Submitted:
16 September 2025
Posted:
17 September 2025
You are already at the latest version
Abstract
Chronic pain is a serious concern for the healthcare system, considering the high public expense. Many drugs, such as opioids, non-steroidal anti-inflammatory drugs, amitriptyline, duloxetine, and pregabalin, can be used considering the type of pain (nociceptive, neuropathic, or nociplastic). This is because prescription drugs have a significant negative impact on patient health and the economy, increasing the risk of drug interactions and side effects. Nutraceuticals/supplements may be useful to reduce safety issues, particularly in elderly patients. A new fixed nutraceutical formulation containing lycopene (Solanum lycopersicum), sulforaphane (Brassica oleracea), silymarin (Silybum marianum), reduced glutathione, escin (Aesculus hippocastanum), tryptophan, and green tea (Camellia sinensis) can be used to manage the pain even if its action on pain has not been proved in clinical trials. Nevertheless, the evidence of a strong anti-nociceptive effect by escin and green tea, alongside the antioxidant and anti-neuropathic pain properties of other components, may be useful as adjuvant therapy to reduce drug dosage and prescription. Additionally, patients in polytherapy may benefit from the presence of two hepatoprotective compounds, such as glutathione and silymarin. The aim of this narrative review is to evaluate the data available on both efficacy and safety of the described nutrients in the management of pain.
Keywords:
chronic pain
; nutrients
; antioxidants
; safety
; interactions
1. Introduction
The International Association for the Study of Pain (IASP) defines chronic pain as an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage [1]. Chronic pain has a prevalence of 20% in Western World [2] and it can be classified as nociceptive (tissue or potential tissue damage), neuropathic (disease or injury affecting the nervous system) and nociplastic (in absence of tissue or nerve damage but with persistent activation of the nociceptive system) [3,4]. Drug prescription for chronic pain management is useful for symptom management; in particular: i) opioids modulating opioid receptors μ, κ and δ they are commonly used for both nociceptive and neuropathic pain [5,6,7]; ii) antidepressants (e.g. amitriptyline and duloxetine) increasing serotonin and norepinephrine levels decrease neuropathic pain and improve mood disorders [8,9]; iii) gabapentinoids (e.g. gabapentin and pregabalin) acting on α2δ subunit of voltage gated calcium channels improve neuropathic pain [10,11]. Finally, non-steroidal-anti-inflammatory drugs (NSAIDs) inhibits cyclooxygenases (COX) 1 and 2 enzymes, reducing nociceptive and inflammatory pain. Paracetamol (acetaminophen), an atypical NSAID, has a centrally located mechanism of action on COX shows antinociceptive properties [12,13].
Nevertheless, opioids, antidepressants, anti-epileptics and /or NSAIDs could induce side effects and/or drug interactions, particularly in both elderly and poly-treated patients [4]. Opioids are characterized by tolerance, dependence, abuse and by the insurgence of a high number of side effects including stypsis, and confusion [7,14]. Other central acting drugs including gabapentin, pregabalin, serotonin and norepinephrine reuptake inhibitors (SNRI), amitriptyline determine dizziness and confusion [13,15,16]. Amitriptyline acts on multiple receptors including H1, α1 and M1 receptors causing several side effects including drowsiness, weight gain, hypotension, QT increase, urinary retention [17]. Gabapentin and pregabalin need judicious monitoring of estimated glomerular filtration rate (eGFR) since they are mainly eliminated by kidney [16]. Duloxetine may increase blood pressure and is a major cytochrome (CYP450) 2D6 inhibitor [8]. Drugs like NSAIDs can induce bleeding, gastrointestinal, renal, and cardiovascular side effects, whereas paracetamol liver insufficiency [18,19,20]. In this context, nutraceuticals may strengthen drugs’ action and allow to reduce the dosage of pharmaceuticals [21,22]. Nutraceuticals are derived from plants or foods, generally characterized by adjuvant activity. The term “nutraceutical” describes “a food or part of a food, such as a dietary supplement, that has a medical or health benefit, including the prevention and treatment of disease”. Despite the presence of several substances used as nutraceutical supplement in pain management, including palmitoylethanolamide (PEA), alpha-lipoic acid and acetyl-L-carnitine, in this narrative review, we describe the role of new substances that could be involved in chronic pain management, such as lycopene (Solanum lycopersicum), sulforaphane (SFN, Brassica oleracea), silymarin (Silybum marianum), reduced glutathione, escin (Aesculus hippocastanum), tryptophan and green tea (Camellia sinensis) [23], could be used. Lycopene is a natural pigment of the carotenoid family, easily found in fruits and vegetables, especially tomatoes. It exerts antioxidant, anti-cancer and anti-inflammatory action. Lycopene seems to have several potential benefits in cardiovascular illnesses and cancer. It could be potentially useful in patients with prostatic cancer, benign prostate hyperplasia (BPH), diabetes and obesity [24,25]. Silymarin (Silybum marianum) is a flavonolignan complex. This compound exerts several actions including hepatoprotective, hypocolesterolemic, antioxidant, anti-inflammatory and anticancer properties [26]. Reduced glutathione (GSH) has anti-oxidant and hepatoprotective effects, through the transformation of hydrogen peroxide in water [24,27]. Escin (Aesculus hippocastanum) is used in blunt trauma or venous insufficiency, for its anti-oedema and anti-inflammatory properties. Its action is dependent from triterpene saponins and has glucorticoid-like activity, reducing pain and swelling [28]. Sulforaphane is present in cabbage, broccoli, and Brussels sprouts. It has anti-inflammatory, anti-cancer, and antioxidant effects. Its properties appear to be beneficial for patients with urological comorbidities. The mechanisms of its actions seem to include the inhibition of phase I metabolic enzymes and the arrest of the cell cycle in the G2/M and G1 phases, which contribute to its antioxidant and anticancer effects. [24,29]. Tryptophan is an essential amino acid that the human body cannot produce and must be obtained through diet. This compound offers various potential benefits, including the modulation of mood, sleep, chronic pain, attention, and social functioning. As a precursor to serotonin, tryptophan plays a key role in regulating these functions and the symptoms associated with their pathological disruptions [30].
Green tea, a widely recognized commercial product, exerts its effects through plant polyphenols, with epigallocatechin-3-gallate (EGCG) being the most significant. This extract provides a range of beneficial effects, including antioxidant, cardiovascular, muscular, and anti-cancer properties. Its mechanisms of action are diverse, encompassing the inhibition of mutagenesis, transformation, angiogenesis, genotoxicity, cell proliferation, and more. Multiple targets may be involved in these processes. [31,32].
Despite the presence of several nutraceuticals/supplements available on market, their clinical efficacy is often suboptimal due to low dosage of single components and absence of clinical randomized trials. In this narrative review we aim to outline the pharmacological characteristics of a new fixed combination nutrient and demonstrate how it might be used to treat chronic pain collecting the available evidence for each single component.
2. Referent Scientific Databases
The PubMed, Embase, and Cochrane library databases were searched for articles published until 17 March 2025. Publications found using the primary search's reference lists were included in the secondary search. Before the full-text articles were obtained for eligibility assessment, the records were first filtered by title and abstract. After then, all reference lists were searched for citations in the remaining publications. Papers were deemed eligible if they included any of the words “pain,” “nutraceuticals,” “escin,” “sulforaphane,” “glutathione,” “tryptophan,” “green tea,” “silymarin,” or “lycopene.” All citations were downloaded into Mendeley, and duplicates were deleted. After the initial round of exclusions, the full-text articles were retrieved and subjected to two separate eligibility checks to prevent bias of exclusion. The current review includes the research that was deemed eligible. Manuscripts that lacked complete texts, showed no signs of pain-related effects, or were not in English were excluded.
3. Pharmacological Effects on Pain
3.1. Lycopene (Solanum lycopersicum) and Glutathione
In an experimental model of diabetic neuropathy induced by streptozotocin, Kuhad et al. [33] showed that lycopene reduces hyperalgesia through Tumor Necrosis Factor (TNF)-α and nitric oxide (NO) inhibition. The authors also consider COX 2 inhibition as another possible mechanism of lycopene’s action in this setting. In agreement, Sengupta et al. [34] reported in experimental study that diallylsulfide, lycopene and theaflavin have an antioxidative effects able to reduce colon carcinogenesis. The effect was related to the reduced expression of cyclooxygenase-2 and inducible nitric oxide synthase.
