
Submitted:
01 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
Rising obesity and associated multi-systemic complications amplify the health burden. Euphorbia kansui (EK) extract is clinically recognized for managing obesity. In human study, 240 obese individuals were categorized into two cohorts: those receiving solely herbal medicine (HM group), and those administered EK concomitantly with herbal medicine (EK group). An in vivo examination using C57BL/6-Lepob/Lepob mice elucidated mechanisms involving macrophages and gut microbiota, with associated metabolic advantages. The clinical study revealed a significant 7.22% body weight reduction during 91.55 average treatment days, and examined 16.71% weight loss at 300 days after treatment. In the whole subjects, 60.4%, 21.3% and 6.3% achieved weight reductions exceeding 5%, 10% and 15%, respectively. Impressively, the EK group exhibited superior weight loss compared to the HM group (EK: -7.73% vs. HM: -6.27%, p=0.012). The anti-obesity effect was positively associated with EK therapy frequency and herbal medicine duration. In vivo, EK significantly improved insulin sensitivity and mitigated infiltration of adipose tissue macrophages (ATMs) by modulating the CD11c+ and CD206+ subtypes. EK also correlated with increased Bacteroidetes and Firmicutes populations and reduced Proteobacteria and Verrucomicrobia. Consequently, EK is an effective adjunctive anti-obesity therapy offering metabolic benefits by modulating ATMs and gut microbiota profiles.
Keywords:
Keywords Anti-obesity
; herbal remedies
; Euphorbia kansui
; insulin resistance
; gut microbiota
; adipose tissue macrophage
; weight management
Keywords anti-obesity; herbal remedies; Euphorbia kansui; insulin resistance; gut microbiota; adipose tissue macrophage; weight management
1. Introduction
The global attention on obesity is driven by its detrimental effect on a range of health problems, however, there is few effective treatments to target both body weight reduction and improvement of insulin resistance, such as lifestyle, pharmaceutical, and surgical options which are limited by hard maintenance or adverse effects involving psychological, gastrointestinal or cardiovascular events [1,2].
The intricate interplay between the accumulation of body fat and its resultant impact on systemic metabolism and immune equilibrium underscores the overarching significance of this issue [3]. Obesity evolves into a chronic inflammatory state with low grade derived by adipose tissue macrophages (ATMs), primarily connecting obesity to the development of insulin resistance which initiates from aberrant lipolysis and cytokine secretion in adipose tissue [4]. In obese individuals, the precursor monocytes infiltrate adipose tissue in greater numbers and the ATMs are frequently polarized toward the M1 pro-inflammatory profile releasing cytokines which impair insulin signaling [5,6]. Recently, intestinal microbiome is suggested as a therapeutic target for metabolic problems because the changes in microbial phyla have been reported to affect body composition [7]. High fat diet feeding changes gut permeability and elevates lipopolysaccharide (LPS) level, which is essential to trigger infiltration of ATMs. However, weight gain as well as insulin intolerance also arise upon modification of intestinal microbiota, irrespective of microbiota-induced LPS production [8].
Euphorbia kansui radix (EK), also known as Gan Sui (甘遂), is a traditional Korean medicinal herb belonging to Euphorbiaceae family. The therapeutic properties of EK have been reported on cirrhotic ascites [9], pleural effusion [10], diuresis [11] and various cancers[12,13]. Especially, the immunomodulatory activities were reported that EK suppressed Th17 and Th1 differentiation related to excessive inflammation and autoimmune diseases [14]. Van et al. demonstrated that Euphorbia tirucalli, a plant in Euphorbiaceae family, suppressed CD4+ and CD8+ T cells associated with interleukin-2 and interferon, and also inhibited the migration of leukocytes [15]. In the respect of metabolic diseases, previous studies revealed that other species in Euphorbiaceae had anti-diabetic [16] and anti-obesity properties [17], however, there are few studies on EK though EK therapy has been applied in obese patients in South Korea. Therefore, we collected the clinical data about EK therapy, confirmed the in vivo effects on body weight and insulin resistance, and investigated the mechanisms via monocytes, ATMs and intestinal microbiota.
2. Results
2.1. Clinical Results from Human Study
2.1.1. Baseline Characteristics
A total of 480 patients who first visited the Weight Management Center to lose weight taking herbal medicine (HM) treatment based on TKM theory. Among them, 240 patients were studied while the other 240 patients were excluded from the analysis due to overweight not obesity or a lack of follow-up visits (Figure 1).
The number of patients who took EK therapy was 155. Demographic characteristics at baseline did not differ significantly between the EK group and the HM group including gender, age, height, smoking and drinking habits, and follow-up duration. However, we confirmed the significant tendency of patients with high body weight, BMI, and body fluid to perform EK therapy at the first visit (Table 1). The primary procedure of EK therapy entails inducing diarrhea and vomiting typically lasting for 6 to 8 hours. In EK group, 58.95% of patients experienced only diarrhea without vomiting and the number of diarrhea and vomiting was 5.51±2.38 and 0.79±1.24, respectively. The compliance rate of both group was 68.3 ± 23.5 and 67.2 ± 24.5 %, respectively.
2.1.2. Effects on Body Weight
Significant changes in the percentage of body weight reduction were observed from baseline to final visit of each participant in trial period (-7.22 ± 5.16%, p<0.001). The impact on weight loss in the EK group was significantly greater than the corresponding effect in the HM group (-7.73 ± 4.98 % vs. -6.27 ± 5.40 %, p=0.012) (Figure 2a). In total participants, mean changes in BMI from baseline to each final visit was -2.14 ± 1.85 kg/m2 (Figure 2c). The changes in both body weight and BMI demonstrated a statistically significant difference between the EK and HM group (p<0.001) (Figure 2b-c). In total participants, the average bodyweight reduction increased over the course of the treatment, and the estimated mean bodyweight change from baseline to 300 days was -17.6 ± 7.01 % (Figure 2d). At 30, 60, 90 days, the average bodyweight changes were significantly greater in the EK group compared to the HM group (Figure 2d). The percentages of participants in EK group who achieved ≥ 5%, ≥ 10% and ≥ 15% body weight loss were 66.4%, 21.9% and 7.09%, and those in HM group were 57.9%, 20.4% and 6.02%, respectively (Figure 2e). The trial number of EK therapy affected the mean bodyweight reduction by HM treatment (Figure 2f).
2.1.3. Change in the Body Compositions
In the whole participants, fat weights were significantly changed at the final visit compared to the first visit (-3.35±4.94kg, p<0.001), but muscle and body fluid were not significantly changed (p>0.05). The changes in fat weight were not significantly different between the two groups (p=0.15), however, the weights of body fluid and muscle decreased in the EK group and increased in the HM group with significant difference (p<.0.01) (Figure 3).
2.1.4. Adverse Events after EK Therapy and during HM Treatment
There was no severe adverse event or unpredictable event after EK therapy, but 2 patients reported mild abdominal pain until the following day after EK therapy and 1 patient reported mild dizziness in the day of EK therapy. There were two patients in the EK group who dropped out because of systolic blood pressure elevation upper 200 mmHg and no favorable weight loss, respectively. Any serious adverse event was not reported throughout the duration of HM treatment. Among 200 patients observed at 30 days, 72.5 % reported no side effects. The most frequently reported side effect experienced by patients during HM treatment was poor sleep quality, however, its severity was not sufficient to result in treatment discontinuation. Mild constipation, dry mouth, diarrhea and nausea were the subsequent most commonly reported adverse events.
