
Submitted:
31 August 2025
Posted:
01 September 2025
You are already at the latest version
Abstract
Background: Nutraceuticals are bioactive compounds that have shown promise in disease prevention and management. Due to their accessibility and affordability, they have gained increasing interest in obesity management. Some such nutraceuticals are Saccharomyces cerevisiae hydrolysates. Despite this growing interest, clinical practice guidelines rarely address their use, leaving clinicians with limited direction of their usage in routine care. This study aimed to develop a general guidance statement on the appropriateness of a Saccharomyces cerevisiae hydrolysate using a RAND/UCLA consensus process. Methods: A multidisciplinary panel of nine experts was convened to evaluate the appropriateness of a Saccharomyces cerevisiae hydrolysate in various clinical scenarios related to obesity management. Results: The panel deemed the use a Saccharomyces cerevisiae hydrolysate, in combination with lifestyle modifications, as an appropriate intervention for managing obesity-related outcomes. This included its use in patients with specific comorbidities, as an adjunct to standard pharmacotherapy, and in a set of selected clinical scenarios. Conclusions: Combining practitioners' insights with available data, the panel reached consensus that a Saccharomyces cerevisiae hydrolysate represents an appropriate intervention in a range of clinical scenarios for obesity management.
Keywords:
Saccharomyces cerevisiae hydrolysate
; obesity management
; RAND/UCLA appropriateness method
; nutraceuticals
; weight regain prevention
; waist circumference
; inflammation
; consensus
Background
Obesity is a condition in which there is an excess accumulation of adipose tissue and affects nearly all systems in the body.[1,2] Due to its increasing prevalence and implications in well-being, it is considered a major health crisis and a significant threat to global health.[3] Current recommended management strategies include nutritional counseling, structured exercise, psychological and psychiatric support, pharmacotherapy, and bariatric surgery.[2] Although, pharmacotherapy is widely recommended as an integral component of obesity management, significant access barriers limit the use of anti-obesity medications, with only about 2% of eligible patients receiving pharmacological treatment.[4] Additionally, certain medications are not readily available in some regions, or their cost may be prohibitive.[3] Few individuals complete lifestyle modification programs, and many are hesitant to undergo bariatric surgery due to the perception of it being a major invasive procedure.[5] Moreover, even among those who undergo treatment, a substantial proportion eventually regain weight, with similar recurrence rates observed across all intervention types.[6]
Nutraceuticals are bioactive compounds derived from edible sources that have proven beneficial in the prevention and management of disease.[7,8] Owing to their affordability and accessibility, they have attracted growing interest from both patients and healthcare providers.[7,8] Bioactive peptide-rich hydrolysates derived from Saccharomyces cerevisiae have demonstrated efficacy as weight loss-promoting agents across several clinical trials.[9,10,11,12]
Despite the growing availability of nutraceuticals, there remains a significant lack of guidance on their use in routine clinical practice. These products are generally excluded from clinical practice guidelines, leaving clinicians uncertain about their appropriate role in patient care and the validity of manufacturers’ claims.[13] Moreover, clinical trials often fail to capture the complexity and variability of real-world settings. Nevertheless, clinicians are expected to make evidence-based decisions about whether to recommend any given product.[14] The RAND/UCLA Appropriateness Method is a modified Delphi consensus process that combines the best available evidence with expert clinical judgement to evaluate the appropriateness of an intervention for specific scenarios.[14] Within this framework, an intervention is considered “appropriate” when the expected benefits substantially outweigh any potential expected risk, regardless of cost considerations.[14]
To address the current lack of clinical guidance, we convened a panel of clinical experts to assess the appropriateness of this intervention across a range of scenarios commonly encountered in clinical practice using the RAND/UCLA Appropriateness Method. This article presents a guidance statement based on this assessment and intends to support clinicians in making informed decisions about recommending this intervention.
Methods.
RAND/UCLA Appropriateness Method
The RAND/UCLA Appropriateness Method is a formal consensus process that combines the best available evidence with clinical expertise to formulate a group opinion. In situations where available evidence is limited, this methodology supplements this gap with expert opinion. The appropriateness of an approach is determined as whether the expected health benefits outweigh the potential negative consequences by a significant margin to justify a procedure, regardless of cost.[14] This method is a validated, systematic approach for evaluating the appropriateness of interventions at a patient-specific level, particularly in cases where clinical trials are not feasible for every scenario. It has been used to a wide range of interventions.[15,16,17,18,19,20] A diagram of the RAND/UCLA Appropriateness Method is depicted in Figure 1.
Establishment of an Expert Panel
We assembled an expert multidisciplinary panel comprising clinical endocrinologists, nutritionists, internists, general practitioners, and psychiatrists. The experts were recruited through professional contacts and referrals, with eligibility criteria mandating a minimum of five years of experience in managing patients with obesity; those barred from clinical practice were excluded. Panelists received compensation for their time from the study sponsor. However, the funder was not involved in the study’s design, methodology, data analysis, interpretation of results, or panel discussions.
Generation of Scenarios
A comprehensive list of clinical scenarios was developed to reflect the range of conditions and comorbidities commonly encountered in obesity management. An initial draft was refined in collaboration with members of the expert panel to ensure clinical relevance, clarity, and alignment with real-world practice. These scenarios formed the basis of a structured questionnaire, with each item framed according to the Population, Intervention, Comparison, Outcome (PICO) format.
Scenario development followed three key dimensions: (1) the appropriateness of the intervention for managing obesity-related outcomes in patients with specific comorbidities; (2) its appropriateness as an adjunct to conventional pharmacotherapy; and (3) its appropriateness in a set of special clinical situations. All scenarios were stratified by body mass index (BMI) into four categories: 25–29.9 kg/m², 30–34.9 kg/m², 35–39.9 kg/m², and ≥40 kg/m².
The intervention under evaluation consisted in a bioactive peptide-rich Saccharomyces cerevisiae-derived hydrolysate in combination with lifestyle modifications, including medical nutrition therapy, structured exercise, sleep hygiene, and stress management. Interventions which included additional components (such as silymarin, probiotics, minerals, etc.) where excluded from the study.
