
Submitted:
09 June 2025
Posted:
20 June 2025
You are already at the latest version
Abstract
Introduction The rising incidence of hepatocellular carcinoma (HCC) in North America mirrors the growing prevalence of metabolic-associated fatty liver disease (MAFLD). Though MAFLD is now a recognized driver of HCC, its precise influence on tumor biology and patient prognosis remains incompletely understood. This study examines whether MAFLD-associated HCC constitutes a distinct clinical phenotype and explores its prognostic and therapeutic implications. Methods We conducted a retrospective cohort study of 154 adult patients who underwent curative-intent hepatic resection for HCC at a leading U.S. university medical center between January 1, 2011, and December 31, 2020, with follow-up through December 31, 2023. Patients were stratified into MAFLD-positive (n=89) and MAFLD-negative (n=67) groups. Demographic, clinical, and oncologic characteristics were compared. Survival outcomes were assessed using Kaplan-Meier estimates, while multivariate Cox regression was employed to adjust for confounding variables and identify independent prognostic factors. Results Compared to their MAFLD-negative counterparts, MAFLD-positive patients were older (mean age 70.1 vs. 67.4 years, p=0.043), more frequently obese (55% vs. 18%, p<0.001), and less likely to have cirrhosis (27% vs. 64%, p<0.001). They also presented with larger tumors (mean diameter 5.6 cm vs. 3.8 cm, p=0.004), although tumor differentiation and T stage were comparable between groups. Progression-free survival (PFS) was longer among MAFLD-positive patients (median 2.80 vs. 1.21 years, p=0.002), with a hazard ratio of 0.64 (95% CI: 0.42–0.96). Median overall survival (OS) was also numerically higher (4.55 vs. 2.54 years), though the difference did not reach statistical significance (p=0.09). After adjustment for confounders, MAFLD was not independently associated with OS or PFS. In contrast, cirrhosis, serum AFP >100 ng/mL, and advanced tumor stage emerged as independent predictors of poorer outcomes. Conclusions Despite prior suggestions of a unique clinical trajectory for MAFLD-associated HCC, our findings suggest that MAFLD status alone does not independently predict survival following curative-intent resection. Once key oncologic factors are accounted for, outcomes appear similar between MAFLD-positive and MAFLD-negative patients. These results underscore the importance of risk stratification based on established prognostic markers rather than liver disease etiology alone.
Keywords:
hepatocellular carcinoma
; metabolic associated fatty liver disease
; hepatic resection
; survival
Introduction
Emerging evidence suggests that hepatocellular carcinoma (HCC) arising in the context of metabolic-associated fatty liver disease (MAFLD) may exhibit distinct biological behavior compared to HCCs linked to other etiologies. [1] Unlike viral- or alcohol-related HCC, which typically develops in cirrhotic livers, MAFLD-positive HCCs often arise in the absence of cirrhosis, indicating fibrosis-independent pathways to hepatocarcinogenesis. This distinction carries important clinical implications, as patients with MAFLD-positive HCC generally have better-preserved liver function and less portal hypertension, in comparison to patients with other predisposing factors. This difference influences not only treatment options, but also patients’ prognosis, as cirrhosis is associated with a high risk of recurrent disease and complications due to liver decompensation and portal hypertension [2].
Recent studies have identified key differences in tumor microenvironment between the two groups, driven by distinct inflammatory pathways that may influence overall survival (OS) and progression-free survival (PFS) after surgery [3,5]. Molecular investigations have further revealed specific genetic and epigenetic features in MAFLD-positive HCC, including distinct regulatory networks, nucleotide polymorphisms, and the activation of oncogenic pathways such as STAT-1 and STAT- [6,8]. Despite these findings, the clinical significance of these molecular and biological differences on post-resection outcomes remains insufficiently understood [9,12].
Most studies examining survival following hepatic resections for MAFLD-positive HCC versus MAFLD-negative HCC have been conducted in Asian centers, limiting the applicability of their findings to other populations [1]. In a previous meta-analysis of 7,226 patients [1], we found that MAFLD-positive HCC was associated with a more favorable postoperative prognosis compared to MAFLD-negative HCC. However, a key limitation of this analysis was the lack of comprehensive data on critical confounders, particularly the degree of liver dysfunction and the presence of cirrhosis, two major prognostic determinants.
Given the scarcity of research on the outcomes of MAFLD-positive HCC patients undergoing hepatic resections in Western centers, we conducted a retrospective cohort study at a U.S. quaternary academic hospital to compare overall survival (OS) and progression-free survival (PFS) between MAFLD-positive and MAFLD-negative HCC patients. Our analysis adjusted for hepatic dysfunction, cirrhosis, and other established oncologic prognostic factors. Our hypothesis was that previously observed survival advantages among MAFLD-positive patients [1] may be largely attributable to differences in underlying hepatic fibrosis and cirrhosis.
Methods
Study Design
This retrospective cohort study included all consecutive patients who underwent curative hepatic resection for HCC between January 1, 2011, and December 31, 2020, with follow-up extending through December 31, 2023, at a single teaching university hospital in Pennsylvania. Institutional Review Board approval was obtained (PRO 13060220), and the requirement for individual consent was waived due to the retrospective design and use of de-identified data. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki [13] and complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [14].
Inclusion and Exclusion Criteria
Eligible patients were ≥18 years old and had undergone hepatic resection with curative intent for HCC, confirmed by histopathologic evaluation of the final surgical specimen. Patients were excluded if they had prior liver resections, concurrent malignancies, or non-HCC primary liver tumors.
Study Groups
Patients were stratified into two groups based on their clinically identified oncologic risk factors:
- MAFLD-negative HCC
- MAFLD-positive HCC
MAFLD-negative HCC was defined as HCC occurring in patients with underlying liver disease due to viral hepatitis (HBV or HCV), alcohol-related cirrhosis, or other less common etiologies such as primary sclerosing cholangitis, autoimmune hepatitis, hemochromatosis etc. To isolate the impact of MAFLD as the sole predisposing factor in survival analyses, patients with both metabolic conditions and additional risk factors were classified within the MAFLD-negative group to avoid misclassification and ensure analytical clarity.
MAFLD-positive HCC was defined as HCC arising in patients with metabolic conditions in the absence of any other risk factors [15]. Metabolic conditions were defined according to standard criteria [15] and included the following:
- Overweight or obesity, based on World Health Organization (WHO) definitions (adjusted for Asian patients).
- Type 2 diabetes mellitus.
- Metabolic dysregulation.
- Radiologic or histologic evidence of hepatic steatosis or steatohepatitis.
Metabolic dysregulation [16] was defined by the presence of two or more of the following criteria:
- Waist circumference >102 cm (men) or >88 cm (women), adjusted for Asian patients
- Systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg, or current use of antihypertensive medications
- Serum triglycerides ≥150 mg/dL or current use of lipid-lowering medications
- High-density lipoprotein (HDL) cholesterol <40 mg/dL (men) or <50 mg/dL (women)
- Prediabetes, defined as fasting glucose 100–125 mg/dL or HbA1c 5.7–6.4%
- C-reactive protein (CRP) >2 mg/L
Data Collection and Definitions
Data were extracted from electronic medical records using a predefined list of variables. Patients were identified from a prospectively maintained institutional registry that captures demographic and clinical information for all hepatobiliary surgical procedures performed at our center. Collected demographic and clinical variables included age, sex, body mass index (BMI), diabetes status, American Society of Anesthesiologists (ASA) physical status classification [17], and functional status using the Eastern Cooperative Oncology Group (ECOG) scale [18]. Tumor characteristics such as tumor size, number, histologic grade, presence of lymphovascular invasion, presence of cirrhosis were recorded, along with laboratory markers including serum albumin, alpha-fetoprotein (AFP), and Albumin-Bilirubin (ALBI) score to assess liver function [19].
The ALBI score was calculated as (log10 total bilirubin [μmol/L] × 0.66) + (albumin [g/L] × -0.085). Patients were categorized into three ALBI grades based on established cutoffs [20]: ALBI Grade 1 (≤ -2.60), ALBI Grade 2 (-2.60 to -1.39), and ALBI Grade 3 (≥ -1.39). Lower ALBI scores indicated better-preserved liver function, while higher scores reflect worsening hepatic impairment.
The neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count [21], and the platelet-to-lymphocyte ratio (PLR) [22] was calculated by dividing the absolute platelet count by the absolute lymphocyte count [23,24]. Increasing values of NLR and PLR indicated worse outcomes for patients with HCC [24] and both values were analyzed as continuous variables and categorized based on clinical thresholds [24], given their relevance as inflammatory markers.
All surgical pathology slides from hepatic resections were retrospectively reviewed by a single expert liver pathologist (MM) to ensure consistency in grading fibrosis and cirrhosis in the liver parenchyma surrounding HCC. This standardized evaluation minimized interobserver variability and provided uniform classification across all cases. Fibrosis and cirrhosis were assessed using hematoxylin and eosin (H&E) staining, with supplementary Masson's trichrome and reticulin stains employed as needed to better visualize fibrous septa and histologic architectural changes. The degree of fibrosis was staged using the Ishak scoring system [25] and METAVIR fibrosis staging [26]- [28], both of which assess fibrotic progression based on septal thickness, lobular architecture, and the presence of bridging fibrosis. Cirrhosis was defined as Ishak stage 6 or METAVIR F4, characterized by extensive fibrous septa with complete nodular regeneration. In cases where fibrosis severity was borderline between advanced fibrosis and cirrhosis, additional histologic parameters—including perisinusoidal fibrosis, hepatocyte plate thickness, and parenchymal extinction—were used to optimize classification.
