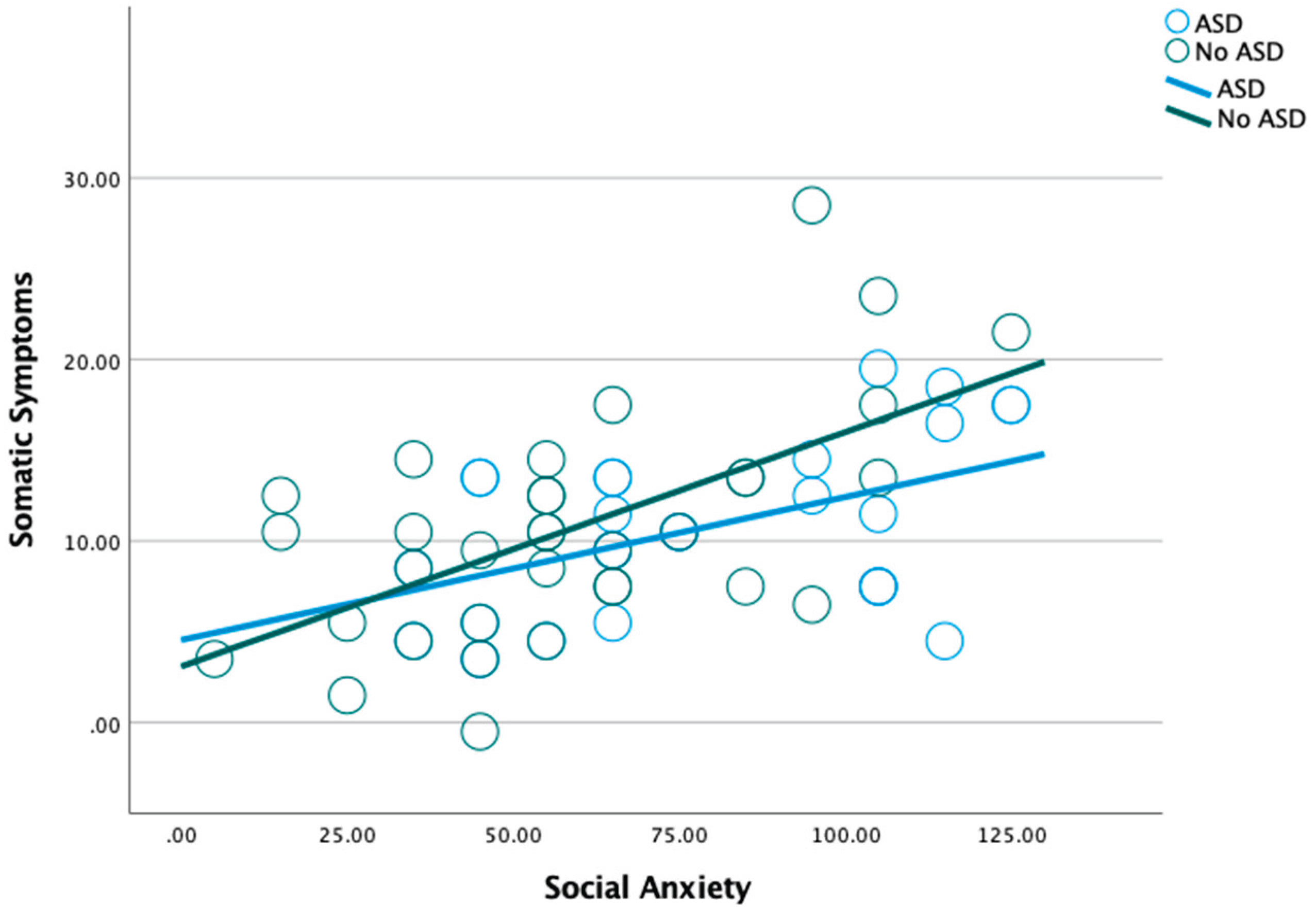

Table 1.
Correlations Between the Four Main Variables (ASD diagnosis, LSAS total score, PHQ total score, DANVA-2 Total score).
Table 1.
Correlations Between the Four Main Variables (ASD diagnosis, LSAS total score, PHQ total score, DANVA-2 Total score).
| ASD | LSAS Total | PHQ Total | DANVA-2 Total | ||
|---|---|---|---|---|---|
| ASD | Pearson Correlation | 1 | -.328** | -.005 | .035 |
| Significance | .010 | .972 | .791 | ||
| (N) | 61 | 61 | 61 | 61 | |
| LSAS Score | Pearson Correlation | -3.28** | 1 | .533** | -.060 |
| Significance | .010 | <.001 | .645 | ||
| (N) | 61 | 61 | 61 | 61 | |
| PHQ Score | Pearson Correlation | -.005 | .533** | 1 | .086 |
| Significance | .972 | <.001 | .508 | ||
| (N) | 61 | 61 | 61 | 61 | |
| DANVA-2 Score | Pearson Correlation | -.035 | -.060 | .086 | 1 |
| Significance | .791 | .645 | .508 | ||
| (N) | 61 | 61 | 61 | 65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