2.2. Results from Animal Model
2.2.1. Body Weight, Glucose Metabolism and Lipid Profile
Both the ob/ob and EK groups demonstrated no significant difference in body and epi fat weights. At 4 and 8 weeks, fasting blood glucose (FBG) of the EK group was significantly lower than that of the ob/ob group (Figure 4). In oral glucose tolerance tests (OGTT), the blood glucose levels at 30 60, 90 and 120 minutes were significantly reduced in the EK group compared to the ob/ob group. The area under the curve (AUC) also showed a similar propensity. The EK group showed decreased fasting serum insulin (FSI) and homeostatic model assessment for insulin resistance (HOMA-IR) compared to the ob/ob group (FSI: 2.62±0.58ng/mL vs. 5.66±1.36ng/mL, p=0.07; HOMA-IR: 48.30±14.29 vs. 175.13±42.40, p<0.05). Among lipids, triglyceride (TG), and non-esterified fatty acid (NEFA) concentrations in the EK group were significantly decreased compared to the ob/ob group (Figure 4).
2.2.2. Safety Profile
To determine the toxic effect of EK on the liver and kidney function, serum levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT) and creatinine were investigated. The creatinine and AST level were not influenced by EK administration, and the difference of ALT level between the EK and ob/ob groups was not significant.
2.2.3. Mechanism of EK Therapy in Macrophages and Monocytes
ATM demonstrated significantly increased in the percentage of total and CD11c+ and decreased in the percentage of CD206+ in the ob/ob group compared to the WT group. The EK group showed significantly reduced percentage of total and CD11c+ ATM, and enhanced percentage of CD206+ ATM (Figure 5). The number of ATM per epi fat weight was significantly decreased in the ob/ob group compared to the WT group, but significantly increased in the EK group compared to the ob/ob group. In monocyte analysis, the ob/ob group had lower percentage of CD11b+/Ly6clow and higher percentage of CD11b+/Ly6chigh than the WT group. However, the EK group demonstrated significantly elevated percentage of CD11b+/Ly6c and decreased percentage of CD11b+/Ly6chigh compared to the ob/ob group (Figure 6).
2.2.4. Mechanism of EK Therapy in Gut Microbiota
In phylum analysis, the two major phyla, both of Bacteroidetes and Firmicutes showed significantly reduced in the ob/ob group compared to the WT group, however, the EK group demonstrated the significant increment in both of them (Bacteroidetes: 73.13±0.42% vs. 58.49±2.39%; Firmicutes: 18.79±1.64% vs. 13.93±0.55%). Verrucomicrobia was the second abundant in the ob/ob group, however, the proportion of Verrucomicrobia substantially decreased in the EK group (2.59±2.16%). The other increasing fecal microbial species in the ob/ob group compared to WT group were Actinobacteria and Proteobacteria, both of which were decreased in the EK group. Deferribacteres phylum was significantly increased in the EK group compared to the ob/ob group (6.24±1.73% vs. 0.38±0.18%). According to Simpson’s method, the diversity indexes of all three groups were not significantly different from each other. However, the results of Principal Coordinate Analysis (PCoA) and Unweighted Pair Group Method with Arithmetic mean (UPGMA) suggested similar pattern of microbiota composition between the WT and EK group, distinctly different from the ob/ob group (Figure 7).
3. Discussion
The current study was the first real-world clinical study with EK therapy and HM treatment for obesity in South Korea, and also investigated its mechanism. The patients who took only HM treatment significantly lost 6.27±5.40 % of body weight, however, the other patients who additionally took once or twice EK therapy significantly demonstrated the additional weight loss of 1.45%. In demographic features, patients in the EK group showed a tendency to have higher BMI, fat, muscle and body fluid. Moreover, the EK therapy during HM treatment significantly attributed to additional effects on the change in BMI, muscle and body fluid. According to in vivo mechanism study, EK therapy showed the significant effects on adipose tissue inflammation at macrophage and monocyte level and changed the gut microbiota towards the pattern of the lean, not that of the obese. Therefore, this article proposed the EK therapy as an effective adjunctive treatment to be combined with HM treatment for obesity.
The EK therapy plus HM treatment showed 7.7 % of body weight, and significant reductions in BMI, muscle and body fluid compared to only HM treatment were observed. In regard of body fat loss, two groups were not statistically different. As the anti-obesity efficacy increased over the HM treatment time, the EK group showed significantly greater weight loss until 90 days, however, the mean change of bodyweight at 300 days was greater in the HM group. We confirmed that anti-obesity efficacy significantly increased according to the number of undergoing EK therapies (p<0.01). Notably, the trial number of EK therapy was concentrated at the early treatment period. In the EK group, all subjects underwent EK therapy within 30 days from baseline, and the number of subjects undergoing EK therapy substantially diminished as 13, 10, 6, 5, 3, and 2 at 60, 90, 120, 180, 300 days, respectively. In previous prospective study with EK therapy [18], one trial of EK therapy contributed to a significant body weight loss of 1.27 kg. Our HM group was shown as similar as the results from the previous studies treated with various polyherbal decoctions such as Bofutsushosan [19], Gambisan [20], Taeeumjowee-Tang [21] and Chegamuiyiin-Tang [22]. Gambisan which showed 6.2 % of body weight loss and 2.87 % of body fat. Taking a compliance rate of Gambisan study was higher than 70 %, the weight loss effect of adjunctive EK therapy was potent losing 7.73 % of body weight and 2.47 % of body fat [20].
Our study assessed safety of EK therapy by self-reported adverse events during treatment period and laboratory blood tests in mice. We observed no toxic effect on liver and kidney in mice, and Lee et al. [18] confirmed no significant difference in AST, ALT, GGT, BUN, creatinine and eGFR before and after EK therapy in human. Also, the adverse events of EK therapy were similar with the results that Lee’s had reported, such as mild to moderate of abdominal pain which lasted within 1-2 days. All our prescriptions for HM treatments included Ma-huang and no severe adverse effect was reported in common with previous studies including dry mouth, constipation, diarrhea, palpitation and insomnia.
The importance of this study is assessing of anti-inflammation effect through various value in cellular level. In obese patients, a persistent, low-grade inflammation is triggered by ATM infiltration and its-derived cytokines, which disrupts the insulin signaling cascade like feedback loop [23]. We investigated the effects of EK on inflammation in this respect. EK therapy decreased the number of ATM in quantitative aspect, and also significantly improved adipose tissue inflammation in qualitative aspect. EK treatment significantly decreased of CD11C+ ATMs, named M1 ATMs, which stands for pro-inflammatory activity of ATMs in adipose tissue, and the same results were shown in analysis of blood Ly6c monocyte types. Lee also suggested that EK modulated ATMs and pro-inflammatory cytokines including TNF-α and IL-6 in the same manner with our results.
Ly6chi monocytes representing pro-inflammatory traits, are recruited to inflammation site by chemo-attractants and differentiates into macrophages or dendritic cells depending on the local cytokines [24]. Ly6clow monocytes are patrolling to differentiate into resident macrophages and promote wound healing [25]. In the obesity inflammation, Ly6chi and Ly6clow monocytes may differentiate into M1 and M2 macrophages [5,26]. As our expectation, Ly6chi of monocyte related pro-inflammation were decreased, while Ly6clow type of monocyte related anti-inflammation were increased by EK.
Alteration of gut microbiota and resultant modulation of intestinal permeability could be a key strategy to ameliorate obesity inflammation [7]. The most definite result in microbiota was the increasing of Verrucomicrobia in ob/ob group. Verrucomicrobia were counted 16.85 % in ob/ob group, however, the WT group and EK group showed only 0.00% and 2.59%. The relationship between Verrucomicrobia and obesity was reported that high-fat feeding induced the increasing of Verrucomicrobia and also the increasing ratio of Verrucomicrobia to Bacteroidetes [27]. Our study showed similar results as this previous study. The mean ratio of Verrucomicrobia to Bacteroidetes was significantly increased in ob/ob group, however, the ratio was decreased in EK group, demonstrating EK had effects on recovering harmful microbial transition.
