
Submitted:
24 September 2025
Posted:
06 October 2025
You are already at the latest version
Abstract
Objective This study is to provide evidence from Nigeria on women’s lived experiences of menopause is sparse, necessitating qualitative inquiry to inform contextually appropriate interventions.DesignProspective cross - sectional study SettingUrban and rural regions of NigeriaPopulation or SampleMidlife womenMethods As part of the MARIE project, semi-structured interviews were conducted with midlife women across urban and rural regions of Nigeria. Participants were purposively sampled to capture diverse socioeconomic backgrounds and menopausal stages. Data were analysed using thematic content analysis, with coding informed by health inequality and gender frameworks, and findings were triangulated by multiple researchers to enhance validity.Results Analysis revealed three overarching themes: (1) structural inequalities in healthcare, including delayed recognition of symptoms, inadequate clinician knowledge, and limited access to hormone replacement therapy; (2) sociocultural and gendered barriers, such as stigma, misperceptions of menopause as a “natural end” requiring no care, and silencing within families; and (3) coping and resilience strategies, encompassing reliance on peer networks, faith-based approaches, and lifestyle adaptations in the absence of formal support. Urban participants reported marginally better access to information and services, while rural women described significant neglect, often relying on informal care.Main Outcome MeasuresThemes emerged from the qualitative interviewsConclusionsThis study highlights profound inequalities shaping menopausal experiences in Nigeria, reflecting gaps in healthcare training, policy attention, and community awareness. The findings emphasise the need for integrated, culturally sensitive strategies, including the incorporation of menopause into primary care, universal access to safe affordable treatments, and targeted public health education.
Keywords:
Menopause
; Nigeria
; Qualitative Analysis
; MARiE Project
Background
Nigeria, with an estimated population of 237.5 million as of mid-2025, comprises approximately 115 million women about 50 percent of the populace[1,2]. Among them, roughly one in three women, nearly 19 million is aged 40 years or older, entering the critical age band for perimenopause, menopause, and post-menopause[3,4]. This life-stage transition unfolds within a complex nexus of biological change, chronic disease burden, sociocultural norms, and systemic inequalities, all shaped by Nigeria’s unique demographic and healthcare landscape [5].
Perimenopause in Nigeria usually occurs during the early 40s, characterised by erratic ovarian steroid production, menstrual irregularity, vasomotor episodes and urogenital symptoms[6]. The symptom burden often coincides with endemic health challenges such as anaemia, hypertension and uterine fibroids which exacerbate distress and complicate diagnosis[7]. Natural menopause the cessation of menses for 12 continuous months typically occurs around age 47 to 50 among Nigerian women, similar to other West African cohorts, though data remain limited[8,9]. Post-menopausal hypo-oestrogenism accelerates risks for osteoporosis, cardiovascular disease, urogenital atrophy, and sexual dysfunction[10]. Despite routine screening for bone mineral density assessment, cardiovascular risk stratification, and genitourinary syndrome of menopause (GSM) evaluation remain sporadic in primary and secondary healthcare, particularly in rural and under-resourced regions[11].
Surgical menopause is a significant phenomenon in Nigeria, driven largely by high prevalence of uterine fibroids and limited access to minimally invasive alternatives. Many women undergo hysterectomy with or without bilateral oophorectomy leading to abrupt onset of menopausal symptoms early in life[12,13]. Unfortunately, structured pre-operative counselling, risk assessment, and post-operative follow-up are not consistently provided, especially outside tertiary centres in urban areas. Medical menopause on the other hand is attributed by premature oestrogen deprivation[14]. These transitions can result in more intense vasomotor, emotional, sexual, and skeletal symptoms than natural menopause, particularly in younger women whose quality of life and reproductive trajectories are still evolving.
Sociocultural contexts deeply influence how menopausal transitions are perceived, communicated, and addressed in Nigeria[15]. Within many communities urban, peri-urban, and rural menopause is considered an inevitable ageing process, to be endured rather than treated[16].
Crucially, Nigeria lacks robust, locally generated evidence on the prevalence, severity, and lived experience of perimenopause, menopause, and post-menopause[17]. Most clinical guidance is borrowed from high-income countries with different population risk profiles, formulations, and care infrastructure[18]. There is a dearth of disaggregated data on symptom patterns, socioeconomic or ethnic disparities, health-economic impacts, and the real-world safety and efficacy of HRT and non-hormonal therapies. Implementation research on task-sharing scalable behavioural interventions, and digital self-help tools adapted to Nigerian contexts is virtually absent. Without such evidence, women’s needs remain invisible, care remains piecemeal, and preventable morbidity continues unmitigated.
Rationale
MARIE Nigeria addresses these critical deficits by generating nationally representative, population-specific data targeting the estimated 36 million women aged 40 and over on the prevalence, symptom burden, and quality-of-life impacts of natural, surgical, and medical menopause in Nigeria. It intentionally captures disaggregated outcomes across socioeconomic, geographic, and cultural strata, thereby illuminating inequities and tailoring interventions to diverse communities. Through co-design with multidisciplinary stakeholders including clinicians, academics, community health workers, and women themselves, the MARIE project explores a multitude of phenomena linked to ageing. The MARIE Nigeria chapter’s mixed-methods design facilitates securing never seen before qualitative and quantitative data to inform practice and policies, as well as comparability of Nigerian data with global benchmarks while generating locally validated evidence for hormone and non-hormone modalities. This paper focuses on the experiences of menopausal women in Nigeria.
Methods
Study Design and Setting
This qualitative study formed part of the Nigerian arm of the MARIE WP2a project, a multi-country investigation into menopausal experiences and health inequalities. The Nigerian qualitative component aimed to explore the lived experiences of perimenopausal, menopausal, and post-menopausal individuals, focusing on barriers to care, sociocultural influences, and health system responses.
