Submitted:
19 June 2025
Posted:
19 June 2025
You are already at the latest version
Abstract
The case describes the following scenario: A 56-day-old Arabian filly presented with classical symptoms of respiratory distress and a rapidly deteriorating condition despite intensive antimicrobial treatment, resulting in death. Post-mortem examination revealed severe bronchopneumonia with characteristic disseminated pus-containing nodules. Microbiological tests and PCR confirmed the presence of R. hoagii carrying the virulence-associated protein A (vapA) gene. The isolate was sensitive to macrolides and fluoroquinolones but showed resistance or intermediate susceptibility to several commonly used antimicrobials. This case highlights the diagnostic and therapeutic challenges posed by this intracellular pathogen and emphasizes the importance of early detection, targeted therapy, and biosecurity measures — especially in the absence of an effective commercial vaccine.
Keywords:
vapA-positive Rhodococcus hoagii
; foal
; PCR
; antimicrobial susceptibility
1. Introduction
Rhodococcus hoagii (formerly: Rhodococcus equi) is a ubiquitous aerobic, nonsporulating, nonmotile Gram-positive bacteria belonging to genus Rhodococcus, Nocardiaceae family [1,2]. It is one of the main causative agents of severe pyogranulomatous bronchopneumonia in foals [2,3]. The disease primarily affects young horses and is associated with high morbidity and mortality, causing serious health and economic losses to the equine industry [2]. Although pyogranulomatous bronchopneumonia is the most common clinical manifestation, many affected foals may have additional extrapulmonary disorders, such as abdominal abscessation, colitis, osteomyelitis, and immune-mediated disorders: nonseptic synovitis, uveitis [4]. The intracellular location of Rhodococcus hoagii, its ability to survive and replicate in macrophages, the formation of abscesses with thick-walled capsules that impede the penetration of antimicrobial agents, as well as the tendency to develop resistance, pose serious challenges in the treatment of affected individuals. That is why there is often an apparent disconnect between the in vitro activity of antimicrobial agents and their in vivo efficacy [2,5]. Control of the disease is also made more difficult by the infection of numerous domestic and wild animal species with an incompletely understood role in the epidemic process, but with potential in the transmission of the pathogen: dogs, cats, cattle, goats, sheep, lamas, camels, buffaloes, roe deer, deer, pigs, wild boars, and wild birds [2,6,7]. Rhodococcus hoagii has gained attention as an opportunistic pathogen in human beings. Żychska et al. [2] note that the number of infections in immunocompromised people has been increasing in recent years, which is very worrying especially due to emerging antibiotic resistance.
The current article presents the case history of the first detection of VapA positive Rhodococcus hoagii in a foal in Bulgaria. The epidemiological and clinicopathological data, the diagnostic approach, and the antimicrobial susceptibility of the isolate are discussed.
2. Case Description
Stable information. A private stud farm stands a total of 55 horses, including 9 stallions, 30 are mares (2 of which are still pregnant), 8 yearlings and older, and 8 foals.
Horse rearing. Summer: outdoor living 24/7 in paddocks. Winter: indoor housing in separated individual stalls. Middle seasons: outdoor in paddocks for 7-8 hours per day if there is no rain, wind, or snow; indoor overnights.
Feeding: 10 - 12 kg good-quality hay, 2 – 4 kg alfalfa, and mineral supplements. Pregnant mares in the last trimester of gestation receive an additional 3 - 4 kg of concentrate.
Breeding management: the owner and manager of the horse farm have adopted a strategy of early foaling of the mares and most of them give birth in the winter months. As a rule, the caretakers of newborns closely monitor when the foal stands up and begins nursing colostrum. This should ideally occur within two hours after birth. If the foal is unable to suckle on its own, colostrum is administered using an orogastric tube or through bottle feeding.
Vaccination and deworming schedule: regular shots for equine influenza, rhinopneumonitis, and tetanus are applied annually. In the first year, foals receive three doses, starting at 6 months, then switch to a single booster dose annually. Regular deworming of all horses is carried out 3 times a year.
Case history. A 56-day-old female Arabian foal born on January 22, 2025, has been registered with the disease.
Physical examination. The previously healthy filly exhibited symptoms of depression, fever (40.8°C), rapid breathing (46 breaths per minute), and an increased heart rate (82 beats per minute). Notably, there was significant respiratory distress characterized by tachypnea, increased effort in breathing, increased coughing reflex, and flaring of the nostrils. Additionally, abdominal breathing and cyanosis of the mucous membranes were observed, along with a scant amount of muco-purulent nasal discharge from both nostrils. Auscultation of the lung field demonstrated crackles and bilateral wheezes. Milk intake was gradually decreased on day 3 and progressed to full inappetence. No other clinical symptoms were identified. The veterinarian's presumed diagnosis is a common cold with subsequent pneumonia and bronchitis. Paraclinical tests such as blood tests, ultrasound or X-rays have not been performed.
