Submitted:
11 October 2025
Posted:
13 October 2025
You are already at the latest version
Abstract
Large-volume paracentesis (LVP) of the peritoneal and pleural cavities is a common therapeutic and diagnostic intervention in patients with liver cirrhosis or advanced heart failure, which are often complicated by ascites or pleural effusion. Although generally considered low-risk, the potential complications of LVP include intrapleural or abdominal hemorrhage or, more commonly, intraabdominal wall hemorrhage, organ puncture, and infection. Performing paracentesis in patients with coagulopathy or bleeding disorders, whether due to underlying disease or resulting from anticoagulant therapy, presents a major clinical dilemma. The safety thresholds for conducting the procedure in such patients vary, and the strategies for mitigating the bleeding risk remain debated, with no consensus reached across different professional societies. Based on our institutional experience and the current international literature, we herein present comprehensive recommendations for the safe and effective execution of LVP, based on evidence synthesis and expert consensus. This review may serve as a practical guide for clinicians performing LVP in high-risk patients.
Keywords:
large-volume paracentesis
; ascites
; pleural effusion
; coagulation management
; ultrasound guidance
1. Introduction
Ascites and pleural effusion are common manifestations of decompensated liver cirrhosis and congestive heart failure (CHF). Large-volume paracentesis (LVP) is often required for symptom relief, prevention of complications such as spontaneous bacterial peritonitis (SBP), and diagnostic evaluation. The balance between bleeding risks and thrombosis in patients with cirrhosis and CHF complicates decision-making, particularly when coagulopathy or anticoagulant therapy is required. Various professional societies, including the Gastroenterological Association and the Society of Interventional Radiology, have proposed clinical guidelines, which may create uncertainty in clinical practice. The present study reviewed the existing literature and proposes a set of consolidated recommendations that are relevant and applicable to every healthcare system, aimed at enhancing safety and standardizing clinical care.
2. Methodology
This work represents a narrative review of the literature, aiming to synthesize available evidence and provide practical recommendations for clinical management. In this study, we conducted a literature search of the PubMed and Open Evidence databases, complemented by a manual review of the relevant society guidelines. The search strategy used terms such as “paracentesis,” “coagulopathy,” “complications,” “bleeding risk,” and “guidelines.” English-language publications from January 2010 to March 2025 were included. Eligible study types included randomized controlled trials, observational studies, meta-analyses, and professional society guidelines. Case reports and non-peer-reviewed materials were excluded. The quality and relevance of the evidence were qualitatively assessed.
2. Section I: Abdominal Paracentesis in Patients with Ascites
2.1. Indications [1,2,3,4]
- Diagnostic: Differentiate ascitic fluid based on the serum–ascites albumin gradient (SAAG) into high (> 1.1 g/dL) and low (< 1.1 g/dL) SAAG.
- Diagnostic evaluation for SBP or suspected hepatocellular carcinoma transformation
- Symptomatic ascites, such as tense ascites causing respiratory compromise or abdominal discomfort
- Refractory ascites requiring repeated therapeutic drainage
2.2. Clinical Recommendations for Peritoneal Paracentesis:
Table 1 lists all recommendations for the preproceural preparations, principles of execution of the procedure, and postprocedural care requirements.

