
Submitted:
23 July 2025
Posted:
25 July 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Sex and gender disparities have emerged as critical determinants of COVID-19 outcomes, with males exhibiting higher hospitalization and mortality rates than females. Sex steroids such as estradiol, progesterone, and testosterone have been proposed as modulators of these differences, given their known roles in inflammation, immune function, and vascular health. However, the precise hormonal mechanisms underlying COVID-19 severity, particularly among individuals with comorbid hypertension—a major risk factor for adverse outcomes—remain unclear. In this study, we investigated circulating levels of key sex hormones and their neuroactive metabolites in 116 hypertensive COVID-19 patients enrolled through an urban academic emergency department. Our findings revealed distinct sex-based hormonal profiles and associations with disease severity. Males exhibited higher serum estradiol and testosterone levels, while progesterone levels were significantly higher in postmenopausal females. Notably, hospitalized patients showed elevated estradiol and progesterone levels compared to non-hospitalized individuals, whereas ICU-admitted patients had significantly lower concentrations of all three hormones. A unique exception was ICU-admitted postmenopausal females, who exhibited increased serum testosterone levels relative to non-ICU females. Additionally, in males, elevated 3α-diol was associated with hospitalization and ICU admission, while lower allopregnanolone and estradiol levels correlated with hypoxia in males and females, respectively. These results highlight a dynamic, sex-specific hormonal response to COVID-19 progression in hypertensive individuals, suggesting early upregulation and late depletion of protective sex steroids. Understanding these patterns may improve clinical risk stratification and inform the development of sex-targeted therapeutic interventions for COVID-19 and related inflammatory conditions.
Keywords:
COVID-19
; reproductive steroids
; sex steroids
; estradiol
; progesterone
; testosterone
; neuroactive steroid and metabolites
; hypertension
; emergency department
Introduction
Since the beginning of the COVID-19 pandemic, sex and gender disparities have been evident with regard to disease prevalence, severity, and mortality [1,2,3,4]. Hospitalization and intensive care unit (ICU) admissions were reported to be higher in males than in females [5,6]. Scully et al. recently reported that the case fatality rate for males is 1.7 times higher than for females [7]. Despite these epidemiological data trends, the underlying molecular mechanisms and pathophysiology have remained unclear [3]. Preliminary speculations on the emerging role of androgens as a potential culprit in association with worse prognosis, and female sex steroids as possibly protective factors [8,9,10,11]. In addition, confluence of sex hormones, aging, and inflammation as closely connected aspects has also been investigated [12,13]. Consistently, several pathological conditions that are a risk factor for Covid-19 symptom severity, including metabolic syndrome and type 2 diabetes are often observed in individuals who express lower blood testosterone levels. [14,15,16]. Previous studies have also observed a correlation between Covid-19 symptom severity and respiratory intensive care unit (RICU) hospitalizations with decreased total and free testosterone blood concentrations [17]. Another study found a significant inverse correlation between baseline serum total testosterone concentration decrease and the percentage increase to be admitted to ICU. Likewise, the total testosterone concentration decrease was significantly correlated with the % probability of mortality [17,18]. While these studies collectively suggest that decreased baseline levels of testosterone may predict Covid-19 symptom severity and mortality specifically in men admitted to ICU, the role and the mechanisms involving sex hormones in Covid-19 illness remain largely elusive.
A major contributing factor to the differing mortality in COVID-19 in men versus women have also been seen in animal models. Male mice expressing SARS CoV infection had higher mortality, and the lower mortality in female mice was attributed to the protective role of estrogen [19]. One of the major forms of estrogen, estradiol, has been shown to dampen the production of excessive innate inflammatory cytokines by monocytes and macrophages [19]. Most critically, the host cell entry receptor for SARS-CoV-2, the angiotensin-converting enzyme 2 (ACE2) is regulated by estrogen [11,20].
Among Covid-19 comorbidities and risk factors, high blood pressure or hypertension has been one of the most prevalent and critical in increasing the odds for hospitalization, ICU admission, and mortality [21]. Like for Covid-19, hypertension shows a strong sex dimorphism, which points to sex steroids as a possible underlying cause [22]. Indeed, experimental studies have observed that testosterone and estrogen play an important role in regulating blood pressure and hypertension. For example, estrogens may induce vasodilation which results in lower blood pressure, whereas androgens have been reported to induce both vasoconstriction and vasorelaxation [23,24,25]. Some studies in women have observed higher testosterone and estradiol levels in individual with hypertension [26,27,28]. However, studies that investigated the role of sex steroid levels in hypertension have generally originated mixed results. Intriguingly, the role of sex steroids in the underlaying mechanisms contributing to Covid-19 symptom severity and mortality in individuals who suffer hypertension remains under-investigated.
Overall, with the understanding that male sex is a risk factor for developing severe SARS CoV infection, in this investigation, we aimed to characterize the predominant sex hormones progesterone, estradiol, and testosterone in Covid-19 disease severity and progression in serum obtained from patients with hypertension. We also studied the serum concentrations of progesterone’s metabolites, including the isomers of allopregnanolone, epipregnanolone, pregnanolone, and isoallopregnanolone and the metabolites of testosterone, including 3alpha-diol and 3beta-diol. A better understanding of sex differences and the role of sex steroids in Covid-19 would help to optimize diagnostic strategies but also the proper pharmacological management of patients with Covid-19.
Methods
Study Population
Participants enrolled in this study were patients treated or admitted through an urban academic emergency department between August 2020 and April 2021 in Chicago, USA. Male participants had to be >21 years of age, and female participants had to be 50 years of age and above, with a documented history of hypertension, tested positive for SARS-CoV-2, consented to participate in the study and had blood drawn. Those that were unable to verbalize comprehension of the study or had impaired decision making were excluded from the study [29].
An electronic informed consent (e-consent) was obtained from all participants under a protocol approved by the UIC Institutional Review Board (IRB). The e-consent was recorded for each participant on RedCap (Research Electronic Data Capture).
This study was conducted in accordance with ethical standards for human subjects research and was approved by the University of Illinois Chicago (UIC) Institutional Review Board (IRB Protocol # 2020-0567).
