
Submitted:
06 August 2025
Posted:
07 August 2025
You are already at the latest version
Abstract
Background: The aging process is accompanied by a number of new challenges, including those of declining physical health, psychological health, and social inclusion. The present study, carried out within the Erasmus+ project, analyzes the impact of an adapted yoga program on the quality of life of older people with limited opportunities in Bucharest and Rome. Yoga has been previously associated with better self-awareness, facilitating emotional adjustment, and reducing stress.
Methods: The study included 60 total participants aged 65 years and older, with 30 participants in Rome and 30 in Bucharest. These participants faced financial disadvantages and limited access to recreational activities. Each participant followed a yoga program consisting of 12 sessions, with 90-minute sessions held twice a week. Pre and post-intervention assessments focused on emotional state, mobility, and self-awareness.
Results: The study indicated a statistically significant improvement in emotional well-being, a reduction in feelings of loneliness, and an increase in social engagement. Furthermore, the program resulted in increased social inclusion, providing a favorable framework for positive interactions between participants.
Conclusions: This data suggests that yoga is an effective method for improving the quality of life of older people and promoting an active lifestyle. The results can serve as a basis for public policy aimed at supporting the health and well-being of older persons.
Keywords:
yoga program
; older persons with limited opportunities
; quality of life
; self-awareness
; social inclusion
; active aging
1. Introduction
Demographic shifts serve as an important statistical measure for policy-makers worldwide, and currently indicate a drastic increase in the share of the population made up of older people. The population of the European Union on January 1, 2024 was estimated at 449.3 million people. Older people aged 65 years and over made up 21.6% of this number, up 0.3% from 2023 and 2.9% from 2014. Italy (24.3%) and Portugal (24.1%), had the highest shares, while Luxembourg (15.0%) and Ireland (15.5%) had the lowest. In 2024, compared to 2023, the share of older people increased in 26 EU countries and decreased only in Malta. In Romania, their share is 20.0% [1].
Older people have come to the attention of healthcare practitioners as a particularly vulnerable population. A systematic review that included 38 publications, for example, captures six dimensions of the vulnerability of older adults: physical, psychological, relational, moral, sociocultural, political/economic and existential/spiritual delimiting between two categories: basic human vulnerability and situational vulnerability [2]. From such studies, it seems that older people are not only a group correlated to high medical costs, but more importantly, a population in need of practitioner intervention to ensure optimal quality of life.
However, approaching aging from a healthcare perspective is a challenge, due to its associated physical and psychological decline; aging causes molecular and cellular changes that lead to an increase in the risk of developing somatic diseases [3]. These include type II diabetes [4], chronic kidney disease, neurodegenerative diseases (ex. Alzheimer’s disease, Parkinson’s disease) [5], and cardiovascular disease. Osteoarthritis also represents a class of emerging disorders for which age is a main risk factor; these diseases serve as one of the most common sources of pain and disability for older people [6,7]. A study on 60 people in Indonesia showed that the most common chronic diseases faced by people over 65 are high blood pressure (50%), diabetes mellitus (23.7%), ischemic heart disease (6.7%), and arthritis (3.3%). All the above diseases are usually not a direct result of aging, but rather of not mitigating risk factors in the course of one’s daily life [8]. This suggests that daily lifestyle choices are important in diminishing somatic disease presence among older populations, and therefore, abetting quality of life overall.
Studies support this idea that lifestyle choices affect disease, which in turn affects older persons’ quality of life. For example, the aforementioned study from Indonesia further indicated that duration of a chronic disease, along with variables such as marital status, educational level, income, residence and level of physical activity, are linked to the quality of life of older persons [9]. Another study conducted on 100 people aged 65 and over demonstrated that there is a significant correlation between the presence of chronic disease, the type of disease, and the amount of diseases a patient experiences with that patient’s quality of life [10].
The change in life satisfaction experienced by many older people, however, is not just a testament to the diseases and disabilities that develop with age. The mechanism of retirement as a process in today’s societies, the independence of children, and the loss of a life partner all lead to an impact on the quality of life [11]. In addition to the previously established physical and psychological decline because of disease, the above changes usually produce a sense of social exclusion, further diminishing older persons’ quality of life. To evaluate these phenomena and potential methods of intervention, a study carried out “on a sample of 170 Australian workers who made the transition to retirement in the last 12 months” identified the importance of social factors in ensuring an optimal quality of life [12]. The study aimed to correlate membership in several groups before and after retirement, and how maintenance of that membership affected perception of physical and mental health and life satisfaction. The results showed the supporting role that group membership has in limiting the negative effects of retirement. Questionnaires provided to participants in this study indicate that sustained membership in social groups through the retirement process serves to cushion retirement’s blow to perception of mental health and daily social interaction levels [12]. A similar study carried out in Portugal on 1201 participants showed that the aging process comes with a reduction of quality of life, regardless of variables such as emotional and physical health, gender, and education [13].
Clearly, both disease and social changes make aging a stress that the individual must adapt to, a process with profound implications at all levels. As demonstrated through the aforementioned studies, it entails multiple difficult transitions: an adaptation from self-sufficiency and a sense of power to a certain degree of helplessness, a diminution of personal capacities, and complications in accommodating to an increasingly less malleable environment. However, the effects of these inevitable changes on a patient’s quality of life depend not only on their extent, but also on the patient’s unique perception of these changes.
Various studies have demonstrated that subjective perception of these age-related changes is directly linked to the development of psychological disorders, such as depression and anxiety [14]. These psychological impacts are not a direct consequence of the aging process, rather being mediated by the stereotypes that we attribute to age. Decreased utility in everyday life is associated with a lowered perception of one’s adequacy and worth, essentially leading to a loss of meaning in life overall [15]. Thus, a vicious cycle is created in which the lack of a fulfilled meaning in life due to loss of social and physiological utility only leads to more physical and mental health problems, further lowering utility [16,17]. Positive emotions such as acceptance appear when the individual perceives their life as fulfilling, while a lack thereof leads to emotions such as fear, anger, and frustration [18].
To add, data collected from 1,021 participants between the ages of 50 and 67 highlighted the role that a negative outlook on the future has in the onset of depression. The study notes that loneliness tends to steer subjective perception of age-related changes in an even more negative direction, leading to higher prevalence of depression symptoms [19]. The authors of the previous study in Portugal further note that the presence of depressive and anxiety disorders only serves to burden the “trajectory of the quality of life” [13].
Altogether, health optimization efforts for older adults, constructed using the above evidence, should be a main goal of practitioners. Practitioners must consider how disease prevalence, aging-related social changes, and a negative outlook on aging all work together to impact older persons’ quality of life. By proxy, these efforts should also be undertaken by policymakers in healthcare. The data suggests that aging-related issues are complex and could benefit from a multi-faceted approach and new research into potential interventions. The abilities of older people are not only related to their individual capabilities, but also to interactions with the environment. This opens a wide array of potential interventions and public policies that can be implemented.
One of these potential interventions is the practice of yoga. Yoga has been associated with the improvement of several psychological measures that may have a considerable positive impact on quality of life. Yoga as an intervention strategy has become increasingly popular in Western culture due to its physical and mental health benefits. Yoga is an ancient discipline originating in India that unites the physical and mental planes. It does so through a connection between muscle activity and a careful focus on breathing and self-awareness [20]. Yoga encapsulates a variety of different types, but research is lacking regarding health impact differences between these types [21]. The different types include physical postures (asana), breathing techniques (pranayama), meditation techniques (pratyahara, dharana, dhyana, samadhi) and ethical teachings (yamas and niyamas) [22]. Kavitha S and Kumudini Achchi [2] note that asana and pranayama are considered the cheapest means of gaining strength and energy for institutionalized elderly. According to an integrative review of six clinical trials that evaluated the benefits of yoga interventions, Hatha Yoga was used most frequently, and the benefits obtained included reductions in anger, anxiety, and fear of falling, as well as increased well-being, self-efficacy, improvements in executive and immunological function, strength, and balance [24].
Like other forms of physical activity, the design of a yoga intervention program must take into account the conditions and abilities of the older people, both their strengths and limitations. For instance, yoga can transiently increase intraocular pressure and lead to progressive optic neuropathy, specifically in older people with glaucoma [25]. Musculoskeletal complications, including back, shoulder, or neck pain, have been reported as common adverse effects of yoga practice [26]. Frequent peripheral nerve injuries have been reported in seniors taking sedative medication [27]. The above examples suggest that yoga has the potential to be effective, but only when it is thoughtfully and systematically integrated into an individual’s overall health and self-care program. This can only occur through deliberate and open dialogue between clients, health professionals, and yoga professionals [28]. There are many studies providing information helpful in making such a decision: a meta-analysis of 75 studies showed that chair yoga resulted in positive results for older people and is a practice that should be used on a large scale [29]. This is a form of yoga adapted specifically for older people with mobility issues. It adapts traditional poses to a seated or standing position, offering gentler stretching and strengthening exercises.
