Submitted:
29 September 2025
Posted:
30 September 2025
Read the latest preprint version here
Abstract
Heat exposure is rapidly becoming one of the most pressing health issues of the 21st century. Much work to date has focused on the impact of high heat conditions on outdoor workers but not focused on indoor workers who may be exposed to high heat conditions, such as restaurant workers. Restaurant workers are frequently exposed to high heat conditions at work both due to increasing environmental temperatures and occupational factors. Of particular concern to heat exposed workers are the impact of occupational heat exposure on the kidneys, which has shown to cause acute kidney injury simply from working in the heat. Therefore, the purpose of this scoping review is to identify what studies have been completed investigating the impact of heat exposure on kidney functioning in restaurant workers. We followed Arksey and O’Malley’s 5-step framework for conducting scoping reviews. Searches were conducted in PubMed, CINAHL, Embase, and Web of Science. Of the 287 studies identified, 246 were screened at the title and abstract level and four full texts were screened. Ultimate, 2 journal articles and 1 conference proceeding were included in this review. All three studies were conducted internationally, with two collecting data primarily in the winter or spring. None of the studies utilized similar protocols for measuring heat strain (both environmental and physiological) nor measuring kidney function. Based on the findings of this review, there is a critical need for additional research to investigate the impact of occupational heat exposure on kidney functioning in restaurant workers, both globally and within the United States.
Keywords:
restaruant workers
; climate change
; heat exposure
; kidney function
Introduction
Heat exposure is one of the most significant global public health threats of the 21st century [1] and the summer of 2024 was the hottest summer on record.[2] Increasing global temperatures are leading to increased rates of heat-related illness (HRI), with every 1°C morbidity from heat-related illnesses increases by 35% and mortality increases by 18%.[3] Rising temperatures are also thought to have produced one of the first environmentally-driven chronic diseases, chronic kidney disease of non-traditional etiology (CKDnt).[4,5] Daily occupational heat exposure, leading to repeated acute kidney injury (AKI) due to renal ischemia secondary to heat-induced volume depletion[6] and inflammatory changes in the kidney[7] is thought to be the primary risk factor for developing CKDnt.[8,9,10] Besides the general population, extreme heat isbecoming more dangerous for workers every year, as strong evidence suggests the odds of developing AKI in farmworkers increases by 47% for 5°F increase in environmental temperature.[11] Similarly, construction workers are at a higher risk of developing AKI[12] and CKD[13] likely due to strenuous outdoor work in extreme heat. However, limited studies exist showing the effects of indoor heat exposure on workers’ kidney health.[14]
Within the restaurant industry, workers report work environments that are made intolerable by high heat conditions where the ambient air temperature frequently reaches temperatures of 100°F (34°C). [15,16] Not only do these high ambient temperatures impact workers, but workers face extra sources of heat from restaurant ovens, which can reach temperatures up to 750°F.[17] The prevalence of heat-related illness (HRI) symptoms in restaurant workers ranges from 20-65%,[18] further highlighting the need to understand the relationship between occupational heat exposure and kidney functioning in this working group.
Understanding the association between excessive indoor heat and worker health is increasingly recognized as a public health priority.[19] Due to an anticipated dearth of literature investigating the impacts of occupational heat exposure on kidney functioning in indoor workers, a scoping review methodology was chosen for an initial examination of the literature on indoor heat exposure and kidney health in restaurant workers.
Objectives
The primary objective of this paper is to outline and examine the existing literature about indoor heat exposure and kidney health in restaurant workers. The secondary objective was to identify gaps in the existing research for future research assessing occupational heat-related illnesses and kidney function in restaurant workers.
Methods
Design
This review followed the PRISMA-ScR[20] guidelines and Arksey and O’Malley’s five step methodological framework for conducting scoping reviews.[21] Arksey and O’Malley[21] suggest the following five steps for conducing scoping reviews: 1) research question identification; 2) identifying potential studies through an in-depth database search utilizing PubMed, Web of Science, EMBASE, and CINAHL; 3) study inclusion based on pre-determined inclusion criteria; 4) charting of the data; and 5) collating, summarizing, and reporting of study results. They also propose a sixth, optional step of consultation, which was not utilized in this review. No formal protocol was registered for this review given its rapid nature.
Research Question
Following step 1 of the Arksey and O’Malley framework,[21] we identified our research question as: what studies have been conducted to assess the connection between occupational heat exposure and kidney function in restaurant workers?