Primary and Secondary Outcomes
The primary outcomes were:
- OS defined as the time from hepatic resection to death from any cause
- PFS defined as the time from hepatic resection to first radiographic evidence of HCC recurrence
The secondary outcomes included:
- Morbidity and mortality rates at 90-day and 1-year
Follow up
All patients were followed postoperatively according to established international guidelines, including those from the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD) [29]. Patients underwetn cross-sectional imaging of the abdomen and pelvis—using ultrasound (US), computed tomography (CT), or magnetic resonance imaging (MRI)—as well as chest imaging (chest X-ray or CT) and measurement of serum alpha-fetoprotein (AFP) levels. Surveillance was performed every Patients in this study were evaluated every 3–4 months for the first 3 years and then every 6 months through year five in outpatient hepatobiliary clinics.
Statistical Analysis
Continuous variables were assessed for normality using the Shapiro-Wilk test and visually inspected through histograms and Q-Q plots. Normally distributed variables were reported as means with standard deviations (SD) and compared using Student’s t-tests for two-group comparisons or one-way ANOVA for multiple-group comparisons. Non-normally distributed variables were summarized as medians with interquartile ranges (IQR) and analyzed using the Mann-Whitney U test or the Kruskal-Wallis test when comparing multiple groups. Categorical variables were expressed as frequencies and percentages, with group differences assessed using the chi-square test or Fisher’s exact test for smaller sample sizes. Ordinal categorical variables were evaluated using the Cochran-Armitage test for trend.
Survival analyses were performed using the Kaplan-Meier method to estimate OS and PFS, with differences between MAFLD-positive and MAFLD-negative groups assessed using log-rank tests. PFS was defined as the time from the date of hepatic resection to the first radiographic evidence of disease progression or death from any cause, whichever occurred first. Disease progression was assessed using standardized imaging criteria, including dynamic contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI), in accordance with international guidelines for HCC surveillance [29]. Specifically, we utilized the Liver Imaging Reporting and Data System (LI-RADS), developed by the American College of Radiology, which provides a comprehensive framework for HCC diagnosis in at-risk populations [30]. LI-RADS standardizes the interpretation and reporting of liver imaging findings, enhancing diagnostic accuracy and consistency. Patients who remained alive and free of disease progression at the last follow-up were censored at the date of their most recent imaging assessment. To determine the independent impact of MAFLD on OS and PFS, Cox proportional hazards regression models were constructed, adjusting for relevant demographic, clinical, and oncologic variables, including age, sex, body mass index (BMI), ASA classification, ECOG performance status, cirrhosis, AFP level, tumor size, tumor differentiation, microvascular invasion, and T stage. The proportional hazards assumption was evaluated using Schoenfeld residuals tests and log-minus-log survival plots. If the assumption was violated, stratified Cox models were applied. Results were reported as hazard ratios (HR) with 95% confidence intervals (CI).
Missing data were assessed for patterns and addressed using multiple imputation by chained equations (MICE), with primary analyses repeated using complete case analysis for sensitivity testing. Pre-specified subgroup analyses were performed by stratifying patients based on cirrhosis status, AFP level (<100 ng/mL vs. ≥100 ng/mL), and tumor stage (T1-T2 vs. T3-T4). Interaction terms were tested using likelihood ratio tests, and subgroup-specific hazard ratios were visualized using forest plots. All statistical analyses were conducted using R software (R Foundation for Statistical Computing, Vienna, Austria), with a two-tailed p-value <0.05 considered statistically significant.
Results
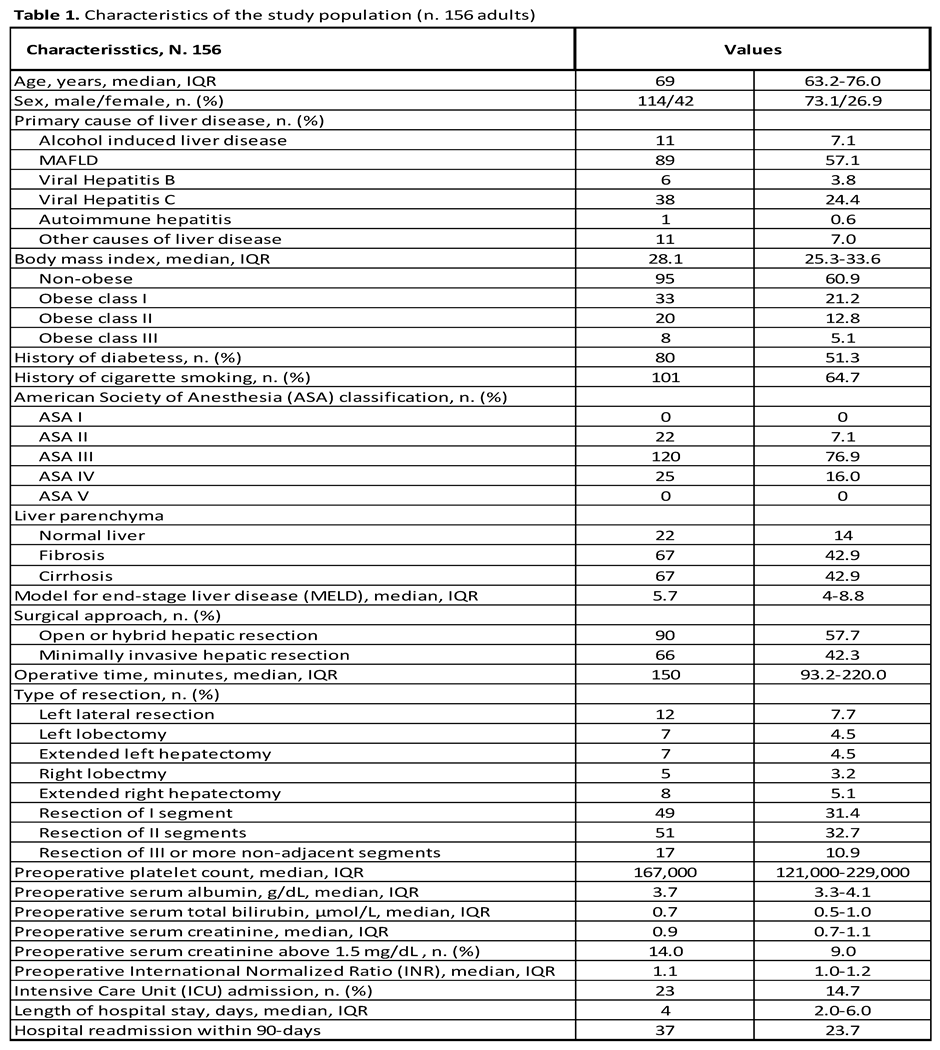
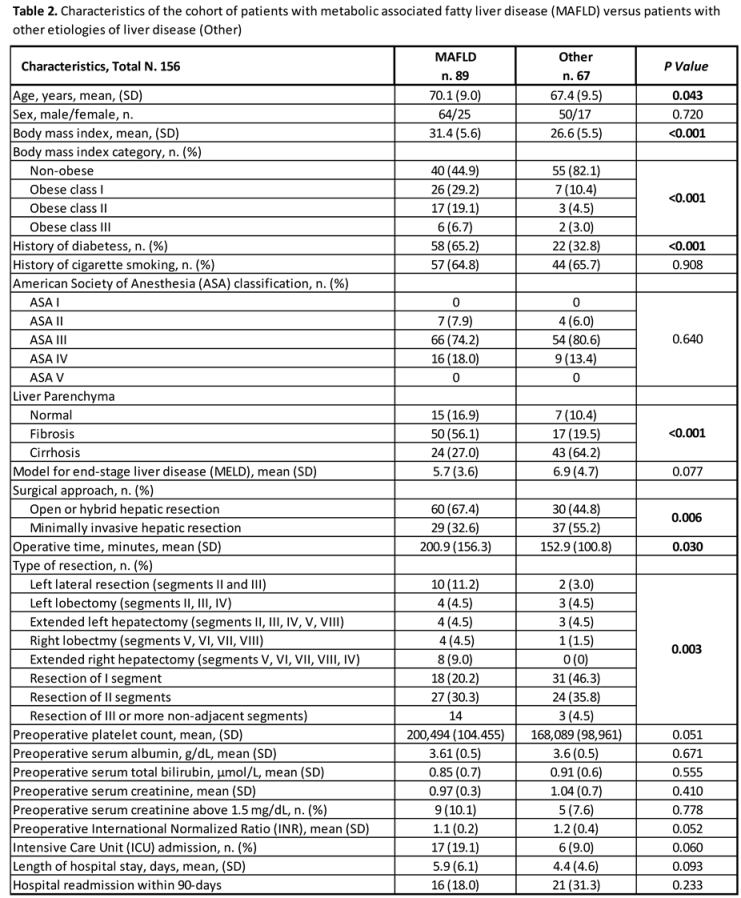
A total of 156 adult patients who underwent hepatic resection for HCC met the inclusion criteria for analysis. Of these, 89 (57.0%) patients were classified as MAFLD-positive, and 67 patients (42.9%) as MAFLD-negative. Baseline demographic and clinical characteristics of the study population are summarized in Table 1 with the key difference between the two groups highlighted in Table 2. MAFLD-positive patients were significantly older, with a mean age of 70.1 years (SD = 9.0) compared to 67.4 years (SD= 9.5) in the MAFLD-negative group (P= 0.043). The MAFLD-positive group also had a higher BMI, with a mean of 31.4 (SD= 5.6) versus 26.6 (SD= 5.5) in the MAFLD-negative group (P< 0.001). Obesity was more prevalent among MAFLD-positive patients, with 29.2% classified as Obese Class I, 19.1% as Obese Class II, and 6.7% as Obese Class III, compared to 10.4%, 4.5%, and 3.0%, respectively, in the MAFLD-negative group (P< 0.001 for each obesity class). Additionally, the prevalence of diabetes was significantly higher in MAFLD-positive patients (65.2% vs. 32.8%, P< 0.001). In contrast, MAFLD-positive patients had a significantly lower prevalence of cirrhosis (27.0% vs. 64.2%, P< 0.001). The surgical approach also differed between groups, with 67.4% of MAFLD-positive patients undergoing open or hybrid hepatic resection, compared to 44.8% in the MAFLD-negative group (P= 0.006). Moreover, the median operative time was significantly longer for MAFLD-positive patients (200.9 minutes, SD = 156.3) compared to MAFLD-negative patients (152.9 minutes, SD= 100.8, P= 0.030). The proportions of missing data for the study cohort are outlined in Supplementary Table S1.