Systematic Review
We conducted a systematic literature review to gather relevant evidence. Scientific articles were compiled in an online repository and disseminated among the expert panel members prior to the rating rounds. The literature review was conducted in March and April 2025 consulting Pubmed, SciELO, ClinicalTrials.gov, and Cochrane’s CENTRAL. To identify relevant studies, we used the following search terms: ("Saccharomyces cerevisiae" OR "S. cerevisiae" OR "Saccharomyces" OR "Yeast" OR "Bakers yeast") AND ("polysaccharide*" OR "hydrolysate*" OR "neuropeptide Y" OR "*weight*" OR "fat" OR "obes*"). Additionally, a snowballing strategy and expert consultation were employed to identify any additional studies. PICOS for inclusion of studies is displayed in Table 1.
Two-Round Consensus
The expert panel convened for a face-to-face meeting in Mexico City in May 2025. During this session, panelists completed the first round of ratings using a structured questionnaire, in which each scenario was evaluated on a 9-point scale, where "1" indicated "highly inappropriate" and "9" indicated "highly appropriate." Ratings were processed on-site in real time. Following the initial round, a trained moderator facilitated a structured discussion to elicit expert insights, promote broad participation, and encourage the expression of diverse perspectives. The discussion was followed by two brief presentations summarizing relevant literature and evidence pertaining to the intervention under evaluation. Subsequently, a second round of ratings was conducted (Supplementary Dataset S1). In this round, panelists received a revised version of the questionnaire that included their initial ratings alongside summary statistics of their peers ratings. Panel members were invited to either maintain or modify their ratings based on the information and viewpoints presented during the discussion and presentations.
Statistical Analysis
Panelists’ ratings were collected via a custom-designed web form and stored locally on a server running XAMPP (Apache Friends, 2023). The collected data was exported into a Comma-Separated Values format and visualized with Microsoft Excel (Microsoft Corporation, Redmond, WA; 2010), manually verified for accuracy, and then converted to Tab-Separated Values (TSV) format. Data integrity was independently verified twice by two separate individuals. For analysis, the median score and agreement status for each scenario were calculated using a Python script (Python Language Reference, version 3.12; Python Software Foundation, Wilmington, DE; 2023), following the RAND/UCLA Appropriateness Method guidelines (Santa Monica, California: RAND, 2001).[14] Agreement was defined as having no more than two panelists rate outside the three-point range that includes the median. [14]
Ethical Compliance
No bioethical committee approval was required due to the nature of this study. However, all participants provided consent for participation and data use.
Results
Summary of Participants and Answers
The expert panel was comprised of 4 clinical endocrinologists, 1 specialist in internal medicine, 1 psychiatrist, 1 general practitioner, and 2 clinical nutritionists. Eight of them had a primary role in private institutions in México and one of them in an academic institution in the United States. Collectively, experts rated 344 scenarios with a 100% answer rate. Agreement was reached in all 344 scenarios (100%) with all 344 of them (100%) rated as “Appropriate”.
Appropriateness of the Intervention for Managing Obesity-Related Outcomes in Patients with Specific Comorbidities
Experts rated four outcomes (reduction of excess adiposity, reduction of waist circumference, reduction of weight regain, and reduction of low-grade chronic systemic inflammation and oxidative stress) across thirteen clinical conditions: (1) all patients with excess adiposity; (2) patients aged 65 years or older; (3) those receiving antidepressants; (4) those with anxiety disorder; (5) with binge-eating disorder; (6) with a history of pancreatitis; (7) with a history of cholelithiasis; (8) with metabolic dysfunction–associated steatotic liver disease; (9) with arrhythmia; (10) with heart failure; (11) with hypertension; (12) at high risk of cardiovascular disease; and (13) with chronic kidney disease. Each condition was further stratified by BMI into the following categories: 25–29.9 kg/m², 30–34.9 kg/m², 35–39.9 kg/m², and ≥40 kg/m². A total of 208 scenarios were evaluated, and an “Appropriate” agreement was reached for all these scenarios.

Table 2.
Median of ratings of the appropriateness of the intervention with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate in addition to lifestyle modifications for managing obesity-related outcomes in patients with specific comorbidities and stratified by BMI. The boxes in green indicate that an agreement was reached, defined as having no more than two panelists rating outside the three-point range that includes the median. BMI = Body Mass Index.
Table 2.
Median of ratings of the appropriateness of the intervention with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate in addition to lifestyle modifications for managing obesity-related outcomes in patients with specific comorbidities and stratified by BMI. The boxes in green indicate that an agreement was reached, defined as having no more than two panelists rating outside the three-point range that includes the median. BMI = Body Mass Index.
