Submitted:
30 September 2025
Posted:
01 October 2025
You are already at the latest version
Abstract
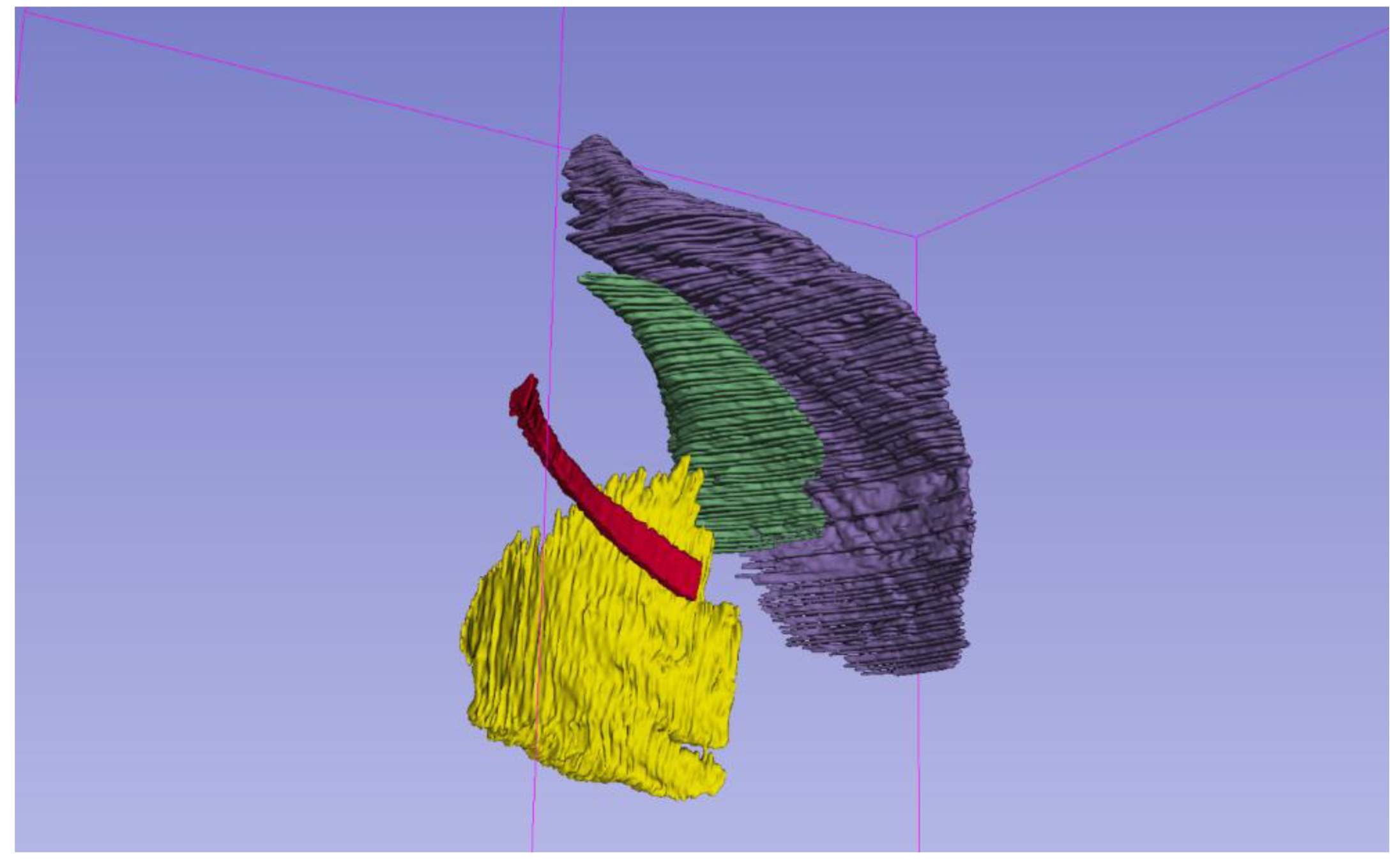
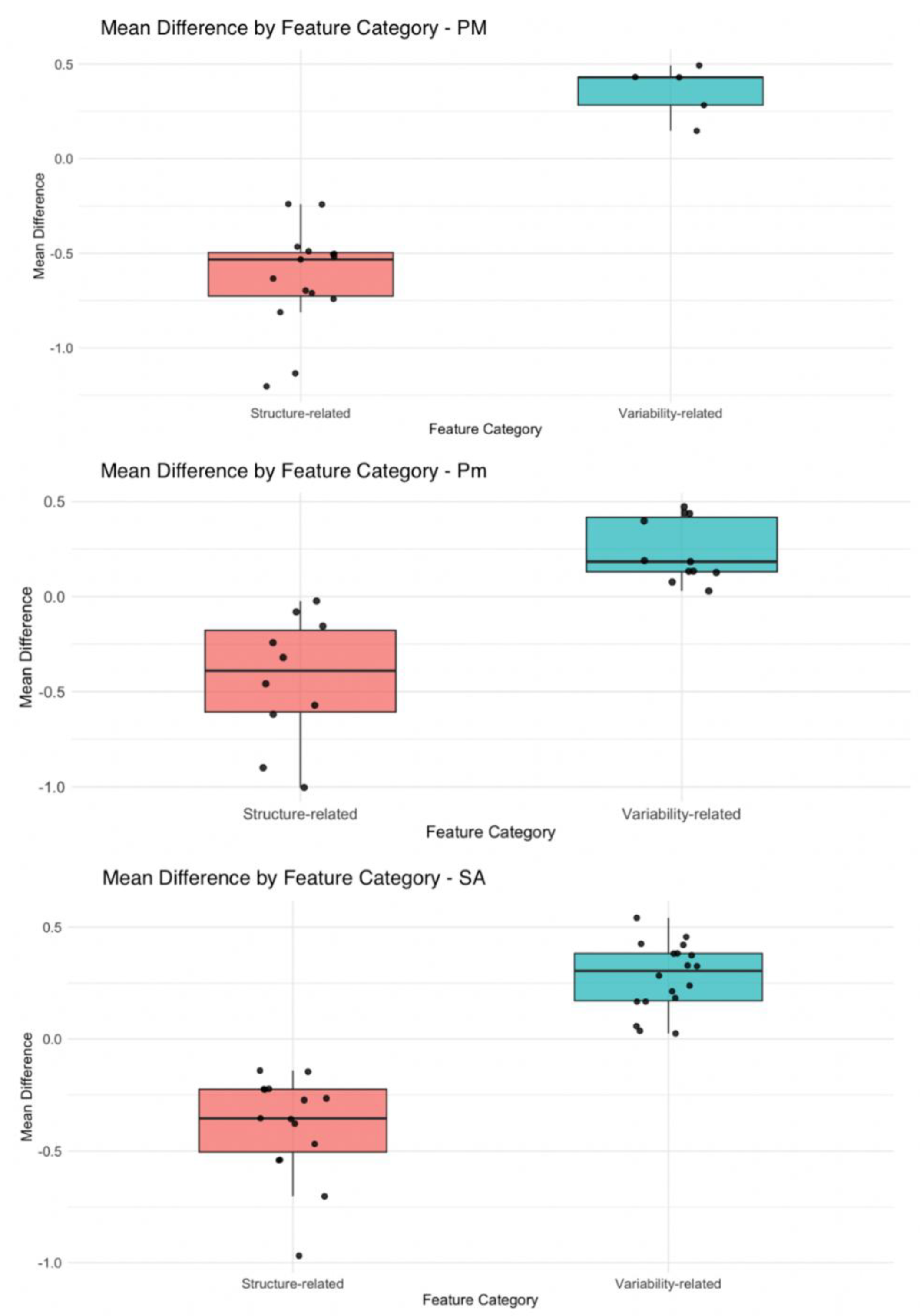
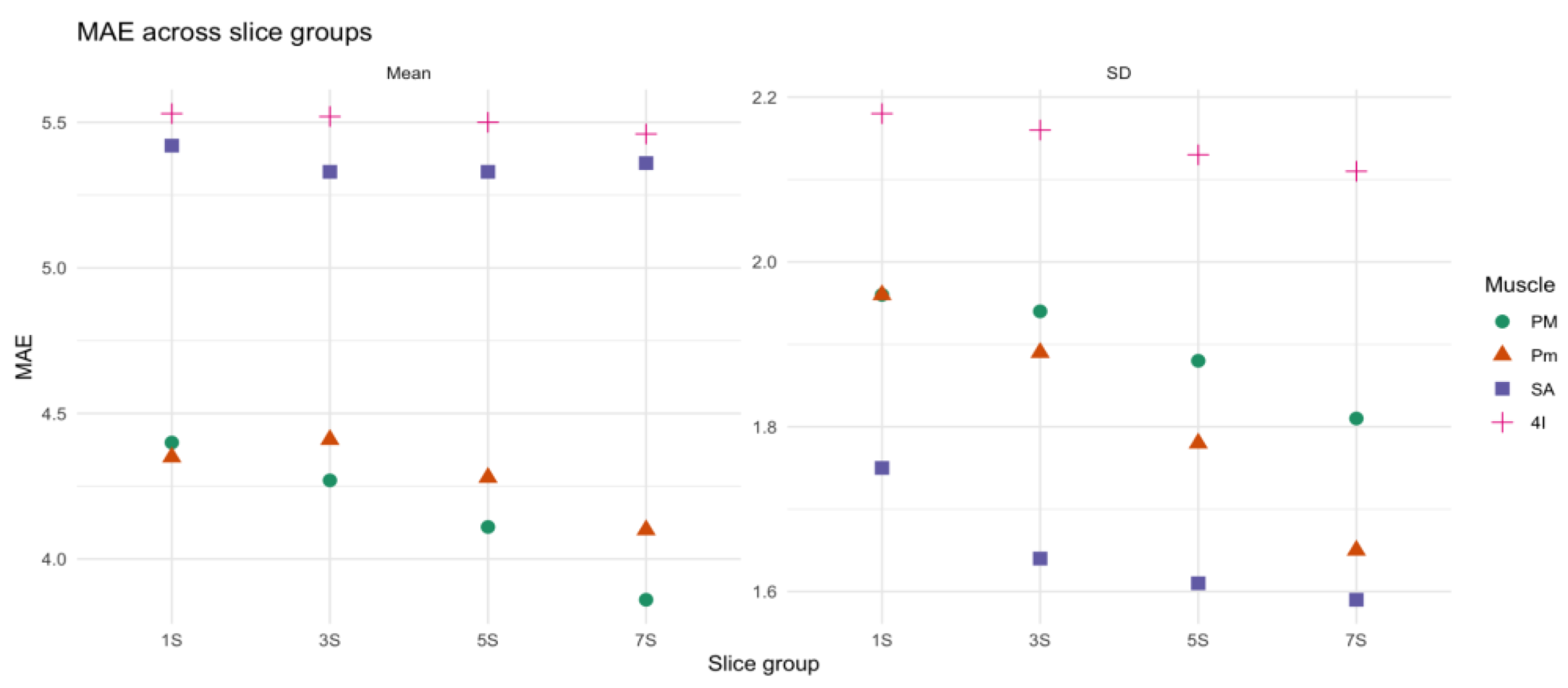
Background/Objectives: Respiratory muscle sarcopenia worsens outcomes in chronic lung disease, and quantitative CT may provide objective biomarkers; this study aimed to develop a time-efficient segmentation protocol and identify radiomic biomarkers of respiratory muscle sarcopenia. Methods: This retrospective study analyzed 30 unenhanced chest CT from adult patients. The whole volume of the pectoralis major (PM), pectoralis minor (Pm), serratus anterior (SA), and fourth intercostal (4I) muscles were manually segmented. Patients were classified as sarcopenic or non-sarcopenic. Radiomics features and mean muscle density were extracted using PyRadiomics. Features associated with sarcopenia were selected using LASSO regression and backward stepwise