Submitted:
10 September 2025
Posted:
10 September 2025
Read the latest preprint version here
Abstract
Background/Objectives: Obesity and insulin resistance (IR) increase the risk for mood disorders and may impair emotional experiences. This study investigated whether obesity and/or IR moderated the links between brain potentials and affective processing during young adulthood. Methods: Thirty young adults completed a passive picture-viewing task utilizing the International Affective Picture System while real-time electroencephalography was simultaneously recorded. Two event-related potential components—early posterior negativity (EPN) and late positive potential (LPP)—were quantified. Affective processing parameters included the mean valence ratings and stimulus-to-response-onset reaction times in response to unpleasant, pleasant, and neutral images. Body fat percentage and Homeostatic Model Assessment for Insulin Resistance values were measured. Hierarchical moderated regression analysis was utilized to test the interrelationships between brain potentials, adiposity, IR, and affective processing parameters. Results: In the Negative–Neutral valence condition, lean and insulin-sensitive participants gave less negative valence ratings to unpleasant versus neutral images when late-window LPP amplitudes were larger, whereas respective counterparts showed no such relationship. Contrariwise, obesity and IR did not moderate the links between LPP amplitudes and affective processing parameters in the Positive–Neutral or Negative–Positive conditions. Additionally, EPN amplitudes and affective processing scores were not moderated by obesity or IR across any of the valence conditions. Conclusions: Lean and insulin-sensitive young adults showed attenuated negative affective processing of unpleasant versus neutral stimuli through increased brain activity, whereas obese and insulin-resistant young adults did not. In contrast, obesity and IR did not modify the relationship between neural activity and positive affective processing in young adults.
Keywords:
affective processing
; early posterior negativity (EPN)
; electroencephalography (EEG)
; emotion
; event-related potentials (ERPs)
; insulin resistance
; late positive potential (LPP)
; neurophysiology
; obesity
1. Introduction
Global adult obesity rates have more than doubled from 7% in 1990 to 16% in 2022 [1]. Obesity increases the risk for multitudinous health conditions, including mood disorders [2,3] and altered emotional processing [4,5]. Specifically, obesity is generally associated with enhanced automatic negative affective processing (i.e., more difficulties in suppressing the automatic processing of information associated with negative emotions) [4,6,7] and attenuated automatic positive affective processing (i.e., diminished automatic processing of information associated with positive emotions) [5]. Although there is a notable dearth of evidence that has examined the mechanisms underlying how obesity may alter neural activity and consequent affective processing, insulin resistance (IR) has been proposed as one such mechanism. Insulin, a pancreatic hormone, functions in whole-body glycolytic processes [8]. IR emerges when target tissues are less responsive to insulin stimulation [9]. Excess body fat is an independent inducer of IR [10,11,12], in part by increasing the size of adipocytes to allow for more triglyceride storage, which promotes cell dysfunction and inflammation [13]. Specifically, hypertrophic (enlarged) adipocytes produce and secrete pro-inflammatory molecules, including cytokines, reactive oxygen species, and a surfeit of free fatty acids. These free fatty acids can enter non-adipose organ cells (e.g., hepatocytes, muscle fibers) and become misallocated to ectopic fat depots in these organs, thereby promoting lipotoxicity. Such lipotoxic molecules dysregulate the cellular organelles, resulting in the release of a plethora of reactive oxygen species and begetting systemic inflammation. Chronically, low-grade systemic inflammation provokes systemic dysregulation by impairing insulin function and glucose homeostasis [12]. Given this, it is unsurprising that obesity and IR are risk factors for many of the same health conditions. For instance, similarly to adiposity, IR increases the risk for mood disorders [14,15] and emotional processing modifications [16]. Yet there remains a substantial paucity of studies that have investigated how obesity and especially IR influence affective processing.
Neurophysiologically, affective processing neurocircuitry involves widespread brain regions. Affective processing commences with an automatic, nonconscious response to an emotional stimulus, which is signaled by elevated amygdala activity [17]. Information about emotional arousal is subsequently relayed from the amygdala and basal ganglia to the ventrolateral prefrontal cortex (vlPFC), anterior insula, supplementary motor area, as well as the angular and superior temporal gyri. The former two regions evaluate the affective input to determine whether the affective arousal necessitates regulation, while the lattermost three regions respectively simulate the motor, somatosensory, and language processes to enhance an emotional experience. If regulation is required, the vlPFC and anterior insula further project this information to the dorsolateral prefrontal cortex (dlPFC), where affect regulation occurs (i.e., downregulation of negatively-valenced stimuli and/or upregulation of positively-valenced stimuli). Subsequently, the dlPFC projects a feedforward signal directly or through the anterior middle cingulate gyrus back to the amygdala, basal ganglia, supplementary motor area, as well as the angular and superior temporal gyri. All aforementioned regions then contribute to the production of a newly-regulated emotional state [18].
Obesity and IR may impair affective processing by inducing brain structural and functional alterations in regions that modulate affective processing. For example, greater adiposity has been linked to fewer dopamine striatal D2 receptors [19], which, in turn, associates with impaired prefrontal metabolism within the orbitofrontal and anterior cingulate cortices in those with obesity [20]. These obesity-related neural modifications may reduce prefrontal modulation of affective input from the amygdala and basal ganglia, resulting in amplified responses to unpleasant stimuli and enhanced negative affective processing. Furthermore, considering that antagonistic action against dopamine D2/D3 receptors has been found to attenuate striatal activity in response to rewarding stimuli [21], this may explain why blunted positive affective processing has also been found in these subjects [5]. Additionally, a neuroimaging study observed blunted activity in the amygdalae of subjects with obesity, which was linked to a greater susceptibility to feelings of negative affectivity, particularly fear [22]. IR is also linked to brain structural and functional alterations. Peripheral IR impedes central signaling, causing central IR [23] and hindering brain glucose metabolism. Chronic central IR engenders progressive brain atrophy [24]. IR-induced atrophy is most pronounced in brain structures that function in affective processing/regulation (e.g., prefrontal cortices, medial temporal lobe, parietal gyri [25]), which may consequently impede emotional processing function over time. Central IR has also been associated with impediments in dopamine turnover and mitochondrial dysfunction, which, in turn, was related to a higher risk of mood disorders [14]. Taken together this suggests that impairments in affective processing among those with obesity and/or IR may be partially attributed to the diminished top-down modulation of affectivity due to obesity-/IR-linked brain structural and functional alterations.
Empirical evidence has most frequently utilized functional magnetic resonance imaging (fMRI) to investigate how obesity and/or IR influence neural activity and underlying affective processing. Consequently, the underlying electrophysiological mechanisms to elucidate these interrelationships remain underexplored. However, electroencephalography (EEG) may be an adequate alternative neuroimaging approach for investigating such associations, as EEG has superior temporal resolution and is significantly less expensive than fMRI [26,27]. Event-related potentials (ERPs) are defined as voltage fluctuations in the electroencephalogram that are induced by a particular event or stimulus [28]. Each ERP component is functionally differentiated according to: 1) polarity (direction of amplitude deflection); 2) scalp distribution; 3) latency (time and duration of electrocortical activity); and 4) sensitivity to particular task-linked manipulations [29]. Two ERP components—early posterior negativity (EPN) and late positive potential (LPP)—index affective processing [30]. The EPN is a negative, occipitotemporal potential with an electrocortical activity trough approximately 200–300 milliseconds (ms) post-stimulus exposure. Larger (i.e., more negative) EPN voltage amplitudes reflect an increase in postsynaptic potentials in the extrastriate visual cortex [31] and indicate elevated automatic, nonconscious, visual attention to and sensory processing of emotional versus neutral stimuli [32]. EPN is particularly sensitive to positively-valenced stimuli [33]. The LPP is a positive, centroparietal potential that commences 300–400 ms post-stimulus exposure [34,35]. Higher (i.e., more positive) LPP voltage amplitudes reflect an increase in prolonged postsynaptic potentials in the parietal and prefrontal cortices [36], and amplitude deflections are consistently higher in response to emotional versus neutral stimuli [37,38]. As LPP amplitudes are sustained throughout the continuance of image presentation [34], LPP is generally segmented into three distinctive latency windows that reflect the functional relevance of neural responses during three sequential affective processing stages: 1) automatic emotional response; 2) sustained attention to and ongoing evaluation of emotional stimuli; and 3) prolonged affective processing, affect regulation (when applicable), and possibly memory encoding [30,39,40,41,42,43,44]. LPP amplitudes in the early latency window peak in the centroparietal area [44,45,46] and functionally index emotional salience in terms of motivated attention during passive picture-viewing tasks, with amplitudes reflecting the level of arousal elicited by emotional stimuli [39,40,44]. In contrast, LPP amplitudes during the later latency windows shift to a more frontal distribution [44,45,46] and reflect greater processing of as well as sustained attention towards affective stimuli relative to neutral during passive picture-viewing tasks [40,41,44]. Late-window LPP amplitudes may also be more sensitive to valence-specific differentiation compared to the early-window LPP [47]. As such, individuals with obesity and IR would be expected to have higher late-window LPP amplitudes and enhanced affective processing in response to unpleasant stimuli as well as lower late-window LPP amplitudes and attenuated affective processing in response to pleasant stimuli compared to lean and insulin-sensitive individuals, respectively. Crucially, however, no studies to date have investigated how the relationships between brain potentials and negative or positive affective processing may differ by levels of body fat or IR, warranting investigation.
To help fill these gaps, this study was conducted with two primary aims: 1) to investigate whether obesity and/or IR moderated the relationships between brain potentials and underlying negative and positive affective processing in young adults; and 2) to test whether EEG is a sufficient neuroimaging modality to assess these interrelationships. The central hypotheses were: 1) young adults without obesity or IR will show attenuated negative affective processing through lower late-window LPP amplitudes in response to unpleasant stimuli compared to respective counterparts; and 2) young adults without obesity or IR will show enhanced positive affective processing through higher late-window LPP amplitudes in response to pleasant stimuli compared to respective counterparts.
2. Materials and Methods
2.1. Participants
Thirty young adults who inhabited the Ames, Iowa, USA location were invited to participate. The sample size was chosen in accordance with the results obtained from a power analysis conducted using G*power 3.1.9.7 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany), from which the a priori power analysis determined that a sample size of 26 participants was required to test for a linear multiple regression, fixed model, R2 increase, with a large effect size (Cohen’s f2 = 0.35), α = 0.05, power = 0.80, and the total number of predictors = 7 (3 predictors, 4 covariates).
Inclusion criteria were:
- aged 18–39 years; and
- overnight fasting capability (no more than 16 consecutive hours).
Exclusion criteria included:
- cerebrovascular/neurological diseases (e.g., stroke, multiple sclerosis, traumatic brain injury, cerebral hematoma);
- major cardiovascular events;
- major psychiatric disorders (e.g., major depressive disorder, generalized anxiety disorder, schizophrenia, autism spectrum disorders, attention deficit hyperactivity disorder, bipolar disorder);
- recent drug, alcohol, or substance abuse (≤6 months);
- diabetes mellitus I/II;
- blood pressure ≥21.3/14.7 kPa (≥160/110 mmHg)
- fasting blood glucose values of <3.9 mmol/L (<70 mg/dL) or >6.9 mmol/L (>125 mg/dL);
- current use of medications that impact weight, insulin levels, serum biomarkers, or affective processing (e.g., systemic corticosteroids, weight reduction medications, atypical antipsychotics);
- have ferrous metal implants or shrapnel around the head/eyes;
- currently pregnant; and
- currently use nicotine/tobacco products.
Approval from the Iowa State University Institutional Review Board was obtained.
2.2. Study Design and Protocol
To investigate if obesity and/or IR moderated brain potentials and affective processing, a cross-sectional, observational design was utilized. Study visits included an initial screening and two follow-up visits within a one-month timeframe.
2.2.1. Initial Screening Visit
Each potential participant had the consent form thoroughly explained, with signatures obtained during the initial screening visit. Subsequently, the medical history of each potential subject was thoroughly queried. Additionally, height and weight were obtained.
2.2.2. First Follow-Up Visit
During the first follow-up visit, height and weight were reobtained, and each participant’s body fat percentage (BF%) was measured by a dual-energy X-ray absorptiometry scan (DEXA/DXA; Hologic Discovery v.12.3, Hologic, Inc., Marlborough, Massachusetts, USA). Fasting blood serum was collected, from which fasting glucose and insulin values were quantified. Utilizing these values, IR was gauged for each participant in accordance with the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) formula: (fasting glucose (mmol/L) * fasting insulin (pmol/L))/22.5 ([glucose (mg/dL) * insulin (µIU/mL)]/405) [48]. Physical activity levels were self-reported as part of the body composition analysis and categorized as: 1) sedentary (no engagement in physical activity beyond basic movements from daily life); 2) low active (<150 (moderate) or <75 (vigorous) minutes of activity weekly); 3) active (150–300 (moderate) or 75–150 (vigorous) minutes of activity per week); and 4) very active (>300 (moderate) or >150 (vigorous) minutes of weekly activity [49]). Participants were subsequently dichotomized via whether physical activity levels totaled <150 (moderate) or <75 (vigorous) minutes weekly (sedentary/low active) versus ≥150 (moderate) or ≥75 (vigorous) minutes weekly (active/very active), as done previously [50].
2.2.3. Second Follow-Up Visit
Subjects completed the International Affective Picture System (IAPS) task [51] while brain activity was concomitantly recorded via EEG during the second follow-up visit. Participants were singly shown 64 randomized neutral (n=21), unpleasant (n=22), and pleasant (n=21) images for two seconds each, then instructed to rate the magnitude of pleasantness or unpleasantness of each image (i.e., valence ratings), where 1=“very positive,” 2=“somewhat positive,” 3=“somewhat negative,” and 4=“very negative.” Unpleasant and pleasant images were matched for normative arousal ratings to ensure that differences in neural responses were attributable to valence rather than arousal. The task photo identification numbers used in this study are listed in Table A1. IAPS task parameters were scored in E-Prime*3 [52]. Affective processing parameters included the mean valence ratings (an indicator of the magnitude of negativity or positivity felt in response to unpleasant or pleasant stimuli, respectively [53]) of and stimulus-to-response-onset reaction times (RTs, which reflect affective processing and attentional engagement [54] and are sensitive to valence-specific differentiation [55]) to unpleasant, pleasant, and neutral images. As done in prior work [56,57,58,59], in order to optimally gauge valence-specific affective processing, the scores of each emotionally-valenced condition (i.e., negative, positive) were subsequently compared to the scores of the control (i.e., neutrally-valenced) or oppositely-valenced conditions as follows:
- Negative minus Neutral;
- Positive minus Neutral; and
- Negative minus Positive.
However, because valence ratings reflect opposite degrees of unpleasantness or pleasantness for emotionally-valenced pictures, the calculation for the mean valence rating scores in the oppositely-valenced contrasted condition (i.e., Negative minus Positive) was accordingly adjusted as: Negative minus (4 – Positive).
2.3. Electroencephalography
As described previously [50], EEG was recorded using an electrode array cap comprised of 64 Ag/AgCl electrodes (Sands Research, El Paso, Texas, USA), in alignment with the standards defined by the 10-10 International System of electrode placement, and was interfaced to a digital bio-potential amplifier (DBPA-1; Sensorium Inc., Charlotte, Vermont, USA). A sampling rate of 2,048 Hz was used. Utilizing EEGlab (Version 2021.1 [60]) in MatLab (Version R2022a, MathWorks, Inc., Natick, Massachusetts, USA), the EEG preprocessing procedure included:
- the application of a high-pass (≤0.1 Hz) filter followed by a low-pass (≥30 Hz) filter (using gain 1,000, 16-bit A/D conversion);
- continuous EEG data was epoched into two-second segments post-stimulus onset (0–2.0 second latency window);
- standardized the whole-brain amplitude values via average reference computation;
- eliminated noisy channels through an automatic epoch rejection method (channel fluctuations ≥1,000 µV);
- eliminated artifacts using a peer-reviewed algorithm and statistical parameters [63]; and
- exported the whole time-course grand means for each valence condition to a .csv file.
