
Submitted:
12 August 2025
Posted:
13 August 2025
You are already at the latest version
Abstract
Background/Objectives: Transdermal bicarbonate (TBC) or carnosine (TC) have been sold as a convenient way to improve performance, though little evidence indicates they are ef-fective. The purpose of this study was to investigate if TBC or TC, applied as advertised, improve high-intensity endurance cycling. Methods: Using the Zwift online platform, fif-teen cyclists completed four ~50-km cycling trials that included three long sprints and three short climbs, plus a final lap time trial (TT). Trials included a familiarization (FAM) trial followed by three randomized trials using a TBC, TC, or placebo (PLAC) lotion. Trial data were analyzed using general linear models to compare differences between condi-tions across ~50-km cycling trials. Results: Mean ± SD 60-min mean max power (MMP) was 2.9 ± 0.9 W/kg and ranged from 1.3 to 4.1 W/kg. Trials were five 9.1 km laps lasting 89.8 ± 17.0 min long. Relative to MMP60, interval laps (2 – 4) were ridden at 86.4 ± 7.3% and climbs at 131.6 ± 21.1%, while sprints averaged 83.2 ± 17.7% of MMP30s. The lap 5 TT was ridden at 95.4 ± 8.7% of MMP20 and 87.5% ± 7.4% of MHR. While there were no statistical differences in performance between any treatment trial, FAM trials were significantly lower (p < 0.05) in power output measures, but not HR and RPE. Conclusions: Based on the available evidence from this and prior research, there appears to be no apparent ergogenic benefit from either TBC or TC during high intensity cycling performance.
Keywords:
Mixed-reality cycling
; Zwift
; transdermal bicarbonate
; transdermal carnosine
; human performance
1. Introduction
The sports supplement industry was valued at $45.2 billion in 2023 and is expected to grow 7.5% from 2023 to 2030 [1]; however, regulation of most supplements is relatively nonexistent and efficacy is often dubious, with the burden of proof placed on the consumer [2]. This makes empirical testing of manufacturer claims essential. While standard practice in the past has been to rely on “gold standard” exercise laboratory testing, such restrictions limit evaluation due to the resources required and the challenges of recruiting suitable participants to visit the lab multiple times. For most sports supplements the most important reference standard is exercise performance, which is predictably reliable day-to-day [3,4]. Recent advances in technology have given affordable lab quality tools to everyday athletes; two of the more notable tools include bicycle power meters [5] and smart bicycle trainers [6,7,8]. The advent of these tools paired with mixed reality (MR) training platforms, like Zwift, transformed indoor leisure, fitness, and competitive cycling in the last decade [9,10,11,12]. The combination of technologies now allows for remote exercise performance studies to be conducted across the world with a wide range of athletic abilities. As such, it is now possible to perform sport-related evaluations, like testing sports nutrition products, remotely.
Competitive road (indoor/outdoor) cycling relies on a complex mixture of endurance and power determinants, as well as resilience to maintain optimal performance levels near the end of a race, which has been termed “durability” [13,14,15,16,17]. It has been shown that cyclists with higher durability are more likely to be successful [15,17]. Both amateur and professional cyclists perform a variety of training sessions to improve overall performance and consequently, durability. Therefore, any ergogenic aid that can reduce fatigue could improve one’s final TT durability.
Previous work by Stellingwurf et al. [14] suggested evidence-based approaches to utilizing specific supplements to aid performance. One common target is “lactic acid”, which nearly instantaneously dissociates into H+ and La- (lactate), because of the outdated notion that lactate causes fatigue. While lactate has been exonerated as a cause of fatigue [18,19], evidence suggests that increases in H+, which decreases pH, may negatively impact several aspects of muscle power output [19,20]. Therefore, supplements employing buffering agents like bicarbonate (BC) and carnosine, or its precursor beta-alanine (BA), have often been utilized in sport and exercise settings.
Evidence for the use of both BC and BA under specific conditions, generally very high-intensity continuous or intermittent exercise of durations from 30-sec to 10-min [21,22,23,24], however, more recent evidence indicates that certain events lasting longer than 10-min may also benefit [22,23]. The evidence for longer duration activity seems contradictory, but likely relates specifically to sports like cycling that include both intermittent and continuous high-intensity bouts of up to 10-min; examples include repeated sprints, short, steep climbs, or a final burst of power in the final 5-k of the race. Taken together, buffering
supplements would theoretically improve repeated high intensity efforts or improve power in the finale (i.e., durability). To date, however, the preponderance of the evidence has been with ingested BC and BA; nevertheless, topical lotions have also been developed and marketed to athletes for at least a decade and claim similar benefits without commonly reported side effects of either buffer type [18,25].
A thorough review of the literature indicates a paucity of evidence that transdermal BC (TBC) can increase blood pH when applied at twice the dose described on the product bottle (20 g) [26], while another study using thoroughbred racehorses indicated that transdermal carnosine (TC) increased muscle carnosine levels by 46% 60-min after application [27], though no dose was reported. Despite some evidence of absorption, there is no meaningful evidence that either lotion improves exercise performance. For example, Gurton and colleagues published two somewhat conflicting studies on team sport athletes (e.g., hockey, soccer, basketball) showing that oral sodium bicarbonate (OBC) ingestion and TBC results in small, but significant improvement in repeated high-intensity performance [28], though only the OBC resulted in increased pH. The authors speculated that the interaction between the lotions menthol and sodium may have altered effort perception, but this has yet to be tested. However, a similar follow-up study in soccer players failed to replicate these findings, only showing improvement from OBC [29]. In contrast, Seah [30] failed to show any benefit from TBC to intermittent high-intensity sprints in team sport athletes. Finally, both McKay et al. [31] and Kern et al. [32] examined both changes in the acid-base balance and cycling performance in trained cyclists who performed three 30-sec maximal sprints. Like prior research, no changes were seen in any of variables following application of the TBC lotion, though Kern did demonstrate possible increased blood pH.
Research on TC is even more limited but no less equivocal. Initial research by Sharpe and Macias [33], both associated with the development and sale of the product, suggested that TC significantly improved repeated sprint and 1000-m running performance in elite male soccer players. However, the study used sequential, unblinded sessions, where the TC trials were performed last, possibly resulting in an ordering effect. Additionally, the authors appear to report clinical and statistical significance synonymously without explanation or context and the limited methodological details coupled with confusing findings make it difficult to draw meaningful conclusions from this study. A follow-up study by Harnish and Miller [34] using a randomized controlled cross-over design recruited well-trained cyclists to perform three sessions of five maximal 30-sec Wingate sprints. Here the study failed to show any difference between trials in either performance, rating of perceived exertion (RPE; 1-10 scale), blood lactate concentration. More recent data from an unpublished master’s thesis [35] also failed to provide substantial evidence that TC improves repeated sprint performance in rugby players. Most notably, only three of the twelve 6-sec sprints showed significantly higher peak power than the placebo (PLAC) group and there were no differences in average sprint power.
As noted at the outset, sports nutrition supplements are ubiquitous and rely on more marketing hype than science-based evidence. As we have noted here, transdermal buffering lotions would offer a convenient, easy, and cost-effective way to improve performance if they worked as marketed. However, few studies have specifically tested products as marketed, and under sports specific performance challenges. Therefore, the purposes of this study were to use a randomized controlled cross-over trial to investigate whether either TBC or TC, when applied as instructed by company recommendations, would improve either high-intensity intermittent cycling or final time trial performance during a ~50-km cycling trial using the Zwift MR cycling platform. Based on the available research obtained in an ad hoc literature review, we hypothesized that neither TBC nor TC would elicit a significant improvement in performance, heart rate (HR), or RPE differences beyond a similar PLAC lotion.
2. Results
2.1. Baseline Participant Physical, Performance, and Training Characteristics
A total 14 men and 1 woman (n = 15) enrolled and completed the study. Table 1 summarizes the baseline physical, performance, and training characteristics of these individuals. Non-parametric statistical analysis indicated that Zwift Category A riders exhibited a significantly higher 30-sec mean maximal power (MMP30s), as well as 20 and 60 min MMP (MMP20 and MMP60, respectively) than category D riders (see section 4.1 for Zwift Category classification details).
