Submitted:
06 October 2025
Posted:
06 October 2025
You are already at the latest version
Abstract
Background: Agitated adult trauma patients are common in Canadian emergency departments (EDs). Cooperation and monitoring constraints can delay essential imaging and risk missed injury. Objective: To synthesize current guidance and evidence into an educational framework for timely, safe imaging when the trauma exam is unreliable due to agitation. Methods: Narrative review using targeted searches of guideline/agency sources and peer‑reviewed trials/meta‑analyses on agitation control, eFAST, and selective versus whole‑body CT. Outputs were a conceptual evidence map and a worked case. Results: Current research prioritizes parallel resuscitation with early eFAST. Unstable, eFAST‑positive patients usually proceed to hemorrhage control rather than CT. For stable or stabilized adults with an unreliable exam, brief, monitored behavioral control (single, guideline‑supported regimen) creates a one‑trip imaging window under continuous SpO₂/NIBP/ECG (± capnography). Teams select an up‑front imaging approach: selective CT once cooperation returns and injuries localize (using CCHR/CCR where applicable), or whole‑body CT when multi‑region injury is likely or unreliability persists. The scanner‑side bundle includes named monitoring responsibility, an airway plan, and dose‑optimized protocols. Downstream steps include IR‑supported non‑operative strategies for eligible solid‑organ injury, a 24–48‑hour tertiary trauma survey, and a structured psychiatry handoff to limit re‑sedation. Conclusions: In agitated adult trauma, a single, monitored trip to obtain the necessary imaging after brief, guideline‑aligned behavioral control may improve safety and throughput. This educational synthesis requires local policy alignment and prospective evaluation.
Keywords:
emergency medicine
; trauma
; agitation
; emergency imaging
Introduction
Emergency departments (EDs) across Canada continue to operate under sustained crowding and access blocks. In 2024-2025, participating sites reported >16.1 million unscheduled ED visits; among patients admitted to hospital, 90% completed their ED stay within 48.5 hours (versus 8.0 hours for those discharged). These system pressures frame every time-critical decision in trauma care (CIHI, 2025a; CIHI, 2025b).
Within this environment, agitated adult trauma patients, including those with psychiatric comorbidity and/or intoxication, pose a distinct challenge: imaging is often essential, yet cooperation, safety, and monitoring constraints can delay or derail it. Contemporary Canadian evidence includes a randomized trial showing that intramuscular ketamine achieved faster sedation than haloperidol-midazolam in severe agitation. Practical resources (e.g., Emergency Care BC) emphasize parallel resuscitation, early monitoring, and clear thresholds for medication-assisted control. At the same time, national indicators highlight the disproportionate ED burden of mental health and substance-use presentations, underscoring the need for reproducible, efficient approaches for this population. (Barbic & Andolfatto, 2021; Stone et al., 2023; CIHI, 2025c)
Imaging remains central when examination is unreliable. Point-of-care ultrasound rapidly rules in hemoperitoneum, pericardial effusion, and pneumothorax (PTX), but a negative scan does not reliably exclude injury. When cooperation permits, Canadian decision rules (the Canadian CT Head Rule and the Canadian C-Spine Rule), provide validated frameworks to target imaging. When they cannot be applied (e.g., persistent agitation), clinicians often adopt a lower threshold for CT; the ACR Appropriateness Criteria support early CT when clinical assessment is limited (Netherton et al., 2019; Stiell et al., 2001a; Stiell et al., 2001b; Shyu et al., 2020).
This narrative review synthesizes existing guidance into a conceptual evidence map (logic model) and a worked case for agitated adult trauma in Canadian EDs, spanning initial stabilization and eFAST, an up-front selective CT versus whole-body CT decision, scanner-side safety, and post-imaging handoffs. It is an educational synthesis, not a clinical practice guideline. Clinicians should follow institutional policies, provincial regulations, and current specialty guidance.
Methods
This is a narrative, practice-oriented review. We followed SANRA guidance for narrative reviews and borrowed relevant reporting items from PRISMA-S to describe searches. Information sources included PubMed, open-access publisher sites, and authoritative guideline/agency sites (ACR Appropriateness Criteria; ACR-SIR sedation parameter; ACEP 2024 agitation policy; CIHI; Emergency Care BC; CADTH).
Search strategy: iterative queries (Jan 2010-Sept 20, 2025; English) plus domain-restricted searches (e.g., acsearch.acr.org, cihi.ca, emergencycarebc.ca) and landmark Canadian rules (CCHR, CCR). We complemented this with reference-list chaining and grey-literature sweeps (CADTH Grey Matters; PRESS 2015 as framework for peer-checking search strings).
Eligibility: adult (≥16 y) ED trauma literature relevant to (1) agitation control enabling imaging, (2) imaging strategy in unreliable exams (eFAST; selective CT vs WBCT), (3) scanner-side sedation/monitoring and post-imaging handoff. Data extraction: One author performed selection and data extraction; other authors reviewed extracted tables/figures and resolved discrepancies by consensus.
