
Submitted:
20 July 2025
Posted:
21 July 2025
You are already at the latest version
Abstract
Background: Laron Syndrome (LS) is a rare hereditary disease of dwarfism occurring with few exceptions in Jewish, Muslim and Asian populations or their descendants spread over all continents. It is caused by deletions or mutations in the GH-Receptor gene resulting in high serum levels of a structurally and biologically normal, but inactive GH and low to undetectable IGF-I. Aim: To summarize the disabilities and handicaps observed in patients with LS, from infancy through adult age. Results: Diagnosing, treating and following a cohort of 76 patients with LS, many since infancy into adult age, enabled our department to study not only their growth and social achievements, but also the difficulties these patients encounter in life. The longstanding IGF-I deficiency caused somatic and biochemical changes which lead to disabilities starting already in infancy and becoming more severe with advancing age. The most serious handicaps LS patients have are dwarfism, progressive obesity, diabetes, fatty liver, cardiovascular disease, neurological and orthopedic problems, leading to difficulties in vocational training, occupation and social life, all lowering the Quality of Life (QoL) of these patients. Conclusion: Early initiation of IGF-I replacement treatment of patients with Laron Syndrome prevents and reverses part of the handicaps of the longstanding IGF-I deficiency.
Keywords:
Laron Syndrome
; GH insensitivity
; GH-Receptor
; IGF-I deficiency
; disabilities
; dwarfism
; obesity
; diabetes
; cardiovascular disease
1. Introduction
Laron Syndrome (LS – OMIM #262500, MedDRA #10082851, SCID #38196001, ICD-10 E34.3, GARD 6859, UMLS C0271568, MeSH D046150, Orpha 633) or GH insensitivity is a rare disease of growth failure falling in the category of “Orphan Diseases”. It constitutes the best characterized entity of congenital IGF-I deficiency [1]. LS was first described in 1966 [2] and 1968 [3] in Yemenite Jews. Following these reports, more patients were diagnosed in children originating from the Mediterranean, Mid-Eastern, Asian or South and Central America [4,5]. Despite their resemblance with genetic isolated growth hormone (GH) deficiency [6], these patients had high serum GH and low to undetectable insulin-like growth factor I (IGF-I) which did not respond to exogenous GH administration [7,8] demonstrating GH insensitivity [9,10]. Analyzing liver membranes from two LS patients it was found that the resistance to GH is due to the inability of the GH molecule to bind to its receptor [11]. Chromatography and PCR methods revealed that the underlying pathology is caused by deletions or mutations in the GH-Receptor gene [12,13]. The great majority of the defects were found to be in the extracellular domain of the GH-Receptor gene [14]. The analysis of our cohort, all comprising consanguineous families, led to the conclusion that LS is genetically transmitted by a fully penetrant autosomal recessive mechanism [15]. It is noteworthy that only patients homozygous or double heterozygotes for the GH-R defects express the full characteristics of the syndrome. The resemblance of the bone X-rays of our patients with the skeleton of an 18,000 year old female dwarf on the Island of Flores led us to the hypothesis that the founder gene originated in Indonesia [16]. For over 50 years we have followed a large cohort of LS patients [17], many since early childhood into adult age. This enabled us to study not only the clinical and biochemical consequences of IGF-I deficiency and IGF-I replacement in LS patients but also their adjustment in the society at various age levels.
The aim of this report is to describe the disabilities and handicaps observed in our large cohort of patients with Laron Syndrome.
2. Subject and Methods
The data were extracted from the Medical Records of the Endocrinology and Diabetes Research Unit of the Schneider Children’s Medical Center. Sixty nine patients and their families lived in Israel and 7 were referred from other countries.
Only patients with a proven and documented diagnosis of Laron Syndrome, i.e. high serum GH, low serum IGF-I and lack of response upon GH administration with or without genetic analysis were included in the study.
The study was approved by the Rabin Medical Center Ethics Committee (RMC: 619-22).
3. Results
Following are the main disabilities and handicaps observed in LS patients studied by us.
3.1. Growth and Development
Dwarfism was present already at birth (42-46 cm) and progressed until closure of the long bone epiphysis leading to an adult height of 116-142 cm in males and 108-136 cm in females [18] (Figure 1). The upper/lower body ratio revealed short lower limbs compared to the trunk. The head circumference (i.e. brain volume) is below normal [19], and there is underdevelopment of the facial bones [20,21] which leads to a protruding forehead, saddle nose, sunset look and sparse hair resulting already since infancy in a characteristic abnormal facies [3,6] (Figure 2). The hands and feet are small (acromicria) [22,23], which results in difficulties in finding appropriate clothing. Some infants were obliged to wear doll shoes [24] not finding small sized shoes. These unusual features together with the dwarfism draw attention, causing stress to parents and antagonism in surrounding people. Due to the abnormal structure of the cranium LS patients have a retarded growth of the ocular globe [25,26] causing myopia and need for spectacles. The retinal vascularization is reduced [27] and with advancing age, a minority develop glaucoma. Some are born with strabismus or cataracts; all these impair vision. LS patients also develop a neurosensory hearing defect [28]. Teeth development, size, morphology and composition are defective [29] and need orthodontic treatment. Due to immaturity of the carbohydrate system, infants and young children suffer from hypoglycemia and seizures [30]. This feature is reversed with the increase in the degree of the adipose tissue during puberty.
3.2. School Age
To adjust to the dwarfism low benches and tables are needed. Deficiencies in protein metabolism such as abnormal amino acid pattern [31] and low procollagen levels [32] lead to underdevelopment of the muscular system and weakness [33,34] which impedes mobility, participation in competitive sport activities and to carry heavy school bags. Children with LS also find it difficult to manage the steps getting on and off regular school buses. Due to their abnormal appearance, obesity and size, LS children are often bullied by their classmates.