Data Collection
Semi-structured interviews were conducted with 21 participants recruited from urban and peri-urban communities across Nigeria, ensuring diversity in menopausal stage, education level, and occupational background. Participants were identified via purposive and snowball sampling, with inclusion criteria encompassing self-identification as biologically female, aged 40–65 years, and current or past experience of menopause (natural, surgical, or medical). Interviews were conducted in English or local languages, depending on participant preference, and were audio-recorded with consent. Field notes were taken to capture non-verbal cues and contextual details. Interviews lasted 45–90 minutes and were transcribed verbatim; where applicable, professional translation into English was undertaken, followed by accuracy checks.
Analytical Framework
The Delanerolle and Phiri Framework for equity-centred qualitative analysis was applied (Table 1). This framework is specifically designed for women’s health research in diverse and underrepresented populations, integrating thematic analysis with an intersectional equity lens. It operationalises analysis in four iterative stages:
Data Analysis
Analysis followed a hybrid inductive deductive thematic approach. Deductive coding was guided by the Delanerolle and Phiri framework domains, while inductive coding allowed emergent themes (Table 2) to be captured. Two researchers independently coded the transcripts and coding decisions were discussed with the principal investigator to resolve discrepancies, and ensure intercoder reliability. Reflexivity was maintained through analytic memos and discussion of positionality, recognising how researcher backgrounds could influence interpretation. Triangulation of interview data with field notes enhanced trustworthiness, and an audit trail was maintained to support transparency. Saturation was assessed when no new codes or themes emerged in subsequent transcripts.
Ethics
The study received ethical approval from the Nnamdi Azikiwe University Teaching Hospital (Reference: RUIH/CS/66/VOL 16/VER 3/388/2023/121). The study was conducted in accordance with the Declaration of Helsinki.
Results
We analysed 21 interviews (Table 3) with Nigerian women traversing peri- to post-menopause using the Delanerolle–Phiri framework’s four interrelated domains of Biological, Psychological, Socio-cultural, Health System to integrate symptom profiles with context and care experiences.
Biological Domain: Symptom Profiles, Physiology, Comorbidity
Participants described a wide spectrum of vasomotor phenotypes. Some reported highly visible episodes whilst others downplayed the severity. A minority of participants denied classic symptoms altogether (PID-07, PID-13).
“Dace my colleagues with sweat that’s all over my face” (PID-03)
“The only noticeable symptom… was internal heat… manageable” (PID-14).
Sleep split between restorative routines and insomnia were identified. Restorative sleepers emphasised regularity although where heat and power reliability intruded, women improvised whilst some rated their quality of sleep to be poor.
“I sleep like a baby… once it’s seven–eight I’m sleeping off” (PID-13)
“I slept well… 9 p.m.–4:30/5 a.m.” (PID-14)
“Rechargeable fan… has been helping me to sleep better” (PID-03)
“I would rate my sleep… around 4 out of 10” (PID-06)
“I woke… ~3 and didn’t sleep again” (PID-12).
Musculoskeletal and pelvic symptom burden ranged from activity-linked strain, continuous pain to intermittent pelvic pain and stress-related incontinence.
“Once I stand… 30 minutes, I’ll start looking for a place to sit” (PID-08)
“After long shifts” (PID-16)
“Continuous pain: YES… stops usual activities: YES” (PID-17).
“If I don’t get the bathroom on time, I might leak” (PID-03)
Hypertension was common within the sample alongside of diabetes. Some participants used HRT and others didn’t as they experienced mild symptoms or preferred to not use western medication. Those using HRT confirmed they felt better.
“Every day I don’t miss taking my drug” (PID-11)
HRT—“BETTER” (PID-18; PID-19).
Supplements were widespread but variably effective.
“Starflower oil… don’t see any change” (PID-03)
“Evening primrose” helps (PID-17).
Psychological domain: emotion, cognition, behaviour
Across cases, women described a wide affective range, from pronounced dysphoria and irritability to durable positive affect. Mood disturbance was commonly situational intensifying during work, heat, or interpersonal strain and often accompanied by a drive to withdraw. Several participants reported episodic but profound loss of motivation and calm, whereas others articulated stable wellbeing and resistance to low mood. This heterogeneity indicates that state of affect during the menopausal transition is highly context-dependent, with occupational and environmental stressors amplifying symptoms in some, and personal resources buffering others.
Signals of hopelessness and suicidality were present in a non-trivial subset. These endorsements typically co-occurred with untreated pain, financial pressure, or hostile workplaces, and were rarely paired with clear crisis pathways. The variability of these accounts ranging from episodic worry to direct acknowledgement that life may not be worth living underscores the need for routine risk enquiry and brief safety planning within menopause care.
“Sadness and aggressiveness without knowing the exact reason” (PID-21)
“Wanting to be alone” (PID-15)
“I felt hopeless YES” (PID-17)
“life is not worth living: YES” (PID-18)
“I feel like I’m no longer beautiful, no longer myself” (PID-06).
Formal therapy was rare and variably appraised
“I don’t really appreciate… cognitive behavioural therapy” (PID-03)
Cognitive complaints centred on concentration lapses and mental fatigue. Many participants adopted pragmatic compensations such as external memory supports, micro-breaks, pacing and activity trimming to stabilise functioning; others relied on social support, notably confiding in trusted peers. Avoidant coping provided short-term relief but risked social disconnection, while approach-oriented strategies were associated with sustained role performance.
Attitudes to formal psychological therapy particularly cognitive behavioural therapy (CBT) were mixed. Several women expressed low familiarity or scepticism; others were open to trying CBT but had not accessed it; one reported prior use. In a few interviews, participants asserted that CBT “doesn’t help” despite no reported exposure, suggesting expectancy barriers and the need for plain-language explanations and guided self-help to support uptake. Where sleep remained intact and routines were stable, affective symptoms appeared more containable; in contrast, insomnia or heat-fragmented sleep was associated with greater cognitive–affective intrusiveness.
“Very often, especially during work hours” (PID-15)
“I don’t even know what depression is… always very happy” (PID-13)
Participants compensated for focus lapses
“I… jot down notes” (PID-16)
and used pacing/rest: “let me stop… going to morning mass… I got my strength back” (PID-08).
