
Submitted:
11 February 2026
Posted:
12 February 2026
You are already at the latest version
Abstract
Irritable bowel syndrome (IBS) is a common gastrointestinal disorder marked by abdominal discomfort, altered bowel habits, and comorbidities like anxiety, fatigue, and poor sleep. Existing treatments often fall short of long-term relief and fail to address root causes, leaving many patients with persistent symptoms. This contributes to a substantial burden on individuals and healthcare systems, highlighting the need for new, mechanism-based therapies. Emerging evidence suggests that gastrointestinal symptoms may be caused by the cumulative burden of epithelial injury and insufficient time for mucosal maintenance and repair. This paper explores the hypothesis that structured intermittent fasting regimes could represent a safe, low-cost, and underutilized therapeutic strategy for IBS by promoting gut renewal and restoring homeostasis. We review the multifactorial pathophysiology of IBS and explore how fasting may counter these mechanisms. Evidence from IBS and IBD studies shows that intermittent fasting can reduce inflammation, enhance autophagy, regulate gut motility, and reshape the microbiota, thereby strengthening the gut barrier and dampening immune responses. Notably, fasting induces autophagy, a key cellular recycling process essential for intestinal barrier maintenance and microbial defense, which may be impaired in IBS. Although clinical studies on fasting regimes and IBS are limited, evidence from related populations and mechanistic research supports further exploration. As a practical, circadian-aligned approach that does not restrict specific foods, intermittent fasting may reduce epithelial injury and allow time for repair. The shift from “what to eat” to “when to eat” offers a new, physiology-based potential tool for IBS treatment.
Keywords:
irritable bowel syndrome
; intermittent fasting
; gut homeostasis
; inflammation
; autophagy
Background
Irritable bowel syndrome (IBS) can be a debilitating condition, affects millions worldwide and remains notoriously difficult to manage. Despite decades of research, treatment options largely focus on symptom suppression rather than addressing root causes — and for many patients, long-term relief remains elusive. In recent years, different fasting regimes have emerged as biologically plausible, low-cost interventions with the potential to influence multiple mechanisms implicated in IBS. This paper explores the hypothesis that structured intermittent fasting could improve intestinal homeostasis and reduce symptom burden in IBS.
Methods
This hypothesis paper is based on a targeted, non-systematic review of the literature. Relevant human, animal, and mechanistic studies were identified through iterative searches of the biomedical literature and by cross-referencing key publications in the fields of intermittent fasting, gastrointestinal physiology, immune regulation, and gut–brain interactions. The included evidence was selected to illustrate plausible biological pathways and conceptual links relevant to the proposed hypothesis, rather than to provide an exhaustive or systematic synthesis of the available literature.
The Condition, Its Prevalence and Its Comorbidities
IBS is a functional gastrointestinal disorder characterized by abdominal pain and changes in stool form and frequency (diarrhea, constipation, or both), as defined by the Rome IV criteria [1], in the absence of detectable pathology on standard medical testing [2]. Reliable biomarkers for IBS are lacking [3]. The global prevalence of IBS is estimated at 9.2%, though this varies widely between countries—even when standardized diagnostic criteria and methods are applied [4]. Prevalence is consistently higher among women than men [4].
In addition to gastrointestinal symptoms, IBS is frequently accompanied by comorbidities such as anxiety, depression, fibromyalgia, chronic fatigue syndrome, and sleep disturbances [5]. It is often unclear whether IBS leads to these conditions or arises as a consequence of them. However, in the case of mood disorders, some evidence suggests that gastrointestinal symptoms may precede psychological symptoms [6]. Both the GI symptoms and comorbidities contribute to significantly reduced quality of life [7], and patients have reported a willingness to sacrifice years of life expectancy for effective relief [8]. The disorder also imposes a substantial economic burden, both through direct healthcare costs and through indirect costs such as reduced work productivity and disability benefits [8].
Because there is currently no known cure for IBS, treatment strategies typically focus on symptom relief through medications, dietary interventions, or supplements. However, these approaches do not address the underlying pathophysiology and may fail to produce long-term improvement [6]. Surveys indicate that many IBS patients experience unmet needs and are dissatisfied with the care they receive from the healthcare system [7,9]. Given the significant burden IBS places on both individuals and society, there is a clear need to expand the therapeutic toolbox available to patients and clinicians to improve outcomes and reduce long-term costs.
The Multifaceted Pathophysiology of IBS
The pathophysiology of IBS remains incompletely understood, but current evidence points to a complex interplay between the gut and the central nervous system. Disruptions in the gut–brain axis contribute to key features of the disorder, including altered gastrointestinal motility, visceral hypersensitivity, and changes in central pain processing [10].
In a comprehensive review published in The Lancet, Holtmann et al. summarize the diverse pathological features associated with IBS, emphasizing its heterogeneous and multifactorial nature [6]. Their analysis highlights that, compared with healthy individuals, IBS patients exhibit a range of inflammation-related abnormalities, such as gut microbiota dysbiosis, low-grade mucosal inflammation, increased intestinal permeability, and both local (gut-specific) and systemic (humoral) immune activation. These findings challenge the traditional notion of IBS as a functional disorder rooted solely in gut–brain axis dysregulation and support its reclassification as a disorder with measurable biological alterations [6].
The Role of Diet in IBS
Although food reactions are not included in the most common diagnostic criteria for IBS, a majority of patients report that meals exacerbate their symptoms [11]. In recent years, the role of diet has gained increasing attention both in research and in clinical management of IBS [12]. However, identifying true individual dietary triggers remains challenging, and many patients continue to experience symptoms despite significant dietary modifications [13].
Several studies have shown that IBS patients often report intolerances to specific foods, food groups, or food components [11,14]. Yet, when these self-reported intolerances are tested under double-blind, placebo-controlled conditions, only a small proportion can be reliably reproduced [15]. This discrepancy may be due to the dose-dependent or delayed nature of food-related symptoms, making it difficult to pinpoint true dietary triggers. As a result, patients may unnecessarily eliminate benign foods - in the worst case a risk factor for disordered eating behavior such as avoidant/restrictive food intake disorder [16] - while continuing to consume unrecognized triggers.
Despite the well-known limitations of self-reported dietary intake in observational studies, robust evidence exists from controlled human trials for specific dietary triggers of IBS symptoms. For example, fermentable carbohydrates such as fructose and sorbitol [17], as well as lactulose—a synthetic carbohydrate used medically [18]—have been shown to reliably provoke gastrointestinal symptoms in individuals with IBS under controlled conditions. In another intervention study, bran intake was associated with symptom worsening in the majority of IBS participants, though a minority reported relief [19].
While most treatment strategies target the colon, evidence suggests that the small intestine may also play a role. Using confocal laser endomicroscopy, immediate structural and functional changes—along with infiltration of inflammatory cells—have been observed in the duodenal tissue of IBS patients after exposure to common dietary components such as cow’s milk, wheat, yeast, and soy [20,21]. These findings highlight the importance of considering small intestinal responses when evaluating dietary influences in IBS.
Limitations to Dietary Symptom Management
Elimination diets, such as the low FODMAP diet or very low-carbohydrate diets, have demonstrated efficacy in alleviating IBS symptoms [22,23,24,25,26]. Notably, the recent CARIBS trial showed that dietary interventions resulted in greater symptom improvement than pharmacological treatment [26]. However, these dietary approaches are highly restrictive, often leading to a limited variety of food options and requiring substantial patient involvement. They may also pose social and practical challenges, making long-term adherence difficult. While adherence can be significantly improved through the support of a dietitian [27], such professional guidance is not always available or systematically offered to patients within clinical care pathways [28].