3.3. Sexual Development and Puberty
3.4. Adult Life
The progressive obesity [39] (Figure 3), not depending on food intake [40] impedes a normal life routine and causes clinical and biochemical complications, such as insulin resistance, glucose intolerance, diabetes, hyperlipidemia, fatty liver and cardiovascular disease, all the characteristics of the “Metabolic Syndrome” [41].
3.5. Limitation in Mobility
Two of our patients and 25% of the Ecuadorian patients have congenital dislocation of the hip or Perthes Disease [42]. If not treated, together with the weakness of the muscular system and marked obesity causes serious walking impairment. A reduced left heart output and reduced lung function also impair exercise capacity [43].
3.6. Neurological Abnormalities
Using X-rays, CT and MRI examinations of the skull and brain, we found a series of structural pathologies in the central nervous system (CNS) leading to neurologic deficits [44]. Among these are underdeveloped sinuses, degenerative changes of the white matter with occasional cerebellar atrophy and progressive development of spinal stenosis [45]. An unusual brain lesion was found in one of our patients [46]. A similar lesion was reported in a LS patient from Mexico [47]. Both were adult female patients who died suddenly. Few patients had focal epilepsy [48] and due to the reduced dimensions of the larynx and obesity LS patients suffer from sleep apnea [49,50].
3.7. Psycho-Social Aspects
Psychological studies of LS children and adults revealed that part of the children present a low score on the Wechsler and Bender tests [51,52]. The low stature and academic limitations in some patients caused difficulties in vocational training and finding occupations [17]. A minority achieved academic degrees, one even a PhD degree. Part of the patients with a healthy partner are married and have children. Others have difficulties in finding partners.
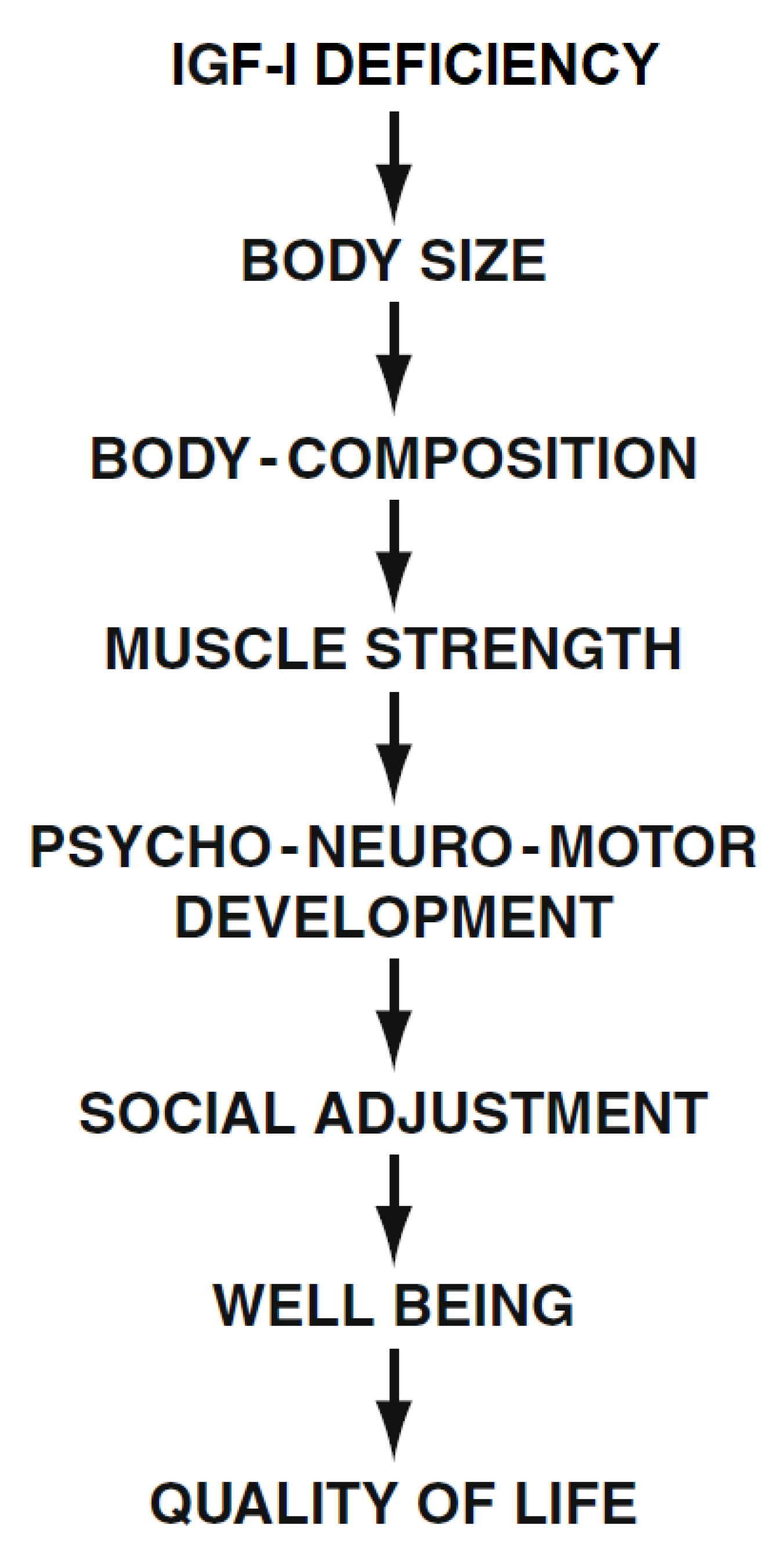
The many handicaps, social limitations and difficulties at any age are reflected in the emotional states, disappointment and even depression in most of the LS patients. Raising a child with Laron Syndrome, and being a patient with many limitations causes great psychological problems in the family and in the patient him(her)self with a negative impact on the Quality of Life [53] (Figure 4). The fact that patients with LS are protected from developing malignancies [54,55] was not found to affect their QoL.