2.2. Overall Trial Characteristics and Outcomes
All participants completed testing without any adverse events reported; however, individual trial data (i.e., Zwift files) for 2 participants were lost due to technical issues. In addition, 1 of these participants also failed to complete their self-report trial training log resulting in additional data loss. Both participants declined to repeat these trials resulting in the overall loss of all data associated with 1 TBC trial as well as 1 PLAC trial and training log. Two additional participants HR data were lost due to technical failure for their familiarization trial (FAM) only (1 participant: laps 1 – 5; 1 participant: laps 2 – 5). All analyses were still carried out following an intention to treat paradigm. Trial-by-lap data are summarized in Table 2.
2.2.1. Trial Characteristics
Neither environmental temperature (67.6 ± 5.4°F; 1 missing report: 1 PLAC trial) nor trial weight loss (-0.6 ± 0.6 kg; 2 missing reports: 1 FAM trial, 1 PLAC trial) differed significantly across trials (respectively, p = 0.969 and p = 0.941. Participants also ingested similar amounts of fluid (0.9 ± 0.5 L) and carbohydrates (40.8 ± 38.0 g; across all trials (respectively, p = 0.849 and p = 0.879). Overall, trials lasted 89.8 ± 17.0 min in duration. And for all lotion trials (TBC, TB, and PLAC), participants allowed their assigned creams to absorb a similar amount of time before beginning each trial (74.4 ± 11.0.2 min; p = 0.776).
2.2.2. Trial Average Power (Laps 2 – 4)
Results of a 4x3 repeated measures ANOVA produced significant main effects for differences by trial condition (p < 0.001, η²p = 0.929) with post hoc pairwise comparisons showing that FAM trials were significantly lower (p < 0.05) than TBC, TC, and PLAC trials. However, no differences (p > 0.05) were observed across laps based on trial condition (p > 0.05), thus there were no significant differences in average power for laps 2 – 4 (p = 0.316).
2.2.3. Trial Average HR and RPE (Laps 2 – 4)
ANOVA produced non-significant differences for both HR by trial condition (p = 0.782) and RPE (p = 0.499).
2.3. Hill Climb Segment Charactersitics and Outcomes
2.3.1. Hill Climb Segment Average Power (Laps 2 – 4)
Hill climb segments were ridden at 131.6 ± 21.1% of MMP60 ANOVA produced significant differences in average hill climb by trial condition (p < 0.001, η²p = 0.606), with post hoc pairwise comparisons showing that FAM trials were significantly lower (p < 0.001) than TBC, TC, and PLAC trials, while TBC trials were significantly higher (p = 0.038) than TC trials hill climb at 7.7 W. There were no significant differences between TBC and PLAC (p = 0.697) or TC and PLAC (p = 0.310).
2.4. Sprint Segment Charactersitics and Outcomes
2.4.1. Sprint Segment Average Power (Laps 2 – 4)
Sprint lap segment average power (laps 2 – 4) were ridden at 86.4 ± 7.3% of MMP30s. ANOVA results indicated significant differences in sprint power by trial condition (p < 0.001, η²p = 0.843), where post hoc comparisons revealed significantly lower sprint power for FAM trials compared to TBC trials (p < 0.001) and PLAC trials (p = 0.007), but not TC trials (p = 0.131). No significant differences were noted between TBC and TC trials (p = 0.259) or TC and PLAC trials (p = 0.725).
2.5. Time Trial Charactersitics and Outcomes
2.5.1. Time Trial Average Power (Lap 5)
The lap 5 TT was 15.7 ± 3.1-min in duration and ridden at 95.4 ± 8.7% of MMP20 and 87.5% ± 7.4% of MHR. Lap 5 TT power was not significant different (p = 0.697) across trial conditions.
2.5.2. Time Trial Average HR and RPE (Lap 5)
Result of ANOVA indicated significant main effects for TT HR (p < 0.001, η²p = 0.994) but no significant individual effects (p > 0.05). RPE results also indicated significant main effects (p < 0.001, η²p = 0.989) where FAM trial RPE was significantly lower than TC trial RPE (p = 0.026) with no other significant differences. Overall trial RPE was not significant different between trial conditions (p = 0.068); FAM = 6.8 ± 1.1, TBC = 7.0 ± 1.6, TC = 7.2 ± 1.3, PLAC = 6.6 ± 1.6.
2.9. Placebo Effects
For the purposes of this study, we considered accurate identification of supplement and PLAC as those individuals who correctly identified all three correctly; only two individuals achieved this, and one admitted he had used one of the products in the past. Overall, from the 44 reported total applications, 25 “believed” they received a real supplement with 20 of those being correct, however, results of Fisher’s exact test comparison, participants were equally likely to accurately identify a lotion correctly (p = 0.101), as well as identify any of the three lotions as a supplement (p = 0.922); see supplemental PLAC data for more results. As a secondary analysis, however, we wanted to examine whether trials where individuals believed they received an actual supplement performed better than those who believed they received a PLAC. Here, those who believed they received a real supplement (“Yes” = 24 vs “No” = 19) performed similarly across all aspects of each trial with the largest, albeit non-significant difference in the Lap 5 TT; 233.7 ± 69.5 W vs. 221.5 ± 72.8 W (p = 0.579). While not significant, there was a mean advantage ranging from 2.4% in sprints to 5.5% in the TT, with wide variations (CV% = 20.7 vs 23.9%) across participants including several negative responders; Appendix B1, Placebo related analyses, presents extensive graphic representations of PLAC and supplement ratings data.
3. Discussion
The purposes of this study were to investigate the ergogenic effects of both TBC and TC on a 50 km cycling trial that included three 300 m sprints and three 900 m hill climbs, as well as a final 9.1 km TT using the Zwift MR cycling platform. Participants applied the lotions based on instructions provided by the company and completed the supplement lotion trials in a randomly determined order Based on the available research, the authors hypothesized that neither TBC nor TC would elicit any measurable performance, HR, or RPE differences from individuals provided with similar a mentholated PLAC.
3.1. Trial Data
We believe our trials were able to test whether the claims made for these marketed products improved performance for high intensity repeated and sustained efforts, as well as overall endurance. Zwift’s MR platform combined with a smart bicycle trainer allowed participants to complete a 90 – 120-min trial that included short steep climbing efforts at ~132% MMP60 and long sprinting efforts at ~83% of MMP30s over nearly 30-km before concluding with a 10-km TT performed at over 95% MMP20, 90% MHR, and an RPE over 8. Indoor trials provided a controlled thermal environment where weight loss was negligible, indicating dehydration did not play a significant role in performance.
3.1.1. Laps 2 – 4 Repeated Efforts and Endurance
As noted, each trial consisted of three laps that included one 900-m steep climb ridden as fast as possible, followed by 4-km of steady riding before a 300-m sprint. The purpose was to examine whether either TBC or TC, buffers, outperformed a PLAC regarding higher average power for these six high-intensity intervals. Based on our results there was significant improvement in performance from FAM trials but largely negligible improvement in hill climb or sprint power. Specifically, average hill climb power for our TC group was about 8 W lower than the other condition groups, which could be accounted for daily variation [3] or small accuracy differenced in the bicycle trainer used [8]. Similarly, Wingate-type sprints, like we used, can vary as much as 10% [36], thus the 4.8% difference between our PLAC and TC group is reasonable. Additionally, there were no discernible differences average lap power, HR nor RPE.
3.1.2. Durability of Time Trial Performance
Cyclists who exhibit greater durability during events are more likely to succeed [15,17] therefore, any ergogenic aid that can reduce fatigue and preserve MMP would improve one’s final TT durability. Based on the marketing claims of both TBC and TC, we should expect an improvement in 10-km TT power output following ~30-km of “moderate-hard” cycling (RPE ~6.4) with six hard intervals. However, our findings indicate that neither TBC nor TC offer any ergogenic benefit to performance with both power, HR, and RPE remarkably similar across all TT’s, which were ridden at nearly MMP20.
Taken together, these data align with the majority of past research on both TBC [29,30,31,32] and TC [34]. However, close inspection of the other studies does not lend strong support for performance enhancement of repeated sprints, as one study showed only a trivial 1.9% improvement for TBC [28], while another using TC [35] showed significant increases in peak power for just three of twelve 6-sec bike sprints in rugby players, but no differences in average 6-sec power. Finally, an early study in elite soccer players using TC [33] showed significant improvements in 1000-m running TT performance but not repeated sprints. However, significant methodological issues call into question the validity of these data, including a lack of randomization, blinding, or placebo lotions, where TC trials were conducted last and produced improvements as great as 15% in one subject.
