
Submitted:
25 July 2025
Posted:
28 July 2025
You are already at the latest version
Abstract
Metabolic dysfunction-associated steatotic liver disease (MASLD) - previously known as nonalcoholic fatty liver disease (NAFLD) - is currently the most common chronic liver disease globally. Observational studies have reported that MASLD is independently associated with extrahepatic disorders, such as chronic kidney disease (CKD). Severe forms of MASLD (i.e. steatohepatitis and liver fibrosis) are even more strongly associated with the risk of incident kidney dysfunction. Hypothetically, MASLD could directly promote CKD through liver-derived endocrine and metabolic mediators, hemodynamic alterations, immune-mediated mechanisms and oxidative or cellular stress. However, proving that MASLD directly causes CKD is difficult due to the multiple shared cardiometabolic and systemic risk factors, such as obesity, hypertension and type 2 diabetes mellitus, which serve as confounding variables. Moreover, studies on the association between MASLD and CKD have differed in their designs, sampling methods, disease definitions and inclusion criteria, precluding more robust evidence supporting a causal relationship. Furthermore, few studies have explored specific issues, such as the new nomenclature for Steatotic Liver Disease, the relationship between these diseases in pediatric populations, the impact of MASLD plus alcohol intake (MetALD) on CKD, and therapeutic options targeting MASLD and CKD simultaneously. Answers to these issues are essential, as the appropriate management of patients with MASLD may prevent or ameliorate kidney dysfunction. The aims of the present study are to describe shared risk factors between MASLD and CKD, the possible direct pathogenic effect of MASLD on kidney structure and function, and gaps in the current literature, to indicate future research directions.
Keywords:
metabolic dysfunction-associated liver disease
; nonalcoholic fatty liver disease
; chronic kidney disease
; metabolic syndrome
; obesity
; diabetes mellitus
1. Introduction
The term metabolic dysfunction-associated steatotic liver disease (MASLD) was recently proposed as part of a new nomenclature system to replace nonalcoholic fatty liver disease (NALFD) and metabolic dysfunction-associated fatty liver disease (MAFLD) [1]. Due to its rapidly increasing incidence, MASLD has become the most common chronic liver disease throughout the world, the prevalence of which is approximately 38% of the adult population [2]. Most cases of MASLD consist of isolated hepatic steatosis, but 12% to 40% of these may evolve to metabolic dysfunction-associated steatohepatitis (MASH), which presents with inflammation and ballooning degeneration of hepatocytes. Of these, 35% develop early hepatic fibrosis, usually beginning in a perisinusoidal pattern. In 15% of such cases, progression to advanced fibrosis or cirrhosis occurs (Figure 1) [3]. As a result, MASLD is now the second leading cause of liver transplantation in the United States and Europe [4].
Some extrahepatic disorders, such as cardiovascular disease, extrahepatic cancers and chronic kidney disease (CKD), have also been shown to be associated with MASLD [5]. Indeed, the prevalence of CKD among the general population is around 10% but reaches 20%-50% among individuals with MASLD, aggravating the long-term economic burden as well as increasing morbidity and mortality rates [6,7,8].
Chronic kidney disease (CKD) is defined by persistent abnormalities in kidney function or structure for at least three months, typically with progressive decline. Diagnosis is based on a sustained glomerular filtration rate (GFR) below 60 ml/min/1.73 m² or evidence of kidney damage, such as albuminuria, abnormal urinary sediment, electrolyte or tubular disorders, structural abnormalities seen on imaging or histology, or a history of kidney transplantation [9].
Key histological features shared across all forms of CKD include interstitial fibrosis, tubular atrophy, global glomerulosclerosis, and arterial intimal thickening (Figure 2a) [10]. In contrast, certain findings may point to a specific underlying cause, such as diabetic nodular glomerulosclerosis (Figure 2b) [11].
MASLD and CKD share cardiometabolic risk factors, such as obesity, dyslipidemia, type 2 diabetes mellitus (T2DM), and hypertension [12,13]. However, MASLD has been shown to be independently associated with CKD even when adjusted for cardiometabolic covariates [8,14,15,16]. Hypothetically, MASLD could cause CKD through liver-induced specific dysregulations [17]. However, proving this independent association is difficult, as other systemic disorders of a genetic, dietary, infectious, or immunological nature have also been shown to predispose individuals to both MASLD and CKD. These disorders may serve as additional confounding variables that have not been uniformly included in studies [17,18,19,20,21,22,23,24].
This pathogenic complexity, along with nomenclature change from NAFLD to MAFLD and then MASLD, has given rise to considerable diversity in study designs. Furthermore, some specific research issues have not yet been widely investigated, which is the case for pediatric populations, the impact of MASLD combined with alcohol intake (MetALD) on kidney dysfunction, and outcomes in patients treated for both MASLD and CKD [25,26,27].
Filling these gaps in knowledge and clarifying the interplay between MASLD and CKD would allow clinicians to manage patients accordingly. For instance, risk stratification and the prevention and treatment of MASLD may be warranted if this condition proves to be associated with an increased risk of CKD [8,28,29].
The aim of the present study was to conduct a literature review on this relationship. After a brief summarization of the new steatotic liver disease nomenclature and its implications in research and clinical practice, we discuss pathogenic links between MASLD and CKD, including mechanisms through which MASLD may directly cause CKD. Finally, we address some gaps in the literature and provide directions for future research.
2. Bibliographic Search Strategy and Selection Criteria
The authors searched the PubMed database up to June 2025 for articles published in English using the following terms: “metabolic dysfunction-associated steatotic liver disease” OR “MASLD” OR “ steatotic liver disease” OR “SLD” OR “alcoholic liver disease” or ALD” OR “MASLD and increased alcohol intake” OR “MetALD” OR “metabolic dysfunction-associated fatty liver disease” OR “MAFLD” OR “non-alcoholic fatty liver disease” OR “NAFLD” OR “non-alcoholic steatohepatitis” OR “NASH” OR “metabolic dysfunction-associated steatohepatitis” OR “MASH” AND “chronic kidney disease” OR “CKD”. The authors performed additional queries using more specific terms: “epidemiology”, “pathogenesis”, “pediatric”, “children”, “management”, “obesity”, “diabetes”, “arterial hypertension", and “metabolic syndrome” The final selection was based on the relevance and novelty of the articles.
3. New Steatotic Liver Disease Nomenclature
Until 2020, fatty liver disease was divided into two mutually exclusive groups: NAFLD and alcoholic liver disease (ALD) [1,30]. The diagnosis of NAFLD was based on the exclusion of excessive alcohol intake and other competing causes of steatosis, such as viral hepatitis or drugs [31,32]. Despite its time-established use, the term NAFLD was criticized due to its focus on exclusionary criteria rather than emphasizing its relationship with metabolic syndrome [33].
In 2020, Eslam et al. suggested the term metabolic dysfunction-associated fatty liver Disease (MAFLD) to replace NAFLD [34]. The diagnosis of MAFLD is entirely inclusive, requiring steatosis plus one major metabolic criterion (T2DM or overweight/obesity) or – in lean, non-diabetic individuals – at least two cardiometabolic risk abnormalities, irrespective of alcohol intake or other competing causes of steatosis [34]. This has led to criticisms, as metabolic and non-metabolic etiologies can coexist in the same patient, leading to a lack of specificity and diagnostic inaccuracies [33,35,36]. Moreover, the word ‘fatty’ persisted in the MAFLD terminology, which is considered stigmatizing [1,30].
In 2023, steatotic liver disease (SLD) was recommended as a broad term to comprise the causes of liver steatosis [1]. SLD is divided into five subgroups: 1- MASLD (which includes major metabolic criteria but excludes alcohol consumption greater than 20 g/day for women and 30 g/day for men); 2- MetALD (consisting of MASLD plus alcohol intake 20-50 g/day for women and 30-60 g/day for men); 3- ALD (average alcohol intake > 50 g/day for women and > 60 g/day for men); 4- specific etiology SLD (including monogenic diseases, drug-induced liver injury, and viral hepatitis); and 5- cryptogenic SLD [1]. This terminology improves specificity and substitutes the word “fatty” for the more technical word “steatotic” [1].
As the diagnostic criteria for these three nomenclature systems are slightly different, the impact of the new MASLD criteria on research related to CKD has not yet been widely tested [2,37,38]. However, NAFLD, MAFLD, and MASLD are all related to metabolic syndrome and diagnostic agreement among these classifications is greater than 90%, according to some studies [33,38,39]. Therefore, the terms will be equivalent in this review and used in accordance with the respective references.
4. Shared Risk Factors Between MASLD and CKD
Metabolic syndrome-related conditions – such as obesity, insulin resistance, T2DM, hypertension, and dyslipidemia – are known to promote MASLD and CKD [13]. Other factors - including genetic polymorphisms, nutritional aspects, gut dysbiosis, aging, platelet activation, and sarcopenia - have more recently proved to be associated with MASLD and CKD, often with a bidirectional cause-and-effect relationship [7,40,41,42,43,44] (Figure 3).
4.1. Metabolic Syndrome
The prevalence of MASLD and CKD among individuals with obesity is 75% and 33%, respectively, which is much higher than the prevalence of these diseases in the general population (38% and 10%, respectively) [45,46]. Furthermore, individuals with MASLD and obesity have higher proportions of MASH (34%) and significant fibrosis (20%) [46,47]. Ectopic fat accumulation in the liver and kidneys may cause organ damage by direct compression or production of inflammatory cytokines, oxidative stress, procoagulant and fibrogenic factors, increased levels of leptin, and decreased levels of adiponectin [21,48,49,50]. Central obesity has been associated with the dysfunction of peroxisome proliferator-activated receptor-gamma (PPAR-γ), which is a regulator of fat storage and adipogenesis [49]. All these factors ultimately lead to increased insulin resistance, endothelial activation, thrombosis, fibrosis, hemodynamic disorders, and inflammation, aggravating both MASLD and CKD [25,38].
Insulin resistance and T2DM are also strongly linked to MASLD and CKD. According to a meta-analysis, the prevalence of NAFLD among individuals with T2DM is around 68%, which is almost twice that of the general population [51]. The prevalence of steatohepatitis (66%) and advanced fibrosis (15%) in this group is also higher than in non-diabetics, reflecting the further detrimental impact of insulin resistance on the progression of this liver disease [52,53].
T2DM is the most common etiology of CKD [54]. Insulin resistance stimulates fat accumulation in the kidney parenchyma and contributes to renal artery atherosclerosis, leading to macrovascular complications [11]. Hyperglycemia, in turn, generates advanced glycation end-products, promoting microvascular disease and glomerular injury, including nodular glomerulosclerosis, leading to proteinuria and the deterioration of the estimated glomerular filtration rate (eGFR) [55].
Atherosclerotic dyslipidemias and hypertension lead to the activation of the renin-angiotensin-aldosterone system [50,56]. Angiotensin II exacerbates insulin resistance and induces the progression of MAFLD and CKD through oxidative stress, parenchymal inflammation, and fibrosis [57,58]. Once installed, MASLD and CKD may worsen insulin resistance, dyslipidemia, and hypertension through inflammation, oxidative stress, uremia, metabolic acidosis, sedentarism, and further activation of the renin-angiotensin-aldosterone system [7].
4.2. Genetic Polymorphisms
Some genetic polymorphisms have been linked to NAFLD and CKD but the most relevant is the rs738409 C > G mutation in the patatin-like phospholipase domain-containing 3 gene (PNPLA3), which is present in liver and kidney tissues [24,43]. This gene variant causes lipid accumulation and organ inflammation and is associated with a higher risk of NAFLD/steatohepatitis and liver fibrosis as well as renal glomerular and tubular lesions, independently of metabolic factors [59].
Beyond PNPLA3, several genetic variants have been implicated in the shared pathophysiology of metabolic dysfunction-associated steatotic liver disease (MASLD) and chronic kidney disease (CKD). Notably, the TM6SF2 (rs58542926) and MBOAT7 (rs641738) variants are associated with increased hepatic steatosis and fibrosis, with emerging evidence linking them to renal impairment, possibly through systemic inflammation and lipid dysregulation. The GCKR (rs1260326) variant, which enhances hepatic lipogenesis via altered glucose metabolism, contributes to hepatic fat accumulation and may indirectly influence renal function through insulin resistance [60].
4.3. Nutritional Aspects and Gut Dysbiosis
Hypercaloric diets can result in lipid accumulation in the liver and kidneys [20,44]. Fructose, which is present in sweeteners, is particularly harmful, as its metabolism generates uric acid, promoting insulin resistance, dyslipidemia, and nephrotoxicity, and contributing to further fat deposition in the liver [49,61]. One experimental study showed that rats with impaired fructose absorption had less lipid accumulation and renal insufficiency when compared to normal controls [61].