Synthesis: qualitative, thematic review to assemble (i) a conceptual evidence map (logic model) and (ii) a worked case demonstrating application to an agitated adult trauma scenario. No clinical tools were validated; materials are presented for scholarly synthesis and local adaptation only.
Limitations: not systematic; study counts and formal risk-of-bias were not performed; selection bias is possible; we anchored statements to guideline-level sources and peer-reviewed trials/meta-analyses. (Baethge et al., 2019; Rethlefsen et al., 2021; CADTH, 2016; McGowan et al., 2016)
Results
Triage & eFAST-First in the Unreliable Exam
Why eFAST early: With agitated patients or otherwise unreliable trauma exams, bedside extended FAST (eFAST) gives rapid, actionable answers while resuscitation continues. eFAST is well supported for ruling-in hemoperitoneum, pericardial effusion, and PTX; however, a negative eFAST does not safely rule out injury, so it should be followed by selective CT when clinical suspicion persists. (Netherton et al., 2019) CAEP positions PoCUS, including eFAST, as core ED practice in Canada. (Lewis et al., 2019)
Thoracic adjuncts: In supine trauma patients, portable CXR is relatively insensitive for PTX; thoracic ultrasound detects PTX more accurately and is often preferred at the bedside where operator expertise and equipment are available. (Alrajab et al., 2013; Ebrahimi et al., 2014)
From eFAST to the next step:
- Unstable patients with positive eFAST or high suspicion of injury: Hemorrhage control is typically prioritized (e.g., straight to OR) over CT. In this context, eFAST has largely supplanted diagnostic peritoneal lavage (DPL) for rapid intra-abdominal bleeding assessment (American College of Surgeons, 2021).
- Stable or stabilized patients but eFAST exam unreliable: the ACR Appropriateness Criteria for Major Blunt Trauma endorses early CT in polytrauma or when clinical assessment is limited. (American College of Radiology, 2025)
Pelvic considerations: If pelvic injury is suspected, particularly among hemodynamically or mechanically unstable patients, centers commonly apply a pelvic binder and obtain an early pelvic radiograph before transfer to CT. A confirmed fracture may warrant early readiness planning (e.g., personnel and blood products) per local trauma protocols. International guidance similarly recommends early pelvic X-ray and eFAST in unstable pelvic trauma. (Coccolini et al., 2017a; Bradley et al., 2021).
Agitation Control to Enable Imaging
Objective. Create a brief, safe window to obtain the necessary imaging (eFAST, then selective CT or WBCT) without unnecessary repeat sedations or loss of monitoring/airway control. This section summarizes adult ED practice principles. (Roppolo et al., 2020; American College of Emergency Physicians, 2024)
Non-pharmacologic: Recommended as the first line in the literature. Among these recommendations are the use of verbal de-escalation and environmental controls, early correction of fixable contributors (hypoxia, pain, hypoglycemia, withdrawal), and continuous monitoring before giving medications (Stone et al., 2023).
Pharmacologic strategies (select a single, guideline-supported regimen initially, reassess frequently, and avoid stacking sedatives unless clinically indicated):
- A.
- Rapid single-agent dissociation with ketamine. Evidence from a Canadian RCT supports faster onset versus haloperidol-midazolam in severe agitation (Barbic & Andolfatto, 2021).
- B.
- Antipsychotic + benzodiazepine combination (e.g., droperidol + midazolam) as a guideline supported option when dissociation is not chosen or is contraindicated (American College of Emergency Physicians, 2024).
- C.
- Alternatives include haloperidol ± lorazepam, or IM olanzapine. Avoid co-administration with parenteral benzodiazepines per the product monograph (Eli Lilly Canada, 2020). Agent selection should align with local formulary and policy.
Monitoring & safety: Continuous SpO2/NIBP/ECG (with capnography when moderate sedation is anticipated) and assignment of qualified personnel responsible for continuous monitoring during transport and scanning, in accordance with ASA/ACR/CAS standards and local policy. If used, physical restraints should follow institutional policy and law and be limited to the briefest interval necessary, with frequent reassessment and documentation.
Reassessment and timing to CT. Guidelines suggest reassessing sedation depth and cardiorespiratory status at short intervals. Once a safe, cooperative window is achieved, imaging in a single trip under active monitoring is recommended by ACR. If the window is inadequate or deteriorates, guidelines recommend pausing and addressing airway/ventilation, analgesia, or contributing physiology rather than reflexively stacking sedatives (American College of Radiology, 2025; American Society of Anesthesiologists Task Force…, 2018; Canadian Anesthesiologists’ Society, 2025)
Imaging Decision Node: Selective CT vs Whole-Body CT (WBCT)
Purpose: In agitated adult trauma with an unreliable eFAST exam, the aim is to obtain a complete diagnostic dataset in one safe, monitored trip. The up-front choice between selective CT and WBCT depends on mechanism/physiology, how reliable the exam is after behavioral control, and early signals from eFAST/portable films. This section summarizes how teams commonly approach that decision for local adaptation. (American College of Radiology, 2025)
Scenarios where WBCT is considered:
- Persistently unreliable or unobtainable eFAST exam despite initial sedation.