In the analysis of Genus-level, Alistipes belonging to Bacteroidetes was significantly decreased in ob/ob group and recovered in EK group even higher than the WT group. Alistipes correlates negatively with leukocytes and present more abundantly in healthy subjects compared to non-alcoholic fatty liver disease patients mediated by inflammation [28,29]. Moreover, a human study confirmed that successful weight loss significantly enriched Alistipes [29]. Notably, the dominant phyla, Firmicutes was decreased in ob/ob group and increase in EK group contradicting to other results. Turnbaugh et al. [30] found an increase in the abundance of Firmicutes associated with diet induced obesity. These compositional changes were completely reversed after a return to a normal diet, which suggests that diet is the main contributing factor to obesity-associated changes in the gut microbiota [31]. In our study, the diets of all experimental groups were identical, the results of genetically obese and obese individuals with high-fat dietary habits were thought to be different for microorganisms. Indeed, the critical biomarker of obesity is uncertain among Firmicutes, Bacteroidetes, Firmicutes:Bacteroidetes ratio and other phyla, and remains to be determined [32].
Deferribacteres shown low proportion in both WT group and ob/ob group were obviously increased in EK group. In a study of diet-induced weight modification, Mucispirillum, the only genus of Deferribacteres was positively correlated with serum leptin levels [33], and also have several systems for scavenging reactive oxygen species induced by inflammation [34]. Interestingly, Mucispirillum were known not to be affected by the prebiotic treatment [35]. Therefore, EK could be a potent option to promote the growth of Mucispirillum finally leading to weight reduction.
We had several limitations. In our pragmatic real-world clinical study, a disparity in the number of follow-up bioelectrical impedance analysis (BIA) results limited sufficient analyses in body composition changes such as fat, muscle, and body fluid, and attributed to the data imbalance between the EK and HM groups. Also, the fidelity of the intervention was restricted due to the real-world conditions, lacking placebo or randomization. Second, the compliance of HM treatment and EK therapy was low compared to the other retrospective study with HM treatment [20]. Additionally, the final body weight was recorded at not the end-of-treatment but last-prescription-date during the study period. These approaches would have underestimated the potential weight loss effects associated with both HM treatment and EK therapy. Third, the number of each mice groups were too small to make a generalization human, and the additional studies should be needed with large number of animal and human study. However, our study had enough patients to be the first real-world clinical study although clinical trials with EK therapy were rare because of its toxicity. In past, the anti-inflammatory benefits of EK was studied focusing on various cancers and gastrointestinal tract associated diseases. However, this study was also the first research of EK in obesity and glucometabolism to investigate potent anti-inflammatory mechanism about macrophages and Ly6c monocytes, suggesting a positive role in host energy metabolism by the transition of microbiota.
4. Materials and Methods
4.1. A Real-World Clinical Study
4.1.1. Study Design and Eligible Patients
This study was an open-label, pragmatic cohort study encompassing outpatients who visited the Weight Management Center in Kyunghee University Korean Medicine Hospital (Seoul, South Korea) to treat obesity between January 1, 2022, and December 31, 2022. Eligible patients were included according to the following criteria:
(1) Men and women aged 15 years or older with BMI over 25.
(2) Among the patients who visited the hospital for weight loss, those who decided to receive HM treatment.
(3) Patients who visited the hospital at least twice to confirm the change of body weight.
The patients who denied to take HM for weight loss or could not be checked the follow-up body weight were excluded. All eligible patients underwent HM treatment, of which the contents of the prescription were different from each patient. At the first visit, all patients measured their body weight and performed BIA using InBody720 (InBody Inc., Seoul, Korea) and were recommended not to take any other medicines or supplements for weight loss during HM treatment period. We divided patients into two groups according to whether EK therapy was performed: the EK group who underwent EK therapy at least once plus conventional HM, and the HM group who were prescribed only conventional HM without EK therapy. We compared the changes of body weight and other body compositions before and after HM treatment between the EK group and HM group.
This real-world clinical study was approved its protocol by Kyung Hee University Korean Medicine Hospital Institutional Review Board (KOMCIRB 2023-07-001) and the written informed consent was obtained from all participants.
4.1.2. EK Therapy and HM Treatment
EK was provided from the Department of Pharmaceutical preparation of Kyunghee University Korean Medicine Hospital. EK capsule contains 400 mg of EK powder. EK therapy is performed as a 1-day course at home. Patients were prescribed 8 to 12 EK capsules at a single time, taking 4-5 capsules every 2 -minutes on an empty stomach. After 1-2 hours, multiple episodes of diarrhea and vomiting would occur over a period of 6-8 hours along with abdominal pain or nausea. We notified in advance that 1) severe abdominal pain could be relaxed with a hot pack or antispasmodics, and 2) dehydration might occur after more than 10 times of diarrhea and a can of soft drink could be helpful. All participants were prescribed HM which was Gami-Samhwang-san (Ephedra Herba, Armeniacae Semen, Acori Gramineri Rhizoma, Raphani Semen, Coicis Semen, Phellodendri Cortex, Atractylodes Chinensis Rhizome, Rhei Radix et Rhizoma), and TKM clinical doctors at Weight Management Center in Kyunghee University Korean Medicine Hospital modulated the prescriptions according to health problems of each patient.
4.1.3. Lifestyle Modification
On the first visit, all patients were counseled on correcting their lifestyle based on a common diet and exercise regimen. Our center highlighted to take regular 2 or 3 meals in a day, avoid fruits and confections including sweet drinks and sauces, and walk for an hour, 1-2 times a week until sweating.
4.2. Animal Study
4.2.1. Study Design, Animal and EK Preparation
The experimental animals were wild-type male C57BL/6 mice (WT group, n=5) and obese male C57BL/6-Lepob/ Lepob (ob/ob) mice (Central Lab Animals Inc., Korea). The ob/ob mice were randomly assigned into two groups: the ob/ob group (n=5) and the EK group (n=5). The EK group had treated with EK powder (200 mg/kg) was orally administered twice a week for 8 weeks, while the WT and ob/ob groups took normal saline. EK was purchased from the Department of Pharmaceutical Preparation of Kyunghee University Korean Medicine Hospital (Seoul, South Korea). All experiments were carried out in accordance with guidelines from the Korean National Institute of Health Animal Facility.
4.2.2. Weight Measurements and Blood Analysis
Body weights were recorded at the beginning and end of the experiment using CAS 2.5D scale (Seoul, Korea) in the morning. The weights of epididymal fat pads were measured at 8 weeks after scarification. To evaluate glucose metabolism, we examined FBG at 2, 4, and 8 weeks using ACCU-CHECK Performa (Australia) and performed OGTT at 6 weeks after glucose (2 g/kg body weight) feeding. Also, FSI was analyzed at 8 weeks using ELISA reader by 450 nM, and HOMA-IR was calculated using FBG and FSI. We analyzed the lipid profiles, including total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), TG, and NEFA, as well as the safety profile, including AST, ALT, and creatinine levels, using blood samples collected from heart at 8 weeks.
