Submitted:
01 July 2025
Posted:
03 July 2025
Read the latest preprint version here
Abstract
Activity pattern (AP) concepts are widely used in interdisciplinary chronic pain (CP) care. It is assumed that AP can be objectively measured with accelerometry, but previous results show inconsistencies which may be attributed to methodical choices. This scoping review aims to provide insight in the process of methodical reasoning for measuring AP concepts within CP. This process comprises (1) defining the concept, (2) its operationalization with variables and indicators, (3) measurement properties and data processing and (4) interpreting results. Five databases were searched for full-text publications from inception to November 2024 and publications were included when AP were measured with triaxial accelerometers for at least five consecutive days in adults with primary musculoskeletal CP. The searches yielded 11648 papers. Fifteen papers were included and summarized in three tables: 1. Study characteristics, 2. Concepts, definitions and operationalization, 3. Measurement properties and data processing. Clinically relevant results are summarized and compared. Concepts were diverse and could be divided into behavioral concepts and concepts derived from physics. Methods were heterogeneous and reporting of methods was incomplete in multiple cases. This review provides recommendations for future research steps that could facilitate the comparison of upcoming studies and their application in daily practice. As a first step in securing comparability and usability of future research, consensus is needed on clinically relevant AP concepts, definitions, operationalization, data processing, and measurement methods.
Keywords:
activity pattern
; physical activity
; chronic pain
; accelerometry
; wearable sensors
; inertial measurement unit
; data processing
1. Introduction
Chronic pain (CP), defined as pain persisting or recurring for at least three months [1], significantly impacts various aspects of daily life, including physical, mental, social, economic [2,3] and spiritual [4] domains. Individuals with CP often experience negative emotions, fatigue, depression, deconditioning, sleep dysfunctions and reduced self-efficacy [5]. These challenges can lead to limitations in expressing the self, work, leisure and family life and to social isolation [2,3]. For healthcare providers, CP presents a complex challenge due to the interplay of biological, social, and psychological factors. Often, there is no definitive intervention to resolve CP, leading healthcare interventions to focus on self-management and mitigating the negative consequences, such as limitations in activities, participation, and quality of life [6,7].
It is hypothesized that CP interferes with activity patterns (AP) within daily living [8,9,10,11,12,13]. AP have been defined as the temporal structure of physical activity and sedentary behavior accumulated over a specified period during waking hours [14]. Therefore, AP capture the succession of activity and rest, rather than cumulative measures like total activity per day. It is theorized that AP in individuals with CP differ from those in healthy populations, are influenced by coping styles and are associated with various health-related outcomes [15,16,17,18,19]. Several theoretical models have been proposed to characterize AP in CP, including the avoidance-endurance model [13].
Traditionally, AP have been assessed using self-report questionnaires. More recently, objective measurement using accelerometry has gained attention [20,21,22]. However, consensus on optimal assessment methods remains lacking. Comparisons of questionnaires with accelerometer outcomes have yielded no or inconsistent associations [23,24,25]. This evokes uncertainty about the validity of questionnaire outcomes for measuring AP on the one hand, and the effects of methodical choices in accelerometry on the other hand [23,26,27,28,29]. Self-report instruments are inherently subjective, relying, amongst others, on retrospective recall, personal perceptions and emotional state, which limits their ability in capturing actual behavior. The validity of accelerometry is influenced by incidental user-related factors, such as variations in the wear angle of the sensor.
More importantly, validity of accelerometry is structurally affected by methodical choices, including variables in data processing, and outcome variable selection. For example, very short epoch lengths may introduce unnecessary noise, whereas overly long epoch lengths may obscure temporal detail. Moreover, accelerometer studies often rely on coarse metrics such as total time per day [30,31,32] which fail to capture the nuanced temporal structure of activity and rest.
To interpret findings from previous studies and relate them to methodical choices, detailed insight into these methods is needed. AP are constructs – abstract representations that require clear definitions and operationalization for empirical investigation. This process involves thoroughly defining the concept followed by its operationalization with measurable variable and outcome measures.
Although recent reviews have explored behavior-related activity parameters from accelerometry[33,34] and cumulative activity in CP populations [35], no review has specifically focused on AP parameters relevant to CP. Therefore, this scoping review aims to provide an overview of methods for extracting AP parameters relevant to CP care from accelerometer time series. The primary aim is to elucidate the process of methodical reasoning for extracting AP from accelerometer data in patients with CP. This will inform researchers on the usability and availability of methods to investigate AP in patients with CP, and on the underlying concepts and definitions. The secondary aim is to interpret and compare clinically relevant findings in light of methods employed.
The review is structured around the methodical reasoning process, encompassing: (1) selection of the AP-related concept, (2) its definition or specification (conceptualization), (3) the definition of variables and indicators that can be observed and measured (operationalization), (4) the measurement properties and the methods for extracting the indicators from raw accelerometer data, and (5) any associations of the AP-outcome measures with symptoms or disabilities.
This scoping review [36] includes studies employing triaxial accelerometers to assess AP in individuals with chronic primary musculoskeletal pain. This condition is defined as CP in the muscles, bones, joints, or tendons that is characterized by significant emotional distress or functional disability, that cannot be accounted for by another condition[1,37].
2. Materials and Methods
The research protocol has been published in the Open Science Framework (OSF; OSF | Accelerometry in chronic pain). This scoping review is conducted and reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews PRISMA-ScR guidelines [38]. A scoping review is the most appropriate method to fit our aim, as it allows us to provide an overview of the volume and the focus of available literature, examine how research has been conducted, identify key characteristics, and identify knowledge gaps [36,39].
2.1. Eligibility Criteria
According to the recommendations of JBI Manual of Evidence Synthesis (Chapter 11, Scoping Reviews) [39], population, concept and context of interest were defined. This review focusses on the population of adults with chronic primary musculoskeletal pain as a main condition. The concept of study is the investigation of AP with triaxial accelerometry. The context of study is physical activity in daily life. All analytical methods were included if AP were involved, with emphasis on the temporal structure of activity versus sedentary behavior.
Full-text publications were included with (1) populations over 18 years, (2) primary musculoskeletal CP, (3) AP as a primary outcome measure, (4) triaxial accelerometers and (5) at least five consecutive days of physical activity measurement. In line with the definition of primary CP, publications were excluded if the sample consisted of individuals with musculoskeletal CP resulting from identifiable underlying conditions. Primary CP was selected as the focus of this review because it emphasizes the interaction between pain and AP, rather than the interaction between physical impairments and AP, as seen in conditions such as M. Parkinson or severe osteoarthritis. With mixed samples, papers were included when at least 50% of the sample fulfilled the second inclusion criterium. When subgroups were investigated separately, only data pertaining to the subgroup that met the inclusion criteria were considered.
The minimum of five consecutive measurement days is based on the recommendations of Verbunt et al. (2012; [40]) for assessing physical activity in CP, as well as prior reliability studies in the general population [41], older adults[42], and individuals with rheumatoid arthritis [43]. Eligible publications included peer-reviewed articles, gray literature and dissertations, provided they were written in English, German, Dutch, or French.
2.2. Search Strategy
PubMed, Embase and Cinahl databases were searched from inception until November 2024. For gray literature the first ten pages of Google Scholar were scanned and dissertations were searched in ProQuest via PsycInfo. The search strategies were developed in cooperation with a specialized information specialist (TE). The search strings for PubMed, Embase, Cinahl, GoogleScholar and PsycInfo were composed by TE. The search strings are included in Appendix A. Search was restricted to title, abstract and MeSh terms and included CP, physical behavior, accelerometry and synonyms. Synonyms were based on keyword, MeSh terms (PubMed) and Emtree terms (Embase) of relevant publications. The PubMed, Embase and Cinahl searches were performed by TE. Dissertations were searched by AD in consultation with TE. Finally, references of the included articles were scanned for missed publications.
2.3. Processing of Search Results and Selection
References found in PubMed were removed from the Embase and Cinahl results by subtracting PMID-numbers. The outcome was deduplicated in RefWorks Legacy via the close deduplication method and this was double-checked with SR-accelerator Deduplicator.
Selection on inclusion criteria was done in two steps, with (1) a screening phase and (2) a selection phase. Both phases were performed by AD and HW independently with all search results. Inclusions after both screening and selection were compared, discrepancies were discussed, and decisions were made. A third researcher (MV) could be consulted in case of persistent doubt.
For the screening phase title and abstract of all references were imported into Active Learning for Systematic Reviews (ASReview) Lab software [50]. With ASReview the screening phase was assisted with an AI-approach, namely Active Learning with different Machine Learning (ML)-algorithms. With this approach, the number of references that need to be manually labeled as relevant or irrelevant is reduced by approximately 90 percent, while maintaining or even improving reliability [51]. The active learning method (the ‘ASReview Pipeline’) is summarized in box 1 and is extensively elucidated by Van der Schoot et al. (2021) [50] and Boetje and Van der Schoot (2024) [51]. The 6 preselected key references were used to check the results of the ASReview-assisted screening phase.
For step 1, ‘adding prior knowledge for training’, AD and HW independently screened and labelled 100 references manually and compared, discussed and adjusted the selection. Steps 2 and 3 were performed by AD and HW independently as well. The resulting two shortlists of included references were compared, and discrepancies were discussed which resulted in a final shortlist. These papers were read full-text and accordance with all inclusion criteria led to final inclusion for this scoping review.
As a final step titles of all reference lists of the included papers were screened independently by HW and AD. The selection phase was similar as with the other databases.
Box 1. Active Learning for Systematic Reviews, the ASReview pipeline.
Step 1: Prior knowledge is added for training the ML-model by manually screening and labelling the first 100 references as ‘include’ or ‘exclude’. With this prior knowledge the ML-learning classifier Term Frequency-Inverted Document Frequency (TF-IDF) with Naive Bayes, is trained to predict study relevance. This results in a ranking of all references in the order of relevance.
Step 2: In the active learning part, the references are manually labelled as relevant or irrelevant one-by-one. Each decision is used to train the ML-model after which the ranking of relevance is adjusted, and a new reference is presented. Decision rules are available to decide whether sufficient references have been assessed to yield a reliable ranking: when (1) all key references are selected, (2) at least twice the expected number of relevant references has been screened, (3) at least 10% of the total dataset has been screened and (4) screening of at least 50 successive records does not reveal new relevant records.
Step 3: The resulting labelling and ranking of references are used to train the deep learning model Sentence BERT with Fully Connected Neural Network (FCNN). Applying this model results in another ranking of relevance. After this ranking, unlabeled records are presented one-by-one in the order of relevance and judged manually until 50 successive records are labeled as irrelevant.
2.4. Data Extraction
The study characteristics were extracted from the included articles by the researchers (AD and HW), along with the information necessary to understand the process of methodical reasoning for the quantification of AP. This process involved the successive steps of conceptualizing and operationalizing the concept, followed by selecting measurement properties and data processing. Methodical reasoning concludes with the interpretation of results in relation to the study’s aims.
To find evidence for the existence of concepts or associations with a concept, the concept must be clearly stated and quantifiably defined. The operational definition should include information on the variables (the properties or characteristics) of the concept and its indicators (the methods of quantifying the variables).
This process of conceptualization and operationalization was extracted from the included papers and consisted of four successive steps: (1) formulating the theoretical concept of the study related to AP within CP, (2) defining the concept as precisely as possible (conceptualization), (3) operationalizing the concept with concrete and specific variables, which are the properties and characteristics of the concept, and (4) identifying the concomitant indicators, which quantify variables.
This process is clarified by an example in Figure 1. Additionally, measurement properties and data processing were summarized, along with any association with symptoms or disabilities, differences between groups and differences pre- and post-treatment.
3. Results
As illustrated in Figure 2, after deduplication, the search in PubMed, Cinahl and Embase yielded 11366 records. With ranking and labelling according to the ASReview pipeline, in total 2300 of 11366 references were screened and labelled by HW and AD (in step 1 100 by HW and 100 by AD, in step 2 2 times 1000, and in step 3 2 times 50). Forty-two references were labelled as relevant, which included all 6 key references. These 42 papers were read full text and inventoried on the inclusion criteria after which 14 papers were included. Ten publications were excluded because they were posters, meeting abstracts or commentaries instead of full text peer reviewed papers. 17 papers were excluded because they did not meet at least one of the inclusion criteria, of which 16 did not investigate AP according to the definition of ‘the temporal structure of physical activity and sedentary behavior accumulated over a specified time period during waking hours,’ and one had a measurement period of one day for investigating activity variability during the day. Of these 17 excluded papers one used a biaxial accelerometer instead of triaxial. In one paper [52] the number of accelerometer-axes was not specified, and, on inquiry, the author could not clarify the number of axes. Paraschiv et al. (2008) used a biaxial and a uniaxial accelerometer on different body locations and Paraschiv et al. (2012) used three biaxial accelerometers which was assumed to deliver at least the same dimensionality and order of detail as one triaxial accelerometer. Therefore, these two studies by Paraschiv et al. were included. One publication could not be found.
With Google Scholar, 14 papers were ranked as relevant of which 13 could be excluded by reading title and abstract. One publication was selected for full text reading and was excluded because it did not investigate AP. Screening of the titles of ProQuest results yielded 6 records for reading the abstract after which one dissertation was screened full text [53]. This dissertation was excluded based on the inclusion criteria. After scanning the reference lists of the 14 included papers 26 titles and abstracts were screened and all were excluded because they did not meet the inclusion criteria. One publication [54] that was not found in the databases was added from the personal archives, which yielded 15 papers for this scoping review.
3.1. Study Characteristics
The included studies are described in Table 1. Most studies had a cross-sectional set-up. Three studies had a longitudinal set up to investigate treatment outcomes [49], associations between changed behavior-type and disability and quality of life [46] or associations between changed activity level and changed pain intensity [55]. CP sample size ranged from 15 to 292. Some studies included a sample without pain [22,56,57] or with acute pain [55] for comparison. Most participants were recruited from multidisciplinary pain centers and hospital departments of rehabilitation. In two studies participants were recruited from the general population through their physician [58,59] and one study recruited participants with advertisement on a university campus [60]. In most studies women were predominant and age ranged from 20 to over 74 years (SD 8). In most studies the type of CP was not specified. We assumed that CP in tertiary multidisciplinary pain centers, as in Andrews et al. (2023, 2015 and 2014), Liszka-Hackzell et al. (2004), Paraschiv et al. (2012 and 2008) predominantly comprised primary musculoskeletal CP. In Fanning et al. (2024 and 2023) inclusion criteria were CP in at least two sites of neck, shoulder, back, hip or knee, without specification on the cause of pain. We assumed that this pain mainly comprised chronic primary musculoskeletal pain.
