Submitted:
19 August 2025
Posted:
20 August 2025
Read the latest preprint version here
Abstract
Background/Objectives: Posterior cortical atrophy, also referred to as Benson’s syndrome, is a presentation of Alzheimer’s disease that occurs in 5-15% of Alzheimer’s patients. Visual processing is the predominant affected modality in posterior cortical atrophy, and symptoms such as prosopagnosia, simultanagnosia, alexia, optic ataxia, and visual hallucinations may occur, as well as blurred vision and visual distortions. Posterior cortical atrophy is considered to be a disease without known cause or effective treatment. Methods: We report here a patient with posterior cortical atrophy who responded to a personalized, precision medicine protocol. Results: The patient had improved MRI volumetrics, symptoms, and cognitive testing. She regained the ability to read, use her computer, and undertake computer-based brain training, among other cognitive improvements. She has now sustained her improvement for over one year, and continues to regain her independence and confidence. Conclusions: These results argue for additional laboratory testing in the evaluation of patients with posterior cortical atrophy, and support the possibility of utilizing a similar approach in a proof-of-concept trial.
Keywords:
Case report
; Alzheimer’s
; agnosia
; agraphia
; Gerstmann’s
; volumetrics
; brain training
; precision medicine
1. Introduction
In 1988, Prof. D. Frank Benson described five patients with a previously-undescribed neurodegenerative syndrome involving atrophy of the parietal and occipital brain regions, and associated symptoms [1]. This syndrome was dubbed posterior cortical atrophy (PCA), and the symptoms included alexia, agraphia, visual agnosia, and components of Balint’s, Gerstmann’s, and transcortical sensory aphasia syndromes, while memory, insight, and judgment were relatively preserved until late in the course. MRI and CT scans showed atrophy predominating in the parietal and occipital regions. At the time of the initial publication, no pathological specimen was available, and therefore the authors could only speculate on the underlying neuropathology, which they suggested may be an atypical variant of Alzheimer’s disease, a lobar atrophy analogous to what occurs in frontotemporal lobar degeneration, or a novel neuropathological entity. It has turned out that the vast majority of patients with PCA have Alzheimer’s disease [2], although occasionally PCA is associated with other conditions such as diffuse Lewy body disease, corticobasal degeneration, or Creutzfeldt-Jakob disease [3].
Since the initial description of PCA by Benson and colleagues, it has been noted that 5-15% of Alzheimer’s disease cases present as PCA [4]. PCA patients are often early onset Alzheimer’s disease patients, with the initial symptoms occurring prior to age 65. In a review of early onset Alzheimer’s by Mendez [5], it was pointed out that PCA is one of the features that is associated more commonly with early onset than late onset Alzheimer’s, whereas amnestic presentations are more common with late onset AD.
The cause(s) of PCA are unknown, and no effective treatment has been demonstrated [3]. However, it has been noted previously that patients with early onset Alzheimer’s and non-amnestic presentations often have evidence of toxin exposure or tick-borne illness [6], and that treating these potential contributors may be associated with improved cognition.
We report here a patient with early-onset Alzheimer’s presenting as PCA, who responded to a personalized, precision medicine protocol that included treatment of Bartonella infection and mycotoxins, with marked improvement in symptoms and MRI volumetrics, regaining the ability to read and use the computer, among other salutary effects. We hope that this case report may help to add to the standard evaluation of patients with PCA, identify potentially treatable contributors in some cases, and provide support for the performance of a proof-of-concept clinical trial.
2. Materials and Methods
This case study was taken from a patient evaluated and treated by the authors. No identifying information was included. The patient consented to the description. The evaluation and treatment methods have been described previously ([7]).
3. Results
A 63-year-old woman presented with visual complaints. At the age of 54, she had had an automobile accident without head trauma, and following that, complained repeatedly that something was “not right” about her vision. She also felt that, overall, her brain “simply wasn’t right”. She felt her memory was not the same and her ability to think as she formerly had was somehow different. However, multiple medical evaluations failed to reach a diagnosis. Furthermore, she was told there was nothing wrong, when she knew in fact this was untrue.