4.2.3. Analysis of ATMs and Monocytes
Stromal vascular cell (SVC) were segregated from the epi fat samples at the end of the study. The fat samples were soaked in the solution of phosphate buffered saline (PBS) and 2% bovine serum albumin (BSA), and isolated by collagenase (Sigma, USA) and DNase Ⅰ (Roche, USA). The cell number of SVC was counted by cellometer (Nexcelom Bioscience LLC, USA). To prepare before fluorescence activated cell sorting (FACS) analysis, FcBlock (BD Pharmingen, USA) was mixed at the ratio of 1:100, and the fluorephore-conjugated antibodies were added to react with the samples as follows; CD45-PerCP-Cy5.5 (Biolgend, USA), CD68-APC (Biolgend, USA), CD11c-phycoerythrin (Biolgend, USA), CD206-FITC (Biolgend, USA), CD11b-PE (Biolgend, USA), Ly6c-APC. All samples were put into FACS tubes after washing with 2% FBS/PBS solution, and analyzed by FACS Caliber (BD bioscience, USA) and FlowJo (Tree star inc., USA); the percentage of macrophages with CD45+/CD68+, CD45+/CD68+/CD206+ and CD45+/CD68+/CD11c+, and that of monocytes with CD45+/CD11b+/Ly6c-, CD45+/CD11b+/Ly6c+ and CD45+/CD11b+/Ly6c++.
4.2.4. Analysis of the Composition of the Fecal Microbiota
At 8 weeks, the fecal samples were collected, and their DNA were extracted following amplifying by polymerase chain reaction (PCR). The Basic Local Alignment Search Tool (BLAST) found regions of local similarity between sequences to analyze taxonomic composition for each sample from Phylum to Species level. In diversity analysis, we used Simpson’s diversity index to calculate alpha diversity. PCoA and UPGMA Clustering tree were used to assess the variation
4.3. Statistical Analysis
The continuous variables were reported the clinical study using the mean and standard deviation (SD), presented as mean ± SD, and the animal study using the mean and standard error of the mean (SEM), presented as mean ± SEM. We compared the continuous variables between EK group and the other group using Mann-Whitney U test, only for baseline age and height using student t-test. Linear regression was performed to estimate the size of the weight loss effect according to the HM treatment period. We conducted an analysis of variance (ANOVA) and a Tukey’s post-hoc to compare the weight loss outcomes across the numbers of EK therapy sessions in clinical study, and to analyze group differences in animal study. The change of body weight before and after obesity treatment was analyzed by Wilcoxon signed rank test. We also used student t-test to check if a final weight loss was different between different subgroups of gender and behavioral factor. All statistical analyses were performed using PRISM 7 (Graphpad software Inc., La Jolla, CA). All p values were two-tailed and significance was set at p < 0.05.
5. Conclusions
We can infer effect of Euphorbia kansui treatment grounds of the results related to anti-inflammation and alteration of microbial community composition. These different types of microorganisms might be linked to change in nutrient absorption and energy regulation. Additionally, we can also assert that leading changes in adipose tissue macrophage and blood Ly6chi monocytes level by Euphorbia kansui treatment can reduce systemic inflammation activity and finally impact on insulin-signaling network.
Author Contributions
Conceptulation and methodology, J.-W. N. and B.-C. L.; investigation, data curation and writing-original draft preparation, J.-W. N. and J.-H. Y.; writing-review and editing, J.-W. N. and B.-C. L.; funding acquisition and project administration, B.-C. L. All the authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Korea health Technology R & D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HFD20C0022).
Institutional Review Board Statement
The human study was approved its protocol by Kyung Hee University Korean Medicine Hospital Institutional Review Board (KOMCIRB 2023-07-001) and conducted in accordance with the guidelines of the Declaration of Helsinki. The animal study was approved by the Animal Care Committee at Kyunghee University (KHMC-IACUC 2016-032) and we checked the ARRIVE guidelines.
Informed Consent Statement
Written informed consent was obtained from all participants.
Data Availability Statement
The data are from the corresponding author upon reasonable request.
Conflicts of Interest
The authors have no conflicts of interest.
References
- Wyatt, H.R. Update on treatment strategies for obesity. J Clin Endocrinol Metab 2013, 98, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Tham, K.W.; Abdul Ghani, R.; Cua, S.C.; Deerochanawong, C.; Fojas, M.; Hocking, S.; Lee, J.; Nam, T.Q.; Pathan, F.; Saboo, B.; et al. Obesity in South and Southeast Asia-A new consensus on care and management. Obes Rev 2023, 24, e13520. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y. ; NakayamaO. ; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J Clin Invest 2004, 114, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Qiu, T.; Li, L.; Yu, R.; Chen, X.; Li, C.; Proud, C.G.; Jiang, T. Pathophysiology of obesity and its associated diseases. Acta Pharm Sin B 2023, 13, 2403–2424. [Google Scholar] [CrossRef] [PubMed]
- Russo, L.; Lumeng, C.N. Properties and functions of adipose tissue macrophages in obesity. Immunology 2018, 155, 407–417. [Google Scholar] [CrossRef]
- Li, Y.H.; Zhang, Y.; Pan, G.; Xiang, L.X.; Luo, D.C.; Shao, J.Z. Occurrences and Functions of Ly6C(hi) and Ly6C(lo) Macrophages in Health and Disease. Front Immunol 2022, 13, 901672. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.J.; West, N.P.; Cripps, A.W. Obesity, inflammation, and the gut microbiota. Lancet Diabetes Endocrinol 2015, 3, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Aron-Wisnewsky, J.; Warmbrunn, M.V.; Nieuwdorp, M.; Clement, K. Metabolism and Metabolic Disorders and the Microbiome: The Intestinal Microbiota Associated With Obesity, Lipid Metabolism, and Metabolic Health-Pathophysiology and Therapeutic Strategies. Gastroenterology 2021, 160, 573–599. [Google Scholar] [CrossRef] [PubMed]
- Tong, G.D.; Zhou, D.Q.; He, J.S.; Zhang, L.; Chen, Z.F.; Xiao, C.L.; Peng, L.S. Clinical research on navel application of Shehuang Paste combined with Chinese herbal colon dialysis in treatment of refractory cirrhotic ascites complicated with azotemia. World J Gastroenterol 2006, 12, 7798–7804. [Google Scholar] [CrossRef]