3.8. Treatment
The only treatment of LS is replacement of the genetic deficiency of IGF-I. IGF-I is a peptide which needs to be injected daily, preferably once a day [56,57]. Administering it twice or in greater doses causes unnecessary and unpleasant adverse effects [58]. IGF-I treatment accelerates linear growth [50,56,60] and growth of the head circumference (i.e. brain size) [19]. Even when the treatment is continuous, most children do not reach normal height. Whereas short-term treatment reduces adiposity, long-term administration of IGF-I stimulates development of obesity [61]. As IGF-I treatment is at present approved only for children, to stimulate growth, the handicaps of the late complications are not prevented. In a short clinical trial of IGF-I treatment of adult patients with LS we found beneficial effects of IGF-I such as lowering of blood insulin, cholesterol [62] and serum Lp(a) [63], and improved left heart ventricular function [64].
4. Discussion
Laron Syndrome is a rare disease but a unique model for understanding the role of IGF-I in the process of growth and body composition [1,65]. After its discovery in 1966 [2], more and more patients were referred to our clinic and reports from other countries were published in the scientific literature. Long-term follow up was reported only by two clinics with many patients (i.e. that in Ecuador [66] and Israel [17]). As our patients lived in a small country with easy access to a multidisciplinary medical team and provision of complete insurance for all medical expenses, we had a better opportunity to follow our patients than the Ecuadorian colleagues, whose patients are dispersed in locations far from the clinic and some of their examinations had to be performed in the USA. Comparing the findings between the two cohorts, it is evident that the patients in Ecuador had all the complications, disabilities and handicaps found in our LS patients [67,68], including morphological changes in the brain structure [69]. It is noteworthy that the patients in Ecuador showed a high incidence of cardiac disease (27%), even stroke, alcoholism and a high incidence of accidences (20%) [67]. It thus seems that independent of the local conditions, the disease lead to a reduced QoL.
Future Perspectives
All of the disabilities and handicaps of patients with LS are inherent to the genetic IGF-I deficiency. Height can be improved by early initiation of IGF-I replacement treatment. Even if normal height cannot be achieved, social adjustment is improved. The recently introduced weight reduction treatments using GLP-1 receptor agonists or gastric sleeve operation started in few of our patients, reduce the obesity and reverses part of its biochemical complications. The marked loss of weight also had positive psychological effects. Unfortunately, both treatments by IGF-I and GLP-1-R antagonist are available to only a small number of LS patients due to regulatory and economic causes in some countries. Same is true for pregestational diagnosis and implantation of only healthy embryos in an attempt to prevent new patients with LS in families at risk. Gene therapy may be also a future treatment possibility [70].
5. Conclusions
Patients with Laron Syndrome due to defects in the GH-R gene and resulting lifelong IGF-I deficiency suffer from many disabilities starting in infancy, comprising biochemical and clinical changes in all body systems. These abnormalities cause many physical handicaps and psycho-social problems, only partially alleviated by IGF-I replacement treatment.
References
- Laron, Z.; Werner, H. Laron syndrome - A historical perspective. Rev Endocr Metab Disord. 2021, 22, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Mannheimer, S. Measurement of human growth hormone. Description of the method and its clinical applications. Isr J Med Sci. 1966, 2, 115–119. [Google Scholar] [PubMed]