| Section | Recommendation |
| Preprocedural Recommendations | |
| Obtain verbal consent and document. Written consent should be obtained only if required by institutional policy. | |
| 2. First-Time Paracentesis | Provide a full explanation of the risks in the patient’s native language. Document the explanation, clinician’s name, and language used. |
| 3. Exclude Acute Infection | Postpone the procedure if active infection is suspected. |
| 4. Management of Anticoagulants | Warfarin: Stop 5 d prior; confirm INR <1.7. DOACs/ Clexane (LMWH): Skip the last dose before the procedure. |
| 5. Laboratory Testing in Suspected Coagulopathy | If no known coagulopathy exists and recent laboratory test results show a platelet count of >20 000/μL and INR <1.7, omit repeat tests. If platelet count is <20 000/μL: Administer 6 units of platelets (~5000/unit) [1]. If INR >1.7: Administer up to 3 units of FFP (~0.3 INR correction per unit) [1]. |
| 6. Aspirin | No need to withhold before procedure. |
| 7. Clopidogrel (Plavix) | Withhold for 72 h before drainage. |
| 8. Baseline Vitals | Record temperature, pulse, BP, and oxygen saturation. |
| Technique Recommendations | |
| 1. Ultrasound Guidance | Mandatory for all procedures. |
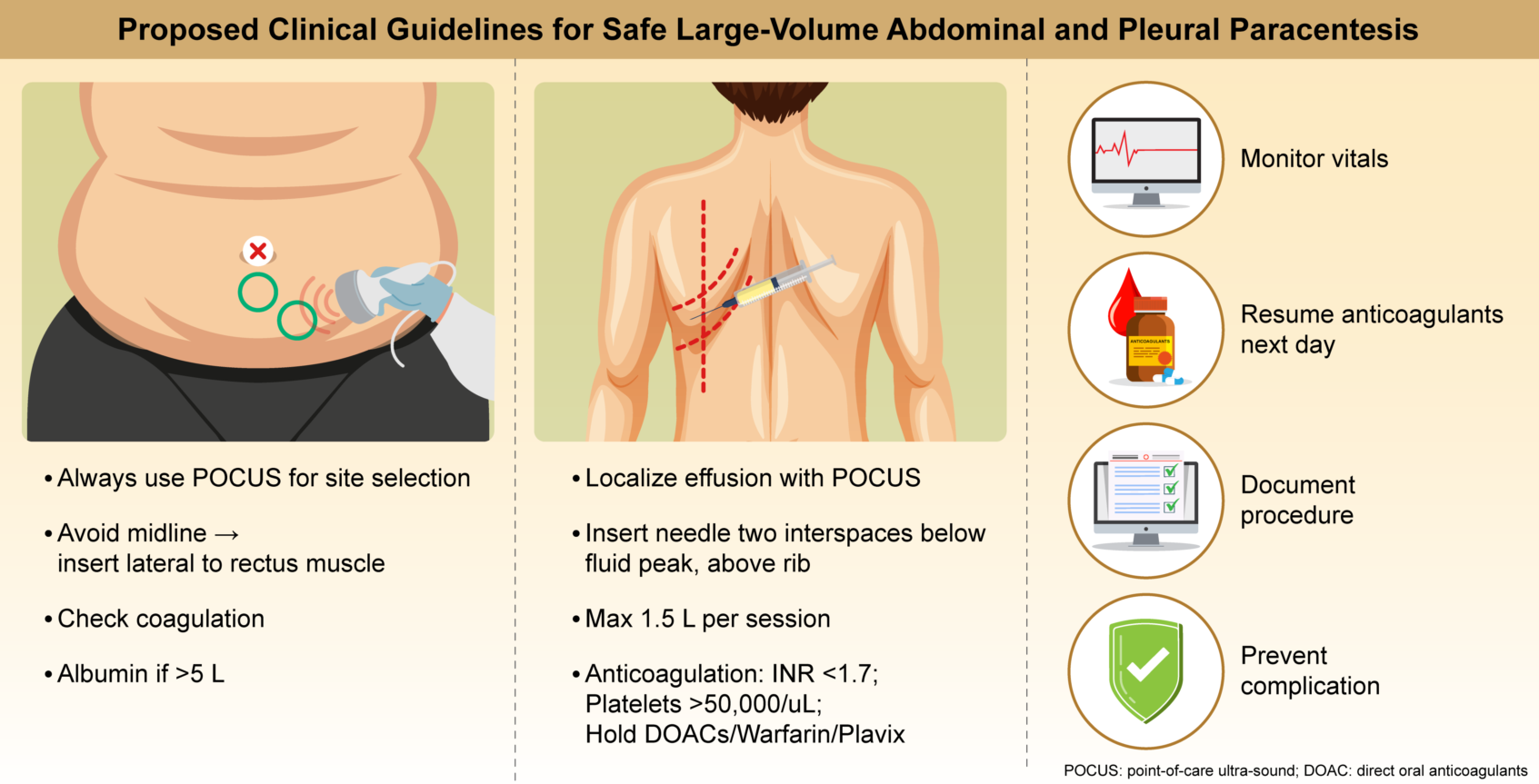
| 2. Needle Placement | Avoid the midline. Insert 8 cm lateral to the midline and 5 cm above the pubic symphysis or 2 cm below the umbilicus. |
| 3. Drainage System | Use either an 8F Seldinger kit or 18G cannula. |
| 4. Volume | No restriction on the amount of peritoneal fluid drained (unlike pleural effusion). |
| 5. Diagnostic Fluid Sampling | Always analyze fluid for cell count. If neutrophil count is >250/mm3 → suspect SBP. If a catheter is in place → perform culture testing. |
| 6. Device Options | Either an 8F Seldinger set or 18G peripheral catheter is acceptable. |
| 7. Initial/Diagnostic Studies | Analyze fluid for: cell count, culture, albumin, TP, amylase, BNP (optional), cytology. |
| 8. Albumin Administration |
Administer 8 g albumin for each 1 L of drainage (only >5 L) (to prevent paracentesis-induced circulatory dysfunction) |
| Postparacentesis Care | |
| 1. Observation | Monitor patients for 1 h after catheter removal |
| 2. Bed Rest | Keep patient in bed for the first 30 min postremoval. |
| 3. Discharge Criteria | Discharge only after documentation of stable BP and HR. Ensure parameters are recorded. |
| 4. Leakage from Site . |
If leakage occurs, place a pressure bandage. If leakage does not stop, a single suture may be placed. Remove suture after 1 week. |
| 5. Resuming Anticoagulation | Resume anticoagulants (including clopidogrel) the day after the procedure. |
| Bleeding Management | |
| 1. Bloody Aspirate | Serosanguinous initial fluid is acceptable. If bloody fluid follows clear drainage → stop immediately. If the initial aspirate is blood → abort and remove the catheter. |