3.2. Performance Replication and Perceived Effort
An important aspect of this study was its relative difficulty, including several high-intensity repeats of 30-sec to 3-min in duration, a final maximal TT, and an overall trial time of 90 – 120-min. Across all trials we saw no significant difference in session RPE which ranged from 6.6 for FAM, up to 7.1 for TC trials. Nonetheless, our participants demonstrated an ability to produce consistent performances after just a single familiarization trial. Thus, we are confident that these data demonstrate the quality of our study design and resulting conclusions.
3.3. Placebo Effects and Menthol
One of the challenges of supplement studies are potential PLAC (or nocebo) effects that have been shown to result in moderate effects which could result in 5% or greater performance changes [34,37,38,39]. In the present study, participants were asked whether they believed they received the supplement or PLAC, as well as to provide qualitative and quantitative feedback on their opinions of the supplement. There were no overall differences in any performance measures between those who believed they received the actual supplement, though there appeared to be large variations across all subjects indicating that individual responses to PLAC effects could provide significant benefit to those who believe a supplement works. One interesting finding, however, was that supplement ratings and potential performance effects were independent of the ratings, where TBC was rated significantly lower than the other two lotions. In other words, individuals do not need to “like” or “prefer” a supplement for it to be effective. However, this may not apply to nocebo’s, as an earlier study on TC by the lead author [34] noted that the four negative responders all reported a significant dislike of menthol; it is noteworthy that no participants in the present study expressed negative comments regarding menthol.
An interesting unintended set of results from this study were the varying concentrations (dose) of menthol received from each lotion, ranging from 0.8% for TBC, 1% for P, and 1.25% for TC. In addition to lack of effect from supplement ingredient and PLAC effects, there also did not appear to be any effect from topical application of menthol across dosages either. This finding supports prior research showing no performance enhancement when apply topical menthol in a range of conditions [40,41,42]. One of the earlier TBC studies [28] suggested that the interaction between the menthol and TBC could explain their reported significant 1.9% improvement in repeated sprint performance. However, this seems unlikely based on the literature and the present study, in particular. Moreover, performance gains of less than 2% could be accounted for by random daily variation or a PLAC effect, noting that our smallest, and non-significant, PLAC effect was 2.4%.
3.4. Does Transdermal Delivery Make Sense for Buffers?
There is great appeal for transdermal application over either oral or hypodermic injection [43]. Specific to either bicarbonate or carnosine, ingestion can either be potential detrimental due to GI distress [25] or an inability to absorb the supplement in the gut [18,27], respectfully. Therefore, transdermal application would offer a convenient delivery route. As is typical for first and second-generation transdermal delivery systems, however, both TBC and TC are limited by the inherent challenges of skin absorption, as both topicals are hydrophilic and delivered in high doses, while carnosine is a peptide [43,44]. Based on the available ingredient lists, both products presumably attempt to enhance absorption using lipid and/or alcohol-based chemical enhancers. Nonetheless, evidence for absorption of either product is limited.
A recent paper by Gibson et al. [26] indicated a significant change in pH utilizing a TBC dosage 80 ml (~26.4 g of BC), which was only slightly more than most of the TBC performance research [28,29,31]. However, the small sample size, discrepancies between the paper and the raw data (provided by the authors), and the lack of an exercise challenge make conclusions impossible. Results from Kern et al. [32] showed a small, but significant change on blood acid-base markers but no performance improvements. What is intriguing, however, is that while Gibson et al. used a dosage four-times higher than manufacture recommendations, Kern et al. used a dosage of just 16.6 ml (5.5 g BC), which was also less than the 20 ml used in the present study. Therefore, based on the available evidence, we cannot say whether TBC alters blood buffering capacity.
Unlike TBC, absorption of TC is limited to a single study on equine published by Dieter et al. [27] indicating that application of the same TC used in the present study increased intramuscular carnosine concentrations by 46%. While this increase is on par with chronic oral BA ingestion [18], there is cause for skepticism. First, it is unclear what dosage of TC was used in the study. The authors note that the TC product used contained a 1.5% carnosine-complex concentration, which as used in the present study would be 0.15-g of carnosine in 10-ml of gel. Assuming this is an effective dose for a 70-80-kg human, then a dose 6-fold higher should be needed for a 500-kg horse. As noted in the paper, however, the lead author Dieter has direct ties to Velocity Animal Sciences, which markets an identical TC product that advises an application of 40 to 60-ml should be used [45]. The authors state that the gel was applied to a 25-cm2 area; this is implausible because just 10-ml of this gel easily coats ~3800-cm2 (i.e., both lower extremities). Thus, based on the limited evidence, we cannot know whether TC is absorbed into the muscles.
3.5. Assimilation of Present Finding with Prior Transdermal Research
As noted above, the present study failed to show any indication of performance improvement from either TBC or TC when compared to PLAC. This finding was not surprising based on all the published research we could identify, including this study; these studies are summarized in Table 3 with primary findings and a rated for quality using the Downs and Black methodological quality checklist [46]. Six of these studies tested TBC and 4 TC, with studies comparing TBC to oral BC (OBC), and only the present study comparing TBC and TC with PLAC. Four of the TBC and one of the TC studies reported using a matching PLAC, however, based on our own experience with both products and unpublished data testing TBC and TC blinding, it is unlikely any lotion with BC would feel or apply like an identical lotion without BC. Five of the studies were industry funded, but only one [33] failed to disclose their conflict of interest, which was also the only study not to use either a randomized trial or identifiable PLAC. Three studies were not peer-reviewed [30,32,35] and one had no detailed data published [30]. We were, however, able to obtain an unpublished manuscript for Kern et al. [32] and the complete dataset for Brockelbank [35], but we received no response from the other TC-related studies [27,33]. From these data were able to able to assess the quality of the reported findings and confirm their results. We note that despite the small (<2% improvement) seen in repeated sprint performance, the results were well within the range of a PLAC effect [37,38], or as noted by the Gurton et al. (2003) [28], possibly due to the menthol in the product, as there was no evidence of change in acid-base balance. Finally, based on the limited details provided about their study design, gaps in their reported results, and the rather remarkable individual responses of some of their subjects (> 10%), we fundamentally question the conclusions by Sharpe et al. that the TC lotion employed enhances sport performance [33]. Taken together, we believe there is insufficient evidence that either TBC or TC provided any performance enhancement in either intermittent sprint or endurance sport conditions.
3.6. Novelty and Limitations
This is one of just a few studies to adopt a remote approach to conducting an RCT, as well as one of growing number of studies utilizing MR platforms like Zwift [10]. Such virtual environments create exciting new opportunities to conduct large scale cycling and possibly running trials in relatively controlled environment on virtual riding routes. At the time of the study design, it was believed that such a platform would expand the potential subject pool. However, one significant limitation of our study proved to be converting interested participants into enrolled and completed participants. Other specific limitations to the study included a lack of physiological data like VO2 and blood lactate, or markers of acid-base balance. Nonetheless, a primary purpose of the study was to test marketing claims against actual performance outcomes in a challenging trial. Finally, we acknowledge that our study lacked blinding of the research team and employed supplements that were easily distinguishable from one another. However, the impact of this limitation may have been of little consequence as most participants (13/15) failed to accurately identify all the lotions correctly, with more than half preferring or identifying the PLAC as a supplement as well.
3.7. Applications and Implications
The major applications and implications of this study are that neither TBC nor TC appear to have any discernable performance effect beyond a potential and highly variable PLAC effect. Thus, athletes and coaches should use these results to make informed choices on whether a product is worth the expense of purchase. The authors cannot discount the potential benefits of a PLAC effect in sports and thus make no specific judgement or recommendation for or against the use of any of these lotions, including the PLAC, to achieve that effect. Finally, as previously noted, our participants demonstrated that a single familiarization trial may be sufficient for even novice cyclists to perform replicable performance trials. This should encourage researchers to employ the use of MR platforms, like Zwift, for future research.
4. Materials and Methods
4.1. Ethics Approval and Participant Characteristics
All methodology was reviewed and approved by the Mary Baldwin University (Staunton, VA, USA) Institutional Review Board (IRB). All participants were self-reported trained cyclists recruited between May 2023 and April 2025 from across the continental USA via social media and met the following inclusion criteria: apparently healthy men and women between 18 – 55 years of age; self-reported weekly bicycle training experience such that they could cycle continuously for over 2-hrs; and had access to both a high-quality smart trainer and the Zwift virtual cycling platform (Zwift, Inc., Long Beach, CA, USA). However, individuals meeting all other criteria without access to Zwift were offered free access two-weeks prior beginning their trials through completion of the study. Exclusion Criteria included: individuals outside the inclusionary age range; and those self-reporting any known medical condition that would preclude participation (e.g., acute musculoskeletal injuries, illness, etc.). All participants were informed of the purposes and requirements of the study and provided written consent prior to enrollment.