| All patients with excess adiposity | Patients with excess adiposity and age 65 or more | Patients with excess adiposity receiving antidepressants | Patients with excess adiposity and anxiety disorder | Patients with excess adiposity and binge-eating disorder | Patients with excess adiposity and history of pancreatitis | Patients with excess adiposity and history of cholelithiasis | Patients with excess adiposity and Metabolic dysfunction–associated steatotic liver disease | Patients with excess adiposity and arrythmia | Patients with excess adiposity and heart failure | Patients with excess adiposity and hypertension | Patients with excess adiposity and high risk of cardiovascular disease | Patients with excess adiposity and chronic kidney disease | BMI | |
| Reducing excess adiposity | 9 | 9 | 9 | 8.5 | 8.5 | 8 | 8 | 9 | 9 | 9 | 9 | 8.5 | 8 | 25–29.9 kg/m² |
| 9 | 9 | 9 | 8.5 | 8.5 | 8 | 8 | 9 | 9 | 9 | 9 | 8.5 | 8 | 30–34.9 kg/m² | |
| 9 | 9 | 9 | 8.5 | 8 | 8 | 8 | 9 | 9 | 9 | 9 | 8.5 | 8 | 35–39.9 kg/m² | |
| 9 | 9 | 9 | 8.5 | 8 | 8 | 8 | 9 | 9 | 9 | 9 | 8.5 | 8 | >40 kg/m² | |
| Reducing waist circumference | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9 | 9 | 9 | 9 | 9 | 25–29.9 kg/m² |
| 9 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9 | 9 | 9 | 9 | 9 | 30–34.9 kg/m² | |
| 9 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9 | 9 | 8.5 | 9 | 9 | 35–39.9 kg/m² | |
| 9 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9 | 9 | 9 | 9 | 9 | >40 kg/m² | |
| Reducing weight regain | 9 | 9 | 8.5 | 9 | 9 | 8 | 8 | 9 | 9 | 8 | 9 | 9 | 9 | 25–29.9 kg/m² |
| 9 | 9 | 8.5 | 9 | 9 | 8 | 8 | 9 | 9 | 9 | 9 | 9 | 9 | 30–34.9 kg/m² | |
| 9 | 9 | 8.5 | 9 | 9 | 8 | 8 | 9 | 9 | 9 | 9 | 9 | 9 | 35–39.9 kg/m² | |
| 9 | 9 | 8.5 | 9 | 9 | 8 | 8 | 9 | 9 | 9 | 9 | 9 | 9 | >40 kg/m² | |
| Reducing low-grade chronic systemic inflammation and oxidative stress | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 25–29.9 kg/m² |
| 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 30–34.9 kg/m² | |
| 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 35–39.9 kg/m² | |
| 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 9 | >40 kg/m² |
Appropriateness of the Intervention as an Adjunct to Conventional Pharmacotherapy
Experts assessed the appropriateness of prescribing a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate as an adjunct to GLP-1 receptor agonists, naltrexone/bupropion, orlistat, or phentermine for reducing the impact of clinical obesity across seven physiological domains: (1) cardiovascular (hypertension, heart failure); (2) musculoskeletal (knee and hip pain, rigidity, limitations in range of motion); (3) reproductive (polycystic ovary syndrome, anovulation); (4) metabolic (hyperglycemia, dyslipidemia); (5) hepatic (metabolic dysfunction–associated steatotic liver disease); (6) respiratory (sleep apnea/hypopnea, dyspnea, wheezing); and (7) daily life activities. Each scenario was stratified by BMI into four categories: 25–29.9 kg/m², 30–34.9 kg/m², 35–39.9 kg/m², and ≥40 kg/m². Agreement was reached across all 112 evaluated scenarios, supporting the appropriateness of this intervention as a complementary therapy to established pharmacological treatments and lifestyle modifications.
Table 3.
Median of ratings of the appropriateness of the intervention with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate in addition to lifestyle modifications as an adjunct to conventional pharmacotherapy and stratified by BMI. The boxes in green indicate that an agreement was reached, defined as having no more than two panelists rating outside the three-point range that includes the median. BMI = Body Mass Index. GLP-1 RA = glucagon-like peptide-1 receptor agonist.
Table 3.
Median of ratings of the appropriateness of the intervention with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate in addition to lifestyle modifications as an adjunct to conventional pharmacotherapy and stratified by BMI. The boxes in green indicate that an agreement was reached, defined as having no more than two panelists rating outside the three-point range that includes the median. BMI = Body Mass Index. GLP-1 RA = glucagon-like peptide-1 receptor agonist.
| Cardiovascular | Musculoskeletal | Reproductive | Metabolic | Daily-life limitations | Hepatic | Respiratory | BMI | |
| GLP-1 RA | 8 | 8 | 8.5 | 8 | 8 | 8.5 | 8 | 25–29.9 kg/m² |
| 8 | 8 | 8.5 | 8 | 8 | 8.5 | 8 | 30–34.9 kg/m² | |
| 8 | 8 | 8.5 | 8 | 8 | 8.5 | 8 | 35–39.9 kg/m² | |
| 8 | 8 | 8.5 | 8 | 8 | 8.5 | 8 | >40 kg/m² | |
| Naltrexone/Bupropion | 8 | 8 | 8 | 8 | 8 | 8 | 8 | 25–29.9 kg/m² |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | 30–34.9 kg/m² | |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | 35–39.9 kg/m² | |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | >40 kg/m² | |
| Orlistat | 8 | 8 | 8 | 8 | 8 | 8 | 8 | 25–29.9 kg/m² |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | 30–34.9 kg/m² | |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | 35–39.9 kg/m² | |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | >40 kg/m² | |
| Phentermine | 8 | 8 | 8 | 8 | 8 | 8 | 8 | 25–29.9 kg/m² |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | 30–34.9 kg/m² | |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | 35–39.9 kg/m² | |
| 8 | 8 | 8 | 8 | 8 | 8 | 8 | >40 kg/m² |
Appropriateness of the Intervention in a Set of Special Clinical Situations
Experts evaluated the appropriateness of a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate in six special clinical scenarios: (1) prevention of progression to clinical obesity; (2) GLP-1 receptor agonist dose reduction; (3) maintenance of low-dose GLP-1 receptor agonist therapy; (4) use prior to initiating pharmacological treatment or bariatric surgery; (5) prevention of weight regain; and (6) transition to a medication-free period. All scenarios were stratified by BMI into the following categories: 25–29.9 kg/m², 30–34.9 kg/m², 35–39.9 kg/m², and ≥40 kg/m². Agreement was reached across all 24 scenarios, supporting the appropriateness of the intervention as part of a comprehensive obesity management strategy.
Table 4.
Median of ratings of the appropriateness of the intervention with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate in addition to lifestyle modifications in a set of special clinical situations and stratified by BMI. The boxes in green indicate that an agreement was reached, defined as having no more than two panelists rating outside the three-point range that includes the median. BMI = Body Mass Index; GLP-1 RA = Glucagon-Like Peptide-1 Receptor Agonists.
Table 4.