Oncological Characteristics
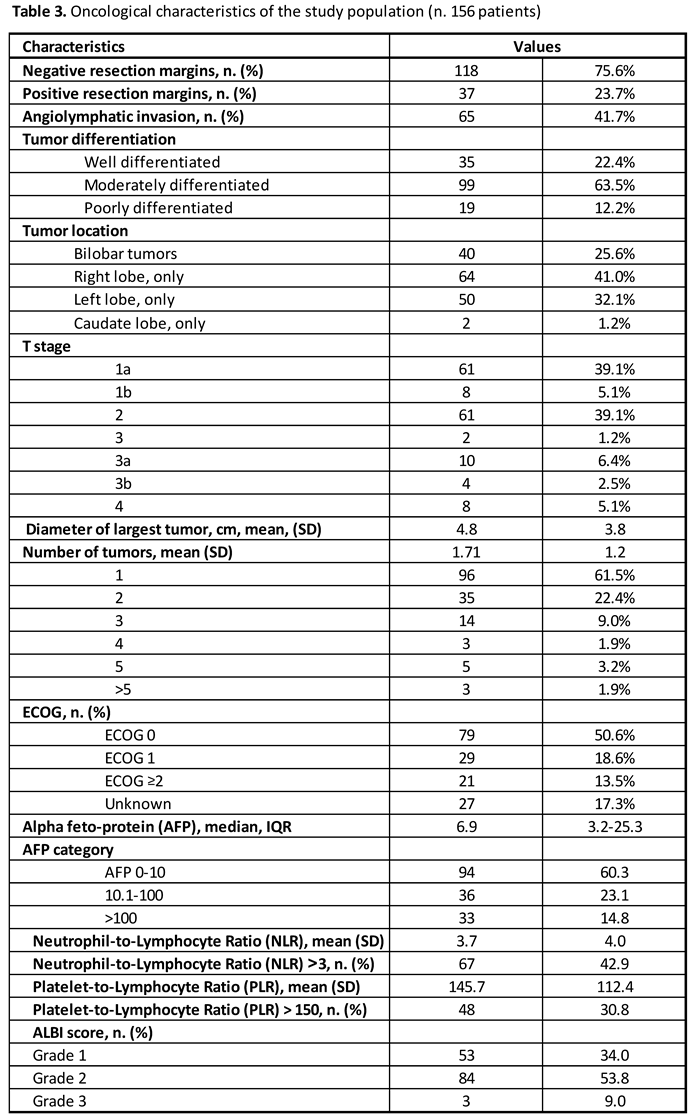
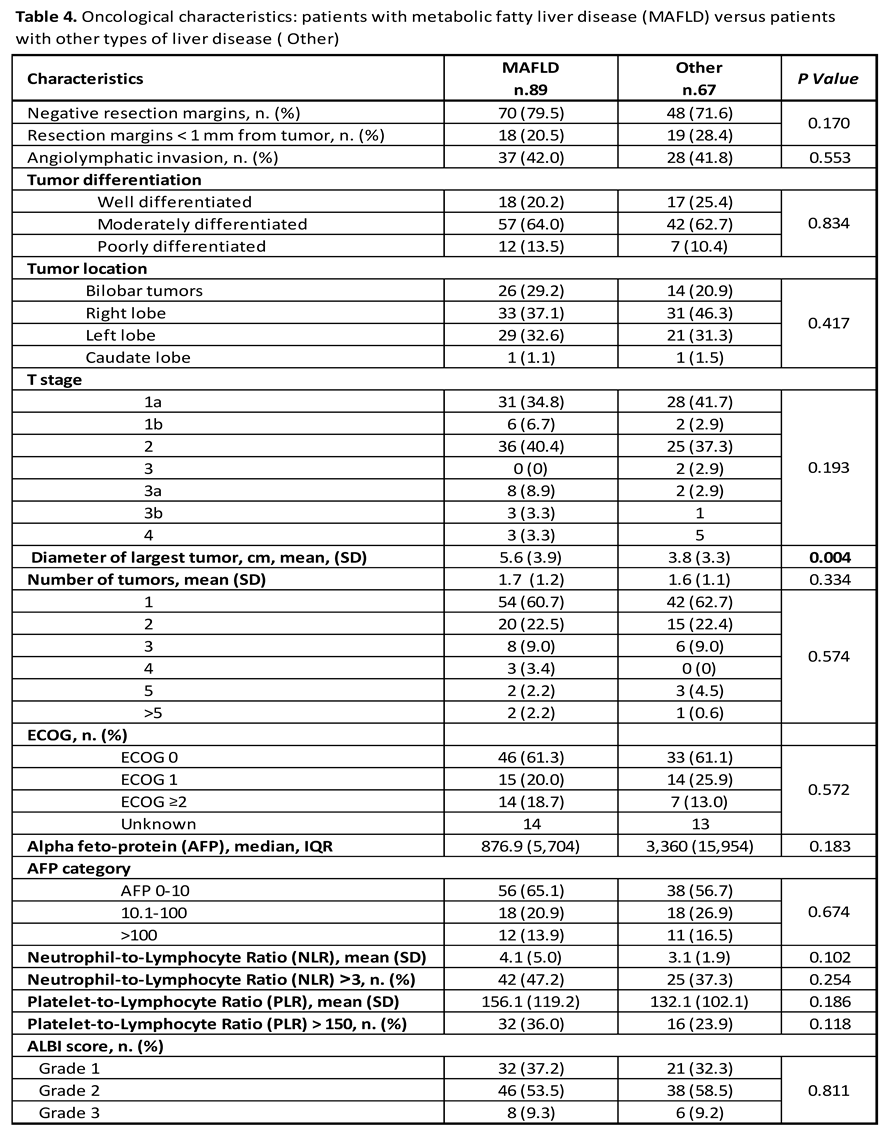
Oncologic characteristics of the study population are presented in Table 3, and key differences between MAFLD-positive and MAFLD-negative groups are summarized in Table 4. MAFLD-positive patients demonstrated a higher frequency of bilobar tumors compared to MAFLD-negative patients (29.2% vs. 20.9%, P = 0.321), although this difference was not statistically significant. Tumor size, on the other hand, differed significantly between groups, with MAFLD-positive patients exhibiting larger tumors (mean diameter 5.6 cm vs. 3.8 cm, P = 0.004). Tumor differentiation was similar across groups, with no statistically significant differences in the proportion of well-differentiated (20.2% vs. 25.4%, P = 0.569), moderately differentiated (64.0% vs. 62.7%, P = 0.995), or poorly differentiated tumors (13.5% vs. 10.4%, P = 0.774). Likewise, the prevalence of angiolymphatic invasion did not differ between groups (42.0% vs. 41.8%, P = 0.553). Although not statistically significant, there was a trend toward more advanced T-stage (T3 or higher) in the MAFLD-positive group (15.5% vs. 10.5%, P = 0.193). ECOG performance status was comparable between the groups, with a non-significant trend toward better functional status in the MAFLD-positive cohort (P = 0.572). Median alpha-fetoprotein (AFP) levels were higher in MAFLD-positive patients (876.9 ng/mL, IQR 5,704) compared to those in the MAFLD-negative group (3,360 ng/mL, IQR 15,954), though the difference was not statistically significant (P = 0.183). The extent of missing oncologic data for the study cohort is detailed in Supplementary Table S2.
Unadjusted Survival Analysis
The median follow up duration for the study cohort was 44.0 months (95%CI 29.8-58.1). Mortality at 90 days occurred in 11 patients (7.1%), and one-year mortality was observed in 25 patients (16.0%). Kaplan-Meier curves illustrating OS and PFS for the entire cohort are shown in Figure 1A and Figure 1B, respectively. Among MAFLD-positive patients, the 90-day mortality rate was 7.9%, compared to 6.0% in the MAFLD-negative group (P = 0.759). One-year mortality was 13.5% in the MAFLD-positive group versus 19.4% in the MAFLD-negative group (P = 0.380). Kaplan-Meier analysis of 5-year OS showed a trend toward improved survival in MAFLD-positive patients, although the difference did not reach statistical significance (P = 0.09; Figure 2). In contrast, PFS was significantly longer in the MAFLD-positive group compared to the MAFLD-negative group (P = 0.002; Figure 3).
