
Submitted:
08 July 2025
Posted:
08 July 2025
You are already at the latest version
Abstract
Introduction: Acute neuromuscular fatigue impairs athletic performance and increases the risk of musculoskeletal injury. Recovery strategies such as manual massage (MM) and intermittent pneumatic compression (IPC) have been proposed to mitigate these effects, although their efficacy remains controversial. Objective: To compare the MM and IPC effects on muscle damage recovery, lower limb strength, and power in Under-20 soccer athletes. Methods: A cross-sectional crossover studyn was conducted with twenty male youth athletes (n = 20) from the under-20 category (18.65 ± 0.67 years) of Paysandu Sport Club – Brazil, who underwent a fatigue protocol followed by either MM or IPC, with a seven-day washout between sessions. The following variables were assessed: serum creatine kinase (CK), quadriceps and hamstrings isometric voluntary contraction (IVC), and vertical jump (VJ). Results: CK decreased following the MM (pre: 382.50 ± 163.02 U/L; post: 305.40 ± 239.98 U/L; p=0.042) but not for IPC (pre: 337 ± 114.50 U/L; post: 199 ± 89.50 U/L); p=0.16). After the crossover, IPC elicited a significant reduction in CK (pre: 307 ± 198 U/L; post: 256 ± 84.75 U/L; p=0.028), whereas MM did not reach statistical significance (pre: 316.70 ± 116.66 U/L; post: 252.50 ± 91.77 U/L; p=0.094). Neither intervention (MM or IPC) resulted in significant improvements in Quadriceps or Hamstring (p>0.05) IVC or VJ height (p>0.05). Conclusion: MM and IPC are viable recovery tools to mitigate biochemical markers of muscle stress without compromising performance, a crucial consideration for high-performance environments where recovery windows are narrow.
Keywords:
muscle fatigue
; functional recovery
; creatine kinase
; physical performance
; football
1. Introduction
Acute neuromuscular fatigue is a common physiological response in high-demand intermittent sports such as soccer and can significantly impair athletic performance while increasing the risk of musculoskeletal injuries [1,2] This type of fatigue negatively affects muscle contractile capacity, strength, and motor coordination, and may persist for up to 72 hours post-exercise [3,4]. As a result, post-exercise recovery strategies have become increasingly adopted to mitigate the deleterious effects of repeated exertion and optimize the return to functional condition [5]
Among these strategies, manual massage (MM) and intermittent pneumatic compression (IPC) stand out and are widely used in athletic settings. MM is recognized for its analgesic effects, its ability to reduce muscle stiffness, and its enhancement of perceived recovery [6]. However, the evidence regarding its effects on muscular strength and power remains inconclusive[7,8,9]. In contrast, IPC has been employed to enhance venous and lymphatic return and to facilitate the clearance of pro-inflammatory metabolites, potentially reducing delayed-onset muscle soreness and serum creatine kinase (CK) levels [10].Nevertheless, controlled trials suggest that the effects of IPC on neuromuscular performance remain controversial, particularly in acute settings [11,12].
Despite the widespread use of these recovery modalities, there remains a gap in the literature regarding direct comparisons between MM and IPC in young athletes, particularly within soccer. Furthermore, few studies have concurrently assessed both biochemical markers of muscle damage, such as CK, and functional neuromuscular performance measures, including maximal voluntary isometric contraction and vertical jump performance, under methodologically controlled protocols. Given the potential impact of recovery strategies during critical phases of the competitive calendar, understanding the true efficacy of these interventions is essential for informing clinical and training decisions [12].
Thus, this study aimed to compare the effects of MM and IPC on muscle damage recovery, as well as on lower limb strength and power in Under-20 soccer athletes. The initial hypothesis proposed that both MM and IPC would reduce serum CK levels and enhance musculoskeletal performance, as measured by quadriceps isometric voluntary contraction (Q-IVC), hamstring isometric voluntary contraction (H-IVC), and vertical jump performance (VJ).
2. Materials and Methods
2.1. Ethical Considerations
The procedures of the present study were carried out in accordance with Law 14.874/2024 of the Brazilian National Health Council. The study was submitted and approved by the Augusto Motta University Centre ethics committee [7.163.787] and was conducted in accordance with the Declaration of Helsinki.
2.2. Participants
Twenty male youth athletes (Table 1) from the under-20 category of Paysandu Sport Club – Brazil, regularly engaged in soccer team with a minimum of two years of competitive experience, were recruited for this study. Inclusion criteria were: (i) being clinically healthy; (ii) absence of musculoskeletal injuries within the last six months; and (iii) regular participation in structured soccer training programs (minimum of three times/ weeks). Exclusion criteria included the use of anti-inflammatory medications, presence of neurological, cardiovascular, or musculoskeletal disorders, and any medical contraindication to the proposed recovery techniques.