2.4. Event-Related Potential Components
Grand-mean averaged waveforms were utilized to quantify the EPN and LPP components as follows:
To serve as ERP indices of valence-specific affective processing, EPN and LPP amplitudes of each emotionally-valenced condition (i.e., negative, positive) were then compared to the amplitudes of the control (i.e., neutrally-valenced) or oppositely-valenced conditions as follows [56,57,58,59]:
- Negative–Neutral;
- Positive–Neutral; and
- Negative–Positive.
2.5. Statistical Analysis
Participants were stratified into two separate groups based on BF% (lean (n=8) versus obese (n=22)) and HOMA-IR (insulin-sensitive (n=18) versus insulin-resistant (n=12)) values to assess between-group differences. Lean versus obese were respectively defined as a BF% of <25% (males) and <35% (females) versus ≥25% (males) and ≥35% (females) [72]. As previously recommended [73,74], HOMA-IR values of <2.0 versus ≥2.0 defined insulin sensitivity versus IR, respectively. Statistical comparisons of participant characteristics were conducted using chi-square, Fisher’s exact, or independent-samples t-tests in SPSS Statistics (Version 31.0.0.0; IBM Corp., Armonk, New York, USA). Significance was set at p≤0.05 for group comparisons.
Hierarchical moderated regression analyses tested whether obesity and/or IR moderated the relationships between brain potentials and affective processing utilizing the PROCESS macro for SPSS (Version 4.2 [75]). All continuous variables were mean-centered prior to analysis to eliminate multicollinearity issues. A multiple imputations procedure in SPSS was applied to impute missing affective processing parameters (n=2). The first step of each moderation model tested whether the predictor and moderator variables independently accounted for a significant proportion of the variance for the outcome variable. For each contrasted valence condition, the first step included a predictor (EPN, LPP voltage amplitudes), a moderator (BF%, HOMA-IR), an outcome variable (valence ratings, RTs), and all significant (p≤0.10) covariates (age, physical activity levels, race/ethnicity, sex). In the second step, each moderation model was retested after the addition of the interaction term (predictor*moderator), with all covariates readded. In both steps, each non-significant covariate was singly eliminated from each model in descending order of significance. The Bonferroni correction was applied to correct for multiple comparison of associations, in which p≤0.0063 was considered statistically significant.
3. Results
3.1. Participant Characteristics
As delineated in Table 1, demographic and clinical characteristics were compared between stratified adiposity (lean versus obese) and IR (insulin-sensitive versus insulin-resistant) groups. In summary, subjects with obesity and IR had more insulin dysregulation compared to respective counterparts. Additionally, subjects with obesity showed greater glucose dysregulation. Finally, subjects with IR participated in less weekly physical activity and had higher BF%s and diastolic blood pressure.
EPN and LPP grand-mean averaged waveforms across the sample are illustrated for each valence condition in Figure 1a,b. For EPN (Figure 1b), positively-valenced images elicited the largest (i.e., most negative) amplitudes, while negatively-valenced images evoked the smallest. For LPP (Figure 1b), negatively-valenced pictures generated the largest (i.e., most positive) amplitudes across all latency windows, while positively-valenced pictures evoked the smallest during the early latency window and neutrally-valenced pictures evoked the smallest during the later latency windows.
3.3. Neural Amplitudes by Categorical Groups
Table 2 presents the comparisons of the differenced grand-mean averaged EPN and LPP waveforms in each contrasted picture condition (i.e., Negative minus Neutral, Positive minus Neutral, and Negative minus Positive) by stratified adiposity (also see Figure 2a–f (differenced waveforms) and Supplementary Figure S1a–f (non-differenced waveforms for each separate valence condition)) and IR levels (also see Figure 3a–f (differenced waveforms) and Supplementary Figure S2a–f (non-differenced waveforms for each separate valence condition)). Concisely, participants without obesity or IR elicited higher LPP amplitudes during the late latency window in response to unpleasant versus neutral pictures than did lean or insulin-sensitive counterparts, respectively (see Figures 2b/Supplementary Figure S1b and 3b/Supplementary Figure S2b). Furthermore, participants with obesity evoked larger LPP amplitudes during the early latency window in the contrasted Negative–Positive valence condition (see Figure 2f/Supplementary Figure S1f).
3.4. Affective Processing Parameters by Categorical Groups
Differences in affective processing parameters were assessed by stratified adiposity and IR groups for each contrasted valence condition (see Table 3). In summary, participants with IR had slower RTs in response to unpleasant versus neutral images in comparison to insulin-sensitive subjects. Additionally, participants with obesity gave overall higher (i.e., more negative) valence ratings to emotional pictures in the contrasted Negative–Positive valence condition.
3.5. Neural Amplitudes and Affective Processing
Table 4 displays the correlation matrix between the ERPs and affective processing parameters in each contrasted condition. Succinctly, EPN amplitudes negatively correlated with RTs in the Negative–Positive condition, where greater amplitudes were linked to more negative valence ratings of unpleasant pictures relative to pleasant.
Notably, across all contrasted valence conditions, LPP amplitudes during the late latency window were consistently inversely associated with mean valence ratings, suggesting that higher late-window LPP amplitudes were correlated with less overall negative (for the Negative–Neutral and Negative–Positive conditions) and more overall positive (for the Positive–Neutral condition) valence ratings; however, none of these inverse associations reached statistical significance.
3.6. Moderation Analyses
3.6.1. Negative–Neutral Picture Condition
The results of how BF% and HOMA-IR values moderated the relationships between neural activity and affective processing scores in response to unpleasant versus neutral pictures are shown in Table 5 for valence ratings and in Table 6 for RTs. Further slope analyses in Figure 4a,b illustrate that, exclusively in participants with low BF% and low-to-medium HOMA-IR values, greater LPP amplitudes during the late latency window were associated with less negative valence ratings in response to unpleasant pictures relative to neutral.
3.6.2. Positive–Neutral Picture Condition
Table 7 and Table 8 present the results of the moderation analyses for predicting valence ratings and RTs, respectively, in the Positive–Neutral trials. Contrary to what was anticipated, BF% and IR were not found to moderate the associations between EPN or LPP amplitudes during any of the latency windows and affective processing scores for pleasant versus neutral stimuli.
3.6.3. Negative–Positive Picture Condition
The results of the moderation analyses are displayed in Table 9 for valence ratings and Table 10 for RTs in the Negative–Positive condition. In contrast with what was hypothesized, BF% and IR did not moderate the links between EPN or LPP amplitude deflections during any of the latency windows and affective processing parameters of unpleasant stimuli relative to pleasant.
4. Discussion
The electrophysiological mechanisms underlying how adiposity and especially IR influence the link between brain potentials and affective processing remain scarcely investigated. The paucity of studies that have investigated such interrelationships, however, have most frequently done so using fMRI (e.g., [16,22,76,77]). The single study that utilized EEG, however, assessed middle-aged adults [78]. Yet, considering the advantages of EEG in comparison of fMRI, including EEG’s superior temporal resolution and less costly utilization [26,27], it is crucial to test whether EEG is a sufficient alternative neuroimaging approach for testing such interrelationships. Therefore, EEG was utilized to investigate whether obesity and/or IR moderated the relationship between brain potentials and affective processing in young adults.
In the Negative–Neutral trials, young adults without obesity or IR displayed significantly greater LPP amplitudes during the late latency window, in contrast with what was expected. However, among these participants, larger LPP responses were linked to less negative ratings of unpleasant images, suggesting that stronger neural engagement was associated with a dampening of negative emotional experience. This pattern further implies that IR may be one mechanism through which obesity alters the neural basis of prolonged negative affective processing. By contrast, this relationship was absent in young adults with obesity and/or IR, indicating a disruption in the typical coupling between neural activity and emotional evaluation. Ordinarily, increased activity in the dlPFC in response to unpleasant stimuli reflects more top-down control to suppress affective responses [18], with successful down-regulation of negatively-valenced stimuli being subsequently manifested as reduced LPP amplitudes [79]. Hence, an inverse relationship between late-window LPP amplitudes and valence ratings (where lower values indicated less negative valence ratings) to unpleasant stimuli in lean, insulin-sensitive young adults was unexpected. Despite this, the finding of an inverse LPP amplitudes–valence ratings correlation is in congruence with findings from several studies (e.g., [80,81,82,83]). Rather than indicating an unsuccessful dampening of negatively-valenced stimuli and a concomitant enhancement of negative affective processing, higher LPP amplitudes in the late latency window may instead reflect more effortful spontaneous emotion regulation, as previously suggested [80,83]. Taken together, these findings suggest that lean, insulin-sensitive individuals may attenuate negative affective processing of unpleasant stimuli through greater cognitive effort to automatically regulate these negatively-valenced stimuli spontaneously. Additional longitudinal studies are critical to gain a clearer understanding of the electrophysiological mechanisms underlying how adiposity, IR, and associated brain structural and functional alterations influence negative affective processing.
In the contrasted Positive–Neutral valence trial, obesity and IR were not found to moderate the links between LPP amplitudes across any of the latency windows and affective processing scores, implying that neural responses to pleasant stimuli and associated positive affective processing may be spared from obesity- and/or IR-induced brain structural and functional alterations in young adulthood. These results are in concurrence with some [84,85], but not all [86,87], previous findings. Moreover, obesity and IR did not moderate the relationships between brain potentials and underlying affective processing in the contrasted Negative–Positive condition. This suggests that, similarly to the early-window LPP, late-window LPP may also be more strongly driven by arousal than by valence and, thus, may not be valence-biased [34,88,89], although this contrasts some prior study findings (e.g., [47]). Inconsistencies exist in the body of literature that has compared the LPP responses to unpleasant versus pleasant stimuli, with some studies finding no differences in LPP amplitudes between either emotional condition across a wide range of age groups [90,91] and other studies finding valence-specific differentiation, although these findings appeared to be arousal-dependent [47,89]. Significant methodological, LPP quantification, and sample heterogeneity may partially account for such discordant findings. In addition, the null results found in this study could be in part explained by differences in the neurocircuitry involved between negative and positive affective processing. Specifically, the processing of negative emotions more heavily involves activity from the amygdala, anterior insula, anterior cingulate cortex, visual cortex, as well as the dlPFC and vlPFC [92,93], whereas the processing of positive emotions more substantially relies upon activity in the medial prefrontal cortex, orbitofrontal cortex, ventral striatum, nucleus accumbens, and ventral tegmental area [94,95]. Hence, the brain structures involved in positive affective processing may be less susceptible to obesity- and/or IR-linked structural and functional alterations compared to the brain structures that modulate negative affective processing. Nevertheless, future studies are crucial to better understand how obesity and IR may impact brain potentials and positive affective processing.
Finally, BF% and HOMA-IR did not moderate the links between EPN amplitudes and affective processing parameters across any of the contrasted valence conditions. Hence, this suggests that obesity and IR do not impact visual attention allocation to emotional versus neutral stimuli in young adulthood. To our knowledge, this study is the first to investigate whether obesity and/or IR moderated the relationship between EPN amplitudes and affective processing. Nonetheless, these results are not surprising when considering that the scalp distribution of the EPN component over the occipitotemporal sites reflects visual cortical activity [96], a largely insulin-independent region [97]. One study demonstrated this by showing that insulin infusion had no effect on subsequent visual evoked potentials [98]. Nevertheless, additional research is needed to clarify whether obesity and/or IR influence EPN amplitudes and underlying visual attention allocation to emotional versus neutral stimuli.
This study was not without limitations. First, the sample size was small, hence limiting the generalizability of this study’s findings. Second, the utilization of the EEG neuroimaging modality in conjunction with the cross-sectional study design barred any causal implications. Third, neural activity measured during exposure to emotional images in a laboratory setting may not necessarily translate to real-world settings. Fourth, HOMA-IR is an index of short-term IR and may not have accurately reflected chronic IR in all subjects.
This study also included several strengths. First, the central research questions were novel. Second, EEG provided an inexpensive, non-invasive neuroimaging approach which showed findings that were largely congruent with earlier fMRI findings. Third, body composition was measured directly via DEXA, which provided a significantly more accurate quantification of BF% in comparison to indirect measures (e.g., BMI [99]).
5. Conclusions
Obesity and IR moderate the relationship between brain potentials and negative affective processing, but not positive affective processing, in young adults. Specifically, increased neural responses to unpleasant stimuli were associated with attenuated negative affective processing in lean and insulin sensitive young adults, whereas no such correlation was found in young adults with obesity or IR. This finding suggests that higher body fat levels may disrupt the typical coupling between neural activity and emotional evaluation, and IR may be one mechanism to explain how obesity alters negative affective processing. These data furthermore support prior findings that obesity and IR are both risk factors for mood disorders in young adulthood. In addition, the degree of reflexive visual attention to emotional stimuli is not moderated by obesity or IR in young adulthood. Finally, EEG appears to be a sufficient neuroimaging approach for investigating these interrelationships. Additional work is warranted to investigate these interrelationships long-term using EEG, particularly for positive affective processing.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Figures S1a–f: Non-differenced Negative, Neutral, and Positive EPN and LPP waveforms by body fat percentage; Figures S2a–f: Non-differenced Negative, Neutral, and Positive EPN and LPP waveforms by insulin resistance levels.
Author Contributions
Conceptualization, A.W.; methodology, B.L., B.K., T.W. and K.M.; software, A.W.; validation, B.L. and B.K.; formal analysis, B.L.; investigation, B.K., T.W. and K.M.; resources, A.W.; data curation, B.L.; writing—original draft preparation, B.L.; writing—review and editing, B.L., B.K., T.W., K.M., Q.W., P.M., M.F., A.Z. and A.W.; visualization, B.L. and B.K.; supervision, B.K., T.W., K.M., Q.W. and A.W.; project administration, A.W.; funding acquisition, A.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Institute on Aging, grant number R00-AG047282, and by the Alzheimer’s Association Research Grant to Promote Diversity, grant number AARGD-17-529552.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Iowa State University (protocol code: 15-101 and date of approval: 26 June 2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participant(s) to publish this paper.
Data Availability Statement
Dataset available on request from the authors.
Acknowledgments
The authors would like to thank Amy Pollpeter and Tianqi Li for their contributions to the development of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| BF% | Body fat percentage |
| BMI | Body mass index |
| BP | Blood pressure |
| DEXA/DXA | Dual-energy X-ray absorptiometry scan |
| dlPFC | Dorsolateral prefrontal cortex |
| EEG | Electroencephalography |
| eLPP | Late positive potential in the early latency window |
| EPN | Early posterior negativity |
| ERP | Event-related potential |
| fMRI | Functional magnetic resonance imaging |
| Hemoglobin A1c | Glycated hemoglobin |
| HOMA-IR | Homeostatic model assessment for insulin resistance |
| IR | Insulin resistance/resistant |
| IS | Insulin sensitivity/sensitive |
| lLPP | Late positive potential in the late latency window |
| LPP | Late positive potential |
| mLPP | Late positive potential in the middle latency window |
| ms | Milliseconds |
| RT | Reaction time |
| vlPFC | Ventrolateral prefrontal cortex |
Appendix A

Table A1.
International Affective Picture System task photo identification numbers by valence condition.
Table A1.
International Affective Picture System task photo identification numbers by valence condition.
| Negative | Neutral | Positive |
|---|---|---|
| 3030, 3060, 3071, 3100, 3102, 3130, 3150, 3170, 6020, 6230, 6313, 6570, 9040, 9140, 9181, 9253, 9265, 9320, 9420, 9433, 9570, 9571 | 2372, 2383, 2514, 2840, 5410, 6150, 6900, 7000, 7002, 7006, 7009, 7010, 7035, 7080, 7130, 7170, 7175, 7233, 7491, 7550, 7705 | 1340, 1463, 2165, 2306, 2374, 4603, 4611, 4652, 4656, 4810, 5202, 5611, 5764, 6250, 7200, 7250, 7508, 8118, 8251, 8500, 9400 |
A Table displays the photo identification number for each photo used in the negatively-, neutrally-, and positively-valenced picture conditions during the International Affective Picture System task.
