
Submitted:
08 November 2023
Posted:
09 November 2023
You are already at the latest version
Abstract
Chronic Low Back Pain (CLBP), defined as pain persisting for at least 12 weeks, is a significant public health issue, with prevalence intensifying due to an ageing global population, amassing approximately 619 million cases in 2020 and projected to escalate to 843 million by 2050. Given the multitude of therapeutic modalities available for CLBP, this research sought to ascertain their respective efficacies in ameliorating pain and disability. We specifically scrutinized Multidisciplinary Biopsychosocial Rehabilitation (MBR) among adults enduring non-specific low back pain for over 12 weeks, excluding acute pain conditions and pre-study surgical interventions. MBR is an approach encompassing various modalities, including exercise, behavioral therapies, educational programs, and work conditioning aspects, necessitating a comprehensive Network Meta-Analysis (NMA) to fully grasp the extensive scope of its impact. The constructed network comprised diverse MBR modalities (behavioral, educational, and work conditioning) alongside exercise therapy (ET), minimal intervention, and usual care, serving as controls with pain and disability as outcomes. Through the analysis of 4,619 initially identified studies, 93 were included, encompassing a total of 8,059 participants. The NMA conducted substantiated that both ET and MBR modalities were notably effective in alleviating CLBP, with education-oriented MBR emerging as the most efficacious for pain mitigation and behavior-focused MBR for disability reduction. Nevertheless, the discerned differences amongst the treatments were minimal and uncertain, highlighting that no modality was definitively superior to the others. The analysis revealed low global and local inconsistency within the network, underscoring the reliability of the observed outcomes. Given the intricate nature of CLBP, embodying various facets, our findings advocate for a combined therapeutic approach to optimize treatment efficacy. Nonetheless, the presence of high study heterogeneity and potential biases necessitates cautious interpretation of the results, prompting future research.
Keywords:
chronic low back pain
; multidisciplinary biopsychosocial rehabilitation
; exercise therapy
; network meta-analysis
1. Introduction
Chronic low back pain (CLBP) is characterized by pain and discomfort localized below the inferior margin of the 12th ribs and above the inferior gluteal folds, persisting for a duration of at least 12 weeks, usually without a specific cause of the pain [1]. In contrast, acute low back pain is often transient and has a clear underlying cause, such as mechanical injury while the etiology of CLBP is often multifactorial, encompassing structural, biomechanical, neurological, psychological, and social elements. While the general prognosis is good, the high prevalence rate is what makes CLBP a major public health issue, especially given that CLBP prevalence increases linearly with age [2] and the global population is ageing [3]. In 2020 number of low back pain cases was estimated to be 619 million (95% Uncertainty Intervals (UI) 554 – 694), with a projected number of cases rising to 843 million (95%: UI 59 – 933) by year 2050 [4]. Globally pooled, overall cost, per patient, per annum was estimated at 10,100 (95% CI 6,100$ – 14,200$) [5].
According to clinical guidelines, exercise therapy (ET) is broadly recommended as the first line of treatment for reducing pain and disability with no clear evidence supporting any specific modality over the others [6]. Given the multifactorial nature of CLBP causes, as well as the influence of psychosocial patient aspects of pain and disability [7], exercise therapy is often paired with various other forms such as pharmacotherapy (paracetamol, nonsteroidal anti-inflammatory drugs), patient education, psychosocial interventions, work hardening, and multidisciplinary rehabilitation. Alternatively, invasive treatments, such as surgery, spinal injections, and radiofrequency denervation are also used [6,8,9]. An updated overview that collected national clinical practice guidelines identified that 9 out of 11 guidelines recommend multidisciplinary rehabilitation [8].
Multidisciplinary biopsychosocial rehabilitation (MBR) is a comprehensive approach to the management of conditions like chronic low back pain (CLBP). It is rooted in the biopsychosocial model, which posits that biological, psychological, and social factors all play significant roles in human functioning in the context of disease or illness [10]. Key to the MBR approach is that the intervention program should be delivered by a team of healthcare professionals from different backgrounds. This team may include physicians, psychologists, physiotherapists, social workers, occupational therapists, and others. At least two professionals from different backgrounds should be involved in the intervention delivery [11]. It’s vital that the various components of the intervention are integrated and that there is active communication between the providers responsible for different aspects of the patient’s care.
While research into MBR as a treatment option for CLBP has shown [10,12] its viability, similarly to ET there are no recommendations as to what modality of MBR has the largest effect on pain and disability, nor how does ET, a first-line treatment, compare with various modalities of MBR. A network meta-analysis, which simultaneously compares multiple treatment modalities, is potentially more effective for comparing treatment options. The research question posed in this systematic review is:
How do the modalities of multidisciplinary biopsychosocial rehabilitation (MBR) compare to exercise therapy (ET), usual care (UC), and minimal intervention (MI) in terms of efficacy for short-term pain and disability relief in individuals with chronic low back pain?
2. Materials and Methods
2.1. Protocol and registration
2.2. Eligibility criteria
Study characteristics adhered to the PICOS framework:
Population: The systematic review focused on adult individuals (18+ years old) with non-specific low back pain persisting for longer than 12 weeks. Studies examining individuals with serious medical conditions that mimic CLBP symptoms such as trauma injury, compressive vertebral fracture, disc herniation, spinal stenosis, rheumatic disease, and cancer were excluded. Conditions like disc degeneration, bulging disc, and osteoarthritis of facet joints were included, given their commonality and often non-severe symptoms. In terms of context, studies in outpatients’ clinics and other clinical settings were included. No context-related exclusion criteria were identified.
Intervention: In the context of this systematic review, MBR was characterized as an intervention that includes a physical component, such as an exercise program or similar physiotherapy intervention, combined with at least one other component drawn from the psychological or social and occupational domains of the biopsychosocial model. We initially considered studies examining four modalities: behavioral (MBR-BE), biofeedback, work/physical conditioning programs (MBR-WR), education programs (MBR-ED) based on previous systematic reviews [10,15].
Studies where surgical intervention was undertaken at any point before intervention were excluded, but studies that used pharmacotherapy along investigated therapeutic modalities were included.
Comparator: Three comparators were used for the network. Exercise therapy (ET), and two Controls - minimal intervention (MI) or usual care (UC). Comparator was classified as MI if the study stated explicitly that no therapy was provided for the participants. This includes participants on waiting lists and participants who were instructed how to generally manage CBLP but were never given any specifics on exercise or how to modify their activities. UC received standard care for CLBP, usually including some form of physiotherapy and/or general exercises for lower back issues. Studies featuring surgical intervention before ET, MI, or UC as comparators were excluded.
Outcome: The main outcomes were pain and disability. Pain was primarily measured via the Visual Analogue Scale, McGill Pain Questionnaire, Numerical Rating Scale, while disability was measured via the Roland Morris Disability Questionnaire, Quebec Back Pain Disability Scale, Oswestry Low Back Pain Disability Questionnaire, Pain Disability Index, and Hannover Functional Ability Questionnaire. For inclusion, only outcomes measured immediately after intervention were considered for this study.
Study Design: Only randomized controlled trials (RCT) were included in the systematic review.
2.3. Information sources & Search strategy
Information sources included the following electronic databases: MEDLINE, PEDro, EMBASE, CINAHL, CENTRAL, and PsycINFO. The literature search included studies up to March 4, 2022. No gray literature, clinical trial registries or regulatory agencies websites were searched. Authors of included studies were contacted if any clarification or additional data was needed for their studies. The complete search strategy is available in supplement materials (Document S1).
2.4. Study selection
Studies were screened by title and abstract independently by two researchers (KD & LE). Any disagreements were resolved by a third researcher (IJ). Full text selection was conducted by the same researchers. Studies were considered eligible if they compared any combination of ET, MBR, and either Control (MI or UC). Studies were excluded if the pain experienced by the participants was explicitly stated to be specific and acute. If no such statements were made, we examined the inclusion criteria for specific diagnoses and reviewed the sample description for reported pain duration to determine whether the underlying cause of the pain was nonspecific. Studies were also excluded if they did not measure pain or disability. The review process utilized the Covidence review management system [16].
2.5. Data collection process & Data items
Raw data were extracted to a prepared data extraction form from eligible studies by two researchers (KD & LE). A third researcher (IJ) extracted data that needed recalculation (i.e., standard errors (SE) to standard deviations (SD), or medians to means), or if only the graphically presented data were available. If it was not possible to extract the data, authors of the original studies were contacted twice to supply their data. The last step was to check whether the extracted data matched the data used in previous similar systematic reviews and meta-analyses [10,17]. As a final measure, due to strong relationships between means and SDs of all studies, the SDs for two studies with missing data were imputed using a linear regression model.
Along with the intervention groups, mean, SD and sample size, the following variables of interest were extracted with the purpose of inclusion in the analysis: specific measures used for both pain and disability outcome assessment, number of male and female participants per intervention group, mean duration of therapeutic intervention in weeks, mean length of therapeutic interventions in hours per week, mean age, mean BMI, mean duration of symptoms in months.
2.6. Geometry of the network
The network incorporates multidisciplinary biopsychosocial rehabilitation with following modalities: behavioral (MBR-BE), education programs (MBR-ED), work/physical conditioning (MBR-WR), and exercise therapy (ET). Finally, Usual Care (UC) and Minimal Intervention (MI) were also included as nodes. Minimal intervention was used as the reference treatment. Geometry of the network is represented in network diagram (Figure 1).
2.7. Risk of bias within individual studies and across studies
Risk of bias was assessed at the study level by Cochrane’s Risk of Bias 2 tool [18]. Studies were categorized by their Overall Risk of Bias into low bias, some concerns and high bias categories. The Overall Risk of Bias in our network meta-analysis was determined by an algorithm that considered the importance and level of bias across different domains. We identified D1, D3, and D4 as the most impactful domains for the bias assessment due to their inherent attributes in study design and data management. Rob 2 algorithm for Overall Risk of Bias is detailed in the supplement materials (Document S2). Rob 2 was visualized by robvis tool [19].