Taken together, these narratives depict a biopsychosocial loop: vasomotor discomfort, sleep disruption, and workplace pressure heighten arousal and negative affect; coping responses then shape trajectories either narrowing participation through withdrawal or preserving function through planning, pacing, and social connection. A stepped, preference-sensitive approach combining brief CBT elements, sleep strategies, and low-cost occupational adjustments aligns with expressed needs and the observed spectrum of risk and resilience.
Socio-Cultural Domain: Norms, Roles, Stigma, Socioeconomic Position
Menopause intersected with demanding occupational roles, often amplifying pre-existing pressures. Stress levels rose markedly from pre-menopausal baselines, with participants describing peaks of “8 or 9 out of 10” during symptomatic phases. Contributing factors included shift work, environmental heat, and the demands of public-facing duties. However, meaningful and autonomous roles acted as buffers, offering a sense of control, purpose, and fulfilment. For some, work particularly advisory or volunteer roles was described as a source of joy, independence, and personal agency.
“8 or 9 out of 10” (PID-03; also PID-15)
“My work is just to advise… I feel so comfortable” (PID-11)
“Volunteering gives me joy… I drive myself” (PID-13)
Cultural Explanations and Stigma
Cultural and spiritual frameworks shaped how women understood and navigated menopause. For some, menopause was framed as a natural or divinely guided life stage, influencing their rejection of hormonal therapies. At the same time, visible symptoms such as excessive sweating prompted embarrassment and a tendency towards social withdrawal. These experiences highlight the interplay between personal belief systems, cultural norms, and the social stigma surrounding menopausal symptoms.
“I believe in allowing God… wouldn’t advise… hormonal drugs” (PID-11)
“Face… colleagues with sweat” (PID-03)
“Quiet time and space” (PID-15)
Financial and logistical challenges were persistent and deeply intertwined with symptom burden. Participants cited the costs of transportation, high workloads, and low incomes as ongoing stressors. The pressure of meeting household expenses and managing bills exacerbated the physical and emotional impact of menopause, while also constraining access to timely and appropriate care.
“Transportation cost, workload” (PID-18; PID-19)
“Low income” and “bills to pay” (PID-20)
Health System: Organisation, Quality, and Access
Anticipatory information Gaps
Many participants entered menopause with little or no guidance from health professionals, leading to uncertainty and reactive care-seeking. This contrasted with the experiences of those who had received early information, who emphasised its value in enabling informed decisions and preparedness. Participants repeatedly expressed the need for education before symptom onset.
“Nobody has ever told me… I’ve never had… knowledge” (PID-11)
“Information is power” (PID-14)
“At an early stage” (PID-18; echoed PID-12, PID-21)
Primary Care and Pathways
Care was often fragmented and episodic. While some participants described supportive primary care interactions, others reported generic advice and long waiting times. Screening services, such as Pap smears, were offered without integrated menopause management. There was a strong demand for dedicated menopause services, including specialist clinics, counselling, and peer support.
“Doctor… advised Pap smear… negative” (PID-02)
“Long wait times… limited HRT discussions” (PID-16)
“Specialised clinics, counselling and support groups” (PID-16/21)
Resourcing and Affordability
Structural and financial barriers significantly hindered access to quality menopause care. Women described an absence of local doctors, high hospital costs, and perceptions of poor-quality services. These limitations drove some towards self-management with supplements, while physiotherapy and psychological support remained inaccessible for many.
“NO DOCTORS” and “high cost of hospital bills” (PID-19/20)
“Lack of quality care” (PID-17)
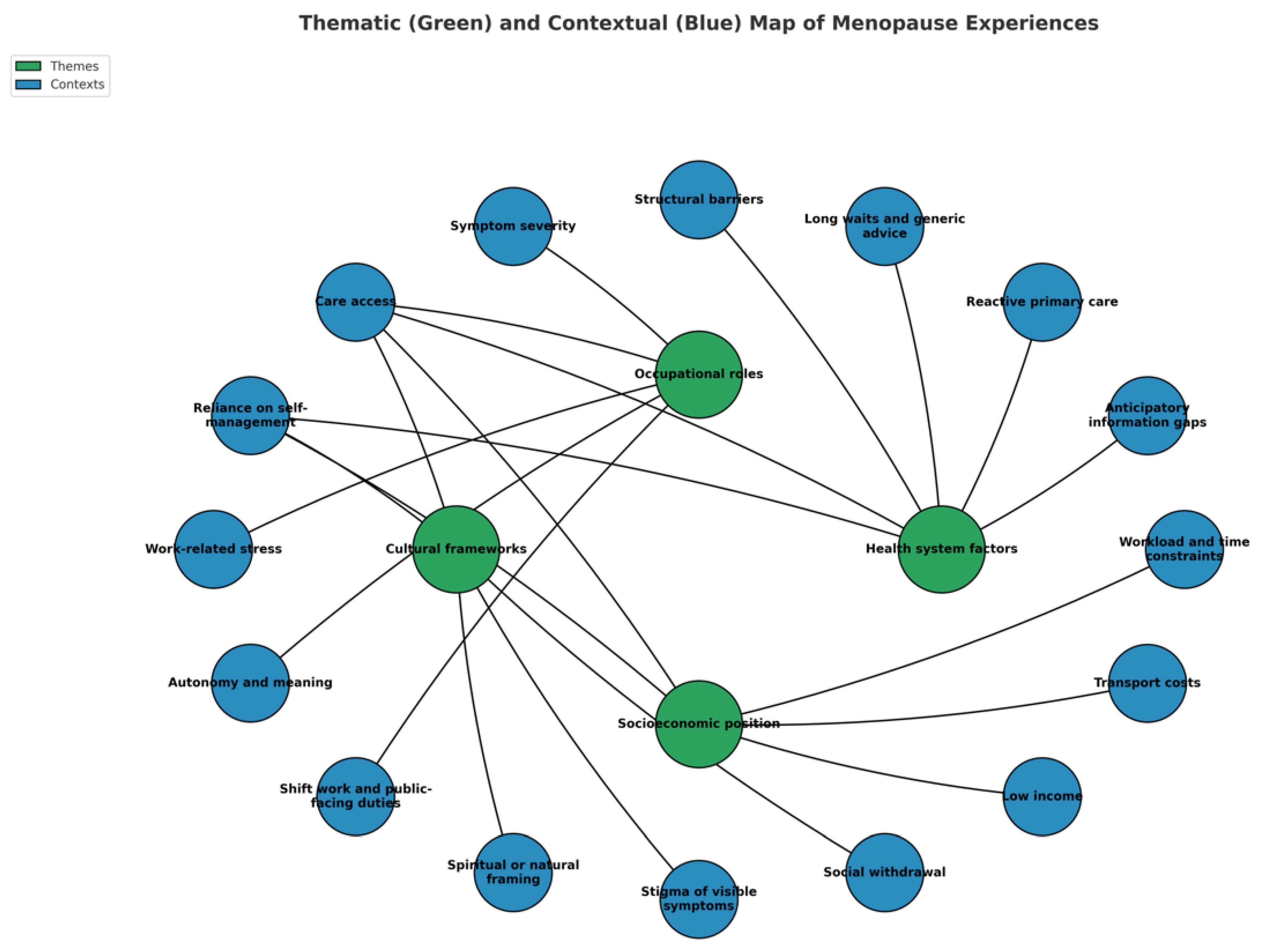
Cross-Correlation Context
Analysis across the 21 transcripts revealed complex interdependencies between occupational roles, cultural frameworks, socioeconomic positioning, and health system structures in shaping menopausal experiences. Work-related stress and identity emerged as pivotal drivers, with symptom severity often modulated by the degree of autonomy and meaning derived from employment. Women in advisory or voluntary roles reported emotional resilience despite physical discomfort, whereas those in shift-based, public-facing, or high-pressure roles experienced intensified symptom burden.
