
Submitted:
29 July 2025
Posted:
30 July 2025
You are already at the latest version
Abstract
Background: The interplay between glomerular hyperfiltration (GHF) and renal dysfunction and hepatic fibrosis in metabolic-associated steatotic (or fatty) liver disease (MASLD or MAFLD) remains insufficiently understood. Therefore, we examined the association in a relatively healthy population. Methods: Between 2002 and 2019, 47,741 adults (18–70 years old) participated in the study and underwent baseline liver ultrasonography and annual renal function assessments. Hepatic steatosis was diagnosed using ultrasonography, and GHF was defined as an estimated residual glomerular filtration rate exceeding the 95th percentile based on age- and sex-specific thresholds. The progression of liver fibrosis was assessed using noninvasive markers. Chronic kidney disease (CKD) and advanced liver fibrosis progression were the primary and secondary endpoints, respectively. Results: Patients with MASLD but without GHF did not exhibit an increased risk of CKD progression. However, GHF was independently associated with a higher risk of CKD progression, particularly in patients with MASLD (adjusted hazard ratio (HR): 3.88 [95% CI 3.66–4.11]). GHF alone led to a slight increase in advanced liver fibrosis risk, whereas its presence in patients with MASLD significantly exacerbated fibrosis progression (adjusted HR, 1.36 [95% CI 1.24–1.48]). In patients with coexisting GHF and MASLD, CKD development was associated with a 24% additional risk of advanced liver fibrosis (adjusted HR, 1.24; 95% CI, 1.19–1.29). Consistent findings were also noted based on the MAFLD definition. Conclusions: GHF is associated with future CKD and liver fibrosis progression, serving as a prognostic marker in patients with MASLD (or MAFLD), emphasizing the need for timely identification and monitoring.
Keywords:
glomerular hyperfiltration
; non-alcoholic fatty liver disease
; chronic kidney disease
; liver fibrosis
; prognostic marker
1. Introduction
The incidence and prevalence of metabolic-associated steatotic liver disease (MASLD), previously known as metabolic-associated fatty liver disease (MAFLD) and historically classified as non-alcoholic fatty liver disease (NAFLD) [1,2], have been increasing globally [3,4]. This trend is clinically significant because MASLD/MAFLD represents an abnormal metabolic phenotype closely associated with metabolic syndrome. Notably, MASLD/MAFLD is associated with an elevated risk of cardiovascular disease (CVD) and progressive renal dysfunction [4,5]. Glomerular hyperfiltration (GHF) has recently emerged as a potential early marker of metabolic abnormalities in non-obese individuals. Moreover, the complex interplay between hepatic and renal functions is well documented, highlighting the need for further investigation to clarify the underlying mechanisms governing these interactions [6,7].
Several studies have assessed the relationship between MASLD and chronic kidney disease (CKD). For instance, a recent review suggested that MASLD is an independent risk factor for CKD, particularly in middle-aged individuals 45–54 years [8]. While another study reported that the pathophysiology of MASLD and metabolic-associated steatohepatitis (MASH) extends beyond the liver and involves multiple organs, including the skeletal muscle, adipose tissue, pancreas, gut microbiota, immune system, and central nervous system [9]. Despite this growing body of evidence, no study has directly examined the association between GHF and renal function decline in patients with MASLD or MAFLD. The observed differences in estimated glomerular filtration rate (eGFR) patterns between the MASLD/MAFLD and non-MASLD/MAFLD populations highlight the need for longitudinal studies to assess how renal function trajectories differ across metabolic disease stages. Furthermore, re-evaluation of whether GHF constitutes a significant risk factor for liver fibrosis based on the newly defined MASLD/MAFLD criteria rather than the previous NAFLD classification remains crucial [7].
Therefore, in this study, we aimed to establish an operational threshold for GHF and examine its pleiotropic effects on CKD progression and hepatic fibrosis in individuals with MASLD or MAFLD.
2. Materials and Methods
2.1. Study Population and Design
We used data from the Kangbuk Samsung Health Study, which included adults who underwent regular comprehensive health checkups at the Kangbuk Samsung Hospital Total Healthcare Centers in Seoul and Suwon, South Korea. We initially included 52,606 adults aged 18–70 years who underwent liver ultrasound at baseline and annual renal function assessments between January 3, 2002, and December 31, 2019. Individuals with an eGFR < 60, kidney-related diseases, diabetes, cancer, liver cirrhosis, viral hepatitis, and missing data were excluded from the analysis. Additionally, individuals with daily alcohol consumption of 30 g or more for men and 20 g or more for women were excluded. Consequently, 47,741 participants were included in the final analysis (Supplementary Figure S1). Diagnoses of MASLD/MAFLD and GHF were established at the baseline. During the follow-up period, the primary endpoint was CKD progression, and the secondary endpoint was the progression of liver fibrosis. This study was approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBSMC 202503031). The study data were collected and stored in a de-identified format to ensure participant confidentiality. No personally identifiable information is included. Because this was a retrospective study that analyzed de-identified data, the requirement for informed consent was waived. None of the participants received any financial compensation.
2.2. Anthropometric and Laboratory Measurements
Lifestyle habits and medical histories of the study participants were collected using self-administered questionnaires. Participants independently completed the forms and provided information on their health status and treatment experience. Alcohol consumption was calculated as the average daily intake based on total weekly alcohol consumption. Smoking status was categorized as either 'yes' or 'no,” whereas regular physical activity was defined as engaging in moderate-intensity or higher exercise at least three times per week.
Trained personnel performed all the anthropometric measurements. Blood pressure was measured in both arms using a standard sphygmomanometer after the participants rested adequately in a seated position. Body mass index (BMI) was calculated using the body weight measured while wearing a light gown, and height was measured using an automated device. Waist circumference (WC) was measured using a tape measure at the midpoint between the lowest rib and the highest point of the iliac crest, while the participants stood with their feet 25–30 cm apart, evenly distributed weight, and exhaled.
All biochemical analyses were conducted in a standardized laboratory setting using certified equipment. Blood samples were collected after the participants fasted for at least 12 h. Fasting blood glucose levels were measured using the hexokinase method (Modular D2400, Hitachi, Tokyo, Japan). Glycated hemoglobin (HbA1c) were assessed using an immunoturbidimetric assay (Cobra Integra 800 automated analyzer; Roche Diagnostics, Basel, Switzerland). Triglyceride (TG) levels were determined using an enzymatic colorimetric method and high-density lipoprotein (HDL) cholesterol levels were measured using a selective inhibition method. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were analyzed using the Bayer reagent packages on an automated chemistry analyzer (Advia 1650 autoanalyzer, Bayer Diagnostics, Leverkusen, Germany).
2.3. Diagnosis of MASLD/MAFLD and Advanced Liver Fibrosis
Hepatic steatosis (fatty liver) was confirmed using ultrasound-based examinations [10]. Trained examiners performed ultrasound examinations, with final confirmation by an independent radiologist. The reliability of the diagnosis of fatty liver was maintained at a high level with an inter-examiner agreement of 0.74 and an intra-observer agreement of 0.94, based on the kappa value [11]. The diagnoses of MASLD [12] or MAFLD [13] were based on the newly proposed definitions. The NAFLD Fibrosis Score (NFS) and Fibrosis-4 (FIB-4) index were used to identify advanced liver fibrosis because they are widely applicable in clinical practice and have been validated for reliability in multiple studies and guidelines [14,15]. Progression of liver fibrosis was defined as an absolute increase in one or both indices at follow-up compared to baseline.
2.4. Definition of GHF and CKD Progression
We defined the GHF cut-off as an eGFR residual > 95th percentile within an age- and sex-specific group based on the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation to maintain consistency with our previous studies related to GHF [6,16]. CKD progression was defined based on the modified Kidney Disease: Improving Global Outcomes (KDIGO) criteria and previous studies on the significance criteria for renal function deterioration, incorporating additional thresholds to account for hyperfiltration-related changes [17,18,19]:
- (1)
-
For individuals without hyperfiltration:
- eGFR persistently ≤ 60 mL/min/1.73m² for ≥ 12 months, or
-
At follow-up, eGFR ≤ 89 mL/min/1.73m² with at least one of the following:

- A sustained annual decline in eGFR ≥ 5 mL/min/1.73m² was observed in subsequent follow-ups.