3.2. Concepts of Investigation, Definitions, Variables and Indicators
In most papers a quantifiable definition of the concept of study was available or could be derived from reasoning. As a next step, operational definitions should describe how the concept of study was measured and how the measurements were interpreted. Concepts, their definitions and the definition of variables and their indicators are summarized in Table 2 and elucidated in the following sections.
Concepts and Definitions (Conceptualization)
The concepts used to investigate AP were diverse (Table 2), and the meaning of these concepts could be extracted from all papers. Definitions and specifications of these concepts are presented in Table 2. A distinction could be made between concepts related to behavioral patterns and those derived from physics.
Six papers [44,45,46,48,49,61] utilized existing models of behavioral patterns related to activity and rest as their research concept, analyzing accelerometer time series, sometimes combined with pain intensity time series.
Huijnen et al. (2011_1) defined persistence as continuing activities despite pain until task completion, resulting in forced rest due to increased pain. Additionally, a longer daily uptime was attributed to persistence because persisters tend to postpone rest. This definition was also adopted in Huijnen et al. (2020). Besides persistence, Huijnen et al. (2011_1, 2011_2 and 2020) investigated avoidance. In Huijnen et al. (2011_1) an avoider was defined as “an avoider will try to escape from activities for which they expect an increase of pain or injury.” Although definitions of avoidance and persistence were lacking in Huijnen et al. (2011_2), it can be deduced from the analyses that they were consistent with Huijnen et al. (2011_1), as verbally confirmed by the first author.
In line with the definition of persistence in these Huijnen-papers, Andrews et al. (2014) defined overactivity as engaging in high levels of activity that result in severe pain aggravation and a subsequent period of inactivity where an individual is unable to function. Daily tasks are resumed when pain subsides or when frustration stimulates new activity. Consequently, overactive persons exhibit a “sawtooth” AP with large fluctuations in pain and activity. Andrews et al. (2015 and 2023) expanded this definition to include pain aggravation after prolonged sedentary periods. Andrews et al. (2023) also introduced the concept of pacing, defined as a lower frequency of overactivity.
Time series of pain were included in four of the six papers on persistence and overactivity due to the hypothesized relationship between pain and activity in these behavioral patterns. Andrews et al. (2014) and Huijnen et al. (2011_2) did not include pain levels, focussing on fluctuation values of physical activity intensities (Andrews et al. 2014 and Huijnen et al. 2011_2), daily uptime and mean activity (Huijnen et al. 2011_2).
The remaining nine papers used physics derived measures to capture temporal patterns or complexity. Fanning et al. (2024) investigated activity intensity patterns using fitted Fourier functions on time series of steps per minute. Fanning et al. (2023) examined the pattern of activity and rest accumulation, described by the total time of activity and rest per day and the breaks within bouts of rest and activity. Liszka-Hackzell et al. (2004) aimed to examine the causal relation between activity level and pain by calculating the cross-correlation between time series of activity level and pain with different time lags. They hypothesized that activity correlates with pain, possibly with some time lag, in acute pain but not in CP.
Neikrug et al. (2017) and Sarwar et al. (2022) focused on the concept of rhythmicity of rest and activity during the day. This focus was chosen because consistent functioning might be hampered by fluctuating symptoms of pain, fatigue, mood and physical impairment (Neikrug et al., 2010). Moreover, reduced activity levels, sleep disturbances and circadian dysregulation have been observed in populations with CP (Sarwar et al. 2022). Both papers a fitted a cosine curve on accelerometry time series and extracted parameters from this curve to describe the diurnal rhythmicity of rest and activity.
Paraschiv et al. (2008) choose the dynamics of human activity as the study concept. This was more clearly defined in Paraschiv et al. (2012) as the temporal and dynamical structure of human physical activity. Paraschiv et al. (2016) adopted the same concept, and all three papers build on the method of constructing time series of activity type and intensity of walking derived from accelerometry as presented in Paraschiv et al. (2004). Paraschiv et al. (2008) focused on dynamics of these physical activity parameters, Paraschiv et al. (2012) added intensity classes to the PA parameters and focused on the complexity of these time series and Paraschiv et al. (2016) focused on deriving and applying a composite score from the outcome scores of the different deduced time series. All three Paraschiv-papers used advanced and mainly non-linear statistical methods to capture dynamics of physical activity.
Zheng et al. (2023) addressed the concept of physical activity intensity patterns in chronic low back pain. Physical activity intensity patterns were defined as the temporal organization of intensity levels and the transitions between intensity levels. This concept was chosen because it was recognized that, for instance, with a certain amount of accumulated sedentary time, it makes a difference whether someone alternates sedentary time with small bouts of activity or not. They used the data driven method of unsupervised learning (Hidden semi-Markow Model) to detect physical activity intensity levels from the vector magnitude time series.
Variables and Indicators (Operationalization)
In all the papers, observable and measurable variables for operationalizing the concept of study were defined, and descriptions of the procedures for quantifying these variables were included.
In the six papers that used behavioral concepts [44,45,46,48,49,61], variables were formulated to inventory the occurrence or nonoccurrence of the behavior. Due to the expected sawtooth pattern with overactivity, Andrews et al. (2014) focused on the fluctuation of activity levels. They calculated a fluctuation value from time series of activity counts per minute, which is the root mean square of the difference of two successive cumulative 15-minute vector magnitudes. In Andrews et al. (2015 and 2023), the outcome measures emphasized the concomitant pain increase with overactivity (Figure 3A), rather than focusing on the fluctuation values related to sawtooth pattern. They used conditional statements to count the occurrence of significant pain increases after activity or prolonged sedentary tasks.
Huijnen et al (2011_1) compared variables related to avoidance and persistence between persons classified as avoider or persister with the POAM-P self-report questionnaire. Persisters were expected to have a longer daily uptime, a higher average activity level and more fluctuations in activity level compared to avoiders. Daily uptime was quantified as the daily wear-time of the accelerometer. Activity level was quantified as mean activity counts per day, and 80% power of highest activity score. Fluctuations in activity levels were quantified as the root mean square of the difference of two subsequent 15-minute activity counts. Additionally, it was hypothesized that in persisters, the time series of activity level and pain are associated.
To quantify the level of persistence, Huijnen et al. (2011_2) calculated the daily uptime and a linear composite score of daily uptime, mean total activity score and a fluctuation score. These parameters were calculated according to the methods of Huijnen et al. (2011_1). To investigate differences in activity behavior between individuals classified as avoider, persister, mixed performer or healthy performer, Huijnen et al. (2020) used cumulative variables such as overall daily activity level and total sedentary time, as well as variables representing the distribution of activity and rest over time. The distribution variables included the number of bouts of physical activity and sedentary behavior, the median duration of bouts, the variance of bout length, the number of bouts divided by total duration for activity and rest separately as a measure of fragmentation and cumulative time of bouts above median bout length divided by total time of rest or activity (W-index), expressing the relatively higher contribution of longer bouts with a higher value.
To investigate the timing of activity and rest as well as the amplitude of activity intensity, Fanning et al. (2024) fitted a 9-basis Fourier-function on each participant’s time series of steps per minute. Subsequently, they performed a functional Principal Component Analysis to identify a set of Fourier functions capturing the most variability. In Fanning et al. (2023) the concept of accumulation of rest and physical activity was operationalized using a combination of cumulative measures and breaks within bouts of rest and activity. These measures included minutes per day in a seated or lying position, average number of steps per day, minutes per day at different classes of stepping frequency, the number of shifts from sitting to standing and the frequency of classes of bout lengths for different activity intensities.
Neikrug et al. (2017) extracted day to day rhythmic features of activity and rest using cosinor-based techniques and determined correlations with fibromyalgia symptoms. Parameters extracted from the cosine curves were mesor (mean activity level), amplitude (distance between mesor and peak level), Phi (time of day of peak activity level) and the standard errors. Besides these three parameters, Sarwar et al. (2022) extracted six other rhythmic features with a cosinor model, quantifying the most and least active minutes, complexity of the time series, nocturnal activity and intradaily variability. Some of these parameters and a fitted cosinor model are shown in Figure 3B and 3C.
Liszka-Hackzell et al. (2004) calculated the cross-correlation of interpolated time series of pain levels with time series of activity counts per minute. Cross-correlation was determined with a time lag of the pain time series of -60, -30, 0, 30 and 60 minutes, with which they investigated whether a pain level increase was ahead of activity level increase, synchronous, or delayed.
Paraschiv et al. derived different time series types of postures and activity intensity from accelerometer data, refining their methods in successive papers (2008, 2012, 2016), based on the method presented in Paraschiv et al. (2004). In the 2004 paper, four different postures (lying, sitting, standing and walking) and the intensity of walking were derived from accelerometer data using discrete wavelet transformation, Savitzky-Golay filters, vector functions and gait analysis parameters. In Paraschiv et al. (2008) different time series were constructed using these methods, including the sequence of posture allocation (Figure 3D), the sequence of the duration of walking episodes, the timing of transitions from rest to activity and vice versa, and the duration of activity relative to the duration of rest before and after activity, represented as a symbolic sequence. Nonlinear analyses were applied to these time series to investigate the physical activity pattern, including three types of fractal analysis and symbolic dynamic statistics.
Paraschiv et al. (2012) added intensity to the four activity types (lying, sitting, standing and walking) based on different acceleration thresholds for each activity type. This results in 18 possible physical activity states: two classes of sitting and lying, four classes of standing and twelve classes of walking. This classification resulted in a time series of 18 possible symbols (Figure 3E). From these time series complexity metrics, quantitative metrics, a composite deterministic score and a composite statistical score were derived.
Exploring the ability of a composite score to characterize physical behavior, Paraschiv et al. (2016) performed a factor analysis on outcome variables. These outcome variables were based on the same procedure as Paraschiv et al. (2012) to classify 18 physical activity states. Variables were percentage of time being active, percentage of time walking, 0,975th quartile of length of activity periods, duration of sedentary periods following activity (expressed as Kolmogorov-Smirnov distance) and three types of entropy. Moreover, the association between pain intensity and activity behavior was assessed with multiple regression and discriminant analysis.
Zheng et al. (2023) applied unsupervised learning (Hidden Semi-Markow modelling, HSMM) where ML-algorithms were used to discover a set of hidden states in unlabeled accelerometer data. These hidden states were derived from time series of vector magnitude acceleration averaged in 5-second bouts. The modelling identified five hidden states corresponding to five different activity levels. Bout lengths, total time per day in these five states and transition frequencies between all five activity levels were compared between groups with and without chronic low back pain. The results were also compared with the same outcome measures derived from time series constructed with the conventional cut-points approach.
In summary, AP related research concepts were operationalized in many ways. Figure 3 provides an impression of the variation of methods used. Methods included a measure of fluctuation by subtracting two successive bouts of activity intensity, timing and amplitude of activity intensity quantified by fitted Fourier-functions, parameters derived from a fitted cosine curve, non-linear analyses, complexity metrics and variables that quantify fluctuations and distribution like transition frequency and W-index.
3.3. Measurement Properties and Data Processing
Measurement properties provide information on how data were collected to quantify the required variables. Data processing refers to the conversion of raw accelerometer data into the outcome measure needed for further analysis (see Table 3).
Measurement properties and data processing were heterogeneous (Table 3). Thirteen papers used triaxial accelerometers and two papers used a combination of multiple biaxial and/or uniaxial accelerometers [22,56]. In two studies the accelerometer was worn on the non-dominant arm [55] or wrist [54] and in one study the side of the wrist-worn accelerometer was not specified [60]. In one study the accelerometer was attached to the waist [49], in two studies to the upper midline of the thigh [58,59], and in another study to the front right hip [47]. Five studies used multiple accelerometers on multiple wear locations (chest and both thighs [44], sternum and mediolateral axis of thigh [57], sternum with mediolateral axis of thigh and shank [56] and chest with thigh and shank [22]. In four studies the wear-location was not reported [45,46,48,61].
Measurement frequency ranged from 30 to 128 Hz, with frequencies from 30 to 40 Hz being predominant. Measurement frequency was not reported in seven studies [45,46,49,55,58,59,60]. Sampling duration ranged from 5 to 21 days, with a duration of five days being predominant. Of the studies that sampled five days, two studies included one weekend day [48,61], four studies only included weekdays [22,56,57,60] and four studies didn’t specify which weekdays were covered [44,49,58,59]. Valid data was defined in most studies. Epoch length ranged from one second to one hour, with one minute being predominant.
Four studies sampled pain intensity during the day and used these time series to investigate AP since pain was part of the definition and operationalization of the concept of research [45], [46,48,49,61]. Time series of pain were measured with 11-point visual analogue scale [49,61] or a 7-point likert-scale [45]. The pain measurement instrument was not specified in Andrews et al. 2023. Many other variables were sampled to investigate associations, associations through time and differences between subgroups. These variables include age, sex, self-reported measures of pain intensity, pain duration, pain interference, health-related quality of life, medication intake, approach to activity, depression, anxiety, self-discrepancy type, fatigue, impairment, functioning, mood, sleep and central sensitization symptoms.
Triaxial accelerometry results in time series of acceleration around x-, y- and z- axes, with the number of values per second dependent on sampling frequency. These time series were converted to another parameter in most of the included papers. In general, the description of conversion methods was limited. Some authors only refer to software packages and some to manuals or websites of the accelerometer manufacturer that were no longer available on the web.
For data processing six studies transformed the acceleration time series to activity counts per minute, also named vector counts per minute [45,46,48,49,55,61]. This method operates on the assumption that counts per minute is associated with the energy expenditure of activities and therefore with activity intensity. The vector magnitude of acceleration was calculated from the triaxial acceleration values and to yield counts per minute the number of times per minute of exceedance of a predefined threshold value was counted. The threshold for a count was not specified in the papers. Two studies transformed the acceleration time series to steps per minute and postures of lying, sitting or standing [58,59].
Paraschiv et al. [22,56,57] processed accelerometer data with discrete wavelet transformation, Savitzky-Golay filters and a numerical gradient. Subsequently they constructed time series of activity type with a previously developed algorithm [62]. They used different methods to detect different activities, postures and intensity of walking. Zheng et al. (2023) used raw accelerometer data from which the gravity effects were removed and then computed vector magnitude. This acceleration was averaged over five seconds. Unsupervised learning was applied to these time series which resulted in time series of five activity intensity classes. For comparison of result with a traditional method, they applied the cut-off points approach as well. With this approach the tri-axial acceleration signal was converted to vector magnitude and thresholds were defined for different activity levels.