- Shen, J.; Wang, J.; Shang, E.X.; Tang, Y.P.; Kai, J.; Cao, Y.J.; Zhou, G.S.; Tao, W.W.; Kang, A.; Su, S.L.; et al. The dosage-toxicity-efficacy relationship of kansui and licorice in malignant pleural effusion rats based on factor analysis. J Ethnopharmacol 2016, 186, 251–256. [Google Scholar] [CrossRef]
- Li, H.; Lei, F.; Wang, Y.; Xiao, X.; Hu, J.; Cheng, X.; Xing, D.; Hua, L.; Lin, R.; Du, L. [Effect of Euphorbia kansui on urination and kidney AQP2, IL-1beta and TNF-alpha mRNA expression of mice injected with normal saline]. Zhongguo Zhong Yao Za Zhi 2012, 37, 606–610. [Google Scholar] [PubMed]
- Feng, X.; Li, J.; Li, H.; Chen, X.; Liu, D.; Li, R. Bioactive C21 Steroidal Glycosides from Euphorbia kansui Promoted HepG2 Cell Apoptosis via the Degradation of ATP1A1 and Inhibited Macrophage Polarization under Co-Cultivation. Molecules 2023, 28. [Google Scholar] [CrossRef]
- Hou, J.J.; Shen, Y.; Yang, Z.; Fang, L.; Cai, L.Y.; Yao, S.; Long, H.L.; Wu, W.Y.; Guo, D.A. Anti-proliferation activity of terpenoids isolated from Euphorbia kansui in human cancer cells and their structure-activity relationship. Chin J Nat Med 2017, 15, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Jang, Y.W.; Hyung, K.E.; Lee, D.K.; Hyun, K.H.; Park, S.Y.; Park, E.S.; Hwang, K.W. Therapeutic Effects of Methanol Extract from Euphorbia kansui Radix on Imiquimod-Induced Psoriasis. J Immunol Res 2017, 2017, 7052560. [Google Scholar] [CrossRef]
- Van Sickle, M.D.; Duncan, M.; Kingsley, P.J.; Mouihate, A.; Urbani, P.; Mackie, K.; Stella, N.; Makriyannis, A.; Piomelli, D.; Davison, J.S.; et al. Identification and functional characterization of brainstem cannabinoid CB2 receptors. Science 2005, 310, 329–332. [Google Scholar] [CrossRef]
- Guo, J.; Zhou, L.Y.; He, H.P.; Leng, Y.; Yang, Z.; Hao, X.J. Inhibition of 11b-HSD1 by tetracyclic triterpenoids from Euphorbia kansui. Molecules 2012, 17, 11826–11838. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, E.Y. The effect of Hyungbangdojucksan-Gami and Kamsuchunilhwan on the obesity in the rats. J. Sasang Constitutional Medicine 2000, 12, 184–194. [Google Scholar] [CrossRef]
- Lee, S.W.; Na, H.Y.; Seol, M.H.; Kim, M.; Lee, B.C. Euphorbia kansui Attenuates Insulin Resistance in Obese Human Subjects and High-Fat Diet-Induced Obese Mice. Evid Based Complement Alternat Med 2017, 2017, 9058956. [Google Scholar] [CrossRef] [PubMed]
- Uneda, K.; Kawai, Y.; Yamada, T.; Kaneko, A.; Saito, R.; Chen, L.; Ishigami, T.; Namiki, T.; Mitsuma, T. Japanese traditional Kampo medicine bofutsushosan improves body mass index in participants with obesity: A systematic review and meta-analysis. PLoS One 2022, 17, e0266917. [Google Scholar] [CrossRef] [PubMed]
- Jo, D.H.; Lee, S.; Lee, J.D. Effects of Gambisan in overweight adults and adults with obesity: A retrospective chart review. Medicine (Baltimore) 2019, 98, e18060. [Google Scholar] [CrossRef]
- Reum Lee, D.-Y.L. , Min-Ji Kim, Hyang-Sook Lee, Ka-Hye Choi, Seo-Young Kim, Young-Woo Lim, Young-Bae Park. Gamitaeeumjowee-Tang for weight loss in diabetic patients: A retrospective chart review. Journal of Korean Medicine 2021, 42, 46–58. [Google Scholar] [CrossRef]
- Su-Min, R.S.-H.J. , Jong-Soo Lee, Sung-Soo Kim, Hyun-Dae Shin. The Effect of Very Low Calorie Diet and Chegamuiyiin-tang on Bone Mineral Density. Journal of Korean Medicine for Obesity Research 2005, 5, 87–95. [Google Scholar]
- McArdle, M.A.; Finucane, O.M.; Connaughton, R.M.; McMorrow, A.M.; Roche, H.M. Mechanisms of obesity-induced inflammation and insulin resistance: insights into the emerging role of nutritional strategies. Front Endocrinol (Lausanne) 2013, 4, 52. [Google Scholar] [CrossRef]
- Kratofil, R.M.; Kubes, P.; Deniset, J.F. Monocyte Conversion During Inflammation and Injury. Arterioscler Thromb Vasc Biol 2017, 37, 35–42. [Google Scholar] [CrossRef]
- Auffray, C.; Fogg, D.; Garfa, M.; Elain, G.; Join-Lambert, O.; Kayal, S.; Sarnacki, S.; Cumano, A.; Lauvau, G.; Geissmann, F. Monitoring of blood vessels and tissues by a population of monocytes with patrolling behavior. Science 2007, 317, 666–670. [Google Scholar] [CrossRef]
- Shi, C.; Pamer, E.G. Monocyte recruitment during infection and inflammation. Nat Rev Immunol 2011, 11, 762–774. [Google Scholar] [CrossRef]
- Li, X.; Guo, J.; Ji, K.; Zhang, P. Bamboo shoot fiber prevents obesity in mice by modulating the gut microbiota. Sci Rep 2016, 6, 32953. [Google Scholar] [CrossRef]
- Jiang, W.; Wu, N.; Wang, X.; Chi, Y.; Zhang, Y.; Qiu, X.; Hu, Y.; Li, J.; Liu, Y. Dysbiosis gut microbiota associated with inflammation and impaired mucosal immune function in intestine of humans with non-alcoholic fatty liver disease. Sci Rep 2015, 5, 8096. [Google Scholar] [CrossRef]
- Louis, S.; Tappu, R.M.; Damms-Machado, A.; Huson, D.H.; Bischoff, S.C. Characterization of the Gut Microbial Community of Obese Patients Following a Weight-Loss Intervention Using Whole Metagenome Shotgun Sequencing. PLoS One 2016, 11, e0149564. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Ley, R.E.; Mahowald, M.A.; Magrini, V.; Mardis, E.R.; Gordon, J.I. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444, 1027–1031. [Google Scholar] [CrossRef]
- Boulange, C.L.; Neves, A.L.; Chilloux, J.; Nicholson, J.K.; Dumas, M.E. Impact of the gut microbiota on inflammation, obesity, and metabolic disease. Genome Med 2016, 8, 42. [Google Scholar] [CrossRef] [PubMed]
- Murphy, E.F.; Cotter, P.D.; Healy, S.; Marques, T.M.; O’Sullivan, O.; Fouhy, F.; Clarke, S.F.; O’Toole, P.W.; Quigley, E.M.; Stanton, C.; et al. Composition and energy harvesting capacity of the gut microbiota: relationship to diet, obesity and time in mouse models. Gut 2010, 59, 1635–1642. [Google Scholar] [CrossRef] [PubMed]
- Ravussin, Y.; Koren, O.; Spor, A.; LeDuc, C.; Gutman, R.; Stombaugh, J.; Knight, R.; Ley, R.E.; Leibel, R.L. Responses of gut microbiota to diet composition and weight loss in lean and obese mice. Obesity (Silver Spring) 2012, 20, 738–747. [Google Scholar] [CrossRef]
- Loy, A.; Pfann, C.; Steinberger, M.; Hanson, B.; Herp, S.; Brugiroux, S.; Gomes Neto, J.C.; Boekschoten, M.V.; Schwab, C.; Urich, T.; et al. Lifestyle and Horizontal Gene Transfer-Mediated Evolution of Mucispirillum schaedleri, a Core Member of the Murine Gut Microbiota. mSystems 2017, 2. [Google Scholar] [CrossRef] [PubMed]
- Everard, A.; Lazarevic, V.; Gaia, N.; Johansson, M.; Stahlman, M.; Backhed, F.; Delzenne, N.M.; Schrenzel, J.; Francois, P.; Cani, P.D. Microbiome of prebiotic-treated mice reveals novel targets involved in host response during obesity. ISME J 2014, 8, 2116–2130. [Google Scholar] [CrossRef]
Figure 1.
The flow chart of clinical study.