Literature Search
Identification of potential studies is step 2 of the Arksey and O’Malley framework.[21] This was achieved by searching PubMed, Web of Science, EMBASE, and CINAHL. Search terms were crafted by adjusting the search terms of Smith et al. 2021 to focus on restaurant workers rather than farm workers. The search terms were originally developed for PubMed, translated for Web of Science, EMBASE, and CINAHL, and were reviewed by DS and SFC before the searches were conducted. Searches were limited to the time of January 1, 2015, through the latest search date of August, 22, 2025 and were limited to either English or Spanish articles, as the author team does not possess linguistic abilities in additional languages. No geographic limitation was included in the search. After the initial database search, the reference list was exported into Covidence, duplicates were removed, and titles and abstracts were reviewed by CG and SFC. If there was conflict between the two primary reviewers, DS served as the adjudicator. The references of included articles at the level of title and abstract were also searched for additional articles to include in this review. This process was then repeated at the level of full text review with CG and SFC serving as primary reviewers and DS as adjudicator.
Eligibility Criteria
Step 3 of the framework is to identify included articles based on inclusion & exclusion criteria.[21] Inclusion criteria for this review were 1) primary research with restaurant workers and 2) assessed the relationship between occupational heat exposure and kidney function. Exclusion criteria included 1) non-English or non-Spanish articles and 2) focus on outdoor, heat exposed occupations.
Data Extraction
For step 4 of the framework,[21] each author was assigned a single article from which to extract data. Author DS then verified the extracts and created the final data extraction table. The table included variables recommended by Arksey and O’Malley and included: 1) author(s), publication year, and study location (i.e., country); 2) intervention and standard of comparison, if applicable; 3) study population (and control); 4) study aims; 5) methodology; 6) outcome measures (specifically measurement of heat strain and kidney function); and 7) principal results.
Results
A total of 287 studies were identified in this review (Figure 1). Ultimately, three studies were included for final analysis during this review (Table 1). Two of the studies, Saif Eldin et al.2 and Singh et al.3 were complete journal articles. The work of Venugopal et al. was a published abstract.4 All of the studies were cross-sectional with restaurant workers that assessed the relationship between occupational heat exposure and kidney function.[22,23,24] The articles were published between 2016 and 2022 with data collection primarily occurring in the winter. Research was conducted in India[22,24] and Egypt.[23] Two studies sampled workers from commercial kitchens,[22,24] and the third study sampled workers in a hospital kitchen.[23] Participants included exclusively male kitchen workers, male and female kitchen workers, and commercial kitchen workers (no demographics reported). Controls for the studies varied, including indirectly heat-exposed (food prep, washing, and storage areas), other staff (office workers and service areas), and the work of Venugopal et al.,[24] having no control reported.
Heat Strain
Environmental
Environmental measures of heat strain in the included studies were the calculated heat index, calculated wet-bulb globe temperature index, and an occupational assessment to identify heat risk environment (overcrowding, ventilation). In the study done by Eldin et al.,[23] the exposed group mean value of the wet bulb globe temperature (WBGT) was (32.4+/-1.4), which exceeded the threshold limit value of (28 degrees Celsius) recommendations. Venugopal et al., reported that 66% of workers were exposed to WBGT levels higher than the threshold limit value, with an average exposure of 30.1°C±2.7°C.[24] Singh et al. utilized a calculated humidex value to quantify environmental heat strain.[22]
Physiological
Physiological measures of heat exposure included in the studies were self-reported heat-related symptoms, core body temperature, and sweat rate. One study collected no physiological measures of heat strain, other than dehydration.[22] Eldin et al., additionally collected data on the amount of water consumed by kitchen workers compared to controls. Heat-exposed workers were found to have consumed significantly less water than controls (p-value < 0.001).[23]
Kidney Function
All three studies included assessed kidney function.[22,23,24] Measures of kidney health included microalbuminuria,[22] uranalysis of interleukin-18 (IL-18) and neutrophil gelatinase-associated Lipocalin (NGAL),[23] and serum creatinine (to calculate GFR).[24] Kidney function results are reported in Table 1.
Discussion
This review found few studies investigating the association of occupational heat exposure in restaurants and kidney function in workers, none of which were conducted in the U.S. While this is expected, given the scholarly emphasis on outdoor workers,[12,14,25] it also represents an area for future research to elucidate the impacts of heat exposure on restaurant workers. While it is assumed that indoor workers have access to adequate cooling measures, such as air conditioning, this is not the case for many restaurant workers.[15,16] Importantly, the existing studies were limited to commercial and institutional (hospital) kitchens, with no research conducted in smaller, traditional restaurant settings. These smaller kitchens often have fewer resources, less sophisticated ventilation, and more variable staffing, which may amplify the health risks of heat exposure, not only in the kitchen, but also in the front of the house.