Then in her early 60s, she began to experience more definitive symptoms, such as blurry vision, optic ataxia, and difficulty seeing multiple objects in her visual field (simultanagnosia). She developed difficulty reading, and was unable to use her computer or drive an automobile. In one instance, while she was driving she felt that the scene in front of her rippled, just as one might see when one watches a movie and the screen ripples to represent going back in time. When her vision returned there was another car right next to her that she hadn’t seen. It was at this time she stopped driving.
In addition to her declining vision, her memory began to decline rapidly, depression set in, and she became angry that no one seemed to be able to help her. She began to isolate herself from friends, concerned about their reaction to her verbal repetitions. Travel was tiring and there was generally a period of disorientation upon arrival at the destination. Her affect became flat. She joined a support group for patients and care partners of those with Alzheimer’s, and since she was still verbally proficient, she was able to explain to the other care partners what this condition was like. A few years later, they reflected to her that for the first year after they had met her, she had not smiled.
With her blurry vision and her increasing loss of memory, she stopped reading. She had trouble keeping track of what she was reading and because she could not see the words well, she became irritated and frustrated. She had difficulty organizing and became irritated and then apathetic. Her office became cluttered.
She began to rely fully on her husband for meal preparation, management of medication, and direction of what to do throughout the day. She was determined to find a way to beat her illness, but she did not have the faculties to follow through.
Her MRI volumetrics showed parietal and occipital atrophy, with parietal lobe volume at <1st percentile for age, occipital lobe volume at the 10th percentile, temporal lobe volume at the 41st percentile, and frontal lobe volume at the 13th percentile (Table 1). Based on her symptoms and atrophy pattern, a diagnosis of PCA was made.
She participated in a pharmaceutical trial for an anti-amyloid antibody for 1.5 years, but after the completion of the trial, found that she had been in the placebo-control group.
She took donepezil for a few years without noticing any symptomatic improvement. When she discontinued donepezil, she did not notice any acceleration of decline, but did notice that the headaches she had had abated.
Laboratory evaluation showed her to be ApoE4 heterozygous, with WBC 4400/mL, HOMA-IR of 0.73, hemoglobin A1c 5.1%, homocysteine 6.2 mM, estradiol 0 pg/mL, progesterone 13.66 ng/mL, TSH 1.22 mU/mL, vitamin D 32.9 ng/mL, serum copper 155 mg/dL, serum zinc 132 mg/dL, ALT 16 units/L, AST 30 units/L, blood mercury 5 mcg/L, MMP-9 135 ng/mL (normal < 331 ng/mL), TGF-1 11,360 pg/mL (normal < 2380 pg/mL), LDL 122 mg/dL, LDL particle number 1449 nM, triglycerides 57 mg/dL, albumin 4.4 g/dL, and glutathione 585 mM.
She failed the visual contrast sensitivity test (https://www.vcstest.com/). Plasma p-tau 181 was elevated at 1.72 pg/mL (normal range 0-0.97 pg/mL). A sleep study disclosed mild sleep apnea, with an apnea/hypopnea index of 9.9.
Urinary mycotoxin analysis was positive for ochratoxin, aflatoxin, trichothecenes, gliotoxin, and zearalenone. Antibodies to Borrelia and Bartonella were positive (IgM). Urinary mercury was increased at 10 mg/g of creatinine (normal < 1.3), and lead was also increased at 6.2 mg/g creatinine (normal < 1.2).