Once enrolled, participants completed an intake survey which provided the research team with basic physical and demographic information, endurance training characteristics, and details of recent cycling performance (see Appendix A.1). They were then provided with a unique ID number used for all trial records and study files [47]Within the context of this study, MMP values were derived from participants’ self-reported highest sustained power output for 60-min, or functional threshold power (FTP), across a 4-wk period prior to testing; where MMP60 was considered equal to FTP [47,48]. If participants were unable to provide this information, then the highest recorded power during the FAM trial was used to estimate this value. Additionally, participants were stratified into the original Zwift Categories based on individual functional threshold power (FTP) output defined as: Zwift A ≥ 4.0 W/kg; 3.9 W/kg ≥ Zwift B ≥ 3.2 W/kg; 3.1 W/kg ≥ Zwift C ≥ 2.5 W/kg; and Zwift D < 2.5 W/kg [48]. Participants’ MHR was similarly defined as the highest self-reported HR during exercise within the 3-months preceding enrollment or as the highest recorded measure across all trials in the study.
4.2. Study Design
During development of the project, it was decided that in addition to statistical significance, a performance improvement of 3 – 5% was likely necessary to demonstrate the efficacy of any one of the lotions provided (i.e., clinical significance) [37]. This improvement threshold was chosen based on prior research [34], as well as to accommodate 3 factors: potential day-to-day variation in performance [3]; potential placebo/nocebo effects [34,37]; and typical reported error for bicycle power meters and smart trainers [5]. A sample size calculation was conducted using this efficacy threshold in JMP Pro (version 17.0; SAS Institute Inc., Cary, NC, USA) which indicated that at least 14 participants were needed to achieve statistical power (β = 0.80; α = 0.05). This assumed that repeated measures analyses of variance (RM-ANOVA; within-factors) would be used to analyze cycling performance changes using power output data.
This study employed a randomized (Research Randomizer, www.randomizer.org) single-blind placebo-controlled 3 x 3 block crossover design with enrollment of no more than 5 participants at a time. Each participant completed 4 trials included an initial FAM trial followed by the 3 counterbalanced lotion trials using a TBC supplement, a TC supplement, and a PLAC (see Figure 1). While a single researcher (CRH) was aware of which condition was provided to each subject, all trials were completed remotely from across the continental United States, so no direct interaction occurred regarding lotions. All trials were conducted within the same 9.1 km MR Zwift course called “Hilly Route” (see Figure 2), where a total of 5 laps were completed for each trial.
4.3. Trial Details
Participants were provided detailed instructions on how each trial should be completed as part of the consent process and with a one-page “Quick Start” sheet that specifically outlined the order randomized-blinded lotions trials following the FAM trial. Participants were advised to maintain their usual diet and to complete all trials within the same time of day (±2 hrs) [49]. All trials were conducted indoors within temperature-controlled settings. Participants were instructed to use at least 1 high-powered fan during their ride, drink water ad libitum, and consume at least 30 – 60 g of carbohydrates during each trial. Participants were asked to maintain this pattern across all 4 trials. The FAM trial was always completed first to minimize any performance or learning improvements [50,51,52,53]. Following the first trial (always a FAM trial), data were reviewed for any irregularities or deviations from trial instructions, with feedback or recommendations being communicated to participants at this time only (no further feedback was provided following subsequent trials).
As noted above and in Figure 1, each trial consisted of 5 laps along a 9.1 km virtual loop that included one 900 m hill climb and one 300 m flat sprint; these segments had distinct start and finish banners. Participants were instructed to complete lap 1 at a self-determined “easy pace” as a warm-up. Upon completing lap 1 (noted by start and finish banners) they were asked to maintain about 70% of their MMP20 for laps 2, 3, and 4, except for the hill climb and sprint segments; during which participants were instructed to “race” as fast as possible. For the final lap (lap 5), participants completed a maximal time trial (TT) with explicit instructions to evenly pace themselves across the entire 9.1 km course (i.e., not race segments); fixed duration and distance TT’s have been shown to produce highly reliable performance outcomes [54,55,56].
Each participant provided their own bicycle attached to their own smart trainer as well as their own HR monitor. Power output and HR data were recorded continuously through the Zwift app via a Bluetooth low energy connection and subsequently uploaded using trial training logs (see section 4.4). Participants were also instructed to record their RPE (1 – 10 scale) following each lap and overall for each trial at least 30-min after each trial using provided trial training logs (see section 4.4 and Appendix A.2) [57]. Each trial session file was uploaded using the trial training log form and then subsequently transferred to a private Strava account (Strava Inc., San Francisco, CA, USA) where data for each lap and segment were extracted for later analysis.
4.4. Trial Training Logs
Each participant was provided a link to a Google form that could be easily completed during and/or after each trial and included a final section for Zwift file (.fit) uploads (see Appendix A.2). Each trial training log included the following data points to be collected:
- Supplement application and Trial start times.
- Trial designation (FAM, X, Y, or Z).
- Supplement rating and comments, and belief it was a supplement or PLAC.
- Environmental temperature as well as pre- and post-trial body weight.
- The Zwift virtual bike and wheels used (kept unchanged across trials as they affect game speeds).
- RPE (1 – 10) for each lap and overall trial RPE [57].
- The volume of fluids consumed and details on carbohydrate intake.
4.5. Supplmenent and Placebo Lotions
The supplement lotions used in this study were readily available on the market that included a TBC lotion containing 0.5% menthol (AMP PR, Momentous, Park City, UT, USA) and TC gel containing 1.25% menthol (LactiGo™, Outplay Inc., Las Vegas, NV, USA). Because the appearance, consistency, smell, and menthol content of the two supplements was completely different, a popular and easy to apply lotion containing 0.8% menthol (Muscle Moisturizing Shea Butter Lotion, The Village Co. LLC, Eden Prairie, MN, USA) was used for the PLAC. Unlike prior research, our purpose was to test market claims, thus each supplement was provided in precisely metered dosages using an Ozeri ZK14-T digital scale (Ozeri Corp, San Diego, CA, USA) as recommended on the packaging of each product (20 ml for TBC and 10 ml for TC), while 15 ml of the PLAC lotion was provided. Each participant was shipped the supplements using clear, BPA-free plastic jars marked only with the supplement letter codes X (TBC), Y (TC), or Z (PLAC). Participants were instructed to apply the entire contents of the supplement container to the legs and gluteus maximus no less than 1-hr prior to their expected trial start time; being sure to scrape the interior of the container to obtain any remaining lotion if needed. The application time and trial start times were recorded in the trial training log.
To assess how participant perceptions of each lotion may have influenced performance, they were asked to answer a series of questions about each lotion used in their trial logs (excluding the familiarization trial, trial 1; See Appendix A.2). Specifically, they were asked to comment on the lotion (e.g., like/dislike, the smell, texture, etc.), to rate the lotion between 1 – 5 stars (1 star: Bad; 5 stars: Great), and finally they were asked whether they believed they received the supplement or PLAC. Accurate supplement identification was only considered if the participant was able to identify all lotions accurately.
4.6. Performance Measures
Performance data across laps 2 – 5 used for analysis included entire lap average power (laps 2 – 4), hill climb segment and sprint segment average power (laps 2 – 4), TT average power (lap 5), entire lap average HR and RPE (laps 2 – 4), and TT average HR and RPE (lap 5). Data from laps 2 – 4 were also averaged and compared to the three MMP values reported in table 1. Specifically, hill climb segment average power was compared to MMP60 (i.e., FTP) and sprint segment average power was compared to MMP30s (i.e., Wingate).