- Laron, Z.; Pertzelan, A.; Karp, M. Pituitary dwarfism with high serum levels of growth hormone. Isr J Med Sci. 1968, 4, 883–894. [Google Scholar] [PubMed]
- Rosenbloom, A.L.; Guevara-Aguirre, J.; Rosenfeld, R.G.; Fielder, P.J. The little women of Loja: growth hormone receptor-deficiency in an inbred population of southern Ecuador. N Engl J Med. 1990, 323, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.G.; Rosenbloom, A.L.; Guevara-Aguirre, J. Growth hormone (GH) insensitivity due to primary GH receptor deficiency. Endocr Rev. 1994, 15, 369–390. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. Deficiencies of growth hormone and somatomedins in man. Spec Top Endocrinol Metab. 1983, 5, 149–199. [Google Scholar] [PubMed]
- Daughaday, W.H.; Laron, Z.; Pertzelan, A.; Heins, J.N. Defective sulfation factor generation: a possible etiological link in dwarfism. Trans Assoc Am Physicians. 1969, 82, 129–138. [Google Scholar] [PubMed]
- Laron, Z.; Pertzelan, A.; Karp, M.; Kowadlo-Silbergeld, A.; Daughaday, W.H. Administration of growth hormone to patients with familial dwarfism with high plasma immunoreactive growth hormone. Measurement of sulfation factor, metabolic, and linear growth responses. J Clin Endocrinol Metab. 1971, 33, 332–342. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Kowadlo-Silbergeld, A.; Eshet, R.; Pertzelan, A. Growth hormone resistance. Ann Clin Res. 1980, 12, 269–277. [Google Scholar] [PubMed]
- Laron, Z. Laron syndrome (primary growth hormone resistance or insensitivity): the personal experience 1958-2003. J Clin Endocrinol Metab. 2004, 89, 1031–1044. [Google Scholar] [CrossRef] [PubMed]
- Eshet, R.; Laron, Z.; Pertzelan, A.; Dintzman, M. Defect of human growth hormone in the liver of two patients with Laron type dwarfism. Isr J Med Sci. 1984, 20, 8–11. [Google Scholar] [PubMed]
- Godowski, P.J.; Leung, D.W.; Meacham, L.R.; Galgani, J.P.; Hellmiss, R.; Keret, R.; Rotwein, P.S.; Parks, J.S.; Laron, Z.; Wood, W.I. Characterization of the human growth hormone receptor gene and demonstration of a partial gene deletion in two patients with Laron type dwarfism. Proc Natl Acad Sci USA. 1989, 86, 8083–8087. [Google Scholar] [CrossRef] [PubMed]
- Amselem S, Duquesnoy P, Attree O, Novelli G, Bousnina S, Postel-Vinay MC, Goosens M. Laron dwarfism and mutations of the growth hormonereceptor gene. N Engl J Med. 1989, 321, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Shevah, O.; Laron, Z. Genetic Aspects. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 29–52. [Google Scholar]
- Adam, A.; Josefsberg, Z.; Pertzelan, A.; Zadik, Z.; Chemke, J.M.; Laron, Z. Occurrence of four types of growth hormone related dwarfism in Israeli communities. Eur J Pediatr. 1981, 137, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Hershkovitz, I.; Kornreich, L.; Laron, Z. Comparative skeletal features between Homo floresiensis and patients with primary growth hormone insensitivity (Laron Syndrome). Am J Phys Anthropol. 2007, 134, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Kauli, R. Fifty seven years of follow-up of the Israeli cohort of Laron Syndrome patients-From discovery to treatment. Growth Horm IGF Res. 2016, 28, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Kauli, R. Linear growth pattern of untreated Laron syndrome patients. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 63–89. [Google Scholar]
- Laron, Z.; Iluz, M.; Kauli, R. Head circumference in untreated and IGF-I treated patients with Laron syndrome: comparison with untreated and hGH-treated children with isolated growth hormone deficiency. Growth Horm IGF Res. 2012, 22, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Scharf, A.; Laron, Z. Skull changes in pituitary dwarfism and the syndrome of familial dwarfism with high plasma immunoreactive growth hormone--a Roentgenologic study. Horm Metab Res. 1972, 4, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Konfino, R.; Pertzelan, A.; Laron, Z. Cephalometric measurements of familial dwarfism and high plasma immunoreactive growth hormone. Am J Orthod. 