Gut dysbiosis occurs when the microbiota undergoes a reduction in its normal diversity, which is usually associated with Western diets and metabolic syndrome [62]. In gut dysbiosis, the predominance of harmful bacteria, along with a reduction in beneficial bacterial populations, results in the production of nephrotoxins and hepatotoxins [20,63].
Dietary choline is converted to trimethylamine-N-oxide (TMAO) by harmful gut microbiota. TMAO promotes atherosclerosis, the activation of inflammatory pathways, and oxidative stress, potentially stimulating renal interstitial fibrosis [20,21]. TMAO also inhibits the farnesoid X receptor, which is a hepatic bile acid receptor that regulates bile acid homeostasis and balances glucose and lipid metabolism in multiple tissues [63,64].
Bacterial toxins may also damage tight junctions in the gut epithelia, increasing mucosal permeability. Thus, proinflammatory cytokines and lipopolysaccharides (endotoxins) enter portal and systemic circulation. After reaching the liver, lipopolysaccharides activate Toll-like receptors (TLR) on hepatocytes, Kupffer cells, and stellate cells, leading to hepatic fibrosis [65]. In the kidneys, TLR activation by endotoxins leads to fibrosis and inflammation. Moreover, systemic urea levels rise with the impairment of renal function, further increasing intestinal permeability, thus engendering a vicious cycle [54,66,67].
4.4. Aging
Low antioxidant capacity and mitochondrial function are common in older people [41,42]. Together, these conditions promote inflammation, fibrosis, and fat accumulation in individuals with NAFLD as well as renal interstitial fibrosis and atherosclerosis [42,68].
Furthermore, aging is associated with sarcopenia, decreased levels of adiponectin (an insulin sensitizer) and increased liver secretion of fetuin-A, which is a protein associated with insulin resistance, inflammation, adipogenesis, and atherogenesis [69].
Other age-related phenomena include damage to sinusoidal endothelial cells in the liver, increased serum levels of uric acid, and decreased urinary levels of klotho protein, which is a marker of vascular calcification and the progression of CKD [38].
4.5. Platelet Activation
Platelet activation also has a bidirectional relationship with NAFLD and CKD and is intertwined with cardiometabolic disorders. For instance, oxidative stress, very low-density lipoprotein cholesterol, and intestinal dysbiosis all contribute to excessive platelet activation [13,70]. Activated platelets secrete proinflammatory cytokines (IL-6, TNF-alpha) and growth factors, such as endothelial growth factor, platelet-derived growth factor, insulin-like growth factor 1(IGF-1), transforming growth factor (TGF)-beta, and fibroblast growth factor (FGF) [70,71]. These molecules promote oxidative stress, hypercoagulation, endothelial activation, and inflammation, ultimately leading to atherosclerosis and parenchymal fibrosis in the kidneys and liver [72,73]. In the opposite direction, MASLD and CKD promote platelet activation by inducing inflammation, endothelial activation, oxidative stress, and – in CKD – the accumulation of uremic toxins [40].
4.6. Sarcopenia
Another example of a bidirectional detrimental effect is found between MASLD/CKD and sarcopenia [40]. Sarcopenic muscles release myostatin, which is a member of the TGF-beta superfamily that can promote liver inflammation and the activation of hepatic stellate cells, culminating in liver fibrosis [74]. On the other hand, steatotic livers do not deal with energy substrates properly, often resulting in the catabolism of amino acids that would otherwise be used in muscle anabolism, thus aggravating sarcopenia [40,75]. Likewise, pro-inflammatory cytokines released by the liver accelerate muscle catabolism [75]. In cases of cirrhosis induced by NAFLD, hyperammonemia may aggravate the condition by inducing autophagy in myocytes [76].
Systemic inflammation and insulin resistance induced by sarcopenia worsens renal function [19]. In the opposite direction, CKD induces sarcopenia through low grade systemic inflammation, protein loss due to dialysis, accelerated protein catabolism, and reduced anabolism, along with metabolic acidosis and sedentarism [77].
5. MASLD as a Possible Direct Cause of CKD
Several studies have shown that MASLD is associated with CKD independently of many of the risk factors mentioned above [14,15,78,79,80,81,82,83,84,85]. This association is even more pronounced in the occurrence of severe liver disease (i.e., MASH and/or liver fibrosis) [7,15].
A meta-analysis showed that, compared with individuals without MAFLD at baseline, those with MAFLD had a greater risk of incident CKD even when adjusted for cardiovascular comorbidities (HR = 1.35 [95% CI: 1.18, 1.52]) [14]. Another meta-analysis revealed that NASH was associated with a higher incidence of CKD than steatosis alone (HR = 2.12 [95% CI: 1.42, 3.17]) [15]. Likewise, the incidence of CKD was higher among individuals with advanced fibrosis than those without this condition (HR = 3.29 [95% CI: 2.30–4.71]), also independently of cardiometabolic variables [15].
Table 1 summarizes the results of the meta-analyses and longitudinal studies addressing the association between MASLD and the risk of incident CKD.
These data from literature have led to the hypothesis that MASLD may directly affect kidney structure and function through intrinsic liver-driven mechanisms, as represented in Figure 4 and described below:
5.1. Endocrine and Metabolic Mediators
NAFLD not only develops as a result of insulin resistance but also actively contributes to its progression, establishing a vicious cycle [86]. Hepatic fat accumulation leads to the production of lipotoxic intermediates, pro-inflammatory cytokines and hepatokines which impair insulin signaling and disrupt insulin receptor pathways. Additionally, mitochondrial dysfunction and oxidative stress, along with endoplasmic reticulum stress exacerbate these effects [50,70,87]. Notably, insulin resistance induced by NAFLD has been shown to promote macrovascular and microvascular complications that lead to proteinuria and CKD, even before the onset of diabetes [88,89]. If overt diabetes emerges during the course of NAFLD, the decline in renal function may be even faster; indeed, diabetes is the main etiology of CKD [11,55].
Along with insulin resistance, liver-generated atherogenic dyslipidemia, characterized by elevated levels of triglyceride-rich lipoproteins, small dense LDL particles, and reduced HDL cholesterol, contributes macrovascular renal complications (atherosclerotic plaques), as well as systemic inflammation, endothelial dysfunction, and oxidative stress, all of which promote glomerular injury and tubulointerstitial fibrosis [50,70,90].
MASLD also alters liver secretion of hepatokines (hormone-like proteins that regulate systemic metabolic processes), aggravating renal injury. Hepatokines such as fetuin-A promote renal insulin resistance and inflammation, while proteins like angiopoietin-like protein 8 (ANGPTL8) and selenoprotein P are implicated in lipid imbalance and oxidative stress, exacerbating nephron damage [40,69,91].
Lastly, steatotic livers produce uremic toxins similar to those associated with gut dysbiosis, notably indoxyl sulfate, p-cresyl sulfate, and trimethylamine N-oxide (TMAO). Once in the bloodstream, these toxins accumulate in renal tissue, where they induce oxidative stress, and pro-inflammatory and pro-fibrotic signaling pathways, including those mediated by transforming growth factor-beta (TGF-β) [21,66].
5.2. Hemodynamic Alterations
MASLD can lead to subclinical portal hypertension even in the absence of cirrhosis, in a kind of hepatorenal reflex [92]. Indeed, increased intrahepatic vascular resistance may occur in pre-fibrotic stages of NAFLD as a consequence of fat accumulation and necro-inflammatory changes [93]. These changes may activate the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system, causing disturbances in renal perfusion, with consequent glomerular hyperfiltration and endothelial injury [58]. If hepatic fibrosis ensues, portal hypertension worsens, which is in line with evidence showing that NAFLD with fibrosis is more associated with the risk of developing CKD than steatosis alone [94]. Nevertheless, the hepatorenal reflex hypothesis, although interesting, requires further exploration in experimental and clinical research [40,95].
5.3. Immune-Mediated Mechanisms
MASLD, particularly when it progresses to MASH, leads to the intrahepatic production and systemic release of pro-inflammatory mediators such as tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), interleukin-1β (IL-1β) and C-reactive protein (CRP)[71,87]. These molecules circulate and act at distant sites, in a paracrine-like effect of liver inflammation, known as the “inflammatory spillover” hypothesis, which could explain how MASLD drives systemic immune activation [40,93,96]. In the kidney, these mediators may promote endothelial dysfunction, immune cell infiltration, mesangial expansion, and interstitial fibrosis.[21,49]
Since inflammation and the coagulation cascade are closely linked, pro-coagulant factors - such as plasminogen activator inhibitor-1 (PAI-1), tissue factor and thrombin - are usually activated as a consequence of the MASLD inflammatory environment [71,96]. PAI-1 inhibits fibrinolysis and contributes to renal interstitial fibrosis, while thrombin and tissue factor induce endothelial damage and microvascular thrombosis, leading to progressive obliteration of the renal microvasculature that supplies tubules and glomeruli, possibly contributing to nephron loss [18,95].
5.4. Oxidative and Cellular Stress Pathways
Steatosis and the necro-inflammatory alterations present in MASLD are significant sources of reactive oxygen species (ROS) due to mitochondrial overload and dysfunction. These ROS can be released into systemic circulation, damaging circulating proteins and lipoproteins, and promoting lipid peroxidation [96,97,98]. In renal endothelial and tubular epithelial cells, ROS can lead to inflammation, apoptosis, and fibrosis.[10,95]
Endoplasmic reticulum (ER) stress also occurs during MASLD progression, triggered by excessive free fatty acids and unfolded protein accumulation in hepatocytes. This results in systemic release of misfolded proteins and lipotoxic intermediates (e.g., diacylglycerols, ceramides), that can be harmful to renal tubular cells [7,17].
Importantly, ER stress and oxidative stress can both activate signaling pathways like the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-kB), upregulating immune cells recruitment and stimulating the production of pro-inflammatory cytokines, hence forming a self-perpetuating loop with inflammation and further damaging the liver and kidneys [21,71,87].
6. Gaps and Limitations in Literature
Coupled with the complexity of the pathogenic mechanisms linking MASLD and CKD, gaps and limitations in the literature further hamper the elucidation of the relationship between these conditions [7,8,17].
6.1. Heterogeneity Among Studies
Designs, sampling methods, disease definitions, and inclusion criteria have varied among studies [14,38]. This is exemplified by the results of a recent meta-analysis investigating the association between MAFLD and CKD, in which high heterogeneity was found among both cross-sectional and longitudinal studies (I2 = 97.7% and I2 = 84.6%, respectively) [14]. This interstudy diversity precludes proper comparisons between individual study results.
One of the main causes of heterogeneity is the multitude of shared risk factors between MASLD and CKD, which act as confounding variables. Studies have considered traditional cardiometabolic covariates but have not adjusted for other risk factors in multivariate analyses, such as gut dysbiosis, unhealthy diets, old age, and sarcopenia [42,74,99,100].
Another source of divergence among studies is the variation in sample sizes and diagnostic definitions. Large population-based studies have used screening methods for the diagnosis of NAFLD/MAFLD, such as ultrasound or serum biomarkers [84,101,102,103,104,105]. Although widely available, ultrasound is not sufficiently sensitive to detect steatosis levels of less than 20% and is inaccurate in individuals with obesity [106]. Low specificity is found with serum biomarkers due to being based on variables such as platelet count, liver enzymes, obesity, and diabetes status, all of which can be altered in multiple conditions other than NAFLD [107]. Moreover, few studies have used liver histology due to the invasiveness of biopsies, despite histology being the gold standard for the diagnosis of NAFLD, persisting as the only tool capable of distinguishing steatohepatitis from steatosis alone [97]. Such studies have usually had a cross-sectional design, small number of participants, and very specific inclusion criteria, impeding the generalization of the results [93,108,109,110,111].
Inclusion criteria for CKD have also been different among studies. Some studies have excluded albuminuria from the definition of CKD, whereas others have not [14,15]. Secondly, most studies define CKD as an eGFR < 60 mL/min/1.73 m2, which corresponds to CKD stages 3 to 5 [54,112]. Consequently, the relationship between NAFLD and early stages of CKD (1 and 2) is under-investigated [17]. Thirdly, eGFR is a proxy equation - based on age, gender, weight, and serum creatinine - to estimate the actual measured GFR (mGFR) [112]. Although mGFR is the gold standard for measuring renal function, it has not been used in research due to its cost and impracticality [10]. However, eGFR has a 30% rate of discordance with mGFR. For instance, eGFR underestimates mGFR in individuals with obesity and overestimates mGFR in older women and individuals with cirrhosis [112]. Lastly, as renal histology has not been used, we do not know if a specific kind of kidney injury is preferentially associated with MASLD [10,113].
