Submitted:
02 September 2025
Posted:
03 September 2025
You are already at the latest version
Abstract
Background: Distal pancreatectomy is a potentially curative treatment for tumors of the pancreatic body and tail. Minimally invasive approaches, notably laparoscopic and robotic techniques, have gained increasing acceptance. This network meta-analysis aimed to compare perioperative outcomes of open, laparoscopic, and robotic distal pancreatectomy. Methods: A systematic search of MEDLINE, EMBASE, Web of Science, and Scopus identified studies comparing at least two approaches. Both Bayesian and frequentist network meta-analyses were conducted. Results: Sixty-seven studies including 18,113 patients met inclusion criteria. Surface under the cumulative ranking (SUCRA) analysis showed robotic surgery ranked first in 84.6% of measured parameters, accumulating 92.3% of total points. Laparoscopy showed intermediate results, while open surgery ranked lowest. Robotic, but not laparoscopic, surgery significantly reduced 30-day mortality (Odds Ratio [OR] = 0.37, 95% Confidence Interval [CI] 0.16–0.84) and lowered conversion rates compared with laparoscopy (OR = 0.30, 95% Credible Interval [CrI] 0.22–0.40). Both robotic and laparoscopic approaches, compared with open surgery, were associated with reduced blood loss (-304 mL and -273 mL), fewer transfusions (OR 0.25 and 0.30), smaller transfused volumes (-1.98 and -1.86 units), shorter ICU stays (-4.0 and -2.3 days), fewer reinterventions (OR 0.45 and 0.56), and shorter hospital stays (-8.8 and -6.9 days). Conclusions: Robotic distal pancreatectomy appears safe and confers significant advantages over open and laparoscopic surgery, including reduced 30-day mortality, lower conversion rates, and improved perioperative outcomes, when performed in appropriately equipped, high-volume settings.
Keywords:
distal pancreatectomy
; robotic surgery
; laparoscopy
; open approach
; network meta-analysis
; meta-regression
Introduction
The incidence of pancreatic ductal adenocarcinoma (PDAC) has increased in recent decades, making it the twelfth most common cancer and the sixth leading cause of cancer-related mortality worldwide [1]. Tumors located in the body and tail of the pancreas account for approximately 20–25% of all PDAC cases [2]. Additionally, the widespread use of advanced imaging modalities has led to an increase in the incidental detection of asymptomatic pancreatic lesions, including pancreatic neuroendocrine tumors (pNETs) and cystic neoplasms [3,4].
Distal pancreatectomy is the procedure of choice for resectable lesions of the pancreatic body and tail. Since the introduction of laparoscopic distal pancreatectomy (LDP) in 1994 [5] and robotic distal pancreatectomy (RDP) in 2003 [6], there has been increasing interest in minimally invasive distal pancreatectomy (MIDP). Randomized controlled trials [7,8] and large series from high-volume centers [9,10,11] have demonstrated that MIDP offers several advantages over open distal pancreatectomy (ODP), including reduced intraoperative blood loss, shorter hospital stays, faster recovery, and comparable oncologic outcomes [12].
Both the Miami [13] and Brescia [14] guidelines now support the use of MIDP as a standard alternative to ODP for benign, low-grade malignant, and selected malignant lesions, provided that the procedure is performed by experienced surgeons in high-volume centers. Despite the technical advantages offered by the robotic platform, such as high-resolution three-dimensional visualization, tremor filtration, motion scaling, and improved ergonomics, laparoscopy remains the most widely used minimally invasive approach to distal pancreatectomy [15].
With the growing number of heterogeneous studies comparing distal pancreatectomy surgical techniques, a network meta-analysis to further explore open, laparoscopic, and robotic distal pancreatectomy is needed. This method integrates both direct and indirect evidence, allowing for a more comprehensive evaluation of each technique.
Therefore, this study aimed to conduct a network meta-analysis comparing the perioperative outcomes of open, laparoscopic, and robotic distal pancreatectomy.
Methods
Network meta-analysis (NMA) provides a comprehensive overview of treatment options by facilitating indirect comparisons between various surgical approaches.
We conducted an indirect comparison of different surgical techniques concerning the primary and secondary outcomes. Our investigation focused on identifying the “relatively most” minimally invasive surgical approach, robotic, laparoscopic, or open, for left pancreatectomies.
Protocol and Registration
This study followed the PRISMA-NMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses incorporating Network Meta-analyses) guidelines [16]. The study protocol was registered on the Open Science Framework (OSF—osf.io/ghtaz).
Eligibility Criteria
We included randomized controlled trials (RCTs), prospective non-randomized comparative studies, and retrospective cohort studies that compared any two or more of the following surgical techniques for distal pancreatectomy: open (OG), laparoscopic (LG), and robotic (RG) surgery. Studies were eligible if they reported at least one of the following perioperative outcomes: patient age, sex, ASA status, history of cardiovascular comorbidities, intraoperative blood loss, quantity of transfused blood, conversion to open surgery, ICU stay, operative time, reintervention, readmission, in-hospital or 30-day mortality, 90-day major complications, and postoperative hospital stay length. The exclusion criteria were as follows: (1) non-comparative studies; (2) case reports or case series with fewer than 10 patients; (3) studies on central or total pancreatectomy; (4) animal studies; and (5) abstracts without full-text availability.
Information Sources and Search Strategy
A systematic search was conducted in MEDLINE (via PubMed), EMBASE, Web of Science, and Scopus from inception to December 2024. The search included MeSH terms and keywords such as “distal pancreatectomy”, “left pancreatectomy”, “robotic”, “laparoscopic”, “minimally invasive”. Manual searches of the references of relevant studies and systematic reviews were also performed.
Study Selection
All search results were imported into Paperpile and screened. Duplicates were removed, and title and abstract screening was performed. The full texts of potentially eligible studies were assessed independently, with disagreements resolved through discussion or consultation with a third reviewer.
Data Collection Process and Data Items
The data were extracted using a standardized collection form. The extracted information included the first author, year of publication, country, study design, number of patients in each arm, surgical approach (open, laparoscopic, robotic), patient demographics (age, sex), ASA status, comorbidities, and all predefined perioperative outcomes. When available, we recorded means with standard deviations, medians with interquartile ranges, and event counts with sample sizes.
Risk of Bias Assessment
For non-randomized studies, the Newcastle-Ottawa Scale (NOS) was applied, and papers with a score of 6 and above were selected. For prospective randomized controlled trial (RCT), the Cochrane Risk of Bias 2.0 tool was applied. Discrepancies were resolved through consensus (Table 1).
Outcome Measures
Seventeen predefined perioperative outcomes were analyzed in this study. Continuous outcomes (e.g., operative time, blood loss, and hospital stay) were expressed as mean differences (MD), whereas dichotomous outcomes (e.g., mortality and reintervention) were reported using odds ratios (OR). Each outcome was pooled using both frequentist and Bayesian network meta-analyses.
Geometry of the Network
Network plots were constructed for each outcome to assess the structure of the available comparisons across the interventions. The number of direct and indirect comparisons per network was recorded.
Summary Measures and Statistical Analysis
Frequentist NMA was performed using the netmeta package in R (version 4.3.0), applying a random-effects model based on the DerSimonian-Laird method for variance estimation. For Bayesian NMA, we used the gemtc, BUGSnet, and bnma packages with Markov Chain Monte Carlo (MCMC) simulations implemented in JAGS. Three chains were run for 10,000 iterations after a burn-in of 5,000 iterations, with convergence evaluated using the Gelman–Rubin diagnostic.
Treatment rankings were evaluated using the Surface Under the Cumulative Ranking curve (SUCRA). To better visualize the results, we used Litmus Rank-O-Gram and Radial SUCRA plots [17].
Network inconsistency was assessed using global (design-by-treatment interaction) and local (node-splitting) approaches. The consistency between direct and indirect evidence was evaluated, being declared when P < 0.05 [18].
Model fit was evaluated by comparing the deviance information criterion (DIC), residual deviance, and leverage plots. We investigated the deviance of the model using the residual deviance from the NMA model, unrelated mean effect (UME) inconsistency model, per-arm residual deviance, and leverage plot for all studies [19].
Meta-regression was conducted using publication year and sample size as covariates to explore sources of heterogeneity [20].
Assessment of Inconsistency and Small-Study Effects
Inconsistency between direct and indirect comparisons was explored using global tests and node-splitting models. Funnel and comparison-adjusted funnel plots were generated to assess potential publication bias and small-study effects.
Additional Analyses
Prespecified sensitivity analyses included (1) restricting studies with a low risk of bias and (2) excluding outliers. Subgroup analyses were conducted based on the publication year and surgical volume.
Software
Results
Search Results
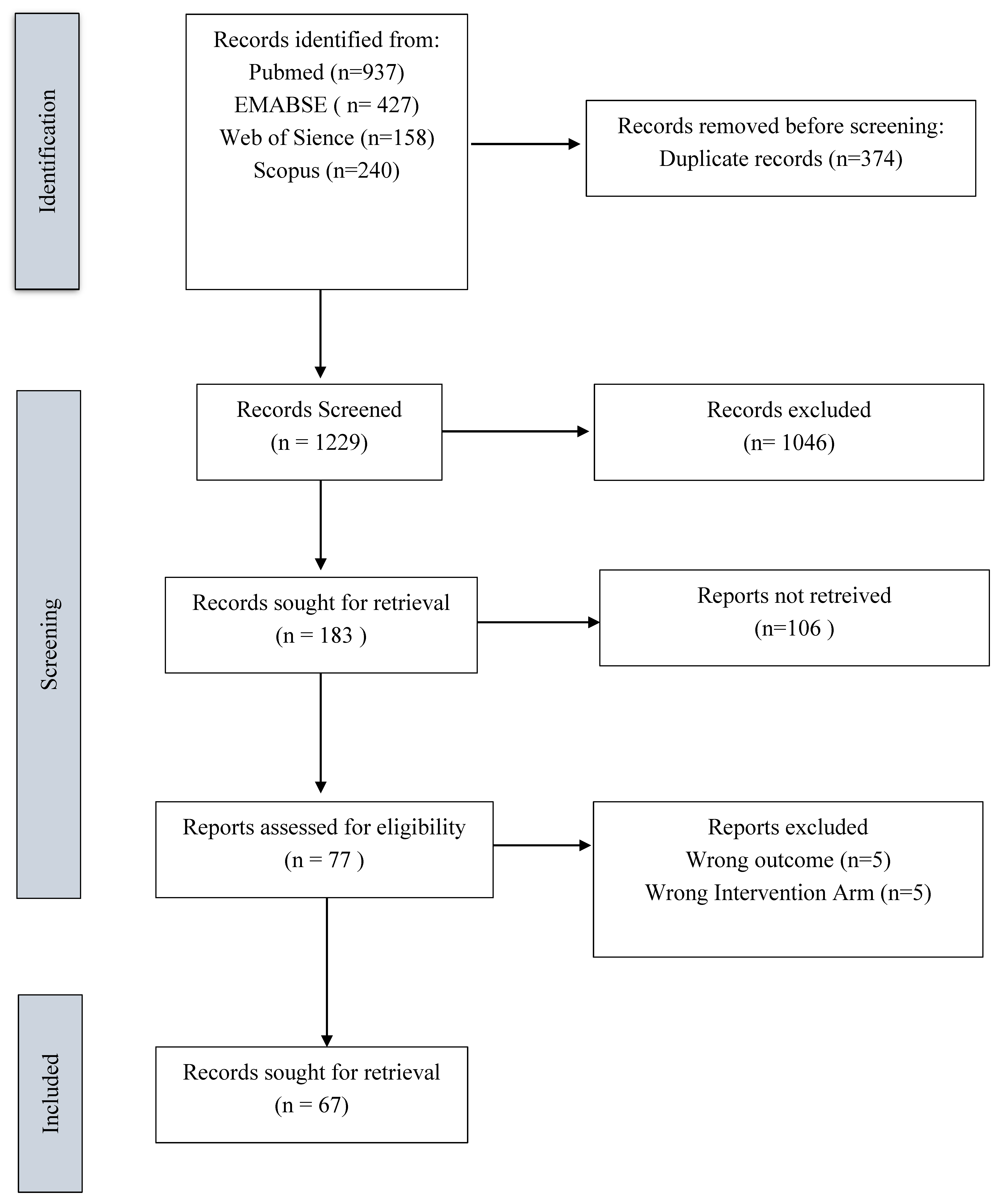
Characteristics of the Included Studies
We included 67 studies in the network meta-analysis (NMA). The baseline characteristics are presented in Table 2.
Outcomes NMA:
We examined 17 parameters that comprise preoperative, intraoperative and short term postoperative results. The outcomes are summarized in Table 3.
Age of Patients
For the age of the patients (mean 59.5 years), there were 59 studies including 17,542 patients in the network (Supplementary Table 1, Supplementary Figure 1). There were 52 two-arm and 7 multi-arm studies. A total of 73 pairwise comparisons were available. Specifically, eight trials compared open vs. robotic, 29 trials open vs. laparoscopic, and 36 trials laparoscopic vs. robotic (Supplementary Figure 2).
In the frequentist NMA, the robotic group (RG) had a statistically significantly lower mean age than the open group (OG), with a mean difference (MD) of –1.65 years (95% confidence interval [CI], –3.00 to –0.30). There was no significant difference in age between the laparoscopic group (LG) and OG (MD = –0.72, 95% CI –1.86 to 0.41) or between RG and LG (MD = –0.93, 95% CI –1.93 to 0.07) (Supplementary Figure 3, Supplementary Figure 4, Supplementary Table 1). There was no significant inconsistency between the direct and indirect comparisons for age (Supplementary Table 2). In the Bayesian NMA, patients in the RG were also significantly younger than those in the OG (MD, –1.67 years; 95% –3.11 to –0.26) (Supplementary Figure 5 and Supplementary Table 3). No significant differences in age were found between the RG and LG (MD = –0.93, 95% CrI –1.97 to 0.11) or the LG and OG (MD = –0.74, 95% CrI –1.95 to 0.43) (Supplementary Figure 6, Supplementary Figure 7).
The model showed no evidence of lack of fit (no significant residual deviance) (Supplementary Figure 8, Supplementary Figure 9, Supplementary Figure 10).
Meta-regression indicated that patients in the OG were older in earlier studies (Supplementary Figure 11), with the age difference between groups diminishing in more recent years (i.e. no age selection difference in the most recent studies) (Supplementary Figure 12)
Sex of Patients
Regarding the sex distribution of patients, there were 63 studies with a total of 18,030 patients in the network (Supplementary Figure 14). Of these, 55 were two-arm studies and eight were multi-arm studies. The network included 79 pairwise comparisons. The number of trials comparing OG vs RG, OG vs LG, and LG vs RG were 9, 30, and 36, respectively (Supplementary Figure 15).
In the frequentist NMA, both the RG (pooled Odds Ratio, OR [OR] = 0.73, 95% CI 0.64–0.82) and LG (OR = 0.76, 95% CI 0.69–0.84) had a significantly lower proportion of male patients than the OG (Supplementary Figure 16). There was no significant difference in sex distribution between the RG and LG (OR = 0.93; 95% CI: 0.85–1.03) (Supplementary Figure 17 and Supplementary Table 4). There was no evidence of inconsistency between the direct and indirect estimates for sex (Supplementary Table 5).
ASA Status
Forty studies (54 pairwise comparisons; 10,318 patients) reported the proportion of patients with ASA class I–II (Supplementary Figure 18, Supplementary Figure 19). There were no statistically significant differences between the RG, LG, and OG in the proportion of patients classified as ASA I–II (i.e., no approach had significantly healthier or sicker patients by ASA status) (Supplementary Figure 20, Supplementary Table 6). The SUCRA rankings for ASA I–II rates were very similar among the three groups, with no significant separation (indicating that no approach consistently ranked healthier or worse in terms of ASA status) (Supplementary Figure 21 Supplementary Figure 22). No inconsistencies were observed between the direct and indirect comparisons (Supplementary Figure 23).
Meta-regression with the year of study as a covariate showed no significant change in the relative ASA status over time (Supplementary Figure 24).
Previous Cardiovascular Diseases
Pre-existing cardiovascular comorbidity was reported in 12 studies (18 pairwise comparisons), totaling 3,307 patients (Supplementary Figure 25, Supplementary Figure 26). There were no significant differences between the surgical approaches in terms of the proportion of patients with a history of cardiovascular disease (Supplementary Figure 27, Supplementary Table 7). In other words, the baseline rates of cardiovascular comorbidities were comparable among the OG, LG, and RG populations (Supplementary Figure 28). This suggests that patient selection in terms of cardiovascular health was similar across the groups. No inconsistency was observed among the comparisons (Supplementary Table 8).
In the Bayesian NMA, the results were similar to those of the frequentist NMA (Supplementary Figure 29, Supplementary Table 9, Supplementary Figure 30 Supplementary Figure 31, Supplementary Figure 32). We observed no deviance between the studies (Supplementary Figure 33, Supplementary Figure 34, Supplementary Figure 35).
The meta-regression analysis revealed that the effect differences decreased over time (Supplementary Figure 36).
Operative Time
Operative time was reported in 61 studies (79 pairwise comparisons), including 16,230 patients (Supplementary Figure 37, Supplementary Figure 38). In the frequentist NMA, the robotic approach was associated with a significantly longer operation duration than open surgery (MD = +25.93 min, 95% CI 7.68–44.18) (Supplementary Figure 39, Supplementary Table 10). The laparoscopic approach had a slight mean increase in operative time compared to the open approach, but this was not statistically significant (MD = +7.63 min, 95% CI –7.59 to +22.85). There was no evidence of inconsistency among the studies (Supplementary Table 11). Based on the SUCRA rankings for the shortest operative time, open surgery was the best (rank 1), followed by laparoscopic (rank 2) and robotic (rank 3) surgeries (Supplementary Figure 40). In the Bayesian NMA, the results were similar: robotic distal pancreatectomy had an average of approximately 27.2 min longer operative time than open (95% CrI 4.3 to 50.3 min) (Supplementary Figure 41, Supplementary Table 12). Laparoscopic vs open surgery remained a small, non-significant difference in the Bayesian analysis. The approach rankings by operative time in the Bayesian framework matched the frequentist results (OG fastest, followed by LG and RG) (Supplementary Figure 42, Supplementary Figure 43). There was no inconsistency between the studies (Supplementary Figure 44 Supplementary Figure 45, Supplementary Figure 46, Supplementary Figure 47).
