
Submitted:
05 September 2025
Posted:
08 September 2025
You are already at the latest version
Abstract
Background/Objectives: Breast cancer incidence is increasing in younger Ghanaian women. However, few epidemiological studies have evaluated the modifiable risk factors in this population. Additionally, these studies have classified breast cancer in Ghanaian women based on the global menopausal case classification. This study reclassified premenopausal and postmenopausal breast cancer in a Ghanaian cohort, assessing the risk factors using the observed menopausal age in Ghanaian women of 48 years, rather than the global standard of 50 years. Methods: Women di-agnosed with breast cancer and scheduled for surgery from December 2018 to March 2023 were recruited across four hospitals in Ghana for the Ghana Breast Cancer Omics Project (BCOPGh), and data were collected using a questionnaire. Cross-tabulation and linear regression were used to evaluate the relationships between categorical variables and age at diagnosis. Results: Out of a total of 262 women recruited, 34.4% were classified as having premenopausal breast cancer; while early-onset breast cancer (EOBC) accounted for 14.9% of all cases. The molecular subtypes were predominantly Hormone receptor (HR)-positive (61%) while triple-negative breast cancer (TNBC) accounted for 16%. The tumours were predominantly at stage II (62%) and grade 2 (51%) with invasive carcinoma NST (56%) being the most common subtype. Within this cohort, nulliparity increased EOBC risk by 13.5-fold, while having a first birth after the age of 23 doubled the odds of premenopausal breast cancer. Reproductive factors (menarche and menopause) and lifestyle (al-cohol intake, smoking, contraceptive use, and breastfeeding duration) were not associated with premenopausal breast cancer in this cohort. About 13% of participants reported a family history of breast cancer, and 79% had prior knowledge of the disease. Conclusion: This study supports pre-vious reports of relatively higher incidence of aggressive disease in young Ghanaian women and the protective effect of early age at first birth. It further underscores the need to investigate its genetic underpinnings, whilst highlighting the importance of public education on self-examination tech-niques to reduce advanced disease presentation in Ghanaian women.
Keywords:
Breast cancer
; Ghanaian
; risk factors
; early-onset breast cancer
; premenopausal
; late-onset
; postmenopausal
; association
; reproductive factors
1. Introduction
According to the International Agency for Research on Cancer (IARC), breast cancer is the second most diagnosed cancer worldwide with an estimated 2.3 million new cases diagnosed in 2022 [1]. With over 665,000 associated deaths reported in 2022, it is the fourth leading cause of cancer-related mortalities in both sexes [2]. Approximately 8.6% of the newly diagnosed cases were recorded in African women. Despite the reported lower incidence (the second least affected continent), Africa recorded the third highest (13.7%) proportion of breast cancer-related deaths [2]. About 33% of the new breast cancer cases and 27% of the deaths were recorded in women diagnosed younger than 50 years (premenopausal breast cancer), representing a significant and growing public health burden in indigenous African populations [3]. Without early diagnosis and timely access to interventional resources, breast cancer mortality in sub-Saharan Africa is projected to surge to about a million deaths annually by 2030 [4]. In Ghana, the data shows that female breast cancer accounted for 31.4% (5,026) of newly diagnosed cancer cases and 24% (2,368) of all cancer-related mortalities, positioning it as the leading incident cancer and cause of cancer-related deaths in Ghanaian women [2]. Approximately 50% of the incidence and related mortalities were observed in premenopausal women. By 2030, the newly diagnosed premenopausal breast cancer cases and their associated deaths are projected to increase by approximately 47% [5]. Extensive research has identified several nonmodifiable (including age, race, genetics, gender, and reproductive factors) and modifiable (including lifestyle-related factors and environmental exposure) factors believed to influence breast carcinogenesis [6,7,8,9]. Although nonmodifiable, reproductive factors including ages at menarche and menopause, parity and gravidity have been variably associated with breast cancer across populations [10,11]. Yet, few studies have evaluated the association between breast cancer and the modifiable risk factors and reproductive health in Ghanaian women.
Breast cancer is a multifactorial disease mediated by an interplay between genomic and non-genetic factors, with racially varied presentations [12,13]. Despite its widespread prevalence, the aetiology of breast cancer remains unclear [14,15]. Several studies have identified several non-genetic factors including early menarche [16], delayed age at first full-term pregnancy and birth [17], late menopause[18,19], habits like smoking [20,21], alcohol consumption [22,23,24], contraceptive use [25,26] and body mass index [27,28] as contributing to an increased risk of developing breast cancer. Importantly, breast cancer is a hormonal disease with varied presentations at different ages of diagnosis [29]. Classification of breast cancer into premenopausal (diagnosed in women younger than 50 years) and postmenopausal (diagnosed in women at least 50 years old) breast cancer was developed primarily to identify and streamline age-associated risk factors. This classification stratifies cases using 50 years as the global average menopausal age [30,31,32], representing mostly Eurocentric and Caucasian populations. However, it does not consider the different age structures in different populations which significantly influences the proportions of premenopausal and postmenopausal breast cancer cases [33]. This may explain the inconsistent and conflicting risk assessment reports published across different populations [27,34]n thus underscoring the need for case stratification that employs population-specific demographic features.
Menopausal age profiles vary across populations [35] with women of African ancestry reaching menopause relatively earlier than their White American and European counterparts [36]. Furthermore, the African population has the largest proportion of individuals younger than 16 years, making up approximately 40% of the population, compared to the global average of 25% [37]. This suggests that evaluating these risk factors in Indigenous African populations using the globally generated menopausal case stratifications may misrepresent the actual proportion of premenopausal and postmenopausal cases and their associated risk factors. In Ghana, there has been a considerable increase in the incidence of breast cancer in young women (<50 years) [38,39,40,41]. Despite evidence that 91% of the Ghanaian population is younger than 55 years [42] and the average menopausal age in Ghanaian women is 48 years [43,44], the few studies evaluating the non-genetic risk factors still relied on the global case stratification [45,46]. The only study that attempted to reclassify premenopausal and postmenopausal cases while profiling the patterns of breast tumour presentation in Ghanaian women used the study cohort’s average menopausal age of 46.6 years [41]. Study-specific case classifications and risk assessments may not adequately represent the risk profile in the population. Thus, this study aimed to reclassify breast cancer cases using the Ghanaian population’s average age at menopause and reevaluate their associated non-genetic risk factors. The youthful age structure of the Ghanaian population provides an ideal context to investigate premenopausal breast cancer-associated risk factors.
2. Materials and Methods
2.1. Study Design and Ethical Considerations
This is a hospital-based, descriptive cross-sectional analysis of baseline data from a cohort of Ghanaian women diagnosed with breast cancer. Written informed consent was obtained from all participants prior to enrolment, ensuring adherence to the Declaration of Helsinki.
2.2. Participant Recruitment and Study Sites
Ghanaian wwomen diagnosed with breast cancer and scheduled for surgery were recruited from four (4) hospitals in two (2) regions of Ghana from December 2018 to March 2023 for a larger project, the Ghana Breast Omics Project (BCOPGh). The recruitment sites were the Korle-Bu Teaching Hospital, Greater Accra Regional Hospital, Ghanuba Specialist Clinic in the Greater Accra region and Ho Teaching Hospital in the Volta region. In this study, a Ghanaian woman was defined as a citizen by descent (born to at least one Ghanaian parent), belonging to an indigenous Ghanaian ethnic group. The inclusion and exclusion criteria for participant recruitment are detailed below:
2.2.1. Inclusion Criteria
Ghanaian women, aged at least 18 years, diagnosed with breast cancer and willing to offer informed consent.
2.2.2. Exclusion Criteria
Women under 18 years old, unable/unwilling to offer informed consent and non-Ghanaians.
2.3. Data Collection and Analysis
After recruitment, a structured questionnaire, comprising three sections capturing key thematic areas, was administered to consenting participants. Section one was designed to obtain general demographics (age, tribe, occupation and residence), section two captured participants’ reproductive history, medical history and clinical presentation, while section three captured participants’ lifestyle history (smoking, alcohol intake, contraceptive use and use of bleaching creams) and breast cancer knowledge. Data was captured using the REDcap (www.redcap.ug.edu.gh) electronic data capture platform. The data were exported and analysed using the R statistical software version 4.3.2. In this study, the cases were categorized using the previously reported average menopausal age (48 years) in Ghanaian women [43,44,47], as the cutoff threshold into premenopausal (<48 years old) and postmenopausal (≥48 years old) breast cancer cases. This study further grouped the cases into Early-onset breast cancer (EOBC), which are cases diagnosed younger than 40 years, and late-onset breast cancer (LOBC), comprising those diagnosed 40 years and older, based on previous studies [6,38,48,49], although other studies have used 45 years [50]. Participants’ ethnicity was self-defined and coded into 14 Ghanaian ethnolinguistic groups, representing 11 of Ghana’s 16 regions. Gravidity was defined as the number of pregnancies, including full-term births, stillbirths, and abortions, while parity referred to the number of pregnancies that resulted in stillbirths or live births. Symptoms prompting hospital visits were recorded, allowing for the analysis of clinical presentation patterns. Knowledge of breast cancer was defined as awareness of breast cancer prior to diagnosis, assessed by a “Yes” or “No” response to having heard of breast cancer before diagnosis and the ability to identify at least one symptom of the disease. A series of statistical tests were conducted to compare groups; the Mann-Whitney U test was employed for group comparisons and Fisher’s exact and Chi-square tests used to assess associations between categorical variables. To evaluate associations between risk factors and the two age-based outcomes, we first conducted univariate logistic regressions on each original categorical predictor (menarche age, parity, gravidity, first-birth age, contraceptive use, and occupation). To avoid sparse-cell bias (minimum events-per-variable ≥ 10) and improve model stability, we collapsed each multi-level predictor into a binary variable using epidemiologically established cut-points and similar directional effects in the univariate ORs. For the premenopausal (diagnosis < 48 years vs ≥ 48 yrs.) and early-onset (diagnosis < 40 yrs. vs. ≥ 40 yrs.) groups, we then ran parsimonious multivariate logistic regressions including only the strongest predictors: occupation and age at first birth for premenopausal group, and parity and occupation for EOBC. We report adjusted odds ratios (OR), 95% confidence intervals (CI), p-values, area under the ROC curve (AUC), and the Hosmer–Lemeshow goodness-of-fit test. A two-sided p < 0.05 denoted statistical significance.
