
Submitted:
24 August 2025
Posted:
27 August 2025
You are already at the latest version
Abstract
Background and Objectives: This study aimed to identify radiographic predictors and opti-mal cut-off values for determining the need for additional pedicle subtraction osteotomy (PSO) in patients with iatrogenic flatback syndrome following short-segment (≤3 levels) fusion surgery. Materials and Methods: From 2011 to 2022, a total of 49 patients who un-derwent deformity correction for iatrogenic flatback following short-segment fusion at a single institution were included. We divided all patients into group A (n= 33, only ACR) and group B (n= 16, ACR combined with PSO). Among group A patients, we further di-vided them into two subgroups: The Excessive group, who developed excessive anterior disc height distraction (EADH) during surgery, and the Non-excessive group, who did not. The Receiver Operating Characteristic (ROC) curve was used to determine the cut-off val-ues for spinopelvic parameters associated with the decision to perform additional PSO. Results: Group A had a significantly lower number of previously fused segments com-pared to Group B (p < 0.001). Preoperative C7 sagittal vertical axis (C7SVA, p=0.026) and its correction (p=0.003) in group B were greater than those in group A. Group B showed a significantly more kyphotic preoperative fused segment angle (FSA) compared to Group A (p = 0.001). Postoperatively, EADH occurred in 7 patients (21.2%) in Group A, while no cases were observed in Group B. Subgroup analysis revealed that the dynamic segment angle (DA) was significantly lower in the Excessive group compared to the Non-excessive group (p 242.8mm, FSA > -3.2°, and DA < 4.3°. Conclusions: ACR alone and ACR combined with PSO showed satisfactory outcomes in patients with iatro-genic flat back. In particular, we highly recommend ACR combined with the PSO in pa-tients with preoperative C7SVA > 242.8 mm, FSA > -3.2°, or DA < 4.3°.
Keywords:
iatrogenic flatback
; deformity
; anterior column realignment
; pedicle subtraction osteotomy
; sagittal balance
1. Introduction
Th“Iatrogenic Flatback” commonly refers to a postoperative spinal deformity characterized by a reduction in lumbar lordosis (LL) following spinal fusion surgery, leading to sagittal imbalance and back pain [1,2]. When sagittal imbalance is mild, conservative treatment can be used to manage symptoms. However, as spinal deformity advances, compensatory mechanisms gradually diminish, eventually resulting in severe sagittal imbalance that necessitates reconstructive surgery [3]. In the early era of modern spinal instrumentation, iatrogenic loss of lumbar lordosis was commonly associated with the use of straight rods and distractive techniques, particularly when applied to distal segments, resulting in “fixed” iatrogenic flatback [4]. Previous studies have shown that pedicle subtraction osteotomy (PSO) yields acceptable radiographic correction and clinical outcomes in patients with “fixed” iatrogenic flatback [3,5,6]. Furthermore, the rate of major complications is comparable to that observed in primary adult spinal deformity surgeries [7].
Nowadays, the use of pedicle screws combined with interbody cages has been shown to be effective in restoring physiological lumbar lordosis in the surgical treatment of degenerative spondylolisthesis and spinal stenosis, regardless of the presence of instability. Nevertheless, achieving the desired degree of lordosis can be challenging when cage placement or rod contouring is suboptimal. Furthermore, loss of the initially corrected angle may occur over time due to complications such as pseudarthrosis or adjacent segment degeneration, which are more frequently observed in contemporary cases of iatrogenic flatback following short-segment fusion surgery [8,9,10]. In such cases, where some unfused segments remain in the lumbar region, referred to as 'flexible' iatrogenic flatback, anterior column realignment (ACR) is recommended due to its advantage in achieving harmonious alignment with fewer mechanical complications [11,12]. Nonetheless, in cases of severe sagittal imbalance or thoracolumbar kyphosis requiring substantial correction angles, additional PSO may be necessary [13].
However, there is still no consensus on the optimal surgical strategy for patients who develop iatrogenic flat back syndrome, especially, after short-segment fusion surgery. This study aimed to evaluate the effectiveness of ACR in treating iatrogenic flatback syndrome following short-segment lumbar fusion and to identify preoperative radiographic parameters and their optimal cut-off values for determining the need for additional PSO.
2. Materials and Methods
This study was a retrospective analysis of patients with iatrogenic flatback syndrome who underwent surgery to reconstruct spinal alignment at our single institution, performed by two experienced spine surgeons. We reviewed 158 patients who developed iatrogenic flatback syndrome after previous fusion surgery between March 2011 and May 2022. The inclusion criteria were: (1) patients who underwent long-level surgery (≥5 levels), (2) those who underwent ACR, and (3) a follow-up period of more than 2 year. The exclusion criteria were: (1) previous fusion level ≥ 4 levels, (2) underwent PSO without ACR or had a history of prior ACR, cervical, or lower extremity surgery (3) for patients with severe coronal imbalance (Cobb’s angle ≥ 40°), (4) patients with pathophysiological kyphosis, and (5) patients with improper or incomplete radiographs. Finally, we enrolled 49 patients who underwent deformity correction surgery for flatback syndrome that occurred after short-segment (≤ 3 levels) fusion surgery. These 49 patients were divided into two groups according to the surgical procedure: Group A (n = 33, only ACR) and Group B (n = 16, ACR combined with PSO). Among patients in Group A, an additional analysis was performed by dividing them into two subgroups: those who developed excessive distraction of anterior disc height during perioperative surgery (“Excessive group”) and those who did not (“Non-excessive group”).
2.1. Radiographic Evaluation
Preoperative and postoperative spinopelvic parameters were measured on standing lateral radiographs. These parameters included the sagittal vertical axis (SVA), thoracic kyphosis (TK), lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), lower lumbar lordosis (LLL), defined as the angle from the upper endplate of L4 to the upper endplate of S1, and Fused segment angle (FSA), which was defined as the angle between the superior endplate of the fused level and the inferior endplate of the fused level [14].
Flexion and extension lateral radiographs of the lumbar spine were used to assess lumbar flexibility and adjacent segment mobility. Dynamic lumbar lordosis (DL) was defined as the difference in the lumbar lordosis angle between flexion and extension. Dynamic segment angulation (DA) was defined as the change in adjacent segment angulation between flexion and extension [15].
2.2. Clinical Evaluation and Complications
Patient-reported outcome measures (PROMs) were assessed preoperatively and at 6 months postoperatively using the Oswestry Disability Index (ODI) and the Visual Analogue Scale (VAS) of low back. Perioperative major complications and postoperative complications were recorded. In terms of postoperative complications. Excessive distraction of anterior disc height (EADH) was defined as the presence of an excessive anterior disc angle (>30°) between adjacent endplates, measured on postoperative standing lateral radiographs. (Figure 1).