| 2. Bleeding Response | a. Monitor for 4 h with vitals assessed every hour. b. Repeat hemoglobin testing after 1 h. Perform blood type testing. |
| Admission Criteria Post-Paracentesis | |
| 1. SBP | Confirmed SBP diagnosis. |
| 2. Hemodynamic Instability | Hemodynamic changes or a drop in hemoglobin level >1 g/dL. |
| 3. Severe Pain or Hematoma | VAS ≥ 7 + expanding hematoma → consider urgent abdominal CT angiography. |
Abbreviations: BNP, brain natriuretic peptide; BP, blood pressure; Clexane, brand name for low molecular weight heparin (LMWH); CT, computed tomography; DOACs, direct oral anticoagulants; FFP, fresh frozen plasma; INR, international normalized ratio; LMWH, low molecular weight heparin; SBP, spontaneous bacterial peritonitis; TP, total protein; VAS, visual analog scale.
2.3. Major Complications [2,3,5,6]
a. Hemorrhage (0.3%–1%) [3,6]: The incidence of hemorrhage is reduced by 50% with ultrasound (US) guidance [13]. Bleeding during paracentesis typically results from an injury to a branch of the inferior epigastric artery of the abdominal wall. Bleeding can occur in two ways.
1. Immediate return of blood through the catheter. This usually indicates direct injury to the artery, resulting in immediate blood reflux. This complication generally leads to the development of abdominal wall hematoma [9,10].
2. Gradual increase in bleeding during the procedure. In such instances, the drainage initially appears serous and progressively becomes hemorrhagic. This suggests arterial bleeding into the peritoneal cavity surrounding the catheter, which leads to increasingly bloody fluid.
b. Bowel perforation: This recognized but rare complication occurred in <1% of patients in a large series of diagnostic paracenteses. The risk is higher in patients with intra-abdominal adhesions, prior abdominal surgery, or distorted anatomy due to underlying disease [14,15]. Clinically, bowel perforation may present acutely with the return of fecal material; gas through the paracentesis catheter; or more insidiously with signs of peritonitis, sepsis, or polymicrobial peritoneal infection. Immediate recognition is critical as delayed diagnosis increases peritonitis and sepsis risks. Management depends on the clinical scenario. Stable patients without peritonitis may be managed conservatively with bowel rest and broad-spectrum antibiotics; however, surgical intervention is indicated for patients with generalized peritonitis or clinical deterioration [15,16]. To minimize risk, the needle should be inserted at sites with the lowest likelihood of underlying bowel, such as the left lower quadrant lateral to the rectus abdominis or the midline 2 cm below the umbilicus, and never through surgical scars or areas with suspected adhesions [14].