Multivariate Survival Analysis
In multivariate analysis, MAFLD-positive status was not an independent predictor of OS (adjusted hazard ratio [HR] = 0.91; 95% CI: 0.45–1.84; P = 0.785) or PFS (adjusted HR = 0.58; 95% CI: 0.28–1.19; P = 0.139). For OS, independent predictors of worse outcomes included the presence of cirrhosis (adjusted HR = 2.32; 95% CI: 1.16–4.64; P = 0.018), poor performance status (ECOG ≥2; adjusted HR = 2.67; 95% CI: 1.29–5.50; P = 0.008), and elevated serum AFP levels (>100 ng/mL; adjusted HR = 2.89; 95% CI: 1.45–5.76; P = 0.003) (Table 5).
For PFS, tumor burden and AFP levels emerged as the only independent prognostic factors. Patients with two tumors had a significantly increased risk of disease progression (adjusted HR = 2.34; 95% CI: 1.12–4.93; P = 0.024), and those with three or more tumors had an even higher risk (adjusted HR = 3.10; 95% CI: 1.27–7.60; P = 0.013). High AFP levels (>100 ng/mL) also remained a strong predictor of worse PFS (adjusted HR = 3.12; 95% CI: 1.59–6.09; P < 0.001) (Table 6).
Discussion
Several important findings emerged from this study, which represents one of the few available analyses of outcomes in a consecutive cohort of patients treated at a high-volume Western medical center. Despite being older, more frequently obese, diabetic, and having larger tumors, patients with MAFLD-positive HCC demonstrated superior OS and PFS compared to those with MAFLD-negative HCC after undergoing hepatic resections with curative intent. The median OS in MAFLD-positive patients was 4.5 years (95% CI: 3.3–5.7) versus 2.5 years (95% CI: 1.7–3.3) in MAFLD-negative patients (P = 0.098). Similarly, the median PFS was significantly longer in MAFLD-positive patients (2.80 years, 95% CI: 1.4–4.1) compared to MAFLD-negative patients (1.2 years, 95% CI: 0.7–1.7, P = 0.002).
These findings align with prior research, including a recent meta-analysis of over 7,000 patients undergoing hepatic resection for HCC, which reported superior OS and PFS in MAFLD-positive groups compared to MAFLD-negative HCC [1]. However, a key limitation of existing evidence is the lack of studies assessing whether these survival differences stem from intrinsic oncologic factors or disparities in liver function and cirrhosis severity—two well-established prognostic determinants that are more prevalent in MAFLD-negative patients [31].
Given that cirrhosis and hepatic dysfunction are associated with higher perioperative morbidity, mortality, and risk of tumor recurrence, our primary aim was to evaluate post-resection outcomes while accounting for these key confounders [32]. By utilizing granular data on baseline performance status, liver function, and degree of fibrosis-cirrhosis, this study provides a more accurate assessment of postoperative outcomes in patients with MAFLD-positive versus MAFLD-negative HCC.
The most notable finding of the current study is that, after adjusting for differences in hepatic function and degree of liver fibrosis-cirrhosis, MAFLD status was not an independent predictor of OS or PFS. Instead, postoperative outcomes were primarily determined by ECOG performance status, serum AFP levels, and tumor burden, confirming the dominant role of systemic health and tumor characteristics in determining survival following hepatic resection, as previously reported by other groups [33]- [35].
An ECOG performance status of ≥2 was independently associated with a 2.4-fold increased risk of mortality (adjusted HR = 2.40, 95% CI: 1.20–4.78, p = 0.013), underscoring the impact of baseline functional status on surgical outcomes. Similarly, elevated serum AFP levels (>100 ng/mL) emerged as a strong prognostic biomarker, significantly predicting both OS (adjusted HR = 3.12, 95% CI: 1.59–6.09, P<0.001) and PFS (adjusted HR= 2.71, 95% CI: 1.49–4.92, P= 0.001). Tumor burden was also a critical determinant of survival, with patients presenting with two lesions experiencing a significantly higher risk of disease progression (adjusted HR= 2.17, 95% CI: 1.21–3.89, P= 0.010). The risk nearly doubled in those with three or more lesions (adjusted HR= 1.99, 95% CI: 0.99–4.01, P= 0.054), highlighting the prognostic weight of intrahepatic tumor burden regardless of underlying liver disease.
Patients with MAFLD-positive HCC exhibited different fibrosis-cirrhosis characteristics compared to MAFLD-negative patients [31]. Our findings confirmed that most MAFLD-positive HCC cases arose in non-cirrhotic livers, suggesting a fibrosis-independent pathway of tumorigenesis [2]. This contrasts with viral- and alcohol-related HCC, where chronic liver injury typically progresses to cirrhosis before malignant transformation [36]. This distinction has important clinical implications, particularly for HCC screening and surveillance, as current guidelines primarily target cirrhotic patients and may overlook high-risk individuals with MAFLD [29]. In our cohort, only 27.0% of MAFLD-positive patients had cirrhosis, significantly lower than 64.2% observed in the MAFLD-negative group (P < 0.001). These findings align with Pais et al. [37], who reported cirrhosis in 30.5% of MAFLD-positive cases compared to 68.3% in MAFLD-negative HCC. In contrast, HCC in patients with hepatitis B or C patients is associated with cirrhosis in 85–90% of cases [37].
Beyond differences in cirrhosis prevalence and hepatic function, our findings indicate that MAFLD-positive patients presented with significantly larger tumors than MAFLD-negative patients (mean 5.6 cm vs. 3.8 cm, P = 0.004), a trend consistently reported in previous studies by Pais et al. [37], Wakai et al. [38], Nishio et al. [39], and Wong et al. [40]. The underlying reasons for this disparity in tumor size remain unclear but may be attributed to differences in HCC surveillance adherence, delayed tumor detection due to body habitus or unique tumor growth kinetics in the setting of metabolic dysfunction. Given the growing global burden of MAFLD, there is an urgent need to refine risk stratification models by incorporating metabolic, inflammatory, and genetic markers beyond fibrosis alone. Developing non-invasive biomarkers and personalized screening strategies for high-risk MAFLD patients could enable earlier detection, timely treatment, and ultimately improved outcomes.
The pathogenesis of MAFLD-related HCC is increasingly recognized as multifactorial, involving a complex interplay of chronic metabolic inflammation, insulin resistance, oxidative stress, and lipotoxicity [41]. These metabolic disturbances induce the release of pro-inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), which contribute to hepatocyte injury, genomic instability, and malignant transformation [42]. Unlike viral- or alcohol-related HCC, which typically arises in cirrhotic livers, MAFLD-positive HCC can develop independently of advanced fibrosis, suggesting the presence of fibrosis-independent carcinogenic pathways. Emerging evidence indicates that epigenetic modifications, including DNA methylation, histone modifications, and non-coding RNA alterations, may play a critical role in promoting tumor progression in MAFLD-associated HCC, further distinguishing it from other etiologies [43]. These molecular alterations influence gene expression, metabolic dysregulation, and oncogenic pathway activation, which may contribute to tumor development even in non-cirrhotic livers [43].
Despite the differences in tumor size, key oncologic characteristics did not significantly differ between MAFLD-positive and MAFLD-negative patients. The rates of angiolymphatic invasion, tumor differentiation grade, and multifocality were comparable between groups, suggesting that MAFLD does not inherently drive a more aggressive HCC phenotype. Moreover, the achievement of negative resection margins at similar rates across both cohorts indicates that larger tumor size in MAFLD-associated HCC did not compromise the oncologic integrity of surgical resections.
This study is among the few conducted in Western medical centers, offering insights into MAFLD-associated HCC in non-Asian populations, where genetic backgrounds, dietary habits, and environmental exposures differ from those in Asian cohorts. In our cohort of 156 patients, only five (3.2%) were of Asian descent, underscoring geographic and demographic distinctiveness of this study population compared to prior Asian-centered studies.
A major strength of this study lies in its detailed assessment of hepatic function and fibrosis staging. Unlike earlier studies that relied on surrogate fibrosis markers, we employed standardized histopathologic evaluation, with all specimens reviewed by a single experienced liver pathologist—minimizing interobserver variability and ensuring consistent classification. The minimal proportion of missing data further enhances the validity of our results.
Despite these strengths, several limitations must be acknowledged. As a retrospective cohort study, selection bias is inherent, and reliance on electronic medical records limited our ability to fully capture the nuanced clinical reasoning behind treatment decisions. Specifically, we were unable to comprehensively assess the factors influencing the selection of hepatic resection versus liver transplantation in patients with cirrhosis or advanced liver dysfunction. Decisions regarding surgical candidacy often involve a complex interplay of tumor biology, liver reserve, comorbidities, and institutional treatment algorithms, which could not be fully accounted for in our analysis. The single-center design further constrains the generalizability of our findings to broader populations with varying clinical, demographic, and practice patterns. Given that Western centers report lower HCC incidence than Asian institutions, our study cohort was relatively small, particularly in comparison to large-scale datasets from Asia, where MAFLD-related HCC is increasingly recognized. Other factors also contribute to this limited sample size. At our center, patients with moderate to severe liver dysfunction or portal hypertension are preferentially referred for liver transplantation rather than resection, given the superior long-term survival associated with transplantation in selected candidates [44]. Therefore, these institutional factors must be considered when interpreting the applicability of our findings to different healthcare settings. Another limitation is the lack of granular data on preoperative locoregional or systemic therapy. Given that hepatic resection is the preferred first-line treatment for resectable HCC, the proportion of patients who received preoperative therapy was negligible. More importantly, our study did not incorporate molecular profiling, which is increasingly recognized as a critical component of HCC characterization.
