
Submitted:
09 September 2025
Posted:
10 September 2025
You are already at the latest version
Abstract
This study investigated the effectiveness of a structured recreational training program in enhancing psychological well-being and reducing prevalent motor behaviors among children with Autism Spectrum Disorder (ASD). An experimental pre-test/post-test design was applied to a purposive sample of eight children with ASD (aged 6–12 years) enrolled at the Jude Institute for Special Education. The intervention spanned eight weeks, with three training sessions per week, and was evaluated through both caregiver-reported psychological assessments and systematic video-based observation of motor behaviors. Ten caregivers participated in the evaluation process using stand-ardized pre- and post-intervention questionnaires. Motor behaviors were quantified from surveillance recordings, focusing on the frequency of specific actions. Statistical analysis using paired-samples t-tests revealed significant reductions in aggressive and irrational behaviors, alongside marked improvements in social communication. Like-wise, repetitive motor patterns—including spinning, hand flapping, clapping, rocking, foot tapping, noise-triggered ear covering, and inappropriate object use—showed sub-stantial declines. These findings highlight the potential of recreational training as a vi-able, non-invasive approach to improving socio-emotional and motor outcomes in children with ASD. Incorporating such programs into rehabilitation frameworks within special education contexts could offer meaningful support for the holistic de-velopment of this population.
Keywords:
psychological variables
; recreational training programs
; Autism Spectrum Disorder
; motor behaviors
; special education
1. Introduction
Autism Spectrum Disorder (ASD) is a lifelong neurodevelopmental condition characterized by persistent deficits in social communication and interaction, accompanied by restricted, repetitive patterns of behavior, interests, or activities [1,2,3]. These symptoms typically emerge in early childhood and may vary in presentation and severity, making ASD a heterogeneous condition. Globally, the prevalence of ASD has increased over the past two decades, with recent estimates suggesting that approximately 1 in 100 children are affected [1,2,3].
This upward trend has heightened the urgency for effective, evidence-based interventions that address the multifaceted challenges faced by children with ASD and their families.
Children with ASD frequently experience delays or atypical patterns in cognitive, social, and motor development [4,5]. Difficulties in initiating and maintaining reciprocal social interactions, alongside impairments in imaginative and exploratory play, are common [6,7]. They may engage with objects in a non-purposeful, repetitive manner, limiting opportunities for creativity and adaptive skill acquisition. Motor impairments often manifest as stereotyped movements—such as hand flapping, spinning, repetitive clapping, or rocking—combined with a strong adherence to routines and resistance to change [8,9]. These patterns can be accompanied by emotional and behavioral challenges, including aggression, self-injury, tantrums, and non-compliance [10]. Collectively, these factors can significantly reduce a child’s ability to participate in daily activities, thus influencing their quality of life and placing substantial emotional and logistical burdens on caregivers [10].
Emerging research emphasizes the potential of physical activity interventions—particularly structured recreational programs—to support psychological well-being and motor development in children with ASD. Recreational training offers a safe, engaging, and non-invasive approach that integrates physical exercise with therapeutic objectives, making it suitable for a wide range of ability levels. Unlike purely clinical interventions, recreational activities are inherently motivating and socially oriented, providing opportunities for sensory regulation, skill-building, and peer interaction [8,9]. They can target both maladaptive behaviors and deficits in motor coordination through structured routines, adaptable challenges, and enjoyable tasks [8,9].
Several studies have reported benefits of adapted physical activity for individuals with ASD. Previous studies found that small games and recreational exercises reduced social withdrawal and improved social communication [11,12], while others reported enhanced balance, concentration, and reduced psychological stress following sport-based interventions [13,14]. Physical activity has also been shown to improve sensory processing and attentional control, contributing to reduced frequency of stereotyped behaviors [15]. Furthermore, Estabillo identified a link between stereotyped behaviors and underlying emotional regulation difficulties, suggesting that interventions which enhance mood stability may concurrently reduce such behaviors [16]. In addition, Mehmet Ilkım found that. aerobic exercise interventions, for example, have been associated with improved mood regulation and fewer episodes of anger in children with ASD [17].
Theoretical frameworks help explain these observed effects. Sensory Integration Theory posits that structured physical activity can improve the brain’s ability to process and respond to sensory input, thereby reducing maladaptive motor responses [18,19]. From a neurobiological perspective, exercise has been linked to neuroplastic changes, increased endorphin release, and improved autonomic regulation—all of which can positively influence mood, attention, and motor coordination [20,21]. Social Learning Theory further suggests that structured group activities can enhance social skills through modeling, reinforcement, and repeated practice in a supportive environment [22,23].
Despite the promising evidence, the majority of existing research has been conducted in Western or high-income contexts, often within school-based or clinical rehabilitation programs. Studies in low- and middle-income countries, particularly in the Arab region, remain limited [24,25]. In Palestine, localized research exploring the psychological and motor benefits of recreational-based interventions for children with ASD remains notably scarce. Academic studies have largely focused on traditional therapeutic modalities—such as parent training and behavioral therapy (e.g., IY-ASD in Nablus; behavioral programs in Hebron) and qualitative work on family-cultural dynamics [26,27]. While NGOs like Autism Superhero Palestine and the Gaza Community Mental Health Programme offer enriched recreational experiences (e.g., art therapy, hydrotherapy, animal-assisted therapy, summer camps), these initiatives lack systematic evaluation [28]. The absence of peer-reviewed evidence limits understanding of how cultural, infrastructural, and resource-related factors influence the feasibility and efficacy of such programs in the Palestinian context [29,30].
The present study responds to this gap by evaluating the impact of a structured recreational training program on both psychological variables (aggressive behavior, irrational behavior, and social communication) and common repetitive motor behaviors among children with ASD in Palestine. The program was designed to be contextually appropriate, drawing on the researcher’s professional experience in multiple sports disciplines—including karate, football, and swimming—and on direct engagement with children with ASD in educational and recreational settings. By integrating sport-based activities into a structured therapeutic framework, this intervention seeks to combine the motivational benefits of play with evidence-based strategies for behavior and skill development.
The study’s central hypothesis is that participation in the recreational training program will result in statistically significant improvements in the targeted psychological and motor outcomes. More specifically, it is expected that children will demonstrate reduced aggressive and irrational behaviors, enhanced social communication, and decreased frequency of repetitive motor patterns such as spinning, hand flapping, and rocking. In addition to its scientific contribution, this research aims to provide a practical, replicable model that can be implemented in special education centers and rehabilitation programs in Palestine and similar contexts.
By situating recreational training within a broader framework of developmental support for children with ASD, this study contributes to the growing body of literature advocating for holistic, multidimensional approaches to intervention. It also addresses the need for culturally relevant evidence that can inform policy, resource allocation, and community engagement in support of this vulnerable population.
2. Materials and Methods
2.1 Study Design
A single-group pre-test/post-test experimental design was employed to examine the effectiveness of recreational training units on selected psychological variables and motor behaviors in children with Autism Spectrum Disorder (ASD). This design enabled direct comparison of pre-intervention and post-intervention measurements, allowing assessment of within-group changes.
2.2. Participants
The study sample was drawn from the Jude Institute for Special Education (Ramallah and Al-Bireh, Palestine).
- Children with ASD: Fifteen children (ages 6–12 years) diagnosed by qualified physicians and psychologists, enrolled at the Jude Institute for Special Education (Ramallah and Al-Bireh, Palestine). From this population, ten children were purposively selected based on inclusion criteria: confirmed diagnosis of moderate ASD, regular attendance, absence of additional physical or cognitive impairments, ability to participate in training, and presence of clear motor behavior challenges.
- Caregivers: Ten female caregivers working at the same institute, all with direct daily contact with the selected children were recruited via comprehensive sampling to assess psychological variables via questionnaires.
Table 1 presents the demographic and anthropometric characteristics of the children, confirming sample homogeneity (skewness values within ±1).
2.3. Ethical Considerations
Official permission to conduct the study was obtained from the head of the academic department and the administration of Jude Institute. Written informed consent was secured from the children’s legal guardians.
2.4. Variables
- Independent Variable: Recreational training units program.
-
Dependent Variables:
- ⚬
- Psychological variables: Aggressive behavior, irrational behavior, and social communication.