In addition, dietary recommendations for IBS management may conflict with general dietary guidelines, which can create confusion for patients attempting to self-manage their symptoms. For example, many of the fermentable carbohydrates associated with IBS symptoms are also classified as dietary fibers—non-digestible carbohydrates that are typically fermented by the gut microbiota. While a high intake of fiber is widely promoted as beneficial for intestinal health [29], this general advice may be counterproductive for IBS patients in the absence of individualized dietary guidance.
The temporal relationship between dietary triggers and IBS pathology remains unclear and adds to the complexity of understanding the condition. A central question is whether dietary factors contribute to the development of IBS pathology, thereby leading to symptoms, or whether an underlying IBS pathology increases sensitivity to dietary triggers: the “chicken or egg” dilemma.
Coffee consumption serves as a useful example of this uncertainty. While it is frequently self-reported as a symptom trigger among IBS patients [12] and has been linked to symptom recurrence upon reintroduction following exclusion [30], its causal role remains unresolved. To date, no randomized controlled trial (RCT) has specifically examined the effect of coffee consumption on IBS symptoms. Only one prospective study has investigated the association, finding that coffee intake was associated with a reduced risk of developing IBS [31]. In contrast, cross-sectional studies have yielded inconsistent results, reporting both increased and decreased odds of IBS symptoms associated with coffee consumption [31].
The Role of the Microbiome in IBS
There is increasing recognition that disturbances in the intestinal microbiome may be both a contributor to and consequence of intestinal inflammation in IBS. While advances in sequencing technologies have generated vast amounts of microbiome data from IBS patients, no universally accepted microbial signature has been identified that can reliably distinguish IBS patients from healthy individuals or serve as a diagnostic biomarker [32].
Nonetheless, comparative studies have identified recurring microbial features in IBS. These include an increased abundance of Firmicutes, a higher Firmicutes-to-Bacteroidetes ratio [32], and elevated levels of Proteobacteria, including potentially pathogenic strains such as Escherichia coli and methanogens [33]. Conversely, IBS patients often show a reduction in beneficial microbes, particularly Bifidobacterium species and butyrate-producing bacteria such as Faecalibacterium prausnitzii, which are crucial for maintaining gut barrier integrity and modulating inflammation [32,33,34].
Machine learning approaches have shown promise in identifying microbial signatures associated with IBS symptom severity, successfully distinguishing patients with mild, moderate, and severe symptoms, as well as differentiating IBS from IBD [34,35]. However, inconsistencies between studies, interindividual variability, and differences across IBS subtypes have hindered the development of a unified microbial profile, challenging the notion of a taxonomically defined IBS-related dysbiosis.
The complexity of diet-microbiome-host interactions is still being unraveled, and current understanding remains incomplete. Most microbiome studies rely on fecal sampling, which primarily reflects the microbial composition of the distal colon. While informative, these samples may not accurately capture structural and functional alterations in the small intestine or upper gastrointestinal tract. Direct sampling studies demonstrate that the distal ileal microbiota is distinct from both colonic and fecal communities, being dominated by facultative, oral-type taxa and characterized by low biomass and high ecological sensitivity [36]. Furthermore, much of the existing research focuses on bacterial taxa, often overlooking the roles of the mycobiome, phageome, and the broader interplay between microbial kingdoms in shaping gut function. This limited understanding has implications for treatment development. Research into alternative therapies, such as fecal microbiota transplantation (FMT), has yielded mixed results: while some clinical trials report symptom improvement, others have found no consistent benefit, and the long-term efficacy of FMT in IBS remains uncertain [37]. These findings underscore the need for a more comprehensive ecological perspective that includes host factors and microbial functionality, not just composition, in efforts to restore gut homeostasis.
In a recent paradigm-shifting paper, Lee et al. [38] argue for moving beyond compositional analysis toward an ecological framework that conceptualizes the gut as a homeostatic ecosystem. Under normal conditions, the host maintains hypoxic environments in the colon that favor obligate anaerobic fermenters. However, disruptions caused by inflammation, antibiotics, or dietary insults can increase luminal oxygen, allowing facultative anaerobes - often associated with disease - to dominate. According to this model, observed shifts in microbial composition may be symptoms of a disrupted environment, rather than the primary cause of dysbiosis. This reframing invites a broader therapeutic perspective: rather than targeting specific microbes, interventions might aim to restore ecological balance and host-microbial homeostasis, offering novel avenues for managing IBS.
This shift in thinking can be exemplified by the intestinal barrier - including the mucus barrier - which serves as the first line of defense by shielding the epithelium from pathogens, mechanical stress, and dietary antigens [39]. Disruption of the mucus barrier has been implicated in a range of gastrointestinal disorders, including IBS, inflammatory bowel disease (IBD), and metabolic conditions [40]. For example, mice deficient in MUC2 - the primary colonic mucin - exhibit a thinner, more penetrable mucus layer that allows commensal microbes to approach the epithelial surface. These mice are highly vulnerable to intestinal infections, develop spontaneous colitis even in the absence of pathogens, and show increased risk of tumor formation driven by low-grade inflammation and epithelial proliferation [40]. Dietary factors can significantly influence mucus barrier function, as demonstrated in preclinical studies. Maltodextrin, a synthetic polysaccharide widely used in ultra-processed foods, has been shown to disrupt gut microbial balance, promote adherence of pathobionts, degrade mucins, and increase intestinal permeability [41]. Similarly, carboxymethylcellulose, a synthetic emulsifier, has been found to deplete commensal bacteria within the mucus layer, thin the mucus barrier, increase inflammatory responses, and promote microbial encroachment in animal models [42]. Emerging evidence also highlights the importance of the mucus barrier in preventing food allergies and sensitivities [40]. Hence, seeking to avoid dietary factors that have the potential to compromise host-microbial homeostasis via the mucus lining, could be more useful than dietary interventions seeking to reduce symptoms that occur as a result.
Can Insights from IBD Be Helpful for Understanding IBS?
It has been proposed that IBS may represent a subclinical or low-grade form of IBD, due to considerable overlap in underlying mechanisms [43]. Supporting this, many patients with IBD experience IBS-like symptoms during remission, suggesting a continuum in symptom expression between the two conditions [44]. Moreover, both IBS and IBD patients display mucosal biofilms and disruptions in bile acid metabolism to a far greater extent than healthy controls [45]. Dysbiosis is another hallmark shared between IBS and IBD. Both conditions are associated with reduced gut microbial diversity, loss of beneficial bacterial species (such as Faecalibacterium prausnitzii and Bifidobacterium spp.), and increased abundance of potentially pathogenic bacteria, particularly within the phylum Proteobacteria [34,46]. These features reflect a common inflammatory component in the microbial ecosystem of both disorders. Evidence from nutritional interventions also points to shared responses. For instance, FODMAP restriction has been shown to reduce gastrointestinal symptoms in IBD patients during remission, although this symptom improvement does not correspond to changes in inflammatory biomarkers such as C-reactive protein (CRP) or fecal calprotectin [22,47]. This finding highlights a broader concern in both IBS and IBD: that symptom-targeted treatments may not adequately address underlying pathology [6].