- A reduction of ≥ 30% in eGFR was observed compared with the previous follow-up.
- (2)
-
For individuals with hyperfiltration:
- eGFR persistently ≤ 60 mL/min/1.73m² for ≥ 12 months, or
-
At follow-up, eGFR ≤ 89 mL/min/1.73m² with at least one of the following:
- A sustained annual decline in eGFR of ≥ 5 mL/min/1.73m² was observed in subsequent follow-ups.
- A reduction of ≥ 30% in eGFR was observed compared with the previous follow-up.
- (3)
-
Urinary albumin-creatinine ratio (UACR):
- Newly detected UACR ≥ 30 mg/g at follow-up in previously negative patients
- A ≥ 30% increase from baseline.
However, in this study, a substantial proportion of the UACR data required for statistical analysis was missing, preventing the application of diagnostic criterion '3' for CKD progression
2.5. Statistical Analysis
All statistical analyses were performed separately for the MASLD and MAFLD groups. Additional classifications were made on the basis of the presence or absence of GHF. A Cox proportional hazards model was employed to determine hazard ratios (HRs) with 95% confidence intervals (CI) for CKD progression and worsening liver fibrosis. Model 1 was an unadjusted analysis that did not adjust for the confounding variables. Model 2 was adjusted for age and sex, whereas Model 3 included further adjustments for baseline eGFR, BMI, SBP, regular exercise, and current smoking status. Kaplan–Meier estimates were used to assess event probabilities over time, facilitating the calculation of interval and cumulative survival rates at each follow-up time point. Restricted cubic spline analysis was used to estimate the baseline log cumulative hazard, and locally weighted smoothing (LOWESS) of the generalized additive model was used to derive pointwise estimates and CI curves. Continuous variables are presented as mean ± standard deviation (SD) and were compared using an independent t-test when appropriate. Data are expressed as median (interquartile range, IQR) and were compared using the Mann–Whitney U test for skewed distributions. One-way analysis of variance (ANOVA) was performed for comparisons between more than two independent continuous variables, whereas the Kruskal–Wallis test was used for non-normally distributed variables. The study participants were further stratified into subgroups based on age, sex, BMI, and waist circumference (WC). Model 3 was used for additional subgroup analyses. The Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were applied to evaluate the model performance and select the optimal model based on the trade-off between goodness-of-fit and model complexity. In general, lower AIC or BIC values indicate a better model fit. Statistical significance was set at two-sided p < 0.05. All statistical analyses were performed using STATA version 16.1 (StataCorp, College Station, TX, USA).
3. Results
3.1. Characteristics of Study Participants
Of the 47,741 study participants (65.0% male), 11,666 and 11,170 were diagnosed with MASLD and MAFLD, respectively. Notably, most patients diagnosed with MASLD and MAFLD were male (90.0% and 90.4%, respectively). The median follow-up period was 4,893 days (IQR, 3,372–5,655 days; total person-years [PY], 546,255.15) for CKD progression and 767 days (IQR, 637–1,477 days; total PY, 156,571.44) for advanced liver fibrosis. While no significant differences were observed in age (mean 35.33 ± 5.20) among the groups, patients diagnosed with MASLD or MAFLD exhibited significantly higher BMI and WC compared to those without these conditions (BMI values: 22.46 vs. 26.17 and 22.45 vs. 26.36, respectively; WC (cm) values: 76.51 vs. 87.69 and 76.56 vs. 88.10, respectively). Additionally, most metabolic parameters and lifestyle factors were unfavorable in the MASLD and MAFLD groups. Notably, contrary to our initial expectations, patients diagnosed with MASLD or MAFLD had a relatively lower eGFR (mL/min/1.73m²) compared to those without the disease (86.17 vs. 83.17 and 86.16 vs. 83.16, respectively). At baseline, both the NFS and FIB-4 indices were categorized as low-risk across all groups, with no significant differences in scores. These characteristic trends were similar between the MASLD and MAFLD groups (Table 1).
3.2. Primary Outcome
The risk of CKD progression was analysed according to the presence of MASLD, MAFLD, and baseline GHF (Table 2 and Supplementary Table S1-1 and -2). The presence of MASLD or MAFLD, without considering GHF, appeared to increase the risk of CKD progression in unadjusted analyses (HR: 1.30, 95% CI 1.26–1.35, for MASLD; HR: 1.31, 95% CI 1.26–1.36, for MAFLD); however, this statistical significance disappeared when adjusted for confounders, particularly GHF (Supplementary Table S1-1). These results remained consistent in detailed analyses based on the presence or absence of GHF (Table 2). In contrast, the presence of hyperfiltration significantly increased the risk of CKD progression regardless of MASLD/MAFLD status (HR: 3.55, 95% CI 3.37–3.73) even after adjustment (Supplementary Table S1-2). In the detailed analyses (Table 2), the risk of CKD progression in the presence of hyperfiltration was similar between patients with MASLD (HR, 3.62; 95% CI 3.26–4.03) and those without MASLD (HR, 3.69; 95% CI 3.48–3.91) in the unadjusted model. However, in the adjusted model, the HR significantly decreased in those without MASLD (HR, 2.56; 95% CI 2.30–2.86), but increased slightly in the MASLD group (HR: 3.88, 95% CI 3.66–4.11), showing an opposite trend. A similar pattern was observed in the MAFLD group (adjusted HR 2.55 (95% CI 2.28–2.85) vs. 3.87 (95% CI 3.65–4.10) (Table 2).
In the Kaplan–Meier analysis, patients with both GHF and MASLD had the highest cumulative incidence of CKD progression during the first four years of follow-up. However, from that point onward, the cumulative incidence rate converged to the same level as that of the group without MASLD. However, patients without GHF consistently exhibited lower cumulative incidence throughout the follow-up period compared to those with GHF, and even within the non-GHF group, individuals with MASLD showed a persistently higher cumulative incidence than those without MASLD (Figure 1). This finding is similarly observed when applying the MAFLD criteria (Supplementary Figure S2).
3.3. Secondary Outcome
The risk of advanced liver fibrosis was also analyzed based on the presence of baseline GHF in patients with MASLD or MAFLD (Table 3 and Supplementary Table S2-1 & -2). The presence of MASLD/MAFLD, without considering GHF, appeared to moderately increase the risk of advanced liver fibrosis in the unadjusted analyses (HR: 1.31, 95% CI 1.28–1.33, for MASLD; HR: 1.31, 95% CI 1.28–1.34, for MAFLD). The HR slightly decreased but remained statistically significant (1.20, 95% CI 1.17–1.23, for MASLD and MAFLD, respectively) when adjusted for confounders, particularly GHF (Supplementary Table S2-2). Regardless of the presence of MASLD/MAFLD, the presence of GHF alone showed a slightly increasing trend in the risk of advanced liver fibrosis with statistical significance (HR: 1.09, 95% CI 1.04–1.14) even after adjustment (Supplementary Table S2-2). These results are consistent with those of the detailed analyses (Table 3). Notably, hyperfiltration significantly increased the risk of fibrosis progression in patients with MASLD or MAFLD. In the unadjusted model, the HR for fibrosis progression was 1.45 (95% CI 1.33–1.58) in the MASLD group. After adjustment, the HR slightly decreased but remained significant (HR: 1.36, 95% CI 1.24–1.48). These results and trends were consistent in the MAFLD group, with an adjusted HR of 1.37 (95% CI 1.25–1.50) (Table 3).
The cumulative incidence by the Kaplan–Meier analysis showed a sharp increase in risk within the first two years of follow-up, particularly in patients with GHF with concomitant MASLD. During the early period, even in the absence of MASLD, patients with GHF exhibited a slightly higher cumulative incidence compared to those with MASLD alone but without GHF. However, this trend reversed after approximately 2 years. From around 4 years of follow-up, the cumulative incidence appeared to converge within MASLD and non-MASLD groups, regardless of GHF status. Nevertheless, within each group stratified by MASLD status, the presence of GHF was consistently associated with a higher cumulative incidence throughout the observation period (Figure 2). This finding is also observed when applying the MAFLD criteria (Supplementary Figure S3).