Gas Chromatography-Mass Spectrometry Neuroactive Steroid Assays
Serum samples were allowed to settle for at least 30 minutes and then were centrifuged for 10 minutes at 3,000 rpm and 4°C to remove clots. Serum was aliquoted into 0.5 mL cryovials and stored at −80°C until time of sex steroid assays. We measured levels of progesterone, testosterone, and estradiol examining absolute levels of each (pg/ml). Extraction, high performance liquid chromatography (HPLC), derivatization, and Gas Chromatography-Mass spectrometry (GC/MS) quantification analyses of sex steroids were performed as previously described [30,31]. Samples were extracted in ethyl acetate and lyophilized.
Sex steroids of interest were then purified and separated using HPLC. Tritiated sex steroids (American Radiolabeled Chemicals, St. Louis, MO, USA) were added to monitor the HPLC retention profile, while deuterated internal standards consisting of 2 pmol of deuterium-labeled sex steroids (CDN Isotopes, Pointe-Claire, QC, and Steraloids, Newport, RI, USA) were used to allow quantification of the compound of interest and correct for procedural losses. Each steroid of interest was then derivatized in heptafluorobutyric acid (HFBA) (ThermoFisher, USA) for GC/MS. Mass spectrometry analysis was performed in the standard electron impact mode for progesterone, testosterone, and estradiol measurements. The quantity of each steroid of interest was calculated by dividing the area under the peak of the steroid in the sample by the area under the peak of the deuterated internal standard. Progesterone sensitivity is ~.03 ng/mL with intra-assay coefficient of variation (CV) of ~4%. The detection limit for each steroid is approximately 10 fmol/mL. Intra-assay CV for these sex steroids is <5%.
Analytic Methods
Univariate analysis was conducted to assess the distribution of sex steroids and the other demographic and clinical variables. Measures of central tendency were examined for continuous variables, and frequencies were assessed for categorical variables. Bivariate analyses were conducted to assess the difference in sex steroids by demographic and clinical variables, when stratified by sex. Analyses were done using SAS 9.4 (SAS Institute, Cary, NC, USA). A p-value of 0.05 was used for statistical significance. Chi-Square test and fisher’s exact test were used to assess associations by sex, and Mann Whitney U tests were used to assess difference in the level of hormones by sex and other clinical variables.
Results
Demographic Characteristics
The demographic and clinical outcomes of a total of 116 participants with hypertension enrolled through an urban academic emergency department are detailed in Table 1. The majority (55.6%) were non-Hispanic Black, 34.8% were Hispanic, 5.2% were non-Hispanic White, and the remaining patients were of other racial and ethnic groups. 54.3% of the sample was male, and 47% were >65 years of age (84.5% were >50 years of age). Only 20.1% of participants had private insurance, and 43.1% were Medicare, 23.3% Medicaid, and the remaining were either ‘Other’ insurance, no insurance or unknown.
The majority of the participants were hospitalized (83.6%), and 28.4% were hospitalized for >7 days. The individuals who had been admitted to ICU were 15.5%, and 4 of them had received ventilator support (Table 1). There were no differences in demographic characteristics and clinical outcomes by sex, as presented in Table 1.
Sex Steroid Levels in Male and Females with Hypertension and COVID-19 Infection
Figure 1 shows that, as expected, progesterone levels in serum were higher in females (p=0.03) than in males, while testosterone (p=0.01) and allopregnanolone (p= 0.069) concentrations were lower both in terms of mean and median in females. No difference was observed with respect to other hormones.
Sex Steroid Levels and Clinical Outcomes in Subjects with Hypertension and COVID-19 Infection
Serum testosterone concentrations were much lower in Covid-19 hospitalized males with hypertension than in non-hospitalized males (p=0.016) (Figure 1). In contrast, the testosterone metabolite, 3alpha-diol content was higher in hospitalized males when compared to non-hospitalized males (p=0.049). No differences were observed in sex steroid levels among females by hospitalization status. Serum 3alpha-diol content was also higher in males that were admitted to ICU than males that were not admitted and was marginally significant (p=0.06).
The progesterone metabolite, allopregnanolone concentrations in serum were lower in males that were hypoxic than in males that were not hypoxic (p=0.046). In females, serum estradiol content was much lower in those with hypoxia than those without hypoxia (p=0.0147).
In males, the progesterone metabolite, isoallopregnanolone serum content was higher in those that had a longer length of stay (>7days; p=0.018).
Sex Steroid Concentrations and Symptoms in Male and Females with Hypertension and COVID-19 Infection
We analyzed disease progression, defined by symptoms of hypoxia, shortness of breath, fever, loss of taste or smell, and fatigue, and found sex-stratified differences in hormones levels. Progesterone levels in males that had a fever were marginally significantly higher (p = 0.05) than in males who did not had fever, while its metabolite, epipregnanolone, serum concentrations were lower among those that had chest pain (p=0.019). In patients who presented with fever also serum testosterone concentration tended to be higher (p=0.053). The testosterone metabolite, 3alpha-diol, concentrations in serum were higher for those subjects who had loss of smell/taste, even though did not reach significance (p=0.06). The loss of smell/taste was associated with a tendency of lower concentration levels of epipregnanolone in serum (p=0.057) (Figure 2).
Sex Dimorphism in Steroid Levels and Hospitalization and ICU Admission
When stratified by hospitalization and sex, serum progesterone levels did not differ by hospitalization or sex in patients with hypertension and Covid-19 infection. However, some differences were noted. Hospitalized females had generally lower serum estradiol concentration, while hospitalized males had higher estradiol levels. In contrast, progesterone levels were higher in hospitalized females compared to hospitalized males, while hospitalized males had highest estrogen levels compared to all the 3 categories. Consistent with males having higher serum estradiol levels relative to females, male ICU patients had higher estradiol levels relative to female ICU patients. However, male ICU patients had lower estradiol levels compared to males not admitted to the ICU. Similarly, female ICU patients had significantly lower estradiol levels compared to females not admitted to ICU. Serum progesterone concentration was lower in ICU males and females relative to males and females not admitted in the ICU.
In general, across all three main sex hormones examined (progesterone, estradiol, and testosterone), ICU patients of both sexes had lower levels of hormones compared to non-ICU patients, except for ICU females who had higher serum testosterone concentration compared to non-ICU females.