The possible presence of publication bias was evaluated using funnel plots and Egger’s test.
2.8. Summary measures
Data collection and analysis were performed based on outcomes and specific data points. Diverse visual analogue scales for pain outcomes were rescaled to 0-100, employing a similar approach as in the most recent Cochrane review on a related topic [17]. As for disability outcomes, multiple scales were also utilized. These Health-Related Quality of Life Questionnaires (HRQoL), which are inherently more complicated than visual analogue scales, were maintained as raw data for the calculation of Hedges’ g standardized mean difference (SMD) effect size estimators [20].
Since we are primarily interested in modalities of MBR, if a particular study had more than one ET modalities, their means and SDs were pooled together according to procedures for pooling groups descried in Cochrane’s manual [21].
2.9. Planned methods of analysis
All statistical analyses were conducted using the R statistical software (version 4.3.1), utilizing the netmeta package for network meta-analysis (NMA) [22].
For the analysis, a frequentist random-effects NMA was conducted, and multi-arm studies were integrated into the network. The non-independence of these multi-arm studies was addressed by reweighting all comparisons within each study.
2.10. Assessment of Heterogeneity & Inconsistency
Due to high expected heterogeneity, the restricted maximum-likelihood estimator (REML) was used for calculating between-study variance (tau2), with Q-profile for calculating the confidence interval of tau2 and tau. Treatment rankings were determined using P-scores, which are the frequentist counterparts of SUCRA values [20]. Global inconsistency was evaluated using the Q statistic based on full design-by-treatment interaction random effects model (DBT model), whereas local inconsistencies were assessed through node-splitting analysis.
2.11. Additional analyses
Given that we expected high heterogeneity and inconsistency, a Bayesian network meta-analysis, using the same dataset and non-informative priors, employing Markov Chain Monte Carlo simulation with 105 iterations and a burn-in period of 5,000 iterations was performed as a sensitivity analysis to better assess uncertainty and to perform a network meta-regression analysis using RoB 2 as a covariate. Treatment rankings by surface under the cumulative ranking curve (SUCRA) values were compared to rankings by frequentist P-value rankings.
3. Results
3.1. Study selection & Included studies charateristics
Initial databases search identified 4619 references and 4616 studies. Automated duplication screen removed 1836 as duplicates. Title and abstract screening phase removed 2308 studies and 380 additional studies were removed during full-text screening phase. Two thirds (66.8%) of the removed studies compared interventions that were of no interest for this systematic review and subsequent meta-analysis. Finally, 93 (87 for pain outcomes and 74 for disability outcomes) studies were marked for data extraction and analysis [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115]. PRISMA flow diagram can be found in supplement materials (Figure S1).
For screening, the inter-rater reliability, assessed using Cohen’s kappa, demonstrated moderate agreement in title and abstract screening (κ = 0.542), and fair agreement during the full-text screening phase (κ = 0.357).
Table 1 summarizes the basic parameters of population in the included studies. In our study, we included a total of 93 trials with a combined participant count of 8,059 individuals.
Most of the included studies (84 studies, 96.55%) employed the Visual Analogue Scale (VAS) as the primary instrument to gauge pain outcomes, with values ranging from 0-10 or 0-100. A few other scales, like McGill Pain Questionnaire (MGPQ, 2 studies, 2.3%), and Pain Rating Chart (PRC, 1 study, 1.15%), were also used. Regarding disability outcomes, the Roland-Morris Disability Questionnaire (RMDQ, 41 studies, 47.13%) and the Oswestry Disability Index (ODI, 30 studies, 39.19%) were the most utilized. Other scales used include the Quebec Back Pain Disability Scale (QBPDS, 3 studies, 4.05%) and Physical Disability Index (DI, 1 study, 1.35%). Table of study characteristics of pain and disability outcomes, comparisons, and number of participants per study is available in supplement materials (Table S1).
3.2. Presentation of network structure & summary of network geometry
Figure 1 shows a network structure for pain and disaiblity outcomes respectively. Blue, light blue and gray tringles show presence of multi-arm studies in these particlular comparisons of nodes. Unsurprisingly, Exercise therapy in general, followed by minimal intervention and usual care are the most connected nodes to the network, while MBR modalities have fewer connections. There was only one included study evaluating biofeedback and it was merged into behavioral MBR group (MBR-BE) as these modalities are more closely related than the others.
3.3. Risk of bias within studies
Summary of the risk of bias, using Risk of Bias 2 tool is presented in Figure 2. In evaluating the risk of bias in our collected studies on chronic low back pain treatment we observed variability in quality. The risk of bias arising from the randomization process was generally low or of some concern, indicating satisfactory randomization procedures. Bias due to deviations from intended interventions varied, with some studies flagged for high bias, suggesting potential implementation discrepancies. Most studies maintained solid data integrity, indicated by the predominantly low bias due to missing outcome data. Conversely, we noted substantial variations in bias in the measurement of outcomes and in the selection of reported results, with several studies presenting high bias. Ultimately, the overall bias ranged broadly across studies. These variances underscore the necessity for caution and rigorous interpretation in interpretation of analysis. Complete risk of bias figure for included studies can be found in supplement documents (Figures S2–S5).
3.4. Results of comparions & synthesis of results
The league table (Table 2) summarizes the comparative effects of different interventions on pain outcomes, with Minimal Intervention (MI) serving as the reference therapy. In this table, the lower triangle presents the network meta-analysis (NMA) estimates, which integrate both direct and indirect evidence to provide comprehensive comparisons between interventions. Conversely, the upper triangle showcases direct comparisons derived solely from head-to-head trials between the specific interventions. A positive mean difference indicates that the row intervention is more effective than the column intervention by the stated amount.
Looking at NMA estimations, MBR education (ED) demonstrated the largest mean difference in reducing pain outcomes, with a value of 18.18 (95% CI: 13.06 to 23.30). This was closely followed by MBR behavioral (BE) with a mean difference of 16.96 (95% CI: 10.47 to 23.46). MBR work conditioning/hardening (WR) showed a mean difference of 12.72 (95% CI: 2.05 to 23.39) in pain reduction, while exercise therapy (ET) exhibited a mean difference of 12.37 (95% CI: 8.40 to 16.34). It’s noteworthy that some comparisons included negative lower limits in their confidence intervals, indicating nonsignificant effect. Table of mean differences and standard errors of pain and disability outcomes by study, is available in supplement materials (Tables S2 and S3).
Table 3 shows the direct comparison and NMA estimates concerning disability outcomes across varying interventions. A positive, higher value of standardized mean difference indicates that the row intervention is more effective than the column intervention by the stated amount. Looking at indirect estimations and using minimal intervention (MI) as the reference, MBR behavioral (MBR-BE) exhibited largest SMD of 0.88 (95% CI 0.46 to 1.30) with no direct comparison available.
MBR education (MBR-ED) displayed a significant reduction in disability with a standardized mean difference (SMD) of 0.67 (95% CI: 0.40; 0.94) while exercise therapy (ET) showed a relatively similar efficacy with an SMD of 0.53 (95% CI: 0.32; 0.74) in comparison to MI. The range of the associated 95% CIs underscores the variability and uncertainty in some of these estimates, making it crucial to interpret results with caution.
In the assessment of pain and disability outcomes, the treatments ranked based on their probabilities that a particular treatment is better than another treatment chosen at random (P-scores) revealed distinct hierarchies (Table 4). For pain outcomes, the MBR-ED took precedence with the highest P-score of 0.899, followed closely by MBR-BE at 0.826, and MBR-WR at 0.559. Parallel trends were observed in disability outcomes. MBR-BE led with a P-score of 0.940, MBR-ED was second at 0.761.
Modalities ranked 1st and 2nd for pain outcomes have very similar probabilities, which decline more sharply for the 3rd ranked modality in both outcomes. While examining rankings provides an approximation of the most useful therapeutic modality, it doesn’t paint the full picture. Although the calculation of P-scores accounts for variance, visually inspecting a forest plot with effect size estimates against a common reference therapy reveals the confidence surrounding the point estimate, and consequently, confidence in the rankings. Figure 3 summarizes MD/SMD for pain and disability when compared to minimal intervention. From the figure, for pain outcomes, MBR-ED appears the most successful, with MBR-BE as a close runner-up. Evaluating the SMDs and 95% CIs for disability outcomes, the first three modalities: MBR-BE, MBR-ED, and ET are all quite similar. While MBR-BE has the largest effect size, it’s reasonably uncertain which one is truly the most effective.
3.5. Exploration for heterogeneity & inconsistency
For the network assessing pain outcomes, the total Q statistic of 920.85 with 85 degrees of freedom (df) signifies considerable heterogeneity within the network (p<0.001). This heterogeneity can be partitioned into two parts: within-designs and between-designs. Significant heterogeneity was observed both within designs (Q=628.07, df=74, p<0.001) and between designs (Q=292.78, df=11, p<0.001). Under the assumption of a full design-by-treatment interaction random effects model, the Q statistic was non-significant (Q = 14.39, df=11, p=0.2124), suggesting no notable inconsistency between designs. Local inconsistency assessments highlighted two significant inconsistencies. Specifically, the comparisons ’exercise therapy vs MBR education’ and ’exercise therapy vs minimal intervention’ were found inconsistent with p-values of 0.044 and 0.046, respectively. Other therapeutic comparisons did not demonstrate significant inconsistency.
For the network assessing disability outcomes, significant heterogeneity was present, as indicated by a total Q statistic of 316.89 (df=70, p<0.001). The heterogeneity within designs was substantial (Q=282.52, df=65, p<0.001), and between designs, it was also significant (Q=34.37, df =5, p<0.001). Under the presumption of a full design-by-treatment interaction random effects model, the Q statistic for between designs was 9.53 (df=5, p=0.090), indicating possible inconsistency. When focusing on specific comparisons, three stood out. The comparisons ’exercise therapy vs minimal intervention’, ’MBR education vs minimal intervention’, and ’exercise therapy vs MBR education’ were statistically significant with p-values of 0.021, 0.008, and 0.045, respectively. All other comparisons were non-significant.