Treatment: After the onset of the first clinical sign, the farm's attending physician initiated intensive antimicrobial therapy with Shotapen® (Virbac, France, a long-acting pencillin-streptomycin injectable solution in a standard therapeutic dose by IM injection) in combination with T.M.P.S.® inj. (trimethoprim-sulfamethoxazole solution administered at a dosage of 15 mg/kg every 12 hours by intravenous route). Due to the lack of improvement in the general condition, on the 3rd day, the treatment was continued with off-label use of Gentamox® (Hipra, Spain, amoxicillin-gentamicin, injectable solution in a standard therapeutic dose by IM injection). Supportive and symptomatic treatment includes administering fluids, vitamins, and non-steroidal anti-inflammatory drugs (Phenylarthrite®, Vetoquinol, France at dose of 2.2 mg/kg, SID for 3 days).
Outcome: Despite treatment, the clinical symptoms deteriorated, and no improvement in the patient's general condition was noted over time. The filly died on March 24, 2025, at the age of 61 days. The illness lasted for 5 days, during which the foal exhibited signs of severe respiratory failure, such as shallow or irregular breathing and prolonged pauses between breaths. There were also observations of bluish or grayish discoloration of the mucous membranes and a loss of consciousness.
Gross pathology: A post-mortem examination was conducted, revealing suppurative bronchopneumonia with bilateral lung congestion and consolidation. There were multiple disseminated focal to coalescing nodules in the lung parenchyma, ranging in size from a few millimeters to 6 cm (Figure 1A, D). The nodules contained a white-yellowish substance that was visible on their cut surfaces (Figure. 1B). A single nodular area of caseation, measuring 6.2 cm, was found in the cranioventral region of the right lung (Figure 1C). The findings also included pleural effusions, and hemorrhages in the distal part of the trachea and bronchi enlarged mediastinal lymph nodes.
Sampling: The lung with the adjacent lymph nodes was submitted to the microbiology laboratory of the Faculty of Veterinary Medicine at Trakia University (Stara Zagora, Bulgaria).
Other cases: The owner reported a similar case of illness in a foal of comparable age that resulted in a fatal outcome three years ago. During the partial autopsy performed at the time, the attending veterinarian identified intussusception as the cause of death. However, a full autopsy was not conducted, and no samples were submitted for etiological diagnosis.
Diagnosis. The preliminary diagnosis, based on the available evidence, including epidemiological data, clinical symptoms, and necropsy findings, includes a bacterial infection with commonly reported pyogenic organisms such as Streptococcus zooepidemicus, Rhodococcus hoagii, Corynebacterium pseudotuberculosis, Actinobacillus equuli or others comonly reported as potential causes of similar conditions [8,9]. Diagnosis was confirmed by conventional microbiological examination, followed by PCR identification of the isolate with subsequent detection of VapA virulence gene.
Microbiological testing: A conventional microbiological tests were performed, including inoculations of liquid broth media (Soyabean Casein Digest Medium, HiMedia®, India) with subsequent subcultures, as well as solid nutrient media (Blood Agar Base, HiMedia®, India supplemented with 5% defibrinated bovine blood and MacConkey Agar w/ 0.15% Bile Salts, CV and NaCl, HiMedia®, India), incubated at 37° and aerobic conditions for 7 days [10].
The initial confirmation of the isolates as R. hoagii was conducted through an analysis of culture characteristics, visualization of typical cellular morphology in Gram-stained smears, and primary characterization tests. Bacteriological testing revealed that the isolate was catalase positive, oxidase negative, and incapable of fermenting carbohydrates. After 24 hours of aerobic incubation on bovine blood agar at 37°C, translucent, nonhemolytic, smooth and shiny colonies, which tended to merge due to strong mucus production, were barely noticeable (Figure 2A). After 48 hours of cultivation, the isolate forms larger, smooth, irregularly round, mucoid colonies that appear whitish on solid medium. A close-up of colonies shows hyphae-like structures (substrate mycelium or filamentous structures) surrounding the colonies (Figure 2B). After 72 hours, the colonies display a pale pink color and a slimy texture (Figure 2C). The isolate was non-hemolytic but induced enhanced 'spade-shaped' β-hemolysis of Staphylococcus aureus when cross-streaked - positive CAMP test (Figure 2D).