selection. Four sets of slices consisting of one, three, five, and seven slices were then sampled from each muscle around a fixed anatomical landmark. Deviations of each set of slices from whole-muscle metrics were evaluated using MAE and MAPE. Results: Features selection identified 25 biomarkers of sarcopenia in PM, 24 in Pm, and 34 in SA. Variability-related features were significantly associated with sarcopenia (OR = 2.26; P = .012), while structural features showed an inverse association (OR = 0.18; P = .004). Mean muscle density and most radiomic features were well represented by single slice for every muscle. In the PM and Pm eight and six radiomic features were better approximated segmenting more than one slice (p < 0.05). Conclusions: Radiomics enables quantitative assessment of sarcopenia. For SA, a simplified segmentation protocol consisting of a single slice enables to approximate muscle density and radiomics of whole muscle volume. For PM and Pm, three or more slices allow a better representation of 8 and 6 radiomic features respectively.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Analysis of Muscle Density and Radiomics and Correlation with Demographics
2.3. Definition of a Simplified Segmentation Protocol for Respiratory Muscle
3. Results
3.1. Patients’ Characteristic
3.2. Density Characterization
3.3. Radiomics Features Analysis
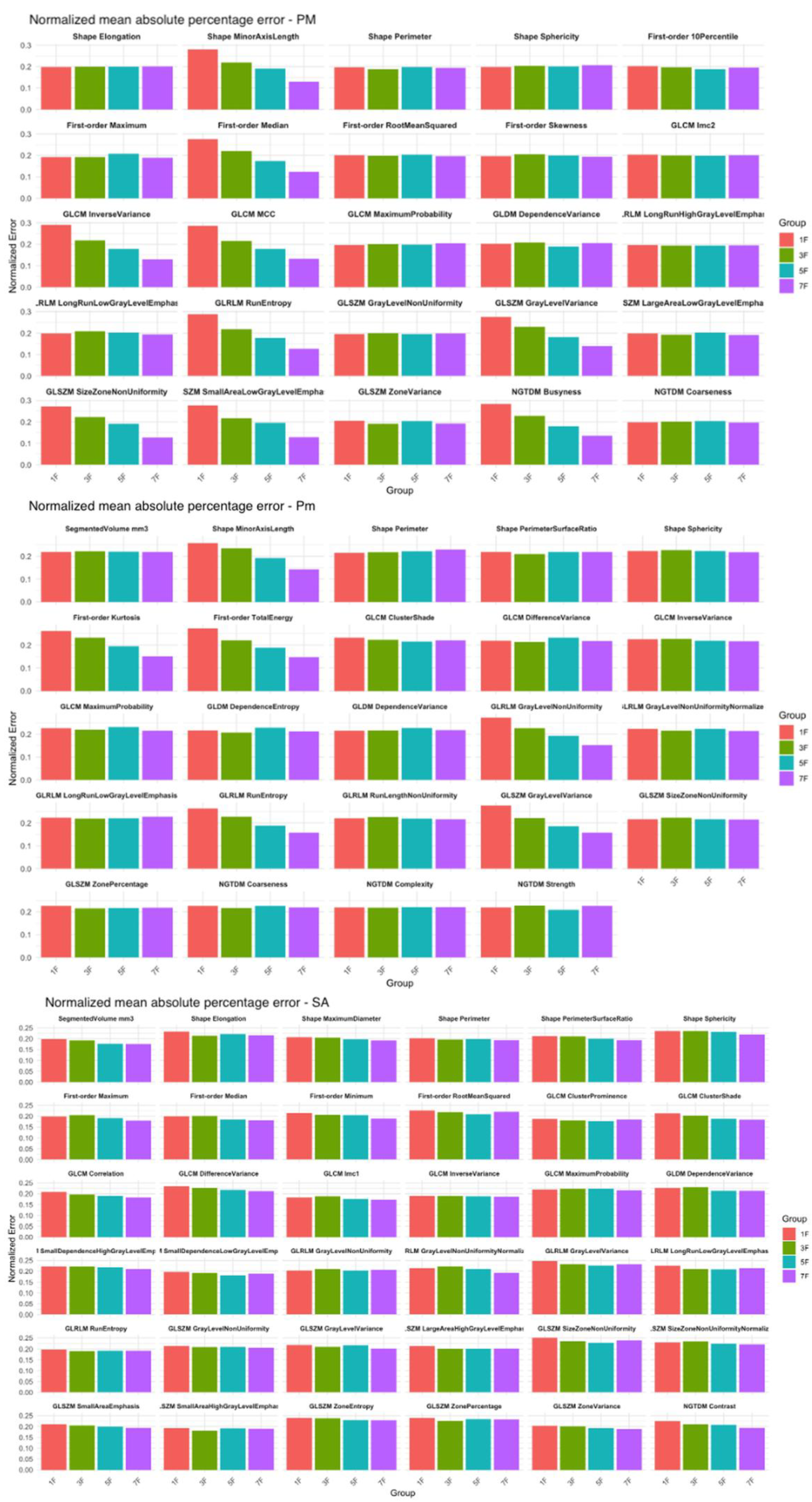
3.4. Comparison of Density and Radiomics in Small Slice Sets and in the Entire Muscle Volume
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CT | Computed Tomography |
| OR | Odds Ratio |
| COPD | Chronic Obstructive Pulmonary Disease |
| HU | Hounsfield Units |
| SD | Standard Deviation |
| PM | Pectoralis Major |
| Pm | Pectoralis Minor |
| 4I | Fourth intercostal muscle |
| SA | Serratus Anterior |
| BMI | Body Mass Index |
| MAE | Mean Absolute Error |
| MAPE | Mean Absolute Percentage Error |
| LASSO | Least Absolute Shrinkage and Selection Operator |