3.4. Other Outcomes and Subgroup Analyses.
Additional analyses of the association between CKD progression and the relative risk of advanced liver fibrosis in patients with MASLD or MAFLD were performed (Supplementary Table S3). The results indicated that even in the GHF group, CKD progression alone, in the absence of MASLD, did not increase the relative risk of advanced liver fibrosis (adjusted HR 0.98, 95% CI 0.95–1.00). The relative risk of advanced liver fibrosis increased only when CKD progression was observed in patients with MASLD (adjusted HR 1.24, 95% CI 1.19–1.29). Similar trends were also observed in the MAF-LD group. No significant difference was observed in the risk of advanced liver fibrosis between the MASLD and MAFLD groups (Supplementary Table S4).
In this study, we conducted a subgroup analysis by applying criteria based on age (mean age, 35.3 years), sex, obesity (BMI, 25.0), and WC (90.0 cm for men and 80.0 cm for women). The relative risk of CKD progression was significantly higher in all subgroups of patients with both MASLD and GHF than in those without (Figure 3). Except for the age criterion, the p-interaction value was ≥ 0.05 in all subgroups, and the relatively younger patient group (below the mean age) exhibited a higher relative risk (Supplementary Table S5-1). Similarly, in the analysis of advanced liver fibrosis, the relative risk was consistently higher in all subgroups of patients with both MASLD and GHF than in those without. However, differences in statistical significance were observed, with a lack of statistical significance in younger patients (< 35.3 years), females, and patients with lower obesity levels (BMI < 25.0) (Supplementary Table S6-1). These findings were also observed in the MAFLD group, which showed a similar pattern (Supplementary Tables S5-2 and S6-2).
In the assessment of CKD progression based on the baseline eGFR, using the 50th–55th percentiles as the reference, we observed an exponentially increasing trend in CKD progression at eGFR levels above the 90th percentile (Supplementary Figure S4A). The risk of advanced liver fibrosis increased dramatically when eGFR levels were ≥ 90 percentile, especially ≥ 95 percentile, compared with the reference 50th–55th percentile (Supplementary Figure S4B). Regardless of sex, the GHF cutoff values showed a decreasing trend with increasing age, which is consistent with our previous study [6]. However, the magnitude of the change and linearity were significantly lower in men (Supplementary Figure S5).
4. Discussion
4.1. Principal Findings
Our study identified GHF as an independent risk factor for CKD progression in a relatively healthy population without diabetes or pre-existing renal disease; however, neither MASLD nor MAFLD alone significantly increased CKD progression in the absence of hyperfiltration. In addition, we confirmed that the risk of advanced liver fibrosis further increased when GHF was present in patients with MASLD/MAFLD. Moreover, CKD progression was associated with a significantly increased risk of liver fibrosis, particularly in patients with MASLD/MAFLD. These results confirmed the lack of significant differences between the MASLD and MAFLD groups. Thus, our findings underscore the complex interplay between metabolic liver disease and renal function, and reinforce the notion of bidirectional organ crosstalk between the kidney and liver in metabolic disorders [20,21]. This further emphasizes the need for closer monitoring of renal function in patients with MASLD/MAFLD, particularly those with early signs of renal impairment, to prevent further hepatic complications. Given the observed time-dependent risk trends, early detection and intervention for GHF in patients with MASLD/MAFLD may offer a strategy for mitigating both CKD progression and advanced liver fibrosis.
4.2. Comparison with Previous Work
Our findings are consistent with those of previous studies that have highlighted GHF as a surrogate marker of CKD risk in metabolic disorders [22,23]. Additionally, Zhang et al. (2024) [24] demonstrated that liver fibrosis in patients with MASLD was significantly associated with an increased risk of insulin resistance, type 2 diabetes, and CKD progression. Gao et al. (2024) [25] also demonstrated that the risk of CKD in patients with MASLD/MAFLD increases with the severity of hepatic steatosis. Even after remission, patients with prior moderate to severe hepatic steatosis have a higher risk of developing CKD. CKD was defined as an advanced disease state with an eGFR of < 60. mL/min/1.73 m2 in these studies.
Unlike previous studies, we not only investigated the presence of GHF, but also aimed to comprehensively analyze how GHF influences the progression of CKD and liver fibrosis in patients with MASLD/MAFLD, as well as in those without such metabolic abnormalities, using long-term real-world clinical data. Additionally, CKD progression included all stages except stage 1, as it can also occur within the early stages, including Stage 2 [17]. Furthermore, we conducted a comparative analysis to determine whether CKD progression in patients with GHF is merely a consequence of GHF itself, or a contributing factor in a vicious cycle that exacerbates fibrosis. The results of the comparative analysis of the relative risk of advanced liver fibrosis within the GHF group confirmed that the risk increased further when CKD progression occurred in the presence of preexisting MASLD or MAFLD rather than with CKD progression alone. This finding provides a distinct clinical value that differentiates our study from previous studies.
Notably, an unexpected finding of this study was that patients diagnosed with MASLD/MAFLD at baseline exhibited lower eGFR than those without MASLD/MAFLD. This contradicts our initial assumption that patients with MASLD/MAFLD, given their metabolic syndrome-like condition, would exhibit a higher eGFR owing to a hyperfiltration state. We previously reported that patients with GHF, but without NAFLD, had a higher risk of developing NAFLD in the future [6]. This suggests that individuals who do not currently have NAFLD but remain in the GHF state are at increased risk of developing NAFLD later. However, not all patients with established NAFLD exhibit GHF. A possible explanation for this discrepancy is the dynamic nature of GHF across the different stages of metabolic disease. In our study, patients with MASLD/MAFLD were slightly more obese than those without, and metabolically healthy obesity was associated with a risk of hyperfiltration and a mild decrease in eGFR [26]. Li et al. (2011) [23] demonstrated that early metabolic syndrome is often accompanied by an increased GFR driven by renal adiposity and microvascular proliferation; however, this phenomenon may not persist as metabolic dysfunction advances. Similarly, Kishi (2025) [27] redefined GHF as a transient phenomenon that may initially reflect adaptive renal changes but ultimately predisposes individuals to glomerular injury and progressive dysfunction. In addition to GHF, increased glomerular capillary pressure, glomerular enlargement, and tubuloglomerular feedback dysfunction contribute to progression of hyperfiltration-induced renal damage. Additionally, activation of the renin-angiotensin system (RAS) and endothelial dysfunction further exacerbate glomerular stress. Moreover, enhanced sodium-glucose cotransporter 2 (SGLT2) activity leads to increased sodium reabsorption in the proximal tubule, reducing distal tubule sodium delivery, which, in turn, promotes glomerular overdistension and perpetuates the hyperfiltration state [28]. Persistent GHF induces glomerular hypertension and mechanical stress, leading to glomerulosclerosis and tubular damage.
Another notable finding of our study is that unlike previous research, MASLD or MAFLD alone, without GHF, did not increase the risk of CKD progression; rather, it showed a tendency to decrease in a healthy population. Although the unadjusted raw data analysis initially suggested that MASLD/MAFLD itself increased the risk of CKD progression, this significance disappeared after adjusting for confounding factors, and the risk was even lower. The participants in our study were relatively healthy and young, and although the MASLD/MAFLD group was slightly more obese than those without this condition, they were not severely obese (BMI, approximately 26). Although obesity is a well-established risk factor for CKD development and progression, some studies have suggested that once CKD is established, a higher BMI is paradoxically associated with improved survival rates. This implies that excess body weight may have protective effects [29]. Of course, this requires considerable caution in interpretation. Thus, our findings align with the previous suggestion that, to some extent, in the absence of hyperfiltration, individuals with mild obesity may experience a slower CKD progression. This indicates that the presence of fatty liver alone, without GHF, is insufficient to guarantee CKD progression.
However, persistent GHF was associated with a greater risk of CKD progression in patients with established MASLD/MAFLD than in those without. Consistent with the previously discussed theory, this finding suggests that an early hyperfiltration state may be an adaptive process that temporarily masks CKD progression. Thus, regardless of the underlying cause, GHF is a definite risk factor for long-term progression of CKD. This phenomenon is ultimately validated by long-term follow-up exceeding 6 years of cumulative incidence of CKD progression, during which the cumulative incidence rates converge irrespective of the presence of MASLD/MAFLD, and are solely dependent on the presence of GHF.