Once the proper adaptations are made, older people are sure to benefit from the implementation of a yoga program into their lifestyles. In recent years, many studies have analyzed the impacts of yoga on older populations and recorded positive results. One study conducted on patients with known hypertension incorporated an integrative yoga program as an auxiliary to classical treatment. Patients subsequently showed significant reductions in systolic and diastolic blood pressure, negative emotions, anxiety symptoms, and perceived distress [30]. Another study that focused on the effects of yoga to reduce the risk of falling in older patients showed that it provides an improvement in the senior’s mobility and a reduction in the fear of falling [31].
Yoga has also been reported to heighten cognitive abilities. The effects of a yoga program on the executive function of working memory, as well as mental flexibility, were studied in an eight-week yoga practice study. Participants in the yoga intervention group showed a significant improvement in memory performance [32]. Further, a study carried out at the University of Chile in Santiago compared the effects of yoga and mindfulness interventions versus psychological education sessions on older people with mild cognitive deficits. This study identified the positive effects of interventions in the first category, and their necessity in Alzheimer’s disease prevention strategies [33].Intervention as early as possible, in the early stage of age-related cognitive impairment prevents the worsening of associated symptoms. A meta-analysis that included 12 studies and a total of 752 participants aged 60+ aimed to correlate long-term yoga practice and quality of life, and the results showed a positive correlation [34].
One mechanism by which the practice of yoga induces these many positive effects is the stimulation of interoception. This term refers to representation of the internal states of the body at the conscious and preconscious level [35]. It plays an important role in physiological and psychological well-being, influencing homeostasis, decision-making, body representation, decision-making, and self-awareness [36,37,38].
More interestingly, introception also aids in one’s emotional regulation [39], and seems to decrease with age [40]. Evidence that interoceptive mechanisms decline across life [41] raises many questions about the extent to which this impacts social-emotional decline. This also implies that raising interoception can regulate older patients’ emotional well-being.
Several studies have noticed this connection and explored the impact of yoga in developing interoceptive capacity. A three-month program of yoga interventions applied to a community in Hungary highlighted its impact on interoceptive awareness, with noteworthy effects on abilities such as observing internal stimuli, attention regulation, self-regulation, body listening, and confidence [42]. It appears that conscious observation of the psychological present moment (ex. current sensations, emotions, thoughts) leads to an improvement in the quality of life, to an increase in feelings of spiritual well-being and to a decrease in depression symptoms, but according to some studies, not to a correction of the cognitive deficit [43].
All in all, recognizing the older person’s innate learning abilities is the foundation that underlies these intervention strategies. Fortunately, studies focused on crystallized intelligence suggest an optimistic approach to the relationship between aging and learning ability [44]. Although biological changes associated with aging reduce learning capacities and weaken adaptive mechanisms, certain elements (such as compensatory resources and environmental support) facilitate them [45]. Modern research on brain neuroplasticity also counters the myth that the acquisition and performance of motor skills decline with age. Current studies show that although motor performance declines with aging, constant training counteracts that by inducing changes in brain structure and functionality. This allows older people to maintain their motor learning capacity [46]. For instance, a study assessing the brain-behavior correlation during motor task learning identified brain regions associated with various components of motor performance [47]. Overall, it appears that the acquisition of new skills is independent of age, rather depending on the existence of a social context and the difficulty level of the schemes to be learned [48].
The complex and abundant scientific data cited above, combined with recognizing the older person as a physiologically and psychologically more vulnerable adult (but with intact learning abilities), led us to the idea of developing a study within an Erasmus+ project [49].
The Erasmus+ project “Increasing the quality of life for older people with reduced possibilities in Bucharest and Rome—QuoL65+” aims to use adapted yoga to develop self-awareness of the body, breathing, emotions, feelings and thoughts. Ideally, this awareness would increase social inclusion and participation. The innovativeness of the study comes, at least for the Bucharest community, from its attempted introduction to a group often rigid in response to change. This focus on social awareness is particularly important given the details on older populations outlined above: a complex meta-analysis carried out by Eurich (2018) shows that self-awareness represents an important social competence. It is associated with increased satisfaction in social interactions, social and personal control, and feelings of happiness. It additionally reduces anxiety, stress, and depression [50]. Through self-awareness, we aim to target the subjective perception of aging so critical in an older person’s quality of life. Moreover, as a social and physical activity, the study will address the disease and social exclusion that often steers older persons’ subjective perception in a negative direction.
The participants selected had below average financial means as demonstrated by their income. Studies have shown that older people’s income is correlated with their social and medical opportunities [9]. Consequently, we determined that this group was most in need of the project’s help.
2. Materials and Methods
The general objective of the project is to improve the quality of life of older people (65+) living in Bucharest and Rome with limited possibilities due to income (and subsequently, health and social) barriers.
The specific objectives of this study were the following:
- (i)
- Improving the quality of life of the subjects through their participation in the yoga sessions, aiming at an increase in the relevant indicators, measured by standardized instruments. The instrument selected was WHOQOL-BREF (World Health Organization Quality-of-Life Scale – Short Form) [51].
- (ii)
- (iii)
- Stimulating the social involvementof the subjects by encouraging them to actively recommend the course, so that each subject recommends the program to other people in the target group. This works in strengthening social and community networks.
2.1. Study Design and Participants
The study used a quasi-experimental design with measurements both before and after the intervention. Also included was a three-month follow-up after the completion of the adapted yoga course, without a control group.
The participants were recruited from two locations (Bucharest, Romania and Rome, Italy) to ensure sociocultural diversity and external validity.
2.1.1. Inclusion Criteria
Inclusion criteria of the subjects were as follows: adults over 65 years old, who were living in less served areas of Bucharest and Rome, earning low incomes (pensions under 3000 RON/month for Romania and under 1000 Euro/month for Italy), and experiencing loneliness (widower, single, divorced), physical deficiencies (ex. arthritis, rheumatism, reduced mobility) and psychological dysfunctions (ex. anxiety, depression, fear of aging, impaired cognitive abilities).
2.1.2. Exclusion Criteria
Exclusion criteria of the subjects were as follows: severe cognitive impairment (ex. dementia), severe mobility limitations (ex. people immobilized in bed or requiring full assistance to move), uncontrolled chronic conditions (ex. severe hypertension, advanced heart failure), recent major surgery (performed in the last three months), severe psychiatric disorders (ex. schizophrenia, severe bipolar disorder), and lack of informed consent due to cognitive or legal incapacity.
2.1.3. Description of Group Participants
The subjects of the two groups were older people aged between 65-99 years. The average age of Romanian subjects was 71.9, and the average age of Italian subjects was 77.9. The participants have different housing conditions: those from Romania live at their own home, while those from Italy are residents in senior housing.
The distribution of participants in the two study groups was as follows:
- (1)
- Social status
All of the participants live alone. Their marital status distribution is as follows, and illustrated within Figure 1:
- ○
- Romania: 40% single, 23.33% divorced, 36.67% widowed;
- ○
- Italy: 30% single, 6.67% divorced, 63.33% widowed
- (2)
- Physical and mental disorders
In the two groups, the majority have physical and psychological disorders, as demonstrated by the statistics below and Figure 2:
- ○
- Romania: 33.33% physical disorders, 20% mental disorders;
- ○
- Italy: 36.67% physical disorders, 26.67% mental disorders;
- (3)
- Quality of life
In the two groups, the majority subjectively report a lowered quality of life, as shown in Figure 3:
- ○
- Romania: 26.67% reported lowered quality of life;
- ○
- Italy: 36.67% reported lowered quality of life.
2.1.4. Implementation of the Intervention
60 participants, 30 from each country, followed an adapted yoga program. In Romania, this entailed 12 sessions of 90 minute length, while in Italy, it entailed 18 sessions of 60 minute length. In both cases, the sessions were held twice a week. Pre and post-intervention evaluation was carried out using the WHOQOL-BREF and MAIA instruments to measure the impact on physical, psychological, and social health. Data was collected anonymously, ensuring participant confidentiality.
To evaluate the impact of the yoga program on participants, the study was designed as long-term research, with pre- intervention measurements, post-intervention measurements, and a follow-up 3 months after the end of the adapted Yoga course. All of these measures were taken using the same instruments.
2.2. Ethical Considerations
The study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of “Ana Aslan” National Institute of Gerontology and Geriatrics (Approval code: 178/23.11.2023).
All participants were informed about the purpose and methodology of the study and provided written informed consent before participation. Confidentiality and anonymity were maintained throughout the study. Personal data has been anonymized and stored securely, accessible only to authorized researchers. The study complied with the General Data Protection Regulation (GDPR) data protection standards.
2.3. Measures
The evaluation tools were selected according to the project objective:
- WHOQoL-BREF (World Health Organization Quality of Life Scale – Short Form): a self-report questionnaire assesses quality of life from a health-related perspective, including physical, psychological, social and environmental dimensions. A higher score indicates a higher quality of life [51].
