
Submitted:
04 July 2025
Posted:
07 July 2025
You are already at the latest version
Abstract
Background: Digital ulcers (DUs) are among the most debilitating vascular complications in SSc and are commonly attributed to microvascular damage. However, recent evidence suggests a potential involvement of macrovascular abnormalities, including subclinical atherosclerosis and altered hemodynamic parameters. Objectives: This study aimed to investigate the association between a history of DUs and macrovascular involvement in SSc patients through carotid and vertebral Doppler ultrasonography, with a focus on hemodynamic indices such as Peak Systolic Velocity (PSV), End-Diastolic Velocity (EDV), Resistive Index (RI), and Intima-Media Thickness (IMT). Methods: A cross-sectional study was conducted on 107 SSc patients. Clinical, serological, cardiovascular, and metabolic data were collected, and carotid-vertebral ultrasound was performed. Patients were stratified based on DU history. Statistical analyses assessed associations between DU status and carotid-vertebral US findings. Results: Patients with DUs showed significantly higher PSV in both right (86.9±67.9 vs 64.2±20.5 cm/s, p=0.010) and left ICA (78.9±29.6 vs 63.4±18.2 cm/s, p=0.002). Right ICA RI vas elevated in the DU group (p =0.021). PSV in the external carotid arteries was also increased bilaterally in DU patients (p<0.005). DU-positive patients had a higher prevalence of left carotid plaques (p=0.012) and right-sided ICA RI >0.75 (p=0.01). Logistic regression identified DU history as an independent predictor of ICA PSV (β=33.72, p=0.002) and carotid plaque presence at any sides (OR 14.34, p=0.012). Conclusions: A history of digital ulcers in SSc patients is associated with altered carotid hemodynamics and increased subclinical atherosclerotic burden. These findings suggest that DUs may reflect not only microvascular damage but also macrovascular dysfunction, supporting the need for integrated vascular assessment in SSc clinical practice.
Keywords:
Systemic Sclerosis
; Digital Ulcers
; Macrovascular impairment
; cardiovascular risk
; carotid hemodynamics
1. Introduction
Historically, vasculopathy in Systemic sclerosis (SSc) has been considered a microcirculatory disorder, however, accumulating evidence suggests that medium- and large-caliber arteries may also be implicated, revealing a complex scenario that extends beyond microcirculation [1,2]. Indeed, microvascular damage represents the hallmark of the disease, with the endothelial dysfunction driving a pivotal role even at early stages [3]. The main clinical manifestations of SSc-related vasculopathy include Raynaud’s phenomenon (RP) and puffy hands, which are observed even in patients with very early diagnosis of SSc (VEDOSS), while fingertip pitting scars, digital ulcers (DUs), telangiectasias, and pulmonary arterial hypertension (PAH) tend to appear in established forms of the disease [4,5].
Insightfully, DUs are among the most debilitating complications of SSc and have been widely acknowledged as markers of severity of the SSc-related vasculopathy. They may provoke significant pain, impaired hand function, increased risk of infection, and reduced quality of life of affected patients [6]. DUs are defined as the loss of epidermal continuity extending into the dermis, with different degree of exposure of the underlying tissues, potentially evolving towards gangrene and digital loss [7].
In SSc, DUs development has been predominantly attributed to microvascular injury, however, in the general population the primary causes of digital ischemia include arterial abnormalities, extrinsic vascular compression, thromboembolic events, and atherosclerosis, the latter predominantly resulting from plaque accumulation in large-caliber arteries [8,9,10,11].
In this context, recent research has shown that the endothelial dysfunction is also present at brachial arteries and correlates with microvascular damage at nailfold level, suggesting a continuum of vascular injury spanning both micro- and macrovascular beds [12]. As suggested by the Italian multicentre observational GIRRCS study, a slightly increase of clinical and subclinical atherosclerosis is displayed by SSc patients compared to available controls. In addition, the authors demonstrated that both traditional cardiovascular risk factors and SSc-specific features, such as ischemic digital ulcers, played a synergistic role in the development of cardiovascular complications [13].
To detect pre-atherosclerotic changes, most studies have employed B-mode vascular ultrasound at carotid and peripheral arteries beds [14]. These non-invasive techniques have proven effective in identifying early vascular abnormalities, such as intima-media thickness (IMT) and arterial stiffness, which have been consistently observed at higher rates in SSc. These findings are notably occurring even in the absence of traditional cardiovascular risk factors and despite a relatively low incidence of clinically overt cardiovascular events in SSc patients [15].
However, doppler ultrasound at both carotid and peripheral arteries levels, could provide various hemodynamically significant indices other than IMT, among which Peak Systolic Velocity (PSV), End-Diastolic Velocity (EDV) and, Resistive Index (RI). These hemodynamic indices have been already validated as predictors of macrovascular dysfunction in other populations, such as Type 2 Diabetes Mellitus patients [16]. Briefly, PSV reflects the maximum blood flow velocity during systole and it is particularly useful in identifying areas of arterial narrowing [17]. EDV, on the other hand, represents blood flow velocity during diastole, and it is particularly sensitive to downstream vascular resistance [18]. RI, quantifying the resistance to blood flow within a vessel, is used to evaluate end-organ perfusion [19].
Lastly, given the conflicting data regarding which SSc-specific features best explain clinical or subclinical atherosclerosis and macrovascular impairment, our study investigates the association between DUs, widely recognized as a clinical surrogate of microvascular injury, and Doppler ultrasound indices of the carotid and vertebral arteries. Utilizing non-invasive Doppler hemodynamic measurements, including cIMT, PSV, EDV, and RI our objective is to elucidate the emerging interplay between microvascular and macrovascular compartments. By employing widely accessible and routinely performed ultrasound imaging techniques, we further aim to support the integration of macrovascular ultrasound assessment into clinical practice for SSc patients.
2. Materials and Methods
2.1. Study Population and Sample Definition
We conducted a cross-sectional observational study involving a cohort of one-hundred and seven SSc patients attending the Scleroderma Unit of ASST Ovest Milanese, Legnano Hospital (Milan, Italy). Participants, aged ≥18 years and able to provide informed consent, were selected based on their fulfillment of the 2013 ACR/EULAR for a definitive diagnosis of SSc [20]. Patients with severe heart failure, a positive history of congenital heart disease, current malignancies or anti-neoplastic treatment and individuals who underwent cardiac surgery, percutaneous coronary, carotid and vertebral intervention, pacemaker implant and carotid-vertebral endarterectomy were excluded from the study. Severe cognitive impairment and pregnancy status served as further exclusion criteria.
Participants were recruited from September 2024 to May 2025, and the study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki, with the protocol number S00125/2023 obtained from the Ethic Committee of Milan Area 3.
2.2. Data Collection
Patients’ demographic and anthropometric characteristics were extracted from medical records. Data collection included information on age, sex, weight, height, Body Mass Index, Body Surface area and previous or smoking status. Data concerning age at enrollment and SSc diagnosis were also gathered from clinical records, as well as for disease duration.
Based on data of previous evaluations, all patients’ disease specific characteristics were assessed, including the presence of RP, puffy hands, telangiectasias, prior and current history of DUs, fingertip pitting scars, sclerodactyly, skin sclerosis, calcinosis, microstomia and microcheilia, musculoskeletal and upper and/or lower gastrointestinal involvements. Interstitial Lung disease (ILD), PAH and Cardiomyopathy were detected through chest High Resolution Computed Tomography (HRCT), Right Heart Catheterization (RHC) and cardiac Magnetic Resonance Images (cMRI), respectively. Modified Rodnan Skin Score (mRSS) was employed to assess skin sclerosis extension [21].
Serological classification based on the positivity for anticentromere antibodies (ACA), anti-topoisomerase I (anti-Scl70) antibodies and anti-RNA polymerase III antibodies (ARA) were collected from patient medical history. Based on the most recent assessment, Nailfold Videocapillaroscopy (NVC) patterns were classified according to the Cutolo criteria and categorized into early, active, and late patterns [22].
Current medication status with a potential influence on macro- and microvascular functionality were gathered, including anti-hypertensive treatment (such as calcium channel blockers (CCBs), angiotensin converting enzyme inhibitors (ACEis), angiotensin receptor blockers (ARBs), beta-blockers, diuretics), low-dose aspirin, intravenous Iloprost, endothelin receptor antagonists (ERAs), phosphodiesterase type 5 inhibitors (PDE5i) and lipid-lowering treatment. Data on glucocorticoid usage and immunosuppressive treatments were also evaluated.
2.3. Cardiovascular and Atherosclerotic Risk Assessment
Data regarding comorbidities such as Type 2 Diabetes Mellitus, Systemic Arterial Hypertension, Arrhytmias, Hyperuricemia, Dyslipidemia with a known and established influence on cardiovascular system were taken into account, as well as the previous familiar and personal history for cardio- and cerebrovascular events. Patients were clinically evaluated to obtain information regarding the presence of cardiopalmus, angina pectoris and heart-related dyspnea.
All recruited participants underwent standardized measurement of hemodynamic parameters at rest, in a quiet environment, thirty minutes prior to the execution of the carotid-vertebral Doppler ultrasound. Specifically, systolic and diastolic blood pressure levels, as well as heart rate (HR), were recorded in duplicate, with each measurement taken five minutes apart using an automated oscillometric sphygmomanometer on the dominant arm after at least 10 minutes of supine rest [23]. Cardiovascular risk scores were calculated using the validated Framingham and ASCVD (Atherosclerotic Cardiovascular Disease) risk equations, incorporating clinical variables such as age, sex, blood pressure, lipid profile, diabetes status, and smoking habits, in accordance with ACC/AHA guidelines [24,25,26].
2.4. Biochemical and Metabolic Assessments
Venous blood samples were collected within the same month as the carotid and vertebral Doppler ultrasound examination. All laboratory analyses were performed in the institutional central laboratory, following standardized protocols. The metabolic and cardiovascular profile included the measurement of total cholesterol, HDL cholesterol (HDL), LDL cholesterol (LDL), triglycerides, fasting glucose, high-sensitivity troponin T (hs-TnT), N-terminal pro–brain natriuretic peptide (NT-proBNP), uric acid, c-reactive protein (CRP) and hemoglobin (Hb). Units of measurement were as follows: cholesterol and triglycerides (mg/dL), glucose (mg/dL), troponin T (ng/L), NT-proBNP (pg/mL), uric acid (mg/dL), Hb (g/dL) and CRP (mg/l). Lipid parameters were assessed enzymatically, cardiac markers by electrochemiluminescence immunoassay, and Hb using an automated hematology analyzer.