As seen in heat exposure studies from other industries, such as construction[12,13] and agriculture,[11,26,27] the studies in this review had varying protocols for assessing heat stress and kidney functioning.[22,23,24] The lack of standardized protocols for assessing heat stress and kidney functioning make comparisons across studies difficult to interpret[27] and potentially create confusion for employers on how to best protect their workforce from the dangers of heat. Thus, opening employers up to liability[28] and potentially contributing to underreporting of occupational-related heat morbidity. Furthermore, the appropriateness of certain measures warrants scrutiny. For example, relying solely on self-reported heat symptoms or cross-shift urine samples may underestimate risk compared to validated biomarkers or continuous physiologic monitoring. Similarly, the use of inappropriate control groups, such as office or service staff, raises concerns about validity, as these workers may or may not experience the same occupational demands as kitchen staff. Future studies should ensure controls reflect comparable work environments and exposures.
Environmental monitoring was also inconsistently applied.[22,23,24] While some studies utilized WBGT, humidex, or heat index, others relied primarily on physiologic measures without concurrent environmental data. Given the dynamic and variable heat loads in kitchens, future research should always incorporate objective environmental monitoring alongside physiologic and renal measures. Moreover, most data collection occurred in cooler months, such as winter or spring, which likely underestimates true risk. Summer data collection should be considered essential, as peak heat conditions are when workers face the highest physiological burden.[29,30]
Food safety regulations represent another major consideration when designing any intervention to decrease restaurant worker heat exposure and any resulting kidney dysfunction. Many local municipalities do not allow kitchen workers to keep hydration beverages, including water, near food preparation areas.[31,32] However, even in those municipalities that do allow beverages in hot areas of the kitchen, such as the state of Georgia,[33] may not know of these rules allowing them to keep water with them during a work shift. These policy inconsistencies may potentially restrict any effort to mitigate occupational heat strain in the restaurant industry.
Due to indoor workers’ vulnerability to excessive heat, recent studies highlight a need for updated occupational health regulations to protect indoor workers.[14,34] For workers within the United States, the Occupational Health and Safety Administration (OSHA) and National Institute for Occupational Safety and Health (NIOSH) have recommended criteria for occupational exposure to heat and hot environments. However, their recommendations are grossly outdated. Currently, it is unclear how many states include indoor workers in their heat standards. However both California[35] and Minnesota explicitly mention indoor workers in their heat standards and policies.[36] California’s adoption of an indoor heat standard in July 2024 has introduced significant protections for restaurant workers by requiring safety measures when indoor temperatures reach 82°F or higher, aiming to prevent heat-related illnesses.[37] This highlights the immediate need for new research studies to further explore the relationship between cumulative indoor heat exposure, hydration behaviors, and kidney health outcomes.
Limitations
We did not search Proquest dissertation or theses, potential missing non-peer reviewed academic work that was completed as part of doctoral dissertations or theses. Additionally, none of the authors had access to occupational health specific databases, such as such as the National Institute for Occupational Safety and Health or the Occupational Safety and Health Administration Database.
Conclusion
Indoor heat exposure is an emerging occupational health issue that has received far less attention than outdoor work in agriculture or construction. Restaurant workers are frequently assumed to have access to air conditioning, yet many workplaces lack sufficient cooling, leaving employees vulnerable to repeated heat stress. Given the lack of enforceable, indoor heat standards, particularly within the United States, there is still much to learn about the specific, long-term health effects of repeated occupational heat exposure in restaurant workers and interventions to protect these workers.
Funding
This work was funded in part by National Institutes of Health/National Institute of Nursing Research award K01NR021272.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Appendix A
- PubMed
(("Restaurants"[Mesh] OR "Food Services"[Mesh] OR restaurant worker* OR food service worker* OR kitchen staff OR kitchen worker* OR kitchen employee* OR kitchen environment* OR kitchen* OR cook* OR chef* OR line cook* OR dishwasher* OR dish washer* OR waiter* OR waitress* OR server* OR host* OR hostess* OR "back of the house" OR "front of the house")) AND (("Acute Kidney Injury"[Mesh] OR "Renal Insufficiency"[Mesh] OR "Kidney Diseases"[Mesh] OR acute kidney injur* OR AKI OR acute renal injur* OR acute renal insufficienc* OR kidney dysfunction OR kidney function) AND ("Occupational Exposure"[Mesh] OR "Heat Stress Disorders"[Mesh] OR "Threshold Limit Values"[Mesh] OR "Maximum Allowable Concentration"[Mesh] OR occupational exposure OR heat stress OR heat strain OR heat exhaustion OR heat stroke OR sunstroke OR heat-related illness OR heat related illness OR dehydration OR hydration)) AND ("Humans"[Mesh]) AND (english[lang] OR spanish[lang])
- Embase