2.3. Procedures
All procedures were randomized (by computer software - www.randomizer.org.br) and counterbalanced across subjects and experimental conditions to compare the MM and IPC effects on muscle damage recovery, lower limb strength, and power in soccer player under-20 category of Paysandu Sport Club – Brazil. Subjects visited the laboratory 2 times with at least 7 days hours between visits (Figure 1). During the IPC condition, participants underwent bilateral lower-limb compression for a total duration of 20 minutes. In the MM condition, participants received unilateral kneading and stroking techniques applied to the anterior and posterior thigh and the posterior lower leg for the same 20-minute period, thereby equalizing the intervention volume across experimental conditions. To minimize potential carryover effects, a seven-day washout period was implemented between intervention phases. During this interval, participants were instructed to maintain their regular training routines while refraining from any additional recovery interventions. After the washout period, a crossover design was implemented to increase the statistical power and reducing interindividual variability.
2.4. Instruments
2.4.1. Intermittent Pneumatic Compression (IPC)
The IPC intervention was performed using a Reboot Go® sequential compression device. The equipment was applied to the lower limbs via inflatable compression boots with serially arranged chambers that promoted intermittent compression in a distal-to-proximal sequence, following the parameters outlined by [13]. The protocol consisted of a compression cycle at a fixed pressure of 80 mmHg, applied continuously for a total of 20 minutes. The configuration was standardized for all participants to ensure reproducibility and consistency of mechanical stimuli, with the aim of optimizing venous return, reducing muscular edema, and supporting physiological post-exercise recovery processes.
2.4.2. Manual Massage (MM)
The MM intervention followed an adapted protocol from Abrantes et al. [29], totaling 20 minutes of application. All massage techniques were administered by a single experienced researcher to ensure procedural consistency and reproducibility. Initially, participants were placed in the supine position and subjected to effleurage and petrissage techniques, applied unilaterally to the quadriceps musculature. These maneuvers were directed from distal to proximal, beginning at the mid-thigh and extending to the inguinal region, delivered in a single set of 2.5 minutes per limb. Subsequently, participants were repositioned in the prone position, and the same techniques were applied unilaterally to the hamstrings (from the popliteal fossa to the ischial tuberosity) and gastrocnemius muscles (from the Achilles tendon to the gastrocnemius heads at the popliteal region), also in a single set of 2.5 minutes per limb. Pressure intensity was self-regulated by participants using a subjective discomfort/pain scale ranging from 0 to 6, as described by MacDonald et al. [15], to ensure an effective yet tolerable stimulus tailored to each individual's threshold.
2.4.3. Measurements
Muscle Fatigue: Muscle fatigue was assessed through the analysis of serum CK levels, using a portable biochemical analyzer (Simplex Eco Poc®). Blood samples were collected at two time points: pre-intervention (CK-pre) and immediately post-intervention (CK-post). Samples were obtained via capillary puncture from the index finger (30 μL), following antisepsis with 70% alcohol, with the first blood drop discarded. Reagents were prepared at room temperature, and cartridges were discarded after each reading, in accordance with the procedures described by Leite et al. [16], to ensure methodological standardization and minimize bias.
2.4.4. Vertical Jump Performance (VJ):
VJ performance was evaluated using the Jumptest® contact platform (Hidrofit Ltda, Brazil), connected to the Multisprint® software, which has been validated by Ferreira et al. [17]. After familiarization with the equipment, each athlete performed two submaximal jumps followed by three maximal-effort vertical jumps, with a 10-second rest interval between attempts. Data were automatically processed by the software system.
2.4.5. Isometric Voluntary Contraction (IVC):
IVC strength of the knee extensor (Q-IVC) and flexor (H-IVC) muscle groups was measured using the Medeor® isometric dynamometer, following the protocol described by Pinto-Ramos et al. [18]. For Q-IVC, participants were positioned in a seated posture with the knee flexed at 60° and stabilized using straps at the hip joint and mid-thigh. The dynamometer was affixed 5 cm proximal to the medial malleolus on the anterior aspect of the leg. For H-IVC, participants were positioned prone, with the knee flexed at 30°, stabilized at the lumbar spine and thigh. The dynamometer was positioned on the posterior aspect of the leg, also 5 cm proximal to the medial malleolus.
2.5. Statistical Analysis
Data were organized using an electronic spreadsheet (Microsoft Excel 360®) and all statistical procedures were performed using R software (v.4.5) through the RStudio interface, with a significance level set at p<0.05. Prior to hypothesis testing, data were assessed for normality using the Shapiro-Wilk test followed by the symmetry, kurtosis and graphical distribution analysis (histograms and QQ plot) and for homogeneity of variances with Levene’s test. When the assumption of sphericity was violated (as tested by Mauchly’s test), Greenhouse-Geisser corrections were applied. Given the within-subjects crossover design, two-way repeated measures analyses of variance (ANOVA) were employed to examine the main effects of intervention (MM vs IPC), time (pre- and post-intervention), and their interaction on the dependent variables: Q-IVC, H-IVC, VJ, and serum CK levels. Post hoc pairwise comparisons were adjusted using Bonferroni correction to control for Type I error inflation.
3. Results
Figure 1 illustrates the step-by-step methodological approach used for data collection in this study and Table 1 presents the demographic and clinical characteristics of the participants included in the study. Table 2 presents the effects of the MM and IPC interventions on various physiological variables before and after the interventions.