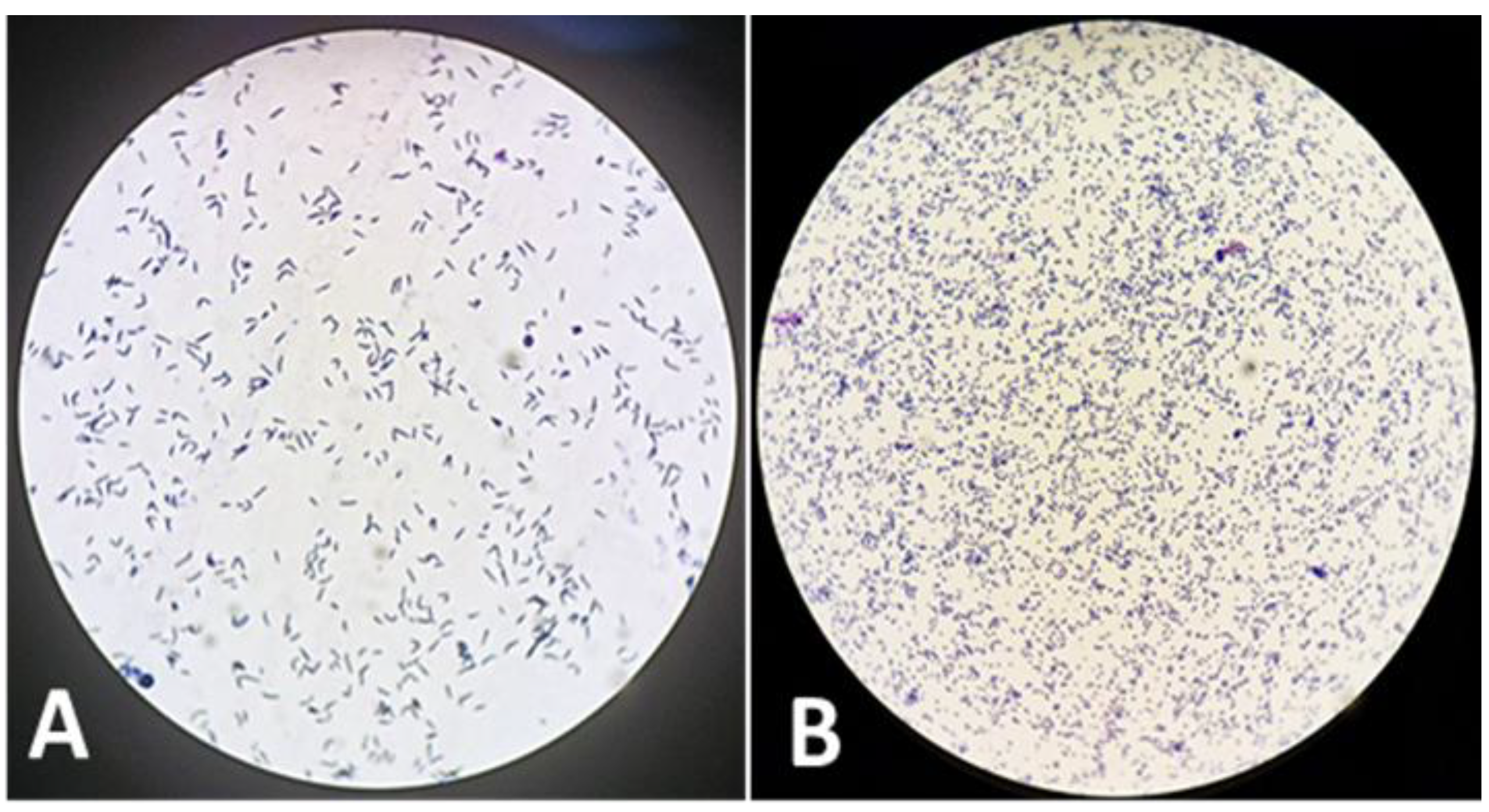
The cell morphology of R. hoagii during different growth phases shows that in the exponential phase, the cells are typically rod-shaped, whereas in the stationary phase, they tend to acquire a coccoid (spherical) shape (Figure 3).
Sensitivity to antimicrobials: Susceptibility to various antimicrobial agents was determined in vitro by the Kirby-Bauer disk diffusion technique on Mueller-Hinton medium enriched with bovine blood (HiMedia®, India). After 24 hours of incubation, the diameters of the zones of growth inhibition were measured. The results were interpreted using the three-point Kirby–Bauer scale and classified as susceptible (S), intermediate (I), or resistant (R) based on current EUCAST and CLSI standards. Our findings showed that the isolate was sensitive to azithromycin, erythromycin, tulathromycin, clarithromycin, marbofloxacin, amoxicillin/clavulanic acid, streptomycin and gentamicin. The strain demonstrated intermediate sensitivity to rifampicin, enrofloxacin, chloramphenicol, and trimethoprim-sulfonamides. However, it was resistant to penicillin, cephalexin, oxytetracycline, and clindamycin.
Identification of organism and detection of VapA virulence gene: a swab sample of cultivated bacteria was submitted to the commercial Laboratory Laboklin GmbH & Co. KG (Germany) for Rhodococcus hoagii and Rhodococcus hoagii vapA PCR. Swab sample was incubated for 20 minutes in cobas PCR Media (Roche Diagnostics GmbH, Mannheim, Germany), 200 μl of the supernatant were automatically pipetted by a Hamilton Microlab STARlet (Hamilton Germany GmbH – Robotics, Gräfelfing, Germany) into a MagNa Pure 96 Processing Cartridge (Roche Diagnostics GmbH, Mannheim, Germany). Automated total NA extraction was performed by the “MagNA Pure 96 DNA and Viral NA small volume kit” (Roche Diagnostics GmbH, Mannheim, Germany) according to the manufacturer’s instructions. The resulting NA were eluted in a volume of 100 μl. Isolated NA was stored at -20 °C. To control the successful NA extraction, an extraction control using the DNA or RNA Process Control (Detection) Kit (Roche Diagnostics GmbH, Mannheim, Germany) was included in every sample.
To prepare the master mixes for R. hoagii and R. hoagii vapA the DNA Process Control Detection Kit (Roche Diagnostics GmbH) was used. Preparation of mastermixes, mixture with NA and the PCR itself were performed in separate rooms. Positive and negative controls were included in every PCR-run.