1975, 68, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Konen, O.; Silbergeld, A.; Lilos, P.; et al. Hand size and growth in untreated and IGF-I treated patients with Laron syndrome. J Pediatr Endocrinol Metab. 2009, 22, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Silbergeld, A.; Lilos, P.; Laron, Z. Foot length before and during insulin-like growth factor-I treatment of children with Laron syndrome compared to human growth hormone treatment of children with isolated growth hormone deficiency. J Pediatr Endocrinol Metab. 2007, 20, 1325–1328. [Google Scholar] [CrossRef] [PubMed]
- Shurka, E.; Laron, Z. Adjustment and rehabilitation problems of children and adolescents with growth retardation. I. Familial dwarfism with high plasma immunoreactive human growth hormone. Isr J Med Sci. 1975, 11, 352–357. [Google Scholar] [PubMed]
- Bourla, D.H.; Laron, Z.; Snir, M.; Lilos, P.; Weinberger, D.; Axer-Siegel, R. Insulinlike growth factor I affects ocular development: a study of untreated and treated patients with Laron syndrome. Ophthalmology. 2006, 113, 1197.e1–5. [Google Scholar] [CrossRef] [PubMed]
- Kornreich, L.; Konen, O.; Lilos, P.; Laron, Z. The globe and orbit in Laron syndrome. AJNR Am J Neuroradiol. 2011, 32, 1560–1562. [Google Scholar] [CrossRef] [PubMed]
- Hellström, A.; Carlsson, B.; Niklasson, A.; Segnestam, K.; Boguszewski, M.; de Lacerda, L.; Savage, M.; Svensson, E.; Smith, L.; Weinberger, D.; Albertsson Wikland, K.; Laron, Z. IGF-I is critical for normal vascularization of the human retina. J Clin Endocrinol Metab. 2002, 87, 3413–3416. [Google Scholar] [CrossRef] [PubMed]
- Attias, J.; Zarchi, O.; Nageris, B.I.; Laron, Z. Cochlear hearing loss in patients with Laron syndrome. Eur Arch Otorhinolaryngol. 2012, 269, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. The Teeth in Patients with Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 213–217. [Google Scholar]
- Laron, Z. Laron-type dwarfism (hereditary somatomedin deficiency): a review. Adv Int Med. 1984, 51, 117–150. [Google Scholar]
- Barazani, C.; Werner, H.; Laron, Z. Changes in plasma amino acids metabolites, caused by long-term IGF-I deficiency, are reversed by IGF-I treatment - A pilot study. Growth Horm IGF Res. 2020, 52, 101312. [Google Scholar] [CrossRef] [PubMed]
- Klinger, B.; Jensen, L.T.; Silbergeld, A.; Laron, Z. Insulin-like growth factor-I raises serum procollagen levels in children and adults with Laron syndrome. Clin Endocrinol (Oxf). 1996, 45, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Brat, O.; Ziv, I.; Klinger, B.; Avraham, M.; Laron, Z. Muscle force and endurance in untreated and human growth hormone or insulin-like growth factor-I-treated patients with growth hormone deficiency or Laron syndrome. Horm Res. 1997, 47, 45–48. [Google Scholar] [CrossRef] [PubMed]
- Epstein, Y.; Hadid, A.; Laron, Z.; Moran, D.S.; Vaisman, N. Muscle–Bone Relationship in Patients with Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 171–174. [Google Scholar]
- Laron, Z.; Klinger, B. Effect of insulin-like growth factor-I treatment on serum androgens and testicular and penile size in males with Laron syndrome (primary growth hormone resistance). Eur J Endocrinol. 1998, 138, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. Development and biological function of the female gonads and genitalia in IGF-I deficiency -- Laron syndrome as a model. Pediatr Endocrinol Rev. 2006, 3 Suppl 1, 188–191. [Google Scholar] [PubMed]
- Laron, Z.; Kauli, R. Sexual Development in Patients with Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 101–118. [Google Scholar]