3.1. Serum CK Concentration
CK levels significantly decreased following the MM (pre: 382.50 ± 163.02 U/L; post: 305.40 ± 239.98 U/L; p=0.042), suggesting a positive effect in reducing muscle damage (Table 2). In the IPC, although a reduction was observed (pre: 337 ± 114.50 U/L; post: 199 ± 89.50 U/L), it was not statistically significant (p=0.16) (Table 2). After the crossover, IPC elicited a significant reduction in CK levels (pre: 307 ± 198 U/L; post: 256 ± 84.75 U/L; p=0.028), whereas MM did not reach statistical significance (pre: 316.70 ± 116.66 U/L; post: 252.50 ± 91.77 U/L; p=0.094) (Table 2).
3.2. Isometric Voluntary Contraction (IVC)
Neither intervention (MM or IPC) resulted in significant improvements in Q-IVC (Table 2). In the MM, mean values decreased from 44.64 ± 12.39 kgf to 42.74 ± 9.56 kgf (p=0.59), and in the IPC from 45.08 ± 12.92 kgf to 43.07 ± 10.18 kgf (p=0.58) (Table 2). Following the crossover, although there was a slight increase in IVC values, they were not statistically significant (MM: p=0.27; IPC: p=0.164) (Table 2). H-IVC remained unchanged post-intervention, with no significant differences observed, MM varied from 29.27 ± 8.16 kgf to 29.84 ± 7.14 kgf (p=0.74), and IPC from 28.91 ± 8.66 kgf to 30.14 ± 7.96 kgf (p=0.47) (Table 2). No significant differences were observed in the crossover analysis either (Table 2).
3.3. Vertical Jump Performance
Neither intervention led to a significant increase in VJ height (Table 2). In the MM, mean values decreased from 39.81 ± 3.40 cm to 39.29 ± 3.34 cm (p=0.53), and in the IPC from 39.58 ± 4.09 cm to 39.23 ± 3.41 cm (p = 0.64) (Table 2). Post-crossover results also showed no statistically significant differences (MM: p=0.46; IPC: p=0.23) (Table 2).
4. Discussion
The present study compared the effects of MM and IPC on muscle damage recovery, strength, and lower limb power in Under-20 male soccer athletes. The main findings indicate a significant post-intervention reduction in serum CK levels in both MM (p=0.042) and the IPC (p=0.028). Additionally, neuromuscular performance outcomes (Q-IVC, H-IVC, and VJ) did not show statistically significant differences for either intervention (p>0.05). These findings partially confirm the initial hypothesis of this study.
Serum CK levels in the MM group decreased significantly from 382.5 ± 163.02 U/L to 305.4 ± 239.98 U/L (p=0.042). Physiologically, such reductions may suggest a potential attenuation of acute muscle damage, which is often associated with repeated eccentric efforts and exercise-induced muscle microtrauma, common features of soccer training and competition[19].These results are supported by quantitative evidence [20], who conducted a randomized trial with 18 participants undergoing eccentric elbow exercises. The application of massage (consisted of effleurage (stroking) of the hand (30 seconds), wrist to elbow (1 minute), and elbow to shoulder (1 minute); petrissage (kneading) of the wrist to the elbow (30 seconds) and elbow to shoulder (30 seconds) two hours post-exercise significantly reduced the CK peak value for the massage condition (982 ± 356 IU/L) was 36% lower than that for the control condition (2704 ± 637 IU/L).
Similarly, in a systematic review by Guo et al. [21], 11 studies reported significant reductions (p=0.03) in serum CK levels following massage (used western massage techniques or Swedish massage techniques including effleurage and petrissage) compared to control groups, with a standardized mean difference (SMD) of –0.58 (95% CI: –1.02 to –0.14), indicating a moderate effect in reducing CK concentration. Rasooli et al. [22] investigated the impact of various recovery methods (massage, active recovery, and passive rest) on blood lactate levels and swimming performance in professional athletes. The results indicated that massage, performed using effleurage and petrissage techniques, was significantly more effective than passive recovery in reducing lactate concentration, with post-intervention values of 7.10 ± 1.27 mmol/L for the massage group versus 10.94 ± 2.05 mmol/L for passive recovery (p=0.031) [23].
In our study, the application of IPC resulted in a significant reduction in CK levels, suggesting a beneficial physiological effect on post-exercise muscle recovery. These findings diverge from previous investigations [24], who reported no significant changes in CK activity between the IPC and control groups (p<0.882) in 67 physically active men [25]. Similarly, a systematic review and meta-analysis by Maia et al. [24] described the effects of IPC on muscle function and pain as trivial to small, with high variability in muscle damage biomarkers. Despite the absence of statistically significant improvements in IVC (p=0.164) and VJ height (p=0.23), no decline in performance was observed. This supports the idea that IPC, although it does not improve acute neuromuscular outcomes, does not impair function and may represent a valuable complementary approach to reduce delayed onset muscle soreness and aid in the perception of recovery in athletes [26].