4.7. Statistical Analyses
Data were screened and cleaned for accuracy and completeness prior to performing any statistical analyses. Descriptive statistics were computed as means ± SD for all physical characteristics and performance measures, unless otherwise noted. Due to small sample sizes within individual Zwift category classes, Kruskal-Wallace analysis was completed followed by a post hoc Dunn test for multiple comparisons, when significance was detected. One of the main outcomes to be tested was how TBC and TC versus PLAC would affect repeated hill climb power output and sprint power output, lap HR, and lap RPE for laps 2 – 4. Therefore, 4X3 repeated measure ANOVAs and partial eta-squared effect sizes were used to compare differences in each dependent variable (power, HR, RPE) by trial condition (FAM, TBC, TC, and PLAC) and lap (2 – 4) over time. A second main outcome to be tested was the effect of each of the four conditions on final TT performance, which was tested using 4X1 ANOVAs comparing average lap power, HR, and RPE. Mauchley’s Test of Sphericity confirmed equality the variance differences between all combinations of related groups. If violated, Greenhouse-Geisser adjustments were used [58]. Follow up pairwise comparisons and simple effects tests were planned using Tukey’s LSD for all significant main effects and interactions. Finally, analysis of potential placebo effects was performed using Fisher’s Exact test for categorical variables due to the small sample sizes within survey categories. Additional analysis comparing placebo effects of those who “believed” they used a real supplement versus those who did not was performed using paired T-tests. All statistical procedures were performed with the Statistical Package for Social Sciences (version 30; IBM Corp., Armonk, NY, USA) with α < 0.05 set a priori.
5. Conclusions
In conclusion, this study failed to show any evidence of performance enhancement for either TBC or TC lotions compared to PLAC in a group of trained cyclists completing a moderate duration endurance trial that included several repeated high-intensity efforts and a final time trial. However, the study does support the use of MR platforms like Zwift for the completion of cycling performance trials over a variety of virtual terrain settings.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org
Author Contributions
Conceptualization, C.H; methodology, C.H. and M.H.; validation, C.H., M.H, and M.B.; formal analysis, M.B.; investigation, C.H.; resources, C.H.; data curation, C.H.; writing—original draft preparation, C.H.; writing—review and editing, C.H., M.H, and M.B.; visualization, C.H., M.H, and M.B.; project administration, C.H. and M.H.; funding acquisition, C.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received technical support from Zwift, LLC in the form of free access for any participant that required a membership.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Mary Baldwin University IRB (IRB# MBU0000483804-042423CRH) on April 27, 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available in an online repository: https://osf.io/x4dqu/ (accessed on 8 August 2025).
Acknowledgments
The authors wish to thank Eric Min and Henry Nixon of Zwift, LLC for their support of this research. We also thank Dr. Martyn Beavin and Dr. John Halliwill for graciously sharing their data, as well as Dr. Mark Kern for sharing an unpublished manuscript for additional review.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BA | Beta-alanine |
| BC | Bicarbonate |
| END | Endurance trials ≥ 90-min |
| FAM | Familiarization trial |
| FTP | Functional threshold power equal 60-min maximal power |
| HI | High-intensity intervals |
| HR | Heart Rate |
| MMP | Mean maximal power |
| MMP20 | Mean maximal power for 20-min |
| MMP30s | Mean maximal power for 30-sec |
| MMP60 | Mean maximal power for 60-min |
| MR | Mixed reality |
| OBC | Oral bicarbonate |
| PLAC | Placebo |
| RCT | Randomized controlled trial |
| RPE | Rating of perceived exertion |
| RS | Repeated sprint |
| S | Sprint |
| TBC | Transdermal bicarbonate |
| TC | Transdermal carnosine |
Appendix A
Appendix A.1. Participant Intake Form
Sample participant intake survey completed with informed consent for enrollment.
Appendix A.2. Example Trial Training Log
Sample participant trial log completed and submitted after all 4 trials.
Appendix B
Appendix B.1
Placebo related analyses.
References
- Grand View Research Sports Nutrition Market Size, Share & Trends Analysis Report By Product Type (Sports Supplements, Sports Drinks), By Formulation, By Consumer Group, By Sales Channel, By Region, And Segment Forecasts, 2024 - 2030; Grand View Research, 2023; p. 140.
- Loraine, K. Supplement Regulation for Sports Nutrition Supplements. Journal of Legal Medicine 2018, 38, 271–285. [CrossRef]
- Paton, C.D.; Hopkins, W.G. Variation in Performance of Elite Cyclists from Race to Race. European Journal of Sport Science 2006, 6, 25–31. [CrossRef]
- Chase, J.G.; Moeller, K.; Shaw, G.M.; Schranz, C.; Chiew, Y.S.; Desaive, T. When the Value of Gold Is Zero. BMC Res Notes 2014, 7, 404. [CrossRef]
- Ferguson, H.A.; Harnish, C.; Chase, J.G. Using Field Based Data to Model Sprint Track Cycling Performance. Sports Med - Open 2021, 7, 20. [CrossRef]
- Morais, J.E.; Bragada, J.A.; Magalhães, P.M.; Marinho, D.A. The Accuracy and Reliability of the Power Measurements of the TACX Neo 2T Smart Trainer and Its Agreement against the Garmin Vector 3 Pedals. Journal of Functional Morphology and Kinesiology 2024, 9, 138.
- Zadow, E.K.; Fell, J.W.; Kitic, C.M. The Reliability of a Laboratory-Based 4 Km Cycle Time Trial on a Wahoo KICKR Power Trainer. Journal of Science and Cycling 2016, 5, 23–27.
- Hoon, M.W.; Michael, S.W.; Patton, R.L.; Chapman, P.G.; Areta, J.L. A Comparison of the Accuracy and Reliability of the Wahoo KICKR and SRM Power Meter. Journal of Science and Cycling 2016, 5, 11–15.
- Reed, J.; Dunn, C.; Beames, S.; Stonehouse, P. E ‘Ride on!’: The Zwift Platform as a Space for Virtual Leisure. Leisure Studies 2023, 42, 188–202.
- Devine, A.; Devine, F.; Burns, A. An Examination of the Virtual Event Experience of Cyclists Competing on Zwift. Event Management 2024, 28, 151–167.
- Westmattelmann, D.; Stoffers, B.; Sprenger, M.; Grotenhermen, J.-G.; Schewe, G. The Performance-Result Gap in Mixed-Reality Cycling–Evidence from the Virtual Tour de France 2020 on Zwift. Frontiers in Physiology 2022, 13, 868902.
- McIlroy, B.; Passfield, L.; Holmberg, H.-C.; Sperlich, B. Virtual Training of Endurance Cycling–a Summary of Strengths, Weaknesses, Opportunities and Threats. Frontiers in sports and active living 2021, 3, 631101.
- Joyner, M.J.; Coyle, E.F. Endurance Exercise Performance: The Physiology of Champions: Factors That Make Champions. The Journal of Physiology 2008, 586, 35–44. [CrossRef]
- Stellingwerff, T.; Bovim, I.M.; Whitfield, J. Contemporary Nutrition Interventions to Optimize Performance in Middle-Distance Runners. International Journal of Sport Nutrition and Exercise Metabolism 2019, 29, 106–116. [CrossRef]
- Barsumyan, A.; Soost, C.; Burchard, R. Enhanced Durability Predicts Success in Amateur Road Cycling: Evidence of Power Output Declines. Front. Sports Act. Living 2025, 7, 1530162. [CrossRef]
- Jones, A.M. The Fourth Dimension: Physiological Resilience as an Independent Determinant of Endurance Exercise Performance. The Journal of Physiology 2024, 602, 4113–4128. [CrossRef]
- Maunder, E.; Seiler, S.; Mildenhall, M.J.; Kilding, A.E.; Plews, D.J. The Importance of ‘Durability’ in the Physiological Profiling of Endurance Athletes. Sports Med 2021, 51, 1619–1628. [CrossRef]
- Trexler, E.T.; Smith-Ryan, A.E.; Stout, J.R.; Hoffman, J.R.; Wilborn, C.D.; Sale, C.; Kreider, R.B.; Jäger, R.; Earnest, C.P.; Bannock, L. International Society of Sports Nutrition Position Stand: Beta-Alanine. Journal of the International Society of Sports Nutrition 2015, 12, 30.
- Harris, R.C.; Sale, C. Beta-Alanine Supplementation in High-Intensity Exercise. Acute topics in sport nutrition 2012, 59, 1–17.
- Carr, A.J.; Hopkins, W.G.; Gore, C.J. Effects of Acute Alkalosis and Acidosis on Performance: A Meta-Analysis. Sports medicine 2011, 41, 801–814.
- Peart, D.J.; Siegler, J.C.; Vince, R.V. Practical Recommendations for Coaches and Athletes: A Meta-Analysis of Sodium Bicarbonate Use for Athletic Performance. The Journal of Strength & Conditioning Research 2012, 26, 1975–1983.