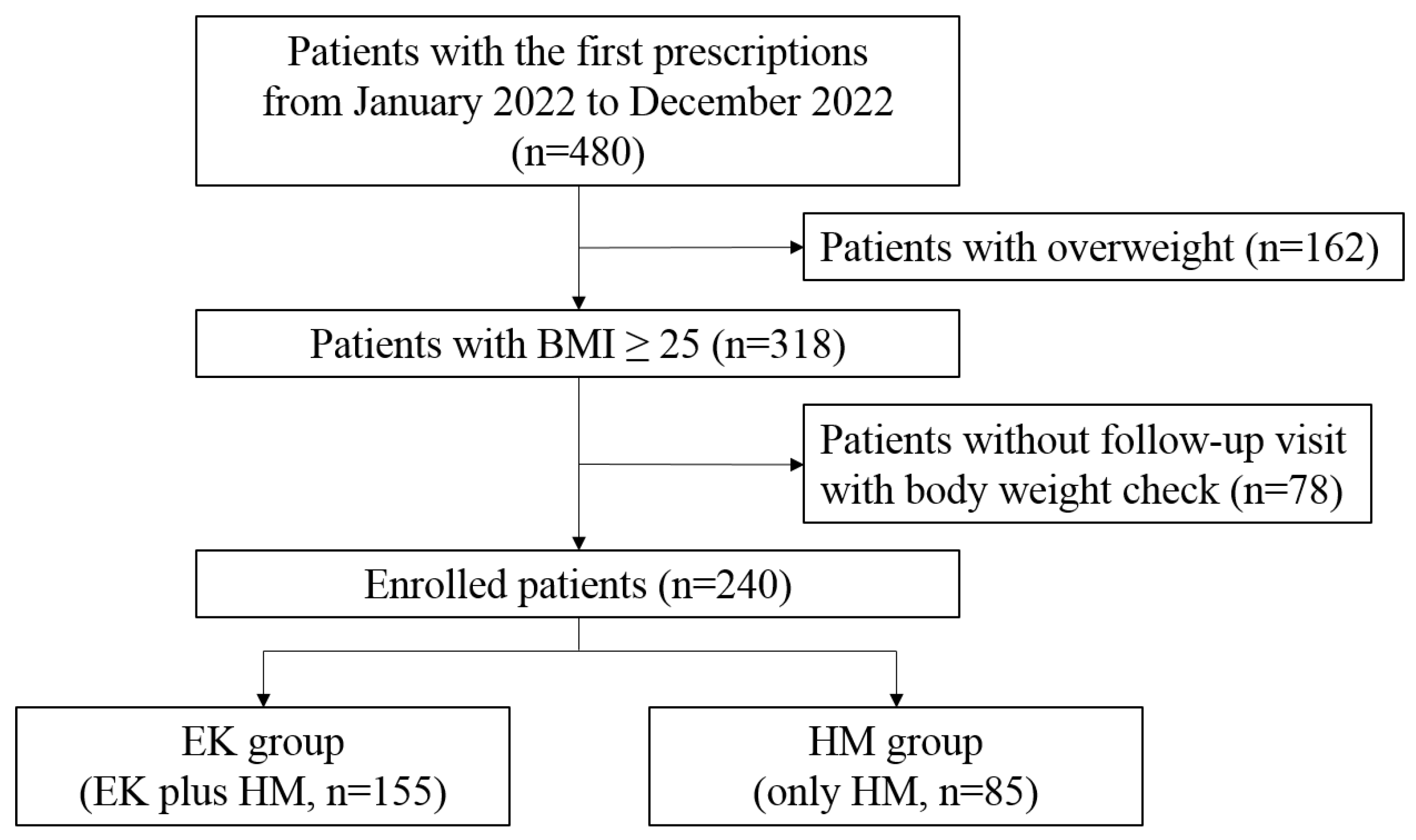
Figure 2.
Anti-obesity outcomes of EK therapy and HM treatment. Change in body weight by (a) percentage and (b) kg, and (c) BMI from baseline to the final visit. (d) Mean changes from baseline in bodyweight. (e) Proportions of participants achieving body weight reductions of at least 5, 10 and 15%. (f) Mean body weight changes according to the trial number of EK therapy throughout the treatment period. *p<0.05; ** p<0.01; ***p<0.001 versus HM group. §§§p<0.001, versus the EK once group BMI, body mass index.
Figure 2.
Anti-obesity outcomes of EK therapy and HM treatment. Change in body weight by (a) percentage and (b) kg, and (c) BMI from baseline to the final visit. (d) Mean changes from baseline in bodyweight. (e) Proportions of participants achieving body weight reductions of at least 5, 10 and 15%. (f) Mean body weight changes according to the trial number of EK therapy throughout the treatment period. *p<0.05; ** p<0.01; ***p<0.001 versus HM group. §§§p<0.001, versus the EK once group BMI, body mass index.
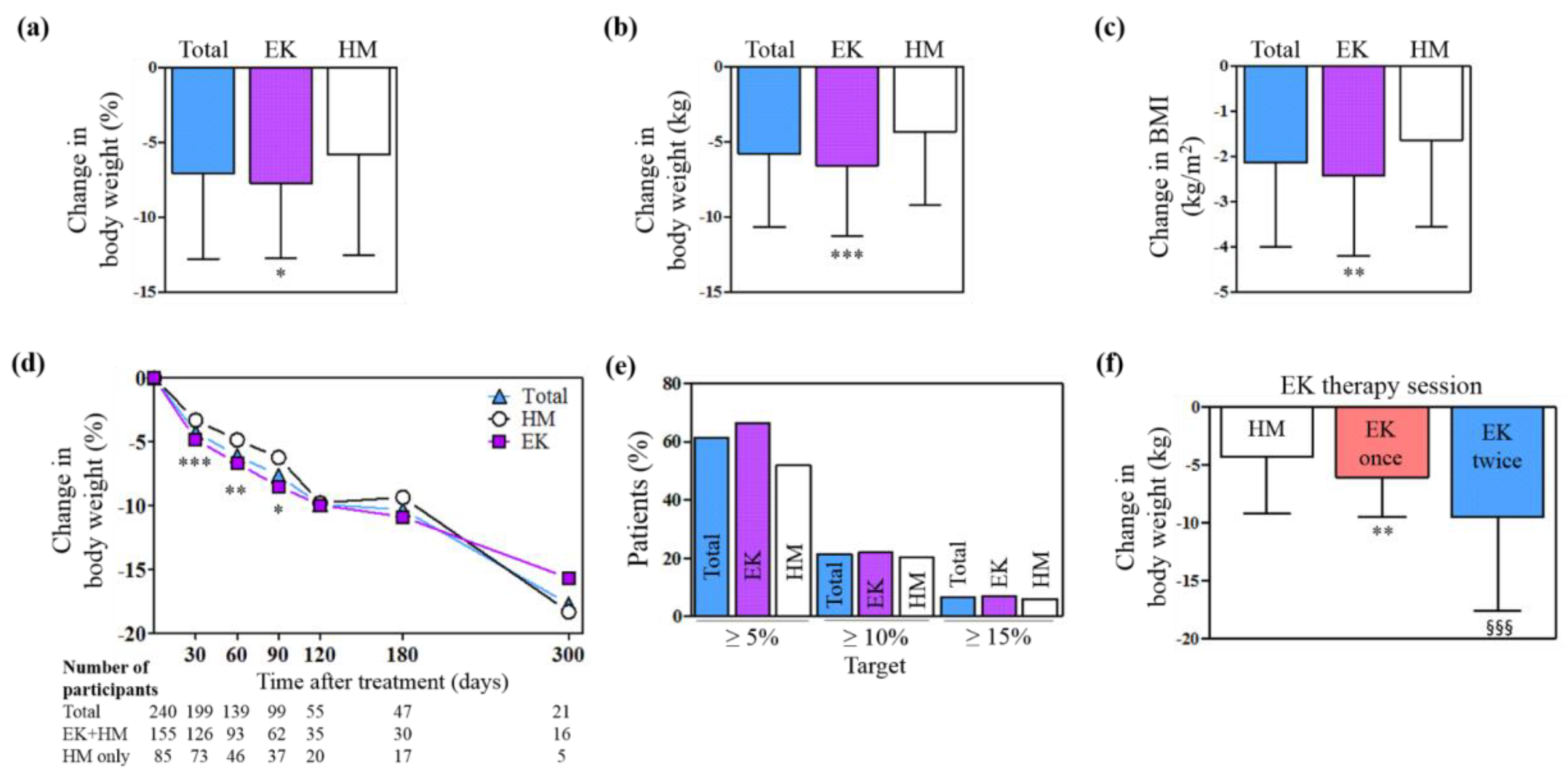
Figure 3.