3.4. Associations, Differences Between Groups and Differences Pre and Post Treatment
Understanding the associations between selected indicators and related behavior types or relevant clinical outcome parameters, as well as differences between groups and changes through interventions, may provide valuable insights into the usefulness and clinical value of these indicators.
All papers had a primary or secondary aim to examine associations, differences between groups or changes from pre- to post-treatment. Due to the heterogeneity of concepts, methods and outcome measures used, no firm conclusions can be drawn from the included papers. Results of some papers can be compared because of overlapping concepts, definitions and outcome measures.
Papers examined associations of objective AP parameters with self-reported behavior types such as avoidance or persistence [45,48] and behavior types classified by their treating consultant [44] (Figure 4). They also examined associations of objective AP parameters with self-discrepancy type [44] (Figure 5) and clinical outcome scores [45,54,56,57,58,59,60] (Figure 6). Since the quality of evidence is not rated, only the direction of these associations is summarized in Figure 4 to 6 as negative (-), no significant association (No), or positive (+).
Most associations of self-reported behavior-type with objective AP parameters were not significant, except for a positive association of self-reported persistence with activity fluctuation[48] and daily uptime [45], and of daily uptime with mental quality of life within objective avoiders [45]. This suggests that individuals with higher self-reported persistence have more activity fluctuations and longer daily uptime. This is understandable, as persisters probably are likely more active throughout the day than avoiders, increasing their chances of intensity fluctuations and longer daily uptime. Additionally, among individuals reporting activity avoidance, quality of life might improve with a longer daily uptime. However, given the large number of associations investigated in some studies, the risk of a type I error is considerable.
One paper examined associations of objective AP parameters with self-discrepancy types [46] (Figure 5). This study found more objective persistence with higher scores on self-discrepancy type ideal-other, which suggests that persons who are close to the ideal person from the perspective of a significant other, showed more objective persistence behavior. Furthermore, patients with increasing distance in time from their ideal-self from their own perspective had increasing daily uptime and patients getting closer to their ideal-self had decreasing daily uptime. In addition, patients with increasing distance in time between the actual-self and the ideal-self from the perspective of a significant other had decreasing daily uptime.
Seven papers examined associations of objective AP parameters with clinical outcome measures. These outcome measures were pain intensity [45,54,56,57,58,59,60], pain interference [58,59,60], health-related quality of life [58], fatigue [54], mood [54] and disability [54,60] (Figure 6). Associations were investigated with AP parameters that capture (1) the amount of activity, (2) timing of activity, (3) activity intensity, (4) distribution over different activity intensities, (5) complexity and (6) variability. The diversity of AP parameters and outcome measures complicated comparison and interpretation and when comparable parameters were used, associations were inconsistent between studies.
Amount of activity was represented with (maximum) step count, stepping time, percentage of time being active, activity counts, change (∆) in steps per day and change in stepping time. Maximum step counts and percentage of time being active were negatively correlated with pain intensity [56,60], indicating decreasing pain intensity with increasing active time. None of the other parameters for amount of activity correlated significantly with pain intensity.
Timing of activity was represented by phi, ‘Later start of activity’ and ‘∆ later start of activity. Phi was positively correlated with pain intensity, indicating higher pain levels with later activity peak, while start of activity did not have a significant association.
Activity intensity was expressed as mesor, change in sedentary intensity time, change in light intensity time, change in moderate intensity time. Mesor and change in moderate intensity time were negatively associated with pain intensity, indicating decreasing pain intensity when average activity intensity increases and when daily moderate intensity time increases after intervention. Change in light intensity time was positively correlated with pain intensity, indicating more pain with more light intensity time. Amplitude was positively correlated, indicating more pain with higher maximum intensity.
Distribution over activity intensities was indicated with bouts per intensity class, change of number of bouts of classified lengths per intensity class and percentage of time per intensity class. Bouts per intensity class did not correlate with pain intensity and changed bout lengths for the different intensity classes did not associate consistently with changed pain intensity. The change of bouts of classified length per intensity class is hard to interpret and its clinical meaning is unsure.
Complexity measures correlated negatively with pain intensity and intradaily variability correlated positively. These two outcomes seem contradictory since level of complexity is partly dependent on variability.
Most of these measures for amount, intensity, timing, distribution, complexity and variability were used to investigate associations with pain interference as well. Increased intradaily variability was found to increase pain interference. Moreover, a later start of activity was not associated with pain interference at baseline, but retarding the start of activity after a 12-week intervention program was found to increase pain interference. Decreasing the number of 5-10 minutes bouts of light intensity and 10-20 minutes bouts of moderate intensity seemed to increase pain. None of the other parameters correlated significantly with pain interference.
Scores on fatigue, mood and disability increased with later timing of peak activity (phi) [54], while another study found that fatigue was not significantly associated with timing of activity[58]. In one study disability increased with increasing intradaily variability [60]. Scores on fatigue, mood and disability decreased with higher amplitude and higher average activity level [54], but this was refuted by another study in which fatigue increased with increasing activity levels expressed as steps/day[58]. Retarding the start of activity was associated with decreased quality of life and increasing the steps per day improved quality of life.
Other studies investigated differences between groups or changes pre- and post-treatment. Andrews et al. (2023) found that a 15-week occupational therapy intervention resulted in significant reductions in objective overactivity periods. Six other studies compared differences between subgroups, grouped by different characteristics. One study [44] compared objective activity parameters in persisters and avoiders as classified by their treating consultant and found no differences. Another study [45] compared objective activity parameters of persisters and avoiders as classified by a self-report questionnaire and found longer daily uptime in persisters, but no differences in activity level.
One study [55] examined the cross-correlation between time series of activity level and pain between subjects with acute pain and CP. They found a positive association in acute pain and no association in CP.
Paraschiv et al (2008) compared groups with CP and no pain and found differences in the temporal organization of daily life with a scaling component from detrended fluctuation analysis, a different distribution of walking episodes and a different timing of rest-activity transitions. Moreover, they found that short activity with subsequent long rest appeared more frequently in CP and long activity with subsequent short rest appeared more frequently in no pain. Paraschiv et al. (2016) compared groups with different pain levels and found that the number and duration of activity periods differed between groups, as well as the complexity of the temporal pattern of activity.
Lastly, Zheng et al. (2023) compared groups with and without central sensitization (CS) using both a traditional cut-off points approach, and a time series generated with ML. They found no differences between individuals with and without CS when activity level time series were generated with the cut-off points approach. However, many differences were observed with the ML-generated time series. Participants without CS had (1) shorter bout durations of activities with lower intensity and longer bout durations of activities with higher intensity, (2) less accumulated time per day at rest and light physical activity, (3) more time per day at moderate at vigorous activity, (4) more frequent and shorter sedentary states, (5) more frequent transitions from rest, light, moderate-vigorous to sedentary, suggesting more rest after activity, (6) fewer transitions from light to moderate activity, suggesting less persistence and (7) more continuous time in both active and inactive states.
Discussion and Conclusion
With this scoping review we aimed to create an overview of methodical reasoning within studies investigating AP in patients with CP with accelerometers. This methodical reasoning included the consecutive steps of (1) choosing and defining the concept of research, (2) operationalizing the concept, (3) choosing measurement properties and methods for data processing and (4) interpreting and comparing results. With this information we aimed (1) to provide insight into the availability and usability of concepts and measurement methods and (2) to enable interpretation and comparison of results.
Concepts and Measurement Methods
The research concepts were diverse, encompassing both behavioral concepts and physics derived concepts. Behavioral concepts included avoidance, persistence (also known as overactivity), and pacing. Physics derived concepts involved the temporal association of pain with activity, activity rhythms, the multidimensionality of activity behavior, the dynamics of activity, and intensity patterns. Behavioral concepts were defined using hypotheses and theories extracted from the literature. Operationalization was achieved through decision rules or parameters reflecting various aspects such as the amount of activity, timing of activity, activity intensity, distribution of different activity intensities, bout length within activity intensity classes, transitions, complexity, variability, activity level, fluctuations, distribution, transitions and the correlation of pain with activity level.
Similar to the diversity in concepts and definitions, measurement methods and data processing were heterogeneous. This heterogeinity included variations in wear locations, measurement frequencies, durations, epoch lengths, and conversion methods. Moreover, the reporting of data processing methods was incomplete in multiple studies, which is crucial for interpreting and comparing results and conclusions. Outcome measures were also heterogeneous.
Comparison of Results
The variability of methods and outcome measures limits the ability to compare results and may account for the diverse directions of associations found. Extracting the conceptualization and operationalization from the included papers revealed some inconsistencies within the papers on behavioral concepts. Two studies [46,61] defined overactivity as high activity levels followed by severe pain aggravation and subsequent inactivity, operationalizing this with a fluctuation value of an activity intensity parameter. However, they did not include pain intensity during the day. This limits the value of the outcomes, as fluctuations in activity intensity alone are a normal pattern in activity behavior. One study [44] defined persistence as having activity levels similar to healthy participants, but did not explain the reasoning behind the operationalization with distribution measures and transition measures.
The diversity of measurement properties and methods used to convert raw accelerometer data, as shown in Table 3, resulted in a diversity of outcomes with unknown validity. Moreover, these varied outcomes are difficult to compare. For example, multiple studies converted raw data to vector counts per minute and used cut-off points as a measure of activity intensity [45,48,49,55,61,64] and two studies converted raw data to steps/minute, and classified this to activity intensities[58,59]. Another set of studies converted raw data to time series of type of activity, intensity of walking, sitting, lying and standing [22,56,57].
Conversion methods might affect the validity of the measurement method. A systematic review [65] concluded that cut-off points developed on healthy populations are not applicable to clinical populations. Additionally, Staudenmayer et al. (2015) found that ML-models perform better than traditional linear and cut-off points models in estimating activity intensities [66]. The improved performance of a ML model in converting accelerometer data to activity intensity might influence measured associations or differences between groups. This is evidenced by the study of Zheng et al. (2023), which found no differences in physical activity between groups of chronic low back pain patients with and without central sensitization using the traditional cut-points approach. However, significant differences were found for five AP parameters using an ML approach.
While the number of significant associations between behavior type and objective AP parameters was small, the associations founds were plausible. Persisters may indeed have more fluctuations in activity and longer days than avoiders. In addition, Paraschiv et al. (2016) was one of the limited number of studies that consistently found associations between pain intensity and objective AP parameters. Although this was expected, such associations were not consistently found in many of the other included studies. The more advanced methods to process accelerometer data and the more sophisticated AP parameters applied in Paraschiv et al. (2016) might explain this consistency within this specific study. This indicates the added value of advanced methods for data processing and extracting outcome measures in this field of research. A recent scoping review summarized more advanced methods to operationalize the concept of AP from accelerometer data [33].
Strengths and Limitations
The strength of this study lies in the structured and detailed extraction of information on the methodical reasoning process within studies measuring AP. This method and its conclusions emphasize the importance of sound and clean conceptualization and operationalization in this complex field of behavioral research.
Although we provided a detailed overview of the research conducted on this topic, certain aspects were not addressed in this review. Future research should provide insights into and establish consensus on measurement properties, such as accelerometer calibration and sampling frequency, as well as data processing aspects, including epoch length, the use of filters, the number of days required to obtain a reliable representation of behavior, and the validity of algorithms in real-life settings. These topics are covered in recent research [67,68,69].
It is difficult to reach sound conclusions on useful and useable methods and parameters for analyzing AP within CP due to the small number of available studies, small sample sizes, the great diversity of measuring and conversion methods, the diversity of outcome measures and incomplete method reporting. Moreover, the use of cut-off points as a conversion method has limited validity and therefore creates noise, thereby limiting the value of the conclusions drawn.
Recommendations
The clinical significance of objectively measuring AP is considerable. Healthcare professionals working with patients with chronic pain play a crucial role in helping patients to manage their pain and improve their ability to engage in desired activities. daily functioning and participation. Currently, they lack objective information to guide their treatment decisions. In daily practice, it is essential to recognize that the choice of measurement method impacts validity and, consequently, the added value for clinical reasoning.
Uniformity of methods is needed to develop insights into the usefulness and clinimetric properties of objective AP parameters. The current standard is ML, therefore measurement properties and data processing should be investigated with this method. Previous research has proposed some recommendations on measurement properties. For example, a systematic review on ML to convert accelerometer data to activity measures concluded that performance does not increase with sampling frequencies higher than 20 to 30 Hz [70]. Although more research is needed on this topic, it might be recommended to use these relatively low sampling frequencies. Moreover, with ML methods, performance might be independent of sensor placement [70,71] and performance does not improve with multiple sensors. Adherence is higher with wrist sensors than with waist sensors [67,72]. Hence, it might recommended to use a single wrist sensor, preferably at the dominant wrist, as one study found higher accuracy at the dominant wrist [73] compared to another study with nondominant wrist placement [74]. However, more research is needed to confirm these recommendations.
No information appears to be available on the effect of epoch length on output and accuracy in adults. Additionally, research in free-living settings using criterion measures like direct observations is needed to determine criterion validity.
Comprehensive reporting of methods is essential to ensure interpretability, comparability, and progress in the research field. Regarding accelerometry, reporting should include wear location, sensor brand and model, sampling frequency, feature extraction method, window size or epoch length, and the number of axes.
Due to the limited number of studies, heterogeneity of concepts, definitions and methods, incomplete method reporting and the lack of replicated research, it is unclear which types of concepts and methods are most suitable and useful for investigating AP in CP populations. Behavioral concepts are based on existing theories of activity behavior within CP. As indicated by this review, the majority of accelerometry based outcome measures showed no associations with behavioral concepts. Therefore, it might be recommended to build future research on data driven approaches, such as ML, Hidden Markov Modelling, or conventional statistical methods like principal component analysis. Data driven methods may provide more comprehensive and detailed insights into pattern parameters relevant to daily practice, particularly when these parameters are associated with clinical outcomes. Conversely, while data driven methods can extract activity pattern parameters, their clinical significance may remain ambiguous and thus require interpretation by the researcher.