Comprehensive details regarding the heterogeneity and inconsistency of both network meta-analysis models are provided in the supplementary materials (Tables S3–S6, Figures S6 and S7).
3.6. Risk of bias across studies
For pain outcome Egger’s test showed no statistically significant results (p = 0.124). Visual inspection of the plot suggested a potential asymmetry, indicating the possibility that studies demonstrating non-positive effects of the experimental therapeutic modalities as opposed to Minimal intervention may be underrepresented in the published literature. While it is important to note that Egger’s test, despite its widespread use, is known to have low power and can fail to detect bias [116], funnel plot shows no significant symmetry deviation.
For disability outcomes both Egger’s test (p=0.003) and visual assessment of funnel plot suggest a possibility of publication bias. Funnel plots for both outcomes are available in the supplement materials (Figures S8 and S9).
3.7. Results of additional analyses
The results of the Bayesian network meta-analysis (BNMA), employing a non-informative prior distribution, largely corroborated the findings from the frequentist network meta-analysis (NMA). For pain-related outcomes, node-splitting analysis revealed no statistically significant inconsistencies among the comparisons. Notably, the therapeutic modalities were ranked according to SUCRA scores in a manner consistent with the frequentist ranking.
Similar outcomes were observed for disability-related endpoints. As in the frequentist NMA, the results exhibited substantial consistency, with the only inconsistency identified occurring in the comparisons between exercise therapy (ET) and minimal intervention (MI), as well as between ET and MBR-ED (MBR education), and between MBR-ED and MI. Table 5 presents the SUCRA scores for both pain and disability outcomes, demonstrating that the rankings of therapeutic modalities align with those derived from the P-scores.
Within the Bayesian framework, we conducted a network meta-regression employing the RoB 2 Overall domain as a moderator. Interestingly, this model did not provide any meaningful explanations for inconsistencies within the network. Furthermore, there were no significant differences in effect sizes when considering the grouping of studies into ‘low risk,’ ‘some concerns,’ and ‘high risk’ categories for both pain and disability outcomes. However, it is worth noting that effect sizes generally appeared more substantial in ‘low risk’ studies. For a comprehensive BNMA analysis of both outcomes, refer to the supplementary materials (Figures S10–S15).
4. Discussion
The aim of the research was to discern the efficacy of multidisciplinary biopsychosocial rehabilitation (MBR) modalities relative to exercise therapy (ET) for short-term pain and disability relief in chronic low back pain sufferers.
Our results support the previous research in regards the efficacy of ET and MBR modalities versus minimal intervention and usual care. The efficacy of ET versus minimal intervention or usual care is well established [17]. The MBR approach has less evidence to support its efficacy, but previous studies do show promise when compared to usual care [12] or exercise therapy [10]. When indirectly compared hierarchy emerged in the P-scores of the pain outcomes, with MBR-ED leading, followed by MBR-BE. Parallel to the findings on pain outcomes, a P-score ranking for disability outcomes positioned MBR-BE at the top rank, followed by MBR-ED. Both MBR-ED and MBR-BE showed larger effects on pain and disability than ET and MBR-WR which in turn, expectedly, showed larger effects than UC and MI. This demonstrates that better outcomes are associated with modalities that have enhanced physiotherapy interventions with a cognitive aspect, either through behavioral or educational modalities.
This should be examined through the multifactorial nature of chronic low back pain (CLBP). A recent systematic review [117] found that increased pain intensity, elevated body weight, lifting heavy objects at work, challenging work postures, and depression are the most commonly observed risk predictors for CLBP. Additionally, behaviors that aren’t adaptive, general anxiety, functional limitations during the episode, and particularly physically demanding work are distinctly linked to the persistence of symptoms. The most frequently identified protective factor against CLBP was regular physical activity. Given this variety of risk factors, it stands to reason that effectively addressing CLBP requires a multifaceted approach, as suggested by our results.
Defining which of these MBR approaches is superior is much more challenging. To our knowledge there is no previous attempt to try to assess different types of MBR against each other. While the results produced rankings, giving MBR-ED and MBR-BE highest rank of pain and disability outcomes, respectively, there is a high degree of uncertainty within the results, evidenced by wide confidence intervals, significant heterogeneity, and some local inconsistency within the network. This was generally anticipated, given similar findings in other studies [10,12,17] and because, by design, studies were broadly included and categorized to be relevant to clinicians, researchers, and policymakers, but such high heterogeneity is a deterrent to producing confident results. Even though ranking treatments favored MBR-ED for pain and MBR-BE for disability outcomes, the differences between the various MBR modalities are too minimal and uncertain to be clinically significant. Furthermore, for disability outcomes, ET cannot be reliably differentiated from its MBR counterparts.
4.1. Limitations
High heterogeneity, especially within designs, was present. Although consistency assessed under the assumption of a full design-by-treatment interaction random effects model was non-significant, three comparisons also showed local inconsistency. Employing the RoB 2 Overall domain as a moderator in the Bayesian framework, however, did not yield any significant results in explaining network heterogeneity and inconsistency. Regarding the exploration of heterogeneity, lack of sample characteristics data in many studies, such as age, male to female ratio, BMI, duration of symptoms, and use of medications prevented us from exploring the effects of study modifiers.
Additionally, in this analysis we did not analyze different forms of ET, which may help to narrow down the effect modifiers and differences in the effect sizes.
There is some evidence of publication bias in disability outcomes. The results of Egger’s test for pain outcomes were non-significant, the test’s low power warrants caution in its interpretation, potential underrepresentation of studies showing non-positive effects compared to Minimal intervention must be considered.
Furthermore, the inclusion of a diverse range of scales to measure disability outcomes introduces challenges in direct comparisons and synthesis of results.
Finally, like other systematic reviews, the undocumented use of pain medications might have influenced the results of the primary studies, thus making our estimates possibly biased.
4.2. Recommendations for stakeholders
Clinicians: Recognizing the multifaceted etiology of CLBP, while exercise therapy (ET) remains a mainstay, it might be prudent to augment ET with educational sessions. These sessions could elucidate potential pain triggers, preventive measures, and coping strategies for disability. Additionally, clinicians should remain attuned to patients’ psychological well-being, and, when deemed necessary, consider referrals for behavioral interventions to broadly address CLBP’s dual physical and emotional facets.
Researchers: The strength of network meta-analysis (NMA) lies in its ability to discern comparative effectiveness across a spectrum of treatments. However, ensuring that the results remain unbiased mandates careful attention to potential sources of heterogeneity and inconsistency within the network. Delving deeper into patient characteristics like age, gender distribution, BMI, clinical setting, intervention duration, and intensity could shed light on these disparities. Moreover, recognizing the intricacies of CLBP, it’s advisable to blend various interventions, encompassing educational components, behavioral modifications, and pain management tactics with ET in experimental designs to discern the optimal therapeutic combination.
Policy-Makers: CLBP’s impact transcends individual suffering, translating into significant socio-economic ramifications. Notably, MBR modalities, by virtue of involving multiple professionals, inherently command higher costs. While preliminary evidence suggests a potential edge in efficacy over ET, it would be counterintuitive to further compound the financial burdens associated with CLBP by advocating for costlier treatments without discernible clinical superiority. Hence, a thorough cost-benefit analysis is warranted to ascertain the most economically viable and clinically efficacious treatment modalities, potentially integrating salient components of MBR into standard ET.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, I.J. and I.L..; methodology, I.J and I.L.; validation, I.J.; formal analysis, I.J.; data curation, K.D and L.E.; writing—original draft preparation, I.J.; writing—review and editing, I.L.; visualization, I.J.; supervision, I.L. and J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Allegri, M.; Montella, S.; Salici, F.; Valente, A.; Marchesini, M.; Compagnone, C.; Baciarello, M.; Manferdini, M.E.; Fanelli, G. Mechanisms of Low Back Pain: A Guide for Diagnosis and Therapy. F1000Research 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of Chronic Low Back Pain: Systematic Review. Rev. Saúde Pública 2015, 49, 1. [Google Scholar] [CrossRef] [PubMed]
- World Social Report 2023: Leaving No One Behind In An Ageing World. Available online: http://desapublications.un.org/publications/world-social-report-2023-leaving-no-one-behind-ageing-world (accessed on 9 September 2023).