Based on these parameters, the following metabolic indices were further calculated: (1) the Triglyceride-glucose index (TyG index) was derived by taking the natural logarithm of the product of fasting triglyceride and fasting glucose levels divided by two [27]; (2) the LDL/HDL ratio was calculated by dividing the concentration of LDL cholesterol by that of HDL cholesterol [28]; (3) the Triglyceride/HDL ratio (TG/HDL) was obtained by dividing serum triglycerides by HDL cholesterol [29]; (4) the Atherogenic Index of Plasma (AIP) was expressed as the base-10 logarithm of the ratio between serum triglycerides and HDL cholesterol [30]; (5) the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) was calculated, where available, by multiplying fasting glucose (in mg/dL) by fasting insulin (in µU/mL) and dividing the result by 405 [31].
2.5. Ultrasound Examination
Ultrasound examination of the supra-aortic vessels was performed using a GE Vivid T8 ultrasound system equipped with a high-frequency linear transducer (8 MHz). All patients were examined in the supine position, with the neck slightly extended and rotated contralaterally to the side under evaluation, to optimize image acquisition. For the common carotid artery (CCA), internal carotid artery (ICA), external carotid artery (ECA), and vertebral artery (VA), both transverse and longitudinal scans were performed using B-mode imaging, color Doppler, and pulsed-wave Doppler techniques.
Intima-media thickness (IMT) was measured in the longitudinal plane of the CCA, on the far wall, approximately 1 cm proximal to the carotid bifurcation [32]. The IMT value was calculated as the mean of three separate consecutive measurements. Atherosclerotic plaques were defined as focal structures that protrude into the arterial lumen by at least 0.5 mm, or by 50% of the surrounding IMT value, or that exhibit a thickness greater than 1.5 mm, measured from the intima–lumen interface to the media–adventitia interface [33]. For each vessel, peak systolic velocity (PSV) and end-diastolic velocity (EDV) were recorded using pulsed-wave Doppler, maintaining an angle of insonation between 45°-60°. In addition, resistance indices (RI) were calculated for the CCA, ICA, and ECA to assess vascular resistance and aid in the hemodynamic interpretation. The RI was calculated using the following formula: “RI = (PSV − EDV) / PSV”, and the validated cut-off of 0.75 was considered for the analysis [34].
In the presence of atherosclerotic plaques, the degree of stenosis was first assessed morphologically according to the criteria of the North American Symptomatic Carotid Endarterectomy Trial (NASCET) [35]. A complementary hemodynamic evaluation was also performed based on the classification proposed by Grant et al. and applied in cases of stenosis >50% or PSV >125 cm/s [36].
As most of participant were undergoing monthly Iloprost infusion US examination was performed two weeks apart the last infusion, to avoid any influence in SBP, DBP and HR on examined velocities. Moreover, to avoid intra and interobserver bias, the images were acquired and further evaluated two-fold by two experienced sonography examiners (F.L. – seven years of experience and L.C., five years of experience) who were blinded for patient data and characteristics.
2.6. Statistical Analysis
Patients' data were summarized as mean and standard deviation for normally distributed variables or as median and interquartile range (IQR) for skewed ones. Discrete or qualitative variables were summarized as counts and percentages. Mean differences of continuous variables were assessed using Student’s t-test or Mann-Whitney U-test, depending on whether the data followed a parametric or non-parametric distribution. Chi-squared and Fisher’s exact tests were used to compare categorical variables based on sample size. Linear regression analysis determined predictors for mean PSV at ICA and ECA. Additionally, a binary logistic regression model was developed to investigate potential risk factors associated with the presence of atherosclerotic plaques at any site. Covariates included in both analyses were selected a priori based on their well-established roles in plaque formation as supported by literature evidences. These variables comprised age, sex, BMI, LDL/HDL ratio, AIP, Framingham risk score, ASCVD risk score, and SBP, and as per the main purpose of the study history of DUs was also incorporated.
A p-value of ≤0.05 or a 95% confidence interval not crossing zero were considered statistically significant. All statistical analyses were performed using IBM SPSS Statis-tics version 27 (IBM SPSS Software, Armonk, NY, USA).
3. Results
3.1. Patient Clinical Characteristics
A total of 107 patients were enrolled, with 76 (71.0%) having no history of DUs and 31 (29.0%) reporting past DUs. Female prevalence was significantly higher in the non-DUs group (96.1% vs 71.0%, p<0.001). Mean age at enrollment was similar between groups (62.3±12.0 vs 58.8±12.7 years, p=0.189), but patients with DUs were diagnosed earlier (43.4±15.2 vs. 49.9±13.2 years, p=0.041). Disease duration, BMI, and BSA showed no significant differences [Table 1].
Regarding autoantibodies, anti-Scl-70 positivity was more frequent in the DUs-group (35.5% vs 7.9%, p=0.001), whereas ACA and ARA antibodies were comparable. Skin involvement, measured by the mRSS, was greater in DUs-group (8.5±8.4 vs 2.1±2.3, p<0.001). According to the LeRoy classification, dcSSc was more common in the DUs-group (38.7% vs. 1.3%, p=0.001), while limited and sine scleroderma subsets predominated in non-DUs patients. NVC patterns also differed: early/active patterns were more frequent in non-DUs patients (76.3% vs 45.2%, p=0.002), and late patterns prevailed among DUs patients (54.8% vs. 23.7%, p=0.002). Moreover, several clinical features correlated with a history of DUs, including puffy hands (p=0.005), telangiectasias (p=0.001), pitting scars (p<0.001), sclerodactyly (p=0.001), calcinosis (p=0.003), friction rubs (p=0.001), and microstomia (p<0.001).
Upper gastrointestinal involvement was more prevalent in DUs patients (80.6% vs. 56.6%, p=0.019), while lower gastrointestinal symptoms, arthritis, renal crisis, cardiomyopathy, and PAH did not differ significantly. Lastly, ILD was notably more frequent in the DUs group (48.4% vs. 11.8%, p<0.001).
Regarding therapies, antihypertensive medication usage along with lipids and uric acid lowering therapies were comparable. The only differences emerged with the use of ERAs and sildenafil, as expected for the prevention of DUs. (p<0.001 for both). [Supplementary Table S1].
3.2. Cardiovascular Risk Assessment and Metabolic Indices
Patients with DUs reported more commonly angina pectoris (19.4% vs 5.3%, p=0.023), and hyperuricemia (16.1% vs 1.3%, p=0.003). However, no differences emerged for dyspnea, cardiopalmus, arrhythmias, hypertension, dyslipidemia, or T2DM [Table 2].
Notably, metabolic parameters, including total cholesterol, HDL, LDL, triglycerides, fasting glucose, insulin, and calculated indices such as TyG index, HOMA-IR, LDL/HDL ratio, TG/HDL ratio, and Atherogenic Index of Plasma (AIP) showed no significant differences between groups. Similarly, inflammatory and cardiac biomarkers (CRP, hs-TnT, NT-proBNP, uric acid) were comparable. Blood pressure and heart rate, measured twice five minutes apart, did not differ significantly. Moreover, Framingham risk scores were higher in DU-positive patients (p=0.048), indicating increased cardiovascular risk, whereas ASCVD risk scores were similar [Figure 1].
3.3. Carotid Ultrasound Findings
Carotid ultrasound revealed a higher prevalence of atherosclerotic plaques in the left carotid artery in DUs patients (51.6% vs 26.3%, p=0.012). Similarly, right carotid plaques were more frequent in the DUs (45.2% vs. 31.6%) but without statistical significance. DUs patients exhibited a greater prevalence of bilateral localization of the plaques (38.7% vs 13.2%, p=0.003), while the two groups did not differ when any side (left, right or both) was considered, however a trend toward significance was detected (58.1% vs 38.2%, p=0.059) [Figure 2].
On the left side, plaque prevalence in the carotid bulb was 11.8% in the non-DUs group and 25.8% in the DUs group, without reaching statistical significance. Plaques at the bulb–ICA transition were detected in 3.9% of non-DUs and 9.7% of DUs patients, while isolated ICA plaques were found in 7.9% and 16.1% of patients. In contrast, the right side revealed that carotid bulb plaques were significantly more frequent in patients with a history of DUs compared to those without (29.0% vs 11.8%, p=0.02). While plaques at the bulb–ICA site were seen in 9.7% of DUs patients and 6.6% of non-DUs (p=0.69), and ICA plaques in 29.0% vs 9.2%, respectively (p=0.07), showing a trend toward significance. [Figure 3].
Moreover, the number of patients reporting a stenosis percentage at the plaque site comprised between 0-49% were 18 out of 76 patients in the non-DUs, while 10 out 31 in the DUs group (p=0.4673), however, patients with a grade of stenosis more the 50% were 2/76 in the non-DUs group and 4/31 in the DUs group (p=0.057), showing a trend toward significance in the latter group.
3.4. Doppler Hemodynamic Parameters
From a vascular standpoint no significant differences were observed in EDV or cIMT measurements [Table 3]. However, patients with DUs exhibited higher carotid blood flow velocities, still falling within the normal physiological range (PSV<125 cm/s), with a significant bilateral increase in PSV of the ICA (right: 86.9±67.9 vs 64.2±20.5 cm/s, p=0.01; left: 78.9±29.6 vs 63.4±18.2 cm/s, p=0.001), as was PSV in the ECA (right: 75.0±24.2 vs 87.7±25.3 cm/s, p=0.018; left: 71.7±20.1 vs 86.1±24.1 cm/s, p=0.002).
Moreover, significant increases in RI were noted in the right ICA in the DUs group compared to DUs negative controls (p=0.021 and p=0.013, respectively). Finally, the ICA/CCA PSV ratio on the right side was significantly elevated in DUs patients (1.48±1.21 vs 1.16±0.33; p=0.043).
Furthermore, on the right side, DUs patients more frequently had elevated pulsatility index (PI >1.2) and resistive index (RI >0.75) in the ICA (35.5% vs 13.5%, p=0.01), along with more carotid stenosis (12.9% vs 2.7%, p=0.04). On the left side, elevated PI and RI in the ICA were also more common in DUs patients (35.5% vs 8.1%, p<0.001). No differences were found for cIMT > 0.9 mm, or elevated RI in the CCA or ECA, between the groups.