('restaurant'/exp OR 'food service'/exp OR restaurant*:ti,ab OR 'food service*':ti,ab OR 'kitchen staff':ti,ab OR 'kitchen worker*':ti,ab OR 'kitchen employee*':ti,ab OR kitchen*:ti,ab OR cook*:ti,ab OR chef*:ti,ab OR 'line cook*':ti,ab OR dishwasher*:ti,ab OR 'dish washer*':ti,ab OR waiter*:ti,ab OR waitress*:ti,ab OR server*:ti,ab OR host*:ti,ab OR hostess*:ti,ab OR 'back of the house':ti,ab OR 'front of the house':ti,ab) AND ('acute kidney injury'/exp OR 'renal insufficiency'/exp OR 'kidney disease'/exp OR 'acute kidney injur*':ti,ab OR aki:ti,ab OR 'acute renal injur*':ti,ab OR 'acute renal insufficienc*':ti,ab OR 'renal insufficienc*':ti,ab OR 'kidney dysfunction':ti,ab OR 'kidney function':ti,ab OR 'kidney disease*':ti,ab) AND ('occupational exposure'/exp OR 'heat stress'/exp OR 'heat exhaustion'/exp OR 'heat stroke'/exp OR 'sunstroke'/exp OR 'occupational exposure':ti,ab OR 'heat stress':ti,ab OR 'heat strain':ti,ab OR 'heat exhaustion':ti,ab OR 'heat stroke':ti,ab OR sunstroke:ti,ab OR 'heat-related illness':ti,ab OR 'heat related illness':ti,ab OR dehydration:ti,ab OR hydration:ti,ab OR 'threshold limit value*':ti,ab OR 'maximum allowable concentration':ti,ab) AND [humans]/lim AND ([english]/lim OR [spanish]/lim) AND [2015-2025]/py
- CINAHL
(TI (restaurant* OR "food service*" OR kitchen* OR cook* OR chef* OR "line cook*" OR dishwasher* OR waiter* OR waitress* OR server* OR host* OR hostess* OR "back of the house" OR "front of the house") OR AB (restaurant* OR "food service*" OR kitchen* OR cook* OR chef* OR "line cook*" OR dishwasher* OR waiter* OR waitress* OR server* OR host* OR hostess* OR "back of the house" OR "front of the house")) AND (TI ("acute kidney injur*" OR AKI OR "acute renal injur*" OR "acute renal insufficienc*" OR "renal insufficienc*" OR "kidney dysfunction" OR "kidney function" OR "kidney disease*") OR AB ("acute kidney injur*" OR AKI OR "acute renal injur*" OR "acute renal insufficienc*" OR "renal insufficienc*" OR "kidney dysfunction" OR "kidney function" OR "kidney disease*")) AND (TI ("occupational exposure" OR "heat stress" OR "heat strain" OR "heat exhaustion" OR "heat stroke" OR sunstroke OR "heat-related illness" OR "heat related illness" OR dehydration OR hydration) OR AB ("occupational exposure" OR "heat stress" OR "heat strain" OR "heat exhaustion" OR "heat stroke" OR sunstroke OR "heat-related illness" OR "heat related illness" OR dehydration OR hydration))
Date limited 1/1/2015-08/22/2025
English and Spanish
Web of Science (with “Select All Databases” selected).
TS=(restaurant* OR "food service*" OR "kitchen staff" OR "kitchen worker*" OR "kitchen employee*" OR kitchen* OR cook* OR chef* OR "line cook*" OR dishwasher* OR "dish washer*" OR waiter* OR waitress* OR server* OR host* OR hostess* OR "back of the house" OR "front of the house") AND TS=("acute kidney injur*" OR AKI OR "acute renal injur*" OR "acute renal insufficienc*" OR "renal insufficienc*" OR "kidney dysfunction" OR "kidney function" OR "kidney disease*") AND TS=("occupational exposure" OR "heat stress" OR "heat strain" OR "heat exhaustion" OR "heat stroke" OR sunstrate OR "heat-related illness" OR "heat related illness" OR dehydration OR hydration OR "threshold limit value*" OR "maximum allowable concentration")
Limited to English or Spanish
Pub date: 2015-01-01 to 2025-08-22
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist
| SECTION | ITEM | PRISMA-ScR CHECKLIST ITEM | REPORTED ON PAGE # |
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 2-3 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 3 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | 4 |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 5 |
| Information sources* | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 4 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | Appendix |
| Selection of sources of evidence† | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 4-5 |
| Data charting process‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 5; Table 1 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 5 |
| Critical appraisal of individual sources of evidence§ | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | n/a |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 5 |
| RESULTS | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 5; Figure 1 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 5-7 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | na |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 5-7 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 5-7 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 7-10 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 10 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 10 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 11 |
References
- Watts, N.; Amann, M.; Ayeb-Karlsson, S.; Belesova, K.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Chambers, J.; Cox, P. M.; Daly, M.; Dasandi, N.; Davies, M.; Depledge, M.; Depoux, A.; Dominguez-Salas, P.; Drummond, P.; Ekins, P.; Flahault, A.; Frumkin, H.; Georgeson, L.; Ghanei, M.; Grace, D.; Graham, H.; Grojsman, R.; Haines, A.; Hamilton, I.; Hartinger, S.; Johnson, A.; Kelman, I.; Kiesewetter, G.; Kniveton, D.; Liang, L.; Lott, M.; Lowe, R.; Mace, G.; Odhiambo Sewe, M.; Maslin, M.; Mikhaylov, S.; Milner, J.; Latifi, A. M.; Moradi-Lakeh, M.; Morrissey, K.; Murray, K.; Neville, T.; Nilsson, M.; Oreszczyn, T.; Owfi, F.; Pencheon, D.; Pye, S.; Rabbaniha, M.; Robinson, E.; Rocklöv, J.; Schütte, S.; Shumake-Guillemot, J.; Steinbach, R.; Tabatabaei, M.; Wheeler, N.; Wilkinson, P.; Gong, P.; Montgomery, H.; Costello, A. The Lancet Countdown on Health and Climate Change: From 25 Years of Inaction to a Global Transformation for Public Health. The Lancet (British edition) 2018, 391 (10120), 581–630. [CrossRef]
- Weikert, G.; Younger, S.; SubbaRao, M. 2024 is the Warmest Year on Record. NASA Scientific Visualization Studio. https://svs.gsfc.nasa.gov/14743/ (accessed 2025-09-22).