3. Results
3.1. General Demographics
3.1.1. Participants’ Age Profiles and Case Group Incidence
A total of 262 women diagnosed with breast cancer were recruited. Table 1 summarises the case groups, their reproductive factors, and general demographics. The participants were 27 to 85 years old, with a median age of 54 years. The modal age (peak breast cancer incidence age) was 50 years (Figure 1A). Notably, 37.4% of cases were premenopausal breast cancer when the cases were classified using 50 years (Figure 1B) as opposed to 34.4%, using 48 years (Figure 1C); early-onset breast cancer (EOBC) accounted for 14.9% of all the cases (Figure 1B and C, respectively). The median age at diagnosis was 35 years for EOBC and 41 years for premenopausal breast cancer (Table 1). Participants in this study were mostly traders or businesswomen (47%); 27% were students, unemployed or retired, and 26% comprised clerical, farmers, and professional workers (Figure S1). Generally, the participants resided mostly in peri-urban (53%) and urban (44%) settings. The participants belonged mainly to the Akan (45%), Ga-Adangbe (24%) and Ewe (22%) ethnolinguistic groups; approximately 9% comprised eight other ethnolinguistic groups (Table S1). About 86% of the participants have had a mammogram. Occupation, menstrual status and mammogram screening history showed considerable associations with the age at diagnosis.
3.1.2. Participants’ Reproductive Factors
The median age at menopause in this study was 48 years, with the youngest and oldest menopausal participants being 27 and 60 years old, respectively (Table 1). About 65% of the participants were menopausal, 26% were still menstruating, 8.6% had irregular menstruation and 1.4% (two women) had never menstruated (Figure 2). The median age at menopause was considerably lower (42, p=0.005) in the premenopausal case group; only one EOBC participant was menopausal. Age at menarche ranged from 10 to 25 years with a median of 15; significantly lower (14, p<0.001) in the EOBC cases. Generally, women in this study were multiparous and multigravid, with three births and four pregnancies on average, respectively (Table 1). Significantly lower parities were observed in participants diagnosed before the age of 48 years (2, p<0.001) and lowest in participants diagnosed at ages below 40 years (1, p<0.001). Gravidity was also considerably lower in the premenopausal (3, p<0.001) group; this was lowest in women diagnosed younger than 40 years (2, p<0.001). The overall primiparity age in this study ranged from 15 to 54 years, with a median of 24 years. This was significantly higher in the premenopausal breast cancer cases (27, p<0.001).
Table 2 shows the association between the reproductive factors and the age at diagnosis. Notably, 9% of the women have never given birth, 32% had 2 children, 28% had 3 and 31% had more than three children. Approximately 17% of the participants had never been pregnant, 29% had more than 4 pregnancies, and 32% had been pregnant at most three times. This study’s participants breastfed for 18 months on average; 67% breastfed for more than 12 months, 28% for 6–12 months, 5% for at most 5 months, and 5.4% never breastfed. Overall, menopause, menarche, gravidity, parity, and primiparity correlated considerably with the age at diagnosis, while breastfeeding showed no association in our cohort.
3.2. Medical History and Clinical Presentations
Table 3 summarises the breast cancer clinicopathological characteristics of our cohort. Approximately 60.7% of the participants reported lumps in the breast and 15.6% reported painful breasts; 23.7% of the participants reported a range of symptoms including flaky skin, open wounds, discoloured breasts, and distorted breast shape (Figure S2). Approximately 68% of the participants detected these symptoms via self-examination and 32% via medical examination (Table 1). Invasive Carcinoma NST, Invasive Ductal Carcinoma and Ductal Carcinoma in situ constituted 56%, 18% and 13% of the cases, respectively; Figures S3 and S4 show the distribution of the other (6.1%) tumours. Tumour type was not associated with the symptoms presented (Figure S5) or breastfeeding duration (Figure S6). Only 47 of the participants had stage classifications and 149 had grade classifications. Approximately 60% of cases were stage II; stages I, III and IV accounted for 19%, 15% and 4%, respectively. Grade 2 accounted for 51% of all the cases; grades 1 and 3 constituted 21% and 28%, respectively. Hormone receptor-positive (ER+/PR+; ER+/PR-; ER-/PR+, including HER2-equivocal) accounted for 59.7% and hormone receptor-negative (ER-/PR- including HER2-equivocal), 20.6% of the cases; approximately 16% were triple-negative breast cancer (TNBC) and 4.6% were HER2-enriched. Generally, there was no association between the clinical presentations and age at diagnosis.
3.3. Participants’ Lifestyle and Family History
Table 4 highlights the lifestyle and family history of the participants. Approximately 21% of the participants were unaware of the disease prior to their diagnosis. Regarding habits, 99% of the participants had never smoked, 73% never drank alcohol, 13% had used skin-bleaching creams, 29% had used a contraceptive and 13% reported having a family history of cancer. Of those who drank alcohol, 21% drink occasionally and 5% drink frequently (weekly and monthly). Contraceptive use was significantly associated with diagnosis before 40 years (p=0.005).
3.4. Regression Analysis and Risk Assessment
Univariate analyses showed that the odds of being diagnosed younger than 48 years significantly decreased with every unit increase in the ages at menarche, menopause as well as number of pregnancies (Gravidity) and births (parity) (Table S2); The age at first birth increased the odds of being diagnosed before 48 years. Further categorization indicated that menarche (<15 years) decreased the odds, and zero births (parity = “never”) considerably increased the odds of being diagnosed younger than 48 years (including EOBC); The odds o being diagnosed with EOBC were higher in women who had never been pregnant. A multivariate logistic regression analysis, summarised in Table 5, was conducted to evaluate the strongest predictors of age at diagnosis based on results from the univariate analysis summarised in Table S3. In this study’s cohort, a reduced logistic model including occupation and first birth age showed that unemployed women had 82% lower odds of being diagnosed younger than 48 years (OR 0.118, 95% CI 0.045–0.31, p < 0.001), while first birth ≥ 24 years doubled the odds (OR 2.11, 95% CI 1.15–3.86, p = 0.016). This model discriminated well (AUC = 0.7194) and calibrated acceptably (Hosmer–Lemeshow χ² = 1.21, p = 0.5465). The logistic model shows that nulliparous women had 13.5-fold higher odds of diagnosis before 40 years (OR 13.49, 95% CI 5.06–35.98, p < 0.001), and unemployed women had 88% lower odds (OR 0.118, 95% CI 0.051–0.66, p = 0.009). The model’s AUC was 0.7190, and Hosmer–Lemeshow χ² = 0.74 (p = 0.3909), indicating good fit.
4. Discussion
This study aimed to more accurately define premenopausal and postmenopausal breast cancer classification and assess the non-genetic risk factors in Ghanaian women. The International Agency for Research on Cancer (IARC) ranked breast cancer as the foremost cancer diagnosed (5,026, 31.4% of all new cancers) and the leading cause of cancer-related deaths (2,369, 24% of newly associated deaths) in Ghanaian women [1,2]. Approximately 52% of the incident cases were observed in women younger than 50 years old (premenopausal breast cancer) and are predicted to increase by 41% over the next decade[2]. Currently, the menopausal classification of breast cancer uses age 50 years as a proxy for the global average menopausal age [31,32]. Meanwhile, available reports indicate that menopause occurs earlier in African women than in European American and European women [36]. Breast cancer is a hormonal disease with varying presentations at diagnosis [29], hence the classification into premenopausal and postmenopausal cases. The variations in menopausal age have been associated with genetic variations [51,52], socioeconomic factors [53,54,55] and lifestyle [56]. Considering the ethnic variations in breast cancer presentation and differences in age at menopause, using the global average (50 years) to evaluate breast cancer in Indigenous Africans will misrepresent their case proportions as well as prevailing risk factors. In Ghana, the few studies that have investigated the known non-genetic breast cancer risk factors have classified the cases using the global average menopausal age of 50 years [39,45], which is higher than the 48 years previously reported [43,44] in Ghanaian women and observed in this study. More so, Ghartey et al. [41], who attempted to classify the cases, used the menopausal age (46.6 years) observed in their study cohort, which is not representative of the average menopausal age in Ghanaian women. Thus, this study is the first to classify breast cancer in Ghanaian women using the established national menopausal age of 48 years into premenopausal (diagnosed <48 years) and postmenopausal (diagnosed ≥48 years) breast cancers.
With this classification, 34.4% of the cases were premenopausal breast cancer, whereas this proportion increased to 37.4% using the controversial 50-year threshold – highlighting the influence of age classifications on prevalence estimation. Although both estimations are higher than the global estimate of 30.9%, they were lower than the estimated incidence in Africa (49.2%) and Asia (39%) [29]. These, however, were higher than those reported in Europe (19.9%), Oceania (32.2%) and Latin America and the Caribbean (LAC) (28.7%). In West Africa, 55.4% of the cases are reportedly premenopausal [29] and previous studies in Ghana have estimated 63.3% [41], 50% [45], 50.6% [39] and 58.9% [46]. Beyond the cut-off age used in the case classification in this study, the lower prevalences observed for both the 48- and 50-year age, compared to the previous reports, are likely attributable to the smaller sample size and the participant recruitment criteria. This notwithstanding, the observed prevalence, compared to those reported in the European and American populations, further supports evidence that Ghanaian women diagnosed with breast cancer are often younger. EOBC (participants diagnosed younger than 40 years) accounted for approximately 15% of all cases, compared to the previously reported 20.2% [38]; this observation may also be attributed to the sample size.
The observed median and modal (50 years) ages validate the decade-earlier breast cancer peak incidence reported in sub-Saharan African women, compared to their White American (62.4 years) and African American (60.8 years) counterparts [57,58,59]. Additionally, the average age (40 years) of participants diagnosed younger than 48 years (including EOBC) corroborates reports of breast cancer diagnosis in younger Ghanaian women [38,45]. More so, the median age in women diagnosed younger than 48 years (40 years) contradicts the estimated age (50 years) in low-and-middle-income countries [33]. Importantly, over 80% of the Ghanaian population has been younger than 50 years for over 2 decades [37,42,60]. This may partly explain the relatively higher number of premenopausal breast cancer cases observed in Ghanaian women. However, younger age at diagnosis is partly attributable to familial genetic predispositions[61] and environmental factors including ionizing radiations[62] and air pollutants like polyaromatic hydrocarbons (PAH) [63]. This highlights the need to explore both the genetic and environmental breast cancer risk factors peculiar to Ghanaian women.
Risk assessments between premenopausal and postmenopausal breast cancer cases have highlighted fundamental aetiological differences associated with reproductive health [17,57,64]. Parity and age at first birth were the only significant predictors of premenopausal breast cancer in our study, consistent with a previous report (Robertson. Primiparity after age 30 has been associated with an increased risk of postmenopausal breast cancer [17]. This study reported a median primiparity age of 24 years and a 2-fold increase in the risk of premenopausal breast cancer with primiparity beyond 23 years (≥24 years). The observed median primiparity age in our study was relatively higher than the average reported in Ghanaian women (20.7 years) [65]. This may explain the observed odds of developing premenopausal breast cancer and supports evidence that early primiparity is protective against premenopausal breast cancer [66,67,68].