Furthermore, on the right side, DUs patients more frequently had elevated resistive index (RI >0.75) in the ICA (35.5% vs 13.5%, p=0.01), along with more carotid stenosis (12.9% vs 2.7%, p=0.04). On the left side, elevated RI in the ICA were also more common in DUs patients (35.5% vs 8.1%, p<0.001). No differences were found for CCA IMT > 0.9 mm, or increased RI in the CCA or ECA between the groups. [Figure 4].
3.5. Regression Analyses
Firstly, two multivariable linear regressions were performed to identify predictors of mean PSV at the ICA and ECA.
For the ICA, the history of DUs was an independent predictor of higher PSV (β=33.72, p=0.002). Traditional cardiovascular risk factors were not significant. In the ECA model, age predicted lower PSV (β=-1.37, p=0.022), while ASCVD risk score had a borderline positive association (β=2.22, p=0.06). DUs were not a significant determinants.
Secondly, in binary logistic regression model employing plaques at any site as dependent variable, revealed that both SBP and DUs were significantly associated with plaque presence (adjusted OR 1.09, p=0.019; adjusted OR 2.25, p=0.015, respectively). [Figure 4] Other included variables were age, sex, BMI, Framingham and ASCVD risk scores, LDL/HDL ratio, which failed to prove associations.
4. Discussion
Our study provided evidence on the relationship between microvascular damage and macrovascular impairment in SSc from a peculiar clinical standpoint. Previous evidence have underscored that SSc patients exhibit increased cardiovascular mortality compared to healthy controls, and cardiac alterations can also be found in milder form of the disease despite a lower prevalence of traditional cardiovascular risk factors across these populations [37,38]. In fact, cardiovascular mortality in SSc is estimated to be attributable to atherosclerotic events in up to 29% of cases, according to EUSTAR data, signifying a shift from SSc-specific causes (e.g., renal crisis, pulmonary hypertension) towards more generalized vascular complications. [39,40,41]
Various studies have tried to define SSc-related features which best contribute to macrovascular impairment and cardiovascular events prediction. For instance, a study of Caimmi et al, analyzing with ultrasound different medium-large vessels beds, such as carotid, upper and lower limbs arteries, revealed association with Forced Vital Capacity, Diffusing Capacity of the lungs for Carbon Monoxide, limited cutaneous SSc and calcinosis in defining macrovascular impairment [42]. In this context, a peculiar interest has gained by the potential interconnection between microvascular changes, defined as per the late NVC pattern or reduced capillary density, and altered endothelial function detected with flow mediated vasodilatation at brachial arteries and arterial stiffness [12].
However, from a clinical standpoint, controversial data are reported in literature regarding the role of digital ulcers in predicting the macrovascular impairment of SSc patients. A study on a large Japanese SSc cohort lacked to demonstrate the association with DUs and atherosclerotic plaque formation, on the other hand, data becoming from GIRRCS study emphasized the role of DUs as independent predictor of overt clinical atherosclerosis, lacking confirmation on subclinical atherosclerotic changes [13,43]. In light of this dichotomy and by selecting DUs as a clinical surrogate of severe vasculopathy in SSc, we confirmed a greater prevalence of atherosclerotic plaques, especially at left carotid and bilaterally in our population reporting a history of DUs.
Moreover, although increased cIMT has long been recognized as a marker of cardiovascular morbidity and mortality, our findings suggest that it alone may not suffice to stratify vascular risk in SSc patients [44]. Previous studies by Bartoli et al., Soltesz et al., and more recently by Sedky Abdou et al., have reported significantly increased cIMT in SSc patients compared to healthy controls, consistent with early arterial rearrangement toward increased stiffness. However, these changes do not always correlate with plaque presence or Doppler hemodynamic indices [45,46,47].
To clarify, in our analysis only a few plaques determined hemodynamic significant alterations of the interested vascular beds, pointing to the presence of subclinical atheromatous process at this level. Moreover, this was elucidated by the comparable values of bilateral cIMT between the two groups, failing to reach the standardized cut-off of 0.9 mm indicative atherosclerotic process. This observation suggests that cIMT alone is not capable of defining plaque formation. This aligns with previous findings of Frerix et al. who demonstrated discordance between plaque burden and cIMT in both SSc and systemic lupus erythematosus (SLE), suggesting that plaque formation may occur independently of intima-media thickening [48]. Moreover, Schiopu’s work noted increased expression of serum proteins, including IL-2, IL-6, CRP, keratinocyte growth factor, intercellular adhesion molecule 1, endoglin, plasminogen activator inhibitor 1 and insulin-like growth factor binding protein 3 associated with carotid plaque in SSc population. While, myeloid progenitor inhibitory factor 1, serum amyloid A, thrombomodulin, N-terminal pro-brain natriuretic peptide (BNP), and Clara cell secretory protein 16 kD correlated with cIMT. Notably, these molecules are implicated in both fibrosis and vasculopathy process, highlighting the presence of other SSc related intrinsic mechanisms at play. [49]
Supporting this, Doppler findings in our cohort revealed that peak systolic velocities in the ICA and ECA were increased in DUs patients, even though these values remained below clinical thresholds. Elevated PSV, alongside increased RI, particularly in the ICA, suggest reduced arterial compliance to distal resistance, even in the absence of critical stenosis. This observation reinforces the hypothesis that macrovascular impairment in SSc stems from a dual pathogenic origin: one is established by the classical atherosclerosis, and the other is the SSc-specific fibrotic vasculopathy. Remarkably, the observed increase in PSV, not paralleled by changes in EDV, points to a mechanism beyond simple luminal narrowing due to atherosclerosis, as increases in EDV are exclusively reported in proximity to atherosclerotic plaques [50].
Definitively, the history of DUs might sort a proactive effect on determining these hemodynamics alterations occurring at most distal branches of carotid instead of CCA, which may reflect functional vessel stiffening and precedes clinically overt atherosclerosis or ischemic events.
Nevertheless, as demonstrated by Cannarile et al, traditional risk factors may not be sufficient in defining the risk of overt cardiovascular events, nor they seem to be associated with subtle atheromatous processes in SSc patients. Endothelial cell injury induced by anti-endothelial antibodies, ischemia/reperfusion damage, immune-mediated cytotoxicity represent the main causes of vascular injury together with an impaired vascular repair mechanism that determine a defective vasculogenesis [51].
Our research revealed that in DUs patients, despite the presence of macrovascular alterations, no differences in classical cardiometabolic risk factors were found. Parameters such as the atherogenic index of plasma, TyG, HOMA-IR, and lipid ratios (TG/HDL and LDL/HDL) were similar between the groups, as were rates of hypertension, diabetes, smoking, and dyslipidemia. DUs patients had higher cardiovascular risk as estimated by the Framingham score, but not by the ASCVD risk estimator. These discrepancies point to the inadequacy of traditional cardiovascular risk models in capturing the unique vascular pathology of SSc, where fibrosis-induced vessel remodeling may drive cardiovascular morbidity independently of general population based factors [52].
Furthermore, the paradox of increased plaque burden and cardiovascular mortality in the absence of classic metabolic derangement suggests a need to redefine cardiovascular screening in SSc. Carotid ultrasound and Doppler assessments emerge as valuable tools in clinical practice. Sanz Perez I et al. found that carotid ultrasound and coronary artery calcium (CAC) scoring were more effective in detecting subclinical atherosclerosis in SSc than conventional risk charts [53]. While they did not find disease-related factors associated with plaque formation, our findings indicate that DUs may serve as a useful marker of underlying systemic vasculopathy, as demonstrated by their power in predicting both PSV and plaque presence at multivariate analysis.
Our study presents several strengths. Firstly, the comprehensive evaluation of both microvascular (DUs and NVC) and macrovascular (carotid ultrasound, Doppler hemodynamics, and cIMT) parameters within the same cohort allowed for an integrated assessment of vascular pathology from a real-life clinical perspective. Second, the rigorous ultrasound methodology applied, with blinded dual-operator assessments improving the reliability of imaging data and minimizing operator bias.
Despite these strengths, certain limitations must be acknowledged. The cross-sectional design of the study inherently restricts causal inferences regarding the temporal relationship between microvascular damage, macrovascular impairment, and cardiovascular events. Longitudinal follow-up would be necessary to clarify whether the observed vascular changes predict future cardiovascular morbidity and mortality in SSc. Moreover the monocentric recruitment could limit the generalizability of this findings.
Furthermore, the lack of standardized cut-off values for Doppler indices in SSc populations adds complexity to interpreting results and comparing findings across different studies, future efforts should aim to elucidate common accepted thresholds in this cohort.
5. Conclusions
In conclusion, the data supports the concept that macrovascular disease in SSc arises from both atherosclerotic and fibrotic mechanisms. Traditional cardiovascular risk scores and metabolic parameters fail to account for this vascular burden, emphasizing the need for SSc-specific vascular assessment strategies. Incorporating DU status and non-invasive vascular imaging into routine clinical practice could allow earlier identification of patients at elevated risk, opening a window for timely preventive interventions and potentially improving cardiovascular outcomes in this high-risk population.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Medication Usage.