With regards to ethnicity, most studies on the association between NAFLD and CKD have been conducted in Asia, the US, and western Europe and have reported different results [114,115]. In contrast, few studies have been conducted in other regions, such as Latin America, where the prevalence of NAFLD reaches 44.4% [2].
Lastly, although longitudinal studies have shown a higher incidence of CKD in individuals with MASLD, the bidirectional association between cardiometabolic disorders and these diseases raises the question of whether the opposite might also occur - i.e., CKD may be a predisposing factor for MASLD [25,49,116]. Indeed, CKD is known to promote dysglycemia, dyslipidemia, atherosclerosis, sarcopenia, and systemic inflammation - all of which are causes of liver steatosis [77,90,117]. In this respect, studies comparing the incidence of MASLD in individuals with and without CKD at baseline are still lacking [118].
6.2. Studies in Pediatric Populations
The estimated prevalence of MAFLD in overweight or obese children is 33.78% [119]. As in adults, it is associated with atherosclerosis, dyslipidemia, insulin resistance, and hypertension [25,120,121]. Despite the similarities to adult MAFLD with regards to epidemiology and pathogenesis, some histological differences are found [97]. For instance, lipid accumulation in children occurs preferentially in zone 1 hepatocytes or in a panacinar fashion and is usually associated with portal fibrosis and inflammation rather than ballooned hepatocytes and perisinusoidal fibrosis, as seen in adults [97,121]. Progression to steatohepatitis and cirrhosis may occur but the incidence of these conditions remains under-investigated [122,123]. Considering these differences and due to the scarcity of studies involving pediatric populations, the risk of children and adolescents developing CKD is largely unknown [25].
Pacifico et al. compared the prevalence of low eGFR or abnormal albuminuria among 268 overweight/obese children with NAFLD, 328 overweight/obese children without NAFLD, and 130 healthy normal-weight controls. NAFLD was independently associated with impaired eGFR and/or microalbuminuria (OR = 2.54 [95% CI: 1.16, 5.57]) [124]. In contrast, another study compared kidney function in 80 children with biopsy-proven NAFLD and 59 children of normal weight matched for age and sex. Despite higher levels of insulin resistance in the NAFLD group, albuminuria and creatinine clearance did not differ significantly between groups [89].
In terms of NAFLD severity, a recent study involving 1,164 children with biopsy-proven NAFLD/MASLD found that the prevalence of glomerular hyperfiltration was independently associated with significant liver fibrosis (OR = 1.45), but the incidence of kidney function deterioration did not differ according to NAFLD/MASLD severity in 2 years of follow-up [79]. Therefore, more prospective studies involving pediatric patients and longer follow-up periods are needed [125].
6.3. Impact of Alcohol Intake and MetALD
As alcohol intake and metabolic syndrome are common throughout the world, steatotic liver disease of a dual etiology (now termed MetALD) is expected to be frequent [126,127]. Studies have shown that MAFLD combined with alcohol consumption increases the risk of insulin resistance, T2DM, liver injury, and hepatic fibrosis in a dose-dependent manner according to the number of drinks per week and number of cardiometabolic factors [127,128,129]. From a mechanistic viewpoint, therefore, the risk of CKD would be expected to be higher in such individuals. Nevertheless, the impact of MetALD on kidney function remains unclear [26].
One study showed that moderate alcohol intake was in fact a protective factor for CKD in individuals with NAFLD (OR = 0.37 [95% CI 0.22, 0.65]), even after adjusting for confounding factors [130]. Along the same line, a meta-analysis of 15 cohort studies showed that individuals with moderate and high alcohol intake had a 24% (RR = 0.76 [95% CI: 0.70, .83)] and 21% (RR = 0.79 [95% CI: 0.71, 0.88]) lower risk of CKD, respectively, compared to non- or occasional drinkers [131]. Conversely, another study reported a higher risk of incident CKD in individuals with MASLD (HR = 1.20 [95% CI: 1.08, 1.33]) and those with ALD (HR = 1.41 [95% CI: 1.05, 1.88]) but not those with MetALD (HR = 1.11 [95% CI: 0.90, 1.36], p = 0.332) after adjusting for age, sex, eGFR, current smoking habit, T2DM, systemic hypertension, and dyslipidemia [83]. Considering these conflicting findings, further studies are needed to clarify the association between MetALD and CKD.
6.4. Treatment Options for Both MASLD and CKD
The management of MASLD and CKD is mainly focused on weight loss and lifestyle changes through exercise and hypocaloric diets [132]. These measures have been associated with improvements in liver inflammation and fibrosis [132,133].
In severe obesity, bariatric surgery has also proved to be associated with the regression of steatohepatitis, an improvement in the glomerular filtration rate, and lower levels of albuminuria [134]. Exercise is also recommended to avoid sarcopenia [28].
Resmetirom, which is a thyroid hormone receptor-beta (THR-beta) agonist, is the first drug approved by the US Food and Drug Administration for the treatment of NASH. In a phase 3 randomized controlled trial, resmetirom showed greater efficacy compared to placebo in terms of resolution of NASH and improvement in liver fibrosis [135]. The impact of this drug on kidney function remains to be investigated [136].
Less specific pharmacotherapy has also been used in the management of metabolic dysfunction-related diseases and cardiovascular diseases, with varying degrees of beneficial effects on both CKD and MAFLD [19]. Some classes of drugs that have shown favorable results in this context are renin-angiotensin system inhibitors, PPAR-γ agonists, incretin receptor agonists, and glucagon-like peptide receptor agonists [19,137].
New drugs targeting other pathogenic mechanisms are under investigation. Farnesoid X receptor agonists have been associated with a regression in both kidney and liver diseases by reducing inflammation, oxidative stress, fibrosis, and apoptosis [49]. Gut microbiome modulators, such as prebiotics and TMAO inhibitors, have shown conflicting results in preclinical studies and better definitions as to their efficacy are awaited [20]. Randomized control trials involving patients treated for MASLD and investigating the development of CKD as an endpoint are also warranted [7].
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
7. Conclusions and Future Directions for Research
MASLD and CKD have some risk factors in common, but MASLD may directly induce CKD. This association has been elucidated, but limitations in literature still need to be overcome, especially the gaps in research involving specific groups of patients. The recently adopted nomenclature - which is based on clearly defined subgroups - is likely to make inclusion criteria more homogeneous in future research. Given the systemic repercussions of MASLD, it is crucial that clinicians remain vigilant in monitoring patients with MASLD as a potential high-risk group for CKD. Early identification and intervention could be key in preventing the progression of both diseases.
Future research should focus on several important areas. First, a deeper understanding of the pathogenesis of MASLD on a cellular and molecular level is needed to identify the precise mechanisms by which it may lead to kidney damage. This will allow for the development of targeted treatments that can mitigate its harmful effects on the kidneys.
Recent diagnostic advances in MASLD are likely to enhance the precision of inclusion and exclusion criteria in future research. Among noninvasive tests, MRI and serum biomarkers are likely to become both more affordable and accurate as technologies continue to evolve [107,138]. Cutting-edge approaches include AI-assisted histological analysis, which enhances diagnostic consistency in biopsy interpretation, and multiomic profiling (e.g., metabolomics, proteomics) for identifying molecular signatures of disease progression [139].
An important area requiring attention is the pediatric population. Although MASLD is increasingly recognized in children and adolescents, its long-term renal consequences remain poorly defined. Future studies should explore early biomarkers of kidney injury in pediatric MASLD, to prevent the transition from early metabolic liver disease to multi-organ dysfunction in adulthood [25].
Another emerging priority is MetALD, a recently defined entity that combines features of metabolic dysfunction with alcohol-induced liver injury. The interplay between MetALD and kidney disease is largely unexplored but may be clinically significant, particularly as both alcohol use and metabolic disorders frequently coexist. Future research should investigate whether MetALD confers an additive or synergistic risk for CKD compared to MASLD or alcohol-related liver disease alone [140].
Lastly, as the global prevalence of obesity continues to rise, and as populations age, the burden of both MASLD and CKD is expected to increase. Addressing these growing public health challenges will require a concerted effort, involving not only scientific research but also public health strategies focused on promoting healthy lifestyles and mitigating the effects of an increasingly sedentary and nutritionally poor environment [28,141]. Clinicians and researchers alike must work together to clarify the full scope of the interplay between MASLD and CKD and to develop effective therapeutic strategies to combat this dual disease burden.
Author Contributions
Marcelo do Rego Maciel Souto Maior conceived the study, conducted the literature review, and wrote the first draft of the manuscript. Edmundo Pessoa Lopes and Emilia Chagas Costa supervised the research and critically revised the manuscript for important intellectual content. Nathália de Lacerda Interaminense Ribeiro and Hannah Vicentini Vitoriano Silva contributed to data organization and prepared the figures and tables. All authors reviewed and approved the final version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
none.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MASLD | Metabolic dysfunction-associated steatotic liver disease |
| NAFLD | Nonalcoholic fatty liver disease |
| CKD | Chronic kidney disease |
| MetALD | MASLD abd increased alcohol intake |
| MAFLD | Metabolic dysfunction-associated fatty liver disease |
| MASH | Metabolic dysfunction-associated steatohepatitis |
| NASH | Nonalcoholic steatohepatitis |
| GFR | Glomerular filtration rate |
| e-GFR | Estimated glomerular filtration rate |
| m-GFR | Measured glomerular filtration rate |
| T2DM | Type 2 diabetes mellitus |
| ALD | Alcoholic liver disease |
| SLD | Steatotic liver disease |
| PPAR-γ | Peroxisome proliferator-activated receptor-gamma |
| PNPLA3 | Patatin-like phospholipase domain-containing 3 gene |
| TMAO | Trimethylamine-N-oxide |
| TLR | Toll-like receptor |
| IL-6 | Interleukin-6 |
| IL-1β | Interleukin-1 beta |
| TNF-α | Tumour necrosis factor-alpha |
| TGF-β | Transforming growth factor-beta |
| IGF-1 | Insulin-like growth factor-1 |
| FGF | Fibroblast growth factor |
| HR | Hazard ratio |
| FLI | Fatty liver index |
| CI | Confidence interval |
| ICD-10 | International Classification of Diseases - tenth revision |
| UACR | Urinary albumin-creatinine ratio |
| OR | Odds ratio |
| RR | Relative risk |
| LDL | Low-density lipoprotein |
| HDL | High- density lipoprotein |
| ANGPTL8 | Angiopoietin-like protein 8 |
| RAAS | Renin-angiotensin-aldosterone system |
| CRP | C-reactive protein |
| ROS | Reactive oxygen species |
| NF-KB | Kappa-light-chain-enhancer of activated B cells |
| ER | Endoplasmic reticulum |
| PAI-1 | Plasminogen activator inhibitor-1 |
References
- Rinella ME, Lazarus J V., Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 2023;78:1966–86. [CrossRef]
- Younossi ZM, Kalligeros M, Henry L. Epidemiology of metabolic dysfunction-associated steatotic liver disease. Clin Mol Hepatol 2025;31:S32–50. [CrossRef]
- [Lekakis V, Papatheodoridis G V. Natural history of metabolic dysfunction-associated steatotic liver disease. Eur J Intern Med 2024;122:3–10. [CrossRef]
- Devarbhavi H, Asrani SK, Arab JP, Nartey YA, Pose E, Kamath PS. Global burden of liver disease: 2023 update. J Hepatol 2023;79:516–37. [CrossRef]
- Adinolfi LE, Marrone A, Rinaldi L, Nevola R, Izzi A, Sasso FC. Metabolic dysfunction-associated steatotic liver disease (MASLD): a systemic disease with a variable natural history and challenging management. Explor Med 2025;6. [CrossRef]