Multiparity is reportedly a protective factor [69]. Our study found no association between multiparity and premenopausal breast cancer, consistent with a previous report 70] [66]. However, we detected a markedly increased risk of EOBC, approximately 13.5 folds higher, in nulliparous women. While our findings may suggest that multiparity, irrespective of the number of births, did not influence the age at diagnosis in our study cohort, our modest sample size highlights the need for a high-powered study to better assess this association.
Similar to previous reports [70,71,72], the median menarcheal age observed was 15 years. This is relatively higher than the estimated age in African American (12.2 years) and Caucasian American (12.9 years) [73] women, but comparable to the 14.5 years estimated in Nigerians and most SSA women [74]. Menarche was not associated with premenopausal breast cancer in this cohort, contradicting reports indicating an association of early menarche (<12 years) with breast cancer in Asia, Europe, Oceania, and North America [16]. Although this study’s age at menarche was significantly lower (14 years) among women diagnosed before age 40, it is comparable to the estimated average menarcheal age (13.82 years; 11–15 years) in Ghanaian women [70,71,72]. This may suggest that age at menarche is not a significant contributing risk factor for premenopausal breast cancer in this study, consistent with previous reports from Ghana [64], Senegal [11] and Mexico [75].This further underscores the importance of population-specific profiling of breast cancer risk factors.
A slight increase in breast cancer risk has been associated with increasing menopausal age after 50 years [16]. The average menopausal age in this study (48 years) was relatively lower but within the estimated range (45–51 years) in Ghanaian women [43], comparable to that reported in the Nigerian population (48 years) [76] and within the global range (45–55 years) [32]. Due to the number of participants who either forgot their ages at menopause or were still menstruating, this study could neither evaluate the association between menopausal age and age at diagnosis in this cohort nor comment on the relationship between premenopausal breast cancer and menopausal age.
Lifestyle choices including alcohol intake [22], smoking [77], and contraceptive use [25] have previously been associated with an increased risk of breast cancer. Contrary to these reports, there was no observed association between alcohol intake or duration and smoking with breast cancer in this study cohort. It is worth noting that alcohol intake and smoking among women are culturally uncommon in most Ghanaian communities, which may explain their lack of association with breast cancer in our cohort. Contrary to an earlier report [25] indicating a 7% increase in the relative risk of breast cancer in women who have ever used contraceptives, contraceptive use was not associated with premenopausal breast cancer in this study. This suggests that alcohol intake, irrespective of frequency, smoking and contraceptive use may not be contributing risk factors in this study’s cohort. Additionally, breastfeeding duration (≤6 months) has been associated with an increased risk of breast cancer [78]. Participants in this study breastfed for 18 months on average and the duration showed no relationship with the age at diagnosis. This could explain the lack of protective effect of breastfeeding in our population, where breastfeeding is culturally normative and nearly all women breastfeed for extended periods, similar to observations in Black South African women [79]. Additionally, potential recall bias regarding the exact duration of breastfeeding could have contributed to misclassification, diminishing the observed association. Nonetheless, this suggests that having ever breastfed or the duration of breastfeeding may not have influenced the age at diagnosis in this study’s cohort, similar to reports by Butt et al. [80]. This is contrary to previous indications of a reduced risk for at least 12 months of breastfeeding [81,82] and breastfeeding being a protective factor [83].
Consistent with previous reports, Invasive Carcinoma No Special Type (NST) was the most common breast cancer subtype in our cohort [38]. Similarly, the proportion was higher in LOBC (57%), compared to EOBC (54%) in our cohort. The observed proportion was, however, higher in the premenopausal case group (64%) compared to 51% in the postmenopausal case group; this may further highlight the impact of age classification on the disease characteristics. The proportion of ductal carcinoma in situ in our cohort was similarly higher in EOBC (16%), compared to LOBC (13%). Invasive lobular carcinoma was recorded in 2.7% and 5.1% of the EOBC and LOBC cases, respectively, comparable to previously reported frequencies in EOBC (3%) and LOBC (5%) [84]. Invasive ductal carcinoma was the second most diagnosed type in this study, contrary to previous studies reporting it as the most common [46,85]. However, this study’s overall frequency of invasive ductal carcinoma and ductal carcinoma in situ compared to others like invasive lobular carcinoma, aligns with the general trend where most breast cancers are ductal carcinomas. Mucinous carcinoma is rare and constitutes 2% of breast cancer cases globally [86]. In our study, it accounted for approximately 3% of all the cases, similar to the 3.1% reported by Akakpo et al. [38]. However, contrary to observations made by Akakpo et al. [38], who recorded a 3.7% prevalence of mucinous carcinoma in EOBC cases, none was recorded in the EOBC cases in this study. Our observation may dwell on the number of participants in this study (262), compared to 2,418 participants in the study by Akakpo et al. Meanwhile, the proportion of mucinous carcinoma observed in the LOBC cases (3.4%) in this study was marginally higher than that reported by the same study (3.1%).
Hormone receptor (HR) positive tumours were the most prevalent receptor subtypes in this study and were more frequent in postmenopausal cases, as previously reported [38,84]. Similar to the report by Akakpo et al. [38], HR-negative tumours were more frequent in the cases diagnosed younger than 48 years (25%), compared to 17% in the postmenopausal cases. However, the proportion of HER2-enriched tumours recorded in this study was lower than was reported by Akakpo et al. [38]. This may be attributed to the sample size in this study and the absence of molecular subtype data for 42% of the participants. The report by Akakpo et al. [38] indicated that TNBC was the most prevalent molecular subtype in EOBC cases, accounting for 26.4% of the cases similar to the 25% prevalence previously reported in Indigenous African women [87]. With 12% prevalence, Bosompem et al. [47] also reported that TNBC was the most prevalent in young-onset breast cancer. In this study, TNBC accounted for 19% of all the subtypes in the EOBC cases but was not the most predominant molecular subtype, similar to reports by Andrikopoulou et al. [84]. Although our observation is partly attributable to the sample size, the TNBC frequency in this study’s EOBC cases was higher (19%) than the 12% reported by Bosompem et al. [47]. Notably, the frequency of TNBC tumours in this study’s EOBC cases is 1.2-fold higher than in the LOBC cases. This is marginally higher than the 1.1-fold higher TNBC frequency in EOBC cases (26.4%) than in LOBC cases (24%) reported by Akakpo et al [38]. Though no relationship was observed between the tumour stage and grade, the participants presented mainly with stage 2 and grade 2 tumours. Our finding is inconsistent with most previous reports showing higher proportions of advanced tumours in Ghanaian women [38,41,47,88]. However, it corroborates the approximately 51% grade 2 presentation reported in West Africa [87]. Even so, this observation may also be because participants presenting with advanced disease are often immediately put on neoadjuvant therapy before surgery and may have been missed because only participants scheduled for surgery were recruited. In this study, stages III and IV were 1.8 and 1.4-fold higher, respectively, and grade 3 tumours 1.32-fold higher in the premenopausal cases, compared to the postmenopausal cases. Although no stage IV tumour was recorded in the EOBC cases, the proportion of grade 3 tumours was 1.32-fold higher than observed in the LOBC cases, comparable to the 1.4-fold by Bosompem et al. [47] and higher than 1.2-fold by Adrikopoulou et al. [84]. The increased grade 3 tumours and TNBC proportions in the EOBC group in this study corroborate literature suggesting Ghanaian EOBC cases present with more aggressive tumours [38,89,90]. Advanced disease presentations have been associated with late detection and lack of knowledge or awareness of the disease [91]. The lower proportion of tumour stage and grade observed in this study may be due to sample size as well as the number of participants with incomplete tumour classification data. Despite this, the observed proportions may also point to early detection in this cohort owing to increasing awareness of the disease in Ghana. Although Ghana lacks national screening programs, several breast cancer awareness and screening initiatives, mostly spearheaded by local non-governmental institutions, are conducted throughout the year, with activities typically amplified in October. These activities aim to overcome the myths, misconceptions and sociocultural beliefs that have been previously linked to poor disease outcomes in the country, while encouraging and supporting early diagnosis. In our study, approximately 79% of the participants were aware of breast cancer before diagnosis, with premenopausal cases (85%) demonstrating higher awareness compared to postmenopausal cases (75%). This awareness may have contributed to the proportion of participants who detected the tumour via self-examination (68%) as opposed to medical exams (32%) and partly explains the reduced risk of EOBC associated with students and retirees in this study. Students are generally more technologically adept, with easy access to health information; retirees have greater peer experience with diseases and are more responsive to symptoms. While awareness does not stop the disease from developing, it informs lifestyle choices that might decrease their risk of developing the disease at a younger age or being diagnosed at advanced stages. This high rate of self-detection highlights the potential of early detection programs, especially in regions with limited regular medical screening. It further underscores the need for improved public health campaigns focused on self-examination techniques in this population.
Overall, participants in this study reported a 13% family history of cancer, the highest recorded in Ghana to the best of our knowledge. About 10% of women diagnosed with EOBC reported a known family history of breast cancer. This is higher than the previous 6.5% reported by Ahearn et al. [92] but lower than 12.9%, which was reported by Bosompem et al. [47]. This may be attributed to increasing knowledge of the disease. Increasing knowledge on breast cancer encourages dialogue among relatives which can reveal the disease pattern in the family. Meanwhile, the increasing familial history of cancer may also account for the younger age at diagnosis in Ghanaians. Breast cancer is a complex genetic disease; the younger age at onset and proportion of familial cancer history make this population ideal for investigating potentially novel genetic breast cancer risk factors.
The findings of this study should be interpreted with a few limitations in mind. This cross-sectional study’s selection criteria only recruited breast cancer patients scheduled for surgery, potentially excluding those undergoing other forms of therapy at the time of recruitment. This may have inadvertently biased the proportion of the cases. Additionally, this study relied on clinical data available at the point of participant recruitment. There were missing clinical information that could not be retrieved due to the pathology centres' varied participant identification systems for tumour diagnosis. Finally, information beyond the clinicopathological data were provided by the participants, some of whom were unable to recollect pertinent reproductive health details including ages at menarche, first birth, menarche and menopause. This may have also influenced the results of the risk assessment.