- MAIA (Multidimensional Assessment of Interoceptive Awareness) is a self-report questionnaire that analyzes different aspects of interoceptive awareness, such as perception of body sensations, regulation of attention, emotional awareness and self-regulation. The questionnaire includes several items rated on a Likert scale, where higher scores indicate a higher level of interoceptive awareness. MAIA is frequently used in research and in the clinical field to explore the connection between bodily sensations, emotions and well-being [35,36,37,38].
2.4. Procedure
Quantitative assessments were performed separately in Bucharest and Rome, following the same protocol and using the same standardized instruments outlined above. In Romania, the participants were evaluated at the centers of the two partners - “Ana Aslan” National Institute of Gerontology and Geriatrics (AA-NIGG) and National Group for the Study and Practice of Yoga (GNSPY). In Italy, the evaluations took place in the assisted living centers, where participants were under the coordination of Sarva Yoga International (SYI).
All assessments were conducted individually in a controlled environment to ensure optimal concentration and reduced distractions. The evaluation sessions lasted approximately 45-60 minutes, and participants had the opportunity to ask clarifying questions.
After completing the pre-questionnaires, the participants took part in the first yoga sessions. Subsequently, post and follow-up questionnaires were administered to assess the short and long-term effects of the intervention.
The same tools were applied to the target group in Rome. However, the forms were scanned and sent for centralization to the partner AA-NIGG in Romania, which constitutes the scientific board in this project.
2.5. Statistical Analysis
Data was analyzed using descriptive statistics (means, standard deviations, variances) to characterize changes in each domain. Paired samples t-tests were used to assess significant differences between pre, post, and follow-up measurements. Pearson correlations were calculated to examine the stability of changes between measurements. All analysis was performed using SPSS v25 software, with a significance level of p < 0.05.
3. Results
Descriptive statistical results showed significant differences between pre, post and follow-up scores for each domain of the WHOQOL-BREF (Table 1).
The physical health, psychological health, social relations and environment domains showed a significant increase from the pre-program stage to the post-program stage, as well as maintenance in the follow-up stage.
Paired samples t-tests showed significant differences between pre and post-program measurements for all domains (p < 0.001), indicating significant improvements after the intervention (Table 2).
- Physical health showed a significant increase between pre and post metrics (t = -6.067, p < 0.001).
- Psychological health showed a significant increase between pre and post metrics (t = -5.574, p <0.001).
- Social relations showed a significant increasebetween pre and post metrics (t = -3.613, p = 0.001).
- The perception of the environment showed a significant increase between pre and post metrics (t = -6.747, p < 0.001).
The differences between post and follow-up measurements were significant only for social relations (t = 2.628, p = 0.011) and the environment (t = 3.882, p < 0.001). For physical and psychological health, no significant differences were observed (p > 0.05). This indicates physical and psychological health increases were maintained following the adapted yoga program.
Additionally, the differences between the pre and follow-up measurements showed significant improvements for physical (t = -3.029, p = 0.004) and psychological health (t = -2.996, p = 0.004), but not for social relationships (t = -0.400, p = 0.691).
Furthermore, correlations between pre, post and follow-up yoga course measurements were calculated to examine the stability of changes (Table 3).
The results showed significant correlations between pre and post measurements for all domains. Most notably, psychological health had a very high correlation between pre and post measurements (r = 0.715, p < 0.001).
Correlations between post and follow-up were significant for physical (r = 0.466, p < 0.001) and psychological (r = 0.396, p = 0.002) health, but not significant for social relationships (r = 0.421, p = 0.001) and the environment (r = -0.089, p = 0.500).
Descriptive analysis of the MAIA test shows significant changes in the three stages of the study: after the intervention (post), most dimensions showed improvements compared to the initial level (pre) (Table 4.).
The largest increases were seen in “emotional awareness” (+0.52 points), “self-regulation” (+0.54) and “trusting” (+0.62).
In the follow-up phase, these improvements were maintained or continued to increase slightly. For example, “noticing” increased from 3.70 (post) to 3.88, and “trusting” reached 3.86. Dimensions such as “not distracting” and “attention regulation” remained relatively stable after the intervention.
The variability of responses (standard deviations) remained relatively constant over time, suggesting that changes were not influenced by extreme factors. Overall, the statistical analysis indicates a significant improvement in interoceptive awareness after the intervention, with maintenance of these changes.
Comparing pre and post values, significant differences were observed for several dimensions on the MAIA test (Table 5.).
For example, “pre-noticing” to “post-noticing” showed a mean difference of -0.28 (t(59) = -2.15, p = 0.036), indicating significant improvement. Similarly, “pre-emotional awareness” to “post-emotional awareness” showed a significant increase (t(59) = -3.45, p = 0.001).
Comparing post and follow-up values, most differences were not significant, suggesting maintenance of improvements over time. For example, “post-noticing” to “follow-up noticing” was not significant (t(59) = -1.46, p = 0.150), demonstrating a stability of the effect.
Comparing pre and follow-up metrics, some dimensions showed significant improvements, such as “pre-trusting” and “follow-up trusting” (t(59) = -4.63, p <0.001) and “pre-self-regulation” to “follow-up self-regulation (t(59) = -4.11, p <0.001), confirming the lasting effects of the intervention.
Comparing Pre and Post values, correlations were observed for dimensions on Test MAIA (Table 6.).
Highly significant correlations (p < 0.001) between pre, post and follow-up values for dimensions such as “noticing” (ρ = 0.613 between pre and follow-up) and “attention regulation” (ρ = 0.620 between pre and follow-up) suggest consistency of measurements. The “not distracting” dimension had weaker correlations between pre and post (ρ = 0.205, p = 0.117), suggesting greater variability in individual responses. The high correlations at follow-up for “trusting” (ρ = 0.602, p < 0.001) indicate a stabilization of this dimension after the intervention.
4. Discussion
4.1. Analysis
(1) Participation in the yoga sessions led to a significant increase in the participants’ quality of life indicators in the areas of physical health, psychological health, social relationships, and perception of the environment.
The statistical results revealed a significant increase in WHOQOL scores in all areas analyzed. The physical health, psychological health, social relations and environment domains registered significant improvements between the pre-program and post-program stages, and these effects were maintained in the follow-up stage. Paired samples t-tests indicated significant differences between pre and post-program for all domains (p < 0.001), confirming the beneficial effects of the intervention.
The differences between post and follow-up measurements were significant only for social relations (p = 0.011) and the environment (t = 3.882, p < 0.001), indicating a possible subsequent adaptation of the participants. For physical and psychological health, no significant differences were observed (p > 0.05), suggesting a stabilization of the effects over time.
(2) Participation in the yoga sessions led to a significant increase in participants’ interoceptive capacity, according to the 8 key competencies for lifelong learning.
Analysis of the MAIA test revealed significant improvements in participants’ interoceptive ability. After the intervention, most dimensions showed statistically significant increases compared to the initial level (pre), the highest being observed in “emotional awareness” (+0.52), “self-regulation” (+0.54) and “trusting” (+0.62). As implied, this indicates greater emotional awareness, self-regulation and trust in one’s own body. In the follow-up stage, these improvements were maintained or even continued to increase slightly. For instance, “noticing” increased from 3.70 (post) to 3.88 (follow-up), and “trusting” reached 3.86. The “not distracting” and “attention regulation” dimensions remained relatively stable after the intervention.
(3) Participation in the yoga sessions led to an increase in the level of social involvement of the participants. This occurred as participants recommended the course to other people in the target population, demonstrating a multiplier effect on the community and the strengthening of social networks.
Data collected through post-intervention questionnaires indicated a high level of recommendation among participants. Moreover, the analysis of the correlations between the improvements observed in the WHOQOL and MAIA dimensions and the desire to share the positive experience with others showed significant correlations, especially for social relationships and confidence in one’s own body.
The statistical results obtained confirm the validity of the formulated hypotheses, demonstrating through t-tests, correlation analyses, and descriptive statistics that the yoga intervention had significant effects on the quality of life, interoception and social involvement of participants. All reported significant differences (p < 0.05) and high correlations scientifically support the positive impact of the program on participants. Furthermore, improvements were maintained in the long term.
In Italy, there is a stronger culture of active aging, with an emphasis on prevention and maintaining a healthy lifestyle, which may explain participants’ greater openness to relaxation and mindfulness techniques. Participants in Italy may have better access to information about the benefits of yoga and other practices for maintaining mental and physical health, which could explain their greater responsiveness to the intervention. Italy has a longer history of exposure to practices such as yoga and mindfulness, and these practices are more widely accepted and promoted.
In Romania, older persons may have a more traditional mentality, perceiving aging as an inevitable process of decline, which may influence the slower adoption of alternative methods of maintaining health. The observed differences in psychological health improvement between the Romanian participants and the Italian participants may be explained by these variations in each culture’s perception of personal development. They may also indicate the need for differentiated strategies for the implementation of such programs, depending on the specific cultural context of each community. The awareness level of the benefits of such practices in Romania may be lower, which implies the need for wider information campaigns. Yoga may be perceived in Romania as a less familiar practice, which may explain the initial resistance of some participants and the need for a longer period of adaptation.