References
- Maltais F, Decramer M, Casaburi R, Barreiro E, Burelle Y, Debigaré R, Dekhuijzen PN, Franssen F, Gayan-Ramirez G, Gea J, Gosker HR, Gosselink R, Hayot M, Hussain SN, Janssens W, Polkey MI, Roca J, Saey D, Schols AM, Spruit MA, Steiner M, Taivassalo T, Troosters T, Vogiatzis I, Wagner PD; ATS/ERS Ad Hoc Committee on Limb Muscle Dysfunction in COPD. An official American Thoracic Society/European Respiratory Society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2014 May 1;189(9):e15-62. [CrossRef]
- Singer J, Yelin EH, Katz PP, Sanchez G, Iribarren C, Eisner MD, Blanc PD. Respiratory and skeletal muscle strength in chronic obstructive pulmonary disease: impact on exercise capacity and lower extremity function. J Cardiopulm Rehabil Prev. 2011 Mar-Apr;31(2):111-9. [CrossRef]
- Kim NS, Seo JH, Ko MH, Park SH, Kang SW, Won YH. Respiratory Muscle Strength in Patients With Chronic Obstructive Pulmonary Disease. Ann Rehabil Med. 2017 Aug;41(4):659-666. [CrossRef]
- Figueiredo RIN, Azambuja AM, Cureau FV, Sbruzzi G. Inspiratory Muscle Training in COPD. Respir Care. 2020 Aug;65(8):1189-1201. [CrossRef]
- McDonald ML, Diaz AA, Ross JC, San Jose Estepar R, Zhou L, Regan EA, Eckbo E, Muralidhar N, Come CE, Cho MH, Hersh CP, Lange C, Wouters E, Casaburi RH, Coxson HO, Macnee W, Rennard SI, Lomas DA, Agusti A, Celli BR, Black-Shinn JL, Kinney GL, Lutz SM, Hokanson JE, Silverman EK, Washko GR. Quantitative computed tomography measures of pectoralis muscle area and disease severity in chronic obstructive pulmonary disease. A cross-sectional study. Ann Am Thorac Soc. 2014 Mar;11(3):326-34. [CrossRef]
- 6 Mai DVC, Drami I, Pring ET, Gould LE, Lung P, Popuri K, Chow V, Beg MF, Athanasiou T, Jenkins JT; BiCyCLE Research Group. A systematic review of automated segmentation of 3D computed-tomography scans for volumetric body composition analysis. J Cachexia Sarcopenia Muscle. 2023 Oct;14(5):1973-1986.