Zhang et al. [35], documented, in experimental models of peripheral nerve injury, that repeated intrathecal lycopene administration improved neuropathic pain. In this model, the increase of TNF-α associated with damage resulted in the downregulation of connexin 43 (Cx43) in astrocytes. This protein plays a role in both gap-junction formation and pain transduction. Lycopene reverts this mechanism, restoring the expression of Cx43. In experimental models, Lu et al. [36] found that lycopene can slow down disc degeneration by changing Nuclear factor (erythroid-derived 2)-like-2 factor (Nrf2) and lowering oxidative stress. Additionally, this compound decreases damage to the extracellular cartilage matrix of nucleus pulposus cells. These findings could have positive implications for the management of both cervical pain and low-back pain.
Moreover, Yin et al. [37], in an experimental model of burn injury, observed the increase of mechanical pain threshold in the dorsal horn after lycopene administration. These authors documented, in the lycopene-treated group, an increased expression of mammalian target of rapamycin (mTOR), glial fibrillary acidic protein (GFAP), p4EBP, ionized calcium-binding adapter molecule (Iba) 1 decreased and sirtuin (SIRT) 1. Shen et al. [38], reviewing data from experimental models of neuropathic pain in the literature, found that lycopene decreased cold and heat hyperalgesia and increased GSH, superoxide dismutase (SOD), and catalase (CAT). In an animal model, Goel et al [39] showed that lycopene reduces both cold and thermal hyperalgesia, oxidative stress and neurological damage including demyelination and swelling. In agreement, Hu et al. [40], reported that lycopene administration in animal model of neuropathic pain, enhances limb motility, most likely via lowering oxidative stress and cell-apoptosis.
Additionally, lycopene has a neuroprotective effect on microglia in experimental settings as shown by Hsiao et al. [41]. These authors, analyzing the effect of lycopene in microglia cell culture stimulated by lipopolysaccharide, showed a neuroprotective effect. The authors highlighted the importance of dietary lycopene, which they believe to be the most powerful antioxidant on the market, in nutraceuticals.
Despite the absence of dedicated papers on reduced glutathione and pain, a significant role of autophagy impairment/modulation and oxidative stress has been described in experimental models of neuropathic pain [42]. Therefore, we can suppose that the administration of glutathione may be useful to eventually contrast pain related to oxidative stress (see also the Lycopene section).
3.2. Silymarin (Silybum marianum)
Only a few data about silymarin's specific action in pain have been published.
Hassani et al. [43], showed in experimental models that intraperitoneal silymarin prevents formalin-induced nociception, through the inhibition of prostaglandin E2 (PGE2), leukotrienes, NO, interleukin (IL) 1-β and TNF-α. Silymarin is also a scavenger, and this may account for its beneficial properties. In contrast the authors documented that silymarin has not effect in experimental models of nerve injury (neuropathic pain).
Zugravu et al. [44] in a double-arm study with 122 rheumatoid arthritis patients, evaluated the antinociceptive and anti-inflammatory effects of silymarin as an add-on treatment to conventional disease-modifying antirheumatic drugs. The oral administration of silymarin improved patients’ clinical conditions in terms of morning stiffness, pain (both intensity and duration), disease activity, the number of tender and sensitive joints, functional status, and mood. On the other hand, there was no discernible improvement in inflammatory markers. In a clinical study, in patients with Rheumatoid Arthritis, Elahi et al., documented that a three-month treatment with silymarin (3 doses of 140 mg/day) induces a decrease on high-sensitivity C-reactive protein levels suggesting that Silymarin could be used as an adjuvant in the treatment of rheumatoid arthritis [45].
3.3. Escin (Aesculus hippocastanum)
Escin exerts its antinociceptive actions through different mechanisms: 1) Increase of glucocorticoid receptor (GR) expression, with glucocorticoid-like activity; 2) inhibition of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and hyaluronidase, which explains the anti-inflammatory and anti-edema activity; 3) inhibition of the bradykinin pathway [28,46]; protection of the endothelium from hypoxic damage through reactive oxygen species (ROS) reduction, platelet endothelial cell adhesion molecule-1 (PECAM-1) expression modulation, phospholipase A2 expression, leukotriene B4, and neutrophil adhesiveness decrease [28,46,47].
Several studies on nociceptive pain (and particularly blunt trauma) have been published [46,47,48,49]. Wetzel et al. [50] analyzing the effect of escin-containing gel (1% or 2%) in 158 patients with sport trauma, documented that escin gel produced faster tenderness and pain reduction.
Despite escin’s principal effect in nociceptive pain, Zhang et al. [51], investigated its efficacy in an experimental model of neuropathic pain induced by chronic constriction injury (CCI) of the sciatic nerve. In this study, the administration of escin for 14 days resulted in neuropathic pain improvement through the increasing of thermal threshold, the downregulation of TNF and IL1ß, toll-like receptor 4 (TLR4), NF-κB, glial fibrillary acidic protein (GFAP), and nerve growth factor (NGF).
3.4. Tryptophan
The tryptophan pathway and metabolites play a role in pain modulation [52]. In particular, damage and potential harms on the tryptophan-kynurenine pathway are co-players in chronic pain insurgence and persistence, particularly in nociplastic pain [52]. Despite this observation, norepinephrine, but not serotonin (of which tryptophan is a precursor), is involved in pain improvement. Therefore, SNRI and not selective serotonin reuptake inhibitors (SSRI), are used in the treatment of neuropathic pain. However, some guidelines suggest using SSRIs to modulate behavioural symptoms in patients with fibromyalgia [4,53,54]. King [55], in five patients managed with oral tryptophan, observed an improvement in pain symptoms and sensory deficits following rhizotomy and cordotomy. Schweiger et al., [56] reported that a nutraceutical containing tryptophan plus vitamin D, coenzyme Q10, alpha-lipoic acid, and magnesium, showed a statistically significant pain improvement in patients with fibromyalgia, 1 and 3 months after the beginning of the treatment.
3.5. Green Tea (Camellia sinensis)
Green tea has anti-inflammatory, anti-nociceptive, and antioxidant effects. Epigallocatechin-3-gallate (EGCG), the main component of green tea, provides nociceptive pain-relieving properties by inhibiting the expression of genes that generate inflammatory cytokines. According to preclinical studies, green tea is clinically effective in alleviating nociceptive pain, especially that which is brought on by rheumatoid arthritis and osteoarthritis [57].
In a double-blind, placebo-controlled, randomized clinical trial, Eshghpour et al. [58] found that green tea lowers the mean VAS value and the amount of analgesics used after surgery in 44 patients who had third molar surgery, without any adverse effects.
In an open-label randomized clinical trial, 50 knee osteoarthritis patients were randomly assigned to receive diclofenac tablets alone or diclofenac plus green tea tablets [42]. In comparison to the diclofenac alone group, individuals treated with diclofenac + green tea shown statistically significant improvements in Visual Analogue Scale (VAS) pain, total Western Ontario and McMaster Universities (WOMAC), and WOMAC physical function. Gastrointestinal side effects were observed by just one subject. Inflammatory cytokines were successfully decreased by epigallocatechin-3. Weight loss associated with green tea could be another potential (although small) advantage.
Additionally, green tea extracts are quite effective topically for nociceptive pain, particularly when combined with other therapies. We showed that the combination of high-intensity pulsed magnetic fields (PEMFs) and a topical cream containing devil’s claw, green tea, and arnica effectively reduced low back pain [57]. PEMFs may vehiculate this compound deeply, leading to increased therapeutic efficacy. In this study, the treatment induced a statistically significant decrease of NRS (from 7.59 ± 2.49 to 1.90 ± 2.26).
Numerous experimental research have been carried out in neuropathic pain models in addition to its well-known effectiveness in nociceptive pain. Neuronal nitric oxide synthases (nNOS)/NO, chemokine (C-X3-C motif) ligand 1 (CX3CL1), Janus kinase (JNK), NF-κB, and TNF-α are the primary targets that epigallocatechin-3 modulates in experimental models. The reduction of CX3CL1,52, which affects the microglia-neuron networking, decreased thermal hyperalgesia, suggesting that epigallocatechin-3 acting on nNOS/NO lessens allodynia. Lastly, hyperalgesia and pain perception are effectively reduced by the action of epigallocatechin-3 on JNK and NF-κB. [59].