2.3. Statistical Analysis
All statistical analyses were performed using SPSS (version 22, IBM SPSS Statistics). Student’s t-test was used to compare demographics, spinopelvic parameters, clinical outcomes, and complications between the two groups. Radiological spinopelvic parameters, postoperative complications, and patient-reported outcomes were compared between the two groups. Paired t-tests were used to compare preoperative and postoperative data within each group. A p-value < 0.05 was considered statistically significant. The Receiver Operating Characteristic (ROC) curve was used to determine the cut-off values for spinopelvic parameters associated with the decision to perform PSO
3. Results
3.1. Demographic and Surgical Data
The patients enrolled in our study had an average age of 72.6 ± 6.6 in group A and 67.1±6.8 in group B; both groups didn’t have significant differences (p=0.420). In demographic and surgical data, in terms of body mass index (BMI), follow-up duration, instrumented level, or posterior lumbar interbody fusion (PLIF) segment, there was a no significant difference (p>0.05). Group A had fewer previous fusion levels than Group B (1.1 ± 0.2 vs. 2.2 ± 0.8, p < 0.001). The operation time in Group A was also significantly shorter than that in Group B (404.9 ± 91.4 minutes vs. 506 ± 154.8 minutes, p = 0.032). In contrast, the number of ACR levels didn’t have a statistically significant difference (2.5 ± 0.6 vs 1.9 ± 0.9, p= 0.530), however, the estimated blood loss (EBL) in group B was slightly higher than in group A. Still, it didn’t have a statistically significant difference (1845ml ± 929.9 vs 2260 ± 1447.8ml, p= 0.348). In Group B, the proportion of PSO level was located at L3 (n = 9, 56.3%) and L4 (n = 7, 43.7%) (Table 1).
3.2. Radiographic Parameters
When comparing radiographic parameters between the two groups (Table 2). Preoperatively, Group B showed a significantly greater C7-SVA compared to Group A (293.8 ± 90.3 mm vs. 219.8 ± 76.4 mm, p = 0.026). Although the postoperative C7-SVA did not differ significantly between groups (30.7 ± 45.5 mm vs. 61.7 ± 66.1 mm, p = 0.195), the correction was significantly larger in Group B (263.0 ± 79.9 mm vs. 157.9 ± 84.9 mm, p = 0.003). There were no statistically significant differences in TK, LL, LLL, T1PA, SS, PT, PI, or PI–LL mismatch in the two groups (p>0.05). Notably, FSA showed significant differences between groups in both preoperative and postoperative parameters. Group B demonstrated a significantly less lordotic (more kyphotic) preoperative FSA (5.1 ± 8.0° vs. −7.2 ± 7.5°, p = 0.001), a more lordotic postoperative FSA (−26.6 ± 12.6° vs. −7.8 ± 7.8°, p < 0.001), and a significantly greater correction angle (−31.6 ± 8.9° vs. −0.6 ± 2.3°, p < 0.001) compared to Group A.
3.3. Clinical Outcomes and Complications
Both groups showed significant postoperative improvements in the VAS score of low back and ODI after 6 months (p < 0.05), and there were no significant differences between the groups preoperatively or postoperatively (p > 0.05) (Table 3).
The incidence of perioperative and postoperative complications is presented in Table 4. Perioperative motor deficit occurred in 1 patient in Group A and in 2 patients in Group B (6.1% vs 12.5%, p= 0.440). All patients recovered within one year after the operation. Interestingly, seven patients (21.2%) in Group A experienced EADH perioperatively, whereas no patients in Group B did so (p=0.047). There was no statistically significant difference in postoperative complications between the two groups, and no revision surgery was required.
3.4. Preoperative Radiographic Parameters Depend on Complication
Based on the EADH complication identified in Group A, we performed an additional analysis of preoperative spinopelvic parameters, lumbar flexibility, and adjacent segment motion between the Excessive and Non-excessive groups (Table 5). Regarding adjacent segment motion, DA was significantly smaller in the Excessive group than in the Non-excessive group (2.8 ± 1.1° vs. 9.1 ± 3.5°, p < 0.001). Preoperative LL in the Excessive group was 11.3 ± 13.6°, indicating a more kyphotic angle than the 4.1 ± 7.4° observed in the Non-excessive group, although this difference was not statistically significant (p = 0.054). Other preoperative radiographic parameters didn’t differ significantly between the two groups.
3.5. Receiver Operating Characteristic Curves Determining Optimal Cut-Off Values of Spinopelvic Parameters
The optimal cut-off values of the preoperative radiographic parameters for selecting PSO were C7-SVA > 242.8 mm (95% CI 0.72-0.99), FSA > -3.2° (95% CI 0.55-0.95), and DA < 4.3° (95% CI 0.87-1.0), respectively. The AUC was 0.86 for C7SVA, 0.75 for FSA, and 0.96 for DA. At these thresholds, the sensitivity and specificity for C7SVA were 80.0% and 75.0%, FSA 70.0% and 70.0%, while those for DA were 84.6% and 95.8% (Figure 2).
4. Discussion
The surgical treatment of iatrogenic flatback is highly complex, as it involves revision surgery following a prior procedure. Given that the extent of correction plays a critical role in determining clinical outcomes (such as postoperative SVA and LL), meticulous preoperative surgical planning is essential. To date, ACR has been established as an effective technique for reconstructing spinal alignment in adult spinal deformity, offering a lower complication rate compared to pedicle subtraction osteotomy PSO [11,12]. This approach is particularly beneficial in cases of iatrogenic flatback, where previous posterior fusion surgery often results in significant scarring and adhesions around the dura and posterior elements [12]. These conditions necessitate complex dissections for adequate exposure, making PSO technically challenging at previously fused vertebral levels. Jason M. Frerich et al. [16] reported a case series demonstrating that performing ACR at the proximal segments in patients with iatrogenic flatback led to significantly improved radiographic spinopelvic alignment (postoperative C7-SVA: 61 ± 31 mm, LL: -40.6 ± 15.7°, and PI-LL: 12.8 ± 13.0°) and better clinical outcomes compared to those who underwent PSO. In our study, the group A, which included patients with a previous fusion of fewer than two levels, achieved significant improvements in spinopelvic parameters despite presenting severe spinal deformities (Figure 3a,b). Specifically, C7-SVA improved from 219.8 ± 76.4 mm preoperatively to 61.7 ± 66.1 mm postoperatively, LL increased from 9.6 ± 19.4° to -51.1 ± 10.2°, and the PI-LL mismatch decreased from 65.1 ± 19.1° to 7.2 ± 6.2°. These findings further support the effectiveness of ACR in restoring sagittal alignment in complex iatrogenic spinal deformities.