- Faurie, C.; Varghese, B. M.; Liu, J.; Bi, P. Association between High Temperature and Heatwaves with Heat-Related Illnesses: A Systematic Review and Meta-Analysis. The Science of the total environment 2022, 852, 158332. [CrossRef]
- Johnson, R. J.; Sánchez-Lozada, L. G.; Newman, L. S.; Lanaspa, M. A.; Diaz, H. F.; Lemery, J.; Rodriguez-Iturbe, B.; Tolan, D. R.; Butler-Dawson, J.; Sato, Y.; Garcia, G.; Hernando, A. A.; Roncal-Jimenez, C. A. Climate Change and the Kidney. ANN NUTR METAB 2019, 74 (Suppl 3), 38–44. [CrossRef]
- Sorensen, C.; Garcia-Trabanino, R. A New Era of Climate Medicine — Addressing Heat-Triggered Renal Disease. NEW ENGL J MED 2019, 381 (8), 693–696. [CrossRef]
- Liu, J.; Varghese, B. M.; Hansen, A.; Borg, M. A.; Zhang, Y.; Driscoll, T.; Morgan, G.; Dear, K.; Gourley, M.; Capon, A.; Bi, P. Hot Weather as a Risk Factor for Kidney Disease Outcomes: A Systematic Review and Meta-Analysis of Epidemiological Evidence. SCI TOTAL ENVIRON 2021, 801, 149806. [CrossRef]
- Hansson, E.; Glaser, J.; Jakobsson, K.; Weiss, I.; Wesseling, C.; Lucas, R. A. I.; Wei, J. L. K.; Ekström, U.; Wijkström, J.; Bodin, T.; Johnson, R. J.; Wegman, D. H. Pathophysiological Mechanisms by Which Heat Stress Potentially Induces Kidney Inflammation and Chronic Kidney Disease in Sugarcane Workers. NUTRIENTS 2020, 12 (6), 1639. [CrossRef]
- Chapman, C. L.; Hess, H. W.; Lucas, R. A. I.; Glaser, J.; Saran, R.; Bragg-Gresham, J.; Wegman, D. H.; Hansson, E.; Minson, C. T.; Schlader, Z. J. Occupational Heat Exposure and the Risk of Chronic Kidney Disease of Nontraditional Origin in the United States. AM J PHYSIOL-REG I 2021, 321 (2), R141–R151. [CrossRef]
- Wesseling, C.; Glaser, J.; Rodríguez-Guzmán, J.; Weiss, I.; Lucas, R.; Peraza, S.; da Silva, A. S.; Hansson, E.; Johnson, R. J.; Hogstedt, C.; Wegman, D. H.; Jakobsson, K. Chronic Kidney Disease of Non-Traditional Origin in Mesoamerica: A Disease Primarily Driven by Occupational Heat Stress. REV PANAM SALUD PUBL 2020, 44 (1), 1–13. [CrossRef]
- Smith, D. J. The Importance of an Occupational History: Chronic Kidney Disease vs Chronic Kidney Disease of Non-Traditional Etiology. WORKPLACE HEALTH SAF 2024, 72 (4), 161–161. [CrossRef]
- Mix, J.; Elon, L.; Vi Thien Mac, V.; Flocks, J.; Economos, E.; Tovar-Aguilar, A. J.; Stover Hertzberg, V.; McCauley, L. A. Hydration Status, Kidney Function, and Kidney Injury in Florida Agricultural Workers. J OCCUP ENVIRON MED 2018, 60 (5), e253–e260. [CrossRef]
- Tourula, E.; Specht, J. W.; Hite, M. J.; Walker, C.; Garcia, S.; Khandpekar, O.; Yoder, H. A.; Zoh, R. S.; Johnson, B. D.; Wegman, D. H.; Glaser, J.; Amorim, F.; Schlader, Z. J. Hyperthermia Predicts Cross-Shift Acute Kidney Injury Risk in Construction Workers. KIDNEY INT REP 2025, 10 (8), 2856–2859. [CrossRef]
- Acharya, P.; Boggess, B.; Zhang, K. Assessing Heat Stress and Health among Construction Workers in a Changing Climate: A Review. INT J ENV RES PUB HE 2018, 15 (2), 247. [CrossRef]