Median of ratings of the appropriateness of the intervention with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate in addition to lifestyle modifications in a set of special clinical situations and stratified by BMI. The boxes in green indicate that an agreement was reached, defined as having no more than two panelists rating outside the three-point range that includes the median. BMI = Body Mass Index; GLP-1 RA = Glucagon-Like Peptide-1 Receptor Agonists.
| BMI | ||
| Prevention of progression to clinical obesity | 8 | 25–29.9 kg/m² |
| 8 | 30–34.9 kg/m² | |
| 8 | 35–39.9 kg/m² | |
| 8 | >40 kg/m² | |
| GLP-1 RA dose reduction | 9 | 25–29.9 kg/m² |
| 9 | 30–34.9 kg/m² | |
| 9 | 35–39.9 kg/m² | |
| 9 | >40 kg/m² | |
| Maintenance of low-dose GLP-1 RA receptor agonist therapy | 9 | 25–29.9 kg/m² |
| 9 | 30–34.9 kg/m² | |
| 9 | 35–39.9 kg/m² | |
| 9 | >40 kg/m² | |
| Prior to initiating pharmacological treatment or bariatric surgery | 8.5 | 25–29.9 kg/m² |
| 8.5 | 30–34.9 kg/m² | |
| 8.5 | 35–39.9 kg/m² | |
| 8.5 | >40 kg/m² | |
| Prevention of weight regain | 9 | 25–29.9 kg/m² |
| 9 | 30–34.9 kg/m² | |
| 9 | 35–39.9 kg/m² | |
| 9 | >40 kg/m² | |
| Transition to a medication-free period | 9 | 25–29.9 kg/m² |
| 9 | 30–34.9 kg/m² | |
| 9 | 35–39.9 kg/m² | |
| 9 | >40 kg/m² |
Discussion
We conducted a formal consensus process using the RAND/UCLA Appropriateness Method to develop expert guidance on the clinical use of a nutraceuticals derived from a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate across three key dimensions: the appropriateness of the intervention for managing obesity-related outcomes in patients with specific comorbidities; as an adjunct to conventional pharmacotherapy for obesity, and appropriateness in a set of special clinical situations.
Excess adiposity is now recognized as a defining feature of obesity, with independence of BMI.[1] Accordingly, interventions should not focus solely on weight reduction, but also on decreasing adiposity, improving obesity-related manifestations, and preventing end-organ damage.[1] Even in patients with preclinical obesity, early interventions should aim to prevent progression to clinical obesity and reduce the risk of associated comorbidities.[1]
Tailoring pharmacological treatment to individual patient characteristics is a fundamental aspect of effective obesity management.[4] Various drug classes have shown meaningful weight-loss benefits, improved metabolic profiles, and reduced obesity-related complications, especially when used alongside lifestyle modifications. [21] Nonetheless, their real-world impact is often constrained by inconsistent individual responses, treatment discontinuation, side effects, and limited accessibility; most notably due to high costs. [2,4,21] A recent projection from the Congressional Budget Office suggested that expanding Medicare coverage to include anti-obesity medications—such as GLP-1 receptor agonists, GIP/GLP-1 dual agonists, and legacy agents like orlistat, bupropion/naltrexone, and phentermine/topiramate—starting in 2026 could raise federal expenditures by $35 billion over a nine-year span. [22] In contrast, anticipated healthcare savings from better health outcomes would be relatively modest, with per-user annual costs significantly surpassing estimated offsets. [22]
Beyond economic implications, clinical decision-making must also consider patient-specific risk factors and contraindications associated with anti-obesity pharmacotherapies. For example, glucagon-like peptide-1 receptor agonists (GLP-1 RAs) should be used with caution in elderly patients, and those with depression, cholelithiasis, or arrhythmias, and are contraindicated in individuals with a history of pancreatitis.[4] Similarly, naltrexone/bupropion should also be used cautiously in elderly patients and those with chronic kidney disease, heart failure, or metabolic dysfunction–associated steatotic liver disease (MASLD); it is contraindicated in patients with uncontrolled hypertension.[4] Orlistat also requires caution in the elderly and in individuals with binge-eating disorder, depression, pancreatitis, cholelithiasis, or heart failure.[4] Phentermine while effective in the short term, is not recommended for long-term use and should be avoided or used cautiously in patients with anxiety or depressive disorders, as well as those with elevated cardiovascular risk.[4] When considering a clinical scenario with a patient with any of these risk factors or contraindications, the expert panel convened that an intervention with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate is appropriate due to its safety profile.
Saccharomyces cerevisiae hydrolysates have demonstrated a favorable safety profile across several clinical trials. For example, in a study by Valero-Pérez et al., the only adverse effect significantly more frequent than placebo was bloating, reported in 24% of participants.[11] Similarly, in a trial by Santas et al., only one participant reported flatulence as an adverse event. [12] Across three studies involving a total of 217 patients, only one individual discontinued participation due to side effects. [10,11,12] In addition to its safety, the intervention has shown clinically meaningful efficacy. In the study by Valero-Pérez et al., participants with obesity experienced an average weight loss of 5.27 kg over 12 weeks, of which 3.44 kg corresponded to fat mass, along with a 1.99 kg/m² reduction in BMI.[11] Similarly, Santas et al. (2017) reported a 1.5 cm reduction in waist circumference after 12 weeks of treatment. [12] These outcomes may be partly mediated by ghrelin-related appetite suppression, as observed in both animal models and human studies.[10,23]
Saccharomyces cerevisiae hydrolysates have consistently demonstrated efficacy in promoting weight loss and reducing fat mass. For instance, Jung et al reported significant reductions in weight, BMI, and fat mass after 8 weeks of treatment compared to placebo.[10] Notably, participants receiving the intervention also demonstrated a significant decrease in calorie intake and a reduced preference for sweet flavors compared to placebo (p<0.05), despite changes in physical activity.[10] In a separate study the same group, daily caloric intake was decreased by an average of 264.38 Kcal after 10 weeks of treatment (p<0.01), resulting in a mean reduction of 3.43 kg in body weight (p<0.001), 1.19 in BMI (p<0.001), and 3.2kg in fat mass (p<0.001) relative to placebo.[24] Similarly, Mosikanon et al. reported a significant reduction of waist circumference of 8.19cm after 6 weeks of treatment compared to placebo (p<0.05).[25]
Weight regain following successful weight loss remains a major challenge in long-term obesity management. [6] This phenomenon occurs regardless of the intervention used to induce weight loss; whether behavioral therapy, pharmacotherapy, or bariatric surgery, and the rate of regain appears consistent across different treatment modalities.[6] While the underlying pathophysiological mechanisms are only partially understood, current evidence implicates low-grade inflammation in adipose tissue, and circulating immune cell activation in post-weight-loss regain.[6] Saccharomyces cerevisiae hydrolysates have demonstrated immunomodulatory effects, including reductions in pro-inflammatory cytokines (IL-6, TNF-α) and elevations in anti-inflammatory IL-10, as shown in a clinical study by Mosikanon et al.[25] [6,26]In line with these mechanisms, Valero-Pérez et al. reported 2 kg less weight regain at 9 months in patients receiving this intervention compared to placebo.[11] Based on this body of evidence, our expert panel concluded that administration of a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate is appropriate for preventing weight regain and mitigating low-grade systemic inflammation and oxidative stress.