- Miao L, Targher G, Byrne CD, Cao YY, Zheng MH. Current status and future trends of the global burden of MASLD. Trends in Endocrinology and Metabolism 2024;35:697–707. [CrossRef]
- Sun D-Q, Targher G, Byrne CD, Wheeler DC, Wong VW-S, Fan J-G, et al. An international Delphi consensus statement on metabolic dysfunction-associated fatty liver disease and risk of chronic kidney disease. Hepatobiliary Surg Nutr 2023;12:386–403. [CrossRef]
- Al Ashi S, Rizvi AA, Rizzo M. Altered kidney function in fatty liver disease: confronting the “MAFLD-renal syndrome.” Frontiers in Clinical Diabetes and Healthcare 2025;5. [CrossRef]
- KDIGO W. Chapter 1: Definition and classification of CKD. Kidney Int Suppl (2011) 2013;3:19–62. [CrossRef]
- Trevisani F, Di Marco F, Capitanio U, Dell’Antonio G, Cinque A, Larcher A, et al. Renal histology across the stages of chronic kidney disease. J Nephrol 2021;34:699–707. [CrossRef]
- Oshima M, Shimizu M, Yamanouchi M, Toyama T, Hara A, Furuichi K, et al. Trajectories of kidney function in diabetes: a clinicopathological update. Nat Rev Nephrol 2021;17:740–50. [CrossRef]
- Kaya E, Yilmaz Y. Metabolic-associated Fatty Liver Disease (MAFLD): A Multi-systemic Disease Beyond the Liver. J Clin Transl Hepatol 2022;10:329–38. [CrossRef]
- Bilson J, Hydes TJ, McDonnell D, Buchanan RM, Scorletti E, Mantovani A, et al. Impact of Metabolic Syndrome Traits on Kidney Disease Risk in Individuals with MASLD: A UK Biobank Study. Liver International 2024. [CrossRef]
- Agustanti N, Soetedjo NNM, Damara FA, Iryaningrum MR, Permana H, Bestari MB, et al. The association between metabolic dysfunction-associated fatty liver disease and chronic kidney disease: A systematic review and meta-analysis. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 2023;17:102780. [CrossRef]
- Musso G, Gambino R, Tabibian JH, Ekstedt M, Kechagias S, Hamaguchi M, et al. Association of Non-alcoholic Fatty Liver Disease with Chronic Kidney Disease: A Systematic Review and Meta-analysis. PLoS Med 2014;11:e1001680. [CrossRef]
- Mantovani A, Petracca G, Beatrice G, Csermely A, Lonardo A, Schattenberg JM, et al. Non-alcoholic fatty liver disease and risk of incident chronic kidney disease: an updated meta-analysis. Gut 2022;71:156–62. [CrossRef]
- Byrne CD, Targher G. NAFLD as a driver of chronic kidney disease. J Hepatol 2020;72:785–801. [CrossRef]
- Lonardo A, Mantovani A, Targher G, Baffy G. Nonalcoholic Fatty Liver Disease and Chronic Kidney Disease: Epidemiology, Pathogenesis, and Clinical and Research Implications. Int J Mol Sci 2022;23:13320. [CrossRef]
- Zhang XL, Gu Y, Zhao J, Zhu PW, Chen WY, Li G, et al. Associations between skeletal muscle strength and chronic kidney disease in patients with MASLD. Communications Medicine 2025;5. [CrossRef]
- Caussy C, Rieusset J, Koppe L. The Gut Microbiome and the Gut-Liver-Kidney Axis in Metabolic-Associated Steatotic Liver Disease and Chronic Kidney Disease. Clinical Journal of the American Society of Nephrology 2025. [CrossRef]
- Gusev E, Solomatina L, Zhuravleva Y, Sarapultsev A. The Pathogenesis of End-Stage Renal Disease from the Standpoint of the Theory of General Pathological Processes of Inflammation. Int J Mol Sci 2021;22:11453. [CrossRef]
- Mambrini SP, Grillo A, Colosimo S, Zarpellon F, Pozzi G, Furlan D, et al. Diet and physical exercise as key players to tackle MASLD through improvement of insulin resistance and metabolic flexibility. Front Nutr 2024;11. [CrossRef]
- Valenzuela PL, Carrera-Bastos P, Castillo-García A, Lieberman DE, Santos-Lozano A, Lucia A. Obesity and the risk of cardiometabolic diseases. Nat Rev Cardiol 2023;20:475–94. [CrossRef]
- Romeo S, Kozlitina J, Xing C, Pertsemlidis A, Cox D, Pennacchio LA, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2008;40:1461–5. [CrossRef]
- Nardolillo M, Rescigno F, Bartiromo M, Piatto D, Guarino S, Marzuillo P, et al. Interplay between metabolic dysfunction-associated fatty liver disease and renal function: An intriguing pediatric perspective. World J Gastroenterol 2024;30:2081–6. [CrossRef]
- Ciardullo S, Mantovani A, Morieri ML, Muraca E, Invernizzi P, Perseghin G. Impact of MASLD and MetALD on clinical outcomes: A meta-analysis of preliminary evidence. Liver International 2024;44:1762–7. [CrossRef]
- Stefan N, Yki-Järvinen H, Neuschwander-Tetri BA. Metabolic dysfunction-associated steatotic liver disease: heterogeneous pathomechanisms and effectiveness of metabolism-based treatment. Lancet Diabetes Endocrinol 2025;13:134–48. [CrossRef]
- Byrne CD, Armandi A, Pellegrinelli V, Vidal-Puig A, Bugianesi E. Μetabolic dysfunction-associated steatotic liver disease: a condition of heterogeneous metabolic risk factors, mechanisms and comorbidities requiring holistic treatment. Nat Rev Gastroenterol Hepatol 2025. [CrossRef]
- Pipitone RM, Ciccioli C, Infantino G, La Mantia C, Parisi S, Tulone A, et al. MAFLD: a multisystem disease. Ther Adv Endocrinol Metab 2023;14:204201882211455. [CrossRef]
- Loomba R, Wong VW. Implications of the new nomenclature of steatotic liver disease and definition of metabolic dysfunction-associated steatotic liver disease. Aliment Pharmacol Ther 2024;59:150–6. [CrossRef]
- Diaz LA, Ajmera V, Arab JP, Huang DQ, Hsu C, Lee BP, et al. An Expert Consensus Delphi Panel in MetALD: Opportunities and Challenges in Clinical Practice. Clinical Gastroenterology and Hepatology 2025. [CrossRef]
- Kanwal F, Neuschwander-Tetri BA, Loomba R, Rinella ME. Metabolic dysfunction-associated steatotic liver disease: Update and impact of new nomenclature on the American Association for the Study of Liver Diseases practice guidance on nonalcoholic fatty liver disease. Hepatology 2024;79:1212–9. [CrossRef]
- Noureddin M, Wei L, Castera L, Tsochatzis EA. Embracing Change: From Nonalcoholic Fatty Liver Disease to Metabolic Dysfunction-Associated Steatotic Liver Disease Under the Steatotic Liver Disease Umbrella. Clinical Gastroenterology and Hepatology 2024;22:9–11. [CrossRef]
- Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J Hepatol 2020;73:202–9. [CrossRef]
- Gofton C, Upendran Y, Zheng MH, George J. MAFLD: How is it different from NAFLD? Clin Mol Hepatol 2023;29:S17–31. [CrossRef]
- Pennisi G, Infantino G, Celsa C, Di Maria G, Enea M, Vaccaro M, et al. Clinical outcomes of MAFLD versus NAFLD: A meta-analysis of observational studies. Liver International 2024. [CrossRef]
- Sripongpun P, Kaewdech A, Udompap P, Kim WR. Characteristics and long-term mortality of individuals with MASLD, MetALD, and ALD, and the utility of SAFE score. JHEP Reports 2024;6. [CrossRef]
- Bilson J, Mantovani A, Byrne CD, Targher G. Steatotic liver disease, MASLD and risk of chronic kidney disease. Diabetes Metab 2024;50:101506. [CrossRef]
- Suzuki K, Tamaki N, Kurosaki M, Takahashi Y, Yamazaki Y, Uchihara N, et al. Concordance between metabolic dysfunction-associated steatotic liver disease and nonalcoholic fatty liver disease. Hepatology Research 2024;54:600–5. [CrossRef]
- Sandireddy R, Sakthivel S, Gupta P, Behari J, Tripathi M, Singh BK. Systemic impacts of metabolic dysfunction-associated steatotic liver disease (MASLD) and metabolic dysfunction-associated steatohepatitis (MASH) on heart, muscle, and kidney related diseases. Front Cell Dev Biol 2024;12. [CrossRef]
- O’Sullivan ED, Hughes J, Ferenbach DA. Renal Aging: Causes and Consequences. Journal of the American Society of Nephrology 2017;28:407–20. [CrossRef]
- Du K, Wang L, Jun JH, Dutta RK, Maeso-Díaz R, Oh SH, et al. Aging promotes metabolic dysfunction-associated steatotic liver disease by inducing ferroptotic stress. Nat Aging 2024;4:949–68. [CrossRef]
- Hakim A, Lin KH, Schwantes-An TH, Abreu M, Tan J, Guo X, et al. A comprehensive evaluation of candidate genetic polymorphisms in a large histologically characterized MASLD cohort using a novel framework. Hepatol Commun 2025;9. [CrossRef]
- Jurek JM, Zablocka-Sowinska K, Clavero Mestres H, Reyes Gutiérrez L, Camaron J, Auguet T. The Impact of Dietary Interventions on Metabolic Outcomes in Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD) and Comorbid Conditions, Including Obesity and Type 2 Diabetes. Nutrients 2025;17. [CrossRef]
- Prasad R, Jha RK, Keerti A. Chronic Kidney Disease: Its Relationship With Obesity. Cureus 2022. [CrossRef]
- Quek J, Chan KE, Wong ZY, Tan C, Tan B, Lim WH, et al. Global prevalence of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in the overweight and obese population: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2023;8:20–30. [CrossRef]
- Younossi ZM, Zelber-Sagi S, Lazarus J V., Wai-Sun Wong V, Yilmaz Y, Duseja A, et al. Global Consensus Recommendations for Metabolic Dysfunction-Associated Steatotic Liver Disease and Steatohepatitis. Gastroenterology 2025. [CrossRef]
- Carvalho KD, Daltro C, Daltro C, Cotrim HP. Renal injury and metabolic dysfunction-associated steatotic liver disease in patients with obesity. Arq Gastroenterol 2025;62. [CrossRef]
- Theofilis P, Vordoni A, Kalaitzidis RG. Interplay between metabolic dysfunction-associated fatty liver disease and chronic kidney disease: Epidemiology, pathophysiologic mechanisms, and treatment considerations. World J Gastroenterol 2022;28:5691–706. [CrossRef]
- Neeland IJ, Ross R, Després JP, Matsuzawa Y, Yamashita S, Shai I, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol 2019;7:715–25. [CrossRef]
- Younossi ZM, Golabi P, Price JK, Owrangi S, Gundu-Rao N, Satchi R, et al. The Global Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis Among Patients With Type 2 Diabetes. Clinical Gastroenterology and Hepatology 2024;22:1999-2010.e8. [CrossRef]
- Inukai Y, Ito T, Yokoyama S, Yamamoto K, Imai N, Ishizu Y, et al. Type 2 Diabetes and Hypertension as Risk Factors for Advanced Fibrosis in Biopsy Proven Metabolic Dysfunction–Associated Steatotic Liver Disease. J Dig Dis 2025. [CrossRef]
- Younossi ZM, Golabi P, de Avila L, Paik JM, Srishord M, Fukui N, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J Hepatol 2019;71:793–801. [CrossRef]
- Francis A, Harhay MN, Ong ACM, Tummalapalli SL, Ortiz A, Fogo AB, et al. Chronic kidney disease and the global public health agenda: an international consensus. Nat Rev Nephrol 2024;20:473–85. [CrossRef]
- Furuichi K, Shimizu M, Yamanouchi M, Hoshino J, Sakai N, Iwata Y, et al. Clinicopathological features of fast eGFR decliners among patients with diabetic nephropathy. BMJ Open Diabetes Res Care 2020;8:e001157. [CrossRef]
- Gao Z, Deng H, Qin B, Bai L, Li J, Zhang J. Impact of hypertension on liver fibrosis in patients with metabolic dysfunction-associated fatty liver disease 2025. [CrossRef]
- Matthew Morris E, Fletcher JA, Thyfault JP, Scott Rector R. The role of angiotensin II in nonalcoholic steatohepatitis. Mol Cell Endocrinol 2013;378:29–40. [CrossRef]
- Ng WH, Yeo YH, Kim H, Seki E, Rees J, Ma KS-K, et al. Renin-angiotensin-aldosterone system inhibitor use improves clinical outcomes in patients with metabolic dysfunction-associated steatotic liver diseases: Target trial emulation using real-world data. Hepatology 2025. [CrossRef]
- Mantovani A, Targher G. PNPLA3 variation and kidney disease. Liver International 2025;45. [CrossRef]
- Rocha S, Oliveira CP, Stefano JT, Yokogawa RP, Gomes-Gouvea M, Zitelli PMY, et al. Polymorphism’s MBOAT7 as Risk and MTARC1 as Protection for Liver Fibrosis in MASLD. Int J Mol Sci 2025;26:6406. [CrossRef]
- Fan C-Y, Wang M-X, Ge C-X, Wang X, Li J-M, Kong L-D. Betaine supplementation protects against high-fructose-induced renal injury in rats. J Nutr Biochem 2014;25:353–62. [CrossRef]
- Jiang J, Liu Y, Yang H, Ma Z, Liu W, Zhao M, et al. Dietary fiber intake, genetic predisposition of gut microbiota, and the risk of metabolic dysfunction-associated steatotic liver disease. Food Research International 2025;211:116497. [CrossRef]
- Buchynskyi M, Kamyshna I, Halabitska I, Petakh P, Kunduzova O, Oksenych V, et al. Unlocking the gut-liver axis: microbial contributions to the pathogenesis of metabolic-associated fatty liver disease. Front Microbiol 2025;16. [CrossRef]
- Zhang D, Wang Q, Li D, Chen S, Chen J, Zhu X, et al. Gut microbiome composition and metabolic activity in metabolic-associated fatty liver disease. Virulence 2025;16. [CrossRef]
- Woo C, Jeong W-I. Immunopathogenesis of liver fibrosis in steatotic liver disease. Clin Mol Hepatol 2024. [CrossRef]
- Farris AB, Colvin RB. Renal interstitial fibrosis: Mechanisms and evaluation. Curr Opin Nephrol Hypertens 2012;21:289–300. [CrossRef]
- Villarroel C, Karim G, Sehmbhi M, Debroff J, Weisberg I, Dinani A. Advanced Fibrosis in Metabolic Dysfunction-Associated Steatotic Liver Disease Is Independently Associated With Reduced Renal Function. Gastro Hep Advances 2024;3:122–7. [CrossRef]
- Hill GS, Heudes D, Barié J. Morphometric study of arterioles and glomeruli in the aging kidney suggests focal loss of autoregulation 1. vol. 63. 2003.