- Smith, D. J.; Mac, V.; Thompson, L. M.; Plantinga, L.; Kasper, L.; Hertzberg, V. S. Using Occupational Histories to Assess Heat Exposure in Undocumented Workers Receiving Emergent Renal Dialysis in Georgia. Workplace Health Saf 2022, 70 (5), 251–258. [CrossRef]
- Garza, F. Heat Waves Make Restaurant Kitchens Unsafe. Workers Are Fighting Back. - Eater. Eatery. https://www.eater.com/2024/6/11/24176122/climate-change-heat-wave-restaurant-kitchen-safety-worker-protests (accessed 2025-01-16).
- Wakim, O. With federal heat protections pending, Atlanta food service workers swelter. Atlanta Journal Constitution. https://www.ajc.com/food-and-dining/with-federal-heat-protections-pending-atlanta-food-service-workers-swelter/TN7VPDCD7VANNCANOVQZ2OXD6Q/ (accessed 2025-01-16).
- Ciarmiello, M.; Morrone, B. Why Not Using Electric Ovens for Neapolitan Pizzas? A Thermal Analysis of a High Temperature Electric Pizza Oven. Energy Procedia 2016, 101, 1010–1017. [CrossRef]
- Restaurant Opportunities Centers United. Beat the Heat: Restaurant Workers Fight for a Safe and Dignified Work Environment; 2023. https://drive.google.com/file/d/1gBTefVhXOTzxAcHuiAmyRqciwr1ahfcx/view.
- Morris, N. B.; Jay, O.; Flouris, A. D.; Casanueva, A.; Gao, C.; Foster, J.; Havenith, G.; Nybo, L. Sustainable Solutions to Mitigate Occupational Heat Strain – an Umbrella Review of Physiological Effects and Global Health Perspectives. Environ Health 2020, 19 (1), 95–24. [CrossRef]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O’Brien, K. K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M. D. J.; Horsley, T.; Weeks, L.; Hempel, S.; Akl, E. A.; Chang, C.; McGowan, J.; Stewart, L.; Hartling, L.; Aldcroft, A.; Wilson, M. G.; Garritty, C.; Lewin, S.; Godfrey, C. M.; Macdonald, M. T.; Langlois, E. V.; Soares-Weiser, K.; Moriarty, J.; Clifford, T.; Tunçalp, Ö.; Straus, S. E. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169 (7), 467–473. [CrossRef]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. International Journal of Social Research Methodology 2005, 8 (1), 19–32. [CrossRef]
- Singh, A.; Kamal, R.; Mudiam, M. K. R.; Gupta, M. K.; Satyanarayana, G. N. V.; Bihari, V.; Shukla, N.; Khan, A. H.; Kesavachandran, C. N. Heat and PAHs Emissions in Indoor Kitchen Air and Its Impact on Kidney Dysfunctions among Kitchen Workers in Lucknow, North India. PLoS ONE 2016, 11 (2), e0148641. [CrossRef]
- Saif Eldin, S.; Radwan, A.; Khalifa, M. EVALUATION OF OCCUPATIONAL INDOOR HEAT STRESS IMPACT ON HEALTH AND KIDNEY FUNCTIONS AMONG KITCHEN WORKERS. Egypt. J. Occup. Med. 2022, 46 (3), 93–108. [CrossRef]
- Venugopal, V.; Latha, P. K.; Shanmugam, R. Occupational Heat Exposures and Renal Health Implications-a Cross-Sectional Study among Commercial Kitchen Workers in South India. Occupational and Environmental Medicin 2021, 78 (SUPPL 1), A22.