In our study, both groups showed severe preoperative C7-SVA, with Group A 219.8 ± 76.4 mm and Group B showing an even greater average of 293.8 ± 90.3 mm. These values are substantially higher than those reported in previous studies. For example, Munish et al. [7] analyzed 351 cases of iatrogenic flatback and reported an average SVA of 128.4 ± 70.6 mm, while Laine et al. [17] reported an average SVA of 121.6 ± 129.3 mm in a multicenter cohort of 273 patients with fixed sagittal imbalance. These earlier studies primarily focused on cases following long-level fusion, where the imbalance was mainly attributed to insufficient initial correction or subsequent loss of alignment over time. In contrast, our findings suggest that additional factors, such as progressive degenerative changes in the remaining flexible segments and the gradual decline in compensatory mechanisms, may contribute to the more pronounced sagittal malalignment observed in our cohort. These observations are consistent with those of Diebo et al. [10], who reported that segmental degenerative changes can induce compensatory alterations at adjacent levels, ultimately resulting in global sagittal imbalance. Moreover, as compensatory mechanisms deteriorate over time, particularly in elderly individuals, sagittal malalignment may become more severe despite relatively limited local deformity. It is further supported by the study by Cho et al. [18], which analyzed 34 elderly patients with degenerative sagittal imbalance and reported a mean SVA of 220.8 ± 78.3 mm. Their results highlighted that while degenerative imbalance may initially present as flexible, it tends to progressively stiffen, often leading to marked anterior deviation of the C7 plumb line exceeding 20 cm.
Although ACR is effective in many cases, to our knowledge, it may be insufficient to achieve the necessary angular correction for proper deformity reconstruction in patients with severe sagittal imbalance or fixed sagittal deformity. Therefore, additional PSO is required to achieve optimal sagittal realignment. This is demonstrated in previous studies [19,20], which recommend a hybrid ACR+PSO strategy for patients with severe fixed sagittal deformity because more benefit from superior lordotic correction and PI-LL correction, compared with the ACR-only group. This combined approach also offers biomechanical advantages, such as reducing the risk of rod fractures and hardware failure. However, a notable limitation of the previous study is the lack of a clear description regarding the specific indications for performing additional PSO. In current study, when the previous fusion segment extended beyond two levels and was associated with a more severe C7-SVA (293.8 ± 90.3 mm compared to Group A, p=0.026), we frequently performed an additional PSO. This approach was necessary due to the limited number of flexible segments available for ACR to sufficiently correct such severe spinal deformities. Although, postoperatively, the number of ACR levels between the two groups did not show a significant difference (2.5 ± 0.6 vs. 1.9 ± 0.9, p = 0.053). This was because, in Group B, ACR was frequently extended to the L1–L2 level, whereas in Group A, it was not. Performing ACR at this level presents technical challenges due to the subdiaphragmatic location of L1–L2, which is often obstructed by the 12th rib and diaphragm. These anatomical constraints can limit surgical exposure and hinder the placement of hyperlordotic cages [11]. Consequently, achieving sufficient segmental lordosis at L1–L2 was often difficult, necessitating the use of additional PSO to accomplish appropriate sagittal realignment [16]. As a result, Group B achieved a significantly greater correction in C7-SVA compared to Group A (263.0 ± 79.9 mm vs. 157.9 ± 84.9 mm, p = 0.003). Postoperatively, C7-SVA was reduced to 30.7 ± 45.5 mm in Group B and 61.7 ± 66.1 mm in Group A, although this difference did not reach statistical significance (p = 0.195). Further analysis using ROC curve identified a preoperative C7–SVA cut-off value of 242.8 mm as a significant predictor for the necessity of additional PSO. This finding suggests that patients with sagittal imbalance exceeding this threshold are unlikely to achieve sufficient realignment through ACR alone and may require more extensive corrective strategies, such as the addition of PSO, to effectively restore global sagittal alignment.
In addition to severe sagittal imbalance, PSO is also indicated for kyphotic spinal deformities, such as post-traumatic kyphosis. Wenhao Hu et al. [21], reported that PSO combined with interbody cage insertion resulted in favorable outcomes in patients with post-traumatic kyphosis. A substantial correction angle was achieved safely, as the procedure aids in restoring spinal column height and reducing the risk of spinal cord buckling or kinking. Despite short-segment fusion surgery, focal iatrogenic kyphosis remains a potential complication, often resulting from technical factors such as suboptimal cage positioning, inadequate rod contouring, or interbody cage subsidence. As reported by Diebo et al. [10], insufficient attention to segmental alignment and device placement may inadvertently induce kyphosis, particularly in levels with preserved disc height and preexisting lordosis. In such cases, PSO may be necessary as an additional corrective measure to restore sagittal alignment. In our cohort, patients in Group B who underwent additional PSO showed a significantly more kyphotic FSA compared to those in Group A who did not (5.1 ± 8.0° vs -7.2 ± 7.5°, p = 0.001), suggesting that segmental hypolordosis or kyphosis may serve as a key radiographic indicator for the necessity of PSO (Figure 3c,d). Further ROC curve analysis identified a preoperative FSA cut-off value of less than 3.2° as predictive of the need for additional PSO. These findings suggest that PSO should be considered when the fused segment fails to achieve or maintain appropriate lordotic alignment, particularly in cases with residual or progressive segmental kyphosis.
The primary PSO vertebrae were L3 (56.3%) and L4 (43.7%), which is consistent with prior research. G. Lainé et al. [17], reported in a multicenter cohort study that PSO levels were predominantly at L3 and L4 (75.3%) in patients with fixed sagittal imbalance. Similarly, Munish C. Gupta et al. [7], found that L3 (43.6%) was the most common PSO site in revision patients. To our knowledge, PSO should be performed at the level of maximal deformity to achieve optimal sagittal correction [22]. In patients with iatrogenic flatback, prior fusion was frequently located at the lower lumbar spine (L4 to S1), and due to adjacent segment degeneration or focal kyphosis within the fused segment, the upper instrumented vertebra or the immediately adjacent vertebra often becomes the apex of the deformity [16,22]. Additionally, performing PSO above L3 poses an increased risk of neurological deficits due to the proximity of the spinal cord and conus medullaris [23]. This risk is particularly concerning in patients with prior posterior surgery, where the posterior elements may be extensively scarred and adhered, making surgical exposure and correction more complex [12].
There was no significant difference in ODI and VAS for low back pain between the two groups, either preoperatively or postoperatively (p > 0.05). However, both groups showed significant postoperative improvement (p < 0.05). Although the surgical methods differed between the two groups, as shown in Table 2, there was no difference in postoperative spinopelvic parameters. This may explain why there was no significant difference in clinical outcomes between the groups after surgery. Nevertheless, previous studies [22,24,25] have suggested that achieving a C7-SVA less than 5 cm and a PI-LL mismatch less than 10° is associated with improved quality of life and functional outcomes. However, in elderly patients (age > 70 years), several studies [22,26] recommend achieving less stringent goals, specifically a C7-SVA less than 8 cm and a PI-LL mismatch less than 15°. These recommendations align closely with our study results. In Group A, with a mean age of 72.6 ± 6.6 years, the mean C7-SVA was 61.7 ± 66.1 mm, and the PI-LL mismatch was 7.2 ± 6.2°. In Group B, with a mean age of 67.1 ± 6.8 years, the mean C7-SVA was 30.7 ± 45.5 mm, and the PI-LL mismatch was 9.8 ± 11.1°.