She was treated with a personalized, precision medicine approach that included:
Treatment of Bartonella for three months:
ABart ½ dropper po bid
Azithromycin 500 mg po qd
Doxycycline 100 mg po bid
Rifampin 300 mg po bid
Megasporebiotic 295 mg po bid
Treatment of mycotoxin exposure (ongoing for 2.5 years):
Bentonite clay 450 mg po bid
Activated charcoal 560 mg po bid
Chlorella 125 mg po tid
Welchol 625 mg po bid
Saccharomyces boulardii 235 mg po tid
InterFase Plus 675 mg po bid
Nystatin 500 mg po qid
Argentyn nasal spray, 2 sprays to each nostril bid
Amphotericin B 150 mg po bid
BE spray (mupirocin and EDTA) 2 sprays in each nostril bid
Treatment of lead and mercury for six months
DMSA 200 mg twice per week
In addition to the treatments above, she began a plant-rich, mildly ketogenic diet, with fasting of 12-14 hours each night. She used a breathalyzer device (Biosense) to track her acetone levels, scoring in the 30’s on average, which correlates to approximately 3 mM beta-hydroxybutyrate in the blood.
Due to a pain in her foot (which is common with Bartonella), her exercise was limited, but she used a Peloton and walked infrequently. She checked her oxygen saturation at night using a Wellue ring, and her SpO2 was an average of 96-98%, with few drops and none below 90%. She used a Sunlight sauna for diaphoresis and detoxification 2-3x/week. She began bioidentical hormone replacement therapy, valacyclovir, and took supplements tailored to her laboratory data, including Ashwagandha, Bacopa, Gotu kola, Cataplex b-gf (bovine liver, organic beet (root), nutritional yeast, defatted wheat germ, rice bran, organic sweet potato, organic carrot, and bovine adrenal), pregnenolone, DHEA, S-adenosyl methionine, NAD, glutathione, methyl-B12, zinc, vitamin D, multivitamins, magnesium threonate, pro-resolving mediators, and 5-hydroxytryptophan.
She received glutathione intravenously weekly for 10 weeks to support detoxification, ozone treatment for her pathogens, and used a grounding mat, but no change in her symptoms were linked temporally to these treatments. However, when she began exercise with oxygen therapy (EWOT), she noticed an immediate improvement in her symptoms. She was unable to do computer brain training initially, due to her vision. She also had cranial sacral therapy monthly.
In April 2023, she began vision exercises and training, which are ongoing.
As she began treatment, the first change noted was stabilization, without further decline. Next, her memory began to improve. She remembered more details in stories from a few days prior and in some cases a few weeks prior. Her engagement picked up tremendously and in the support group she began discussing how the group could collectively help others. She regained her sharp wit and her ability to tell engaging stories.
Her attitude toward life became more focused on the future. She began talking about her bucket list and started to make to-do lists again. Her feelings began to change, from her initial anger that no one had helped her 10 years prior, to being grateful for what she can do presently.
Over the year after treatment was initiated, her inability to read resolved, and she began reading without difficulty. She is once again reading with purpose and great interest. Her ability to use the computer returned, and she was once again able to do computer-based brain training.
Her engagement with others improved, and she became a leader in her Alzheimer’s support group, helping others in the group. She served as a panelist regarding her own case history in front of an audience of 100 people, answering questions extemporaneously, and accurately, for over an hour.
She responded to vision training, and whereas she initially struggled with tracking and saccadic movements, she improved these markedly, and also improved her vergence and binocular vision.
She has begun driving in parking lots but recognizes that she is not yet ready for road driving.
Her mycotoxins decreased: ochratoxin A from 36.09 to 10.98 ng/g creatinine (normal <7.5 ng/g creatinine), mycophenolic acid 213 to 37.4 (normal <37.4), zearalenone 293 to undetectable (normal <3.2). Her TGF-1 decreased from 11,360 to 6323 pg/mL (normal < 2380 pg/mL).
Her MRI volumetrics showed marked improvement (Table 1): her parietal lobe volume increased from <1st percentile to the 22nd percentile (Figure 1); her occipital lobe volume increased from the 10th to 25th percentile; and her hippocampal volume increased from the 6th to 32nd percentile (Figure 2). Her p-tau 181 improved modestly, from 1.72 pg/mL to 1.68 pg/mL to 1.52 pg/mL.