Moreover, we recommend being cautious in comparing self-report AP-questionnaires with objectively measured AP, as questionnaires and accelerometers measure different concepts. Self-report questionnaires depend on recalling behavior and measure perceptions, thoughts and feelings, while accelerometers measure actual movement. This explains the inconsistent associations found between accelerometry and questionnaires to investigate AP.
In daily practice it is important to recognize that questionnaires and accelerometers measure different concepts and therefore can be complementary. Scores on questionnaires are affected by many patient-specific psychosocial confounders. For example, participants with a more depressed mood tend to rate their behavior more negatively [75], and the perception of one’s own behavior is influenced by reference groups. Discrepancies between questionnaires and accelerometer data provide further information on the appreciation of one’s own behavior. For instance, an unrealistic negative appreciation is mostly maladaptive, and this information could help in formulating treatment goals and interventions.
For securing comparability and usability of future research, consensus is needed on AP concepts, definitions, operationalization and measurement methods. A Delphi-study or workshops might be a first step towards consensus on recommendations for methods in future research. It is plausible that the combination of insights and methods from movement sciences, behavioral sciences, physics and data science and observations from daily practice will yield the most meaningful understanding of valid and relevant methods for investigating AP in CP. Consequently, multidisciplinary research is needed, involving researchers and experts from daily practice.
Conclusion
This scoping review highlighted the importance of sound and clear methodical reasoning when aiming to measure activity pattern concepts with accelerometers in health care, especially within the context of chronic pain. In previous research, the diversity of methods and limited reporting in many cases have hindered the validation of these studies’ methods and results.
Author Contributions
Conceptualization, A.D.. and H.W.; methodology, A.D., H.W. and T.E.; formal analysis, A.D. and H.W.; investigation, A.D. and H.W.; writing—original draft preparation, A.D., I.H. and H.W.; writing—review and editing, M.V. and R.S.; visualization, A.D. ; supervision, R.S.; project administration, H.W.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AP | Activity patterns |
| CP | Chronic pain |
Appendix A. Search Strings
Concepts:
- Chronic pain
- Accelerometry
- NOT animals
PubMed
(("Chronic Pain"[Mesh] OR "Chronic Pain"[tiab:~5] OR "Chronic Pains"[tiab:~5]) AND ("Accelerometry"[Mesh] OR "Actigraphy"[Mesh] OR "Fitness Trackers"[Mesh] OR "Telemedicine"[Mesh] OR "Wearable Electronic Devices"[Mesh] OR Accelero*[tiab] OR Actigraph*[tiab] OR Telemetr*[tiab] OR "Fitness Tracker"[tiab:~5] OR "Fitness Trackers"[tiab:~5] OR "Fitness Tracking"[tiab:~5] OR "Activity Tracker"[tiab:~5] OR "Activity Trackers"[tiab:~5] OR "Activity Tracking"[tiab:~5] OR "Tele-Referral"[tiab] OR " Tele-Referrals"[tiab] OR "TeleReferral"[tiab] OR " TeleReferrals"[tiab] OR "Virtual Medicine"[tiab] OR "Virtual-Medicine"[tiab] OR "Mobile Health"[tiab] OR "Mobile-Health"[tiab] OR "mHealth"[tiab] OR "Telehealth"[tiab] OR "Tele-health"[tiab] OR "Wearable Electronic Device"[tiab] OR "Wearable Electronic Devices"[tiab] OR "Wearable Device"[tiab] OR "Wearable Devices"[tiab] OR "Electronic Skin"[tiab] OR "Electronic Skins"[tiab] OR "Wearable Technology"[tiab] OR "Wearable Technologies"[tiab] OR (("Movement"[Mesh:NoExp] OR "Locomotion"[Mesh] OR ((Activity[tiab] OR Activities[tiab]) AND (Physical*[tiab] OR Behaviour*[tiab] OR Behavior*[tiab] OR Motor*[tiab] OR Pattern*[tiab])) OR Movement*[tiab] OR Motion*[tiab] OR Locomotion*[tiab]) AND ("Pain Measurement"[Mesh] OR Measur*[tiab] OR Meter[tiab] OR Sensor*[tiab])))) NOT (("Adolescent"[Mesh] OR "Child"[Mesh] OR "Infant"[Mesh]) OR ("Models, Animal"[Mesh]))
Embase
((('Chronic pain'/exp OR (Chronic NEAR/5 Pain*):ti,ab) AND ('Accelerometry'/exp OR 'Actimetry'/exp OR 'Activity tracker'/exp OR 'Telemedicine'/exp OR 'Wearable computer'/exp OR 'Ambulatory monitoring'/exp OR (Accelero* OR Actigraph* OR Actimetr* OR Telemetr* OR ((Fitness OR Activity) NEAR/5 Track*) OR "Tele-Referral" OR "Tele-Referrals" OR "TeleReferral" OR "TeleReferrals" OR "Virtual Medicine" OR "Virtual-Medicine" OR "Mobile Health" OR "Mobile-Health" OR "mHealth" OR "Telehealth" OR "Tele-health" OR "Wearable Electronic Device*" OR "Wearable Device*" OR " Wearable computer*" OR "Electronic Skin*" OR "Wearable Technolog*" OR ((Ambulatory OR Outpatient*) NEAR/5 Monitoring)):ti,ab OR (('Movement (physiology)'/exp OR 'Motor activity'/exp OR (Movement* OR Motion* OR Locomotion* OR ((Activity OR Activities) NEAR/5 (Physical* OR Behaviour* OR Behavior* OR Motor* OR Pattern*))):ti,ab) AND ('Measurement'/exp OR 'Pain measurement'/exp OR (Measur* OR Meter OR Sensor*):ti,ab)))) NOT ([animals]/lim OR ('adolescent'/exp OR 'child'/exp))) AND [embase]/lim
CINAHL
((MH "Chronic Pain" OR (Chronic N5 Pain*)) AND (MH "Accelerometry+" OR MH "Actigraphy" OR MH "Fitness Trackers" OR MH "Telemedicine+" OR Accelero* OR Actigraph* OR Actimetr* OR Telemetr* OR ((Fitness OR Activity) N5 Track*) OR "Tele-Referral" OR "Tele-Referrals" OR "TeleReferral" OR "TeleReferrals" OR "Virtual Medicine" OR "Virtual-Medicine" OR "Mobile Health" OR "Mobile-Health" OR "mHealth" OR "Telehealth" OR "Tele-health" OR "Wearable Electronic Device*" OR "Wearable Device*" OR "Wearable computer*" OR "Electronic Skin*" OR "Wearable Technolog*" OR ((Ambulatory OR Outpatient*) N5 Monitoring) OR ((MH "Movement+" OR MH "Motor Activity+" OR MH "Locomotion+" OR Movement* OR Motion* OR Locomotion* OR ((Activity OR Activities) AND (Physical* OR Behaviour* OR Behavior* OR Motor* OR Pattern*))) AND (MH "Pain Measurement" OR Measur* OR Meter OR Sensor*)))) NOT ((MH "Adolescence" OR MH "Child+") OR MH "Animals")
Psychinfo
(Chronic N5 Pain*) AND (Accelero* OR Actigraph* OR Actimetr* OR Telemetr* OR ((Fitness OR Activity) N5 Track*) OR "Tele-Referral" OR "Tele-Referrals" OR "TeleReferral" OR "TeleReferrals" OR "Virtual Medicine" OR "Virtual-Medicine" OR "Mobile Health" OR "Mobile-Health" OR "mHealth" OR "Telehealth" OR "Tele-health" OR "Wearable Electronic Device*" OR "Wearable Device*" OR "Wearable computer*" OR "Electronic Skin*" OR "Wearable Technolog*" OR ((Ambulatory OR Outpatient*) N5 Monitoring) OR Movement* OR Motion* OR Locomotion* OR ((Activity OR Activities) N5 (Physical* OR Behaviour* OR Behavior* OR Motor* OR Pattern*)) AND (Measur* OR Meter OR Sensor*))) AND (ZZ "dissertation")
Google Scholar
(Chronic AND Pain*) AND (Accelero* OR Actigraph* OR Actimetr* OR Telemetr* OR ((Fitness OR Activity) AND Track*) OR "Tele-Referral" OR "Tele-Referrals" OR "TeleReferral" OR "TeleReferrals" OR "Virtual Medicine" OR "Virtual-Medicine" OR "Mobile Health" OR "Mobile-Health" OR "mHealth" OR "Telehealth" OR "Tele-health" OR "Wearable Electronic Device*" OR "Wearable Device*" OR "Wearable computer*" OR "Electronic Skin*" OR "Wearable Technolog*" OR ((Ambulatory OR Outpatient*) AND Monitoring) OR Movement* OR Motion* OR Locomotion* OR ((Activity OR Activities) AND (Physical* OR Behaviour* OR Behavior* OR Motor* OR Pattern*)) AND (Measur* OR Meter OR Sensor*)))
References
- R. D. Treede et al. A classification of chronic pain for ICD-11. 2015, Lippincott Williams and Wilkins. [CrossRef]
- H. Breivik, B. Collett, V. Ventafridda, R. Cohen, and D. Gallacher. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. European Journal of Pain 2006, 10, 287. [Google Scholar] [CrossRef] [PubMed]
- S. Van Rysewyk et al. Understanding the Lived Experience of Chronic Pain: A Systematic Review and Synthesis of Qualitative Evidence Syntheses. Br J Pain 2023, 17, 592–605. [Google Scholar] [CrossRef] [PubMed]
- R. De-Diego-Cordero, C. Velasco-Domínguez, A. Aranda-Jerez, and J. Vega-Escaño. The Spiritual Aspect of Pain: An Integrative Review. J Relig Health 2024, 63, 159–184. [Google Scholar] [CrossRef]
- S. M. Meints and R. R. Edwards. Evaluating psychosocial contributions to chronic pain outcomes. Dec. 20, 2018, Elsevier Inc. [CrossRef]
- S. P. Cohen, L. Vase, and W. M. Hooten. Chronic Pain 1 Chronic pain: an update on burden, best practices, and new advances. 2021. [Online]. Available: www.thelancet.com.
- A. L. Hassett and D. A. Williams. Non-pharmacological treatment of chronic widespread musculoskeletal pain. 2011, Bailliere Tindall Ltd. [CrossRef]
- D. Cane, W. R. Nielson, and D. Mazmanian. Patterns of pain-related activity: Replicability, treatment-related changes, and relationship to functioning. Pain 2018, 159, 2522–2529. [Google Scholar] [CrossRef]
- M. Racine et al. Pain-related Activity Management Patterns and Function in Patients with Fibromyalgia Syndrome. Clinical Journal of Pain 2018, 34, 122–129. [Google Scholar] [CrossRef]
- R. Esteve, C. Ramírez-Maestre, M. L. Peters, E. R. Serrano-Ibáñez, G. T. Ruíz-Párraga, and A. E. López-Martínez. Development and initial validation of the activity patterns scale in patients with chronic pain. Journal of Pain 2016, 17, 451–461. [Google Scholar] [CrossRef]
- H. P. J. Kindermans, J. Roelofs, M. E. J. B. Goossens, I. P. J. Huijnen, J. A. Verbunt, and J. W. S. Vlaeyen. Activity patterns in chronic pain: Underlying dimensions and associations with disability and depressed mood. Journal of Pain 2011, 12, 1049–1058. [Google Scholar] [CrossRef]
- S. Van Damme and H. Kindermans. A self-regulation perspective on avoidance and persistence behavior in chronic pain: New theories, new challenges?,” Feb. 21, 2015, Lippincott Williams and Wilkins. [CrossRef]
- M. I. Hasenbring, D. Psych, and J. A. Verbunt. Fear-avoidance and Endurance-related Responses to Pain: New Models of Behavior and Their Consequences for Clinical Practice. Clin J Pain 2010, 26 [Online]. Available: www.clinicalpain.com|747.
- N. D. Ridgers, E. Denniss, A. J. Burnett, J. Salmon, and S. J. J. M. Verswijveren. Defining and reporting activity patterns: a modified Delphi study. International Journal of Behavioral Nutrition and Physical Activity 2023, 20. [CrossRef]
- D. Cane, W. R. Nielson, M. Mccarthy, and D. Mazmanian. Pain-related Activity Patterns Measurement, Interrelationships, and Associations With Psychosocial Functioning. 2013. [Online]. Available: www.clinicalpain.com|435.