3.6. Sulforaphane (Brassica oleracea)
The anti-inflammatory and antioxidant effects of SFN have been observed in experimental models. Among the most important targets Nrf 2, IL-1β, TNFα, and calcitonin gene-related peptide (CGRP) have been described [60].
In an animal model of chronic constriction injury (CCI)-induced neuropathic pain, Wang and Wang [61] found that intraperitoneal SFN reduced inflammatory cytokines and decreased pain and allodynia in a dose-dependent way. The administration of naloxone reduced the effects of SFN on behavioral sensitivity without altering the levels of inflammatory cytokines. The authors found that administering SFN enhanced the expression of μ-opioid receptors, most likely due to a selective effect on neurons rather than immune cells. Similar outcomes regarding the reduction of inflammatory modulators were seen in other neuropathic pain models, such as diabetic neuropathy [62,63]. In agreement, Redondo and colleagues [64] reported that the administration of SFN (5 and 10 mg/kg) reduced inflammatory pain and improved the analgesic effects of morphine by preventing oxidative stress and inflammatory reactions brought on by peripheral inflammation. This suggests that SFN, both by itself and in combination with morphine, may be a novel treatment option for chronic inflammatory pain.
Lucarini et al. [65] provide further insights on SFN’s action in neuropathic pain induced by oxaliplatin. They showed, in a preclinical study, an involvement of hydrogen sulfide (H₂S) release and the modulation of potassium Kv7 channels by isothiocyanates. Therefore, the neuroprotective effects of SFN as well as its effects on neuropathic pain could be related to the decrease of reactive oxygen species (ROS) and inflammation as well as to the activation of potassium channels induced by H₂S.
The authors showed in a preclinical investigation that isothiocyanates cause the emission of hydrogen sulfide and modulate potassium Kv7 channels. Therefore, the effects of SFN in neuropathic pain modulation may be associated with the activation of potassium channels and the reduction of ROS and inflammation.
Guadarrama-Enríquez et al. [66] evaluated the effects of intraperitoneal SFN in an experimental model of edema and nociceptive pain. Antinociceptive effects were evaluated with the plantar test. The compound showed central and peripheral action, and its efficacy was comparable to NSAIDs or opioids (i.e., tramadol, ketorolac, and indomethacin). The authors report that SFN works similarly to one of the most potent NSAIDs, ketorolac, by inhibiting COX-2, the nucleotide-binding domain, the leucine-rich-containing family, pyrin domain-containing (NLRP) 3, IL-6, IL-1β, NF-κB, and maybe other inflammatory cascade targets. It is noteworthy that variations in myrosinase activity, an enzyme triggered by simple chopping or chewing, are responsible for variations in SFN bioavailability among various human Brassica oleraceae varieties.
Finally, Lu et al. [67] highlighted the action of SFN in delaying intervertebral disc degeneration through the activation of Nrf-2. Sulforaphane, increasing Nrf2 entry in the nucleus, determined the increase of heme oxygenase-1 (HO-1) and therefore an increased clearance of ROS. Sulforaphane increases Nrf-2 transcription, decreasing the methylation of the initial 15 CPGs of the Nrf-2 promoter. Another SFN mechanism of action is the prevention of Kelch-like ECH-associated protein 1 (Keap1) binding with Nrf-2 (chemical modification of cysteine residues (mainly cys151) of Keap1. This leads to a reduced ubiquitination/degradation of Nrf-2, with an increase of its beneficial effect.
4. Discussion
Pain is a complex and subjective symptom, strictly imbricated with lifestyle and behavioral impairment. Its pathogenesis is various and not completely known, involving several mechanisms including inflammation, damage to nervous system and persistent sensitization [3,70,71]. Multiple treatments are available to manage this clinical condition [4,53,72,73].
In this context, the role of nutraceuticals appears to be very useful to reduce drugs prescription. The global nutraceuticals market size was valued at USD 712.97 billion in 2023 [74]. Patients are constantly pursuing therapeutic options that are safe, due to the increasing diffidence to drug prescription and consumption and the high number of drugs consumed, especially by the elderly. [75,76]. We describe a new possible nutraceutical association in pain treatment. Nevertheless, the nutraceuticals/supplement that are more commonly used in this clinical setting are different. Palmitoylethanolamide is an endogenous fatty acid amide, and lipid modulator. It enhances the effects of endocannabinoids or phytocannabinoids acting on peroxisome proliferator-activated receptor (PPAR-α), transient receptor potential vanilloid type 1 (TRPV1, allosteric modulation), G protein-coupled receptor 55 (GPR55), and cannabinoid receptors. Furthermore, it mitigates the activity of inflammatory enzymes and inhibits mast cell degranulation [77].
Acetyl-l-carnitine is a neuroprotective and neurotrophic molecule, particularly effective in neuropathic pain [78,79]. It is both a drug and a nutraceutical depending on the dosages. This endogenous substance modulates pain through different actions: antioxidant activity, an increase of mitochondrial function and repair factors such as nerve growth factor (NGF), activation of metabotropic glutamate receptor 2 (mGlu2) and of NF-kB and increasing the expression of mGlu2.
Alpha-lipoic acid is a substance found in red meats, vegetables, and potatoes. It has antioxidant effects, neuroprotective effects through the Protein kinase B (PKB) pathway, and NF-kB inhibitory activity [80,81].
All these compounds show good clinical efficacy in pain modulation [79,81,82] with an excellent safety profile. Nevertheless, the available combination of nutraceuticals created by pharmaceutical industries is numerous, and no head-to-head comparison of these products exists.
To prescribe the appropriate nutraceutical in certain clinical circumstances, it may be very helpful to undertake clinical research comparing the effectiveness of various chemicals in nociceptive, nociplastic, and neuropathic pain. Similarly, a good therapeutic pharmacological approach is not possible in the absence of high-quality human pharmacokinetics investigations. Since nutraceuticals are subject to less stringent regulations than pharmaceuticals, they frequently lack evidence on pharmacokinetics and efficacy in real-world settings, despite having generally acceptable safety standards. Actually, only safety evaluations are often needed by the European Food Safety Authority (EFSA) and other international organizations. The bioavailability, half-life, and other pharmacokinetic properties of the same chemical may vary depending on the nutraceutical formulation. Additionally, a number of nutraceuticals are derived from plants that typically include many components, making it difficult to isolate the active ingredient. [83,84].
Due to its antioxidant, anti-inflammatory, and neuroprotective properties as well as its hepatoprotective effects, a new formulation that contains silymarin, green tea, tryptophan, escin, lycopene, SFN, and reduced glutathione may present an opportunity for patients who have received multiple treatments [26,27]. Furthermore, tryptophan offers an advantage in modulating mood and sleep, giving patients a complete range of clinical benefits [24]. The presence of substances of well-known clinical efficacy like escin, green tea and silymarin renders this co-formulation reliable.
The compounds show synergistic anti-inflammatory and antioxidant effects, potentially acting both on innate and humoral immune response, and reducing apoptosis [31,47,85]. These compounds may together increase the effect of other drugs used in pain management, allowing to a dosage reduction. For example, SFN increasing the μ opioid receptor expression [66], could reduce the drug tolerance that is one of the main concerns related to opioid prescription [86]. Nevertheless, these and other effects must still be demonstrated with more solid evidence in clinical studies.
Although there is considerable clinical support for treating nociceptive pain, there is little information on how well it works for neuropathic pain, despite this being rationally demonstrated [38]. An ideal option is a multimodal treatment that incorporates non-pharmacological, nutraceutical, and pharmaceutical techniques [57,87,88]. The compound may be useful in nociplastic and neuropathic pain also considering the role of lycopene in modulating microglia [41,89,90,91]. Considering these findings, it is logical that if the most of the preclinical data will be validated in clinical trials, this novel nutraceutical could end up becoming a substance utilized as an adjuvant for all forms of pain.
We decided to investigate the combination of these molecules because 1) no other such association is already on the market; 2) the effects of the included compounds are synergistic and may cover all types of pain; and 3) a high level of safety is expected.
Notwithstanding the excitement around the realization of its potential, more work must be done to enhance this compound's function in pain relief. Besides, clinical trials for nociceptive, neuropathic, and nociplastic pain must demonstrate the effectiveness of the nutraceutical combination. This narrative review proofs that a nutraceutical containing SFN, green tea, glutathione, escin, lycopene, silymarin and tryptophan may be useful as adjuvant for pain management, considering the synergic action of its compounds. Furthermore, the hepatoprotective action of silymarin and glutathione helps to prevent liver injury.