c. SBP during peritoneal paracentesis refers to a peritoneal infection that arises from a direct, identifiable intraabdominal source that disrupts the integrity of the gastrointestinal or genitourinary tracts. Secondary peritonitis is typically polymicrobial, involving both aerobic and anaerobic organisms, most commonly gram-negative rods (such as Escherichia coli and Klebsiella spp.), anaerobes (such as Bacteroides spp. and Clostridium spp.), and gram-positive cocci (such as Enterococcus spp.). The Infectious Diseases Society of America and the American Society for Microbiology emphasize that, in contrast to SBP, secondary peritonitis is usually polymicrobial and may include anaerobic microbiota, and that peritoneal fluid should be sent for both aerobic and anaerobic cultures in an anaerobic transport system [16]. Diagnosis during paracentesis is suggested by the presence of multiple organisms on Gram staining or culture, elevated ascitic fluid neutrophil count, and biochemical features such as low glucose, high lactate dehydrogenase, and low protein levels. Clinical suspicion should be high in patients with severe abdominal symptoms or evidence of sepsis. Imaging (e.g., computed tomography) is often required to identify the source [11]. Management requires the prompt administration of broad-spectrum antibiotics covering both aerobic and anaerobic organisms and urgent surgical or interventional radiology evaluation to control the infection source, as medical therapy alone is insufficient. Without timely intervention, mortality is high [11,17].
d. Postparacentesis circulatory dysfunction (PICD) manifests as effective hypovolemia and renal impairment, usually after the removal of >5 L. The American College of Radiology states that PICD can develop in up to 80% of patients with cirrhosis if volume expansion (typically using albumin) is not performed at the time of paracentesis. The pathophysiology involves a rapid drop in intraabdominal pressure, leading to increased venous return, transiently increased cardiac output, and subsequent activation of the renin-angiotensin-aldosterone and sympathetic nervous systems, resulting in decreased effective arterial blood volume and free water retention [18].
e. Puncture site leakage following large-volume peritoneal paracentesis is a recognized complication, with reported rates varying from 0% to 23% [15]. The primary cause is persistent ascitic fluid flow through the needle tract, which may be exacerbated by high intraabdominal pressure, large-volume removal, or technical failure of sealing the skin and subcutaneous tissues after catheter removal. The initial management options include conservative measures [15]. The first-line approach involves the application of a pressure dressing directly over the puncture site, which is effective in most cases. The use of the Z-tract technique during the procedure, in which the skin is displaced before needle insertion to create a zigzag tract, may help prevent leakage, although evidence for its efficacy is limited. If leakage persists, additional options include continued pressure dressings, use of ostomy appliances to collect fluid, or, rarely, placement of a suture at the site [15]. Rarely, persistent or high-volume leaks may require further intervention such as peritoneal drains or surgical closure. Infection should be ruled out if the leak is prolonged or is associated with local erythema.
3. Section II: Thoracocentesis in Patients with Pleural Effusion
3.1. Indications [13,19,20,21]
a. New or unexplained pleural effusion, to differentiate between transudate and exudate based on Light’s criteria
b. Suspected infection (empyema or parapneumonic effusion), especially if the effusion is loculated or shows signs of sepsis
c. Suspected malignancy, particularly in patients with cancer history or unilateral/bloody effusions
d. Suspected tuberculous pleuritis based on the regional epidemiology and clinical presentation
e. Symptomatic relief of dyspnea, especially in patients with large pleural effusions causing lung compression and impaired ventilation. This indication is common in malignant effusion, heart failure, or hepatic hydrothorax
f. Large effusion with signs of respiratory compromise such as tachypnea, hypoxemia, or use of accessory muscles
g. Effusion refractory to medical management; for example: diuretic-resistant pleural effusions in CHF
h. Recurrent pleural effusion requiring repeated drainage as a bridge to pleurodesis or indwelling pleural catheter placement in patients with malignancy.