Future research should consider integrating radiomics with multi-omics approaches (genomics, proteomics, and metabolomics) to improve risk stratification and refine surveillance strategies in MAFLD-associated HCC. Unlike cirrhosis-driven HCC, MAFLD lacks universal screening guidelines. This gap in surveillance, combined with the higher prevalence of obesity and metabolic dysfunction in MAFLD patients, contributes to delayed diagnosis, as larger body habitus can reduce the sensitivity of ultrasound—the primary imaging modality used for HCC screening. Consequently, tumors in MAFLD-associated HCC tend to be larger at diagnosis, making early detection more challenging. By extracting and analyzing quantitative imaging features from CT, MRI, or PET scans, radiomics may help identify tumor phenotypes and vascular patterns associated with biological aggressiveness and complement molecular profiling for more precise risk stratification. Integrating radiomics with multi-omics data has the potential to improve early detection, guide post-resection surveillance, and ultimately enhance long-term outcomes, laying the foundation for precision oncology in MAFLD-associated HCC.
In conclusion, this study suggests that the survival advantage observed in MAFLD-associated HCC after hepatic resection is primarily driven by better liver function and a lower prevalence of cirrhosis rather than intrinsic tumor differences. The larger tumor size in MAFLD patients underscores the need to optimize surveillance strategies, enabling earlier detection and improved outcomes, particularly as the global burden of MAFLD continues to rise.
Financial Support
This study was supported by an internal grant from the University of Pittsburgh in the amount of $50,000. The funding body had no role in the study design, data collection, analysis, interpretation, or manuscript preparation.
Contributions
Michele Molinari: conceptualization, developed the study design and analytical approach, data collection, data curation, statistical analysis, writing and editing of the manuscript. Christof Kaltenmeier: conceptualization, data collection, data curation, statistical analysis, editing of the manuscript.Abiha Abdullah: writing of the manuscript, editing of the manuscript. Dooman Arefan: conceptualization, data curation, statistical and computational analysis, editing of the manuscript. Shandong Wu: data curation, statistical and computation analysis, editing of the manuscript. Christopher Buros: editing of the manuscript and data curation. Vrishketan Sethi: editing of the manuscript and data curation. Hao Liu: editing of the manuscript and data curation. Charbel Elias: editing of the manuscript and data curation. Berkay Demirors: editing of the manuscript and data curation. Jason Mial-Anthony: data collection, editing of the manuscript. Alessandro Furlan: writing of the manuscript, data curation, statistical and computational analysis. Marta Minervini: review of all the histologic samples, data curation, writing of the initial version of the manuscript, critical revision. Samer Tohme: data curation, writing of the initial version of the manuscript, critical revision.David Geller: data curation, writing of the initial version of the manuscript, critical revision. Xingyu Zhang: conducted
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Conflict of interest
The authors declare that they have no conflicts of interest related to this work.
References
- Molinari, M.; Kaltenmeier, C.; Samra, P.B.; et al. Hepatic Resection for Hepatocellular Carcinoma in Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis of 7226 Patients. Ann Surg Open. 2021, 2, e065. [Google Scholar] [CrossRef] [PubMed]
- Beudeker, B.J.B.; Guha, R.; Stoyanova, K.; JNMIJ; de Man, R.A.; Sprengers, D.; Boonstra, A. Cryptogenic non-cirrhotic HCC: Clinical, prognostic and immunologic aspects of an emerging HCC etiology. Sci Rep. 2024, 14, 4302. [Google Scholar] [CrossRef] [PubMed]
- Pocha, C.; Xie, C. Hepatocellular carcinoma in alcoholic and non-alcoholic fatty liver disease—one of a kind or two different enemies? Translational Gastroenterology and Hepatology 2019, 4. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.H.; Yu, M.C.; Chan, K.M.; et al. Prognostic effect of steatosis on hepatocellular carcinoma patients after liver resection. Eur J Surg Oncol. 2011, 37, 618–22. [Google Scholar] [CrossRef]
- Ertle, J.; Dechêne, A.; Sowa, J.-P.; et al. Non-alcoholic fatty liver disease progresses to hepatocellular carcinoma in the absence of apparent cirrhosis. International Journal of Cancer. 2011, 128, 2436–2443. [Google Scholar] [CrossRef]
- Grohmann, M.; Wiede, F.; Dodd, G.T.; et al. Obesity drives STAT-1-dependent NASH and STAT-3-dependent HCC. Cell. 2018, 175, 1289–1306. [Google Scholar] [CrossRef]
- Laurent-Puig, P.; Zucman-Rossi, J. Genetics of hepatocellular tumors. Oncogene. 2006/06/01 2006, 25, 3778–3786. [Google Scholar] [CrossRef]
- Song, T.-J.; Fong, Y.; Cho, S.-J.; et al. Comparison of hepatocellular carcinoma in American and Asian patients by tissue array analysis. Journal of Surgical Oncology. 2012, 106, 84–88. [Google Scholar] [CrossRef]
- Su, C.-W.; Chau, G.-Y.; Hung, H.-H.; et al. Impact of Steatosis on Prognosis of Patients with Early-Stage Hepatocellular Carcinoma After Hepatic Resection. Annals of Surgical Oncology. 2015/07/01 2015, 22, 2253–2261. [Google Scholar] [CrossRef]
- Wakai, T.; Shirai, Y.; Sakata, J.; Korita, P.V.; Ajioka, Y.; Hatakeyama, K. Surgical Outcomes for Hepatocellular Carcinoma in Nonalcoholic Fatty Liver Disease. Journal of Gastrointestinal Surgery. 2011/08/01/ 2011, 15, 1450–1458. [Google Scholar] [CrossRef]
- Viganò, L.; Conci, S.; Cescon, M.; et al. Liver resection for hepatocellular carcinoma in patients with metabolic syndrome: A multicenter matched analysis with HCV-related HCC. Journal of Hepatology. 2015/07/01/ 2015, 63, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Lyu, H.; He, Y.; Xia, Y.; Li, J.; Shen, F. Comparison of Hepatectomy for Patients with Metabolic Syndrome-Related HCC and HBV-Related HCC. Journal of Gastrointestinal Surgery. 2018/04/01/ 2018, 22, 615–623. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Brubaker, L.; Curfman, G. The 2024 Revision to the Declaration of Helsinki: Modern Ethics for Medical Research. JAMA. 2025, 333, 30–31. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007, 370, 1453–7. [Google Scholar] [CrossRef]
- Song, B.G.; Choi, S.C.; Goh, M.J.; et al. Metabolic dysfunction-associated fatty liver disease and the risk of hepatocellular carcinoma. JHEP Rep. 2023, 5, 100810. [Google Scholar] [CrossRef] [PubMed]
- NIH (National Heart L, and Blood Institute). What is Metabolic Syndrome? 02-28-2025, 2025. https://www.nhlbi.nih.gov/health/metabolic-syndrome?
- Hendrix, J.M.; Garmon, E.H. American Society of Anesthesiologists Physical Status Classification System. StatPearls. 2025.
- Azam, F.; Latif, M.F.; Farooq, A.; Tirmazy, S.H.; AlShahrani, S.; Bashir, S.; Bukhari, N. Performance Status Assessment by Using ECOG (Eastern Cooperative Oncology Group) Score for Cancer Patients by Oncology Healthcare Professionals. Case Rep Oncol. Sep- 2019, 12, 728–736. [Google Scholar] [CrossRef]
- Ananchuensook, P.; Sriphoosanaphan, S.; Suksawatamnauy, S.; et al. Validation and prognostic value of EZ-ALBI score in patients with intermediate-stage hepatocellular carcinoma treated with trans-arterial chemoembolization. BMC Gastroenterol. 2022, 22, 295. [Google Scholar] [CrossRef]
- Kudo, M. Newly Developed Modified ALBI Grade Shows Better Prognostic and Predictive Value for Hepatocellular Carcinoma. Liver Cancer. 2022, 11, 1–8. [Google Scholar] [CrossRef]
- Wei, Y.; Huang, X.; Pei, W.; Zhao, Y.; Liao, H. MRI Features and Neutrophil-to-Lymphocyte Ratio (NLR)-Based Nomogram to Predict Prognosis of Microvascular Invasion-Negative Hepatocellular Carcinoma. J Hepatocell Carcinoma 2025, 12, 275–287. [Google Scholar] [CrossRef]
- Chan, K.S.; Shelat, V.G. The role of platelet-lymphocyte ratio in hepatocellular carcinoma: a valuable prognostic marker. Transl Cancer Res. 2022, 11, 4231–4234. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Zhang, P.; Qi, J.; et al. Prognostic value of platelet to lymphocyte ratio in hepatocellular carcinoma: a meta-analysis. Sci Rep. 2016, 6, 35378. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Cai, J.Y.; Li, H.; et al. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio as Prognostic Predictors for Hepatocellular Carcinoma Patients with Various Treatments: a Meta-Analysis and Systematic Review. Cellular Physiology and Biochemistry. 2017, 44, 967–981. [Google Scholar] [CrossRef]
- Calvaruso, V.; Burroughs, A.K.; Standish, R.; et al. Computer-assisted image analysis of liver collagen: relationship to Ishak scoring and hepatic venous pressure gradient. Hepatology. 2009, 49, 1236–44. [Google Scholar] [CrossRef]
- Ferenci, P.; Aires, R.; Beavers, K.L.; et al. Predictive value of FIB-4 and APRI versus METAVIR on sustained virologic response in genotype 1 hepatitis C patients. Hepatol Int. 2014, 8, 83–93. [Google Scholar] [CrossRef]
- Ho, S.Y.; Wang, L.C.; Hsu, C.Y.; Liu, P.H.; Hsia, C.Y.; Huang, Y.H.; Huo, T.I. Metavir Fibrosis Stage in Hepatitis C-Related Hepatocellular Carcinoma and Association with Noninvasive Liver Reserve Models. J Gastrointest Surg. 2020, 24, 1860–1862. [Google Scholar] [CrossRef]
- Liao, R.; Fu, Y.P.; Wang, T.; et al. Metavir and FIB-4 scores are associated with patient prognosis after curative hepatectomy in hepatitis B virus-related hepatocellular carcinoma: a retrospective cohort study at two centers in China. Oncotarget. 2017, 8, 1774–1787. [Google Scholar] [CrossRef]
- Eps. EASL Policy Statement Risk-based Surveillance for Hepatocellular Carcinoma Among Patients with Cirrhosis. 02-28-2025, 2025. Accessed 02-25-2025, 2025. https://easl.eu/publication/easl-policy-statement-risk-based/.