Meta-regression analysis revealed no significant change in relative operative times over the years of publication, nor any influence of the study sample size on operative time differences (Supplementary Figure 48 and 49). In summary, robotic distal pancreatectomy tends to have a longer operating time than open or laparoscopic surgery, while laparoscopic surgery is roughly similar to open surgery in duration.
Conversion to Open
Thirty-eight studies (10,586 patients) reported conversion to open surgery (conversion events occurred in the laparoscopic or robotic arms) (Supplementary Figure 50 Supplementary Figure 51). In the network analysis (comparing only RG vs. LG, since OG by definition has no conversion), the robotic approach had a significantly lower conversion-to-open rate than the laparoscopic approach.
The odds of conversion were 65.3% lower with robotic surgery compared with laparoscopy (OR = 0.347, 95% CI 0.248–0.441 for RG vs. LG) (Figure 2). Accordingly, the laparoscopic approach had approximately 2.8 times higher odds of conversion than the robotic approach (OR = 2.88 for LG vs. RG, 95%CI 2.27–4.03) (Supplementary Table 14). Based on SUCRA, the robotic approach ranked as the best (lowest conversion rate) and laparoscopic as the worst for this outcome (Figure 3).
There was no evidence of inconsistency in this two-treatment network (Figure 4, Figure 5, Figure 6).
Frequentist and Bayesian analyses confirmed a significantly lower conversion risk for RG versus LG (Supplementary Figure 52). Meta-regression did not show any significant effect of publication year or study size on conversion rates (i.e. the conversion advantage of robotic remained fairly consistent across study timelines and sizes) (Figure 7, Figure 8).
Intraoperative Blood Loss
A total of 51 studies (46 two-arm and five multi-arm) reported intraoperative blood loss, encompassing 12,257 patients in the network (Supplementary Figure 60). There were 61 pairwise comparisons evaluating blood loss among the three approaches (Supplementary Figure 61).
In the frequentist NMA, both RG and LG were associated with significantly lower blood loss than OG. The mean difference in blood loss was –279.45 mL (95% CI –318.23 to –240.61) for RG vs OG, and –248.99 mL (95% CI –283.41 to –214.57) for LG vs OG. There was no significant difference in blood loss between the RG and LG groups in the frequentist analysis (Supplementary Figure 62, Supplementary Table 15). No inconsistencies were detected in the network (Supplementary Table 16). According to the SUCRA rankings, the interventions were ordered from least to most blood loss as follows: RG (best), LG, and OG (worst) (Supplementary Figure 63). In the Bayesian NMA, both RG and LG showed significantly lower blood loss than OG, with MD of –303.98 mL (95% CrI –382.8 to –229.26) for RG and –272.89 mL (95% CrI –340.15 to –209.01) for LG versus open (Supplementary Figure 64, Supplementary Table 17). The ranking of approaches from best to worst by Bayesian analysis remained RG, then LG, then OG (Supplementary Figure 65, Supplementary Figure 66). There was no notable model deviance or lack of convergence in the Bayesian analysis (Supplementary Figure 68, Supplementary Figure 69, Supplementary Figure 70). Meta-regression (Supplementary Figure 71) suggested that the differences in blood loss between open and minimally invasive approaches have become smaller in more recent studies compared to older (>10 years) studies (Supplementary Figure 72, Supplementary Figure 73). Conversely, a meta-regression using the number of included patients as a covariate showed that studies with larger sample sizes tended to report an even greater mean blood loss reduction in RG and LG versus OG (Supplementary Figure 74), although this trend was not statistically significant.
Intraoperative Bleeding More than 500 ml
Three studies (1,427 patients) reported the number of patients experiencing intraoperative blood loss greater than 500 mL (Supplementary Figure 76). The laparoscopic group showed a significantly lower incidence of ≥500 mL of blood loss than the open surgery group (OR 0.32, 95% CI 0.23–0.46) (Supplementary Figure 77, Supplementary Table 18). For the robotic group, the rate of high-volume bleeding was also lower than open, with an OR of 0.11 (95% CI 0.01–1.07), although this did not reach statistical significance due to wide confidence intervals (likely reflecting fewer events in the robotic arms). There were no direct comparisons between RG and LG for this outcome in the available studies, but the point estimates suggested that both modalities reduced the risk of major bleeding relative to open surgery. No inconsistencies were detected in the analysis (Supplementary Table 19). These findings indicate that minimally invasive approaches tend to have a lower risk of excessive intraoperative bleeding, with laparoscopy showing a significant reduction and robotics showing a similar trend.
Number of Patients Receiving Transfusions
Thirty studies (38 pairwise comparisons) with 9,248 patients reported the number of patients who received blood transfusions intraoperatively or postoperatively (any transfusion event) (Supplementary Figure 78 and 79). Both minimally invasive approaches were associated with significantly lower transfusion rates than open surgery. The odds of requiring a blood transfusion were OR = 0.25 (95% CI 0.19–0.34) for RG vs. OG and OR = 0.30 (95% CI 0.24–0.37) for LG vs. OG, indicating that both robotic and laparoscopic distal pancreatectomies had substantially reduced transfusion requirements relative to open surgery (Supplementary Figure 80, Supplementary Table 20). There was no significant difference in the transfusion rate between the RG and LG. No inconsistency was detected in the network (Supplementary Table 21). SUCRA-based rankings placed the robotic approach as best (rank 1), laparoscopic as rank 2, and open as rank 3 (worst) in terms of the lowest transfusion rates (Supplementary Figure 81).
The Quantity of Blood Transfusion
Four studies (six pairwise comparisons; 363 patients) analyzed the mean number of blood units transfused per patient (Supplementary Figure 82 and 83).
Both minimally invasive approaches were associated with a lower volume of blood transfusion than open surgery. The mean difference in transfused units was –1.98 (95% CI –3.42 to –0.54) for RG vs. OG and –1.86 (95% CI –3.12 to –0.59) for LG vs. OG, indicating that, on average, patients in the robotic and laparoscopic groups received approximately two fewer units of blood than those in the open group (Supplementary Figure 84, Supplementary Table 22). There was no significant difference in the transfusion quantity between the RG and LG. No inconsistencies were observed across these studies (Supplementary Table 23).
Intensive Care Unit Length of Stay
Nine studies (1,272 patients) reported the postoperative ICU length of stay (Supplementary Figure 85 and 86). Both the RG and LG were associated with a significantly shorter ICU stay duration than the OG. The mean difference in ICU days was –4.01 (95% CI –5.97 to –2.05) for RG vs. OG and –2.27 (95% CI –3.71 to –0.83) for LG vs. OG (Supplementary Figure 87, Supplementary Table 24). Thus, on average, patients who underwent robotic distal pancreatectomy spent approximately four fewer days in the ICU than those who underwent open surgery, and laparoscopic patients spent approximately two fewer days than those who underwent open surgery. There was no significant difference in ICU stay between the RG and LG in the NMA. No inconsistencies were observed (Supplementary Table 25). According to the SUCRA, the ranking from shortest to longest ICU stay was RG best (rank 1), LG rank 2, and OG worst (rank 3) (Supplementary Figure 88). These results suggest a clear benefit of minimally invasive approaches in reducing the need for prolonged critical care, likely reflecting overall lower perioperative stress and fewer complications.
Reintervention Rate
Thirty-seven studies (11,568 patients) reported the reoperation rate after surgery. RG and LG were associated with a lower reintervention rate than the open approach (0.451, 95%CrI 0.225 to 0.836 and 0.560, 95%CrI 0.322 to 0.962, respectively) (Supplementary Table 26).
There was no significant difference in the reintervention rate between the RG and LG.
SUCRA rankings for reintervention risk indicated robotic surgery as the best (rank 1, lowest reintervention rate), laparoscopic surgery as rank 2, and open surgery as rank 3 (highest reintervention) (Supplementary Figure 92). There was no evidence of inconsistency in the network (node split analysis, P > 0.05; Supplementary Figure 93).
Hospital Length of Stay
A total of 63 studies (18,113 patients; 54 two-arm and 9 multi-arm studies) provided data on the length of postoperative hospital stay (Supplementary Figure 97 and 98). Both minimally invasive approaches showed significantly shorter hospital stays than open surgery (Supplementary Figure 101). Pooled estimates indicated that RG patients had a shorter length of in-hospital stay than OG, with a MD of -8.77 days (95% CrI–13.34 to-4.22), while LG had a MD of -6.93 days (95% CrI-10.67 to-3.23) (Supplementary Table 29).
No inconsistencies were observed in this network (Supplementary Figure 104). According to the SUCRA, robotic surgery ranked best (shortest stay), laparoscopic surgery second, and open surgery worst for this outcome (Supplementary Figure 102 and 103). A meta-regression did not show any statistically significant temporal trends; the advantage of minimally invasive surgery in shortening hospital stay persisted over the study years without obvious change. These results underscore the major benefit of laparoscopic and robotic distal pancreatectomy: a faster recovery and discharge from the hospital compared to the open approach, with the robotic approach possibly offering the greatest reduction in hospital stay.
Readmission Rate
Thirty-one studies (34 comparisons) investigated the hospital readmission rates after distal pancreatectomy (Supplementary Figure 110, Supplementary Figure 111). No statistically significant differences in the 30-day readmission rates were found among the three approaches (Supplementary Figure 112, Supplementary Table 30). No inconsistency was detected in this network (Supplementary Table 31). The cumulative rank probabilities did not clearly favor any approach; the SUCRA values were very close, indicating that the likelihood of being the best or worst in terms of readmissions was similar across the open, laparoscopic, and robotic groups (Supplementary Figure 113). Overall, the choice of surgical approach did not significantly influence the need for readmission shortly after surgery.
In-Hospital Mortality
Nine studies (1,009 patients) reported in-hospital (same-admission) mortality (Supplementary Figure 114 and 115). No significant differences were observed in in-hospital mortality among the open, laparoscopic, and robotic groups (Supplementary Figure 117 and 119).
30. -Day Mortality
Thirty-one studies, including 12,127 patients, examined 30-day postoperative mortality (Supplementary Figure 125 and 126).
The RG was associated with significantly lower 30-day mortality (OR 0.159, 95%CrI 0.0294–0.459) (Figure 8). The LG also presented a lower 30-morality, although the statistical significance was marginal (OR = 0.477, 95%CrI 0.164–0.954) (Figure 9, Table 4).
According to the SUCRA values, the RG ranked first, LG second, and OG third (Figure 10 and Figure 11). In the frequentist NMA, the LG did not maintain statistical significance (Supplementary Figure 127 Supplementary Figure 128, Supplementary Figure 129, Supplementary Table 32, Supplementary Figure 130).

Table 4.
Treatment effects for all studies: comparison of all treatment pairs. Outcomes 30-day mortality. Bayesian NMA.
Table 4.
Treatment effects for all studies: comparison of all treatment pairs. Outcomes 30-day mortality. Bayesian NMA.
| Laparoscopic | Open | Robotic | |
|---|---|---|---|
| Laparoscopic | Laparoscopic | 2.1 (1.05, 6.1) | 0.34 (0.1, 0.83) |
| Open | 0.48 (0.16, 0.95) | Open | 0.16 (0.03, 0.46) |
| Robotic | 2.97 (1.2, 9.78) | 6.29 (2.18, 34.05) | Robotic |
No inconsistencies were detected between the comparisons (Supplementary Figure 131, Supplementary Figure 132). No deviance was observed (Supplementary Figure 133, 134, and 135).
No publication bias was detected (Supplementary Figure 140).
90. -Day Major Complications
Three studies (1,427 patients) reported 90-day major complications (typically Clavien–Dindo grade III or higher) (Supplementary Figure 141 and 142). No significant differences were observed between the groups in the incidence of major complications within 90 days postoperatively (Supplementary Figure 145). The pooled estimates for RG vs. OG and LG vs. OG suggested no large effect (ORs close to 1 with wide CrIs due to limited data), and RG vs. LG was similarly non-significant (Supplementary Table 37).
Summary
In summary, our analysis on the ranks according to the SUCRA values clearly shows that robotic surgery demonstrates superior performance across most outcomes, achieving the best ranking (Rank 1) in 84.6% of the measured outcomes and scoring 92.3% of the maximum possible points (Figure 12, Figure 13, Figure 14, Figure 15, Figure 16). Laparoscopic surgery showed moderate performance, whereas open surgery ranked lowest in this comparison.
Discussions
This network meta-analysis provides an updated and comprehensive comparison of the perioperative outcomes of open, laparoscopic, and robotic distal pancreatectomy for resectable lesions of the left pancreas. Based on the SUCRA rankings, robotic surgery demonstrated superior performance across most evaluated outcomes, achieving the highest rank (Rank 1) in 84.6% of the assessed parameters and accounting for 92.3% of the maximum possible performance score. Specifically, the robotic approach was associated with better intraoperative outcomes, including reduced blood loss, fewer transfusions, and a lower volume of transfused blood products. These advantages translated into shorter ICU and hospital stays, fewer reinterventions, and lower rates of both 30-day mortality and 90-day major complications. Laparoscopic surgery generally showed intermediate performance, whereas open surgery consistently ranked lowest in this comparative analysis.
The mean age of patients in the RG was significantly lower than that of the OG, but not significantly different from the LG. However, these age differences have diminished in more recent publications compared to earlier ones. In a previous meta-analysis, patients undergoing RDP were significantly younger than those undergoing LDP [92]. The current findings suggest that with increased familiarity and broader implementation of the robotic platform in pancreatic surgery, the indications for RDP have expanded to include older patients with more comorbidities.
Operative time was significantly longer in the RG, consistent with previous studies from high-volume centers [93]. This increase may be attributed to the docking and instrument exchange times. Additionally, the lack of tactile sensation may contribute to more cautious and slower maneuvers, particularly during the early stages of the learning curve. Meta-regression analysis revealed no significant change in relative operative times over the years of publication, nor any influence of the study sample size on this parameter. This persistent difference may reflect a trend toward applying robotic surgery to more complex cases and malignancies, as well as its adoption in smaller centers [94]. Three studies in our analysis compared all three techniques head-to-head [27,54,61], consistently reporting the longest operative time in the RG and the shortest in the OG group. However, a previously published meta-analysis [95] found comparable operative times across the three techniques. Operative time is closely related to surgical experience and standardization of the technique [96], with optimized outcomes reported after 40 robotic procedures [97]. In the present analysis, we included results from expert centers alongside those that were still in the early stages of the learning curve. From this perspective, the open approach ranked highest in the SUCRA scores, likely reflecting the broader experience of surgeons with open surgery.
The conversion rate in the RG was significantly lower than that in the LG, and meta-regression showed that this advantage remained consistent across different study timelines and sizes. This is a noteworthy finding, especially considering that experience with LDP is generally greater than that with RDP. Since laparoscopy remains the most widely used minimally invasive approach for distal pancreatectomy [15], it is plausible that most publications on RDP originate from high-volume centers with significant expertise in robotic surgery.
The favorable intraoperative outcomes of MIDP were reflected in better postoperative outcomes in both the RG and LG than in the OG. These findings emphasize the general advantages of minimally invasive techniques over open surgery, with the robotic approach potentially offering the greatest reduction in hospital stay. Additionally, in-hospital and 30-day mortality rates were significantly lower for the RG than for the OG and marginally better for the LG than for the OG. However, the surgical approach had no significant influence on the readmission rate or 90-day major complications, suggesting that these long-term outcomes may be more closely related to disease-specific or organ-specific complications than to the surgical technique used.
Although this network meta-analysis offers important comparative insights into open, laparoscopic, and robotic distal pancreatectomy, several limitations must be acknowledged. Most of the included studies were retrospective, which may have introduced various forms of bias. Nevertheless, the inclusion of prospective studies and one randomized trial adds strength to the overall evidence. Some heterogeneity existed among the studies in terms of patient selection, surgical expertise, and perioperative protocols, which reflect real-world clinical practice. Although many comparisons were indirect, the absence of statistical inconsistency in the network and the application of established statistical methods strengthened the credibility of the results.
Conclusions
This network meta-analysis highlights the perioperative advantages of minimally invasive distal pancreatectomy over the open approach, with RDP being safe and providing significant postoperative advantages over the other two approaches, including 30-day mortality and lower conversion rate. However, caution is warranted when interpreting these findings, as most robotic data are derived from high-volume expert centers.
Conflicts of Interest statements
NAH - nothing to declare, ES - nothing to declare, IN – nothing to declare.
Author Contributions (CRediT)
Nasser Abdul Halim: conceptualization, investigation, resources, data curation, writing – original draft. Eran Sadot: conceptualization, investigation, writing – review & editing, supervision. Ionut Negoi: conceptualization, methodology, formal analysis, investigation, writing – original draft, writing – review & editing, visualization, supervision, project administration.