- ⚬
- Motor behaviors: Eight of the most common stereotypical behaviors among the sample, identified via preliminary observation and video analysis (spinning in circles, hand flapping, repetitive clapping, jumping in place, rocking back and forth, repetitive foot tapping, covering ears when exposed to loud sounds, inappropriate object use).
2.5. Instruments
- Psychological Variables Scale: Adapted from recently published studies, containing 21 negatively worded items across three subscales (aggressive behavior, irrational behavior, social communication). Responses were rated on a 3-point Likert scale: always (3), sometimes (2), rarely (1) [31,32,33]. Content validity was confirmed by expert review, and reliability coefficients (ICC) ranged from 0.89 to 0.95.
- Motor Behavior Observation Protocol: Developed through a three-phase process—review of institutional behavioral records, direct classroom observation, and CCTV video analysis. Inter-rater reliability (ICC) ranged from 0.88 to 0.94 across behaviors.
2.6 Intervention – Recreational Training Units Program
The intervention consisted of 24 structured recreational training sessions delivered over 8 weeks (three sessions/week, each lasting 60 minutes). Sessions were conducted in a classroom equipped for physical activity, under the supervision of the researcher (Sundays and Thursdays) and a trained caregiver (Tuesdays).
- Warm-up (12 min): Story-based movement activities to engage attention.
- Main part (40 min): Targeted physical and play-based exercises designed to reduce specific motor stereotypies, incorporating progressive difficulty and variety (e.g., balancing games, guided ball activities, interactive group tasks).
- Cool-down (8 min): Breathing and relaxation exercises.
Program design followed principles of safety, progression, and suitability for children with ASD. Intensity was moderate (<65% maximum effort), with adaptations as needed.
2.7. Pilot Study
A pilot test (29 February–9 March 2025) with five non-study children with ASD was conducted to ensure feasibility, adjust activity durations, confirm equipment suitability, and assess safety measures.
2.8. Data Collection Procedures
-
Pre-test:
- ⚬
- Psychological variables: caregiver questionnaires administered on 10 March 2025.
- ⚬
- Motor behaviors: video-recorded observation sessions from 3–9 March 2025, one hour/day for seven days.
- Intervention: Implementation of the recreational units from 11 March to 11 May 2025.
-
Post-test:
- ⚬
- Psychological variables: questionnaires administered on 12 May 2025.
- ⚬
- Motor behaviors: video-recorded observation sessions from 12–21 May 2025, identical in timing and duration to pre-test procedures.
2.9. Equipment and Materials
- Physical activity equipment: plastic balls (n=10), small colored balls (n=10), balloons (various sizes/colors), hoops (various sizes/colors), adhesive tapes (5 cm width, various colors), whistle (n=1), building blocks (LEGO), double-surface exercise mats (n=2), chalk, measuring tape.
- Recording and timing devices: two Smart Cameras for continuous observation, stopwatch, medical scale, Casio calculator.
2.10. Reliability and Validity
Inter-rater reliability was assessed via Intraclass Correlation Coefficient (ICC) using data from a separate sample (n=5). Table 2 and Table 3 present the reliability and self-validity coefficients for psychological and motor behavior measures, respectively, confirming high reliability (ICC range: 0.88–0.95, p<0.05).
2.11. Data Analysis
Data were coded and analyzed using IBM SPSS Statistics v.25. Descriptive statistics (means, standard deviations, skewness) were calculated. Reliability was assessed via Intraclass Correlation Coefficient (ICC). Differences between pre- and post-test means were analyzed using paired samples t-test, with significance set at α ≤ 0.05. Percentage change was computed as:
2.12. Generative Artificial Intelligence (GenAI)
Generative artificial intelligence tools (ChatGPT, GPT-5) were employed exclusively for linguistic refinement and structural formatting of the Materials and Methods section to ensure compliance with the MDPI Psychology journal guidelines. These tools were not utilized for data generation, statistical analyses, study design, or interpretation of research findings.
3. Results
The analysis revealed significant improvements in both psychological variables and motor behaviors among children with ASD following the implementation of the recreational training units.
3.1. Psychological Variables
Paired samples t-tests indicated statistically significant reductions in all measured psychological variables between pre-test and post-test scores (Table 4). Specifically, aggressive behavior decreased by 38.93%, irrational behavior by 50.40%, and social communication avoidance by 40.54%. The overall composite psychological score showed a 43.56% reduction (p < 0.001 for all).
These results are illustrated in Figure 1, which show consistent post-intervention declines in mean scores across all psychological domains.
The magnitude of these improvements suggests that the program effectively addressed emotional regulation and social interaction challenges, potentially by providing structured, engaging, and socially reinforcing activities that promoted self-control and reduced maladaptive responses.
3.2. Motor Behaviors
All eight targeted repetitive motor behaviors showed statistically significant reductions after the intervention (Table 5). The most pronounced decrease was observed in “covering ears when exposed to loud sounds or music” (59.25% reduction), followed by “inappropriate object use” (26.47% reduction), “repetitive clapping” (19.40% reduction), and “spinning/circling” (15.79% reduction). Other behaviors, including hand flapping, jumping in place, rocking back and forth, and foot tapping, also showed meaningful declines (p < 0.05 for all).
Figure 2, Figure 3, Figure 4 and Figure 5 visually depict these trends, highlighting consistent post-intervention decreases in frequency for each motor behavior.
The targeted design of the recreational units—linking specific physical activities to individual behaviors—appears to have facilitated these improvements. For example, balance and direction-following games effectively substituted for spinning, while fine-motor and object-manipulation tasks redirected hand flapping into purposeful actions.
4. Discussion
The present study examined the effects of an eight-week recreational training units program on selected psychological variables—aggressive behavior, irrational behavior, and social communication—as well as on the most common motor behaviors in children with ASD. The findings revealed statistically significant improvements in both domains, confirming the study hypotheses and aligning with existing evidence supporting structured physical activity as a therapeutic tool for children with developmental disorders.
4.1. Psychological Outcomes
The results, as presented in Table 4 and illustrated in Figure 1 A and B in the Results section, demonstrated substantial reductions in aggressive behavior, irrational behavior, and social communication difficulties, with percentage decreases ranging from −38.93% to −50.40%. The composite psychological score also improved markedly (−43.56%). These improvements likely stem from the program’s intentional integration of cooperative games, positive reinforcement, and a safe, structured environment that fosters emotional security and trust.
These findings are consistent with previous studies [34,35], who reported similar reductions in aggression and improvements in social engagement following adapted physical activity interventions. Likewise, Sarabzadeh and Toscano highlighted the role of targeted physical activities in promoting self-regulation [36,37], while others demonstrated the potential of recreational programs to enhance non-verbal communication skills. Together, these converging results suggest that the social and psychological benefits of structured recreational activities may be replicable across cultural and institutional contexts when programs are appropriately adapted [38,39].
4.2. Motor Behavior Outcomes
The analysis of motor behaviors (Table 5; Figure 2, Figure 3 and Figure 4, A-H) revealed significant reductions across all eight targeted stereotypical movements, with the largest decrease observed in covering ears when exposed to loud sounds or music (−59.25%) and notable improvements in inappropriate object use (−26.47%) and repetitive clapping (−19.40%). Even behaviors with smaller relative changes, such as rocking (−8.80%) and repetitive foot tapping (−7.08%), showed statistically significant improvement.
These outcomes support the hypothesis that recreational units, designed to redirect stereotypical motor patterns into purposeful, goal-directed activities, can effectively reduce maladaptive behaviors. This aligns with other studies that found that increased engagement in structured physical activity reduced stereotypical movements in individuals with ASD. The program’s use of progressive task complexity, sensory-rich materials, and activity variation likely enhanced motor control, attention, and sensory integration, further contributing to the observed behavioral changes [8,9,40].
4.3. Broader Implications
By addressing both psychological and motor domains, recreational training units offer a dual-benefit intervention strategy for children with ASD. On a psychosocial level, improvements in emotional regulation and social communication can enhance peer relationships, classroom participation, and family interactions. On a functional level, reductions in repetitive behaviors may facilitate engagement in everyday tasks, thereby promoting independence and improving overall quality of life. These combined benefits underscore the value of integrating structured recreational interventions into special education and rehabilitation programs.
4.4. Limitations
While the results are promising, several limitations must be considered when interpreting the findings:
The study included only ten children from a single institution in Palestine, which limits statistical power and generalizability across broader ASD populations with varying cultural, socio-economic, and linguistic backgrounds [41,42]. Without a non-intervention or alternative-intervention group, it is not possible to conclusively attribute the observed changes solely to the program, as maturation or increased caregiver engagement could also contribute to improvements [43,44].