Nevertheless, no statistically significant differences (p>0.05) were observed in Q-IVC, H-IVC or VJ for either the IPC or MM (Table 2). These findings are consistent with those of Hilbert et al. [26], who found no improvements in muscle strength following massage therapy (effleurage, tapotement and petrissage) after an eccentric exercise protocol in a crossover study. Similarly, Dawson et al. [27] reported that 30 minutes of massage (effleurage and petrissage) applied to half-marathon runners did not alter quadriceps or hamstring strength parameters (peak torque). Supporting these findings, Davis et al. [28], in a comprehensive meta-analysis involving 29 studies and over 1.000 participants, concluded that massage therapy (petrissage, effleurage and tapotement) did not lead to statistically significant improvements in muscle strength, jump height, speed, or endurance in volleyball, basketball, cycling and boxing athletes. The absence of significant effects on strength-related variables may also be attributed to the intensity and duration of the massage protocol. According Abrantes et al. [29], massage (manual and instrumental massage) administered prior to strength and power assessments may enhance maximal repetition and muscular power performance.
Both MM and IPC promote recovery primarily through passive mechanisms, such as enhanced circulation, lymphatic drainage, and modulation of the autonomic nervous system. MM stimulates cutaneous and deep mechanoreceptors, which may reduce nociceptive input and increase parasympathetic activity [6] while IPC mimics the muscle pump, improving venous return and fluid clearance [30]. Despite these physiological benefits, neither technique induces sufficient neuromuscular activation or mechanical load to acutely improve strength or power. These strategies may thus serve to optimize recovery without compromising neuromuscular function. Physiologically, both MM and IPC operate through predominantly passive mechanisms, enhancing circulation, lymphatic drainage, and the subjective perception of recovery. However, they do not provide sufficient neural or mechanical stimulus to elicit acute strength or power adaptations, although they do not impair performance either [6].
Although no statistically significant changes were observed in Q-IVC (Δ=3.2%; p=0.219), H-IVC (Δ=2.7%; p=0.281), or VJ performance (Δ=1.9%; p=0.337), it is noteworthy that no functional impairment occurred. This indicates that neither MM or IPC negatively impacted neuromuscular performance following exercise-induced fatigue. The ability to maintain strength and power metrics post-intervention may itself be considered a positive outcome in athletic recovery settings, particularly when athletes are exposed to high training or competition demands. These findings suggest that, while MM and IPC may not acutely enhance performance, they also do not compromise it, supporting their continued use as non-invasive strategies that may contribute to recovery without detrimental effects [6, 7, 27, 31].
It is plausible to consider several aspects related to the present study, including the relatively small sample size. However, given that the sample comprised the entire roster of youth players from a professional football club, with no dropouts or exclusions, this strengthens the study’s internal validity and reduces the risk of sampling bias [32]. Another limitation concerns the methodological variability in the application of MM reported in the literature, as there is no consensus on the ideal protocol in the sports context. To mitigate this factor, a standardized protocol adapted from [29] was used and applied by a trained professional to ensure consistency of the protocol used. Similarly, the IPC was based on the most commonly used parameters in systematic reviews and applied studies in sports recovery, with pressure, duration, and sequence standardized according to current recommendations [27, 31].
Furthermore, the results did not reveal statistically significant changes, either improvements or impairments, in neuromuscular performance. This may be related to the acute nature of the intervention, the low sensitivity of some variables to short-term changes, or the preservation of the athletes’ functional status following intense training loads, as previously reported by Davis et al. [28]. To minimize external interference, all sessions were conducted at the same time of day, in a controlled environment, by a single experienced evaluator, using a crossover design with a seven-day washout period, in accordance with methodological recommendations for clinical trials with small samples [31]. Nevertheless, further longitudinal studies with larger samples, multiple intervention sessions, and varying protocols are recommended to deepen the understanding of the physiological effects of these recovery techniques.
5. Conclusions
In this cross-sectional crossover study, both MM and IPC were evaluated for their acute effects on muscle damage and neuromuscular performance in elite U-20 soccer players. The findings revealed that both interventions elicited significant reductions in serum CK levels, an established marker of muscle damage, suggesting a beneficial effect on post-exercise recovery. Notably, MM produced an immediate reduction in CK following the first intervention phase (p=0.042), while IPC demonstrated a delayed but significant effect after the crossover (p=0.028). Despite these biochemical benefits, neither intervention significantly altered IVC or VJ performance, indicating no acute enhancement, or impairment, of neuromuscular output. These results align with previous evidence that passive recovery modalities such as MM and IPC may not stimulate sufficient neuromuscular adaptation to impact strength or power outcomes in the short term.
From a practical standpoint, these findings support the use of MM and IPC as viable recovery tools to mitigate biochemical markers of muscle stress without compromising performance, a crucial consideration for high-performance environments where recovery windows are narrow. Coaches and sports performance practitioners may consider integrating these techniques post-exercise or between training sessions to facilitate recovery while maintaining neuromuscular readiness. Future investigations should explore the cumulative effects of repeated sessions over time and assess whether individualized protocols may yield greater functional benefits.
6. Limitations
This study is not without limitations. First, the small sample size, although controlled for by the crossover design, may limit generalizability. Second, the acute nature of the interventions may not reflect the cumulative effects of repeated recovery sessions. Third, only biochemical and neuromechanical markers were assessed; future studies should consider incorporating perceptual and hormonal indicators to provide a more holistic understanding.