The pattern of increased risk of CKD progression with higher baseline eGFR in participants with normal renal function, which becomes more pronounced in states of hyperfiltration, aligns with the findings of previous studies [30]. Additionally, consistent with previous studies [6], our study reaffirmed that the risk of advanced liver fibrosis increases dramatically when eGFR levels are ≥ 90 percentile, especially ≥ 95 percentile, compared to the reference 50th–55th percentile. However, a difference from the previous study was that the risk of fibrosis also appeared to increase slightly below the reference range. These discrepancies should be interpreted in the context of the fact that, in addition to the differences in reference values, this study included patients with pre-existing MASLD/MAFLD. Moreover, the lower magnitude of change and lack of linearity in the GHF threshold for men compared to our previous study likely reflects population heterogeneity, as most MASLD/MAFLD patients in this study were male at baseline.
4.3. Limitations and Conclusions
Although our study provides robust longitudinal data on the association between GHF, CKD progression, and hepatic fibrosis in patients with MASLD/MAFLD, some limitations require consideration. First, the retrospective study design may have introduced a selection bias, which limits causal inference. Second, we relied on eGFR rather than direct measurements of renal function such as inulin or iohexol clearance. Although eGFR is widely used in epidemiological studies, it may overestimate or underestimate the renal function, particularly in patients with GHF. Third, the diagnosis of advanced liver fibrosis was based on non-invasive indices (FIB-4 and NFS) rather than histological confirmation. Although these indices have been validated in clinical practice, they may not fully capture fibrosis severity. Fourth, our study population comprised relatively healthy Korean adults, which may limit the generalizability of our findings to other ethnic groups and individuals with advanced metabolic disease. Finally, although we accounted for multiple confounders, residual confounding factors could not be excluded. For example, dietary factors, medication use, and genetic predispositions have not been fully accounted for. One reassuring point is that medications that can affect kidney function and fatty liver, particularly RAS blockers, SGLT2 inhibitors, and GLP-1 receptor agonists, were not widely used in Korea during the study period. Additionally, patients requiring these medications were rarely included in the study, allowing us to exclude their influence.
In conclusion, our results highlight time-dependent effects of GHF on CKD progression and hepatic fibrosis. Our findings provide compelling evidence that GHF plays a crucial role in CKD progression and advanced liver fibrosis in patients with MASLD/MAFLD. Consequently, these results underscore the importance of the early detection and monitoring of GHF, particularly in individuals with metabolic liver disease. However, the underlying mechanism remains unclear. Therefore, further research is required to explore how early stage GHF shifts from an adaptive to a pathological state, and whether interventions targeting hyperfiltration can mitigate long-term renal and hepatic complications. Given the complex interplay between renal and hepatic dysfunction, a multidisciplinary approach is essential to optimize long-term outcomes in patients with metabolic disorders.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1-1: Risk of CKD progression by the presence of baseline GHF; Table S1-2: Risk of CKD progression in patients with MASLD or MAFLD.; Table S2-1: Risk of advanced liver fibrosis by the presence of baseline GHF; Table S2-2: Risk of advanced liver fibrosis in patients with MASLD or MAFLD; Table S3: Risk of advanced liver fibrosis in patients with GHF and MASLD/MAFLD associated with CKD progression during follow-up; Table S4: Comparison of the relative risk of advanced liver fibrosis according to MASLD and MAFLD in patients with GHF and CKD progression; Table S5-1: Subgroup analysis for the risk of CKD progression in patients with MASLD by baseline GHF; Table S5-2: Subgroup analysis for the risk of CKD progression in patients with MAFLD by baseline GHF; Table S6-1: Subgroup analysis for the risk of advanced liver fibrosis in patients with MASLD by baseline GHF; Table S6-2: Subgroup analysis for the risk of advanced liver fibrosis in patients with MAFLD by baseline GHF; Figure S1: Diagram for study subjects; Figure S2: Commutative incidence of chronic kidney disease progression according to baseline GHF and MAFLD; Figure S3: Commutative incidence of advanced liver fibrosis according to baseline GHF and MAFLD; Figure S4: Hazar ratio* of CKD progression (A) and advanced liver fibrosis (B) according to baseline eGFR in patients with MASLD; Figure S5: Distribution of eGFR corresponding to the definition of glomerular hyperfiltration according to age (years) and sex;.
Author Contributions
Conceptualization: D.-J.K. and E.-J.R.; Formal analysis: Y.-T.K.; Methodology: D.-J.K.; Data curation: D.-J.K., S.-J.M., H.K., S.M.L., S.E.P., C.-Y.P., W.-Y.L., S.R.C., and E.-J.R.; Writing - original draft: D.-J.K.; Writing - review & editing: D.-J.K. and E.-J.R.; Resources: E.-J.R.; Supervision and Validation: E.-J.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding, and none of the authors received any financial support related to this work.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBSMC 202503031).
Informed Consent Statement
The study used retrospectively collected, de-identified data to ensure participant confidentiality. As no personally identifiable information was included, the requirement for informed consent was waived.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We sincerely thank the Department of Academic Research at Samsung Kangbuk Hospital for their technical support in manuscript formatting and for their meticulous work on figures and tables. We are especially grateful to Soo-Jung Woo for her commitment and professional assistance during the preparation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MASLD | Metabolic-Associated Steatotic Liver Disease |
| MAFLD | Metabolic-Associated Fatty Liver Disease |
| NAFLD | Non-Alcoholic Fatty Liver Disease |
| CVD | Cardiovascular Disease |
| GHF | Glomerular Hyperfiltration |
| CKD | Chronic Kidney Disease |
| eGFR | Estimated Glomerular Filtration Rate |
| BMI | Body Mass Index |
| WC | Waist Circumference |
| HbA1c | Glycated Hemoglobin |
| TG | Triglyceride |
| HDL | High-Density Lipoprotein |
| AST | Aspartate Aminotransferase |
| ALT | Alanine Aminotransferase |
| NFS | NAFLD Fibrosis Score |
| FIB-4 | Fibrosis-4 Index |
| CKD-EPI | Chronic Kidney Disease Epidemiology Collaboration |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| UACR | Urinary Albumin-Creatinine Ratio |
| HR | Hazard Ratio |
| CI | Confidence Interval |
| LOWESS | Locally Weighted Scatterplot Smoothing |
| SD | Standard Deviation |
| IQR | Interquartile Range |
| ANOVA | Analysis of Variance |
| AIC | Akaike Information Criterion |
| BIC | Bayesian Information Criterion |
| PY | Person-Years |
| MASH | Metabolic-Associated Steatohepatitis |
| RAS | Renin-Angiotensin System |
| SGLT2 | Sodium-Glucose Cotransporter 2 |
References