- High-energy injury mechanism or suspicion for multi-region injury (e.g., head/neck + chest/abdomen/pelvis).
- Positive eFAST with uncertainty about other compartments.
In these settings, WBCT is often associated with shorter time to completion of imaging and overall ED work-up, while randomized and observational data suggest no clear mortality advantage over selective strategies (Sierink et al., 2016; Arruzza et al., 2020; Fathi et al., 2024).
Scenarios where selective CT is considered:
- After agitation control, the patient regains cooperation and injuries localize clinically.
- Decision rules can be applied (e.g., CCHR, CCR) to focus imaging.
When rules cannot be applied (e.g., exam remains unreliable), clinicians often adopt a lower threshold for CT, consistent with ACR Appropriateness Criteria supporting early CT when clinical assessment is limited (Stiell et al., 2001a; Stiell et al., 2001b; Stiell et al., 2003).
Protocol. A common WBCT sequence is non-contrast head and cervical spine, followed by contrast-enhanced chest/abdomen/pelvis in a single trip; exact sequencing and contrast strategy should follow institutional protocols. Use of CTA head/neck when blunt cerebrovascular injury risk is present; thoracic/lumbar CT for high-risk or unexaminable patients; MRI selectively for ligamentous/cord concerns is noted in the literature (Kim et al., 2020).
Dose optimization should inform protocol selection (e.g., iterative reconstruction, split-bolus single-pass techniques, local low-dose WBCT protocols), balanced against diagnostic yield and scanner capability (American College of Radiology, 2025).
Downstream Surgical Implications
Pacing of decisions. The initial imaging strategy sets the tempo for operative versus non-operative management. WBCT is often associated with shorter time to completion of imaging and overall ED work-up, facilitating earlier definitive decisions; mortality appears neutral versus selective strategies in randomized and observational data (Sierink et al., 2016; Arruzza et al., 2020; Jiang et al., 2014).
Solid-organ injury triage: On contrast-enhanced CT, findings such as arterial contrast extravasation (“blush”) or expanding hematoma may prompt consideration of early angioembolization within guideline-supported non-operative strategies for spleen and liver, when hemodynamics permit (Gilyard et al., 2020).
Missed-injury minimization: Many centers perform a Tertiary Trauma Survey (TTS) at 24–48 hours to detect occult injuries after the initial ED phase. In obtunded or persistently unreliable adults, revisit cervical-spine clearance after negative high-quality CT per institutional policy (Keijzers et al., 2012; Patel et al., 2015; Holmstrom et al., 2021)
Psychiatric Handoff & Disposition
Purpose: After imaging and time-critical surgical decisions, a structured, safety-first handoff to psychiatry is often used to reduce re-agitation, avoid sedation stacking, and set clear observation/boarding plans grounded in trauma- and violence-informed care (TVIC). Local policy governs sedation, restraints, and transfer thresholds (Public Health Agency of Canada, 2025; Xie et al., 2022).
Guiding principles: The literature emphasizes TVIS, advises for a single “sedation plan owner” and asks the reader to avoid co-administration of IM olanzapine with parenteral benzodiazepines per product monographs. (Eli Lilly Canada, 2020)
Structured handoff (I-PASS): Many services adapt I-PASS to this transition: Illness severity, Patient summary (mechanism, injuries, eFAST/CT results), Action list (monitoring, analgesia, de-escalation steps), Situation awareness/contingencies (re-agitation plan, airway triggers, sitter/security), and Synthesis by receiver to confirm understanding. These elements align with TeamSTEPPS/I-PASS implementation literature and can be tailored to local workflows. (Agency for Healthcare Research and Quality, 2017; Franco Vega et al., 2024; Heilman et al., 2016)
Violence-risk & observation planning: When permitted by institutional policy, brief validated tools (e.g., Brøset Violence Checklist) may inform observation planning. “Boarding bundles” (quiet room, consistent staff, scheduled PO meds, limiting stimuli) function as quality-improvement strategies rather than standards and are adapted locally (Sammut et al., 2023; Lawrence et al., 2024).
Disposition & boarding: Surgical/ICU transfer is prioritized when indicated, with psychiatry follow-up arranged. If medically ready for psychiatric care, confirm vital sign stability, symptom control, and an agreed medication/monitoring plan that minimizes repeat sedation during boarding. Align disposition steps with institutional policy and provincial regulations. (Varner, 2023).
Discussion
Worked Case: Applying the Conceptual Evidence Map
Presentation: A 35-year-old man, unrestrained driver in a high-speed MVC, arrives combative and incoherent (HR 128, BP 102/68, RR 28, SpO2 95% on NRB). Primary survey proceeds with eFAST, which shows right-upper-quadrant free fluid; chest windows are limited by motion. He is too agitated for a reliable neurologic or C-spine exam.
Initial stabilization and eFAST: Resuscitation continues in parallel with eFAST to rapidly identify life-threatening injury, recognizing that a negative eFAST would not exclude injury in this unreliable exam.