Interestingly, seven cases of EASD were observed exclusively in patients who underwent ACR alone, despite the use of the same hyperlordotic cage. This phenomenon may be attributed to increased mechanical stress at adjacent segments with pre-existing degeneration, particularly involving the anterior longitudinal ligament (ALL). Minor intraoperative trauma, such as inadvertent injury to the ALL during disc preparation or anterior distraction during cage insertion and rod application, may predispose these segments to localized structural failure. To enhance segmental stability, supplemental dual rods were applied at the adjacent level during the perioperative period. However, two of these cases progressed to nonunion by two years postoperatively and required revision surgery. As a result, the anterior disc height may exceed the intended correction angle of the hyperlordotic cage, which is typically 23° to 30° [13]. This hypothesis is consistent with the rationale for performing ACR at flexible and non-ankylosed segments, where controlled correction is more safely achievable [11]. It also implies that only ACR alone can’t achieve an appropriate lordotic curve, so posteriorly based spinal osteotomy, such as PSO, is required. Therefore, we subdivided group A into two subgroups to investigate the optimal timing for performing additional PSO. There were no significant differences in preoperative spinopelvic parameters between the two subgroups (p > 0.05). Although DL also did not significantly differ, DA in the excessive subgroup was 2.8 ± 1.1°, significantly lower than that in the Non-excessive group (9.1 ± 3.5°, p = 0.001). These findings suggest that the flexibility of the adjacent segment plays a more crucial role in deciding to perform additional PSO than the overall lumbar flexibility. We identified the cutoff value of DA for predicting the occurrence of EASD; based on our results, we recommend performing additional PSO when the DA is less than 4.3°.
The primary limitation of our study is the small sample size and its single-institution, retrospective nature. Future studies with larger sample sizes and multi-center participation are warranted to validate these findings. Despite these limitations, our study was rigorously designed with strict inclusion and exclusion criteria, focusing solely on patients who underwent short-segment fusion surgery and subsequently developed iatrogenic flatback deformity. Patients who underwent short-segment fusion surgery often developed adjacent segment disease, such as stenosis, and subsequently underwent revision surgery involving only one or two adjacent levels. Since such cases were excluded from our cohort, the final sample size was inevitably limited. As a result, it was challenging to assemble a sufficiently large cohort, despite the increasing incidence of iatrogenic flatback in recent years.
5. Conclusions
Both ACR alone and combined with PSO effectively corrected iatrogenic flatback after short-segment fusion (≤3 levels). Additional PSO is recommended for patients with severe preoperative sagittal imbalance (C7-SVA > 242.8 mm), Segmental kyphotic spinal deformity (FSA > 3.2°), or limited adjacent segmental flexibility (DA < 4.3°) to optimize alignment and minimize complications.
Author Contributions
Conceptualization, S.-M.K., X.J.L. and I.-S.S.; methodology, X.J.L.; formal analysis, S.-M.K.; data curation, M.L.J.; writing—original draft preparation, S.-M.K. and I.-S.S.; writing—review and editing, X.J.L..; visualization, M.L.J.; supervision, Y.-C.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Kyung Hee University Hospital at Gangdong (protocol code KHNMC 2025-04-039).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACR | Anterior column realignment |
| ALL | Anterior longitudinal ligament |
| BMI | Body mass index |
| C7SVA | C7 sagittal vertical axis |
| DA | Dynamic segment angulation |
| DL | Dynamic lumbar lordosis |
| DSI | Degenerative sagittal imbalance |
| EADH | Excessive distraction of anterior disc height |
| EBL | Estimated blood loss |
| FSA | Fused segment angle |
| LL | Lumbar lordosis |
| LLL | Lower lumbar lordosis |
| ODI | Oswestry Disability Index |
| PI | Pelvic incidence |
| PI–LL | Pelvic incidence minus lumbar lordosis |
| PLIF | Posterior lumbar interbody fusion |
| PROMs | Patient-reported outcome measures |
| PSO | Pedicle subtraction osteotomy |
| PT | Pelvic tilt |
| ROC | Receiver operating characteristic |
| SVA | Sagittal vertical axis |
| SS | Sacral slope |
| TK | Thoracic kyphosis |
References
- Booth, K.C.; Bridwell, K.H.; Lenke, L.G.; Baldus, C.R.; Blanke, K.M. Complications and Predictive Factors for the Successful Treatment of Flatback Deformity (Fixed Sagittal Imbalance). Spine 1999, 24, 1712–1720. [Google Scholar] [CrossRef]
- Wiggins, G.C.; Ondra, S.L.; Shaffrey, C.I. Management of Iatrogenic Flat-Back Syndrome. Neurosurg. Focus 2003, 15, E8. [Google Scholar] [CrossRef]
- Jagannathan, J.; Sansur, C.A.; Shaffrey, C.I. Iatrogenic Spinal Deformity. Neurosurgery 2008, 63 (Suppl. 3), 104–116. [Google Scholar] [CrossRef]
- Lagrone, M.O.; Bradford, D.S.; Moe, J.H.; Lonstein, J.E.; Winter, R.B.; Ogilvie, J.W. Treatment of Symptomatic Flatback after Spinal Fusion. J. Bone Joint Surg. Am. 1988, 70, 569–580. [Google Scholar] [CrossRef]
- Savage, J.W.; Patel, A.A. Fixed Sagittal Plane Imbalance. Global Spine J. 2014, 4, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Louie, P.K.; Iyer, S.; Khanna, K.; Harada, G.K.; Khalid, A.; Gupta, M.; Burton, D.; Shaffrey, C.; Lafage, R.; Lafage, V.; et al. Revision Strategies for Harrington Rod Instrumentation: Radiographic Outcomes and Complications. Global Spine J. 2022, 12, 654–662. [Google Scholar] [CrossRef]