References
- Leiphrakpam, P.D.; Chowdhury, S.; Zhang, M.; Bajaj, V.; Dhir, M.; Are, C. Trends in the Global Incidence of Pancreatic Cancer and a Brief Review of Its Histologic and Molecular Subtypes. J. Gastrointest. Cancer 2025, 56, 71. [Google Scholar] [CrossRef]
- Ryan, D.P.; Hong, T.S.; Bardeesy, N. Pancreatic Adenocarcinoma. N. Engl. J. Med. 2014, 371, 1039–1049. [Google Scholar] [CrossRef]
- Zhu, S.; Wang, W.-T.; Shang, X.-S.; Ni, T.; Wu, W.-C.; Lou, W.-H.; Zeng, M.-S.; Rao, S.-X. Difference Analysis in Prevalence of Incidental Pancreatic Cystic Lesions between Computed Tomography and Magnetic Resonance Imaging. BMC Med. Imaging 2019, 19, 43. [Google Scholar] [CrossRef]
- Santo, E.; Bar-Yishay, I. Pancreatic Solid Incidentalomas. Endosc. Ultrasound 2017, 6, S99–S103. [Google Scholar] [CrossRef]
- Cuschieri, A. Laparoscopic Surgery of the Pancreas. J. R. Coll. Surg. Edinb. 1994, 39, 178–184. [Google Scholar]
- Giulianotti, P.C.; Coratti, A.; Angelini, M.; Sbrana, F.; Cecconi, S.; Balestracci, T.; Caravaglios, G. Robotics in General Surgery, Personal Experience in a Large Community Hospital. Arch. Surg. 2003, 138, 777–784. [Google Scholar] [CrossRef]
- de Rooij, T.; van Hilst, J.; van Santvoort, H.; Boerma, D.; van den Boezem, P.; Daams, F.; van Dam, R.; Dejong, C.; van Duyn, E.; Dijkgraaf, M.; et al. Minimally Invasive versus Open Distal Pancreatectomy (LEOPARD): A Multicenter Patient-Blinded Randomized Controlled Trial: A Multicenter Patient-Blinded Randomized Controlled Trial. Ann. Surg. 2019, 269, 2–9. [Google Scholar] [CrossRef]
- Björnsson, B.; Larsson, A.L.; Hjalmarsson, C.; Gasslander, T.; Sandström, P. Comparison of the Duration of Hospital Stay after Laparoscopic or Open Distal Pancreatectomy: Randomized Controlled Trial: Duration of Hospital Stay after Distal Pancreatectomy. Br. J. Surg. 2020, 107, 1281–1288. [Google Scholar] [CrossRef]
- Song, K.B.; Kim, S.C.; Park, J.B.; Kim, Y.H.; Jung, Y.S.; Kim, M.-H.; Lee, S.-K.; Seo, D.-W.; Lee, S.S.; Park, D.H.; et al. Single-Center Experience of Laparoscopic Left Pancreatic Resection in 359 Consecutive Patients: Changing the Surgical Paradigm of Left Pancreatic Resection. Surg. Endosc. 2011, 25, 3364–3372. [Google Scholar] [CrossRef]
- Sánchez-Cabús, S.; Adam, J.-P.; Pittau, G.; Gelli, M.; Cunha, A.S. Laparoscopic Left Pancreatectomy: Early Results after 115 Consecutive Patients. Surg. Endosc. 2016, 30, 4480–4488. [Google Scholar] [CrossRef]
- van Hilst, J.; de Rooij, T.; Klompmaker, S.; Rawashdeh, M.; Aleotti, F.; Al-Sarireh, B.; Alseidi, A.; Ateeb, Z.; Balzano, G.; Berrevoet, F.; et al. Minimally Invasive versus Open Distal Pancreatectomy for Ductal Adenocarcinoma (DIPLOMA): A Pan-European Propensity Score Matched Study. Ann. Surg. 2019, 269, 10–17. [Google Scholar] [CrossRef]
- Korrel, M.; Jones, L.R.; van Hilst, J.; Balzano, G.; Björnsson, B.; Boggi, U.; Bratlie, S.O.; Busch, O.R.; Butturini, G.; Capretti, G.; et al. Minimally Invasive versus Open Distal Pancreatectomy for Resectable Pancreatic Cancer (DIPLOMA): An International Randomised Non-Inferiority Trial. The Lancet Regional Health - Europe 2023, 31, 100673. [Google Scholar] [CrossRef]
- Asbun, H.J.; Moekotte, A.L.; Vissers, F.L.; Kunzler, F.; Cipriani, F.; Alseidi, A.; D’Angelica, M.I.; Balduzzi, A.; Bassi, C.; Björnsson, B.; et al. The Miami International Evidence-Based Guidelines on Minimally Invasive Pancreas Resection. Ann. Surg. 2020, 271, 1–14. [Google Scholar] [CrossRef]
- Abu Hilal, M.; van Ramshorst, T.M.E.; Boggi, U.; Dokmak, S.; Edwin, B.; Keck, T.; Khatkov, I.; Ahmad, J.; Al Saati, H.; Alseidi, A.; et al. The Brescia Internationally Validated European Guidelines on Minimally Invasive Pancreatic Surgery (EGUMIPS). Ann. Surg. 2023, 279, 45–57. [Google Scholar] [CrossRef]
- van der Heijde, N.; Vissers, F.L.; Manzoni, A.; Zimmitti, G.; Balsells, J.; Berrevoet, F.; Bjornsson, B.; van den Boezem, P.; Boggi, U.; Bratlie, S.O.; et al. Use and Outcome of Minimally Invasive Pancreatic Surgery in the European E-MIPS Registry. International Hepato-Pancreato-Biliary Association 2023, 25, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Nevill, C.R.; Cooper, N.J.; Sutton, A.J. A Multifaceted Graphical Display, Including Treatment Ranking, Was Developed to Aid Interpretation of Network Meta-Analysis. J. Clin. Epidemiol. 2023, 157, 83–91. [Google Scholar] [CrossRef]
- van Valkenhoef, G.; Dias, S.; Ades, A.E.; Welton, N.J. Automated Generation of Node-Splitting Models for Assessment of Inconsistency in Network Meta-Analysis. Res. Synth. Methods 2016, 7, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Dias, S.; Ades, A.E.; Welton, N.J.; Jansen, J.P.; Sutton, A.J. Network Meta-Analysis for Decision-Making; John Wiley & Sons, 2018; ISBN 9781118647509.
- Donegan, S.; Dias, S.; Tudur-Smith, C.; Marinho, V.; Welton, N.J. Graphs of Study Contributions and Covariate Distributions for Network Meta-Regression. Res. Synth. Methods 2018, 9, 243–260. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Nikolakopoulou, A.; Papakonstantinou, T.; Salanti, G.; Efthimiou, O.; Schwarzer, G. Netmeta: An R Package for Network Meta-Analysis Using Frequentist Methods. J. Stat. Softw. 2023, 106. [Google Scholar] [CrossRef]
- Warn, D.E.; Thompson, S.G.; Spiegelhalter, D.J. Bayesian Random Effects Meta-Analysis of Trials with Binary Outcomes: Methods for the Absolute Risk Difference and Relative Risk Scales. Stat. Med. 2002, 21, 1601–1623. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.; Schmid, C. Bnma: Bayesian Network Meta-Analysis Using “JAGS.” CRAN: Contributed Packages 2019.
- Owen, R.K.; Bradbury, N.; Xin, Y.; Cooper, N.; Sutton, A. MetaInsight: An Interactive Web-Based Tool for Analyzing, Interrogating, and Visualizing Network Meta-Analyses Using R-Shiny and Netmeta. Res. Synth. Methods 2019, 10, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Nikolakopoulou, A.; Higgins, J.P.T.; Papakonstantinou, T.; Chaimani, A.; Del Giovane, C.; Egger, M.; Salanti, G. CINeMA: An Approach for Assessing Confidence in the Results of a Network Meta-Analysis. PLoS Med. 2020, 17, e1003082. [Google Scholar] [CrossRef]
- Session Details Available online:. Available online: https://events.cochrane.org/colloquium-2023/session/1473545/nmastudio-a-fully-interactive-web-application-for-producing-and-visualizing-network-meta-analyses (accessed on 28 June 2025).
- Rodriguez, M.; Memeo, R.; Leon, P.; Panaro, F.; Tzedakis, S.; Perotto, O.; Varatharajah, S.; de’Angelis, N.; Riva, P.; Mutter, D.; et al. Which Method of Distal Pancreatectomy Is Cost-Effective among Open, Laparoscopic, or Robotic Surgery? Hepatobiliary Surg. Nutr. 2018, 7, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Abu Hilal, M.; Hamdan, M.; Di Fabio, F.; Pearce, N.W.; Johnson, C.D. Laparoscopic versus Open Distal Pancreatectomy: A Clinical and Cost-Effectiveness Study. Surg. Endosc. 2012, 26, 1670–1674. [Google Scholar] [CrossRef]
- Alfieri, S.; Butturini, G.; Boggi, U.; Pietrabissa, A.; Morelli, L.; Vistoli, F.; Damoli, I.; Peri, A.; Fiorillo, C.; Pugliese, L.; et al. Short-Term and Long-Term Outcomes after Robot-Assisted versus Laparoscopic Distal Pancreatectomy for Pancreatic Neuroendocrine Tumors (PNETs): A Multicenter Comparative Study. Langenbecks Arch. Surg. 2019, 404, 459–468. [Google Scholar] [CrossRef]
- Aly, M.Y.F.; Tsutsumi, K.; Nakamura, M.; Sato, N.; Takahata, S.; Ueda, J.; Shimizu, S.; Redwan, A.A.; Tanaka, M. Comparative Study of Laparoscopic and Open Distal Pancreatectomy. J. Laparoendosc. Adv. Surg. Tech. A 2010, 20, 435–440. [Google Scholar] [CrossRef]
- Baker, M.S.; MBA; Bentrem, D. J.; Ujiki, M.B.; Ba, S.S.; LPN; Talamonti, M.S. A Prospective Single Institution Comparison of Peri-Operative Outcomes for Laparoscopic and Open Distal Pancreatectomy. Surgery 2009, 146, 635–645. [Google Scholar] [CrossRef]
- Benizri, E.I.; Germain, A.; Ayav, A.; Bernard, J.-L.; Zarnegar, R.; Benchimol, D.; Bresler, L.; Brunaud, L. Short-Term Perioperative Outcomes after Robot-Assisted and Laparoscopic Distal Pancreatectomy. J. Robot. Surg. 2014, 8, 125–132. [Google Scholar] [CrossRef]
- van Bodegraven, E.A.; van Ramshorst, T.M.E.; Bratlie, S.O.; Kokkola, A.; Sparrelid, E.; Björnsson, B.; Kleive, D.; Burgdorf, S.K.; Dokmak, S.; Koerkamp, B.G.; et al. Minimally Invasive Robot-Assisted and Laparoscopic Distal Pancreatectomy in a Pan-European Registry a Retrospective Cohort Study. [CrossRef]
- Butturini, G.; Partelli, S.; Crippa, S.; Malleo, G.; Rossini, R.; Casetti, L.; Melotti, G.L.; Piccoli, M.; Pederzoli, P.; Bassi, C. Perioperative and Long-Term Results after Left Pancreatectomy: A Single-Institution, Non-Randomized, Comparative Study between Open and Laparoscopic Approach. Surg. Endosc. 2011, 25, 2871–2878. [Google Scholar] [CrossRef]
- Butturini, G.; Damoli, I.; Crepaz, L.; Malleo, G.; Marchegiani, G.; Daskalaki, D.; Esposito, A.; Cingarlini, S.; Salvia, R.; Bassi, C. A Prospective Non-Randomised Single-Center Study Comparing Laparoscopic and Robotic Distal Pancreatectomy. Surg. Endosc. 2015, 29, 3163–3170. [Google Scholar] [CrossRef] [PubMed]
- Casadei, R.; Ricci, C.; D’Ambra, M.; Marrano, N.; Alagna, V.; Rega, D.; Monari, F.; Minni, F. Laparoscopic versus Open Distal Pancreatectomy in Pancreatic Tumours: A Case-Control Study. Updates Surg. 2010, 62, 171–174. [Google Scholar] [CrossRef]
- Chang, J.H.; Wehrle, C.; Woo, K.; Naples, R.; Stackhouse, K.A.; Dahdaleh, F.; Joyce, D.; Simon, R.; Augustin, T.; Walsh, R.M.; et al. Comparing Oncologic and Surgical Outcomes of Robotic and Laparoscopic Distal Pancreatectomy: A Propensity-Matched Analysis. Surg. Endosc. 2024, 38, 5678–5685. [Google Scholar] [CrossRef]
- Chen, P.; Zhou, B.; Wang, T.; Hu, X.; Ye, Y.; Guo, W. Comparative Efficacy of Robot-Assisted and Laparoscopic Distal Pancreatectomy: A Single-Center Comparative Study. J. Healthc. Eng. 2022, 2022, 7302222. [Google Scholar] [CrossRef]
- Chen, J.W.; van Ramshorst, T.M.E.; Lof, S.; Al-Sarireh, B.; Bjornsson, B.; Boggi, U.; Burdio, F.; Butturini, G.; Casadei, R.; Coratti, A.; et al. Robot-Assisted versus Laparoscopic Distal Pancreatectomy in Patients with Resectable Pancreatic Cancer: An International, Retrospective, Cohort Study. Ann. Surg. Oncol. 2023, 30, 3023–3032. [Google Scholar] [CrossRef]
- Daouadi, M.; Zureikat, A.H.; Zenati, M.S.; Choudry, H.; Tsung, A.; Bartlett, D.L.; Hughes, S.J.; Lee, K.K.; Moser, A.J.; Zeh, H.J. Robot-Assisted Minimally Invasive Distal Pancreatectomy Is Superior to the Laparoscopic Technique. Ann. Surg. 2013, 257, 128–132. [Google Scholar] [CrossRef]
- De Pastena, M.; Esposito, A.; Paiella, S.; Surci, N.; Montagnini, G.; Marchegiani, G.; Malleo, G.; Secchettin, E.; Casetti, L.; Ricci, C.; et al. Cost-Effectiveness and Quality of Life Analysis of Laparoscopic and Robotic Distal Pancreatectomy: A Propensity Score-Matched Study. Surg. Endosc. 2021, 35, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- De Pastena, M.; Esposito, A.; Paiella, S.; Montagnini, G.; Zingaretti, C.C.; Ramera, M.; Azzolina, D.; Gregori, D.; Kauffmann, E.F.; Giardino, A.; et al. Nationwide Cost-Effectiveness and Quality of Life Analysis of Minimally Invasive Distal Pancreatectomy. Surg. Endosc. 2024, 38, 5881–5890. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Kawka, M.; Gall, T.M.H.; Wadsworth, C.; Habib, N.; Nicol, D.; Cunningham, D.; Jiao, L.R. Robotic Distal Pancreatectomy Yields Superior Outcomes Compared to Laparoscopic Technique: A Single Surgeon Experience of 123 Consecutive Cases. Cancers (Basel) 2023, 15, 5492. [Google Scholar] [CrossRef]
- DiNorcia, J.; Schrope, B.A.; Lee, M.K.; Reavey, P.L.; Rosen, S.J.; Lee, J.A.; Chabot, J.A.; Allendorf, J.D. Laparoscopic Distal Pancreatectomy Offers Shorter Hospital Stays with Fewer Complications. J. Gastrointest. Surg. 2010, 14, 1804–1812. [Google Scholar] [CrossRef]
- Duran, H.; Ielpo, B.; Caruso, R.; Ferri, V.; Quijano, Y.; Diaz, E.; Fabra, I.; Oliva, C.; Olivares, S.; Vicente, E. Does Robotic Distal Pancreatectomy Surgery Offer Similar Results as Laparoscopic and Open Approach? A Comparative Study from a Single Medical Center: Robotic Distal Pancreatectomy. Int. J. Med. Robot. 2014, 10, 280–285. [Google Scholar] [CrossRef]
- Eom, B.W.; Jang, J.-Y.; Lee, S.E.; Han, H.-S.; Yoon, Y.-S.; Kim, S.-W. Clinical Outcomes Compared between Laparoscopic and Open Distal Pancreatectomy. Surg. Endosc. 2008, 22, 1334–1338. [Google Scholar] [CrossRef]
- Finan, K.R.; Cannon, E.E.; Kim, E.J.; Wesley, M.M.; Arnoletti, P.J.; Heslin, M.J.; Christein, J.D. Laparoscopic and Open Distal Pancreatectomy: A Comparison of Outcomes. Am. Surg. 2009, 75, 671–679. [Google Scholar] [CrossRef]
- Fox, A.M.; Pitzul, K.; Bhojani, F.; Kaplan, M.; Moulton, C.-A.; Wei, A.C.; McGilvray, I.; Cleary, S.; Okrainec, A. Comparison of Outcomes and Costs between Laparoscopic Distal Pancreatectomy and Open Resection at a Single Center. Surg. Endosc. 2012, 26, 1220–1230. [Google Scholar] [CrossRef] [PubMed]
- Goh, B.K.P.; Chan, C.Y.; Soh, H.-L.; Lee, S.Y.; Cheow, P.-C.; Chow, P.K.H.; Ooi, L.L.P.J.; Chung, A.Y.F. A Comparison between Robotic-Assisted Laparoscopic Distal Pancreatectomy versus Laparoscopic Distal Pancreatectomy: Robotic vs Laparoscopic Distal Pancreatectomy. Int. J. Med. Robot. 2017, 13, e1733. [Google Scholar] [CrossRef]