- Chernyak, V.; Fowler, K.J.; Kamaya, A.; et al. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: Imaging of Hepatocellular Carcinoma in At-Risk Patients. Radiology. 2018, 289, 816–830. [Google Scholar] [CrossRef]
- Ertle, J.; Dechene, A.; Sowa, J.P.; et al. Non-alcoholic fatty liver disease progresses to hepatocellular carcinoma in the absence of apparent cirrhosis. Int J Cancer. 2011, 128, 2436–43. [Google Scholar] [CrossRef]
- Pinter, M.; Trauner, M.; Peck-Radosavljevic, M.; Sieghart, W. Cancer and liver cirrhosis: implications on prognosis and management. ESMO Open. 2016, 1, e000042. [Google Scholar] [CrossRef]
- Hoffmann, K.; Muller-Butow, V.; Franz, C.; Hinz, U.; Longerich, T.; Buchler, M.W.; Schemmer, P. Factors predictive of survival after stapler hepatectomy of hepatocellular carcinoma: a multivariate, single-center analysis. Anticancer Res. 2014, 34, 767–76. [Google Scholar] [PubMed]
- Yeh, C.N.; Lee, W.C.; Chen, M.F.; Tsay, P.K. Predictors of long-term disease-free survival after resection of hepatocellular carcinoma: two decades of experience at Chang Gung Memorial Hospital. Ann Surg Oncol. 2003, 10, 916–21. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.W.; Chen, Y.S.; Lin, C.C.; et al. Significant predictors of overall survival in patients with hepatocellular carcinoma after surgical resection. PLoS One. 2018, 13, e0202650. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021, 7, 6. [Google Scholar] [CrossRef]
- Pais, R.; Fartoux, L.; Goumard, C.; Scatton, O.; Wendum, D.; Rosmorduc, O.; Ratziu, V. Temporal trends, clinical patterns and outcomes of NAFLD-related HCC in patients undergoing liver resection over a 20-year period. Aliment Pharmacol Ther. 2017, 46, 856–863. [Google Scholar] [CrossRef]
- Wakai, T.; Shirai, Y.; Sakata, J.; Korita, P.V.; Ajioka, Y.; Hatakeyama, K. Surgical outcomes for hepatocellular carcinoma in nonalcoholic fatty liver disease. J Gastrointest Surg. 2011, 15, 1450–8. [Google Scholar] [CrossRef]
- Nishio, T.; Hatano, E.; Sakurai, T.; et al. Impact of Hepatic Steatosis on Disease-Free Survival in Patients with Non-B Non-C Hepatocellular Carcinoma Undergoing Hepatic Resection. Ann Surg Oncol. 2015, 22, 2226–34. [Google Scholar] [CrossRef]
- Wong, C.R.; Njei, B.; Nguyen, M.H.; Nguyen, A.; Lim, J.K. Survival after treatment with curative intent for hepatocellular carcinoma among patients with vs without non-alcoholic fatty liver disease. Aliment Pharmacol Ther 10612017, 46, 1061–1069. [Google Scholar] [CrossRef]
- Rada, P.; Gonzalez-Rodriguez, A.; Garcia-Monzon, C.; Valverde, A.M. Understanding lipotoxicity in NAFLD pathogenesis: is CD36 a key driver? Cell Death Dis. 2020, 11, 802. [Google Scholar] [CrossRef]
- Ande, S.R.; Nguyen, K.H.; Gregoire Nyomba, B.L.; Mishra, S. Prohibitin-induced, obesity-associated insulin resistance and accompanying low-grade inflammation causes NASH and HCC. Sci Rep. 2016, 6, 23608. [Google Scholar] [CrossRef]
- Bae, S.D.W.; George, J.; Qiao, L. From MAFLD to hepatocellular carcinoma and everything in between. Chin Med J (Engl). 2022, 135, 547–556. [Google Scholar] [CrossRef]
- Koh, J.H.; Tan, D.J.H.; Ong, Y.; et al. Liver resection versus liver transplantation for hepatocellular carcinoma within Milan criteria: a meta-analysis of 18,421 patients. Hepatobiliary Surg Nutr. 2022, 11, 78–93. [Google Scholar] [CrossRef]
Figure 1.
Kaplan-Meier survival curves depicting overall survival (OS) (Panel A) and progression-free survival (PFS) (Panel B) in a consecutive cohort of patients undergoing curative-intent hepatic resection for hepatocellular carcinoma.
Figure 1.
Kaplan-Meier survival curves depicting overall survival (OS) (Panel A) and progression-free survival (PFS) (Panel B) in a consecutive cohort of patients undergoing curative-intent hepatic resection for hepatocellular carcinoma.
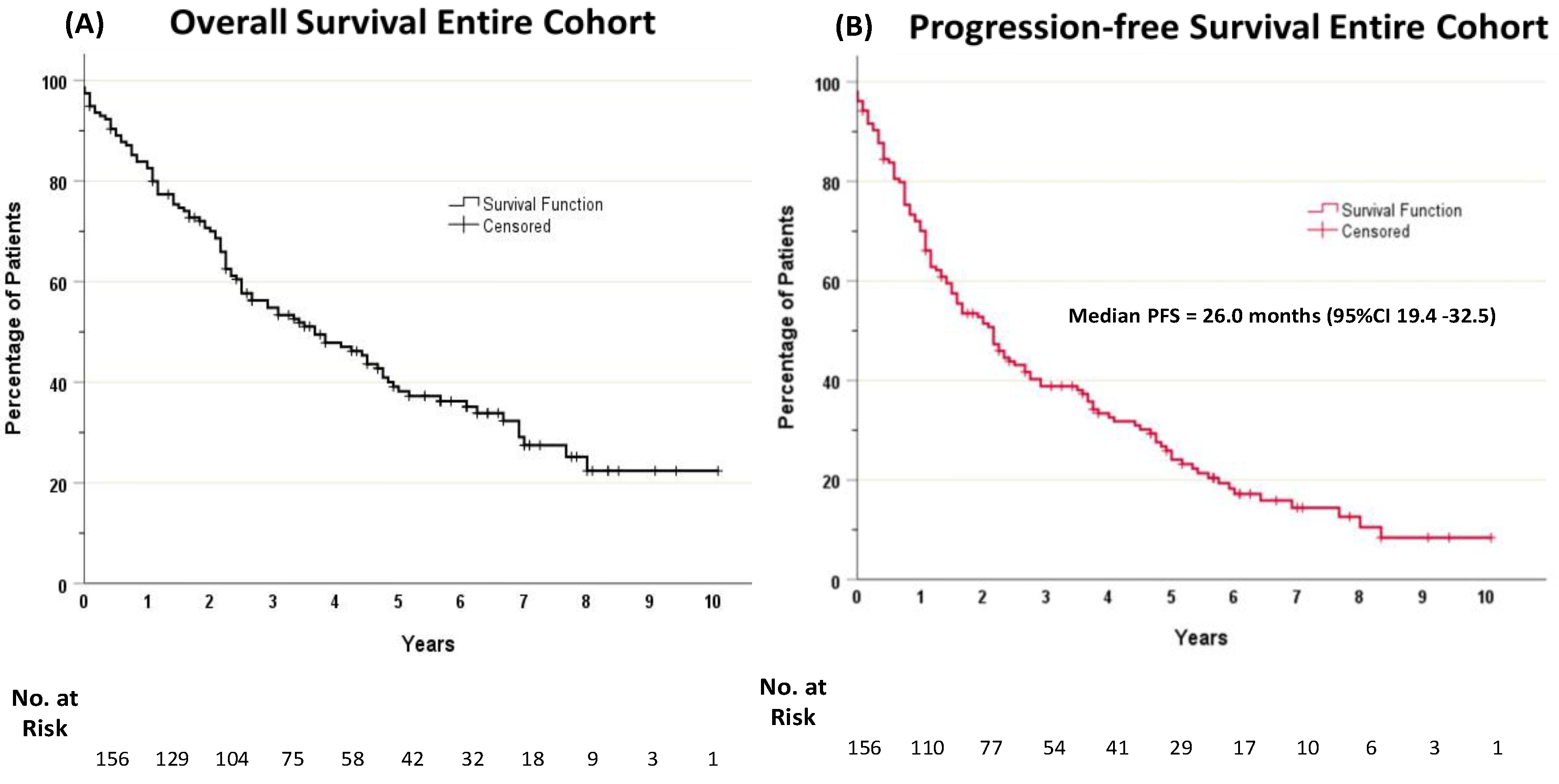
Figure 2.