Behavioral control to enable imaging: De-escalation and environmental controls are attempted without effect. The team then uses a single, guideline-supported rapid-onset regimen under continuous monitoring to create a short imaging window, avoiding stacking sedatives unless clinically indicated.
Up-front imaging approach: Given the high-energy mechanism and persistently unreliable exam after sedation, the team elects whole-body CT (WBCT), head/C-spine non-contrast followed by contrast-enhanced chest/abdomen/pelvis, as a one-trip strategy to obtain a complete diagnostic data set. In other scenarios where the exam localizes after agitation control, a selective CT approach is often considered.
Scanner-side safety: Transfer to CT occurs with qualified personnel assigned to continuous monitoring, audible alarms on, and a pre-scan pause confirming the airway plan and contrast protocol, aligned with ASA/ACR/CAS standards and local policy.
Findings and downstream actions: CT shows a splenic laceration and rib fractures. Trauma surgery proceeds to the OR. A 24–48-hour tertiary trauma survey and structured handoff planning are arranged to minimize missed injuries and re-agitation during any subsequent boarding.
Alternative reasonable path: At some centers, an initial selective CT approach may be chosen when the exam becomes reliable after sedation or based on local protocol and scanner availability; both strategies are guideline-supported when applied to the appropriate patient profile.
Conclusion
Canadian EDs face ongoing crowding and access-block. In agitated adult trauma, reliable imaging is both a safety and throughput issue. This review synthesizes existing guidance into a conceptual evidence map (logic model) and a worked case for local adaptation.
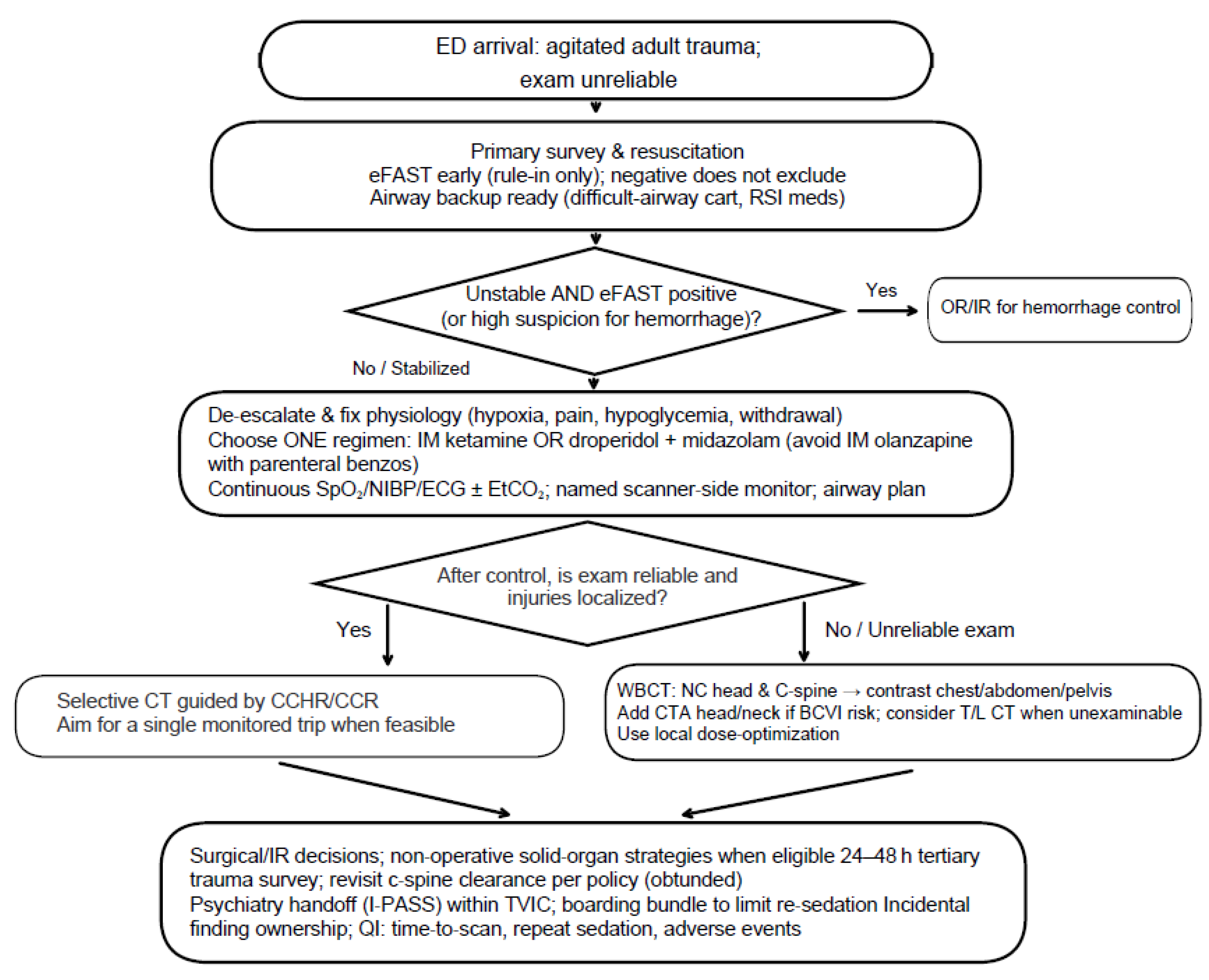
The map emphasizes: early stabilization with eFAST; monitored sedation to create a brief imaging window when agitation impedes assessment; a single, up-front imaging approach; selective CT when the exam is reliable, or WBCT when unreliability persists; and scanner-side safety with qualified personnel assigned to continuous monitoring, aligned with ASA/ACR/CAS standards and institutional policy. Structured surgical and psychiatric handoffs, radiation-dose optimization, a 24–48-hour tertiary trauma survey, and explicit follow-up for incidental findings help close the loop. Figure 1 depicts the model; the worked case illustrates one pathway through it.