- Guerrero-Ortiz, M.A.; Sánchez-Velazquez, P.; Burdío, F.; Gimeno, M.; Podda, M.; Pellino, G.; Toledano, M.; Nuñez, J.; Bellido, J.; Acosta-Mérida, M.A.; et al. Cost-Effectiveness of Robotic vs Laparoscopic Distal Pancreatectomy. Results from the National Prospective Trial ROBOCOSTES. Surg. Endosc. 2024, 38, 6270–6281. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Song, K.B.; Madkhali, A.A.; Hwang, K.; Yoo, D.; Lee, J.W.; Youn, W.Y.; Alshammary, S.; Park, Y.; Lee, W.; et al. Robotic versus Laparoscopic Distal Pancreatectomy for Left-Sided Pancreatic Tumors: A Single Surgeon’s Experience of 228 Consecutive Cases. Surg. Endosc. 2020, 34, 2465–2473. [Google Scholar] [CrossRef] [PubMed]
- Jarufe, N.; Soto, P.; Ahumada, V.; Pacheco, S.; Salinas, J.; Galindo, J.; Bächler, J.-P.; Achurra, P.; Rebolledo, R.; Guerra, J.F.; et al. Laparoscopic versus Open Distal Pancreatectomy: Comparative Analysis of Clinical Outcomes at a Single Institution. Surg. Laparosc. Endosc. Percutan. Tech. 2018, 28, 62–66. [Google Scholar] [CrossRef]
- Jiang, Y.; Zheng, K.; Zhang, S.; Shao, Z.; Cheng, P.; Zhang, Y.; Jin, G.; He, T. Robot-Assisted Distal Pancreatectomy Improves Spleen Preservation Rate versus Laparoscopic Distal Pancreatectomy for Benign and Low-Grade Malignant Lesions of the Pancreas. Transl. Cancer Res. 2020, 9, 5166–5172. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Sutandi, N.; Sen, G.; Hammond, J.; Manas, D.M.; French, J.J.; White, S.A. Comparative Analysis of Open, Laparoscopic and Robotic Distal Pancreatic Resection: The United Kingdom’s First Single-Centre Experience. J. Minim. Access Surg. 2022, 18, 77–83. [Google Scholar] [CrossRef]
- Kang, C.M.; Kim, D.H.; Lee, W.J. Ten Years of Experience with Resection of Left-Sided Pancreatic Ductal Adenocarcinoma: Evolution and Initial Experience to a Laparoscopic Approach. Surg. Endosc. 2010, 24, 1533–1541. [Google Scholar] [CrossRef] [PubMed]
- Khaled, Y.S.; Malde, D.J.; Packer, J.; De Liguori Carino, N.; Deshpande, R.; O’Reilly, D.A.; Sherlock, D.J.; Ammori, B.J. A Case-Matched Comparative Study of Laparoscopic versus Open Distal Pancreatectomy. Surg. Laparosc. Endosc. Percutan. Tech. 2015, 25, 363–367. [Google Scholar] [CrossRef]
- Kim, S.C.; Park, K.T.; Hwang, J.W.; Shin, H.C.; Lee, S.S.; Seo, D.W.; Lee, S.K.; Kim, M.H.; Han, D.J. Comparative Analysis of Clinical Outcomes for Laparoscopic Distal Pancreatic Resection and Open Distal Pancreatic Resection at a Single Institution. Surg. Endosc. 2008, 22, 2261–2268. [Google Scholar] [CrossRef]
- Kooby, D.A.; Gillespie, T.; Bentrem, D.; Nakeeb, A.; Schmidt, M.C.; Merchant, N.B.; Parikh, A.A.; Martin, R.C.G., 2nd; Scoggins, C.R.; Ahmad, S.; et al. Left-Sided Pancreatectomy: A Multicenter Comparison of Laparoscopic and Open Approaches. Ann. Surg. 2008, 248, 438–446. [Google Scholar] [CrossRef]
- Lai, E.C.H.; Tang, C.N. Robotic Distal Pancreatectomy versus Conventional Laparoscopic Distal Pancreatectomy: A Comparative Study for Short-Term Outcomes. Front. Med. 2015, 9, 356–360. [Google Scholar] [CrossRef]
- Lai, H.-F.; Shyr, Y.-M.; Shyr, B.-S.; Chen, S.-C.; Wang, S.-E.; Shyr, B.-U. Minimally Invasive Distal Pancreatectomy: Laparoscopic versus Robotic Approach-A Cohort Study. Health Sci. Rep. 2022, 5, e712. [Google Scholar] [CrossRef]
- Ser Yee Lee MBBS MSc MMed FRCS(Ed); Allen MD FACS, P. ; Sadot, E.; D’Angelica MD FACS, M.; DeMatteo MD FACS, R.; Facs, Y.F.M.D.; Jarnagin MD FACS, W.; Facs, T.P.K. Distal Pancreatectomy: A Single Institution’s Experience in Open, Laparoscopic, and Robotic Approaches. Journal of the American College of Surgeons 2015, 220, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Q.; Kabir, T.; Koh, Y.-X.; Teo, J.-Y.; Lee, S.-Y.; Kam, J.-H.; Cheow, P.-C.; Jeyaraj, P.R.; Chow, P.K.H.; Ooi, L.L.; et al. A Single Institution Experience with Robotic and Laparoscopic Distal Pancreatectomies. Ann. Hepatobiliary. Pancreat. Surg. 2020, 24, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Ielpo, B.; Duran, H.; Diaz, E.; Fabra, I.; Caruso, R.; Malavé, L.; Ferri, V.; Nuñez, J.; Ruiz-Ocaña, A.; Jorge, E.; et al. Robotic versus Laparoscopic Distal Pancreatectomy: A Comparative Study of Clinical Outcomes and Costs Analysis. Int. J. Surg. 2017, 48, 300–304. [Google Scholar] [CrossRef]
- Limongelli, P.; Belli, A.; Russo, G.; Cioffi, L.; D’Agostino, A.; Fantini, C.; Belli, G. Laparoscopic and Open Surgical Treatment of Left-Sided Pancreatic Lesions: Clinical Outcomes and Cost-Effectiveness Analysis. Surg. Endosc. 2012, 26, 1830–1836. [Google Scholar] [CrossRef]
- Liu, R.; Liu, Q.; Zhao, Z.-M.; Tan, X.-L.; Gao, Y.-X.; Zhao, G.-D. Robotic versus Laparoscopic Distal Pancreatectomy: A Propensity Score-Matched Study. J. Surg. Oncol. 2017, 116, 461–469. [Google Scholar] [CrossRef]
- Lof, S.; van der Heijde, N.; Abuawwad, M.; Al-Sarireh, B.; Boggi, U.; Butturini, G.; Capretti, G.; Coratti, A.; Casadei, R.; D’Hondt, M.; et al. Robotic versus Laparoscopic Distal Pancreatectomy: Multicentre Analysis. [CrossRef]
- Lyman, W.B.; Passeri, M.; Sastry, A.; Cochran, A.; Iannitti, D.A.; Vrochides, D.; Baker, E.H.; Martinie, J.B. Robotic-Assisted versus Laparoscopic Left Pancreatectomy at a High-Volume, Minimally Invasive Center. Surg. Endosc. 2019, 33, 2991–3000. [Google Scholar] [CrossRef]
- Magge, D.R.; Zenati, M.S.; Hamad, A.; Rieser, C.; Zureikat, A.H.; Zeh, H.J.; Hogg, M.E. Comprehensive Comparative Analysis of Cost-Effectiveness and Perioperative Outcomes between Open, Laparoscopic, and Robotic Distal Pancreatectomy. HPB (Oxford) 2018, 20, 1172–1180. [Google Scholar] [CrossRef]
- Marino, M.V.; Mirabella, A.; Gomez Ruiz, M.; Komorowski, A.L. Robotic-Assisted versus Laparoscopic Distal Pancreatectomy: The Results of a Case-Matched Analysis from a Tertiary Care Center. Dig. Surg. 2020, 37, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.S.; Doumane, G.; Mura, T.; Nocca, D.; Fabre, J.-M. Laparoscopic versus Open Distal Pancreatectomy: A Single-Institution Case-Control Study. Surg. Endosc. 2012, 26, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Morelli, L.; Guadagni, S.; Palmeri, M.; Franco, G.; Caprili, G.; D’isidoro, C.; Bastiani, L.; Candio, G.; Pietrabissa, A.; Mosca, F. A Case-Control Comparison of Surgical and Functional Outcomes of Robotic-Assisted Spleen-Preserving Left Side Pancreatectomy versus Pure Laparoscopy. Journal of the Pancreas 2016, 17, 30–35. [Google Scholar]
- Najafi, N.; Mintziras, I.; Wiese, D.; Albers, M.B.; Maurer, E.; Bartsch, D.K. A Retrospective Comparison of Robotic versus Laparoscopic Distal Resection and Enucleation for Potentially Benign Pancreatic Neoplasms. Surg. Today 2020, 50, 872–880. [Google Scholar] [CrossRef]
- Nakamura, Y.; Uchida, E.; Aimoto, T.; Matsumoto, S.; Yoshida, H.; Tajiri, T. Clinical Outcome of Laparoscopic Distal Pancreatectomy. J. Hepatobiliary. Pancreat. Surg. 2009, 16, 35–41. [Google Scholar] [CrossRef]
- Nickel, F.; Distler, M.; Limen, E.F.; Wise, P.A.; Kowalewski, K.-F.; Tritarelli, P.M.; Perez, D.; Izbicki, J.R.; Kersebaum, J.-N.; Egberts, J.-H.; et al. Initial Learning Curves of Laparoscopic and Robotic Distal Pancreatectomy Compared with Open Distal Pancreatectomy: Multicentre Analysis. Br. J. Surg. 2023, 110, 1063–1067. [Google Scholar] [CrossRef]
- Qu, L.; Zhiming, Z.; Xianglong, T.; Yuanxing, G.; Yong, X.; Rong, L.; Yee, L.W. Short- and Mid-Term Outcomes of Robotic versus Laparoscopic Distal Pancreatosplenectomy for Pancreatic Ductal Adenocarcinoma: A Retrospective Propensity Score-Matched Study. Int. J. Surg. 2018, 55, 81–86. [Google Scholar] [CrossRef]
- Raoof, M.; Nota, C.L.M.A.; Melstrom, L.G.; Warner, S.G.; Woo, Y.; Singh, G.; Fong, Y. Oncologic Outcomes after Robot-Assisted versus Laparoscopic Distal Pancreatectomy: Analysis of the National Cancer Database: RAOOFet Al. J. Surg. Oncol. 2018, 118, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Kwon, J.; Lee, J.H.; Park, S.Y.; Park, Y.; Lee, W.; Song, K.B.; Hwang, D.W.; Kim, S.C. Robotic versus Laparoscopic Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma: A Propensity Score-Matched Analysis. Hepatobiliary Pancreat. Dis. Int 2023, 22, 154–159. [Google Scholar] [CrossRef]
- Souche, R.; Herrero, A.; Bourel, G.; Chauvat, J.; Pirlet, I.; Guillon, F.; Nocca, D.; Borie, F.; Mercier, G.; Fabre, J.-M. Robotic versus Laparoscopic Distal Pancreatectomy: A French Prospective Single-Center Experience and Cost-Effectiveness Analysis. Surg. Endosc. 2018, 32, 3562–3569. [Google Scholar] [CrossRef] [PubMed]
- Stauffer, J.A.; Rosales-Velderrain, A.; Goldberg, R.F.; Bowers, S.P.; Asbun, H.J. Comparison of Open with Laparoscopic Distal Pancreatectomy: A Single Institution’s Transition over a 7-Year Period. HPB (Oxford) 2013, 15, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Velanovich, V. Case-Control Comparison of Laparoscopic versus Open Distal Pancreatectomy. J. Gastrointest. Surg. 2006, 10, 95–98. [Google Scholar] [CrossRef]
- Vicente, E.; Núñez-Alfonsel, J.; Ielpo, B.; Ferri, V.; Caruso, R.; Duran, H.; Diaz, E.; Malave, L.; Fabra, I.; Pinna, E.; et al. A Cost-Effectiveness Analysis of Robotic versus Laparoscopic Distal Pancreatectomy. Int. J. Med. Robot. 2020, 16, e2080. [Google Scholar] [CrossRef]
- Vijan, S.S.; Ahmed, K.A.; Harmsen, W.S.; Que, F.G.; Reid-Lombardo, K.M.; Nagorney, D.M.; Donohue, J.H.; Farnell, M.B.; Kendrick, M.L. Laparoscopic vs Open Distal Pancreatectomy: A Single-Institution Comparative Study. Arch. Surg. 2010, 145, 616–621. [Google Scholar] [CrossRef]
- Waters, J.A.; Canal, D.F.; Wiebke, E.A.; Dumas, R.P.; Beane, J.D.; Aguilar-Saavedra, J.R.; Ball, C.G.; House, M.G.; Zyromski, N.J.; Nakeeb, A.; et al. Robotic Distal Pancreatectomy: Cost Effective? Surgery 2010, 148, 814–823. [Google Scholar] [CrossRef]
- Wellner, U.F.; Lapshyn, H.; Bartsch, D.K.; Mintziras, I.; Hopt, U.T.; Wittel, U.; Krämling, H.-J.; Preissinger-Heinzel, H.; Anthuber, M.; Geissler, B.; et al. Laparoscopic versus Open Distal Pancreatectomy-a Propensity Score-Matched Analysis from the German StuDoQ|Pancreas Registry. Int. J. Colorectal Dis. 2017, 32, 273–280. [Google Scholar] [CrossRef]
- Weng, Y.; Jin, J.; Huo, Z.; Shi, Y.; Jiang, Y.; Deng, X.; Peng, C.; Shen, B. Robotic-Assisted versus Open Distal Pancreatectomy for Benign and Low-Grade Malignant Pancreatic Tumors: A Propensity Score-Matched Study. Surg. Endosc. 2021, 35, 2255–2264. [Google Scholar] [CrossRef]
- Xourafas, D.; Ashley, S.W.; Clancy, T.E. Comparison of Perioperative Outcomes between Open, Laparoscopic, and Robotic Distal Pancreatectomy: An Analysis of 1815 Patients from the ACS-NSQIP Procedure-Targeted Pancreatectomy Database. J. Gastrointest. Surg. 2017, 21, 1442–1452. [Google Scholar] [CrossRef]
- Yan, J.-F.; Kuang, T.-T.; Ji, D.-Y.; Xu, X.-W.; Wang, D.-S.; Zhang, R.-C.; Jin, W.-W.; Mou, Y.-P.; Lou, W.-H. Laparoscopic versus Open Distal Pancreatectomy for Benign or Premalignant Pancreatic Neoplasms: A Two-Center Comparative Study. J. Zhejiang Univ. Sci. B 2015, 16, 573–579. [Google Scholar] [CrossRef]
- Zhang, J.; Jin, J.; Chen, S.; Gu, J.; Zhu, Y.; Qin, K.; Zhan, Q.; Cheng, D.; Chen, H.; Deng, X.; et al. Minimally Invasive Distal Pancreatectomy for PNETs: Laparoscopic or Robotic Approach? Oncotarget 2017, 8, 33872–33883. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, W.; Jiang, J.; Ye, Y.; Hu, W.; Zhai, Z.; Bai, X.; Liang, T. A Comparison of Robotic versus Laparoscopic Distal Pancreatectomy: A Single Surgeon’s Robotic Experience in a High-Volume Center. Surg. Endosc. 2022, 36, 9186–9193. [Google Scholar] [CrossRef]
- Cho, C.S.; Kooby, D.A.; Schmidt, C.M.; Nakeeb, A.; Bentrem, D.J.; Merchant, N.B.; Parikh, A.A.; Martin, R.C.G., 2nd; Scoggins, C.R.; Ahmad, S.A.; et al. Laparoscopic versus Open Left Pancreatectomy: Can Preoperative Factors Indicate the Safer Technique? Ann. Surg. 2011, 253, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Nassour, I.; Zureikat, A.; Paniccia, A. Perioperative and Oncologic Outcomes of Open, Laparoscopic, and Robotic Distal Pancreatectomy for Pancreatic Adenocarcinoma. Updates Surg. 2021, 73, 947–953. [Google Scholar] [CrossRef]
- van Ramshorst, T.M.E.; van Bodegraven, E.A.; Zampedri, P.; Kasai, M.; Besselink, M.G.; Abu Hilal, M. Robot-Assisted versus Laparoscopic Distal Pancreatectomy: A Systematic Review and Meta-Analysis Including Patient Subgroups. Surg. Endosc. 2023, 37, 4131–4143. [Google Scholar] [CrossRef] [PubMed]
- Boggi, U.; Donisi, G.; Napoli, N.; Partelli, S.; Esposito, A.; Ferrari, G.; Butturini, G.; Morelli, L.; Abu Hilal, M.; Viola, M.; et al. Prospective Minimally Invasive Pancreatic Resections from the IGOMIPS Registry: A Snapshot of Daily Practice in Italy on 1191 between 2019 and 2022. Updates Surg. 2023, 75, 1439–1456. [Google Scholar] [CrossRef]
- Wong, P.; Lewis, A.; Thornblade, L.W.; Maker, A.V.; Fong, Y.; Melstrom, L.G. Robotic Pancreatectomy for Pancreatic Adenocarcinoma: Evolving Trends in Patient Selection and Practice Patterns across a Decade. HPB (Oxford) 2025. [Google Scholar] [CrossRef]
- Gavriilidis, P.; Roberts, K.J.; Sutcliffe, R.P. Comparison of Robotic vs Laparoscopic vs Open Distal Pancreatectomy. A Systematic Review and Network Meta-Analysis. HPB (Oxford) 2019, 21, 1268–1276. [Google Scholar] [CrossRef]
- Zureikat, A.H.; Moser, A.J.; Boone, B.A.; Bartlett, D.L.; Zenati, M.; Zeh, H.J. 250 Robotic Pancreatic Resections. Ann. Surg. 2013, 258, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Shakir, M.; Boone, B.A.; Polanco, P.M.; Zenati, M.S.; Hogg, M.E.; Tsung, A.; Choudry, H.A.; Moser, A.J.; Bartlett, D.L.; Zeh, H.J.; et al. The Learning Curve for Robotic Distal Pancreatectomy: An Analysis of Outcomes of the First 100 Consecutive Cases at a High-Volume Pancreatic Centre. HPB (Oxford) 2015, 17, 580–586. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Bayesian random effect consistency model forest plot for outcome conversion rate.