Further, in Italy, there is a more developed network of social support for the older persons, including community programs and government initiatives that encourage participation in group activities. This may explain why participants from Italy had a faster improvement in psychological well-being. The phenomenon of social isolation in Romania is more pronounced, especially among the older with low incomes or without close family. This makes the social benefits of the yoga program more significant.
The results also showed that Romanian participants had a greater improvement in physical health, suggesting that their initial level of physical activity was lower compared to Italian participants. This may be influenced by urban infrastructure, the availability of spaces for physical activity, and local habits related to movement and exercise.
These differences underline the importance of including these yoga programs in public health strategies for the older, especially in vulnerable communities, with an emphasis on customizing intervention programs according to the cultural and socio-economic specifics of each community. In Romania, a greater focus on information and changing mindsets may be needed, while in Italy, the program can be optimized to include other forms of group activities and psychosocial support.
4.2. Study Limitations and Future Research Directions
Although the results are promising, there are some limitations that need to be considered:
- The sample size is relatively small, which limits the applicability of the results. Future studies should include a larger number of participants to ensure higher external validity.
- The current study focused on the immediate effects of yoga practice, with a follow up a few months later. Further research is needed to analyze whether the improvements recorded persist over longer periods of time.
- Though differences in Romanian and Italian results were analyzed and potential reasons were given, the study did not attempt to explore in depth how socio-economic and cultural differences influence the adoption and maintenance of yoga practice. Participants from Romania and Italy had different reactions, suggesting the need for personalized approaches.
- The study did not include a control group that would allow for the comparison of the effects of yoga with other types of interventions. This aspect limits the possibility of establishing with assurance that all positive effects are due exclusively to yoga practice.
- Motivational factors influencing program participation and post-study retention have not been examined in detail. Understanding these factors could contribute to the creation of more effective and sustainable programs.
- Although the results indicate improvements on psychological and emotional levels, the effect of yoga on cognitive functions, such as memory, attention, and mental flexibility, has not been specifically investigated. This could be an important area for future research.
- Future research should include examining the long-term effects of yoga practice, comparing the impact of different types of yoga on different age groups and specific needs, and investigating the impact on cognitive ability and long-term stress management.
5. Conclusions
The sustainable objective of this study concerns the development of good lifestyle changes and habits for older adults, and its theoretical implementation within regular intervention plans for older adults. The project’s inclusion of two different older communities in Bucharest and Rome permits a global reach in our conclusions. The study’s ideal success in two different European countries supports the idea that the program can first be implemented into local policy, and then perhaps later into the policy of the larger European community.
Our results supported the hypothesis that participation in yoga sessions leads to a significant increase in the participants’ quality of life in the areas of physical health, psychological health, social relationships and perception of the environment. The significant increases observed in all WHOQOL domains between the pre-program and post-program stages, with their maintenance in the follow-up stage, underline the positive impact of the intervention.
The present study confirms that yoga contributes to the improvement of general well-being, with a lasting long-term effect in terms of physical and psychological health. This supports the relevance of yoga practice inclusion in health and personal development programs. Furthermore, the significant differences between post and follow-up stages in terms of social relationships and the environment suggests that yoga can also influence the social and environmental aspects of the participants’ lives.
The hypothesis regarding the increase in participants’ interoceptive capacity, measured by MAIA, was validated by the study results. The significant increases in dimensions such as “emotional awareness”, “self-regulation”, and “confidence” indicate a considerable development of body awareness and emotional management skills. The consistent improvements observed during the follow-up period confirm that yoga can support greater connection to one’s own body and more effective self-regulation of emotional responses. In addition, the significant correlations between pre, post and follow-up measurements suggest that the changes are stable and persistent, which highlights the long-term benefits of yoga practice in interoception. These results emphasize the importance of yoga in increasing awareness and self-regulation, with important implications for stress management and improving mental health.
The study also validated the hypothesis of increased levels of social involvement of the participants, demonstrating a multiplier effect of the intervention on the community. Participants expressed a significant tendency to recommend the course to others, which indicates that the positive experience with yoga extends beyond the initial group of participants, having an impact on social networks. The significant correlations between the improvements observed in the dimensions of quality of life and interoception and the willingness to share the experience suggest that these changes not only have a personal impact, but a social one. These recommendations and interactions serve to strengthen interpersonal relationships and increase cohesion in social support groups.
Based on these findings, it is suggested that yoga practice should be more widely integrated into health and personal development programs, both for its beneficial effects on physical and psychological health and for its support in increasing interoception. Future research could also explore the possible mechanisms by which yoga influences quality of life and interoception, as well as its impact on other social and community dimensions. This study lays the foundation for using yoga as an effective tool in health promotion programs.
Author Contributions
Conceptualization: R.D.1 and D.-C.B.1; methodology: R.D.1 and A.R.1; investigation: D.-C.B.1, I.G.1, A.R.1 and P.S.1; analysis: A.-E.S., A.R.1 and I.G.1; resources: R.D.1, A.R.2 , S.V.3 and A.I.3; writing-original draft preparation: R.D.1, A.R.1 and D.-C.B.1; supervision: R.D.1 and A.R.2; project administration: R.D.1, A.R.2 and M.B.3 (1”Ana Aslan” National Institute of Gerontology and Geriatrics; 2Sarva Yoga International; 3Grupul Național de Studiu și Practică Yoga). All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by funding from the ERASMUS+ Project 2023-1-RO01-KA210-ADU-000164010 “Increasing the quality of life for older people with reduced possibilities in Bucharest and Rome - QuoL65+” (funded by the European Commission).
Institutional Review Board Statement
Approval was obtained from the Scientific Council of “Ana Aslan” National Institute of Gerontology and Geriatrics. It also has the Advisory Opinion of the Ethical Council and the Opinion of Research Ethics Commission of AA-NIGG no. 178 of 23.11.2023. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. All ethical, integrity, and confidentiality criteria are respected, respecting all patients’ rights.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the reported results of this study are available upon request from the corresponding author.
Acknowledgments
The work presented in this article is part of the ERASMUS+ Project QuoL65+. All the authors are members of the ERASMUS+ Project. Special thanks are extended to the SYI, including Sabrina Tinelli, Sara Cignitti, Maura Grava, Lucia Morotti and Marcella Pagano, coordinated by Antonietta Rozzi, the technical support of Simona Opris and Irina Stoica from Research Department from AA-NIGG, and all participants from Italy and Romania, for their invaluable contributions and active engagement throughout the study.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
| AA-NIGG | “Ana Aslan” National Institute of Gerontology and Geriatrics |
| SYI | Sarva Yoga International |
| GNSPY | Grupul National de Studiu si Practica Yoga |
| WHOQOL-BREF | World Health Organization Quality of Life Questionnaire-Short Form |
| MAIA | Multidimensional Assessment of Interoceptive Awareness |
References
- Eurostat. (2024). Population structure and ageing. Statistics Explained. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed on 13 December 2024).
- Sanchini, V., Sala, R., & Gastmans, C. (2022). The concept of vulnerability in aged care: A systematic review of argument-based ethics literature. BMC Medical Ethics, 23(84). [CrossRef]
- Noto, S. (2023). Perspectives on aging and quality of life. Healthcare, 11(15), 2131. [CrossRef]
- Gopalraj, R. (2017). The older adult with diabetes and the busy clinicians. Primary Care, 44(3), 469–479. [CrossRef]
- Cleeland, C., Pipingas, A., Scholey, A., & White, D. (2019). Neurochemical changes in the aging brain: A systematic review. Neuroscience & Biobehavioral Reviews, 98, 306–319. [CrossRef]
- Arden, N., & Nevitt, M. C. (2006). Osteoarthritis: Epidemiology. Best Practice & Research Clinical Rheumatology, 20, 3–25. [CrossRef]
- Lawrence, R. C., Felson, D. T., Helmick, C. G., et al. (2008). Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis & Rheumatism, 58, 26–35. [CrossRef]
- Noale, M., Limongi, F., & Maggi, S. (2020). Epidemiology of cardiovascular diseases in the elderly. In Advances in Experimental Medicine and Biology (Vol. 1216, pp. 29–38). [CrossRef]
- Maringka, M. C. G., Rahardjo, T. B. W., & Suratmi, T. (2023). Quality of elderly life with chronic diseases in the working area of Kembangan District Hospital. Jurnal Indonesia Sosial Sains, 4(10), 1048–1057. [CrossRef]
- Öztürk, A., Şimşek, T. T., Yümin, E. T., Sertel, M., & Yümin, M. (2011). The relationship between physical, functional capacity and quality of life (QoL) among elderly people with a chronic disease. Archives of Gerontology and Geriatrics, 53(3), 278–283. [CrossRef]
- Stahl, S. T., Emanuel, J., Albert, S. M., Dew, M. A., Schulz, R., Robbins-Welty, G., & Reynolds, C. F. III. (2017). Design and rationale for a technology-based healthy lifestyle intervention in older adults grieving the loss of a spouse. Contemporary Clinical Trials Communications, 8, 99–105. [CrossRef]
- Haslam, C., Lam, B. C. P., Ghafoori, E., Steffens, N. K., Haslam, S. A., Bentley, S. V., Cruwys, T., & La Rue, C. J. (2023). A longitudinal examination of the role of social identity in supporting health and well-being in retirement. Psychology and Aging, 38(7), 615–626. [CrossRef]
- Ribeiro, O., Teixeira, L., Araújo, L., Rodríguez-Blázquez, C., Calderón-Larrañaga, A., & Forjaz, M. J. (2020). Anxiety, depression and quality of life in older adults: Trajectories of influence across age. International Journal of Environmental Research and Public Health, 17(9039). [CrossRef]
- Bodner, E., & Bergman, Y. S. (2016). Loneliness and depressive symptoms among older adults: The moderating role of subjective life expectancy. Psychiatry Research, 237, 78–82. [CrossRef]
- Steger, M. F. (2012). Experiencing meaning in life: Optimal functioning at the nexus of well-being, psychopathology, and spirituality. In P. T. P. Wong (Ed.), The human quest for meaning: Theories, research, and applications (2nd ed., pp. 165–184). Routledge. https://www.scirp.org/reference/referencespapers?referenceid=2656062.
