Submitted:
26 September 2025
Posted:
09 October 2025
You are already at the latest version
Abstract
Endometriosis manifests as ectopic endometrial tissue outside the uterine cavity. This common disease can sometimes appear at unusual anatomical sites or within the intestinal tract, growing as a lesion and mimicking cancer. Such tumor-like endometriosis lesions are relatively uncommon and biologically intriguing. This study is a retrospective case series of 14 patients presenting with tumor-like endometriosis at a single institution between 2011 and 2022. Unlike conventional endometriosis, these tumor-like lesions were generally sizable and clinically presented as a groin mass, aorta wall, omentum, bowel wall, and lymph nodes, all of which raised suspicion for malignancy, despite eleven (78.6%) of the 14 cases having a history or clinical signs of endometriosis. Laser capture microdissection was used to isolate epithelial cells from endometriotic glands in tissue sections prepared from formalin-fixed paraffin-embedded blocks, and the microdissected epithelium was analyzed for cancer-driver mutations. A total of 11 cancer-driver mutations were identified in 6 (43%) of the 14 patients, with four patients harboring multiple mutations. Recurrent mutations included KRAS-activating mutations in four cases and ARID1A-inactivating mutations in two cases. Additional mutations involved PIK3CA, CTNNB1, CHD4, MYD88, and STAG1. The mutation frequency in cancer driver genes within this cohort was comparable to that observed in conventional endometriosis located in pelvic tissues, ovaries, and fallopian tubes, suggesting that these mutations may have roles beyond their canonical tumor-promoting functions in tumor-like endometriosis.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Sample Selection
2.2. Preparation of Tissue for Whole-Exome Sequencing
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Competing interests statement and acknowledgements
Institutional Review Board Statement
References