However, after everything exposed, one question still remains and that is:
What about the safety of herbal medicinal products and active substances?
The safety of medicinal plants is a crucial topic in pharmacy, as many people worldwide use herbal remedies either as alternatives to or in conjunction with conventional medicines. While medicinal plants can offer therapeutic benefits, their safety depends on several factors. Namely, therapeutic benefits of some medicinal plants depend on their toxicity, adulteration with incorrect species or synthetic drugs [92], interaction with prescribed medications [93], and even contamination with heavy metals, pesticides, or microbes due to poor cultivation/processing practices [94]. Thus, there are different regulatory aspects to avoid or to minimize the potential health hazards. For instance, since 2007 WHO provides comprehensive guidelines for herbal medicines covering various aspects, including quality control, Good Manufacturing Practices (GMP), Good Agricultural and Collection Practices (GACP), safety monitoring, and regulation and registration to ensure the safety, efficacy, and quality of herbal products [95]. Also, the United States Food and Drugs Administration classifies most herbal products as dietary supplements, which means they are subject to limited regulation compared to prescription drugs, according to US federal law [96]. Nevertheless, it seems that the best regulations on herbal substances and preparations, which gives companies a clear reference point to for successful development of and application of herbal medicinal product(s) are established in European Union. Namely, in the Directive 2001/83/EC of the European Parliament and of The Council on the Community code relating to medicinal products for human use [97] is giving complete definitions of terms and all procedures about assessment, placing on the market and analyzing the herbal medicinal products. The roof committee responsible for giving the scientific opinions on herbal substances and preparations on behalf of the European Medicines Agency (EMA) is the Committee on Herbal Medicinal Products (HMPC) [98]. In spite of some complains and/or at least, not affirmative opinions of some producers of herbal medicinal products, there is a quite order in EU about bringing herbal medicinal products to market within the EU and, about establishing EU standards for national procedures. Moreover, in the Directive 2001/83/EC of the European Parliament and of The Council on the Community code relating to medicinal products for human use, all pathways and procedures about registration of certain herbal medicinal product whether for traditional use, or its stand alone or mixed application are completely defined and explained and also there is a List of the national competent authorities on the European Economic Area in charge for food, medicinal and health products [99]. It is also important to point out that on the initiative and under organization of the Global Coalition for Regulatory Science Research (GCRSR) the Global Summit on Regulatory Sciences that took place in Beijing on September 2018 (GSRS2018) [100], the participants of the summit agree that establishing transparent analytical approaches and data analytics methods plays a crucial role in future developing and evaluating the technologies for assessment of natural supplements and medicines.
5. Conclusions
Pain is a complex, multifactorial condition that often requires a multimodal therapeutic approach. In this context, nutraceuticals represent a promising adjunct to conventional pharmacological treatments, particularly given their favorable safety profiles and potential to target various pain mechanisms, including nociceptive, neuropathic, and nociplastic pathways. The compounds discussed—such as palmitoylethanolamide, acetyl-L-carnitine, alpha-lipoic acid, silymarin, green tea extract, tryptophan, escin, lycopene, sulforaphane, and glutathione—exhibit synergistic antioxidant, anti-inflammatory, neuroprotective, and hepatoprotective properties, suggesting that their combined use may enhance therapeutic efficacy while reducing reliance on conventional drugs.
Despite encouraging preclinical and limited clinical data, robust evidence from well-designed human trials is still lacking. Furthermore, the variability in nutraceutical formulations, bioavailability, and pharmacokinetics underscores the need for stringent quality control and regulatory oversight. The regulatory frameworks established in the European Union, particularly under Directive 2001/83/EC, offer a comprehensive model for the safe development and evaluation of herbal medicinal products. However, global harmonization and improved methodological standards in clinical research are imperative to fully establish the efficacy, safety, and therapeutic role of these compounds in pain management. If future clinical trials substantiate the promising preclinical findings, the proposed nutraceutical combination could serve as a valuable adjuvant in the comprehensive management of pain across diverse patient populations.
6. Patents
IT202300005970A1 Drolessano: Preparato energizzante, antiossidante e detossificante ad uso orale a base di licopene Broccoli, Cardo mariano, glutatione ridotto, ippocastano, teina e triptofano
Author Contributions
According to Contributor Roles Taxonomy (CRediT) all the authors contributed equally in all aspects of conceptualization, writing and review and editing the manuscript. The authors have taken full responsibility for the content of this publication.
Funding
This work received no external funding.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
This work is a part of overall investigations within the BFC Interreg IPA ADRION project.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- IASP International Association for the Study of Pain -Terminology. Available online: https://www.iasp-pain.org/resources/terminology/ (accessed on Jun 18, 2023).
- IASP High Impact Chronic Pain- International Association for the Study of Pain. Available online: https://www.iasp-pain.org/resources/fact-sheets/high-impact-chronic-pain/#:~:text=Chronic pain is a major,than three months %5B2%5D. (accessed on Dec 9, 2024).
- Cohen, S.P.; Vase, L.; Hooten, W.M. Series Chronic Pain 1 Chronic pain : an update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Marcianò, G.; Vocca, C.; Evangelista, M.; Palleria, C.; Muraca, L.; Galati, C.; Monea, F.; Sportiello, L.; De Sarro, G.; Capuano, A.; et al. The Pharmacological Treatment of Chronic Pain: From Guidelines to Daily Clinical Practice. Pharmaceutics 2023, 15, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Arif, A.W.; Bhan, C.; Kumar, D.; Malik, M.B.; Sayyed, Z.; Akhtar, K.H.; Ahmad, M.Q. Managing Chronic Pain in the Elderly: An Overview of the Recent Therapeutic Advancements. Cureus 2018, 10, 1.10. [Google Scholar] [CrossRef] [PubMed]
- Corder, G.; Castro, D.C.; Bruchas, M.R.; Scherrer, G. Endogenous and exogenous opioids in pain. Annu. Rev. Neurosci. 2018, 41, 453–473. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.O.; Christie, R.; Harris, E.; Penning, J.; Mcvicar, J. Tramadol and Tapentadol: Clinical and Pharmacologic Review. Available online: https://resources.wfsahq.org/atotw/tramadol-and-tapentadol-clinical-and-pharmacologic-review/ (accessed on Jul 24, 2022).
- Knadler, M.P.; Lobo, E.; Chappell, J.; Bergstrom, R. Duloxetine: Clinical pharmacokinetics and drug interactions. Clin. Pharmacokinet. 2011, 50, 281–294. [Google Scholar] [CrossRef]
- Birkinshaw, H.; Friedrich, C.M.; Cole, P.; Eccleston, C.; Serfaty, M.; Stewart, G.; White, S.; Moore, R.A.; Phillippo, D.; Pincus, T. Antidepressants for pain management in adults with chronic pain: a network meta-analysis. Cochrane Database Syst. Rev. 2023, 2023, CD014682. [Google Scholar] [CrossRef]
- Urits, I.; Li, N.; Berardino, K.; Artounian, K.A.; Bandi, P.; Jung, J.W.; Kaye, R.J.; Manchikanti, L.; Kaye, A.M.; Simopoulos, T.; et al. The use of antineuropathic medications for the treatment of chronic pain. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 493–506. [Google Scholar] [CrossRef]
- O’Connor, A.B.; Dworkin, R.H. Treatment of Neuropathic Pain: An Overview of Recent Guidelines. Am. J. Med. 2009, 122, S22–S32. [Google Scholar] [CrossRef]
- Koes, B.W.; Backes, D.; Bindels, P.J.E. Expert Opinion on Pharmacotherapy Pharmacotherapy for chronic non-specific low back pain : current and future options Pharmacotherapy for chronic non-specific low back pain : current and future options. Expert Opin. Pharmacother. 2018, 19, 537–545. [Google Scholar] [CrossRef]
- McDonagh, Marian S. Selph, S.S.; Buckley, D.I.; Holmes, Rebecca S. Mauer, K.; Ramirez, S.; Hsu, F.C.; Dana, T.; Fu, R.; Chou, R. Nonopioid Pharmacologic Treatments for Chronic Pain; Agency for Healthcare Research and Quality: Rockville (USA), 2020. [Google Scholar]
- Benyamin, R.; Trescot, A.M.; Datta, S.; Buenaventura, R.; Adlaka, R.; Sehgal, N.; Glaser, S.E.; Vallejo, R. Opioid complications and side effects. Pain Physician 2008, 11, 105–120. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpaa, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: Systematic review, meta-analysis and updated NeuPSig recommendations. Lancet Neurol 2015, 14, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Asconapé, J.J. Use of antiepileptic drugs in hepatic and renal disease. In Handbook of Clinical Neurology; 2014. [Google Scholar]
- Thour, A.; Marwaha, R. Amitriptyline. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537225/ (accessed on Jul 25, 2022).