- Greenblatt-Kimron, L., Kagan, M., & Zychlinski, E. (2022). Meaning in life among older adults: An integrative model. International Journal of Environmental Research and Public Health, 19(24), 16762. [CrossRef]
- Martela, F., & Steger, M. F. (2016). The three meanings of meaning in life: Distinguishing coherence, purpose, and significance. The Journal of Positive Psychology, 11, 531–545. [CrossRef]
- King, L. A., Hicks, J. A., Krull, J. L., & Del Gaiso, A. K. (2006). Positive affect and the experience of meaning in life. Journal of Personality and Social Psychology, 90(1), 179–196. [CrossRef]
- Bergman, Y. S., & Segel-Karpas, D. (2018). Future time perspective, loneliness, and depressive symptoms among middle-aged adults: A mediation model. Journal of Affective Disorders, 241, 173–175. [CrossRef]
- Dubey, S., Malviya, S. J., Pant, H., & Kushwaha, E. P. (2022). A review on yoga practice and its effects. In Challenges and Opportunities in Nutrition, Environment and Agriculture. Rathore Academic Research Publication. https://www.researchgate.net/publication/355409364_Therapeutic_role_of_yoga_in_neuropsychological_disorders.
- Rao, R. V. (2019). Yoga practice and health among older adults. În D. Gu & M. E. Dupre (Eds.), Encyclopedia of Gerontology and Population Aging (pp. XX–XX). Springer, Cham. [CrossRef]
- Telles, S., & Singh, N. (2013). Science of the mind: Ancient yoga texts and modern studies. Psychi-atric Clinics, 36(1), 93–108. [CrossRef]
- Kavitha, S., & Achchi, K. (2015). A study on the significance of yoga in geriatric care. International Journal of Applied Research, 1(7), 749–751. https://www.allresearchjournal.com/archives/2015/vol1issue7/PartM/1-7-124-125.pdf.
- Martens, N. L. (2022). Yoga interventions involving older adults: Integrative review. Journal of Gerontological Nursing, 48(2), 43–52. [CrossRef]
- de Barros, D. S., Bazzaz, S., Gheith, M. E., Siam, G. A., & Moster, M. R. (2008). Progressive optic neuropathy in congenital glaucoma associated with the Sirsasana yoga posture. Ophthalmic Surgery, Lasers and Imaging, 39, 339–340. [CrossRef]
- Cramer, H., Quinker, D., Schumann, D., Wardle, J., Dobos, G., & Lauche, R. (2019). Adverse effects of yoga: A national cross-sectional survey. BMC Complementary and Alternative Medicine, 19, Article 190. [CrossRef]
- Staudt, M. D., Prabhala, T., Sheldon, B. L., Quaranta, N., Zakher, M., Bhullar, R., Pilitsis, J. G., & Argoff, C. E. (2020). Current strategies for the management of painful diabetic neuropathy. Journal of Diabetes Science and Technology. [CrossRef]
- Bonura, K. B. (2011). The psychological benefits of yoga practice for older adults: Evidence and guidelines. International Journal of Yoga Therapy, 21, 129–142. PMID: 22398354 . [CrossRef]
- Veneri, D., & Gannoti, M. E. (2021). Take a seat for yoga with seniors: A scoping review. OBM Geriatrics, 6(2), Article 197. [CrossRef]
- Roche, L., & Hesse, B. (2014). Application of an integrative yoga therapy program in cases of essential arterial hypertension in public healthcare. Complementary Therapies in Clinical Practice, 20(4), 285–290. [CrossRef]
- Galantino, M. L., Green, L., Decesari, J. A., Mackain, N. A., Rinaldi, S. M., Stevens, M. E., et al. (2012). Safety and feasibility of modified chair-yoga on functional outcome among elderly at risk for falls. International Journal of Yoga, 5(2), 146–150. [CrossRef]
- Gothe, N. P., Kramer, A. F., & McAuley, E. (2014). The effects of an 8-week Hatha yoga intervention on executive function in older adults. The Journals of Gerontology: Series A, 69(9), 1109–1116. [CrossRef]
- Farhang, M., Rojas, G., Martínez, P., Behrens, M. I., Langer, Á. I., Diaz, M., & Miranda-Castillo, C. (2022). The impact of a yoga-based mindfulness intervention versus psycho-educational session for older adults with mild cognitive impairment: The protocol of a randomized controlled trial. International Journal of Environmental Research and Public Health, 19(22), 15374. [CrossRef]
- Berlingieri, F., Colagrossi, M., & Mauri, C. (2023). Loneliness and social connectedness: Insights from a new EU-wide survey. European Commission. https://publications.jrc.ec.europa.eu/repository/handle/JRC133351.
- Casabianca, E., & Kovacic, M. (2022). Loneliness among older adults – A European perspective. European Commission. https://publications.jrc.ec.europa.eu/repository/handle/JRC129421.
- Panigrahi, M., Shree, P., & Swain, D. P. (2023). Effect of integrated approach of yoga therapy on loneliness in elderly: An interventional study. Biomedicine, 43(1), 47–51. [CrossRef]
- Tulloch, A., Bombell, H., Dean, C., & Tiedemann, A. (2018). Yoga-based exercise improves health-related quality of life and mental well-being in older people: A systematic review of randomised controlled trials. Age and Ageing, 47(4), 537–544. [CrossRef]
- Suksasilp, C., & Garfinkel, S. N. (2022). Towards a comprehensive assessment of interoception in a multi-dimensional framework. Biological Psychology, 168, Article 108262. [CrossRef]
- Tsakiris, M., & Critchley, H. (2016). Interoception beyond homeostasis: Affect, cognition and mental health. Philosophical Transactions of the Royal Society B: Biological Sciences, 371(1708), 20160002. [CrossRef]
- Monti, A., Porciello, G., Panasiti, M. S., & Aglioti, S. M. (2022). The inside of me: Interoceptive constraints on the concept of self in neuroscience and clinical psychology. Psychological Research, 86(8), 2468–2477. [CrossRef]
- Füstös, J., Gramann, K., Herbert, B. M., & Pollatos, O. (2013). On the embodiment of emotion regulation: Interoceptive awareness facilitates reappraisal. Social Cognitive and Affective Neuroscience, 8(8), 911–917. [CrossRef]
- Khalsa, S. S., Rudrauf, D., & Tranel, D. (2009). Interoceptive awareness declines with age. Psychophysiology, 46(6), 1130–1136. [CrossRef]
- Pollatos, O., Matthias, E., & Keller, J. (2015). When interoception helps to overcome negative feelings caused by social exclusion. Frontiers in Psychology, 6, Article 786. [CrossRef]
- Beier, M. E., & Ackerman, P. L. (2005). Age, ability, and the role of prior knowledge on the acquisition of new domain knowledge: Promising results in a real-world learning environment. Psychology and Aging, 20(2), 341–355. [CrossRef]
- Tournier, I. (2022). Learning and adaptation in older adults: An overview of main methods and theories. Learning, Culture and Social Interaction, 37, Article 100466. [CrossRef]
- Gooijers, J., Pauwels, L., Hehl, M., Seer, C., Cuypers, K., & Swinnen, S. P. (2024). Aging, brain plasticity, and motor learning. Ageing Research Reviews, 102, Article 102569. [CrossRef]
- Durand-Ruel, M., Park, C.-h., Moyne, M., Maceira-Elvira, P., Morishita, T., & Hummel, F. C. (2023). Early motor skill acquisition in healthy older adults: Brain correlates of the learning process. Cerebral Cortex, 33(12), 7356–7368. [CrossRef]
- Voelcker-Rehage, C. (2008). Motor-skill learning in older adults—A review of studies on age-related differences. European Review of Aging and Physical Activity, 5, 5–16. [CrossRef]
- Bălan, D.-C., Drăghici, R., Găiculescu, I., Rusu, A., Stan, A.-E., & Stan, P. (2025). An optimal beneficiary profile to ensure focused interventions for older adults. Geriatrics, 10, Article 59. [CrossRef]
- Eurich, T. (2018). What self-awareness really is (and how to cultivate it). Harvard Business Review, 4(4), 1–9.https://membership.amavic.com.au/files/What%20self-awareness%20is%20and%20how%20to%20cultivate%20it_HBR_2018.pdf.