Cultural explanations intersected with health-seeking behaviours, influencing acceptance or rejection of clinical interventions. Spiritual framings of menopause as a natural or divinely guided process reduced inclination towards pharmacological management, particularly hormonal therapy. This was compounded by stigma surrounding visible symptoms, leading to concealment strategies such as withdrawal from social interaction.
Socioeconomic constraints consistently amplified symptom impact, with transportation costs, low income, and heavy workloads limiting both access to care and capacity for self-care. These pressures disproportionately affected women in lower-income brackets, creating a cyclical reinforcement of health inequalities.
Health system factors acted as both barriers and partial facilitators. Across transcripts, anticipatory information was either absent or provided too late to enable proactive management. While some participants benefited from supportive primary care engagement, most described reactive, generic consultations, long waiting times, and fragmented service delivery. Calls for specialised clinics, integrated counselling, and peer support groups were recurrent, reflecting unmet needs for holistic, tailored provision.
Structural deficits particularly scarcity of trained clinicians, high hospital fees, and perceptions of poor-quality care further entrenched inequities, pushing some towards self-management with supplements. The convergence of occupational strain, cultural framing, financial limitation, and inadequate health infrastructure created a multi-layered context in which menopause was not solely a biological transition but a socially and structurally mediated life stage, with substantial implications for equity in women’s health.
Figure 1.
Themes and contextual factors linked to the menopausal experience of Nigerian women.
Discussion
Interpretation
The study provides an unprecedented insight into menopause-related experiences in Nigeria, highlighting multidimensional health inequalities across clinical, social, and structural domains. The findings reveal that menopausal symptoms spanning vasomotor, psychological, cognitive, and musculoskeletal domains are often under-recognised and undertreated. Barriers to care were consistently reported, including inadequate healthcare provider knowledge, fragmented care pathways, lack of culturally sensitive health information, and socioeconomic constraints that limit access to appropriate treatment such as HRT. While symptom burden was comparable to reports from high-income settings, contextual differences emerged, particularly in symptom attribution, health-seeking behaviours, and societal perceptions of menopause. Crucially, the narratives reflect a convergence of biological transition and gendered sociocultural realities, where menopause is both a physiological process and a lived social experience influenced by cultural norms, economic structures, and health system limitations. This dual framing makes these findings especially relevant to shaping Nigeria’s response to midlife women’s health (Table 4).
Colloquial expressions such as “internal heat,” “weak bones,” or “body pains” are often used instead of medical terminology, reflecting embodied idioms of distress. Nonetheless, expectations around domestic labour, caregiving, religious observance, and social respectability often deter discussion of intimate symptoms like sexual pain, urinary discomfort, or depressed mood. While menopause may confer social recognition and elder status for some women, for others it intensifies marginalisation especially when symptoms impair productivity in informal sector economies. Intersectional factors including education level, household income, marital status, physical disability, and rurality further influence women’s ability to seek and receive care.
Clinical Impact
In the Nigerian healthcare context, the results emphasise an urgent need for targeted clinical interventions and professional training. Current clinical practice often lacks standardised protocols for menopause diagnosis and management, with many healthcare providers relying on symptomatic judgement rather than structured screening tools or evidence-based guidelines[19]. Misdiagnosis and the conflation of menopausal symptoms with psychiatric illness or unrelated chronic disease were recurrent themes in participant accounts. Furthermore, limited availability of HRT due to both supply chain issues and cost significantly constrains therapeutic options. These gaps perpetuate symptom burden and diminish quality of life, particularly among women in rural and semi-urban areas who face additional challenges in accessing secondary or tertiary care.
From a critical standpoint, these results expose an equity gap: although Nigeria’s health system is increasingly addressing non-communicable diseases, midlife women’s health remains peripheral in policy and training. Without integrating menopause care into primary healthcare protocols, opportunities for early intervention and holistic management will remain missed. The study therefore presents a call to embed menopause-specific screening, counselling, and treatment pathways within Nigeria’s existing primary care framework.
Healthcare systems in Nigeria face substantial structural barriers. Primary health clinics are under-resourced, workforce continuity is fragile, and national training curricula lack comprehensive modules on menopause care for doctors, nurses, midwives, pharmacists, and community health extension workers[20,21]. Access to HRT particularly safer options like transdermal oestrogens or oral micronised progesterone is limited by cost, inconsistent supply chains, and regulatory hurdles. Counselling on HRT’s benefits and risks, especially regarding venous thromboembolism, hypertension, and breast cancer, is not standardised or widely practiced. Non-hormonal options (e.g. selective serotonin reuptake inhibitors/serotonin-noradrenaline reuptake inhibitors for hot flushes, pelvic floor training, moisturisers, vaginal lignocaine) are unevenly available, particularly in public facilities. Diagnostic overshadowing due to comorbidities, such as thyroid disorders, depression, and anaemia is common. Systematic bone and cardiovascular screening post-menopause is sporadic and often unaffordable.