4. Discussion
Been noted previously that non-amnestic presentations of Alzheimer’s disease, such as PCA, primary progressive aphasia (PPA), and many with early-onset Alzheimer’s (onset before 65 years of age [5], tend to be associated with biotoxin exposure and/or tick-borne illness [6]. This patient had both, and treatment of these potential contributors, along with basic metabolic support, led to marked improvement in her cognitive symptoms, as well as MRI volumetrics. Her ability to read, use her computer, and undergo computer-based brain training all returned. Furthermore, her previous long-term decline has been replaced by ongoing improvement.
Dr. R. Shoemaker described chronic inflammatory response syndrome (CIRS), which is associated with biotoxins and tick-borne illnesses such as Borrelia, Bartonella, Ehrlichia, and Babesia. It has been noted previously that laboratory testing characteristic of CIRS, such as increased C4a and TGF-1, also occurs commonly in non-amnestic presentations of Alzheimer’s disease, such as PCA and PPA [6]. This patient was found to have a markedly elevated TGF-1; however, her MMP-9, which is also commonly elevated in CIRS, was in the normal range. She also had some of the symptoms and conditions associated with CIRS, such as fatigue, memory loss, pain, disorientation, and depression.
The improvement that occurred with treatment might argue that she did not have Alzheimer’s disease, but her elevated p-tau 181, ApoE4 heterozygosity, progressive decline over several years, symptoms typical of PCA, and MRI showing marked parietal lobe atrophy (and to a lesser extent, hippocampal and occipital lobe atrophy), all support the diagnosis of Alzheimer’s disease.
Considering that PCA represents approximately 5-15% of patients with Alzheimer’s disease, there may be between 330,000 and one million PCA patients in the United States. Since the cause(s) of PCA have not been identified, and no effective treatment has been developed, it may be productive to include in the evaluation of potential PCA patients testing that includes the identification of tick-borne illnesses such as Borrelia, Bartonella, Babesia, and Ehrlichia, as well as tests for mycotoxin exposure, detoxification status, and immune status. Furthermore, the case history presented here suggests that a proof-of-concept trial should be considered, as a step toward effective treatment for PCA.
5. Conclusions
These results demonstrate the potential for successful treatment of PCA, not simply slowing decline but improving symptoms and MRI volumetrics. The results also argue for additional laboratory testing in the evaluation of patients with posterior cortical atrophy to include tick-borne illnesses, mycotoxins, and heavy metals, and support the potential to utilize a similar approach in a proof-of-concept trial.
Author Contributions
Conceptualization, D.B. and K.R.; methodology, N.N., D.B., C.K., and K.R.; data curation, K.R. and D.B.; writing—original draft preparation, D.B.; writing—review and editing, K.R., N.N., C.K., and D.B. All authors have read and agreed to the published version of the manuscript.
Funding
No grant funds were used in this work.
Institutional Review Board Statement
The manuscript is to record the diagnosis and treatment process of PCA patients, and ethical approval is not required.
Informed Consent Statement
Informed consent for treatment was obtained for all treatment with non-standard therapeutics. As noted above, the evaluation and treatment methods have been described previously [7].
Data Availability Statement
Data for this manuscript were obtained from patient records and anonymized for publication. These data have not been deposited in a public data base..
Acknowledgments
We thank the Age Well Simply support group for their ongoing support of this patient, especially Dan Percival. We also thank Dr. Brian Mann for visual analysis, April Barna for visual training of the patient, and Karen Rowan for cranial sacral therapy. We thank the Apollo Health Company for development of the ReCODE reports and Molly Susag for manuscript and image preparation.
Conflicts of Interest
DEB is a consultant for Apollo Health and Life Seasons, neither of which was involved in this study or had any access to the study findings.