- von Steinbüchel, N., Lischetzke, T., Gurny, M., & Eid, M. (2006). Assessing quality of life in older people: Psychometric properties of the WHOQOL-BREF. European Journal of Ageing, 3(2), 116–122. [CrossRef]
Figure 1.
Distribution on Social Status.
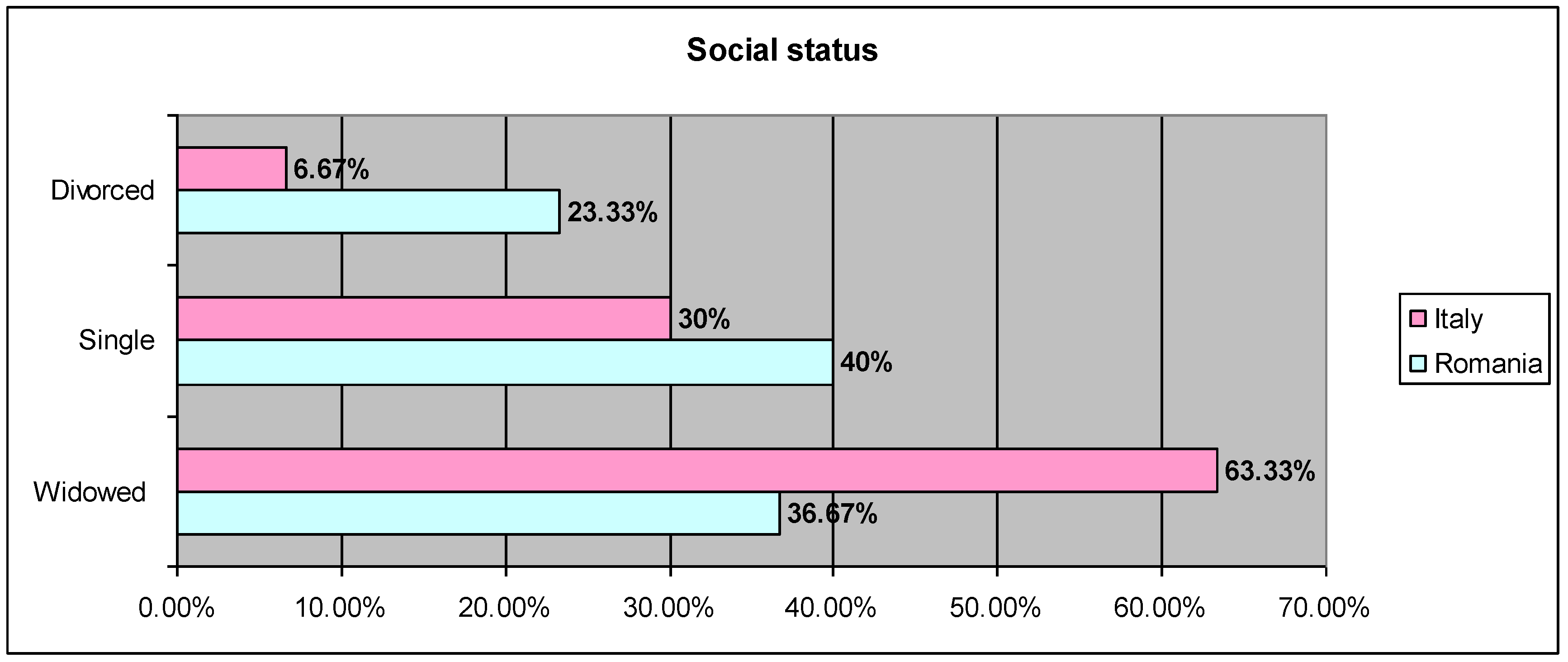
Figure 2.
Distribution on physical and mental disorders.
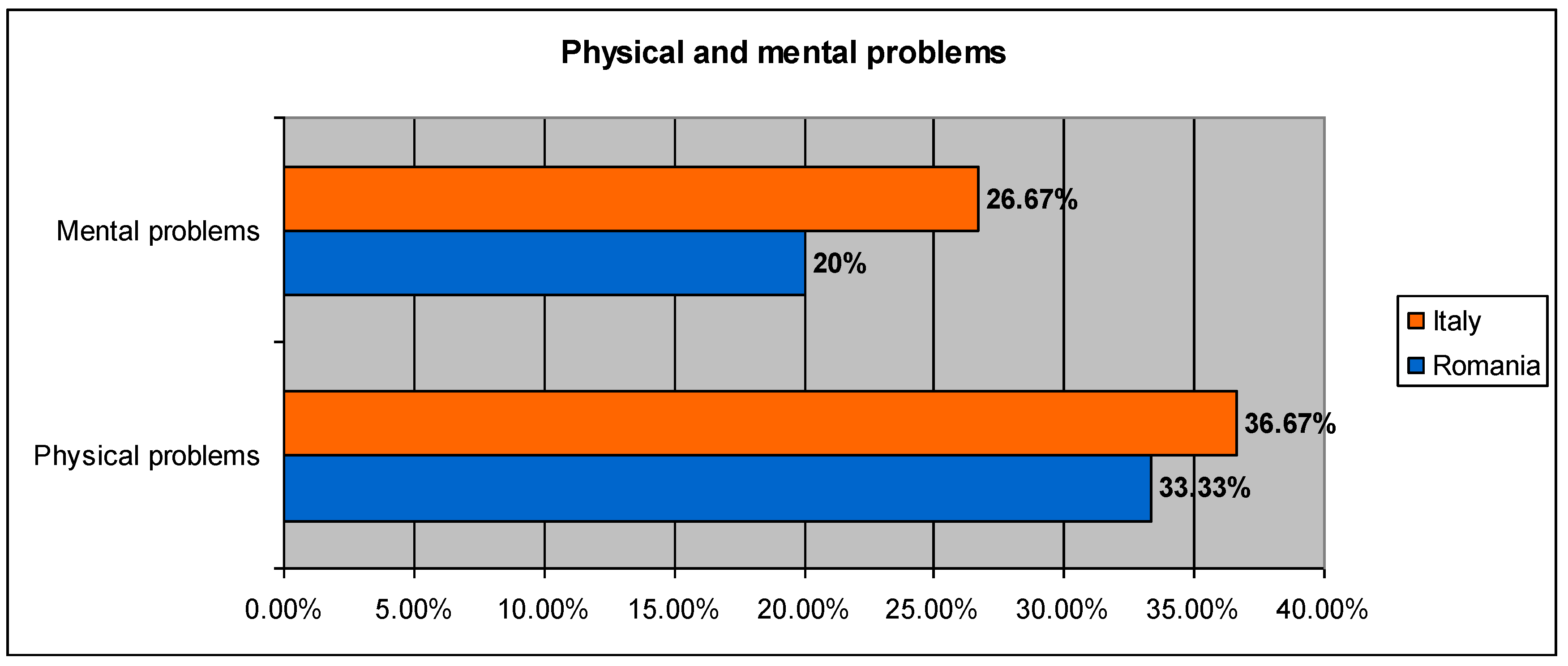
Figure 3.
Distribution on impact on quality of life.