- Yang, A.; Zhu, X.; Zhang, L.; Ding, Y. Transitioning from NAFLD to MAFLD and MASLD: Consistent prevalence and risk factors in a Chinese cohort. J. Hepatol. 2024, 80, e154–e155. [Google Scholar] [CrossRef]
- Bae, J.C. No More NAFLD: The Term Is Now MASLD. Endocrinol. Metab. (Seoul) 2024, 39, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.H.; Jeong, S.J.; Wang, J.H.; Choi, Y.J.; Oh, H.M.; Cho, J.H.; Ahn, Y.C.; Son, C.G. The Clinical Diagnosis-Based Nationwide Epidemiology of Metabolic Dysfunction-Associated Liver Disease in Korea. J. Clin. Med. 2023, 12, 7634. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.C.Z.; Anand, V.V.; Razavi, A.C.; Alebna, P.L.; Muthiah, M.D.; Siddiqui, M.S.; Chew, N.W.S.; Mehta, A. The Global Epidemic of Metabolic Fatty Liver Disease. Curr. Cardiol. Rep. 2024, 26, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Jung, I.; Koo, D.J.; Lee, W.Y. Insulin Resistance, Non-Alcoholic Fatty Liver Disease and Type 2 Diabetes Mellitus: Clinical and Experimental Perspective. Diabetes Metab. J. 2024, 48, 327–339. [Google Scholar] [CrossRef]
- Koo, D.J.; Lee, M.Y.; Jung, I.; Moon, S.J.; Kwon, H.; Rhee, E.J.; Park, C.Y.; Lee, W.Y.; Oh, K.W.; Park, S.E. Increased Risk of NAFLD in Adults with Glomerular Hyperfiltration: An 8-Year Cohort Study Based on 147,162 Koreans. J. Pers. Med. 2022, 12, 1142. [Google Scholar] [CrossRef]
- Dalbeni, A.; Garbin, M.; Zoncape, M.; Romeo, S.; Cattazzo, F.; Mantovani, A.; Cespiati, A.; Fracanzani, A.L.; Tsochatzis, E.; Sacerdoti, D.; et al. Glomerular Hyperfiltration: A Marker of Fibrosis Severity in Metabolic Associated Steatotic Liver Disease in an Adult Population. Int. J. Mol. Sci. 2023, 24, 15837. [Google Scholar] [CrossRef]
- Sandireddy, R.; Sakthivel, S.; Gupta, P.; Behari, J.; Tripathi, M.; Singh, B.K. Systemic impacts of metabolic dysfunction-associated steatotic liver disease (MASLD) and metabolic dysfunction-associated steatohepatitis (MASH) on heart, muscle, and kidney related diseases. Front. Cell Dev. Biol. 2024, 12, 1433857. [Google Scholar] [CrossRef]
- Kimura, T.; Yamazaki, T.; Estrela, G.R. Editorial: Multi-organ linkage pathophysiology and therapy for NAFLD and NASH. Front. Endocrinol. (Lausanne) 2024, 15, 1418066. [Google Scholar] [CrossRef]
- Hamer, O.W.; Aguirre, D.A.; Casola, G.; Lavine, J.E.; Woenckhaus, M.; Sirlin, C.B. Fatty liver: imaging patterns and pitfalls. Radiographics 2006, 26, 1637–1653. [Google Scholar] [CrossRef]
- Ryu, S.; Chang, Y.; Choi, Y.; Kwon, M.J.; Kim, C.W.; Yun, K.E.; Jung, H.S.; Kim, B.K.; Kim, Y.J.; Ahn, J.; et al. Age at menarche and non-alcoholic fatty liver disease. J. Hepatol. 2015, 62, 1164–1170. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J. Hepatol. 2023, 79, 1542–1556. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus, P. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K.; Isaacs, S.; Barb, D.; Basu, R.; Caprio, S.; Garvey, W.T.; Kashyap, S.; Mechanick, J.I.; Mouzaki, M.; Nadolsky, K.; et al. American Association of Clinical Endocrinology Clinical Practice Guideline for the Diagnosis and Management of Nonalcoholic Fatty Liver Disease in Primary Care and Endocrinology Clinical Settings: Co-Sponsored by the American Association for the Study of Liver Diseases (AASLD). Endocr. Pract. 2022, 28, 528–562. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.M.; Kang, M.K.; Moon, J.S.; Park, J.G. Performance of Simple Fibrosis Score in Non-Alcoholic Fatty Liver Disease with and without Type 2 Diabetes. Endocrinol. Metab. (Seoul) 2023, 38, 277–281. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Levin, A.; Ahmed, S.B.; Carrero, J.J.; Foster, B.; Francis, A.; Hall, R.K.; Herrington, W.G.; Hill, G.; Inker, L.A.; Kazancioglu, R.; et al. Executive summary of the KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease: known knowns and known unknowns. Kidney Int. 2024, 105, 684–701. [Google Scholar] [CrossRef]
- Levey, A.S.; Inker, L.A.; Matsushita, K.; Greene, T.; Willis, K.; Lewis, E.; de Zeeuw, D.; Cheung, A.K.; Coresh, J. GFR decline as an end point for clinical trials in CKD: a scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am. J. Kidney Dis. 2014, 64, 821–835. [Google Scholar] [CrossRef]
- Levey, A.S.; Gansevoort, R.T.; Coresh, J.; Inker, L.A.; Heerspink, H.L.; Grams, M.E.; Greene, T.; Tighiouart, H.; Matsushita, K.; Ballew, S.H.; et al. Change in Albuminuria and GFR as End Points for Clinical Trials in Early Stages of CKD: A Scientific Workshop Sponsored by the National Kidney Foundation in Collaboration With the US Food and Drug Administration and European Medicines Agency. Am. J. Kidney Dis. 2020, 75, 84–104. [Google Scholar] [CrossRef]
- Yokoyama, H.; Araki, S.I.; Kawai, K.; Yamazaki, K.; Shirabe, S.I.; Sugimoto, H.; Minami, M.; Miyazawa, I.; Maegawa, H.; Group, J.S. The Prognosis of Patients With Type 2 Diabetes and Nonalbuminuric Diabetic Kidney Disease Is Not Always Poor: Implication of the Effects of Coexisting Macrovascular Complications (JDDM 54). Diabetes Care 2020, 43, 1102–1110. [Google Scholar] [CrossRef]
- Friedman, S.L.; Neuschwander-Tetri, B.A.; Rinella, M.; Sanyal, A.J. Mechanisms of NAFLD development and therapeutic strategies. Nat. Med. 2018, 24, 908–922. [Google Scholar] [CrossRef] [PubMed]
- Brenner, B.M.; Lawler, E.V.; Mackenzie, H.S. The hyperfiltration theory: a paradigm shift in nephrology. Kidney Int. 1996, 49, 1774–1777. [Google Scholar] [CrossRef]
- Li, Z.; Woollard, J.R.; Wang, S.; Korsmo, M.J.; Ebrahimi, B.; Grande, J.P.; Textor, S.C.; Lerman, A.; Lerman, L.O. Increased glomerular filtration rate in early metabolic syndrome is associated with renal adiposity and microvascular proliferation. Am. J. Physiol. Renal Physiol. 2011, 301, F1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Song, W.J.; Chen, W.; Pan, Z.; Zhang, J.; Fan, L.; Li, J. Metabolic dysfunction-associated steatotic liver disease-related hepatic fibrosis increases risk of insulin resistance, type 2 diabetes, and chronic kidney disease. Eur. J. Gastroenterol. Hepatol. 2024, 36, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Li, Y.; Zhang, Y.; Zhan, X.; Tian, X.; Li, J.; Wang, R.; He, Y.; Wang, A.; Wu, S. Severity and Remission of Metabolic Dysfunction-Associated Fatty/Steatotic Liver Disease With Chronic Kidney Disease Occurrence. J. Am. Heart Assoc. 2024, 13, e032604. [Google Scholar] [CrossRef]
- Zhang, H.; Chen, R.; Xu, X.; Yang, M.; Xu, W.; Xiang, S.; Wang, L.; Jiang, X.; Hua, F.; Huang, X. Metabolically healthy obesity is associated with higher risk of both hyperfiltration and mildly reduced estimated glomerular filtration rate: the role of serum uric acid in a cross-sectional study. J. Transl. Med. 2023, 21, 216. [Google Scholar] [CrossRef]
- Kishi, S. Redefining glomerular hyperfiltration: pathophysiology, clinical implications, and novel perspectives. Hypertens. Res. 2025, 48, 1176–1178. [Google Scholar] [CrossRef]
- Koh, E.S.; Kim, G.H.; Chung, S. Intrarenal Mechanisms of Sodium-Glucose Cotransporter-2 Inhibitors on Tubuloglomerular Feedback and Natriuresis. Endocrinol. Metab. (Seoul) 2023, 38, 359–372. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Rhee, C.M.; Chou, J.; Ahmadi, S.F.; Park, J.; Chen, J.L.; Amin, A.N. The Obesity Paradox in Kidney Disease: How to Reconcile it with Obesity Management. Kidney Int. Rep. 2017, 2, 271–281. [Google Scholar] [CrossRef]
- Helal, I.; Fick-Brosnahan, G.M.; Reed-Gitomer, B.; Schrier, R.W. Glomerular hyperfiltration: definitions, mechanisms and clinical implications. Nat. Rev. Nephrol. 2012, 8, 293–300. [Google Scholar] [CrossRef]
Figure 1.