5. Conclusions
Premenopausal and postmenopausal breast cancer was reclassified using 48 years, the menopause age reported in the Ghanaian population. Approximately 34.4% of the participants were classified as having been diagnosed with premenopausal breast cancer, as opposed to 37.4% using the controversial 50-year threshold. In this study, age at first birth above 23 years and nulliparity emerged as the only reproductive factors examined in this study that independently influenced the odds of age at diagnosis. Furthermore, this study confirms the reported high prevalence and aggressive biology of premenopausal breast cancer in Ghanaian women. Additionally, this study suggests the potential of public health campaigns focused on self-examination techniques in early detection and possibly reducing advanced breast cancer presentations in Ghanaian women. Furthermore, it records the highest reported family history of breast cancer in Ghanaian women. Breast cancer is a complex genetic disease with racial variations, and the African population, being the most genetically diverse, presents a unique opportunity to identify novel breast cancer genes and gene variants specific to indigenous African populations. The paucity of genetic data on the Ghanaian population, combined with the proportions of familial history recorded in this study underscores the need to investigate both germline and somatic genetic risk factors in Ghanaian women.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Occupation of the Participants; Figure S2: Range of symptoms reported by the participants; Figure S3: Breast cancer subtypes in the EOBC and LOBC groups; Figure S4: Breast cancer subtypes in pre and postmenopausal breast cancer groups; Figure S5: Relationship between the tumour subtypes and symptoms; Figure S6: Relationship between Breastfeeding duration and tumour subtypes; Table S1: Regional origin of the Ethnolinguistic groups of the Participants
Author Contributions
Conceptualization L.P. and C.A.A.; formal analysis, C.A.A.; writing—original draft preparation, C.A.A., E. L. L., C.D.A., V.A., C.S. and A.U; writing—review and editing, C.A.A., L. P., G.A.A., V.A., C.S., E.L.L., C.D.A., H.F., J.N., J.N.C., F.D., L.E., A.T., R.A., R.W. and A.U.; funding acquisition, L.P.; supervision, L.P. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: This research was supported by funds from a World Bank African Centres of Excellence, grant number (WACCBIP+NCDs: Awandare) and a DELTAS African Initiative, grant number (DEL-22-014: Awandare). C.A.A. was supported by a WACCBIP-World Bank ACE Masters/PhD fellowship (WACCBIP+NCDs: Awandare). L.P. received support from the Science for Africa Foundation to the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) programme [DEL-22-014] through the Wellcome and the UK Foreign, Commonwealth & Development Office as well as UNESCO and the International Development Research Centre, Canada, as Building a New Generation of Academics in Africa (BANGA-Africa) project, funded by the Carnegie Corporation of New York. The views expressed herein do not represent those of UNESCO-TWAS, OWSD, IDRC or its Board of Governors. The APC was funded by the DELTAS African grant (DEL-22-014).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ghana Health Service Ethics Review Committee (GHS-ERC 006/12/20), Noguchi Memorial Institute for Medical Research Institutional Review Board (NMIMR-IRB 004/18-19), Korle-Bu Teaching Hospital Institutional Review Board (KBTH-IRB/00009/2018), Ho Teaching Hospital Administration, and the Ethics committee of the College of Basic and Applied Sciences (ECBAS 045/18-19).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy.
Acknowledgments
We would like to acknowledge Mr Samuel Degraft Mensah, Francis Asiedu Ampaw, Michelle Abena Buckman, Elizabeth Mbirbah, Naa Dedei Quarshie, Precious Opurum and Queenster Owusu for their assistance with participant recruitment and data collection. We are also grateful to Dr Nelson Affram for assisting with Patient recruitment and Mr. Francis Djabeng for re-examining our regression models.
Conflicts of Interest
The authors declare no conflicts of interest. The sponsors had no role in the design, execution, interpretation, or writing of the manuscript.
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians 2024, 74, 229–263. [Google Scholar] [CrossRef]
- GLOBOCAN. Cancer Today. Available online: https://gco.iarc.fr/today/en/dataviz/pie?mode=cancer&group_populations=1&populations=288&sexes=2&types=0&age_end=9&cancers=20 (accessed on October 17, 2024).
- Black, E.; Richmond, R. Improving early detection of breast cancer in sub-Saharan Africa: why mammography may not be the way forward. Globalization and Health 2019, 15, 3–3. [Google Scholar] [CrossRef] [PubMed]
- Ngwa, W.; Addai, B.W.; Adewole, I.; Ainsworth, V.; Alaro, J.; Alatise, O.I.; Ali, Z.; Anderson, B.O.; Anorlu, R.; Avery, S.; et al. Cancer in sub-Saharan Africa: a Lancet Oncology Commission. The Lancet Oncology 2022, 23, e251–e312. [Google Scholar] [CrossRef] [PubMed]
- GLOBOCAN. Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow/en/dataviz/bubbles?types=1&sexes=1_2&mode=cancer&group_populations=1&multiple_populations=1&multiple_cancers=1&cancers=20&populations=903_904_905_908_909_935&apc=cat_ca20v1.5_ca23v-1.5&group_cancers=1&bar_mode=stacked&years=2035 (accessed on October 17, 2024).
- Daly, A.A.; Rolph, R.; Cutress, R.I.; Copson, E.R. A Review of Modifiable Risk Factors in Young Women for the Prevention of Breast Cancer. Breast cancer (Dove Medical Press) 2021, 13, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.Y.; Stoll, C.R.; Anandarajah, A.; Doering, M.; Colditz, G.A. Modifiable risk factors in women at high risk of breast cancer: a systematic review. Breast cancer research : BCR 2023, 25. [Google Scholar] [CrossRef]
- Maas, P.; Barrdahl, M.; Joshi, A.D.; Auer, P.L.; Gaudet, M.M.; Milne, R.L.; Schumacher, F.R.; Anderson, W.F.; Check, D.; Chattopadhyay, S.; et al. Breast Cancer Risk From Modifiable and Nonmodifiable Risk Factors Among White Women in the United States. JAMA Oncology 2016, 2, 1295–1302. [Google Scholar] [CrossRef]
- Łukasiewicz, S.; Czeczelewski, M.; Forma, A.; Baj, J.; Sitarz, R.; Stanisławek, A. Breast Cancer-Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies-An Updated Review. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Galukande, M.; Wabinga, H.; Mirembe, F. Breast cancer survival experiences at a tertiary hospital in sub-Saharan Africa: a cohort study. World journal of surgical oncology 2015, 13, 1–8. [Google Scholar] [CrossRef]
- Gueye, M.; Gueye, S.; Gueye, M.; Diallo, M.; Gassama, O.; Biaye, B.; Lemine, A.; Niasse, A.; Mbodji, A.; Moreau, J. A hospital based case control study of female breast cancer risk factors in a Sub-Saharan African country. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 2016, 5, 2328–2332. [Google Scholar] [CrossRef]
- Shulman, L.P. Genetic and Genomic Factors in Breast Cancer. In Management of the Patient at High Risk for Breast Cancer. In Management of the Patient at High Risk for Breast Cancer, Hansen, N.M., Ed.; Springer New York: New York, NY, 2013; pp. 29–47. [Google Scholar]
- Anothaisintawee, T.; Wiratkapun, C.; Leedsitthichai, P.; Kasamesup, V.; Wongwaisayawan, S.; Srinakarin, J.; Thakkinstian, A. Risk factors of breast cancer: a systematic review and meta-analysis. journals.sagepub.com 2013, 25, 368–387. [Google Scholar] [CrossRef]
- Hackney, L. Aetiology and Epidemiology of Breast Cancer. In Digital Mammography: A Holistic Approach, Mercer, C., Hogg, P., Kelly, J., Eds.; Springer International Publishing: Cham, 2022; pp. 51–69. [Google Scholar]
- Admoun, C.; Mayrovitz, H.N. The Etiology of Breast Cancer. In Breast Cancer. In Breast Cancer, Mayrovitz, H.N., Ed.; Exon Publications: Brisbane, 2022; pp. 21–30. [Google Scholar]
- Hamajima, N.; Hirose, K.; Tajima, K.; Rohan, T.; Friedenreich, C.M.; Calle, E.E.; Gapstur, S.M.; Patel, A.V.; Coates, R.J.; Liff, J.M.; et al. Menarche, menopause, and breast cancer risk: individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. The Lancet. Oncology 2012, 13, 1151–1151. [Google Scholar] [CrossRef]
- Kelsey, J.L.; Gammon, M.D.; John, E.M. Reproductive Factors and Breast Cancer. Epidemiologic Reviews 1993, 15, 36–47. [Google Scholar] [CrossRef]
- Colditz, G.A.; Rosner, B. Cumulative Risk of Breast Cancer to Age 70 Years According to Risk Factor Status: Data from the Nurses' Health Study. American Journal of Epidemiology 2000, 152, 950–964. [Google Scholar] [CrossRef]
- Mullooly, M.; Khodr, Z.G.; Dallal, C.M.; Nyante, S.J.; Sherman, M.E.; Falk, R.; Liao, L.M.; Love, J.; Brinton, L.A.; Gierach, G.L. Epidemiologic Risk Factors for In Situ and Invasive Breast Cancers Among Postmenopausal Women in the National Institutes of Health-AARP Diet and Health Study. American journal of epidemiology 2017, 186, 1329–1340. [Google Scholar] [CrossRef]
- Catsburg, C.; Miller, A.B.; Rohan, T.E. Active cigarette smoking and risk of breast cancer. International journal of cancer 2015, 136, 2204–2209. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Miller, A.B.; Rohan, T.E. Cigarette smoking and breast cancer risk: update of a prospective cohort study. Breast cancer research and treatment 2006, 100, 293–299. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.A.; Goyal, A.; Terry, M.B. Alcohol Intake and Breast Cancer Risk: Weighing the Overall Evidence. Current breast cancer reports 2013, 5, 208–221. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: a comprehensive dose-response meta-analysis. British journal of cancer 2015, 112, 580–593. [Google Scholar] [CrossRef]
- Smith-Warner, S.A.; Spiegelman, D.; Yaun, S.S.; Van Den Brandt, P.A.; Folsom, A.R.; Goldbohm, R.A.; Graham, S.; Holmberg, L.; Howe, G.R.; Marshall, J.R.; et al. Alcohol and breast cancer in women: a pooled analysis of cohort studies. JAMA 1998, 279, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Calle, E.E.; Heath, C.W.; Miracle-McMahill, H.L.; Coates, R.J.; Liff, J.M.; Franceschi, S.; Talamini, R.; Chantarakul, N.; Koetsawang, S.; RachawatRachawat, D.; et al. Breast cancer and hormonal contraceptives: Collaborative reanalysis of individual data on 53 297 women with breast cancer and 100 239 women without breast cancer from 54 epidemiological studies. Lancet 1996, 347, 1713–1727. [Google Scholar] [CrossRef]
- Hang, Z.; Xun, L.; Jing, F.; Yang, W. Oral contraceptive use and risk of breast cancer: a meta-analysis of prospective cohort studies. The European journal of contraception & reproductive health care : the official journal of the European Society of Contraception 2012, 17, 402–414. [Google Scholar] [CrossRef]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. The Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Suzuki, R.; Saji, S.; Toi, M.; Gnant, M.; Markopoulos, C. Impact of body mass index on breast cancer in accordance with the life-stage of women. Frontiers in Oncology 2012, 2, 123–123. [Google Scholar] [CrossRef] [PubMed]
- Heer, E.; Harper, A.; Escandor, N.; Sung, H.; McCormack, V.; Fidler-Benaoudia, M.M. Global burden and trends in premenopausal and postmenopausal breast cancer: a population-based study - ClinicalKey. Lancet Global Health 2020, 8, e1027–e1037. [Google Scholar] [CrossRef]
- Organization, W.H. Menopause. Available online: https://www.who.int/news-room/fact-sheets/detail/menopause (accessed on December 5, 2024).