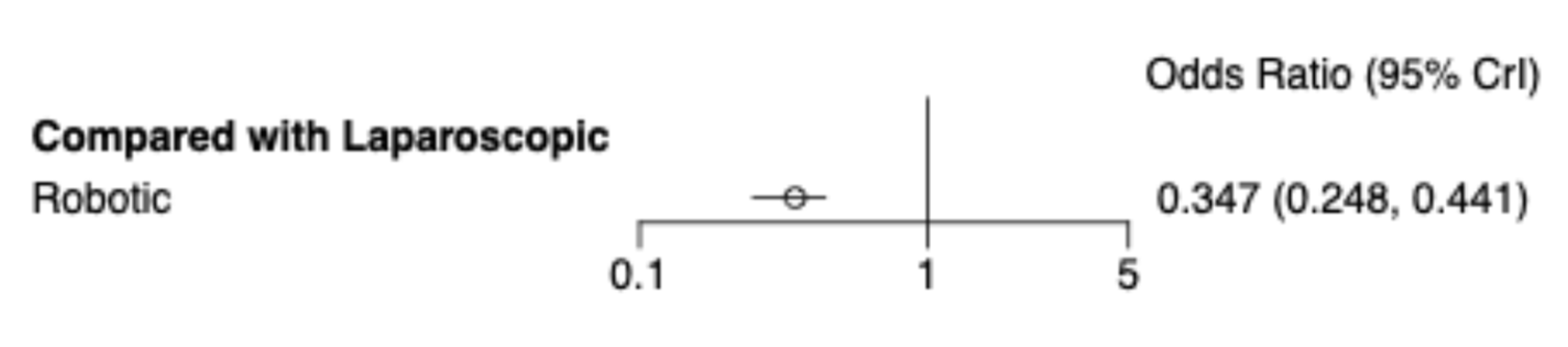
Figure 3.
Radial SUCRA plot: Outcomes conversions. Higher SUCRA values indicate better treatments; size of nodes represent number of participants and thickness of lines indicate number of trials conducted.
Figure 3.
Radial SUCRA plot: Outcomes conversions. Higher SUCRA values indicate better treatments; size of nodes represent number of participants and thickness of lines indicate number of trials conducted.
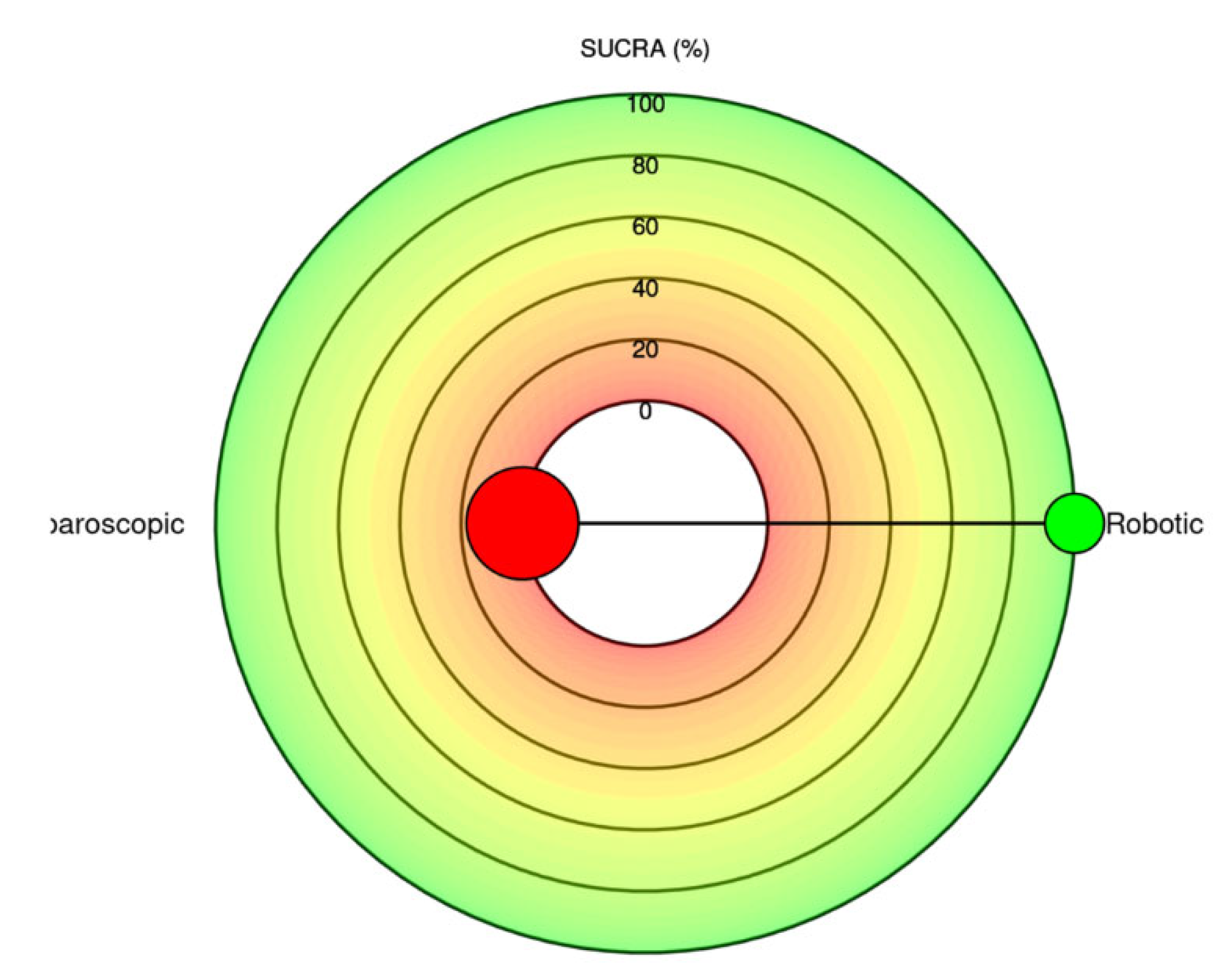
Figure 4.
Residual deviance from NMA model and UME inconsistency model for all studies.
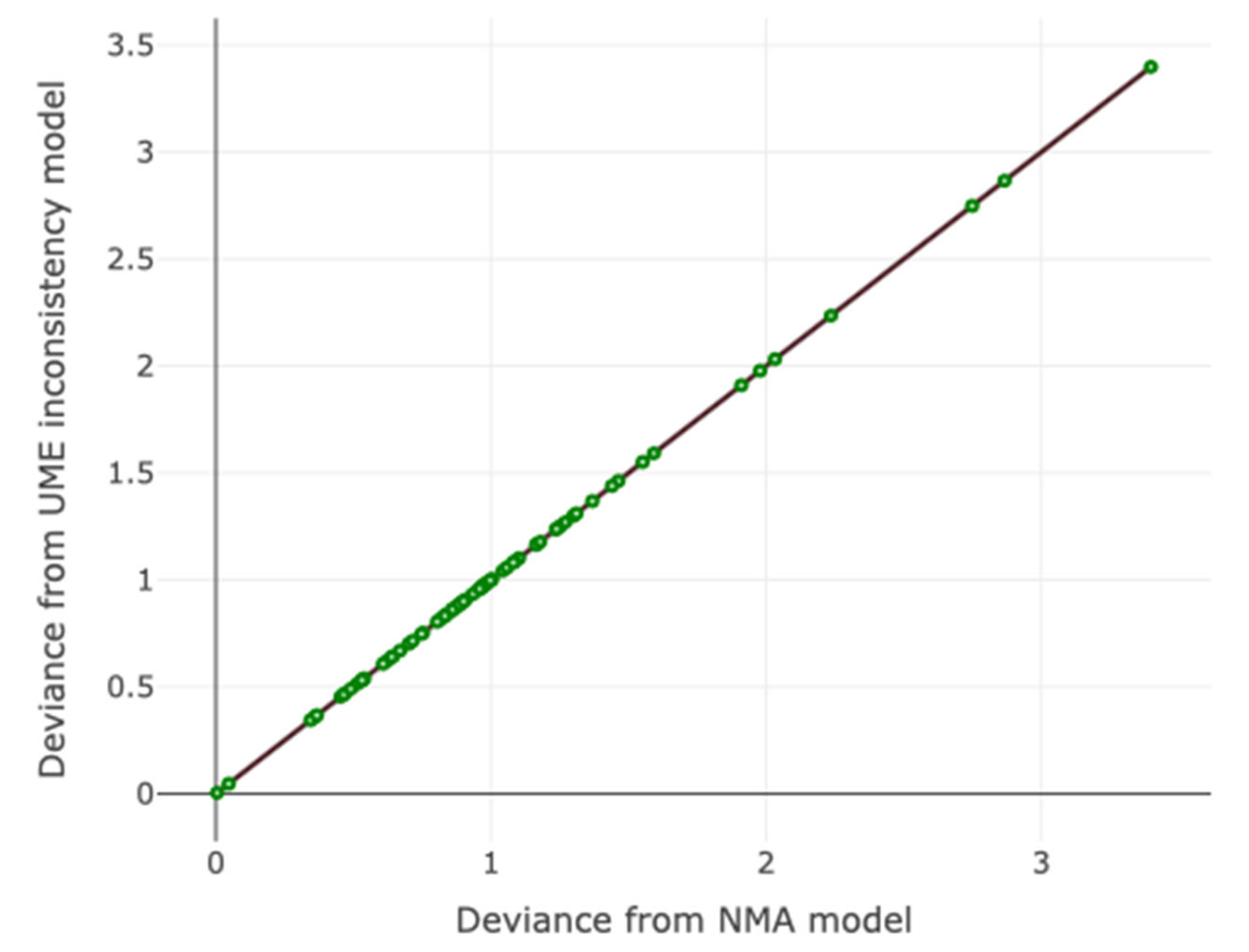
Figure 5.
Per-arm residual deviance for all studies. This stem plot represents the posterior residual deviance per study arm.
Figure 5.
Per-arm residual deviance for all studies. This stem plot represents the posterior residual deviance per study arm.
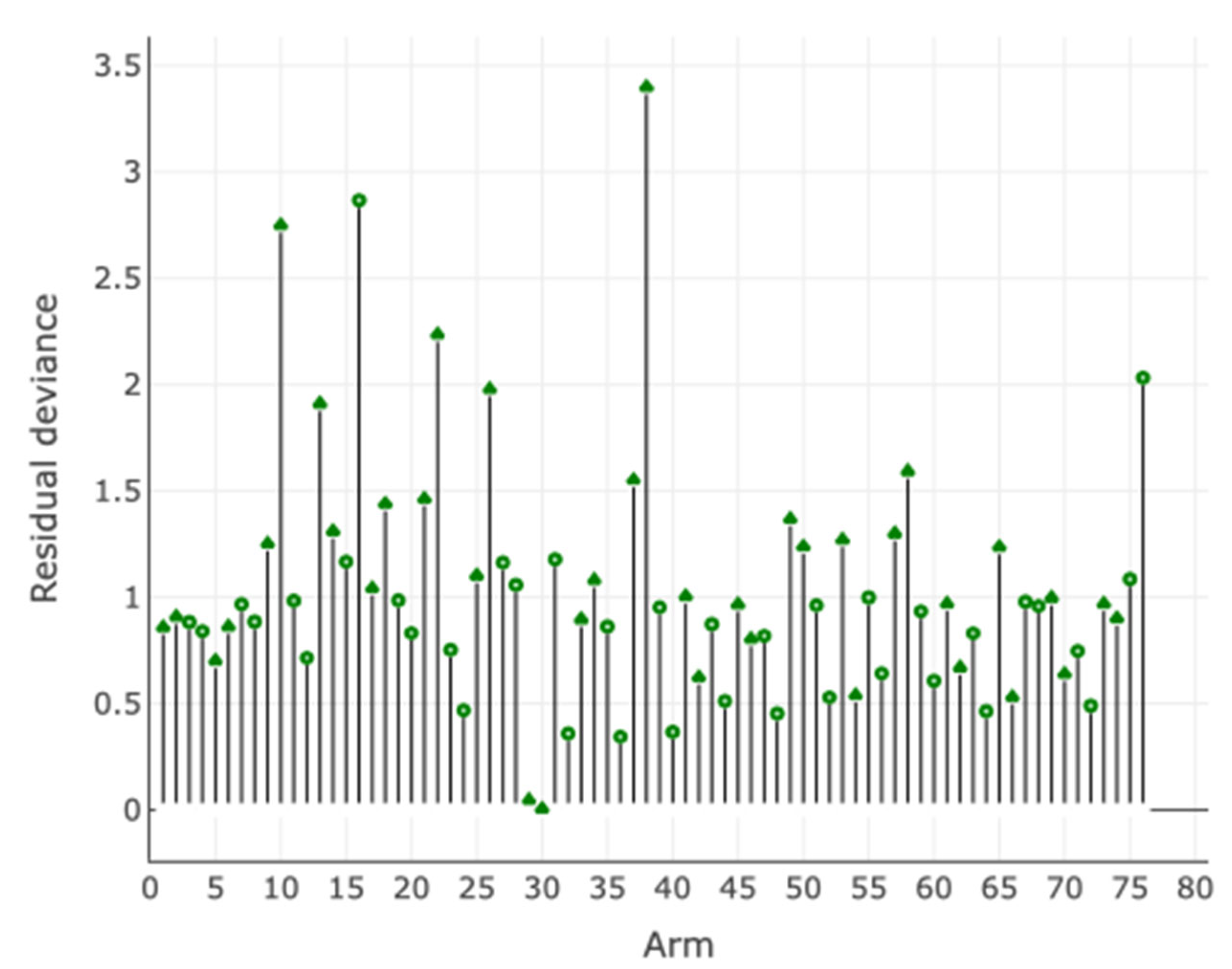
Figure 6.
Leverage plot for all studies.
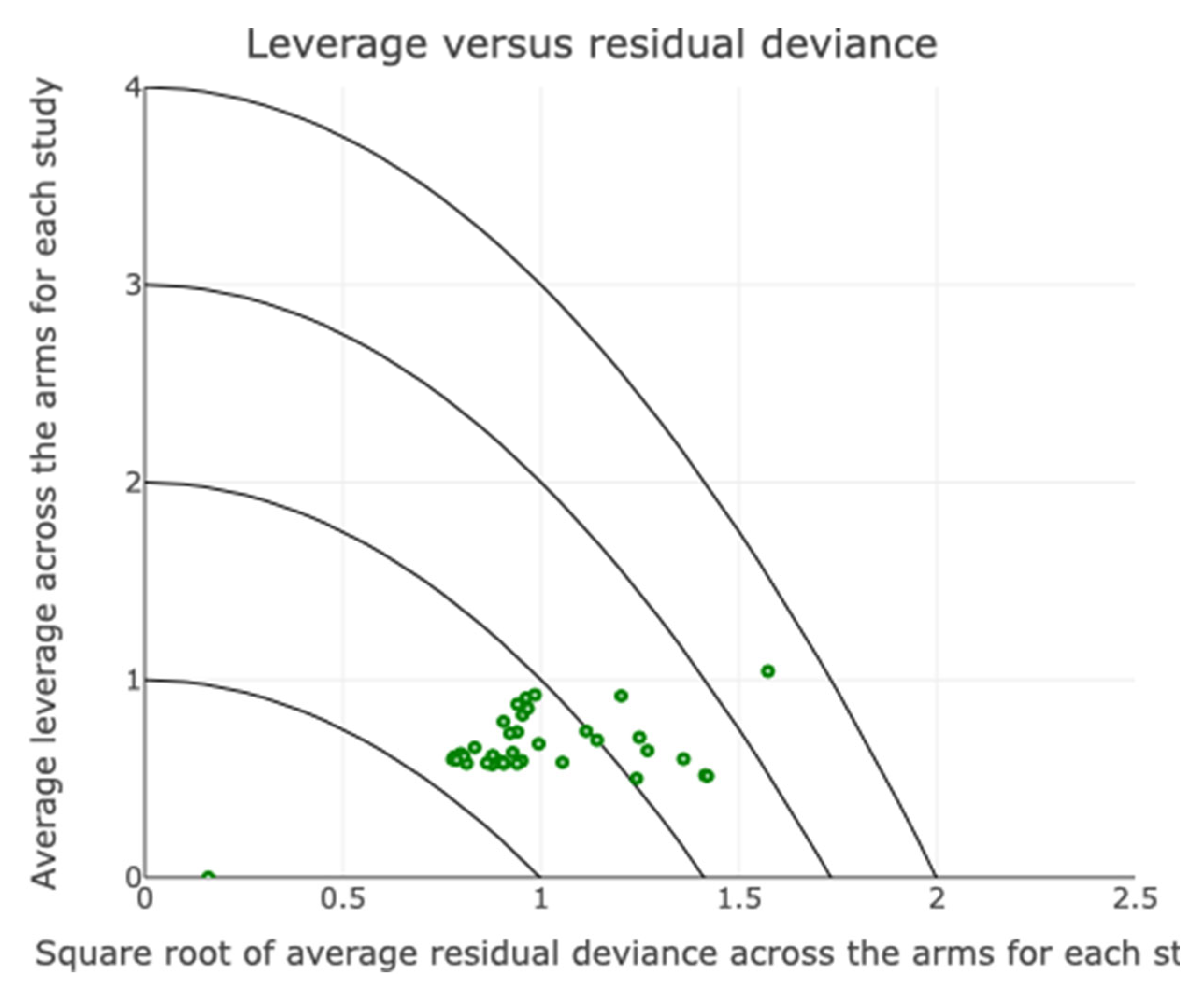
Figure 7.
Regression plot for the outcome conversions having as covariate the year of study publication.
Figure 7.
Regression plot for the outcome conversions having as covariate the year of study publication.