Author Contributions
Conceptualization, T.C.E.; J.C.O.M.C.; J.G.S.; E.R.M. and I.R.T.J.; methodology, T.C.E.; J.C.O.M.C.; J.G.S.; E.R.M. and I.R.T.J..; validation, T.C.E.; J.C.O.M.C.; J.G.S.; M.R-A.; L.T.S.; L.B.G.C.; J.V-A.; E.R.M. and I.R.T.J.; formal analysis, T.C.E.; J.C.O.M.C.; J.G.S.; M.R-A.; L.T.S.; L.B.G.C.; J.V-A.; E.R.M. and I.R.T.J.; investigation, T.C.E.; E.R.M.; and I.R.T.J.; data curation, T.C.E.; J.C.O.M.C.; J.G.S.; M.R-A.; L.T.S.; L.B.G.C.; J.V-A.; E.R.M. and I.R.T.J.; writing—original draft preparation, T.C.E.; J.C.O.M.C.; J.G.S.; M.R-A.; L.T.S.; L.B.G.C.; J.V-A.; E.R.M. and I.R.T.J.; writing—review and editing, T.C.E.; J.C.O.M.C.; J.G.S.; M.R-A.; L.T.S.; L.B.G.C.; J.V-A.; E.R.M. and I.R.T.J.; supervision, E.R.M.; and I.R.T.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research Ethics Committee of Centro Universitário Augusto Motta (protocol number 7.163.787, approved in 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank the participating athletes and coaching staff for their commitment and cooperation during all phases of the study. We also acknowledge the support of the Centro Universitário Augusto Motta (UNISUAM) for infrastructure access.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Akyildiz, Z.; Ocak, Y.; Clemente, F.M.; Birgonul, Y.; Günay, M.; Nobari, H. Monitoring the Post-Match Neuromuscular Fatigue of Young Turkish Football Players. Sci. Rep. 2022, 12, 13835. [Google Scholar]
- Brownstein, C.G.; Dent, J.P.; Parker, P.; Hicks, K.M.; Howatson, G.; Goodall, S.; Thomas, K. Etiology and Recovery of Neuromuscular Fatigue Following Competitive Soccer Match-Play. Front. Physiol. 2017, 8, 831. [Google Scholar]
- Nedelec, M.; Mccall, A.; Carling, C. Recovery in Soccer : Part II-Recovery Strategies . Physical Performance and Subjective Ratings after a Soccer-Specific Exercise Simulation : Comparison of Natural Grass versus Artificial Turf. 2013.
- Robineau, J.; Jouaux, T.; Lacroix, M.; Babault, N. Neuromuscular Fatigue Induced by a 90-Minute Soccer Game Modeling. Journal of Strength and Conditioning Research 2012, 26, 555–562. [Google Scholar]
- Poppendieck, W.; Wegmann, M.; Ferrauti, A.; Kellmann, M.; Pfeiffer, M.; Meyer, T. Massage and Performance Recovery: A Meta-Analytical Review. Sports Med 2016, 46, 183–204. [Google Scholar]
- Weerapong, P.; Hume, P.A.; Kolt, G.S. The Mechanisms of Massage and Effects on Performance, Muscle Recovery and Injury Prevention. Sports Med 2005, 35, 235–256. [Google Scholar]
- Dakić, M.; Toskić, L.; Ilić, V.; Đurić, S.; Dopsaj, M.; Šimenko, J. The Effects of Massage Therapy on Sport and Exercise Performance: A Systematic Review. Sports 2023, 11, 110. [Google Scholar] [CrossRef]
- Chase, J.E.; Peeler, J.D.; Barr, M.J.; Gardiner, P.F.; Cornish, S.M. The Impact of a Single Bout of Intermittent Pneumatic Compression on Performance, Inflammatory Markers, and Myoglobin in Football Athletes. 2020, 33–38.
- Cochrane, D.; Booker, H.; Mundel, T.; Barnes, M. Does Intermittent Pneumatic Leg Compression Enhance Muscle Recovery after Strenuous Eccentric Exercise? Int J Sports Med 2013, 34, 969–974. [Google Scholar]
- Overmayer, R.G.; Driller, M.W. Pneumatic Compression Fails to Improve Performance Recovery in Trained Cyclists. International Journal of Sports Physiology and Performance 2018, 13, 490–495. [Google Scholar]
- Hill, J.; Howatson, G.; Van Someren, K.; Leeder, J.; Pedlar, C. Compression Garments and Recovery from Exercise-Induced Muscle Damage: A Meta-Analysis. Br J Sports Med 2014, 48, 1340–1346. [Google Scholar]
- Hader, K.; Rumpf, M.C.; Hertzog, M.; Kilduff, L.P.; Girard, O.; Silva, J.R. Monitoring the Athlete Match Response: Can External Load Variables Predict Post-Match Acute and Residual Fatigue in Soccer? A Systematic Review with Meta-Analysis. Sports Med - Open 2019, 5, 48. [Google Scholar]
- Heapy, A.M.; Hoffman, M.D.; Verhagen, H.H.; Thompson, S.W.; Dhamija, P.; Sandford, F.J.; Cooper, M.C. A Randomized Controlled Trial of Manual Therapy and Pneumatic Compression for Recovery from Prolonged Running – an Extended Study. Research in Sports Medicine 2018, 26, 354–364. [Google Scholar] [PubMed]
- Abrantes, R.; Monteiro, E.R.; Vale, R.G.D.S.; De Castro, J.B.P.; Bodell, N.; Hoogenboom, B.J.; Leitão, L.; Serra, R.; Vianna, J.M.; Da Silva Novaes, J. The Acute Effect of Two Massage Techniques on Functional Capability and Balance in Recreationally Trained Older Adult Women: A Cross-over Study. Journal of Bodywork and Movement Therapies 2021, 28, 458–462. [Google Scholar] [PubMed]
- MacDonald, G.Z.; Button, D.C.; Drinkwater, E.J.; Behm, D.G. Foam Rolling as a Recovery Tool after an Intense Bout of Physical Activity. Medicine & Science in Sports & Exercise 2014, 46, 131–142. [Google Scholar]
- Leite, R.D.; Prestes, J.; Rosa, C. Acute Effect of Resistance Training Volume on Hormonal Responses in Trained Men. 2011, 2, 322–328.