Real-time PCR assays with hydrolysis probes (qPCR) were performed on a LightCycler® 96 (Roche Diagnostics GmbH, Mannheim, Germany). The PCR-program started with an initial denaturation step for 30 s at 95 °C, followed by 40 cycles of 5 s at 95 °C and 30 s at 60 °C. qPCRs were applied as qualitative assays (negative/positive). Samples were regarded as positive with a Cq-value of <35, evaluated at a threshold of 0.05.
The following primers and probes for R. hoagii and R. hoagii vapA were used: Rhod-F 5`- CGA CAA GCG CTC GAT GTG – 3`, Rhod-R 5‘-TGC CGA AGC CCA TGA AGT- 3‘and Rhod-probe 5‘-FAM – TGG CCG ACA AGA CCG ATC AGC C – BHQ-3` and vapA-R 5`-CAG CAG TGC GAT TCT CAA TAG TG-3`, vapA-F 5´-GAA GTC GTC GAG CTG TCA TAG CT-3`and vapA-probe 5´-FAM-CAG AAC CGA CAA TGC CAC TGC CTG-BHQ – 3´.
PCR tests confirmed the presence of vapA-positive R. hoagii.
3. Discussion
The case history data presents a sporadic, fatal respiratory infection in a young foal that represents the first proven case of a virulent strain of R. hoagii in Bulgaria.
The Rhodococcus bacterium is a ubiquitous soil microorganism predominantly found in the feces of herbivorous animals, especially horses. Takai [11] notes that despite its widespread environmental distribution, infections caused by the bacterium are endemic on certain farms, occur sporadically on others, and may remain undetected in the majority of equestrian facilities. Strains of R. hoagii exhibit variability in virulence; only those expressing the highly immunogenic surface protein called virulence-associated protein (VapA) are pathogenic to foals. In farms where the disease has not been diagnosed, low-level environmental contamination has been observed. In contrast, high frequencies of virulent strains have been reported in endemic farms, both in soil from pastures, within stables, and in the feces of foals [8,11,12].
The disease typically manifests as chronic bronchopneumonia with suppuration and abscess formation [13]. A less common form is the acute variant, lasting from a few hours to several days [14]. Rhodococcosis is either a sporadic or endemic disease, with the mortality rate ranging from 30% in foals suffering from pneumonia [15] to 57% in those affected by pneumonia and extrapulmonary disorders (EPDs) [16,17].
In this case the disease develops slowly over time, appears suddenly and progresses acutely over five days, with a gradual worsening of the filly’s condition despite treatment. It is manifested in a typical respiratory form, with severe pulmonary lesions and respiratory distress. EPDs were not observed in contrast to many others outbreaks [17].
Although the disease has been known for a long time, many aspects of the infection remain unexplored. The prevalence of the infection has been better understood with the introduction of ultrasonography as a screening tool. In horse breeding farms that utilize thoracic ultrasonography, it has been discovered that over 50% of foals exhibit lung lesions, such as parenchymal consolidation and abscess formation, without demonstrating any clinical symptoms. Among those infected, 20 to 25% develop clinical signs and require antibiotic treatment [12]. This means multiple factors influence levels of clinical manifestation and vary across horse farms. Disease rates can be affected by several factors, including the levels of environmental contamination, the presence of a high number of susceptible foals, colostrum management, and other conditions that lead to a decrease in overall resistance of the foals. One of the key factors in improving neonatal protection is ensuring timely intake of colostrum [18], as the epitheliochorial placentation in mares prevents the transplacental transfer of protective maternal antibodies to the fetus [19]. Colostrum, rich in immunoglobulins is generally considered an essential source of protection against infectious agents during the neonatal period [18]. While some studies confirm the importance of colostrum intake in protecting foals against R. equi [20], others have found it insufficient for complete protection [21]. In our case, despite the timely intake of an adequate amount of colostrum, it was insufficient to prevent the disease and its fatal outcome. A possible explanation is provided by a study by Gardner et al. [22], found that hospitalized horses had lower phagocytic activity and opsonizing capacity than normal. The study suggests that there is not necessarily a correlation between IgG levels and opsonizing capacity in some foals.
Key factors for successful disease control include timely diagnosis, appropriate treatment of affected animals, and maintaining environmental hygiene to reduce the risk of infection [14]. The most recommended antibiotics for treatment are macrolides (erythromycin, clarithromycin, or azithromycin) in combination with rifampin. These antibiotics are lipophilic, allowing them to penetrate affected tissues and macrophages, where they exhibit bacteriostatic or bactericidal action depending on their concentration [5]. Macrolide antibiotics possess a positive charge in aqueous solution, especially at physiological pH levels. This positive charge is essential for their interactions with bacterial ribosomes, as well as with lipids and other biological macromolecules. Macrolides are classified as weak bases and exhibit lipophilic characteristics, with a relatively high molecular weight of approximately 500 Daltons. They tend to be unstable in acidic environments [23]. However, newer derivatives like azithromycin and roxithromycin demonstrate improved stability in acidic conditions [24]. Azithromycin has an advantage because pus is acidic, with a pH range of 5.5 to 7.2 [25]. However, these antibiotics are expensive and not readily available in practice, leading veterinarians to often initiate treatment with other more accessible agents, which may be less effective, as in our case. An increasing problem is the development of resistance of R. equi to macrolides and rifampin on some farms, complicating treatment [5]. In our case, the isolate showed intermediate sensitivity to rifampin, which is particularly concerning. Therefore, it is important to conduct sensitivity tests on all isolates to monitor resistance and select appropriate treatment. Due to the intracellular localization and sequestration nature of the inflammation, there is often a discrepancy between the in vitro activity of antimicrobial agents and their in vivo efficacy, posing another challenge in selecting antimicrobial agents [5].