References
- Brauer, M.; Roth, G.A.; Aravkin, A.Y.; Zheng, P.; Abate, K.H.; Abate, Y.H.; Abbafati, C.; Abbasgholizadeh, R.; Abbasi, M.A.; Abbasian, M. , et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. The Lancet 2024, 403, 2162–2203. [Google Scholar] [CrossRef]
- Panda, S.S.; Nayak, A.; Shah, S.; Aich, P. A systematic review on the association between obesity and mood disorders and the role of gut microbiota. Metabolites 2023, 13. [Google Scholar] [CrossRef]
- McElroy, S.L.; Kotwal, R.; Malhotra, S.; Nelson, E.B.; Keck, P.E.; Nemeroff, C.B. Are mood disorders and obesity related? A review for the mental health professional. J. Clin. Psychiatry 2004, 65, 634–651. [Google Scholar] [CrossRef]
- Romero-Rebollar, C.; García-Gómez, L.; Báez-Yáñez, M.G.; Gutiérrez-Aguilar, R.; Pacheco-López, G. Adiposity affects emotional information processing. Front. Psychol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Wegener, I.; Wawrzyniak, A.; Imbierowicz, K.; Conrad, R.; Musch, J.; Geiser, F.; Wermter, F.; Liedtke, R. Evidence for attenuated affective processing in obesity. Psychol Rep 2008, 103, 35–47. [Google Scholar] [CrossRef]
- Hanson, J.A.; Wagner, G.; Dretsch, M. Cognitive disinhibition and infrequent moderate-to-intense physical activity linked with obesity in U.S. soldiers. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 2021, 26, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Scarpina, F.; Varallo, G.; Castelnuovo, G.; Capodaglio, P.; Molinari, E.; Mauro, A. Correction to: Implicit facial emotion recognition of fear and anger in obesity. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 2021, 26, 1281–1281. [Google Scholar] [CrossRef]
- Woods, S.C.; Seeley, R.J.; Baskin, D.G.; Schwartz, M.W. Insulin and the blood-brain barrier. Curr. Pharm. Des. 2003, 9, 795–800. [Google Scholar] [CrossRef]
- Freeman, A.; Pennings, N. Insulin resistance; StatPearls Publishing Inc.: Treasure Island, FL, 2019. [Google Scholar]
- Hardy, O.T.; Czech, M.P.; Corvera, S. What causes the insulin resistance underlying obesity? Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Dhokte, S.; Czaja, K. Visceral adipose tissue: The hidden culprit for type 2 diabetes. Nutrients 2024, 16. [Google Scholar] [CrossRef]
- Ahmed, B.; Sultana, R.; Greene, M.W. Adipose tissue and insulin resistance in obese. Biomed. Pharmacother. 2021, 137, 111315. [Google Scholar] [CrossRef] [PubMed]
- Stenkula, K.G.; Erlanson-Albertsson, C. Adipose cell size: Importance in health and disease. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 2018, 315, R284–R295. [Google Scholar] [CrossRef] [PubMed]
- Kleinridders, A.; Cai, W.; Cappellucci, L.; Ghazarian, A.; Collins, W.R.; Vienberg, S.G.; Pothos, E.N.; Kahn, C.R. Insulin resistance in brain alters dopamine turnover and causes behavioral disorders. Proc Natl Acad Sci U S A 2015, 112, 3463–3468. [Google Scholar] [CrossRef]
- Martin, H.; Bullich, S.; Martinat, M.; Chataigner, M.; Di Miceli, M.; Simon, V.; Clark, S.; Butler, J.; Schell, M.; Chopra, S. , et al. Insulin modulates emotional behavior through a serotonin-dependent mechanism. Mol. Psychiatry 2024, 29, 1610–1619. [Google Scholar] [CrossRef]
- Marsh, C.A.; Berent-Spillson, A.; Love, T.; Persad, C.C.; Pop-Busui, R.; Zubieta, J.K.; Smith, Y.R. Functional neuroimaging of emotional processing in women with polycystic ovary syndrome: A case-control pilot study. Fertil Steril 2013, 100, 200–207.e201. [Google Scholar] [CrossRef]
- Breiter, H.C.; Etcoff, N.L.; Whalen, P.J.; Kennedy, W.A.; Rauch, S.L.; Buckner, R.L.; Strauss, M.M.; Hyman, S.E.; Rosen, B.R. Response and habituation of the human amygdala during visual processing of facial expression. Neuron 1996, 17, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Kohn, N.; Eickhoff, S.B.; Scheller, M.; Laird, A.R.; Fox, P.T.; Habel, U. Neural network of cognitive emotion regulation--An ALE meta-analysis and MACM analysis. NeuroImage 2014, 87, 345–355. [Google Scholar] [CrossRef]
- de Weijer, B.A.; van de Giessen, E.; van Amelsvoort, T.A.; Boot, E.; Braak, B.; Janssen, I.M.; van de Laar, A.; Fliers, E.; Serlie, M.J.; Booij, J. Lower striatal dopamine D2/3 receptor availability in obese compared with non-obese subjects. European Journal of Nuclear Medicine and Molecular Imaging Research 2011, 1, 37. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wang, G.J.; Telang, F.; Fowler, J.S.; Thanos, P.K.; Logan, J.; Alexoff, D.; Ding, Y.S.; Wong, C.; Ma, Y. , et al. Low dopamine striatal D2 receptors are associated with prefrontal metabolism in obese subjects: Possible contributing factors. NeuroImage 2008, 42, 1537–1543. [Google Scholar] [CrossRef]
- Osugo, M.; Wall, M.B.; Selvaggi, P.; Zahid, U.; Finelli, V.; Chapman, G.E.; Whitehurst, T.; Onwordi, E.C.; Statton, B.; McCutcheon, R.A. , et al. Striatal dopamine D2/D3 receptor regulation of human reward processing and behaviour. Nat. Commun. 2025, 16, 1852. [Google Scholar] [CrossRef]
- Park, B.-y.; Hong, J.; Park, H. Neuroimaging biomarkers to associate obesity and negative emotions. Sci. Rep. 2017, 7, 7664. [Google Scholar] [CrossRef]
- Sripetchwandee, J.; Chattipakorn, N.; Chattipakorn, S.C. Links between obesity-induced brain insulin resistance, brain mitochondrial dysfunction, and dementia. Front. Endocrinol. (Lausanne) 2018, 9, 496. [Google Scholar] [CrossRef] [PubMed]
- Bingham, E.M.; Hopkins, D.; Smith, D.; Pernet, A.; Hallett, W.; Reed, L.; Marsden, P.K.; Amiel, S.A. The role of insulin in human brain glucose metabolism: An 18fluoro-deoxyglucose positron emission tomography study. Diabetes 2002, 51, 3384–3390. [Google Scholar] [CrossRef]
- Willette, A.A.; Xu, G.; Johnson, S.C.; Birdsill, A.C.; Jonaitis, E.M.; Sager, M.A.; Hermann, B.P.; La Rue, A.; Asthana, S.; Bendlin, B.B. Insulin resistance, brain atrophy, and cognitive performance in late middle-aged adults. Diabetes Care 2013, 36, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Gevins, A.; Smith, M.E.; McEvoy, L.K.; Leong, H.; Le, J. Electroencephalographic imaging of higher brain function. Philos Trans R Soc Lond B Biol Sci 1999, 354, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Eryilmaz, H.H.; Duru, A.D.; Parlak, B.; Ademoglu, A.; Demiralp, T. Neuroimaging of event related brain potentials (ERP) using fMRI and dipole source reconstruction. Annu Int Conf IEEE Eng Med Biol Soc 2007, 2007, 3384–3387. [Google Scholar] [CrossRef]
- McWeeny, S.; Norton, E.S. Understanding event-related potentials (ERPs) in clinical and basic language and communication disorders research: A tutorial. Int. J. Lang. Commun. Disord. 2020, 55, 445–457. [Google Scholar] [CrossRef]
- Woodman, G.F. A brief introduction to the use of event-related potentials in studies of perception and attention. Atten Percept Psychophys 2010, 72, 2031–2046. [Google Scholar] [CrossRef]
- Brown, S.B.; van Steenbergen, H.; Band, G.P.; de Rover, M.; Nieuwenhuis, S. Functional significance of the emotion-related late positive potential. Front Hum Neurosci 2012, 6, 33. [Google Scholar] [CrossRef]
- Luck, S.J. Event-related potentials. 2012.
- Schupp, H.T.; Junghöfer, M.; Weike, A.I.; Hamm, A.O. The selective processing of briefly presented affective pictures: An ERP analysis. Psychophysiology 2004, 41, 441–449. [Google Scholar] [CrossRef]
- Frank, D.W.; Sabatinelli, D. Hemodynamic and electrocortical reactivity to specific scene contents in emotional perception. Psychophysiology 2019, 56, e13340. [Google Scholar] [CrossRef]
- Cuthbert, B.N.; Schupp, H.T.; Bradley, M.M.; Birbaumer, N.; Lang, P.J. Brain potentials in affective picture processing: Covariation with autonomic arousal and affective report. Biol. Psychol. 2000, 52, 95–111. [Google Scholar] [CrossRef]
- Moran, T.P.; Jendrusina, A.A.; Moser, J.S. The psychometric properties of the late positive potential during emotion processing and regulation. Brain Res 2013, 1516, 66–75. [Google Scholar] [CrossRef]
- Liu, Y.; Huang, H.; McGinnis-Deweese, M.; Keil, A.; Ding, M. Neural substrate of the late positive potential in emotional processing. The Journal of Neuroscience 2012, 32, 14563–14572. [Google Scholar] [CrossRef] [PubMed]
- Keil, A.; Bradley, M.M.; Hauk, O.; Rockstroh, B.; Elbert, T.; Lang, P.J. Large-scale neural correlates of affective picture processing. Psychophysiology 2002, 39, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Schupp, H.T.; Cuthbert, B.N.; Bradley, M.M.; Cacioppo, J.T.; Ito, T.; Lang, P.J. Affective picture processing: The late positive potential is modulated by motivational relevance. Psychophysiology 2000, 37, 257–261. [Google Scholar] [CrossRef]
- Hajcak, G.; Dunning, J.P.; Foti, D. Motivated and controlled attention to emotion: Time-course of the late positive potential. Clin. Neurophysiol. 2009, 120, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Hajcak, G.; MacNamara, A.; Olvet, D.M. Event-related potentials, emotion, and emotion regulation: An integrative review. Dev. Neuropsychol. 2010, 35, 129–155. [Google Scholar] [CrossRef]
- Schupp, H.T.; Flaisch, T.; Stockburger, J.; Junghöfer, M. Emotion and attention: Event-related brain potential studies. In Progress in Brain Research, Anders, S., Ende, G., Junghofer, M., Kissler, J., Wildgruber, D., Eds. Elsevier: 2006; Vol. 156, pp. 31-51.
- Fields, E.C. The P300, the LPP, context updating, and memory: What is the functional significance of the emotion-related late positive potential? Int. J. Psychophysiol. 2023, 192, 43–52. [Google Scholar] [CrossRef]
- Dolcos, F.; Cabeza, R. Event-related potentials of emotional memory: Encoding pleasant, unpleasant, and neutral pictures. Cognitive, Affective, & Behavioral Neuroscience 2002, 2, 252–263. [Google Scholar] [CrossRef]
- Macnamara, A.; Foti, D.; Hajcak, G. Tell me about it: Neural activity elicited by emotional pictures and preceding descriptions. Emotion 2009, 9, 531–543. [Google Scholar] [CrossRef]
- Foti, D.; Hajcak, G.; Dien, J. Differentiating neural responses to emotional pictures: Evidence from temporal-spatial PCA. Psychophysiology 2009, 46, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Hajcak, G.; Weinberg, A.; MacNamara, A.; Foti, D. ERPs and the Study of Emotion. In The Oxford Handbook of Event-Related Potential Components, Kappenman, E.S., Luck, S.J., Eds. Oxford University Press: 2011; 10.1093/oxfordhb/9780195374148.013.0222p. 0.
- O’Hare, A.J.; Atchley, R.A.; Young, K.M. Valence and arousal influence the late positive potential during central and lateralized presentation of images. Laterality 2017, 22, 541–559. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- U. S. Department of Health and Human Services. Physical Activity Guidelines for Americans; U.S. Dept of Health and Human Services: Washinton, D.C, 2018. [Google Scholar]
- Larsen, B.A.; Klinedinst, B.S.; Wolf, T.; McLimans, K.E.; Wang, Q.; Pollpeter, A.; Li, T.; Mohammadiarvejeh, P.; Fili, M.; Grundy, J.G. , et al. Adiposity and insulin resistance moderate the links between neuroelectrophysiology and working and episodic memory functions in young adult males but not females. Physiol Behav 2023, 271, 114321. [Google Scholar] [CrossRef]
- Lang, P.J.; Bradley, M.M.; Cuthbert, B.N. International affective picture system (IAPS): Affective ratings of pictures and instruction manual, Technical Report A-8; University of Florida: Gainesville, FL, 2008. [Google Scholar]
- Psychology Software Tools. E-Prime. Availabe online: https://pstnet.com/products/e-prime/. (accessed on 3 August 2024).