- Saunders, B.; Sunderland, C.; Harris, R.C.; Sale, C. β-Alanine Supplementation Improves YoYo Intermittent Recovery Test Performance. Journal of the International Society of Sports Nutrition 2012, 9, 39. [CrossRef]
- De Oliveira, L.F.; Dolan, E.; Swinton, P.A.; Durkalec-Michalski, K.; Artioli, G.G.; McNaughton, L.R.; Saunders, B. Extracellular Buffering Supplements to Improve Exercise Capacity and Performance: A Comprehensive Systematic Review and Meta-Analysis. Sports Med 2022, 52, 505–526. [CrossRef]
- Saunders, B.; De Oliveira, L.F.; Dolan, E.; Durkalec-Michalski, K.; McNaughton, L.; Artioli, G.G.; Swinton, P.A. Sodium Bicarbonate Supplementation and the Female Athlete: A Brief Commentary with Small Scale Systematic Review and Meta-analysis. European Journal of Sport Science 2022, 22, 745–754. [CrossRef]
- Grgic, J.; Pedisic, Z.; Saunders, B.; Artioli, G.G.; Schoenfeld, B.J.; McKenna, M.J.; Bishop, D.J.; Kreider, R.B.; Stout, J.R.; Kalman, D.S.; et al. International Society of Sports Nutrition Position Stand: Sodium Bicarbonate and Exercise Performance. Journal of the International Society of Sports Nutrition 2021, 18, 61. [CrossRef]
- Gibson, B.M.; Needham, K.W.; Kaiser, B.W.; Wilkins, B.W.; Minson, C.T.; Halliwill, J.R. Transcutaneous Delivery of Sodium Bicarbonate Increases Intramuscular pH. Front. Physiol. 2023, 14, 1142567. [CrossRef]
- Dieter, B.P.; Macias, C.J.; Sharpe, T.J.; Roberts, B.; Wille, M.; Young, A.; Reisenauer, C.; Cantrell, B.; Bayly, W.M. Transdermal Delivery of Carnosine into Equine Skeletal Muscle. Comparative Exercise Physiology 2021, 17, 429–434. [CrossRef]
- Gurton, W.H.; Greally, J.; Chudzikiewicz, K.; Gough, L.A.; Lynn, A.; Ranchordas, M.K. Beneficial Effects of Oral and Topical Sodium Bicarbonate during a Battery of Team Sport-Specific Exercise Tests in Recreationally Trained Male Athletes. Journal of the International Society of Sports Nutrition 2023, 20, 2216678. [CrossRef]
- Gurton, W.H.; Gough, L.A.; Siegler, J.C.; Lynn, A.; Ranchordas, M.K. Oral but Not Topical Sodium Bicarbonate Improves Repeated Sprint Performance During Simulated Soccer Match Play Exercise in Collegiate Athletes. International Journal of Sport Nutrition and Exercise Metabolism 2024, 34, 362–371. [CrossRef]
- Seah, J.Z.H. Effect of Sodium Bicarbonate in a Transdermal Delivery System on Physiological Par: A Double Blind, Placebo-Controlled, Randomised, Crossover Study. 2019.
- McKay, A.K.A.; Peeling, P.; Binnie, M.J.; Goods, P.S.R.; Sim, M.; Cross, R.; Siegler, J. Topical Sodium Bicarbonate: No Improvement in Blood Buffering Capacity or Exercise Performance. International Journal of Sports Physiology and Performance 2020, 15, 1005–1011. [CrossRef]
- Kern, M.; Misell, L.M.; Ordille, A.; Alm, M.; Salewske, B. Double-Blind, Placebo Controlled, Randomized Crossover Pilot Study Evaluating The Impacts Of Sodium Bicarbonate in a Transdermal Delivery System on Physiological Parameters and Exercise Performance: 2402 Board #238 June 1 11 00 AM - 12 30 PM. Medicine & Science in Sports & Exercise 2018, 50, 595. [CrossRef]
- Sharpe, T.M.; Macias, C.J. Evaluation of the Efficacy of LactigoTM Topical Gel as an Ergogenic Aid. J. Exerc. Physiol. Online 2016, 19, 15–23.
- Harnish, C.R.; Miller, B. Transdermal Carnosine Gel Fails to Improve Repeated Wingate Performance in Trained Male Cyclists: A Randomized Controlled Cross-over Trial. J. Sports Sci. Nutr. 2023, 4, 106–111. [CrossRef]
- Brockelbank, N. The Application of a Topical Carnosine Gel and Its Effects on Intermittent High-Intensity Exercise Performance in Olympic-Level Rugby Sevens Players, The University of Waikato, 2024.
- Ravindrakumar, A.; Bommasamudram, T.; Tod, D.; Edwards, B.J.; Chtourou, H.; Pullinger, S.A. Daily Variation in Performance Measures Related to Anaerobic Power and Capacity: A Systematic Review. Chronobiology International 2022, 39, 421–455. [CrossRef]
- Hurst, P.; Schipof-Godart, L.; Szabo, A.; Raglin, J.; Hettinga, F.; Roelands, B.; Lane, A.; Foad, A.; Coleman, D.; Beedie, C. The Placebo and Nocebo Effect on Sports Performance: A Systematic Review. European Journal of Sport Science 2020, 20, 279–292. [CrossRef]
- Halson, S.L.; Martin, D.T. Lying to Win—Placebos and Sport Science. International journal of sports physiology and performance 2013, 8, 597–599.
- Garcia Matta, G. Placebo Effects on Cycling Performance in Virtual-Reality and Laboratory Environments, Canterbury Christ Church University, 2023.
- Barwood, M.J.; Gibson, O.R.; Gillis, D.J.; Jeffries, O.; Morris, N.B.; Pearce, J.; Ross, M.L.; Stevens, C.; Rinaldi, K.; Kounalakis, S.N. Menthol as an Ergogenic Aid for the Tokyo 2021 Olympic Games: An Expert-Led Consensus Statement Using the Modified Delphi Method. Sports Medicine 2020, 50, 1709–1727.
- Jeffries, O.; Waldron, M. The Effects of Menthol on Exercise Performance and Thermal Sensation: A Meta-Analysis. Journal of science and medicine in sport 2019, 22, 707–715.
- Stevens, C.J.; Best, R. Menthol: A Fresh Ergogenic Aid for Athletic Performance. Sports medicine 2017, 47, 1035–1042.
- Prausnitz, M.R.; Langer, R. Transdermal Drug Delivery. Nat Biotechnol 2008, 26, 1261–1268. [CrossRef]
- Ramadon, D.; McCrudden, M.T.C.; Courtenay, A.J.; Donnelly, R.F. Enhancement Strategies for Transdermal Drug Delivery Systems: Current Trends and Applications. Drug Deliv. and Transl. Res. 2022, 12, 758–791. [CrossRef]
- Velocity Animal Sciences Inc. Equine Velocity Recovery Topical Emulgel: Equestrian Horse Wellness Available online: https://www.equinevelocity.com/ (accessed on 17 July 2025).
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. Journal of Epidemiology & Community Health 1998, 52, 377–384. [CrossRef]
- Pinot, J.; Grappe, F. The Record Power Profile to Assess Performance in Elite Cyclists. Int J Sports Med 2011, 32, 839–844. [CrossRef]
- Borszcz, F.; Tramontin, A.; Bossi, A.; Carminatti, L.; Costa, V. Functional Threshold Power in Cyclists: Validity of the Concept and Physiological Responses. Int J Sports Med 2018, 39, 737–742. [CrossRef]
- Reilly, T.; Atkinson, G.; Waterhouse, J. Chronobiology and Physical Performance. Exercise and sport science 2000, 24, 351–372.
- Thomas, K.; Stone, M.R.; Thompson, K.G.; St Clair Gibson, A.; Ansley, L. Reproducibility of Pacing Strategy during Simulated 20-Km Cycling Time Trials in Well-Trained Cyclists. European journal of applied physiology 2012, 112, 223–229.
- Foster, C.; Hendrickson, K.J.; Peyer, K.; Reiner, B.; deKoning, J.J.; Lucia, A.; Battista, R.A.; Hettinga, F.J.; Porcari, J.P.; Wright, G. Pattern of Developing the Performance Template. British journal of sports medicine 2009, 43, 765–769.