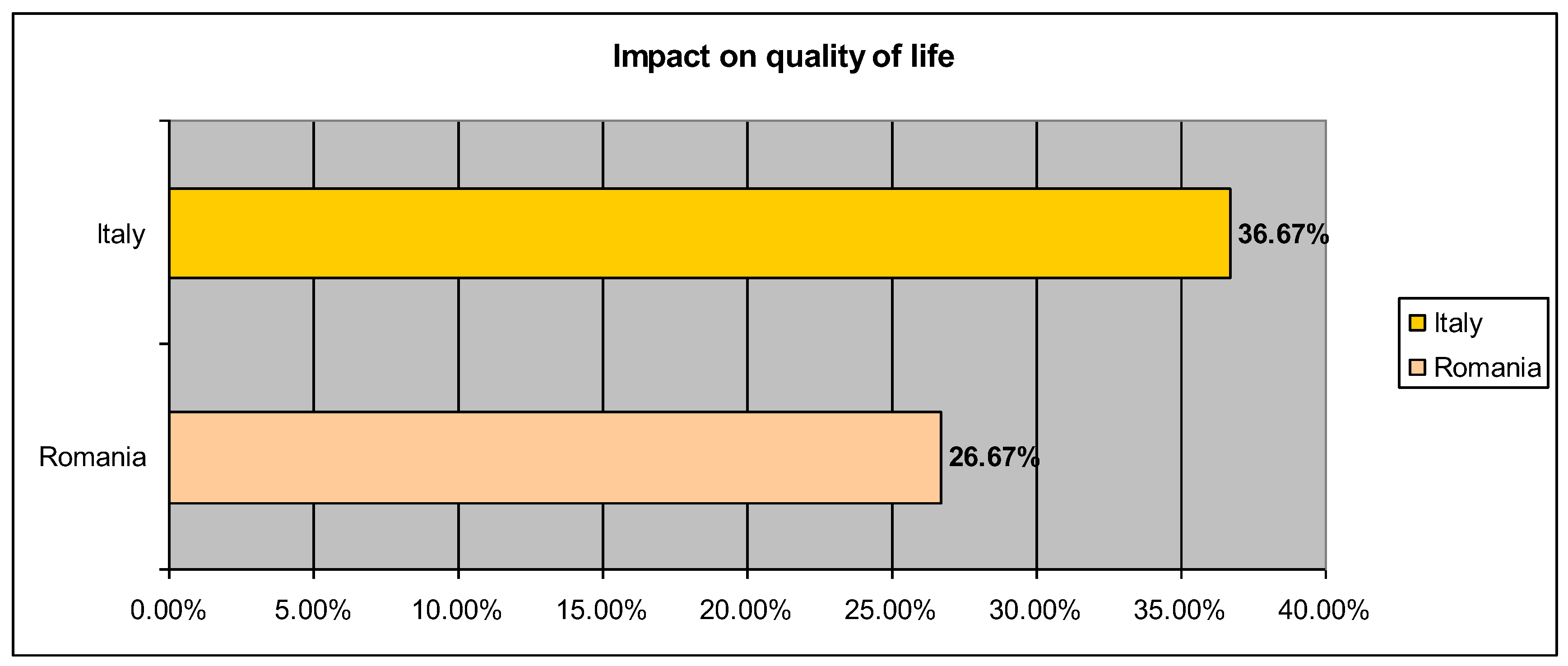

Table 1.
Descriptive statistics Test WHOQOL.
| N | Minimum | Maximum | Mean | Std. Deviation | Variance | |
| PreD1_Physical Health | 60 | 17.86 | 89.29 | 54.95 | 13.90 | 193.214 |
| PreD2_Psychological Health | 60 | 17.50 | 95.00 | 57.04 | 18.97 | 360.071 |
| PreD3_Social Relations | 60 | 16.67 | 100.00 | 65.06 | 17.55 | 308.148 |
| PreD4_Environment | 60 | 17.75 | 100.00 | 59.67 | 15.209 | 231.328 |
| PostD1_ Physical Health | 60 | 42.86 | 86.75 | 65.36 | 10.64 | 113.231 |
| PostD2_Psychological Health | 60 | 31.75 | 98.25 | 66.60 | 14.369 | 206.487 |
| PostD3_ Social Relations | 60 | 33.33 | 100.00 | 72.57 | 14.76 | 217.957 |
| PostD4_Environment | 60 | 37.50 | 97.92 | 75.97 | 14.426 | 208.134 |
| Follow-upD1_Physical Health | 60 | 17.86 | 100.00 | 62.29 | 15.040 | 226.229 |
| Follow-upD2_Psychological Health | 60 | 8.33 | 95.75 | 64.719 | 19.683 | 387.452 |
| Follow-upD3_Social Relations | 60 | 8.33 | 100.00 | 66.14 | 19.628 | 385.293 |
| Follow-upD4_Environment | 60 | 12.50 | 96.50 | 64.03 | 17.723 | 314.117 |
| Valid N (listwise) | 60 |
Table 2.
Paired Samples t Test WHOQOL.
| Paired Differences | t | df |
Sig. (2-tailed) |
||||
| Mean | Std. Deviation | Std. Error Mean | |||||
| Pair 1 | PreD1_PhysicalHealth& PostD1_ PhysicalHealth |
-10.409 | 13.289 | 1.715 | -6.067 | 59 | 0.000 |
| Pair 2 | PostD1_PhysicalHealth& Follow-upD1_PhysicalHealth |
3.067 | 13.798 | 1.781 | 1.722 | 59 | 0.090 |
| Pair 3 | PreD1_PhysicalHealth& Follow-upD1_PhysicalHealth |
-7.342 | 18.774 | 2.423 | -3.029 | 59 | 0.004 |
| Pair 4 | PreD2_PsychologicalHealth& PostD2_PsychologicalHealth |
-9.565 | 13.291 | 1.715 | -5.574 | 59 | 0.000 |
| Pair 5 | PostD2_PsychologicalHealth& Follow-upD2_PsychologicalHealth |
1.886 | 19.237 | 2.483 | 0.759 | 59 | 0.451 |
| Pair 6 | PreD2_PsychologicalHealth& Follow-upD2_PsychologicalHealth |
-7.679 | 19.855 | 2.563 | -2.996 | 59 | 0.004 |
| Pair 7 | PreD3_SocialRelations& PostD3_ SocialRelations |
-7.508 | 16.098 | 2.078 | -3.613 | 59 | 0.001 |
| Pair 8 | PostD3_SocialRelations& Follow-upD3_SocialRelations |
6.429 | 18.946 | 2.446 | 2.628 | 59 | 0.011 |
| Pair 9 | PreD3_SocialRelations& Follow-upD3_SocialRelations |
-1.079 | 20.908 | 2.699 | -0.400 | 59 | 0.691 |
| Pair 10 | PreD4_Environment& PostD4_Environment |
-16.300 | 18.713 | 2.415 | -6.747 | 59 | 0.000 |
| Pair 11 | PostD4_Environment& Follow-upD4_Environment |
11.940 | 23.826 | 3.075 | 3.882 | 59 | 0.000 |
| Pair 12 | PreD4_Environment& Follow-upD4_Environment |
-4.359 | 16.895 | 2.181 | -1.999 | 59 | 0.050 |
Table 3.
Correlations between stages on domains Test WHOQOL.
| Paired Samples Correlations | ||||
| N | Correlation | Sig. | ||
| Pair 1 | PreD1_ PhysicalHealth& PostD1_ PhysicalHealth |
60 | 0.439 | 0.000 |
| Pair 2 | PostD1_PhysicalHealth& Follow-upD1_ PhysicalHealth |
60 | 0.466 | 0.000 |
| Pair 3 | PreD1_PhysicalHealth& Follow-upD1_ PhysicalHealth |
60 | 0.160 | 0.222 |
| Pair 4 | PreD2_PsychologicalHealth& PostD2_ PsychologicalHealth | 60 | 0.715 | 0.000 |
| Pair 5 | PostD2_PsychologicalHealth& Follow-upD2_PsychologicalHealth | 60 | 0.396 | 0.002 |
| Pair 6 | PreD2_PsychologicalHealth& Follow-upD2_ PsychologicalHealth | 60 | 0.473 | 0.000 |
| Pair 7 | PreD3_ SocialRelations& PostD3_ SocialRelations |
60 | 0.515 | 0.000 |
| Pair 8 | PostD3_SocialRelations& Follow-upD3_ SocialRelations |
60 | 0.421 | 0.001 |
| Pair 9 | PreD3_SocialRelations& Follow-upD3_ SocialRelations |
60 | 0.372 | 0.003 |
| Pair 10 | PreD4_Environment& PostD4_Environment |
60 | 0.203 | 0.119 |
| Pair 11 | PostD4_Environment& Follow-upD4_Environment |
60 | -0.089 | 0.500 |
| Pair 12 | PreD4_Environment& Follow-upD4_Environment |
60 | 0.482 | 0.000 |
Table 4.