- Gupta, M.C.; Ferrero, E.; Mundis, G.; Smith, J.S.; Shaffrey, C.I.; Schwab, F.; Kim, H.J.; Boachie-Adjei, O.; Lafage, V.; Bess, S.; et al. Pedicle Subtraction Osteotomy in the Revision Versus Primary Adult Spinal Deformity Patient: Is There a Difference in Correction and Complications? Spine 2015, 40, E1169–E1175. [Google Scholar] [CrossRef] [PubMed]
- Potter, B.K.; Lenke, L.G.; Kuklo, T.R. Prevention and Management of Iatrogenic Flatback Deformity. J. Bone Joint Surg. Am. 2004, 86, 1793–1808. [Google Scholar] [CrossRef] [PubMed]
- Diebo, B.G.; Shah, N.V.; Boachie-Adjei, O.; Zhu, F.; Rothenfluh, D.A.; Paulino, C.B.; Schwab, F.J.; Lafage, V. Adult Spinal Deformity. Lancet 2019, 394, 160–172. [Google Scholar] [CrossRef]
- Diebo, B.G.; Balmaceno-Criss, M.; Lafage, R.; McDonald, C.L.; Alsoof, D.; Halayqeh, S.; DiSilvestro, K.J.; Kuris, E.O.; Lafage, V.; Daniels, A.H. Sagittal Alignment in the Degenerative Lumbar Spine: Surgical Planning. J. Bone Joint Surg. Am. 2024, 106, 445–457. [Google Scholar] [CrossRef]
- Zhang, H.; Carreon, L.Y.; Dimar, J.R., II. The Role of Anterior Spine Surgery in Deformity Correction. Neurosurg. Clin. N. Am. 2023, 34, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.K.; Mummaneni, P.V.; Shaffrey, C.I. Approach Selection: Multiple Anterior Lumbar Interbody Fusion to Recreate Lumbar Lordosis Versus Pedicle Subtraction Osteotomy: When, Why, How? Neurosurg. Clin. N. Am. 2018, 29, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Uribe, J.S.; Schwab, F.; Mundis, G.M.; Xu, D.S.; Januszewski, J.; Kanter, A.S.; Okonkwo, D.O.; Hu, S.S.; Vedat, D.; Eastlack, R.; et al. The Comprehensive Anatomical Spinal Osteotomy and Anterior Column Realignment Classification. J. Neurosurg. Spine 2018, 29, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Hirai, T.; Yoshii, T.; Egawa, S.; Sakai, K.; Inose, H.; Yuasa, M.; Yamada, T.; Ushio, S.; Kato, T.; Arai, Y.; et al. Increased Height of Fused Segments Contributes to Early-Phase Strut Subsidence after Anterior Cervical Corpectomy with Fusion for Multilevel Ossification of the Posterior Longitudinal Ligament. Spine Surg. Relat. Res. 2020, 4, 294–299. [Google Scholar] [CrossRef]
- Chou, S.H.; Lin, S.Y.; Shen, P.C.; Tu, H.P.; Huang, H.T.; Shih, C.L.; Lu, C.C. Pain Control Affects the Radiographic Diagnosis of Segmental Instability in Patients with Degenerative Lumbar Spondylolisthesis. J. Clin. Med. 2021, 10, 17. [Google Scholar] [CrossRef]
- Frerich, J.M.; Dibble, C.F.; Park, C.; Bergin, S.M.; Goodwin, C.R.; Abd-El-Barr, M.M.; Shaffrey, C.I.; Than, K.D. Proximal Lumbar Anterior Column Realignment for Iatrogenic Sagittal Plane Adult Spinal Deformity Correction: A Retrospective Case Series. World Neurosurg. 2025, 193, 884–892. [Google Scholar] [CrossRef]
- Lainé, G.; Le Huec, J.C.; Blondel, B.; Fuentes, S.; Fiere, V.; Parent, H.; Lucas, F.; Roussouly, P.; Tassa, O.; Bravant, E.; et al. Factors Influencing Complications after 3-Columns Spinal Osteotomies for Fixed Sagittal Imbalance from Multiple Etiologies: A Multicentric Cohort Study about 286 Cases in 273 Patients. Eur. Spine J. 2022, 31, 3673–3686. [Google Scholar] [CrossRef]
- Cho, K.J.; Kim, K.T.; Kim, W.J.; Lee, S.H.; Jung, J.H.; Kim, Y.T.; Park, H.B. Pedicle Subtraction Osteotomy in Elderly Patients with Degenerative Sagittal Imbalance. Spine 2013, 38, E1561–E1566. [Google Scholar] [CrossRef]
- Godzik, J.; Hlubek, R.J.; de Andrada Pereira, B.; Xu, D.S.; Walker, C.T.; Farber, S.H.; Turner, J.D.; Mundis, G.; Uribe, J.S. Combined Lateral Transpsoas Anterior Column Realignment with Pedicle Subtraction Osteotomy to Treat Severe Sagittal Plane Deformity: Cadaveric Feasibility Study and Early Clinical Experience. World Neurosurg. 2019, 121, e589–e595. [Google Scholar] [CrossRef]
- Sadrameli, S.S.; Davidov, V.; Lee, J.J.; Huang, M.; Kizek, D.J.; Mambelli, D.; Rajendran, S.; Barber, S.M.; Holman, P.J. Hybrid Anterior Column Realignment–Pedicle Subtraction Osteotomy for Severe Rigid Sagittal Deformity. World Neurosurg. 2021, 151, e308–e316. [Google Scholar] [CrossRef]
- Hu, W.; Wang, B.; Run, H.; Zhang, X.; Wang, Y. Pedicle Subtraction Osteotomy and Disc Resection with Cage Placement in Post-Traumatic Thoracolumbar Kyphosis, a Retrospective Study. J. Orthop. Surg. Res. 2016, 11, 112. [Google Scholar] [CrossRef]
- Kim, Y.J.; Bridwell, K.H.; Lenke, L.G.; Cheh, G.; Baldus, C. Results of Lumbar Pedicle Subtraction Osteotomies for Fixed Sagittal Imbalance: A Minimum 5-Year Follow-Up Study. Spine 2007, 32, 2189–2197. [Google Scholar] [CrossRef]
- Hyun, S.J.; Kim, Y.J.; Rhim, S.C. Spinal Pedicle Subtraction Osteotomy for Fixed Sagittal Imbalance Patients. World J. Clin. Cases 2013, 1, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Lewis, S.J.; Lenke, L.G.; Baldus, C.; Blanke, K. Pedicle Subtraction Osteotomy for the Treatment of Fixed Sagittal Imbalance. J. Bone Joint Surg. Am. 2003, 85, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Schwab, F.J.; Patel, A.; Shaffrey, C.I.; Smith, J.S.; Farcy, J.P.; Boachie-Adjei, O.; Hostin, R.A.; Hart, R.A.; Akbarnia, B.A.; Burton, D.C.; et al. Sagittal Realignment Failures following Pedicle Subtraction Osteotomy Surgery: Are We Doing Enough? J. Neurosurg. Spine 2012, 16, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Boody, B.S.; Rosenthal, B.D.; Jenkins, T.J.; Patel, A.A.; Savage, J.W.; Hsu, W.K. Iatrogenic Flatback and Flatback Syndrome: Evaluation, Management, and Prevention. Clin. Spine Surg. 2017, 30, 142–149. [Google Scholar] [CrossRef]
Figure 1.