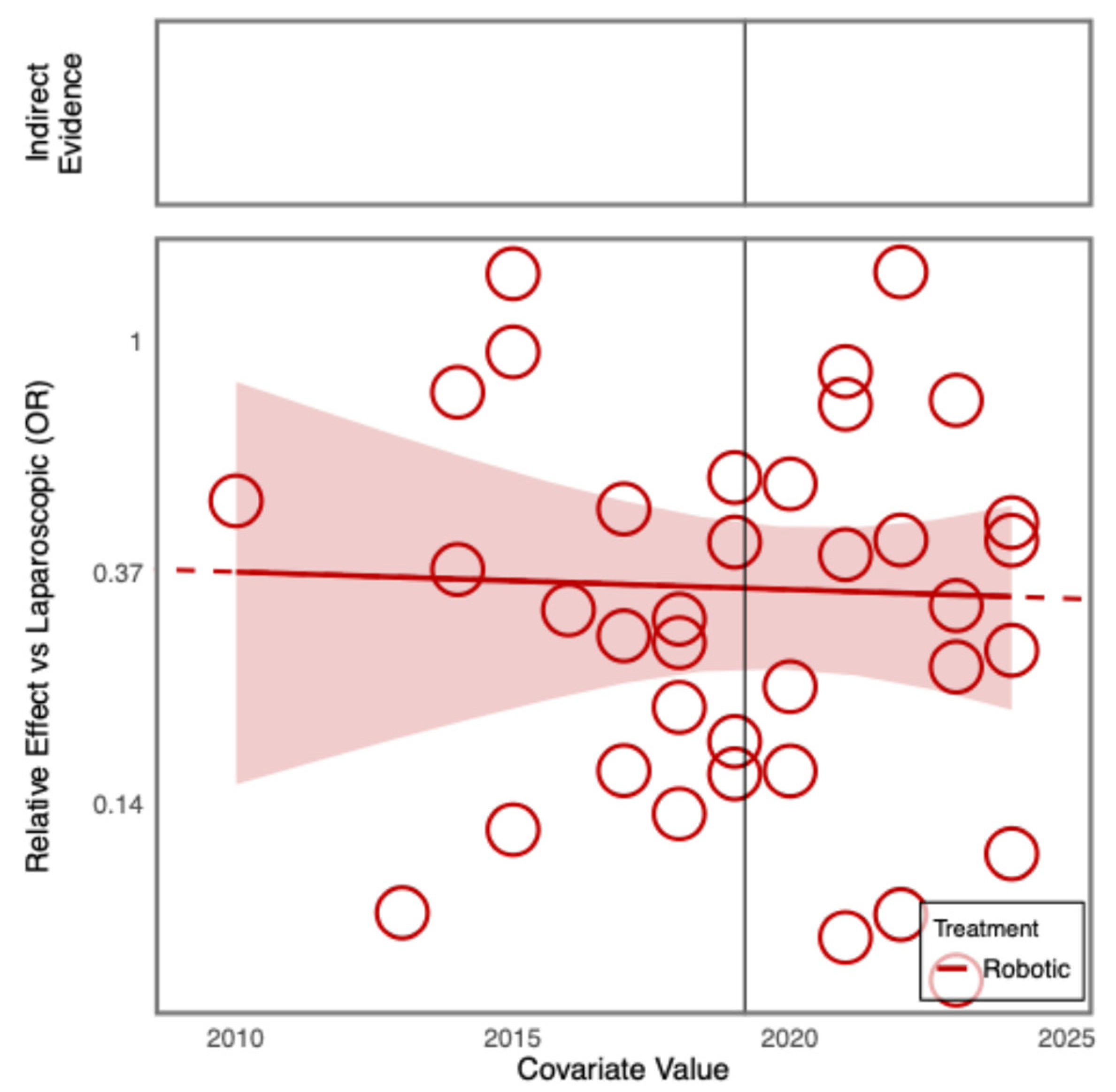
Figure 8.
Regression plot for the outcome conversions having as covariate the number of patients in the included studies.
Figure 8.
Regression plot for the outcome conversions having as covariate the number of patients in the included studies.
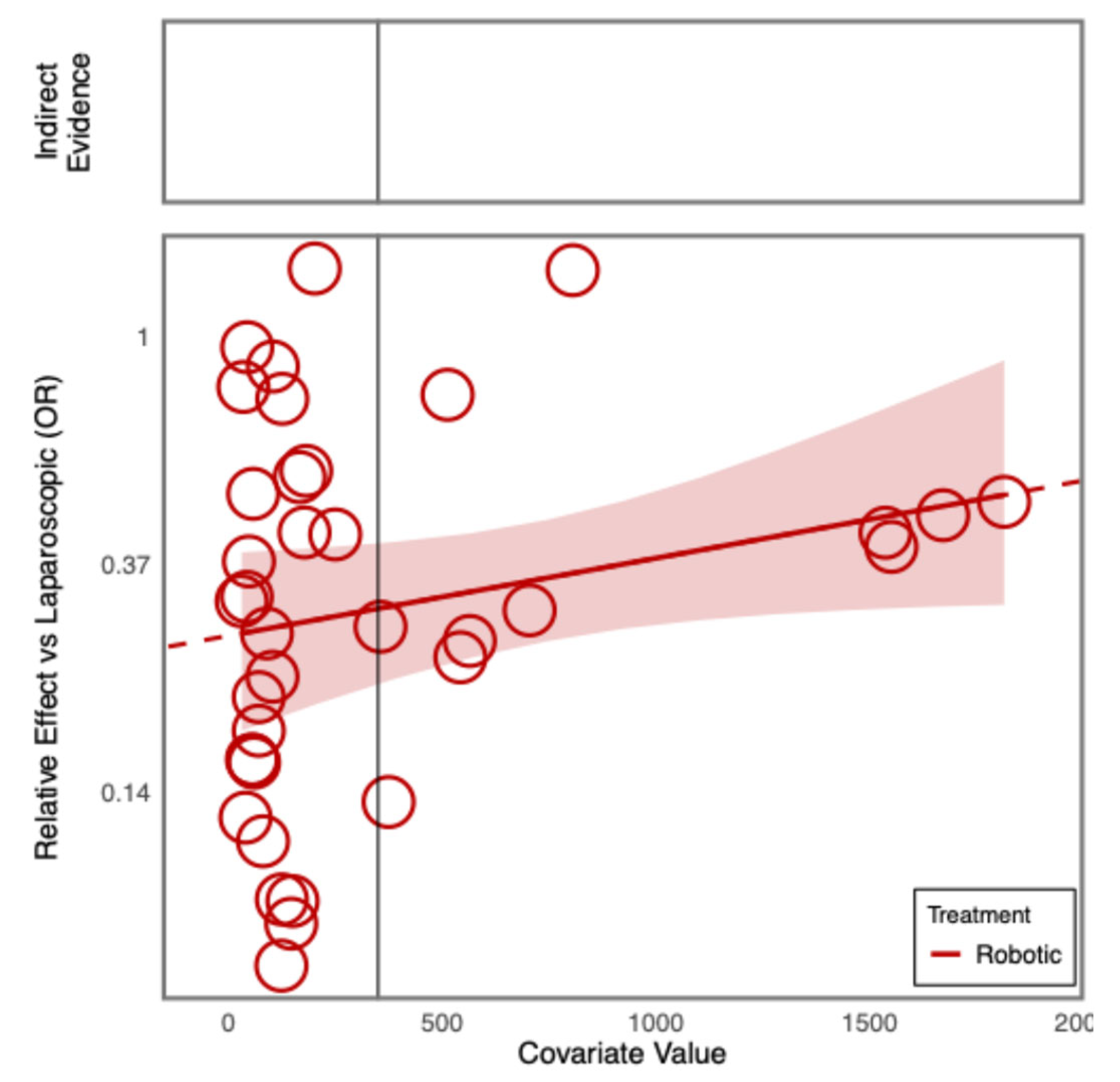
Figure 9.
Bayesian random effect consistency model forrest plot for outcome 30-day mortality. Between-study standard deviation (log-odds scale): 0.62 . 95% credible interval: 0.02 , 1.86 .
Figure 9.
Bayesian random effect consistency model forrest plot for outcome 30-day mortality. Between-study standard deviation (log-odds scale): 0.62 . 95% credible interval: 0.02 , 1.86 .
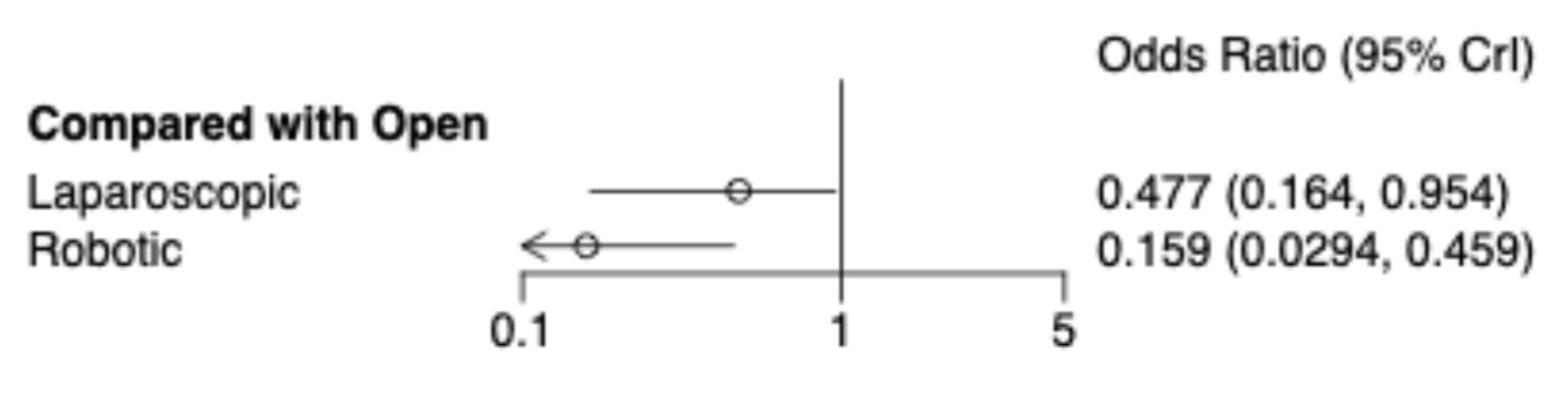
Figure 10.
Litmus Rank-O-Gram: Outcomes 30-day mortality. Higher SUCRA (Surface Under the Cumulative Ranking Curve) values and cumulative ranking curves nearer the top left indicate better performance.
Figure 10.
Litmus Rank-O-Gram: Outcomes 30-day mortality. Higher SUCRA (Surface Under the Cumulative Ranking Curve) values and cumulative ranking curves nearer the top left indicate better performance.
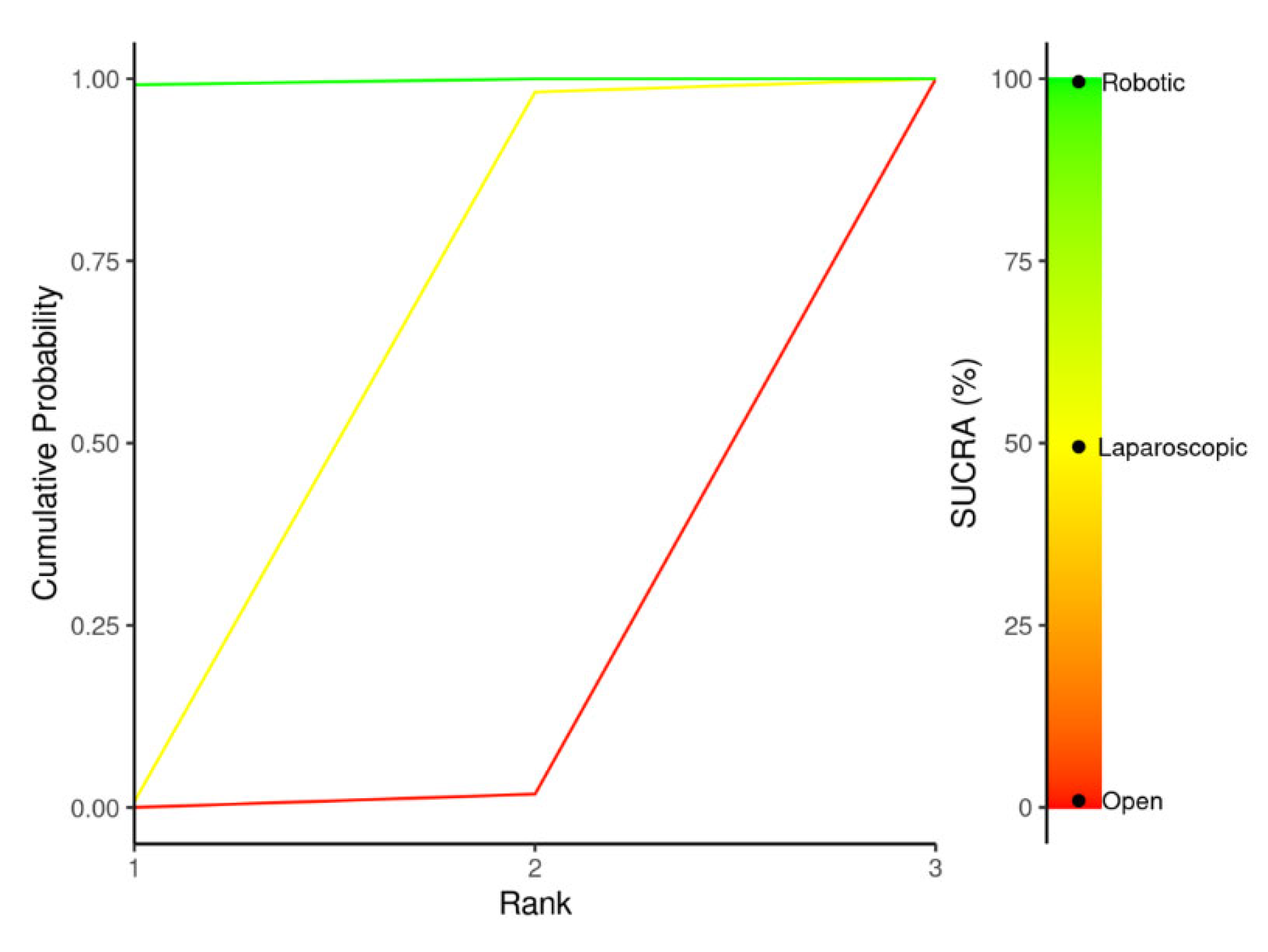
Figure 11.
Radial SUCRA plot: Outcomes 30-day mortality. Higher SUCRA values indicate better treatments; size of nodes represent number of participants and thickness of lines indicate number of trials conducted.
Figure 11.
Radial SUCRA plot: Outcomes 30-day mortality. Higher SUCRA values indicate better treatments; size of nodes represent number of participants and thickness of lines indicate number of trials conducted.
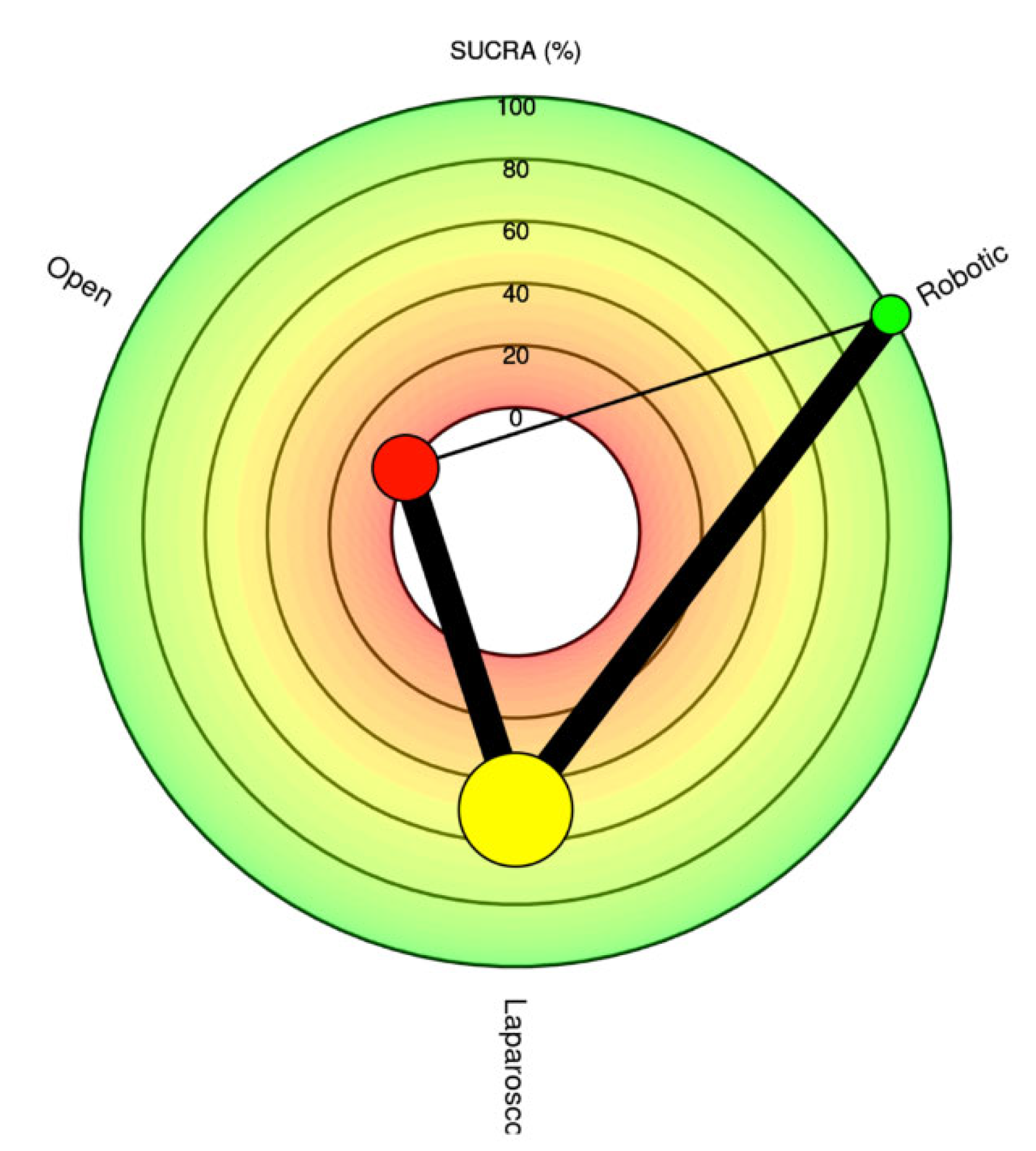
Figure 12.
Stacked Bar Chart Treatment Performance Distribution.