The eight-week program length was adequate to detect short-term changes but insufficient to evaluate whether improvements were sustained. No long-term follow-up data were collected, consistent with gaps reported in previous ASD intervention studies [45,46]. Psychological variables were based on caregiver questionnaires, which may be subject to expectation bias, and motor behaviors were recorded during scheduled observation periods, potentially missing variability in behavior across different times and contexts [47,48].
The presence of cameras and heightened researcher–caregiver interaction may have influenced participant behavior, leading to short-term performance improvements (Hawthorne effect) [49]. Additionally, the program was tailored to the resources and environment of the Jude Institute, including specialized equipment and trained facilitators. Feasibility in less resource-rich settings remains untested [50,51].
Although the sample was restricted to moderate ASD cases, individual variations in cognitive ability, sensory sensitivity, and comorbid conditions may have influenced responsiveness to the intervention. These were not analyzed separately, and subgroup-specific patterns may have been masked [47,52].
These limitations highlight that, while encouraging, the results should be interpreted as preliminary evidence rather than definitive proof of the program’s effectiveness.
4.5. Future Research Directions
Building on the findings of the present study, future research should aim to strengthen the evidence base for recreational training units as an intervention for children with ASD by adopting more rigorous and inclusive research designs. Large-scale, randomized controlled trials conducted across multiple institutions and geographic regions would provide the statistical power and diversity needed to generalize findings beyond the current, context-specific sample [46,54]. Such trials should deliberately recruit participants from a range of socio-economic, cultural, and linguistic backgrounds, thereby ensuring that the intervention’s effectiveness is tested in varied real-world settings [55,56].
Long-term follow-up is particularly crucial. While the current results are encouraging, they only capture short-term outcomes immediately after the eight-week program. Subsequent studies should track participants for several months or even years after the intervention to determine whether improvements in psychological and motor domains are sustained over time or require ongoing reinforcement [46,57]. Longitudinal designs could also shed light on the developmental trajectory of children who participate in structured recreational programs, potentially revealing cumulative benefits that extend into adolescence [58,59].
In addition, further investigation into the specific components of recreational training units could yield valuable insights. The program used in this study integrated a variety of activities, ranging from cooperative games to sensory-motor challenges. Future research could systematically isolate and compare these elements to determine which are most effective for reducing particular types of repetitive behaviors or for enhancing specific psychological variables such as emotional regulation or social communication [60,61]. Such work could enable the creation of tailored intervention packages for children with different ASD profiles.
The incorporation of technology into recreational interventions presents another promising avenue. Tools such as virtual reality, interactive motion-sensing games, and wearable devices for movement tracking could enhance engagement, provide objective feedback, and allow for real-time adjustments to activity difficulty [62,63]. Technology could also facilitate remote delivery, making interventions more accessible in areas where trained personnel or specialized facilities are limited [64,65].
Furthermore, it would be valuable to explore the role of caregivers and educators not merely as observers but as active facilitators of recreational units. Training non-specialist staff to deliver the program could test whether similar benefits can be achieved without direct researcher supervision, thereby increasing the scalability of the intervention [66,67]. This approach could also foster stronger home–school continuity, with families able to reinforce learned skills in daily routines [68,69].
Finally, future studies should examine how individual differences within the ASD population—such as severity of symptoms, cognitive ability, sensory processing patterns, or presence of comorbid conditions—influence responsiveness to recreational programs. Stratified analyses could reveal which subgroups benefit most from specific activities, enabling more personalized, effective, and efficient intervention planning [70,71].
By addressing these lines of inquiry, future research can move from demonstrating preliminary efficacy to establishing robust, contextually adaptable models for recreational training units. Such models have the potential to become an integral part of comprehensive care strategies for children with ASD worldwide, promoting not only motor and psychological improvements but also long-term inclusion, independence, and quality of life.
5. Conclusions
The present study demonstrated that an eight-week structured recreational training program produced significant improvements in both psychological and motor outcomes among children with ASD in a Palestinian special education setting. Specifically, the intervention was associated with marked reductions in aggressive and irrational behaviors, improvements in social communication, and notable decreases in the frequency of common repetitive motor patterns. These findings suggest that recreational training can serve as an effective, engaging, and culturally adaptable non-pharmacological intervention targeting multiple developmental domains simultaneously.
The integration of such programs into rehabilitation and educational frameworks may offer meaningful benefits, particularly in resource-limited contexts where access to specialized therapeutic services is constrained. Nevertheless, given the small sample size, absence of a control group, and short follow-up period, the results should be interpreted with caution. Further research employing larger, multi-center samples, randomized controlled designs, and long-term follow-up is recommended to confirm these findings, examine their sustainability, and identify the most effective program components for different ASD profiles.
Supplementary Materials
N.A
Author Contributions
G.T., A.M.T., O.D., D.K., T.R. and R.A. wrote and edited the manuscript. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
N.A.
Informed Consent Statement
N.A.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request. Access to the datasets is restricted to protect the privacy and confidentiality of participating children, in accordance with the ethical requirements of the Jude Institute for Special Education.
Acknowledgments
The authors would like to express their sincere gratitude to the Jude Institute for Special Education (Ramallah and Al-Bireh, Palestine) for their valuable support and cooperation in facilitating the implementation of this study. Generative artificial intelligence tools (ChatGPT, GPT-5) were employed exclu-sively for linguistic refinement and structural formatting of the Materials and Methods section to ensure compliance with the MDPI Psychology journal guidelines. These tools were not utilized for data generation, statistical analyses, study design, or inter-pretation of research findings.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviation used in this manuscript:
| ASD | Autism Spectrum Disorder |
| ICC | Intraclass Correlation Coefficient |
| CCTV | Closed-Circuit Television |
| WHO | World Health Organization |
References
- Robert Jason Grant. Chapter 13: Play Therapy for Children with autism Spectrum Disorder. In Prescriptive play therapy : tailoring interventions for specific childhood problems; The Guilford Press: New York, United States of America, 2019; pp 213–230.
- Natasha Marrus; John Constantino. Chapter 8: Autism Spectrum Disorder. In Handbook of Preschool Mental Health: Development, Disorders, and Treatment; The Guilford Press: New York, United States of America, 2016; pp 187–219.
- DAWN LEE GARZON; NANCY BARBER STARR; JENNIFER CHAUVIN. Chapter 29: Neurodivergence and Behavioral and Mental Health Disorders. In Burns’ Pediatric Primary Care; Evolve-Elsevier, 2024; pp 419–455.