- L. M. McCracken and V. M. Samuel. The role of avoidance, pacing, and other activity patterns in chronic pain. Pain 2007, 130, 119–125. [Google Scholar] [CrossRef]
- N. E. Andrews, J. Strong, and P. J. Meredith. Activity pacing, avoidance, endurance, and associations with patient functioning in chronic pain: A systematic review and meta-analysis. 2012, W.B. Saunders. [CrossRef]
- M. M. Wertli, E. Rasmussen-Barr, U. Held, S. Weiser, L. M. Bachmann, and F. Brunner. Fear-avoidance beliefs - A moderator of treatment efficacy in patients with low back pain: A systematic review. Spine Journal 2014, 14, 2658–2678. [Google Scholar] [CrossRef]
- E. Fehrmann, L. Fischer-Grote, T. Kienbacher, K. Tuechler, P. Mair, and G. Ebenbichler. Perceived psychosocial stressors and coping resources in chronic low back pain patients as classified by the avoidance-endurance model. Frontiers in Rehabilitation Sciences. [CrossRef]
- A. Paraschiv-Ionescu et al. Concern about Falling and Complexity of Free-Living Physical Activity Patterns in Well-Functioning Older Adults. Gerontology 2018, 64, 603–611. [Google Scholar] [CrossRef] [PubMed]
- K. ; Ohashi et al. Decreased Fractal Correlation in Diurnal Physical Activity in Chronic Fatigue Syndrome. Methods Inf Med 2004, 43, 26–29. [Google Scholar] [CrossRef]
- A. Paraschiv-Ionescu, E. Buchser, B. Rutschmann, and K. Aminian. Nonlinear analysis of human physical activity patterns in health and disease. Phys Rev E Stat Nonlin Soft Matter Phys 2008, 77. [CrossRef]
- S. A. Prince, K. B. Adamo, M. E. Hamel, J. Hardt, S. Connor Gorber, and M. Tremblay. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. 06, 2008. [CrossRef]
- M. L. Stevens et al. Feasibility, Validity, and Responsiveness of Self-Report and Objective Measures of Physical Activity in Patients With Chronic Pain. PM and R 2019, 11, 858–867. [Google Scholar] [CrossRef]
- M. G. H. Van Weering, M. M. R. Vollenbroek-Hutten, and H. J. Hermens. The relationship between objectively and subjectively measured activity levels in people with chronic low back pain. Clin Rehabil 2011, 25, 256–263. [Google Scholar] [CrossRef]
- J. A. Verbunt, I. P. J. Huijnen, and A. Köke. Assessment of physical activity in daily life in patients with musculoskeletal pain. Mar. 2009. [CrossRef]
- P. Kelly, C. Fitzsimons, and G. Baker. Should we reframe how we think about physical activity and sedentary behaviour measurement? Validity and reliability reconsidered? International Journal of Behavioral Nutrition and Physical Activity 2016, 13. [Google Scholar] [CrossRef]
- F. A. Carvalho et al. Reliability and validity of two multidimensional self-reported physical activity questionnaires in people with chronic low back pain. Musculoskelet Sci Pract 2017, 27, 65–70. [Google Scholar] [CrossRef]
- M. L. Stevens et al. Feasibility, Validity, and Responsiveness of Self-Report and Objective Measures of Physical Activity in Patients With Chronic Pain. PM and R 2019, 11, 858–867. [Google Scholar] [CrossRef]
- K. D. McGovney, A. F. Curtis, and C. S. McCrae. Actigraphic Physical Activity, Pain Intensity, and Polysomnographic Sleep in Fibromyalgia. Behavioral Sleep Medicine 2023, 21, 383–396. [Google Scholar] [CrossRef]
- P. K. Morelhão et al. Physical activity and disability measures in chronic non-specific low back pain: a study of responsiveness. Clin Rehabil 2018, 32, 1684–1695. [Google Scholar] [CrossRef]
- C. G. Ryan, S. Wellburn, S. McDonough, D. J. Martin, and A. M. Batterham. The association between displacement of sedentary time and chronic musculoskeletal pain: an isotemporal substitution analysis. Physiotherapy (United Kingdom) 2017, 103, 471–477. [Google Scholar] [CrossRef]
- A. Backes, T. Gupta, S. Schmitz, G. Fagherazzi, V. van Hees, and L. Malisoux. Advanced analytical methods to assess physical activity behavior using accelerometer time series: A scoping review. Jan. 01, 2022, John Wiley and Sons Inc. [CrossRef]
- Y. T. Liang, C. Wang, and C. K. Hsiao. Data Analytics in Physical Activity Studies With Accelerometers: Scoping Review. 2024, JMIR Publications Inc. [CrossRef]
- M. Berger, A. M. Bertrand, T. Robert, and L. Chèze. Measuring objective physical activity in people with chronic low back pain using accelerometers: a scoping review. 2023, Frontiers Media SA. [CrossRef]
- Z. Munn, M. D. J. Peters, C. Stern, C. Tufanaru, A. McArthur, and E. Aromataris. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol 2018, 18. [Google Scholar] [CrossRef]
- Geneva: World Health Organization. ICD-11 for morbidity and mortality statistics, MG30.02 Chronic primary musculoskeletal pain. https://icd.who.int/browse/2024-01/mms/en#1236923870.”.
- A. C. Tricco et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. 02, 2018, American College of Physicians. [CrossRef]
- G. C. M. P. M. Z. T. A. K. H. Peters MDJ. Chapter 11: Scoping reviews (2020 version). in JBI Manual for Evidence Synthesis, Aromataris E and Munn Z, Eds., JBI 2020, ch. 11. [CrossRef]
- J. A. Verbunt, I. P. J. Huijnen, and H. A. M. Seelen. Assessment of Physical Activity by Movement Registration Systems in Chronic Pain Methodological Considerations SPECIAL TOPIC SERIES 496 |.” [Online]. Available: www.clinicalpain.com.
- M. Danilevicz, S. Vidil, B. Landré, A. Dugravot, V. T. van Hees, and S. Sabia. Reliable measures of rest-activity rhythm fragmentation: how many days are needed? European Review of Aging and Physical Activity 2024, 21. [Google Scholar] [CrossRef]
- T. L. Hart, A. M. Swartz, S. E. Cashin, and S. J. Strath. How many days of monitoring predict physical activity and sedentary behaviour in older adults? International Journal of Behavioral Nutrition and Physical Activity 2011, 8. [Google Scholar] [CrossRef]
- C. M. O’Brien et al. Number of days required to measure sedentary time and physical activity using accelerometery in rheumatoid arthritis: a reliability study. Rheumatol Int 2023, 43, 1459–1465. [Google Scholar] [CrossRef]
- I. P. J. Huijnen, F. C. Schasfoort, R. J. E. M. Smeets, E. Sneekes, J. A. Verbunt, and J. B. J. Bussmann. Subgrouping patients with chronic low back pain: What are the differences in actual daily life behavior between patients classified as avoider or persister? J Back Musculoskelet Rehabil 2020, 33, 303–311. [Google Scholar] [CrossRef]
- I. P. J. Huijnen et al. Differences in activity-related behaviour among patients with chronic low back pain. European Journal of Pain 2011, 15, 748–755. [Google Scholar] [CrossRef]
- I. P. J. Huijnen et al. Effects of self-discrepancies on activity-related behaviour: Explaining disability and quality of life in patients with chronic low back pain. Pain 2011, 152, 2165–2172. [Google Scholar] [CrossRef]
- X. Zheng, M. F. Reneman, R. H. S. Preuper, E. Otten, and C. J. Lamoth. Relationship between physical activity and central sensitization in chronic low back pain: Insights from machine learning. Comput Methods Programs Biomed 2023, 232. [CrossRef]
- N. E. Andrews, J. Strong, and P. J. Meredith. Overactivity in chronic pain: Is it a valid construct? Pain 2015, 156, 1991–2000. [Google Scholar] [CrossRef]
- N. E. Andrews, D. Ireland, M. Deen, and M. Varnfield. Clinical utility of a mHealth assisted intervention for activity modulation in chronic pain: The pilot implementation of pain ROADMAP. European Journal of Pain (United Kingdom) 2023, 27, 749–765. [Google Scholar] [CrossRef]
- R. van de Schoot et al. An open source machine learning framework for efficient and transparent systematic reviews. Nat Mach Intell 2021, 3, 125–133. [Google Scholar] [CrossRef]
- J. Boetje and R. van de Schoot. The SAFE procedure: a practical stopping heuristic for active learning-based screening in systematic reviews and meta-analyses. Syst Rev 2024, 13. [CrossRef]
- A. Korszun, E. A. Young, N. Cary Engleberg, C. B. Brucksch, J. F. Greden, and L. A. Crofford. Use of actigraphy for monitoring sleep and activity levels in patients with fibromyalgia and depression. J Psychosom Res 2002, 52, 439–443. [Google Scholar] [CrossRef]
- R. F. M. Solis. Physical activity and its association with pain-related distress and pain processing before and after exercise-induced low back pain. Dissertation.. 2016.
- A. B. Neikrug, G. Donaldson, E. Iacob, S. L. Williams, C. A. Hamilton, and A. Okifuji. Activity rhythms and clinical correlates in fibromyalgia. Pain 2017, 158, 1417–1429. [Google Scholar] [CrossRef]
- J. J. Liszka-Hackzell and D. P. Martin. An analysis of the relationship between activity and pain in chronic and acute low back pain. Anesth Analg 2004, 99, 477–481. [Google Scholar] [CrossRef]
- A. Paraschiv-Ionescu, C. Perruchoud, E. Buchser, and K. Aminian. Barcoding human physical activity to assess chronic pain conditions. PLoS One 2012, 7. [CrossRef]
- A. Paraschiv-Ionescu, C. Perruchoud, B. Rutschmann, E. Buchser, and K. Aminian. Quantifying dimensions of physical behavior in chronic pain conditions. J Neuroeng Rehabil 2016, 13. [CrossRef]
- Fanning, A. K. Brooks, M. B. Irby, K. W. N’dah, and W. J. Rejeski. Associations Between Patterns of Daily Stepping Behavior, Health-Related Quality of Life, and Pain Symptoms Among Older Adults with Chronic Pain: A Secondary Analysis of Two Randomized Controlled Trials. Clin Interv Aging 2024, 19, 459–470. [Google Scholar] [CrossRef]
- Fanning et al. Associations between patterns of physical activity, pain intensity, and interference among older adults with chronic pain: a secondary analysis of two randomized controlled trials. Frontiers in Aging 2023, 4. [CrossRef]
- A. Sarwar, E. O. Agu, J. Polcari, J. Ciroli, B. Nephew, and J. King. PainRhythms: Machine learning prediction of chronic pain from circadian dysregulation using actigraph data — a preliminary study. Smart Health 2022, 26. [CrossRef]
- N. E. Andrews, J. Strong, P. J. Meredith, and R. G. D’arrigo. Association Between Physical Activity and Sleep in Adults With Chronic Pain: A Momentary, Within-Person Perspective. 2014. [Online]. Available: https://academic.oup.com/ptj/article/94/4/499/2735639.
- A. Paraschiv-Ionescu, E. E. Buchser, B. Rutschmann, B. Najafi, and K. Aminian. Ambulatory system for the quantitative and qualitative analysis of gait and posture in chronic pain patients treated with spinal cord stimulation. Gait Posture 2004, 20, 113–125. [Google Scholar] [CrossRef] [PubMed]
- J. C. Brond. ActigraphCounts. https://github.com/jbrond/actigraphcounts.
- H. P. J. Kindermans, J. Roelofs, M. E. J. B. Goossens, I. P. J. Huijnen, J. A. Verbunt, and J. W. S. Vlaeyen. Activity patterns in chronic pain: Underlying dimensions and associations with disability and depressed mood. Journal of Pain 2011, 12, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- M. S. Bianchim, M. A. McNarry, L. Larun, and K. A. Mackintosh. Calibration and validation of accelerometry to measure physical activity in adult clinical groups: A systematic review. Dec. 01, 2019, Elsevier Inc. [CrossRef]
- J. Staudenmayer, S. He, A. Hickey, J. Sasaki, and P. Freedson. Methods to estimate aspects of physical activity and sedentary behavior from high-frequency wrist accelerometer measurements. J Appl Physiol 2015, 119, 396–403. [Google Scholar] [CrossRef]
- J. H. Migueles et al. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sep. 01, 2017, Springer International Publishing. [CrossRef]
- S. Chan et al. CAPTURE-24: A large dataset of wrist-worn activity tracker data collected in the wild for human activity recognition. 2024. [CrossRef]
- A. Narayanan, F. Desai, T. Stewart, S. Duncan, and L. MacKay. Application of raw accelerometer data and machine-learning techniques to characterize human movement behavior: A systematic scoping review. 2020, Human Kinetics Publishers Inc. [CrossRef]
- V. Farrahi, M. Niemelä, M. Kangas, R. Korpelainen, and T. Jämsä. Calibration and validation of accelerometer-based activity monitors: A systematic review of machine-learning approaches. 01, 2019, Elsevier B.V. [CrossRef]
- C. Ozemek, M. M. Kirschner, B. S. Wilkerson, W. Byun, and L. A. Kaminsky. Intermonitor reliability of the GT3X+ accelerometer at hip, wrist and ankle sites during activities of daily living. Physiol Meas 2014, 35, 129–138. [Google Scholar] [CrossRef]
- R. M. Pulsford et al. The impact of selected methodological factors on data collection outcomes in observational studies of device-measured physical behaviour in adults: A systematic review. 01, 2023, BioMed Central Ltd. [CrossRef]
- S. E. Crouter, J. I. Flynn, and D. R. Bassett. Estimating physical activity in youth using a wrist accelerometer,”. Med Sci Sports Exerc 2015, 47, 944–951. [CrossRef]
- J. L. Chandler, K. Brazendale, M. W. Beets, and B. A. Mealing. Classification of physical activity intensities using a wrist-worn accelerometer in 8-12-year-old children. Pediatr Obes 2016, 11, 120–127. [Google Scholar] [CrossRef]
- I. P. J. Huijnen et al. Do depression and pain intensity interfere with physical activity in daily life in patients with Chronic Low Back Pain? Pain 2010, 150, 161–166. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the process of conceptualization and operationalization of a concept, and an example from one of the included papers in this review (Andrews et al., 2015).
Figure 1.
Flow chart of the process of conceptualization and operationalization of a concept, and an example from one of the included papers in this review (Andrews et al., 2015).
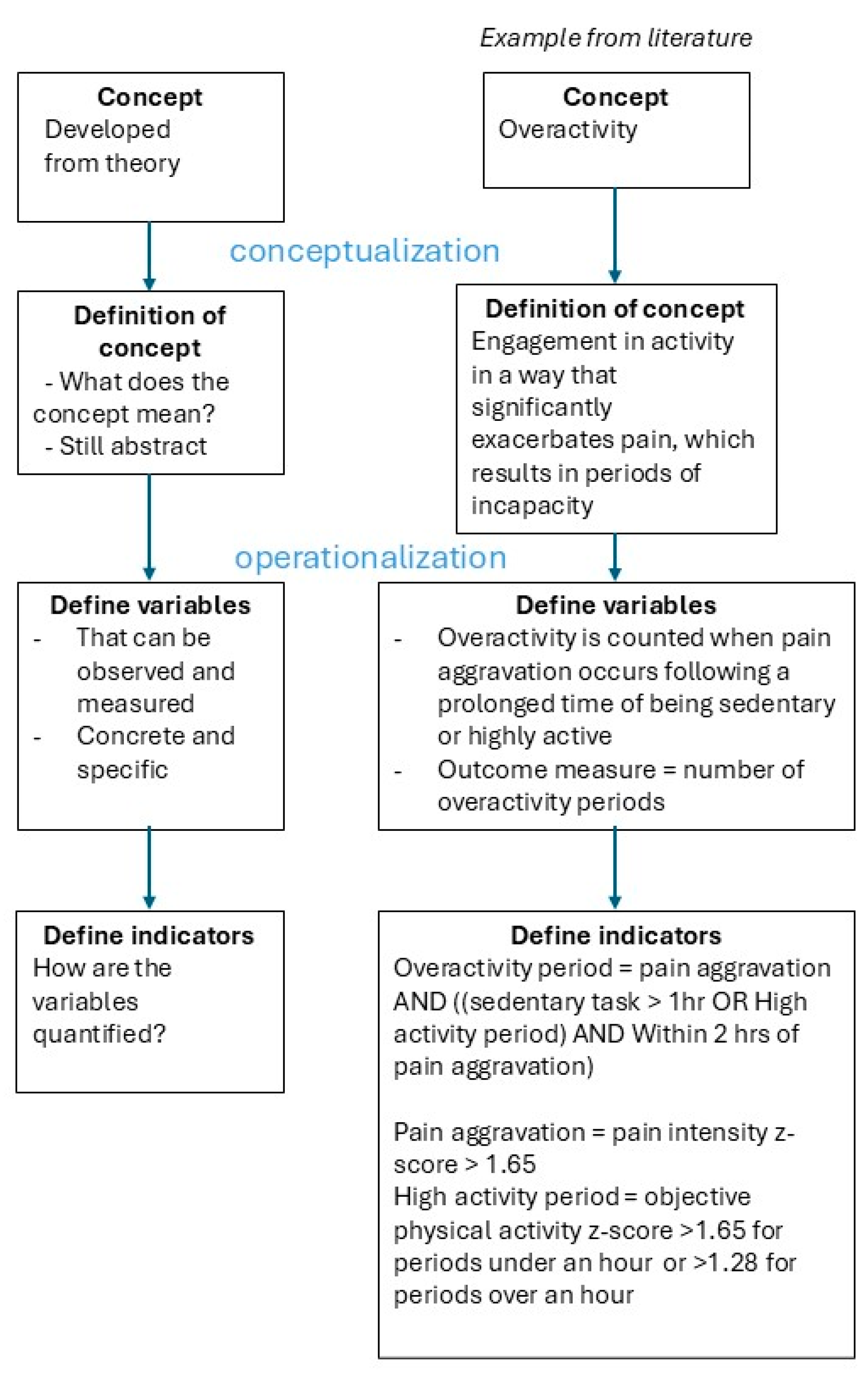
Figure 2.