Berghaus et al. [26] found that clarithromycin was more active than azithromycin, erythromycin, and gamithromycin against intracellular R. hoagii, while Giguère et al. [27] reported that enrofloxacin, gentamicin, and vancomycin were significantly more active than other drugs, with doxycycline being the least active. Some studies have demonstrated the effective use of weekly tulathromycin at a dose of 2.5 mg/kg body weight administered intramuscularly [28,29]. A similar study in Germany showed results comparable to those of azithromycin and the combination of azithromycin with rifampin [30]. The duration of therapy, which generally ranges between 3 and 12 weeks, depends on the severity of the initial lesions and the clinical response [5]. Despite the availability of active antibiotics and long-term therapeutic courses, the prognosis is not very encouraging. Giguére [5] summarizes that before the introduction of the combination of erythromycin and rifampin as the treatment of choice in the early 1980s, the prognosis of infected foals was poor, with survival rates as low as 20%. Later, it rose to 88% using erythromycin and rifampin [31]. It must be emphasized that while in the treatment of clinically manifest disease the effectiveness varies between 59% and 72% in some studies, in farms implementing a screening program to identify and treat foals with subclinical lesions, the survival rate approaches 100% [5].
The filly was treated with combinations of penicillin-streptomycin and amoxicillin-gentamicin, but without effect. Penicillins and aminoglycosides possess low molecular weights, which facilitate their diffusion toward areas of lower concentration. However, their classification as hydrophilic compounds impedes this diffusion process [25]. Many authors in the past have claimed that aminoglycosides either do not penetrate mammalian cells or penetrate poorly. However, in vivo studies have indicated that the primary mechanism for the uptake of aminoglycosides is endocytosis. Notably, these compounds are not distributed uniformly within the cells; instead, they predominantly localize within lysosomes [32]. The effectiveness of penicillins against intracellular bacteria is regarded as limited. Studies have shown that penicillin antibiotics also have poor cell penetration [33,34].
The prolonged, expensive, and uncertain treatment raises the question of disease prevention. Unfortunately, there is still no effective commercial vaccine available, despite recent progress in vector-based vaccines [35]. On affected farms, it is recommended to implement early detection and monitoring, targeted treatment, biosecurity, and environmental management. It is also important to manage certain factors effectively, such as preventing overcrowding, ensuring housing in well-ventilated and dust-free areas, minimizing dirt or dusty surfaces, rotating pastures, and isolating foals that show clinical signs of illness [36]. Foals should be closely monitored for early recognition of disease. This monitoring should include daily rectal temperature checks, serologic surveillance, measuring plasma fibrinogen levels every two weeks, and conducting physical examinations, ultrasonography, or X-rays as needed [37].
An important part of control is also the disinfection of the environment with appropriate disinfectants [38], especially given the high levels of shedding in feces [14,39], exhaled air, and respiratory secretions [40]. Contaminated soil plays a significant role — R. hoagii is often defined as a coprophilic soil-associated actinomycete [41]. Comprehensive farm management practices could potentially reduce the risk of pathogen spread and the occurrence of infections in susceptible foals, other animal species, and humans.
4. Conclusions
This report identifies the first confirmed case of R. hoagii infection in horses in Bulgaria and contributes to our understanding of its widespread distribution. This finding should alert both owners and veterinarians to potential health issues in foals on breeding farms. Rhodococcus infection has a prolonged subclinical phase, and its clinical symptoms can be indistinguishable from those caused by other pneumonic bacteria. Additionally, this infection requires specific medications and an extended course of treatment. The epidemiological significance of this particular case is crucial, as foals with pneumonia are the primary source of virulent R. hoagii contamination in the environment. Timely diagnostic measures, such as ultrasonography, bloodwork, and a thorough clinical examination, are essential to accurately assess each case of disease. To prevent permanent environmental contamination by virulent strains, it is essential to isolate sick foals, commence disease-specific therapy, and routinely sanitize and disinfect the surroundings. Ultimately, this will impact the incidence of infections and, as a result, decrease the overall use of antibiotics.