While no RCTs to date have examined the effects of very low-carbohydrate or ketogenic diets on IBD symptoms or disease activity, case reports suggest that ketogenic diets may improve outcomes in select patients, potentially by eliminating common dietary triggers [48]. In animal models of colitis induced with dextran sulfate sodium (DSS), ketogenic diets have shown mixed results, further emphasizing the need for human studies [49,50]. A variety of dietary strategies have been proposed to alleviate both symptoms and inflammation in IBD [51]. Among these, intermittent fasting regimens stand out due to their universal accessibility, low cost, and minimal need for clinical supervision. Given the inflammatory features observed in IBS and its pathophysiological similarities with IBD, it is worth exploring whether dietary strategies that reduce inflammation in IBD could also be beneficial for IBS patients.
The Therapeutic Potential of Fasting
Over the past few decades, the body of literature on fasting strategies has grown rapidly. However, this field continues to face challenges due to the lack of standardized protocols and consistent terminology. To address this issue, we adopt the definitions proposed in a recent expert consensus publication on fasting terminology [52]. Intermittent fasting is used here as an umbrella term for repetitive fasting regimens lasting up to 48 hours, including time-restricted eating, while fasting-mimicking diets are discussed separately where mechanistically relevant. Table 1 presents fasting-related terms used in this work, as defined in the consensus publication [52].
Interventions involving various forms of fasting have demonstrated broad health benefits across conditions with distinct etiologies. In humans, fasting has been shown to improve markers of insulin resistance, dyslipidemia and systemic inflammation, and has led to meaningful improvements in obesity, hypertension, asthma, and rheumatoid arthritis - conditions in which inflammation is part of the clinical picture [53,54].
Although research on fasting in IBD remains limited, early results are encouraging. Fasting-mimicking diets have been associated with reduced inflammation and symptom improvement in both human patients and animal models of IBD [55]. For instance, in a case study involving a female patient with ulcerative colitis, eight weeks of TRE led to a significant reduction in inflammatory markers including CRP and calprotectin [56]. Additionally, several ongoing or recently completed clinical trials are actively investigating the therapeutic potential of fasting regimens in IBD patients [57,58,59], underscoring increasing scientific interest in this approach. Given the growing evidence of shared inflammatory and microbial features between IBS and IBD discussed previously in this paper, findings from fasting studies in IBD populations may inform hypotheses relevant to IBS management.
Despite a growing interest, fasting-based interventions remain only minimally explored in the context of IBS. To date, we have identified one previously published study in which a 10-day fasting intervention led to improvements in multiple IBS symptoms compared to a control group [60]; however, this protocol involved total starvation under medical supervision, limiting its practicality as a self-managed therapeutic strategy. In addition, preliminary findings from a recent pilot intervention conducted by our research group suggest that an 8-week TRE regimen in an uncontrolled setting may be associated with clinically meaningful reductions in IBS symptom severity across subtypes, supporting the feasibility and biological plausibility of structured fasting approaches while underscoring the need for controlled trials [61].
Based on current evidence and shared disease mechanisms, we hypothesize that increasing time spent in a fasting state could alleviate IBS symptoms by targeting underlying inflammatory and microbial dysregulation. While RCTs on intermittent fasting in IBS are still lacking, mechanistic studies suggest that fasting can attenuate gut inflammation - supporting the rationale for exploring structured fasting as a feasible, low-cost, and accessible adjunctive therapy for IBS.
Underappreciated Need for Renewal in IBS?
The fact that meals induce damage to the epithelium has generally received little attention in IBS management. The intestinal tract is exposed to constant mechanical, chemical, and microbial challenges, necessitating rapid and continuous epithelial renewal, occurring approximately every 3–5 days in the small intestine [62] and every 5–7 days in the colon [63]. In both the small intestine and colon stem cells located at the base of the crypts divide to produce transient cells which proliferate, differentiate, and migrate along defined axes. In the small intestine, differentiated cells (including absorptive enterocytes, Goblet cells, enteroendocrine cells, and Paneth cells) migrate upward along the crypt–villus axis, while in the colon—where villi are absent—they migrate toward the luminal surface. In both regions, fully matured cells are ultimately shed into the intestinal lumen via apoptosis [62,63]. This highly dynamic turnover is tightly regulated by both endogenous signals and exogenous stimuli from the gut microbiota. Notably, microbial metabolites like short-chain fatty acids (SCFAs) enhance proliferation and differentiation of epithelial cells, thereby contributing to epithelial homeostasis [62]. Thus, the integrity of the intestinal epithelium depends on the orchestrated interaction between stem cells, niche signals, and the gut microbiota.
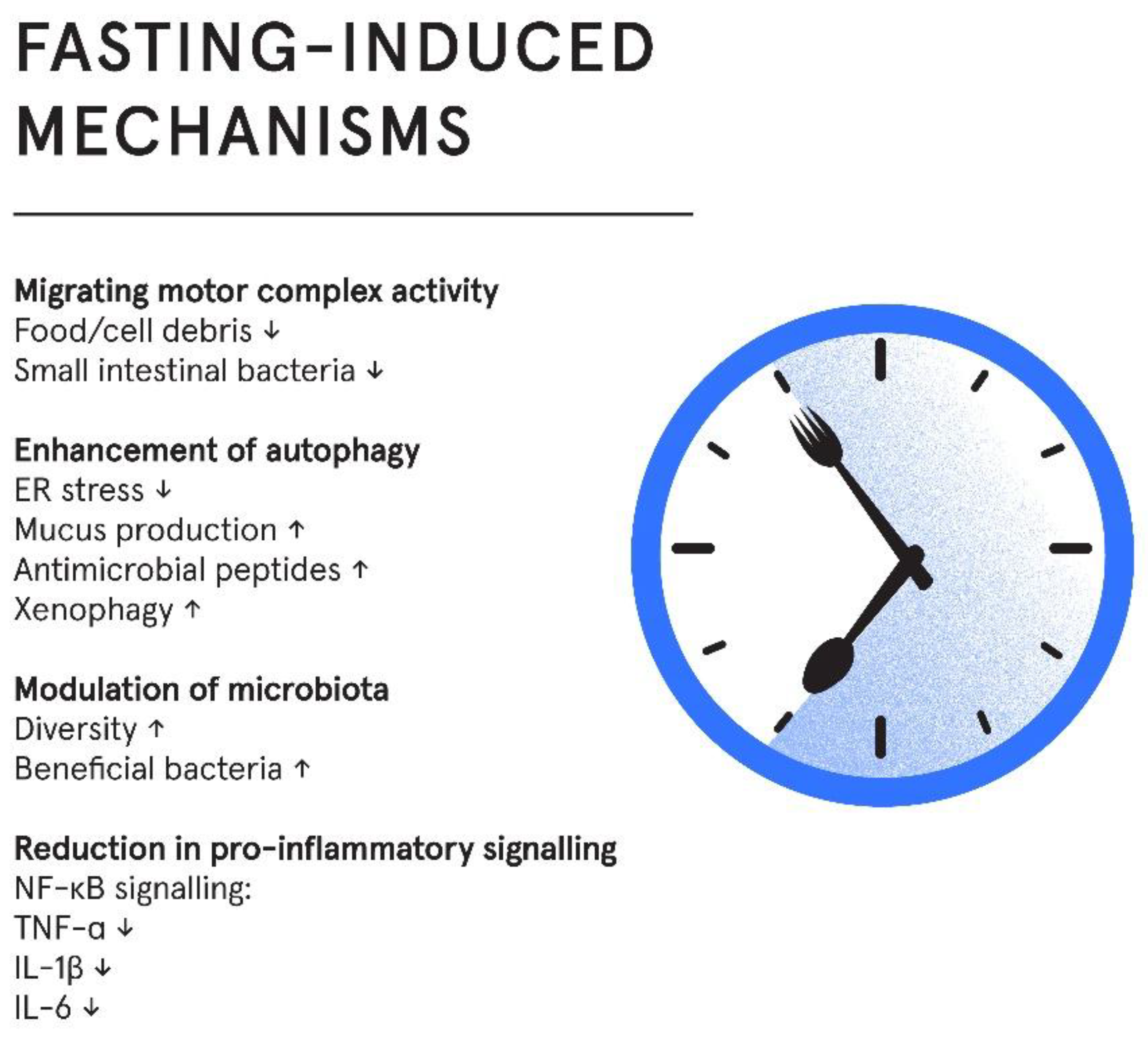
Regenerative processes induced by fasting have received little attention in the field of IBS, but research indicates that periods of fasting that allow for maintenance, repair and renewal could be a missing link in understanding disease pathology. Several mechanisms that influence the homeostatic environment of the gut may be involved, including pro-inflammatory signaling, migrating motor complex activity, modulation of gut microbiota, reduction of pro-inflammatory cytokines and enhancement of autophagy. Table 2 summarizes proposed pathways through which intermittent fasting may influence IBS, integrating clinical, translational, and mechanistic evidence across biological levels, whereas subsequent sections discuss proposed mechanisms.