- Laron, Z.; Sarel, R.; Pertzelan, A. Puberty in Laron type dwarfism. Eur J Pediatr. 1980, 134, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Klinger, B. Body fat in Laron syndrome patients: effect of insulin-like growth factor I treatment. Horm Res. 1993, 40, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, S.; Laron, Z.; Bed, M.A.; Vaisman, N. The obesity of patients with Laron Syndrome is not associated with excessive nutritional intake. Obes Res Clin Pract. 2009, 3, 1–52. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Kauli, R.; Silbergeld, A. Adult patients with Laron syndrome tend to develop the metabolic syndrome. Growth Horm IGF Res. 2024, 78, 101605. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Kauli, R. Orthopedic Problems in Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 323–324. [Google Scholar]
- Ben-Dov, I.; Gaides, M.; Scheinowitz, M.; Wagner, R.; Laron, Z. Reduced exercise capacity in untreated adults with primary growth hormone resistance (Laron syndrome). Clin Endocrinol (Oxf). 2003, 59, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Kornreich, L.; Horev, G.; Schwarz, M.; Karmazyn, B.; Laron, Z. Craniofacial and brain abnormalities in Laron syndrome (primary growth hormone insensitivity). Eur J Endocrinol. 2002, 146, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Kornreich, L.; Horev, G.; Schwarz, M.; Karmazyn, B.; Laron, Z. Laron syndrome abnormalities: spinal stenosis, os odontoideum, degenerative changes of the atlanto-odontoid joint, and small oropharynx. AJNR Am J Neuroradiol. 2002, 23, 625–631. [Google Scholar] [PubMed]
- Kornreich, L.; Laron, Z. An unusual brain lesion in a patient with Laron Syndrome. Endocrine. 2024, 84, 1266–1267. [Google Scholar] [CrossRef] [PubMed]
- Castilla-Cortazar, I.; Femat-Roldán, G.; Rodríguez-Rivera, J.; Aguirre, G.A.; García-Magariño, M.; Martín-Estal, I.; Espinosa, L.; Díaz-Olachea, C. Mexican case report of a never-treated Laron syndrome patient evolving to metabolic syndrome, type 2 diabetes, and stroke. Clin Case Rep. 2017, 5, 1852–1855. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, L.; Laron, Z.; Kornreich, L.; Scheuerman, O.; Goldberg-Stern, H.; Kraus, D. Focal Epilepsy in Individuals with Laron Syndrome. Horm Res Paediatr. 2022, 95, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Dagan, Y.; Abadi, J.; Lifschitz, A.; Laron, Z. Severe obstructive sleep apnoea syndrome in an adult patient with Laron syndrome. Growth Horm IGF Res. 2001, 11, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Kauli, R.; Rosenzweig, E. Sleep and Sleep Disorders in Patients with Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 317–320. [Google Scholar]
- Frankel, J.J.; Laron, Z. Psychological aspects of pituitary insufficiency in children and adolescents with special reference to growth hormone. Isr J Med Sci. 1968, 4, 953–961. [Google Scholar] [PubMed]
- Laron, Z. Psychological Aspects in Patients with Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 325–333. [Google Scholar]
- Laron, Z. Adjustment and Rehabilitation Problems of Children, Adolescents, and Adults with Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick , J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 335–337. [Google Scholar]
- Shevah, O.; Laron, Z. Patients with congenital deficiency of IGF-I seem protected from the development of malignancies: a preliminary report. Growth Horm IGF Res. 2007, 17, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Steuerman, R.; Shevah, O.; Laron, Z. Congenital IGF1 deficiency tends to confer protection against post-natal development of malignancies. Eur J Endocrinol. 2011, 164, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z.; Anin, S.; Klipper-Aurbach, Y.; et al. Effects of insulin-like growth factor on linear growth, head circumference, and body fat in patients with Laron-type dwarfism. Lancet. 1992, 339, 1259–1262. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. Emerging treatment options for patients with Laron syndrome. Expert Opinion on Orphan Drugs. 2014, 2, 681–694. [Google Scholar] [CrossRef]
- Laron, Z. Insulin-like growth factor-I treatment of children with Laron syndrome (primary growth hormone insensitivity). Pediatr Endocrinol Rev. 2008, 5, 766–771. [Google Scholar] [PubMed]