Author Contributions
E.C.: Conceptualization, Software, Methodology, Validation, Formal analysis, Investigation, Resources, Data curation, Writing – original draft. F.L.: Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation. Writing – original draft. L.C.: Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation. E.Z.: Resources, Data curation, Writing – original draft. C.G.M.: Resources. Data curation. F.C.: Resources. Data curation. D.B.: Resources. Data curation. L.C.: Resources. Data curation. A.T.: Resources. Data curation. M.I.: Methodology. M.S.C.: Methodology. P.F.: Conceptualization, Validation, Resources, Writing – review & editing, Supervision. A.M.: Conceptualization, Validation, Resources, Supervision Writing – review & editing, Supervision. Project administration.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Milan Area 3.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request. The data is not publicly available due to ethical restrictions.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 95%CI | 95% Confidence Interval |
| ACA | Anti-Centromere Antibodies |
| ACC/AHA | American College of Cardiology / American Heart Association |
| ACEis | Angiotensin-Converting Enzyme Inhibitors |
| ACR/EULAR | American College of Rheumatology / European League Against Rheumatism |
| AIP | Atherogenic Index of Plasma |
| ARA | Anti-RNA Polimerase III Antibodies |
| ARBs | Angiotensin II Receptor Blockers |
| ASCVD | Atherosclerotic Cardiovascular Disease |
| ASST | Azienda Socio-Sanitaria Territoriale |
| β-coeff. | Beta Coefficient |
| β-stand | Standardized Beta Coefficient |
| BMI | Body Mass Index |
| BSA | Body Surface Area |
| CCA | Common Carotid Artery |
| CCBs | Calcium Channel Blockers |
| cIMT | Carotid Intima-Media Thickness |
| cMRI | Cardiac Magnetic Resonance Imaging |
| CRP | C-Reactive Protein |
| DBP | Diastolic Blood Pressure |
| DUs | Digital Ulcers |
| ECA | External Carotid Artery |
| EDV | End-Diastolic Velocity |
| ERAs | Endothelin Receptor Antagonists |
| GIRRCS | Gruppo Italiano per la Ricerca e la Ricerca Clinica sulla Sclerodermia |
| HDL | High-Density Lipoprotein |
| HOMA-IR | Homeostatic Model Assessment of Insulin Resistance |
| HR | Heart Rate |
| HRCT | High-Resolution Computed Tomography |
| hs-TnT | High-Sensitivity Troponin T |
| ICA | Internal Carotid Artery |
| ILD | Interstitial Lung Disease |
| IMT | Intima-Media Thickness |
| IQR | Interquartile Range |
| LDL | Low-Density Lipoprotein |
| mRSS | Modified Rodnan Skin Score |
| NASCET | North American Symptomatic Carotid Endarterectomy Trial |
| NT-proBNP | N-terminal pro Brain Natriuretic Peptide |
| NVC | Nailfold Videocapillaroscopy |
| PAH | Pulmonary Arterial Hypertension |
| PDE5i | Phosphodiesterase Type 5 Inhibitors |
| PSV | Peak Systolic Velocity |
| RI | Resistive Index |
| RP | Raynaud’s Phenomenon |
| SBP | Systolic Blood Pressure |
| Scl-70 | Anti-Topoisomerase I Antibodies |
| SSc | Systemic Sclerosis |
| TG | Triglycerides |
| Tyg | Triglyceride-Glucose Index |
| VEDOSS | Very Early Diagnosis of Systemic Sclerosis |
References
- Mok, M.Y.; Lau, C.S. The burden and measurement of cardiovascular disease in SSc. Nat. Rev. Rheumatol. 2010, 6, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Keret, S.; Rimar, D.; Lansiaux, P.; Feldman, E.; Lescoat, A.; Milman, N.; Farge, D.; MATHEC working group. Differentially expressed genes in systemic sclerosis: Towards predictive medicine with new molecular tools for clinicians. Autoimmun. Rev. 2023, 22, 103314. [Google Scholar] [CrossRef] [PubMed]
- Bandini, G.; Randone, S.B.; Manetti, M.; Dagna, L.; Cerinic, M.M.; Pignone, A.M. Endotheliopathy in systemic sclerosis: from endothelium-dependent vasodilation to the dysfunction of the vascular reserve, is the paradise lost? Arthritis Res. Ther. 2025, 27, 107. [Google Scholar] [CrossRef]
- Lescoat, A. Very Early Diagnosis of Systemic Sclerosis: Deciphering the heterogeneity of systemic sclerosis in the very early stages of the disease. J. Scleroderma Relat. Disord. 2023, 8, 3–6. [Google Scholar] [CrossRef]
- Xu, D.; Li, M.-T.; Hou, Y.; Wang, Q.; Hu, C.-J.; Song, N.; Zhao, J.-L.; Zeng, X.-F.; Zhang, F.-C. Clinical characteristics of systemic sclerosis patients with digital ulcers in China. Clin Exp Rheumatol. 2013, 31, 46–9. [Google Scholar]
- Mouthon, L.; Mestre-Stanislas, C.; Bérezné, A.; Rannou, F.; Guilpain, P.; Revel, M.; Pagnoux, C.; Guillevin, L.; Fermanian, J.; Poiraudeau, S. Impact of digital ulcers on disability and health-related quality of life in systemic sclerosis. Ann. Rheum. Dis. 2010, 69, 214–217. [Google Scholar] [CrossRef] [PubMed]
- Mihai, C.; Distler, O.; Gheorghiu, A.M.; I Constantin, P.; Dobrota, R.; Jordan, S.; Smith, V.; Hachulla, E.; Henes, J.; Siegert, E.; et al. Incidence and risk factors for gangrene in patients with systemic sclerosis from the EUSTAR cohort. Rheumatology 2019, 59, 2016–2023. [Google Scholar] [CrossRef]
- Patnaik, E.; Lyons, M.; Tran, K.; Pattanaik, D. Endothelial Dysfunction in Systemic Sclerosis. Int. J. Mol. Sci. 2023, 24, 14385. [Google Scholar] [CrossRef]
- McMahan ZH, Wigley FM. Raynaud's phenomenon and digital ischemia: a practical approach to risk stratification, diagnosis and management. Int J Clin Rheumtol. 2010, 5, 355–370. [Google Scholar] [CrossRef]
- Edjlali-Goujon, M.; Alison, D.; Technologique, C.H.R.E.U.T.C.D. Acute Digital Ischaemia – What the Radiologist Needs to Know. Eur. Cardiol. Rev. 2011, 7. [Google Scholar] [CrossRef]
- Pahwa R, Jialal I. Atherosclerosis. StatPearls Publishing. 2025.
- Rollando, D.; Bezante, G.P.; Sulli, A.; Balbi, M.; Panico, N.; Pizzorni, C.; Negrini, S.; Brunelli, C.; Barsotti, A.; Cutolo, M.; et al. Brachial Artery Endothelial-dependent Flow-mediated Dilation Identifies Early-stage Endothelial Dysfunction in Systemic Sclerosis and Correlates with Nailfold Microvascular Impairment. J. Rheumatol. 2010, 37, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Liakouli, V.; Verde, I.; Ruscitti, P.; Di Vico, C.; Ruggiero, A.; Mauro, D.; Forte, G.; Navarini, L.; Di Donato, S.; Bearzi, P.; et al. Clinical and subclinical atherosclerosis in patients with systemic sclerosis: an observational, multicentre study of GIRRCS (Gruppo Italiano di Ricerca in Reumatologia Clinica e Sperimentale). Clin. Exp. Rheumatol. 2024, 42, 1645–1655. [Google Scholar] [CrossRef] [PubMed]
- Bedi, R.; Nagra, A.; Fukumoto, T.; Lynum, S.; Sengupta, P.; Aw, J.; Mefford, I.; Panwar, S.R.; Bansal, N.; Insaan, P.; et al. Detection of Subclinical Atherosclerosis in Peripheral Arterial Beds With B-Mode Ultrasound: A Proposal for Guiding the Decision for Medical Intervention and an Artifact-Corrected Volumetric Scoring Index. Glob. Hear. 2014, 9, 367–378. [Google Scholar] [CrossRef]
- Chen LY, Leening MJ, Norby FL, Roetker NS, Hofman A, Franco OH, Pan W, Polak JF, Witteman JC, Kronmal RA, Folsom AR, Nazarian S, Stricker BH, Heckbert SR, Alonso A. Carotid Intima-Media Thickness and Arterial Stiffness and the Risk of Atrial Fibrillation: The Atherosclerosis Risk in Communities (ARIC) Study, Multi-Ethnic Study of Atherosclerosis (MESA), and the Rotterdam Study. J Am Heart Assoc. 2016 ;5(5):e002907.
- Bill, O.; Mazya, M.V.; Michel, P.; Moreira, T.P.; Lambrou, D.; Meyer, I.A.; Hirt, L. Intima-Media Thickness and Pulsatility Index of Common Carotid Arteries in Acute Ischaemic Stroke Patients with Diabetes Mellitus. J. Clin. Med. 2022, 12, 246. [Google Scholar] [CrossRef]
- Morales, M.M.; Anacleto, A.; Filho, C.M.; Ledesma, S.; Aldrovani, M.; Wolosker, N. Peak Systolic Velocity for Calcified Plaques Fails to Estimate Carotid Stenosis Degree. Ann. Vasc. Surg. 2019, 59, 1–4. [Google Scholar] [CrossRef]
- Alexandrov, A.V.; Tsivgoulis, G.; Rubiera, M.; Vadikolias, K.; Stamboulis, E.; Molina, C.A. End-Diastolic Velocity Increase Predicts Recanalization and Neurological Improvement in Patients With Ischemic Stroke With Proximal Arterial Occlusions Receiving Reperfusion Therapies. Stroke 2010, 41, 948–952. [Google Scholar] [CrossRef]
- Delong C, Sharma S. Physiology, Peripheral Vascular Resistance. StatPearls Publishing; 2025 Jan.
- van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, Matucci-Cerinic M, Naden RP, Medsger TA Jr, Carreira PE, Riemekasten G, Clements PJ, Denton CP, Distler O, Allanore Y, Furst DE, Gabrielli A, Mayes MD, van Laar JM, Seibold JR, Czirjak L, Steen VD, Inanc M, Kowal-Bielecka O, Müller-Ladner U, Valentini G, Veale DJ, Vonk MC, Walker UA, Chung L, Collier DH, Ellen Csuka M, Fessler BJ, Guiducci S, Herrick A, Hsu VM, Jimenez S, Kahaleh B, Merkel PA, Sierakowski S, Silver RM, Simms RW, Varga J, Pope JE. 2013 classification criteria for systemic sclerosis: an American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis. 2013 Nov;72(11):1747-55.
- Khanna, D.; Furst, D.E.; Clements, P.J.; Allanore, Y.; Baron, M.; Czirjak, L.; Distler, O.; Foeldvari, I.; Kuwana, M.; Matucci-Cerinic, M.; et al. Standardization of the Modified Rodnan Skin Score for Use in Clinical Trials of Systemic Sclerosis. J. Scleroderma Relat. Disord. 2017, 2, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Cerinic, M.M. Nailfold capillaroscopy and classification criteria for systemic sclerosis. Clin Exp Rheumatol. 2007 Sep-Oct;25(5):663-5.
- Rehman S, Hashmi MF. Blood Pressure Measurement. StatPearls Publishing; 2025 Jan.