Excessive distraction of anterior disc height (EADH) was defined as the presence of an excessive anterior disc angle (>30°) between adjacent endplates.
Figure 1.
Excessive distraction of anterior disc height (EADH) was defined as the presence of an excessive anterior disc angle (>30°) between adjacent endplates.
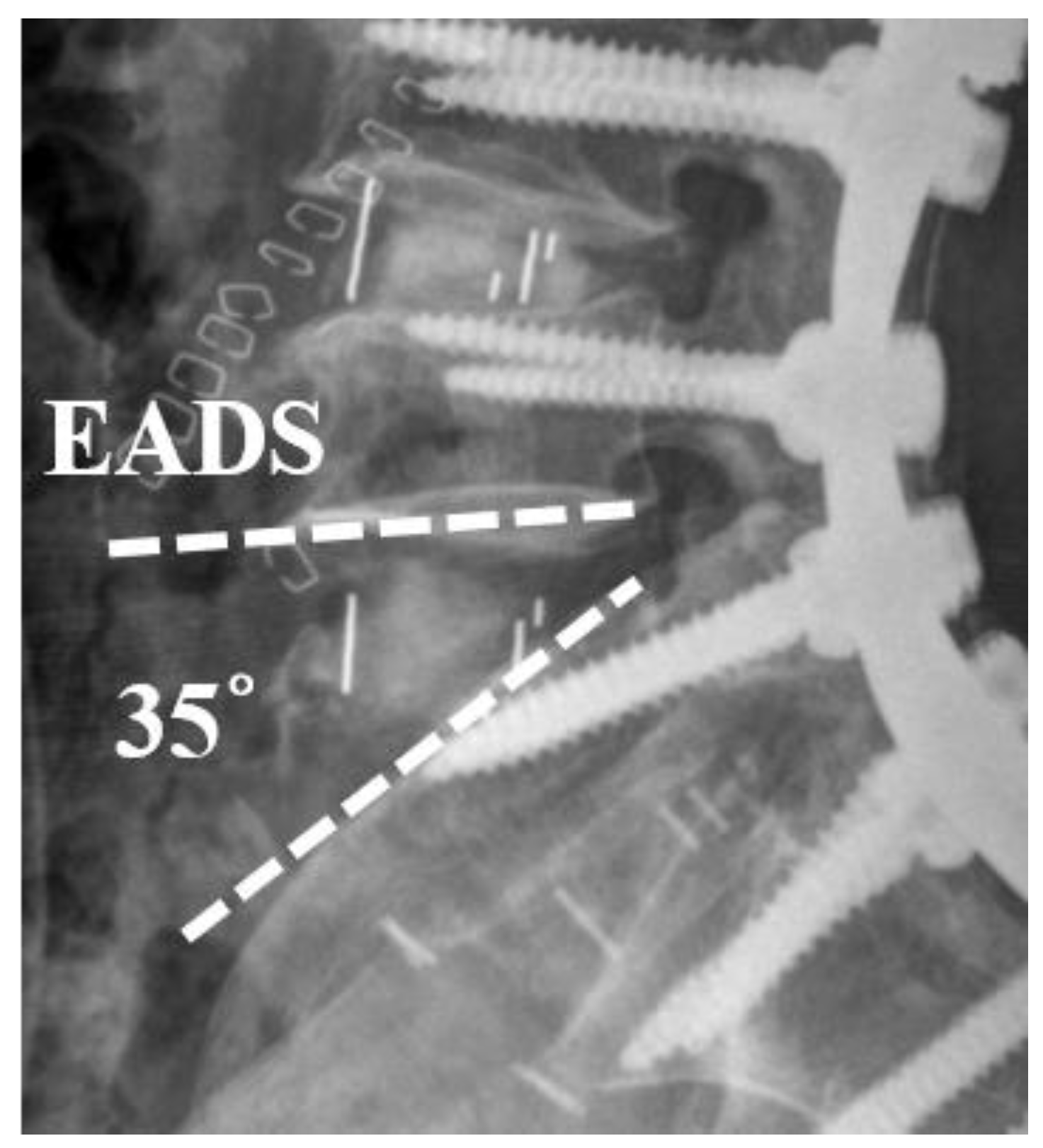
Figure 2.
Receiver operating characteristic curves determining Optimal cut-off values of spinopelvic parameters for indicating additional PSO.
Figure 2.
Receiver operating characteristic curves determining Optimal cut-off values of spinopelvic parameters for indicating additional PSO.
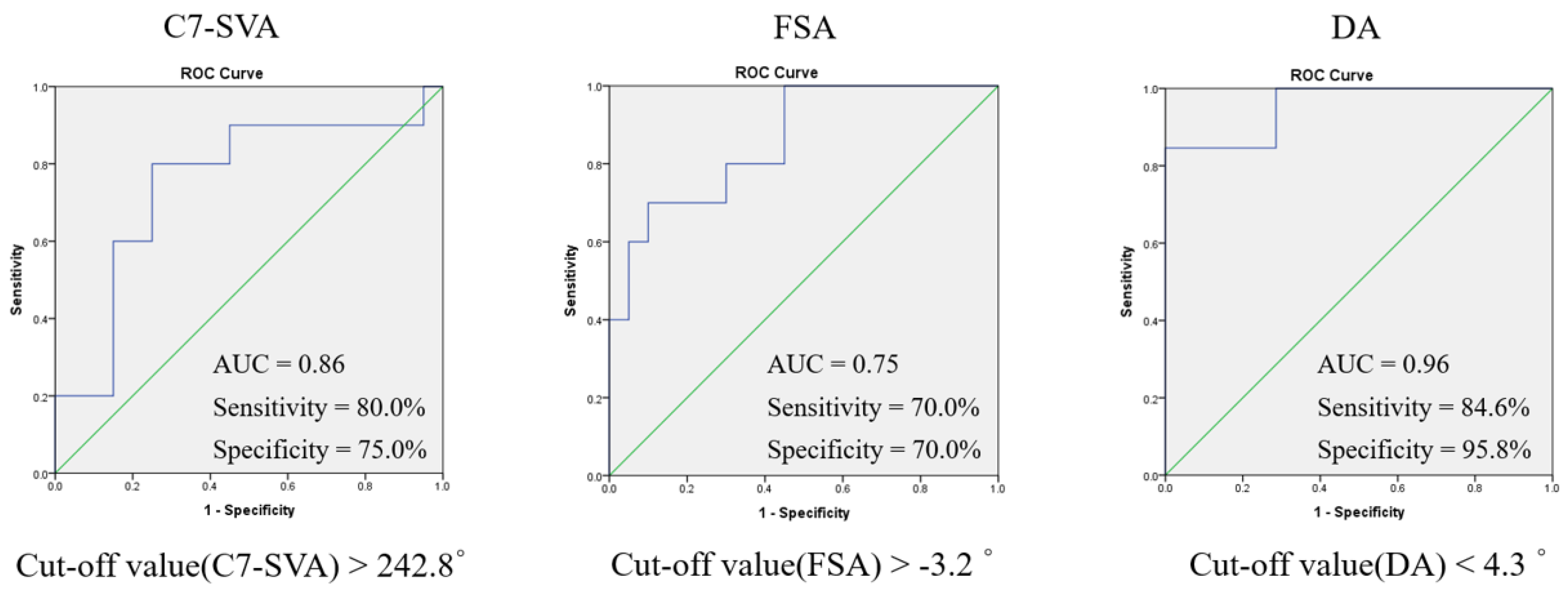
Figure 3.