- Review, W.P. Age of Menopause by Country 2024. Available online: https://worldpopulationreview.com/country-rankings/age-of-menopause-by-country (accessed on October 18, 2024).
- Yisma, E.; Eshetu, N.; Ly, S.; Dessalegn, B. Prevalence and severity of menopause symptoms among perimenopausal and postmenopausal women aged 30-49 years in Gulele sub-city of Addis Ababa, Ethiopia. BMC women's health 2017, 17, 124–124. [Google Scholar] [CrossRef] [PubMed]
- Ghiasvand, R.; Adami, H.-O.; Harirchi, I.; Akrami, R.; Zendehdel, K. Higher incidence of premenopausal breast cancer in less developed countries; myth or truth? BMC Cancer 2014, 14, 343–343. [Google Scholar] [CrossRef]
- Munsell, M.F.; Sprague, B.L.; Berry, D.A.; Chisholm, G.; Trentham-Dietz, A. Body mass index and breast cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status. Epidemiologic Reviews 2014, 36, 114–136. [Google Scholar] [CrossRef]
- Trentham-Dietz, A.; Sprague, B.L.; Hampton, J.M.; Miglioretti, D.L.; Nelson, H.D.; Titus, L.J.; Egan, K.M.; Remington, P.L.; Newcomb, P.A. Modification of breast cancer risk according to age and menopausal status: a combined analysis of five population-based case–control studies. Breast Cancer Research and Treatment 2014, 145, 165–175. [Google Scholar] [CrossRef]
- Sidibe, E.H. La ménopause en Afrique. Annales d'Endocrinologie 2005, 66, 105–107. [Google Scholar] [CrossRef]
- Galal, S. Population of Africa 2021, by age group. Available online: https://www.statista.com/statistics/1226211/population-of-africa-by-age-group/ (accessed on October 5, 2024).
- Akakpo, P.K.; Imbeah, E.G.; Edusei, L.; Naporo, S.; Ulzen-Appiah, K.; Clegg-Lamptey, J.N.; Dedey, F.; Nsaful, J.; Affram, N.; Wiafe, B.; et al. Clinicopathologic characteristics of early-onset breast cancer: a comparative analysis of cases from across Ghana. BMC Women's Health 2023, 23, 5–5. [Google Scholar] [CrossRef] [PubMed]
- Anim, J.T. Breast diseases: Review of surgical material in Korle Bu hospital 1977-1978. Ghana medical journal 1979, 18, 30–33, doi:http://197.255.68.203/handle/123456789/3953. [Google Scholar]
- Mensah, A.C.; Yarney, J.; Nokoe, S.K.; Opoku, S.; Clegg-Lamptey, J.N. Survival Outcomes of Breast Cancer in Ghana: An Analysis of Clinicopathological Features. OALib 2016, 03, 1–11. [Google Scholar] [CrossRef]
- Ghartey, N.F.J.; Anyanful, A.; Eliason, S.; Mohammed Adamu, S.; Debrah, S. Pattern of Breast Cancer Distribution in Ghana: A Survey to Enhance Early Detection, Diagnosis, and Treatment. International Journal of Breast Cancer 2016, 2016, 3645308–3645308. [Google Scholar] [CrossRef]
- O'Neil, A. Age structure in Ghana 2022. 2024.
- Kwawukume, E.Y.; Ghosh, T.S.; Wilson, J.B. Menopausal age of Ghanaian women. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 1993, 40, 151–155. [Google Scholar] [CrossRef]
- Setorglo, J.; Keddey, R.S.; Agbemafle, I.; Kumordzie, S.; Steiner-Asiedu, M. Determinants of Menopausal Symptoms among Ghanaian Women. Current Research Journal of Biological Sciences 2012, 4, 507–512. [Google Scholar]
- Edmund, D.M.; Naaeder, S.B.; Tettey, Y.; Gyasi, R.K. Breast cancer in Ghanaian women: what has changed? American journal of clinical pathology 2013, 140, 97–102. [Google Scholar] [CrossRef]
- Clegg-lamptey, J.N.A.; Hodasi, W.M. A study of breast cancer in korle bu teaching hospital: assessing the impact of health education. Ghana medical journal 2007, 41. [Google Scholar] [CrossRef]
- Bosompem, K.; Yorke, J.; Buckman, T.A.; Brenu, S.G.; Nyantakyi, M.; Aitpillah, F.S.K.; Kyei, I.; Adinku, M.O.; Yorke, D.A.; Obirikorang, C.; et al. Comparative analysis of breast cancer characteristics in young premenopausal and postmenopausal women in Ghana. Scientific Reports 2024, 14, 2704–2704. [Google Scholar] [CrossRef] [PubMed]
- Siddig, A.; Din, T.A.D.A.A.T.; Nafi, S.N.M.; Yahya, M.M.; Sulong, S.; Rahman, W.F.W.A. The Unique Biology behind the Early Onset of Breast Cancer. Genes 2021, 12, 372–372. [Google Scholar] [CrossRef]
- Cathcart-Rake, E.J.; Ruddy, K.J.; Bleyer, A.; Johnson, R.H. Breast Cancer in Adolescent and Young Adult Women Under the Age of 40 Years. JCO Oncology Practice 2021, 17, 305–313. [Google Scholar] [CrossRef]
- Chelmow, D.; Pearlman, M.D.; Young, A.; Bozzuto, L.; Dayaratna, S.; Jeudy, M.; Kremer, M.E.; Scott, D.M.; O’Hara, J.S. Executive Summary of the Early-Onset Breast Cancer Evidence Review Conference. Obstetrics and gynecology 2020, 135, 1457–1478. [Google Scholar] [CrossRef]
- Laven, J.S.E. Genetics of Early and Normal Menopause. Seminars in reproductive medicine 2015, 33, 377–383. [Google Scholar] [CrossRef]
- Thasneem, K.; Kalarani, I.B.; Jayaprasad, P.; Mohammed, V.; Veerabathiran, R. Genes linked with early menopause and the pathogenesis of its associated diseases: a systematic review. Middle East Fertility Society Journal 2022, 27, 1–11. [Google Scholar] [CrossRef]
- Schoenaker, D.A.J.M.; Jackson, C.A.; Rowlands, J.V.; Mishra, G.D. Socioeconomic position, lifestyle factors and age at natural menopause: a systematic review and meta-analyses of studies across six continents. International journal of epidemiology 2014, 43, 1542–1562. [Google Scholar] [CrossRef]
- Cortés, Y.I.; Marginean, V. Key factors in menopause health disparities and inequities: Beyond race and ethnicity. Current Opinion in Endocrine and Metabolic Research 2022, 26, 100389–100389. [Google Scholar] [CrossRef]
- Wise, L.A.; Krieger, N.; Zierler, S.; Harlow, B.L. Lifetime socioeconomic position in relation to onset of perimenopause. Journal of Epidemiology and Community Health 2002, 56, 860–860. [Google Scholar] [CrossRef] [PubMed]
- Mobley, D.L.; Dill, K.A. Binding of small-molecule ligands to proteins: "what you see" is not always "what you get". Structure (London, England : 1993) 2009, 17, 489–498. [Google Scholar] [CrossRef]
- Sighoko, D.; Kamaté, B.; Traore, C.; Mallé, B.; Coulibaly, B.; Karidiatou, A.; Bourgeois, D. Breast cancer in pre-menopausal women in West Africa: analysis of temporal trends and evaluation of risk factors associated with reproductive life. Elsevier 2013, 22, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.; Kleer, C.G.; Martin, I.; Awuah, B.; Nsiah-Asare, A.; Takyi, V.; Braman, M.; E. Quayson, S.; Zarbo, R.; Wicha, M.; et al. African Ancestry and Higher Prevalence of Triple-Negative Breast Cancer: Findings From an International Study. Cancer 2010, 116, 4926–4932. [Google Scholar] [CrossRef]
- Akarolo-Anthony, S.N.; Ogundiran, T.O.; Adebamowo, C.A. Emerging breast cancer epidemic: evidence from Africa. Breast Cancer Research : BCR 2010, 12, S8–S8. [Google Scholar] [CrossRef]
- Ghana Statistical, S. Demographic and Health Survey 1993; Accra, 1994/12// 1994.
- Gabriel, C.A.; Domchek, S.M. Breast cancer in young women. Breast Cancer Research 2010, 12, 212–212. [Google Scholar] [CrossRef]
- Preston, D.L.; Mattsson, A.; Holmberg, E.; Shore, R.; Hildreth, N.G.; Boice, J.D. Radiation Effects on Breast Cancer Risk: A Pooled Analysis of Eight Cohorts. Radiation research 2002, 158, 220–235. [Google Scholar] [CrossRef]
- White, A.J.; Bradshaw, P.T.; Hamra, G.B. Air pollution and Breast Cancer: A Review. Current epidemiology reports 2018, 5, 92–100. [Google Scholar] [CrossRef]
- Figueroa, J.D.; Davis Lynn, B.C.; Edusei, L.; Titiloye, N.; Adjei, E.; Clegg-Lamptey, J.N.; Yarney, J.; Wiafe-Addai, B.; Awuah, B.; Duggan, M.A.; et al. Reproductive factors and risk of breast cancer by tumor subtypes among Ghanaian women: A population-based case-control study. International journal of cancer 2020, 147, 1535–1547. [Google Scholar] [CrossRef]
- Factbook, T.W. Mother's mean age at first birth Available online:. Available online: https://www.cia.gov/the-world-factbook/field/mothers-mean-age-at-first-birth/ (accessed on December 5, 2024).