- S, J.; Arumugam, N.; Parasher, R. K. Effect of physical exercises on attention, motor skill and physical fitness in children with attention deficit hyperactivity disorder: a systematic review. ADHD Attention Deficit and Hyperactivity Disorders 2018, 11 (2), 125–137. [CrossRef]
- Pan, C.-Y.; Tsai, C.-L.; Chu, C.-H.; Sung, M.-C.; Huang, C.-Y.; Ma, W.-Y. Effects of physical exercise intervention on motor skills and executive functions in children with ADHD: a pilot study. Journal of Attention Disorders 2015, 23 (4), 384–397. [CrossRef]
- Bucik, K.; Vitulić, H. S.; Pavel, J. R. Effects of dance-movement therapy on the movement and self-concept of wheelchair users with intellectual disabilities. Hrvatska Revija Za Rehabilitacijska Istraživanja 2023, 59 (1), 59–76. [CrossRef]
- Reed, A. S. Mental health, availability to participate in social change, and social movement accessibility. Social Science & Medicine 2022, 313, 115389. [CrossRef]
- Yang, J.; Li, R. Systematic review and randomized controlled trial meta-analysis of the effects of physical activity interventions and their components on repetitive stereotyped behaviors in patients with autism spectrum disorder. Frontiers in Psychology 2025, 16. [CrossRef]
- Ferreira, J. P.; Ghiarone, T.; Júnior, C. R. C.; Furtado, G. E.; Carvalho, H. M.; Machado-Rodrigues, A. M.; Toscano, C. V. A. Effects of Physical Exercise on the Stereotyped Behavior of Children with Autism Spectrum Disorders. Medicina 2019, 55 (10), 685. [CrossRef]
- Menggo, S.; Ndiung, S.; Midun, H. Integrating 21st-century skills in English material development: What do college students really need? Englisia Journal of Language Education and Humanities 2022, 9 (2), 165. [CrossRef]
- Wang, C.; You, Y.; Zhou, J. The impact of long-term exercise on motor skills in children with ADHD: a three-level meta-analysis. BMC Pediatrics 2025, 25 (1). [CrossRef]
- Ziereis, S.; Jansen, P. Effects of physical activity on executive function and motor performance in children with ADHD. Research in Developmental Disabilities 2015, 38, 181–191. [CrossRef]
- Kruger, G. R.; Silveira, J. R.; Marques, A. C. Motor skills of children with autism spectrum disorder. Brazilian Journal of Kinanthropometry and Human Performance 2019, 21. [CrossRef]
- Monteiro, C. E.; Da Silva, E.; Sodré, R.; Costa, F.; Trindade, A. S.; Bunn, P.; Silva, G. C. E.; Di Masi, F.; Dantas, E. The Effect of Physical Activity on Motor Skills of Children with Autism Spectrum Disorder: A Meta-Analysis. International Journal of Environmental Research and Public Health 2022, 19 (21), 14081. [CrossRef]
- Mokhtar, G.; Abdelbaky, A.; Adly, A.; Ezzat, D.; Hakeem, G. A.; Hassab, H.; Youssry, I.; Ragab, I.; Sherief, L. M.; Zakaria, M.; Hesham, M.; Salama, N.; Salah, N.; Afifi, R. a. A.; El-Ashry, R.; Makkeyah, S.; Adolf, S.; Amer, Y. S.; Omar, T. E. I.; Bussel, J.; Raouf, E. A. E.; Atfy, M.; Ellaboudy, M.; Florez, I. Egyptian Pediatric Guidelines for the Management of Children with Isolated Thrombocytopenia Using the Adapted ADAPTE Methodology—A Limited-Resource Country Perspective. Children 2024, 11 (4), 452. [CrossRef]
- Martínez-González, A. E.; Cervin, M.; Piqueras, J. A. Relationships between emotion regulation, social communication and repetitive behaviors in autism spectrum disorder. Journal of Autism and Developmental Disorders 2021, 52 (10), 4519–4527. [CrossRef]
- Ilkim, M.; Tanir, H.; Özdemi̇R, M.; Bozkurt, İ. The Effect of Physical Activity on Level of Anger among Individuals with Autism. Turkish Journal of Sport and Exercise 2018, 130–135. [CrossRef]
- Wen, L.; Wu, Z. The impact of sensory integration based sports training on motor and social skill development in children with autism spectrum disorder. Scientific Reports 2025, 15 (1). [CrossRef]
- Wuang, Y.-P.; Huang, C.-L.; Tsai, H.-Y. Sensory integration and perceptual-motor profiles in school-aged children with autistic spectrum disorder. Neuropsychiatric Disease and Treatment 2020, Volume 16, 1661–1673. [CrossRef]
- Ezzdine, L. B.; Dhahbi, W.; Dergaa, I.; Ceylan, H. İ.; Guelmami, N.; Saad, H. B.; Chamari, K.; Stefanica, V.; Omri, A. E. Physical activity and neuroplasticity in neurodegenerative disorders: a comprehensive review of exercise interventions, cognitive training, and AI applications. Frontiers in Neuroscience 2025, 19. [CrossRef]
- Al-Wardat, M.; Salimei, C.; Alrabbaie, H.; Etoom, M.; Khashroom, M.; Clarke, C.; Almhdawi, K. A.; Best, T. Exploring the Links between Physical Activity, Emotional Regulation, and Mental Well-Being in Jordanian University Students. Journal of Clinical Medicine 2024, 13 (6), 1533. [CrossRef]
- Hamdani, N.; Hamdadou, D. A multicriteria group decision support system. In IGI Global eBooks; 2021; pp 107–133. [CrossRef]
- Peng, Y.; Zhang, G.; Pang, H. Impact of Short-Duration aerobic exercise intensity on executive function and sleep. arXiv.org. https://arxiv.org/abs/2503.09077.
- Masri, A. T.; Nasir, A. K.; Irshaid, A. G.; Irshaid, F. Y.; Alomari, F. K.; Khatib, F. A.; Al-Qudah, A. A.; Nafi, O. A.; Almomani, M. A.; Bashtawi, M. A. Autism services in low-resource areas. Neurosciences 2023, 28 (2), 116–122. [CrossRef]
- Meimand, S. E.; Amiri, Z.; Shobeiri, P.; Malekpour, M.; Moghaddam, S. S.; Ghanbari, A.; Tehrani, Y. S.; Varniab, Z. S.; Langroudi, A. P.; Sohrabi, H.; Mehr, E. F.; Rezaei, N.; Moradi-Lakeh, M.; Mokdad, A. H.; Larijani, B. Burden of autism spectrum disorders in North Africa and Middle East from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Brain and Behavior 2023, 13 (7). [CrossRef]
- Wahdan, M. M.; Malak, M. Z.; Al-Amer, R.; Ayed, A.; Russo, S.; Berte, D. Z. Effect of incredible years autism spectrum and language delays (IY-ASD) program on stress and behavioral management skills among parents of children with autism spectrum disorder in Palestine. Journal of Pediatric Nursing 2023, 72, 45–52. [CrossRef]
- Shaheen, M. M. A.; Abusharkh, W.; Jundi, W. A. Factors Associated with Improvement of Autistic Spectrum Children on Different Behavior Therapy Programs. Journal of Adolescent and Addiction Research 2023, 2 (1). [CrossRef]
- Autism Superhero Palestine, programs and activities. https://www.autismsuperpali.org (accessed 2025-09-03).
- Gaza Community Mental Health Programme. https://archive.unescwa.org/gaza-community-mental-health-programme (accessed 2025-09-03).
- Assaf, M.; Al-Hayeh, H. Family Culture in Dealing with Children with Autism Spectrum Disorder (Analytical Study). jes.ejournal.unri.ac.id 2024, 534–546. [CrossRef]
- Muhammad, A.-Z. The effect of a psychomotor program on the degree of Self-Concept of the mentally handicapped. Assiut Journal of Sport Science and Arts /Assiut Journal of Sport Science and Arts 2020, 2020 (1), 112–122. [CrossRef]
- Vandoni, M.; Giuriato, M.; Pirazzi, A.; Zanelli, S.; Gaboardi, F.; Pellino, V. C.; Gazzarri, A. A.; Baldassarre, P.; Zuccotti, G.; Calcaterra, V. Motor Skills and Executive Functions in Pediatric Patients with Down Syndrome: A Challenge for Tailoring Physical Activity Interventions. Pediatric Reports 2023, 15 (4), 691–706. [CrossRef]
- Maryam, T. M. S.; Poushaneh, K.; Akbar, K. B. A.; Reza, R. Z. H. Citizenship Education Curriculum for Students with Special Needs. lss.artahub.ir 2023. [CrossRef]
- Skavås, M. R.; Rognlid, M.; Kildahl, A. N. Case study: bipolar disorder and catatonia in an adult autistic male with intellectual disability and Phelan-McDermid syndrome (22q13.33 deletion syndrome): psychopharmacological treatment and symptom trajectories. International Journal of Developmental Disabilities 2024, 1–12. [CrossRef]
- Novitski, P., I. Special olympics movement for persons with intellectual disabilities. https://rep.vsu.by/handle/123456789/33711.