Flow chart of the selection of papers.
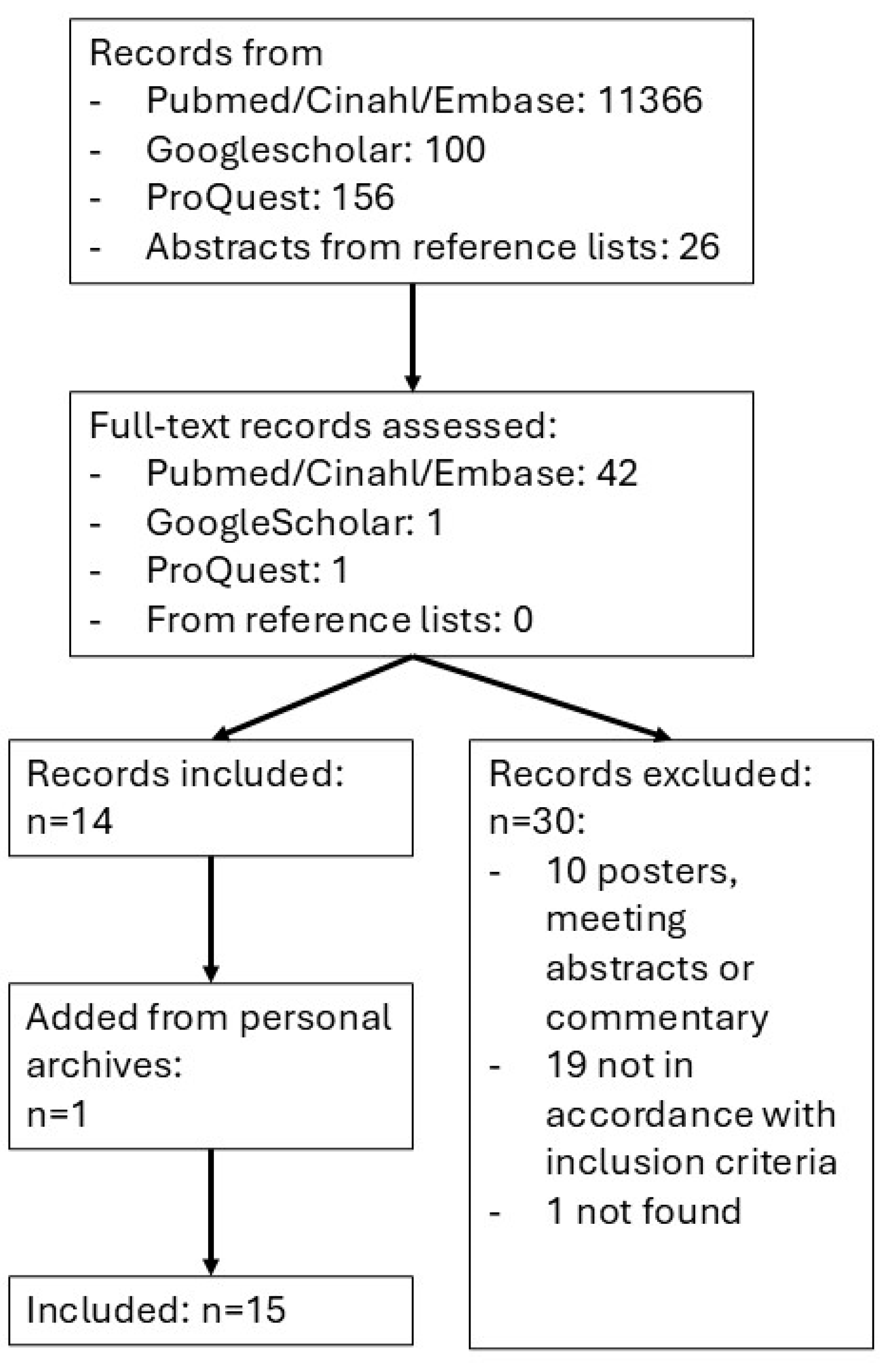
Figure 3.
Impression of the variation of methods used to extract activity patterns from accelerometer time series: overactivity periods, rhythm parameters with cosinor fitting, posture allocation and physical activity states across studies.
Figure 3.
Impression of the variation of methods used to extract activity patterns from accelerometer time series: overactivity periods, rhythm parameters with cosinor fitting, posture allocation and physical activity states across studies.
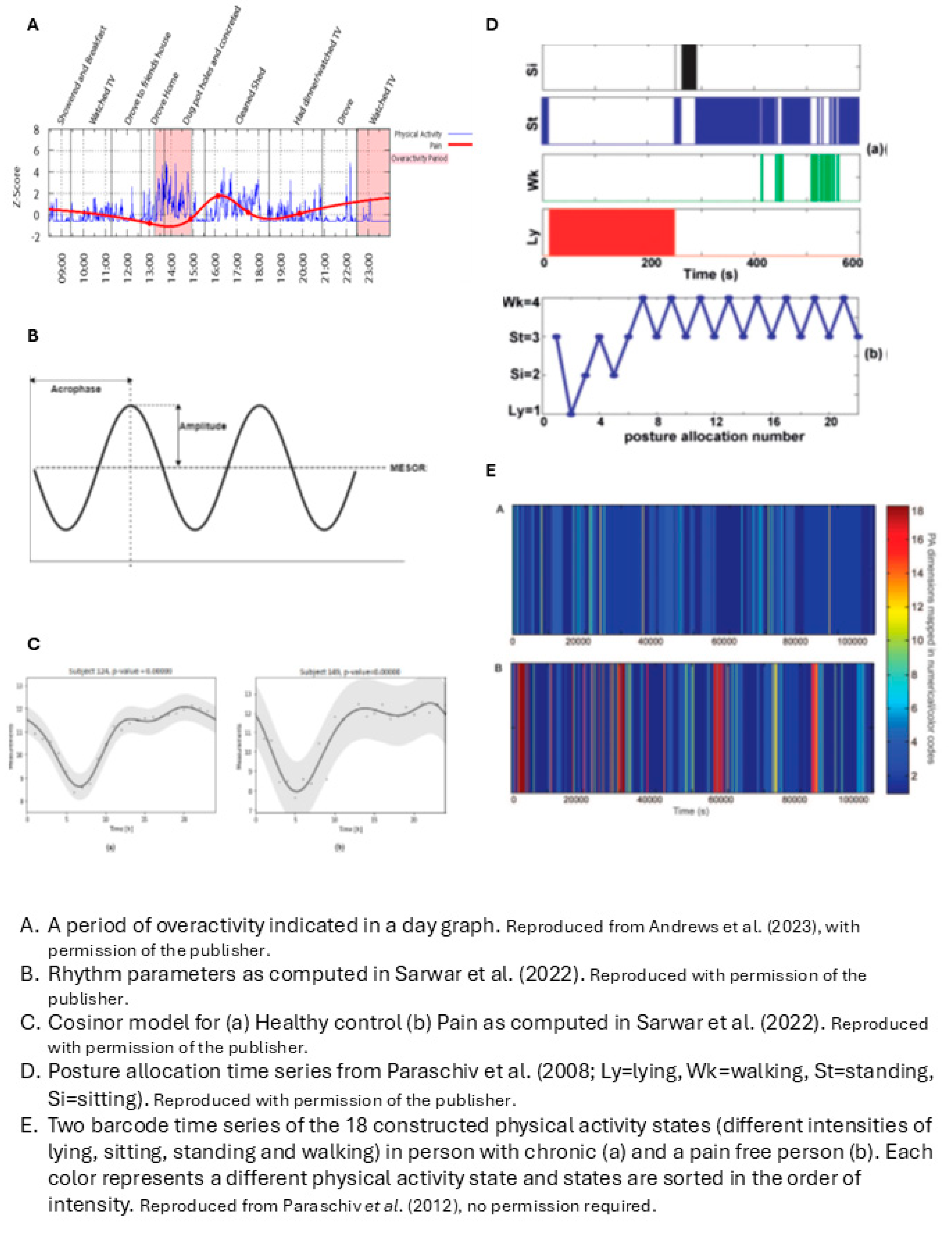
Figure 4.
Direction of associations of objectively measured activity pattern parameters with behavior type.
Figure 4.
Direction of associations of objectively measured activity pattern parameters with behavior type.
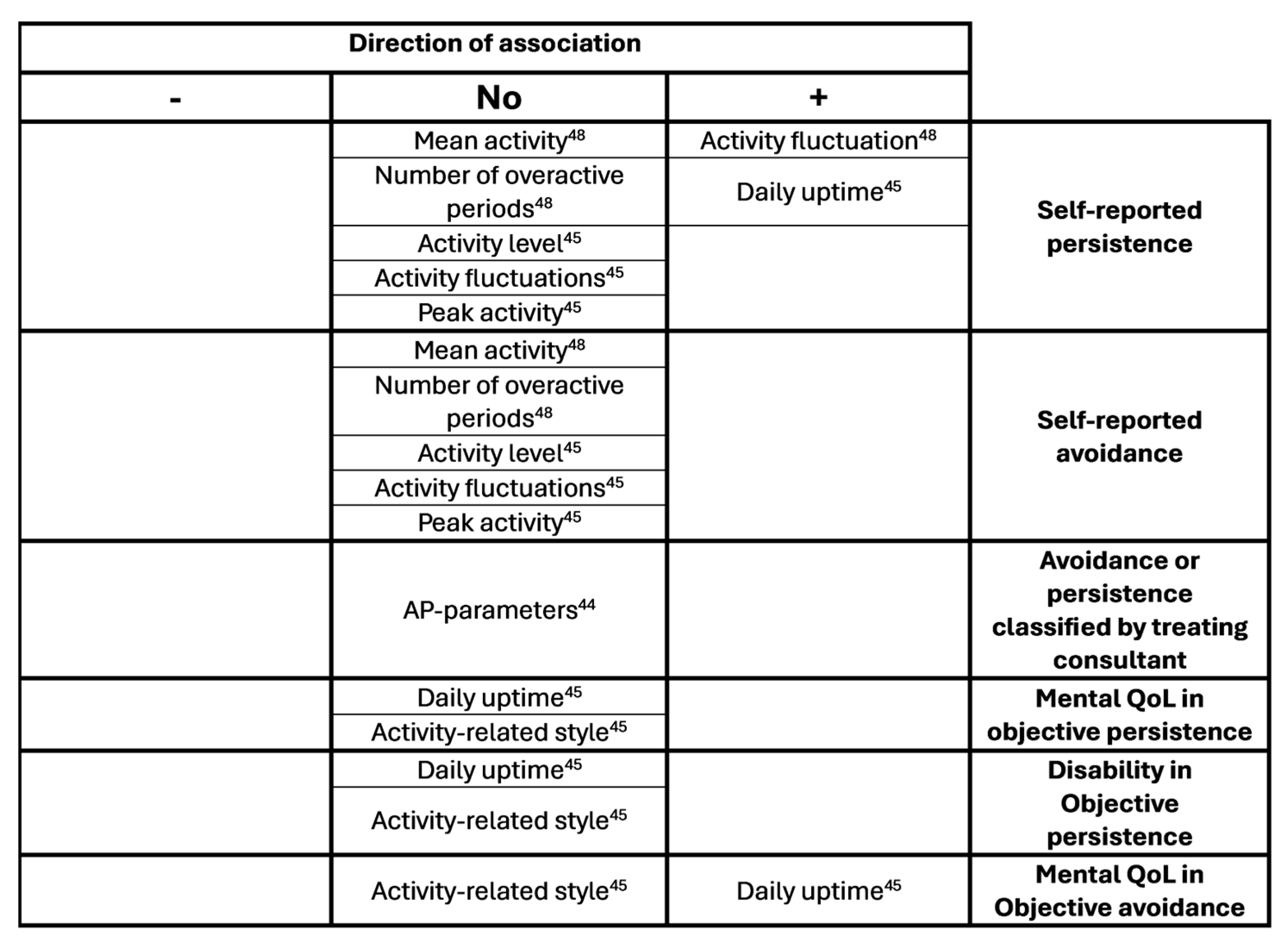
Figure 5.
direction of associations of objectively measured activity pattern parameters with self-discrepancy types.
Figure 5.
direction of associations of objectively measured activity pattern parameters with self-discrepancy types.