- Bulun, S.E. Endometriosis. N Engl J Med 2009, 360, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Nicholes, K.; Shih, I.M. The Origin and Pathogenesis of Endometriosis. Annu Rev Pathol 2020, 15, 71–95. [Google Scholar] [CrossRef] [PubMed]
- Simoens, S.; Dunselman, G.; Dirksen, C.; Hummelshoj, L.; Bokor, A.; Brandes, I.; Brodszky, V.; Canis, M.; Colombo, G.L.; DeLeire, T.; et al. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod 2012, 27, 1292–1299. [Google Scholar] [CrossRef]
- Wilbur, M.A.; Shih, I.M.; Segars, J.H.; Fader, A.N. Cancer Implications for Patients with Endometriosis. Semin Reprod Med 2017, 35, 110–116. [Google Scholar] [CrossRef]
- Chui, M.H.; Wang, T.L.; Shih, I.M. Endometriosis: benign, malignant, or something in between? Oncotarget 2017, 8, 78263–78264. [Google Scholar] [CrossRef]
- Victory, R.; Diamond, M.P.; Johns, D.A. Villar's nodule: a case report and systematic literature review of endometriosis externa of the umbilicus. J Minim Invasive Gynecol 2007, 14, 23–32. [Google Scholar] [CrossRef]
- Andres, M.P.; Arcoverde, F.V.L.; Souza, C.C.C.; Fernandes, L.F.C.; Abrao, M.S.; Kho, R.M. Extrapelvic Endometriosis: A Systematic Review. J Minim Invasive Gynecol 2020, 27, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Dalkalitsis, A.; Salta, S.; Tsakiridis, I.; Dagklis, T.; Kalogiannidis, I.; Mamopoulos, A.; Daniilidis, A.; Athanasiadis, A.; Navrozoglou, I.; Paschopoulos, M.; et al. Inguinal endometriosis: A systematic review. Taiwan J Obstet Gynecol 2022, 61, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, T.; Ishihara, S. Omental Endometriosis. N Engl J Med 2021, 384, e21. [Google Scholar] [CrossRef]
- Anglesio, M.S.; Papadopoulos, N.; Ayhan, A.; Nazeran, T.M.; Noe, M.; Horlings, H.M.; Lum, A.; Jones, S.; Senz, J.; Seckin, T.; et al. Cancer-Associated Mutations in Endometriosis without Cancer. N Engl J Med 2017, 376, 1835–1848. [Google Scholar] [CrossRef] [PubMed]
- Suda, K.; Nakaoka, H.; Yoshihara, K.; Ishiguro, T.; Tamura, R.; Mori, Y.; Yamawaki, K.; Adachi, S.; Takahashi, T.; Kase, H.; et al. Clonal Expansion and Diversification of Cancer-Associated Mutations in Endometriosis and Normal Endometrium. Cell Rep 2018, 24, 1777–1789. [Google Scholar] [CrossRef]