A 72-year-old female diagnosed with iatrogenic flatback following a prior spinal fusion from L4-5. (a) Preoperative radiographs show severe sagittal imbalance, with a C7-SVA of 201.6 mm and LL of 6.1°. (b) After ACR at L2–4 and PLIF at L5 to the sacrum, postoperative radiographs at 2-year follow-up show significant correction, with the C7-SVA reduced to 43.6 mm and LL improved to −44.1°. A 71-year-old female diagnosed with iatrogenic flatback following a prior spinal fusion from L4 to the sacrum. (c) Preoperative radiographs show severe sagittal imbalance, with a C7-SVA of 301.6 mm, LL of 23.8°, and FSA of 5.7°. (d) After ACR at L1-4 and an additional PSO at L3, postoperative radiographs at 2-year follow-up show significant correction, with the C7-SVA reduced to 60.6 mm, LL improved to −55.1°, and FSA corrected to −23.1°.
Figure 3.
A 72-year-old female diagnosed with iatrogenic flatback following a prior spinal fusion from L4-5. (a) Preoperative radiographs show severe sagittal imbalance, with a C7-SVA of 201.6 mm and LL of 6.1°. (b) After ACR at L2–4 and PLIF at L5 to the sacrum, postoperative radiographs at 2-year follow-up show significant correction, with the C7-SVA reduced to 43.6 mm and LL improved to −44.1°. A 71-year-old female diagnosed with iatrogenic flatback following a prior spinal fusion from L4 to the sacrum. (c) Preoperative radiographs show severe sagittal imbalance, with a C7-SVA of 301.6 mm, LL of 23.8°, and FSA of 5.7°. (d) After ACR at L1-4 and an additional PSO at L3, postoperative radiographs at 2-year follow-up show significant correction, with the C7-SVA reduced to 60.6 mm, LL improved to −55.1°, and FSA corrected to −23.1°.
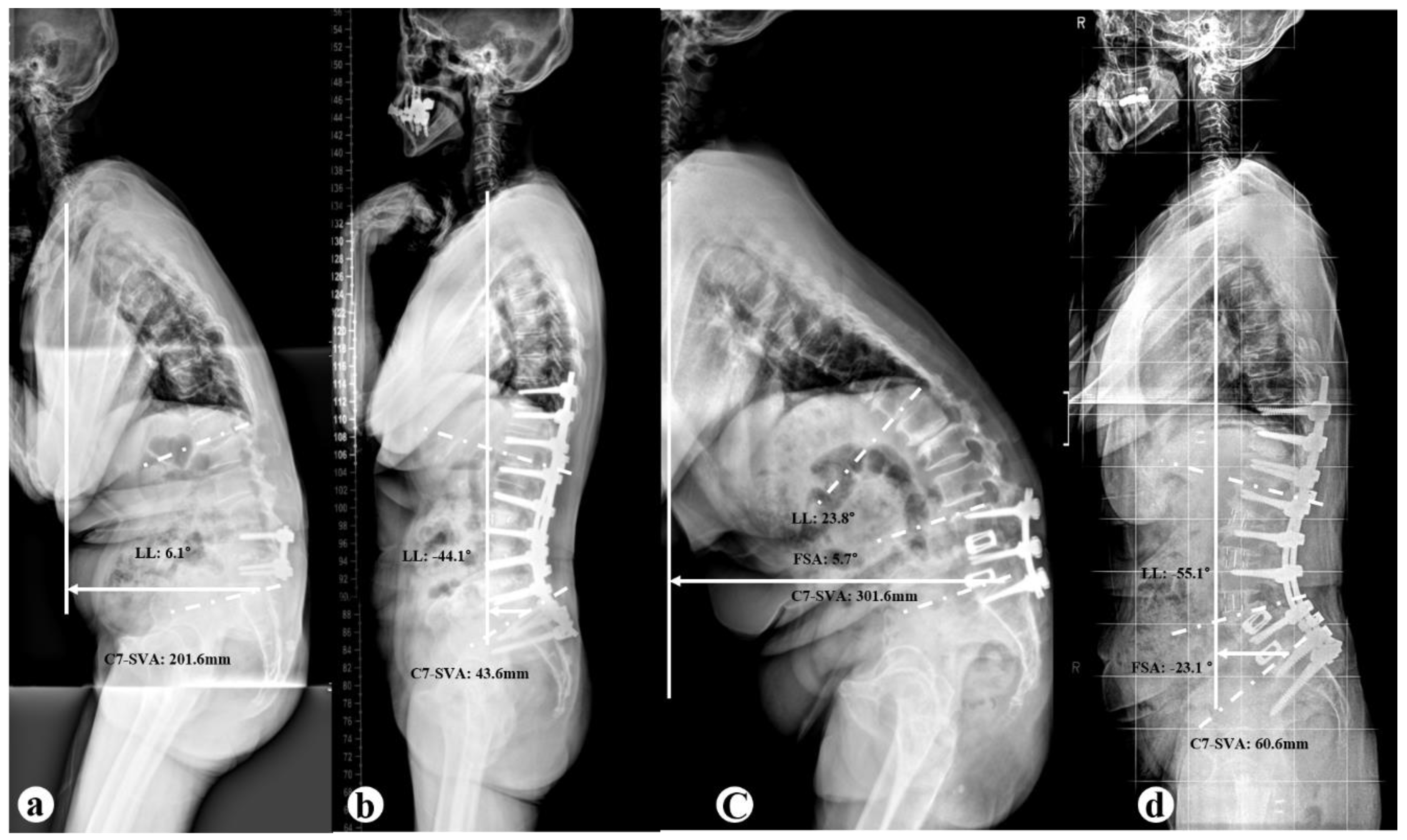

Table 1.