3.2. Clinical Recommendations for Thoracocentesis
Table 2 lists all recommendations for the preproceural preparations, principles of execution of the procedure, and postprocedural care requirements.
| Section | Recommendation |
| Preprocedural Requirements and Recommendations | |
| 1. Imaging | Localize effusion using POCUS. |
| 2. Access Point | Two intercostal spaces below the fluid peak in the posterior mid-clavicular line with the patient seated, arms forward. Above the rib. |
| 3. Needle/Drainage Kit | 20–21G cannula or 6–8F Seldinger catheter. |
| 4. Coagulation Guidelines | No repeat tests if no coagulopathy history and normal test results in the past month. a. DOACs: Stop 48 h prior. b. Warfarin: Stop 5 d prior; confirm INR <1.7. c. Clexane (LMWH): Hold 24 h (2 doses). d. Aspirin: Continue [25]. e. Plavix: Stop 72 h prior [22,25]. f. Platelet count of <50 000/μL: Administer 6 units. g. INR >1.7: Administer ≤3 FFP units. h. TEG: Optional if available. |
| Procedure Guidelines | |
| 1. Bilateral Drainage | Do not perform on the same day. |
| 2. Volume Limit | Do not exceed 1.5 L drainage per session [19]. |
| 3. Drainage Method | Use gravity drainage. Avoid vacuum suction [2]. |
| 4. Anesthesia | Use 1% lidocaine for local anesthesia [19]. |
| 5. Diagnostic Testing | Send pleural fluid for pH, LDH, glucose, protein, cytology, and BNP assessments. |
| Postprocedure Care | |
| 1. Vital Signs | Monitor hourly for 2 h. |
| 2. Imaging | Chest radiography (AP + LAT) 1 h postprocedure [19]. |
| 3. Anticoagulation | Restart the next day. |
| Documentation Checklist | |
| 1. Indication | Document the indication for the procedure. |
| 2. Consent | Obtain and document verbal or written consent. |
| 3. Physical/POCUS Findings | Record the physical exam and POCUS findings. |
| 4. Technique | Document the insertion technique. |
| 5. Vital Signs | Record pre- and postprocedure vital signs. |
| 6. Anticoagulation | Document anticoagulation status and last dose timing. |
| 7. Laboratory test results | Include relevant laboratory test results and hemostasis assessment. |
Abbreviations: AP: anteroposterior; BNP: B-type natriuretic peptide; Clexane: brand name for enoxaparin, a low-molecular-weight heparin; DOACs: direct oral anticoagulants; FFP: fresh frozen plasma; INR: international normalized ratio; LAT: lateral; LDH: lactate dehydrogenase; LMWH: low-molecular-weight heparin; Plavix: brand name for clopidogrel; POCUS: point-of-care ultrasound; TEG: thromboelastography.
3.2. Complications
- Reexpansion pulmonary edema: This is a rare but potentially serious complication, with an incidence of <0.1%, and is associated with rapid or large-volume fluid removal, especially if pleural pressures fall below −20 cm H2O or if >1.5 L is removed quickly. Symptom-limited drainage is recommended to mitigate this risk [4].
- Secondary infections: Complications following thoracentesis include empyema (pus in the pleural space), parapneumonic effusion (infected pleural fluid associated with pneumonia), and, less commonly, cellulitis or soft tissue infection at the puncture site. These complications are rare when sterile technique is used. Empyema and complicated parapneumonic effusion are clinically significant and often require antimicrobial therapy and drainage. According to the Infectious Diseases Society of America and the American Society for Microbiology, the most common pathogens in pleural space infections are Streptococcus anginosus, Staphylococcus aureus (including methicillin-resistant S. aureus in hospital-acquired cases), anaerobes, and Enterobacterales. Hospital-acquired infections are more likely to involve resistant gram-negative bacteria [13].
- Hemorrhage: Hemorrhage is a recognized but rare complication of pleural effusion paracentesis (thoracentesis) with a risk of significant bleeding (including hemothorax or puncture site bleeding) of approximately ≤1%, as indicated in large meta-analyses and cohort studies. The primary mechanism is misplaced needle or catheter insertion, resulting in laceration of the intercostal artery or its branches, which can lead to chest wall hematoma or hemothorax. Injury to other vascular structures or inadvertent puncture of abdominal organs (e.g., the liver and spleen) is rare but possible, especially for low-lying effusions or with improper techniques. Lack of ultrasound guidance, poor knowledge of the local anatomy, and multiple needle passes increase the risk. Vascular ultrasonography with color Doppler can help avoid vessel injury [22,24].