Policy Impact
The absence of dedicated policy frameworks for menopause in Nigeria reinforces a cycle of invisibility in health planning. While maternal health, reproductive health, and gender-based violence feature in national strategies, menopause is largely absent from official documents. This omission translates into under-resourcing, limited data collection, and the exclusion of menopause from essential medicines and health benefit schemes. The findings from this study provide an evidence base to advocate for policy integration linking menopause to Nigeria’s commitments under the Sustainable Development Goals (SDGs), particularly Goal 3 (Good Health and Well-being) and Goal 5 (Gender Equality)[22].
A critical policy implication is the need for inclusion of menopause-related medicines, including HRT, on the National Essential Medicines List, accompanied by subsidy mechanisms to make them affordable. Furthermore, national clinical guidelines should be updated to include menopause management as a priority within women’s health, recognising the condition as a determinant of workforce participation, healthy ageing, and social inclusion. These policy shifts would not only improve access to care but also signal recognition of menopause as a legitimate public health issue.
In workplace and policy domains, formal guidelines or occupational health provisions specific to menopause are virtually non-existent outside large-scale formal employers. Meanwhile, the majority of midlife Nigerian women work in the informal economy—with unpredictable schedules, limited social protection, no paid leave, and often physically demanding roles. These conditions amplify vasomotor and musculoskeletal symptoms and constrain self-management. National health insurance schemes offer limited coverage for menopause-related care, leading to high out-of-pocket spending and treatment discontinuation
Population Context
Menopause in Nigeria is shaped by complex cultural narratives that influence both personal experience and care-seeking behaviour. In many communities, menopause is framed as a natural and inevitable process that does not require medical intervention, while in others, it is associated with myths around diminished femininity, reduced sexual function, or social withdrawal. Such perceptions can delay symptom disclosure and deter healthcare engagement. The study’s results reveal that women often rely on informal support networks family, friends, religious groups rather than clinical services, highlighting both a resource and a gap.
These findings are novel in that they offer granular, context-specific insight into Nigerian women’s lived experiences, which have been largely absent from the global menopause literature dominated by high-income country perspectives. Initiating a broader conversation in Nigeria based on these results could catalyse changes in medical education, public health messaging, and service delivery models. Importantly, the evidence calls for a culturally responsive approach acknowledging local beliefs while addressing misinformation, improving accessibility, and ensuring affordability.
The novelty lies in shifting the discourse from menopause as a private, unspoken matter to a recognised public health priority, embedded in Nigeria’s health and gender equality agendas.
Conclusions
This study provides the first comprehensive, context-specific exploration of menopause in Nigeria, revealing multidimensional health inequalities across clinical, social, and structural domains. Menopausal symptoms are frequently under-recognised and undertreated, with barriers to care shaped by cultural narratives, socioeconomic constraints, and systemic gaps in provider knowledge and service provision. The findings highlight the urgent need to integrate menopause into primary healthcare, policy frameworks, and professional training, ensuring access to affordable, evidence-based treatments such as HRT and non-hormonal options. By reframing menopause as a public health priority linked to workforce participation, healthy ageing, and gender equality, this study provides an evidence base for culturally responsive, equity-driven interventions in Nigeria.
Evidence before this study
Previous evidence on menopause and midlife women’s health in Nigeria has been sparse, fragmented, and often limited to small-scale clinical or sociocultural studies. Health inequalities, particularly in relation to access to hormone replacement therapy (HRT), cultural stigma, and healthcare workforce training, remain underexplored in national and regional literature.
Added value of this study
This study provides the first qualitative, in-depth analysis of Nigerian women’s lived experiences of menopause through the MARIE project, capturing structural, cultural, and health system barriers. It highlights the intersection of gender norms, healthcare access, and sociocultural perceptions in shaping inequalities across the menopausal transition.
Implications of all the available evidence
The synthesis of global and Nigerian evidence demonstrates an urgent need for contextually tailored interventions, including improved clinician training, policy reform, and community-based education. Addressing menopause within Nigeria’s broader women’s health agenda could reduce inequalities, strengthen primary care responses, and enhance quality of life for midlife women.
Author Contributions
GD developed the ELEMI program and the MARIE project. This was furthered by GD and PP. GUE submitted and secured the ethics approval for the study. GHU and team collected data. GD and GUE conducted the data analysis. GD and GUE wrote the first draft and was furthered by all other authors. VP edited and formatted all versions of the manuscript. All authors critically appraised, reviewed and commented on all versions of the manuscript. All authors read and approved the final manuscript.
Funding
No funding
Code Availability
Not applicable
Ethics Approval
Obtained from Nnamdi Azikiwe University Teaching Hospital (RUIH/CS/66/VOL 16/VER 3/388/2023/121)
Consent to Participate
Obtained
Consent for Publication
All authors consented to publish this manuscript
Availability of Data and Material
The PIs and the study sponsor may consider sharing anonymous data upon reasonable a request.