Discussion
This study was conducted in an ethnically diverse sample of 116 male and female patients with hypertension that contracted Covid-19 and were enrolled through an urban academic emergency department [29]. All females were above >50 years old and considered post-menopausal. Their disease severity was assessed by hospitalization, ICU admission, and vasopressor use. In our study, we describe for the first time sex-hormones differences in Covid-19 patients. We show that in males there was a predominance of serum estradiol concentrations compared to postmenopausal females whereas serum progesterone levels were higher in females relative to males. Testosterone levels in serum were higher in males than in postmenopausal women. There was a paradoxical response for serum progesterone and estradiol concentrations for hospitalization vs ICU admission. Among those individuals who were hospitalized, serum progesterone and estrogen concentrations were highest compared to patients who were not hospitalized. In contrast, patients who had been admitted to the ICU had lower serum levels of progesterone, estradiol and testosterone compared to patients not admitted to the ICU. Generally, considering the main sex hormones examined, progesterone, estradiol, and testosterone, subjects who were admitted to the ICU of both sexes showed lower levels of sex steroids when compared to non-ICU patients. One exception were the female patients who were admitted in the ICU who exhibited higher serum testosterone levels when compared to non-ICU females.
Our study showed a sex dimorphism in sex steroid levels and clinical outcomes, including hospitalization and ICU admission. For instance, serum estradiol levels were found lower in post-menopausal females with hypertension and Covid-19 infection who were hospitalized, while in males, estradiol concentrations in serum were higher. Similarly, male subjects who were admitted in the ICU had higher estradiol concentrations versus females ICU patients. Furthermore, females who were hospitalized showed the highest median serum progesterone levels when compared to hospitalized males.
These dynamic, sex-specific changes in circulating sex steroid levels in response to COVID-19, particularly in the context of comorbid hypertension, suggest a general trend toward early upregulation of protective hormones during milder disease, followed by depletion as symptom severity increases. Prior literature has also alluded to the concept of hypothalamic hypogonadism after critical illness [32,33].
In males, high estradiol levels may result from increased aromatization of testosterone, a process catalyzed by the enzyme aromatase, which is upregulated during inflammation and adiposity [34,35]. This conversion is relevant in the context of hypertensive males with Covid-19, a population often characterized by increased metabolic inflammation. Elevated testosterone levels in these patients may reflect a maladaptive or compensatory response [36]. While testosterone has been shown to exert both pro-inflammatory and anti-inflammatory effects [37], high levels have been linked to adverse outcomes in women with Covid-19 [38]. In contrast, estradiol is generally associated with anti-inflammatory actions, with studies suggesting it attenuates pro-inflammatory cytokines through inhibition of NF-κB signaling and reduction of IL-6 and TNF-α production. However, in some contexts, including postmenopausal females with comorbid hypertension, higher estradiol levels have been correlated with increased disease severity, suggesting a possible loss of protective effect [39,40,41]. Emerging data suggest that both low and high testosterone levels, depending on timing and disease stage, can be associated with poor prognosis in Covid-19 [38].
Postmenopausal women show substantial reduction in estradiol production, yielding lower circulating estrogen levels compared to premenopausal women and often even to age-matched men. In individual affected by COVID-19, the decline of endogenous estrogen may contribute to impaired immunomodulation and vascular repair mechanisms, potentially exacerbating outcomes in postmenopausal females, particularly those with underlying cardiovascular conditions such as hypertension.
Interestingly, the hospitalized females group showed the highest median progesterone levels. Progesterone has been shown to have anti-inflammatory and immunomodulatory effects, potentially offering some protective role during moderate disease, though this was not observed at the ICU level.
With respect to hypertension, previous studies have demonstrated that sex hormones influence blood pressure regulation through vascular tone, renal sodium handling, and inflammation [26,28]. Lower estradiol and progesterone levels post-menopause are associated with heightened cardiovascular risk, which may compound the severity of COVID-19 outcomes in this subgroup. In the context of COVID-19, our results are consistent with prior reports that link altered sex steroid levels with immune dysregulation and worse clinical trajectories.
COVID-19 and similar acute inflammatory states can suppress the hypothalamic-pituitary-gonadal axis and disrupt adrenal function. In our study, hospitalized patients displayed higher sex steroid levels than non-hospitalized individuals, which may reflect an early upregulation of steroidogenic pathways. In contrast, ICU patients showed a generalized decline, consistent with endocrine exhaustion. This biphasic response mirrors patterns seen in other forms of systemic stress, for example in neuropsychiatric conditions and underscores the dynamic hormonal regulation during disease progression [42,43,44,45].
The progesterone metabolite, allopregnanolone, a potent positive allosteric modulator of GABAA receptors with well-established anti-inflammatory properties [46], was reduced in hypoxic males, suggesting lowered anti-inflammatory protective mechanisms at a critical phase of illness. Conversely, isoallopregnanolone levels were elevated in males with prolonged hospitalization, however, its dysregulated metabolism remains with unclear functional impact. Epipregnanolone concentrations were lower in males reporting chest pain and trended lower in those with loss of smell/taste, though its functional significance remains less well defined.
The testosterone metabolite 3α-diol was elevated in hospitalized and ICU-admitted males when testosterone was decreased, possibly reflecting increased testosterone metabolism through 5alpha-reductase during systemic inflammation. Overall, these findings point to a disruption in the balance of neuroactive steroids and androgen metabolites during severe COVID-19 infection, with potential implications for inflammatory regulation, but further mechanistic studies are needed to clarify their role.
Although our analysis centered on estradiol, progesterone, and testosterone, other steroids, such as DHEA, cortisol, estrone, and aldosterone, are also likely to shape inflammatory response in COVID-19. Future studies incorporating a broader steroid profile could elucidate interrelated endocrine mechanisms and clarify potential biomarkers of disease severity.
This study has several limitations. First, the sample size was modest, and multiple comparisons increased the potential for type I error. Second, the absence of a healthy control group limits our ability to interpret hormone levels in the context of baseline physiology. Third, although all women were postmenopausal, we lacked detailed information regarding hormone replacement therapy or exact menopausal timing, which may influence hormone levels. While exogenous hormone exposure was not assessed in our study, the potential influence of medications or hormone replacement therapy cannot be excluded. This represents a relevant consideration for future research, particularly in postmenopausal women whose endogenous steroid levels are already diminished and may respond differently to acute physiological stress. Finally, while hormone measurements were performed on serum collected during emergency admission, the time since infection onset was variable and not systematically recorded.