- Toscano, C. V. A.; Barros, L.; Lima, A. B.; Nunes, T.; Carvalho, H. M.; Gaspar, J. M. Neuroinflammation in autism spectrum disorders: Exercise as a “pharmacological” tool. Neuroscience & Biobehavioral Reviews 2021, 129, 63–74. [CrossRef]
- Sarabzadeh, M.; Azari, B. B.; Helalizadeh, M. The effect of six weeks of Tai Chi Chuan training on the motor skills of children with Autism Spectrum Disorder. Journal of Bodywork and Movement Therapies 2019, 23 (2), 284–290. [CrossRef]
- Zhao, M.; Chen, S. The Effects of Structured Physical Activity Program on Social Interaction and Communication for Children with Autism. BioMed Research International 2018, 2018, 1–13. [CrossRef]
- Parsons, L.; Cordier, R.; Munro, N.; Joosten, A. A randomized controlled trial of a Play-Based, Peer-Mediated pragmatic language intervention for children with autism. Frontiers in Psychology 2019, 10. [CrossRef]
- Tse, C. Y. A.; Pang, C. L.; Lee, P. H. Choosing an Appropriate Physical Exercise to Reduce Stereotypic Behavior in Children with Autism Spectrum Disorders: A Non-randomized Crossover Study. Journal of Autism and Developmental Disorders 2017, 48 (5), 1666–1672. [CrossRef]
- Kamio, Y.; Haraguchi, H.; Miyake, A.; Hiraiwa, M. Brief report: large individual variation in outcomes of autistic children receiving low-intensity behavioral interventions in community settings. Child and Adolescent Psychiatry and Mental Health 2015, 9 (1). [CrossRef]
- O’Hara, L.; Smith, E. R.; Barlow, J.; Livingstone, N.; Herath, N. I.; Wei, Y.; Spreckelsen, T. F.; Macdonald, G. Video feedback for parental sensitivity and attachment security in children under five years. Cochrane Library 2019, 2019 (11). [CrossRef]
- Bagaiolo, L. F.; Bordini, D.; Da Cunha, G. R.; Sasaki, T. N. D.; Nogueira, M. L. M.; Pacífico, C. R.; Braido, M. Implementing a community-based parent training behavioral intervention for Autism Spectrum Disorder. Psicologia - Teoria E Prática 2019, 21 (3). [CrossRef]
- Kreslins, A.; Robertson, A. E.; Melville, C. The effectiveness of psychosocial interventions for anxiety in children and adolescents with autism spectrum disorder: a systematic review and meta-analysis. Child and Adolescent Psychiatry and Mental Health 2015, 9 (1). [CrossRef]
- Vivanti, G.; Kasari, C.; Green, J.; Mandell, D.; Maye, M.; Hudry, K. Implementing and evaluating early intervention for children with autism: Where are the gaps and what should we do? Autism Research 2017, 11 (1), 16–23. [CrossRef]
- Pickles, A.; Couteur, A. L.; Leadbitter, K.; Salomone, E.; Cole-Fletcher, R.; Tobin, H.; Gammer, I.; Lowry, J.; Vamvakas, G.; Byford, S.; Aldred, C.; Slonims, V.; McConachie, H.; Howlin, P.; Parr, J. R.; Charman, T.; Green, J. Parent-mediated social communication therapy for young children with autism (PACT): long-term follow-up of a randomised controlled trial. The Lancet 2016, 388 (10059), 2501–2509. [CrossRef]
- Madden, J. M.; Lakoma, M. D.; Lynch, F. L.; Rusinak, D.; Owen-Smith, A. A.; Coleman, K. J.; Quinn, V. P.; Yau, V. M.; Qian, Y. X.; Croen, L. A. Psychotropic Medication Use among Insured Children with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders 2016, 47 (1), 144–154. [CrossRef]
- Rutherford, M.; Baxter, J.; Grayson, Z.; Johnston, L.; O’Hare, A. Visual supports at home and in the community for individuals with autism spectrum disorders: A scoping review. Autism 2019, 24 (2), 447–469. [CrossRef]
- McCambridge, J.; Witton, J.; Elbourne, D. R. Systematic review of the Hawthorne effect: New concepts are needed to study research participation effects. Journal of Clinical Epidemiology 2013, 67 (3), 267–277. [CrossRef]
- Dolan, B. K.; Van Hecke, A. V.; Carson, A. M.; Karst, J. S.; Stevens, S.; Schohl, K. A.; Potts, S.; Kahne, J.; Linneman, N.; Remmel, R.; Hummel, E. Brief Report: Assessment of Intervention Effects on In Vivo Peer Interactions in Adolescents with Autism Spectrum Disorder (ASD). Journal of Autism and Developmental Disorders 2016, 46 (6), 2251–2259. [CrossRef]
- Amal AL Nadaf. A Proposed Strategy for Developing Professional Services Provided to Individuals with Autism Spectrum Disorder Fromthe Perspective of Service Providers in Jordan. Zanco Journal of Humanity Sciences 2024, 28 (s3). [CrossRef]
- Martin, J.; Hamshere, M. L.; Stergiakouli, E.; O’Donovan, M. C.; Thapar, A. Neurocognitive abilities in the general population and composite genetic risk scores for attention-deficit hyperactivity disorder. Journal of Child Psychology and Psychiatry 2014, 56 (6), 648–656. [CrossRef]
- Madden, J. M.; Lakoma, M. D.; Lynch, F. L.; Rusinak, D.; Owen-Smith, A. A.; Coleman, K. J.; Quinn, V. P.; Yau, V. M.; Qian, Y. X.; Croen, L. A. Psychotropic Medication Use among Insured Children with Autism Spectrum Disorder. Journal of Autism and Developmental Disorders 2016, 47 (1), 144–154. [CrossRef]
- Pan, N.; Auyeung, B.; Wang, X.; Lin, L.; Li, H.; Zhan, X.; Jin, C.; Jing, J.; Li, X. Empathizing, systemizing, empathizing-systemizing difference and their association with autistic traits in children with autism spectrum disorder, with and without intellectual disability. Autism Research 2022, 15 (7), 1348–1357. [CrossRef]
- Divan, G.; Hamdani, S. U.; Vajartkar, V.; Minhas, A.; Taylor, C.; Aldred, C.; Leadbitter, K.; Rahman, A.; Green, J.; Patel, V. Adapting an evidence-based intervention for autism spectrum disorder for scaling up in resource-constrained settings: the development of the PASS intervention in South Asia. Global Health Action 2015, 8 (1), 27278. [CrossRef]
- Divan, G.; Vajaratkar, V.; Cardozo, P.; Huzurbazar, S.; Verma, M.; Howarth, E.; Emsley, R.; Taylor, C.; Patel, V.; Green, J. The Feasibility and Effectiveness of PASS Plus, a lay health worker delivered comprehensive intervention for autism spectrum disorders: pilot RCT in a rural low and middle income country setting. Autism Research 2018, 12 (2), 328–339. [CrossRef]
- Sandbank, M.; Bottema-Beutel, K.; Crowley, S.; Cassidy, M.; Dunham, K.; Feldman, J. I.; Crank, J.; Albarran, S. A.; Raj, S.; Mahbub, P.; Woynaroski, T. G. Project AIM: Autism intervention meta-analysis for studies of young children. Psychological Bulletin 2019, 146 (1), 1–29. [CrossRef]
- Eapen, V.; Črnčec, R.; Walter, A. Clinical outcomes of an early intervention program for preschool children with Autism Spectrum Disorder in a community group setting. BMC Pediatrics 2013, 13 (1). [CrossRef]
- Paynter, J.; Trembath, D.; Lane, A. Differential outcome subgroups in children with autism spectrum disorder attending early intervention. Journal of Intellectual Disability Research 2018, 62 (7), 650–659. [CrossRef]
- Bremer, E.; Crozier, M.; Lloyd, M. A systematic review of the behavioural outcomes following exercise interventions for children and youth with autism spectrum disorder. Autism 2016, 20 (8), 899–915. [CrossRef]
- Zhuang, H.; Liang, Z.; Ma, G.; Qureshi, A.; Ran, X.; Feng, C.; Liu, X.; Yan, X.; Shen, L. Autism spectrum disorder: pathogenesis, biomarker, and intervention therapy. MedComm 2024, 5 (3). [CrossRef]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18 (8), 2486. [CrossRef]
- Zhang, M.; Ding, H.; Naumceska, M.; Zhang, Y. Virtual Reality Technology as an Educational and Intervention Tool for Children with Autism Spectrum Disorder: Current Perspectives and Future Directions. Behavioral Sciences 2022, 12 (5), 138. [CrossRef]
- Sokołowska, B. Being in Virtual Reality and its Influence on Brain Health—An Overview of Benefits, Limitations and Prospects. Brain Sciences 2024, 14 (1), 72. [CrossRef]
- Lorenzo, G. G.; Newbutt, N. N.; Lorenzo-Lledó, A. A. Designing virtual reality tools for students with Autism Spectrum Disorder: A systematic review. Education and Information Technologies 2023, 28 (8), 9557–9605. [CrossRef]
- Shire, S. Y.; Shih, W.; Bracaglia, S.; Kodjoe, M.; Kasari, C. Peer engagement in toddlers with autism: Community implementation of dyadic and individual Joint Attention, Symbolic Play, Engagement, and Regulation intervention. Autism 2020, 24 (8), 2142–2152. [CrossRef]
- Elbeltagi, R.; Al-Beltagi, M.; Saeed, N. K.; Alhawamdeh, R. Play therapy in children with autism: Its role, implications, and limitations. World Journal of Clinical Pediatrics 2023, 12 (1), 1–22. [CrossRef]
- Dückers, M. L. A.; Witteveen, A. B.; Bisson, J. I.; Olff, M. The association between disaster vulnerability and post-disaster psychosocial service delivery across Europe. Administration and Policy in Mental Health and Mental Health Services Research 2015, 44 (4), 470–479. [CrossRef]
- Jacobs, J.; Oosterbeek, M.; Tummers, L. G.; Noordegraaf, M.; Yzermans, C. J.; Dückers, M. L. A. The organization of post-disaster psychosocial support in the Netherlands: a meta-synthesis. European Journal of Psychotraumatology 2019, 10 (1). [CrossRef]
- Chan, J. C. N.; Lim, L.-L.; Wareham, N. J.; Shaw, J. E.; Orchard, T. J.; Zhang, P.; Lau, E. S. H.; Eliasson, B.; Kong, A. P. S.; Ezzati, M.; Aguilar-Salinas, C. A.; McGill, M.; Levitt, N. S.; Ning, G.; So, W.-Y.; Adams, J.; Bracco, P.; Forouhi, N. G.; Gregory, G. A.; Guo, J.; Hua, X.; Klatman, E. L.; Magliano, D. J.; Ng, B.-P.; Ogilvie, D.; Panter, J.; Pavkov, M.; Shao, H.; Unwin, N.; White, M.; Wou, C.; W, R. C., MA; Schmidt, M. I.; Ramachandran, A.; Seino, Y.; Bennett, P. H.; Oldenburg, B.; Gagliardino, J. J.; Luk, A. O. Y.; Clarke, P. M.; Ogle, G. D.; Davies, M. J.; Holman, R. R.; Gregg, E. W. The Lancet Commission on diabetes: using data to transform diabetes care and patient lives. The Lancet 2020, 396 (10267), 2019–2082. [CrossRef]
- Pellicano, E.; Houting, J. D. Annual Research Review: Shifting from ‘normal science’ to neurodiversity in autism science. Journal of Child Psychology and Psychiatry 2021, 63 (4), 381–396. [CrossRef]
Figure 1.