Proposed Mechanisms by Which Intermittent Fasting May Promote Gut Homeostasis in IBS
Reduction in Pro-Inflammatory Signaling
Mechanistically, fasting inhibits NF-κB signaling, a central mediator of inflammation, thereby downregulating pro-inflammatory cytokines [70]. Accordingly, IF regimes have reduced levels of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6 in both animal and human trials [70]. However, despite an established mechanistic link between fasting and reduced inflammation, the inclusion of studies on healthy individuals in systematic reviews and meta-analyses as well as the lack of studies on IBS patients, makes results difficult to interpret in the context of IBS pathology.
Migrating Motor Complex Activity
The migrating motor complex (MMC) is a cyclical pattern of electromechanical activity that occurs in the stomach and small intestine during fasting periods [69]. Commonly referred to as the “housekeeper” of the gut, the MMC plays a vital role in clearing residual food particles, mucus, and bacteria, thereby helping to prevent bacterial overgrowth and intestinal inflammation.
Disruptions in MMC activity have been linked to various gastrointestinal disorders, including IBS. Patients with IBS tend to exhibit a shorter duration of postprandial motor activity than healthy individuals, and those with diarrhea-predominant IBS (IBS-D) often show shorter intervals between MMCs compared to those with constipation-predominant IBS (IBS-C). Impaired MMC function is also associated with small intestinal bacterial overgrowth (SIBO) - a condition commonly seen in IBS - highlighting a broader pattern of dysregulated interdigestive motility in the disorder [74]. These findings suggest a pattern of dysregulated interdigestive motility in IBS. However, whether the disturbances in MMC activity are a cause or consequence of IBS remains uncertain. Because the MMC is initiated during fasting and suppressed by food intake [69], fasting protocols may improve MMC activity regulation by prolonging fasting periods, thereby supporting bacterial clearance and contributing to gut homeostasis. Although there is a biological rationale for enhancing MMC function through fasting, direct clinical evidence is warranted to evaluate its therapeutic potential in IBS.
Modulation of Gut Microbiota
Evidence from both human and animal studies indicate that long-term fasting induces a state of remodeling and renewal of both the microbial ecosystem and intestinal tissues, with subsequent reduction in pro-inflammatory events and immune responses [73]. Longer-term fasting also leads to a reduction in microbial density, and a relative increase in microbes capable of utilizing host derived nutrients sources (shedded epithelial cells and mucins), such as Akkermansia muciniphila [73]. Consequently, it has been hypothesized that fasting is a mechanism that enables the host to reset the microbial ecosystem in the gut and to regain control of the microbial activity [73]. Intermittent fasting, including TRE, has been associated with changes in the gut microbiota composition, richness, and diversity. In human studies, intermittent fasting has shown potential to increase microbial richness and α-diversity, although results vary between individuals and fasting regimens, results from human studies are heterogeneous and difficult to interpret [71]. Of interest, beneficial genera such as Akkermansia and Faecalibacterium, have been reported to increase during intermittent fasting [71,72].
Enhancement of Autophagy
Autophagy is a highly conserved, cell-intrinsic recycling mechanism essential for maintaining cellular homeostasis, especially in tissues exposed to environmental stressors like the gut [64]. In intestinal epithelial cells, autophagy plays a critical role in sustaining barrier integrity and immune balance. It is activated in response to stressors such as nutrient deprivation, infection, and organelle damage, facilitating the degradation of dysfunctional components and invasive pathogens [65]. In the gut, autophagy safeguards epithelial function through several key mechanisms. It alleviates endoplasmic reticulum (ER) stress and supports mucus secretion in Goblet cells, while also enabling Paneth cells to release antimicrobial peptides [64,67]. These functions are essential for maintaining the mucosal barrier and preventing microbial translocation. Additionally, autophagy facilitates xenophagy - the selective clearance of invading microbes - thereby limiting inflammation and preserving gut immune tolerance.
Disruption of autophagic pathways has been linked to gut inflammatory conditions by impaired secretion, barrier dysfunction, and heightened inflammatory responses in both animal models and human patients [64,67]. Importantly, fasting is one of the most potent physiological inducers of autophagy. Evidence indicates that food deprivation robustly activates autophagy in various tissues, including the gut, enhancing the cell’s ability to clear damaged components and preserve homeostasis [65]. Current research on the relationship between autophagy and IBS is limited, however a mechanistic link between IBS pathology and impaired autophagy was recently demonstrated, as exosomes derived from IBS patients can suppress autophagy in human colon epithelial cells [66]. Thus, therapeutic strategies aiming to restore autophagy may hold promise in improving IBS-related epithelial dysfunction.
Figure 1.
Fasting influences multiple interconnected domains, including microbiome composition, gut motility, mucosal inflammation and autophagy. These changes may support epithelial integrity and reduce symptom burden.
Figure 1.
Fasting influences multiple interconnected domains, including microbiome composition, gut motility, mucosal inflammation and autophagy. These changes may support epithelial integrity and reduce symptom burden.
Metabolic Effects of Intermittent Fasting
Intermittent fasting exerts systemic metabolic effects that may indirectly influence intestinal homeostasis. Improved insulin sensitivity, lipid regulation, and reductions in low-grade systemic inflammation have been consistently observed in fasting interventions [53,54]. These changes can modulate gut physiology through altered bile acid signaling, adipokine balance, and activation of cellular stress-response pathways such as AMP-activated protein kinase (AMPK)-mechanistic target of rapamycin (mTOR)-autophagy [54], collectively supporting epithelial integrity and immune regulation. Thus, metabolic adaptation represents a plausible intermediary mechanism linking fasting to gastrointestinal outcomes.