- Ferreira, J.; Da Silva Carvalho, R.; Barroso, T.; Szmuchrowski, L.; Śledziewski, D. Effect of Different Types of Recovery on Blood Lactate Removal After Maximum Exercise. Polish Journal of Sport and Tourism 2011, 18, 105–111. [Google Scholar]
- Pinto-Ramos, J.; Moreira, T.; Costa, F.; Tavares, H.; Cabral, J.; Costa-Santos, C.; Barroso, J.; Sousa-Pinto, B. Handheld Dynamometer Reliability to Measure Knee Extension Strength in Rehabilitation Patients—A Cross-Sectional Study. PLoS ONE 2022, 17, e0268254. [Google Scholar]
- Lewis, P.B.; Ruby, D.; Bush-Joseph, C.A. Muscle Soreness and Delayed-Onset Muscle Soreness. Clinics in Sports Medicine 2012, 31, 255–262. [Google Scholar]
- Zainuddin, Z.; Newton, M.; Sacco, P.; Nosaka, K. 174-180 by the National Athletic Trainers’ Association, Inc; †University Technology of Malaysia. Journal of Athletic Training 2005, 40, 174–180. [Google Scholar]
- Guo, J.; Li, L.; Gong, Y.; Zhu, R.; Xu, J.; Zou, J.; Chen, X. Massage Alleviates Delayed Onset Muscle Soreness after Strenuous Exercise: A Systematic Review and Meta-Analysis. Front. Physiol. 2017, 8, 747. [Google Scholar]
- Rasooli, S.A.; Jahromi, M.K. Influence of Massage, Active and Passive Recovery on Swimming Performance and Blood Lactate. 2012, 52, 122–127.
- Wiecha, S.; Jarocka, M.; Wiśniowski, P.; Cieśliński, M.; Price, S.; Makaruk, B.; Kotowska, J.; Drabarek, D.; Cieśliński, I.; Sacewicz, T. The Efficacy of Intermittent Pneumatic Compression and Negative Pressure Therapy on Muscle Function, Soreness and Serum Indices of Muscle Damage: A Randomized Controlled Trial. BMC Sports Sci Med Rehabil 2021, 13, 144. [Google Scholar]
- Maia, F.; Machado, M.V.; Silva, G.; Yuzo Nakamura, F.; Ribeiro, J. Hemodynamic Effects of Intermittent Pneumatic Compression on Athletes: A Double-Blinded Randomized Crossover Study. 2024, 19, 932–938.
- Maia, F.; Nakamura, F.Y.; Pimenta, R.; Tito, S.; Sousa, H.; Ribeiro, J. Intermittent Pneumatic Compression May Reduce Muscle Soreness but Does Not Improve Neuromuscular Function Following Exercise-Induced Muscle Damage: A Randomized Placebo-Controlled Trial. International Journal of Sports Physiology and Performance 2025, 1–7. [Google Scholar]
- Hilbert, J.E.; Sforzo, G.A.; Swensen, T. The Effects of Massage on Delayed Onset Muscle Soreness. British Journal of Sports Medicine 2003, 37, 72–75. [Google Scholar] [PubMed]
- Dawson, L.G.; Dawson, K.A.; Tiidus, P.M. Evaluating the Influence of Massage on Leg Strength, Swelling, and Pain Following a Half-Marathon. ©Journal of Sports Science and Medicine 2004, 3, 37–43. [Google Scholar] [PubMed]
- Davis, H.L.; Alabed, S.; Chico, T.J.A. Effect of Sports Massage on Performance and Recovery: A Systematic Review and Meta-Analysis. BMJ Open Sport Exerc Med 2020, 6, e000614. [Google Scholar] [PubMed]
- Oliveira Abrantes, R.; Monteiro, E.; Ribeiro, M.; Fiuza, A.; Cesar De Oliveira Muniz Cunha, J. Massage Acutely Increased Muscle Strength and Power Force; 2019.