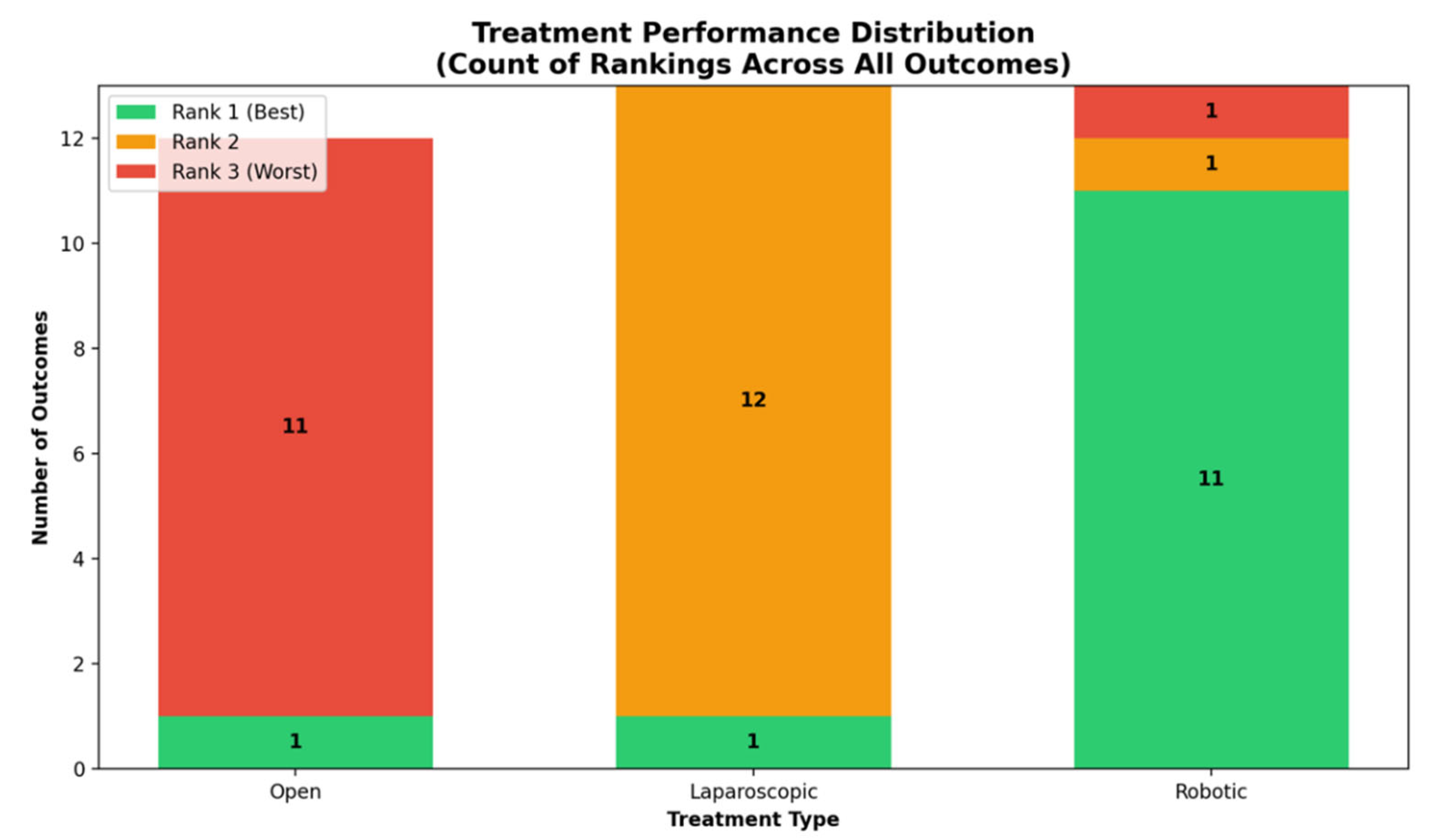
Figure 13.
Treatment Performance Heatmap.
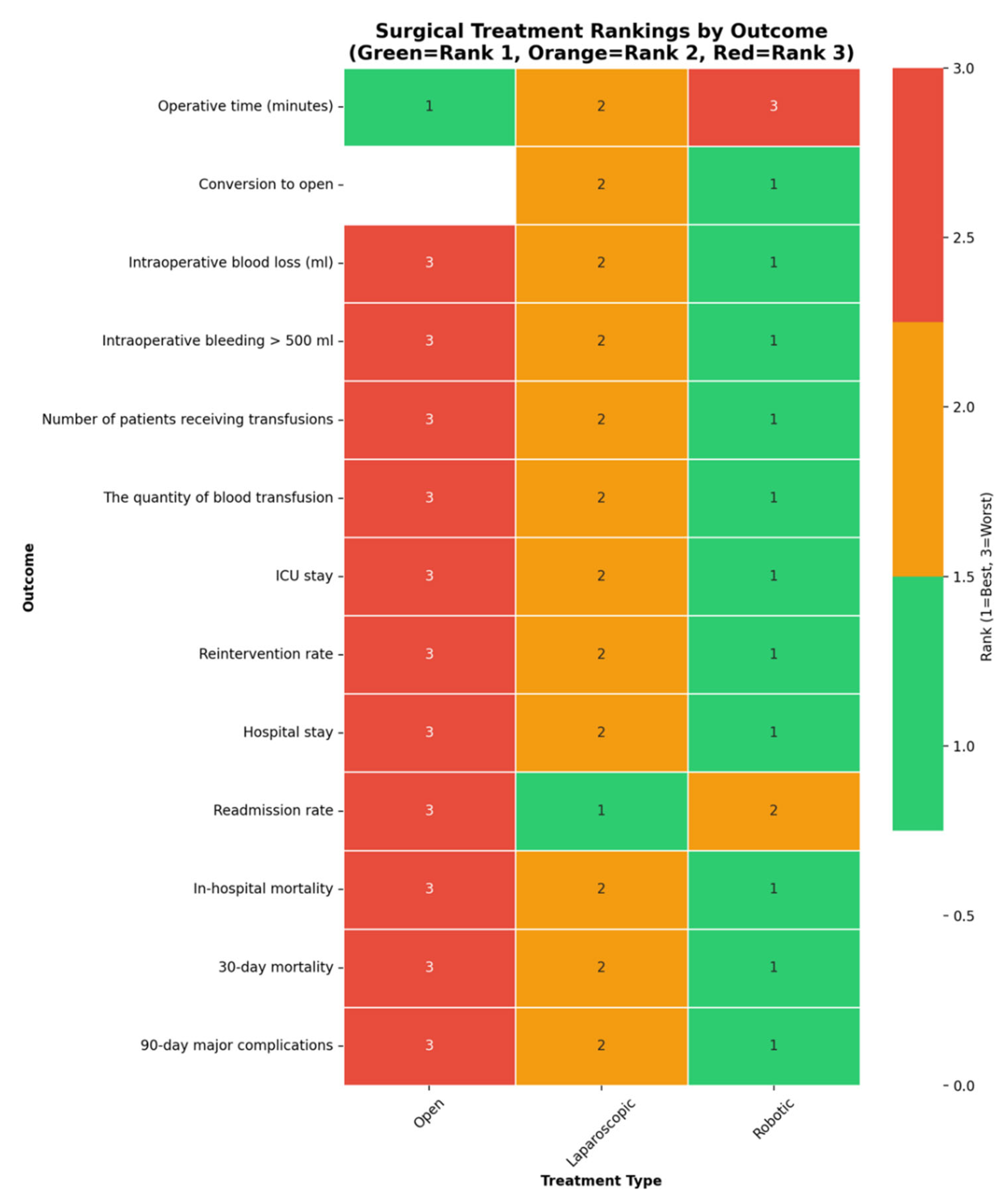
Figure 14.
Radar Chart - Treatment Performance Comparison.
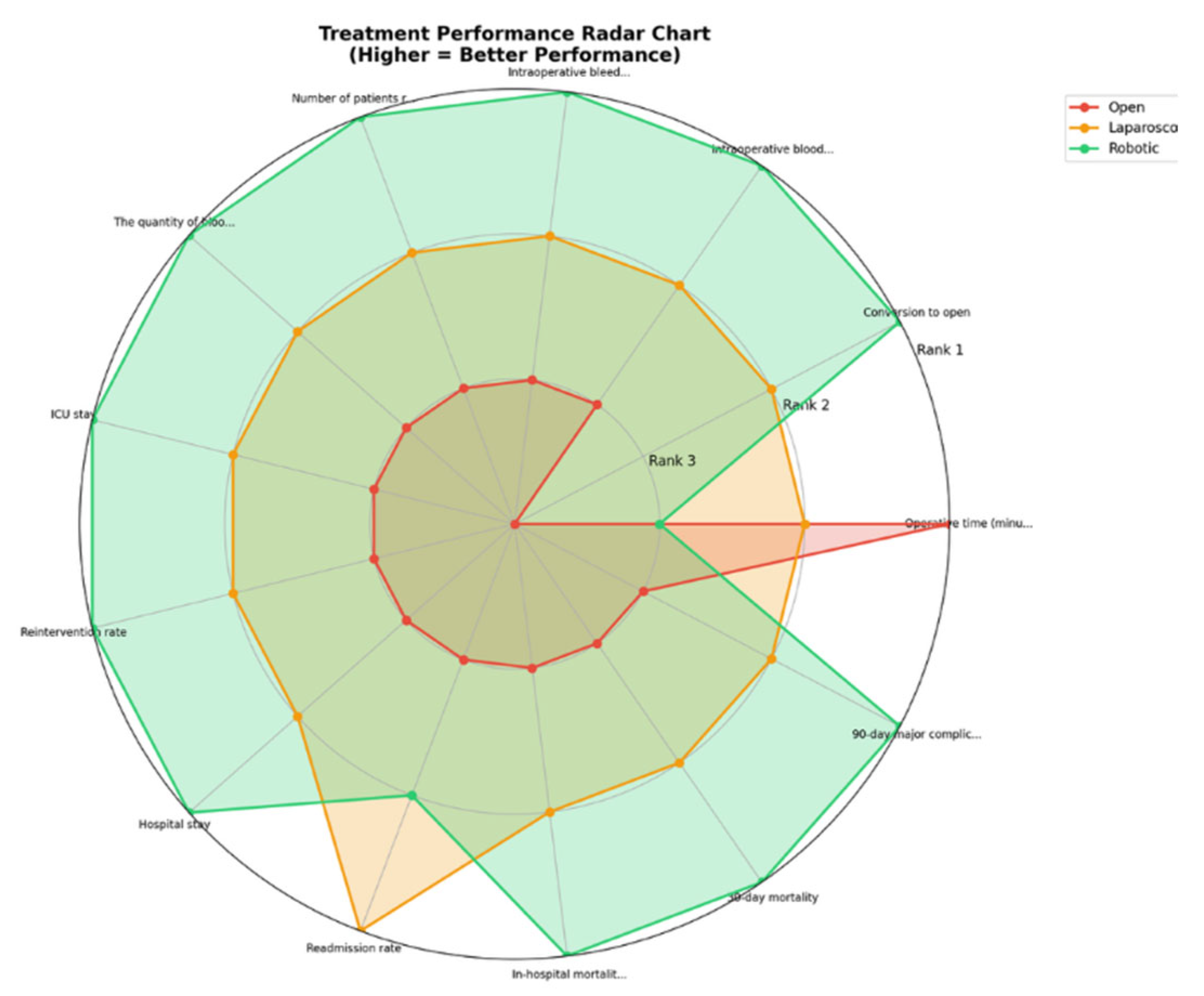
Figure 15.
Horizontal Bar Chart by Outcome Categories.
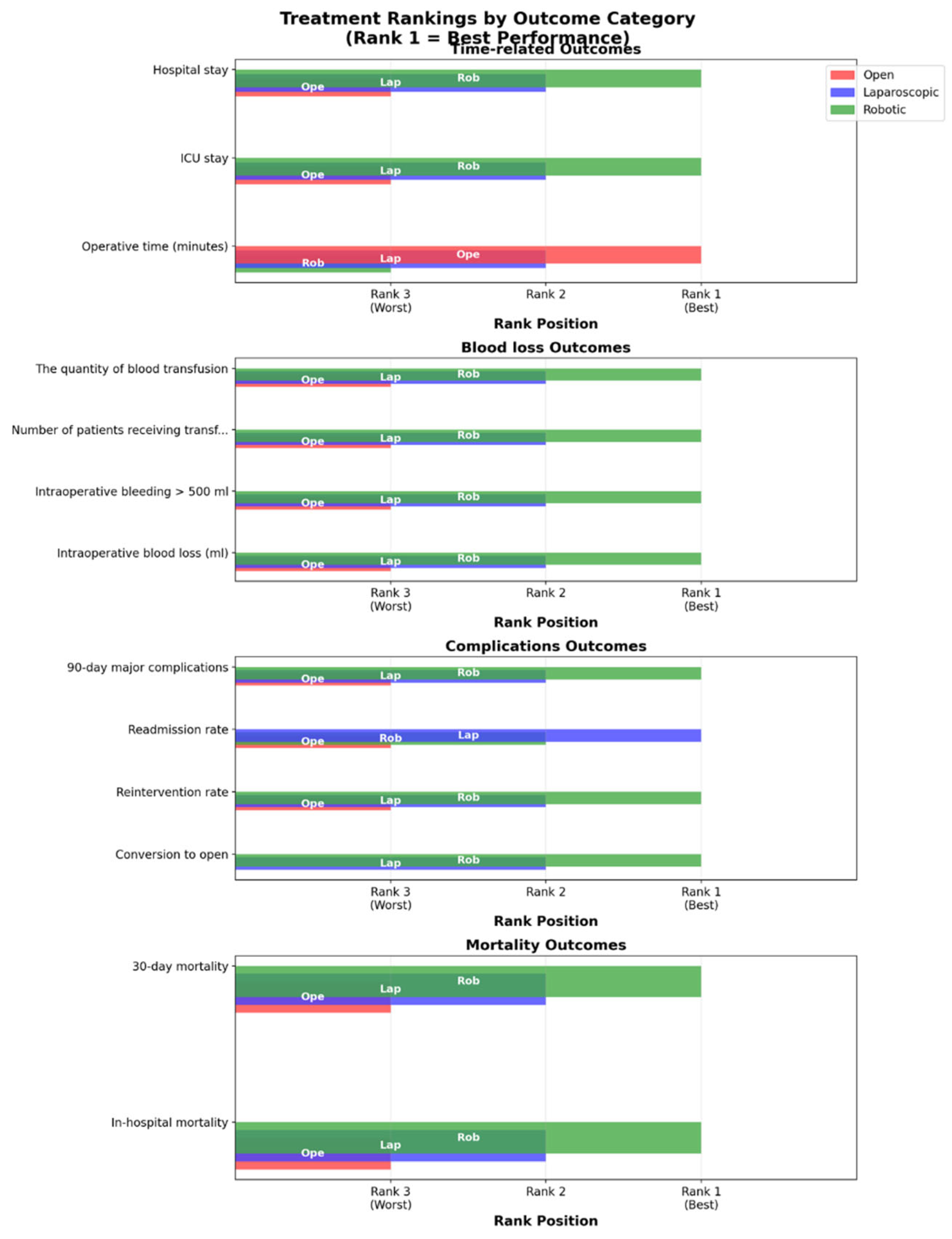
Figure 16.
Comprehensive Performance Analysis.
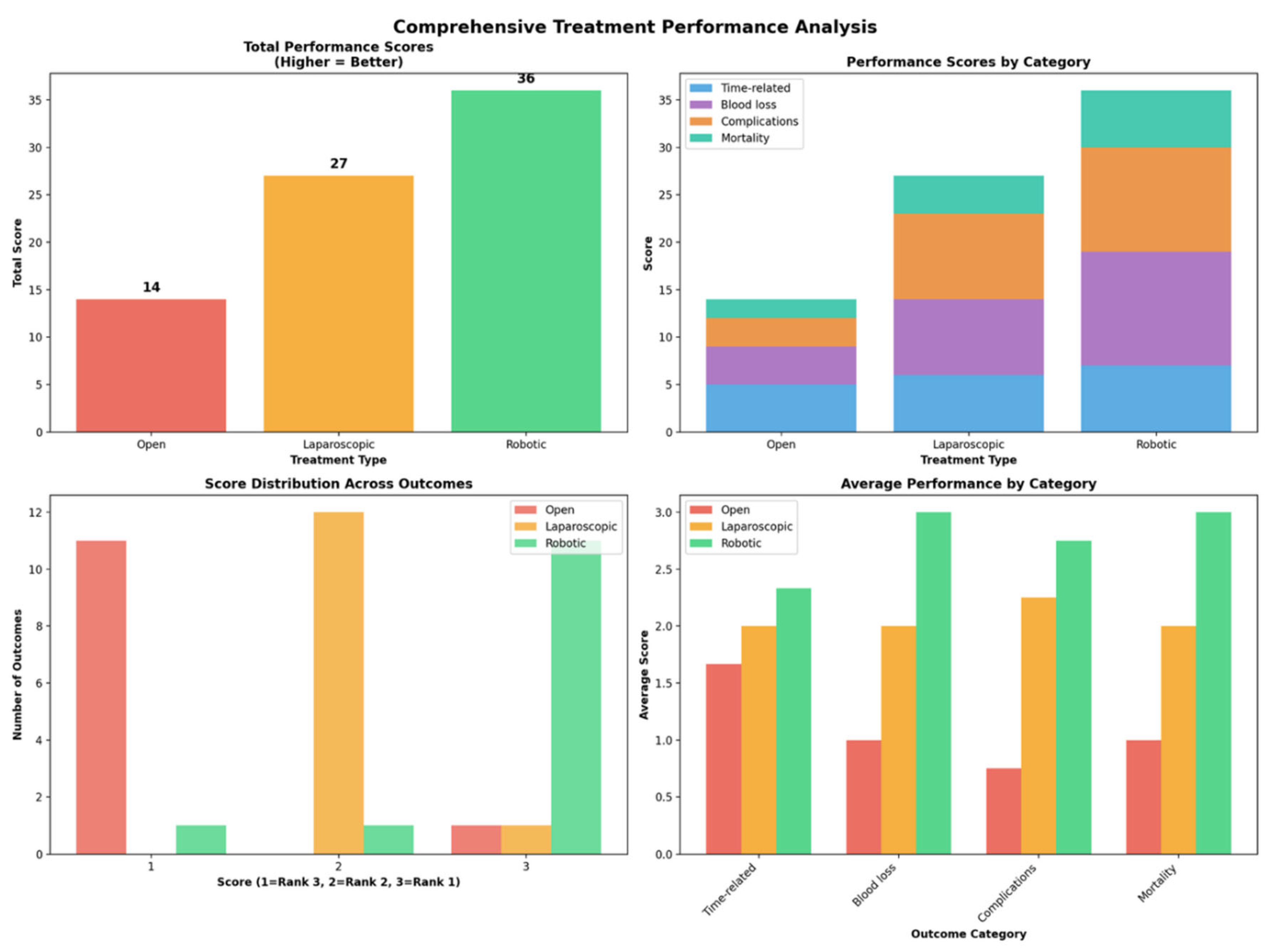
Table 1.