- GBD 2021 Low Back Pain Collaborators Global, Regional, and National Burden of Low Back Pain, 1990-2020, Its Attributable Risk Factors, and Projections to 2050: A Systematic Analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023, 5, e316–e329. [CrossRef] [PubMed]
- Fatoye, F.; Gebrye, T.; Ryan, C.G.; Useh, U.; Mbada, C. Global and Regional Estimates of Clinical and Economic Burden of Low Back Pain in High-Income Countries: A Systematic Review and Meta-Analysis. Front. Public Health 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- George, S.Z.; Fritz, J.M.; Silfies, S.P.; Schneider, M.J.; Beneciuk, J.M.; Lentz, T.A.; Gilliam, J.R.; Hendren, S.; Norman, K.S. Interventions for the Management of Acute and Chronic Low Back Pain: Revision 2021. J. Orthop. Sports Phys. Ther. 2021, 51, CPG1–CPG60. [Google Scholar] [CrossRef] [PubMed]
- Alhowimel, A.; AlOtaibi, M.; Radford, K.; Coulson, N. Psychosocial Factors Associated with Change in Pain and Disability Outcomes in Chronic Low Back Pain Patients Treated by Physiotherapist: A Systematic Review. SAGE Open Med. 2018, 6, 2050312118757387. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.-W.C.; Chenot, J.-F.; van Tulder, M.; Koes, B.W. Clinical Practice Guidelines for the Management of Non-Specific Low Back Pain in Primary Care: An Updated Overview. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2018, 27, 2791–2803. [Google Scholar] [CrossRef]
- Schaafsma, F.G.; Whelan, K.; van der Beek, A.J.; van der Es-Lambeek, L.C.; Ojajärvi, A.; Verbeek, J.H. Physical Conditioning as Part of a Return to Work Strategy to Reduce Sickness Absence for Workers with Back Pain. Cochrane Database Syst. Rev. 2013, 2013, CD001822. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J.; Apeldoorn, A.T.; Chiarotto, A.; Smeets, R.J.E.M.; Ostelo, R.W.J.G.; Guzman, J.; van Tulder, M.W. Multidisciplinary Biopsychosocial Rehabilitation for Chronic Low Back Pain. Cochrane Database Syst. Rev. 2014, CD000963. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, K.; Malmivaara, A.; Pohjolainen, T.; Hurri, H.; Mutanen, P.; Rissanen, P.; Pahkajärvi, H.; Levon, H.; Karpoff, H.; Roine, R. Mini-Intervention for Subacute Low Back Pain: A Randomized Controlled Trial. Spine 2003, 28, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Gianola, S.; Andreano, A.; Castellini, G.; Moja, L.; Valsecchi, M.G. Multidisciplinary Biopsychosocial Rehabilitation for Chronic Low Back Pain: The Need to Present Minimal Important Differences Units in Meta-Analyses. Health Qual. Life Outcomes 2018, 16, 91. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Jurak, I.; Delaš, K.; Erjavec, L.; Locatelli, I. Network Meta-Analysis of Exercise Therapy and Multidisciplinary Biopsychosocial Rehabilitation for Chronic Low Back Pain 2022.
- van Erp, R.M.A.; Huijnen, I.P.J.; Jakobs, M.L.G.; Kleijnen, J.; Smeets, R.J.E.M. Effectiveness of Primary Care Interventions Using a Biopsychosocial Approach in Chronic Low Back Pain: A Systematic Review. Pain Pract. Off. J. World Inst. Pain 2019, 19, 224–241. [Google Scholar] [CrossRef] [PubMed]
- Veritas Health Innovation Covidence Systematic Review Software Available online: www.covidence.org.
- Hayden, J.A.; Ellis, J.; Ogilvie, R.; Malmivaara, A.; Tulder, M.W. van Exercise Therapy for Chronic Low Back Pain. Cochrane Database Syst. Rev. 2021. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2020, n/a. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G.; Schwarzer, G. Ranking Treatments in Frequentist Network Meta-Analysis Works without Resampling Methods. BMC Med. Res. Methodol. 2015, 15, 58. [Google Scholar] [CrossRef] [PubMed]
- Julian PT Higgins; Tianjing Li; Jonathan J Deeks Chapter 6: Choosing Effect Measures and Computing Estimates of Effect. In Cochrane Handbook for Systematic Reviews of Interventions; 2022.
- Balduzzi, S.; Rücker, G.; Nikolakopoulou, A.; Papakonstantinou, T.; Salanti, G.; Efthimiou, O.; Schwarzer, G. Netmeta: An R Package for Network Meta-Analysis Using Frequentist Methods. J. Stat. Softw. 2023, 106, 1–40. [Google Scholar] [CrossRef]
- Ahmed, U.A.; Maharaj, S.S.; Van Oosterwijck, J. Effects of Dynamic Stabilization Exercises and Muscle Energy Technique on Selected Biopsychosocial Outcomes for Patients with Chronic Non-Specific Low Back Pain: A Double-Blind Randomized Controlled Trial. Scand J Pain 2021, 21, 495–511. [Google Scholar] [CrossRef]
- Almhdawi, K.A.; Obeidat, D.S.; Kanaan, S.F.; Oteir, A.O.; Mansour, Z.M.; Alrabbaei, H. Efficacy of an Innovative Smartphone Application for Office Workers with Chronic Non-Specific Low Back Pain: A Pilot Randomized Controlled Trial. Clin Rehabil 2020, 34, 1282–1291. [Google Scholar] [CrossRef]
- Alvani E; Shirvani H; Shamsoddini A Neuromuscular Exercises on Pain Intensity, Functional Disability, Proprioception, and Balance of Military Personnel with Chronic Low Back Pain. J. Can. Chiropr. Assoc. 2021 Aug652193-206 2021.
- Barone Gibbs, B.; Hergenroeder, A.; Perdomo, S.; Kowalsky, R.; Delitto, A.; Jakicic, J. Reducing Sedentary Behaviour to Decrease Chronic Low Back Pain: The Stand Back Randomised Trial. Occup. Env. Med. 2018, 75, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Bodes Pardo, G.; Lluch Girbes, E.; Roussel, N.A.; Gallego Izquierdo, T.; Jimenez Penick, V.; Pecos Martin, D. Pain Neurophysiology Education and Therapeutic Exercise for Patients With Chronic Low Back Pain: A Single-Blind Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Borys, C.; Lutz, J.; Strauss, B.; Altmann, U. Effectiveness of a Multimodal Therapy for Patients with Chronic Low Back Pain Regarding Pre-Admission Healthcare Utilization. PLoS ONE 2015, 10, e0143139. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.O.P.; Maher, C.G.; Latimer, J.; Hodges, P.W.; Herbert, R.D.; Refshauge, K.M.; McAuley, J.H.; Jennings, M.D. Motor Control Exercise for Chronic Low Back Pain: A Randomized Placebo-Controlled Trial. Phys. Ther. 2009, 89, 1275–1286. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Romiti, D. Effectiveness of Back School Program versus Hydrotherapy in Elderly Patients with Chronic Non-Specific Low Back Pain: A Randomized Clinical Trial. Acta Biomed 2014, 85, 52–61. [Google Scholar] [PubMed]
- Cruz-Diaz, D.; Romeu, M.; Velasco-Gonzalez, C.; Martinez-Amat, A.; Hita-Contreras, F. The Effectiveness of 12weeks of Pilates Intervention on Disability, Pain and Kinesiophobia in Patients with Chronic Low Back Pain: A Randomized Controlled Trial. Clin. Rehabil. 2018, 32, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Adams, N.; Salazar, J.A.; Belles, A.; Hazañas, S.; Arroyo-Morales, M. Deep Water Running and General Practice in Primary Care for Non-Specific Low Back Pain versus General Practice Alone: Randomized Controlled Trial. Clin. Rheumatol. 2012, 31, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Darnall, B.D.; Roy, A.; Chen, A.L.; Ziadni, M.S.; Keane, R.T.; You, D.S.; Slater, K.; Poupore-King, H.; MacKey, I.; Kao, M.-C.; et al. Comparison of a Single-Session Pain Management Skills Intervention with a Single-Session Health Education Intervention and 8 Sessions of Cognitive Behavioral Therapy in Adults with Chronic Low Back Pain: A Randomized Clinical Trial. JAMA Netw Open 2021, 13401. [Google Scholar] [CrossRef]
- Devasahayam, A.J.; Siang Lim, C.K.; Goh, M.R.; Lim You, J.P.; Pua, P.Y. Delivering a Back School Programme with a Cognitive Behavioural Modification: A Randomised Pilot Trial on Patients with Chronic Non-Specific Low Back Pain and Functional Disability. Proc Singap. Healthc. 2014, 23, 218–225. [Google Scholar] [CrossRef]
- Donzelli, S.; Di Domenica, F.; Cova, A.M.; Galletti, R.; Giunta, N. Two Different Techniques in the Rehabilitation Treatment of Low Back Pain: A Randomized Controlled Trial. Eur. Medicophys. 2006, 42, 205–210. [Google Scholar]
- Dufour, N.; Thamsborg, G.; Oefeldt, A.; Lundsgaard, C.; Stender, S. Treatment of Chronic Low Back Pain: A Randomized, Clinical Trial Comparing Group-Based Multidisciplinary Biopsychosocial Rehabilitation and Intensive Individual Therapist-Assisted Back Muscle Strengthening Exercises. Spine 2010, 35, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Durmus, D.; Unal, M.; Kuru, O. How Effective Is a Modified Exercise Program on Its Own or with Back School in Chronic Low Back Pain? A Randomized-Controlled Clinical Trial. J. Back Musculoskelet Rehabil. 2014, 27, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Frost, H.; Klaber Moffett, J.A.; Moser, J.S.; Fairbank, J.C. Randomised Controlled Trial for Evaluation of Fitness Programme for Patients with Chronic Low Back Pain. BMJ 1995, 310, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.N.; Costa, L.D.C.M.; Hancock, M.J.; De Souza, F.S.; de Oliveira Gomes, G.V.F.; De Almeida, M.O.; Costa, L.O.P. McKenzie Method of Mechanical Diagnosis and Therapy Was Slightly More Effective than Placebo for Pain, but Not for Disability, in Patients with Chronic Non-Specific Low Back Pain: A Randomised Placebo Controlled Trial with Short and Longer Term Follow-u. Br. J. Sports Med. 2018, 52, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Gardner, T.; Refshauge, K.; McAuley, J.; Hubscher, M.; Goodall, S.; Smith, L. Combined Education and Patient-Led Goal Setting Intervention Reduced Chronic Low Back Pain Disability and Intensity at 12 Months: A Randomised Controlled Trial. Br. J. Sports Med. 2019, 53, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, E.; Wileman, V.; Galea Holmes, M.; McCracken, L.M.; Norton, S.; Moss-Morris, R.; Noonan, S.; Barcellona, M.; Critchley, D. Physical Therapy Informed by Acceptance and Commitment Therapy (PACT) Versus Usual Care Physical Therapy for Adults With Chronic Low Back Pain: A Randomized Controlled Trial. J. Pain 2020, 21, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Goldby, L.J.; Moore, A.P.; Doust, J.; Trew, M.E. A Randomized Controlled Trial Investigating the Efficiency of Musculoskeletal Physiotherapy on Chronic Low Back Disorder. Spine Phila Pa 1976 2006, 31, 1083–1093. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.M.; Maher, C.G.; Lam, P.; Ferreira, M.; Latimer, J. Tai Chi Exercise for Treatment of Pain and Disability in People with Persistent Low Back Pain: A Randomized Controlled Trial. Arthritis Care Res 2011, 63, 1576–1583. [Google Scholar] [CrossRef] [PubMed]
- Haufe S; Wiechmann K; Stein L; Kuck M; Smith A; Meineke S; Zirkelbach Y; Rodriguez Duarte S; Drupp M; Tegtbur U Low-Dose, Non-Supervised, Health Insurance Initiated Exercise for the Treatment and Prevention of Chronic Low Back Pain in Employees. Results from a Randomized Controlled Trial. PLoS ONE 2017 Jun126e0178585 2017.