- Zuj, K.A.; Prince, C.N.; Hughson, R.L.; Peterson, S.D. Enhanced Muscle Blood Flow with Intermittent Pneumatic Compression of the Lower Leg during Plantar Flexion Exercise and Recovery. J Appl Physiol 2018, 124, 302–311. [Google Scholar]
- Dupuy, O.; Douzi, W.; Theurot, D.; Bosquet, L.; Dugué, B. An Evidence-Based Approach for Choosing Post-Exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front. Physiol. 2018, 9, 403. [Google Scholar]
- Bacchetti, P. Current Sample Size Conventions: Flaws, Harms, and Alternatives. BMC Med. 2010, 8. [Google Scholar]
- Senn, S. Seven Myths of Randomisation in Clinical Trials. Statistics in Medicine 2013, 32, 1439–1450. [Google Scholar]
Figure 1.
Flowchart illustrating the process of selection, randomization, and allocation of research participants.
Figure 1.
Flowchart illustrating the process of selection, randomization, and allocation of research participants.
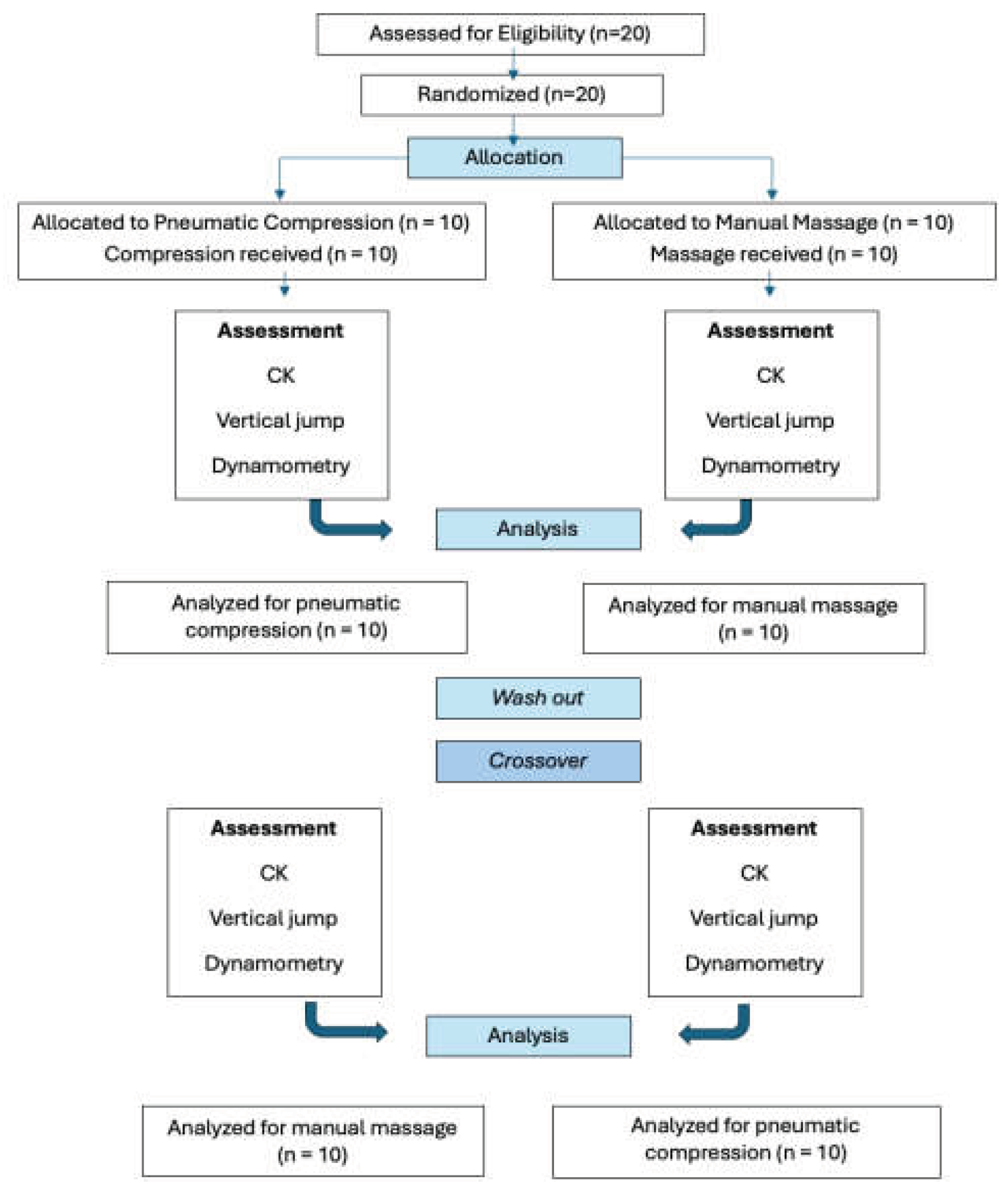

Table 1.