- Bjarnason, I. Gastrointestinal safety of NSAIDs and over-the-counter analgesics. Int. J. Clin. Pract. 2013, 67, 37–42. [Google Scholar] [CrossRef]
- Moore, N.; Pollack, C.; Butkerait, P. Adverse drug reactions and drug–drug interactions with over-the-counter NSAIDs. Ther. Clin. Risk Manag. 2015, 11, 1061–1075. [Google Scholar] [CrossRef]
- Marcianò, G.; Muraca, L.; Rania, V.; Gallelli, L. Ibuprofen in the Management of Viral Infections: The Lesson of COVID-19 for Its Use in a Clinical Setting. J. Clin. Pharmacol. 2023, 63, 975–992. [Google Scholar] [CrossRef] [PubMed]
- Aronson, J.K. Defining ‘nutraceuticals’: neither nutritious nor pharmaceutical. Br. J. Clin. Pharmacol. 2017, 83, 8–19. [Google Scholar] [CrossRef]
- Chiarella, G.; Marcianò, G.; Viola, P.; Palleria, C.; Pisani, D.; Rania, V.; Casarella, A.; Astorina, A.; Scarpa, A.; Esposito, M.; et al. Nutraceuticals for Peripheral Vestibular Pathology: Properties, Usefulness, Future Perspectives and Medico-Legal Aspects. Nutrients 2021, 13, 3646. [Google Scholar] [CrossRef]
- SIA Drolessano- Società Italiana di Andrologia. Available online: https://www.siabc.it/drolessano (accessed on Dec 9, 2024).
- Sebastiani, F.; Alterio, C.D.; Vocca, C.; Gallelli, L.; Palumbo, F.; Cai, T.; Palmieri, A. Effectiveness of Silymarin, Sulforaphane, Lycopene, Green Tea, Tryptophan, Glutathione, and Escin on Human Health : A Narrative Review. Uro 2023, 3, 208–228. [Google Scholar] [CrossRef]
- Zhu, R.; Chen, B.; Bai, Y.; Miao, T.; Rui, L.; Zhang, H.; Xia, B.; Li, Y.; Gao, S.; Wang, X.; et al. Lycopene in protection against obesity and diabetes: a mechanistic review. Pharmacol Res 2020, 159, 104966. [Google Scholar] [CrossRef]
- Mancak, M.; Altintas, D.; Balaban, Y.; Caliskan, U.K. Evidence-based herbal treatments in liver diseases. Hepatol Forum 2024, 5, 50–60. [Google Scholar] [CrossRef]
- Forman, H.J.; Zhang, H.; Rinna, A. Glutathione: overview of its protective roles, measurement, and biosynthesis. Mol Asp. Med 2010, 30, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Marcianò, G.; Vocca, C.; Dıraçoglu, D.; Özda, R.; Gallelli, L. Escin’ s Action on Bradykinin Pathway : Advantageous Clinical Properties for an Unknown Mechanism ? Antioxidants (Basel) 2024, 13, 1130. [Google Scholar] [CrossRef]
- Kamal, M.M.; Akter, S.; Lin, C.-N.; Nazzal, S. Sulforaphane as an anticancer molecule : mechanisms of action, synergistic effects, enhancement of drug safety, and delivery systems. Arch. Pharm. Res. 2020, 43, 371–384. [Google Scholar] [CrossRef]
- Davidson, M.; Rashidi, N.; Nurgali, K.; Apostolopoulos, V. The Role of Tryptophan Metabolites in Neuropsychiatric Disorders. Int J Mol Sci. 2022 Sep 1; 2022, 23, 9968. [Google Scholar] [CrossRef]
- Dou, Q. Molecular mechanisms of green tea polyphenols. Nutr Cancer 2009, 61, 827–835. [Google Scholar] [CrossRef]
- Chaudhary, P.; Mitra, D.; Das, P.K.; Oana, A.; Mon, E.; Janmeda, P.; Martorell, M.; Iriti, M.; Ibrayeva, M.; Sharifi-rad, J.; et al. Camellia sinensis : Insights on its molecular mechanisms of action towards nutraceutical, anticancer potential and other therapeutic applications. Arab. J. Chem. 2023, 16, 104680. [Google Scholar] [CrossRef]
- Kuhad, A.; Sharma, S.; Chopra, K. Lycopene attenuates thermal hyperalgesia in a diabetic mouse model of neuropathic pain. Eur J Pain. 2008 Jul;12(5)624-3 2008, 12, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, A.; Ghosh, S.; Das, R.K.; Bhattacharjee, S.; Bhattacharya, S. Chemopreventive potential of diallylsulfide, lycopene and theaflavin during chemically induced colon carcinogenesis in rat colon through modulation of cyclooxygenase-2 and inducible nitric oxide synthase pathways. Eur J Cancer Prev 2006, 15, 301–5. [Google Scholar] [CrossRef]
- Zhang, F.F.; Morioka, N.; Kitamura, T.; Fujii, S.; Miyauchi, K.; Nakamura, Y.; Hisaoka-nakashima, K.; Nakata, Y. Lycopene ameliorates neuropathic pain by upregulating spinal astrocytic connexin 43 expression. Life Sci. 2016, 155, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Zhou, L.; He, S.; Ren, H.; Zhou, N.; Hu, Z. Lycopene alleviates disc degeneration under oxidative stress through the Nrf2 signaling pathway. Mol. Cell. Probes 2020, 51, 101559. [Google Scholar] [CrossRef] [PubMed]
- Yin, Q.; Wang, J.; Xu, X.; Xie, H. Effect of lycopene on pain facilitation and the SIRT1 / mTOR pathway in the dorsal horn of burn injury rats. Eur. J. Pharmacol. 2020, 889, 173365. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Castro, L.; Fang, C.; Castro, M.; Sherali, S.; White, S.; Wang, R.; Neugebauer, V. Bioactive compounds for neuropathic pain : An update on preclinical studies and future perspectives. J. Nutr. Biochem. 2022, 104, 108979. [Google Scholar] [CrossRef]
- Goel, R.; Tyagi, N. Potential Contribution of Antioxidant Mechanism in the Defensive Effect of Lycopene Against Partial Sciatic Nerve Ligation Induced Behavioral, Biochemical and Histopathological Modification in Wistar Rats. Drug Res. (Stuttg). 2016, 66, 633–638. [Google Scholar] [CrossRef]
- Hu, W.; Wang, H.; Liu, Z.; Liu, Y.; Wang, R.; Luo, X.; Huang, Y. Neuroprotective effects of lycopene in spinal cord injury in rats via antioxidative and anti-apoptotic pathway. Neurosci Lett 2017, 642, 07–112. [Google Scholar] [CrossRef]
- Hsiao, G.; Fong, T.H.; Tzu, N.H.; Lin, K.H.; Chou, D.S.; Sheu, J.R. A Potent Antioxidant, Lycopene, Affords Neuroprotection Against Microglia Activation and Focal Cerebral Ischemia in Rats. In Vivo (Brooklyn). 2004, 356, 351–356. [Google Scholar]
- Li, J.; Tian, M.; Hua, T.; Wang, H.; Yang, M.; Li, W.; Zhang, X.; Yuan, H. Combination of autophagy and NFE2L2 / NRF2 activation as a treatment approach for neuropathic pain. Autophagy 2021, 17, 4062–4082. [Google Scholar] [CrossRef]
- Hassani, F.V.; Rezaee, R.; Sazegara, H.; Hashemzaei, M.; Karimi, G. Effects of silymarin on neuropathic pain and formalin - induced nociception in mice. Iran J Basic Med Sci 2015, 18, 715–20. [Google Scholar]
- Zugravu, G.S.; Pintilescu, C.; Cumpat, C.; Miron, S.D.; Miron, A. Silymarin Supplementation in Active Rheumatoid Arthritis : Outcomes of a Pilot Randomized Controlled Clinical Study. Med. 2024, 60, 999. [Google Scholar] [CrossRef]
- Elahi, M.E.; Elieh-Ali-Komi, D.; Goudarzi, F.; Mohammadi-Noori, E.; Assar, S.; Shavandi, M.; Kiani, A.; Elahi, H. Effects of silymarin as adjuvant drug on serum levels of CTRP3, anti-cyclic citrullinated peptide (CCP), and high-sensitivity C-reactive protein (hs-CRP) in rheumatoid arthritis patients. Mol. Biol. Res. Commun. 2024, 13, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Gallelli, L. Escin: A review of its anti-edematous, antiinflammatory, and venotonic properties. Drug Des. Devel. Ther. 2019, 13, 3425–3437. [Google Scholar] [CrossRef] [PubMed]