The combination of pharmacological agents is a common strategy in therapeutic development, particularly when monotherapy fails to achieve the desired clinical outcomes.[27] Agents with complementary mechanisms of action can enhance efficacy while allowing for lower doses of each component, thereby reducing the risk of dose-dependent side effects and toxicities.[27] For instance, the phentermine/topiramate combination capitalizes on the appetite-suppressing properties of phentermine and the satiety-enhancing effects of topiramate, while naltrexone/bupropion acts through bupropion-mediated stimulation of pro-opiomelanocortin (POMC) neurons and naltrexone’s blockade of inhibitory feedback on these same neurons, ultimately reducing caloric intake.[27,28]
Although no clinical trials have evaluated Saccharomyces cerevisiae hydrolysates in combination with other pharmacological agents, the expert panel agreed, based on the principle of complementary mechanisms of action, that such combinations may offer enhanced efficacy with acceptable safety. This consensus was consistent across all proposed co-interventions (including GLP-1 receptor agonists, naltrexone/bupropion, orlistat, and phentermine) and clinical domains (cardiovascular, musculoskeletal, reproductive, metabolic, hepatic, respiratory, and daily functioning outcomes). Nevertheless, clinical trials are needed to confirm the safety and effectiveness of these proposed combinations.
These rationales led to the evaluation of six special clinical scenarios: (1) prevention of progression to clinical obesity; (2) dose reduction of GLP-1 receptor agonists (GLP-1 RAs); (3) maintenance of low-dose GLP-1 RA therapy; (4) pre-treatment prior to initiating pharmacotherapy or bariatric surgery; (5) prevention of weight regain; and (6) transition to a medication-free period.
Saccharomyces cerevisiae hydrolysates have consistently demonstrated reductions in adiposity across diverse clinical contexts, supporting its appropriateness in delaying the onset of clinical obesity.[10,11,12] When used alongside GLP-1 RAs, this intervention may enhance efficacy through complementary mechanisms of action while enabling dose reduction or maintenance of lower doses. Likewise, initiating treatment with a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate before starting pharmacological or surgical therapies may prime patients with excess adiposity for improved outcomes. Furthermore, its immunomodulatory capacity could help prevent weight regain and facilitate the transition to a medication-free period.[6,25,26] Based on this collective evidence, the expert panel reached consensus that a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate is appropriate for all six clinical scenarios.
Although not formally addressed in the questionnaire, discussions among the experts during the meeting yielded several notable clinical considerations. Clinical nutritionists highlighted the advantage of recommending this intervention to patients, given that it is a non-pharmacological agent and available without a prescription. Reproductive outcomes also emerged as an area of interest; since the intervention reduces both adiposity and low-grade systemic inflammation, it may offer additional benefits for women with reproductive disorders such as infertility or polycystic ovary syndrome. Another point raised was its potential use in patients who are hesitant to initiate pharmacological treatment for weight management. A relevant perioperative application was also identified: given that GLP-1 receptor agonists must be discontinued at least one week prior to surgery due to their effects on gastrointestinal motility, a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate could serve as a temporary substitute during that interval. Finally, particular interest was expressed in its use to support the transition to a medication-free period, especially in patients previously treated with GLP-1 RAs. Clinicians noted that weight regain remains a major concern in this context and recognized the potential of a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate to mitigate this risk while promoting sustained lifestyle changes. These insights reflect the intervention’s perceived value in diverse real-world scenarios and warrant further investigation in future studies.
This study is strengthened by the use of a formal consensus methodology and the inclusion of an expert panel comprising professionals from diverse disciplines. Nonetheless, certain limitations should be acknowledged. First, although the number of panel members is sufficient to obtain reliable results, a larger panel may have enhanced the breadth of perspectives and introduced greater variability in opinion, potentially enriching the consensus process. Second, the panel was composed by professionals of Mexican origin, who considered the conditions of patients in Mexico and Latin America, which limits the extrapolation of their opinion to worldwide scenarios. In a similar way, certain populations were excluded from the beginning, such as children and pregnant women. Third, although the RAND/UCLA Appropriateness Method is well-suited for scenarios lacking high-quality evidence, it inherently relies on expert judgment and cannot substitute for clinical trial data or real-world effectiveness studies. Therefore, specific clinical trials and post-marketing surveillance are warranted to better address these gaps in knowledge. Fourth, although the sponsor had no role in study design or data interpretation, industry funding may introduce perceived bias. This was limited by the introduction of a methodological panel which functioned as an impartial observer and collected and analyzed data independently to reduce the perception of bias. Finally, the limited number of high-quality clinical trials on Saccharomyces cerevisiae hydrolysates constrains the extrapolation of findings beyond short-term use. This limitation, however, underscores the need for future research to validate the intervention's effectiveness and broaden its clinical applicability.