Notwithstanding these limitations, if replicated, the observed biphasic pattern of sex steroids, initial elevation followed by decline with worsening severity, could inform risk stratification. For example, monitoring estradiol or progesterone levels upon hospital admission might help identify patients at risk of progressing to critical illness. Additionally, sex-specific hormonal signatures could guide more personalized treatment approaches, particularly in the context of immunosuppressive therapies or anti-inflammatory interventions.
Conclusions
Our study highlights significant sex differences in serum sex steroid levels among hypertensive patients with COVID-19 and their association with disease severity. Elevated estradiol and progesterone in hospitalized patients—but decreased levels in ICU admissions—suggest a dynamic hormonal response to disease progression. These findings underscore the importance of considering sex steroids in the context of COVID-19 outcomes and support further investigation into their mechanistic and therapeutic roles in infection, inflammation, and critical illness.
Acknowledgments
This work was supported in part by NIH grants R01AA030292 (GP), R01MH134904 (GP). FBA received a Doctoral Dissertation Research Award from the Fulbright Commission Brazil. The project was funded by the Center for Clinical and Translational Science at University of Illinois at Chicago [2020COVID-03]. The authors wish to thank Majd Aljurdi for his help with artwork and editorial assistance.
Disclosure
Graziano Pinna served as a paid consultant to PureTech Health, GABA Therapeutics, and NeuroTrauma Sciences (Alpharetta, GA, USA). He has two patent applications, one on N-palmitoylethanolamine (PEA) and peroxisome proliferator-activated receptor alpha (PPAR-α) agonists US20180369171A1 allowed on May 16, 2023, and one on allopregnanolone analogs US11266663B2 allowed on March 8, 2022, in the treatment of neuropsychiatric disorders.
References
- Sharma G, Volgman AS, Michos ED. Sex Differences in Mortality from COVID-19 Pandemic: Are Men Vulnerable and Women Protected? JACC Case Rep. 2020:10.1016/j.jaccas.2020.04.027. [CrossRef]
- Capuano A, Rossi F, Paolisso G. Covid-19 Kills More Men Than Women: An Overview of Possible Reasons. Front Cardiovasc Med. 2020;7:131-131. [CrossRef]
- Pradhan A, Olsson P-E. Sex differences in severity and mortality from COVID-19: are males more vulnerable? Biol Sex Differ. 2020;11(1):53-53. [CrossRef]
- Mauvais-Jarvis F, Bairey Merz N, Barnes PJ, et al. Sex and gender: modifiers of health, disease, and medicine. The Lancet. 2020;396(10250):565-582. [CrossRef]
- Giagulli VA, Guastamacchia E, Magrone T, et al. Worse progression of COVID-19 in men: Is testosterone a key factor? Andrology. Jan 2021;9(1):53-64. [CrossRef]
- Stasi VD, Rastrelli G. The Role of Sex Hormones in the Disparity of COVID-19 Outcomes Based on Gender. J Sex Med. Dec 2021;18(12):1950-1954. [CrossRef]
- Scully EP, Haverfield J, Ursin RL, Tannenbaum C, Klein SL. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat Rev Immunol. 2020;20(7):442-447. [CrossRef]
- Mauvais-Jarvis F. Do Anti-androgens Have Potential as Therapeutics for COVID-19? Endocrinology. Aug 1 2021;162(8)doi:10.1210/endocr/bqab114.
- Lanser L, Burkert FR, Thommes L, et al. Testosterone Deficiency Is a Risk Factor for Severe COVID-19. Frontiers in endocrinology. 2021;12:694083. [CrossRef]
- Cinislioglu AE, Cinislioglu N, Demirdogen SO, et al. The relationship of serum testosterone levels with the clinical course and prognosis of COVID-19 disease in male patients: A prospective study. Andrology. Jul 19 2021;doi:10.1111/andr.13081.
- Pinna G. Sex and COVID-19: A Protective Role for Reproductive Steroids. Trends in Endocrinology & Metabolism. 2021/01/01/ 2021;32(1):3-6. [CrossRef]
- Dhindsa S, Zhang N, McPhaul MJ, et al. Association of Circulating Sex Hormones With Inflammation and Disease Severity in Patients With COVID-19. JAMA Netw Open. May 3 2021;4(5):e2111398. [CrossRef]
- Gubbels Bupp MR, Potluri T, Fink AL, Klein SL. The Confluence of Sex Hormones and Aging on Immunity. Frontiers in immunology. 2018;9:1269. [CrossRef]
- Dhindsa S, Reddy A, Karam JS, et al. Prevalence of subnormal testosterone concentrations in men with type 2 diabetes and chronic kidney disease. Eur J Endocrinol. 2015;173(3):359-366. [CrossRef]
- Dhindsa S, Ghanim H, Batra M, Dandona P. Hypogonadotropic hypogonadism in men with diabesity. Diabetes Care. 2018;41(7):1516-1525. [CrossRef]
- Balasubramanian V, Naing S. Hypogonadism in chronic obstructive pulmonary disease: incidence and effects. Curr Opin Pulm Med. 2012;18(2):112-117. [CrossRef]
- Rastrelli G, Di Stasi V, Inglese F, et al. Low testosterone levels predict clinical adverse outcomes in SARS-CoV-2 pneumonia patients. Andrology. 2021;9(1):88-98. [CrossRef]
- Çayan S, Uğuz M, Saylam B, Akbay E. Effect of serum total testosterone and its relationship with other laboratory parameters on the prognosis of coronavirus disease 2019 (COVID-19) in SARS-CoV-2 infected male patients: a cohort study. Aging Male. 2020;1-11. [CrossRef]
- Takahashi T, Iwasaki A. Sex differences in immune responses. Science. 2021;371(6527):347. [CrossRef]
- Di Florio DN, Sin J, Coronado MJ, Atwal PS, Fairweather D. Sex differences in inflammation, redox biology, mitochondria and autoimmunity. Redox Biology. 2020/04/01/ 2020;31:101482. [CrossRef]
- Peng M, He J, Xue Y, Yang X, Liu S, Gong Z. Role of Hypertension on the Severity of COVID-19: A Review. J Cardiovasc Pharmacol. 2021 Nov 1;78(5):e648-e655. PMID: 34321401; PMCID: PMC8562915 . [CrossRef]
- Reckelhoff JF. Gender differences in the regulation of blood pressure. Hypertension. 2001;37:1199–208. [CrossRef]
- Caulin-Glaser T, Garcia-Cardena G, Sarrel P, et al. 17 beta-estradiol regulation of human endothelial cell basal nitric oxide release, independent of cytosolic Ca2+ mobilization. Circ Res. 1997;81:885–92. [CrossRef]
- Schror K, Morinelli TA, Masuda A, et al. Testosterone treatment enhances thromboxane A2 mimetic induced coronary artery vasoconstriction in guinea pigs. Eur J Clin Invest. 1994;24 (Suppl 1):50–2. [CrossRef]
- Chou TM, Sudhir K, Hutchison SJ, et al. Testosterone induces dilation of canine coronary conductance and resistance arteries in vivo. Circulation. 1996;94:2614–9. [CrossRef]
- Hughes GS, Mathur RS, Margolius HS. Sex steroid hormones are altered in essential hypertension. J Hypertens. 1989;7:181–7.