- Chekol Abebe E, Tilahun Muche Z, Behaile T/Mariam A, Mengie Ayele T, Mekonnen Agidew M, Teshome Azezew M, et al. The structure, biosynthesis, and biological roles of fetuin-A: A review. Front Cell Dev Biol 2022;10. [CrossRef]
- Castillo-Núñez Y, Almeda-Valdes P, González-Gálvez G, Arechavaleta-Granell M del R. Metabolic dysfunction-associated steatotic liver disease and atherosclerosis. Curr Diab Rep 2024;24:158–66. [CrossRef]
- Hammerich L, Tacke F. Hepatic inflammatory responses in liver fibrosis. Nat Rev Gastroenterol Hepatol 2023;20:633–46. [CrossRef]
- Norman JT, Clark IM, Garcia PL. Hypoxia promotes fibrogenesis in human renal fibroblasts. vol. 58. 2000.
- Elpek GÖ. Cellular and molecular mechanisms in the pathogenesis of liver fibrosis: An update. World J Gastroenterol 2014;20:7260. [CrossRef]
- Deng C, Ou Q, Ou X, Pan D. Association between non-alcoholic fatty liver disease and risk of sarcopenia: a systematic review and meta-analysis. BMJ Open 2024;14:e078933. [CrossRef]
- Altajar S, Baffy G. Skeletal Muscle Dysfunction in the Development and Progression of Nonalcoholic Fatty Liver Disease. J Clin Transl Hepatol 2020;8:1–10. [CrossRef]
- Zhang F, Liu L, Li W. Correlation of sarcopenia with progression of liver fibrosis in patients with metabolic dysfunction-associated steatotic liver disease: a study from two cohorts in China and the United States. Nutr J 2025;24:6. [CrossRef]
- Wilkinson TJ, Miksza J, Yates T, Lightfoot CJ, Baker LA, Watson EL, et al. Association of sarcopenia with mortality and end-stage renal disease in those with chronic kidney disease: a UK Biobank study. J Cachexia Sarcopenia Muscle 2021;12:586–98. [CrossRef]
- Liu W, Sun X. Does metabolic dysfunction-associated fatty liver disease increase the risk of chronic kidney disease? A meta-analysis of cohort studies. BMC Nephrol 2024;25:467. [CrossRef]
- Mouzaki M, Yates KP, Arce-Clachar AC, Behling C, Blondet NM, Fishbein MH, et al. Renal impairment is prevalent in pediatric NAFLD/MASLD and associated with disease severity. J Pediatr Gastroenterol Nutr 2024;79:238–49. [CrossRef]
- Zuo G, Xuan L, Xin Z, Xu Y, Lu J, Chen Y, et al. New Nonalcoholic Fatty Liver Disease and Fibrosis Progression Associate with the Risk of Incident Chronic Kidney Disease. Journal of Clinical Endocrinology and Metabolism 2021;106:E3957–68. [CrossRef]
- Sanyal AJ, Van Natta ML, Clark J, Neuschwander-Tetri BA, Diehl A, Dasarathy S, et al. Prospective Study of Outcomes in Adults with Nonalcoholic Fatty Liver Disease. New England Journal of Medicine 2021;385:1559–69. [CrossRef]
- Liang Y, Chen H, Liu Y, Hou X, Wei L, Bao Y, et al. Association of MAFLD with Diabetes, Chronic Kidney Disease, and Cardiovascular Disease: A 4.6-Year Cohort Study in China. Journal of Clinical Endocrinology and Metabolism 2022;107:88–97. [CrossRef]
- Mori K, Tanaka M, Sato T, Akiyama Y, Endo K, Ogawa T, et al. Metabolic dysfunction-associated steatotic liver disease (SLD) and alcohol-associated liver disease, but not SLD without metabolic dysfunction, are independently associated with new onset of chronic kidney disease during a 10-year follow-up period. Hepatology Research 2024. [CrossRef]
- Heo JH, Lee MY, Kim SH, Zheng M-H, Byrne CD, Targher G, et al. Comparative associations of non-alcoholic fatty liver disease and metabolic dysfunction-associated steatotic liver disease with risk of incident chronic kidney disease: a cohort study. Hepatobiliary Surg Nutr 2024;0:0–0. [CrossRef]
- Gao J, Li Y, Zhang Y, Zhan X, Tian X, Li J, et al. Severity and Remission of Metabolic Dysfunction–Associated Fatty/Steatotic Liver Disease With Chronic Kidney Disease Occurrence. J Am Heart Assoc 2024;13. [CrossRef]
- Zhang W, Song WJ, Chen W, Pan Z, Zhang J, Fan L, et al. Metabolic dysfunction-associated steatotic liver disease-related hepatic fibrosis increases risk of insulin resistance, type 2 diabetes, and chronic kidney disease. Eur J Gastroenterol Hepatol 2024;36:802–10. [CrossRef]
- Targher G, Bertolini L, Rodella S, Lippi G, Franchini M, Zoppini G, et al. NASH Predicts Plasma Inflammatory Biomarkers Independently of Visceral Fat in Men. Obesity 2008;16:1394–9. [CrossRef]
- Yang T, Yang B, Yin J, Hou C, Wang Q. Targeting Insulin Resistance and Liver Fibrosis: CKD Screening Priorities in MASLD. Biomedicines 2025;13. [CrossRef]
- Manco M, Ciampalini P, DeVito R, Vania A, Cappa M, Nobili V. Albuminuria and insulin resistance in children with biopsy proven non-alcoholic fatty liver disease. Pediatric Nephrology 2009;24:1211–7. [CrossRef]
- Mitrofanova A, Merscher S, Fornoni A. Kidney lipid dysmetabolism and lipid droplet accumulation in chronic kidney disease. Nat Rev Nephrol 2023;19:629–45. [CrossRef]
- Pal D, Dasgupta S, Kundu R, Maitra S, Das G, Mukhopadhyay S, et al. Fetuin-A acts as an endogenous ligand of TLR4 to promote lipid-induced insulin resistance. Nat Med 2012;18:1279–85. [CrossRef]
- Baffy G, Bosch J. Overlooked subclinical portal hypertension in non-cirrhotic NAFLD: Is it real and how to measure it? J Hepatol 2022;76:458–63. [CrossRef]
- An JN, Joo SK, Koo BK, Kim JH, Oh S, Kim W. Portal inflammation predicts renal dysfunction in patients with nonalcoholic fatty liver disease. Hepatol Int 2020;14:798–807. [CrossRef]
- Gurun M, Brennan P, Handjiev S, Khatib A, Leith D, Dillon JF, et al. Increased risk of chronic kidney disease and mortality in a cohort of people diagnosed with metabolic dysfunction associated steatotic liver disease with hepatic fibrosis. PLoS One 2024;19. [CrossRef]
- Lonardo A. Association of NAFLD/NASH, and MAFLD/MASLD with chronic kidney disease: an updated narrative review. Metabolism and Target Organ Damage 2024;4. [CrossRef]
- Sun W, Fang Y, Zhou B, Mao G, Cheng J, Zhang X, et al. The association of systemic inflammatory biomarkers with non-alcoholic fatty liver disease: a large population-based cross-sectional study. Prev Med Rep 2024;37:102536. [CrossRef]
- Lai J, Wang HL, Zhang X, Wang H, Liu X. Pathologic Diagnosis of Nonalcoholic Fatty Liver Disease. Arch Pathol Lab Med 2022;146:940–6. [CrossRef]
- Yoneda M, Kobayashi T, Iwaki M, Nogami A, Saito S, Nakajima A. Nonalcoholic Fatty Liver Disease as a Systemic Disease and the Need for Multidisciplinary Care. Gut Liver 2023;17:843–52. [CrossRef]
- Abdallah H, Khalil M, Awada E, Lanza E, Di Ciaula A, Portincasa P. Metabolic dysfunction-associated steatotic liver disease (MASLD). Assessing metabolic dysfunction, cardiovascular risk factors, and lifestyle habits. Eur J Intern Med 2025. [CrossRef]
- Liu A, Huang M, Xi Y, Deng X, Xu K. Orchestration of Gut–Liver-Associated Transcription Factors in MAFLD: From Cross-Organ Interactions to Therapeutic Innovation. Biomedicines 2025;13. [CrossRef]
- Sirota JC, McFann K, Targher G, Chonchol M, Jalal DI. Association between nonalcoholic liver disease and chronic kidney disease: An ultrasound analysis from NHANES 1988-1994. Am J Nephrol 2012;36:466–71. [CrossRef]
- Hydes TJ, Kennedy OJ, Buchanan R, Cuthbertson DJ, Parkes J, Fraser SDS, et al. The impact of non-alcoholic fatty liver disease and liver fibrosis on adverse clinical outcomes and mortality in patients with chronic kidney disease: a prospective cohort study using the UK Biobank. BMC Med 2023;21. [CrossRef]
- Cao Y, Deng Y, Wang J, Zhao H, Zhang J, Xie W. The association between NAFLD and risk of chronic kidney disease: a cross-sectional study. Ther Adv Chronic Dis 2021;12:204062232110486. [CrossRef]
- Gbadamosi SO, Nagelhout E, Sienko D, Lamarre N, Noshad S, Ding Y, et al. Association of Index and Changes in Fibrosis-4 Score with Outcomes in Metabolic Dysfunction-Associated Steatohepatitis. Gastro Hep Advances 2025:100666. [CrossRef]
- Deng Y, Zhao Q, Gong R. Association between metabolic associated fatty liver disease and chronic kidney disease: A cross-sectional study from NHANES 2017–2018. Diabetes, Metabolic Syndrome and Obesity 2021;14:1751–61. [CrossRef]
- Sumida Y. Limitations of liver biopsy and non-invasive diagnostic tests for the diagnosis of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. World J Gastroenterol 2014;20:475. [CrossRef]
- Minichmayr IK, Plan EL, Weber B, Ueckert S. A Model-Based Evaluation of Noninvasive Biomarkers to Reflect Histological Nonalcoholic Fatty Liver Disease Scores. Pharm Res 2024. [CrossRef]
- Targher G, Pichiri I, Zoppini G, Trombetta M, Bonora E. Increased prevalence of chronic kidney disease in patients with Type 1 diabetes and non-alcoholic fatty liver. Diabetic Medicine 2012;29:220–6. [CrossRef]