- Klinger, B.; Laron, Z. Three year IGF-I treatment of children with Laron syndrome. J Pediatr Endocrinol Metab. 1995, 8, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Laron, Z. IGF-I Treatment of Patients with Laron Syndrome. In Laron Syndrome - From Man to Mouse; Laron, Z., Kopchick, J., Eds.; Springer: Berlin, Heidelberg, 2011; pp. 343–380. [Google Scholar]
- Bisker-Kassif, O.; Kauli, R.; Lilos, P.; Laron, Z. Biphasic response of subscapular skinfold thickness to hGH or IGF-1 administration to patients with congenital IGHD, congenital MPHD and Laron syndrome. Obes Res Clin Pract. 2014, 8, e55–e62. [Google Scholar] [CrossRef] [PubMed]
- Klinger, B.; Anin, Z.; Flexer, Z.; Laron, Z. IGF-1 treatment of adult patients with Laron Syndrome. In: Laron Z, Parks J S (eds.) Lessons from Laron syndrome (LS) 1966-1992. 1993, 24, 237–243. [Google Scholar]
- Laron, Z.; Werner, H. Administration of insulin like growth factor I (IGFI) lowers serum lipoprotein(a)-impact on atherosclerotic cardiovascular disease. Growth Horm IGF Res. 2023, 71, 101548. [Google Scholar] [CrossRef] [PubMed]
- Scheinowitz, M.; Feinberg, M.S.; Laron, Z. IGF-I replacement therapy in children with congenital IGF-I deficiency (Laron syndrome) maintains heart dimension and function. Growth Horm IGF Res. 2009, 19, 280–282. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, A.L. A half-century of studies of growth hormone insensitivity/Laron syndrome: A historical perspective. Growth Horm IGF Res. 2016, 28, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, A.L.; Guevara-Aguirre, J.; Rosenfeld, R.G.; Francke, U. Growth hormone receptor deficiency in Ecuador. J Clin Endocrinol Metab. 1999, 84, 4436–4443. [Google Scholar] [CrossRef] [PubMed]
- Guevara-Aguirre, J.; Balasubramanian, P.; Guevara-Aguirre, M.; Wei, M.; Madia, F.; Cheng, C.W.; Hwang, D.; Martin-Montalvo, A.; Saavedra, J.; Ingles, S.; de Cabo, R.; Cohen, P.; Longo, V.D. Growth hormone receptor deficiency is associated with a major reduction in pro-aging signaling, cancer, and diabetes in humans. Sci Transl Med. 2011, 3, 70ra13. [Google Scholar] [CrossRef] [PubMed]
- Guevara-Aguirre, J.; Teran, E.; Lescano, D.; Guevara, A.; Guevara, C.; Longo, V.; Gavilanes, A.W.D. Growth hormone receptor deficiency in humans associates to obesity, increased body fat percentage, a healthy brain and a coordinated insulin sensitivity. Growth Horm IGF Res. 2020, 51, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Nashiro, K.; Guevara-Aguirre, J.; Braskie, M.N.; Hafzalla, G.W.; Velasco, R.; Balasubramanian, P.; Wei, M.; Thompson, P.M.; Mather, M.; Nelson, M.D.; Guevara, A.; Teran, E.; Longo, V.D. Brain Structure and Function Associated with Younger Adults in Growth Hormone Receptor-Deficient Humans. J Neurosci. 2017, 37, 1696–1707. [Google Scholar] [CrossRef] [PubMed]
- Werner, H. Toward gene therapy of Laron syndrome. Gene Ther. 2022, 29, 319–321. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Growth pattern of an untreated girl with Laron Syndrome. Drawn on the Laron Syndrome specific growth chart (Laron Z, et al. Arch Dis Child. 1993, 68: 768-70); Reproduced with permission from Laron Z, Kopchivk JJ. Laron Syndrome - from Man to Mouse. Heidelberg, Springer -Verlag 2011.
Figure 1.
Growth pattern of an untreated girl with Laron Syndrome. Drawn on the Laron Syndrome specific growth chart (Laron Z, et al. Arch Dis Child. 1993, 68: 768-70); Reproduced with permission from Laron Z, Kopchivk JJ. Laron Syndrome - from Man to Mouse. Heidelberg, Springer -Verlag 2011.
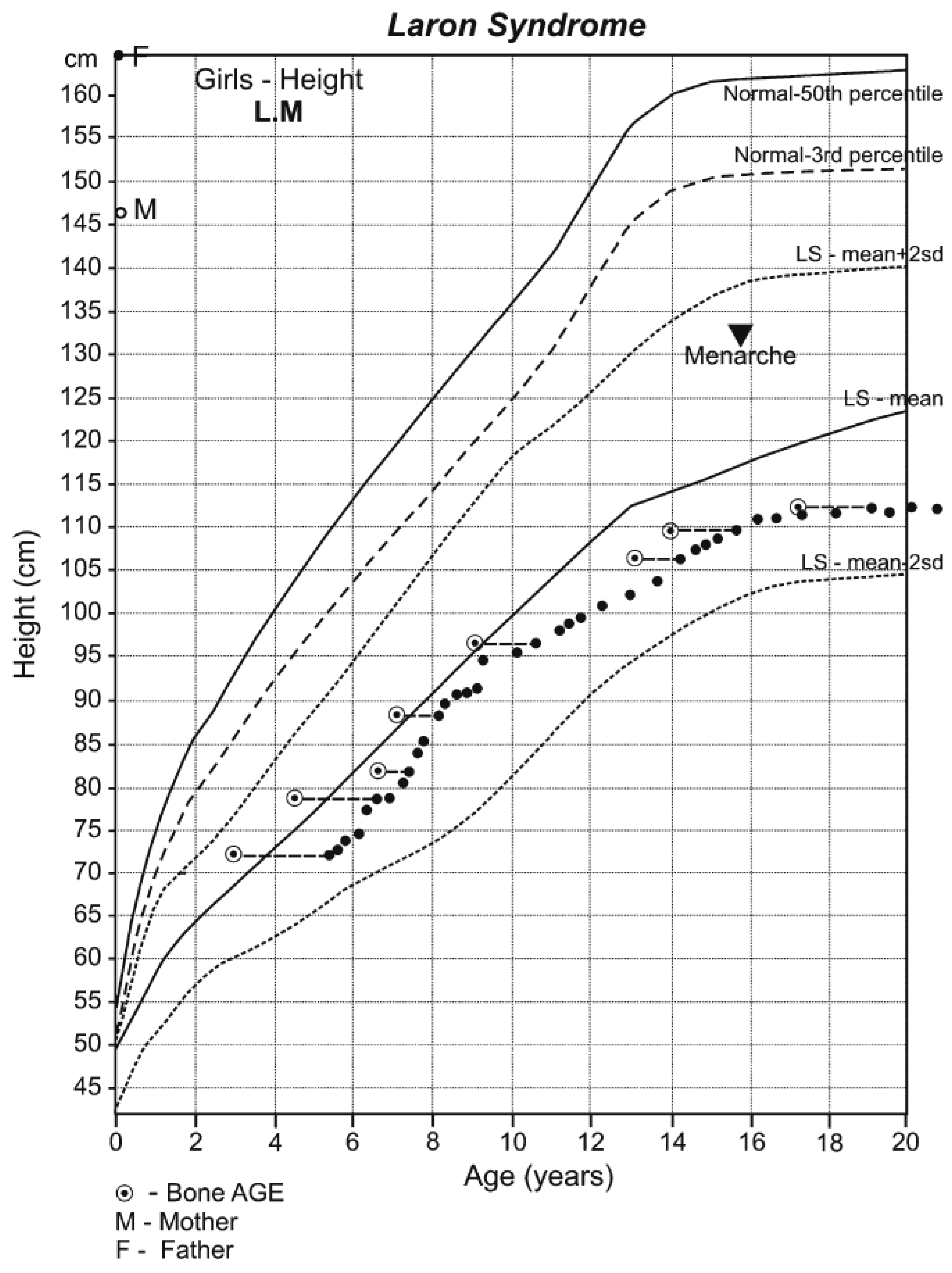
Figure 2.
Characteristic feature of a 1½ years old girl with Laron Syndrome. Note protruding forehead, saddle nose and sparse hair.
Figure 2.
Characteristic feature of a 1½ years old girl with Laron Syndrome. Note protruding forehead, saddle nose and sparse hair.
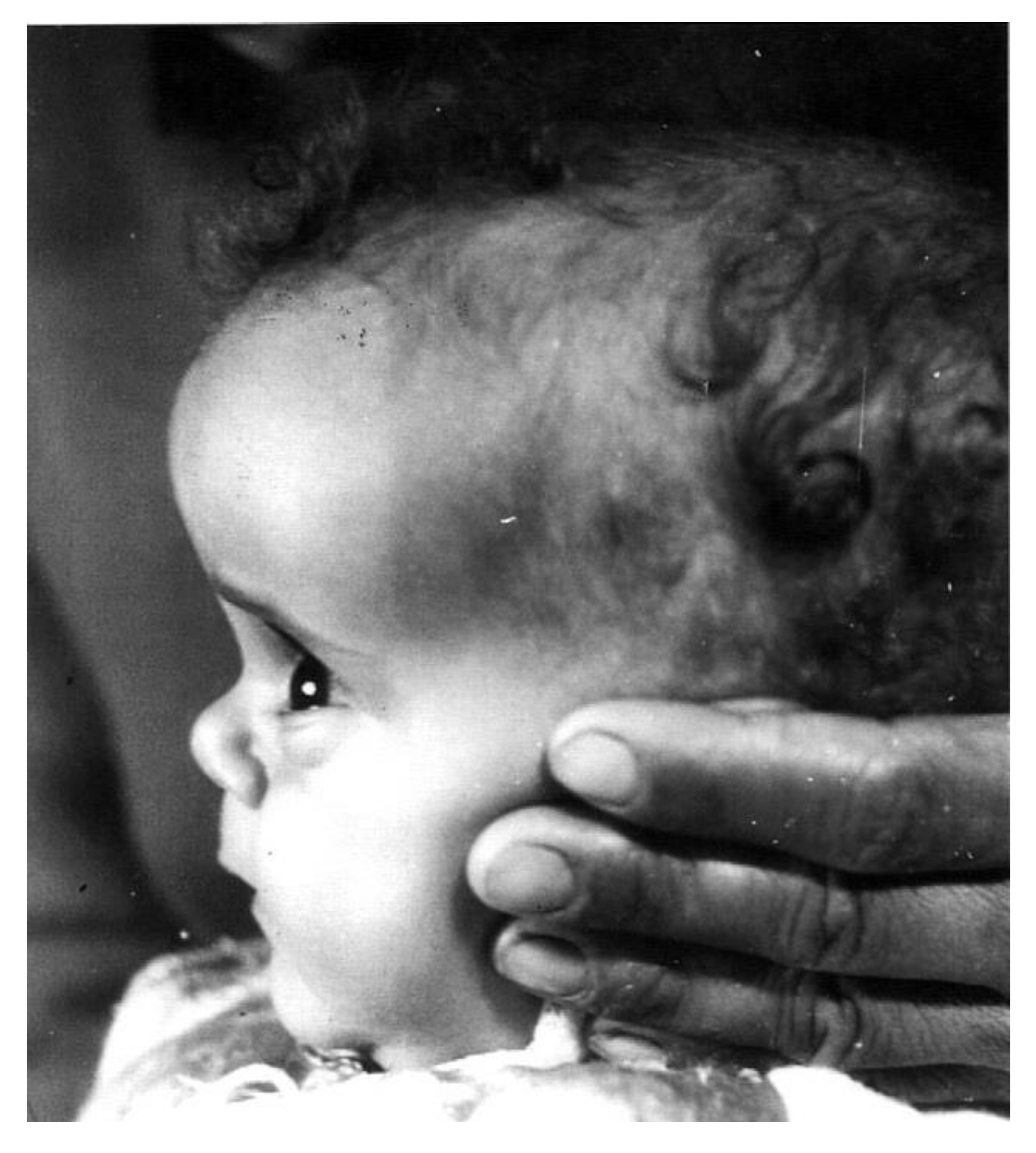
Figure 3.