Considerations for the Application of Intermittent Fasting Regimes in IBS Treatment
While further research is needed to fully understand the long-term effects and mechanisms of intermittent fasting in IBS, early findings suggest promising potential for this approach as a safe, accessible, and non-pharmacological strategy to support symptom management and potentially address underlying pathology. Importantly, early feasibility data from a recent pilot study conducted by our research group indicate that time-restricted eating is well tolerated in individuals with IBS and may confer symptom benefit [61], reinforcing the translational relevance of the mechanistic framework proposed here.
From a clinical perspective, fasting regimens in this context are not intended to induce weight loss. Participants should therefore be instructed to consume nutrient-dense foods and to eat to satiety during eating windows, in order to prevent nutritional deficiencies and support metabolic and overall physiological function. Moreover, as individuals with IBS are at increased risk of disordered eating, any dietary intervention—including intermittent fasting—should be implemented with caution and tailored to the patient’s psychological relationship with food. With thoughtful implementation and continued scientific inquiry, intermittent fasting could emerge as a valuable addition to the therapeutic toolkit for IBS.
Author Contributions
Conceptualization, M.K.; investigation, M.K.; writing - original draft preparation, M.K.; writing - review and editing, A.B., H.F.D., M.M. and J.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Use of Artificial intelligence
Artificial intelligence–based language assistance (ChatGPT, OpenAI) was used to improve the clarity, structure, and readability of the manuscript after initial drafting. All content was critically reviewed, edited, and approved by the authors, who take full responsibility for the manuscript.
Conflicts of Interest
M.K. is the author of a popular science book addressing time-restricted eating and receives royalties from book sales. All other authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AMPK | AMP-activated protein kinase |
| CRP | C-reactive protein |
| DSS | dextran sulfate sodium |
| ER | endoplasmic reticulum |
| FMT | fecal microbiota transplantation |
| FODMAP | fermentable oligosaccharides, disaccharides, monosaccharides, and polyols |
| GI | gastrointestinal |
| IBD | inflammatory bowel disease |
| IBS | irritable bowel syndrome |
| IBS-C | constipation-predominant irritable bowel syndrome |
| IBS-D | diarrhea-predominant irritable bowel syndrome |
| IF | intermittent fasting |
| IL | interleukin |
| MMC | migrating motor complex |
| mTOR | mechanistic target of rapamycin |
| NF-κB | nuclear factor kappa B |
| RCT | randomized controlled trial |
| SCFA | short-chain fatty acid |
| SIBO | small intestinal bacterial overgrowth |
| TNF-α | tumor necrosis factor alpha |
| TRE | time-restricted eating |
References
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology 2016, S0016-5085(16)00223-7. [Google Scholar] [CrossRef]
- Fikree, A.; Byrne, P. Management of Functional Gastrointestinal Disorders. Clin. Med. 2021, 21, 44–52. [Google Scholar] [CrossRef]
- Kim, J.H.; Lin, E.; Pimentel, M. Biomarkers of Irritable Bowel Syndrome. J. Neurogastroenterol. Motil. 2017, 23, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Oka, P.; Parr, H.; Barberio, B.; Black, C.J.; Savarino, E.V.; Ford, A.C. Global Prevalence of Irritable Bowel Syndrome According to Rome III or IV Criteria: A Systematic Review and Meta-Analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 908–917. [Google Scholar] [CrossRef] [PubMed]
- Shiha, M.G.; Aziz, I. Review Article: Physical and Psychological Comorbidities Associated with Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2021, 54 Suppl 1, S12–S23. [Google Scholar] [CrossRef]
- Holtmann, G.J.; Ford, A.C.; Talley, N.J. Pathophysiology of Irritable Bowel Syndrome. Lancet Gastroenterol. Hepatol. 2016, 1, 133–146. [Google Scholar] [CrossRef]
- El-Salhy, M.; Johansson, M.; Klevstul, M.; Hatlebakk, J.G. Quality of Life, Functional Impairment and Healthcare Experiences of Patients with Irritable Bowel Syndrome in Norway: An Online Survey. BMC Gastroenterol. 2025, 25, 143. [Google Scholar] [CrossRef]
- Canavan, C.; West, J.; Card, T. Review Article: The Economic Impact of the Irritable Bowel Syndrome. Aliment. Pharmacol. Ther. 2014, 40, 1023–1034. [Google Scholar] [CrossRef]
- IFFGD’s IBS Patients’ Illness Experience and Unmet Needs Survey - IFFGD. Available online: https://iffgd.org/news/press-release/2020-iffgd-s-ibs-patients-illness-experience-and-unmet-needs-survey/ (accessed on 24 March 2025).
- Ford, A.C.; Sperber, A.D.; Corsetti, M.; Camilleri, M. Irritable Bowel Syndrome. The Lancet 2020, 396, 1675–1688. [Google Scholar] [CrossRef]
- Simrén, M.; Månsson, A.; Langkilde, A.M.; Svedlund, J.; Abrahamsson, H.; Bengtsson, U.; Björnsson, E.S. Food-Related Gastrointestinal Symptoms in the Irritable Bowel Syndrome. Digestion 2001, 63, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Capili, B.; Anastasi, J.K.; Chang, M. Addressing the Role of Food in Irritable Bowel Syndrome Symptom Management. J. Nurse Pract. 2016, 12, 324–329. [Google Scholar] [CrossRef]
- Atkinson, W.; Sheldon, T.A.; Shaath, N.; Whorwell, P.J. Food Elimination Based on IgG Antibodies in Irritable Bowel Syndrome: A Randomised Controlled Trial. Gut 2004, 53, 1459–1464. [Google Scholar] [CrossRef] [PubMed]