- Shaygan, M.; Böger, A.; Kröner-Herwig, B. Valence and arousal value of visual stimuli and their role in the mitigation of chronic pain: What is the power of pictures? The Journal of Pain 2017, 18, 124–131. [Google Scholar] [CrossRef]
- Calvo, M.G.; Avero, P. Reaction time normative data for the IAPS as a function of display time, gender, and picture content. Behav. Res. Methods 2009, 41, 184–191. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Bratslavsky, E.; Finkenauer, C.; Vohs, K.D. Bad is stronger than good. Rev. Gen. Psychol. 2001, 5, 323–370. [Google Scholar] [CrossRef]
- Striepens, N.; Scheele, D.; Kendrick, K.M.; Becker, B.; Schäfer, L.; Schwalba, K.; Reul, J.; Maier, W.; Hurlemann, R. Oxytocin facilitates protective responses to aversive social stimuli in males. Proc Natl Acad Sci U S A 2012, 109, 18144–18149. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Chen, J.; Yang, J.; Ju, E.; Norman, G.J.; Ding, N. Negative mood state enhances the susceptibility to unpleasant events: Neural correlates from a music-primed emotion classification task. PLoS One 2014, 9, e89844. [Google Scholar] [CrossRef]
- Botelho, C.; Pasion, R.; Prata, C.; Barbosa, F. Neuronal underpinnings of the attentional bias toward threat in the anxiety spectrum: Meta-analytical data on P3 and LPP event-related potentials. Biol. Psychol. 2023, 176, 108475. [Google Scholar] [CrossRef]
- Duan, H.; Yao, Z.; Zhang, L.; Kohn, N.; Wu, J. The late positive potentials evoked by negative emotional pictures predict autonomic responses to an acute psychosocial stressor in healthy adults. medRxiv, 1101. [Google Scholar] [CrossRef]
- Delorme, A.; Makeig, S. EEGLAB: An open source toolbox for analysis of single-trial EEG dynamics including independent component analysis. J Neurosci Methods 2004, 134, 9–21. [Google Scholar] [CrossRef]
- Winkler, I.; Haufe, S.; Tangermann, M. Automatic classification of artifactual ICA-components for artifact removal in EEG signals. Behav. Brain Funct. 2011, 7, 30. [Google Scholar] [CrossRef]
- Winkler, I.; Brandl, S.; Horn, F.; Waldburger, E.; Allefeld, C.; Tangermann, M. Robust artifactual independent component classification for BCI practitioners. J. Neural Eng. 2014, 11. [Google Scholar] [CrossRef]
- Mognon, A.; Jovicich, J.; Bruzzone, L.; Buiatti, M. ADJUST: An automatic EEG artifact detector based on the joint use of spatial and temporal features. Psychophysiology 2011, 48, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Farkas, A.H.; Sabatinelli, D. Emotional perception: Divergence of early and late event-related potential modulation. Journal of Cognitive Neuroscience 2023, 35, 941–956. [Google Scholar] [CrossRef]
- Zhang, W.; Jończyk, R.; Wu, Y.J.; Lan, Y.; Gao, Z.; Hu, J.; Thierry, G.; Gao, S. Brain potentials reveal how emotion filters native language access when bilinguals read words in their second language. Cerebral Cortex 2023, 33, 8783–8791. [Google Scholar] [CrossRef] [PubMed]
- Moretta, T.; Buodo, G. Motivated attention to stimuli related to social networking sites: A cue-reactivity study. J Behav Addict 2021, 10, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Nordström, H.; Wiens, S. Emotional event-related potentials are larger to figures than scenes but are similarly reduced by inattention. BMC Neurosci. 2012, 13, 49. [Google Scholar] [CrossRef]
- Kim, B.M.; Lee, J.; Choi, A.R.; Chung, S.J.; Park, M.; Koo, J.W.; Kang, U.G.; Choi, J.S. Event-related brain response to visual cues in individuals with internet gaming disorder: Relevance to attentional bias and decision-making. Transl Psychiatry 2021, 11, 258. [Google Scholar] [CrossRef]
- Willroth, E.C.; Koban, L.; Hilimire, M.R. Social information influences emotional experience and late positive potential response to affective pictures. Emotion 2017, 17, 572–576. [Google Scholar] [CrossRef]
- Goto, N.; Mushtaq, F.; Shee, D.; Lim, X.L.; Mortazavi, M.; Watabe, M.; Schaefer, A. Neural signals of selective attention are modulated by subjective preferences and buying decisions in a virtual shopping task. Biol. Psychol. 2017, 128, 11–20. [Google Scholar] [CrossRef]
- Kessel, E.M.; Huselid, R.F.; Decicco, J.M.; Dennis, T.A. Neurophysiological processing of emotion and parenting interact to predict inhibited behavior: An affective-motivational framework. Front. Hum. Neurosci. 2013, 7, 326. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- Lee, C.H.; Shih, A.Z.; Woo, Y.C.; Fong, C.H.; Leung, O.Y.; Janus, E.; Cheung, B.M.; Lam, K.S. Optimal cut-offs of Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) to identify dysglycemia and type 2 diabetes mellitus: A 15-year prospective study in Chinese. PLoS One 2016, 11, e0163424. [Google Scholar] [CrossRef]
- Balkau, B.; Charles, M.A. Comment on the provisional report from the WHO consultation. European Group for the Study of Insulin Resistance (EGIR). Diabet. Med. 1999, 16, 442–443. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis, Third Edition: A Regression-Based Approach, 3rd ed.; Guilford publications: New York, NY, 2022. [Google Scholar]
- Steward, T.; Picó-Pérez, M.; Mata, F.; Martínez-Zalacaín, I.; Cano, M.; Contreras-Rodríguez, O.; Fernández-Aranda, F.; Yucel, M.; Soriano-Mas, C.; Verdejo-García, A. Emotion regulation and excess weight: Impaired affective processing characterized by dysfunctional insula activation and connectivity. PLoS One 2016, 11, e0152150. [Google Scholar] [CrossRef]
- Chen, Y.-H.; Chen, C.; Jian, H.-Y.; Chen, Y.-C.; Fan, Y.-T.; Yang, C.-Y.; Cheng, Y. The neural correlates of emotional conflict monitoring as an early manifestation of affective and cognitive declines in persons with Type 2 diabetes. Brain Communications 2023, 5. [Google Scholar] [CrossRef]
- Wolf, T.; Tsenkova, V.; Ryff, C.D.; Davidson, R.J.; Willette, A.A. Neural, hormonal, and cognitive correlates of metabolic dysfunction and emotional reactivity. Psychosom. Med. 2018, 80, 452–459. [Google Scholar] [CrossRef]
- Hajcak, G.; Anderson, B.S.; Arana, A.; Borckardt, J.; Takacs, I.; George, M.S.; Nahas, Z. Dorsolateral prefrontal cortex stimulation modulates electrocortical measures of visual attention: Evidence from direct bilateral epidural cortical stimulation in treatment-resistant mood disorder. Neuroscience 2010, 170, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Langeslag, S.J.E.; Surti, K. The effect of arousal on regulation of negative emotions using cognitive reappraisal: An ERP study. Int. J. Psychophysiol. 2017, 118, 18–26. [Google Scholar] [CrossRef]
- Wu, H.; Tang, P.; Huang, X.; Hu, X.; Luo, Y. Differentiating electrophysiological response to decrease and increase negative emotion regulation. Chinese Science Bulletin 2013, 58, 1543–1550. [Google Scholar] [CrossRef]
- Bamford, S.; Broyd, S.J.; Benikos, N.; Ward, R.; Wiersema, J.R.; Sonuga-Barke, E. The late positive potential: A neural marker of the regulation of emotion-based approach-avoidance actions? Biol. Psychol. 2015, 105, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Baur, R.; Conzelmann, A.; Wieser, M.J.; Pauli, P. Spontaneous emotion regulation: Differential effects on evoked brain potentials and facial muscle activity. Int. J. Psychophysiol. 2015, 96, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Vallet, W.; Hone-Blanchet, A.; Brunelin, J. Abnormalities of the late positive potential during emotional processing in individuals with psychopathic traits: A meta-analysis. Psychol. Med. 2020, 50, 2085–2095. [Google Scholar] [CrossRef]
- Bylsma, L.M.; Tan, P.Z.; Silk, J.S.; Forbes, E.E.; McMakin, D.L.; Dahl, R.E.; Ryan, N.D.; Ladouceur, C.D. The late positive potential during affective picture processing: Associations with daily life emotional functioning among adolescents with anxiety disorders. Int. J. Psychophysiol. 2022, 182, 70–80. [Google Scholar] [CrossRef]
- Hajcak, G.; Moser, J.S.; Simons, R.F. Attending to affect: Appraisal strategies modulate the electrocortical response to arousing pictures. Emotion 2006, 6, 517–522. [Google Scholar] [CrossRef]
- Krompinger, J.W.; Moser, J.S.; Simons, R.F. Modulations of the electrophysiological response to pleasant stimuli by cognitive reappraisal. Emotion 2008, 8, 132–137. [Google Scholar] [CrossRef]
- Leite, J.; Carvalho, S.; Galdo-Alvarez, S.; Alves, J.; Sampaio, A.; Gonçalves, O.F. Affective picture modulation: Valence, arousal, attention allocation and motivational significance. Int. J. Psychophysiol. 2012, 83, 375–381. [Google Scholar] [CrossRef]
- Feng, C.; Li, W.; Tian, T.; Luo, Y.; Gu, R.; Zhou, C.; Luo, Y.-j. Arousal modulates valence effects on both early and late stages of affective picture processing in a passive viewing task. Soc. Neurosci. 2014, 9, 364–377. [Google Scholar] [CrossRef]
- Liu, Y.; Huang, H.; McGinnis-Deweese, M.; Keil, A.; Ding, M. Neural substrate of the late positive potential in emotional processing. J Neurosci 2012, 32, 14563–14572. [Google Scholar] [CrossRef]
- Renfroe, J.B.; Bradley, M.M.; Sege, C.T.; Bowers, D. Emotional modulation of the late positive potential during picture free viewing in older and young adults. PLoS One 2016, 11, e0162323. [Google Scholar] [CrossRef] [PubMed]
- Tolomeo, S.; Christmas, D.; Jentzsch, I.; Johnston, B.; Sprengelmeyer, R.; Matthews, K.; Douglas Steele, J. A causal role for the anterior mid-cingulate cortex in negative affect and cognitive control. Brain 2016, 139, 1844–1854. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Qiu, X.; Mo, L.; Li, S.; Xu, F.; Zhang, D. Asynchronous involvement of VLPFC and dlPFC during negative emotion processing: An online transcranial magnetic stimulation study. Neuroscience 2024, 551, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Machado, L.; Cantilino, A. A systematic review of the neural correlates of positive emotions. Braz J Psychiatry 2017, 39, 172–179. [Google Scholar] [CrossRef]
- Rolls, E.T. Emotion, motivation, decision-making, the orbitofrontal cortex, anterior cingulate cortex, and the amygdala. Brain Structure and Function 2023, 228, 1201–1257. [Google Scholar] [CrossRef]
- Schupp, H.T.; Markus, J.; Weike, A.I.; Hamm, A.O. Emotional facilitation of sensory processing in the visual cortex. Psychol. Sci. 2003, 14, 7–13. [Google Scholar] [CrossRef]
- Milstein, J.L.; Ferris, H.A. The brain as an insulin-sensitive metabolic organ. Mol Metab 2021, 52, 101234. [Google Scholar] [CrossRef]
- Benedict, L.; Nelson, C.A.; Schunk, E.; Sullwold, K.; Seaquist, E.R. Effect of insulin on the brain activity obtained during visual and memory tasks in healthy human subjects. Neuroendocrinology 2006, 83, 20–26. [Google Scholar] [CrossRef]
- Laskey, M.A. Dual-energy X-ray absorptiometry and body composition. Nutrition 1996, 12, 45–51. [Google Scholar] [CrossRef]
Figure 1.
Line graphs depict the grand-mean averaged EPN (a) and LPP (b) waveforms across all participants after viewing negatively- (red), neutrally- (green), and positively-valenced (blue) pictures during an International Affective Picture System task. Amplitude was measured in microvolts (µV); time was measured in milliseconds. EPN = early posterior negativity; LPP = late positive potential; ms = milliseconds. Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively.
Figure 1.
Line graphs depict the grand-mean averaged EPN (a) and LPP (b) waveforms across all participants after viewing negatively- (red), neutrally- (green), and positively-valenced (blue) pictures during an International Affective Picture System task. Amplitude was measured in microvolts (µV); time was measured in milliseconds. EPN = early posterior negativity; LPP = late positive potential; ms = milliseconds. Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively.
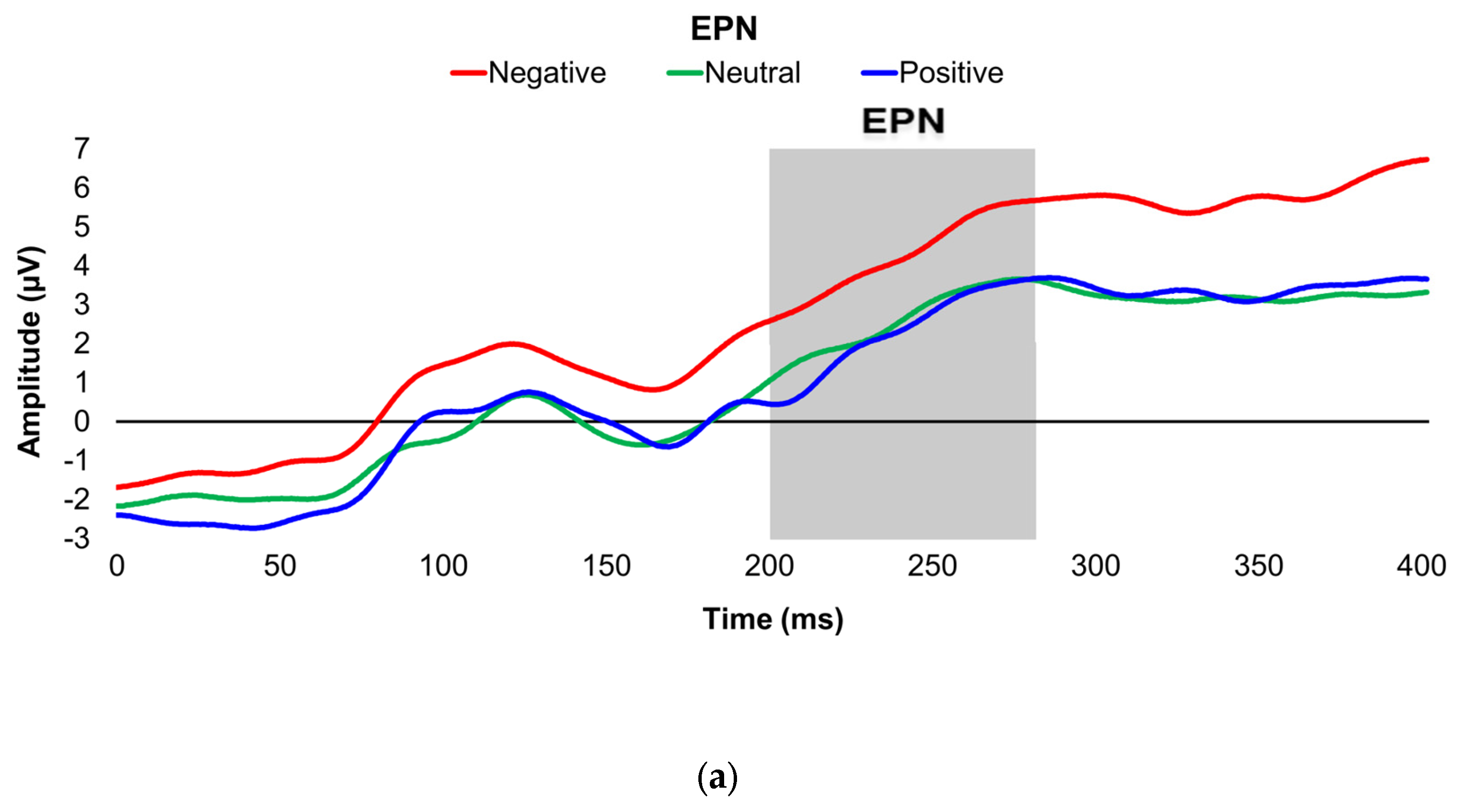
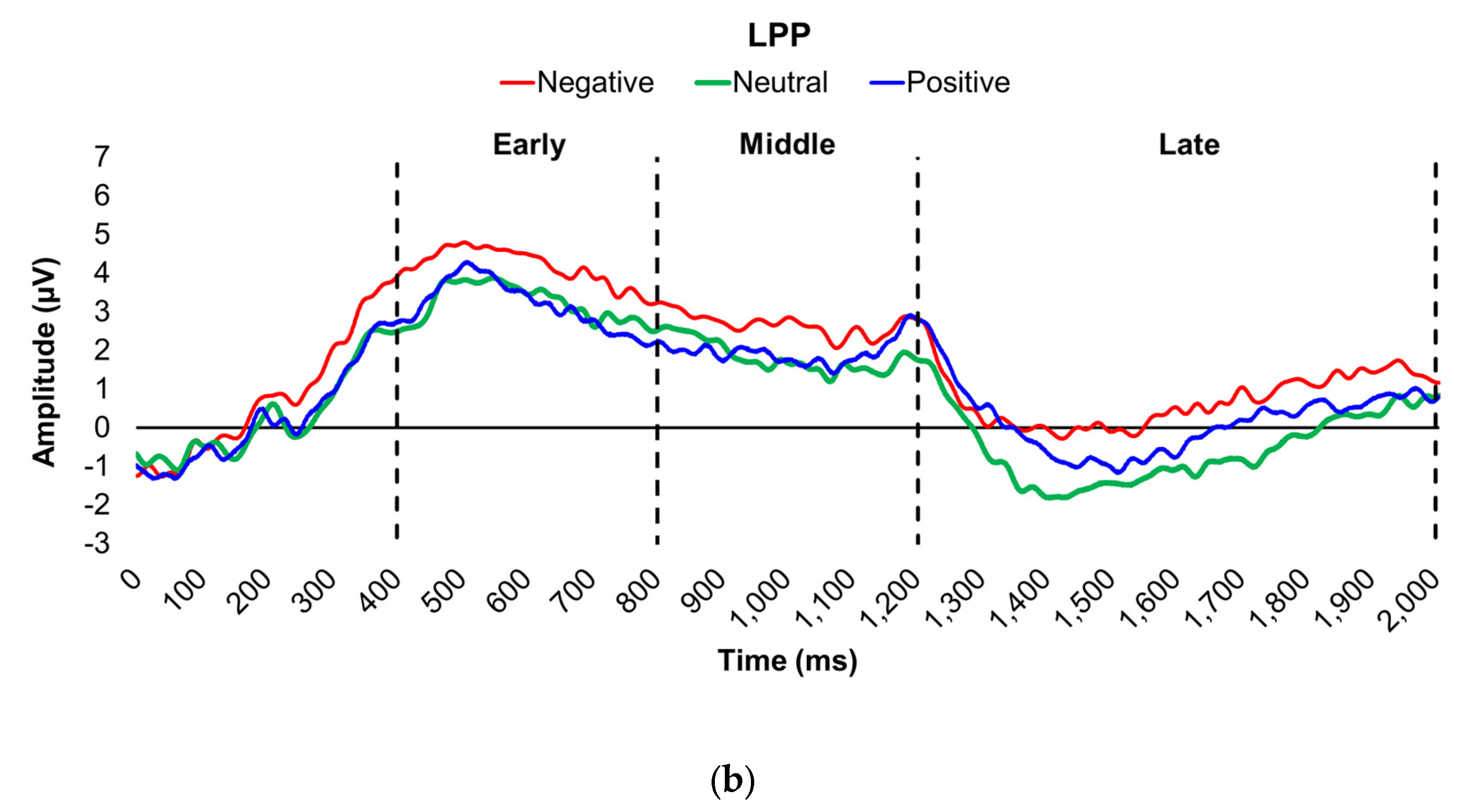
Figure 2.