Conclusions
This RAND/UCLA consensus process evaluated the appropriateness of a bioactive polypeptide-rich Saccharomyces cerevisiae hydrolysate as part of obesity management. Across 344 clinical scenarios, the intervention was rated as “appropriate” by a multidisciplinary panel of experts, with full agreement achieved in all cases. The panel supported its use for managing obesity-related outcomes in patients with diverse comorbidities, as an adjunct to conventional pharmacotherapy, and in a variety of special clinical situations.
The panel also identified several clinically relevant considerations beyond the formal questionnaire, including its utility in patients reluctant to initiate pharmacological therapy, in the perioperative setting, and during transitions to a medication-free period. Given its favorable safety profile, immunomodulatory properties, and accessibility without prescription, this intervention represents a promising adjunct in comprehensive obesity care. While current evidence supports its short-term efficacy, further research is warranted to validate its long-term effectiveness, assess outcomes in broader populations, and explore its role in combination therapies. These findings may inform clinical practice and guide future updates to obesity management recommendations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
J.Y.: Conceptualization, Investigation, Writing – review & editing; C.A.R.: Investigation, Writing – review & editing; R.A.C.: Investigation, Writing – review & editing; C.O.M.: Investigation, Writing – review & editing; A.M.: Investigation, Writing – review & editing; H.S.M.: Investigation, Writing – review & editing; J.V.G.: Investigation, Writing – review & editing; R.V.O.: Investigation, Writing – review & editing; P.Z.: Investigation, Writing – review & editing; B.C.T.: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing; E.R.R.: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing; A.A.P.G.: Conceptualization, Funding acquisition, Project administration, Writing – review & editing.
Funding
This research was funded by Laboratorios Columbia Comercial, S.A. de C.V. Grant Number: Not Applicable. The sponsor provided unrestricted financial support but was not involved in the study design, data collection, analysis, interpretation, or manuscript preparation.
Institutional Review Board Statement
Not applicable for this study as it involved no human participants or animals.
Informed Consent Statement
Not applicable.
Data Availability Statement
De-identified panel ratings (Dataset S1) are provided in the Supplementary Materials.
Acknowledgements
The authors would like to express their sincere gratitude to Lic. Manuel Martínez Domínguez (President), Lic. Marcel Urcuyo Sánchez (General Director), and Lic. María Fernanda Gamez García (Sr. Manager of Marketing and Strategy) at Laboratorios Columbia Comercial, S.A. de C.V. for their institutional support throughout this project. Their invaluable contributions were essential to the completion and publication of this consensus. The sponsor provided unrestricted financial support but was not involved in the study design, data collection, analysis, interpretation, or manuscript preparation.
Conflicts of Interest
J.Y. Has received honoraria as a speaker for Novo Nordisk México, Adium Pharma, Sanofi-Aventis México, and Laboratorios Columbia Comercial; as a speaker and consultant for Armstrong Laboratorios México; and as a speaker, consultant, and consensus participant for Merck Sharp & Dohme Comercializadora. C.A.R. Has received honoraria as a speaker and consultant from Novo Nordisk México, Adium Pharma, Sanofi-Aventis México, Laboratorios Columbia Comercial, Armstrong Laboratorios México, and Merck Sharp & Dohme Comercializadora. R.A.C. Has received honoraria as a speaker in activities organized by Viatris Inc, Laboratorios Columbia Comercial, and Adium Pharma S.A. C.O.M. Has received honoraria from Laboratorios Sanfer, Medix, Laboratorios Columbia Comercial, and Elevate. A.M. Has received honoraria from Global Integral Beauty, S.A. de C.V. H.S.M. Has participated as advisory board member, speaker, and researcher for Novo Nordisk México, Eli Lilly Mexico, Laboratorios Columbia Comercial, and AstraZeneca. J.V.G. Has received honoraria from Laboratorios Silanes, Eli Lilly Mexico, Boehringer Ingelheim México, and MSD México. R.V.O. Has received honoraria and served on advisory boards for Laboratorios Columbia Comercial, Merck, Boehringer Ingelheim, Novo Nordisk, AstraZeneca, BMS, Eli Lilly, and Janssen-Cilag. P.Z. Has received honoraria from Takeda México, Productos Medix, Laboratorios Silanes, Janssen-Cilag, Merck, PepsiCo and Laboratorios Liomont. B.C.T. Holds shares at Aequitas Medica S.A.S. de C.V. E.R.R. Is a full-time employee of Aequitas Medica S.A.S. de C.V. A.A.P.G. Is a full-time employee of Laboratorios Columbia Comercial.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI | Body Mass Index |
| GLP-1 | Glucagon-like peptide-1 |
| GLP-1 RA | Glucagon-like peptide-1 receptor agonist |
| GIP | Glucose-dependent insulinotropic polypeptide |
| MASLD | Metabolic dysfunction-associated steatotic liver disease |
| PICO | Population, Intervention, Comparison, Outcome |
| PICOS | Population, Intervention, Comparison, Outcome, Study design |
| RAND/UCLA | RAND/University of California, Los Angeles (Appropriateness Method) |
| IL-6 | Interleukin-6 |
| IL-10 | Interleukin-10 |
| TNF-α | Tumor necrosis factor-alpha |
| POMC | Pro-opiomelanocortin |
| S. cerevisiae | Saccharomyces cerevisiae |
References
- Rubino F, Cummings DE, Eckel RH, et al.: Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. Published Online First: 9 January 2025. [CrossRef]
- Gaskin CJ, Cooper K, Stephens LD, Peeters A, Salmon J, Porter J: Clinical practice guidelines for the management of overweight and obesity published internationally: A scoping review. Obesity Reviews. 2024, 25. [CrossRef]
- Ng M, Gakidou E, Lo J, et al.: Global, regional, and national prevalence of adult overweight and obesity, 1990–2021, with forecasts to 2050: a forecasting study for the Global Burden of Disease Study 2021. The Lancet. 2025, 405:813–38. [CrossRef]
- Chávez-Manzanera EA, Vera-Zertuche JM, Kaufer-Horwitz M, et al.: Mexican Clinical Practice Guidelines for Adult Overweight and Obesity Management. Curr Obes Rep. 2024. [CrossRef]
- Shi Q, Wang Y, Hao Q, et al.: Pharmacotherapy for adults with overweight and obesity: a systematic review and network meta-analysis of randomised controlled trials. The Lancet. 2024, 403:e21–31. [CrossRef]
- van Baak MA, Mariman ECM: Physiology of Weight Regain after Weight Loss: Latest Insights. Curr Obes Rep. 2025, 14. [CrossRef]
- Alali M, Alqubaisy M, Aljaafari MN, et al.: Nutraceuticals: Transformation of conventional foods into health promoters/disease preventers and safety considerations. Molecules. 2021, 26. [CrossRef]
- Puri V, Nagpal M, Singh I, et al.: A Comprehensive Review on Nutraceuticals: Therapy Support and Formulation Challenges. Nutrients. 2022, 14. [CrossRef]
- Mancebo-Molina R, Castañe-Sitjas FX, Cuñé-Castellana J, et al.: LIGANDO DE GRASAS OBTEN IDO A PARTIR DE LA BIOMASA DEL PROCEDIMIENTO DE ELABORACIÓN DE LA CERVEZA. (2014). , 1–52.