- Gallelli, L.; Cione, E.; Wang, T.; Zhang, L. Glucocorticoid-Like Activity of Escin : A New Mechanism for an Old Drug. Drug Des Devel Ther 2021, 15, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.-Q.; Xu, S.-Q.; Cheng, J.; Cao, X.-L.; Zhang, Y.; Zhou, W.-P.; Huang, Y.-J.; Wang, J.; Hu, X.-M. Anti-inflammatory effect of external use of escin on cutaneous inflammation: possible involvement of glucocorticoids receptor. Chin. J. Nat. Med. 2018, 16, 105–112. [Google Scholar] [CrossRef]
- Pabst, H.; Segesser, B.; Bulitta, M.; Wetzel, D.; Bertram, S. Efficacy and tolerability of escin/diethylamine salicylate combination gels in patients with blunt injuries of the extremities. Int. J. Sports Med. 2001, 22, 430–436. [Google Scholar] [CrossRef]
- Wetzel, D.; Menke, W.; Dieter, R.; Smasal, V.; Giannetti, B.; Bulitta, M. Escin/diethylammonium salicylate/heparin combination gels for the topical treatment of acute impact injuries: a randomised, double blind, placebo controlled, multicentre study. Br J Sport. Med 2002, 36, 183–188. [Google Scholar] [CrossRef]
- Zhang, L.; Chen, X.; Wu, L.; Li, Y.; Wang, L.; Zhao, X.; Zhao, T.; Zhang, L.; Yan, Z.; Wei, G. Ameliorative effects of escin on neuropathic pain induced by chronic constriction injury of sciatic nerve. J. Ethnopharmacol. 2021, 267, 113503. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Török, N.; Fanni, T.; Szab, Á. Co-Players in Chronic Pain : Neuroinflammation and the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines. 2021, 9, 897. [Google Scholar] [CrossRef] [PubMed]
- Colorado Division of Workers’ Compensation Chronic Pain Disorder Medical Treatment Guideline. 2017; 1–178.
- SIGN Scottish Intercollegiate Guidelines Network- Management of chronic pain. Available online: http://www.sign.ac.uk/pdf/SIGN136.pdf (accessed on Jul 17, 2022).
- King, R.B. Pain and tryptophan. J Neurosurg 1980, 53, 44–52. [Google Scholar] [CrossRef]
- Vittorio, S.; Erica, S.; Cinzia, C.; Alvise, M.; Elena, M.; Alessandro, P.; Enrico, P.; Katia, D.; Teresa, V.M.; Luca, D.C. Comparison between Acupuncture and Nutraceutical Treatment with Migratens ® in Patients with Clinical Trial. Nutr.. 2020, 12, 821. [Google Scholar] [CrossRef]
- Pullano, S.A.; Marcianò, G.; Bianco, M.G.; Oliva, G.; Rania, V.; Vocca, C.; Cione, E.; De Sarro, G.; Gallelli, L.; Romeo, P.; et al. FT-IR Analysis of Structural Changes in Ketoprofen Lysine Salt and KiOil Caused by a Pulsed Magnetic Field. Bioengineering 2022, 9, 503. [Google Scholar] [CrossRef]
- Eshghpour, M.; Mortazavi, H.; Mohammadzadeh Rezaei, N.; Nejat, A. Effectiveness of green tea mouthwash in postoperative pain control following surgical removal of impacted third molars: Double blind randomized clinical trial. DARU, J. Pharm. Sci. 2013, 21, 59. [Google Scholar] [CrossRef] [PubMed]
- Bimonte, S.; Cascella, M.; Schiavone, V.; Mehrabi-Kermani, F.; Cuomo, A. The roles of epigallocatechin-3-gallate in the treatment of neuropathic pain: an update on preclinical in vivo studies and future perspectives. Drug Des Devel Ther 2017, 11, 2737–2742. [Google Scholar] [CrossRef]
- Papini, J.Z.B.; Esteves, B. de A.; Oliveira, V.G. de S.; Abdalla, H.B.; Cereda, C.M.S.; de Araújo, D.R.; Tofoli, G.R. Analgesic Effect of Sulforaphane: A New Application for Poloxamer-Hyaluronic Acid Hydrogels. Gels 2024, 10, 460. [Google Scholar] [CrossRef]
- Wang, C.; Wang, C. Anti-nociceptive and anti-inflammatory actions of sulforaphane in chronic constriction injury-induced neuropathic pain mice. Inflammopharmacology 2017, 25, 99–106. [Google Scholar] [CrossRef]
- Negi, G.; Kumar, A.; Sharma, S.S. Nrf2 and NF- κ B Modulation by Sulforaphane Counteracts Multiple Manifestations of Diabetic Neuropathy in Rats and High Glucose-Induced Changes. Curr Neurovasc Res 2011, 8, 294–304. [Google Scholar] [CrossRef]
- Li, S.; Yang, C.; Fang, X.; Zhan, G.; Huang, N.; Gao, J.; Xu, H.; Orlando, G. Role of Keap1-Nrf2 Signaling in Anhedonia Symptoms in a Rat Model of Chronic Neuropathic Pain : Improvement With Sulforaphane. Front Pharmacol 2018, 9, 887. [Google Scholar] [CrossRef] [PubMed]
- Redondo, A.; Chamorro, P.A.F.; Riego, G.; Leánez, S.; Pol, O. Treatment with Sulforaphane Produces Antinociception and Improves Morphine Effects during Inflammatory Pain in Mice. J Pharmacol Exp Ther 2017, 363, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Lucarini, E.; Testai, L.; Micheli, L.; Trallori, E.; Citi, V.; Martelli, A.; Rosalinda, G.; Renato, D.N.; Vincenzo, I.; Ghelardini, C.; et al. Effect of glucoraphanin and sulforaphane against chemotherapy - induced neuropathic pain : Kv7 potassium channels modulation by H 2 S release in vivo. Phytother Res 2018, 32, 1–9. [Google Scholar] [CrossRef]
- Guadarrama-Enríquez, O.; Moreno-Pérez, G.; González-Trujano, ME Ángeles-López, G.; Ventura-Martínez, R.; Díaz-Reval, I.; Cano-Martínez, A.; Pellicer, F.; Baenas, N.; Moreno, D.; García-Viguera, C.A. and antiedema effects produced in rats by B. oleracea var. italica sprouts involving sulforaphane. I. 2023 D.-3226. doi: Antinociceptive and antiedema effects produced in rats by Brassica oleracea var . italica sprouts involving sulforaphane. Inflammopharmacology 2023, 31, 3217–3226. [CrossRef]
- Lu, X.; Xu, G.; Lin, Z.; Song, J.; Zhang, Y.; Wang, H.; Lu, F.; Xia, X.; Ma, X.; Zou, F.; et al. Sulforaphane Delays Intervertebral Disc Degeneration by Alleviating Endoplasmic Reticulum Stress in Nucleus Pulposus. Oxid Med Cell Longev 2023, 2023, 3626091. [Google Scholar] [CrossRef]
- Küçükkurt, I.; Akbel, E.; Ince, S.; Acaröz, D.A.; Demirel, H.H.; Kan, F. Potential protective effect of escin from Aesculus hippocastanum extract against cyclophosphamide-induced oxidative stress on rat tissues. Toxicol. Res. (Camb). 2022, 11, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wu, Y.; Wang, H.; Li, Z.; Ding, X.; Dou, C.; Hu, L.; Du, G.; Wei, G. Deciphering the Molecular Mechanism of Escin against Neuropathic Pain : A Network Pharmacology Study. Evid Based Complement Altern. Med 2023, 16, 3734861. [Google Scholar] [CrossRef]
- Vincent, T.L.; Miller, R.E. Molecular pathogenesis of OA pain_ Past, present, and future. Osteoarthr. Cartil. 2024, 32, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Mao, J. Neuropathic pain: Mechanisms and their clinical implications. BMJ 2014, 348. [Google Scholar] [CrossRef]
- HCANJ Pain Management Guideline. Available online: https://www.hcanj.org/files/2013/09/Pain-Management-Guidelines-_HCANJ-May-12-final.pdf (accessed on Jul 17, 2022).