- Böhn, L.; Störsrud, S.; Törnblom, H.; Bengtsson, U.; Simrén, M. Self-Reported Food-Related Gastrointestinal Symptoms in IBS Are Common and Associated With More Severe Symptoms and Reduced Quality of Life. Off. J. Am. Coll. Gastroenterol. ACG 2013, 108, 634. [Google Scholar] [CrossRef]
- Young, E.; Stoneham, M.D.; Petruckevitch, A.; Barton, J.; Rona, R. A Population Study of Food Intolerance. Lancet Lond. Engl. 1994, 343, 1127–1130. [Google Scholar] [CrossRef]
- Murray, H.B.; Doerfler, B.; Harer, K.N.; Keefer, L. Psychological Considerations in the Dietary Management of Patients With DGBI. Am. J. Gastroenterol. 2022, 117, 985–994. [Google Scholar] [CrossRef]
- Valeur, J.; Øines, E.; Helvik Morken, M.; Juul Holst, J.; Berstad, A. Plasma Glucagon-like Peptide 1 and Peptide YY Levels Are Not Altered in Symptomatic Fructose-Sorbitol Malabsorption. Scand. J. Gastroenterol. 2008, 43, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Valeur, J.; Morken, M.H.; Norin, E.; Midtvedt, T.; Berstad, A. Carbohydrate Intolerance in Patients with Self-Reported Food Hypersensitivity: Comparison of Lactulose and Glucose. Scand. J. Gastroenterol. 2009, 44, 1416–1423. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.Y.; Whorwell, P.J. Bran and Irritable Bowel Syndrome: Time for Reappraisal. Lancet Lond. Engl. 1994, 344, 39–40. [Google Scholar] [CrossRef]
- Fritscher-Ravens, A.; Schuppan, D.; Ellrichmann, M.; Schoch, S.; Röcken, C.; Brasch, J.; Bethge, J.; Böttner, M.; Klose, J.; Milla, P.J. Confocal Endomicroscopy Shows Food-Associated Changes in the Intestinal Mucosa of Patients with Irritable Bowel Syndrome. Gastroenterology 2014, 147, 1012–1020.e4. [Google Scholar] [CrossRef]
- Aguilera-Lizarraga, J.; Florens, M.V.; Viola, M.F.; Jain, P.; Decraecker, L.; Appeltans, I.; Cuende-Estevez, M.; Fabre, N.; Van Beek, K.; Perna, E.; et al. Local Immune Response to Food Antigens Drives Meal-Induced Abdominal Pain. Nature 2021, 590, 151–156. [Google Scholar] [CrossRef]
- Pedersen, N.; Ankersen, D.V.; Felding, M.; Wachmann, H.; Végh, Z.; Molzen, L.; Burisch, J.; Andersen, J.R.; Munkholm, P. Low-FODMAP Diet Reduces Irritable Bowel Symptoms in Patients with Inflammatory Bowel Disease. World J. Gastroenterol. 2017, 23, 3356–3366. [Google Scholar] [CrossRef] [PubMed]
- Halmos, E.P.; Power, V.A.; Shepherd, S.J.; Gibson, P.R.; Muir, J.G. A Diet Low in FODMAPs Reduces Symptoms of Irritable Bowel Syndrome. Gastroenterology 2014, 146, 67–75.e5. [Google Scholar] [CrossRef] [PubMed]
- Algera, J.P.; Demir, D.; Törnblom, H.; Nybacka, S.; Simrén, M.; Störsrud, S. Low FODMAP Diet Reduces Gastrointestinal Symptoms in Irritable Bowel Syndrome and Clinical Response Could Be Predicted by Symptom Severity: A Randomized Crossover Trial. Clin. Nutr. Edinb. Scotl 2022, 41, 2792–2800. [Google Scholar] [CrossRef]
- Austin, G.L.; Dalton, C.B.; Hu, Y.; Morris, C.B.; Hankins, J.; Weinland, S.R.; Westman, E.C.; Yancy, W.S.; Drossman, D.A. A Very Low-Carbohydrate Diet Improves Symptoms and Quality of Life in Diarrhea-Predominant Irritable Bowel Syndrome. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2009, 7, 706–708.e1. [Google Scholar] [CrossRef] [PubMed]
- Nybacka, S.; Törnblom, H.; Josefsson, A.; Hreinsson, J.P.; Böhn, L.; Frändemark, Å.; Weznaver, C.; Störsrud, S.; Simrén, M. A Low FODMAP Diet plus Traditional Dietary Advice versus a Low-Carbohydrate Diet versus Pharmacological Treatment in Irritable Bowel Syndrome (CARIBS): A Single-Centre, Single-Blind, Randomised Controlled Trial. Lancet Gastroenterol Hepatol. 2024, 9, 507–520. [Google Scholar] [CrossRef]
- Tuck, C.J.; Reed, D.E.; Muir, J.; Vanner, S. A236 A REAL-WORLD EVALUATION OF THE LOW FODMAP DIET IMPLEMENTATION: POOR COMPLIANCE IS SIGNIFICANTLY IMPROVED BY GUIDANCE FROM A DIETITIAN. J. Can. Assoc. Gastroenterol. 2019, 2, 461. [Google Scholar] [CrossRef]
- Scarlata, K.; Eswaran, S.; Baker, J.R.; Chey, W.D. Utilization of Dietitians in the Management of Irritable Bowel Syndrome by Members of the American College of Gastroenterology. Off. J. Am. Coll. Gastroenterol. ACG 2022, 117, 923. [Google Scholar] [CrossRef]
- Ioniță-Mîndrican, C.-B.; Ziani, K.; Mititelu, M.; Oprea, E.; Neacșu, S.M.; Moroșan, E.; Dumitrescu, D.-E.; Roșca, A.C.; Drăgănescu, D.; Negrei, C. Therapeutic Benefits and Dietary Restrictions of Fiber Intake: A State of the Art Review. Nutrients 2022, 14, 2641. [Google Scholar] [CrossRef]
- Heizer, W.D.; Southern, S.; McGovern, S. The Role of Diet in Symptoms of Irritable Bowel Syndrome in Adults: A Narrative Review. J. Am. Diet. Assoc. 2009, 109, 1204–1214. [Google Scholar] [CrossRef]
- Wu, S.; Yang, Z.; Yuan, C.; Liu, S.; Zhang, Q.; Zhang, S.; Zhu, S. Coffee and Tea Intake with Long-Term Risk of Irritable Bowel Syndrome: A Large-Scale Prospective Cohort Study. Int. J. Epidemiol. 2023, 52, 1459–1472. [Google Scholar] [CrossRef]
- Shaikh, S.D.; Sun, N.; Canakis, A.; Park, W.Y.; Weber, H.C. Irritable Bowel Syndrome and the Gut Microbiome: A Comprehensive Review. J. Clin. Med. 2023, 12, 2558. [Google Scholar] [CrossRef]
- Chong, P.P.; Chin, V.K.; Looi, C.Y.; Wong, W.F.; Madhavan, P.; Yong, V.C. The Microbiome and Irritable Bowel Syndrome - A Review on the Pathophysiology, Current Research and Future Therapy. Front. Microbiol. 2019, 10, 1136. [Google Scholar] [CrossRef]
- Vich Vila, A.; Imhann, F.; Collij, V.; Jankipersadsing, S.A.; Gurry, T.; Mujagic, Z.; Kurilshikov, A.; Bonder, M.J.; Jiang, X.; Tigchelaar, E.F.; et al. Gut Microbiota Composition and Functional Changes in Inflammatory Bowel Disease and Irritable Bowel Syndrome. Sci. Transl. Med. 2018, 10, eaap8914. [Google Scholar] [CrossRef]
- Tap, J.; Derrien, M.; Törnblom, H.; Brazeilles, R.; Cools-Portier, S.; Doré, J.; Störsrud, S.; Le Nevé, B.; Öhman, L.; Simrén, M. Identification of an Intestinal Microbiota Signature Associated With Severity of Irritable Bowel Syndrome. Gastroenterology 2017, 152, 111–123.e8. [Google Scholar] [CrossRef]