- Robertson, C.; Primic-Zakelj, M.; Boyle, P.; Hsieh, C.C. Effect of parity and age at delivery on breast cancer risk in Slovenian women aged 25-54 years. International Journal of Cancer 1997, 73, 1–9. [Google Scholar] [CrossRef]
- Nguyen, B.; Venet, D.; Lambertini, M.; Desmedt, C.; Salgado, R.; Horlings, H.M.; Rothé, F.; Sotiriou, C. Imprint of parity and age at first pregnancy on the genomic landscape of subsequent breast cancer. Breast Cancer Research 2019, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Warner, E.T.; Colditz, G.A.; Palmer, J.R.; Partridge, A.H.; Rosner, B.A.; Tamimi, R.M. Reproductive factors and risk of premenopausal breast cancer by age at diagnosis: are there differences before and after age 40? Breast Cancer Res Treat 2013, 142, 165–175. [Google Scholar] [CrossRef]
- Hinkula, M.; Pukkala, E.; Kyyrönen, P.; Kauppila, A. Grand multiparity and the risk of breast cancer: population-based study in Finland. Cancer causes & control 2001, 12, 491–500. [Google Scholar] [CrossRef]
- Review, W.P. Age of Menarche by Country 2024. Available online: https://worldpopulationreview.com/country-rankings/age-of-menarche-by-country (accessed on October 18, 2024).
- Adadevoh, S.W.K.; Agble, T.K.; Hobbs, C.; Elkins, T.E. Menarcheal age in Ghanaian school girls. International Journal of Gynecology and Obstetrics 1989, 30, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Ameade, E.P.K.; Garti, H.A. Age at Menarche and Factors that Influence It: A Study among Female University Students in Tamale, Northern Ghana. PloS one 2016, 11, e0155310–e0155310. [Google Scholar] [CrossRef] [PubMed]
- Reagan, P.B.; Salsberry, P.J.; Fang, M.Z.; Gardner, W.P.; Pajer, K. African-American/white differences in the age of menarche: Accounting for the difference. Social Science & Medicine 2012, 75, 1263–1270. [Google Scholar] [CrossRef]
- Garenne, M. Age at menarche in Nigerian demographic surveys. Journal of Biosocial Science 2021, 53, 745–757. [Google Scholar] [CrossRef]
- Estuardo, J.; Irastorza, L.; García Rodríguez, F.; Figueroa Preciado, G.; Marín, I.H.; Ayala, A.R. Early menarche as a risk factor of breast cancer. Ginecología y Obstetricia de México 2006, 74, 568–572. [Google Scholar]
- Okonofua, F.E.; Lawal, A.; Bamgbose, J.K. Features of menopause and menopausal age in Nigerian women. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics 1990, 31, 341–345. [Google Scholar] [CrossRef]
- Reynolds, P. Smoking and breast cancer. Journal of mammary gland biology and neoplasia 2013, 18, 15–23. [Google Scholar] [CrossRef]
- González-Jiménez, E.; García, P.A.; Aguilar, M.J.; Padilla, C.A.; Álvarez, J. Breastfeeding and the prevention of breast cancer: a retrospective review of clinical histories. Journal of clinical nursing 2014, 23, 2397–2403. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Biessy, C.; Joffe, M.; Cubasch, H.; Norris, S.; Vorster, H.H.; Taljaard-Krugell, C.; Gunter, M.J.; Rinaldi, S. Reproductive factors and risk of breast cancer in black South African women. Cancer Causes Control 2021, 32, 415–415. [Google Scholar] [CrossRef]
- Butt, S.; Borgquist, S.; Anagnostaki, L.; Landberg, G.; Manjer, J. Breastfeeding in relation to risk of different breast cancer characteristics. BMC Research Notes 2014, 7, 1–12. [Google Scholar] [CrossRef]
- Stordal, B. Breastfeeding reduces the risk of breast cancer: A call for action in high-income countries with low rates of breastfeeding. Cancer Medicine 2022, 12, 4616–4616. [Google Scholar] [CrossRef]
- Bothou, A.; Zervoudis, S.; Iliadou, M.; Pappou, P.; Iatrakis, G.; Tsatsaris, G.; Peitsidis, P.; Gerende, A.; Chalkidou, A.; Anthoulaki, X.; et al. Breastfeeding and Breast Cancer Risk: Our Experience and Mini-review of the Literature. Materia Socio-Medica 2022, 34, 28–28. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, G.; Bothou, A.; Eirini, O.; Daglas, M.; Iliadou, M.; Antoniou, E.; Palaska, E. Breastfeeding and its Association with Breast Cancer: a Systematic Review of the Literature. Mædica 2024, 19, 106–106. [Google Scholar] [CrossRef] [PubMed]
- Andrikopoulou, A.; Chatzinikolaou, S.; Kyriopoulos, I.; Bletsa, G.; Kaparelou, M.; Liontos, M.; Dimopoulos, M.A.; Zagouri, F. The Mutational Landscape of Early-Onset Breast Cancer: A Next-Generation Sequencing Analysis. Frontiers in Oncology 2022, 11, 797505–797505. [Google Scholar] [CrossRef]
- Ssentongo, P.; Oh, J.S.; Amponsah-Manu, F.; Wong, W.; Candela, X.; Acharya, Y.; Ssentongo, A.E.; Dodge, D.G. Breast Cancer Survival in Eastern Region of Ghana. Frontiers in Public Health 2022, 10, 880789–880789. [Google Scholar] [CrossRef]
- Limaiem, F.; Ahmad, F. Mucinous Breast Carcinoma. In StatPearls; StatPearls Publishing: 2023.
- Hercules, S.M.; Alnajar, M.; Chen, C.; Mladjenovic, S.M.; Shipeolu, B.A.; Perkovic, O.; Pond, G.R.; Mbuagbaw, L.; Blenman, K.R.; Daniel, J.M. Triple-negative breast cancer prevalence in Africa: a systematic review and meta-analysis. BMJ Open 2022, 12, e055735–e055735. [Google Scholar] [CrossRef]
- Espina, C.; McKenzie, F.; dos-Santos-Silva, I. Delayed presentation and diagnosis of breast cancer in African women: a systematic review. Annals of Epidemiology 2017, 27, 659–659. [Google Scholar] [CrossRef]
- Ohene-Yeboah, M.; Adjei, E. Breast cancer in Kumasi, Ghana. Ghana Med J 2012, 46, 8–13. [Google Scholar]
- Jiagge, E.M.; Oppong, J.K.; Awuah, B.; Newman, L.A.; Wicha, M.; Merajver, S. Characteristics of breast cancer in Ghana and prevalence of aggressive disease and high mortality. Journal of Clinical Oncology 2014, 32, 596–596. [Google Scholar] [CrossRef]
- Jedy-Agba, E.; McCormack, V.; Adebamowo, C.; dos-Santos-Silva, I. Stage at diagnosis of breast cancer in sub-Saharan Africa: a systematic review and meta-analysis. The Lancet Global Health 2016, 4, e923–e935. [Google Scholar] [CrossRef]
- Ahearn, T.U.; Choudhury, P.P.; Derkach, A.; Wiafe-Addai, B.; Awuah, B.; Yarney, J.; Edusei, L.; Titiloye, N.; Adjei, E.; Vanderpuye, V.; et al. Breast Cancer Risk in Women from Ghana Carrying Rare Germline Pathogenic Mutations. Cancer Epidemiology Biomarkers and Prevention 2022, 31, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participants’ Case Classification. The age range of all participants recruited (A), proportion of premenopausal and postmenopausal using 50 years (B) and 48 years (C) and EOBC and LOBC (D) case groups. Participants’ age ranged from 27 to 83 years; the peak age at diagnosis (red dashed peaks) was 50 years (A). Approximately 34.4% of the cases were premenopausal breast cancer (B) and 14.9% were EOBC (C). Pre – Premenopausal breast cancer; Post – Postmenopausal breast cancer; EOBC – early-onset breast cancer; LOBC – Late-onset breast cancer.
Figure 1.
Participants’ Case Classification. The age range of all participants recruited (A), proportion of premenopausal and postmenopausal using 50 years (B) and 48 years (C) and EOBC and LOBC (D) case groups. Participants’ age ranged from 27 to 83 years; the peak age at diagnosis (red dashed peaks) was 50 years (A). Approximately 34.4% of the cases were premenopausal breast cancer (B) and 14.9% were EOBC (C). Pre – Premenopausal breast cancer; Post – Postmenopausal breast cancer; EOBC – early-onset breast cancer; LOBC – Late-onset breast cancer.
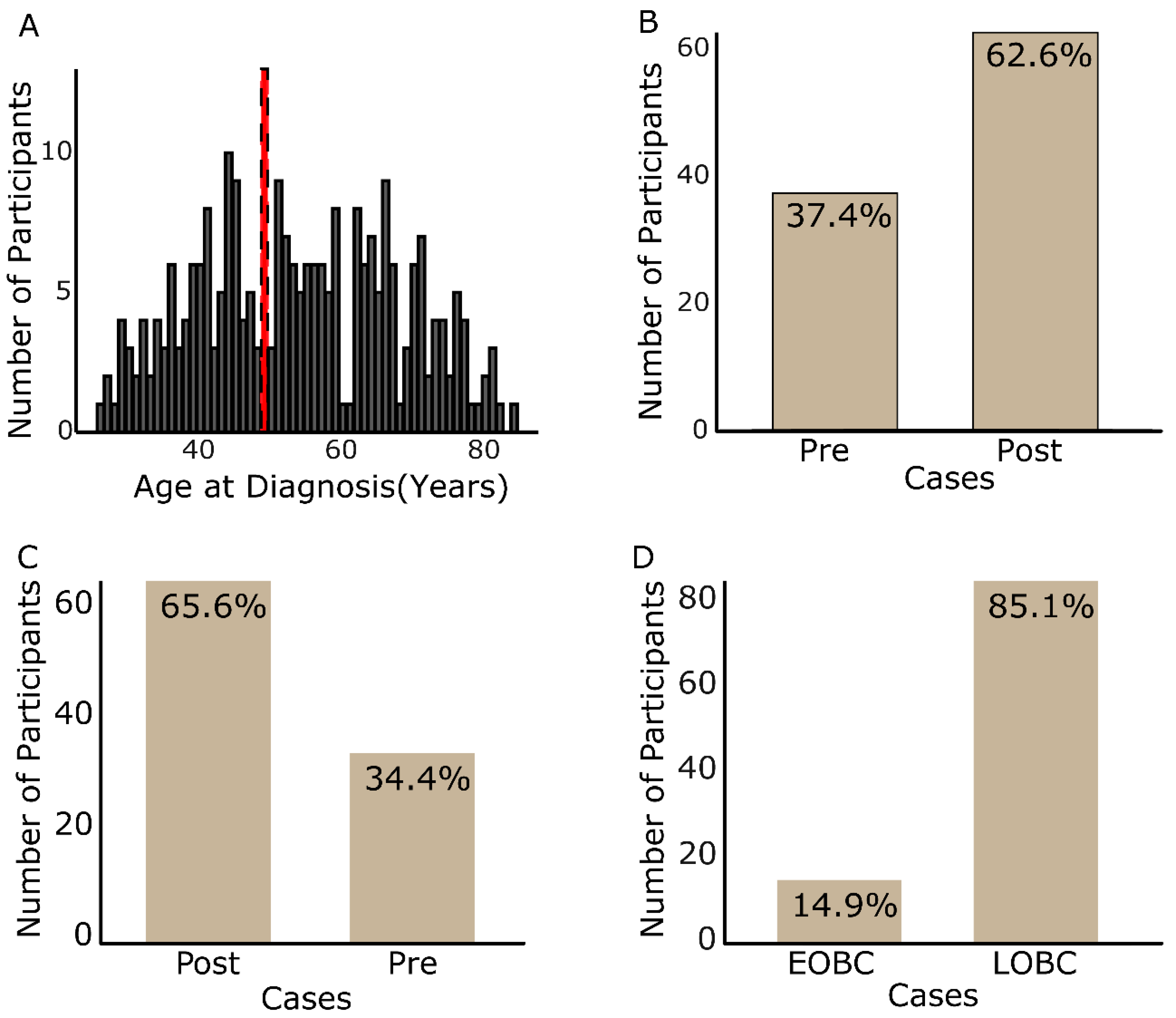
Figure 2.