- Jung EY, Lee JW, Hong YH, Chang UJ, Suh HJ: Low dose yeast hydrolysate in treatment of obesity and weight loss. Prev Nutr Food Sci. 2017, 22:45–9. [CrossRef]
- Valero-Pérez M, Bermejo LM, López-Plaza B, García MA, Palma-Milla S, Gómez-Candela C: Regular consumption of LIPIGO® promotes the reduction of body weight and improves the rebound effect of obese people undergo a comprehensive weight loss program. Nutrients. 2020, 12:1–14. [CrossRef]
- Santas J, Lázaro E, Cuñé J: Effect of a polysaccharide-rich hydrolysate from Saccharomyces cerevisiae (LipiGo®) in body weight loss: randomised, double-blind, placebo-controlled clinical trial in overweight and obese adults. J Sci Food Agric. 2017, 97:4250–7. [CrossRef]
- Batsis JA, Apolzan JW, Bagley PJ, et al.: A Systematic Review of Dietary Supplements and Alternative Therapies for Weight Loss. Obesity. 2021, 29:1102–13. [CrossRef]
- Fitch Kathryn: The Rand/UCLA appropriateness method user’s manual. Rand; 2001.
- Masuda E, Ozsvath K, Vossler J, et al.: The 2020 appropriate use criteria for chronic lower extremity venous disease of the American Venous Forum, the Society for Vascular Surgery, the American Vein and Lymphatic Society, and the Society of Interventional Radiology. J Vasc Surg Venous Lymphat Disord. 2020, 8:505-525.e4. [CrossRef]
- Woo K, Ulloa J, Allon M, et al.: Establishing patient-specific criteria for selecting the optimal upper extremity vascular access procedure. J Vasc Surg. 2017, 65:1089-1103.e1. [CrossRef]
- Saust LT, Siersma VD, Bjerrum L, Hansen MP: Development of quality indicators for the diagnosis and treatment of urinary tract infections in general practice: a RAND appropriateness method. BMJ Open Qual. 2023, 12:e002156. [CrossRef]
- Broder MS, Gibbs SN, Yermilov I: An Adaptation of the RAND/UCLA Modified Delphi Panel Method in the Time of COVID-19. J Healthc Leadersh. 2022, Volume 14:63–70. [CrossRef]
- Carson-Stevens A, Campbell S, Bell BG, et al.: Identifying ‘avoidable harm’ in family practice: a RAND/UCLA Appropriateness Method consensus study. BMC Fam Pract. 2019, 20:134. [CrossRef]
- Saavedra-Fuentes N, Carmona-Montesinos E, Castañeda-Hernández G, et al.: Appropriateness of Ketoanalogues of Amino Acids, Calcium Citrate, and Inulin Supplementation for CKD Management: A RAND/UCLA Consensus. Nutrients. 2024, 16:2930. [CrossRef]
- Grunvald E, Shah R, Hernaez R, et al.: AGA Clinical Practice Guideline on Pharmacological Interventions for Adults With Obesity. Gastroenterology. 2022, 163:1198–225. [CrossRef]
- Congressional Budget Office: How Would Authorizing Medicare to Cover Anti-Obesity Medications Affect the Federal Budget? Washington, D.C.: Congressional Budget Office. (2024). Accessed: April 9, 2025. https://www.cbo.gov/publication/60816.
- Hong KB, Jung EY, Kim JH, Chang UJ, Suh HJ: Yeast hydrolysate as a functional anti-obesity ingredient: appetite suppressive effects of yeast hydrolysate in food deprived mice. Progress in Nutrition. 2015, 17:262–4.
- Jung EY, Cho MK, Hong YH, Kim JH, Park Y, Chang UJ, Suh HJ: Yeast hydrolysate can reduce body weight and abdominal fat accumulation in obese adults. Nutrition. 2014, 30:25–32. [CrossRef]
- Mosikanon K, Arthan D, Kettawan A, Tungtrongchitr R, Prangthip P: Yeast β–Glucan Modulates Inflammation and Waist Circumference in Overweight and Obese Subjects. J Diet Suppl. 2017, 14:173–85. [CrossRef]
- Bertuccioli A, Cardinali M, Biagi M, Moricoli S, Morganti I, Zonzini GB, Rigillo G: Nutraceuticals and herbal food supplements for weight loss: Is there a prebiotic role in the mechanism of action? Microorganisms. 2021, 9. [CrossRef]
- Bays H: Phentermine, topiramate and their combination for the treatment of adiposopathy ('sick fat) and metabolic disease. Expert Rev Cardiovasc Ther. 2010, 8:1777–801. [CrossRef]
- Grilo CM, Lydecker JA, Morgan PT, Gueorguieva R: Naltrexone + Bupropion Combination for the Treatment of Binge-eating Disorder with Obesity: A Randomized, Controlled Pilot Study. Clin Ther. 2021, 43:112-122.e1. [CrossRef]
Figure 1.