Commutative incidence of chronic kidney disease progression according to baseline GHF and MASLD. GHF, glomerular hyperfiltration; MASLD, metabolic dysfunction associated–steatotic liver disease.
Figure 1.
Commutative incidence of chronic kidney disease progression according to baseline GHF and MASLD. GHF, glomerular hyperfiltration; MASLD, metabolic dysfunction associated–steatotic liver disease.
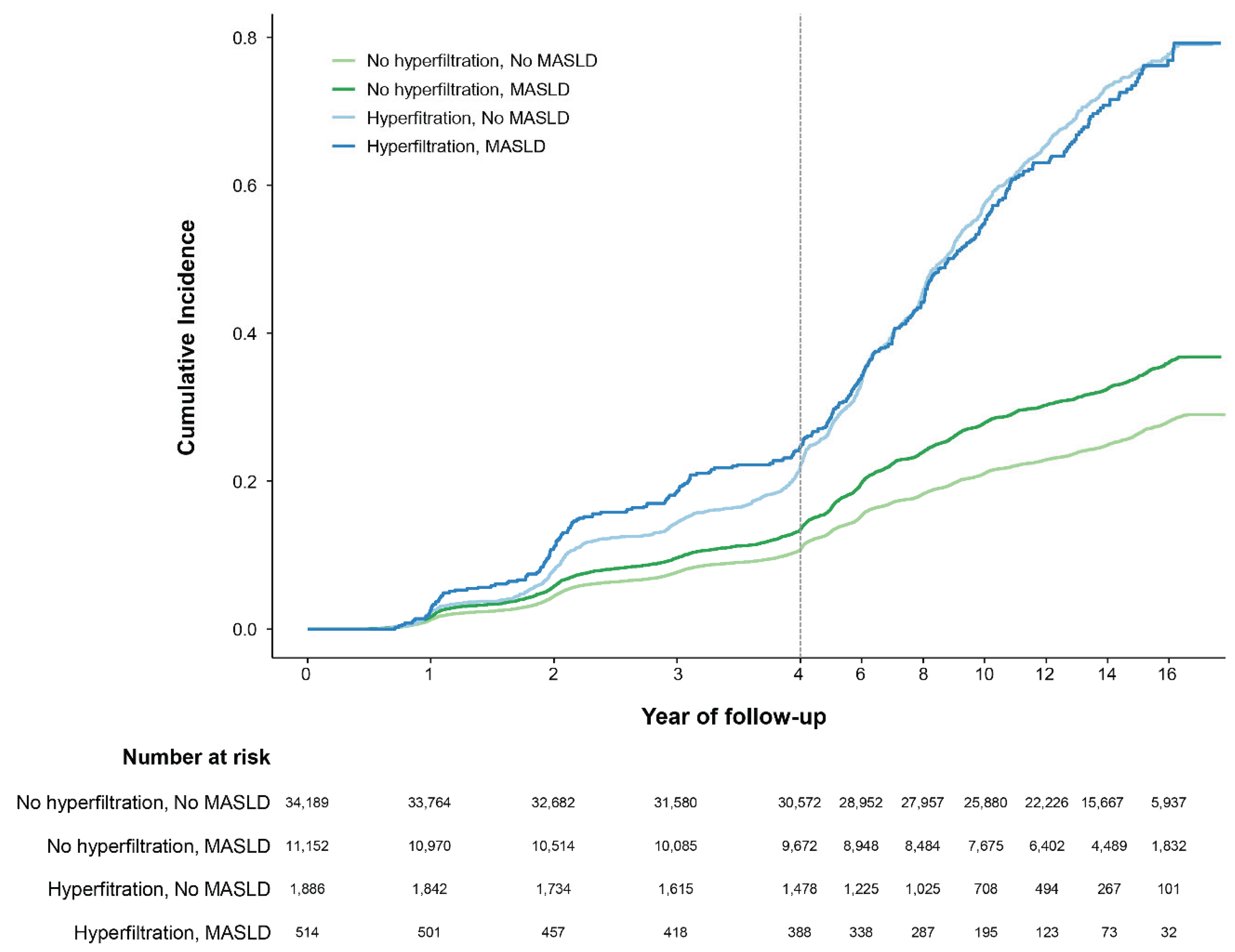
Figure 2.
Commutative incidence of advanced liver fibrosis according to baseline GHF and MASLD. GHF, glomerular hyperfiltration; MASLD, metabolic dysfunction associated–steatotic liver disease.
Figure 2.
Commutative incidence of advanced liver fibrosis according to baseline GHF and MASLD. GHF, glomerular hyperfiltration; MASLD, metabolic dysfunction associated–steatotic liver disease.
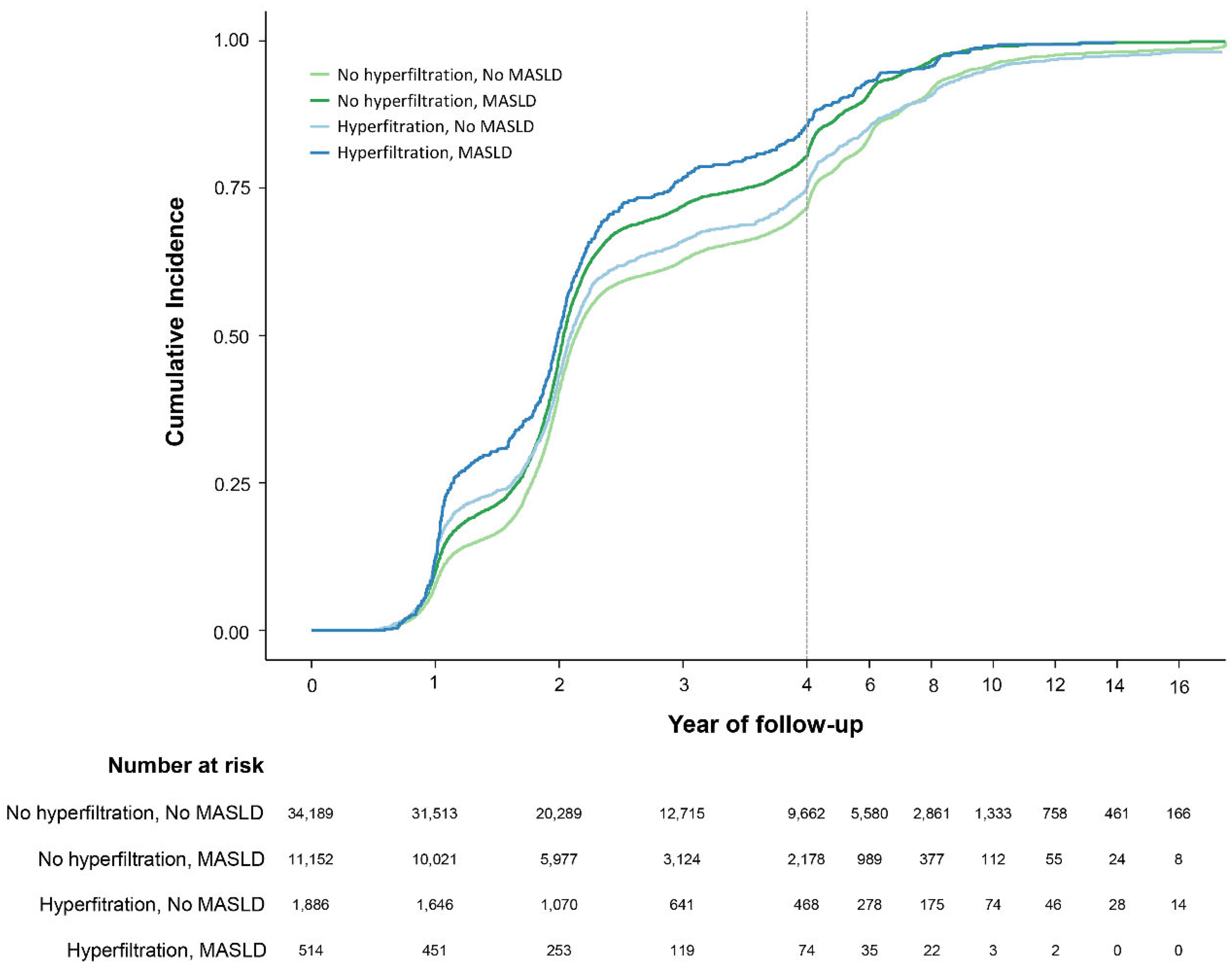
Figure 3.