Elements within this framework may be associated with shorter time to imaging or fewer repeat sedations in component studies and guideline statements; the composite framework has not been prospectively evaluated. Institutions should adapt the map through local governance and evaluate effects via quality-improvement metrics (e.g., time to scan, repeat sedation, adverse events). This educational synthesis is not a clinical practice guideline; clinicians should follow current specialty guidance and local policy.
Author Contributions
E.L. drafted the Emergency Medicine sections and performed the associated literature review. A.A. drafted the Radiology sections and prepared the imaging-related content. N.M. drafted the Psychiatry sections and reviewed the mental-health literature. F.W. drafted the General Surgery sections and contributed to the interpretation of the literature. All authors contributed to revising the manuscript for important intellectual content, approved the final version, and accepted responsibility for the work.
Funding Statement: No author has received financial support, personal fees, or other benefits from commercial entities that could be perceived to influence the submitted work.
Data Availability: No datasets were generated or analyzed during the current study.
Acknowledgements
None.
Declaration of Author’s Competing Interests: The authors declare that they have no competing interests.
References
- Agency for Healthcare Research and Quality. (2017). Tool: I-pass | agency for Healthcare Research and Quality. https://www.ahrq.gov/teamstepps-program/curriculum/communication/tools/ipass.html.
- Alrajab, S., Youssef, A. M., Akkus, N. I., & Caldito, G. (2013). Pleural ultrasonography versus chest radiography for the diagnosis of pneumothorax: Review of the literature and meta-analysis. Critical Care, 17(5). [CrossRef]
- American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Severe Agitation. (2024). Clinical policy: Critical issues in the evaluation and management of adult out-of-hospital or emergency department patients presenting with severe agitation. Annals of Emergency Medicine, 83(1), e1–e30. [CrossRef]
- American College of Radiology, Society of Interventional Radiology, & Society for Pediatric Radiology. (2025). Practice parameter for minimal and/or moderate sedation/analgesia in radiology. https://gravitas.acr.org/PPTS/DownloadPreviewDocument?DocId=95.
- American College of Surgeons. (2021). Trauma Quality Improvement Program (TQIP) best practices in imaging for trauma patients. https://www.facs.org/media/oxdjw5zj/imaging_guidelines.pdf.
- American Society of Anesthesiologists Task Force on Moderate Procedural Sedation and Analgesia; American Association of Oral and Maxillofacial Surgeons; American College of Radiology; American Dental Association; American Society of Dentist Anesthesiologists; & Society of Interventional Radiology. (2018). Practice guidelines for moderate procedural sedation and analgesia 2018. Anesthesiology, 128(3), 437–479. [CrossRef]
- Arruzza, E., Chau, M., & Dizon, J. (2020). Systematic Review and meta-analysis of whole-body computed tomography compared to conventional radiological procedures of trauma patients. European Journal of Radiology, 129, 109099. [CrossRef]
- Baethge, C., Goldbeck-Wood, S., & Mertens, S. (2019). Sanra—a scale for the quality assessment of narrative review articles. Research Integrity and Peer Review, 4(1). [CrossRef]
- Barbic, D., Andolfatto, G., Grunau, B., Scheuermeyer, F. X., Macewan, B., Qian, H., Wong, H., Barbic, S. P., & Honer, W. G. (2021). Rapid agitation control with ketamine in the emergency department: A blinded, randomized controlled trial. Annals of Emergency Medicine, 78(6), 788–795. [CrossRef]
- Bradley, N. L., Kim, M. J., & Menon, M. R. (2021). Binder use and early pelvic radiographs in the management of unstable patients with blunt trauma. Canadian Medical Association Journal, 193(18). [CrossRef]
- CADTH. (2016). Grey Matters: A practical tool for searching health-related grey literature. https://www.cadth.ca/grey-matters.
- Canadian Institute for Health Information. (2025a). Emergency department crowding: Beyond Primary Care Access. CIHI. https://www.cihi.ca/en/primary-and-virtual-care-access-emergency-department-visits-for-primary-care-conditions/emergency-department-crowding-beyond-primary-care-access.
- Canadian Institute for Health Information. (2025b). NACRS emergency department visits and lengths of stay. CIHI. https://www.cihi.ca/en/nacrs-emergency-department-visits-and-lengths-of-stay.