- Targher G, Bertolini L, Rodella S, Lippi G, Zoppini G, Chonchol M. Relationship between Kidney Function and Liver Histology in Subjects with Nonalcoholic Steatohepatitis. Clinical Journal of the American Society of Nephrology 2010;5:2166–71. [CrossRef]
- Targher G, Bertolini L, Rodella S, Zoppini G, Lippi G, Day C, et al. Non-alcoholic fatty liver disease is independently associated with an increased prevalence of chronic kidney disease and proliferative/laser-treated retinopathy in type 2 diabetic patients. Diabetologia 2008;51:444–50. [CrossRef]
- Targher G, Bertolini L, Chonchol M, Rodella S, Zoppini G, Lippi G, et al. Non-alcoholic fatty liver disease is independently associated with an increased prevalence of chronic kidney disease and retinopathy in type 1 diabetic patients. Diabetologia 2010;53:1341–8. [CrossRef]
- Porrini E, Ruggenenti P, Luis-Lima S, Carrara F, Jiménez A, de Vries APJ, et al. Estimated GFR: time for a critical appraisal. Nat Rev Nephrol 2019;15:177–90. [CrossRef]
- Niizuma S, Nakamura S, Ishibashi-Ueda H, Yoshihara F, Kawano Y. Kidney function and histological damage in autopsy subjects with myocardial infarction. Ren Fail 2011;33:847–52. [CrossRef]
- Zhang M, Lin S, Wang M, Huang J, Liu S, Wu S, et al. Association between NAFLD and risk of prevalent chronic kidney disease: why there is a difference between east and west? BMC Gastroenterol 2020;20:139. [CrossRef]
- Miller KC, Geyer B, Alexopoulos AS, Moylan CA, Pagidipati N. Disparities in Metabolic Dysfunction-Associated Steatotic Liver Disease Prevalence, Diagnosis, Treatment, and Outcomes: A Narrative Review. Dig Dis Sci 2024. [CrossRef]
- Zhao D, Zheng X, Wang L, Xie Y, Chen Y, Zhang Y. Overlap prevalence and interaction effect of cardiometabolic risk factors for metabolic dysfunction-associated steatotic liver disease. Nutrition and Metabolism 2025;22. [CrossRef]
- Webster AC, Nagler E V., Morton RL, Masson P. Chronic Kidney Disease. The Lancet 2017;389:1238–52. [CrossRef]
- Pan Z, Alqahtani SA, Eslam M. MAFLD and chronic kidney disease: two sides of the same coin? Hepatol Int 2023;17:519–21. [CrossRef]
- Liu J, Mu C, Li K, Luo H, Liu Y, Li Z. Estimating Global Prevalence of Metabolic Dysfunction-Associated Fatty Liver Disease in Overweight or Obese Children and Adolescents: Systematic Review and Meta-Analysis. Int J Public Health 2021;66. [CrossRef]
- Pacifico L, Nobili V, Anania C, Verdecchia P, Chiesa C. Pediatric nonalcoholic fatty liver disease, metabolic syndrome and cardiovascular risk. World J Gastroenterol 2011;17:3082–91. [CrossRef]
- Mitsinikos T, Mrowczynski-Hernandez P, Kohli R. Pediatric Nonalcoholic Fatty Liver Disease. Pediatr Clin North Am 2021;68:1309–20. [CrossRef]
- Goyal NP, Xanthakos S, Schwimmer JB. Metabolic dysfunction-associated steatotic liver disease in children. Gut 2025;74:669–77. [CrossRef]
- Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, Benson JT, Enders FB, Angulo P. The natural history of non-alcoholic fatty liver disease in children: A follow-up study for up to 20 years. Gut 2009;58:1538–44. [CrossRef]
- Pacifico L, Bonci E, Andreoli G, Di Martino M, Gallozzi A, De Luca E, et al. The Impact of Nonalcoholic Fatty Liver Disease on Renal Function in Children with Overweight/Obesity. Int J Mol Sci 2016;17:1218. [CrossRef]
- Zhang L, El-Shabrawi M, Baur LA, Byrne CD, Targher G, Kehar M, et al. An international multidisciplinary consensus on pediatric metabolic dysfunction-associated fatty liver disease. Med 2024;5:797-815.e2. [CrossRef]
- Arab JP, Díaz LA, Rehm J, Im G, Arrese M, Kamath PS, et al. Metabolic Dysfunction and Alcohol-related Liver Disease (MetALD): Position statement by an expert panel on alcohol-related liver disease. J Hepatol 2024. [CrossRef]
- Di Ciaula A, Bonfrate L, Krawczyk M, Frühbeck G, Portincasa P. Synergistic and Detrimental Effects of Alcohol Intake on Progression of Liver Steatosis. Int J Mol Sci 2022;23:2636. [CrossRef]
- Marti-Aguado D, Calleja JL, Vilar-Gomez E, Iruzubieta P, Rodríguez-Duque JC, Del Barrio M, et al. Low-to-moderate alcohol consumption is associated with increased fibrosis in individuals with metabolic dysfunction-associated steatotic liver disease. J Hepatol 2024. [CrossRef]
- Dixon W, Corey K, Luther J, Goodman R, Schaefer EA. Prevalence and clinical correlation of cardiometabolic risk factors in alcohol-related liver disease and MetALD. J Clin Exp Hepatol 2024:102492. [CrossRef]
- Zheng T, Wang X, Kamili K, Luo C, Hu Y, Wang D, et al. The relationship between alcohol consumption and chronic kidney disease in patients with nonalcoholic fatty liver disease. Scand J Gastroenterol 2024;59:480–8. [CrossRef]
- Li D, Xu J, Liu F, Wang X, Yang H, Li X. Alcohol Drinking and the Risk of Chronic Kidney Damage: A Meta-Analysis of 15 Prospective Cohort Studies. Alcohol Clin Exp Res 2019;43:1360–72. [CrossRef]
- Vilar-Gomez E, Calzadilla-Bertot L, Friedman SL, Gra-Oramas B, Gonzalez-Fabian L, Villa-Jimenez O, et al. Improvement in liver histology due to lifestyle modification is independently associated with improved kidney function in patients with non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2017;45:332–44. [CrossRef]
- Zhang Y, Zhang T, Liu Y, Bai S, Jiang J, Zhou H, et al. Adherence to healthy lifestyle was associated with an attenuation of the risk of chronic kidney disease from metabolic dysfunction–associated fatty liver disease: Results from two prospective cohorts. Diabetes and Metabolic Syndrome: Clinical Research and Reviews 2023;17. [CrossRef]
- Zhang X, Rouillard N, Mao X, Lai R, Cheung R, Sasaki K, et al. Enhanced long-term outcomes with laparoscopic bariatric surgery in patients with severe obesity and metabolic dysfunction-associated steatotic liver disease: a retrospective cohort study. Hepatobiliary Surg Nutr 2023;0:0–0. [CrossRef]
- Harrison SA, Bedossa P, Guy CD, Schattenberg JM, Loomba R, Taub R, et al. A Phase 3, Randomized, Controlled Trial of Resmetirom in NASH with Liver Fibrosis. New England Journal of Medicine 2024;390:497–509. [CrossRef]
- Au K, Yang W. Resmetirom as an important cornerstone of multidisciplinary management of metabolic dysfunction-associated steatohepatitis. Hepatobiliary Surg Nutr 2025;14:290–4. [CrossRef]
- Fan J-G, Xu X-Y, Yang R-X, Nan Y-M, Wei L, Jia J-D, et al. Guideline for the Prevention and Treatment of Metabolic Dysfunction-associated Fatty Liver Disease (Version 2024). J Clin Transl Hepatol 2024;12:955–74. [CrossRef]
- Mathur A, Ozkaya E, Rosberger S, Sigel KM, Doucette JT, Bansal MB, et al. Concordance of vibration-controlled transient elastography and magnetic resonance elastography for fibrosis staging in patients with metabolic dysfunction-associated steatotic liver disease. Eur Radiol 2025. [CrossRef]
- Ratziu V, Hompesch M, Petitjean M, Serdjebi C, Iyer JS, Parwani A V., et al. Artificial intelligence-assisted digital pathology for non-alcoholic steatohepatitis: current status and future directions. J Hepatol 2024;80:335–51. [CrossRef]
- Zerehpooshnesfchi S, Lonardo A, Fan J-G, Elwakil R, Tanwandee T, Altarrah MY, et al. Dual etiology vs. MetALD: how MAFLD and MASLD address liver diseases coexistence. Metabolism and Target Organ Damage 2025;5. [CrossRef]
- Samanta A, Sarma M Sen. Metabolic dysfunction-associated steatotic liver disease: A silent pandemic. World J Hepatol 2024;16:511–6. [CrossRef]
Figure 1.
Histological progression of MASLD. A: Isolated hepatic steatosis (Hematoxylin/ eosin (H.E) (400x magnification); B: steatohepatitis, with ballooned hepatocytes in the center (red arrows), and inflammatory infiltrate (green arrow) (H.E, 400x magnification); C: early perisinusoidal fibrosis (blue dye) around hepatocytes (Masson's trichrome, 400x magnification); D: cirrhosis, with fibrous septa (blue dye) and regenerative nodules displaying steatosis (Masson's trichrome, 40x magnification).
Figure 1.
Histological progression of MASLD. A: Isolated hepatic steatosis (Hematoxylin/ eosin (H.E) (400x magnification); B: steatohepatitis, with ballooned hepatocytes in the center (red arrows), and inflammatory infiltrate (green arrow) (H.E, 400x magnification); C: early perisinusoidal fibrosis (blue dye) around hepatocytes (Masson's trichrome, 400x magnification); D: cirrhosis, with fibrous septa (blue dye) and regenerative nodules displaying steatosis (Masson's trichrome, 40x magnification).
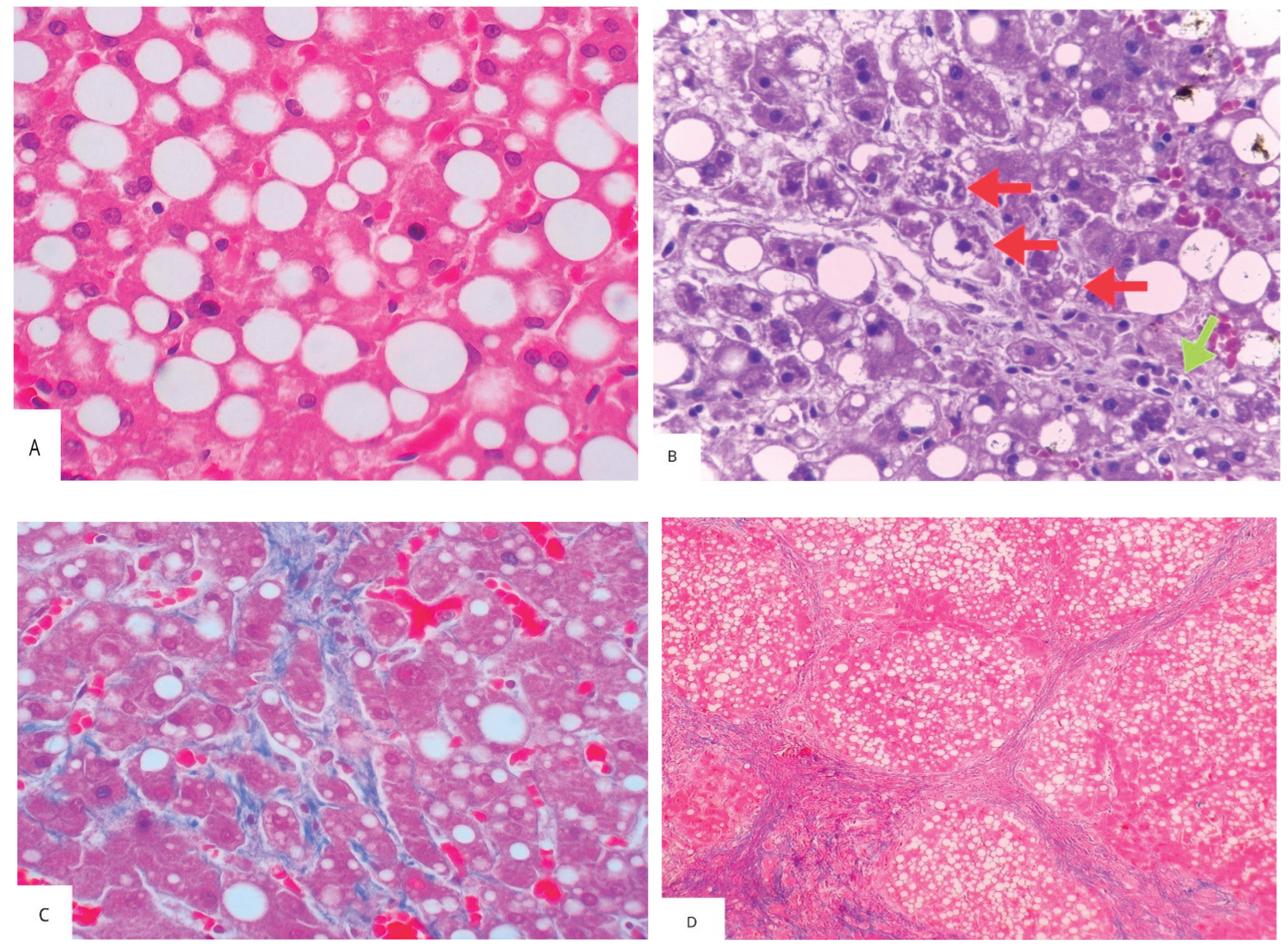
Figure 2.