- Houser, M. C.; Mac, V.; Smith, D. J.; Chicas, R. C.; Xiuhtecutli, N.; Flocks, J. D.; Elon, L.; Tansey, M. G.; Sands, J. M.; McCauley, L.; Hertzberg, V. S. Inflammation-Related Factors Identified as Biomarkers of Dehydration and Subsequent Acute Kidney Injury in Agricultural Workers. Biological Research For Nursing 2021, 23 (4), 676–688. [CrossRef]
- Moyce, S.; Mitchell, D.; Armitage, T.; Tancredi, D.; Joseph, J.; Schenker, M. Heat Strain, Volume Depletion and Kidney Function in California Agricultural Workers. Occup Environ Med 2017, 74 (6), 402–409. [CrossRef]
- Smith, D. J.; Pius, L. M.; Plantinga, L. C.; Thompson, L. M.; Mac, V.; Hertzberg, V. S. Heat Stress and Kidney Function in Farmworkers in the US: A Scoping Review. Journal of Agromedicine 2021, 1–10. [CrossRef]
- Milner, S. Hot Topic Getting Hotter: Employer Heat Injury Liability Mitigation in the Age of Climate Change. ABA Journal of Labor and Employment Law 2022, 36 (1), 177–202.
- Varghese, B. M.; Hansen, A.; Mann, N.; Liu, J.; Zhang, Y.; Driscoll, T. R.; Morgan, G. G.; Dear, K.; Capon, A.; Gourley, M.; Prescott, V.; Dolar, V.; Bi, P. The Burden of Occupational Injury Attributable to High Temperatures in Australia, 2014–19: A Retrospective Observational Study. Medical Journal of Australia 2023, 219 (11), 542–548. [CrossRef]
- Hansson, E.; Glaser, J. R.; Wesseling, C.; Jakobsson, K.; Raines, N. H.; Weiss, I.; Smith, D.; Silva-Peñaherrera, M.; Lucas, R. A. I.; Callejas, P.; Chavarria, D.; Wegman, D. H. Heat-Related Kidney Injury Precedes Estimated GFR Decline in Workers at Risk of CKD. Kidney International Reports 2025, 10 (3), 948–951. [CrossRef]
- NYC Department of Health. Article 81: Food Preparation and Food Establishments. https://www.nyc.gov/assets/doh/downloads/pdf/about/healthcode/health-code-article81.pdf.
- Oregon Health Authority. Food Code Fact Sheet #28; 2019. https://www.oregon.gov/oha/PH/HEALTHYENVIRONMENTS/FOODSAFETY/Documents/FactSheet28EmployeeDrinks.pdf.
- GA Department of Public Health. Georgia Food Service Interpretation Manual; 2025. file:///Users/danielsmith/Downloads/EnvHealthFoodInterpretationManual2025_FINAL.pdf.
- Shi, D. S.; Weaver, V. M.; Hodgson, M. J.; Tustin, A. W. Hospitalised Heat-Related Acute Kidney Injury in Indoor and Outdoor Workers in the USA. Occup Environ Med 2022, 79 (3), 184–191. [CrossRef]
- Cal/OSHA. California Indoor Heat Protections Approved and Go into Effect | California Department of Industrial Relations; 2024–59; 2024. https://www.dir.ca.gov/DIRNews/2024/2024-59.html (accessed 2025-09-27).
- OSHA. Heat - Standards. https://www.osha.gov/heat-exposure/standards (accessed 2025-09-27).
- Cal/OSHA; California. Indoor Heat Illness Prevention. https://www.dir.ca.gov/dosh/heat-illness/indoor.html (accessed 2025-09-27).
Figure 1.
PRISMA Flow Diagram of Included Studies.