Abbreviations
The following abbreviations are used in this manuscript:
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| C4a | complement factor 4a |
| CIRS | chronic inflammatory response syndrome |
| CT | computed tomography |
| DHEA | dehydroepiandrosterone |
| DMSA | dimercaptosuccinic acid |
| EDTA | ethylenediaminetetraacetic acid |
| EWOT | exercise with oxygen therapy |
| HOMA-IR | homeostatic model assessment of insulin resistance |
| IgM | immunoglobulin M |
| LDL | low-density lipoprotein |
| mg | milligram |
| mL | milliliter |
| mM | millimolar |
| MMP-9 | matrix metalloprotease-9 |
| MRI | magnetic resonance imaging |
| NAD | nicotinamide adenine dinucleotide |
| ng | nanogram |
| PCA | posterior cortical atrophy |
| pg | picogram |
| PPA | primary progressive aphasia |
| Prof. | professor |
| SpO2 | oxygen saturation of peripheral capillaries |
| TGF-b1 | transforming growth factor-beta-one |
| TSH | thyroid-stimulating hormone |
| WBC | white blood count |
References
- Benson, D.F.; Davis, R.J.; Snyder, B.D. Posterior cortical atrophy. Arch Neurol 1988, 45, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Best, J.; Chapleau, M.; Rabinovici, G.D. Posterior cortical atrophy: clinical, neuroimaging, and neuropathological features. Expert Rev Neurother 2023, 23, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Staff, M.C. Posterior cortical atrophy. Available online: https://www.mayoclinic.org/diseases-conditions/posterior-cortical-atrophy/symptoms-causes/syc-20376560 (accessed on November 2024).
- Association, A.s. Posterior Cortical Atrophy. Available online: https://www.alz.org/alzheimers-dementia/what-is-dementia/types-of-dementia/posterior-cortical-atrophy (accessed on November 05).
- Mendez, M.F. Early-onset Alzheimer Disease and Its Variants. CONTINUUM: Lifelong Learning in Neurology 2019, 25, 34–51. [Google Scholar] [CrossRef] [PubMed]
- Bredesen, D.E. Inhalational Alzheimer’s disease: an unrecognized - and treatable - epidemic. Aging (Albany NY) 2016, 8, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Bredesen, D.E.; Toups, K.; Hathaway, A.; Gordon, D.; Chung, H.; Raji, C.; Boyd, A.; Hill, B.D.; Hausman-Cohen, S.; Attarha, M.; et al. Precision Medicine Approach to Alzheimer’s Disease: Rationale and Implications. J Alzheimers Dis 2023, 96, 429–437. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Increase in parietal lobe volume following treatment for 15 months. (A) Pre-treatment MRI volumetrics show the highlighted area of atrophy, which is in the parietal lobe. (B) Post-treatment shows no atrophy of the parietal lobe. (C) Pre-treatment graph of parietal lobe volume shows marked atrophy. (D) Post-treatment graph of parietal lobe volume shows borderline normal volume.
Figure 1.
Increase in parietal lobe volume following treatment for 15 months. (A) Pre-treatment MRI volumetrics show the highlighted area of atrophy, which is in the parietal lobe. (B) Post-treatment shows no atrophy of the parietal lobe. (C) Pre-treatment graph of parietal lobe volume shows marked atrophy. (D) Post-treatment graph of parietal lobe volume shows borderline normal volume.