Showing the risk of bias assessment by applying the Newcastle-Ottawa Scale and the Cochrane Risk of Bias 2.0 tool.
Table 1.
Showing the risk of bias assessment by applying the Newcastle-Ottawa Scale and the Cochrane Risk of Bias 2.0 tool.
| Study (year) | Total NOS (0-9) |
|---|---|
| Rodriguez (2018) | 9 |
| Abu Hilal (2012) | 9 |
| Alfieri (2019) | 9 |
| Aly (2010) | 7 |
| Beker (2009) | 9 |
| Benizri (2014) | 8 |
| van Bodegraven (2024) | 9 |
| Butturini (2011) | 8 |
| Butturini (2015) | 8 |
| Casadei (2010) | 9 |
| Chang (2024) | 9 |
| Chen (2022) | 9 |
| Chen (2023) | 9 |
| Daouadi (2013) | 8 |
| De Pastena (2021) | 8 |
| De Pastena (2024) | 9 |
| Ding (2023) | 7 |
| DiNorcia (2010) | 6 |
| Duran (2014) | 7 |
| Eom (2008) | 7 |
| Finan (2009) | 7 |
| Fox (2012) | 8 |
| Goh (2016) | 7 |
| Guerrero-Ortiz (2024) | 7 |
| Hong (2020) | 8 |
| Jarufe (2018) | 9 |
| Jiang (2020) | 9 |
| Kamarajah (2022) | 8 |
| Kang (2010) | 8 |
| Khaled (2015) | 9 |
| Kim(2008) | 6 |
| Kooby (2008) | 8 |
| Lai (2015) | 9 |
| Lai (2022) | 8 |
| Lee (2015) | 9 |
| Lee (2020) | 7 |
| Lelpo (2017) | 7 |
| Limongelli (2012) | 8 |
| Liu (2017) | 9 |
| Lof (2021) | 9 |
| Lyman (2019) | 9 |
| Magge (2018) | 9 |
| Marino (2019) | 9 |
| Mehta (2012) | 8 |
| Morelli (2016) | 9 |
| Najafi (2020) | 9 |
| Nakamura (2009) | 7 |
| Nakamura (2015) | 9 |
| Nickel (2023) | 9 |
| Qu (2018) | 9 |
| Raoof (2018) | 9 |
| Shin (2023) | 9 |
| Souche (2018) | 7 |
| Stauffer (2013) | 9 |
| Velanovich (2006) | 8 |
| Vicente (2019) | 7 |
| Vijan (2010) | 9 |
| Waters (2010) | 7 |
| Wellner (2017) | 9 |
| Weng (2021) | 9 |
| Xourafas (2017) | 9 |
| Yan (2015) | 7 |
| Zhang (2017) | 7 |
| Zhang (2022) | 9 |
| Cho (2011) | 9 |
| Chopra (2021) | 9 |
| Study (year) | Cochrane Risk of Bias 2.0 tool |
| Björnsson (2020) | 4/5 |
Table 2.
Baseline characteristics of the included studies.
| Study | Country | Study period | Study type (RCT/ Retrospective/ Retrospective + prospectively held data base/ Prospective observational/ Prospective observational cu propensity match) | No. Included patients | Comparaison (RDP VS LDP VS ODP) |
|---|---|---|---|---|---|
| Rodriguez_2018[27] | France | 2012-2015 | Retrospective with prospectively maintained database | 89 | RDP VS LDP VS ODP |
| Abu Hilal_2012[28] | UK | 2005-2011 | Retrospective from a prospectively held database | 51 | LDP vs ODP |
| Alfieri_2019[29] | Italy | 2008-2016 | Retrospective | 181 | LDP vs RDP |
| Aly_2010[30] | Japan | 1998-2009 | Retrospective | 75 | LDP vs ODP |
| Beker_2009[31] | USA | 2003-2008 | Prospective Non-randomized | 112 | LDP vs ODP |
| Benizri_2014[32] | France | 2004-2011 | Retrospective with prospectively maintained database | 34 | LDP vs RDP |
| Björnsson_2020[32] | Sweden | 2015-2019 | RCT | 58 | LDP vs ODP |
| van Bodegraven_2024[33] | Pan-European | 2019-2021 | Retrospective with prospectively maintained database | 1672 | RDP vs LDP |
| Butturini_2011[34] | Italy | 1999-2006 | Retrospective non-randomized study | 116 | LDP vs ODP |
| Butturini_2015[35] | Italy | 2011-2014 | Prospective Non-randomized | 43 | LDP vs RDP |
| Casadei_2010[36] | Italy | 2000-2010 | Retrospective case-control study | 44 | LDP vs ODP |
| Chang_2024[37] | USA | 2010-2020 | Retrospective propensity score matching | 1537 | LDP vs RDP |
| Chen_2022[38] | China | 2013-2019 | Retrospective case study | 149 | LDP vs RDP |
| Chen_2023[39] | Internation | 2010-2019 | Retrospective | 542 | LDP vs RDP |
| Daouadi_2013[40] | USA | 2004-2011 | Retrospective | 124 | LDP vs RDP |
| De Pastena_2021[41] | Italy | 2011-2017 | Retrospective propensity score matching | 103 | LDP vs RDP |
| De Pastena_2024[42] | Italy | 2010-2020 | Retrospective | 564 | LDP vs RDP |
| Ding_2023[43] | UK | 2008-2023 | Retrospective with prospectively maintained database | 123 | LDP vs RDP |
| DiNorcia_2010[44] | USA | 1991-2009 | Retrospective with prospectively maintained database | 387 | LDP vs ODP |
| Duran_2014[45] | Spain | 2008-2013 | Retrospective | 47 | LDP vs ODP vs RDP |
| Eom_2008[46] | Korea | 1995-2006 | Retrospective case-control study | 93 | LDP vs ODP |
| Finan_2009[47] | USA | 2002-2007 | Retrospective | 148 | LDP vs ODP |
| Fox_2012[48] | Canada | 2004-2010 | Retrospective | 118 | LDP vs ODP |
| Goh_2016[49] | Singapore | 2006-2015 | Retrospective with prospectively maintained database | 39 | LDP vs RDP |
| Guerrero-Ortiz_2024[50] | Spain | 2022 | Prospective , multicentral national observational study | 80 | LDP vs RDP |
| Hong_2020[51] | South Korea | 2015-2017 | Retrospective | 228 | LDP vs RDP |
| Jarufe_2018[52] | Chile | 2001-2015 | Retrospective | 93 | LDP vs ODP |
| Jiang_2020[53] | China | 2011-2018 | Retrospective | 166 | LDP vs RDP |
| Kamarajah_2022[54] | UK | 2007-2018 | Retrospective | 125 | LDP vs RDP vs ODP |
| Kang_2010[55] | Korea | 1999-2008 | Retrospective | 32 | LDP vs ODP |
| Khaled_2015[56] | UK | 2002-2011 | Retrospective case matched | 44 | LDP vs ODP |
| Kim_2008[57] | South Korea | - | Retrospective | 128 | LDP vs ODP |
| Kooby_2008[58] | USA | 2002-2006 | Retrospective multicentral cohort from a prospectively held database | 667 | LDP vs ODP |
| Lai_2015[59] | China | 1999-2015 | Retrospective from a prospectively held database | 35 | LDP vs RDP |
| Lai_2022[60] | Taiwan | 2011-2020 | Retrospective using a prospectively maintained database | 177 | LDP vs RDP |
| Lee_2015[61] | USA | 200-2013 | Retrospective | 805 | LDP vs RDP vs ODP |
| Lee_2020[62] | Singapore | 2006-2019 | Retrospective from a prospectively held database | 102 | LDP vs RDP |
| Lelpo_2017[63] | Spain | 2011-2017 | Retrospective | 54 | LDP vs RDP |
| Limongelli_2012[64] | Italy | 2000-2010 | Retrospective from a prospectively held database | 45 | LDP vs ODP |
| Liu_2017[65] | China | 2011-2015 | Retrospective propensity score matched study | 355 | LDP vs RDP |
| Lof_2021[66] | Europe | 2011-2019 | Retrospective, Propensity scire matching | 1551 | LDP vs RDP |
| Lyman_2019[67] | USA | 2008-2017 | Retrospective from a prospectively held database | 249 | LDP vs RDP |
| Magge_2018[68] | USA | 2010-2016 | Retrospective from a prospectively held database | 374 | LDP vs ODP vs RDP |
| Marino_2019[69] | Italy | 2014-2017 | Retrospective case matched | 70 | LDP vs RDP |
| Mehta_2012[70] | France | 1998-2009 | Retrospective case-control study | 60 | LDP vs ODP |
| Morelli_2016[71] | Italy | 2010-2014 | Retrospective case matched | 30 | LDP vs RDP |
| Najafi_2020[72] | Germany | 2008-2018 | Retrospective | 56 | LDP vs RDP |
| Nakamura_2009[73] | Japan | 2000-2007 | Retrospective | 36 | LDP vs ODP |
| Nakamura_2015[73] | Japan | 2006-2013 | Retrospective Propensity score matching | 2010 | LDP vs ODP |
| Nickel_2023[74] | Germany | 2007-2020 | Retrospective case matched | 512 | LDP vs RDP vs ODP |
| Qu_2018[75] | China | 2011-2015 | Retrospective propensity score matching | 70 | LDP vs RDP |
| Raoof_2018[76] | USA | 2010-2013 | Retrospective | 704 | LDP vs RDP |
| Shin_2023[77] | Korea | 2015-2020 | Retrospective propensity score matched study | 42 | LDP vs RDP |
| Souche_2018[78] | France | 2011-2016 | Prospective Non-randomized | 38 | LDP vs RDP |
| Stauffer_2013[79] | USA | 2005-2011 | Retrospective | 172 | LDP vs ODP |
| Velanovich_2006[80] | USA | 1996-2005 | Retrospective case matched | 30 | LDP vs ODP |
| Vicente_2019[81] | Spain | 2014-2018 | Prospective Non-randomized | 59 | LDP vs RDP |
| Vijan_2010[82] | USA | 2004-2009 | Retrospective case matched | 200 | LDP vs ODP |
| Waters_2010[83] | USA | 2008-2009 | Retrospective from a prospectively held database | 57 | LDP vs ODP vs RDP |
| Wellner_2017[84] | Germany | 2013-2016 | Retrospective propensity score matched study | 198 | LDP vs ODP |
| Weng_2021[85] | China | 2012-2019 | Retrospective case-control study | 679 | RDP vs ODP |
| Xourafas_2017[86] | USA | 2014 | Retrospective | 1815 | RDP VS LDP VS ODP |
| Yan_2015[87] | China | 2010-2012 | Retrospective | 91 | LDP vs ODP |
| Zhang_2017[88] | China | 2010-2017 | Retrospective | 74 | LDP vs RDP |
| Zhang_2022[89] | China | 2020-2021 | Retrospective | 201 | LDP vs RDP |
| Cho_2011[90] | USA | 1999-2008 | Retrospective using a prospectively maintained database | 693 | LDP vs ODP |
| Chopra_2021[91] | USA | 2008-2019 | Retrospective with prospectively maintained database | 146 | LDP vs ODP vs RDP |
Table 3.
Summary of Findings.
| Outcome | Number of studies | Number of patients | Robotic versus Open | Laparoscopic versus Open | Robotic versus laparoscopic | Ranks based on SUCRA values: I, II, III | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Frequentist NMA | Bayesian NMA | Frequentist NMA | Bayesian NMA | Frequentist NMA | Bayesian NMA | |||||
| Population characteristics |
Age of patients (years) (Frequentist - MD, 95%CI; Bayesian - MD, 95% CrI) |
59 | 17,542 |
-1.65 [-3.00; -0.30] |
-1.67 (-3.11, -0.27) |
-0.72 [-1.86; 0.41] |
-0.74 (-1.95, 0.43) |
-0.93 [-1.93; 0.07] | -0.93 (-1.97, 0.11) |
Robotic Laparoscopic Open |
|
Sex of patients ( male) (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
63 |
18,030 | 0.73 [0.64; 0.82] | - | 0.76 [0.69; 0.84] | - | 0.95 [0.87; 1.05] | - |
Robotic Laparoscopic Open |
|
|
ASA status (grade I-II) (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
40 | 10,318 | - | 1.24 (0.87, 1.8) | - | 1.29 (0.94, 1.78) | - | 0.96 (0.74, 1.27) | Laparoscopic Robotic Open |
|
|
Previous cardiovascular diseases (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
12 | 3,307 | 0.99 [0.62; 1.61] | 0.84 (0.41, 1.45) | 0.94 [0.69; 1.29] | 0.94 (0.62, 1.37) | 1.19 [0.72; 1.96] | 0.9 (0.46, 1.49) | Laparoscopic Robotic Open |
|
| Intra-operative characteristics |
Operative time (minutes) (Frequentist - MD, 95%CI; Bayesian - MD, 95% CrI) |
61 | 16,230 | 25.93 [7.68; 44.18] | 27.17 (4.27, 50.33) | 7.63 [-7.59; 22.85] | 7.84 (-11.24, 26.94) | 18.30 [5.12; 31.49;] | 19.32 (2.74, 36.27) |
Open Laparoscopic Robotic |
|
Conversion to open (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
38 | 10,586 | - | - | - | - | 0.41 [0.34; 0.49] | 0.30 [0.22; 0.40] |
Robotic Laparoscopic |
|
|
Intraoperative blood loss (ml) (Frequentist - MD, 95%CI; Bayesian - MD, 95% CrI) |
51 | 12,257 | -279.45 [-318.28; -240.61] | -303.98 (-382.8, -229.26) | -248.99 [-283.41; -214.57] | -272.89 (-340.15, -209.01) | -30.45 [ -54.66; -6.25] | -31.17 (-81.92, 19.44) |
Robotic Laparoscopic Open |
|
|
Intraoperative bleeding > 500 ml (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
3 | 1,427 | 0.11 [0.01; 1.07] | - | 0.32 [0.23; 0.46] | - | 0.33 [0.03; 3.24] | - | Robotic Laparoscopic Open |
|
|
Number of patients receiving transfusions (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
30 | 9,248 | 0.25 [0.19; 0.34] | - | 0.30 [0.24; 0.37] | - | 0.85 [0.66; 1.10] | - |
Robotic Laparoscopic Open |
|
|
The quantity of blood transfusion (Frequentist - MD, 95%CI; Bayesian - MD, 95% CrI) |
4 | 363 | 1.98 [-3.42; -0.54] | - | -1.86 [-3.12; -0.59] | - | -0.12 [-1.14; 0.89] | - |
Robotic Laparoscopic Open |
|
| Postoperative characteristics |
ICU stay (Frequentist - MD, 95%CI; Bayesian - MD, 95% CrI) |
9 | 1,272 | -4.01 [-5.97; -2.05] | - | -2.27 [-3.71; -0.83] | - | -1.74 [-3.52; 0.04] | - |
Robotic Laparoscopic Open |
|
Reintervention rate (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
37 | 11,568 | - | 0.45 (0.23, 0.84) | - | 0.56 (0.32, 0.96) | - | 0.81 (0.47, 1.3) |
Robotic Laparoscopic Open |
|
|
Hospital stay (Frequentist - MD, 95%CI; Bayesian - MD, 95% CrI) |
63 | 18,113 | -7.63 [-8.65; -6.61] | -8.77 (-13.34, -4.22) | -6.47 [-7.33; -5.60] | -6.93 (-10.67, -3.23) | -1.16 [-1.88; -0.44] | -1.83 (-5.17, 1.55) |
Robotic Laparoscopic Open |
|
| Morbidity and Mortality |
Readmission rate (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
31 | 12,330 | 0.93 [0.67; 1.30] | 0.80 [0.59; 1.09] | 0.86 [0.71; 1.05] | Laparoscopic Robotic Open |
|||
|
In-hospital mortality (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
9 | 1,009 | - | 1.14e-07(5.812-24, 1.36e+06) | 0.76 [0.21; 2.72] | 0.42 [0.04; 2.57] | - | - | Robotic Laparoscopic Open |
|
|
30-day mortality (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
31 | 12,127 |
0.37 [0.16; 0.84] |
- | 0.68 [0.40; 1.17] | - | 0.54 [0.27; 1.07] | - |
Robotic Laparoscopic Open |
|
|
90-day major complications (Frequentist - OR, 95%CI; Bayesian - OR, 95% CrI) |
3 | 1,427 | 0.86 [0.44; 1.68] | 0.87 (0.36, 2.42) | 0.88 [0.51; 1.52] | 0.9 (0.45, 2.3) | 0.98 [0.56; 1.71] | 0.97 (0.42, 1.99) | Robotic Laparoscopic Open |
|
| 95%CI – 95% Confidence Interval; 95%CrI – 95% Credible Interval; MD – mean difference; NMA – network meta-analysis; OR – odds ratio; SUCRA - Surface Under the Cumulative Ranking curve | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