Author Contributions
Conceptualization: B. B-M., P.M. and G.Z.; methodology: P.M. K.K., B.B-M and G.Z.; resources: B.B-M., P.M. and G.Z.; writing—original draft preparation: B.B-M., P.M. and G.Z.; writing—review and editing: B.B-M., P.M. and G.Z. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this case are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| VapA | Virulence-associated protein A |
| DNA | Deoxyribonucleic acid |
| NA | Nucleic acids |
| RNA | Ribonucleic acid |
| EPDs | Extrapulmonary disorders |
References
- Kampfer, P., Dott, W., Martin, K., & Glaeser, S. P. Rhodococcus defluvii sp. nov., isolated from wastewater of a bioreactor and formal proposal to reclassify [Corynebacterium hoagii] and Rhodococcus equi as Rhodococcus hoagii comb. nov. International Journal Of Systematic And Evolutionary Microbiology 2013, 64 (Pt 3), 755–761. [CrossRef]
- Żychska M, Witkowski L, Klementowska A, Rzewuska M, Kwiecień E, Stefańska I, Czopowicz M, Szaluś-Jordanow O, Mickiewicz M, Moroz A, Bonecka J, Kaba J. Rhodococcus equi-Occurrence in Goats and Clinical Case Report. Pathogens 2021, Sep 4;10 (9):1141. [CrossRef] [PubMed] [PubMed Central]
- Giguère, S., Cohen, N. D., Keith Chaffin, M., Hines, S. A., Hondalus, M. K., Prescott, J. F., & Slovis, N. M. Rhodococcus equi: Clinical Manifestations, Virulence, and Immunity. Journal of Veterinary Internal Medicine 2011, 25 (6), 1221–123. [CrossRef]
- Johns, I. Management of Rhodococcus equi pneumonia in foals. Veterinary Medicine: Research and Reports 2013, 49. [CrossRef]
- Giguère, S. Treatment of Infections Caused by Rhodococcus equi. Veterinary Clinics of North America: Equine Practice 2017, 33 (1), 67–85. [CrossRef]
- Bryan, L.K.; Clark, S.D.; Diaz-Delgado, J.; Lawhon, S.D.; Edwards, J.F. Rhodococcus equi Infections in Dogs. Vet. Pathol. 2017, 54, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Lechinski de Paula, C.; Silveira Silva, R.O.; Tavanelli Hernandes, R.; de Nardi Junior, G.; Babboni, S.D.; Trevizan Guerra, S.; Paganini Listoni, F.J.; Giuffrida, R.; Takai, S.; Sasaki, Y.; et al. First Microbiological and Molecular Identification of Rhodococcus equi in Feces of Nondiarrheic Cats. BioMed Res. Int. 2019, 2019, 4278598. [Google Scholar] [CrossRef] [PubMed]
- Barr, B. S. Pneumonia in weanlings. Veterinary Clinics: Equine Practice 2003, 19 (1), 35-49.
- Wilkins, P. A. Lower respiratory problems of the neonate. Veterinary Clinics: Equine Practice 2003, 19 (1), 19-33.
- Quinin PJ, Carter ME, Markey B, Carter GR. Clinical veterinary microbiology, 2004.
- Takai, S. Epidemiology of Rhodococcus equi infections: A review. Veterinary Microbiology 1997, 56(3-4), 167–176.
- Sanz, M. G. Rhodococcus equi–What is New This Decade? Veterinary Clinics: Equine Practice 2023, 39(1), 1-14.
- Zink, M.C., Yager, J.A. and Smart, N.L. Corynebacterium equi infections in horses, 1958-1984: a review of 131 cases. Can. vet. J. 1986, 27, 213-217.
- Muscatello, G.; D. P. Leadon, M. Klay, A. Ocampo-Sosa, D. A. Lewis, U. Fogarty, T. Buckley, J. R. Gilkerson, W. G. Meijer and J. A. Vazquez-Boland, Rhodococcus equi infection in foals: the science of ‘rattles’. Equine vet. J. 2007, 39 (5), 470-478. [CrossRef]
- Ainsworth DM. Associations between physical examination, laboratory, and radiographic findings and outcome and subsequent racing performance of foals with Rhodococcus equi infection: 115 caes (1984-1992). J Am Vet Med Assoc. 1998, 213:510–5.
- Burton AJ, Giguère S, Berghaus LJ, Hondalus MK, Arnold RD. Efficacy of liposomal gentamicin against Rhodococcus equi in a mouse infection model and colocalization with R. equi in equine alveolar macrophages. Vet Microbiol. 2015, 176:292–300.
- Reuss SM, Chaffin MK, Cohen ND. Extrapulmonary disorders associated with Rhodococcus equi infection in foals: 150 cases (1987-2007). J Am Vet Med Assoc. 2009, 235:855–63. [CrossRef]
- Basso, D. P., Balzan, V. Z., Schrenk, R. D., Santos, J. L. L., & Cardoso, J. S. Suspeita de infecção por Rhodococcus equiem pônei neonato: relato de caso. Salão do Conhecimento 2022, 8(8).
- Rizzoni, L.B.; Miyauchi, T.A. Principais doenças dos neonatos equinos. Acta Veterinaria Brasilica 2012, 6(1), 9–16. [Google Scholar]
- Cywes-Bentley, C., J.N. Rocha, A.I. Bordin, M. Vinacur, S. Rehman, T.S. Zaidi, M. Meyer, S. Anthony, M. Lambert, D.R. Vlock, S. Giguere. Antibody to Poly-N-acetyl glucosamine provides protection against intracellular pathogens: Mechanism of action and validation in horse foals challenged with Rhodococcus equi. PLoSPathog 2018, 14 (7) Article e1007160.