- Canadian Institute for Health Information. (2025c). Frequent emergency room visits for help with mental health and substance use. CIHI. https://www.cihi.ca/en/indicators/frequent-emergency-room-visits-for-help-with-mental-health-and-substance-use.
- Canadian Institute for Health Information. (2025d). List of updated indicators and contextual measures, July 2025. CIHI. https://www.cihi.ca/en/list-of-updated-indicators-and-contextual-measures-july-2025.
- Coccolini, F., Stahel, P. F., Montori, G., Biffl, W., Horer, T. M., Catena, F., Kluger, Y., Moore, E. E., Peitzman, A. B., Ivatury, R., Coimbra, R., Fraga, G. P., Pereira, B., Rizoli, S., Kirkpatrick, A., Leppaniemi, A., Manfredi, R., Magnone, S., Chiara, O., … Ansaloni, L. (2017a). Pelvic trauma: WSES classification and Guidelines. World Journal of Emergency Surgery, 12(1). [CrossRef]
- Coccolini, F., Montori, G., Catena, F., Kluger, Y., Biffl, W., Moore, E. E., Reva, V., Bing, C., Bala, M., Fugazzola, P., Bahouth, H., Marzi, I., Velmahos, G., Ivatury, R., Soreide, K., Horer, T., ten Broek, R., Pereira, B. M., Fraga, G. P., … Ansaloni, L. (2017b). Splenic Trauma: WSES classification and guidelines for adult and pediatric patients. World Journal of Emergency Surgery, 12(1). [CrossRef]
- Coccolini, F., Coimbra, R., Ordonez, C., Kluger, Y., Vega, F., Moore, E. E., Biffl, W., Peitzman, A., Horer, T., Abu-Zidan, F. M., Sartelli, M., Fraga, G. P., Cicuttin, E., Ansaloni, L., Parra, M. W., Millán, M., DeAngelis, N., Inaba, K., Velmahos, G., … Catena, F. (2020). Liver trauma: WSES 2020 guidelines. World Journal of Emergency Surgery, 15(1). [CrossRef]
- Dobson, G. R., Chau, A., Denomme, J., Frost, S., Fuda, G., Mc Donnell, C., Milkovich, R., Milne, A. D., Sparrow, K., Subramani, Y., & Young, C. (2025). Guidelines to the practice of anesthesia—Revised edition 2025. Canadian Journal of Anesthesia/Journal Canadien d’anesthésie, 72(1), 15–63. [CrossRef]
- Ebrahimi, A., Yousefifard, M., Kazemi, H. M., Rasouli, H. R., & Safari, S. (2014). Diagnostic accuracy of chest ultrasonography versus chest radiography for pneumothorax detection: A meta-analysis. Tanaffos, 13(4), 29–37.
- Eli Lilly Canada. (2020). ZYPREXA intramuscular (olanzapine) product monograph. Toronto, Canada: Eli Lilly Canada. https://pi.lilly.com/ca/zyprexa-ca-pm.pdf.
- Fathi, M., Mirjafari, A., Yaghoobpoor, S., Ghanikolahloo, M., Sadeghi, Z., Bahrami, A., Myers, L., & Gholamrezanezhad, A. (2024). Diagnostic utility of whole-body computed tomography/pan-scan in trauma: A systematic review and meta-analysis study. Emergency Radiology, 31(2), 251–268. [CrossRef]
- Flammia, F., Chiti, G., Trinci, M., Danti, G., Cozzi, D., Grassi, R., Palumbo, P., Bruno, F., Agostini, A., Fusco, R., Granata, V., Giovagnoni, A., & Miele, V. (2022). Optimization of CT protocol in polytrauma patients: an update. European review for medical and pharmacological sciences, 26(7), 2543–2555. [CrossRef]
- Franco Vega, M. C., Ait Aiss, M., George, M., Day, L., Mbadugha, A., Owens, K., Sweeney, C., Chau, S., Escalante, C., & Bodurka, D. C. (2024). Enhancing Implementation of the I-PASS Handoff Tool Using a Provider Handoff Task Force at a Comprehensive Cancer Center. Joint Commission journal on quality and patient safety, 50(8), 560–568. [CrossRef]
- Gilyard, S., Shinn, K., Nezami, N., Findeiss, L. K., Dariushnia, S., Grant, A. A., Hawkins, C. M., Peters, G. L., Majdalany, B. S., Newsome, J., Bercu, Z. L., & Kokabi, N. (2020). Contemporary Management of Hepatic Trauma: What IRs Need to Know. Seminars in interventional radiology, 37(1), 35–43. [CrossRef]
- Green, S. P., Al-Saedy, S., Thomas, E. C., & Glaser, J. (2024). The utility of whole body computed tomography in trauma activations and the impact of incidental findings on Patient Management: A Review. Cureus. [CrossRef]