- Hemann, B.A.; Bimson, W.F.; Taylor, A.J. The Framingham Risk Score: An Appraisal of Its Benefits and Limitations. Am. Hear. Hosp. J. 2007, 5, 91–96. [Google Scholar] [CrossRef]
- Duttagupta, S.; Thachathodiyl, R.; Rameshan, A.; Venkatachalam, A.; Georgy, S.; Ts, D.; Menon, J. Effectiveness of Framingham and ASCVD Risk Scores in Predicting Coronary Artery Disease - A Comparative Study with Syntax Score. . 2022, 69, 11–12. [Google Scholar]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2023, 147, e674. [Google Scholar] [CrossRef]
- Sun, Y.; Ji, H.; Sun, W.; An, X.; Lian, F. Triglyceride glucose (TyG) index: A promising biomarker for diagnosis and treatment of different diseases. Eur. J. Intern. Med. 2024, 131, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Millán J, Pintó X, Muñoz A, Zúñiga M, Rubiés-Prat J, Pallardo LF, Masana L, Mangas A, Hernández-Mijares A, González-Santos P, Ascaso JF, Pedro-Botet J. Lipoprotein ratios: Physiological significance and clinical usefulness in cardiovascular prevention. Vasc Health Risk Manag. 2009;5:757-65. Epub 2009 Sep 18. PMID: 19774217; PMCID: PMC2747394. [PubMed]
- Babic, N.; Valjevac, A.; Zaciragic, A.; Avdagic, N.; Zukic, S.; Hasic, S. The Triglyceride/HDL Ratio and Triglyceride Glucose Index as Predictors of Glycemic Control in Patients with Diabetes Mellitus Type 2. Med Arch. 2019, 73, 163–168. [Google Scholar] [CrossRef]
- Onat A, Can G, Kaya H, Hergenç G. "Atherogenic index of plasma" (log10 triglyceride/high-density lipoprotein-cholesterol) predicts high blood pressure, diabetes, and vascular events. J Clin Lipidol. 2010 Mar-Apr;4(2):89-98.
- Majid, H.; Masood, Q.; Khan, A.H. Homeostatic Model Assessment for Insulin Resistance (HOMA-IR): A Better Marker for Evaluating Insulin Resistance Than Fasting Insulin in Women with Polycystic Ovarian Syndrome. . 2017, 27, 123–126. [Google Scholar]
- Seekircher, L.; Tschiderer, L.; Lind, L.; Safarova, M.S.; Kavousi, M.; Ikram, M.A.; Lonn, E.; Yusuf, S.; E Grobbee, D.; Kastelein, J.J.P.; et al. Intima-media thickness at the near or far wall of the common carotid artery in cardiovascular risk assessment. Eur. Hear. J. Open 2023, 3, oead089. [Google Scholar] [CrossRef] [PubMed]
- Touboul, P.-J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez, R.H.; et al. Mannheim Carotid Intima-Media Thickness and Plaque Consensus (2004–2006–2011). Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [CrossRef]
- Valaikiene, J.; Schuierer, G.; Ziemus, B.; Dietrich, J.; Bogdahn, U.; Schlachetzki, F. Transcranial Color-Coded Duplex Sonography for Detection of Distal Internal Carotid Artery Stenosis. Am. J. Neuroradiol. 2008, 29, 347–353. [Google Scholar] [CrossRef]
- North American Symptomatic Carotid Endarterectomy Trial Collaborators; Barnett HJM, Taylor DW, Haynes RB, Sackett DL, Peerless SJ, Ferguson GG, Fox AJ, Rankin RN, Hachinski VC, Wiebers DO, Eliasziw M. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991 Aug 15;325(7):445-53.
- Grant, E.G.; Benson, C.B.; Moneta, G.L.; Alexandrov, A.V.; Baker, J.D.; Bluth, E.I.; Carroll, B.A.; Eliasziw, M.; Gocke, J.; Hertzberg, B.S.; et al. Carotid Artery Stenosis: Gray-Scale and Doppler US Diagnosis—Society of Radiologists in Ultrasound Consensus Conference. Radiology 2003, 229, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Jones, X.M.; Bottini, N.; Boin, F.; Marbán, E. Cardiac involvement in systemic sclerosis: A critical review of knowledge gaps and opportunities. J. Scleroderma Relat. Disord. 2025, 10, 91–100. [Google Scholar] [CrossRef]
- Capparelli, E.; Zaccara, E.; Suardi, I.; Laria, A.; Castelnovo, L.; Mauric, E.; Bompane, D.; Tamburello, A.; Iacovantuono, M.; Chimenti, M.S.; et al. Uncovering Subclinical Cardiac Involvement in VEDOSS: An Echocardiographic Driven Study. Sclerosis 2025, 3, 7. [Google Scholar] [CrossRef]
- Sherif, A.A.; Gilvaz, V.J.; Abraham, S.; Saji, A.M.; Mathew, D.; Isath, A.; Rajendran, A.; Contreras, J.; Lanier, G.M.; Reginato, A.M. Systemic sclerosis is associated with increased in-patient mortality in patients hospitalized for heart failure. ESC Hear. Fail. 2024, 11, 1900–1910. [Google Scholar] [CrossRef]
- Tyndall, A.J.; Bannert, B.; Vonk, M.; Airò, P.; Cozzi, F.; Carreira, P.E.; Bancel, D.F.; Allanore, Y.; Müller-Ladner, U.; Distler, O.; et al. Causes and risk factors for death in systemic sclerosis: a study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann. Rheum. Dis. 2010, 69, 1809–1815. [Google Scholar] [CrossRef]
- Györfi, A.; Filla, T.; Polzin, A.; Tascilar, K.; Buch, M.; Tröbs, M.; Matei, A.; Airo, P.; Balbir-Gurman, A.; Kuwert, F.; et al. Evaluation of Systemic Sclerosis Primary Heart Involvement and Chronic Heart Failure in the European Scleroderma Trials and Research Cohort. J. Am. Hear. Assoc. 2025, 14, e036730. [Google Scholar] [CrossRef] [PubMed]
- Caimmi, C.; De Marchi, S.; Bosello, S.L.; Giuggioli, D.; Caramaschi, P.; Di Giorgio, A.; Spinella, A.; Astorino, G.; Canestrari, G.; Cocchiara, E.; et al. Ultrasonography involvement of carotid, upper and lower limb arteries in a large cohort of systemic sclerosis patients. Int. J. Rheum. Dis. 2020, 23, 681–692. [Google Scholar] [CrossRef]
- Motegi, S.; Toki, S.; Hattori, T.; Yamada, K.; Uchiyama, A.; Ishikawa, O. No association of atherosclerosis with digital ulcers in Japanese patients with systemic sclerosis: Evaluation of carotid intima-media thickness and plaque characteristics. J. Dermatol. 2014, 41, 604–608. [Google Scholar] [CrossRef]
- Sayan M, Raaj KB, Hooijenga P, Cassidy S, Nova A, De Ciutiis I, Wang T, Kroeger CM, Stamatakis E, Masedunskas A, De Caterina R, Cagigas ML, Fontana L, Carotid intima-media thickness, cardiovascular disease, and risk factors in 29,000 UK Biobank adults, American Journal of Preventive Cardiology. 2025. Volume 22.
- Bartoli, F.; Blagojevic, J.; Bacci, M.; Fiori, G.; Tempestini, A.; Conforti, M.L.; Guiducci, S.; Miniati, I.; DI Chicco, M.; DEL Rosso, A.; et al. Flow-Mediated Vasodilation and Carotid Intima-Media Thickness in Systemic Sclerosis. Ann. New York Acad. Sci. 2007, 1108, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Sedky Abdou MM, El Desouky SM, Helmy El Kaffas KM, Ahmed Hassan AM. Premature atherosclerosis in systemic sclerosis patients: Its relation to disease parameters and to traditional risk factors. Int J Rheum Dis. 2017 Mar;20(3):383-389.
- Soltész, P.; Kerekes, G.; Dér, H.; Szücs, G.; Szántó, S.; Kiss, E.; Bodolay, E.; Zeher, M.; Timár, O.; Szodoray, P.; et al. Comparative assessment of vascular function in autoimmune rheumatic diseases: Considerations of prevention and treatment. Autoimmun. Rev. 2011, 10, 416–425. [Google Scholar] [CrossRef]
- Frerix, M.; Stegbauer, J.; Kreuter, A.; Weiner, S.M. Atherosclerotic plaques occur in absence of intima-media thickening in both systemic sclerosis and systemic lupus erythematosus: a duplexsonography study of carotid and femoral arteries and follow-up for cardiovascular events. Arthritis Res. Ther. 2014, 16, R54–R54. [Google Scholar] [CrossRef]
- Schiopu, E.; Au, K.M.; McMahon, M.A.; Kaplan, M.J.; Divekar, A.; Singh, R.R.; Furst, D.E.; Clements, P.J.; Ragvendra, N.; Zhao, W.; et al. Prevalence of subclinical atherosclerosis is increased in systemic sclerosis and is associated with serum proteins: a cross-sectional, controlled study of carotid ultrasound. Rheumatology 2014, 53, 704–713. [Google Scholar] [CrossRef]
- Strosberg DS, Haurani MJ, Satiani B, Go MR. Common carotid artery end-diastolic velocity and acceleration time can predict degree of internal carotid artery stenosis. J Vasc Surg. 2017 Jul;66(1):226-231.
- Cannarile F, Valentini V, Mirabelli G, Alunno A, Terenzi R, Luccioli F, Gerli R, Bartoloni E. Cardiovascular disease in systemic sclerosis. Ann Transl Med. 2015 Jan;3(1):8.
- Oreska, S.; Tomcik, M. Atherosclerosis and Cardiovascular Risk in Systemic Sclerosis. Systemic Sclerosis. InTech; 2017.
- Sanz Pérez I, Martínez Valle F, Guillén-Del-Castillo A, Roque Pérez A, Cuéllar Calàbria H, Pizzi MN, Fernández Codina A, Callejas-Moraga E, Orozco Gálvez O, Fonollosa Pla V, Simeón Aznar CP. Subclinical cardiovascular disease and Systemic Sclerosis: A comparison between risk charts, quantification of coronary calcium and carotid ultrasonography. Autoimmun Rev. 2018 Sep;17(9):900-905.