- Sutton-Tyrrell K, Wildman RP, Matthews KA, et al. Sex-hormone-binding globulin and the free androgen index are related to cardiovascular risk factors in multiethnic premenopausal and perimenopausal women enrolled in the Study of Women Across the Nation (SWAN) Circulation. 2005;111:1242–9. [CrossRef]
- Phillips GB, Jing TY, Laragh JH. Serum sex hormone levels in postmenopausal women with hypertension. J Hum Hypertens. 1997;11:523–6. [CrossRef]
- Prendergast HM, Kotini-Shah P, Pobee R, Richardson M, Ardati A, Darbar D, Khosla S. Association of Angiotensin Converting Enzyme Phenotypes and Polymorphisms with Clinical Outcomes in SARS-CoV2 Patients with Hypertension in an Urban Emergency Department. Current Hypertension Reviews. 2024 Oct 15. s.
- Pinna G, Uzunova V, Matsumoto K, Puia G, Mienville JM, Costa E, Guidotti A. Brain allopregnanolone regulates the potency of the GABA(A) receptor agonist muscimol. Neuropharmacology. 2000 Jan 28;39(3):440-8. PMID: 10698010 . [CrossRef]
- Osborne LM, Etyemez S, Pinna G, Alemani R, Standeven LR, Wang XQ, Payne JL. Neuroactive steroid biosynthesis during pregnancy predicts future postpartum depression: a role for the 3α and/or 3β-HSD neurosteroidogenic enzymes? Neuropsychopharmacology. 2025 May;50(6):904-912. Epub 2025 Jan 30. Erratum in: Neuropsychopharmacology. 2025 May;50(6):1021. doi: 10.1038/s41386-025-02109-z. PMID: 39885361; PMCID: PMC12032070 . [CrossRef]
- Wagner AK, McCullough EH, Niyonkuru C, et al. Acute serum hormone levels: characterization and prognosis after severe traumatic brain injury. J Neurotrauma 2011;28:871–88.
- Wagner, J., Dusick, J. R., McArthur, D. L., Cohan, P., Wang, C., Swerdloff, R., Boscardin, W. J., and Kelly, D. F. (2010). Acute gonadotroph and somatotroph hormonal suppression after traumatic brain injury. J Neurotrauma 27, 1007–1019.
- Dossett, L.A., Swenson, B.R., Evans, H.L., Bonatti, H., and Sawyer, R.G. (2008a). Serum estradiol concentration as a predictor of death in critically ill and injured adults. Surg. Infect. 9, 41–48.
- Dossett, L.A., Swenson, B.R., Heffernan, D., Bonatti, H., Metzger, R., Sawyer, R.G., and May, A.K. (2008b). High levels of endogenous estrogens are associated with death in the critically injured adult. J. Trauma 64, 580–585.
- Christeff N, Benassayag C, Carli-Vielle C, Carli A, Nunez EA. Elevated oestrogen and reduced testosterone levels in the serum of male septic shock patients. Journal of steroid biochemistry. Apr 1988;29(4):435-40. [CrossRef]
- Gee A, Sawai R, Differding J, Muller P, Underwood S, Schreiber M. The influence of sex hormone on coagulation and inflammation in the trauma patients. Shock (Augusta, Ga). 03/01 2008;29:334-41. [CrossRef]
- Di Stasi, V., Rastrelli, G., Inglese, F. et al. Higher testosterone is associated with increased inflammatory markers in women with SARS-CoV-2 pneumonia: preliminary results from an observational study. J Endocrinol Invest 45, 639–648 (2022). [CrossRef]
- Van den Berghe, G., Weekers, F., Baxter, R.C., Wouters, P., Iranmanesh, A.., Bouillon, R., and Veldhuis, J.D. (2001). Fiveday pulsatile gonadotropin-releasing hormone administration unveils combined hypothalamic–pituitary–gonadal defects underlying profound hypoandrogenism in men with prolongedcritical illness. J. Clin. Endocrinol. Metab. 86, 3217–3226.
- Kalantaridou, S.N., Makrigiannakis, A., Zoumakis, E., and Chrousos, G.P. (2004). Stress and the female reproductive system. J. Reprod. Immunol. 62, 61–68.
- Mastorakos, G., and Pavlatou, M. (2005). Exercise as a stress model and the interplay between the hypothalamus–pituitary–adrenal and the hypothalamus–pituitary–thyroid axes. Horm. Metab. Res. 37, 577–584.