- Li, L.; Antero, M.F.; Zhang, M.; Chu, T.; Seckin, T.; Ayhan, A.; Pisanic, T.; Wang, T.L.; Cope, L.; Segars, J.; et al. Mutation and methylation profiles of ectopic and eutopic endometrial tissues. J Pathol 2021, 255, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Lac, V.; Verhoef, L.; Aguirre-Hernandez, R.; Nazeran, T.M.; Tessier-Cloutier, B.; Praetorius, T.; Orr, N.L.; Noga, H.; Lum, A.; Khattra, J.; et al. Iatrogenic endometriosis harbors somatic cancer-driver mutations. Hum Reprod 2019, 34, 69–78. [Google Scholar] [CrossRef]
- Orr, N.L.; Albert, A.; Liu, Y.D.; Lum, A.; Hong, J.; Ionescu, C.L.; Senz, J.; Nazeran, T.M.; Lee, A.F.; Noga, H.; et al. KRAS mutations and endometriosis burden of disease. J Pathol Clin Res 2023, 9, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Noe, M.; Ayhan, A.; Wang, T.L.; Shih, I.M. Independent development of endometrial epithelium and stroma within the same endometriosis. J Pathol 2018, 245, 265–269. [Google Scholar] [CrossRef]
- Li, L.; Yue, P.; Song, Q.; Yen, T.T.; Asaka, S.; Wang, T.L.; Beavis, A.L.; Fader, A.N.; Jiao, Y.; Yuan, G.; et al. Genome-wide mutation analysis in precancerous lesions of endometrial carcinoma. J Pathol 2021, 253, 119–128. [Google Scholar] [CrossRef]
- Wu, R.C.; Wang, P.; Lin, S.F.; Zhang, M.; Song, Q.; Chu, T.; Wang, B.G.; Kurman, R.J.; Vang, R.; Kinzler, K.; et al. Genomic landscape and evolutionary trajectories of ovarian cancer precursor lesions. J Pathol 2019, 248, 41–50. [Google Scholar] [CrossRef]
- Tokheim, C.J.; Papadopoulos, N.; Kinzler, K.W.; Vogelstein, B.; Karchin, R. Evaluating the evaluation of cancer driver genes. Proc Natl Acad Sci U S A 2016, 113, 14330–14335. [Google Scholar] [CrossRef]
- Notzold, A.; Moubayed, P.; Sievers, H.H. Endometriosis in the thoracic aorta. N Engl J Med 1998, 339, 1002–1003. [Google Scholar] [CrossRef] [PubMed]
- Beavis, A.L.; Matsuo, K.; Grubbs, B.H.; Srivastava, S.A.; Truong, C.M.; Moffitt, M.N.; Maliglig, A.M.; Lin, Y.G. Endometriosis in para-aortic lymph nodes during pregnancy: case report and review of literature. Fertil Steril 2011, 95, 2429–e2429. [Google Scholar] [CrossRef]