Kaplan-Meier curves illustrating overall survival (OS) following hepatic resection for hepatocellular carcinoma in patients with metabolic-associated fatty liver disease (MAFLD-positive) compared to those with HCC related to non-MAFLD etiologies (MAFLD-negative).
Figure 2.
Kaplan-Meier curves illustrating overall survival (OS) following hepatic resection for hepatocellular carcinoma in patients with metabolic-associated fatty liver disease (MAFLD-positive) compared to those with HCC related to non-MAFLD etiologies (MAFLD-negative).
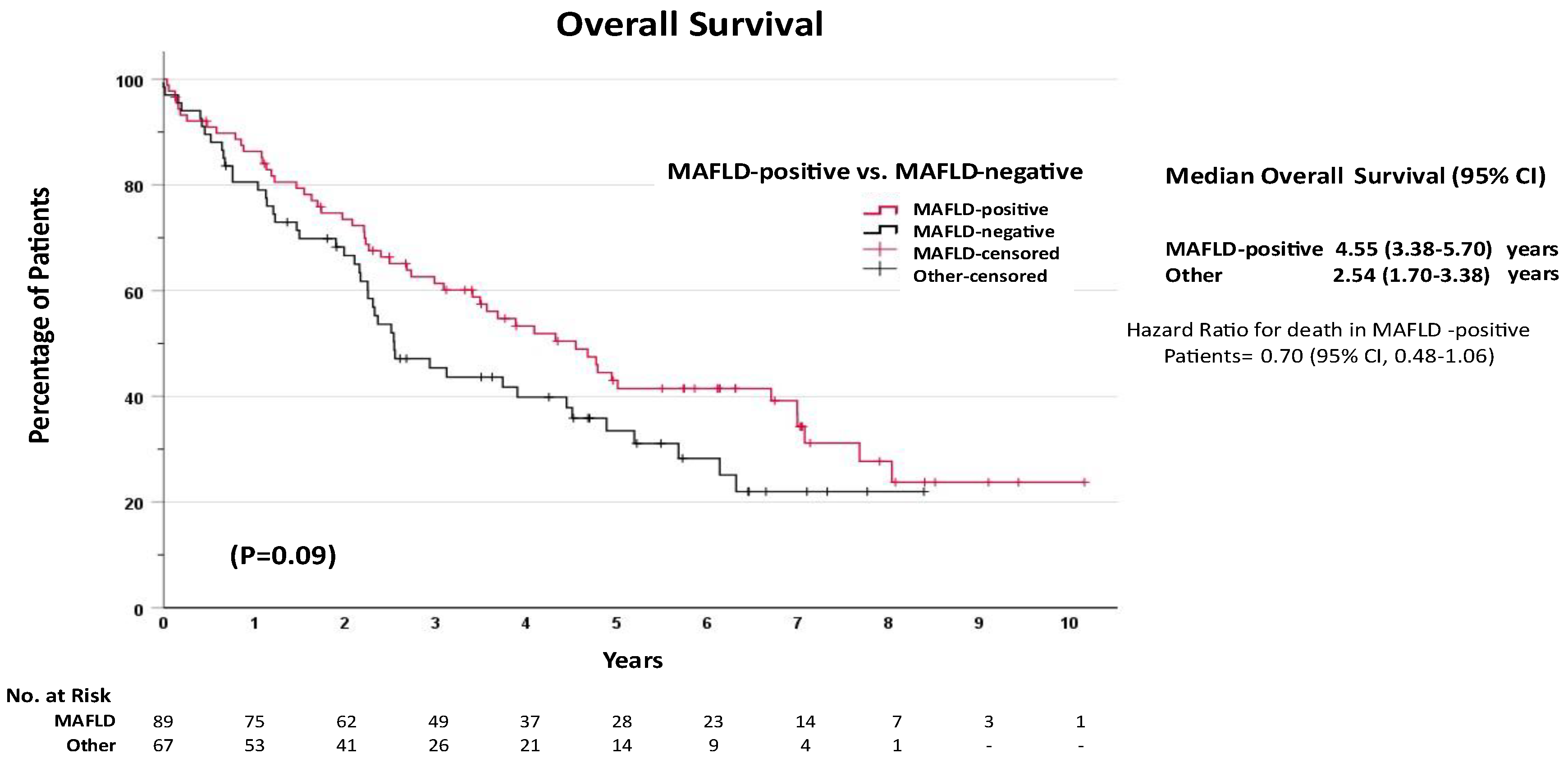
Figure 3.
Kaplan-Meier curves illustrating progression-free survival (PFS) following hepatic resection for hepatocellular carcinoma in patients with metabolic-associated fatty liver disease (MAFLD-positive) compared to those with HCC related to non-MAFLD etiologies (MAFLD-negative).
Figure 3.
Kaplan-Meier curves illustrating progression-free survival (PFS) following hepatic resection for hepatocellular carcinoma in patients with metabolic-associated fatty liver disease (MAFLD-positive) compared to those with HCC related to non-MAFLD etiologies (MAFLD-negative).
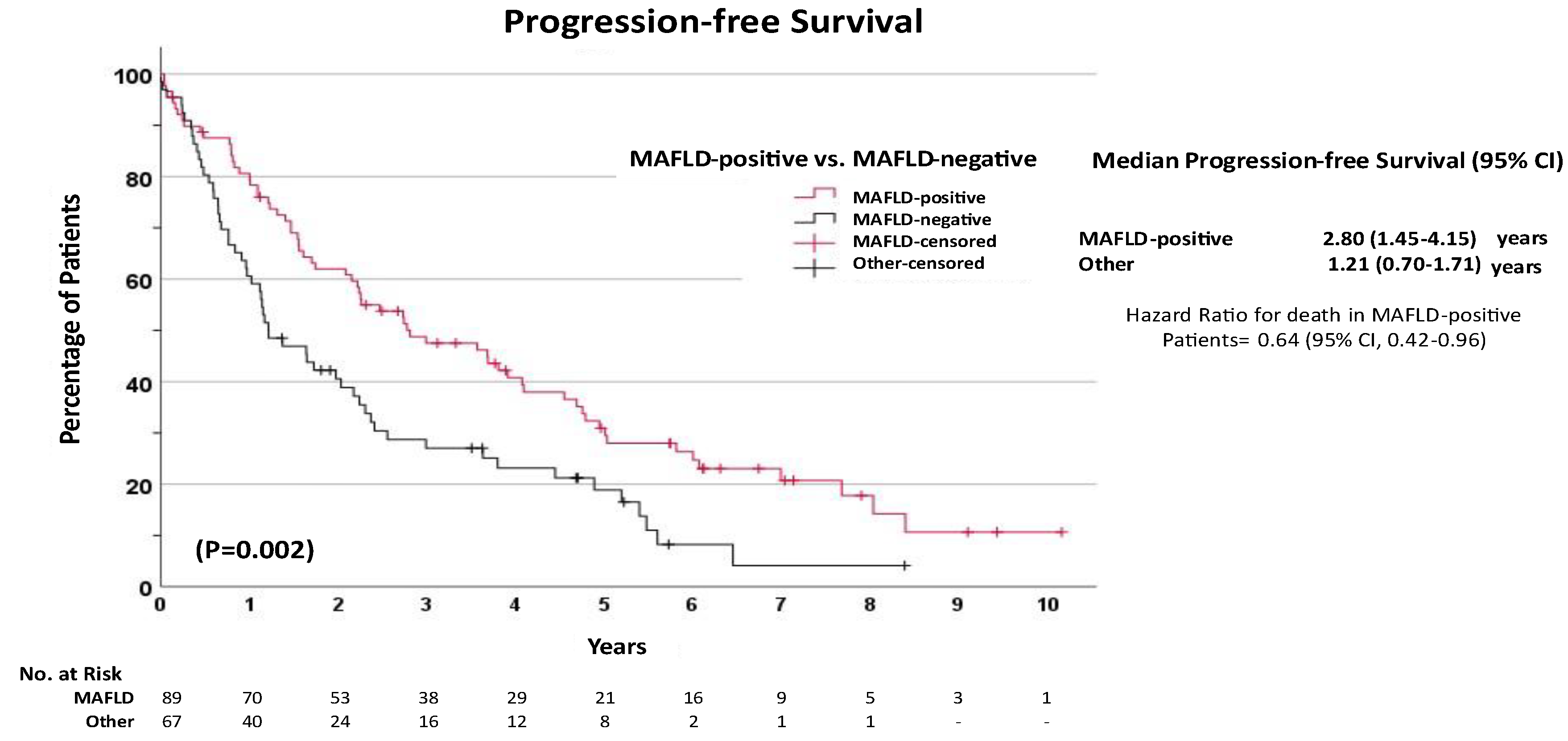

Table 5.
Univariate and multivariate analysis of risk factors for overall survival (OS) after hepatic resection for hepatocellular carcinoma.
Table 5.