Descriptive Statistics Test MAIA.
| N | Minimum | Maximum | Mean | Std. Deviation | Variance | |
| Pre_Noticing | 60 | 0.00 | 5.00 | 3.427 | 1.148 | 1.319 |
| Pre_NotDistracting | 60 | 0.00 | 5.00 | 2.202 | 1.093 | 1.196 |
| Pre_NotWorrying | 60 | 0.00 | 4.80 | 2.469 | 1.29 | 1.669 |
| Pre_AttentionRegulation | 60 | 1.00 | 5.00 | 3.158 | 1.052 | 1.108 |
| Pre_EmotionalAwareness | 60 | 1.67 | 5.00 | 3.401 | 1.094 | 1.197 |
| Pre_SelfRegulation | 60 | 1.00 | 5.00 | 2.959 | 1.180 | 1.393 |
| Pre_BodyListening | 60 | 0.33 | 5.00 | 2.877 | 1.221 | 1.492 |
| Pre_Trusting | 60 | 0.40 | 5.00 | 3.170 | 1.440 | 2.074 |
| Post_Noticing | 60 | 1.00 | 5.00 | 3.704 | 1.048 | 1.098 |
| Post_NotDistracting | 60 | 0.00 | 4.67 | 1.764 | 1.014 | 1.029 |
| Post_NotWorrying | 60 | 0.40 | 4.80 | 2.503 | 0.957 | 0.916 |
| Post_AttentionRegulation | 60 | 1.00 | 4.86 | 3.009 | 1.052 | 1.107 |
| Post_EmotionalAwareness | 60 | 2.20 | 5.00 | 3.923 | 0.834 | 0.697 |
| Post_SelfRegulation | 60 | 0.75 | 5.00 | 3.501 | 1.107 | 1.227 |
| Post_BodyListening | 60 | 0.67 | 5.00 | 3.255 | 1.153 | 1.331 |
| Post_Trusting | 60 | 1.33 | 5.00 | 3.794 | 0.959 | 0.920 |
| Follow-up_Noticing | 60 | 1.50 | 5.00 | 3.879 | 0.937 | 0.878 |
| Follow-up_NotDistracting | 60 | 0.00 | 5.00 | 1.933 | 1.09 | 1.197 |
| Follow-up_NotWorrying | 60 | 0.60 | 4.80 | 2.606 | 0.952 | 0.907 |
| Follow-up_AttentionRegulation | 60 | 0.29 | 5.00 | 3.143 | 1.137 | 1.293 |
| Follow-up_EmotionalAwareness | 60 | 1.00 | 5.00 | 4.076 | 0.930 | 0.867 |
| Follow-up_SelfRegulation | 60 | 0.25 | 5.00 | 3.583 | 1.131 | 1.281 |
| Follow-up_BodyListening | 60 | 0.00 | 5.00 | 3.394 | 1.127 | 1.272 |
| Follow-up_Trusting | 60 | 0.67 | 5.00 | 3.861 | 0.993 | 0.988 |
| Valid N (listwise) | 60 |
Table 5.
Paired Samples t-test MAIA.
| Paired Differences | t | df |
Sig. (2-tailed) |
||||
| Mean | Std. Deviation | Std. Error Mean | |||||
| Pair 1 | Pre_Noticing& Post_Noticing |
-0.276 | 0.996 | 0.128 | -2.150 | 59 | 0.036 |
| Pair 2 | Post_Noticing& Follow-up_Noticing |
-0.175 | 0.930 | 0.120 | -1.457 | 59 | 0.150 |
| Pair 3 | Pre_Noticing& Follow-up_Noticing |
-0.451 | 0.937 | 0.120 | -3.732 | 59 | 0.000 |
| Pair 4 | Pre_NotDistracting& Post_NotDistracting | 0.438 | 1.330 | 0.171 | 2.553 | 59 | 0.013 |
| Pair 5 | Post_NotDistracting& Follow-up_NotDistracting |
-0.169 | 1.025 | 0.132 | -1.277 | 59 | 0.207 |
| Pair 6 | Pre_NotDistracting& Follow-up_NotDistracting |
0.269 | 1.272 | 0.164 | 1.641 | 59 | 0.106 |
| Pair 7 | Pre_NotWorrying& Post_NotWorrying | -0.033 | 1.333 | 0.172 | -0.195 | 59 | 0.846 |
| Pair 8 | Post_NotWorrying& Follow-up_NotWorrying |
-0.103 | 0.861 | 0.111 | -0.929 | 59 | 0.357 |
| Pair 9 | Pre_NotWorrying& Follow-up_NotWorrying |
-0.136 | 1.222 | 0.157 | -0.867 | 59 | 0.389 |
| Pair 10 | Pre_AttentionRegulation& Post_AttentionRegulation | 0.148 | 1.095 | 0.141 | 1.048 | 59 | 0.299 |
| Pair 11 | Post_AttentionRegulation& Follow-up_AttentionRegulation |
-0.133 | 0.961 | 0.124 | -1.073 | 59 | 0.288 |
| Pair 12 | Pre_AttentionRegulation& Follow-up_AttentionRegulation |
0.015 | 0.957 | 0.123 | 0.121 | 59 | 0.904 |
| Pair 13 | Pre_EmotionalAwareness& Post_EmotionalAwareness | -0.521 | 1.170 | 0.151 | -3.451 | 59 | 0.001 |
| Pair 14 | Post_EmotionalAwareness& Follow-up_EmotionalAwareness |
-0.153 | 0.930 | 0.120 | -1.277 | 59 | 0.207 |
| Pair 15 | Pre_EmotionalAwareness& Follow-up_EmotionalAwareness |
-0.675 | 1.129 | 0.145 | -4.629 | 59 | 0.000 |
| Pair 16 | Pre_SelfRegulation& Post_SelfRegulation | -0.541 | 1.272 | 0.164 | -3.296 | 59 | 0.002 |
| Pair 17 | Post_SelfRegulation& Follow-up_SelfRegulation |
-0.082 | 1.061 | 0.136 | -0.600 | 59 | 0.551 |
| Pair 18 | Pre_SelfRegulation& Follow-up_SelfRegulation |
-0.623 | 1.176 | 0.151 | -4.107 | 59 | 0.000 |
| Pair 19 | Pre_BodyListening& Post_BodyListening | -0.377 | 1.245 | 0.160 | -2.350 | 59 | 0.022 |
| Pair 20 | Post_BodyListening& Follow-up_BodyListening |
-0.138 | 1.192 | 0.153 | -0.901 | 59 | 0.371 |
| Pair 21 | Pre_BodyListening& Follow-up_BodyListening |
-0.516 | 1.131 | 0.146 | -3.536 | 59 | 0.001 |
| Pair 22 | Pre_Trusting& Post_Trusting |
-0.623 | 1.421 | 0.183 | -3.397 | 59 | 0.001 |
| Pair 23 | Post_Trusting& Follow-up_Trusting |
-0.067 | 1.114 | 0.143 | -0.467 | 59 | 0.642 |
| Pair 24 | Pre_Trusting& Follow-up_Trusting |
-0.690 | 1.156 | 0.149 | -4.625 | 59 | 0.000 |
Table 6.
Cross-stage correlations on test dimensions MAIA.
| Paired Samples Correlations | ||||
| N | Correlation | Sig. | ||
| Pair 1 | Pre_Noticing& Post_Noticing |
60 | 0.592 | 0.000 |
| Pair 2 | Post_Noticing& Follow-up_Noticing |
60 | 0.566 | 0.000 |
| Pair 3 | Pre_Noticing& Follow-up_Noticing |
60 | 0.613 | 0.000 |
| Pair 4 | Pre_NotDistracting& Post_NotDistracting | 60 | 0.205 | 0.117 |
| Pair 5 | Post_NotDistracting& Follow-up_NotDistracting |
60 | 0.529 | 0.000 |
| Pair 6 | Pre_NotDistracting& Follow-up_NotDistracting |
60 | 0.323 | 0.012 |
| Pair 7 | Pre_NotWorrying& Post_NotWorrying | 60 | 0.326 | 0.011 |
| Pair 8 | Post_NotWorrying& Follow-up_NotWorrying |
60 | 0.593 | 0.000 |
| Pair 9 | Pre_NotWorrying& Follow-up_NotWorrying |
60 | 0.440 | 0.000 |
| Pair 10 | Pre_AttentionRegulation& Post_AttentionRegulation | 60 | 0.459 | 0.000 |
| Pair 11 | Post_AttentionRegulation& Follow-up_AttentionRegulation |
60 | 0.617 | 0.000 |
| Pair 12 | Pre_AttentionRegulation& Follow-up_AttentionRegulation |
60 | 0.620 | 0.000 |
| Pair 13 | Pre_EmotionalAwareness& Post_EmotionalAwareness | 60 | 0.286 | 0.027 |
| Pair 14 | Post_EmotionalAwareness& Follow-up_EmotionalAwareness |
60 | 0.449 | 0.000 |
| Pair 15 | Pre_EmotionalAwareness& Follow-up_EmotionalAwareness |
60 | 0.387 | 0.002 |
| Pair 16 | Pre_SelfRegulation& Post_SelfRegulation | 60 | 0.382 | 0.003 |
| Pair 17 | Post_SelfRegulation& Follow-up_SelfRegulation |
60 | 0.551 | 0.000 |
| Pair 18 | Pre_SelfRegulation& Follow-up_SelfRegulation |
60 | 0.483 | 0.000 |
| Pair 19 | Pre_BodyListening& Post_BodyListening | 60 | 0.452 | 0.000 |
| Pair 20 | Post_BodyListening& Follow-up_BodyListening |
60 | 0.454 | 0.000 |
| Pair 21 | Pre_BodyListening& Follow-up_BodyListening |
60 | 0.539 | 0.000 |
| Pair 22 | Pre_Trusting& Post_Trusting |
60 | 0.352 | 0.006 |
| Pair 23 | Post_Trusting& Follow-up_Trusting |
60 | 0.349 | 0.006 |
| Pair 24 | Pre_Trusting& Follow-up_Trusting |
60 | 0.602 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