- Centini, G.; Ginetti, A.; Colombi, I.; Cannoni, A.; Giorgi, M.; Ferreira, H.; Fedele, F.; Pacifici, M.; Martire, F.G.; Zupi, E.; et al. Endometriosis of the appendix: prevalence, associated lesions, and proposal of pathogenetic hypotheses. A retrospective cohort study with prospectively collected data. Arch Gynecol Obstet 2024, 310, 1669–1675. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research, N.; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Vogelstein, B.; Papadopoulos, N.; Velculescu, V.E.; Zhou, S.; Diaz, L.A., Jr.; Kinzler, K.W. Cancer genome landscapes. Science 2013, 339, 1546–1558. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, A.; Mao T-L. ; Rahmanto, Y.S.; Zeppernick, F.; Ogawa, H.; Wu, R.C.; Wang, T.L.; Shih, I.M. Increased proliferation in atypical hyperplasia/endometrioid intraepithelial neoplasia of the endometrium with concurrent inactivation of ARID1A and PTEN tumour suppressors. J Patho Clin Res 2015, 1, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Suryo Rahmanto, Y.; Shen, W.; Shi, X.; Chen, X.; Yu, Y.; Yu, Z.C.; Miyamoto, T.; Lee, M.H.; Singh, V.; Asaka, R.; et al. Inactivation of Arid1a in the endometrium is associated with endometrioid tumorigenesis through transcriptional reprogramming. Nat Commun 2020, 11, 2717. [Google Scholar] [CrossRef]
- Mandal, J.; Yu, Z.C.; Shih, I.M.; Wang, T.L. ARID1A loss activates MAPK signaling via DUSP4 downregulation. J Biomed Sci 2023, 30, 94. [Google Scholar] [CrossRef]
- Dinulescu, D.M.; Ince, T.A.; Quade, B.J.; Shafer, S.A.; Crowley, D.; Jacks, T. Role of K-ras and Pten in the development of mouse models of endometriosis and endometrioid ovarian cancer. Nat Med 2005, 11, 63–70. [Google Scholar] [CrossRef]
- Cheng, C.W.; Licence, D.; Cook, E.; Luo, F.; Arends, M.J.; Smith, S.K.; Print, C.G.; Charnock-Jones, D.S. Activation of mutated K-ras in donor endometrial epithelium and stroma promotes lesion growth in an intact immunocompetent murine model of endometriosis. J Pathol 2011, 224, 261–269. [Google Scholar] [CrossRef]