- Martens, R. J., J.G. Martens, R. A. Fiske. Failure of passive immunisation by colostrum from immunised mares to protect foals against Rhodococcus equi pneumonia. Equine Veterinary Journal 1991, 23(S12), 19 – 22. [CrossRef]
- Gardner, R. B., Nydam, D. V., Luna, J. A., Bicalho, M. L., Matychak, M. B., & Flaminio, M. J. B. Serum opsonization capacity, phagocytosis, and oxidative burst activity in neonatal foals in the intensive care unit. Journal of veterinary internal medicine 2007, 21(4), 797-805.
- Stepanić, V., Žiher, D., Gabelica-Marković, V., Jelić, D., Nunhuck, S., Valko, K., & Koštrun, S. Physicochemical profile of macrolides and their comparison with small molecules. European journal of medicinal chemistry 2012, 47, 462-472.
- Periti P, Mazzei T, Mini E, Novelli A. Clinical pharmacokinetic properties of the macrolide antibiotics. Effects of age and various pathophysiological states (Part I). Clin Pharmacokinet. 1989 Apr, 16(4):193-214.
- Wagner, C., Sauermann, R., & Joukhadar, C. Principles of antibiotic penetration into abscess fluid. Pharmacology 2006, 78(1), 1-10.
- Berghaus, L. J., Giguère, S., Sturgill, T. L., Bade, D., Malinski, T. J., Huang, R. Plasma pharmacokinetics, pulmonary distribution, and in vitro activity of gamithromycin in foals. J. vet. Pharmacol. Therap. 2011, 35, 59–66.
- Giguère S., E.A. Lee, K.M. Guldbech, L.J. Berghaus. In vitro synergy, pharmacodynamics, and postantibiotic effect of 11 antimicrobial agents against Rhodococcus equi. Veterinary Microbiology 2012, 160 (1–2), 207-213.
- Carlson, K., Kuskie, K., Chaffin, K., Libal, M. C., Giguère, S., Lawhon, S. D., & Cohen, N. D. Antimicrobial activity of tulathromycin and 14 other antimicrobials against virulent Rhodococcus equi in vitro. Vet Ther. 2010, 11(2), E1-E9.
- Arnold-Lehna, D., Venner, M., Berghaus, L. J., Berghaus, R., & Giguère, S.Efficacy of treatment and survival rate of foals with pneumonia: Retrospective comparison of rifampin/azithromycin and rifampin/tulathromycin. Pferdeheilkunde 2019, 35(5), 423-430.
- Venner, M., Credner, N., Lämmer, M., & Giguère, S. Comparison of tulathromycin, azithromycin and azithromycin-rifampin for the treatment of mild pneumonia associated with Rhodococcus equi. Veterinary Record 2013, 173(16), 397–397. [CrossRef]
- Hillidge CJ. Use of erythromycin-rifampin combination in treatment of Rhodococcus equi pneumonia. Vet Microbiol. 1987, 14:337–42. [CrossRef]
- Tulkens, P. M. Intracellular distribution and activity of antibiotics. European Journal of Clinical Microbiology & Infectious Diseases 1991, 10(2), 100–106. [CrossRef]
- Jacobs, R.F.; Wilson, C.B. Intracellular penetration and antimicrobial activity of antibiotics. J. Antimicrob. Chemother. 1983, 12, S13–S20.
- Bongers, S., Hellebrekers, P., Leenen, L. P., Koenderman, L., & Hietbrink, F. Intracellular penetration and effects of antibiotics on Staphylococcus aureus inside human neutrophils: a comprehensive review. Antibiotics 2019, 8(2), 54. [CrossRef]
- Jhandai P., K. Shanmugasundaram, T. K. Bhattacharya, H. Singha, Advances in understanding immunity to Rhodococcus equi infection and vaccine development strategies: A comprehensive review. The Microbe 2024, 3, 100077. [CrossRef]
- Giguere S. Rhodococcus equi infections. In: Wilkins PA, Palmer JE, editors. Recent advances in equine neonatal care. Ithaca (NY): International Veterinary Information Services 2001.
- Giguére, S.; Prescott, F.J. Clinical manifestations, diagnosis, treatament and prevention of Rhodococcus equi infections in foals. Veterinary Microbiology 1997, v.56, n.3-4, p.313-334.
- Mete, A. Antibacterial Efficacy of Some Antiseptics and Disinfectants against Common Bacterial Agents Isolated from Horses in Turkey. Acta Vet Eurasia 2019, 45, 101–107. [Google Scholar] [CrossRef]
- Huber L., S. Giguère, L.J. Berghaus, A. Hanafi, C. Ryan, Fecal shedding of Rhodococcus equi in mares and foals after experimental infection of foals and effect of composting on concentrations of R. equi in contaminated bedding. Veterinary Microbiology 2018, 223, 42-46.
- Muscatello G, Gilkerson JR, Browning GF. Detection of Virulent Rhodococcus equi in Exhaled Air Samples from Naturally Infected Foals. J Clin Microbiol. 2009, 47 (3). [CrossRef]
- Barton, M.D. The ecology and epidemiology of Rhodococcus equi. In: Equine Infectious Diseases VI, Eds: W. Plowright, P.D. Rossdale and J.F. Wade, R&W Publications, Newmarket 1991, pp 77-81.
Figure 1.