Obesity in a 16 years old girl with Laron Syndrome. Reproduced with permission from Laron Z, Kopchivk JJ. Laron Syndrome - from Man to Mouse. Heidelberg, Springer -Verlag 2011.
Figure 3.
Obesity in a 16 years old girl with Laron Syndrome. Reproduced with permission from Laron Z, Kopchivk JJ. Laron Syndrome - from Man to Mouse. Heidelberg, Springer -Verlag 2011.
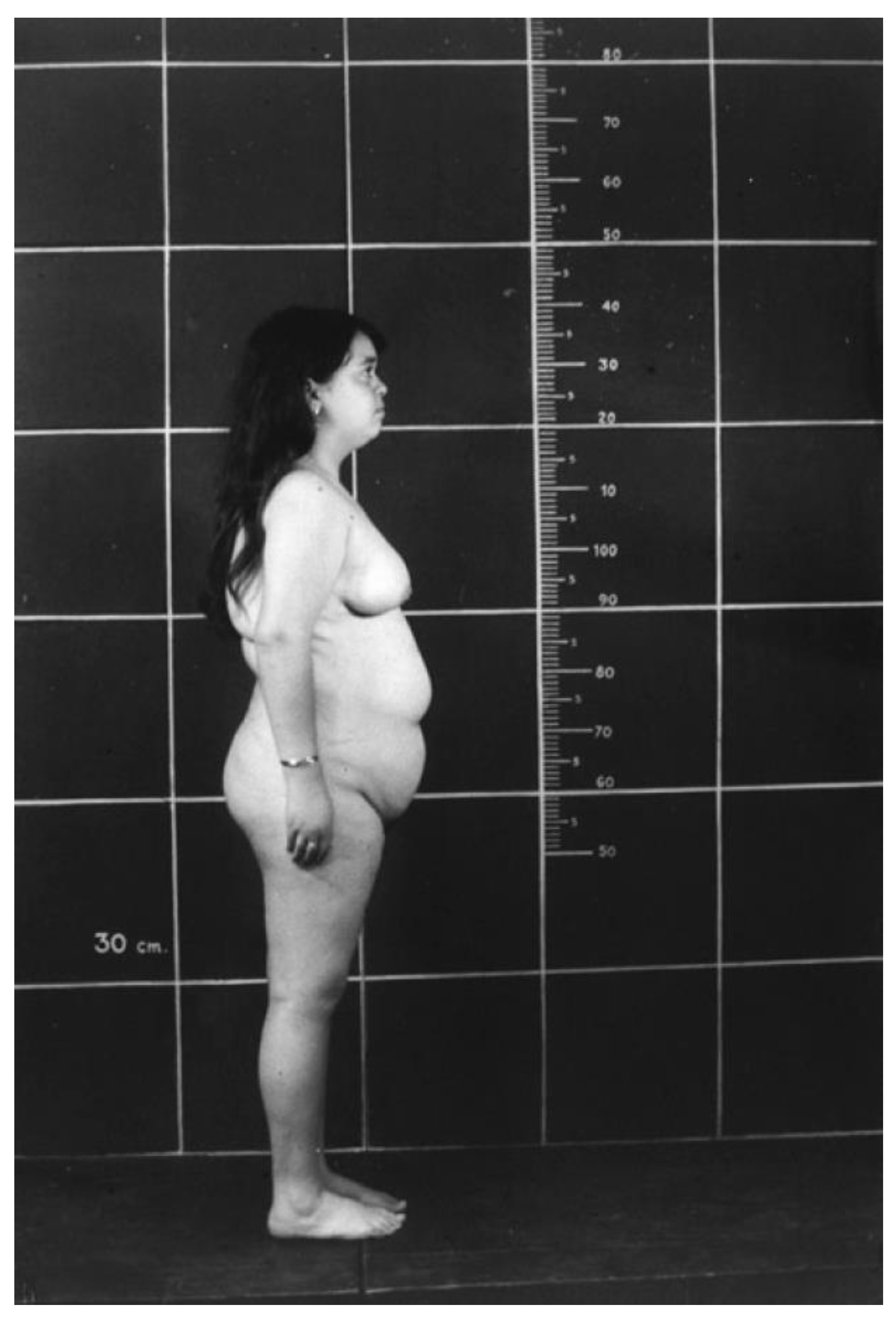
Figure 4.
Effect of long-term IGF-I deficiency on social adjustment and Quality of Life (QoL) in patients with Laron Syndrome. Reproduced with permission from Laron Z, Kopchivk JJ. Laron Syndrome - from Man to Mouse. Heidelberg, Springer -Verlag 2011.
Figure 4.
Effect of long-term IGF-I deficiency on social adjustment and Quality of Life (QoL) in patients with Laron Syndrome. Reproduced with permission from Laron Z, Kopchivk JJ. Laron Syndrome - from Man to Mouse. Heidelberg, Springer -Verlag 2011.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