- Villmones, H.C.; Haug, E.S.; Ulvestad, E.; Grude, N.; Stenstad, T.; Halland, A.; Kommedal, Ø. Species Level Description of the Human Ileal Bacterial Microbiota. Sci. Rep. 2018, 8, 4736. [Google Scholar] [CrossRef]
- Halkjær, S.I.; Lo, B.; Cold, F.; Christensen, A.H.; Holster, S.; König, J.; Brummer, R.J.; Aroniadis, O.C.; Lahtinen, P.; Holvoet, T.; et al. Fecal Microbiota Transplantation for the Treatment of Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. 2023. Available online: http://www.wjgnet.com/. [CrossRef]
- Lee, J.-Y.; Bays, D.J.; Savage, H.P.; Bäumler, A.J. The Human Gut Microbiome in Health and Disease: Time for a New Chapter? Infect. Immun. 2024, 92, e00302–e00324. [Google Scholar] [CrossRef]
- Akdis, C.A. Does the epithelial barrier hypothesis explain the increase in allergy, autoimmunity and other chronic conditions? Nat Rev Immunol. 2021, 21, 739–751. [Google Scholar] [CrossRef]
- Parrish, A.; Boudaud, M.; Kuehn, A.; Ollert, M.; Desai, M.S. Intestinal mucus barrier: a missing piece of the puzzle in food allergy. Trends Mol Med. 2022, 28, 36–50. [Google Scholar] [CrossRef]
- Laudisi, F.; Di Fusco, D.; Dinallo, V.; Stolfi, C.; Di Grazia, A.; Marafini, I.; Colantoni, A.; Ortenzi, A.; Alteri, C.; Guerrieri, F.; et al. The Food Additive Maltodextrin Promotes Endoplasmic Reticulum Stress-Driven Mucus Depletion and Exacerbates Intestinal Inflammation. Cell. Mol. Gastroenterol. Hepatol. 2019, 7, 457–473. [Google Scholar] [CrossRef]
- Chassaing, B.; Koren, O.; Goodrich, J.K.; Poole, A.C.; Srinivasan, S.; Ley, R.E.; Gewirtz, A.T. Dietary Emulsifiers Impact the Mouse Gut Microbiota Promoting Colitis and Metabolic Syndrome. Nature 2015, 519, 92–96. [Google Scholar] [CrossRef]
- Szałwińska, P.; Włodarczyk, J.; Spinelli, A.; Fichna, J.; Włodarczyk, M. IBS-Symptoms in IBD Patients—Manifestation of Concomitant or Different Entities. J. Clin. Med. 2021, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Fairbrass, K.M.; Costantino, S.J.; Gracie, D.J.; Ford, A.C. Prevalence of Irritable Bowel Syndrome-Type Symptoms in Patients with Inflammatory Bowel Disease in Remission: A Systematic Review and Meta-Analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1053–1062. [Google Scholar] [CrossRef]
- Baumgartner, M.; Lang, M.; Holley, H.; Crepaz, D.; Hausmann, B.; Pjevac, P.; Moser, D.; Haller, F.; Hof, F.; Beer, A.; et al. Mucosal Biofilms Are an Endoscopic Feature of Irritable Bowel Syndrome and Ulcerative Colitis. Gastroenterology 2021, 161, 1245–1256.e20. [Google Scholar] [CrossRef]
- Casén, C.; Vebø, H.C.; Sekelja, M.; Hegge, F.T.; Karlsson, M.K.; Ciemniejewska, E.; Dzankovic, S.; Frøyland, C.; Nestestog, R.; Engstrand, L.; et al. Deviations in Human Gut Microbiota: A Novel Diagnostic Test for Determining Dysbiosis in Patients with IBS or IBD. Aliment. Pharmacol. Ther. 2015, 42, 71–83. [Google Scholar] [CrossRef]
- Cox, S.R.; Lindsay, J.O.; Fromentin, S.; Stagg, A.J.; McCarthy, N.E.; Galleron, N.; Ibraim, S.B.; Roume, H.; Levenez, F.; Pons, N.; et al. Effects of Low FODMAP Diet on Symptoms, Fecal Microbiome, and Markers of Inflammation in Patients With Quiescent Inflammatory Bowel Disease in a Randomized Trial. Gastroenterology 2020, 158, 176–188.e7. [Google Scholar] [CrossRef]
- Norwitz, N.G.; Soto-Mota, A. Case Report: Carnivore–Ketogenic Diet for the Treatment of Inflammatory Bowel Disease: A Case Series of 10 Patients. Front. Nutr. 2024, 11, 1467475. [Google Scholar] [CrossRef]
- Li, S.; Zhuge, A.; Wang, K.; Lv, L.; Bian, X.; Yang, L.; Xia, J.; Jiang, X.; Wu, W.; Wang, S.; et al. Ketogenic Diet Aggravates Colitis, Impairs Intestinal Barrier and Alters Gut Microbiota and Metabolism in DSS-Induced Mice. Food Funct. 2021, 12, 10210–10225. [Google Scholar] [CrossRef]
- Kong, C.; Yan, X.; Liu, Y.; Huang, L.; Zhu, Y.; He, J.; Gao, R.; Kalady, M.F.; Goel, A.; Qin, H.; et al. Ketogenic Diet Alleviates Colitis by Reduction of Colonic Group 3 Innate Lymphoid Cells through Altering Gut Microbiome. Signal Transduct. Target. Ther. 2021, 6, 154. [Google Scholar] [CrossRef]
- Gubatan, J.; Kulkarni, C.V.; Talamantes, S.M.; Temby, M.; Fardeen, T.; Sinha, S.R. Dietary Exposures and Interventions in Inflammatory Bowel Disease: Current Evidence and Emerging Concepts. Nutrients 2023, 15, 579. [Google Scholar] [CrossRef] [PubMed]
- Koppold, D.A.; Breinlinger, C.; Hanslian, E.; Kessler, C.; Cramer, H.; Khokhar, A.R.; Peterson, C.M.; Tinsley, G.; Vernieri, C.; Bloomer, R.J.; et al. International Consensus on Fasting Terminology. Cell Metab. 2024, 36, 1779–1794.e4. [Google Scholar] [CrossRef] [PubMed]
- de Cabo, R.; Mattson, M.P. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular Mechanisms and Clinical Applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef]
- Wang, R.; Lv, X.; Xu, W.; Li, X.; Tang, X.; Huang, H.; Yang, M.; Ma, S.; Wang, N.; Niu, Y. Effects of the Periodic Fasting-Mimicking Diet on Health, Lifespan, and Multiple Diseases: A Narrative Review and Clinical Implications. Nutr. Rev. 2024, nuae003. [Google Scholar] [CrossRef] [PubMed]
- Roco-Videla, Á.; Villota-Arcos, C.; Pino-Astorga, C.; Mendoza-Puga, D.; Bittner-Ortega, M.; Corbeaux-Ascui, T. Intermittent Fasting and Reduction of Inflammatory Response in a Patient with Ulcerative Colitis. Medicina (Mex.) 2023, 59, 1453. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. (n.d.). The influence of a fasting mimicking diet on ulcerative colitis (Identifier NCT03615690). Retrieved January 30, 2026. Available online: https://clinicaltrials.gov/ct2/show/NCT03615690.