Pre- and post-test means of aggressive behavior, irrational behavior, social communication avoidance, and total psychological variables (A-D respectively) among children with Autism Spectrum Disorder.
Figure 1.
Pre- and post-test means of aggressive behavior, irrational behavior, social communication avoidance, and total psychological variables (A-D respectively) among children with Autism Spectrum Disorder.
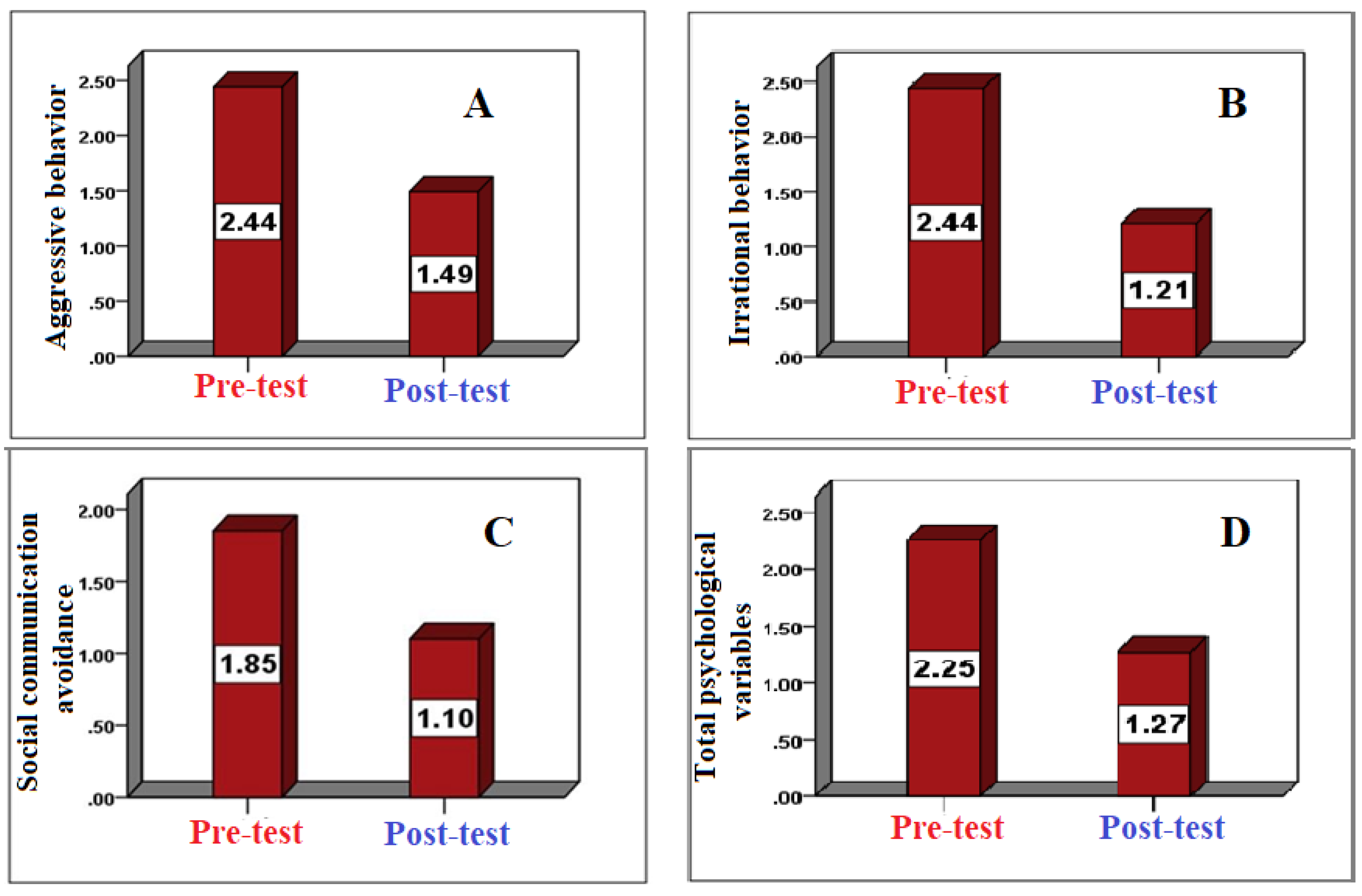
Figure 2.
Pre- and post-test means of spinning/circling (spinning around self) and hand flapping or random waving (A-B respectively) among children with Autism Spectrum Disorder.
Figure 2.
Pre- and post-test means of spinning/circling (spinning around self) and hand flapping or random waving (A-B respectively) among children with Autism Spectrum Disorder.