- Highland, K.B.; Schoomaker, A.; Rojas, W.; Suen, J.; Ahmed, A.; Zhang, Z.; Carlin, S.F.; Calilung, C.E.; Kent, M.; McDonough, C.; et al. Benefits of the Restorative Exercise and Strength Training for Operational Resilience and Excellence Yoga Program for Chronic Low Back Pain in Service Members: A Pilot Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Jaromi, M.; Kukla, A.; Szilagyi, B.; Simon-Ugron, A.; Bobaly, V.K.; Makai, A.; Linek, P.; Acs, P.; Leidecker, E. Back School Programme for Nurses Has Reduced Low Back Pain Levels: A Randomised Controlled Trial. J. Clin. Nurs. 2018, 27, e895–e902. [Google Scholar] [CrossRef]
- Jaromi, M.; Nemeth, A.; Kranicz, J.; Laczko, T.; Betlehem, J. Treatment and Ergonomics Training of Work-Related Lower Back Pain and Body Posture Problems for Nurses. J. Clin. Nurs. 2012, 21, 1776–1784. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.K.; Leboeuf-Yde, C.; Wedderkopp, N.; Sorensen, J.S.; Manniche, C. Rest versus Exercise as Treatment for Patients with Low Back Pain and Modic Changes. A Randomized Controlled Clinical Trial. BMC Med. 2012, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Jousset, N.; Fanello, S.; Bontoux, L.; Dubus, V.; Billabert, C.; Vielle, B.; Roquelaure, Y.; Penneau-Fontbonne, D.; Richard, I. Effects of Functional Restoration versus 3 Hours per Week Physical Therapy: A Randomized Controlled Study. Spine 2004, 29, 487–493; discussion 494. [Google Scholar] [CrossRef] [PubMed]
- Kääpä, E.H.; Frantsi, K.; Sarna, S.; Malmivaara, A. Multidisciplinary Group Rehabilitation versus Individual Physiotherapy for Chronic Nonspecific Low Back Pain: A Randomized Trial. Spine Phila Pa 1976 2006, 31, 371–376. [Google Scholar] [CrossRef]
- Kader, D.; Radha, S.; Smith, F.; Wardlaw, D.; Scott, N.; Rege, A.; Pope, M. Evaluation of Perifacet Injections and Paraspinal Muscle Rehabilitation in Treatment of Low Back Pain. A Randomised Controlled Trial. Ortop Traumatol Rehabil 2012, 14, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Kankaanpää, M.; Taimela, S.; Airaksinen, O.; Hänninen, O. The Efficacy of Active Rehabilitation in Chronic Low Back Pain. Effect on Pain Intensity, Self-Experienced Disability, and Lumbar Fatigability. Spine Phila Pa 1976 1999, 24, 1034–1042. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Akhter, S.; Soomro, R.R.; Ali, S.S. The Effectiveness of Cognitive Behavioral Therapy (CBT) with General Exercises versus General Exercises Alone in the Management of Chronic Low Back Pain. Pak. J. Pharma Sci. 2014, 27, 1113–1116. [Google Scholar]
- Khodadad, B.; Letafatkar, A.; Hadadnezhad, M.; Shojaedin, S. Comparing the Effectiveness of Cognitive Functional Treatment and Lumbar Stabilization Treatment on Pain and Movement Control in Patients With Low Back Pain. Sports Health 2020, 12, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-S.; An, J.; Kim, J.-O.; Lee, M.-Y.; Lee, B.-H. Effects of Pain Neuroscience Education Combined with Lumbar Stabilization Exercise on Strength and Pain in Patients with Chronic Low Back Pain: Randomized Controlled Trial. J. Med. 2022, 12, 303. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Lee, J.; Oh, S.; Kim, S.; Yoon, B. Effectiveness of Simulated Horseback Riding for Patients With Chronic Low Back Pain: A Randomized Controlled Trial. J. Sport Rehabil. 2020, 29, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Kofotolis, N.; Kellis, E. Effects of Two 4-Week Proprioceptive Neuromuscular Facilitation Programs on Muscle Endurance, Flexibility, and Functional Performance in Women with Chronic Low Back Pain. Phys. Ther. 2006, 86, 1001–1012. [Google Scholar] [CrossRef] [PubMed]
- Koldaş Doğan, S.; Sonel Tur, B.; Kurtaiş, Y.; Atay, M.B. Comparison of Three Different Approaches in the Treatment of Chronic Low Back Pain. Clin. Rheumatol. 2008, 27, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Negi, M.P.S.; Sharma, V.P.; Shukla, R.; Dev, R.; Mishra, U.K. Efficacy of Two Multimodal Treatments on Physical Strength of Occupationally Subgrouped Male with Low Back Pain. J. Back Musculoskelet. Rehabil. 2009, 22, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Sharma, V.P.; Negi, M.P.S. Efficacy of Dynamic Muscular Stabilization Techniques (DMST) over Conventional Techniques in Rehabilitation of Chronic Low Back Pain. J. Strength Cond. Res. 2009, 23, 2651–2659. [Google Scholar] [CrossRef] [PubMed]
- Kuvacic, G.; Fratini, P.; Padulo, J.; Antonio, D.I.; De Giorgio, A. Effectiveness of Yoga and Educational Intervention on Disability, Anxiety, Depression, and Pain in People with CLBP: A Randomized Controlled Trial. Complement Ther. Clin. Pr. 2018, 31, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Linden, M.; Scherbe, S.; Cicholas, B. Randomized Controlled Trial on the Effectiveness of Cognitive Behavior Group Therapy in Chronic Back Pain Patients. J. Back Musculoskelet Rehabil 2014, 27, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Masharawi, Y.; Nadaf, N. The Effect of Non-Weight Bearing Group-Exercising on Females with Non-Specific Chronic Low Back Pain: A Randomized Single Blind Controlled Pilot Study. J. Back Musculoskelet Rehabil 2013, 26, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Mazloum, V.; Sahebozamani, M.; Barati, A.; Nakhaee, N.; Rabiei, P. The Effects of Selective Pilates versus Extension-Based Exercises on Rehabilitation of Low Back Pain. J. Bodyw. Mov. Ther. 2018, 22, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- McCaskey, M.A.; Wirth, B.; Schuster-Amft, C.; de Bruin, E.D. Postural Sensorimotor Training versus Sham Exercise in Physiotherapy of Patients with Chronic Non-Specific Low Back Pain: An Exploratory Randomised Controlled Trial. PLoS ONE 2018, 13, e0193358. [Google Scholar] [CrossRef] [PubMed]
- Michalsen, A.; Jeitler, M.; Kessler, C.S.; Steckhan, N.; Robens, S.; Ostermann, T.; Kandil, F.I.; Stankewitz, J.; Berger, B.; Jung, S.; et al. Yoga, Eurythmy Therapy and Standard Physiotherapy (YES-Trial) for Patients With Chronic Non-Specific Low Back Pain: A Three-Armed Randomized Controlled Trial. J. Pain 2021, 22, 1233–1245. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, G.C.; Costa, L.O.; Galvanin, T.; Cabral, C.M. Efficacy of the Addition of Modified Pilates Exercises to a Minimal Intervention in Patients with Chronic Low Back Pain: A Randomized Controlled Trial. Phys. Ther. 2013, 93, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ambrosini, E.; Rocca, B.; Magni, S.; Brivio, F.; Ferrante, S. A Multidisciplinary Rehabilitation Programme Improves Disability, Kinesiophobia and Walking Ability in Subjects with Chronic Low Back Pain: Results of a Randomised Controlled Pilot Study. Eur. Spine J. 2014, 23, 2105–2113. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ambrosini, E.; Rocca, B.; Cazzaniga, D.; Liquori, V.; Foti, C. Group-Based Task-Oriented Exercises Aimed at Managing Kinesiophobia Improved Disability in Chronic Low Back Pain. Eur. J. Pain. 2016, 20, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ferrante, S.; Rocca, B.; Baiardi, P.; Dal Farra, F.; Foti, C. Effect of a Long-Lasting Multidisciplinary Program on Disability and Fear-Avoidance Behaviors in Patients with Chronic Low Back Pain: Results of a Randomized Controlled Trial. Clin. J. Pain 2013, 29, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Iosa, M.; Paolucci, T.; Fusco, A.; Alcuri, R.; Spadini, E.; Saraceni, V.M.; Paolucci, S. Efficacy of Perceptive Rehabilitation in the Treatment of Chronic Nonspecific Low Back Pain through a New Tool: A Randomized Clinical Study. Clin. Rehabil. 2012, 26, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Paolucci, T.; Alcuri, M.R.; Vulpiani, M.C.; Matano, A.; Bureca, I.; Paolucci, S.; Saraceni, V.M. Quality of Life Improved by Multidisciplinary Back School Program in Patıents with Chronic Non-Specific Low Back Pain: A Single Blind Randomized Controlled Trial. Eur. J. Phys. Rehabil. Med. 2011, 47, 533–541. [Google Scholar] [PubMed]
- Moseley, L. Combined Physiotherapy and Education Is Efficacious for Chronic Low Back Pain. Aust. J. Physiother. 2002, 48, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Nambi, G.; Abdelbasset, W.K.; Alsubaie, S.F.; Saleh, A.K.; Verma, A.; Abdelaziz, M.A.; Alkathiry, A.A. Short-Term Psychological and Hormonal Effects of Virtual Reality Training on Chronic Low Back Pain in Soccer Players. J. Sport Rehabil. 2021, 30, 884–893. [Google Scholar] [CrossRef]
- Narouei, S.; Barati, A.H.; Akuzawa, H.; Talebian, S.; Ghiasi, F.; Akbari, A.; Alizadeh, M.H. Effects of Core Stabilization Exercises on Thickness and Activity of Trunk and Hip Muscles in Subjects with Nonspecific Chronic Low Back Pain. J. Bodyw. Mov. Ther. 2020, 24, 138–146. [Google Scholar] [CrossRef]
- Nassif, H.; Brosset, N.; Guillaume, M.; Delore-Milles, E.; Tafflet, M.; Buchholz, F.; Toussaint, J.-F. Evaluation of a Randomized Controlled Trial in the Management of Chronic Lower Back Pain in a French Automotive Industry: An Observational Study. Arch. Phys. Med. Rehabil. 2011, 92, 1927. [Google Scholar] [CrossRef] [PubMed]
- Natour, J.; Cazotti, Ld. e A.; Ribeiro L.H.; Baptista A.S.; Jones A. Pilates Improves Pain, Function and Quality of Life in Patients with Chronic Low Back Pain: A Randomized Controlled Trial. Clin. Rehabil. 2015, 29, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.K.; Wilson, P.H.; Goyen, J. Operant-Behavioural and Cognitive-Behavioural Treatment for Chronic Low Back Pain. BEHAV RES THER 1991, 29, 225–238. [Google Scholar] [CrossRef] [PubMed]
- O’Keeffe, M.; O’Sullivan, P.; Purtill, H.; Bargary, N.; O’Sullivan, K. Cognitive Functional Therapy Compared with a Group-Based Exercise and Education Intervention for Chronic Low Back Pain: A Multicentre Randomised Controlled Trial (RCT). Br. J. Sports Med. 2020, 54, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Okafor UA; Solanke TA; Akinbo SR; Odebiyi DO Effect of Aerobic Dance on Pain, Functional Disability and Quality of Life on Patients with Chronic Low Back Pain. South Afr. J. Physiother. 201268311-14 2012.