- Haskey, N.; Lewis, A.G.; Lavallee, C.; Yousuf, M.; Taylor, L.; Jilani, S.; Gold, S.; Lu, C.; Ghosh, S.; Panaccione, R.; et al. A80 TIME-RESTRICTED FEEDING IMPROVES INFLAMMATORY AND METABOLIC BIOMARKERS IN CROHN’S DISEASE WITH OVERWEIGHT: A RANDOMIZED, PLACEBO-CONTROLLED PILOT TRIAL. J. Can. Assoc. Gastroenterol. 2025, 8, i31. [Google Scholar] [CrossRef]
- Kulkarni, C.; Fardeen, T.; Gubatan, J.; Jarr, K.; Dickson, E.; Jang, H.; Temby, M.; Patel, A.; Singh, G.; Ye, J.; et al. P1035 The Effects of an Intermittent Reduced Calorie Diet on Crohn’s Disease. J. Crohns Colitis 2025, 19, i1909–i1910. [Google Scholar] [CrossRef]
- Kanazawa, M.; Fukudo, S. Effects of Fasting Therapy on Irritable Bowel Syndrome. Int. J. Behav. Med. 2006, 13, 214–220. [Google Scholar] [CrossRef]
- Thompson Clausen, M.; Sverdrup, H.; Brevik, A.; Molin, M.; Kolby, M. Time-Restricted Eating and Symptom Severity in Irritable Bowel Syndrome: Results from a Pilot Study. Preprints 2026, 2026012043. [Google Scholar] [CrossRef]
- Park, J.; Kotani, T.; Konno, T.; Setiawan, J.; Kitamura, Y.; Imada, S.; Usui, Y.; Hatano, N.; Shinohara, M.; Saito, Y.; et al. Promotion of Intestinal Epithelial Cell Turnover by Commensal Bacteria: Role of Short-Chain Fatty Acids. PLoS ONE 2016, 11, e0156334. [Google Scholar] [CrossRef]
- Barker, N. Adult Intestinal Stem Cells: Critical Drivers of Epithelial Homeostasis and Regeneration. Nat. Rev. Mol. Cell Biol. 2014, 15, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Haasis, E.; Bettenburg, A.; Lorentz, A. Effect of Intermittent Fasting on Immune Parameters and Intestinal Inflammation. Nutrients 2024, 16, 3956. [Google Scholar] [CrossRef]
- Deloose, E.; Janssen, P.; Depoortere, I.; Tack, J. The Migrating Motor Complex: Control Mechanisms and Its Role in Health and Disease. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 271–285. [Google Scholar] [CrossRef]
- Vantrappen, G.; Janssens, J.; Hellemans, J.; Ghoos, Y. The Interdigestive Motor Complex of Normal Subjects and Patients with Bacterial Overgrowth of the Small Intestine. J. Clin. Invest. 1977, 59, 1158–1166. [Google Scholar] [CrossRef]
- Ducarmon, Q.R.; Grundler, F.; Maho, Y.L.; de Toledo, F.W.; Zeller, G.; Habold, C.; Mesnage, R. Remodelling of the Intestinal Ecosystem during Caloric Restriction and Fasting. Trends Microbiol. 2023, 31, 832–844. [Google Scholar] [CrossRef]
- Paukkonen, I.; Törrönen, E.-N.; Lok, J.; Schwab, U.; El-Nezami, H. Frontiers | The Impact of Intermittent Fasting on Gut Microbiota: A Systematic Review of Human Studies. [CrossRef]
- Pérez-Gerdel, T.; Camargo, M.; Alvarado, M.; Ramírez, J.D. Impact of Intermittent Fasting on the Gut Microbiota: A Systematic Review. Adv. Biol. n/a, 2200337. [CrossRef]
- Haq, S.; Grondin, J.; Banskota, S.; Khan, W.I. Autophagy: Roles in Intestinal Mucosal Homeostasis and Inflammation. J. Biomed. Sci. 2019, 26, 19. [Google Scholar] [CrossRef]
- Bagherniya, M.; Butler, A.E.; Barreto, G.E.; Sahebkar, A. The Effect of Fasting or Calorie Restriction on Autophagy Induction: A Review of the Literature. Ageing Res. Rev. 2018, 47, 183–197. [Google Scholar] [CrossRef]
- Telpaz, S.; Bel, S. Autophagy in Intestinal Epithelial Cells Prevents Gut Inflammation. Trends Cell Biol. 2023, 33, 817–819. [Google Scholar] [CrossRef]
- Fu, R.; Liu, S.; Zhu, M.; Zhu, J.; Chen, M. Apigenin Reduces the Suppressive Effect of Exosomes Derived from Irritable Bowel Syndrome Patients on the Autophagy of Human Colon Epithelial Cells by Promoting ATG14. World J. Surg. Oncol. 2023, 21, 95. [Google Scholar] [CrossRef]

Table 1.
Fasting-related terms used in this paper.
| Term | Definition |
|---|---|
| Fasting | Any voluntary abstinence from some or all foods or foods and beverages. |
| Intermittent fasting (IF) | Repetitive fasting periods lasting up to 48 hours each, includes time restricted eating. |
| Time restricted eating (TRE) | A dietary regimen with a fasting window of at least 14 h per day in humans, and no limit on energy intake during eating hours |
| Fasting mimicking diet | Any diet specifically composed to induce the metabolic effects of fasting while allowing for a potentially higher caloric intake, including solid foods. |
Table 2.
Proposed pathways through which intermittent fasting or time-restricted eating may influence IBS, integrating clinical, translational, and mechanistic evidence. Domains are organized by biological level, proposed effect, evidence type, and proximity to clinically relevant IBS outcomes. A indicates direct clinical evidence from IBS populations demonstrating symptom-related or patient-reported outcomes, without established mechanistic confirmation; B indicates translational evidence from human physiological studies, related disease models, or interventions affecting pathways plausibly relevant to IBS pathophysiology; C indicates mechanistic or preclinical evidence primarily derived from in vitro studies, animal models, or theoretical frameworks, providing biological plausibility but limited direct clinical validation in IBS. This table is not intended to be exhaustive, but rather to provide an overview of the breadth of proposed pathways and the biological levels at which they have been investigated.
Table 2.
Proposed pathways through which intermittent fasting or time-restricted eating may influence IBS, integrating clinical, translational, and mechanistic evidence. Domains are organized by biological level, proposed effect, evidence type, and proximity to clinically relevant IBS outcomes. A indicates direct clinical evidence from IBS populations demonstrating symptom-related or patient-reported outcomes, without established mechanistic confirmation; B indicates translational evidence from human physiological studies, related disease models, or interventions affecting pathways plausibly relevant to IBS pathophysiology; C indicates mechanistic or preclinical evidence primarily derived from in vitro studies, animal models, or theoretical frameworks, providing biological plausibility but limited direct clinical validation in IBS. This table is not intended to be exhaustive, but rather to provide an overview of the breadth of proposed pathways and the biological levels at which they have been investigated.
| Pathophysiological domain | Biological level(s) involved | Proposed effect or pathway | Proximity to IBS outcomes |
References |
|---|---|---|---|---|
| Autophagy and cellular stress responses | Humans (genetic and observational evidence); animal models; intestinal mucosal tissue; epithelial and immune cells; molecular autophagy pathways | Fasting-induced autophagy supports intestinal epithelial homeostasis, antimicrobial defense, mucus secretion, and immune regulation | C | [64,65,66,67] |
| Interdigestive motility | Humans; animal models; gastrointestinal organ-level physiology; neural and hormonal signaling pathways | Fasting required for MMC activity; impaired interdigestive motility associated with IBS and SIBO |
B | [68,69] |
| Pro-inflammatory signaling |
Humans; animal models; intestinal tissue and immune endpoints; molecular and cellular pathways | Fasting attenuates NF-κB activation and pro-inflammatory cytokine signaling | B | [70] |
| Inflammatory states | Humans; animal models | Fasting leads to improvements in IBD activity, with signals of reduced intestinal inflammation (fecal calprotectin) and systemic inflammatory markers | B | [55,56,58,59] |
| Gut microbiome ecology and composition |
Humans; animal models | Fasting leads to remodeling of gut microbial ecology; influencing community structure, diversity, and functional capacity (no consistent altering of specific taxa) | B | [71,72,73] |
| IBS symptoms | Human pilot intervention (8 weeks) | TRE associated with clinically meaningful reductions in IBS symptom severity (no mechanistic endpoints assessed) | A | [61] |
IBD – inflammatory bowel disease, IBS – irritable bowel syndrome, MMC – migrating motor complex, NF-κB – nuclear factor kappa B, SIBO – small intestinal bacterial overgrowth, TRE – time-restricted eating.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