Histology of CKD. A: yellow arrows: globally sclerotic glomeruli; black arrows: interstitial fibrosis surrounding atrophic tubules; red arrow: arterial intimal thickening (Masson's trichrome, 100x magnification) B: blue arrow: nodular glomerulosclerosis, characteristic of diabetic nephropathy (H.E, 400x magnification).
Figure 2.
Histology of CKD. A: yellow arrows: globally sclerotic glomeruli; black arrows: interstitial fibrosis surrounding atrophic tubules; red arrow: arterial intimal thickening (Masson's trichrome, 100x magnification) B: blue arrow: nodular glomerulosclerosis, characteristic of diabetic nephropathy (H.E, 400x magnification).
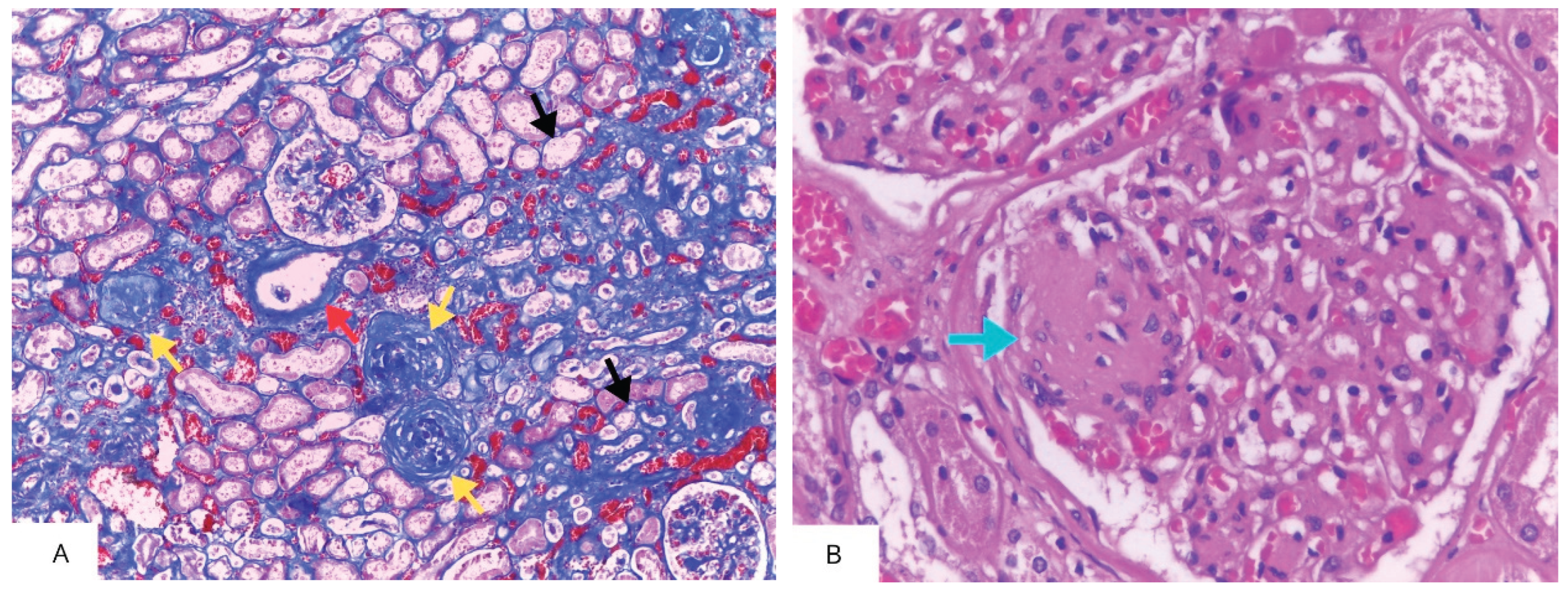
Figure 3.
Shared risk factors for metabolic dysfunction-associated steatotic liver disease (MASLD) and chronic kidney disease (CKD). Double arrows indicate a bidirectional relationship.
Figure 3.
Shared risk factors for metabolic dysfunction-associated steatotic liver disease (MASLD) and chronic kidney disease (CKD). Double arrows indicate a bidirectional relationship.
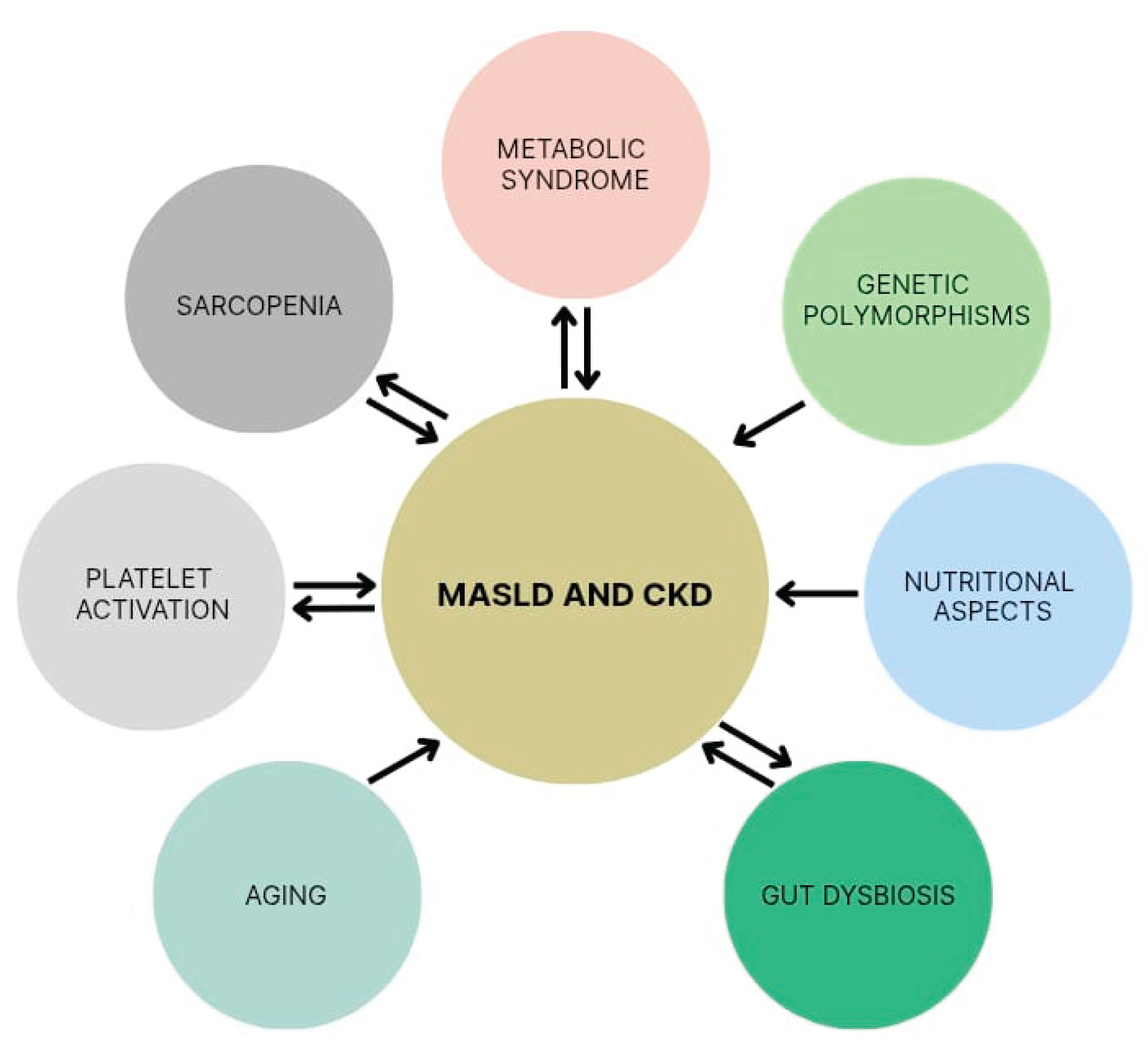
Figure 4.
Hypothetical mechanisms of direct MASLD-induced CKD.
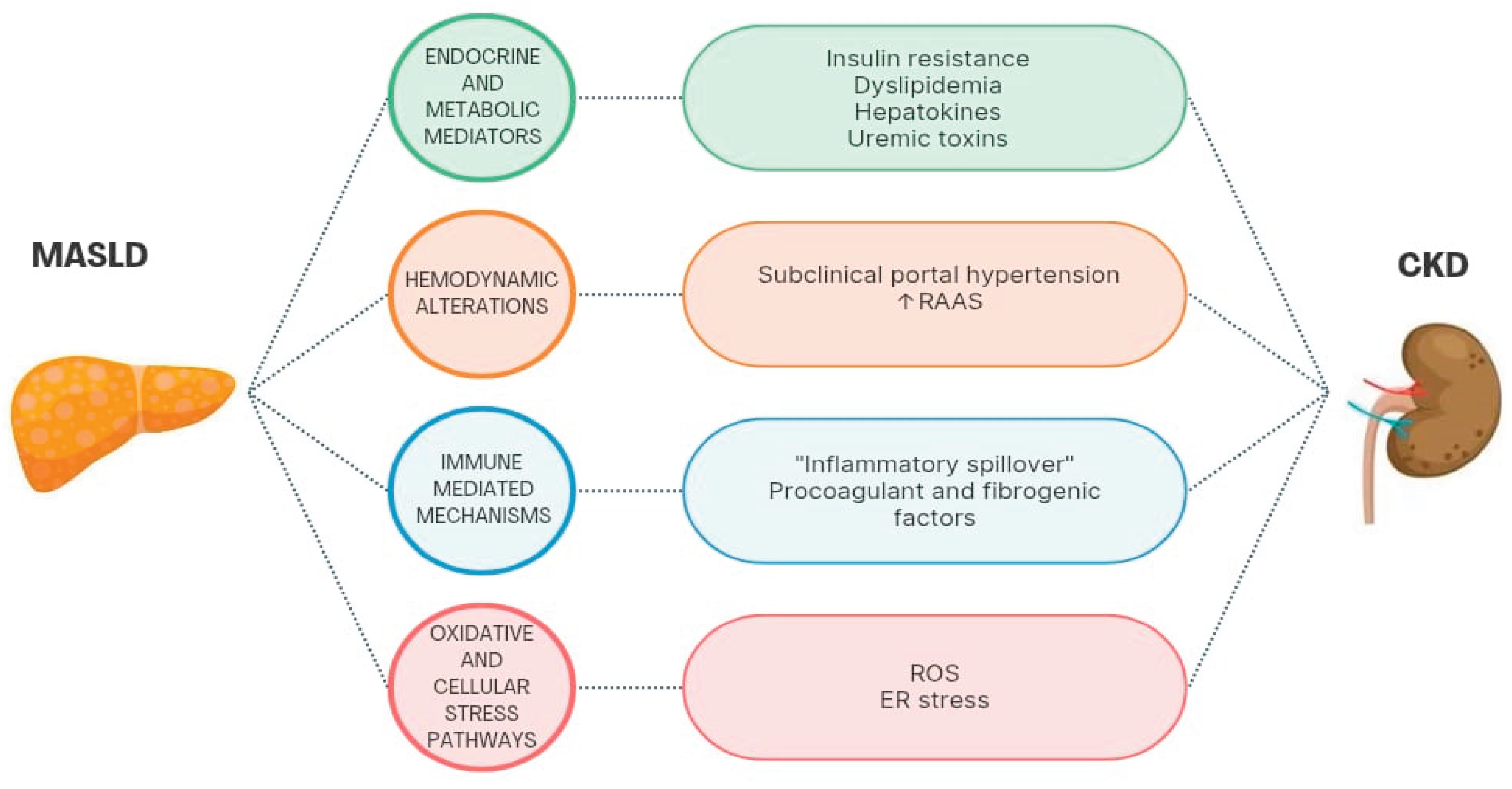

Table 1.