- National Institute for Health and Care Excellence (NICE) Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain. NICE Guidel. 2021.
- GVR Nutraceuticals Market Size & Trends-Grand View Research. Available online: https://www.grandviewresearch.com/industry-analysis/nutraceuticals-market (accessed on Dec 13, 2024).
- Cole, J.A.; Gonçalves-Bradley, D.C.; Alqahtani, M.; Barry, H.E.; Cadogan, C.; Rankin, A.; Patterson, S.M.; Kerse, N.; Cardwell, C.R.; Ryan, C.; et al. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst Rev 2023, 11, CD008165. [Google Scholar] [CrossRef]
- Vocca, C.; Siniscalchi, A.; Rania, V.; Galati, C.; Marcianò, G.; Palleria, C.; Catarisano, L.; Gareri, I.; Leuzzi, M.; Muraca, L.; et al. The Risk of Drug Interactions in Older Primary Care Patients after Hospital Discharge : The Role of Drug Reconciliation. Geriatr. 2023, 8, 1–12. [Google Scholar] [CrossRef]
- Peritore, A.F.; Siracusa, R.; Crupi, R. Therapeutic Efficacy of Palmitoylethanolamide and Its New Formulations in Synergy with Different Antioxidant Molecules Present in Diets. Nutrients 2019, 1–22. [Google Scholar] [CrossRef]
- Onofrj, M.; Ciccocioppo, F.; Varanese, S.; Di Muzio, A.; Calvani, M.; Chiechio, S.; Osio, M.; Thomas, A. Acetyl-L-carnitine: From a biological curiosity to a drug for the peripheral nervous system and beyond. Expert Rev. Neurother. 2013, 13, 925–936. [Google Scholar] [CrossRef]
- Chiechio, S.; Copani, A.; Iv, R.W.G.; Nicoletti, F. Acetyl-L-carnitine in neuropathic pain: experimental data. CNS Drugs. 2007, 21, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Rizzo, M.; Krogager, C.; Kennedy, C.; Georges, C.M.G.; Knežević, T.; Liberopoulos, E.; Vallée, A.; Pérez-Martínez, P.; Wenstedt, E.F.E.; et al. Safety evaluation of α-lipoic acid supplementation: A systematic review and meta-analysis of randomized placebo-controlled clinical studies. Antioxidants 2020, 9, 1–34. [Google Scholar] [CrossRef]
- Tankova, T.; Koev, D.; Dakovska, L. Alpha-lipoic acid in the treatment of autonomic diabetic neuropathy (controlled, randomized, open-label study). Rom J Intern Med 2004, 42, 457–64. [Google Scholar] [PubMed]
- Artukoglu, B.B.; Beyer, C.; Zuloff-Shani, A.; Brener, E.; Bloch, M.H. Efficacy of palmitoylethanolamide for pain: A meta-analysis. Pain Physician 2017, 20, 353–362. [Google Scholar]
- Petkova-Gueorguieva, E.S.; Getov, I.N.; Ivanov, K. V.; Ivanova, S.D.; Gueorguiev, S.R.; Getova, V.I.; Mihaylova, A.A.; Madzharov, V.G.; Staynova, R.A. Regulatory Requirements for Food Supplements in the European Union and Bulgaria. Folia Med. (Plovdiv). 2019, 61, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; Sawarkar, S.; Doshi, G.; Pimple, P.; Shah, J.; Bana, T. Chapter twenty one - Pharmacokinetics and bioavailability of nutraceuticals. In Industrial Application of Functional Foods, Ingredients and Nutraceuticals; Anandharamakrishnan, C., Subramanian, P., Eds.; Elsevier: Amsterdam, Netherlands, 2023; pp. 725–783. [Google Scholar]
- Shavandi, M.; Yazdani, Y.; Asar, S.; Mohammadi, A. The Effect of Oral Administration of Silymarin on Serum Levels of Tumor Necrosis Factor-α and Interleukin-1ß in Patients with Rheumatoid Arthritis. Iran J Immunol 2022, 19, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Somogyi, A.A.; Barratt, D.T.; Coller, J.K. Pharmacogenetics of opioids. Clin. Pharmacol. Ther. 2007, 81, 429–444. [Google Scholar] [CrossRef] [PubMed]
- Marcianò, G.; Siniscalchi, A.; Gennaro, G. Di; Rania, V.; Vocca, C.; Palleria, C.; Catarisano, L.; Muraca, L.; Citraro, R.; Evangelista, M.; et al. Assessing Gender Differences in Neuropathic Pain Management : Findings from a Real-Life Clinical Cross-Sectional Observational Study. J Clin Med 2024, 13, 5682. [Google Scholar] [CrossRef] [PubMed]
- Rania, V.; Marcianò, G.; Casarella, A.; Vocca, C.; Palleria, C.; Calabria, E.; Spaziano, G.; Citraro, R.; Sarro, G. De; Monea, F.; et al. Oxygen – Ozone Therapy in Cervicobrachial Pain : A Real-Life Experience. J Clin Med 2023, 12, 248. [Google Scholar] [CrossRef]
- Tu, Y.; Muley, M.M.; Beggs, S.; Salter, M.W. Microglia-independent peripheral neuropathic pain in male and female mice. Pain 2022, 163, e1129–e1144. [Google Scholar] [CrossRef]
- Clark, A.K.; Old, E.A.; Malcangio, M. Neuropathic pain and cytokines: Current perspectives. J. Pain Res. 2013, 6, 803–814. [Google Scholar] [CrossRef]
- Coraggio, V.; Guida, F.; Boccella, S.; Scafuro, M.; Paino, S.; Romano, D.; Maione, S.; Luongo, L. Neuroimmune-driven neuropathic pain establishment: A focus on gender differences. Int. J. Mol. Sci. 2018, 19. [Google Scholar] [CrossRef]
- Ekar, T.; Kreft, S. Common risks of adulterated and mislabeled herbal preparations. Food Chem Toxicol 2019, 123, 288–297. [Google Scholar] [CrossRef]
- Awortwe, C.; Bruckmueller, H.; Cascorbi, I. Interaction of herbal products with prescribed medications: A systematic review and meta-analysis. Phramcol Res 2019, 141, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Opuni, K.F.M.; Kretchy, J.P.; Agyabeng, K.; Boadu, J.A.; Adanu, T.; Ankamah, S.; Appiah, A.; Amoah, G.B.; Baidoo, M. , Kretchy, I.A. Contamination of herbal medicinal products in low-and-middle-income countries: A systematic review. Heliyon 2023, 9, e19370. [Google Scholar] [CrossRef] [PubMed]
- WHO Guidelines for assessing quality of herbal medicines with reference to contaminants and residues. World Health Organization. 2007. Available online: https://iris.who.int/bitstream/handle/10665/43510/9789241594448_eng.pdf.
- FDA Dietary Supplements. 2024. Available online: https://www.fda.gov/food/dietary-supplements.
- EC Directive 2001/83/EC of the European Parliament and of The Council of 6 November 2001 on the Community code relating to medicinal products for human use. 2021. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:02001L0083-20210526.
- EMA Herbal medicinal products. Available online: https://www.ema.europa.eu/en/human-regulatory-overview/herbal-medicinal-products.
- EMA List of national competent authorities in the EEA. Available online: https://www.ema.europa.eu/en/partners-networks/eu-partners/eu-member-states/national-competent-authorities-human#list-of-national-competent-authorities-in-the-eea-11541.