- Locci A, Pinna G. Neurosteroid biosynthesis down-regulation and changes in GABAA receptor subunit composition: a biomarker axis in stress-induced cognitive and emotional impairment. Br J Pharmacol. 2017 Oct;174(19):3226-3241. Epub 2017 Jun 14. PMID: 28456011; PMCID: PMC5595768 . [CrossRef]
- Dichtel LE, Lawson EA, Schorr M, Meenaghan E, Paskal ML, Eddy KT, Pinna G, Nelson M, Rasmusson AM, Klibanski A, Miller KK. Neuroactive Steroids and Affective Symptoms in Women Across the Weight Spectrum. Neuropsychopharmacology. 2018 May;43(6):1436-1444. Epub 2017 Nov 1. PMID: 29090684; PMCID: PMC5916351 . [CrossRef]
- Rasmusson AM, King MW, Valovski I, Gregor K, Scioli-Salter E, Pineles SL, Hamouda M, Nillni YI, Anderson GM, Pinna G. Relationships between cerebrospinal fluid GABAergic neurosteroid levels and symptom severity in men with PTSD. Psychoneuroendocrinology. 2019 Apr;102:95-104. Epub 2018 Nov 22. PMID: 30529908; PMCID: PMC6584957 . [CrossRef]
- Pinna G. Allopregnanolone (1938-2019): A trajectory of 80 years of outstanding scientific achievements. Neurobiol Stress. 2020 Aug 5;13:100246. PMID: 32875009; PMCID: PMC7451447 . [CrossRef]
- Balan I, Beattie MC, O’Buckley TK, Aurelian L, Morrow AL. Endogenous Neurosteroid (3α,5α)3-Hydroxypregnan-20-one Inhibits Toll-like-4 Receptor Activation and Pro-inflammatory Signaling in Macrophages and Brain. Sci Rep. 2019 Feb 4;9(1):1220. PMID: 30718548; PMCID: PMC6362084 . [CrossRef]
Figure 1.
Distribution of hormones by sex (overall) and by sex and clinical outcomes. Median serum concentrations (pg/mL) of progesterone (P4), allopregnanolone (Allo), pregnanolone (PA), epipregnanolone (Epi), isoallopregnanolone (Iso), estradiol (E2), 3α-androstanediol (3α-diol), 3β-androstanediol (3β-diol), and testosterone (T) are shown across five subpanels: Top left: Median – by Sex: Progesterone levels were significantly higher in postmenopausal females than in males (p=0.03), while testosterone (p=0.01) and allopregnanolone (p=0.069) were lower in females. No significant sex differences were observed for the other hormones. Top right: Median – by Hypoxia and Sex: Among males, hypoxia was associated with significantly lower serum allopregnanolone concentrations (p=0.046). In females, hypoxia was associated with significantly lower estradiol levels (p=0.0147). Middle left: Median – by ICU Admission and Sex: In males, ICU admission was associated with marginally higher serum 3α-diol levels (p=0.06). ICU patients of both sexes had generally lower progesterone, estradiol, and testosterone levels compared to non-ICU patients, except ICU females, who exhibited relatively higher testosterone than non-ICU females. Middle right: Median – by Hospitalization and Sex: Hospitalized males had lower testosterone (p=0.016) and higher 3α-diol (p=0.049) levels than non-hospitalized males. Hospitalized females had the highest median progesterone levels compared to hospitalized males. Estradiol levels were higher in hospitalized males but lower in hospitalized females compared to their respective non-hospitalized counterparts. Bottom center: Median – by Length of Stay and Sex: In males, serum isoallopregnanolone levels were significantly higher in those with a longer length of stay (>7 days; p=0.018). These findings illustrate a sex-dimorphic and outcome-specific profile of circulating sex steroid concentrations in COVID-19 patients with hypertension, indicating possible prognostic and mechanistic relevance. Statistical comparisons were performed using the Mann-Whitney U test. Analyses were conducted in SAS 9.4, with significance set at p < 0.05.
Figure 1.
Distribution of hormones by sex (overall) and by sex and clinical outcomes. Median serum concentrations (pg/mL) of progesterone (P4), allopregnanolone (Allo), pregnanolone (PA), epipregnanolone (Epi), isoallopregnanolone (Iso), estradiol (E2), 3α-androstanediol (3α-diol), 3β-androstanediol (3β-diol), and testosterone (T) are shown across five subpanels: Top left: Median – by Sex: Progesterone levels were significantly higher in postmenopausal females than in males (p=0.03), while testosterone (p=0.01) and allopregnanolone (p=0.069) were lower in females. No significant sex differences were observed for the other hormones. Top right: Median – by Hypoxia and Sex: Among males, hypoxia was associated with significantly lower serum allopregnanolone concentrations (p=0.046). In females, hypoxia was associated with significantly lower estradiol levels (p=0.0147). Middle left: Median – by ICU Admission and Sex: In males, ICU admission was associated with marginally higher serum 3α-diol levels (p=0.06). ICU patients of both sexes had generally lower progesterone, estradiol, and testosterone levels compared to non-ICU patients, except ICU females, who exhibited relatively higher testosterone than non-ICU females. Middle right: Median – by Hospitalization and Sex: Hospitalized males had lower testosterone (p=0.016) and higher 3α-diol (p=0.049) levels than non-hospitalized males. Hospitalized females had the highest median progesterone levels compared to hospitalized males. Estradiol levels were higher in hospitalized males but lower in hospitalized females compared to their respective non-hospitalized counterparts. Bottom center: Median – by Length of Stay and Sex: In males, serum isoallopregnanolone levels were significantly higher in those with a longer length of stay (>7 days; p=0.018). These findings illustrate a sex-dimorphic and outcome-specific profile of circulating sex steroid concentrations in COVID-19 patients with hypertension, indicating possible prognostic and mechanistic relevance. Statistical comparisons were performed using the Mann-Whitney U test. Analyses were conducted in SAS 9.4, with significance set at p < 0.05.