Acknowledgements
MARIE Consortium: Aini Hanan binti Azmi, Alyani binti Mohamad Mohsin, Artini binti Abidin, , Choon-Moy Ho, Chinyere Ukamaka Onubogu, Diana Chin-Lau Suk, Eunice Yien-Mei Sim, Farhawa binti Zamri, Fatin Imtithal binti Adnan, Geok-Sim Lim, Jinn-Yinn Phang, John Yen-Sing Lee, Juhaida binti Jaafar, Karen Christelle, Kim-Yen Lee, Kingsley Chidiebere Nwaogu, Lee-Leong Wong, Min-Huang Ngu, Noorhazliza binti Abdul Patah, Nor Fareshah binti Mohd Nasir, Norhazura binti Hamdan, Nnaedozie Paul Obiegbu, Nurfauzani binti Ibrahim, Nurul Amalina Jaafar, Obinna Kenneth Nnabuchi, Pooja Lama, Puong-Rui Lau, Rakshya Parajuli, Rakesh Swarnakar, Rosdina Abd Kahar, Safilah Binti Dahian, Sapana Amatya, Sing-Yew Ting, Siti Nurul Aiman, Susan Chen-Ling Lo, Damayanthi Dassanayake, Nimesha Wijayamuni, Prasanna Herath, Thamudi Sundarapperuma, Vaitheswariy Rao, Xin-Sheng Wong, Xiu-Sing Wong, Yee-Theng Lau, Heitor Cavalini, Jean Pierre Gafaranga, Emmanuel Habimana, Chigozie Geoffrey Okafor, Oludolamu Oluyemesi Adedayo, Chinelo Onuegbuna Okoye, Babatunde Rufus Kumuyi, Onyebuchi Lynda Ngozi, Nnenna Josephine Egbonnaji, Ganesh Dangal, Om Kurmi, Oluwasegun Ajala Akanni, Perpetua Kelechi Enyinna, Yusuf Alfa, Theresa Nneoma Otis, Catherine Larko Narh Menka, Kwasi Eba Polley, Isaac Lartey Narh, Bernard B. Borteih, Andy Fairclough Michael Nnaa Otis, Jeremy Van Vlymen, Chidiebere Agbo, Francis Chibuike Anigwe, Chidimma Judith Anyaeche, Clementine Kanazayire, Jean Damascene Hanyurwimfura, Nwankwo Helen Chinwe, Stella Matutina Isingizwe, Jean Marie Vianney Kabutare, Dorcas Uwimpuhwe, Melanie Maombi, Ange Kantarama, Uchechukwu Kevin Nwanna, Benedict Erhite Amalimeh, Theodomir Sebazungu, Elius Tuyisenge, Yvonne Delphine Nsaba Uwera, Emmanuel Habimana, Nasiru Sani and Amarachi Pearl Nkemdirim, Fred Tweneboah-Koduah, Nana Afful-Minta, Bernard Mbwele, David Chibuike Ikwuka, Pradip K Mitra, Muhammad Irfan, Rabia Kareem, Cristina Benetti-Pinto, Olisaemeka Nnaedozie Okonkwo, Bethel Chinonso Okemeziem, Bethel Nnaemeka Uwakwe, Goodnews Ozioma Igboabuchi, Ifeoma Francisca Ndubuisi, Rukshini Puvanendram, Manisha Mathur, Rajeswari Kathirvel, Farah Safdar, Raksha Aiyappan, Rukshini Puvanendram, Manisha Mathur, Rajeswari Kathirvel, Farah Safdar, Raksha Aiyappan
Conflicts of Interest
All authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
References
- United Nations sexual and reproductive health agency. Nigeria Population 2025 - United Nations Population Fund, (. https://www.unfpa.org/data/world-population/NG.
- World Bank Group. Population, female - Nigeria, (2024). https://data.worldbank.org/indicator/SP.POP.TOTL.FE.IN?locations=NG.
- StatisticsTimes.com. Demographics of Nigeria, (2024). https://m.statisticstimes.com/demographics/country/nigeria-demographics.php?
- Jaff, N. G. & Crowther, N. J. The association of reproductive aging with cognitive function in Sub-Saharan African women. Physical Exercise and Natural and Synthetic Products in Health and Disease, 71-91 (2021).
- Chikwati, R. P. et al. The association of menopause with cardiometabolic disease risk factors in women living with and without HIV in sub-Saharan Africa: Results from the AWI-Gen 1 study. Maturitas 187, 108069 (2024).
- Ameh, N., Madugu, N., Onwusulu, D., Eleje, G. & Oyefabi, A. Prevalence and predictors of menopausal symptoms among postmenopausal Ibo and Hausa women in Nigeria. Tropical Journal of Obstetrics and Gynaecology 33, 263 (2016).
- Okolo, A. & Aniuga, C. Awareness And Responsiveness to Health Challenges Peculiar to Women: A Global Perceptive. Managamanet, 2015; 244. [Google Scholar]
- Ikeanyi, E. M. & Ikobho, E. H. Age at menopause and the correlates of natural menopause among urban and rural women in the Southern Nigeria. Int J Reprod Contracept Obstet Gynecol, 2021; 10, 1266. [Google Scholar]
- Delanerolle, G.; et al. Menopause: a global health and wellbeing issue that needs urgent attention. The Lancet Global Health, 2025; 13, e196–e198. [Google Scholar]
- OYIBOCHA, E. O. Experiences of Midlife Women and Related Co-Morbidity Issues During Menopausal Transition in Delta State, Nigeria. 2020. [CrossRef]
- Ugwu, U. C. & Ene, O. C. Association between osteoporosis and severe depressive symptoms among postmenopausal women attending tertiary outpatient clinics in Nigeria: a cross-sectional study. BMC Women’s Health, 2025; 25, 400. [Google Scholar]
- Imaralu, J. A Five-Year Review of Laparoscopic Gynaecological Surgeries in a Private-Owned Teaching Hospital, in Nigeria: West Afr J Med. 2022 Feb 28; 39 (2): 111-118. West Africa Journal of Medicine, 2022; 39, 111–118. [Google Scholar]
- Ukah, C. , Okhionkpamwonyi, O., Okoacha, I. & Okonta, P. A 5-year review of hysterectomy at the Delta State University Teaching Hospital, Oghara, southsouth Nigeria. Ibom Medical Journal, 2023; 16, 268–272. [Google Scholar]
- Thisday Newspapers LTD. 2019.
- Angaye, U. S. & Sibiri, E. A. Between stigma and support: how socio-cultural norms shape health decisions among perimenopausal women in bayelsa central, Nigeria. African journal for the psychological studies of social issues, 2025; 28. [Google Scholar]
- Omidoyin, F. Factors Affecting Level of Preparedness For Menopause Among Pre-Menopausal Women in Leo Community, Ido Local Government Area, Oyo State, Nigeria, (2014).