Line graphs show the comparisons of the differenced grand-mean averaged EPN (left) and LPP (right) waveforms in the contrasted picture conditions (i.e., Negative minus Neutral (a–b), Positive minus Neutral (c–d), and Negative minus Positive (e–f) EPN and LPP waveforms) between lean (body fat percentage of <25% (males) and <35% (females), in blue) versus obese (body fat percentage of ≥25% (males) and ≥35% (females), in red) subjects. Amplitude was measured in microvolts (µV); time was measured in milliseconds. EPN = early posterior negativity; LPP = late positive potential; ms = milliseconds. Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively.
Figure 2.
Line graphs show the comparisons of the differenced grand-mean averaged EPN (left) and LPP (right) waveforms in the contrasted picture conditions (i.e., Negative minus Neutral (a–b), Positive minus Neutral (c–d), and Negative minus Positive (e–f) EPN and LPP waveforms) between lean (body fat percentage of <25% (males) and <35% (females), in blue) versus obese (body fat percentage of ≥25% (males) and ≥35% (females), in red) subjects. Amplitude was measured in microvolts (µV); time was measured in milliseconds. EPN = early posterior negativity; LPP = late positive potential; ms = milliseconds. Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively.
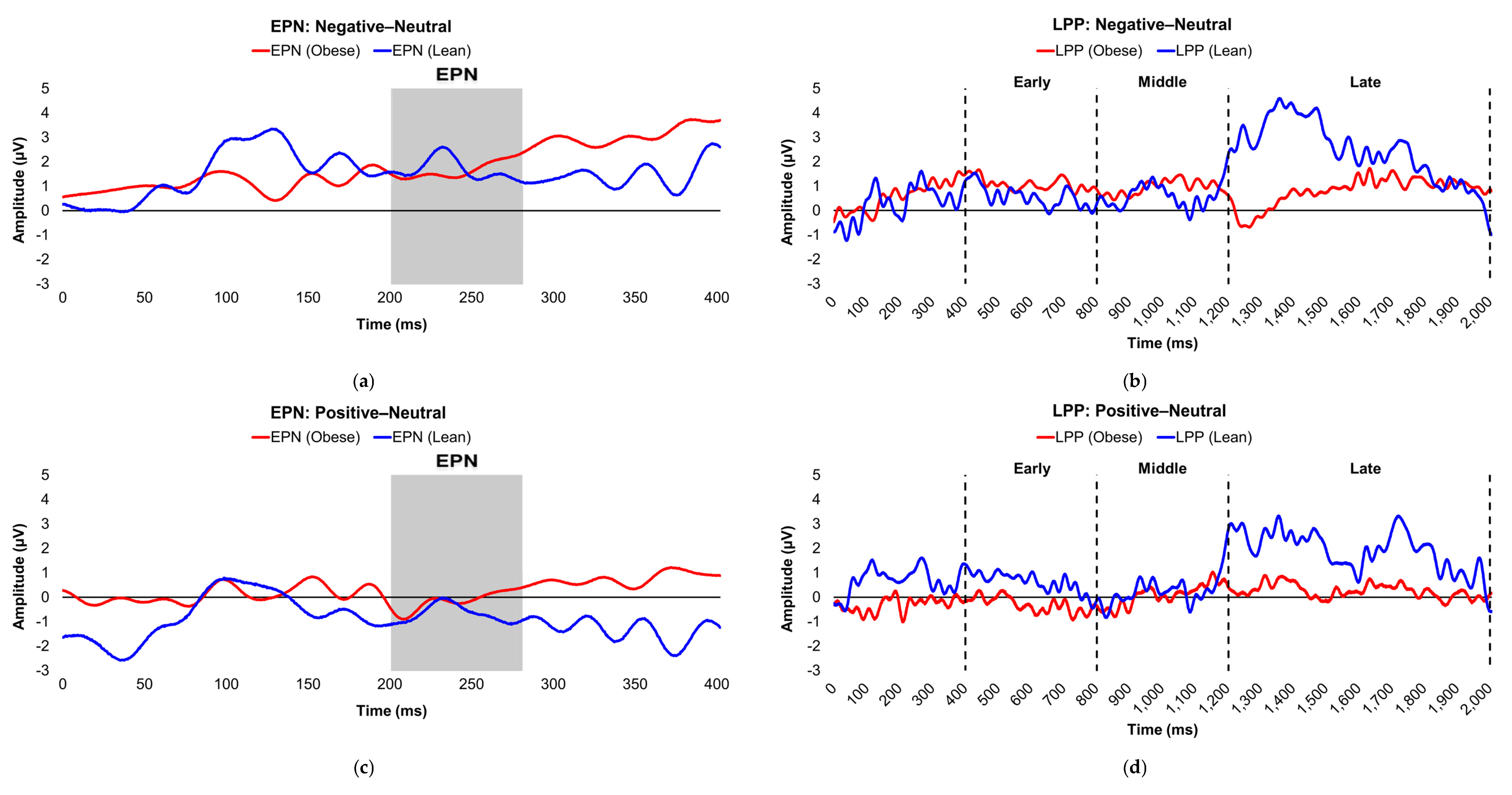
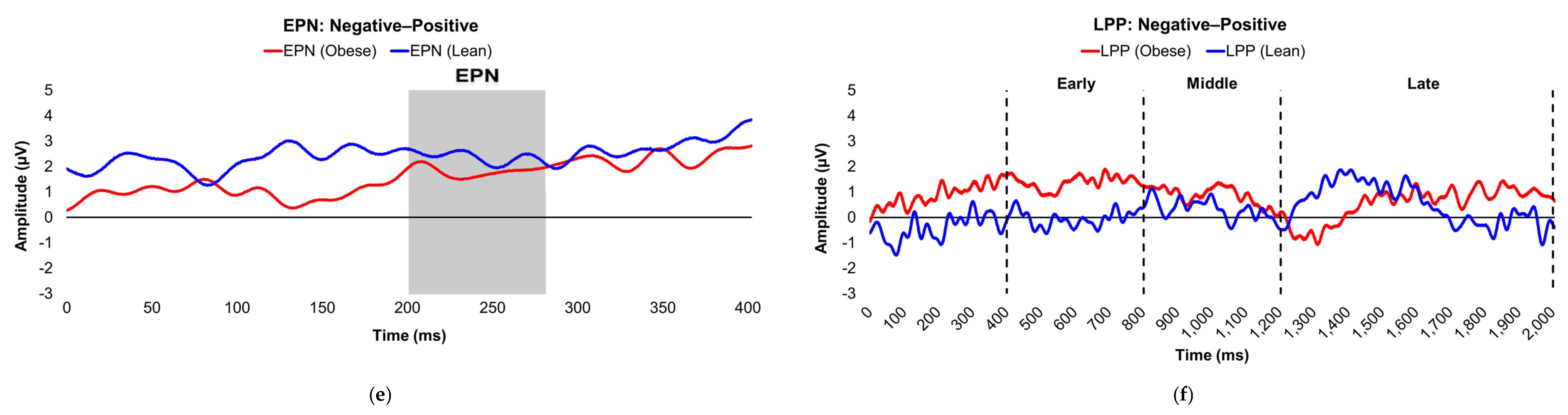
Figure 3.
Line graphs show the comparisons of the differenced grand-mean averaged EPN (left) and LPP (right) waveforms in the contrasted picture conditions (i.e., Negative minus Neutral (a–b), Positive minus Neutral (c–d), and Negative minus Positive (e–f) EPN and LPP waveforms) between insulin-sensitive (HOMA-IR values of <2.0, in blue) versus insulin-resistant (HOMA-IR values of ≥2.0, in red) subjects. Amplitude was measured in microvolts (µV); time was measured in milliseconds. EPN = early posterior negativity; IR = insulin-resistant; IS = insulin-sensitive; LPP = late positive potential; ms = milliseconds. Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively.
Figure 3.
Line graphs show the comparisons of the differenced grand-mean averaged EPN (left) and LPP (right) waveforms in the contrasted picture conditions (i.e., Negative minus Neutral (a–b), Positive minus Neutral (c–d), and Negative minus Positive (e–f) EPN and LPP waveforms) between insulin-sensitive (HOMA-IR values of <2.0, in blue) versus insulin-resistant (HOMA-IR values of ≥2.0, in red) subjects. Amplitude was measured in microvolts (µV); time was measured in milliseconds. EPN = early posterior negativity; IR = insulin-resistant; IS = insulin-sensitive; LPP = late positive potential; ms = milliseconds. Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively.
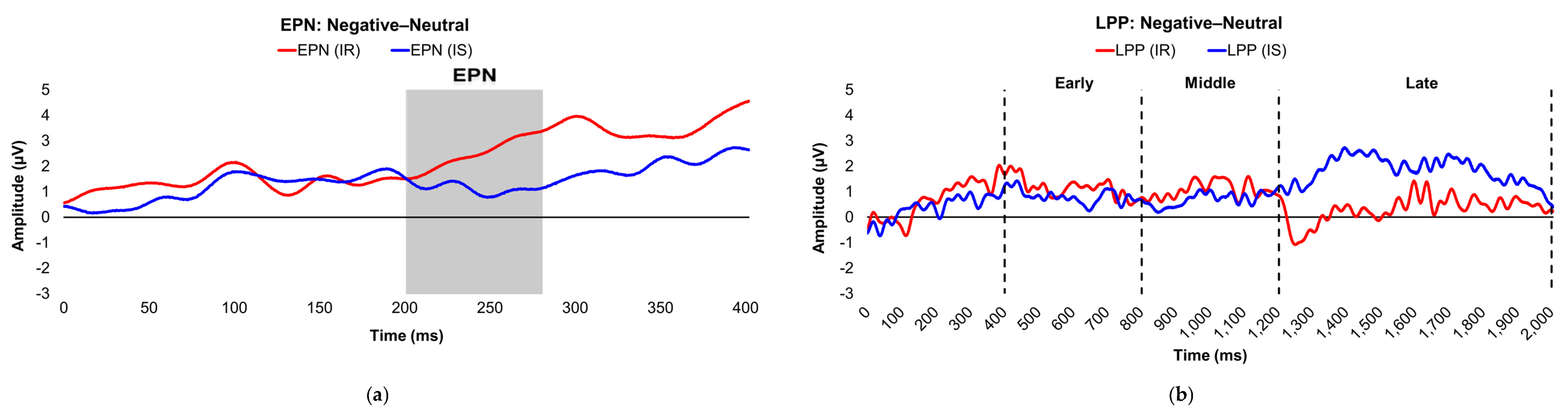
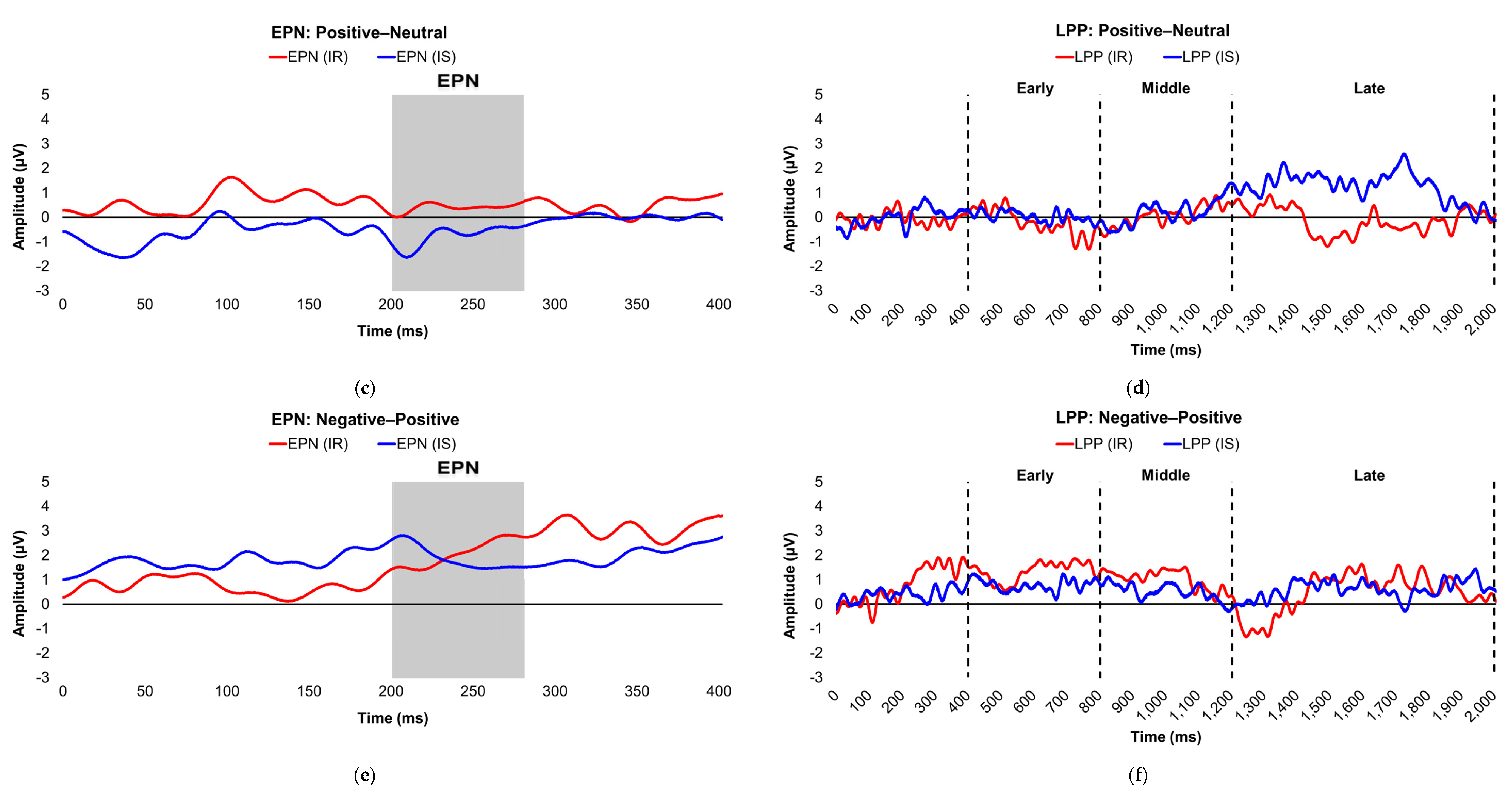
Figure 4.
Interaction plots depict how body fat percentage (a) and HOMA-IR (b) moderated the relationships between the voltage amplitudes of the LPP component during the late latency window and mean valence ratings in the contrasted Negative–Neutral picture condition. Predictor (late-window LPP component voltage amplitudes) and moderator (BF%, HOMA-IR values) variables were tested as continuous variables but are shown as tertiles for visualization. BF% = body fat percentage; HOMA-IR = homeostatic model assessment for insulin resistance; LPP = late positive potential; ms = milliseconds. * and *** = p’s≤0.05 and ≤0.005, respectively. Amplitude deflections (lesser, average, greater) and BF% or HOMA-IR levels (low, medium, high) respectively reflect values at the 16th, 50th, and 84th percentiles of the total sample. Valence ratings represent the mean ratings of the magnitude of pleasantness or unpleasantness of images for each valence condition, where 1=“very positive,” 2=“somewhat positive,” 3=“somewhat negative,” and 4=“very negative,” which were subsequently contrasted as the difference between the mean valence ratings of neutrally-valenced pictures from the mean valence ratings of negatively-valenced pictures (i.e., Negative minus Neutral valence ratings). Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms, respectively. For subjects with low BF% and low-to-medium HOMA-IR values, greater (i.e., more positive) LPP amplitudes during the late latency window were linked to less negative valence ratings in response to unpleasant versus neutral pictures.