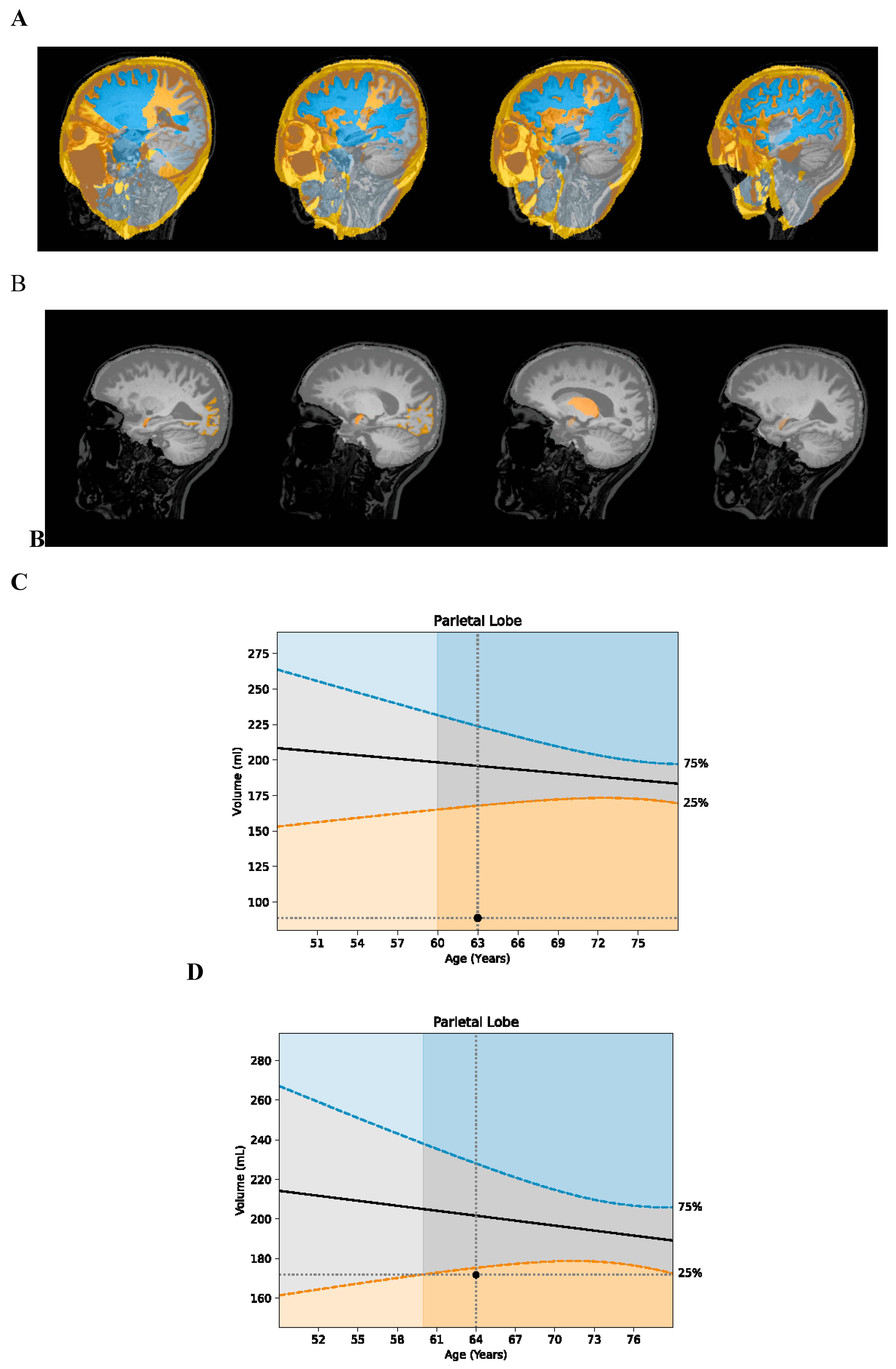
Figure 2.
Increase in hippocampal volume following treatment for 15 months. (A) Pre-treatment graph of hippocampal volume shows atrophy. (B) Post-treatment graph of hippocampal volume shows no atrophy.
Figure 2.
Increase in hippocampal volume following treatment for 15 months. (A) Pre-treatment graph of hippocampal volume shows atrophy. (B) Post-treatment graph of hippocampal volume shows no atrophy.