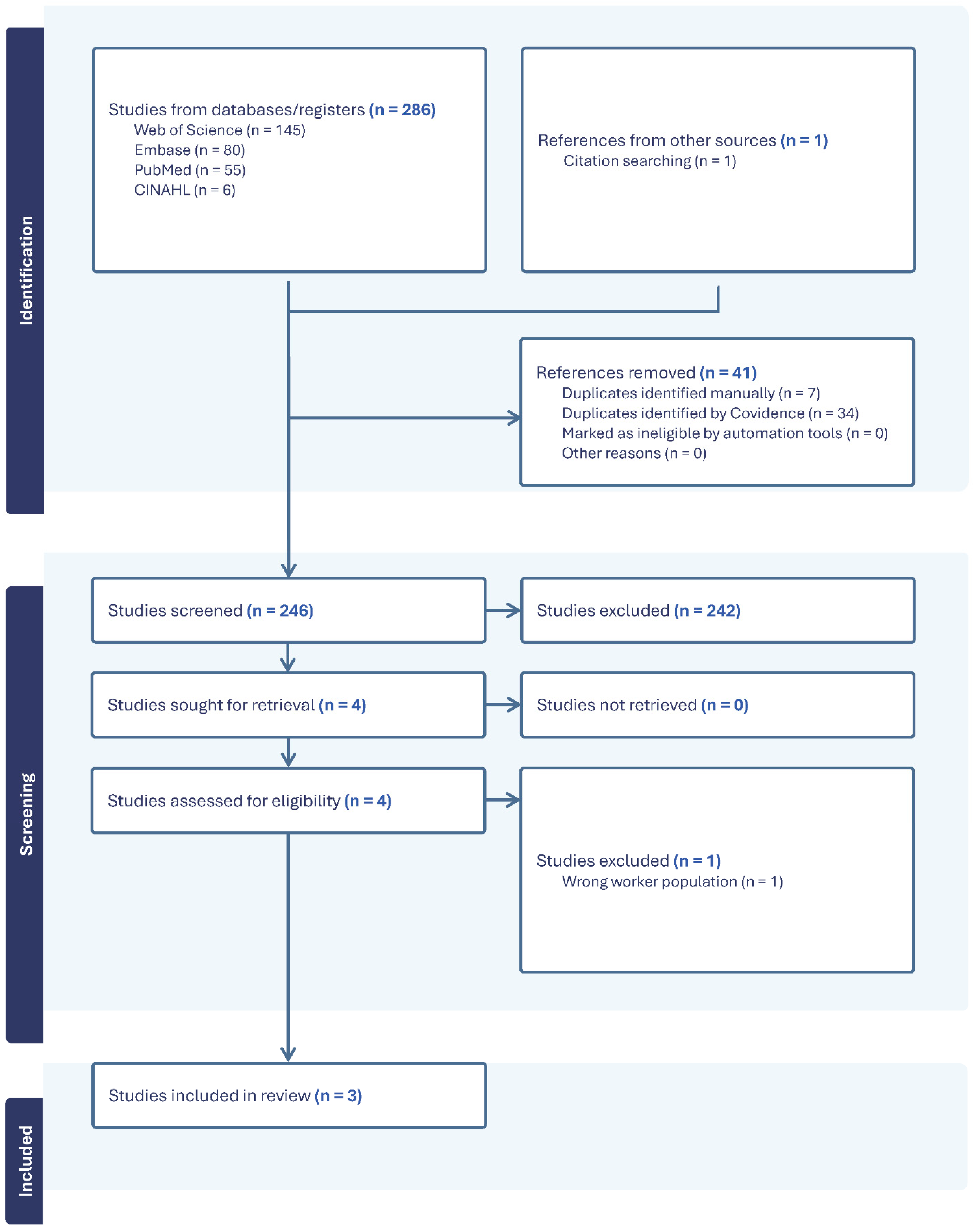

Table 1.
Studies assessing occupational heat exposure and kidney function among kitchen workers.
| Author, Year Location |
Heat Strain Measurements | Season/Timing | Kidney Function Measure | Population (n) | Control Group | Study Design & Aim | Key Findings |
| Singh et al., 2016 Lucknow, India |
Environmental: Heat Index; Humidex (temperature & RH) Physiological: Urine specific gravity |
Winter (Dec 2014) | Urinary albumin–creatinine ratio | n=188 (94 kitchen workers; 94 office/service staff) | Office/service staff | Cross-sectional study of indoor air pollutants, heat, and kidney dysfunction | Kitchen workers had higher urine SG (1.02 vs 1.01), more with elevated ACR (85.1% vs 22.3%), and higher humidex, temperature, and RH than controls. |
| Eldin et al., 2022 Cairo, Egypt |
Environmental: WBGT; Workplace risk factors (ventilation, overcrowding) Physiological: Self-reported heat symptoms |
Spring (Apr–May 2021) | Urinary IL-18 and NGAL | n=87 (40 direct heat-exposed; 47 indirect) | Indirectly exposed workers | Cross-sectional comparative study of hospital kitchens | WBGT exceeded TLV (32.4°C vs 28°C). Directly exposed workers had higher IL-18 and NGAL (p<0.001), more HRI symptoms, and drank less water. |
| Venugopal et al., 2021 South India |
Environmental: WBGT Physiological: Core body temperature, sweat rate, urine specific gravity |
Summer & Winter 2018 | Post-shift serum creatinine → eGFR | n=266 (7 commercial kitchens) | None | Cross-sectional study of heat strain and renal health in kitchens | 66% exceeded WBGT TLV (avg 30.1°C). 82% reported heat strain symptoms. Heat-exposed workers had 2.8× higher risk of reduced eGFR (<90 mL/min/1.73 m²). |
Abbreviations. ACR: Albumin Creatinine Ratio; eGFR: Estimated Glomerular Filtration Rate (mL/min/1.73 m²); HRI: heat related illness; IL-18: Interleukin-18; NGAL: Neutrophil Gelatinase-Associated Lipocalin; RH: relative humidity (percentage); SG: urine specific gravity; TLV: threshold limit value (Celsius); WBGT: wet-bulb globe temperature (Celsius).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