- Hassankhani, A., Freeman, C. W., Banks, J., Parsons, M. S., Wessell, D. E., Hutchins, T. A., Lenchik, L., Burns, J., Eldaya, R. W., Griffith, B., Hickey, S. M., Khan, M. A., Lawrence, B., Paisley, T. S., Reitman, C., Ropper, A. E., Shah, V. N., Steenburg, S. D., Timpone, V. M., … Policeni, B. (2025). ACR appropriateness criteria® Acute Spinal Trauma: 2024 update. Journal of the American College of Radiology, 22(5). [CrossRef]
- Heilman, J. A., Flanigan, M., Nelson, A., Johnson, T., & Yarris, L. M. (2016). Adapting the I-PASS Handoff Program for Emergency Department Inter-Shift Handoffs. The western journal of emergency medicine, 17(6), 756–761. [CrossRef]
- Holmstrom, A. L., Ott, K. C., Weiss, H. K., Ellis, R. J., Hungness, E. S., Shapiro, M. B., & Yang, A. D. (2021). Improving trauma tertiary survey performance and missed injury identification using an education-based quality improvement initiative. The journal of trauma and acute care surgery, 90(6), 1048–1053. [CrossRef]
- Jiang, L., Ma, Y., Jiang, S., Ye, L., Zheng, Z., Xu, Y., & Zhang, M. (2014). Comparison of whole-body computed tomography vs selective radiological imaging on outcomes in major trauma patients: a meta-analysis. Scandinavian journal of trauma, resuscitation, and emergency medicine, 22, 54. [CrossRef]
- Keijzers, G. B., Giannakopoulos, G. F., Del Mar, C., Bakker, F. C., & Geeraedts, L. M. (2012). The effect of tertiary surveys on missed injuries in trauma: A systematic review. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 20(1). [CrossRef]
- Kim, D. Y., Biffl, W., Bokhari, F., Brakenridge, S., Chao, E., Claridge, J. A., Fraser, D., Jawa, R., Kasotakis, G., Kerwin, A., Khan, U., Kurek, S., Plurad, D., Robinson, B. R. H., Stassen, N., Tesoriero, R., Yorkgitis, B., & Como, J. J. (2020). Evaluation and management of Blunt Cerebrovascular Injury: A practice management guideline from the Eastern Association for the surgery of trauma. Journal of Trauma and Acute Care Surgery, 88(6), 875–887. [CrossRef]
- Lawrence, J., Emory, J., Sousa, S., Thompson, D., Jenkins, K., Bettencourt, A. P., McLaughlin, M. K., & Russell-Babin, K. (2024). Implementing the Brøset Violence Checklist in the ED. The American journal of nursing, 124(7), 52–60. [CrossRef]
- Leung, V., Sastry, A., Woo, T. D., & Jones, H. R. (2015). Implementation of a split-bolus single-pass CT protocol at a UK major trauma centre to reduce excess radiation dose in trauma pan-CT. Clinical Radiology, 70(10), 1110–1115. [CrossRef]
- Lewis, D., Rang, L., Kim, D., Robichaud, L., Kwan, C., Pham, C., Shefrin, A., Ritcey, B., Atkinson, P., Woo, M., Jelic, T., Dallaire, G., Henneberry, R., Turner, J., Andani, R., Demsey, R., & Olszynski, P. (2019). Recommendations for the use of point-of-care ultrasound (pocus) by emergency physicians in Canada. CJEM, 21(6), 721–726. [CrossRef]
- McGowan, J., Sampson, M., Salzwedel, D. M., Cogo, E., Foerster, V., & Lefebvre, C. (2016). Press peer review of Electronic Search Strategies: 2015 guideline statement. Journal of Clinical Epidemiology, 75, 40–46. [CrossRef]
- Netherton, S., Milenkovic, V., Taylor, M., & Davis, P. J. (2019). Diagnostic accuracy of eFAST in the trauma patient: a systematic review and meta-analysis. CJEM, 21(6), 727–738. [CrossRef]
- Patel, M. B., Humble, S. S., Cullinane, D. C., Day, M. A., Jawa, R. S., Devin, C. J., Delozier, M. S., Smith, L. M., Smith, M. A., Capella, J. M., Long, A. M., Cheng, J. S., Leath, T. C., Falck-Ytter, Y., Haut, E. R., & Como, J. J. (2015). Cervical spine collar clearance in the obtunded adult blunt trauma patient. Journal of Trauma and Acute Care Surgery, 78(2), 430–441. [CrossRef]
- Public Health Agency of Canada. (2025). Trauma and violence-informed approaches to policy and practice. Government of Canada. https://www.canada.ca/en/public-health/services/publications/health-risks-safety/trauma-violence-informed-approaches-policy-practice.html.