Figure 1.
Box plot showing differences between DU- and DU+ patients on ASCVD Risk Score and Framingham risk scores. Acronyms. DU=Digital Ulcers; ASCVD=Atherosclerotic Cardiovascular Disease.
Figure 1.
Box plot showing differences between DU- and DU+ patients on ASCVD Risk Score and Framingham risk scores. Acronyms. DU=Digital Ulcers; ASCVD=Atherosclerotic Cardiovascular Disease.
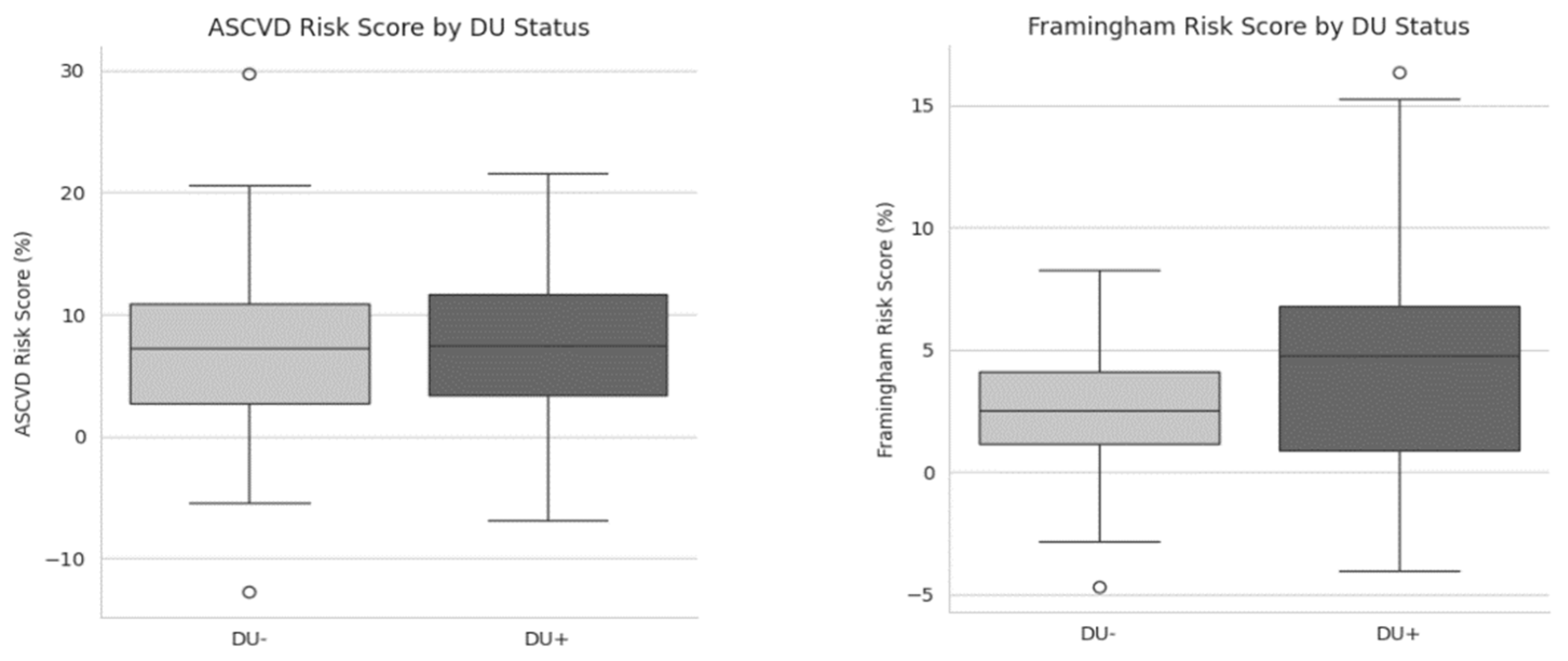
Figure 2.
Atherosclerotic plaques distribution according to the side. Acronyms. DU=Digital Ulcers.
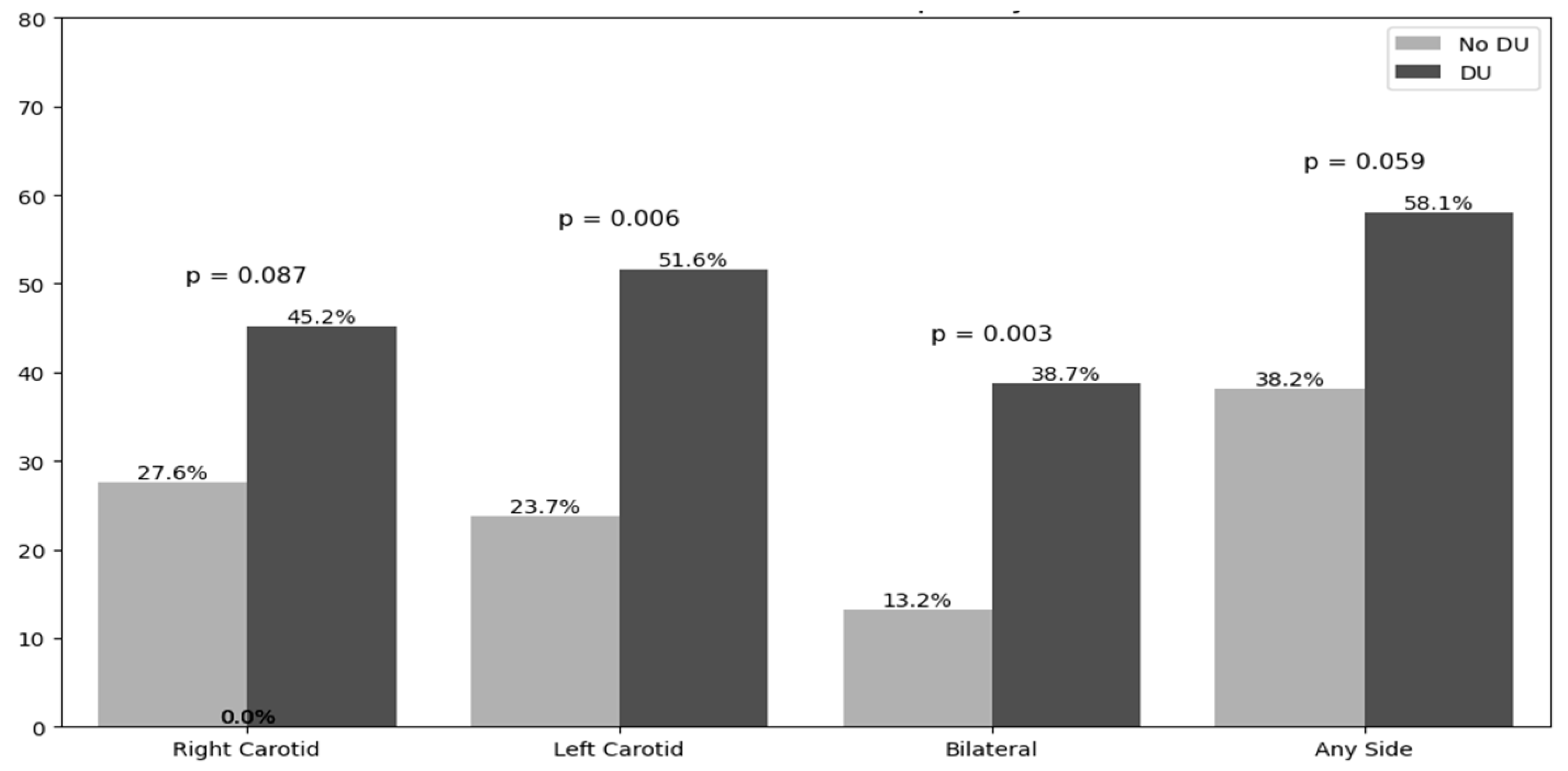
Figure 3.
Bar chart on atherosclerotic plaques localization on both sides of carotid arteries. Acronyms. DU=Digital Ulcers; ICA=Internal Carotid Artery.
Figure 3.
Bar chart on atherosclerotic plaques localization on both sides of carotid arteries. Acronyms. DU=Digital Ulcers; ICA=Internal Carotid Artery.
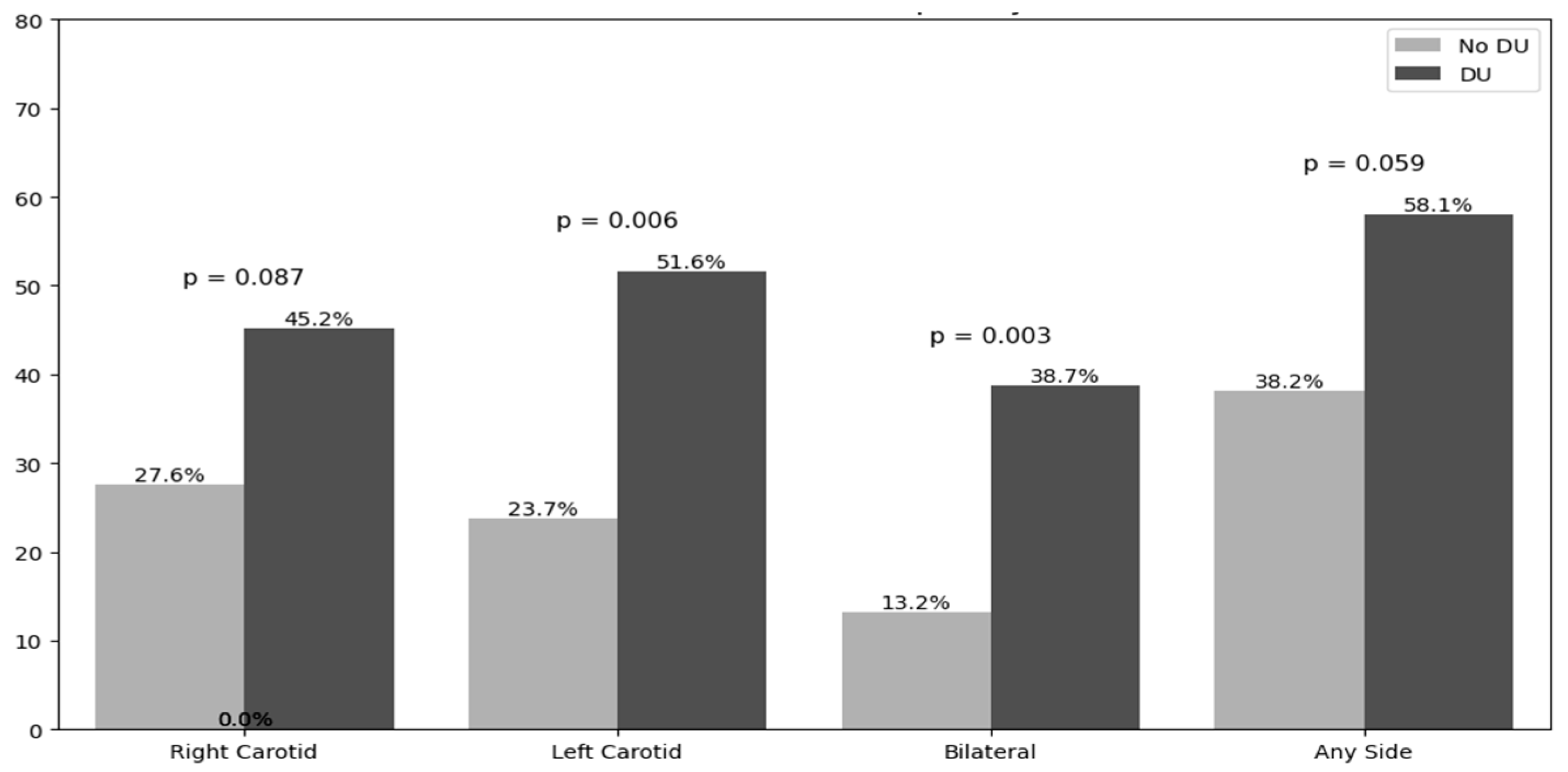
Figure 4.