- Hibbert, A.W.; Billaut, F.; Varley, M.C.; Polman, R.C.J. Familiarization Protocol Influences Reproducibility of 20-Km Cycling Time-Trial Performance in Novice Participants. Front. Physiol. 2017, 8, 488. [CrossRef]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Sports medicine 2000, 30, 1–15.
- Gotti, D.; Codella, R.; Vergallito, L.; Meloni, A.; Arrighi, T.; La Torre, A.; Filipas, L. From Amateur to Professional Cycling: A Case Study on the Training Characteristics of a Zwift Academy Winner. Sports 2025, 13, 234.
- Currell, K.; Jeukendrup, A.E. Validity, Reliability and Sensitivity of Measures of Sporting Performance. Sports Medicine 2008, 38, 297–316. [CrossRef]
- Clark, B.; Paton, C.D.; O’Brien, B.J. The Reliability of Performance during Computer-Simulated Varying Gradient Cycling Time Trials. J Sci Cycling 2014, 3, 29–33.
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A New Approach to Monitoring Exercise Training. J Strength Cond Res 2001, 15, 109–115.
- Maxwell, S.E.; Delaney, H.D.; Kelley, K. Designing Experiments and Analyzing Data: A Model Comparison Perspective; Routledge, 2017; ISBN 1-315-64295-6.
Figure 1.
General study flow. N = 15 enrolled, consented and completed the study.
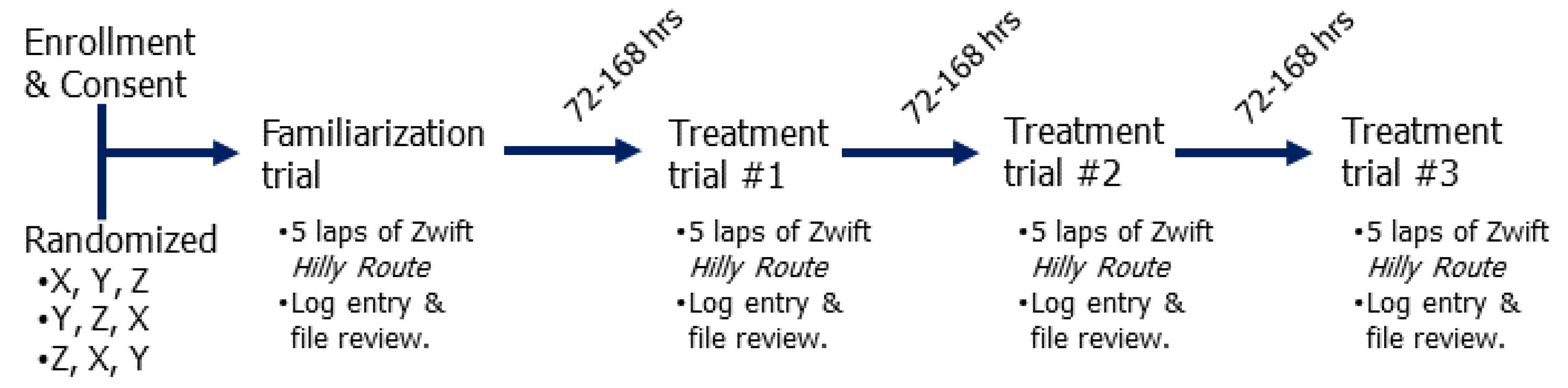
Figure 2.
Graphic representation of the Zwift virtual “Hilly Route” used in all trials. Each participant completed 5 laps of the route as outlined above. Graphic reproduced with permission by VeloViewer © 2025.
Figure 2.
Graphic representation of the Zwift virtual “Hilly Route” used in all trials. Each participant completed 5 laps of the route as outlined above. Graphic reproduced with permission by VeloViewer © 2025.
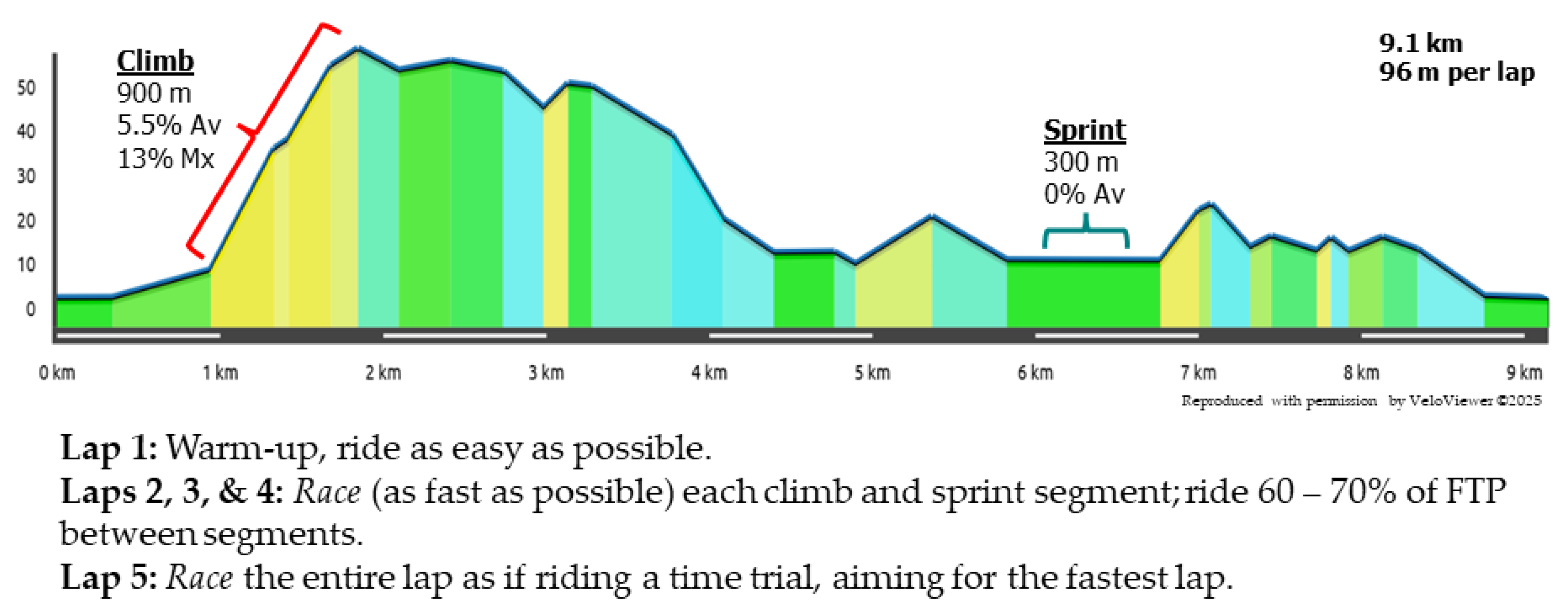

Table 1.
Summary of baseline participant physical, performance, and training characteristics.
| Overall | Zwift A | Zwift B | Zwift C | Zwift D | |
|---|---|---|---|---|---|
| Physical Characteristics | |||||
| n | 15 | 4 | 3 | 4 | 4 |
| Age (years) | 45.1 ± 12.1 | 42.0 (28.0, 50.0) | 54.0 (47, 61) | 46.0 (30.0, 51.0) | 53.5 (18, 55) |
| Height (cm) | 175.6 ± 6.9 | 176.7 (175.0, 180.3) | 181.6 (177.8, 183) | 170.2 (159, 182.9) | 176.1 (167.6, 180.3) |
| Weight (kg) | 74.4 ± 11.6 | 70.5 (65.4, 77.2) | 79.8 (69.5, 88.6) | 75.4 (60.5, 94.0) | 76.1 (55.5, 82.0) |
| RHR (bpm) | 51.3 ± 7.8 | 47.5 (45.0, 51.0) | 45.0 (39.0, 56.0) | 53.5 (48.0, 58.0) | 58.5 (43.0,66.0) |
| MHR (bpm) | 177.1 ± 11.0 | 185.0 (185, 190.0) | 172.0 (168.0, 180.0) | 183.0 (161.0, 194.0) | 164.5 (161.0,181.0) |
| Performance Characteristics | |||||
| MMP30s (W/kg) | 7.1 ± 2.3 | 9.8 (9.2, 10.4)#D | 6.8 (6.7, 6.9) | 6.7 (3.6, 9.3) | 5.8 (2.7, 7.4) |
| MMP20 (W/kg) | 3.2 ± 1.0 | 4.4 (4.0, 4.6)*D | 3.5 (3.5, 3.7) | 2.8 (2.6, 2.9) | 2.2 (1.5, 2.5) |
| MMP60 (W/kg) | 2.9 ± 0.9 | 4.0 (3.6, 4.1)*D | 3.3 (3.2, 3.4) | 2.6 (2.3, 3.1) | 1.9 (1.3, 2.2) |
| Training Characteristics | |||||
| Years training (years) | 13.4 ± 11.8 | 18.5 (3.0, 36.0) | 17.0 (12.0, 31.0) | 6.0 (1.0, 10.0) | 7.0 (2.0, 23.0) |
| 6-wk training Volume (min) | 454.0 ± 209.7 | 630.0 (180.0, 300.0) | 480.0 (480.0, 810.0) | 315.0 (180.0, 480.0) | 330.0 (90.0, 600.0) |
| Typical training ride (min) | 123.0 ± 69.5 | 135.0 (90.0, 240.0) | 135.0 (120.0, 240.0) | 90.0 (60.0, 150.0) | 75.0 (60.0, 90.0) |
| Typical longest ride (min) | 187.3 ± 68.6 | 240.0 (180.0, 300.0)#D | 240.0 (120.0, 300.0) | 150.0 (120.0, 270.0) | 150.0 (60.0, 180.0) |
| Typical Race Duration (min) | 140 ± 86.8 | 60 - 600 | 60 - 300 | 60 – 120 | 60 - 180 |
Mean ± SD or Median (Min, Max). # Significantly different from noted category (p < 0.05; e.g., #A). * Significantly different from noted category (p < 0.01; e.g., *B).