- Ibeachu, C. P. & Uahomo, P. O. Quality of Life in Menopausal Women: Effects of Sociodemographic Factors and Symptoms. South Asian Res J Med Sci, 2024; 6, 178–188. [Google Scholar]
- Balogun, J. A. in The Nigerian healthcare system: pathway to universal and high-quality health care 117-152 (Springer, 2022).
- Islam, R. M.; et al. Menopause in low and middle-income countries: a scoping review of knowledge, symptoms and management. Climacteric, 2025; 1–38. [Google Scholar]
- Abah, V. O. in Healthcare Access-New Threats, New Approaches (IntechOpen, 2022).
- Uno, O. E.-O. , Biya, C., Okoye, N. J.-F., Okoye, C. P. & Ozigbo, A. A. A Review on Sociocultural Barriers Affecting Healthcare Access Among Older Adults in Nigeria. Journal of Pharma Insights and Research, 2025; 3, 032–039. [Google Scholar]
- ESCAP, U. & World Health Organization. SDG 3: Good health and well-being. (2021).

Table 1.
Application of Delanerolle and Phiri framework.
| Stage | Description | Application in MARIE WP2a (Nigeria) |
|---|---|---|
| 1. Contextual familiarisation | Immersion in transcripts to understand cultural, social, and structural contexts influencing participant narratives. | Researchers reviewed each transcript multiple times, alongside field notes, to identify Nigeria-specific contextual factors such as gender role expectations, cultural beliefs about menopause, and urban–rural healthcare disparities. |
| 2. Equity-oriented coding | Generating initial codes that capture both descriptive phenomena and equity-linked determinants (e.g., gender norms, healthcare access, socioeconomic position). | Codes were developed to reflect participants’ accounts of barriers to care, affordability of treatment, social stigma, workplace exclusion, and intersectional disadvantages linked to age, marital status, and economic position. |
| 3. Framework mapping | Organising codes into domains reflecting individual, community, health system, and policy levels, while retaining cross-cutting themes such as stigma, intersectionality, and structural inequality. | Coded data were categorised into four framework domains (individual, community, health system, policy) with cross-cutting Nigerian-specific themes, including religious influences on treatment choice, reliance on informal care networks, and systemic underfunding of women’s health. |
| 4. Integrative interpretation | Synthesising findings to highlight the interplay between lived experiences and systemic factors, situating these within national sociocultural and healthcare contexts. | Themes were integrated to explain how menopause experiences in Nigeria are shaped by sociocultural beliefs, structural health inequities, and policy gaps, highlighting implications for equitable service delivery. |
Table 2.
The codes, sub-codes and operational definitions used as part of the data analysis.
| Code | Sub-code | Operational definition | Example indicator |
|---|---|---|---|
| Vasomotor symptoms | Visible hot flushes at work | Socially noticeable sweating/heat episodes affecting work or interactions. | Facial sweating causing embarrassment at work |
| Mild internal heat, self-managed | Hot flushes/internal heat present but manageable without treatment. | Internal heat managed independently; no escalation | |
| Heat-triggered sleep fragmentation | Sleep disrupted by heat/humidity; improved by environmental cooling. | Night waking in hot weather; uses rechargeable fan | |
| Musculoskeletal pain | Continuous/limiting low-back pain | Ongoing/recurrent LBP restricting activities; medication use reported. | Continuous, activity-limiting LBP; analgesics required |
| Activity-linked low-back pain (LBP) | Intermittent LBP after prolonged shifts/manual tasks; settles with rest. | LBP after long nursing shifts | |
| Pelvic pain (intermittent) | Pelvic/waist pain that comes and goes; often untreated. | Episodic pelvic pain without therapy | |
| Functional selection due to pain | Task modification/avoidance at work because of pain. | Selects lighter duties during flares | |
| Urogenital symptoms | Stress/urgency incontinence | Leakage if toilet access delayed or with urgency; sometimes medicated. | Needs rapid toilet access; prior continence medication |
| No GU symptoms | Explicit denial of urinary incontinence/pelvic pain. | No GU complaints recorded | |
| Sleep | Stable, protective routine | Consistent sleep/wake pattern; refreshing sleep without aids. | Early regular bedtimes; restorative sleep |
| Insomnia with functional impact | Poor sleep (initiation/maintenance/early waking) reducing daytime performance. | Low sleep rating; daytime fatigue/productivity loss | |
| Ad-hoc hypnotic use / no routine | Intermittent sedative use and/or lack of structured sleep routine. | Occasional sleep tablets; no set routine | |
| Psychological symptoms | Mood lability/irritability | Fluctuating mood, irritability or aggression linked to menopause. | Irritability affecting work interactions |
| Low mood/anxiety | Persistent sadness, worry or anxiety during menopause. | Anxiety/mood swings during flares | |
| Cognitive difficulty | Concentration/forgetfulness impairing task performance. | Uses notes/reminders to compensate | |
| Preference for solitude | Desire to withdraw/isolate as coping. | Seeks quiet space; works alone when overwhelmed | |
| Suicidality risk | Hopelessness | Expressed hopelessness related to menopausal burden. | Affirmed hopelessness on direct probe |
| Thoughts life not worth living | Acknowledged thoughts that life is not worth living. | Affirmed SI probe during interview | |
| Work impact & adaptation | Work stress ↑ from baseline | Self-rated stress higher post-menopause vs pre-. | Stress 8–9/10 vs 4–6/10 pre- |
| Shift/night-duty intolerance | Night shifts/long hours newly difficult due to symptoms. | Reduced tolerance for nights/physically heavy tasks | |
| Pacing/micro-breaks/quiet space | Uses breaks, steady pacing, or quiet areas to cope. | Short breaks and quiet room improve functioning | |