- Ciciliot S, Rossi AC, Dyar KA, Blaauw B, Schiaffino S. Muscle type and fiber type specificity in muscle wasting. Int J Biochem Cell Biol. 2013 Oct;45(10):2191-9. [CrossRef]
- van Timmeren JE, Cester D, Tanadini-Lang S, Alkadhi H, Baessler B. Radiomics in medical imaging-”how-to” guide and critical reflection. Insights Imaging. 2020 Aug 12;11(1):91. [CrossRef]
- de Jong EEC, Sanders KJC, Deist TM, van Elmpt W, Jochems A, van Timmeren JE, Leijenaar RTH, Degens JHRJ, Schols AMWJ, Dingemans AC, Lambin P. Can radiomics help to predict skeletal muscle response to chemotherapy in stage IV non-small cell lung cancer? Eur J Cancer. 2019 Oct;120:107-113. [CrossRef]
- Geraghty EM, Boone JM. Determination of height, weight, body mass index, and body surface area with a single abdominal CT image. Radiology. 2003 Sep;228(3):857-63. [CrossRef]
- Derstine, B.A., Holcombe, S.A., Ross, B.E. et al. Skeletal muscle cutoff values for sarcopenia diagnosis using T10 to L5 measurements in a healthy US population. Sci Rep 8, 11369 (2018). [CrossRef]
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, Cooper C, Landi F, Rolland Y, Sayer AA, Schneider SM, Sieber CC, Topinkova E, Vandewoude M, Visser M, Zamboni M; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019 Jan 1;48(1):16-31. doi: 10.1093/ageing/afy169. Erratum in: Age Ageing. 2019 Jul 1;48(4):601. [CrossRef] [PubMed] [PubMed Central]
- Shi L, Shi W, Peng X, Zhan Y, Zhou L, Wang Y, Feng M, Zhao J, Shan F, Liu L. Development and Validation a Nomogram Incorporating CT Radiomics Signatures and Radiological Features for Differentiating Invasive Adenocarcinoma From Adenocarcinoma In Situ and Minimally Invasive Adenocarcinoma Presenting as Ground-Glass Nodules Measuring 5-10mm in Diameter. Front Oncol. 2021 Apr 21;11:618677. [CrossRef]
- Qiao J, Zhang X, Du M, Wang P, Xin J. 18F-FDG PET/CT radiomics nomogram for predicting occult lymph node metastasis of non-small cell lung cancer. Front Oncol. 2022 Sep 28;12:974934. [CrossRef]