Demographic and Surgical Data.
| Variables | Group A (n=33) | Group B (n=16) | P Value |
| Age, years | 72.6±6.6 | 67.1±6.8 | 0.420 |
| Sex (Male: Female) | 3:30 | 1:15 | 0.733 |
| EBL (ml) | 1845±929.9 | 2260±1447.8 | 0.348 |
| BMI (%) | 25.2±3.2 | 25.5±2.2 | 0.742 |
| Operative time, minutes | 404.9±91.4 | 506.0±154.8 | 0.032* |
| Follow-up, moth | 25.2±5.8 | 25.2±4.1 | 0.981 |
| No. of previous fusion level | 1.1±0.2 | 2.2±0.8 | <0.001* |
| No. of instrumented level | 7.6±0.8 | 8.1±0.3 | 0.530 |
| No. of ACR level | 2.5±0.6 | 1.9±0.9 | 0.053 |
| PLIF L5-S1, no. (%) | 16 (40.8) | 4 (25) | 0.117 |
| PSO, no. (%) | |||
| L3 | 9 (56.3) | ||
| L4 | 7 (43.7) | ||
Values are presented as mean ± SD unless otherwise indicated. * Significant difference; n = number of patients; EBL= Estimated blood loss.
Table 2.
Comparison of Radiographic Parameters Between Group A and Group B.
| Parameter | Group A (n=33) | Group B (n=16) | P Value |
| C7-SVA (mm) | |||
| Preoperative | 219.8±76.4† | 293.8±90.3† | 0.026* |
| Postoperative | 61.7±66.1† | 30.7±45.5† | 0.195 |
| correction | 157.9±84.9 | 263.0±79.9 | 0.003* |
| TK (°) | |||
| Preoperative | 8.2±14.1† | -0.4±12.2† | 0.110 |
| Postoperative | 33.4±12.6† | 29.0±13.5† | 0.389 |
| correction | -25.2±13.1 | -29.5±18.8 | 0.372 |
| LL (°) | |||
| Preoperative | 9.6±19.4† | 22.2±20.5† | 0.051 |
| Postoperative | -51.1±10.2† | -49.8±8.7† | 0.728 |
| correction | 60.7±23.3 | 72.0±17.8 | 0.100 |
| LLL (°) | |||
| Preoperative | -7.0±9.8† | -2.4±13.3† | 0.287 |
| Postoperative | -23.9±8.9† | -27.6±10.9† | 0.331 |
| correction | 16.9±10.4 | 25.2±5.8 | 0.127 |
| T1PA (°) | |||
| Preoperative | 53.5±15.4† | 64.6±17.3† | 0.085 |
| Postoperative | 20.8±11.1† | 21.8±8.9† | 0.820 |
| correction | 32.7±16.3 | 42.8±12.9 | 0.099 |
| SS (°) | |||
| Preoperative | 24.4±10.8† | 26.4±9.1† | 0.621 |
| Postoperative | 38.1±7.0† | 34.3±9.6† | 0.230 |
| correction | -13.6±8.4 | -7.9±9.1 | 0.097 |
| PT (°) | |||
| Preoperative | 34.1±12.1† | 33.4±9.3† | 0.885 |
| Postoperative | 20.1±9.5† | 25.1±10.6† | 0.212 |
| correction | 13.9±8.6 | 8.4±9.0 | 0.114 |
| PI (°) | |||
| Preoperative | 58.5±11.0 | 59.9±5.2 | 0.705 |
| Postoperative | 58.3±11.0 | 59.6±5.4 | 0.738 |
| correction | 0.1±1.2 | 0.2±1.2 | 0.726 |
| PI-LL (°) | |||
| Preoperative | 65.1±19.1† | 82.1±20.9† | 0.051 |
| Postoperative | 7.2±6.2† | 9.8±11.1† | 0.658 |
| correction | 57.8±23.4 | 72.2±17.4 | 0.096 |
| FSA (°) | |||
| Preoperative | -7.2±7.5 | 5.1±8.0† | 0.001* |
| Postoperative | -7.8±7.8 | -26.6±12.6† | < 0.001 |
| correction | -0.6±2.3 | -31.6±8.9 | < 0.001 |
Values are presented as mean ± SD unless otherwise indicated. *Significant difference between two groups (P<0.05). †Significant difference between preoperative and postoperative (P<0.05).
Table 3.
Comparison of Clinical Outcomes.
| Variables | Group A (n=33) | Group B (n=16) | P Value |
| ODI | |||
| Preoperative | 28.1±7.8 | 23.5±7.6 | 0.146 |
| Postoperative | 14.5±7.4 | 11.0±7.5 | 0.229 |
| P Value | <0.001* | 0.001* | - |
| VAS-low back | |||
| Preoperative | 5.7±2.1 | 5.4±2.2 | 0.724 |
| Postoperative | 2.9±1.3 | 2.6±1.3 | 0.614 |
| P Value | <0.001* | 0.009* | - |
Values are presented as mean ± SD unless otherwise indicated. *Significant improvement (P<0.05).
Table 4.
Comparison of Incidence of complication between two groups.
| Group A (n=33) | Group B (n=16) | P Value | |
| Perioperative n, (%) | |||
| Dura tear | 2, (6.1%) | 2, (12.5%) | 0.440 |
| Motor deficit | 1, (3.0%) | 2, (12.5%) | 0.195 |
| Blood loss (>4000ml) | 0 | 1, (6.3%) | 0.147 |
| EADH | 7, (21.2%) | 0 | 0.047* |
| Postoperative n, (%) | |||
| Infection | 1, (3.0%) | 1, (6.3%) | 0.593 |
| PJK | 2, (6.1%) | 1, (6.3%) | 0.979 |
| PJF | 2, (6.1%) | 1, (6.3%) | 0.979 |
| Rod fracture | 3, (9.1%) | 2, (12.5%) | 0.712 |
*Significant difference between two groups (P<0.05). EADH: Excessive distraction of anterior disc height.
Table 5.
Preoperative Radiographic Parameters depend on complications.
| Parameter | Excessive group (n=7) |
Non-excessive group (n=26) |
P Value |
| C7-SVA (mm) | 213.2 ± 83.9 | 223.3 ± 75.4 | 0.785 |
| TK (°) | 12.2 ± 10.5 | 7.2 ± 6.5 | 0.081 |
| LL (°) | 11.3 ± 13.6 | 4.1 ± 7.4 | 0.054 |
| LLL (°) | -5.6 ± 12.7 | -7.8 ± 8.3 | 0.643 |
| PT (°) | 36.4 ± 9.9 | 32.8 ± 13.4 | 0.544 |
| PI (°) | 56.2 ± 9.2 | 59.7 ± 12.1 | 0.509 |
| DL (°) | 18.6 ± 10.5 | 21.7 ± 7.4 | 0.458 |
| DA (°) | 2.8 ± 1.1 | 9.1 ± 3.5 | <0.001* |
Values are presented as mean ± SD unless otherwise indicated. *Significant difference between two groups (P<0.05). DL: Dynamic lumbar lordosis; DA: Dynamic segmental angle.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