- Thakkar, S.; Anklam, E.; Xu, A.; Ulberth, F.; Li, J.; Li, B.; Hugas, M.; Sarma, N.; et al. Regulatory landscape of dietary supplements and herbal medicines from a global perspective. Regul Toxicol Pharmacol 2020, 114, 104647. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Structure of nutrients. The components display different effects: Escin, epigallocatechin-3-gallate, sulforaphane and silymarin exert an antioxidant and anti-inflammatory effect. Glutathione and silymarin act as hepatoprotective substances, with glutathione being also an antioxidant. Tryptophan is an adjuvant for side effects associated with pain.
Figure 1.
Structure of nutrients. The components display different effects: Escin, epigallocatechin-3-gallate, sulforaphane and silymarin exert an antioxidant and anti-inflammatory effect. Glutathione and silymarin act as hepatoprotective substances, with glutathione being also an antioxidant. Tryptophan is an adjuvant for side effects associated with pain.
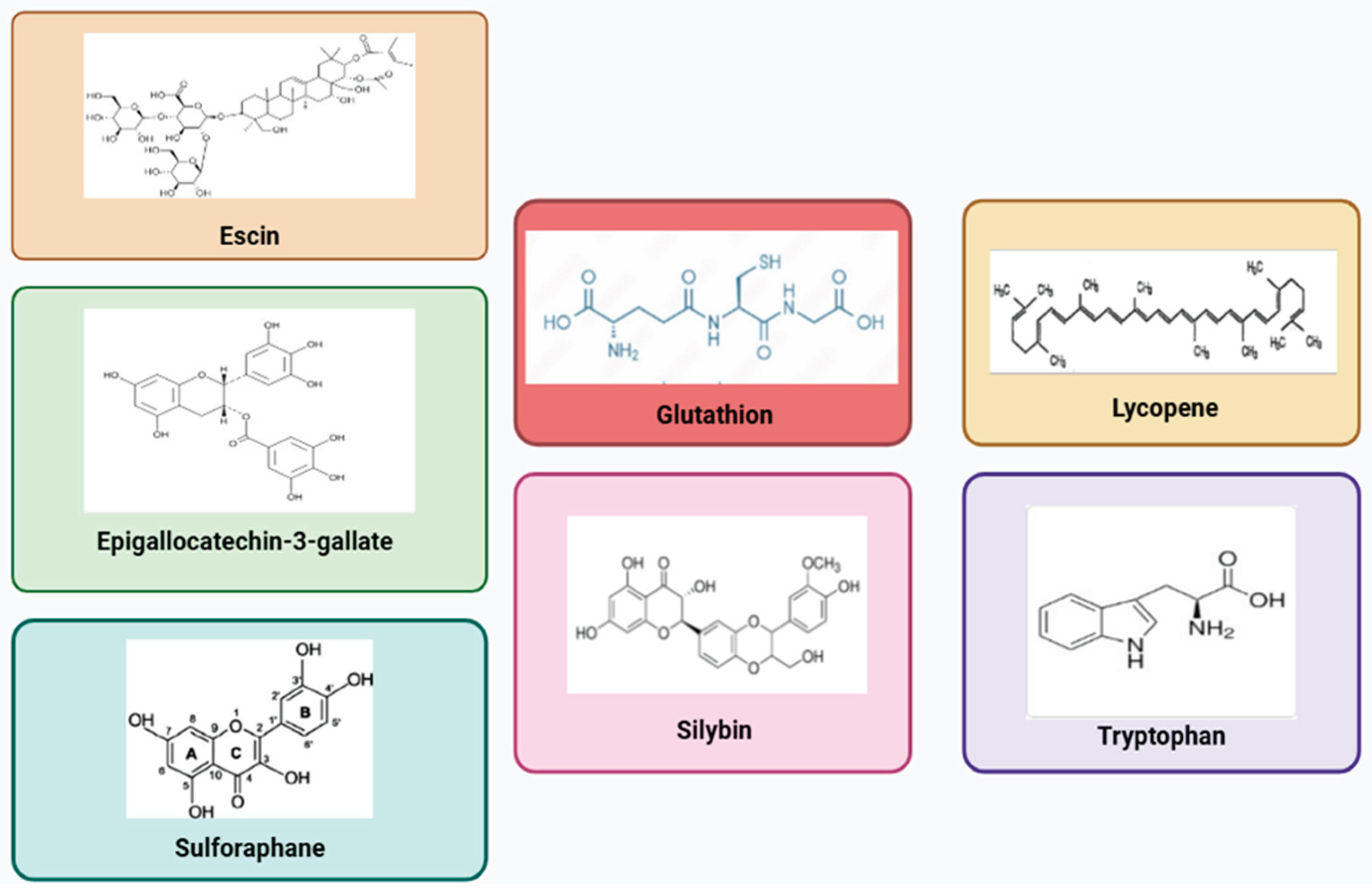

Table 1.
Mechanism of action of each nutraceutical component.
| Compound | Mechanism | References |
| Lycopene | TNF-α and NO inhibition. | [33] |
| COX 2 inhibition | [33] | |
| Restoring the expression of Cx 43 | [35] | |
| Modulation on Nrf2 and autophagy modulation | [36] | |
| Reduced glial activation. Decrease of the expression of markers like pS6, mTOR, GFAP, p4EBP, Iba 1 and SIRT 1. | [37] | |
| Reduction of thermal and cold hyperalgesia, increase of CAT, GSH, SOD, MDA levels and signs of histopathological nerve damage, reduction of cell apoptosis. | [38] | |
| Neuroprotective effect on microglia | [41] | |
| Silymarin | Inhibition of PGE2, leukotrienes, NO, cytokines production IL 1-β and TNF-α reduction, and neutrophils infiltration. Silymarin is also a scavenger, and this may account for its beneficial properties. |
[43] |
| Reduced glutathione | Antioxidant effects | [42] |
| Escin | Glucocorticoid like activity with inhibition of NF-κB and hyaluronidase | [47] |
| Action on bradykinin pathway | [28] | |
| Antioxidant effect and endothelium protection | [46,68] | |
| Downregulation of TNF and IL1ß, TLR4, NF-κB, GFAP and NGF. | [51] | |
| Targeting of MMP9, SRC, PTGS 2, and MAPK 1, PKC, the T-cell receptors signaling pathway, TRP channels, and TNF. | [46,69] | |
| Tryptophan | Improvement of pain related dysfunction including mood disorders and insomnia, acting on serotonin pathway | [56] |
| Green tea | Inhibition of PMNs, NADPH-oxidase, myeloperoxidase, and to favor scavenging of superoxide anions. | [59] |
| Inhibition of nNOS/NO; CX3CL1, JNK, and NF-κB; TNF-α. | [59] | |
| Sulforaphane | Inhibition of Nrf 2, IL-1β, TNFα, COX-2, NLRP 3, NF-κB and CGRP | [60] |
| Increase of IL-10 | [66,67] | |
| Increase of μ opioid receptor expression | [61] | |
| Inhibition of the release of H2S and of potassium Kv7 channels activation | [65] | |
| CAT, catalase; CGRP, calcitonin gene-related peptide; Cx, connexin; COX, cyclooxygenase; H2S, hydrogen sulphide; CX3CL1, chemokine (C-X3-C motif) ligand 1; GFAP, glial fibrillary acidic protein; GSH, reduced glutathione; IL, interleukin; Iba1, ionized calcium-binding adapter molecule 1; JNK, Janus Kinase; MAPK, mitogen-activated protein kinase; MMDA, malondialdehyde; MMP, metalloproteinase; mTOR, mammalian target of rapamycin; NADPH, Nicotinamide Adenine Dinucleotide Phosphate Hydrogen; NGF, nerve growth factor; NF-κB, Nuclear factor kappa-light-chain-enhancer of activated B cells ; NLRP, nucleotide-binding domain, leucine-rich–containing family, pyrin domain–containing; NO, nitric oxide; NOS, nitric oxide synthase; Nrf2, Nuclear factor erythroid 2-related factor 2; PG, prostaglandin; PMN, polymorphonuclear leukocytes; PKC, protein kinase C; PTGS, prostaglandin-endoperoxide synthase; SIRT1, sirtuin 1; SOD, superoxide dismutase; SRC, Steroid Receptor Coactivator; TLR4, toll-like receptor 4; TNF, Tumor Necrosis Factor; TRP, transient receptor potential. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