- Patti, A.; Bianco, A.; Paoli, A.; Messina, G.; Montalto, M.A.; Bellafiore, M.; Battaglia, G.; Iovane, A.; Palma, A. Pain Perception and Stabilometric Parameters in People with Chronic Low Back Pain after a Pilates Exercise Program: A Randomized Controlled Trial. Medicine 2016, 95, e2414. [Google Scholar] [CrossRef] [PubMed]
- Paungmali, A.; Joseph, L.H.; Sitilertpisan, P.; Pirunsan, U.; Uthaikhup, S. Lumbopelvic Core Stabilization Exercise and Pain Modulation Among Individuals with Chronic Nonspecific Low Back Pain. Pain Pr. 2017, 17, 1008–1014. [Google Scholar] [CrossRef] [PubMed]
- Petrozzi, M.J.; Leaver, A.; Ferreira, P.H.; Rubinstein, S.M.; Jones, M.K.; Mackey, M.G. Addition of MoodGYM to Physical Treatments for Chronic Low Back Pain: A Randomized Controlled Trial. Chiropr Man Thera 2019, 27, 54. [Google Scholar] [CrossRef] [PubMed]
- Phattharasupharerk, S.; Purepong, N.; Eksakulkla, S.; Siriphorn, A. Effects of Qigong Practice in Office Workers with Chronic Non-Specific Low Back Pain: A Randomized Control Trial. J. Bodyw. Mov. Ther. 2019, 23, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Pires, D.; Cruz, E.B.; Caeiro, C. Aquatic Exercise and Pain Neurophysiology Education versus Aquatic Exercise Alone for Patients with Chronic Low Back Pain: A Randomized Controlled Trial. Clin. Rehabil. 2015, 29, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Polaski, A.M.; Phelps, A.L.; Smith, T.J.; Helm, E.R.; Morone, N.E.; Szucs, K.A.; Kostek, M.C.; Kolber, B.J. Integrated Meditation and Exercise Therapy: A Randomized Controlled Pilot of a Combined Nonpharmacological Intervention Focused on Reducing Disability and Pain in Patients with Chronic Low Back Pain. Pain Med. 2021, 22, 444–458. [Google Scholar] [CrossRef] [PubMed]
- Rabiei, P.; Sheikhi, B.; Letafatkar, A. Comparing Pain Neuroscience Education Followed by Motor Control Exercises With Group-Based Exercises for Chronic Low Back Pain: A Randomized Controlled Trial. Pain Pr. 2021, 21, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Roche-Leboucher, G.; Petit-Lemanac’H, A.; Bontoux, L.; Dubus-Bausiere, V.; Parot-Shinkel, E.; Fanello, S.; Penneau-Fontbonne, D.; Fouquet, N.; Legrand, E.; Roquelaure, Y.; et al. Multidisciplinary Intensive Functional Restoration versus Outpatient Active Physiotherapy in Chronic Low Back Pain: A Randomized Controlled Trial. Spine 2011, 36, 2235–2242. [Google Scholar] [CrossRef] [PubMed]
- Rydeard, R.; Leger, A.; Smith, D. Pilates-Based Therapeutic Exercise: Effect on Subjects with Nonspecific Chronic Low Back Pain and Functional Disability: A Randomized Controlled Trial. J. Orthop Sports Phys. Ther. 2006, 36, 472–484. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.O.B.D.; Castro, J.B.P.; Nunes, R.A.M.; Silva, G.C.P.S.M.D.; Oliveira, J.G.M.; Lima, V.P.; Vale, R.G.S. Effects of Two Training Programs on Health Variables in Adults with Chronic Low Back Pain: A Randomized Clinical Trial. Pain Manag. 2022. [Google Scholar] [CrossRef]
- Saper, R.B.; Lemaster, C.; Delitto, A.; Sherman, K.J.; Herman, P.M.; Sadikova, E.; Stevans, J.; Keosaian, J.E.; Cerrada, C.J.; Femia, A.L.; et al. Yoga, Physical Therapy, or Education for Chronic Low Back Pain: A Randomized Noninferiority Trial. Ann. Intern. Med. 2017, 167, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Saper, R.B.; Sherman, K.J.; Cullum-Dugan, D.; Davis, R.B.; Phillips, R.S.; Culpepper, L. Yoga for Chronic Low Back Pain in a Predominantly Minority Population: A Pilot Randomized Controlled Trial. Altern Ther. Health Med. 2009, 15, 18–27. [Google Scholar] [PubMed]
- Schinhan, M.; Neubauer, B.; Pieber, K.; Gruber, M.; Kainberger, F.; Castellucci, C.; Olischar, B.; Maruna, A.; Windhager, R.; Sabeti-Aschraf, M. Climbing Has a Positive Impact on Low Back Pain: A Prospective Randomized Controlled Trial. Clin. J. Sport Med. 2016, 26, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Shamsi, M.; Sarrafzadeh, J.; Jamshidi, A.; Zarabi, V.; Pourahmadi, M.R. The Effect of Core Stability and General Exercise on Abdominal Muscle Thickness in Non-Specific Chronic Low Back Pain Using Ultrasound Imaging. Physiother Theory Pr. 2016, 32, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, M.; Caulfield, B. A Pilot Study to Investigate the Effect of Lumbar Stabilisation Exercise Training on Functional Ability and Quality of Life in Patients with Chronic Low Back Pain. Int. J. Rehabil. Res. 2004, 27, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Sherman, K.J.; Cherkin, D.C.; Wellman, R.D.; Cook, A.J.; Hawkes, R.J.; Delaney, K.; Deyo, R.A. A Randomized Trial Comparing Yoga, Stretching, and a Self-Care Book for Chronic Low Back Pain. Arch. Intern. Med. 2011, 171, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Tilbrook, H.E.; Cox, H.; Hewitt, C.E.; Kang’ombe, A.R.; Chuang, L.-H.; Jayakody, S.; Aplin, J.D.; Semlyen, A.; Trewhela, A.; Watt, I.; et al. Yoga for Chronic Low Back Pain: A Randomized Trial. Ann. Intern. Med. 2011, 155, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Torstensen, T.A.; Ljunggren, A.E.; Meen, H.D.; Odland, E.; Mowinckel, P.; Geijerstam, S.A. Efficiency and Costs of Medical Exercise Therapy, Conventional Physiotherapy, and Self-Exercise in Patients with Chronic Low Back Pain: A Pragmatic, Randomized, Single-Blinded, Controlled Trial with 1-Year Follow- Up. Spine 1998, 23, 2616–2624. [Google Scholar] [CrossRef] [PubMed]
- Tritilanunt, T.; Wajanavisit, W. The Efficacy of an Aerobic Exercise and Health Education Program for Treatment of Chronic Low Back Pain. J. Med. Assoc. Thai 2001, 84 Suppl 2, S528–533. [Google Scholar]
- Turner, J.A.; Clancy, S.; McQuade, K.J.; Cardenas, D.D. Effectiveness of Behavioral Therapy for Chronic Low Back Pain: A Component Analysis. J CONSULT CLIN PSYCHOL 1990, 58, 573–579. [Google Scholar] [CrossRef]
- Valenza, M.C.; Rodriguez-Torres, J.; Cabrera-Martos, I.; Diaz-Pelegrina, A.; Aguilar-Ferrandiz, M.E.; Castellote-Caballero, Y. Results of a Pilates Exercise Program in Patients with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial. Clin. Rehabil. 2017, 31, 753–760. [Google Scholar] [CrossRef]
- Van Der Roer, N.; Van Tulder, M.; Barendse, J.; Knol, D.; Van Mechelen, W.; De Vet, H. Intensive Group Training Protocol versus Guideline Physiotherapy for Patients with Chronic Low Back Pain: A Randomised Controlled Trial. Eur. Spine J. 2008, 17, 1193–1200. [Google Scholar] [CrossRef]
- van Erp, R.M.A.; Huijnen, I.P.J.; Ambergen, A.W.; Verbunt, J.A.; Smeets, R.J.E.M. Biopsychosocial Primary Care versus Physiotherapy as Usual in Chronic Low Back Pain: Results of a Pilot-Randomised Controlled Trial. Eur. J. Physiother. 2021, 23, 3–10. [Google Scholar] [CrossRef]
- Vibe Fersum, K.; O’Sullivan, P.; Skouen, J.S.; Smith, A.; Kvale, A. Efficacy of Classification-Based Cognitive Functional Therapy in Patients with Non-Specific Chronic Low Back Pain: A Randomized Controlled Trial. Eur. J. Pain 2013, 17, 916–928. [Google Scholar] [CrossRef]
- Vollenbroek-Hutten, M.M.R.; Hermens, H.J.; Wever, D.; Gorter, M.; Rinket, J.; Ijzerman, M.J. Differences in Outcome of a Multidisciplinary Treatment between Subgroups of Chronic Low Back Pain Patients Defined Using Two Multiaxial Assessment Instruments: The Multidimensional Pain Inventory and Lumbar Dynamometry. Clin. Rehabil. 2004, 18, 566–579. [Google Scholar] [CrossRef] [PubMed]
- Walti, P.; Kool, J.; Luomajoki, H. Short-Term Effect on Pain and Function of Neurophysiological Education and Sensorimotor Retraining Compared to Usual Physiotherapy in Patients with Chronic or Recurrent Non-Specific Low Back Pain, a Pilot Randomized Controlled Trial. BMC Musculoskelet Disord 2015, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Waseem, M.; Karimi, H.; Gilani, S.A.; Hassan, D. Treatment of Disability Associated with Chronic Non-Specific Low Back Pain Using Core Stabilization Exercises in Pakistani Population. J. Back Musculoskelet Rehabil. 2019, 32, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Weifen, W.; Muheremu, A.; Chaohui, C.; Md, L.W.; Lei, S. Effectiveness of Tai Chi Practice for Non-Specific Chronic Low Back Pain on Retired Athletes: A Randomized Controlled Study. J. Musculoskelet Pain 2013, 21, 37–45. [Google Scholar] [CrossRef]
- Williams A; Wiggers J; O’Brien KM; Wolfenden L; Yoong SL; Hodder RK; Lee H; Robson EK; McAuley JH; Haskins R; et al. The Effectiveness of a Healthy Lifestyle Intervention, for Chronic Low Back Pain: A Randomised Controlled Trial. Pain 2018 Jun15961137-1146 2018.