Change in (a) fat weight, (b) muscle weight, and (d) body fluid. (c) Subgroup analysis divided by the number of EK therapy trials. **p<0.01 versus the HM group.
Figure 3.
Change in (a) fat weight, (b) muscle weight, and (d) body fluid. (c) Subgroup analysis divided by the number of EK therapy trials. **p<0.01 versus the HM group.
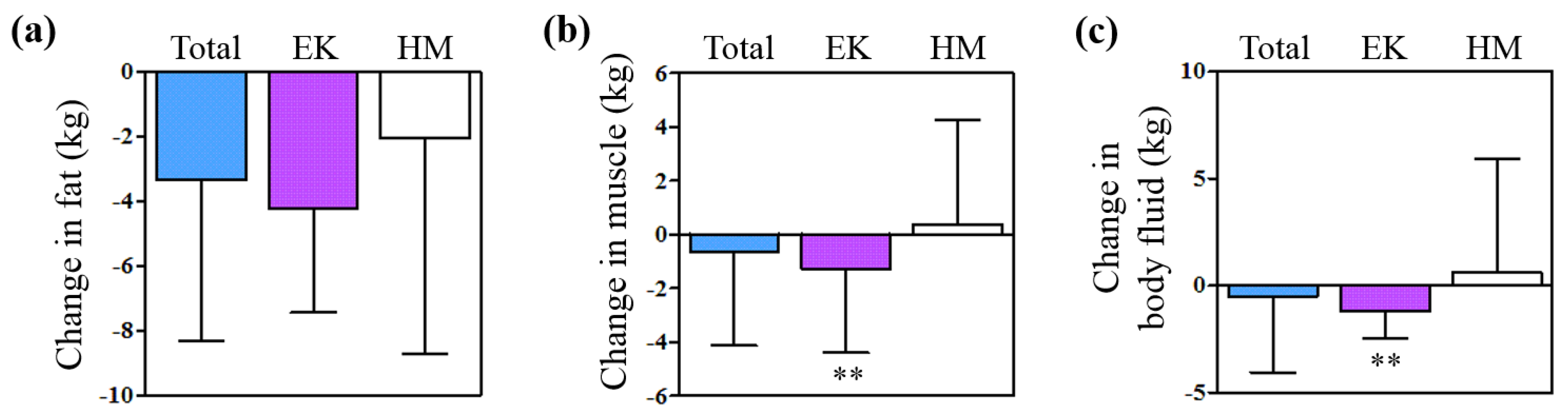
Figure 4.
Metabolic benefits of Euphorbia kansui in the animal study. Comparison between three groups in (a) FBG, (b) HOMA-IR, (c) oral glucose tolerance tests (OGTT) results, (d) AUC of OGTT, (e) NEFA and (f) cholesterols. *p<0.05; ***p<0.01, versus the ob/ob group. §§p<0.01; §§§p<0.001, versus the WT group. FBG, fasting blood glucose; HOMA-IR, homeostatic model assessment for insulin resistance; AUC, area under the curve; NEFA, non-esterified fatty acids; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides.
Figure 4.
Metabolic benefits of Euphorbia kansui in the animal study. Comparison between three groups in (a) FBG, (b) HOMA-IR, (c) oral glucose tolerance tests (OGTT) results, (d) AUC of OGTT, (e) NEFA and (f) cholesterols. *p<0.05; ***p<0.01, versus the ob/ob group. §§p<0.01; §§§p<0.001, versus the WT group. FBG, fasting blood glucose; HOMA-IR, homeostatic model assessment for insulin resistance; AUC, area under the curve; NEFA, non-esterified fatty acids; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides.
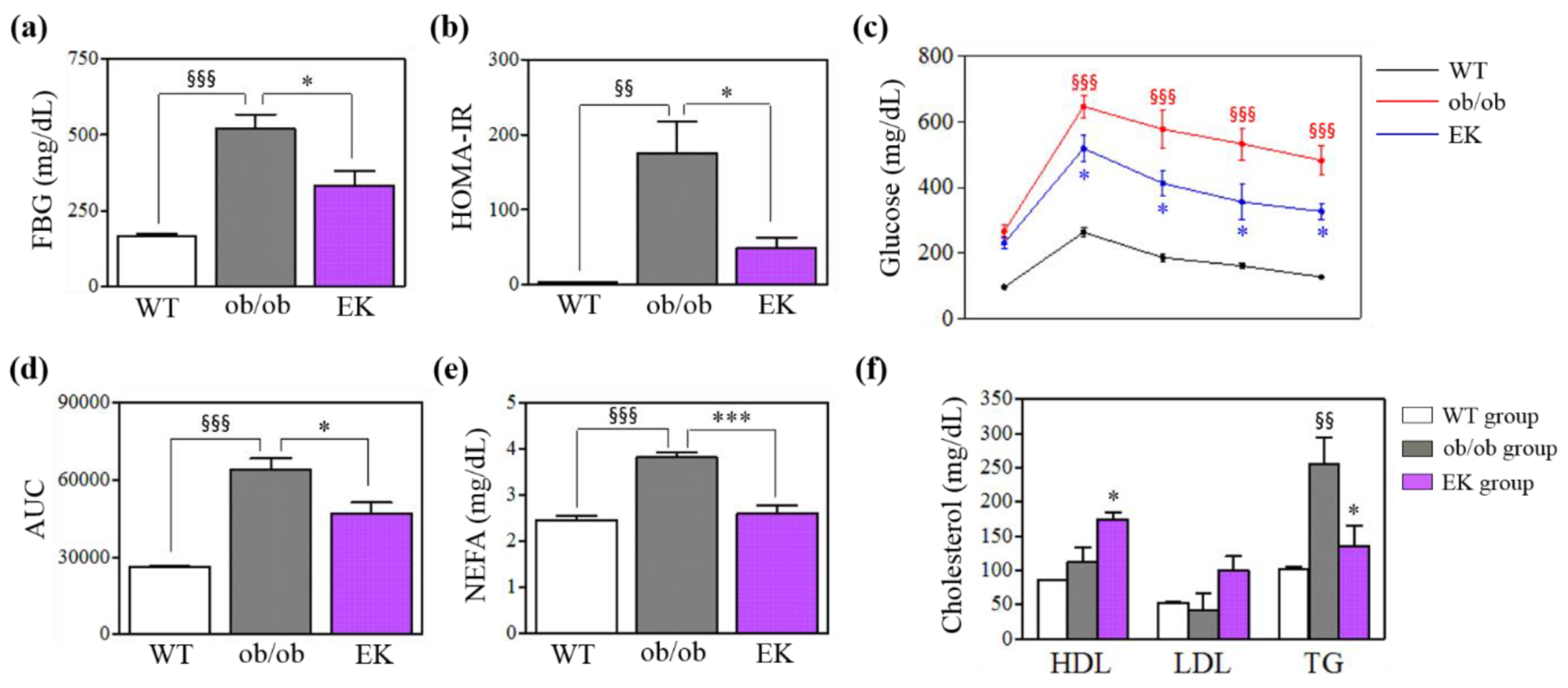
Figure 5.