Subgroup analysis of chronic kidney disease progression according to baseline GHF and MASLD. BMI, body mass index; CI, confidence interval; eGFR, estimated glomerular filtration rate; GHF, glomerular hyperfiltration; HR, hazard ratio; MASLD, metabolic dysfunction-associated steatotic liver disease; SBP, systolic blood pressure. * Adjusted for age, sex, baseline eGFR, BMI, WC, SBP, alcohol intake, and regular exercise. When adjusting for subgroups, variables corresponding to the criteria of the respective groups were excluded from the adjustment variables.
Figure 3.
Subgroup analysis of chronic kidney disease progression according to baseline GHF and MASLD. BMI, body mass index; CI, confidence interval; eGFR, estimated glomerular filtration rate; GHF, glomerular hyperfiltration; HR, hazard ratio; MASLD, metabolic dysfunction-associated steatotic liver disease; SBP, systolic blood pressure. * Adjusted for age, sex, baseline eGFR, BMI, WC, SBP, alcohol intake, and regular exercise. When adjusting for subgroups, variables corresponding to the criteria of the respective groups were excluded from the adjustment variables.
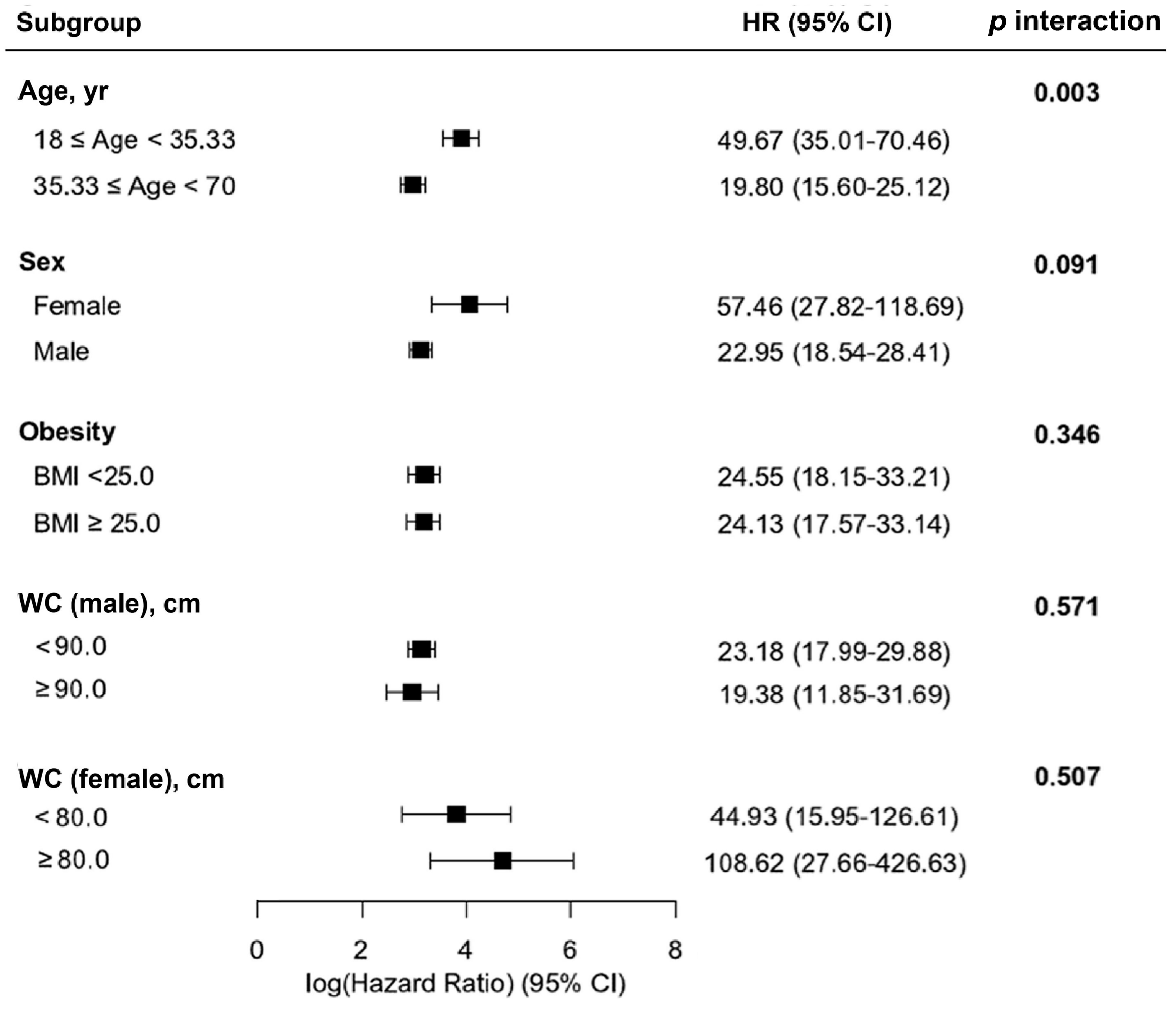

Table 1.
Baseline characteristics of participants by metabolic dysfunction-associated steatotic liver disease and metabolic dysfunction–associated fatty liver disease.
Table 1.
Baseline characteristics of participants by metabolic dysfunction-associated steatotic liver disease and metabolic dysfunction–associated fatty liver disease.
| Characteristics | Total | MASLD | MAFLD | ||||
|---|---|---|---|---|---|---|---|
| No | Yes | p-Value | No | Yes | p-Value | ||
| Number, n (%) | 47,741 | 36,075 (75.57) | 11,666 (24.43) | 36,571 (76.61) | 11,170 (23.39) | ||
| Male, n (%) | 31,008 (65.0) | 20,504 (56.8) | 10,504 (90.0) | < 0.001 | 20,911 (57.2) | 10,097 (90.4) | < 0.001 |
| Age, years | 35.33 (5.20) | 35.13 (5.13) | 35.95 (5.38) | < 0.001 | 35.14 (5.14) | 35.95 (5.36) | < 0.001 |
| BMI, kg/m2 | 23.36 (3.03) | 22.46 (2.59) | 26.17 (2.51) | < 0.001 | 22.45 (2.58) | 26.36 (2.40) | < 0.001 |
| WC, cm | 79.43 (9.27) | 76.51 (8.24) | 87.69 (6.65) | < 0.001 | 76.56 (8.21) | 88.10 (6.47) | < 0.001 |
| FBG, mg/dL | 92.61 (10.71) | 91.27 (9.14) | 96.75 (13.74) | < 0.001 | 91.30 (9.13) | 96.89 (13.91) | < 0.001 |
| Hemoglobin A1c, % | 5.39 (0.31) | 5.36 (0.29) | 5.48 (0.35) | < 0.001 | 5.36 (0.29) | 5.48 (0.35) | < 0.001 |
| SBP, mmHg | 113.55 (13.10) | 111.82 (12.54) | 118.88 (13.36) | < 0.001 | 111.83 (12.52) | 119.17 (13.40) | < 0.001 |
| DBP, mmHg | 73.60 (9.78) | 72.21 (9.34) | 77.90 (9.85) | < 0.001 | 72.22 (9.33) | 78.10 (9.87) | < 0.001 |
| AST, U/L | 24.32 (16.14) | 22.61 (16.79) | 29.59 (12.53) | < 0.001 | 22.66 (16.74) | 29.75 (12.55) | < 0.001 |
| ALT, U/L | 27.51 (26.18) | 22.17 (23.05) | 44.03 (28.29) | < 0.001 | 22.32 (23.16) | 44.49 (28.23) | < 0.001 |
| Triglyceride, mg/dL | 126.53 (81.39) | 107.63 (59.91) | 184.99 (107.20) | < 0.001 | 108.44 (60.65) | 185.76 (108.14) | < 0.001 |
| HDL, mg/dL | 54.55 (11.93) | 56.41 (12.15) | 48.81 (9.12) | < 0.001 | 56.33 (12.13) | 48.73 (9.10) | < 0.001 |
| Cr, mg/dL | 1.04 (0.16) | 1.01 (0.16) | 1.12 (0.14) | < 0.001 | 1.01 (0.16) | 1.12 (0.14) | < 0.001 |
| eGFR, mL/min/1.73m2 | 85.46 (10.84) | 86.17 (10.83) | 83.24 (10.55) | < 0.001 | 86.16 (10.83) | 83.16 (10.54) | < 0.001 |
| Alcohol intake, g/day | 6.38 (7.26) | 5.82 (7.12) | 8.09 (7.42) | < 0.001 | 5.83 (7.12) | 8.15 (7.40) | < 0.001 |
| Smoking, n (%) | < 0.001 | < 0.001 | |||||
| never or ex- | 33,770 (72.2) | 26,709 (75.6) | 7,061 (61.6) | 27,047 (75.5) | 6,723 (61.3) | ||
| current | 13,023 (27.8) | 8,627 (24.4) | 4,396 (38.4) | 8,780 (24.5) | 4,243 (38.7) | ||
| Regular exercise, n (%) | 6,249 (13.1) | 4,944 (13.7) | 1,305 (11.2) | < 0.001 | 4,982 (13.6) | 1,267 (11.3) | < 0.001 |
| FIB-4 | 0.16 (0.08) | 0.17 (0.08) | 0.11 (0.05) | < 0.001 | 0.17 (0.08) | 0.11 (0.05) | < 0.001 |
| NFS | -3.40 (0.84) | -3.34 (0.84) | -3.56 (0.82) | < 0.001 | -3.35 (0.85) | -3.55 (0.81) | < 0.001 |
Values are expressed as n (%), mean (± standard deviation), percentage, or median (interquartile range). ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; Cr, creatinine; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; FBG, fasting blood glucose; FIB-4, fibrosis-4 index; HDL, high-density lipoprotein; MAFLD, metabolic dysfunction–associated fatty liver disease; MASLD, metabolic dysfunction-associated steatotic liver disease; NFS, nonalcoholic fatty liver disease fibrosis score; SBP, systolic blood pressure; TC, total cholesterol; WC, waist circumference.