- Williams, K.; Abildso, C.; Steinberg, L.; Doyle, E.; Epstein, B.; Smith, D.; Hobbs, G.; Gross, R.; Kelley, G.; Cooper, L. Evaluation of the Effectiveness and Efficacy of Iyengar Yoga Therapy on Chronic Low Back Pain. Spine 2009, 34, 2066–2076. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-Y.; Tsai, Y.-A.; Wu, P.-K.; Ho, S.-Y.; Chou, C.-Y.; Huang, S.-F. Pilates-Based Core Exercise Improves Health-Related Quality of Life in People Living with Chronic Low Back Pain: A Pilot Study. J. Bodyw. Mov. Ther. 2021, 27, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Zadro, J.R.; Shirley, D.; Simic, M.; Mousavi, S.J.; Ceprnja, D.; Maka, K.; Sung, J.; Ferreira, P. Video-Game-Based Exercises for Older People With Chronic Low Back Pain: A Randomized Controlledtable Trial (GAMEBACK). Phys. Ther. 2019, 99, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wan, L.; Wang, X. The Effect of Health Education in Patients with Chronic Low Back Pain. J. Int. Med. Res. 2014, 42, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Liu, S.; Zhang, S.; Yu, Q.; Lo, W.L.A.; Li, T.; Wang, C.H. Does M-Health-Based Exercise (Guidance plus Education) Improve Efficacy in Patients with Chronic Low-Back Pain? A Preliminary Report on the Intervention’s Significance. Trials 2022, 23, 190. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Zhang, Y.; Liu, Y.; Tian, X.; Xiao, T.; Liu, X.; Yeung, A.S.; Liu, J.; Wang, X.; Yang, Q. The Effects of Tai Chi Chuan Versus Core Stability Training on Lower-Limb Neuromuscular Function in Aging Individuals with Non-Specific Chronic Lower Back Pain. Med. Kaunas 2019, 55. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Chu, H. Quantifying Publication Bias in Meta-Analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, L.K.; Pyysalo, L.M.; Kankaanpää, M.J. Prognostic Factors for Pain Chronicity in Low Back Pain: A Systematic Review. PAIN Rep. 2021, 6, e919. [Google Scholar] [CrossRef]
Figure 1.
Network structure of pain & disability outcomes.
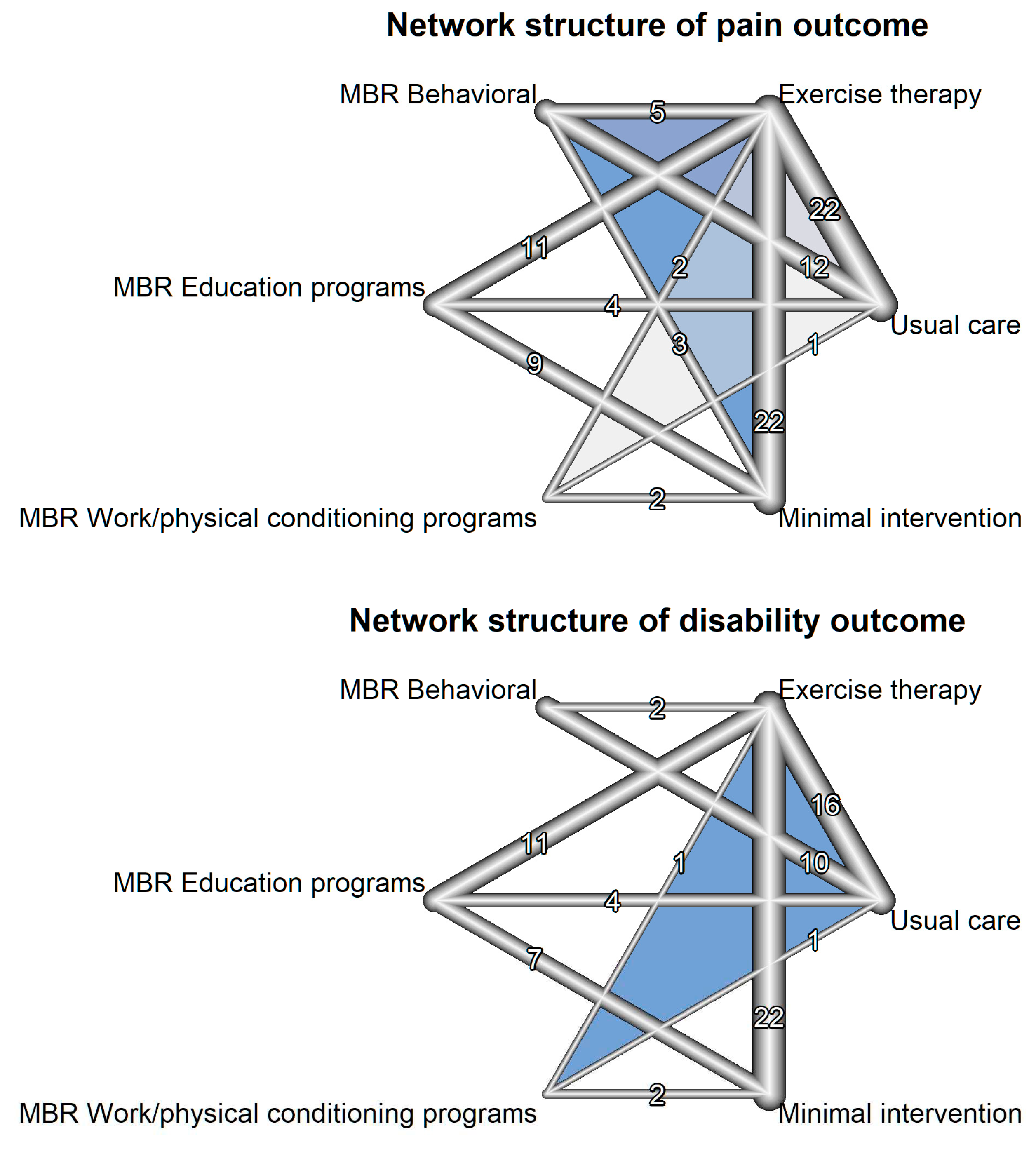
Figure 2.
Summary of risk of bias of included studies.