Main meta-analyses and longitudinal studies on the association between MASLD and CKD.
| Authors, year | Study characteristics | Diagnosis of SLD / CKD | Main findings | Comments |
|---|---|---|---|---|
| Liu et al., 2024 [78] | Systematic review and meta-analysis of 8 cohort studies from Asia and the UK, comprising 598,531 patients. Follow-up ranging from 4.6 to 12.9 years. Aim: to compare the incidence of CKD in persons with MAFLD and controls without MAFLD. |
SLD: MAFLD criteria, diagnosed by ultrasound. CKD: eGFR < 60 mL/min/1.73 m2, proteinuria, or urine albumin/creatinine ratio ≥ 30 mg/g. |
MAFLD was associated with a higher incidence of CKD (HR: 1.38, 95% CI: 1.24-1.53) adjusted for sex, body mass index, cardiovascular disease, diabetes, hypertension, and smoking status | 1.Meta-analysis with high heterogeneity (I2 = 95%). 2.Seven of the eight studies were from Asia. 3.No assessment of MAFLD severity at baseline. |
| Agustanti et al., 2023 [14] | Systematic review and meta-analysis of 11 studies (7 cross- sectional and 4 longitudinal) from Asia, Europe, and the USA, comprising 355,886 patients. Follow-up ranging from 4.6 to 6.5 years Aim: to determine the incidence and prevalence of CKD according to the presence and severity of MAFLD at baseline. |
SLD: MAFLD or NAFLD criteria, diagnosed by ultrasound, transient elastography, or FLI. CKD: eGFR < 60 mL/min/1.73 m2 or UACR of 30 mg/g or greater or proteinuria (positive dipstick test result of +1 or greater). |
MAFLD was associated with higher prevalence (OR = 1.50, 95% CI 1.02-2.23) and incidence (HR = 1.35, 95% CI 1.18-1.52) of CKD adjusted for age, sex, comorbidities, study region, and follow-up duration. Significant liver fibrosis, but not steatosis, was associated with greater likelihood of developing CKD. | 1.Meta-analysis with high heterogeneity (I2: 97.7% for cross-sectional and 84.6% for longitudinal studies). 2.Eexposure group included patients with either NAFLD or MAFLD criteria, leading to possible selection bias. 3.Absence of histological analysis of SLD. |
| Mantovani et al., 2022 [16] | Systematic review and meta-analysis of 13 longitudinal studies from Asia, Europe and the USA, comprising 1.222,032 patients. Median follow-up of 9.7 years. Aim: to determine the incidence of CKD according to the presence and severity of MAFLD at baseline. |
SLD: NAFLD criteria, diagnosed by liver enzymes, blood biomarkers, imaging methods, liver histology or ICD-10 codes. CKD: eGFR < 60 mL/min/1.73 m2 with or without overt proteinuria. |
NAFLD was associated with higher incidence of CKD (HR = 1.43, 95% CI 1.33-1.54) adjusted for age, sex, obesity, hypertension, diabetes and other conventional CKD risk factors. |
1. The authors suggest a possible association between the severity of NAFLD (especially liver fibrosis) and incident CKD but emphasize that the studies that assessed hepatic fibrosis did not include a control group without NAFLD, resulting in insufficient data for a meta-analysis. 2. Meta-analysis with medium to high heterogeneity (I2 = 60.7%). |
| Musso et al., 2014 [15] | Systematic review and meta-analysis of 33 studies (20 cross-sectional and 13 longitudinal) from Asia, the USA, Europe, and Saudi Arabia, comprising 63,902 patients. Follow-up ranging from 3 to 27 years Aim: to determine the incidence and prevalence of CKD according to the presence and severity of NAFLD at baseline. |
SLD: NAFLD criteria, diagnosed by liver histology, imaging (ultrasound, computer tomography, magnetic resonance imaging, or spectroscopy), biochemistry (elevations in serum liver enzymes). CKD: eGFR < 60 ml/min/1.73 m2, or proteinuria (UACR, 24-h albumin excretion rate, fresh morning urine dipstick), or other abnormalities due to tubular disorders or structural abnormalities detected by electrolyte or urinary sediment alterations, histology, imaging, or history of kidney transplantation. |
NAFLD was associated with higher prevalence (OR = 2.12, 95% CI 1.69-2.66) and incidence (HR = 1.79, 95% CI 1.65-1.95) of CKD. NASH was associated with higher prevalence (OR = 2.53, 95% CI 1.58-4.05) and incidence (HR = 2.12, 95% CI 1.42-3.17) of CKD than steatosis alone. Advanced liver fibrosis was associated with higher prevalence (OR = 5.20, 95% CI 3.14-8.61) and incidence (HR = 3.29, 95% CI 2.30-4.71) of CKD than non-advanced fibrosis. All findings were adjusted for diabetes status, traditional risk factors for CKD, obesity, and insulin resistance. | 1.Meta-analysis with substantial heterogeneity (I2 = 77%). 2.Only 5 studies with biopsy-proven NAFLD, totaling 690 patients, leading to possible small study bias. |
| Sanyal, 2021 [81] | Prospective multicenter cohort study from the USA, including 1,773 patients with NAFLD (with or without fibrosis). Median follow-up of 4 years. Aim: to determine longitudinal outcomes according to the severity of NAFLD. | SDL: NAFLD criteria, diagnosed by liver biopsy. CKD: decrease in eGFR of >40% |
Patients with stage F4 fibrosis had a decrease of more than 40% in the eGFR compared to those with stages F0 to F2 fibrosis (2.98 vs. 0.97 events per 100 person-years; HR = 1.9; 95% CI 1.1-3.4) adjusted for age, race, sex, length of biopsy specimen, and diabetes status. | 1.Limited generalizability (study conducted at tertiary care centers with predominantly White populations. 2. F3 fibrosis was not associated with a decrease in eGFR of >40% when compared to F0-F2 (HR = 0.9; 95%CI 0.6-1.6) |
| Gao et al., 2024 [85] | Retrospective cohort study from China, including 79,540 patients. Median follow-up of 12.9 years. Aim: to determine the incidence of CKD according to the presence, severity, and remission of MAFLD/MASLD |
SLD: MAFLD and MASLD criteria, diagnosed by ultrasound. CKD: eGFR < 60 mL/min/1.73m2 or positive proteinuria (≥1+). |
MAFLD/MASLD was associated with a higher incidence of CKD (HR, 1.12 [95% CI, 1.09-1.16]); risk increased according to severity of steatosis (p <0.001). Even after remission of MAFLD/MASLD, patients with prior moderate to severe hepatic steatosis still had a higher risk of CKD. Adjustments: age, sex, smoking, drinking, exercise, education, income, eGFR at baseline, uric acid, ALT, metabolic dysfunction, use of antihyperglycemic, antihypertensive, and antilipidemic agents. |
Most patients in the study were male (80%). |
| Mori et al., 2024 [83] | Retrospective cohort study from Japan, including 12,138 patients. Follow-up of 10 years. Aim: to determine the incidence of CKD according to SLD status at baseline (MASLD, MetALD, ALD, and SLD without metabolic dysfunction) compared to the incidence of CKD in non-SLD control subjects | SLD: MASLD, MetALD, and ALD criteria, diagnosed by ultrasound. CKD: eGFR < 60 mL/min/1.73 m2 or proteinuria by dipstick. |
The incidence of CKD was higher in individuals with MASLD (HR = 1.20; CI 1.08-1.33) and ALD (HR = 1.41; CI 1.05-1.88), but not MetALD (HR = 1.11; CI 0.90-1.36) when compared to those without SLD. Individuals with SLD without metabolic dysfunction had a lower incidence (HR = 0.61 [0.39-0.96]) than those without SLD. Adjustments: age, sex, baseline eGFR, smoking, diabetes, systemic hypertension, and dyslipidemia. |
Study conducted in a single urban clinic (possibility of selection bias) |
| Liang et al., 2022 [82] | Cohort study from China, including 6,873 patients. Follow-up of 4.6 years. Aim: to compare the incidence of extra-hepatic diseases in persons with MAFLD and controls without MAFLD. |
SLD: NAFLD and MAFLD criteria, diagnosed by ultrasound. CKD: eGFR < 60 mL/min/1.73 m2 or UACR 30 μg/mg or greater. |
MAFLD was associated with a higher incidence of CKD (RR = 1.64; 95% CI 1.39-1.94). Similar associations for NAFLD were observed. Adjustments: age, sex, education, smoking status, and leisure-time exercise. | NAFLD and MAFLD were also associated with an increased incidence of diabetes and cardiovascular diseases. |
| Mouzaki et al., 2024 [79] | Prospective multicenter cohort study from the USA, including 1,164 children (age 13 ± 3 years). Median follow-up of 2 years. Aims: to determine the prevalence of hyperfiltration or CKD in children with NAFLD/MASLD and determine links with liver disease severity. |
SLD: MASLD/ NAFLD criteria, diagnosed by biopsy. CKD: Hyperfiltration or eGFR < 90 mL/min/1.73 m2 |
Significant liver fibrosis was associated with hyperfiltration (OR: 1.45). Progression of renal impairment was not associated with change in liver disease severity. Adjustments: BMI, insulin resistance, hemoglobin A1c, blood pressure, age, ethnicity, race, gender, and T2DM. |
1. Most participants were Hispanic. 2. Short follow-up. 3.Study did not include proteinuria as a definition of CKD. |
| Zuo et al., 2021 [80] | Prospective cohort study from China, including 4,042 patients aged 40 years or more. Mean follow-up of 4.4 years. Participants were divided into 4 groups at baseline: 57.4% participants with non-NAFLD, 13.2% with incident NAFLD, 21.6% with persistent NAFLD, and 7.8% with NAFLD resolution. Aim: to assess associations between changes in NALFD status/progression of NAFLD fibrosis and the risk of incident CKD. |
SLD: NAFLD criteria, diagnosed by ultrasound and NAFLD fibrosis score. CKD: UACR 30 mg/g or greater, or eGFR 60 mL/min/1.73 m2 or lower. |
Incident NAFLD was associated with incident CKD (OR = 1.44; 95% CI, 1.003-2.06) compared to non-NAFLD. However, the risk of incident CKD was not significantly different between groups with NAFLD resolution and persistent NAFLD. In the persistent NAFLD group, fibrosis progression was associated with a higher incidence of CKD compared to stable fibrosis (OR = 2.82; 95% CI, 1.22-6.56). Adjustments: baseline and evolution of diabetes, hypertension, and obesity. |
1. The study population consisted of more women and older participants from a community-based population. 2. NAFLD and CKD at baseline and follow-up were determined concurrently, precluding the determination of causation. |
| Heo et al., 2024 [84] | Cohort study from Korea, including 214,145 adults with normal kidney function at baseline. Median follow-up: 6.1 years Aim: to compare the incidence of CKD among 5 groups of participants: Without steatosis, NAFLD-only, MASLD-only, both NAFLD and MASLD, and SLD not categorized as NAFLD or MASLD | SLD: NAFLD, and MASLD criteria, diagnosed by ultrasound. CKD: eGFR <60 mL/min/1.73 m2 or albuminuria. |
The group meeting both NAFLD and MASLD criteria had the highest risk of CKD (HR = 1.21 [95% CI, 1.04-1.42]). The MASLD-only group had a similar risk (HR = 1.96 [95% CI, 1.44-2.67]), but NAFLD alone was not independently associated with CKD or albuminuria. Adjustments: age, sex, education, smoking history, exercise, alcohol intake, history of coronary artery disease, use of anti-hypertensive medications, and levels of eGFR at baseline. |
Authors suggest that MASLD criteria are better than NAFLD criteria at identifying individuals at high risk of incident CKD or albuminuria. |
Abbreviations: SLD, steatotic liver disease; FLI, fatty liver index; CKD, chronic kidney disease; CI, confidence interval, eGFR, estimated glomerular filtration rate; MASLD, metabolic dysfunction-associated steatotic liver disease; HR, hazard ratio; MAFLD, metabolic dysfunction-associated fatty liver disease; NAFLD, nonalcoholic fatty liver disease; ICD-10, International Classification of Diseases - tenth revision; UACR, urinary albumin-creatinine ratio; T2DM, type 2 diabetes mellitus; OR, odds ratio; RR, relative risk; ALD, alcoholic liver disease. Tables may have a footer.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