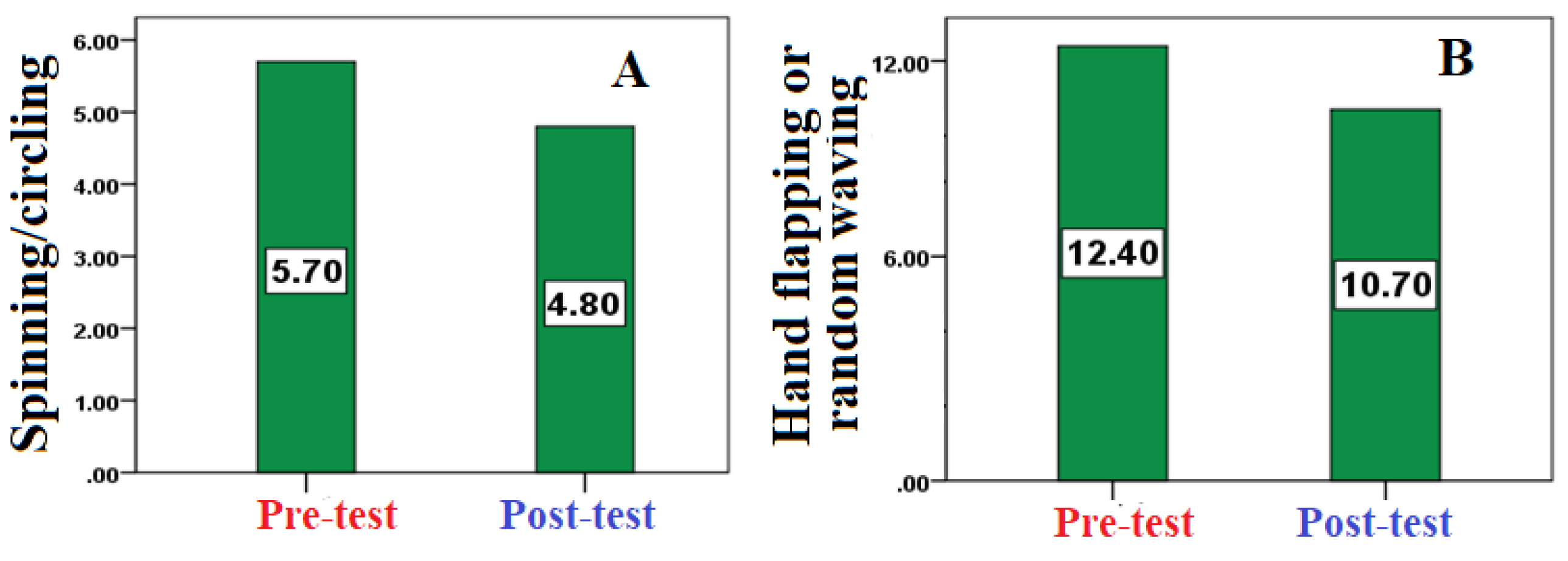
Figure 3.
Pre- and post-test means of repetitive clapping and jumping in place (C-D respectively) among children with Autism Spectrum Disorder.
Figure 3.
Pre- and post-test means of repetitive clapping and jumping in place (C-D respectively) among children with Autism Spectrum Disorder.
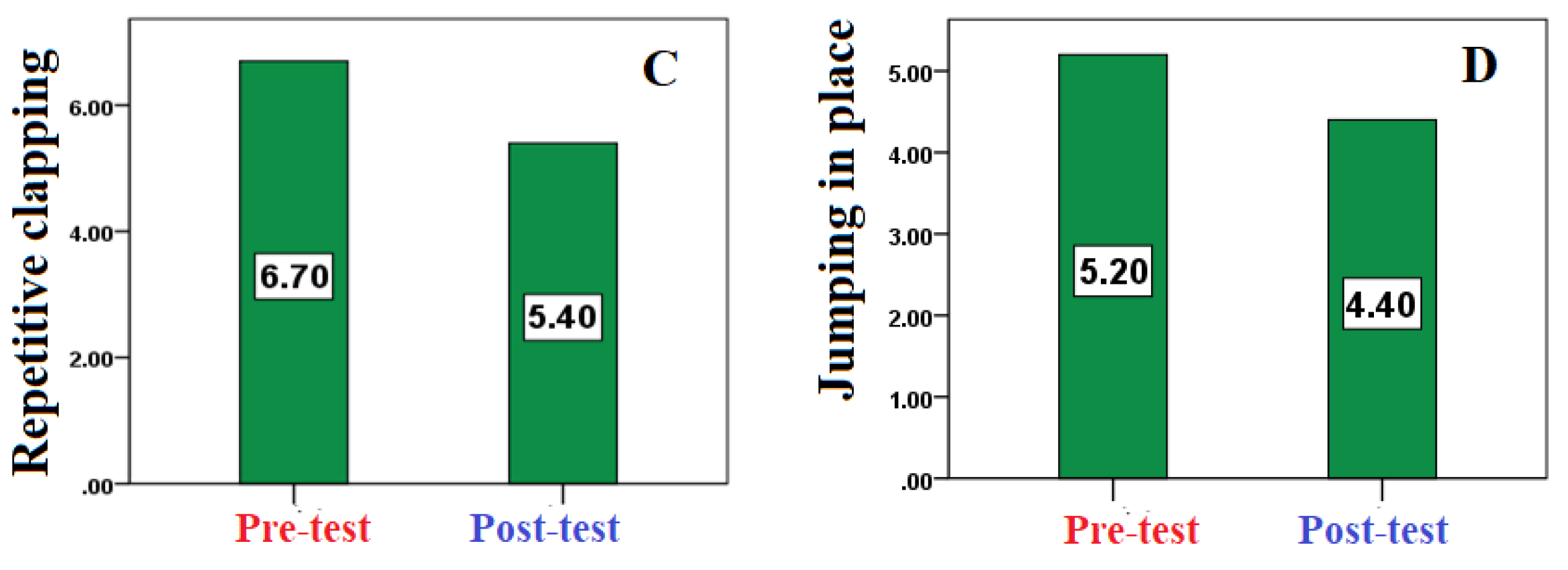
Figure 4.
Pre- and post-test means of rocking back and forth while sitting or standing (E) and repetitive foot tapping (F), among children with Autism Spectrum Disorder.
Figure 4.
Pre- and post-test means of rocking back and forth while sitting or standing (E) and repetitive foot tapping (F), among children with Autism Spectrum Disorder.
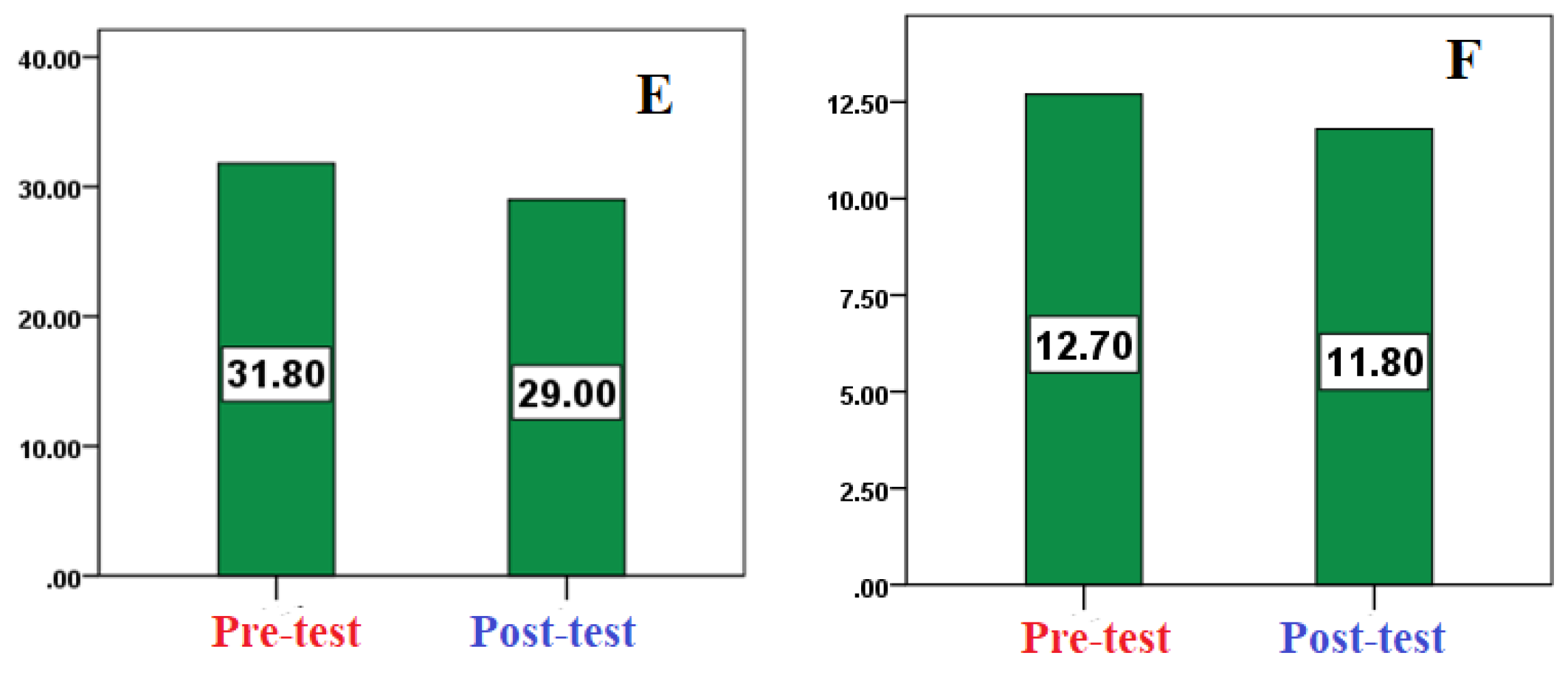
Figure 5.