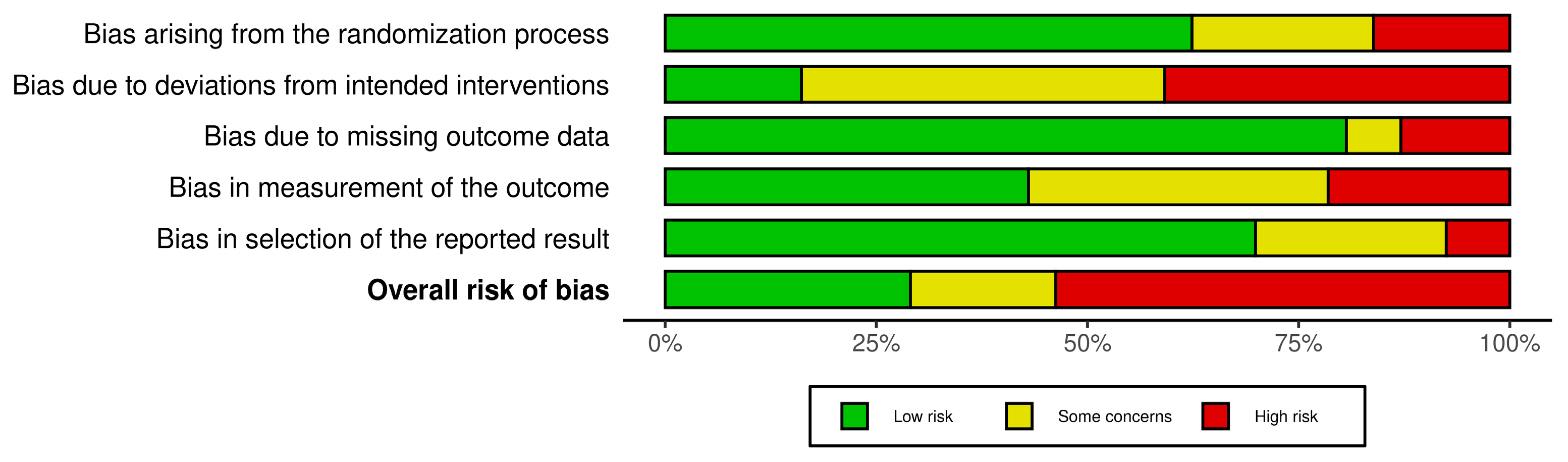
Figure 3.
Exercise therapy and MBR modalities vs minimal intervetion in pain outcomes.
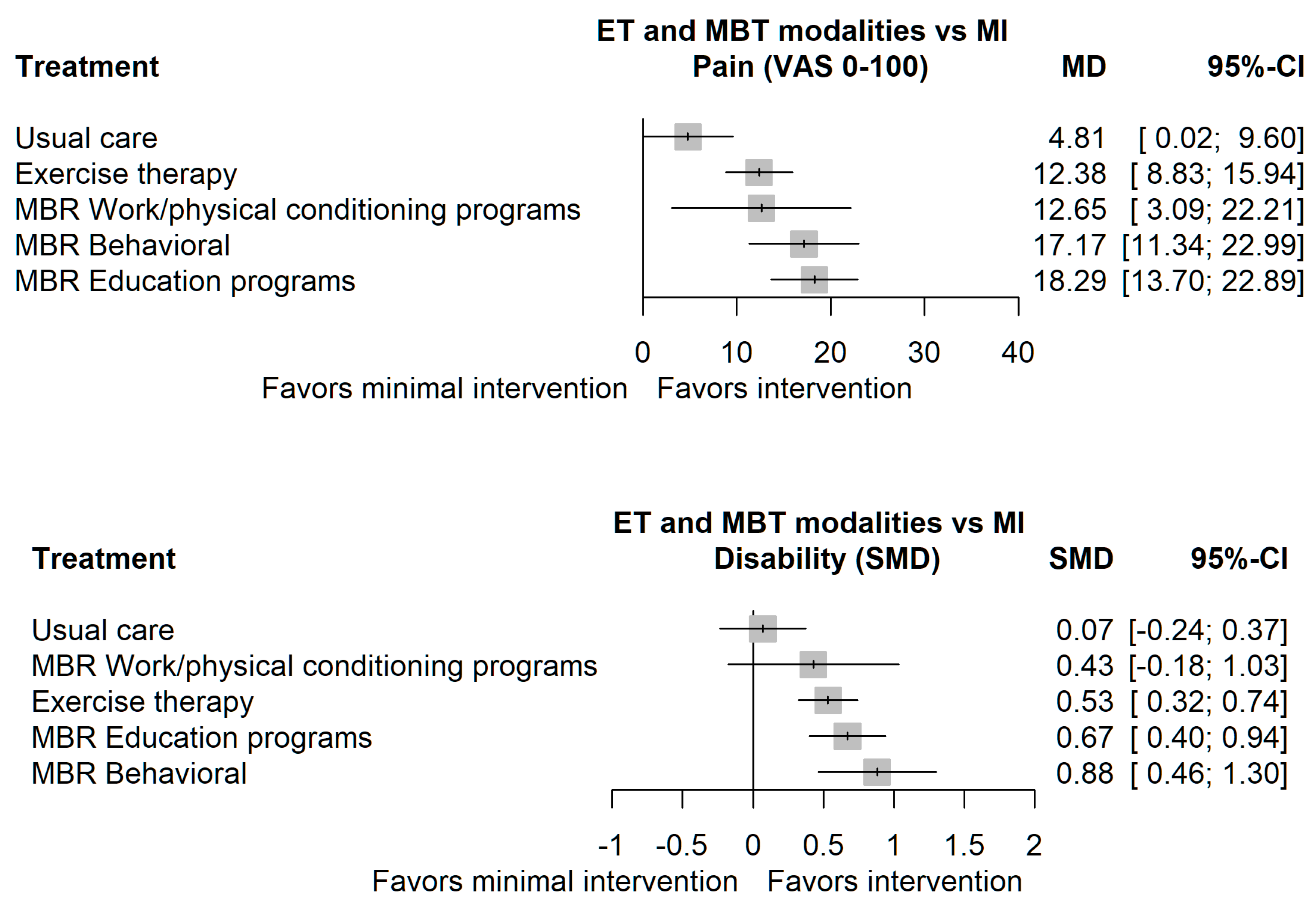

Table 1.
Characteristics of included trials population.
| Population characteristics | Mean (min, max) | # of studies | Sample size |
|---|---|---|---|
| Male [%] | 31.18% | 72 | 6476 |
| Age [years] | 44.61 (21.4 to 73.63) | 88 | 7432 |
| BMI | 25.89 (20.77 to 35) | 61 | 5075 |
| Symptom duration [months] | 53.6 (5.3 to 222) | 40 | 4101 |
| Intervention duration [weeks] | 9.01 (1 to 24) | 84 | 7163 |
| # of hours per week | 2.3 (0.12 to 30) | 80 | 6867 |
Table 2.
League table with direct comparison and NMA estimates of pain outcomes.
| MI | . | 14.56 (10.41; 18.71) |
14.03 (-0.59; 28.65) |
9.96 (-1.68; 21.59) |
14.06 (7.43; 20.68) |
| 4.81 (0.02; 9.60) |
UC | 9.08 (4.90; 13.27) |
0.20 (-17.86; 18.26) |
11.43 (5.59; 17.28) |
11.26 (1.62; 20.90) |
| 12.38 (8.83; 15.94) |
7.57 (3.95; 11.20) |
ET | 1.53 (11.59; 14.64) |
10.27 (1.78; 18.77) |
9.99 (4.17; 15.80) |
| 12.65 (3.09; 22.21) |
7.84 (-1.99; 17.68) |
0.27 (-9.19; 9.73) |
MBR-WR | . | . |
| 17.17 (11.34; 22.99) |
12.36 (7.52; 17.20) |
4.79 (-0.36; 9.93) |
4.52 (-6.02; 15.05) |
MBR-BE | . |
| 18.29 (13.70; 22.89) |
13.49 (8.42; 18.55) |
5.91 (1.67; 10.16) |
5.64 (-4.49; 15.77) |
1.13 (-5.19; 7.44) |
MBR-ED |
Legend: [values: mean difference (95% CI)]; MI = Minimal intervention; UC = Usual care; ET = Exercise therapy; MBR-WR = MBR Work conditioning/hardening; MBR-BE = MBR Behavioral; MBR-ED = MBR Education.
Table 3.
League table with direct comparison and NMA estimates of disability outcomes.
| MI | . | 0.55 (-0.24; 1.35) |
0.66 (0.42; 0.89) |
0.28 (-0.12; 0.68) |
. |
| 0.07 (-0.24; 0.37) |
UC | -0.11 (-1.15; 0.92) |
0.44 (0.17; 0.71) |
0.73 (0.17; 1.30) |
0.81 (0.46; 1.16) |
| 0.43 (-0.18; 1.03) |
0.36 (-0.28; 0.99) |
MBR-WR | -0.05 (-1.10; 0.99) |
. | . |
| 0.53 (0.32; 0.74) |
0.46 (0.23; 0.70) |
0.10 (-0.51; 0.72) |
ET | 0.36 (0.03; 0.69) |
0.37 (-0.36; 1.10) |
| 0.67 (0.40; 0.94) |
0.60 (0.29; 0.91) |
0.24 (-0.40; 0.89) |
0.14 (-0.11; 0.39) |
MBR-ED | . |
| 0.88 (0.46; 1.30) |
0.81 (0.49; 1.13) |
0.45 (-0.24; 1.15) |
0.35 (-0.02; 0.72) |
0.21 (-0.21; 0.64) |
MBR-BE |
Legend: [values: standardized mean difference (95% CI)]; MI = Minimal intervention; UC = Usual care; ET = Exercise therapy; MBR-WR = MBR Work conditioning/hardening; MBR-BE = MBR Behavioral therapy; MBR-ED = MBR Education.
Table 4.
Rankings of P-score scores for pain & disability outcomes.
| Pain outcome | Disability outcome | ||||
|---|---|---|---|---|---|
| Rank | Treatment | P-score | P-score | Treatment | Rank |
| 1 | MBR-ED | 0.899 | 0.940 | MBR-BE | 1 |
| 2 | MBR-BE | 0.826 | 0.761 | MBR-ED | 2 |
| 3 | MBR-WR | 0.559 | 0.559 | ET | 3 |
| 4 | ET | 0.503 | 0.496 | MBR-WR | 4 |
| 5 | UC | 0.207 | 0.161 | UC | 5 |
| 6 | MI | 0.006 | 0.082 | MI | 6 |
MI = Minimal intervention; UC = Usual care; ET = Exercise therapy; MBR-WR = MBR Work conditioning/hardening; MBR-BE = MBR Behavioral therapy; MBR-ED = MBR Education.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