Figure 4.
Interaction plots depict how body fat percentage (a) and HOMA-IR (b) moderated the relationships between the voltage amplitudes of the LPP component during the late latency window and mean valence ratings in the contrasted Negative–Neutral picture condition. Predictor (late-window LPP component voltage amplitudes) and moderator (BF%, HOMA-IR values) variables were tested as continuous variables but are shown as tertiles for visualization. BF% = body fat percentage; HOMA-IR = homeostatic model assessment for insulin resistance; LPP = late positive potential; ms = milliseconds. * and *** = p’s≤0.05 and ≤0.005, respectively. Amplitude deflections (lesser, average, greater) and BF% or HOMA-IR levels (low, medium, high) respectively reflect values at the 16th, 50th, and 84th percentiles of the total sample. Valence ratings represent the mean ratings of the magnitude of pleasantness or unpleasantness of images for each valence condition, where 1=“very positive,” 2=“somewhat positive,” 3=“somewhat negative,” and 4=“very negative,” which were subsequently contrasted as the difference between the mean valence ratings of neutrally-valenced pictures from the mean valence ratings of negatively-valenced pictures (i.e., Negative minus Neutral valence ratings). Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms, respectively. For subjects with low BF% and low-to-medium HOMA-IR values, greater (i.e., more positive) LPP amplitudes during the late latency window were linked to less negative valence ratings in response to unpleasant versus neutral pictures.
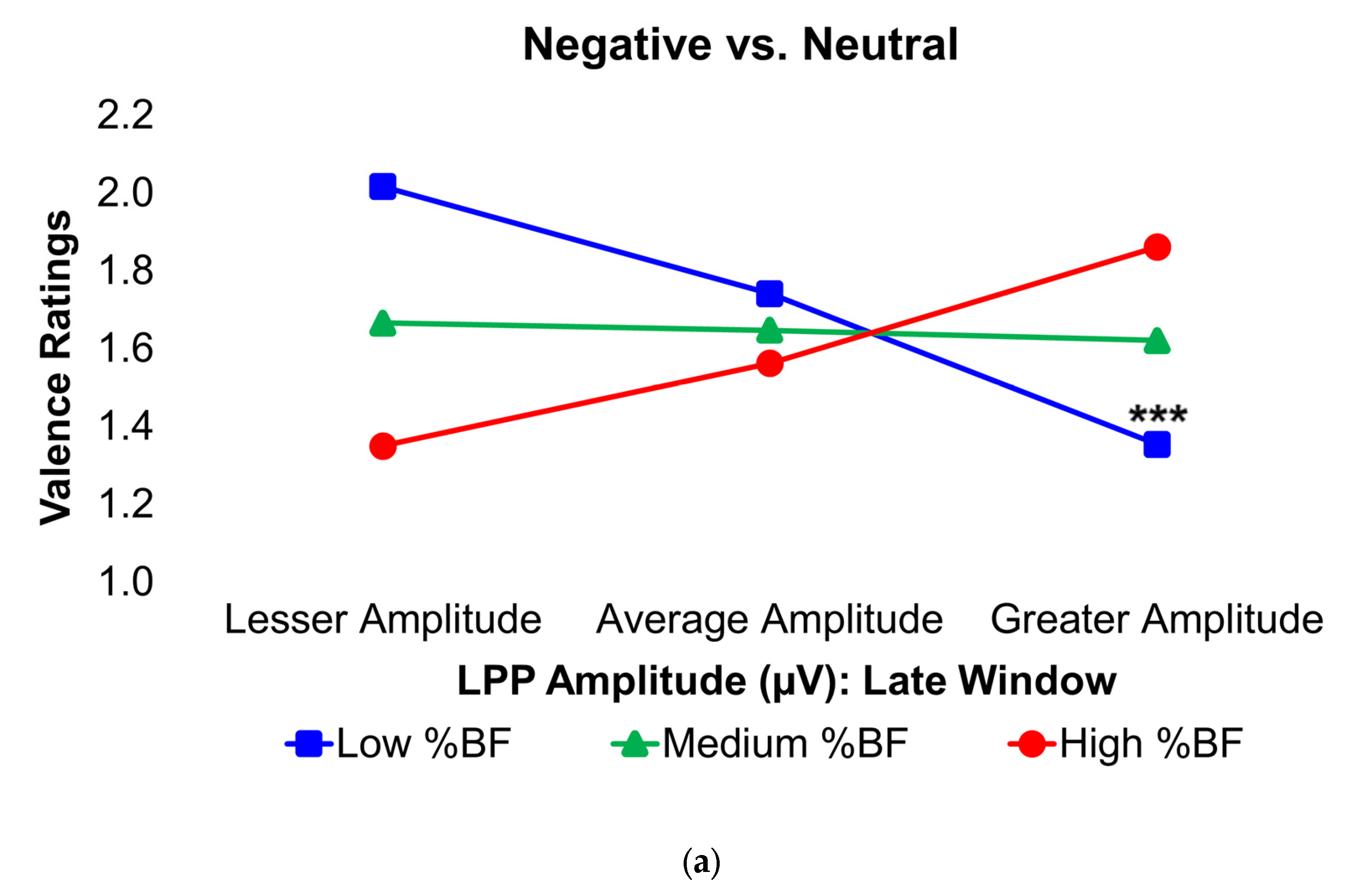
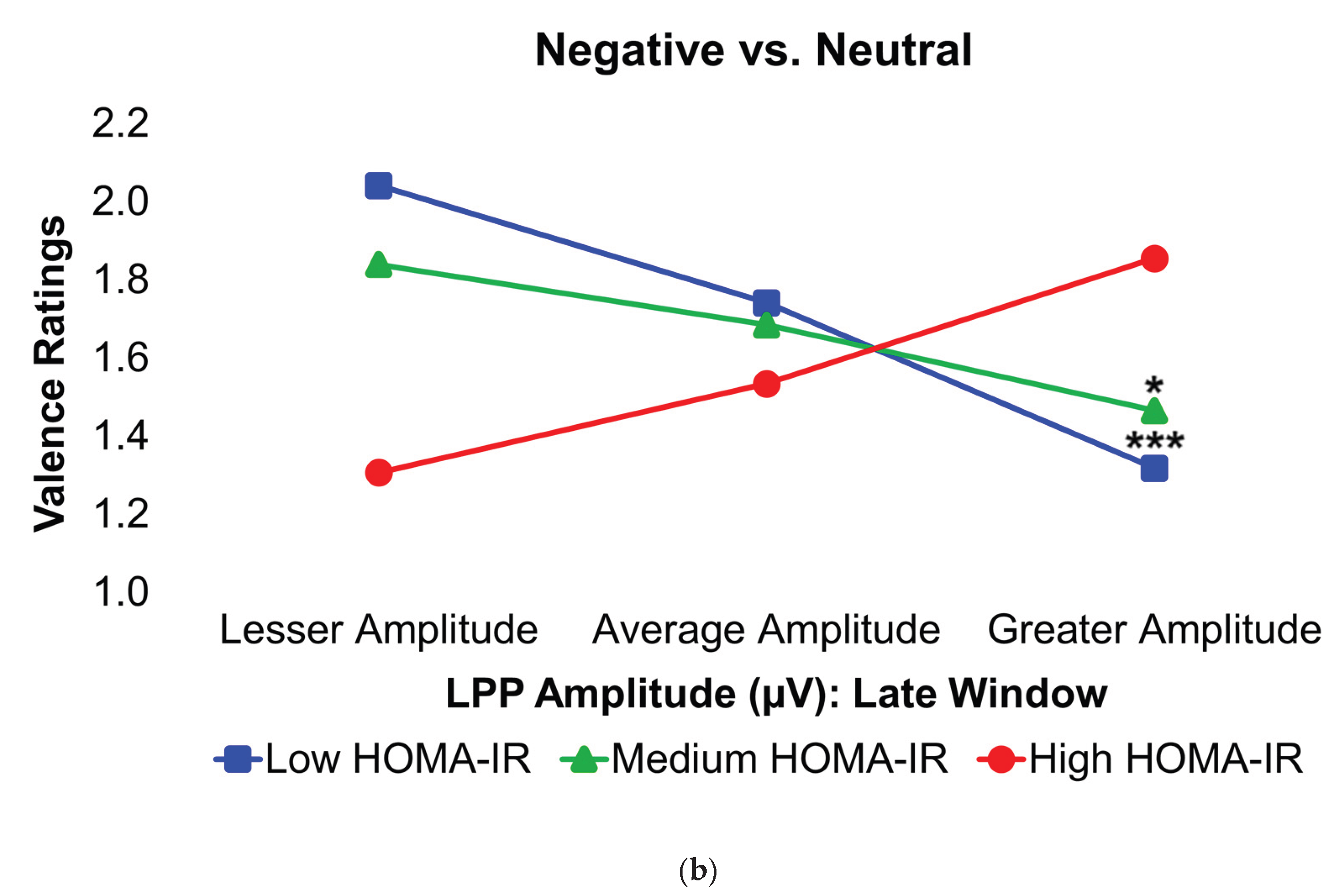
Table 1.
Participant characteristic comparisons by adiposity and insulin groups.
| Adiposity | Insulin | ||||||
|---|---|---|---|---|---|---|---|
| Data (unit) | Total (n=30) | Lean (n=8) | Obese (n=22) | t value/Chi-square | Insulin-sensitive (n=18) | Insulin-resistant (n=12) | t value/Chi-square |
| Age (years) | 25.7 (5.3) | 23.3 (4.1) | 26.5 (5.5) | t= -1.54 | 24.9 (5.6) | 26.8 (4.9) | t= -0.98 |
| Sex (n females (%)) | 15 (50.0%) | 3 (37.5%) | 12 (54.5%) | χ2= 0.68 | 8 (44.4%) | 7 (58.3%) | χ2= 0.56 |
| Activity Level (n (%)) | χ2= 4.18 | χ2= 5.63* | |||||
| Sedentary/Low Active | 20 (66.7%) | 3 (37.5%) | 17 (77.3%) | 9 (50.0%) | 11 (91.7%) | ||
| Active/Very Active | 10 (33.3%) | 5 (62.5%) | 5 (22.7%) | 9 (50.0%) | 1 (8.3%) | ||
| Race/Ethnicity (n (%)) | χ2= 3.62 | χ2= 5.17 | |||||
| White | 24 (80.0%) | 5 (62.5%) | 19 (86.4%) | 13 (72.2%) | 11 (91.7%) | ||
| Asian | 5 (16.7%) | 3 (37.5%) | 2 (9.1%) | 5 (27.8%) | 0 (0.0%) | ||
| Hispanic/Latinx | 1 (3.3%) | 0 (0.0%) | 1 (4.5%) | 0 (0.0%) | 1 (8.3%) | ||
| Black | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| BF% (DEXA) | 37.1 (10.3) | 24.8 (4.7) | 41.6 (7.9) | t= -5.64*** | 31.6 (8.5) | 45.5 (6.7) | t= -4.76*** |
| BMI | 29.3 (8.2) | 21.0 (1.6) | 32.2 (7.5) | t= -6.94*** | 24.5 (5.3) | 36.4 (6.4) | t= -5.74*** |
| BP, diastolic (kPa) | 10.2 (1.7) | 9.6 (2.0) | 10.5 (1.5) | t= -1.26 | 9.7 (1.6) | 11.1 (1.4) | t= -2.33* |
| BP, systolic (kPa) | 16.2 (2.1) | 16.6 (2.8) | 16.0 (1.7) | t= 0.68 | 16.0 (2.4) | 16.6 (1.3) | t= -0.75 |
| Glucose (mmol/L), fasting | 5.0 (0.5) | 4.7 (0.4) | 5.1 (0.4) | t= -2.38* | 4.9 (0.5) | 5.2 (0.5) | t= -1.50 |
| Height (meters) | 1.7 (0.1) | 1.8 (0.1) | 1.7 (0.1) | t= 0.43 | 1.7 (0.1) | 1.7 (0.1) | t= -0.37 |
| Hemoglobin A1c (%) | 5.4 (0.2) | 5.3 (0.1) | 5.4 (0.2) | t= -1.05 | 5.3 (0.2) | 5.4 (0.2) | t= -1.36 |
| HOMA-IR | 2.6 (2.5) | 0.9 (0.3) | 3.3 (2.7) | t= -4.24*** | 1.2 (0.4) | 4.9 (2.8) | t= -8.07*** |
| Insulin (pmol/L), fasting | 69.3 (63.0) | 25.2 (8.5) | 85.4 (66.7) | t= -4.14*** | 31.8 (9.5) | 125.7 (67.5) | t= -4.78*** |
Values are Mean (Standard Deviation) unless otherwise indicated. BF% = body fat percentage; BMI = body mass index; BP=Blood pressure; DEXA = dual-energy X-ray absorptiometry; hemoglobin A1c = glycated hemoglobin; HOMA-IR = homeostatic model assessment for insulin resistance. * and *** = p’s≤0.05 and ≤0.005, respectively. For the stratified adiposity groups, t-values, chi-square, and Fisher’s exact values reflect differences between participants with and without obesity based on a body fat percentage of ≥25% (males) and ≥35% (females) versus <25% (males) and <35% (females), respectively. For the stratified insulin groups, t-values, chi-square, and Fisher’s exact values reflect differences between participants with insulin resistance and insulin sensitivity based on HOMA-IR values of ≥2.0 versus <2.0, respectively. 3.2. Event-Related Potentials.
Table 2.
Comparisons of event-related potentials by adiposity and insulin groups.
| Adiposity | Insulin | ||||||
|---|---|---|---|---|---|---|---|
| ERP Components | Total | Lean | Obese | t value | Insulin-sensitive | Insulin-resistant | t value |
| Negative–Neutral | |||||||
| EPN | 1.7 (2.7) | 1.7 (3.0) | 1.6 (2.6) | t= 0.04 | 1.1 (2.6) | 2.5 (2.6) | t= -1.37 |
| Early LPP | 0.9 (1.9) | 0.6 (2.5) | 1.1 (1.7) | t= -0.64 | 0.8 (2.1) | 1.2 (1.7) | t= -0.47 |
| Middle LPP | 0.8 (2.2) | 0.6 (2.2) | 0.9 (2.2) | t= -0.38 | 0.7 (2.1) | 1.1 (2.4) | t= -0.45 |
| Late LPP | 1.2 (1.8) | 2.4 (2.3) | 0.8 (1.5) | t= 2.31* | 1.8 (1.9) | 0.3 (1.3) | t= 2.37* |
| Positive–Neutral | |||||||
| EPN | -0.3 (2.6) | -0.7 (2.1) | -0.2 (2.8) | t= -0.49 | -0.8 (2.5) | 0.4 (2.6) | t= -1.22 |
| Early LPP | -0.1 (2.3) | 0.6 (1.7) | -0.3 (2.5) | t= 0.96 | 0.0 (2.3) | -0.2 (2.5) | t= 0.26 |
| Middle LPP | 0.1 (2.7) | 0.3 (2.0) | 0.1 (2.9) | t= 0.17 | 0.2 (2.5) | 0.0 (3.1) | t= 0.13 |
| Late LPP | 0.7 (2.2) | 1.9 (2.1) | 0.3 (2.2) | t= 1.87 | 1.2 (1.9) | -0.1 (2.6) | t= 1.69 |
| Negative–Positive | |||||||
| EPN | 2.0 (2.7) | 2.4 (3.1) | 1.8 (2.6) | t= 0.50 | 1.9 (2.9) | 2.1 (2.5) | t= -0.18 |
| Early LPP | 1.0 (1.6) | 0.0 (1.6) | 1.4 (1.4) | t= -2.38* | 0.8 (1.7) | 1.3 (1.4) | t= -0.97 |
| Middle LPP | 0.7 (2.0) | 0.3 (1.2) | 0.9 (2.2) | t= -0.65 | 0.5 (1.9) | 1.0 (2.2) | t= -0.68 |
| Late LPP | 0.5 (2.0) | 0.5 (2.0) | 0.5 (2.0) | t= 0.03 | 0.6 (2.0) | 0.4 (2.0) | t= 0.19 |
Values are Mean (Standard Deviation) unless otherwise indicated. Amplitude was measured in microvolts (µV). EPN = early posterior negativity; ERP = event-related potential; LPP = late positive potential. * = p≤0.05. In each contrasted valence condition, the mean ERP amplitudes of a neutrally- or oppositely-valenced condition were subtracted from the mean ERP amplitudes of an emotionally-valenced condition (i.e., negative or positive) as follows: 1) Negative–Neutral; 2) Positive–Neutral; and 3) Negative–Positive. Early, middle, and late latency windows of the LPP component = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively. For the stratified adiposity groups, t-values reflect differences between participants with and without obesity based on a body fat percentage of ≥25% (males) and ≥35% (females) versus <25% (males) and <35% (females), respectively. For the stratified insulin groups, t-values reflect differences between participants with insulin resistance and insulin sensitivity based on HOMA-IR values of ≥2.0 versus <2.0, respectively.