Menstrual status of participants. About 5.4% of the participants diagnosed at 48 years and older were still menstruating and 16.2% of those diagnosed below 48 years were menopausal. Two participants had never menstruated. Post – postmenopausal; Pre - premenopausal.
Figure 2.
Menstrual status of participants. About 5.4% of the participants diagnosed at 48 years and older were still menstruating and 16.2% of those diagnosed below 48 years were menopausal. Two participants had never menstruated. Post – postmenopausal; Pre - premenopausal.
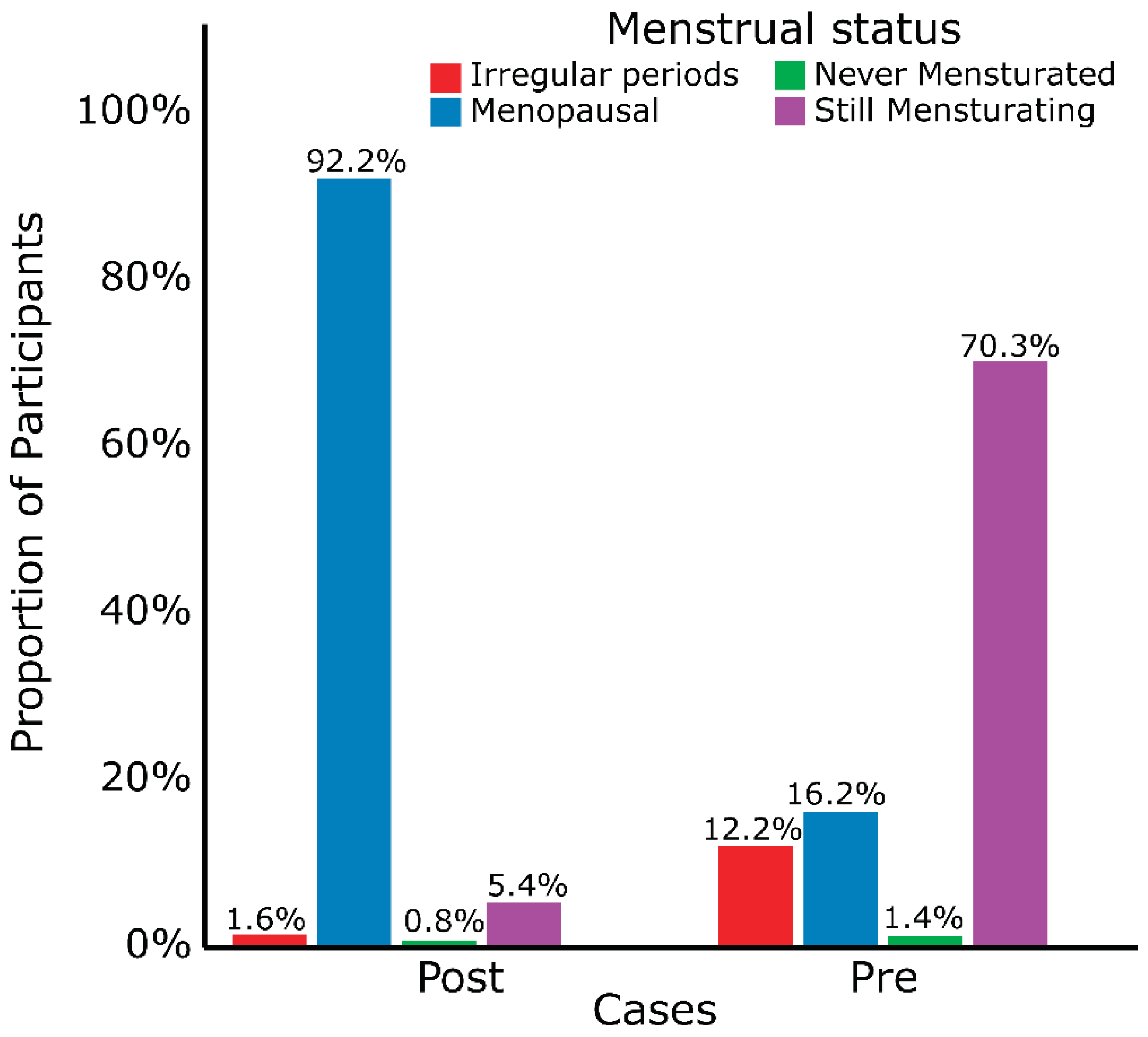

Table 1.
General Demographics.
| Menopausal Description | Onset Description | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | N | Overall N = 2621 |
Post N = 1721 |
Pre N = 901 |
p-value2 | EOBC N = 391 |
LOBC N = 2231 |
p-value3 | |
| Age at Diagnosis | 262 | 54 (27, 85) | 63 (48, 85) | 41 (27, 47) | 35 (27, 39) | 57 (40, 85) | |||
| Menopause age | 120 | 48 (27, 60) | 49 (32, 60) | 42 (27, 45) | <0.001 | 27 (27, 27) | 48 (32, 60) | 0.087 | |
| Menarche age | 192 | 15 (10, 25) | 15 (10, 25) | 15 (11, 19) | 0.005 | 14 (11, 17) | 15 (10, 25) | <0.001 | |
| Primiparity age | 233 | 24 (15, 54) | 23 (15, 54) | 27 (15, 41) | <0.001 | 27 (16, 35) | 24 (15, 54) | 0.024 | |
| Parity | 259 | 3 (0, 9) | 3 (0, 9) | 2 (0, 7) | <0.001 | 1 (0, 4) | 3 (0, 9) | <0.001 | |
| Gravidity | 232 | 4 (0, 10) | 4 (0, 10) | 3 (0, 10) | <0.001 | 2 (0, 5) | 4 (0, 10) | <0.001 | |
| Tribe | 246 | 0.10 | 0.070 | ||||||
| Akan | 110 (45%) | 74 (45%) | 36 (44%) | 16 (50%) | 94 (44%) | ||||
| Ewe | 53 (22%) | 29 (18%) | 24 (29%) | 11 (34%) | 42 (20%) | ||||
| Ga-Adangbe | 60 (24%) | 46 (28%) | 14 (17%) | 3 (9.4%) | 57 (27%) | ||||
| Others | 23 (9%) | 15 (9.1%) | 8 (9.8%) | 2 (6.3%) | 21 (9.8%) | ||||
| Menstrual status | 262 | <0.001 | <0.001 | ||||||
| Postmenopausal | 171 (65%) | 155 (90%) | 16 (18%) | 2 (5.1%) | 169 (76%) | ||||
| Premenopausal | 67 (26%) | 7 (4%) | 60 (67%) | 29 (74%) | 38 (17%) | ||||
| others | 24 (9%) | 10 (6%) | 14 (16%) | 8 (21%) | 16 (7.2%) | ||||
| Occupation | 262 | <0.001 | <0.001 | ||||||
| Others | 67 (26%) | 31 (18%) | 36 (40%) | 18 (46%) | 49 (22%) | ||||
| Student/Unemployed/Retired | 72 (27%) | 67 (39%) | 5 (5.6%) | 3 (8%) | 69 (31%) | ||||
| Trader/Businesswoman | 123 (47%) | 74 (43%) | 49 (54%) | 18 (46%) | 105 (47%) | ||||
| Residence | 252 | 0.2 | 0.7 | ||||||
| Peri-Urban | 133 (53%) | 94 (57%) | 39 (45%) | 19 (51%) | 114 (53%) | ||||
| Rural | 7 (3%) | 5 (3%) | 2 (2%) | 0 (0%) | 7 (3.3%) | ||||
| Urban | 112 (44%) | 66 (40%) | 46 (53%) | 18 (49%) | 94 (44%) | ||||
| Detection | 201 | 0.3 | 0.2 | ||||||
| ME | 64 (32%) | 39 (29%) | 25 (37%) | 6 (22%) | 58 (33%) | ||||
| SE | 137 (68%) | 94 (71%) | 43 (63%) | 21 (78%) | 116 (67%) | ||||
| Mammogram | 253 | 0.009 | <0.001 | ||||||
| No | 35 (14%) | 16 (10%) | 19 (22%) | 12 (32%) | 23 (11%) | ||||
| Yes | 218 (86%) | 149 (90%) | 69 (78%) | 26 (68%) | 192 (89%) | ||||
1n (%) for categorical; Median (Range) for continuous; 2,3Wilcoxon rank sum test; Pearson's Chi-squared test; Fisher's exact test; ME – Medical examination; SE – self-examination; Pre – premenopausal; Post - postmenopausal.
Table 2.