Binary logistic regression with adjusted OR with “plaques at any side” was considered as dependent variable. Acronyms. PSV=Peak Systolic Velocity; ICA=Internal Carotid Artery; ECA=External Carotid Artery; β-Coeff.= Beta-coefficient; β -stand.=Beta-standardized coefficient; CI=Confidence interval; p= p-value; BMI=Body Mass Index; CRP=C-Reactive Protein; SBP=Systolic Blood Pressure; LDL=Low-density lipoprotein; HDL=High-density lipoprotein; ASCVD= Atherosclerotic Cardiovascular Disease.
Figure 4.
Binary logistic regression with adjusted OR with “plaques at any side” was considered as dependent variable. Acronyms. PSV=Peak Systolic Velocity; ICA=Internal Carotid Artery; ECA=External Carotid Artery; β-Coeff.= Beta-coefficient; β -stand.=Beta-standardized coefficient; CI=Confidence interval; p= p-value; BMI=Body Mass Index; CRP=C-Reactive Protein; SBP=Systolic Blood Pressure; LDL=Low-density lipoprotein; HDL=High-density lipoprotein; ASCVD= Atherosclerotic Cardiovascular Disease.
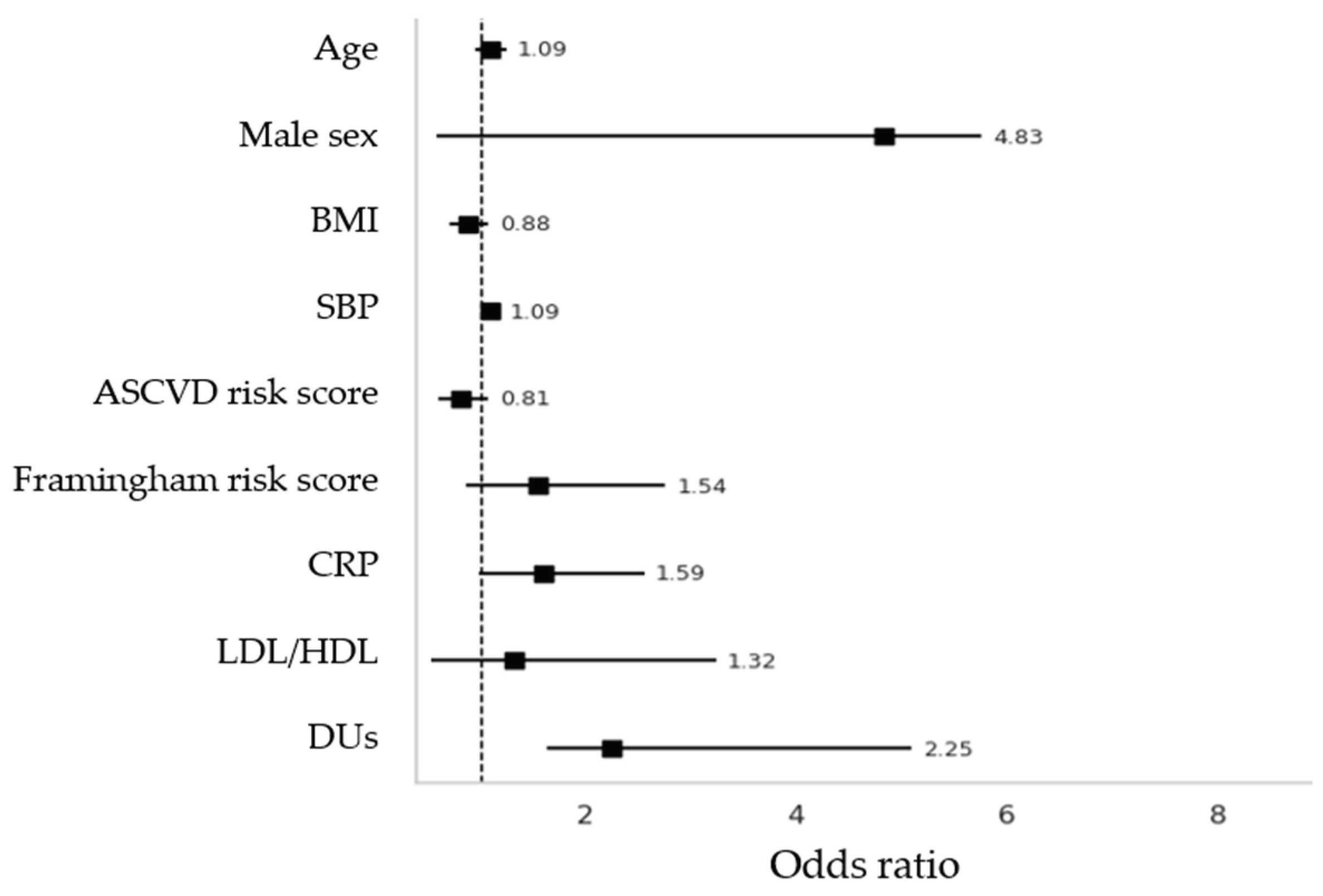

Table 1.
Clinical Characteristics.
| Non-DUs n=76 |
DUs n=31 |
p-value | |
|---|---|---|---|
| Female, n/% | 73 / 96.1 | 22 / 71 | <0.001 |
| Age at enrollment, mean±SD | 61.85±12.4 | 58.8±12.7 | 0.254 |
| Age at diagnosis, mean±SD | 49.9±13.2 | 43.4±15.2 | 0.041 |
| Disease Duration, mean±SD | 68.4±335.6 | 15.0±9 | 0.396 |
| Body Mass Index, (Kg/m2), mean±SD | 23.1±4.7 | 23.4±4.2 | 0.813 |
| Body Surface Area, (m2), mean±SD | 1.64±0.18 | 1.69±0.21 | 0.204 |
| Anti-centromere, n/% | 42 / 55.3 | 12 / 38.7 | 0.138 |
| Anti-Scl70, n/% | 6 / 7.9 | 11 / 35.5 | 0.001 |
| Anti-RNA polimerase III, n/% | 1 / 1.3 | 2 / 6.5 | 0.144 |
| Current Smokers, n/% | 17 / 22.4 | 8 / 25.8 | 0.703 |
| mRSS at last follow up, mean±SD | 2.1±2.3 | 8.5±8.4 | <0.001 |
| LEROY CLASSIFICATION, n/% | |||
| Sine scleroderma | 26 / 34.2 | 2 / 6.5 | 0.001 |
| Limitate | 49 / 64.5 | 17 / 54.8 | 0.001 |
| Diffuse | 1 / 1.3 | 12 / 38.7 | 0.001 |
| NVC pattern, n/% | |||
| Early/active | 58 / 76.3 | 14 / 45.2 | 0.002 |
| Late | 18 / 23.7 | 17 / 54.8 | 0.002 |
| Clinical Manifestations, n/% | |||
| Puffy hands | 60 / 78.9 | 16 / 51.6 | 0.005 |
| Current Digital Ulcers | 0 | 6 / 20 | <0.001 |
| Teleangctasias | 30 / 39.5 | 23 / 74.2 | 0.001 |
| Pitting scars | 16 / 21.1 | 25 / 80.6 | <0.001 |
| Sclerodactily | 33 / 43.4 | 26 / 83.9 | 0.001 |
| Clacinosis | 10 / 13.2 | 12 / 38.7 | 0.003 |
| Friction Rubs | 0 | 4 / 12.9 | 0.001 |
| Arthritis | 24 / 31.6 | 12 / 38.7 | 0.479 |
| Upper GI Involvement | 43 / 56.6 | 25 / 80.6 | 0.019 |
| Lower GI Involvement | 17 / 22.7 | 8 / 25.8 | 0.729 |
| Microstomia | 15 / 19.7 | 17 / 54.8 | <0.001 |
| Scleroderma Renal Crisis | 1 / 1.3 | 1 / 3.2 | 0.508 |
| Cardiomyopathy | 0 | 1 / 3.2 | 0.116 |
| Pulmonary Arterial Hypertension | 1 / 1.3 | 1 / 3.2 | 0.508 |
| Interstitial Lung Disease | 9 / 11.8 | 15 / 48.4 | <0.001 |
Acronyms. DUs=Digital Ulcers; mRSS=Modified Rodnan skin score; NVC=Nail-fold Videocapillaroscopy; GI= Gastrointestinal.
Table 2.