Table 3.
Comparisons of affective processing task scores by adiposity and insulin groups.
| Adiposity | Adiposity | ||||||
|---|---|---|---|---|---|---|---|
| Affective Processing Parameters | Total | Lean | Obese | t value | Insulin-sensitive | Insulin-resistant | t value |
| Rating (Negative–Neutral) | 1.6 (0.4) | 1.5 (0.5) | 1.6 (0.3) | t= -0.37 | 1.6 (0.4) | 1.5 (0.3) | t= 0.57 |
| RT (Negative–Neutral) | 2.6 (206.1) | -1.3 (154.2) | 4.0 (225.2) | t= -0.06 | -59.0 (182.9) | 95.0 (211.6) | t= -2.12* |
| Rating (Positive–Neutral) | -0.4 (0.2) | -0.5 (0.2) | -0.4 (0.2) | t= -1.26 | -0.5 (0.2) | -0.3 (0.2) | t= -0.91 |
| RT (Positive–Neutral) | 25.5 (174.4) | 58.9 (213.0) | 13.4 (162.2) | t= 0.63 | 7.8 (213.8) | 52.1 (91.1) | t= -0.78 |
| Rating (Negative–Positive) | 2.7 (0.2) | 2.5 (0.3) | 2.7 (0.2) | t= -2.39* | 2.6 (0.2) | 2.8 (0.2) | t= -1.64 |
| RT (Negative–Positive) | -17.8 (216.8) | -30.8 (156.0) | -13.0 (238.2) | t= -0.20 | -53.7 (184.3) | 36.2 (257.3) | t= -1.12 |
Values are Mean (Standard Deviation) unless otherwise indicated. Reaction time was measured in milliseconds. RT = reaction time. * = p≤0.05. In each contrasted valence condition, the affective processing parameters of a neutrally- or oppositely-valenced condition were subtracted from the affective processing parameters of an emotionally-valenced condition (i.e., negative or positive) as follows: 1) Negative–Neutral; 2) Positive–Neutral; and 3) Negative–Positive. For the contrasted oppositely-valenced picture condition, valence ratings were calculated as: Negative–(4–Positive). For the stratified adiposity groups, t-values reflect differences between participants with and without obesity based on a body fat percentage of ≥25% (males) and ≥35% (females) versus <25% (males) and <35% (females), respectively. For the stratified insulin groups, t-values reflect differences between participants with insulin resistance and insulin sensitivity based on HOMA-IR values of ≥2.0 versus <2.0, respectively.
Table 4.
Correlation matrix of event-related potentials and affective processing parameters.
| Negative–Neutral | Positive–Neutral | Negative–Positive | ||||
|---|---|---|---|---|---|---|
| ERP Components | Valence Rating | Reaction Time | Valence Rating | Reaction Time | Valence Rating | Reaction Time |
| Negative–Neutral | ||||||
| EPN | -0.15 | 0.11 | - | - | - | - |
| Early LPP | 0.08 | 0.08 | - | - | - | - |
| Middle LPP | -0.01 | 0.16 | - | - | - | - |
| Late LPP | -0.36 | 0.06 | - | - | - | - |
| Positive–Neutral | ||||||
| EPN | - | - | -0.27 | 0.15 | - | - |
| Early LPP | - | - | -0.06 | 0.09 | - | - |
| Middle LPP | - | - | -0.04 | 0.14 | - | - |
| Late LPP | - | - | -0.31 | 0.01 | - | - |
| Negative–Positive | ||||||
| EPN | - | - | - | - | 0.19 | -0.38* |
| Early LPP | - | - | - | - | 0.28 | -0.19 |
| Middle LPP | - | - | - | - | 0.31 | -0.08 |
| Late LPP | - | - | - | - | -0.08 | -0.15 |
Values show bivariate Pearson correlation coefficients between the independent variables (EPN and LPP amplitude deflections) and the dependent variables (valence ratings, reaction times) for each contrasted condition of the International Affective Picture System task. Amplitude was measured in microvolts (µV); reaction time was measured in milliseconds. EPN = early posterior negativity; ERP = event-related potential; LPP = late positive potential. * = p≤0.05. In each contrasted valence condition, the mean ERP voltage amplitudes and affective processing parameters of a neutrally- or oppositely-valenced condition were subtracted from the mean ERP amplitudes and affective processing parameters of an emotionally-valenced condition (i.e., negative or positive) as follows: 1) Negative–Neutral; 2) Positive–Neutral; and 3) Negative–Positive. For the contrasted oppositely-valenced picture condition, valence ratings were calculated as: Negative–(4–Positive). Early, middle, and late LPP latency windows = 400–800 ms, 800–1,200 ms, and 1,200–2,000 ms post-stimulus onset, respectively.
Table 5.
Hierarchical moderated regression results for Negative vs. Neutral valence ratings.
| Step 1 | Step 2 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | β | t | R2 | F | p | β | t | ΔR2 | ΔF | p | ||
| Model 1 | 0.03 | 0.47 | 0.63 | 0.00 | 0.01 | 0.92 | ||||||
| EPN | -0.15 | -0.79 | -0.15 | -0.78 | ||||||||
| BF% | 0.10 | 0.53 | 0.10 | 0.52 | ||||||||
| EPN*BF% | 0.02 | 0.10 | ||||||||||
| Model 2 | 0.02 | 0.33 | 0.73 | 0.00 | 0.01 | 0.93 | ||||||
| EPN | -0.15 | -0.81 | -0.15 | -0.77 | ||||||||
| HOMA-IR | -0.01 | -0.06 | -0.01 | -0.07 | ||||||||
| EPN*HOMA-IR | 0.02 | 0.09 | ||||||||||
| Model 3 | 0.02 | 0.28 | 0.76 | 0.00 | 0.16 | 0.69 | ||||||
| eLPP | 0.10 | 0.51 | 0.11 | 0.57 | ||||||||
| BF% | 0.12 | 0.62 | 0.13 | 0.67 | ||||||||
| eLPP*BF% | 0.08 | 0.40 | ||||||||||
| Model 4 | 0.01 | 0.09 | 0.91 | 0.01 | 0.13 | 0.73 | ||||||
| eLPP | 0.08 | 0.43 | 0.09 | 0.46 | ||||||||
| HOMA-IR | 0.00 | -0.01 | -0.01 | -0.05 | ||||||||
| eLPP*HOMA-IR | 0.07 | 0.36 | ||||||||||
| Model 5 | 0.01 | 0.16 | 0.86 | 0.05 | 1.28 | 0.27 | ||||||
| mLPP | -0.02 | -0.10 | 0.00 | 0.01 | ||||||||
| BF% | 0.11 | 0.56 | 0.15 | 0.76 | ||||||||
| mLPP*BF% | 0.22 | 1.13 | ||||||||||
| Model 6 | 0.00 | 0.00 | 1.00 | 0.06 | 1.65 | 0.21 | ||||||
| mLPP | -0.01 | -0.06 | -0.04 | -0.21 | ||||||||
| HOMA-IR | 0.01 | 0.03 | -0.09 | -0.42 | ||||||||
| mLPP*HOMA-IR | 0.26 | 1.29 | ||||||||||
| Model 7 | 0.13 | 2.06 | 0.15 | 0.25*** | 10.23*** | 0.004 | ||||||
| lLPP | -0.38 | -1.94 | -0.05 | -0.24 | ||||||||
| BF% | -0.06 | -0.28 | -0.08 | -0.46 | ||||||||
| lLPP*BF% | 0.60*** | 3.20*** | ||||||||||
| Model 8 | 0.14 | 2.20 | 0.13 | 0.24*** | 9.89*** | 0.004 | ||||||
| lLPP | -0.40 | -2.12 | -0.20 | -1.18 | ||||||||
| HOMA-IR | -0.12 | -0.63 | -0.11 | -0.69 | ||||||||
| lLPP*HOMA-IR | 0.52*** | 3.14*** | ||||||||||
Table displays the results of each step of the hierarchical moderated regression analyses, which tested whether EPN or LPP voltage amplitudes and BF% or HOMA-IR moderated the mean valence ratings after viewing negatively-valenced versus neutrally-valenced pictures. BF% = body fat percentage; eLPP = late positive potential in the early latency window; EPN = early posterior negativity; HOMA-IR = homeostatic model assessment for insulin resistance; lLPP = late positive potential in the late latency window; mLPP = late positive potential in the middle latency window. *** = p≤0.005. β shows standardized regression coefficients. Only statistically significant covariates (p≤0.10) were included in each model.
Table 6.
Hierarchical moderated regression results for Negative vs. Neutral reaction times.
| Step 1 | Step 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | β | t | R2 | F | p | β | t | ΔR2 | ΔF | p |
| Model 1 | 0.14 | 1.38 | 0.27 | 0.02 | 0.61 | 0.44 | ||||
| EPN | 0.10 | 0.56 | 0.12 | 0.64 | ||||||
| BF% | 0.02 | 0.09 | 0.02 | 0.10 | ||||||
| Age | 0.35 | 1.90 | 0.36 | 1.95 | ||||||
| EPN*BF% | -0.15 | -0.78 | ||||||||
| Model 2 | 0.15 | 2.37 | 0.11 | 0.02 | 0.75 | 0.40 | ||||
| EPN | 0.15 | 0.85 | 0.11 | 0.63 | ||||||
| HOMA-IR | 0.37 | 2.08 | 0.32 | 1.76 | ||||||
| Age | 0.32 | 1.73 | ||||||||
| EPN*HOMA-IR | -0.16 | -0.86 | ||||||||
| Model 3 | 0.16 | 1.65 | 0.20 | 0.00 | 0.01 | 0.91 | ||||
| eLPP | 0.19 | 1.00 | 0.18 | 0.93 | ||||||
| BF% | 0.03 | 0.16 | 0.02 | 0.13 | ||||||
| Age | 0.40 | 2.14 | 0.40 | 2.10 | ||||||
| eLPP*BF% | -0.02 | -0.12 | ||||||||
| Model 4 | 0.32 | 2.91 | 0.04 | 0.09 | 3.38 | 0.08 | ||||
| eLPP | 0.11 | 0.61 | 0.12 | 0.69 | ||||||
| HOMA-IR | 0.38 | 2.09 | 0.30 | 1.75 | ||||||
| Age | 0.32 | 1.79 | 0.36 | 2.02 | ||||||
| Race/Ethnicity | 0.32 | 1.83 | ||||||||
| eLPP*HOMA-IR | -0.31 | -1.84 | ||||||||
| Model 5 | 0.18 | 1.93 | 0.15 | 0.00 | 0.11 | 0.74 | ||||
| mLPP | 0.24 | 1.32 | 0.23 | 1.26 | ||||||
| BF% | -0.01 | -0.07 | -0.02 | -0.13 | ||||||
| Age | 0.41 | 2.21 | 0.41 | 2.19 | ||||||
| mLPP*BF% | -0.06 | -0.33 | ||||||||
| Model 6 | 0.34 | 3.22 | 0.03 | 0.04 | 1.36 | 0.26 | ||||
| mLPP | 0.19 | 1.11 | 0.22 | 1.30 | ||||||
| HOMA-IR | 0.37 | 2.05 | 0.42 | 2.29 | ||||||
| Age | 0.33 | 1.92 | 0.38 | 2.15 | ||||||
| Race/Ethnicity | 0.33 | 1.93 | 0.31 | 1.81 | ||||||
| mLPP*HOMA-IR | -0.21 | -1.17 | ||||||||
| Model 7 | 0.24 | 1.95 | 0.13 | 0.13 | 4.75 | 0.04 | ||||
| lLPP | 0.31 | 1.42 | 0.09 | 0.40 | ||||||
| BF% | 0.25 | 1.13 | 0.28 | 1.39 | ||||||
| Age | 0.37 | 2.11 | 0.39 | 2.34 | ||||||
| Race/Ethnicity | 0.37 | 1.79 | 0.42 | 2.15 | ||||||
| lLPP*BF% | -0.44 | -2.18 | ||||||||
| Model 8 | 0.44*** | 4.92*** | 0.005 | 0.12 | 6.33 | 0.02 | ||||
| lLPP | 0.43 | 2.44 | 0.28 | 1.63 | ||||||
| HOMA-IR | 0.59*** | 3.28*** | 0.58*** | 3.52*** | ||||||
| Age | 0.29 | 1.91 | 0.28 | 2.02 | ||||||
| Race/Ethnicity | 0.52 | 2.97 | 0.49** | 3.07** | ||||||
| lLPP*HOMA-IR | -0.37 | -2.52 | ||||||||
Table displays the results of each step of the hierarchical moderated regression analyses, which tested whether EPN or LPP voltage amplitudes and BF% or HOMA-IR moderated the mean reaction times after viewing negatively-valenced versus neutrally-valenced pictures. BF% = body fat percentage; eLPP = early latency late positive potential; EPN = early posterior negativity; HOMA-IR = homeostatic model assessment for insulin resistance; lLPP = late latency late positive potential; mLPP = middle latency late positive potential. ** and *** = p’s≤0.0063 and ≤0.005, respectively. β shows standardized regression coefficients. Only statistically significant covariates (p≤0.10) were included in each model.
Table 7.