Although this was a narrative review, its primary limitation notably lies in the fact that the examined literature underpinning the recommendations predominantly comprised retrospective studies and case series. This is likely one of the main reasons for the current absence of consensus in the guidelines. A meta-analysis of the literature may serve as an important tool for evaluating the cumulative data therein and for validating our recommendations.
4. Conclusions
Although both abdominal and pleural LVP are considered low-risk interventions, meticulous attention to coagulation status, imaging guidance, and postprocedural monitoring are essential for reducing complications. The guidelines proposed here align with the current literature and have been adapted to high-risk populations. The emphasis on detailed documentation ensures accountability and safety. Adherence to these recommendations can reduce procedural complications and optimize patient outcomes, especially in complex cases involving coagulopathies or anticoagulant therapy.
Author Contributions
Conceptualization, B.C.; Methodology and Literature review: P.V., D.V., and P.R; Writing original draft preparation, B.C., S.E., and S.D.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CHF | congestive heart failure |
| LVP | large-volume paracentesis |
| PICD | post-paracentesis circulatory dysfunction |
| SBP | spontaneous bacterial peritonitis |
| SAAG | serum–ascites albumin gradient |
References
- Moore, K.P.; Aithal, G.P. Guidelines on the management of ascites in cirrhosis. Gut 2021, 70, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Biggin, S.W.; Angeli, P.; Garcia-Tsao, G.; Ginès, P.; Ling, S.C.; Nadim, M.K.; Wong, F.; Kim, W.R. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 74, 1014–1048. [Google Scholar] [CrossRef] [PubMed]
- Ge, P.S.; Runyon, B.A. Treatment of patients with cirrhosis. N Engl J Med 2016, 375, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Pose, E.; Piano, S.; Juanola, A.; Ginès, P. Hepatorenal syndrome in cirrhosis. Gastroenterology 2024, 166, 588–604. [Google Scholar] [CrossRef]
- Runyon, B.A. Management of adult patients with ascites due to cirrhosis: Update 2012. Hepatology 2013, 57, 1651–1653. [Google Scholar] [CrossRef]
- Raco, J.; Bufalini, J.; Dreer, J.; Shah, V.; King, L.; Wang, L.; Evans, M. Paracentesis in anticoagulated patients. Intern Med J 2025, 55, 77–83. [Google Scholar] [CrossRef]
- Tan, J.L.; Lokan, T.; Chinnaratha, M.A.; Veysey, M. Risk of bleeding after abdominal paracentesis in liver disease: A meta-analysis. JGH Open 2024, 8, e70013. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Davitkov, P.; Allen, A.M.; Falck-Ytter, Y.T.; Stine, J.G. AGA technical review on coagulation in cirrhosis. Gastroenterology 2021, 161, 1630–1656. [Google Scholar] [CrossRef]
- Lin, S.; Wang, M.; Zhu, Y.; Dong, J.; Weng, Z.; Shao, L.; Chen, J.; Jiang, J. Hemorrhagic complications following abdominal paracentesis. Medicine 2015, 94, e2225. [Google Scholar] [CrossRef]
- Van Dorin, S.; Schwartz, A.; Tudas, R.; Sanchez, K.; Amarneh, M.; Kuperman, E. Bleeding risks with apixaban during paracentesis. Cureus 2025, 17, e80299. [Google Scholar]
- Ross, J.T.; Matthay, M.A.; Harris, H.W. Secondary peritonitis: Principles of diagnosis and intervention. BMJ 2018, 361, k1407. [Google Scholar] [CrossRef] [PubMed]
- Cusumano, G.; La Via, L.; Terminella, A.; Sorbello, M. Re-expansion pulmonary edema as a life-threatening complication in massive, long-standing pneumothorax: A case series and literature review. J Clin Med 2024, 13, 2667. [Google Scholar] [CrossRef] [PubMed]