Atherosclerotic risk factors and metabolic indices.
| Non-DUs n=76 |
DUs n=31 |
p-value | |
|---|---|---|---|
| Cardiovascular symptoms and related comorbidities | |||
| Angina pectoris, n/% | 4 / 5.3 | 6 / 19.4 | 0.023 |
| Dyspnoea, n/% | 10 / 13.6 | 6 / 19.4 | 0.415 |
| Cardiopalmus, n/% | 7 / 9.2 | 4 / 12.9 | 0.568 |
| Arrhytmias, n/% | 19 / 25 | 13 / 41.9 | 0.083 |
| Systemic Arterial Hypertension, n/% | 22 / 28.9 | 13 / 41.9 | 0.194 |
| Dyslipidemia, n/% | 15 / 19.7 | 9 / 29 | 0.296 |
| Type 2 Diabetes, n/% | 2 / 2.6 | 2 / 6.5 | 0.345 |
| Hyperuricemia, n/% | 1 / 1.3 | 5 / 16.1 | 0.003 |
| Metabolic Assessment, mean±SD | |||
| Total Cholesterol (mg/dl) | 188.3±41.6 | 187.4±39.1 | 0.922 |
| HDL-Cholesterol (mg/dl) | 63.9±16.5 | 60.5±16.2 | 0.342 |
| LDL-Cholesterol (mg/dl) | 115.8±31.5 | 113.3±33.8 | 0.735 |
| Tryglicerides (mg/dl) | 96.9±43.6 | 100.3±48.1 | 0.748 |
| Fasting Glucose (mg/dl) | 91.6±15.8 | 92.9±29.1 | 0.773 |
| Insulin | 17.7±26.8 | 10.9±8.8 | 0.344 |
| TyG index | 8.3±0.5 | 8.1±1.4 | 0.361 |
| c-LDL/c-HDL ratio | 2.04±1.81 | 1.94±0.69 | 0.786 |
| TG/c-HDL ratio | 1.78±1.54 | 1.73±1.09 | 0.891 |
| Atherogenic Index of Plasma | 0.16±0.27 | 0.14±0.37 | 0.712 |
| HOMA-IR Index | 3.8±8.1 | 0.8±0.7 | 0.171 |
| hs-TnT (ng/ml) | 7.9±5.9 | 10.1±11.2 | 0.325 |
| C-Reactive Protein (mg/L) | 1.8±2.2 | 2.7±2.5 | 0.068 |
| NT-proBNP, (pg/ml) | 109.3±106.6 | 139.9±122.5 | 0.202 |
| Uric Acid, (mg/dl) | 4.4±1.1 | 4.5±1.3 | 0.678 |
| 1st SBP (mmHg) | 118.02±16.4 | 121.8±14.1 | 0.334 |
| 1st DBP (mmHg) | 78.8±9.4 | 74.5±13.0 | 0.094 |
| 1st HR (bpm) | 78.9±11.9 | 75.2±10.6 | 0.203 |
| 2nd SBP (mmHg) | 122.3±17.1 | 123.1±20.4 | 0.851 |
| 2nd DBP (mmHg) | 79.8±11.3 | 76.2±9.1 | 0.194 |
| 2nd HR (bpm) | 77.6±9.8 | 75.8±15.7 | 0.541 |
| Familial CV events, n/% | 19 / 25.3 | 9 /29 | 0.694 |
| Personal CV events, n/% | 3 /4.0 | 2 / 6.5 | 0.588 |
| Framingham risk score, mean±SD | 2.9±2.9 | 4.4±4.4 | 0.048 |
| ASCVD risk score, mean±SD | 6.7±6.0 | 7.1±6.6 | 0.787 |
Acronyms. DUs=Digital Ulcers; HDL=High density lipoprotein; LDL=Low-density lipoprotein; TyG=Triglycerides-fasting glucose index; TG=Tryglicerides; HOMA-IR=Homeostasis Model Assessment- Insulin resistance; NT-proBNP=N-terminal-pro-Brain Natriuretic peptide; SBP=Systolic Blood Pressure; DBP=Diastolic Blood Pressure; HR=Heart Rate; CV=Cardiovascular; ASCVD= Atherosclerotic Cardiovascular Disease, hs-TnT=high sensitive Troponin T.
Table 4.
Doppler Ultrasonographic Hemodynamic Parameters at Carotid and Vertebral levels.
| Right scanning | Left Scanning | |||||
|---|---|---|---|---|---|---|
| Carotid-Vertebral US measurements | Non-DUs | DUs | p-value | Non-DUs | DUs | p-value |
| cIMT, mean±SD | 1.17±3.03 | 0.82±0.19 | 0.991 | 0.79±0.19 | 0.85±0.14 | 0.170 |
| Common Carotid Arteries, mean±SD | ||||||
| Peak Systolic Velocity | 56.7±18.8 | 62.5±16.9 | 0.172 | 58.7±20.3 | 64.6±21.0 | 0.205 |
| End Diastolic Velocity | 15.9±6.2 | 16.1±7.1 | 0.973 | 17.1±7.79 | 18.4±7.9 | 0.482 |
| Resistive Index | 0.72±0.06 | 0.74±0.08 | 0.070 | 0.71±0.08 | 0.72±0.06 | 0.887 |
| Internal Carotid Artery, mean±SD | ||||||
| Peak Systolic Velocity | 64.2±20.5 | 86.9±67.9 | 0.010 | 63.4±18.2 | 78.9±29.6 | 0.002 |
| End Diastolic Velocity | 21.2±8.0 | 22.4±10.4 | 0.544 | 23.2±8.5 | 28.2±23.7 | 0.129 |
| Resistive Index | 0.67±0.07 | 0.71±0.09 | 0.021 | 0.63±0.07 | 0.61±0.49 | 0.676 |
| External Carotid Artery, mean±SD | ||||||
| Peak Systolic Velocity | 75.0±24.2 | 87.7±25.3 | 0.002 | 71.7±20.1 | 86.1±24.1 | 0.003 |
| End Diastolic Velocity | 16.5±7.6 | 19.8±12.8 | 0.113 | 14.9±6.2 | 18.6±8.3 | 0.143 |
| Resistive Index | 0.77±0.08 | 0.68±0.65 | 0.654 | 0.79±0.06 | 0.79±0.07 | 0.808 |
| Vertebral Artery, mean±SD | ||||||
| Peak Systolic Velocity | 38.1±11.9 | 42.6±12.1 | 0.218 | 39.5±14.1 | 43.9±13.9 | 0.277 |
| End Diastolic Velocity | 11.6±4.9 | 12.9±5.5 | 0.230 | 13.2±8.4 | 13.6±6.4 | 0.394 |
| Resistive Index | 0.65±0.36 | 0.71±0.08 | 0.627 | 0.64±0.37 | 0.70±0.09 | 0.339 |
| Carotid Stenosis percentage, mean±SD | 25.7±14.3 | 35.6±14.9 | 0.133 | 25.0±011.1 | 27.8±15.7 | 0.547 |
| PSV ICA/CCA, mean±SD | 1.16±0.33 | 1.48±1.21 | 0.043 | 1.13±0.31 | 1.25±0.47 | 0.171 |
Acronym. DUs=Digital Ulcers; cIMT=carotid Intima-Media Thickness; ICA=Internal Carotid Artery, CCA=Common Carotid Artery.
Table 4.
Linear Regression Model Predicting Mean PSV at ICA and ECA as dependent variables (cm/sec). PSV=Peak Systolic Velocity; ICA=Internal Carotid Artery; ECA=External Carotid Artery; β-Coeff.= Beta-coefficient; β -stand.=Beta-standardized coefficient; CI=Confidence interval; p= p-value; BMI=Body Mass Index; CRP=C-Reactive Protein; AIP=Atherogenic Index of Plasma; LDL=Low-density lipoprotein; HDL=High-density lipoprotein; ASCVD= Atherosclerotic Cardiovascular Disease.
Table 4.
Linear Regression Model Predicting Mean PSV at ICA and ECA as dependent variables (cm/sec). PSV=Peak Systolic Velocity; ICA=Internal Carotid Artery; ECA=External Carotid Artery; β-Coeff.= Beta-coefficient; β -stand.=Beta-standardized coefficient; CI=Confidence interval; p= p-value; BMI=Body Mass Index; CRP=C-Reactive Protein; AIP=Atherogenic Index of Plasma; LDL=Low-density lipoprotein; HDL=High-density lipoprotein; ASCVD= Atherosclerotic Cardiovascular Disease.
| Mean PSV at ICA (dependent variable) | Mean PSV at ECA (dependent variable) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| β-Coeff. | β-stand. (95% CI) | p | β-Coeff. | β -stand. (95% CI) | p | ||||
| Constant | 120.83 | -15.75 to 257.42 | 0.082 | 142.58 | 33.16 to 252.01) | 0.012 | |||
| Age | -1.30 | -0.43 (-2.75 to 0.14) | 0.077 | -1.370 | -0.61 (-2.52 to -0.21) | 0.022 | |||
| Sex (Female) | 16.11 | 0.16 (-19.51 to 51.73) | 0.367 | 0.18 | 0.003 (-28.35 to 28.72) | 0.990 | |||
| BMI (Kg/m2) | -0.62 | -0.08 (-2.76 to 1.51) | 0.562 | -0.21 | -0,041 (-1.93 to 1.49) | 0.799 | |||
| SBP (mmHg) | 0.14 | 0.06 (-0.49 to 0.77) | 0.659 | 0.02 | 0.01 (-0.48 to 0.53) | 0.931 | |||
| CRP (mg/L) | -1.19 | -0.05 (-8.43 to 6.03) | 0.740 | 3.55 | 0.22 (-2.24 to 9.35) | 0.223 | |||
| AIP ratio | 11.32 | 0.08 (-31.48 to 54.14) | 0.597 | 5.22 | 0.05 (-29.07 to 39.52) | 0.760 | |||
| LDL/HDL ratio | 1.56 | 0.04 (-11.32 to 14.45) | 0.808 | 0.42 | 0.01 (-9.90 to 10.75) | 0.935 | |||
| Digital Ulcers | 33.71 | 0.48 (13.62 to 53.81) | 0.002 | 7.75 | 0.15 (-8.34 to 23.85) | 0.337 | |||
| Framingham Risk Score | -3.36 | -0.31 (-8.63 to 1.90) | 0.205 | -1.73 | -0.22 (-5.95 to 2.48) | 0.411 | |||
| ASCVD Risk Score | 1.63 | 0.31 (-1.25 to 4.53) | 0.261 | 2.22 | 0.58 (-0.09 to 4.54) | 0.060 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