Pre- and post-test means of covering ears when exposed to loud sounds or music (G) and inappropriate object use (breaking/damaging items) (H), among children with Autism Spectrum Disorder.
Figure 5.
Pre- and post-test means of covering ears when exposed to loud sounds or music (G) and inappropriate object use (breaking/damaging items) (H), among children with Autism Spectrum Disorder.
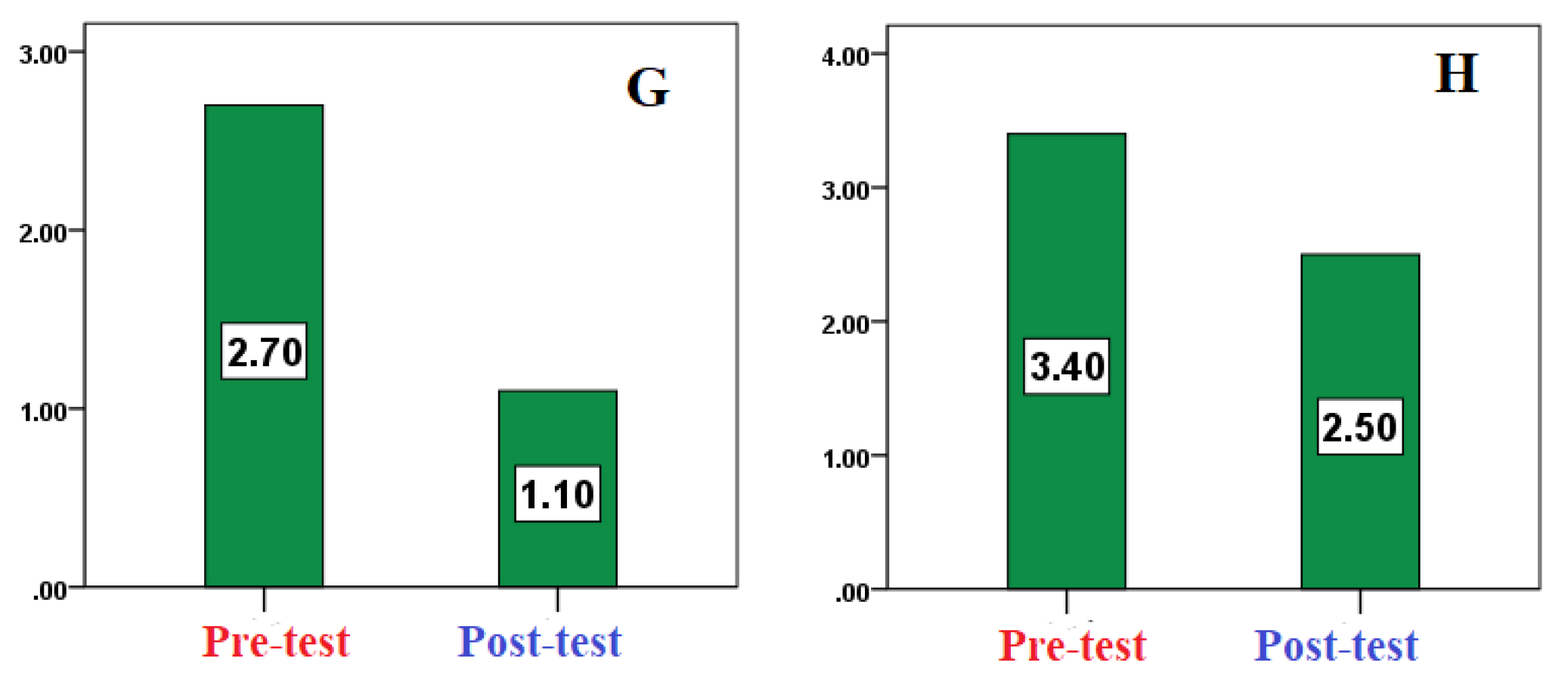

Table 1.
Characteristics and homogeneity of the study sample of children with Autism Spectrum Disorder according to age, height, body mass, and training duration (n = 10).
Table 1.
Characteristics and homogeneity of the study sample of children with Autism Spectrum Disorder according to age, height, body mass, and training duration (n = 10).
| Variable | Mean | Standard Deviation | Skewness |
| Age (years) | 8.43 | 1.9 | 0.12 |
| Height (cm) | 127.43 | 5.41 | -0.04 |
| Body Mass (kg) | 36.11 | 5.06 | -0.93 |
Table 2.
Self-validity and reliability (ICC) of the psychological variables scale.
| Psychological Variable | ICC Reliability | Self-Validity |
| Aggressive behavior | 0.93* | 0.964 |
| Irrational behavior | 0.91* | 0.953 |
| Social communication | 0.89* | 0.943 |
| Overall scale | 0.95* | 0.974 |
| *Statistically significant at α ≤ 0.05 | ||
Table 3.
Self-validity and reliability (ICC) of the motor behavior observations.
| Motor Behavior | ICC Reliability | Self-Validity |
| Spinning and circling (rotating around oneself) | 0.88* | 0.938 |
| Hand flapping or random waving | 0.93* | 0.964 |
| Repetitive clapping | 0.92* | 0.959 |
| Jumping up and down in the same spot | 0.91* | 0.953 |
| Rocking back and forth while sitting or standing | 0.89* | 0.943 |
| Repetitive foot tapping on the ground | 0.94* | 0.969 |
| Covering ears when hearing loud sounds or loud music | 0.90* | 0.948 |
| Inappropriate object use (e.g., breaking or damaging items) | 0.91* | 0.953 |
| *Statistically significant at α ≤ 0.05 | ||
Table 4.
Paired samples t-test results for differences between pre-test and post-test scores of psychological variables among children with Autism Spectrum Disorder (n = 10).
Table 4.
Paired samples t-test results for differences between pre-test and post-test scores of psychological variables among children with Autism Spectrum Disorder (n = 10).
| Psychological Variables | Pre-test Mean ± SD | Post-test Mean ± SD | t-value | Sig. (p) | % Change |
| Aggressive behavior | 2.44 ± 0.22 | 1.49 ± 0.12 | 10.3 | 0.000* | -38.93 |
| Irrational behavior | 2.44 ± 0.13 | 1.21 ± 0.22 | 13.91 | 0.000* | -50.4 |
| Social communication avoidance | 1.85 ± 0.39 | 1.10 ± 0.17 | 7.12 | 0.000* | -40.54 |
| Total score | 2.25 ± 0.14 | 1.27 ± 0.08 | 21.32 | 0.000* | -43.56 |
| *Significant at α ≤ 0.05. | |||||
Table 5.
Paired samples t-test results for differences between pre-test and post-test scores of the most common motor behaviors among children with Autism Spectrum Disorder (n = 10).
Table 5.
Paired samples t-test results for differences between pre-test and post-test scores of the most common motor behaviors among children with Autism Spectrum Disorder (n = 10).
| Motor Behaviors | Pre-test Mean ± SD | Post-test Mean ± SD | t-value | Sig. (p) | % Change |
| Spinning/circling (spinning around self) | 5.70 ± 1.89 | 4.80 ± 1.62 | 3.86 | 0.004* | -15.79 |
| Hand flapping or random waving | 12.40 ± 3.34 | 10.70 ± 2.83 | 4.64 | 0.001* | -13.39 |
| Repetitive clapping | 6.70 ± 1.89 | 5.40 ± 1.84 | 3.88 | 0.004* | -19.4 |
| Jumping in place | 5.20 ± 2.25 | 4.40 ± 2.07 | 3.21 | 0.011* | -15.38 |
| Rocking back and forth while sitting or standing | 31.80 ± 12.55 | 29.00 ± 12.07 | 5.47 | 0.000* | -8.8 |
| Repetitive foot tapping | 12.70 ± 2.41 | 11.80 ± 2.39 | 3.25 | 0.010* | -7.08 |
| Covering ears when exposed to loud sounds/music | 2.70 ± 1.34 | 1.10 ± 0.70 | 6 | 0.000* | -59.25 |
| Inappropriate object use (breaking/damaging items) | 3.40 ± 1.90 | 2.50 ± 1.65 | 3.25 | 0.010* | -26.47 |
| *Significant at α ≤ 0.05. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