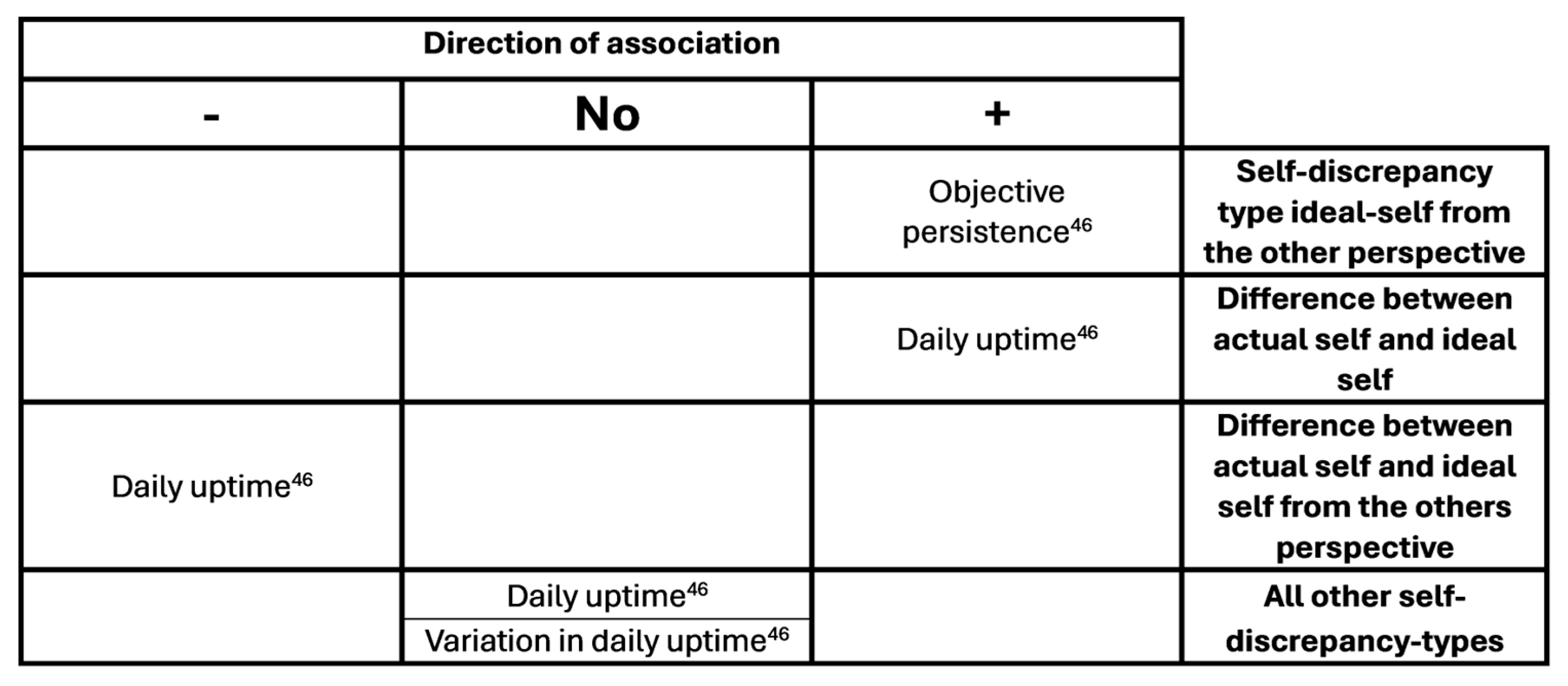
Figure 6.
Direction of associations of objectively measured activity pattern parameters with clinical outcome measures.
Figure 6.
Direction of associations of objectively measured activity pattern parameters with clinical outcome measures.
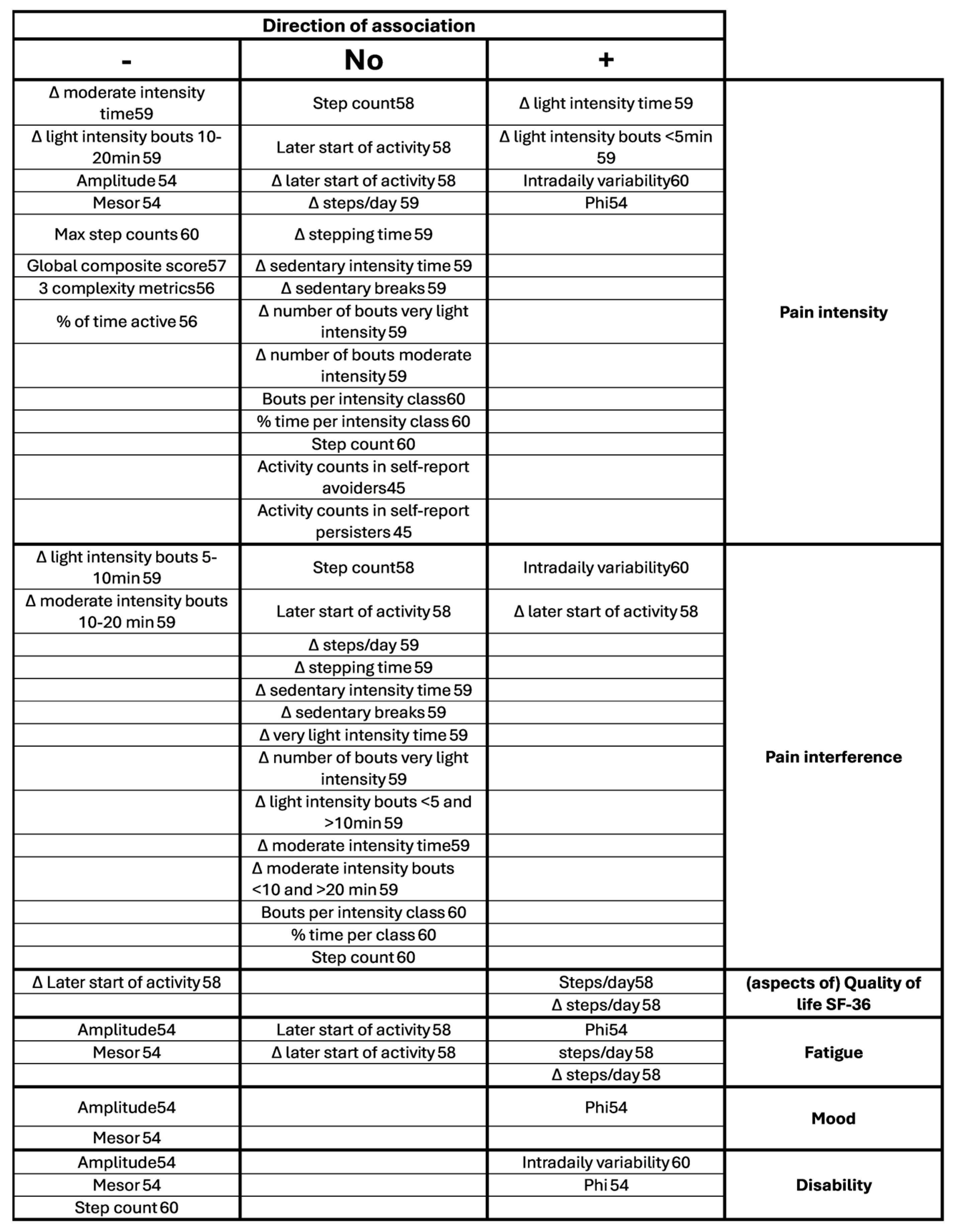

Table 1.
Characteristics of the included papers.
| Author (year) | Study design | Aim of the study related to AP |
Sample size | Sample description | Sex (female/male) |
Age (sd), range |
|---|---|---|---|---|---|---|
| Andrews (2014)[61] | Cross-sectional | (part of the research) Associations of overactivity with sleep |
50 | CP from MPC, outpatient, persistent non-cancer at least 3 months, generalized pain affecting gross movement, English literate, >18yrs, exclusion = sleep disorder. | 30/20 | 53.22 (10.68), 33-73 |
| Andrews (2015)[48] | Cross-sectional | Associations of objective overactivity with self-report overactivity and avoidance |
68 | CP from MPC, non-cancer, generalized distribution with impact on gross movement. | 44/24 | 52.85, (11.40), 25-73 |
| Andrews (2023)[49] | Longitudinal cohort baseline, week 7 and week 13 | Differences in pacing and avoidance pre- and post- treatment | 20 | CP from tertiary MPC, selection on overactivity behavior with difficulty implementing pacing strategies and activity-related exacerbations. | 9/11 | 46.9, (NR), 20-67 |
| Fanning (2023)[59] | Longitudinal cohort, Baseline and week 12 |
Associations of time spent in and bout lengths of different stepping intensities with pain intensity and interference. Change after 12 weeks behavioral program on PA or 12-week control group. |
41 | CP at least at two sites of neck, shoulder, back, hip or knee, included by physician for online telecoaching and mHealth intervention, BMI 30-45 kg/m2, self-reported to be low active, weight stable and no contraindications for exercise. |
30/11 | 69.61 (6.48) |
| Fanning (2024)[58] | Longitudinal cohort, Baseline and week 12 |
Associations of stepping patterns with pain and QoL. Change after 12 weeks behavioral program on weight loss and PA. |
68 | CP at least at two sites of neck, shoulder, back, hip or knee, included by physician for online telecoaching and mHealth intervention, BMI 30-45 kg/m2, self-reported to be low active, weight stable and no contraindications for exercise. |
52/16 | 69.53 (6.74) |
| Huijnen (2011_1)[45] | Cross-sectional | Differences between avoiders, persisters, mixed performers and healthy performers as classified by POAM-P questionnaire Associations of pain intensity with objective activity in avoiders and persisters |
116 | CLBP from MPC, HDR and via advertisement, 18-65, no specific pathology, no psychiatric disease, no pregnancy | 36/43 | Avoiders 45.7 (9.8) , persisters 48.2 (8.4), mixed 44.2 (10.9), functional 50.6 (12.5) |
| Huijnen (2011_2)[46] | Longitudinal cohort, baseline, 6 months | Associations between self-discrepancy type and objective avoidance and persistence. Change over time. |
116 | CLBP from MPC, HDR and via advertisement, 18-65, no specific pathology, no psychiatric disease, no pregnancy | T1 39/45, T2 23/26 | 47.5 (10.5), 47.8 (10.9) |
| Huijnen (2020)[44] | Cross-sectional | Differences in objective avoidance and persistence between patients classified by their treating consultant as avoider or persister | 16 | CLBP from MPC and HDR (>6 months, 18-65), no specific pathology, no pregnancy, no pacemaker, no serious psychiatric disorder | 8/8 | Avoiders 50 37.5-55.0, persisters 46 45.0-59.0 |
| Liszka-Hackzell (2004)[55] | Longitudinal cohort 3 weeks continuously |
Differences between subgroups of chronic and acute pain | 15 CLBP, 15 acute pain | CLBP from MPC, pain >6 months. 18-75yrs, (acute <2wks) | CLBP 7/8 Acute 6/9 |
CLBP 51 (10.2) Acute 46 (10.6) |
| Neikrug (2017)[54] | Cross-sectional | Associations of activity rhythm parameters with FMS symptoms | 292 | Fibromyalgia from MPC, community physicians and advertisement | 272/20 | 45.1 (11.1), 21-65 |
| Paraschiv (2008)[22] | Cross-sectional | Differences of dynamics of human activity between CP and no pain. | 15 CP, 15 no pain | patients from MPC who are candidate for SCS | 7/8 | 66 (14) |
| Paraschiv (2012)[56] | Cross-sectional | Associations of dynamics of physical activity with categorized pain intensity (mild, moderate, severe) and age | 60 CP, 15 no pain | Patients from MPC who are candidate for SCS | 18/42 | No pain: 57 (14), severe pain middle age: 54 (9), moderate pain old age: 71 (14), severe pain old age: 74 (8) |
| Paraschiv (2016)[57] | Cross-sectional | Differences of parameters quantifying the multidimensionality of physical behavior between subgroups mild pain and moderate to severe pain | 74 CP, 18 no pain | 74 CP patients with chronic intractable pain and candidate for SCS | 48/44 | 63 (14) |
| Sarwar (2022)[60] | Cross-sectional | Develop machine learning algorithm to predict pain, pain intensity, pain interference and disability from cumulative and relative activity measures, sleep measures and rest activity rhythm measures. Associations between rhythm measures and pain intensity, interference and disability |
25 CP, 27 no pain | 25 CP mixed | 10/12, (3 sex not specified) | NR |
| Zheng (2023)[47] | Cross-sectional | Differences of physical activity intensity patterns between subgroups in CLBP with high and low central sensitization. Differences with conventional cut-point approach. |
42 | Primary CLBP from MPC | 27/15 | 39.6 (12.6) |
Abbreviations: CP, chronic pain; MPC, Multidisciplinary pain center; HDR, Hospital department of rehabilitation; CLBP, Chronic low back pain; PA, Physical activity; SCS, Spinal cord stimulation; NR, Not reported.
Table 2.
Concepts, definitions of concepts and their operationalization with variables and indicators.
Table 2.