Anti-inflammatory changes in adipose tissue macrophages. (a) Flow cytometry results showing adipose tissue macrophage gating. (b-f) Percentages of adipose tissue macrophages in total, CD11c+ and CD206+ subtypes. *p<0.05, versus the ob/ob group. §§p<0.01; §§§p<0.001, versus WT group.
Figure 5.
Anti-inflammatory changes in adipose tissue macrophages. (a) Flow cytometry results showing adipose tissue macrophage gating. (b-f) Percentages of adipose tissue macrophages in total, CD11c+ and CD206+ subtypes. *p<0.05, versus the ob/ob group. §§p<0.01; §§§p<0.001, versus WT group.

Figure 6.
Anti-inflammatory changes in monocytes. (a) Flow cytometry showing monocyte gating. (b-c) Populations of Ly6-, Ly6c+ and Ly6c++ monocytes. *p<0.05, versus the ob/ob group. §§p<0.01; §§§p<0.001, versus WT group.
Figure 6.
Anti-inflammatory changes in monocytes. (a) Flow cytometry showing monocyte gating. (b-c) Populations of Ly6-, Ly6c+ and Ly6c++ monocytes. *p<0.05, versus the ob/ob group. §§p<0.01; §§§p<0.001, versus WT group.

Figure 7.
The changes in gut microbiota structure and diversity. (a) Percentage of each phylum in the gut microbiota. (b) Diversity of gut microbiota. (c) Principal coordinate anlysis (PCoA) analysis of individuals and UPGMA clustering.
Figure 7.
The changes in gut microbiota structure and diversity. (a) Percentage of each phylum in the gut microbiota. (b) Diversity of gut microbiota. (c) Principal coordinate anlysis (PCoA) analysis of individuals and UPGMA clustering.
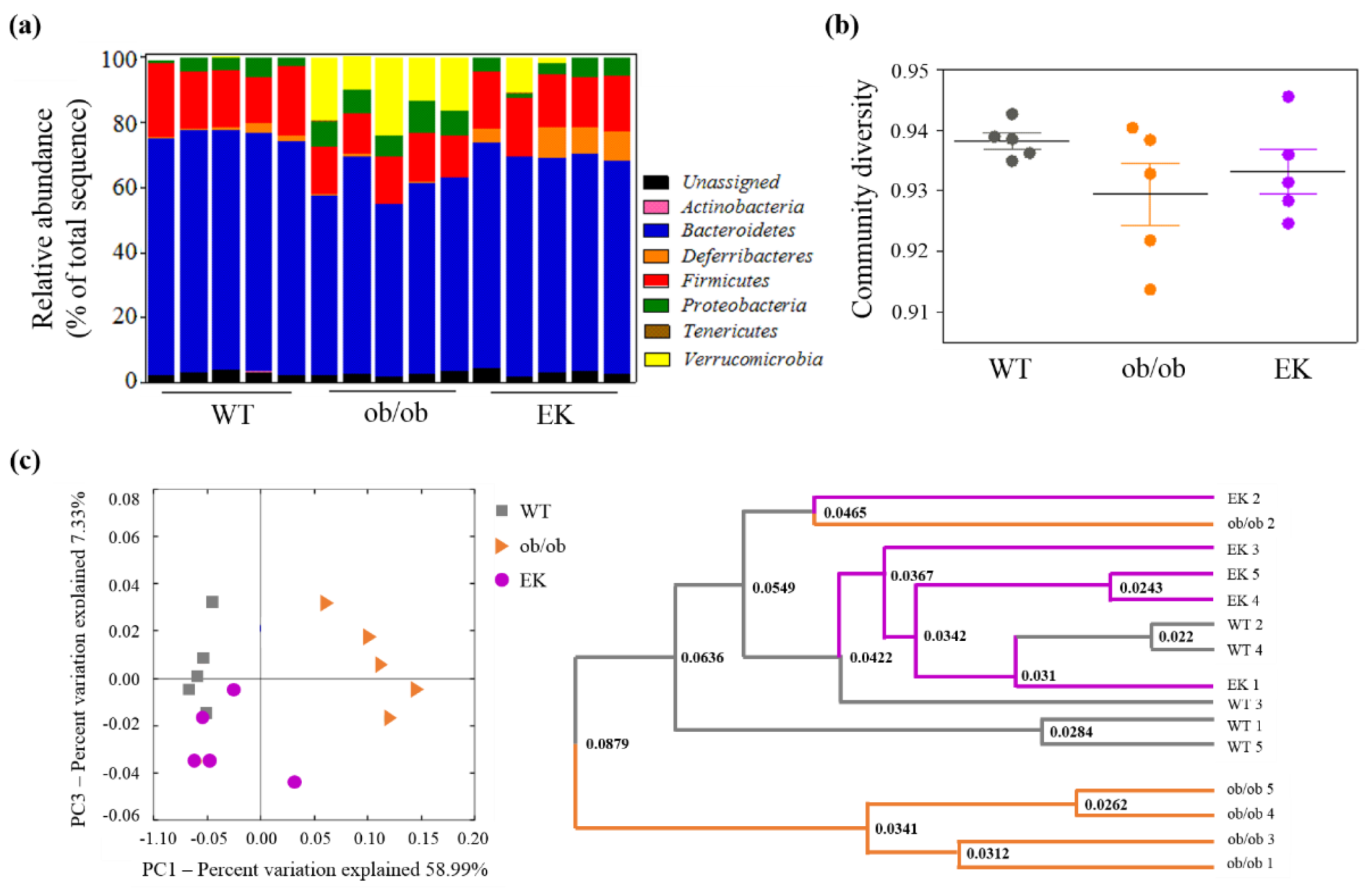

Table 1.
Baseline characteristics of enrolled patients.
| Variables | Total | EK group | HM group | P value |
| N | 240 | 155 | 85 | |
| Age (years) | 41.28 ± 12.17 | 41.75 ± 12.20 | 40.42 ± 12.14 | 0.442 |
| Male (%) | 29.58 | 34.19 | 21.18 | |
| Height (cm) | 164.6 ± 8.41 | 165.4 ± 8.78 | 163.3 ± 7.52 | 0.062 |
| Body weight (kg) | 81.25 ± 14.73 | 84.75 ± 15.38 | 74.88 ± 10.97 | <0.001 |
| BMI (kg/m2) | 29.84 ± 4.12 | 30.85 ± 4.34 | 28.01 ± 2.94 | <0.001 |
| Follow-up duration (days) | 91.55 ± 66.77 | 93.30 ± 70.43 | 88.36 ± 59.78 | 0.903 |
| Fat weight (kg) | 32.27 ± 15.75 | 33.93 ± 17.89 | 28.31 ± 7.49 | <0.001 |
| Muscle weight (kg) | 27.91 ± 6.41 | 28.81 ± 6.60 | 25.80 ± 5.42 | <0.001 |
| Body fluid (kg) | 36.95 ± 7.76 | 38.09 ± 7.96 | 34.26 ± 6.58 | <0.001 |
| Smokers (%) | 16.35 | 18.71 | 12.05 | |
| Non-drinkers (%) | 41.66 | 38.06 | 51.81 |
1 Patients in the EK group received EK and HM treatment. P values show the results from Mann-Whitney U test and student t-test between EK and HM groups. BMI: body mass index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