| Role redesign/supervisory buffer | Shift to supervisory/mentoring duties reduces strain. | Supervisory role with low physical load; volunteer role buffering stress | |
| Workplace supports | Supportive managers, no policy | Informal accommodation without formal menopause policy. | Supervisor understanding but no written policy |
| Desired adjustments | Concrete requests for cooling, toilet access, flexible breaks. | Fans/cool spaces; ready toilet access; flexible rest periods | |
| Care-seeking & literacy | Anticipatory education absent | Reports no prior menopause education from health services. | No clinician-led information before onset |
| Informal knowledge sources | Learnt via family, friends, colleagues or books. | Maternal advice | |
| Reactive care / screening-only | Care sought at symptom peak; screening done without management plan. | Pap smear offered; no menopause plan | |
| Treatment stance & preferences | HRT hesitancy/avoidance | Avoids HRT due to risk beliefs or preference for “natural” care. | Fear of oestrogen risks; spiritual/natural framing |
| HRT used → benefit | Reports HRT with perceived symptom improvement. | On HRT with improvement noted | |
| Supplement reliance | Use of oils/minerals (eg, evening primrose, starflower, calcium). | Evening primrose perceived helpful | |
| Non-pharmacological pacing/rest | Symptom management through rest, pacing, trigger reduction. | Rest periods resolve flares; ceased early morning commitments | |
| Structural & economic barriers | Doctor shortages/quality concerns | Perceived lack of clinicians or poor-quality/generic advice. | Reports of “no doctors” or poor quality care |
| High costs/transport burden | Financial barriers and transport costs limiting access. | Transport costs and hospital bills cited as barriers | |
| Long waits/limited PC support | Long waits; primary care supportive but not menopause-literate. | Limited HRT discussion; generic support only | |
| Social support | Peer confiding | Reliance on friends/peers for emotional support. | Confides in close friend to cope |
| Family labelling symptoms | Family members help name/normalise menopausal symptoms. | Mother identified hot flushes for participant | |
| Comorbidities & parity | Hypertension/diabetes context | NCDs co-exist and influence options/risks. | Comorbidities |
| High parity | ≥3 vaginal births with midlife pelvic-floor implications. | Births | |
| Caesarean for multiples | C/S after multiple gestation. | Triplet pregnancy leading to caesarean | |
| Protective wellbeing | Positive affect/resilience | Stable positive mood and high wellbeing despite menopause. | Consistently happy/energised; no symptoms |
| Meaningful roles & autonomy | Purposeful activity and autonomy buffer distress. | Volunteering; independent driving; supervisory work |
Table 3.
Characteristics of the Participants.
| Participant ID | REGION | AGE (Years) | Menopause stage | Socioeconomic status | Educational Level | Ethnicity | Comorbidies |
|---|---|---|---|---|---|---|---|
| 1 | Awka | 66 | Post-menopause (Natural) | Q3 | Primary | Igbo | No |
| 2 | Nnewi | 61 | Post-menopause (Natural) | Q3 | Secondary | Igbo | No |
| 3 | Enugu | 57 | Post-menopause (Natural) | Q2 | secondary | Igbo | GERD |
| 4 | Lagos | 57 | Post-menopause (Natural) | Q1 | Tertiary | Yoruba | No |
| 5 | Ozubulu | 55 | Post-menopause (Natural) | Q2 | Secondary | Igbo | No |
| 6 | Nnewi | 61 | Post-menopause (Natural) | Q3 | Primary | Igbo | No |
| 7 | Enugu | 59 | Post-menopause (Natural) | Q2 | Secondary | igbo | No |
| 8 | Kano | 58 | Post-menopause (Natural) | Q2 | Secondary | Hausa | Hypertension |
| 9 | Kano | 55 | Post-menopause (Natural) | Q3 | Tertiary | Hausa | No |
| 10 | Oraifite | 65 | Post-menopause (Natural) | Q1 | Tertiary | Igbo | No |
| 11 | Ihiala | 60 | Post-menopause (Natural) | Q1 | Tertiary | Igbo | Hypertension & Diabetes Mellitus |
| 12 | Nnobi | 59 | Post-menopause (Natural) | Q3 | Secondary | Igbo | No |
| 13 | Nnewi | 62 | Post-menopause (Natural) | Q1 | Tertiary | Igbo | No |
| 14 | Nsukka | 58 | Post-menopause (Natural) | Q2 | Secondary | Igbo | No |
| 15 | Ibadan | 64 | Post-menopause (Natural) | Q2 | Tertiary | Yoruba | No |
| 16 | Jalingo | 63 | Post-menopause (Natural) | Q2 | Secondary | Hausa | No |
| 17 | Akure | 61 | Post-menopause (Natural) | Q3 | Secondary | Yoruba | Hypertension and Diabetes mellitus |
| 18 | Lagos | 57 | Post-menopause (Natural) | Q3 | Secondary | Yoruba | No |
| 19 | Lagos | 58 | Post-menopause (Natural) | Q2 | Secondary | Yoruba | No |
| 20 | Lagos | 66 | Post-menopause (Surgical) | Q1 | Tertiary | Yoruba | No |
| 21 | Ojiriver | 65 | Post-menopause (Natural) | Q2 | Secondary | Igbo | No |
Table 4.
Evidence-based recommendations.
| Recommendation | Rationale | Priority Actions |
|---|---|---|
| Integrate menopause care into primary healthcare services | Reduces diagnostic delays, ensures continuity of care | Include menopause screening in routine check-ups; train PHC workers |
| Develop Nigerian-specific clinical guidelines for menopause | Provides standardised care pathways | Collaborate with NMA, FMOH, and women’s health experts |
| Expand access to affordable HRT | Addresses cost and availability barriers | Add HRT to National Essential Medicines List; explore subsidy schemes |
| Implement national menopause awareness campaigns | Reduces stigma, increases health-seeking | Use radio, TV, social media, and community outreach |
| Incorporate menopause education into health professional curricula | Improves provider competence | Revise medical, nursing, and pharmacy curricula |
| Foster community-based support programmes | Builds peer networks and trust | Leverage women’s groups, NGOs, and faith-based organisations |
| Establish menopause research funding streams | Fills data gaps, guides policy | Advocate to national and international funders; link to SDGs |
| Increase African-led menopause research collaborations | Strengthens contextual evidence | Create regional research consortia and mentorship networks |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