- Fiz F, Costa G, Gennaro N, la Bella L, Boichuk A, Sollini M, Politi LS, Balzarini L, Torzilli G, Chiti A, Viganò L. Contrast Administration Impacts CT-Based Radiomics of Colorectal Liver Metastases and Non-Tumoral Liver Parenchyma Revealing the “Radiological” Tumour Microenvironment. Diagnostics (Basel). 2021 Jun 25;11(7):1162. [CrossRef]
- Yao L, Petrosyan A, Chaudhari AJ, Lenchik L, Boutin RD. Clinical, functional, and opportunistic CT metrics of sarcopenia at the point of imaging care: analysis of all-cause mortality. Skeletal Radiol. 2024 Mar;53(3):515-524. Epub 2023 Sep 9. [CrossRef]
- Li T, Wu G. Chest CT Radiomics is Feasible in Evaluating Muscle Change in Diabetes Patients. Curr Med Imaging. 2024;20:1-5. [CrossRef]
- Miao S, An Y, Liu P, Mu S, Zhou W, Jia H, Huang W, Li J, Wang R. Pectoralis muscle predicts distant metastases in breast cancer by deep learning radiomics. Acta Radiol. 2023 Sep;64(9):2561-2569. Epub 2023 Jul 12. [CrossRef]
- Ackermans LGC, Volmer L, Timmermans QMMA, Brecheisen R, Olde Damink SMW, Dekker A, Loeffen D, Poeze M, Blokhuis TJ, Wee L, Ten Bosch JA. Clinical evaluation of automated segmentation for body composition analysis on abdominal L3 CT slices in polytrauma patients. Injury. 2022;53(Suppl 3):S30–S41. [CrossRef]
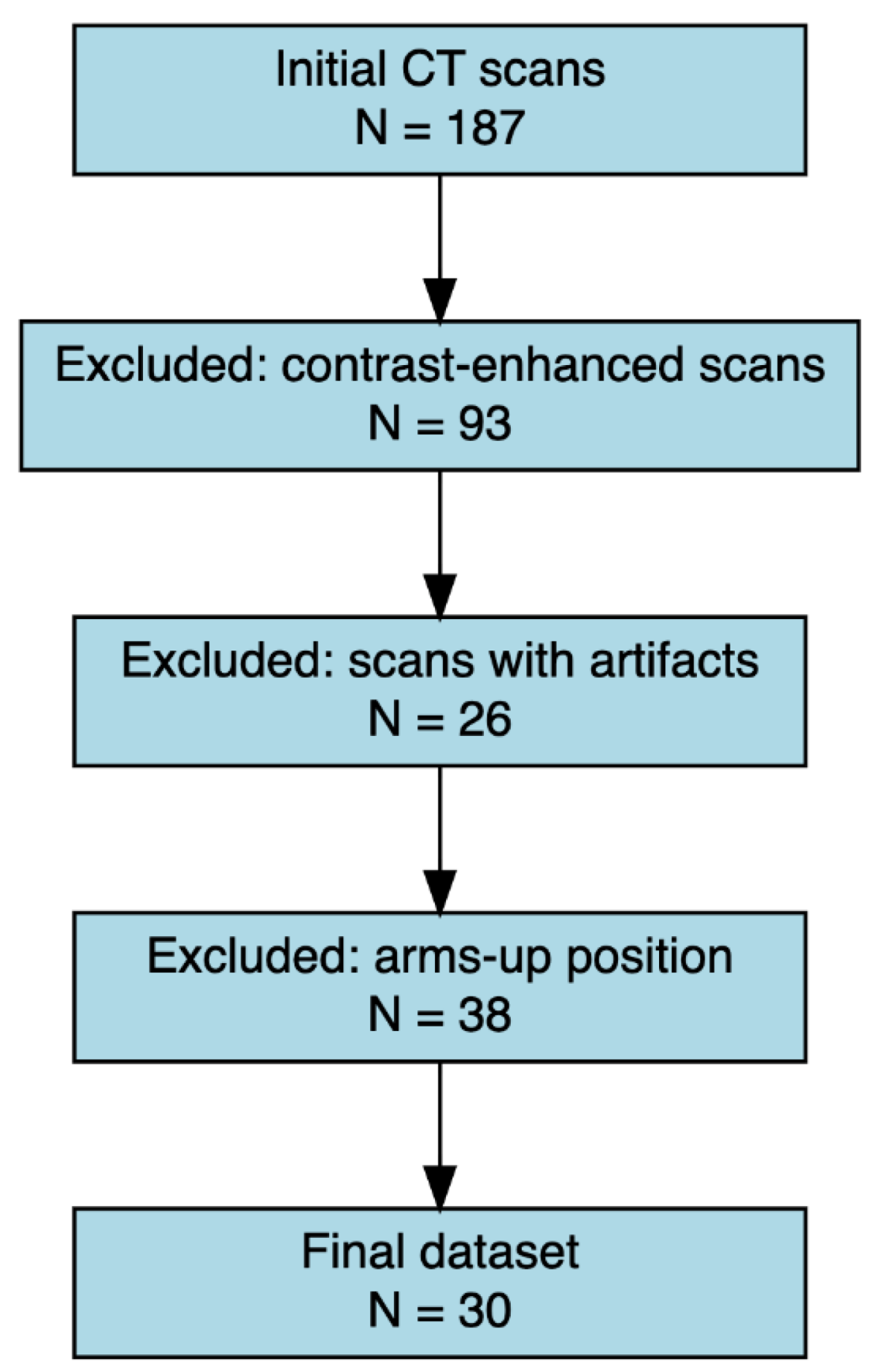


| Inclusion Criteria | Exclusion Criteria |
| Unenhanced CT scans including thoracic region from T1 to L1 | Presence of metallic artifacts (e.g., pacemakers, prostheses, sternal wires) |
| Patient positioned with both arms raised above the head | Age <18 years |
| CT acquired with the same scanner model | Poor image quality |
| Kilovoltage set between 120 and 130 kV | |
| Slice thickness of 2 mm |
| Variable | Total (n = 30) | Sarcopenic (n = 17) | Non-sarcopenic (n = 13) |
| Age (years) | 64.7 ± 17.2 | 70.4 ± 12.5 | 56.1 ± 20.0 |
| BMI (kg/m2) | 23.1 ± 3.3 | 22.0 ± 2.9 | 24.9 ± 3.2 |
| Females (n) | 16 (53%) | 11 (65%) | 5 (38%) |
| Males (n) | 14 (47%) | 6 (35%) | 8 (62%) |
| Caucasian | 28 (93,3%) | 17 (100%) | 11 (85%) |
| Muscle | Total density (HU) | Non-sarcopenic density (HU) | Sarcopenic density (HU) |