- Yoo, J.Y.; Kim, T.H.; Fazleabas, A.T.; Palomino, W.A.; Ahn, S.H.; Tayade, C.; Schammel, D.P.; Young, S.L.; Jeong, J.W.; Lessey, B.A. KRAS Activation and over-expression of SIRT1/BCL6 Contributes to the Pathogenesis of Endometriosis and Progesterone Resistance. Sci Rep 2017, 7, 6765. [Google Scholar] [CrossRef]
- Pandya, D.; Tomita, S.; Rhenals, M.P.; Swierczek, S.; Reid, K.; Camacho-Vanegas, O.; Camacho, C.; Engelman, K.; Polukort, S.; RoseFigura, J.; et al. Mutations in cancer-relevant genes are ubiquitous in histologically normal endometrial tissue. Gynecol Oncol 2024, 185, 194–201. [Google Scholar] [CrossRef]
- Bulun, S.E. Endometriosis and ovulatory menstruation: beyond the Sampson principle. J Clin Invest 2025, 135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhu, F.; Tong, Y.; Shi, D.; Zhang, J. CHD4 R975H mutant activates tumorigenic pathways and promotes stemness and M2-like macrophage polarization in endometrial cancer. Sci Rep 2024, 14, 18617. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Lin, J.; Rong, L.; Wu, S.; Deng, Z.; Fatkhutdinov, N.; Zundell, J.; Fukumoto, T.; Liu, Q.; Kossenkov, A.; et al. ARID1A promotes genomic stability through protecting telomere cohesion. Nat Commun 2019, 10, 4067. [Google Scholar] [CrossRef] [PubMed]

| Extreme endometriosis characteristics (n = 14) | |
|---|---|
| Race, n (%) | |
| White | 4 (28.57) |
| Asian | 3 (21.43) |
| African American | 6 (42.86) |
| Other | 1 (7.14) |
| ASRM stage, n (%) | |
| Stage I | 0 (0) |
| Stage II | 2 (14.29) |
| Stage III | 0 |
| Stage IV | 12 (85.71) |
| Age at surgery (y), mean (SD) | 39.64 (9.32) |
| BMI at surgery (kg/m2), mean (SD) | 29.13 (7.69) |
| Other gynecological conditions, n (%) | |
| Fibroids, n (%) | 8 (57.14) |
| Adenomyosis, n (%) | 5 (35.71) |
| Pregnancy history, n (%) | |
| Nulliparous | 9 (64.29) |
| Parous | 5 (35.71) |
| Smoking history, n (%) | |
| Reports smoking | 4 (28.57) |
| Does not report smoking | 10 (71.43) |
| History of medical treatment for endometriosis, n (%) | 4 (28.57) |
| History of prior surgical management of endometriosis, n (%) | 8 (57.14) |