Concepts, definitions of concepts and their operationalization with variables and indicators.
| Author (year) | Concept related to activity patterns | Definition of concept (conceptualization) | Definition of variables (operationalization) | Indicators for variables |
|---|---|---|---|---|
| Andrews (2014) | (part of the research) Overactivity |
Overactivity: high levels of activity → severe pain aggravation + inactivity → sawtooth activity pattern with pain and activity fluctuating greatly over time |
Sawtooth pattern = higher fluctuation value of timeseries of vector magnitude of activity counts per minute | Fluctuation value = Root mean square of difference of 2 successive cumulative 15 min vector magnitude |
| Andrews (2015) | Overactivity |
Overactivity: being active in a way that significantly exacerbates pain → periods of incapacity |
Level of overactivity = number of overactive periods An overactive period is counted when pain aggravation occurs following a prolonged time of being sedentary or highly active |
Overactive period = pain aggravation (pain intensity z-score >1.65) AND sedentary task > 1hr OR High activity period (objective physical activity z-score > 1.65 for periods under an hour or >1.28 for periods over an hour. Within 2 hrs of pain aggravation |
| Andrews (2023) | Pacing Overactivity |
Overactivity: too long on an activity (being active or sedentary with sustained spinal position) → pain aggravation Pacing: decreased frequency of overactivity periods |
As Andrews (2015) | As Andrews (2015) |
| Fanning (2023) |
The pattern of PA accumulation (i.e. bout length) and rest accumulation | The pattern is described as 1. the time spent in light and moderate physical activity and in rest and 2. the breaks within light and moderate physical activity and rest Hypothesis: Greater sedentary time, fewer sedentary breaks, and sustained participation in more intensive activity will result in worse pain outcome |
Activity intensity equals Steps/minute Time spent in rest = Minutes/day being low-active in a seated or lying posture Time being active = Average daily steps and time stepping at different intensities Number of sedentary breaks = Postural shifts from sit to stand Breaks within activity intensities = count of bouts of a certain length (<1 min, 1-5 min, 5-10 min, 10-20 min and >20 min) for each activity intensity |
Activity intensity: Moderate: 100-125 steps/min Light: 75-100 steps/min Very light: <75 steps/min Rest: minutes classified by software as low-active in seated or lying position |
| Fanning (2024) |
The pattern of PA intensity throughout the day |
PA intensity equals stepping frequency (steps/minute) The PA pattern per participant can be expressed by Fourier functions It is hypothesized that patterns will differentiate in timing of activity and rest and in amplitude |
To summarize the PA pattern per participant, a 9-basis Fourier function is derived from the timeseries of steps/minute | Two different types of Fourier functions were distinguished with functional Principal Component Analysis: 1. Amount of stepping 2. Early vs. late risers |
| Huijnen (2011_1) | Avoidance Persistence |
Avoidance: try to escape from activities that are expected to increase pain or injury → low activity levels Persistence: continue activities until completion → increasing pain → forced rest → sawtooth pattern + longer daily uptime because of postponed rest |
1. Persistence = higher physical activity level, more fluctuations, longer daily uptime than avoiders 2. Persistence = increased pain after increased activity |
1a. Daily uptime = wear time. 1b. Mean total activity score = mean counts per day from raw data 1c. Highest activity score = 80% power of highest activity score of monitoring period 1d. Fluctuation score = sum of activity counts during 15 minutes, then root mean square of difference of 2 subsequent 15 minute-periods 2. Increased pain after activity = association between pain and activity level over time with two level hierarchical linear regression analysis |
| Huijnen (2011_2) | Avoidance Persistence |
Not mentioned, but as Huijnen 2011_1 (oral comment) | Persistence = higher scores on daily uptime and activity related style than avoidance |
Daily uptime as in Huijnen 2011_1. Activity related style is linear combination of daily uptime, mean total activity score, fluctuation score as in Huijnen 2011_1 |
| Huijnen (2020) | Avoidance Persistence |
Avoidance: catastrophizing thoughts about pain + fear of movement → lower daily activity levels Persistence: Continuing activities despite pain → activity levels similar to people without pain |
Avoiders will differ from persisters in 1. Overall daily activity level 2. Duration of being active vs sedentary , 3. Mean general motility (as a measure of intensity; m/s2), and walking motility 4. Number of transitions, and/or 5. Distribution of active vs sedentary behavior |
Distribution measures: 1. Number of active and sedentary bouts, i.e. periods classified as standing, walking, running, cycling or non-cyclic movements vs sitting or lying 2. Median bout length of active and sedentary behavior 3. Covariance of variation of bout length 4. Fragmentation: number of bouts of physical activity or sedentary divided by total duration of activity or sedentary. 5. W-index for activity or sedentary behavior = (total time of bout lengths above median bout length)/total duration. |
| Liszka-Hackzell (2004) | Activity-related pain | Increased activity → increased pain (with acute pain, not with CP) | Cross-correlation between pain level and activity counts per minute with time lag up to 60 minutes | Cross-correlation at different time lags of interpolated pain levels and activity level time series resampled to one sample every 10 min, with time-lags up to 60 min |
| Neikrug (2017) | Activity rhythms in fibromyalgia syndrome (FMS) | Activity rhythms factor in activity level, timing and duration over multiple days | Activity rhythm parameters: 1. Mesor, 2. Amplitude, 3. Phi, averaged over measurement period And the daily variation (standard error) of these 3 parameters compared to weekly average |
1. Mesor = mean activity level in units of the actigraph 2. Amplitude = distance between mesor and peak of curve, according to fitted 24-hr cosine model 3. Phi = time of day of the average peak activity over the week |
| Paraschiv (2008) | Dynamics of human activity |
Dynamics of human activity captured by timeseries of: Sequence of postures Timing Time spent in a posture Any combination |
The temporal pattern of each timeseries is quantified with fractal analysis and symbolic dynamic statistics 4 time series: 1. Sequence of posture allocation. 2. Duration of walking periods. 3. Timing of activity-rest transitions as point process. 4. Context dependent symbolic description of the sequence of successive activity-rest periods. |
1. Detrended Fluctuation Analysis (DFA) on categorical time series of posture allocation of 4 classified postures (lying, sitting, standing, walking) 2. Cumulative Distribution Function and DFA on sequence of walking episodes characterized by their duration 3. Fano Factor Analysis on time series of the moment in time of transitions from rest (sitting and lying) to activity (standing and walking) and v.v. 4. Symbolic dynamics statistics on symbol series created by coding the comparison of the duration of each activity period with the rest periods just before and after. Values are 0 or 1, 0 = rest period equals activity period. Constructing word sequences from the symbol series |
| Paraschiv (2012) | Dynamics of sequences of various physical activity states | Dynamics of states are related to structural complexity. Structural complexity depends on the variety of physical activity states and their occurrence in time |
Structural complexity: metrics from timeseries of physical activity states: 2 states of lying/sitting dependent on acceleration, 4 states of standing dependent on acceleration, 11 states of walking dependent on cadence and duration |
Metrics are determined from timeseries of 18 possible physical activity states, variety of states, temporal structure of state-sequence 1. Complexity metrics: information entropy, Lempel-Ziv complexity and sample entropy 2. Quantitative global metrics: time% spent walking and/or standing 3. Composite deterministic score: sum of the three normalized complexity scores * time% being active 4. Composite statistical score with linear discrimination analysis |
| Paraschiv (2016) | Multidimensionality of physical behavior | Individual physical behavior: Multidimensional attributes (like type, intensity and duration of activities, movements and postures) Dynamic attributes (the change over time) Relational attributes (factors that modulate behavioral patterns) |
Multidimensionality = composite score from metrics quantifying Type Duration Intensity Temporal pattern |
Composite score from factor analysis with metrics: 1. % of time walking, % of time on feet 2. 0.975th upper quartile of bout lengths of being active 3. Excess rest vs deficit rest by plotting cumulative distribution of excess and deficit rest and calculate Kolmogorov-Smirnov distance 4. three types of entropy on timeseries of 18 different states described in Paraschiv 2012 |
| Sarwar (2022) | Rest-activity circadian rhythm |
Rest-activity rhythm is quantified by Parameters derived from a fitted cosine curve Intradaily (hour to hour) variability (IV) as a measure of circadian disturbance. IV = the change of activity level from hour to hour. Higher IV indicates more daytime napping or nighttime arousal |
Rhythm is quantified with 1. Eight rhythmic features from a cosine curve fitted to 24h timeseries of activity counts and 2. Intradaily variability of hour-to-hour activity counts |
Eight rhythmic features from a cosine curve that is fitted to a 24h timeseries of activity counts: 1. Mesor 2. Acrophase 3. Amplitude, 4. Relative amplitude = amplitude/mesor 5. Multi-scale entropy (pearson's sample entropy), 6. Mean activity during the most active 10h (M10, as an estimate of daily activity), 7. Mean activity during the least active 5h (L5, as an estimate of nocturnal activity), 8. rest-activity relative amplitude ((M10-L5)/(M10+L5)), Intradaily variability: Where: N is the total number of datapoints, xi are the individual data points and μ is their mean |
| Zheng .(2023) | Physical activity intensity patterns |
Physical activity intensity patterns: Temporal organization of physical activity intensity levels Transition between physical activity intensity levels |
Pattern: Bout duration of 5 hidden states reflecting 5 intensity levels Accumulated time per hidden state per day Transition probability from one hidden state to every other hidden state Hidden states: Derived from accelerometer time series with a machine learning algorithm Reflect 5 intensity classes |
Pattern = One value of bout duration per intensity class One value of accumulated time per intensity Values for transition probability from each intensity to each other intensity |
Abbreviations: PA, Physical Activity.
Table 3.
Measurement properties and data processing.
| Author (year) | Device | Wear location |
Measurement frequency | Duration | Other principal variables for AP-related concept of study |
Other variables for associations, differences between groups or treatment results |
Valid data definition | Epoch length | Conversion method |
|---|---|---|---|---|---|---|---|---|---|
| Andrews (2014) | GT3X Actigraph | NR | 30 Hz | 5 days + nights, at least 1 weekend day | Pain intensity 11-point VAS, (mood, stress, catastrophizing) 6x/day | Parameters of sleep derived from accelerometry | NR | 1 minute | Activity counts per minute and then vector count per minute |
| Andrews (2015) | GT3X Actigraph | NR | 30 Hz | 5 days, at least 1 weekend day | Pain intensity 11-point VAS, 6 times/day at random intervals. Diary | Self-reported approach to activity (PARQ) | 4 complete days for each parameter | 1 minute | Activity counts per minute and then vector count per minute |
| Andrews (2023) | GT3X Actigraph | Waist | NR | 5 days | Pain intensity (not specified), 1/hr, interpolated to 1/min | Average pain, average activity level, medication intake, self-reported overactivity, avoidance, depression, anxiety, stress and time in leisure, social, rest or productive tasks. | (1) At least 75% of waking hours could be accounted for by diary activities entered in the Pain ROADMAP app and (2) Actigraph data were available for this same time period. At least five of the 7days of monitoring needed to be classified as a valid data collection day for the whole monitoring period to be considered valid |
1 minute | GT3X automatically converses changes in tri-axial acceleration to activity counts per minute. Vector magnitude from activity counts per minute in 3 axes was calculated |
| Fanning (2023) |
ActivPAL 4 |
Upper midline of thigh | NR | 7 days | None | PROMIS Pain intensity scale, PROMIS Pain interference scale | 3 days | NR |
Data processing with PALBatch 8.11.63. Classification to stepping, lying and sitting with CREA algorithm 1.3 Ambulatory activity intensity is derived from stepping cadence bands |
| Fanning (2024) |
ActivPAL 4 |
Upper midline of thigh | NR | 7 days | None | PROMIS Pain intensity scale, PROMIS Pain interference scale, Health-related quality of life with SF-36 (physical function, emotional role limitations, physical role limitations, energy/fatigue, emotional well-being, social function, pain and general health) | 3 days | 1 minute | Data processing with PALBatch 8.11.63. Data classification with CREA algorithm 1.3. Both not specified |
| Huijnen (2011_1) | RT3 | NR | NR | 14 days | Pain intensity 8x/day 7-point Likert-scale | Classification of participants as avoider, persister, mixed performer or functional performer with POAM-P | At least 5 days including 1 weekend day. 1 valid day has at least 10hrs. | 1 minute | 1. Resultant vector from 3D signal. 2. counts per minute of exceedance of predefined threshold. For association with pain: mean activity signal between two pain measurements |
| Huijnen (2011_2) | RT3 | NR | NR | 14 days | None | Self-discrepancy type with HSQ, age, gender, pain duration, mean pain intensity | At least 5 days including 1 weekend day. | 1 minute | As in Huijnen 2011 (1) |
| Huijnen (2020) | VitaMove activity monitor | Chest + left and right thigh | 128 Hz | 5 days | None | Classification of participants as avoider or persister by treating consultant | Number of days flexible. | 1 sec for analyses of postures, motions and transitions | Detection of postures and motions 1/sec with VitaScore Software |
| Liszka-Hackzell (2004) | AW-64 actiwatch | Non-dominant arm | NR | 3 weeks | Pain 11-point VAS at least every 90 minutes | Having chronic or acute LBP | At least 14 complete days of activity and pain | 1 minute | Activity was sampled as accumulated counts/minute |
| Neikrug (2017) | MicroMini-Motionlogger Actigraph | Non-dominant wrist | 32 Hz | 7 days | None | Pain severity and interference (MPI), physical impairment and functioning (FIQ), fatigue (MFI), mood (CESD), sleep (from actigraph) | Equal or less than 1 night missing or less than 8hrs missing data during the day | 1 minute | With actigraph Action-3 software, outcome parameter not specified |
| Paraschiv (2008) | 1 biaxial and 1 uniaxial accelerometer ADXL202 + gyroscope | Biaxial chest, uni-axial thigh, gyroscope thigh + shank | 40 Hz | 5 weekdays, 8hrs/day | None | None | NR | 1 sec | Discrete wavelet transformation, Savitzky-Golay smoothing filters and numerical gradient on raw data. Then: 1. type of activity with previously developed algorithm [62] 2. intensity of walking from mean walking cadence during each walking period. 3. intensity of sitting lying standing with trunk acceleration norm |
| Paraschiv (2012) | 3x biaxial ADXL202 + gyroscope | Sternum, mediolateral thigh, shank | 40 Hz | 5 weekdays, 8hrs/day | None | Pain-score classified as no, moderate and severe pain. Age classified as middle age and old age | NR | 1 sec | As Paraschiv et al. (2008) |
| Paraschiv (2016) | 2x triaxial MMA7341LT + gyroscope |
Sternum and mediolateral axis of thigh | 40 Hz | 5 weekdays, 8hrs/day | None | Pain-score VAS classified as mild pain (VAS≤4) and moderate to severe pain (VAS>4), | NR | 1 sec | As Paraschiv et al. (2008) |
| Sarwar (2022) | Actigraph GT3X | Wrist | NR | 5 days +nights on weekdays | None | Average pain intensity, pain interference and disability with PROMIS-29 v2.0 | Days with at least 20% of complete data were included | 1 hour | Activity and sleep variables with algorithms from ActiLife software, resampled to 1 hr and smoothed with 3h simple moving average |
| Zheng (2023) | GT3X | Front right hip (Anterior superior iliac spine) | 100 Hz | Approx. 1 week, excl sleeping and bathing | None | Central sensitization symptoms with CSI | Days with complete 24hr covered. 4 days, randomly selected | 5 sec | Gravity effects removed from raw data, vector magnitude calculated, averaged over 5s. For comparison with conventional cut points approach: Resampled to 30 Hz, then bandpass Butterworth filter with 4 orders, then filter with coefficient matrices from Brønd [63] |
Abbreviations: NR, not reported; SF-36, 36-item short-form survey; HSQ, Hardin’s selves questionnaire; POAM-P, patterns of activity measure – pain; TSK, Tampa Scale of Kinesiophobia; LBP, low back pain; MPI, multidimensional pain inventory; FIQ, fibromyalgia impact questionnaire; MFI, multidimensional fatigue inventory; CESD, center for the epidemiological studies depression scale; PARQ, physical activity readiness questionnaire; PROMIS-29, patient-reported outcomes measurement information system – 29; CSI, central sensitization inventor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