- Hibbert, R.M.; Atwell, T.D.; Lekah, A.; Patel, M.D.; Carter, R.E.; McDonald, J.S.; Rabatin, J.T. Safety of ultrasound-guided thoracentesis in patients with abnormal preprocedural coagulation parameters. Chest 2013, 144, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Paparoupa, M.; Wege, H.; Creutzfeldt, A.; Sebode, M.; Uzunoglu, F.G.; Boenisch, O.; Nierhaus, A.; Izbicki, J.R.; Kluge, S. Perforation of the ascending colon during implantation of an indwelling peritoneal catheter: A case report. BMC Gastroenterol 2020, 20, 345. [Google Scholar] [CrossRef]
- Wong, C.L.; Holroyd-Leduc, J.; Thorpe, K.E.; Straus, S.E. Does this patient have bacterial peritonitis or portal hypertension? How do I perform a paracentesis and analyze the results? JAMA 2008, 299, 1166–1178. [Google Scholar] [CrossRef]
- Soriano, G.; Castellote, J.; Alvarez, C.; Girbau, A.; Gordillo, J.; Baliellas, C.; Casas, M.; Pons, C.; Román, E.M.; Maisterra, S.; Xiol, X. Secondary bacterial peritonitis in cirrhosis: A retrospective study of clinical and analytical characteristics, diagnosis and management. J Hepatol 2010, 52, 39–44. [Google Scholar] [CrossRef]
- Miller, J.M.; Binnicker, M.J.; Campbell, S.; Carroll, K.C.; Chapin, K.C.; Gilligan, P.H.; Gonzalez, M.D.; Jerris, R.C.; Kehl, S.C.; Patel, R.; Pritt, B.S. Guide to utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clin Infect Dis 2024, ciae104. [Google Scholar] [CrossRef]
- Pinchot, J.W.; Kalva, S.P.; Majdalany, B.S.; Kim, C.Y.; Ahmed, O.; Asrani, S.K.; Cash, B.D.; Eldrup-Jorgensen, J.; Kendi, A.T.; Scheidt, M.J.; Sella, D.M. ACR Appropriateness Criteria® radiologic management of portal hypertension. JACR 2021, 18, S153–S173. [Google Scholar] [CrossRef]
- Asciak, R.; Bedawi, E.O.; Bhatnagar, R.; Clive, A.O.; Hassan, M.; Lloyd, H.; Reddy, R.; Roberts, H.; Rahman, N.M. British Thoracic Society clinical statement on pleural procedures. Thorax 2023, 78, s43–s68. [Google Scholar] [CrossRef]
- Wilcox, M.E.; Chong, C.A.; Stanbrook, M.B.; Tricco, A.C.; Wong, C.; Straus, S.E. Does this patient have an exudative pleural effusion? The Rational Clinical Examination systematic review. JAMA 2014, 311, 2422–2431. [Google Scholar] [CrossRef]
- Yataco, A.C.; Soghier, I.; Hébert, P.C.; Belley-Cote, E.; Disselkamp, M.; Flynn, D.; Halvorson, K.; Iaccarino, J.M.; Lim, W.; Lindenmeyer, C.C.; Miller, P.J. Transfusion of fresh frozen plasma and platelets in critically ill adults: An American College of Chest Physicians clinical practice guideline. Chest 2025. [Google Scholar] [CrossRef]
- Linder, K.; Epelbaum, O. Percutaneous pleural drainage in patients taking clopidogrel: Real danger or phantom fear? JAMA 2014, 311, 2422–2431. [Google Scholar] [CrossRef]
- Sundaralingam, A.; Bedawi, E.O.; Harriss, E.K.; Munavvar, M.; Rahman, N.M. The frequency, risk factors, and management of complications from pleural procedures. Chest 2022, 161, 1407–1425. [Google Scholar] [CrossRef]
- Sagar, A.E.S.; Landaeta, M.F.; Adrianza, A.M.; Aldana, G.L.; Pozo, L.; Armas-Villalba, A.; Toquica, C.C.; Larson, A.J.; Vial, M.R.; Grosu, H.B.; Ost, D.E. Complications following symptom-limited thoracentesis using suction. Eur Respir J 2020, 56, 1902356. [Google Scholar] [CrossRef]
- Dangers, L.; Giovannelli, J.; Mangiapan, G.; Alves, M.; Bigé, N.; Messika, J.; Morawiec, E.; Neuville, M.; Cracco, C.; Béduneau, G.; Terzi, N. Antiplatelet drugs and risk of bleeding after bedside pleural procedures: A national multicenter cohort study. Chest 2021, 159, 1621–1629. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