| Case | Lesions | Presenting symptom(s) | Stage | CDM(s) | Hormonal treatment | Surgical treatment | Other GYN conditions | Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | Umbilical nodule | Dysmenorrhea | 2 | None | Yes | No | Fibroids | Repeat surgery |
| 2 | Groin | Chronic groin pain | 4 | KRAS (c.35G>A; p.Gly12Asp) | No | No | None | Pursuing infertility treatment |
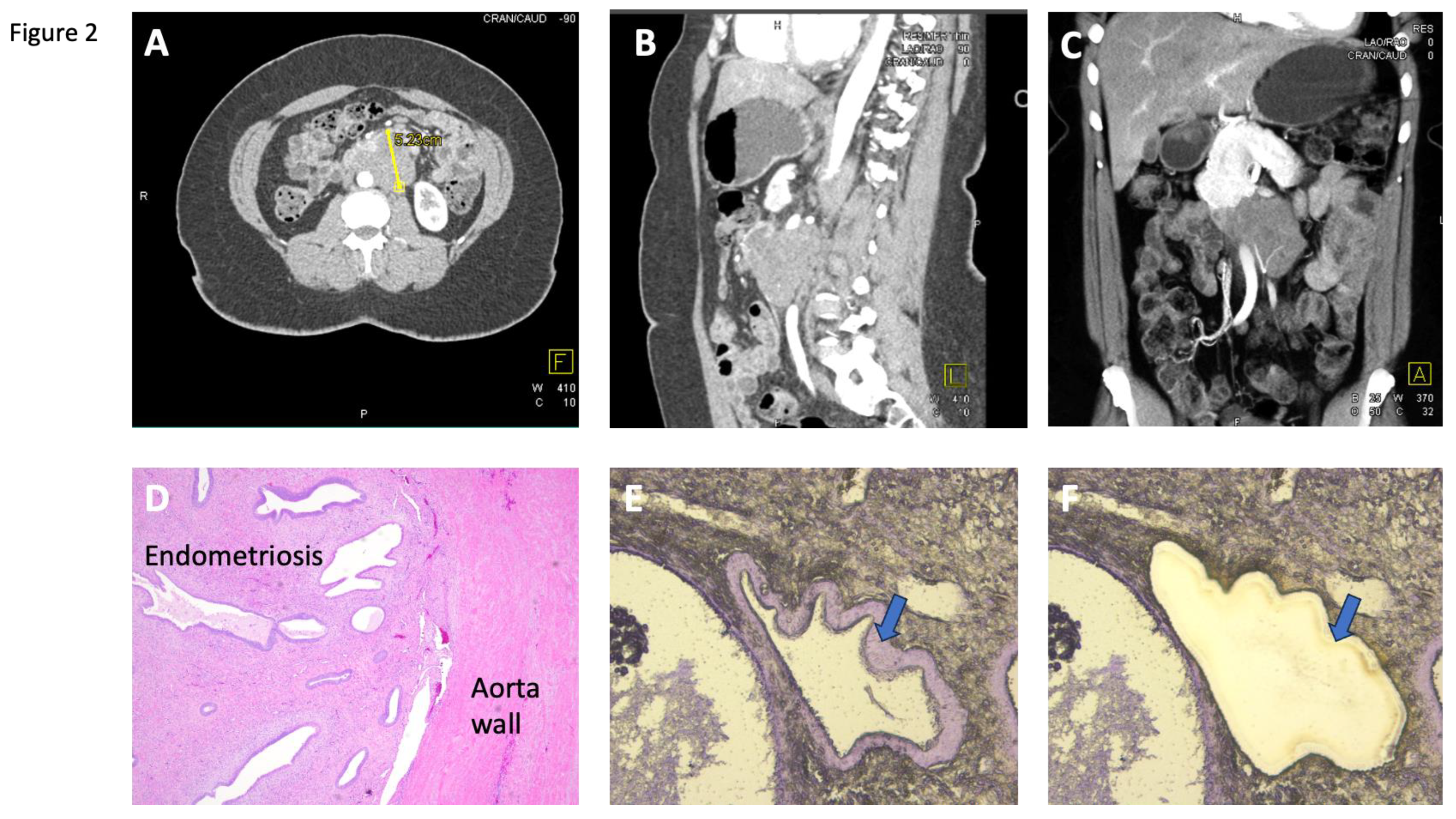
| 3 | Aorta | Chronic pelvic pain | 4 | CTNNB1 (c.599G>A; p.Arg200His), ARID1A (c.4336C>T;p.Arg1446Term) | No | Yes | Fibroids | Lost to follow-up |
| 4 | LN, colonic wall | Chronic pelvic pain, dysmenorrhea | 4 | None | No | No | Fibroids, Adenomyosis | Pain improved |
| 5 | Omentum | Chronic pelvic pain, dysmenorrhea | 4 | None | Yes | No | Adenomyosis | Lost to follow-up |
| 6 | Sigmoid colonic wall, LN | Dysmenorrhea, constipation, SBO | 4 | CHD4 (c.2924G>A; p.Arg975His), MYD88, (C.71C>T; P.ALA24VAL) STAG2 (c.3467+1G>A) | Yes | Yes | Adenomyosis | Pain improved |
| 7 | Omentum and rectal wall | Dysmenorrhea, constipation | 4 | None | No | No | None | Lost to follow-up |
| 8 | Rectosigmmoid colonic wall | Chronic pelvic pain, SBO | 4 | KRAS (c.34G>T; p.Gly12Cys), ARID1A (c.197C>T; p.Pro66Leu) | No | Yes | Fibroids, Adenomyosis | Controlled by progestin |
| 9 | Sigmoind colonic wall | SBO, chronic pelvic pain | 4 | None | No | Yes | Fibroids, Adenomyosis | Post-menopausal after surgery |
| 10 | Colonic wall | Chronic pelvic pain | 4 | KRAS (c.35G>C; P.Gly12Ala) | No | Yes | Fibroids | Concern for recurrence |
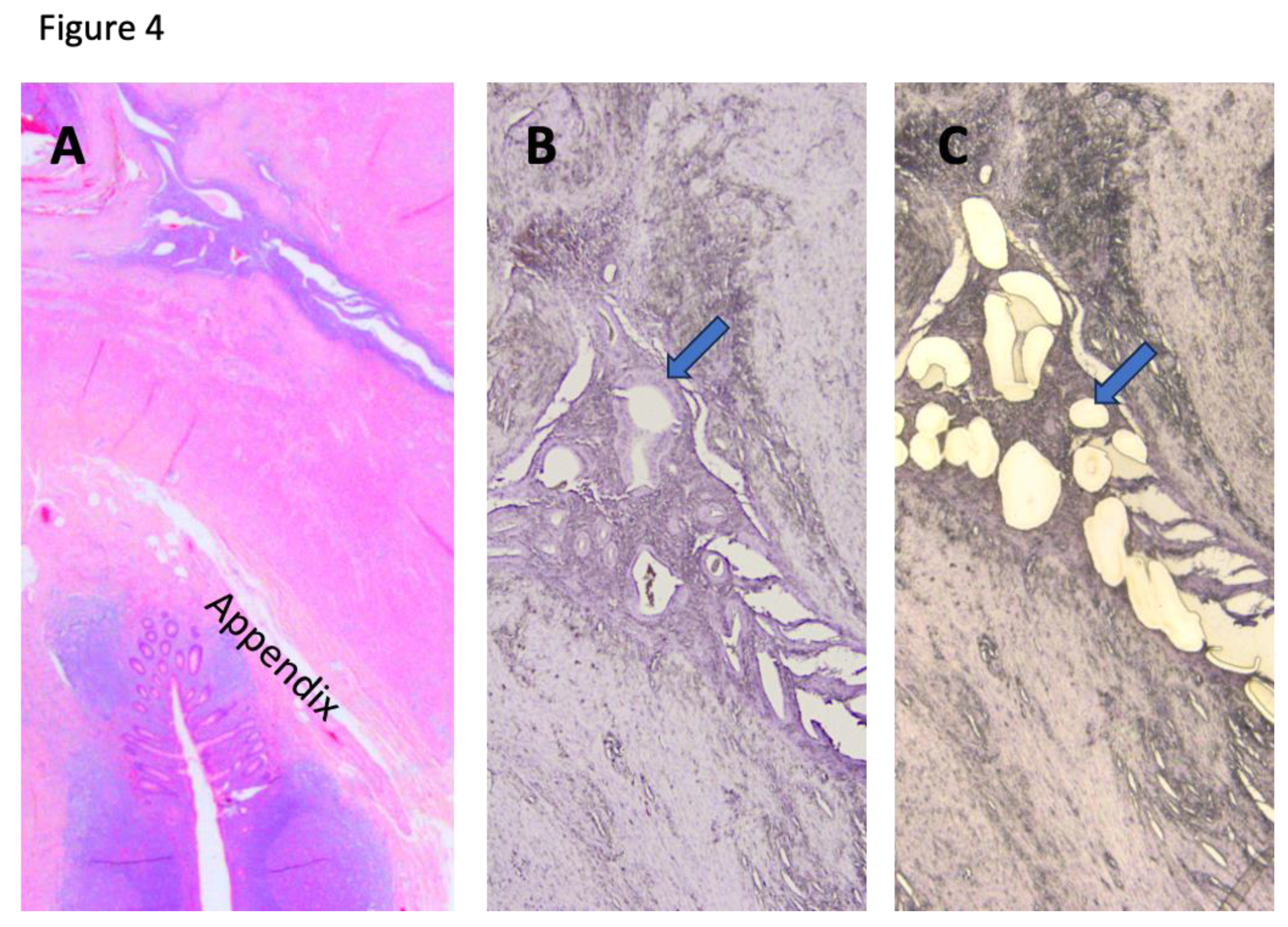
| 11 | Appendix | Chronic pelvic pain | 4 | None | No | Yes | Fibroids | Pain improved |
| 12 | Appendix | Chronic pelvic pain, dyschezia | 2 | KRAS (c.35G>T; p.Gly12Val), PIK3CA (c.1035T>A;Asn345Lys) | No | Yes | Fibroids | Lost to follow-up |
| 13 | Appendix | Chronic pelvic pain, nausea, vomiting, SBO | 4 | None | Yes | Yes | None | Pain continued, controlled by progestin |
| 14 | Appendix | Chronic pelvic pain | 4 | None | No | No | None | Lost to follow-up |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