| SA | 15.0 ± 21.5 | 23.9 ± 16.6 | 3.1 ± 21.6 |
| PM | 25.5 ± 19.9 | 36.9 ± 14.1 | 15.2 ± 18.8 |
| 4I | -27.8 ± 26.3 | -18.4 ± 25.3 | -38.8 ± 23.0 |
| Pm | 27.6 ± 15.4 | 32.8 ± 15.9 | 23.3 ± 13.6 |
| Muscle | Density 18-45 years (HU) | Density 46-69 years (HU) | Density ≥70 years (HU) |
| SA | 34.2 ± 7.7 | 9.1 ± 13.5 | 8.7 ± 18.7 |
| PM | 44.3 ± 9.2 | 17.1 ± 23.9 | 14.2 ± 10.9 |
| 4I | 7.1 ± 11.9 | -37.9 ± 12.6 | -35.4 ± 20 |
| Pm | 41.3 ± 11.8 | 22.9 ± 12.3 | 20.7 ± 9.1 |
| Muscle | Variability-related features | Density-related features |
| Pectoralis Major (PM) | GLCM Inverse Variance, GLCM MCC, GLCM Maximum Probability, GLDM Dependence Variance, GLRLM Run Entropy, GLSZM Gray Level Non Uniformity, GLSZM Gray Level Variance, GLSZM Zone Variance, GLSZM Size Zone Non Uniformity, NGTDM Busyness, NGTDM Coarseness, RLM Long Run Low Gray Level Emphasis, GLCM Imc2 | First-order Maximum, First-order Median, First-order RootMeanSquared, First-order Skewness, First-order 10Percentile |
| Pectoralis Minor (Pm) | GLCM Cluster Shade, GLCM Difference Variance, GLCM Inverse Variance, GLCM Maximum Probability, GLDM Dependence Entropy, GLDM Dependence Variance, GLRLM Gray Level Non Uniformity, GLRLM Run Entropy, GLRLM Run Length Non Uniformity, GLSZM Gray Level Variance, GLSZM Size Zone Non Uniformity, GLSZM Zone Percentage, NGTDM Coarseness, NGTDM Complexity, NGTDM Strength, LRLM Gray Level Non Uniformity Normalized | First-order Kurtosis, First-order TotalEnergy, Segmented Volume mm3 |
| Serratus Anterior (SA) | GLCM Cluster Prominence, GLCM Cluster Shade, GLCM Correlation, GLCM Difference Variance, GLCM Inverse Variance, GLCM Maximum Probability, GLDM Dependence Variance, GLRLM Gray Level Non Uniformity, GLSZM Gray Level Variance, GLSZM Zone Entropy, GLSZM Zone Variance, GLSZM Size Zone Non Uniformity, GLSZM Zone Percentage, NGTDM Contrast, NGTDM Coarseness | First-order Maximum, First-order Median, First-order Minimum, First-order Root Mean Squared, Segmented Volume mm3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