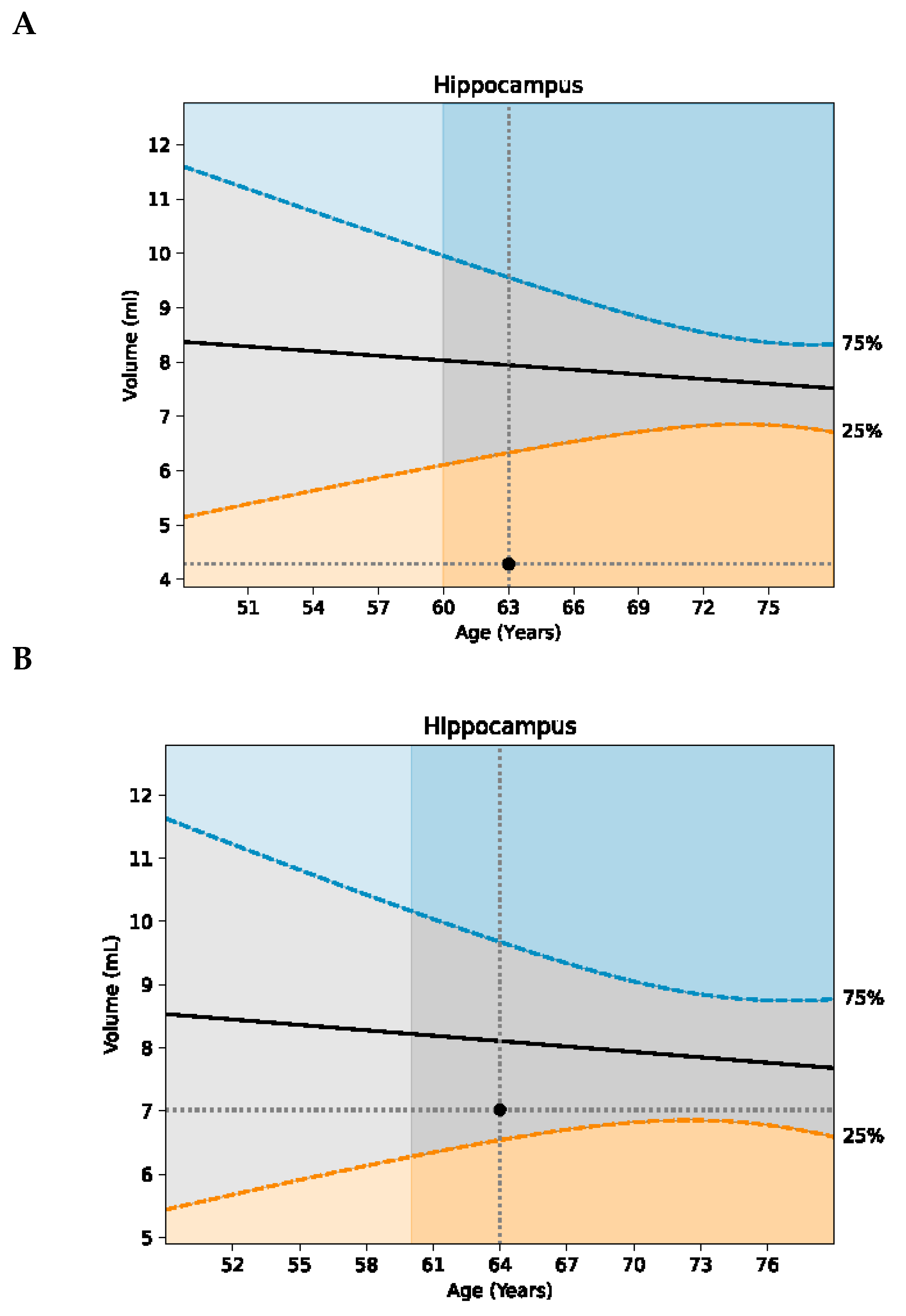

Table 1.
Function and MRI volumetrics (percentiles) prior to and post/during treatment..
| Function 1 | Prior to treatment | After 15 months of treatment 3 |
| Reading | Unable to read※ | Reading voraciously |
| Using a computer | Unable | Able |
| Brain training | Unable | Able |
| Structure | Percentile for age | Percentile for age |
| Total brain | 7.82 percentile | 24.79 |
| Gray matter | 24.14 | 37.98 |
| Frontal lobes | 13.40 | 26.19 |
| Temporal lobes | 41.64 | 23.27 |
| Parietal lobes | 0.49 | 22.23 |
| Occipital lobes | 10.81 | 25.30 |
| Hippocampus | 6.29 | 31.96 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