Anthropometric characteristics of the sample (Mean ± SD and 95%CI).
| Mean ± SD | 95%CI | CV (%) | |||
| Age (years) | 18.65 ± 0.67 | 18.40 – 18.90 | 3.59 | ||
| Height (m) | 1.78 ± 0.07 | 1.75 – 1.81 | 3.93 | ||
| Weight (kg) | 72.8 ± 6.99 | 70.19 – 75.41 | 9.60 | ||
| Body Fat (%) | 12.3 ± 1.63 | 11.69 – 12.91 | 13.25 | ||
SD: Standard Deviation; 95%CI: 95% Confidence Interval; CV: Coefficient of Variation.
Table 2.
Pre- and post-intervention values (mean, standard deviation, and p-value) for serum CK, isometric strength, and vertical jump performance following intermittent pneumatic compression and manual massage, before and after crossover.
Table 2.
Pre- and post-intervention values (mean, standard deviation, and p-value) for serum CK, isometric strength, and vertical jump performance following intermittent pneumatic compression and manual massage, before and after crossover.
| Variables | IPC (Pre)(n=10) | IPC (Post)(n=10) | p-value | Variables | MM (Pre) (n=10) | MM (Post)(n=10) | p-value |
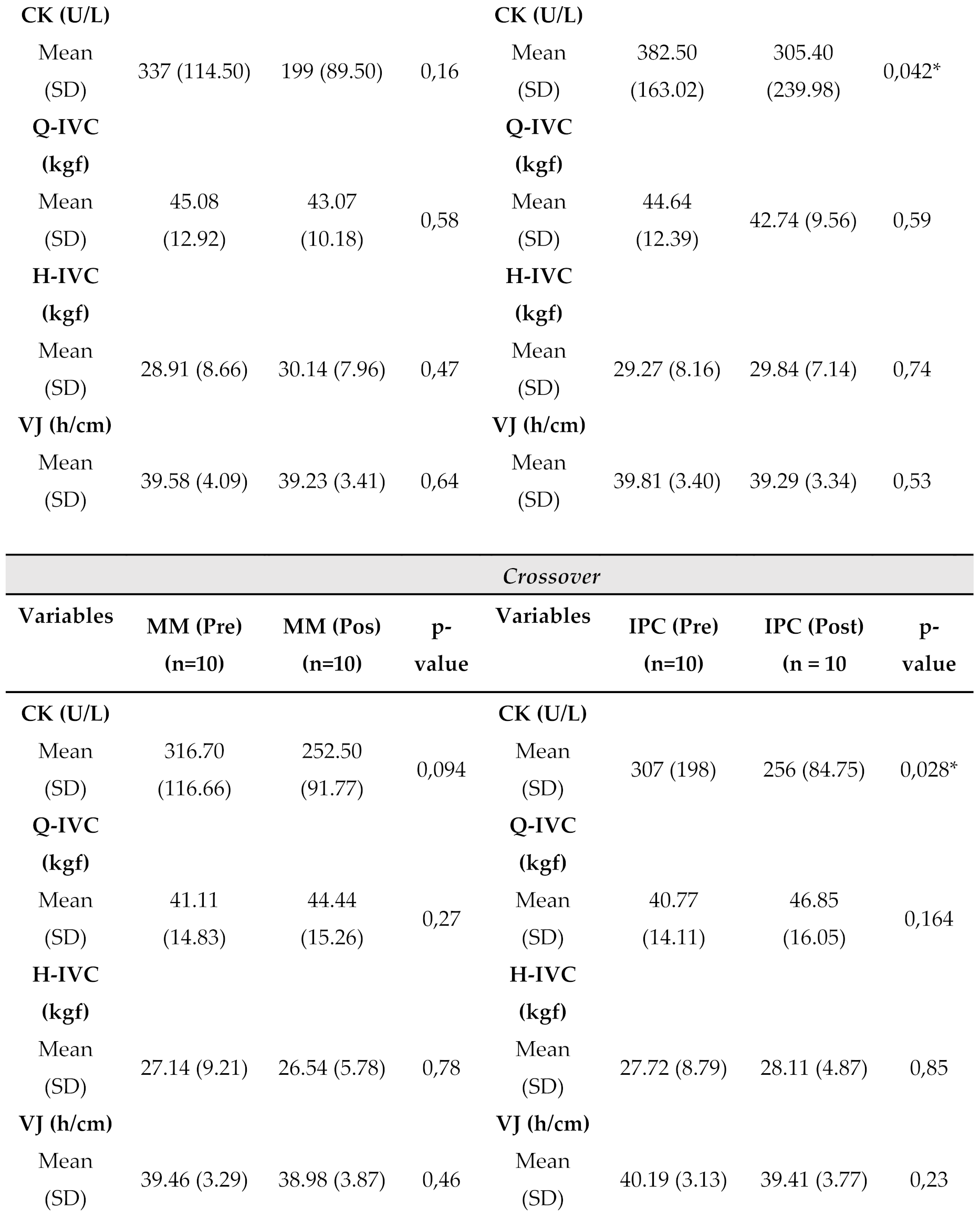 | |||||||
Legend: CK = creatine kinase; Q-IVC = maximum isometric voluntary contraction of the quadriceps; H-ICV = maximum isometric voluntary contraction of the hamstrings; VJ = vertical jump (h/cm); ICP = intermittent pneumatic compression; MM = manual massage. *Statistical difference between Post e Pre-interventio; SD = standard deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