Diagram of the RAND/UCLA Appropriateness Method. a. Before the meeting: (1) Experts were recruited via professional networks and referrals. (2) Clinical scenarios were generated through preliminary discussions with the panel, and a PICO-based questionnaire was developed. (3) A systematic review was conducted. b. During the meeting: (4) Experts independently rated the appropriateness of each intervention across scenarios. (5) Ratings were submitted via a custom web form, stored locally, and manually verified. Data were processed in Python following RAND/UCLA guidelines. Agreement was defined as no more than two ratings falling outside the 3-point range containing the median. (6) Brief presentations and moderated discussion supported consensus-building. (7) Experts re-rated each intervention, incorporating insights from the discussion. c. After the meeting: (8) Final ratings were analyzed to determine agreement levels. Created with BioRender.com. .
Figure 1.
Diagram of the RAND/UCLA Appropriateness Method. a. Before the meeting: (1) Experts were recruited via professional networks and referrals. (2) Clinical scenarios were generated through preliminary discussions with the panel, and a PICO-based questionnaire was developed. (3) A systematic review was conducted. b. During the meeting: (4) Experts independently rated the appropriateness of each intervention across scenarios. (5) Ratings were submitted via a custom web form, stored locally, and manually verified. Data were processed in Python following RAND/UCLA guidelines. Agreement was defined as no more than two ratings falling outside the 3-point range containing the median. (6) Brief presentations and moderated discussion supported consensus-building. (7) Experts re-rated each intervention, incorporating insights from the discussion. c. After the meeting: (8) Final ratings were analyzed to determine agreement levels. Created with BioRender.com. .
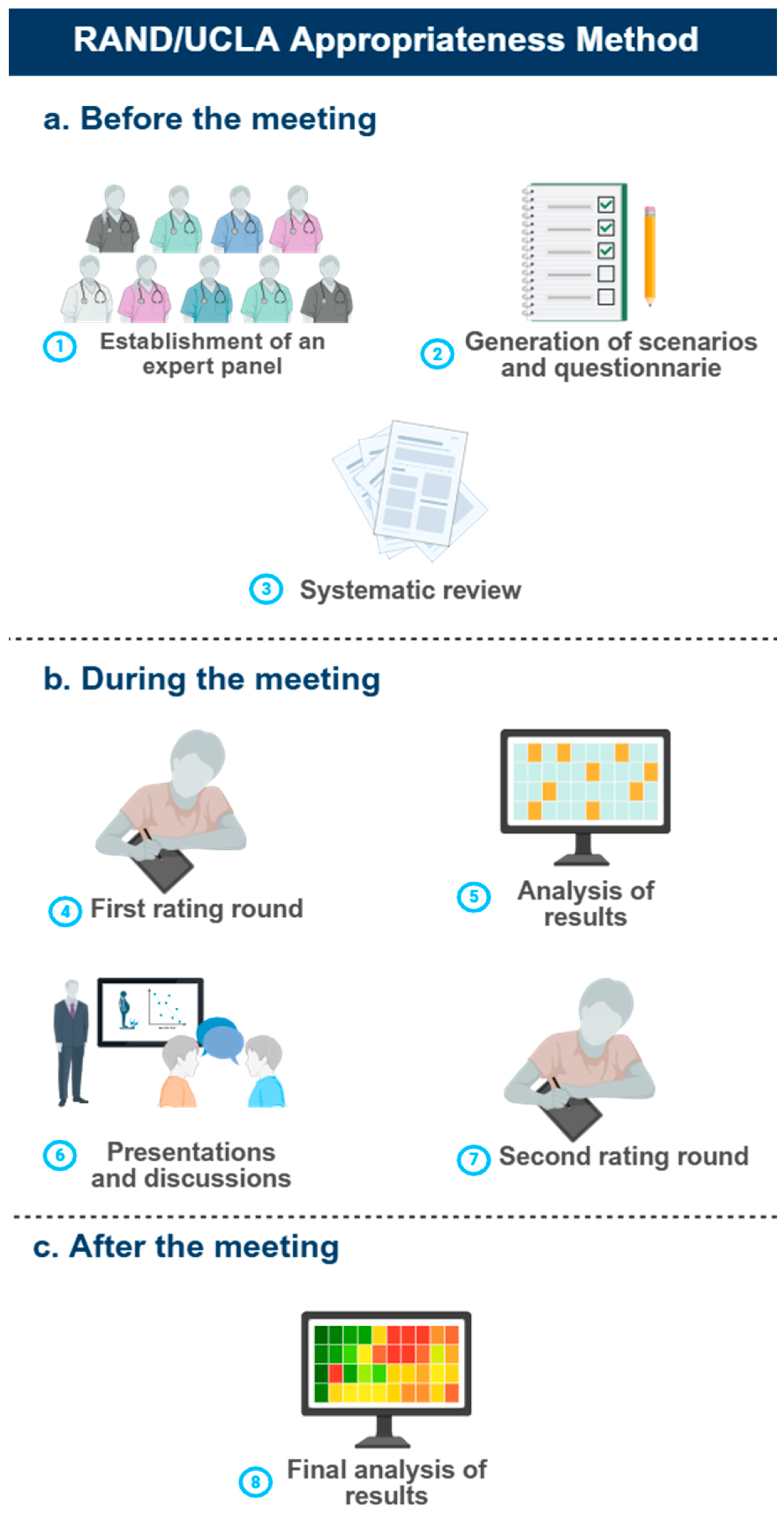
Table 1.
PICOS criteria for inclusion of studies.
| Parameters | Inclusion Criteria |
| Population | Overweight or obese patients |
| Intervention | Bioactive peptide-rich Saccharomyces cerevisiae hydrolysates + lifestyle modifications (medical nutrition therapy, structured exercise, sleep hygiene, and stress management) |
| Comparison | Placebo |
| Outcomes | Changes in body weight, fat composition/mass, BMI, and abdominal perimeter |
| Study Design | Blinded, randomized, placebo-controlled clinical trials |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