Table 2.
Risk of chronic kidney disease progression by the presence of baseline glomerular hyperfiltration in patients with metabolic dysfunction-associated steatotic/fatty liver disease.
Table 2.
Risk of chronic kidney disease progression by the presence of baseline glomerular hyperfiltration in patients with metabolic dysfunction-associated steatotic/fatty liver disease.
| Subject groups | PY | Number | Events | IR per 10000 PY | HR (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |||||
| GHF (-) | |||||||
| MASLD (-) | 414,579.00 | 34,189.00 | 8,781.00 | 211.81 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| MASLD (+) | 127,389.55 | 11,152.00 | 3,710.00 | 291.23 | 1.36 (1.31-1.42) | 1.05 (1.01-1.09) | 0.95 (0.91-0.99) |
| GHF (+) | |||||||
| MASLD (-) | 4,286.60 | 514.00 | 349.00 | 814.16 | 3.62 (3.26-4.03) | 2.79 (2.50-3.10) | 2.56 (2.30-2.86) |
| MASLD (+) | 16,065.92 | 1,886.00 | 1,334.00 | 830.33 | 3.69 (3.48-3.91) | 3.81 (3.60-4.04) | 3.88 (3.66-4.11) |
| Akaike Information Criterion | 296,683.91 | 291,268.91 | 285,665.46 | ||||
| Bayesian Information Criterion | 296,706.59 | 291,306.70 | 285,733.34 | ||||
| GHF (-) | |||||||
| MAFLD (-) | 420,059.90 | 34,664.00 | 8,916.00 | 212.26 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| MAFLD (+) | 121,908.64 | 10,677.00 | 3,575.00 | 293.25 | 1.37 (1.32-1.43) | 1.06 (1.02-1.10) | 0.95 (0.91-1.00) |
| GHF (+) | |||||||
| MAFLD (-) | 4,096.67 | 493.00 | 336.00 | 820.18 | 3.64 (3.26-4.06) | 2.79 (2.50-3.12) | 2.55 (2.28-2.85) |
| MAFLD (+) | 16,255.85 | 1,907.00 | 1,347.00 | 828.62 | 3.67 (3.47-3.89) | 3.81 (3.59-4.03) | 3.87 (3.65-4.10) |
| Akaike Information Criterion | 296,682.56 | 291,268.64 | 285,666.93 | ||||
| Bayesian Information Criterion | 296,705.24 | 291,306.43 | 285,734.81 | ||||
Model 1: no adjustment. Model 2: adjusted for age and sex. Model 3: additionally adjusted for baseline eGFR, BMI, SBP, regular exercise, and current smoking status. BMI, body mass index; CI, confidence interval; eGFR, estimated glomerular filtration rate; GHF, glomerular hyperfiltration; HR, hazard ratio; IR, incidence rate; MAFLD, metabolic dysfunction–associated fatty liver disease; MASLD, metabolic dysfunction-associated steatotic liver disease; PY, person years; SBP, systolic blood pressure.
Table 3.
Risk of advanced liver fibrosis in patients with metabolic dysfunction-associated steatotic liver disease or metabolic dysfunction–associated fatty liver disease according to baseline glomerular hyperfiltration.
Table 3.
Risk of advanced liver fibrosis in patients with metabolic dysfunction-associated steatotic liver disease or metabolic dysfunction–associated fatty liver disease according to baseline glomerular hyperfiltration.
| Subject groups | PY | Number | Events | IR per 10000 PY | HR (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |||||
| MASLD (-) | |||||||
| GHF (-) | 118,084.48 | 34,189.00 | 33,576.00 | 2,843.39 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| GHF (+) | 6,207.03 | 1,886.00 | 1,829.00 | 2,946.66 | 1.05 (1.00-1.10) | 1.07 (1.02-1.12) | 1.08 (1.03-1.13) |
| MASLD (+) | |||||||
| GHF (-) | 30,980.77 | 11,152.00 | 11,112.00 | 3,586.74 | 1.30 (1.27-1.33) | 1.26 (1.23-1.29) | 1.20 (1.17-1.23) |
| GHF (+) | 1,299.16 | 514.00 | 510.00 | 3,925.62 | 1.45 (1.33-1.58) | 1.42 (1.30-1.55) | 1.36 (1.24-1.48) |
| Akaike Information Criterion | 924,208.42 | 922,796.69 | 902,578.24 | ||||
| Bayesian Information Criterion | 924,234.69 | 922,840.48 | 902,656.88 | ||||
| MAFLD (-) | |||||||
| GHF (-) | 119,479.10 | 34,664.00 | 34,049.00 | 2,849.79 | 1.00 (Reference) | 1.00 (Reference) | 1.00 (Reference) |
| GHF (+) | 6,271.58 | 1,907.00 | 1,849.00 | 2,948.22 | 1.04 (0.99-1.09) | 1.07 (1.02-1.12) | 1.08 (1.03-1.13) |
| MAFLD (+) | |||||||
| GHF (-) | 29,586.15 | 10,677.00 | 10,639.00 | 3,595.94 | 1.30 (1.27-1.33) | 1.26 (1.23-1.29) | 1.20 (1.17-1.23) |
| GHF (+) | 1,234.61 | 493.00 | 490.00 | 3,968.86 | 1.47 (1.35-1.61) | 1.44 (1.31-1.57) | 1.37 (1.25-1.50) |
| Akaike Information Criterion | 924,221.65 | 922,804.07 | 902,590.78 | ||||
| Bayesian Information Criterion | 924,247.92 | 922,847.86 | 902,669.42 | ||||
Model 1: no adjustment. Model 2: adjusted for age and sex. Model 3: additionally adjusted for baseline eGFR, BMI, SBP, regular exercise, and current smoking status. BMI, body mass index; CI, confidence interval; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; GHF, glomerular hyperfiltration; HR, hazard ratio; IR, incidence rate; MAFLD, metabolic dysfunction–associated fatty liver disease; MASLD, metabolic dysfunction-associated steatotic liver disease; PY, person years; SBP, systolic blood pressure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