Participants’ Reproductive factors.
| Menopausal Description | Onset Description | |||||||
|---|---|---|---|---|---|---|---|---|
| Reproductive Factors | N | Overall N = 2621 |
Post N = 1721 |
Pre N = 901 |
p-value2 | EOBC N = 391 |
LOBC N = 2231 |
p-value2 |
| Primiparity | 233 | 0.002 | 0.10 | |||||
| 24 | 14 (6%) | 12 (8%) | 2 (2.7%) | 0 (0%) | 14 (6.7%) | |||
| >24 | 109 (47%) | 62 (39%) | 47 (64%) | 16 (67%) | 93 (44%) | |||
| <24 | 110 (47%) | 85 (53%) | 25 (34%) | 8 (33%) | 102 (49%) | |||
| Menarche | 192 | 0.012 | 0.002 | |||||
| 15 | 48 (25%) | 27 (23%) | 21 (28%) | 10 (33%) | 38 (23%) | |||
| >15 | 66 (34%) | 50 (42%) | 16 (22%) | 2 (6.7%) | 64 (40%) | |||
| <15 | 78 (41%) | 41 (35%) | 37 (50%) | 18 (60%) | 60 (37%) | |||
| Menopausal age | 120 | <0.001 | 0.5 | |||||
| 48 | 11 (9%) | 11 (10%) | 0 (0%) | 0 (0%) | 11 (9.2%) | |||
| >48 | 55 (46%) | 55 (50%) | 0 (0%) | 0 (0%) | 55 (46%) | |||
| <48 | 54 (45%) | 44 (40%) | 10 (100%) | 1 (100%) | 53 (45%) | |||
| Gravidity | 262 | 0.018 | <0.001 | |||||
| 0 | 44 (17%) | 24 (14%) | 20 (22%) | 15 (38%) | 29 (13%) | |||
| 4 | 58 (22%) | 40 (23%) | 18 (20%) | 5 (13%) | 53 (24%) | |||
| >4 | 77 (29%) | 60 (35%) | 17 (19%) | 4 (10%) | 73 (33%) | |||
| <4 | 83 (32%) | 48 (28%) | 35 (39%) | 15 (38%) | 68 (30%) | |||
| Parity | 262 | <0.001 | <0.001 | |||||
| 0 | 23 (9%) | 6 (4%) | 17 (19%) | 14 (36%) | 9 (4%) | |||
| 3 | 73 (28%) | 49 (28%) | 24 (27%) | 7 (18%) | 66 (30%) | |||
| >3 | 82 (31%) | 64 (37%) | 18 (20%) | 3 (7.7%) | 79 (35%) | |||
| <3 | 84 (32%) | 53 (31%) | 31 (34%) | 15 (38%) | 69 (31%) | |||
| Breastfeed | 242 | 0.5 | 0.14 | |||||
| No | 12 (5%) | 7 (4%) | 5 (6%) | 3 (11%) | 9 (4.2%) | |||
| Yes | 230 (95%) | 157 (96%) | 73 (94%) | 24 (89%) | 206 (96%) | |||
| Breastfeeding duration | 222 | 0.11 | 0.6 | |||||
| 6-12 | 63 (28%) | 48 (31%) | 15 (22%) | 5 (24%) | 58 (29%) | |||
| >12 | 149 (67%) | 97 (63%) | 52 (76%) | 16 (76%) | 133 (66%) | |||
| <6 | 10 (5%) | 9 (6%) | 1 (2%) | 0 (0%) | 10 (5%) | |||
1n (%) for categorical variables; 2Fisher's exact test; Pearson's Chi-squared test.
Table 3.
Clinicopathological Characteristics of Participants’ Tumours.
| Menopausal Description | Onset Description | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | N | Overall N = 2621 |
Post N = 1721 |
Pre N = 901 |
p-value2 | EOBC N = 391 |
LOBC N = 2231 |
p-value2 |
| Tumours | 212 | 0.5 | >0.9 | |||||
| Carcinoma NST | 2 (1%) | 1 (1%) | 1 (1.3%) | 0 (0%) | 2 (1%) | |||
| Ductal Carcinoma in situ | 28 (13%) | 19 (14%) | 9 (12%) | 6 (16%) | 22 (13%) | |||
| Inflammatory Carcinoma | 2 (1%) | 2 (2%) | 0 (0%) | 0 (0%) | 2 (1%) | |||
| Invasive Carcinoma NST | 119 (56%) | 67 (51%) | 52 (64%) | 20 (54%) | 99 (57%) | |||
| Invasive Ductal Carcinoma | 38 (18%) | 24 (18%) | 14 (18%) | 8 (22%) | 30 (17%) | |||
| Invasive Lobular Carcinoma | 10 (5%) | 9 (7%) | 1 (1.3%) | 1 (3%) | 9 (5%) | |||
| Other Malignant | 13 (6%) | 9 (7%) | 4 (5.2%) | 2 (5%) | 11 (6%) | |||
| Tumour Stage | 47 | 0.5 | 0.8 | |||||
| I | 9 (19%) | 4 (15%) | 5 (25%) | 3 (27%) | 6 (17%) | |||
| II | 29 (62%) | 19 (70%) | 10 (50%) | 6 (55%) | 23 (64%) | |||
| III | 7 (15%) | 3 (11%) | 4 (20%) | 2 (18%) | 5 (14%) | |||
| IV | 2 (4%) | 1 (3.7%) | 1 (5.0%) | 0 (0%) | 2 (5.6%) | |||
| Tumour Grade | 149 | 0.4 | 0.7 | |||||
| 1 | 31 (21%) | 22 (24%) | 9 (16%) | 5 (19%) | 26 (21%) | |||
| 2 | 76 (51%) | 46 (51%) | 30 (52%) | 12 (46%) | 64 (52%) | |||
| 3 | 42 (28%) | 23 (25%) | 19 (33%) | 9 (35%) | 33 (27%) | |||
| Molecular Classification | 152 | 0.7 | 0.9 | |||||
| HER2-enriched | 4 (3%) | 3 (3%) | 1 (1.8%) | 1 (3.8%) | 3 (2.4%) | |||
| HR- | 29 (19%) | 15 (16%) | 14 (25%) | 6 (23%) | 23 (18%) | |||
| HR-_HER2_equivocal | 1 (1%) | 1 (1%) | 0 (0%) | 0 (0%) | 1 (0.8%) | |||
| HR+ | 85 (56%) | 56 (58%) | 29 (52%) | 13 (50%) | 72 (57%) | |||
| HR+_HER2_equivocal | 8 (5%) | 6 (6%) | 2 (3.6%) | 1 (3.8%) | 7 (5.6%) | |||
| TNBC | 25 (16%) | 15 (16%) | 10 (18%) | 5 (19%) | 20 (16%) | |||
| Symptoms | 262 | 0.5 | 0.14 | |||||
| Lump in breast | 159 (60.7%) | 101 (59%) | 58 (64%) | 29 (74%) | 130 (58%) | |||
| Others | 62 (23.7%) | 41 (24%) | 21 (23%) | 7 (18%) | 55 (25%) | |||
| Painful breast | 41 (15.6%) | 30 (17%) | 11 (12%) | 3 (7.7%) | 38 (17%) | |||
1n (%); 2Fisher's exact test; Pearson's Chi-squared test; HR – Hormone Receptor, TNBC – Triple-negative Breast cancer; NST – No Special Type.
Table 4.
Participant’s family history and lifestyle.
| Menopausal Description | Onset Description | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristic | N | Overall N = 2621 |
Post N = 1721 |
Pre N = 901 |
p-value2 | EOBC N = 391 |
LOBC N = 2231 |
p-value2 |
| Contraceptives | 244 | 0.3 | 0.005 | |||||
| No | 174 (71%) | 116 (73%) | 58 (67%) | 18 (51%) | 156 (75%) | |||
| 70 (29%) | 42 (27%) | 28 (33%) | 17 (49%) | 53 (25%) | ||||
| Alcohol | 242 | 0.8 | 0.9 | |||||
| Daily | 3 (1%) | 3 (2%) | 0 (0%) | 0 (0%) | 3 (1%) | |||
| Monthly | 9 (4%) | 6 (4%) | 3 (3%) | 1 (3%) | 8 (3%) | |||
| Not at all | 177 (73%) | 113 (73%) | 64 (73%) | 30 (81%) | 147 (72%) | |||
| Weekly | 2 (1%) | 1 (1%) | 1 (1%) | 0 (0%) | 2 (1%) | |||
| Yearly | 51 (21%) | 31 (20%) | 20 (23%) | 6 (16%) | 45 (22%) | |||
| Smoking | 251 | 0.5 | >0.9 | |||||
| No | 249 (99%) | 160 (99%) | 89 (100%) | 38 (100%) | 211 (99%) | |||
| Yes | 2 (0.8%) | 2 (1%) | 0 (0%) | 0 (0%) | 2 (0.9%) | |||
| Bleaching cream | 262 | 0.070 | 0.3 | |||||
| No | 228 (87%) | 145 (84%) | 83 (92%) | 36 (92%) | 192 (86%) | |||
| Yes | 34 (13%) | 27 (16%) | 7 (7.8%) | 3 (7.7%) | 31 (14%) | |||
| Family History | 262 | 0.7 | 0.5 | |||||
| No | 227 (87%) | 150 (87%) | 77 (86%) | 35 (90%) | 192 (86%) | |||
| Yes | 35 (13%) | 22 (13%) | 13 (14%) | 4 (10%) | 31 (14%) | |||
| Knowledge | 242 | 0.10 | 0.8 | |||||
| Yes | 190 (79%) | 119 (75%) | 71 (85%) | 27 (77%) | 163 (79%) | |||
| No | 52 (21%) | 39 (25%) | 13 (15%) | 8 (23%) | 44 (21%) | |||
1n (%) for categorical; 2Pearson's Chi-squared test; Fisher's exact test.
Table 5.
Multivariate Logistic Regression Analysis .
| Premenopausal | EOBC | |||
|---|---|---|---|---|
| Predictor | ORa (95%CI) | p-value | ORa (95% CI) | p-value |
| Occupation | ||||
| Employed/Self-Employed | __ | __ | __ | __ |
| Unemployed | 0.118 (0.045–0.310) |
<0.001 | 0.183 (0.051–0.656) |
0.009 |
| Primiparity | ||||
| <24 | __ | __ | __ | __ |
| ≥24 | 2.108 (1.151–3.859) |
0.016 | __ | __ |
| Parity | ||||
| Parous | __ | __ | __ | __ |
| Nulliparous | __ | __ | 13.491 (5.059–35.980) |
<0.001 |
a Adjusted odds ratio, CI – Confidence interval. Model performance: Premenopausal group: AUC=0.7194; Hosmer–Lemeshow χ²=1.21, p=0.547; Model performance; EOBC (N=262): AUC=0.7190; Hosmer–Lemeshow χ²=0.74, p=0.3909; Model 1 (premenopausal): included occupation and age at first birth; Model 2 (EOBC): included parity and occupation; Employed/Self-Employed included (traders, business women, farmers, Secretary/Clerical workers and Professional workers; and Student/Unemployed consisted of students and retirees. Model performance: Premenopausal (N=233): AUC=0.7194; Hosmer–Lemeshow χ²=1.21, p=0.547.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