Table 2.
Performance results by lap and trial condition. .
| Lap | Trial Condition |
Entire Lap Average Power (W) |
Average HR (bpm) |
RPE (1 – 10) |
Hill Climb Segment Average Power (W) |
Sprint Segment Average Power (W) |
|---|---|---|---|---|---|---|
| FAM | 140.1 ± 38.9 | 114.4 ± 10.8 | 3.3 ± 1.7 | 159.3 ± 29.3 | 151.2 ± 55.7 | |
| 1 | TBC | 134.8 ± 41.3 | 115.6 ± 15.1 | 2.8 ± 1.6 | 151.7 ± 34.7 | 138.4 ± 56.8 |
| TC | 136.3 ± 40.0 | 116.1 ± 15.4 | 3.1 ± 2.0 | 156.5 ± 34.0 | 121.3 ± 52.0 | |
| PLAC | 136.2 ± 39.2 | 114.5 ± 11.9 | 3.2 ± 1.5 | 153.3 ± 35.1 | 141.3 ± 49.6 | |
| FAM | 180.5 ± 56.3 | 138.4 ± 13.9 | 5.3 ± 1.4 | 267.2 ± 97.5* | 431.0 ± 211.2 | |
| AVG 2-4 | TBC | 180.8 ± 56.4 | 140.8 ± 16.1 | 5.3 ± 1.5 | 300.6 ± 101.6 | 483.0 ± 211.5# |
| TC | 185.1 ± 56.2 | 141.5 ± 16.9 | 5.5 ± 1.6 | 292.9 ± 103.0 | 464.9 ± 207.0 | |
| PLAC | 192.8 ± 52.2 | 143.4 ± 15.6 | 5.3 ± 1.5 | 298.6 ± 101.2 | 488.5 ± 221.8# | |
| FAM | 181.0 ± 58.1 | 133.5 ± 14.6 | 5.6 ± 1.3 | 274.8 ± 100.8 | 437.4 ± 215.7 | |
| 2 | TBC | 185.3 ± 57.2 | 137.8 ± 18.0 | 5.7 ± 1.6 | 309.4 ± 103.5 | 502.8 ± 222.6 |
| TC | 187.3 ± 55.6 | 136.7 ± 17.3 | 5.9 ± 1.6 | 298.8 ± 111.6 | 468.2 ± 235.6 | |
| PLAC | 196.6 ± 52.4 | 138.0 ± 16.8 | 5.6 ± 1.6 | 304.6 ± 102.8 | 494.9 ± 214.8 | |
| FAM | 182.8 ± 55.2 | 136.6 ± 14.4 | 5.6 ± 1.5 | 256.0 ± 101.1 | 414.6 ± 223.0 | |
| 3 | TBC | 181.3 ± 55.2 | 139.8 ± 17.8 | 6.0 ± 1.6 | 292.2 ± 110.0 | 464.4 ± 230.0 |
| TC | 185.3 ± 54.6 | 140.1 ± 18.7 | 5.9 ± 1.6 | 273.0 ± 103.4 | 458.7 ± 225.2 | |
| PLAC | 191.6 ± 52.5 | 141.2 ± 16.6 | 5.8 ± 1.8 | 291.5 ± 107.8 | 475.5 ± 251.6 | |
| FAM | 177.7 ± 57.6 | 138.5 ± 12.7 | 6.6 ± 1.1 | 270.6 ± 104.2 | 440.9 ± 216.9 | |
| 4 | TBC | 175.9 ± 58.8 | 139.5 ± 16.3 | 6.7 ± 1.3 | 300.2 ± 101.8 | 481.8 ± 203.9 |
| TC | 182.8 ± 60.1 | 141.4 ± 15.8 | 6.9 ± 1.0 | 297.0 ± 102.1 | 467.7 ± 188.7 | |
| PLAC | 190.3 ± 52.9 | 143.6 ± 15.0 | 6.5 ± 1.3 | 299.8 ± 102.5 | 495.1 ± 210.8 | |
| FAM | 220.8 ± 76.8* | 152.1 ± 12.2 | 8.2 ± 0.9 | 235.2 ± 66.9 | 247.0 ± 74.4 | |
| 5 | TBC | 232.9 ± 69.5 | 155.7 ± 13.6 | 8.5 ± 1.2 | 246.3 ± 69.9 | 240.7 ± 56.9 |
| TC | 229.5 ± 67.3 | 155.4 ± 15.4 | 8.6 ± 1.2 | 243.4 ± 65.2 | 244.7 ± 63.6 | |
| PLAC | 233.0 ± 73.1 | 156.8 ± 14.0 | 8.3 ± 1.1 | 245.3 ± 72.9 | 236.3 ± 69.8 |
Mean ± SD. * Significantly different from all other trials within row (p < 0.001). # Significantly different from FAM trial within row (p < 0.01). Lap 1 data not analyzed.
Table 3.
Summary of current and prior TBC and TC supplement studies.
| Author | Condition/Treatment | Sport | n | RCT | PLAC | Matched PLAC | Measures | Improvement | DB Score (30) |
|---|---|---|---|---|---|---|---|---|---|
| Harnish et al. 2025 | TBC/TC | Cycling | 15 | Yes | Yes | No | RS, HI, TT, END | No improvement across all measures. | 25 |
| Gurton et. al. 2024 | OBC/TBC | Soccer | 10 | Yes | Yes | No | RS | No change in acid-base balance and no improvement across all measures for TBC. | 24 |
| Gurton et. al. 2023 | OBC/TBC | Team Field Sport | 14 | Yes | Yes | No | RS | No change in acid-base balance, similar < 2% improvement for RS compared to OBC. | 24 |
| McKay et al. 2020 | OBC/TBC | Cycling | 10 | Yes | Yes | No | RS | No change in acid-base balance and no improvement across all measures for TBC. | 23 |
| Kern et al. 2019* | TBC | Cycling | 20 | Yes | Yes | No | S, TT | No change in acid-base balance and no improvement across all measures for TBC. | 22 |
| Seah et al. 2019^ | TBC | Team Field Sport | 10 | Yes | Yes | ? | RS | No improvement across all measures. | 6 |
| Brockelbank 2024# | TC | Rugby | 12 | Yes | Yes | Yes | RS | No improvement in average peak or mean sprint power. | 24 |
| Harnish & Miller 2023 | TC | Cycling | 15 | Yes | Yes | No | RS | No improvement across all measures. | 28 |
| Sharpe & Macias 2016 | TC | Soccer | 11 | No | No | No | RS, TT | Yes. Final TC trials showed small TT improvement. | 12 |
* Unpublished manuscript; ^ Abstract only; # Unpublished manuscript plus dataset. DB: Downs and Black score; RCT: randomized controlled trial; RS: repeated sprint; S: sprint; HI: high-intensity intervals; END: endurance trials ≥ 90-min. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