Univariate and multivariate analysis of risk factors for overall survival (OS) after hepatic resection for hepatocellular carcinoma.
| Characteristics | Univariate Analysis | Multivariate Analysis | ||||||
| HR | 95% Confidence | P Value | Adjusted HR | 95% Confidence | P Value | |||
| LCI | UCI | LCI | UCI | |||||
| Diagnosis of liver disease | ||||||||
| MAFLD-negative | 1 | Reference | - | 1 | Reference | |||
| MAFLD-positive | 0.70 | 0.48 | 1.06 | 0.093 | 0.91 | 0.45 | 1.84 | 0.785 |
| Presence of cirrhosis | 1.62 | 1.09 | 2.42 | 0.019 | 2.32 | 1.16 | 4.64 | 0.018 |
| Age | 1.03 | 1.01 | 1.05 | 0.009 | 1.02 | 0.99 | 1.06 | 0.223 |
| Sex | ||||||||
| Female | 1 | Reference | Reference | |||||
| Male | 1.22 | 0.77 | 1.94 | 0.400 | 1.34 | 0.72 | 2.48 | 0.356 |
| Diabetes | 0.99 | 0.67 | 1.47 | 0.960 | 0.98 | 0.56 | 1.72 | 0.938 |
| Cigarette smoking | 0.87 | 0.57 | 1.33 | 0.522 | 0.57 | 0.32 | 1.03 | 0.062 |
| Obesity | ||||||||
| Non-obese | 1 | Reference | 1 | Reference | ||||
| Obese | 0.663 | 0.434 | 1.011 | 0.056 | 0.76 | 0.41 | 1.40 | 0.380 |
| ECOG | ||||||||
| ECOG 0 | 1 | Reference | 1 | Reference | ||||
| ECOG 1 | 1.35 | 0.81 | 2.27 | 0.253 | 1.74 | 0.95 | 3.18 | 0.075 |
| ECOG ≥2 | 1.89 | 1.11 | 3.24 | 0.019 | 2.67 | 1.29 | 5.50 | 0.008 |
| Number of tumors | ||||||||
| Single lesion | 1 | Reference | 1 | Reference | ||||
| Two lesions | 1.22 | 0.75 | 1.99 | 0.418 | 1.26 | 0.66 | 2.40 | 0.484 |
| Three or more lesions | 1.33 | 0.78 | 2.26 | 0.294 | 1.31 | 0.61 | 2.80 | 0.491 |
| Alpha feto-protein | ||||||||
| 0-10 | 1 | Reference | 1 | Reference | ||||
| 10.1-100 | 1.194 | 0.729 | 1.955 | 0.482 | 1.39 | 0.73 | 2.67 | 0.319 |
| >100 | 1.821 | 1.069 | 3.100 | 0.027 | 2.89 | 1.45 | 5.76 | 0.003 |
| Cellular differentiation | ||||||||
| Well differentiated | 1 | Reference | - | 1 | Reference | - | ||
| Moderately differentiated | 0.305 | 0.089 | 1.042 | 0.058 | 0.17 | 0.01 | 2.06 | 0.162 |
| Poorly differentiated | 0.469 | 0.147 | 1.500 | 0.202 | 0.32 | 0.03 | 4.13 | 0.386 |
| Lymphovascular invasion | 0.634 | 0.181 | 2.232 | 0.478 | 1.05 | 0.52 | 2.12 | 0.894 |
| Tumor stage | ||||||||
| T1 | 1 | Reference | - | 1 | Reference | - | ||
| T2 | 1.086 | 0.693 | 1.700 | 0.719 | 0.91 | 0.41 | 2.00 | 0.817 |
| T3 | 1.98 | 1.055 | 3.715 | 0.033 | 2.91 | 0.92 | 9.18 | 0.069 |
| T4 | 2.464 | 1.098 | 5.529 | 0.029 | 1.91 | 0.61 | 6.01 | 0.269 |
| Neutrophil-to-Lymphocyte Ratio (NLR) >3 | 1.506 | 1.012 | 2.242 | 0.043 | 1.44 | 0.83 | 2.48 | 0.196 |
| Platelet-to-Lymphocyte Ratio (PLR) > 150 | 0.861 | 0.557 | 1.330 | 0.499 | 1.01 | 0.52 | 1.96 | 0.986 |
| ALBI score | ||||||||
| Grade 1 | 1 | Reference | - | 1 | Reference | - | ||
| Grade 2 | 1.717 | 1.074 | 2.746 | 0.024 | 1.05 | 0.57 | 1.92 | 0.876 |
| Grade 3 | 2.121 | 1.017 | 4.424 | 0.045 | 0.73 | 0.27 | 1.98 | 0.536 |
Table 6.
Univariate and multivariate analysis of risk factors for progression-free survival (PFS) after hepatic resection for hepatocellular carcinoma.
Table 6.
Univariate and multivariate analysis of risk factors for progression-free survival (PFS) after hepatic resection for hepatocellular carcinoma.
| Characteristics | Univariate Analysis | Multivariate Analysis | ||||||
| HR | 95% Confidence | P Value | Adjusted HR | 95% Confidence | P Value | |||
| LCI | UCI | LCI | UCI | |||||
| Diagnosis of liver disease | 0.003 | 0.845 | ||||||
| MAFLD-negative | 1 | Reference | 1 | Reference | ||||
| MAFLD-positive | 0.57 | 0.40 | 0.82 | 0.003 | 0.58 | 0.28 | 1.19 | 0.139 |
| Presence of cirrhosis | 1.69 | 1.18 | 2.43 | 0.004 | 1.82 | 0.86 | 3.85 | 0.117 |
| Age | 1.01 | 0.99 | 1.03 | 0.262 | 0.99 | 0.95 | 1.03 | 0.862 |
| Sex | ||||||||
| Female | 1 | Reference | 1 | Reference | ||||
| Male | 1.31 | 0.86 | 1.99 | 0.207 | 1.52 | 0.70 | 3.20 | 0.284 |
| Diabetes | 0.97 | 0.81 | 1.16 | 0.753 | 1.37 | 0.72 | 2.61 | 0.334 |
| Cigarette smoking | 1.03 | 0.70 | 1.50 | 0.898 | 0.59 | 0.29 | 1.19 | 0.144 |
| Obesity | 0.641 | 0.44 | 0.934 | 0.021 | 1.10 | 0.57 | 2.09 | 0.773 |
| ECOG | 0.655 | 0.378 | ||||||
| ECOG 0 | 1 | Reference | 1 | Reference | ||||
| ECOG 1 | 1.19 | 0.74 | 1.92 | 0.468 | 1.42 | 0.69 | 2.94 | 0.336 |
| ECOG ≥2 | 1.21 | 0.72 | 2.04 | 0.462 | 1.00 | 0.10 | 9.52 | 0.998 |
| Number of tumors | 0.004 | 0.016 | ||||||
| Single lesion | 1 | Reference | 1 | Reference | ||||
| Two lesions | 1.86 | 1.20 | 2.89 | 0.005 | 2.34 | 1.12 | 4.93 | 0.024 |
| Three or more lesions | 1.82 | 1.14 | 2.91 | 0.012 | 3.10 | 1.27 | 7.60 | 0.013 |
| Alpha feto-protein | 0.015 | 0.003 | ||||||
| 0-10 | 1 | Reference | 1 | Reference | ||||
| 10.1-100 | 1.44 | 0.93 | 2.22 | 0.100 | 1.68 | 0.97 | 2.93 | 0.065 |
| >100 | 2.00 | 1.21 | 3.30 | 0.007 | 3.12 | 1.59 | 6.09 | <0.001 |
| Cellular differentiation | 0.857 | 0.364 | ||||||
| Well differentiated | 1 | Reference | 1 | Reference | ||||
| Moderately differentiated | 0.69 | 0.21 | 2.29 | 0.547 | 0.72 | 0.22 | 0.58 | 0.898 |
| Poorly differentiated | 0.72 | 0.23 | 2.30 | 0.584 | 0.82 | 0.24 | 2.31 | 0.905 |
| Lymphovascular invasion | 1.07 | 0.75 | 1.54 | 0.697 | 0.58 | 0.26 | 1.29 | 0.184 |
| Tumor stage | 0.096 | 0.658 | ||||||
| T1 | 1 | Reference | 1 | Reference | ||||
| T2 | 1.11 | 0.74 | 1.65 | 0.615 | 0.74 | 0.44 | 1.24 | 0.249 |
| T3 | 1.67 | 0.92 | 3.02 | 0.092 | 1.57 | 0.71 | 3.47 | 0.267 |
| T4 | 2.23 | 1.05 | 4.72 | 0.037 | 1.80 | 0.73 | 4.47 | 0.204 |
| Neutrophil-to-Lymphocyte Ratio (NLR) >3 | 1.50 | 1.04 | 2.14 | 0.028 | 1.43 | 0.94 | 2.19 | 0.098 |
| Platelet-to-Lymphocyte Ratio (PLR) > 150 | 0.77 | 0.52 | 1.14 | 0.189 | 1.00 | 0.54 | 1.85 | 0.996 |
| ALBI score | 0.012 | 0.972 | ||||||
| Grade 1 | 1 | Reference | 1 | Reference | ||||
| Grade 2 | 1.56 | 1.04 | 2.33 | 0.032 | 1.01 | 0.59 | 1.74 | 0.968 |
| Grade 3 | 2.55 | 1.31 | 4.94 | 0.006 | 1.11 | 0.46 | 2.71 | 0.817 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