- Rethlefsen, M. L., Kirtley, S., Waffenschmidt, S., Ayala, A. P., Moher, D., Page, M. J., Koffel, J. B., Blunt, H., Brigham, T., Chang, S., Clark, J., Conway, A., Couban, R., de Kock, S., Farrah, K., Fehrmann, P., Foster, M., Fowler, S. A., Glanville, J., … Young, S. (2021). Prisma-S: An extension to the PRISMA statement for reporting literature searches in systematic reviews. Systematic Reviews, 10(1). [CrossRef]
- Roppolo, L. P., Morris, D. W., Khan, F., Downs, R., Metzger, J., Carder, T., Wong, A. H., & Wilson, M. P. (2020). Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation). Journal of the American College of Emergency Physicians open, 1(5), 898–907. [CrossRef]
- Sammut, D., Hallett, N., Lees-Deutsch, L., & Dickens, G. L. (2023). A Systematic Review of Violence Risk Assessment Tools Currently Used in Emergency Care Settings. Journal of emergency nursing, 49(3), 371–386.e5. [CrossRef]
- Shyu, J. Y., Khurana, B., Soto, J. A., Biffl, W. L., Camacho, M. A., Diercks, D. B., Glanc, P., Kalva, S. P., Khosa, F., Meyer, B. J., Ptak, T., Raja, A. S., Salim, A., West, O. C., & Lockhart, M. E. (2020). ACR appropriateness criteria® major blunt trauma. Journal of the American College of Radiology, 17(5). [CrossRef]
- Sierink, J. C., Treskes, K., Edwards, M. J., Beuker, B. J., den Hartog, D., Hohmann, J., Dijkgraaf, M. G., Luitse, J. S., Beenen, L. F., Hollmann, M. W., Goslings, J. C., & REACT-2 study group (2016). Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial. Lancet (London, England), 388(10045), 673–683. [CrossRef]
- Soares, B. P., Shih, R. Y., Utukuri, P. S., Adamson, M., Austin, M. J., Brown, R. K. J., Burns, J., Cacic, K., Chu, S., Crone, C., Ivanidze, J., Jackson, C. D., Kalnins, A., Potter, C. A., Rosen, S., Soderlund, K. A., Thaker, A. A., Wang, L. L., & Policeni, B. (2024). ACR appropriateness criteria® altered mental status, coma, delirium, and psychosis: 2024 update. Journal of the American College of Radiology, 21(11). [CrossRef]
- Stengel, D., Mutze, S., Güthoff, C., Weigeldt, M., von Kottwitz, K., Runge, D., Razny, F., Lücke, A., Müller, D., Ekkernkamp, A., & Kahl, T. (2020). Association of Low-Dose Whole-Body Computed Tomography with Missed Injury Diagnoses and Radiation Exposure in Patients with Blunt Multiple Trauma. JAMA surgery, 155(3), 224–232. [CrossRef]
- Stiell, I. G., Wells, G. A., Vandemheen, K., Clement, C., Lesiuk, H., Laupacis, A., McKnight, R. D., Verbeek, R., Brison, R., Cass, D., Eisenhauer, M. E., Greenberg, G., & Worthington, J. (2001a). The Canadian CT Head Rule for patients with minor head injury. Lancet (London, England), 357(9266), 1391–1396. [CrossRef]
- Stiell, I. G., Wells, G. A., Vandemheen, K. L., Clement, C. M., Lesiuk, H., De Maio, V. J., Laupacis, A., Schull, M., McKnight, R. D., Verbeek, R., Brison, R., Cass, D., Dreyer, J., Eisenhauer, M. A., Greenberg, G. H., MacPhail, I., Morrison, L., Reardon, M., & Worthington, J. (2001b). The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA, 286(15), 1841–1848. [CrossRef]
- Stiell, I. G., Clement, C. M., McKnight, R. D., Brison, R., Schull, M. J., Rowe, B. H., Worthington, J. R., Eisenhauer, M. A., Cass, D., Greenberg, G., MacPhail, I., Dreyer, J., Lee, J. S., Bandiera, G., Reardon, M., Holroyd, B., Lesiuk, H., & Wells, G. A. (2003). The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. The New England journal of medicine, 349(26), 2510–2518. [CrossRef]
- Stone, A., Salehmohamed, Q., & Stark, B. (2023). Point-of-care emergency clinical summary: Treating acute agitation with ketamine in the emergency department. Emergency Care BC. https://emergencycarebc.ca/clinical_resource/clinical-summary/treating-acute-agitation-with-ketamine-in-the-emergency-department/. /.
- Varner, C. (2023). Without more acute care beds, hospitals are on their own to grapple with emergency department crises. Canadian Medical Association Journal, 195(34). [CrossRef]
- Xie, E. C., Chan, K., Khangura, J. K., Koh, J. J.-K., Orkin, A. M., Sheikh, H., Hayman, K., Gupta, S., Kumar, T., Hulme, J., Mrochuk, M., & Dong, K. (2022). CAEP position statement on improving emergency care for persons experiencing homelessness: Executive summary. Canadian Journal of Emergency Medicine, 24(4), 369–375. [CrossRef]
Figure 1.
Educational logic map - Imaging access in the agitated adult trauma patient. (Educational synthesis for local adaptation; follow institutional policy and current specialty guidance. Not a clinical practice guideline.).
Figure 1.
Educational logic map - Imaging access in the agitated adult trauma patient. (Educational synthesis for local adaptation; follow institutional policy and current specialty guidance. Not a clinical practice guideline.).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