Hierarchical moderated regression results for Positive vs. Neutral valence ratings.
| Step 1 | Step 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | β | t | R2 | F | p | β | t | ΔR2 | ΔF | p |
| Model 1 | 0.44*** | 6.82*** | 0.002 | 0.00 | 0.17 | 0.69 | ||||
| EPN | -0.27 | -1.85 | -0.29 | -1.87 | ||||||
| BF% | 0.32 | 2.11 | 0.32 | 2.05 | ||||||
| Race/Ethnicity | 0.62*** | 4.02*** | 0.61*** | 3.91*** | ||||||
| EPN*BF% | 0.06 | 0.41 | ||||||||
| Model 2 | 0.41*** | 6.03*** | 0.003 | 0.00 | 0.08 | 0.78 | ||||
| EPN | -0.32 | -2.10 | -0.32 | -2.07 | ||||||
| HOMA-IR | 0.27 | 1.70 | 0.27 | 1.66 | ||||||
| Race/Ethnicity | 0.61*** | 3.84*** | 0.61*** | 3.72*** | ||||||
| EPN*HOMA-IR | 0.04 | 0.29 | ||||||||
| Model 3 | 0.45*** | 5.09*** | 0.004 | 0.00 | 0.00 | 1.00 | ||||
| eLPP | -0.15 | -0.93 | -0.15 | -0.86 | ||||||
| BF% | 0.32 | 1.99 | 0.32 | 1.94 | ||||||
| Age | -0.28 | -1.85 | -0.28 | -1.82 | ||||||
| Race/Ethnicity | 0.62*** | 3.99*** | 0.62*** | 3.91*** | ||||||
| eLPP*BF% | 0.00 | -0.01 | ||||||||
| Model 4 | 0.43** | 4.65** | 0.006 | 0.00 | 0.00 | 0.97 | ||||
| eLPP | -0.23 | -1.46 | -0.23 | -1.39 | ||||||
| HOMA-IR | 0.28 | 1.68 | 0.28 | 1.64 | ||||||
| Age | -0.32 | -2.00 | -0.32 | -1.96 | ||||||
| Race/Ethnicity | 0.64*** | 3.90*** | 0.64*** | 3.81*** | ||||||
| eLPP*HOMA-IR | 0.01 | 0.04 | ||||||||
| Model 5 | 0.45*** | 5.01*** | 0.004 | 0.02 | 1.00 | 0.33 | ||||
| mLPP | -0.12 | -0.81 | 0.04 | 0.23 | ||||||
| BF% | 0.35 | 2.24 | 0.51 | 2.55 | ||||||
| Age | -0.27 | -1.78 | ||||||||
| Race/Ethnicity | 0.62*** | 3.97*** | 0.67*** | 4.13*** | ||||||
| Physical Activity | 0.36 | 1.81 | ||||||||
| mLPP*BF% | -0.17 | -1.00 | ||||||||
| Model 6 | 0.32 | 4.11 | 0.02 | 0.05 | 2.08 | 0.16 | ||||
| mLPP | -0.17 | -1.10 | 0.03 | 0.17 | ||||||
| HOMA-IR | 0.29 | 1.76 | 0.46 | 2.32 | ||||||
| Age | -0.29 | -1.83 | ||||||||
| Race/Ethnicity | 0.62*** | 3.77*** | 0.76*** | 4.24*** | ||||||
| Physical Activity | 0.39 | 1.94 | ||||||||
| Sex | -0.33 | -1.91 | ||||||||
| mLPP*HOMA-IR | -0.25 | -1.44 | ||||||||
| Model 7 | 0.54*** | 5.59*** | 0.001 | 0.01 | 0.27 | 0.61 | ||||
| lLPP | -0.29 | -1.76 | -0.31 | -1.81 | ||||||
| BF% | 0.42 | 2.25 | 0.39 | 1.99 | ||||||
| Age | -0.29 | -1.94 | -0.28 | -1.85 | ||||||
| Physical Activity | 0.30 | 1.76 | 0.32 | 1.79 | ||||||
| Race/Ethnicity | 0.61*** | 4.00*** | 0.59*** | 3.72*** | ||||||
| lLPP*BF% | 0.08 | 0.52 | ||||||||
| Model 8 | 0.47*** | 5.46*** | 0.003 | 0.00 | 0.12 | 0.73 | ||||
| lLPP | -0.32 | -2.03 | -0.30 | -1.80 | ||||||
| HOMA-IR | 0.21 | 1.30 | 0.22 | 1.32 | ||||||
| Age | -0.35 | -2.24 | -0.35 | -2.22 | ||||||
| Race/Ethnicity | 0.54*** | 3.44*** | 0.54*** | 3.39*** | ||||||
| lLPP*HOMA-IR | -0.05 | -0.35 | ||||||||
Table displays the results of each step of the hierarchical moderated regression analyses, which tested whether EPN or LPP voltage amplitudes and BF% or HOMA-IR moderated the mean valence ratings after viewing positively-valenced versus neutrally-valenced pictures. BF% = body fat percentage; eLPP = early latency late positive potential; EPN = early posterior negativity; HOMA-IR = homeostatic model assessment for insulin resistance; lLPP = late latency late positive potential; mLPP = middle latency late positive potential. ** and *** = p’s≤0.0063 and ≤0.005, respectively. β shows standardized regression coefficients. Only statistically significant covariates (p≤0.10) were included in each model.
Table 8.
Hierarchical moderated regression results for Positive vs. Neutral reaction times.
| Step 1 | Step 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | β | t | R2 | F | p | β | t | ΔR2 | ΔF | p |
| Model 1 | 0.04 | 0.39 | 0.76 | 0.07 | 2.00 | 0.17 | ||||
| EPN | 0.15 | 0.77 | 0.21 | 1.08 | ||||||
| BF% | -0.09 | -0.47 | -0.08 | -0.44 | ||||||
| EPN*BF% | -0.27 | -1.41 | ||||||||
| Model 2 | 0.03 | 0.37 | 0.70 | 0.01 | 0.38 | 0.54 | ||||
| EPN | 0.16 | 0.82 | 0.16 | 0.84 | ||||||
| HOMA-IR | -0.07 | -0.36 | -0.07 | -0.35 | ||||||
| EPN*HOMA-IR | -0.12 | -0.62 | ||||||||
| Model 3 | 0.01 | 0.18 | 0.84 | 0.00 | 0.01 | 0.93 | ||||
| eLPP | 0.07 | 0.33 | 0.06 | 0.28 | ||||||
| BF% | -0.07 | -0.35 | -0.07 | -0.35 | ||||||
| eLPP*BF% | 0.02 | 0.09 | ||||||||
| Model 4 | 0.01 | 0.13 | 0.88 | 0.02 | 0.42 | 0.53 | ||||
| eLPP | 0.09 | 0.44 | 0.12 | 0.58 | ||||||
| HOMA-IR | -0.03 | -0.18 | -0.04 | -0.23 | ||||||
| eLPP*HOMA-IR | -0.13 | -0.65 | ||||||||
| Model 5 | 0.03 | 0.35 | 0.71 | 0.01 | 0.27 | 0.61 | ||||
| mLPP | 0.13 | 0.67 | 0.16 | 0.79 | ||||||
| BF% | -0.07 | -0.39 | -0.10 | -0.48 | ||||||
| mLPP*BF% | -0.11 | -0.52 | ||||||||
| Model 6 | 0.02 | 0.30 | 0.74 | 0.05 | 1.26 | 0.27 | ||||
| mLPP | 0.14 | 0.73 | 0.21 | 1.06 | ||||||
| HOMA-IR | -0.04 | -0.22 | 0.00 | 0.00 | ||||||
| mLPP*HOMA-IR | -0.23 | -1.12 | ||||||||
| Model 7 | 0.01 | 0.13 | 0.86 | 0.01 | 0.15 | 0.71 | ||||
| lLPP | -0.03 | -0.16 | -0.05 | -0.23 | ||||||
| BF% | -0.11 | -0.51 | -0.13 | -0.60 | ||||||
| lLPP*BF% | 0.08 | 0.38 | ||||||||
| Model 8 | 0.00 | 0.03 | 0.97 | 0.01 | 0.18 | 0.68 | ||||
| lLPP | 0.00 | 0.00 | 0.03 | 0.14 | ||||||
| HOMA-IR | -0.05 | -0.24 | -0.03 | -0.17 | ||||||
| lLPP*HOMA-IR | -0.09 | -0.42 | ||||||||
Table displays the results of each step of the hierarchical moderated regression analyses, which tested whether EPN or LPP voltage amplitudes and BF% or HOMA-IR moderated the mean reaction times after viewing positively-valenced versus neutrally-valenced pictures. BF% = body fat percentage; eLPP = early latency late positive potential; EPN = early posterior negativity; HOMA-IR = homeostatic model assessment for insulin resistance; lLPP = late latency late positive potential; mLPP = middle latency late positive potential. β shows standardized regression coefficients. Only statistically significant covariates (p≤0.10) were included in each model.
Table 9.
Hierarchical moderated regression results for Negative vs. Positive valence ratings.
| Step 1 | Step 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | β | t | R2 | F | p | Β | t | ΔR2 | ΔF | p |
| Model 1 | 0.41*** | 5.96*** | 0.003 | 0.02 | 1.04 | 0.32 | ||||
| EPN | 0.34 | 2.09 | 0.30 | 1.84 | ||||||
| BF% | 0.35 | 2.23 | 0.37 | 2.33 | ||||||
| Race/Ethnicity | -0.42 | -2.51 | -0.36 | -1.98 | ||||||
| EPN*BF% | 0.17 | 1.02 | ||||||||
| Model 2 | 0.35 | 4.68 | 0.01 | 0.05 | 2.15 | 0.16 | ||||
| EPN | 0.41 | 2.41 | 0.46 | 2.71 | ||||||
| HOMA-IR | 0.25 | 1.51 | 0.25 | 1.54 | ||||||
| Race/Ethnicity | -0.47 | -2.67 | -0.40 | -2.29 | ||||||
| EPN*HOMA-IR | 0.25 | 1.47 | ||||||||
| Model 3 | 0.32 | 4.07 | 0.02 | 0.00 | 0.02 | 0.89 | ||||
| eLPP | 0.12 | 0.68 | 0.14 | 0.74 | ||||||
| BF% | 0.61** | 3.02** | 0.43 | 2.36 | ||||||
| Physical Activity | 0.33 | 1.72 | ||||||||
| eLPP*BF% | 0.02 | 0.13 | ||||||||
| Model 4 | 0.26 | 3.04 | 0.05 | 0.02 | 0.50 | 0.49 | ||||
| eLPP | 0.15 | 0.83 | 0.10 | 0.52 | ||||||
| HOMA-IR | 0.22 | 1.24 | 0.28 | 1.40 | ||||||
| Sex | -0.36 | -2.08 | -0.38 | -2.14 | ||||||
| eLPP*HOMA-IR | -0.14 | -0.71 | ||||||||
| Model 5 | 0.03 | 0.12 | 0.99 | 0.06 | 2.11 | 0.16 | ||||
| mLPP | 0.18 | 1.07 | 0.17 | 1.00 | ||||||
| BF% | 0.60** | 3.06** | 0.38 | 2.23 | ||||||
| Physical Activity | 0.33 | 1.75 | ||||||||
| mLPP*BF% | 0.24 | 1.45 | ||||||||
| Model 6 | 0.27 | 3.25 | 0.04 | 0.00 | 0.07 | 0.80 | ||||
| mLPP | 0.19 | 1.09 | 0.18 | 0.97 | ||||||
| HOMA-IR | 0.24 | 1.38 | 0.22 | 1.23 | ||||||
| Sex | -0.34 | -1.95 | -0.34 | -1.93 | ||||||
| mLPP*HOMA-IR | 0.05 | 0.26 | ||||||||
| Model 7 | 0.33 | 4.33 | 0.01 | 0.13 | 5.77 | 0.02 | ||||
| lLPP | -0.16 | -1.00 | -0.16 | -1.05 | ||||||
| BF% | 0.39 | 2.34 | 0.39 | 2.51 | ||||||
| Race/Ethnicity | -0.33 | -1.92 | -0.36 | -2.27 | ||||||
| lLPP*BF% | 0.35 | 2.40 | ||||||||
| Model 8 | 0.24 | 2.78 | 0.06 | 0.04 | 1.27 | 0.27 | ||||
| lLPP | -0.05 | -0.32 | -0.15 | -0.86 | ||||||
| HOMA-IR | 0.26 | 1.53 | 0.18 | 1.00 | ||||||
| Sex | -0.38 | -2.18 | ||||||||
| Race/Ethnicity | -0.39 | -2.11 | ||||||||
| lLPP*HOMA-IR | 0.19 | 1.13 | ||||||||
Table displays the results of each step of the hierarchical moderated regression analyses, which tested whether EPN or LPP voltage amplitudes and BF% or HOMA-IR moderated the mean valence ratings after viewing negatively-valenced versus positively-valenced pictures. BF% = body fat percentage; eLPP = early latency late positive potential; EPN = early posterior negativity; HOMA-IR = homeostatic model assessment for insulin resistance; lLPP = late latency late positive potential; mLPP = middle latency late positive potential. ** and *** = p’s≤0.0063 and ≤0.005, respectively. β shows standardized regression coefficients. Only statistically significant covariates (p≤0.10) were included in each model.
Table 10.
Hierarchical moderated regression results for Negative vs. Positive reaction times.
| Step 1 | Step 2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables | β | t | R2 | F | p | β | t | ΔR2 | ΔF | p |
| Model 1 | 0.36 | 3.52 | 0.02 | 0.03 | 0.89 | 0.36 | ||||
| EPN | -0.48 | -2.82 | -0.35 | -2.05 | ||||||
| BF% | 0.13 | 0.77 | 0.02 | 0.14 | ||||||
| Age | 0.33 | 2.04 | 0.36 | 2.06 | ||||||
| Race/Ethnicity | 0.36 | 1.98 | ||||||||
| EPN*BF% | -0.16 | -0.94 | ||||||||
| Model 2 | 0.41 | 4.30 | 0.01 | 0.00 | 0.17 | 0.68 | ||||
| EPN | -0.44 | -2.64 | -0.45 | -2.63 | ||||||
| HOMA-IR | 0.27 | 1.62 | 0.27 | 1.56 | ||||||
| Age | 0.29 | 1.84 | 0.31 | 1.86 | ||||||
| Race/Ethnicity | 0.39 | 2.28 | 0.37 | 2.06 | ||||||
| EPN*HOMA-IR | -0.07 | -0.41 | ||||||||
| Model 3 | 0.18 | 1.94 | 0.15 | 0.01 | 0.38 | 0.54 | ||||
| eLPP | -0.25 | -1.31 | -0.23 | -1.18 | ||||||
| BF% | 0.11 | 0.59 | 0.13 | 0.67 | ||||||
| Age | 0.35 | 1.97 | 0.33 | 1.75 | ||||||
| eLPP*BF% | 0.12 | 0.62 | ||||||||
| Model 4 | 0.27 | 3.24 | 0.04 | 0.03 | 1.10 | 0.30 | ||||
| eLPP | -0.31 | -1.78 | -0.25 | -1.32 | ||||||
| HOMA-IR | 0.34 | 1.89 | 0.33 | 1.63 | ||||||
| Age | 0.29 | 1.71 | ||||||||
| eLPP*HOMA-IR | 0.20 | 1.05 | ||||||||
| Model 5 | 0.14 | 1.37 | 0.27 | 0.00 | 0.01 | 0.94 | ||||
| mLPP | -0.09 | -0.48 | -0.09 | -0.48 | ||||||
| BF% | 0.05 | 0.28 | 0.05 | 0.26 | ||||||
| Age | 0.35 | 1.89 | 0.35 | 1.81 | ||||||
| mLPP*BF% | 0.01 | 0.07 | ||||||||
| Model 6 | 0.12 | 1.78 | 0.19 | 0.07 | 2.35 | 0.14 | ||||
| mLPP | -0.14 | -0.78 | -0.21 | -1.12 | ||||||
| HOMA-IR | 0.34 | 1.83 | 0.26 | 1.41 | ||||||
| mLPP*HOMA-IR | 0.29 | 1.53 | ||||||||
| Model 7 | 0.19 | 2.00 | 0.14 | 0.01 | 0.27 | 0.61 | ||||
| lLPP | -0.25 | -1.37 | -0.24 | -1.30 | ||||||
| BF% | 0.03 | 0.19 | 0.04 | 0.21 | ||||||
| Age | 0.41 | 2.25 | 0.39 | 2.02 | ||||||
| lLPP*BF% | 0.10 | 0.52 | ||||||||
| Model 8 | 0.23 | 2.63 | 0.07 | 0.01 | 0.33 | 0.57 | ||||
| lLPP | -0.23 | -1.29 | -0.23 | -1.27 | ||||||
| HOMA-IR | 0.22 | 1.25 | 0.23 | 1.25 | ||||||
| Age | 0.36 | 1.99 | 0.35 | 1.85 | ||||||
| lLPP*HOMA-IR | 0.10 | 0.58 | ||||||||
Table displays the results of each step of the hierarchical moderated regression analyses, which tested whether EPN or LPP voltage amplitudes and BF% or HOMA-IR moderated the mean reaction times after viewing negatively-valenced versus positive-valenced pictures. BF% = body fat percentage; eLPP = early latency late positive potential; EPN = early posterior negativity; HOMA-IR = homeostatic model assessment for insulin resistance; lLPP = late latency late positive potential; mLPP = middle latency late positive potential. β shows standardized regression coefficients. Only statistically significant covariates (p≤0.10) were included in each model.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