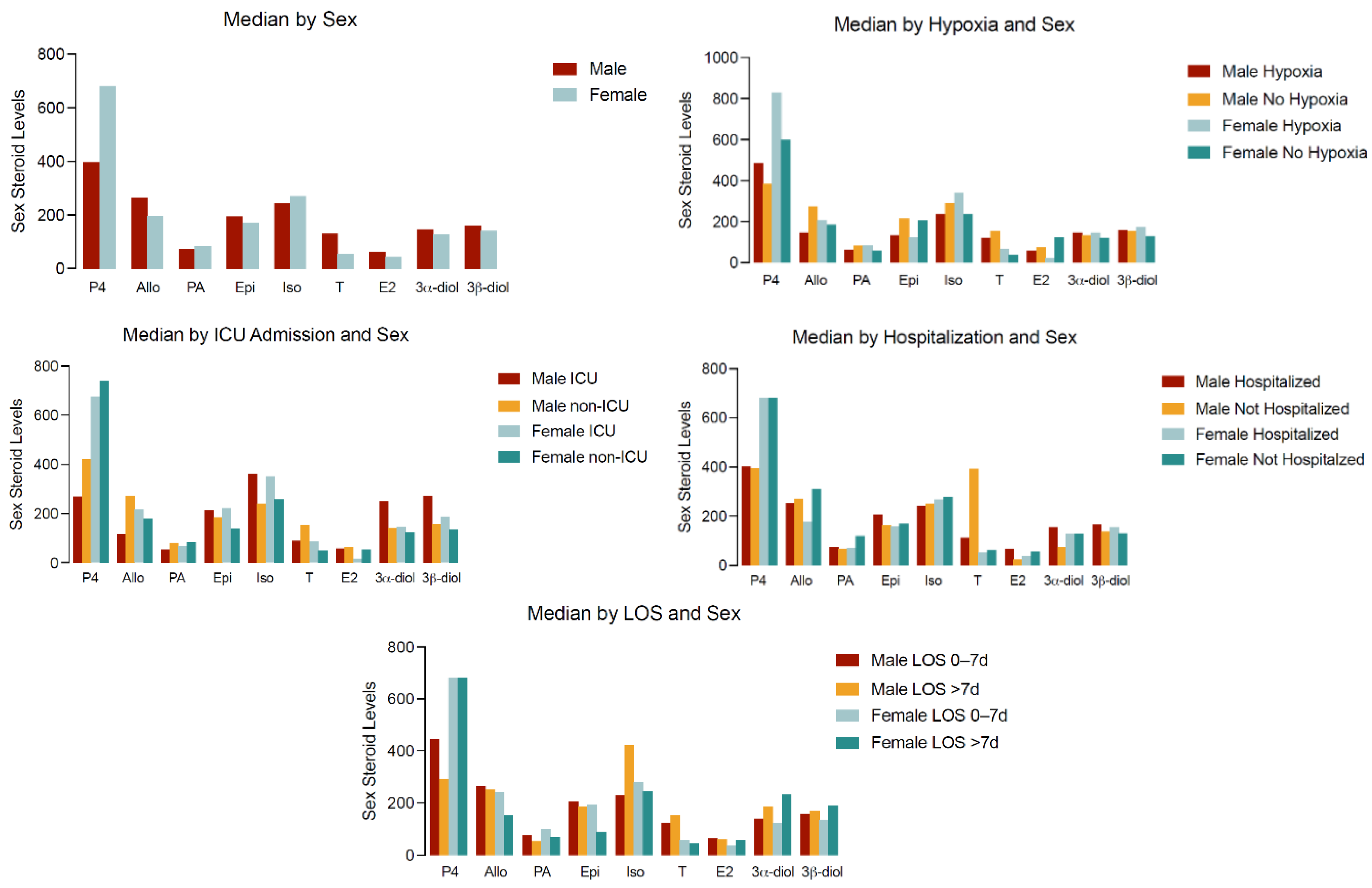
Figure 2.
Distribution of sex steroid hormone concentrations by sex and symptom profile in hypertensive COVID-19 patients. Median serum concentrations (pg/mL) of the same nine sex steroids are presented across five panels, stratified by symptom presence and sex: Top left – Median by Fatigue and Sex: No significant differences in hormone levels were found by fatigue status. Top right – Median by Chest Pain and Sex: In males, epipregnanolone levels were significantly lower in those with chest pain (p=0.019); no significant differences in females. Middle left – Median by Shortness of Breath and Sex: No statistically significant associations observed. Middle right – Median by Loss of Taste/Smell and Sex: In males, 3α-diol levels were higher in those reporting loss of smell/taste (p=0.06); in females, epipregnanolone levels were lower in symptomatic individuals (p=0.057). Bottom center – Median by Fever and Sex: Males with fever showed marginally higher progesterone (p=0.05); in females, testosterone levels were marginally higher in febrile patients (p=0.053). Statistical comparisons were performed using the Mann-Whitney U test. Analyses were conducted in SAS 9.4, with significance defined as p < 0.05.
Figure 2.
Distribution of sex steroid hormone concentrations by sex and symptom profile in hypertensive COVID-19 patients. Median serum concentrations (pg/mL) of the same nine sex steroids are presented across five panels, stratified by symptom presence and sex: Top left – Median by Fatigue and Sex: No significant differences in hormone levels were found by fatigue status. Top right – Median by Chest Pain and Sex: In males, epipregnanolone levels were significantly lower in those with chest pain (p=0.019); no significant differences in females. Middle left – Median by Shortness of Breath and Sex: No statistically significant associations observed. Middle right – Median by Loss of Taste/Smell and Sex: In males, 3α-diol levels were higher in those reporting loss of smell/taste (p=0.06); in females, epipregnanolone levels were lower in symptomatic individuals (p=0.057). Bottom center – Median by Fever and Sex: Males with fever showed marginally higher progesterone (p=0.05); in females, testosterone levels were marginally higher in febrile patients (p=0.053). Statistical comparisons were performed using the Mann-Whitney U test. Analyses were conducted in SAS 9.4, with significance defined as p < 0.05.
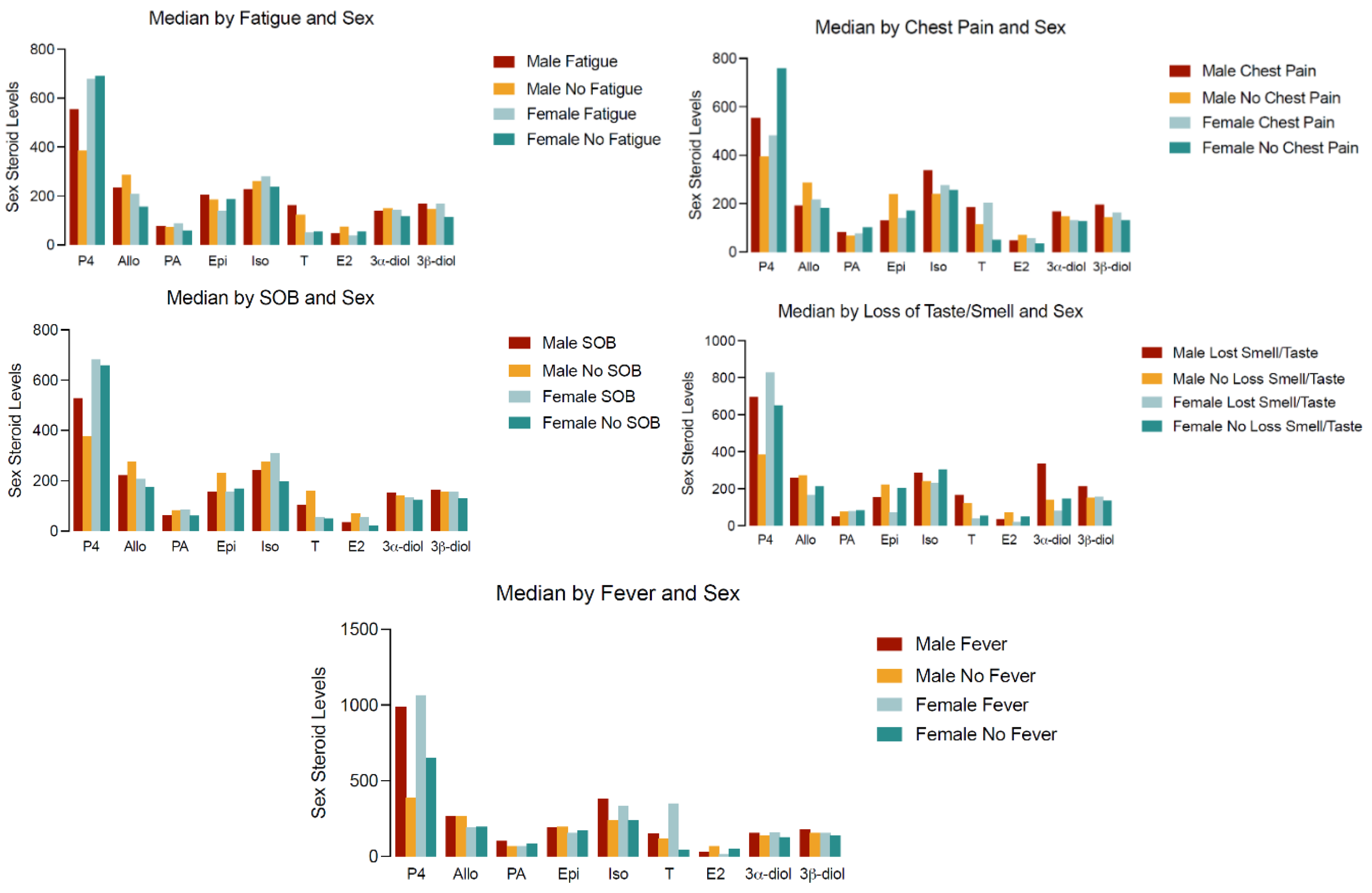

Table 1.
Demographic characteristics and clinical outcomes in subjects with hypertension that were treated or admitted through an urban academic emergency department after contracting Covid-19 (n=116).
Table 1.
Demographic characteristics and clinical outcomes in subjects with hypertension that were treated or admitted through an urban academic emergency department after contracting Covid-19 (n=116).
| Variables | Categories | Overall 123456789N=116 | Female123456789N=53 | Male123456789N=63 |
|---|---|---|---|---|
| Age; Mean (SD) | 62.1 (13.1) | 64.3 (10.1) | 60.3 (15.0) | |
| Age group | >=65 | 55 (47.4%) | 28 (52.8%) | 27 (42.9%) |
| <65 | 61 (52.6%) | 25 (47.2%) | 36 (57.1%) | |
| Sex | Male | 63 (54.3%) | - | 63 (100%) |
| Female | 53 (45.7%) | 53 (100%) | - | |
| Race | NH-Black | 64 (55.2%) | 32 (60.4%) | 32 (50.8%) |
| Hispanic/Latino | 40 (34.5%) | 17 (32.1%) | 23 (36.5%) | |
| NH-White | 6 (5.2%) | |||
| Other* | 6 (5.2%) | |||
| Fever** | Yes | 22 (19.0%) | 9 (17.0%) | 13 (20.6%) |
| No | 94 (81.0%) | 44 (83.0%) | 50 (79.4%) | |
| Shortness of Breath | Yes | 64 (55.2%) | 32 (60.4%) | 32 (50.8%) |
| No | 52 (44.8%) | 21 (39.6%) | 31 (49.2%) | |
| Chest Pain/tightness | Yes | 46 (39.7%) | 20 (37.7%) | 26 (41.3%) |
| No | 70 (60.3%) | 33 (62.3%) | 37 (58.7%) | |
| Loss of smell/taste | Yes | 35 (30.2%) | 18 (34.0%) | 17 (27.0%) |
| No | 81 (69.8%) | 35 (66.0%) | 46 (73.0%) | |
| Fatigue | Yes | 62 (53.4%) | 31 (58.5%) | 31 (49.2%) |
| No | 54 (46.6%) | 22 (41.5%) | 32 (50.8%) | |
| Hospitalized | Yes | 97 (83.6%) | 44 (83.0%) | 53 (84.1%) |
| No | 19 (16.4%) | 9 (17.0%) | 10 (15.9%) | |
| ICU admit | Yes | 18 (15.5%) | 8 (15.1%) | 10 (15.9%) |
| No | 98 (84.5%) | 45 (84.9%) | 53 (84.1%) | |
| Length of Stay | >7 days | 33 (28.4%) | 16 (30.2%) | 17 (27.0%) |
| 0-7 days | 83 (71.6%) | 37 (69.8%) | 46 (73.0%) | |
| Ventilator support | Yes | 4 (3.5%) | ||
| No | 111 (96.5%) | |||
| Hypoxia | Yes | 48 (41.7%) | 26 (49.1%) | 22 (35.5%) |
| No | 67 (58.3%) | 27 (50.9%) | 40 (64.5%) | |
| Vasopressor use | Yes | 6 (5.2%) | ||
| No | 110 (94.8%) |
* includes unknown/missing. ** Fever defined as measured fever above 100.4 degrees F. Greyed boxes are for variables that had very small sample when stratified by sex.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