Gross pathological picture of lesions. (A) Disseminated nodules in the lung parenchyma; (B) White-yellowish substance on the nodular cut surface; (C) Caseation of the nodular area; (D) Nodules with thick-walled capsules.
Figure 1.
Gross pathological picture of lesions. (A) Disseminated nodules in the lung parenchyma; (B) White-yellowish substance on the nodular cut surface; (C) Caseation of the nodular area; (D) Nodules with thick-walled capsules.
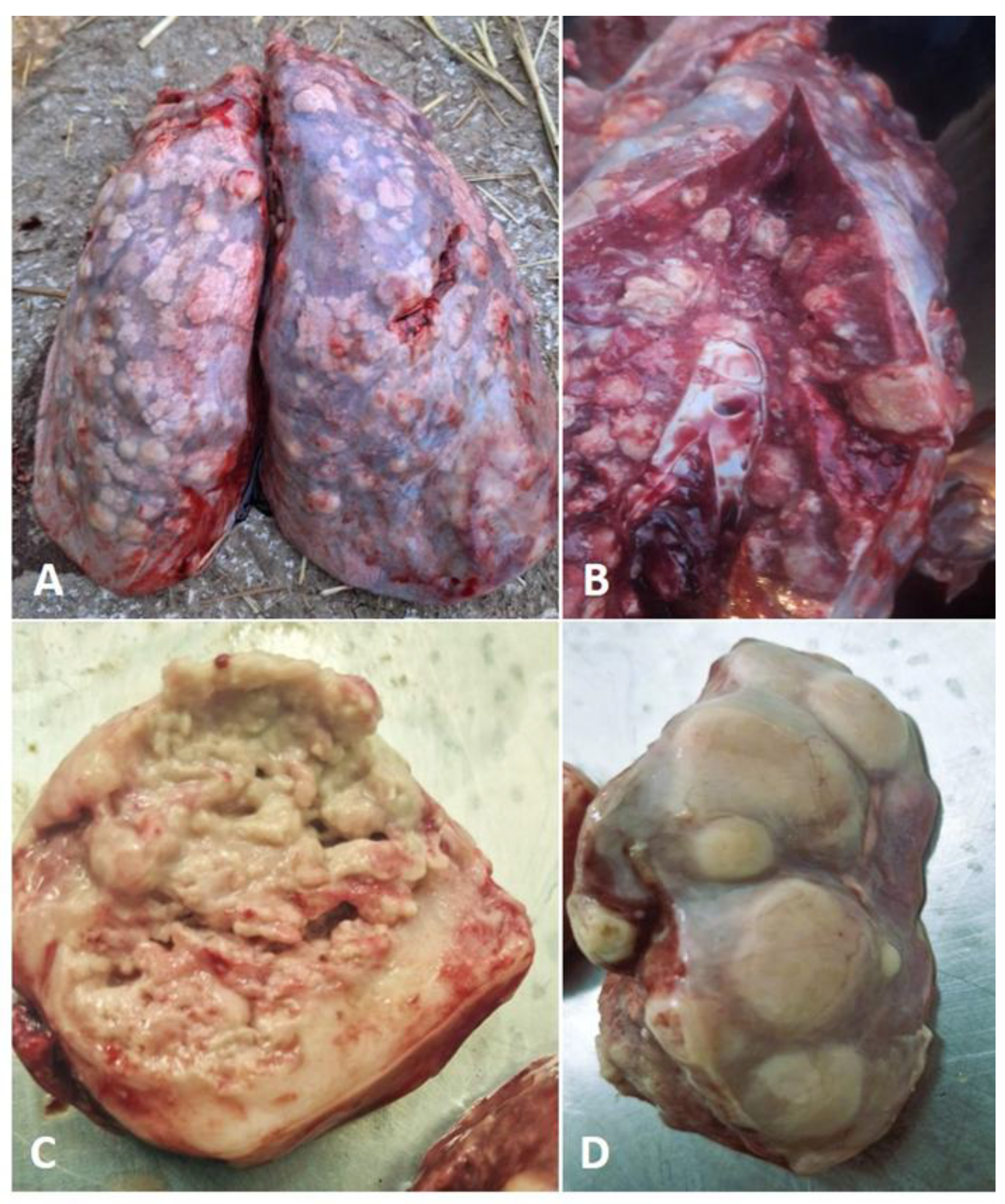
Figure 2.
Culture of R. hoagii inoculated on bovine blood agar 5% at 37°C. (A) Translucent, smooth, shiny, nonhemolytic colonies after 24-hour incubation; (B) Hyphae-like structures after 48-hour incubation; (C) Mucoid, teardrop, coalescing, glistening salmon-colored colonies after 72-hour incubation; (D) Positive CAMP test of R. hoagii (ƚ) with Staphylococcus aureus (⁎).
Figure 2.
Culture of R. hoagii inoculated on bovine blood agar 5% at 37°C. (A) Translucent, smooth, shiny, nonhemolytic colonies after 24-hour incubation; (B) Hyphae-like structures after 48-hour incubation; (C) Mucoid, teardrop, coalescing, glistening salmon-colored colonies after 72-hour incubation; (D) Positive CAMP test of R. hoagii (ƚ) with Staphylococcus aureus (⁎).
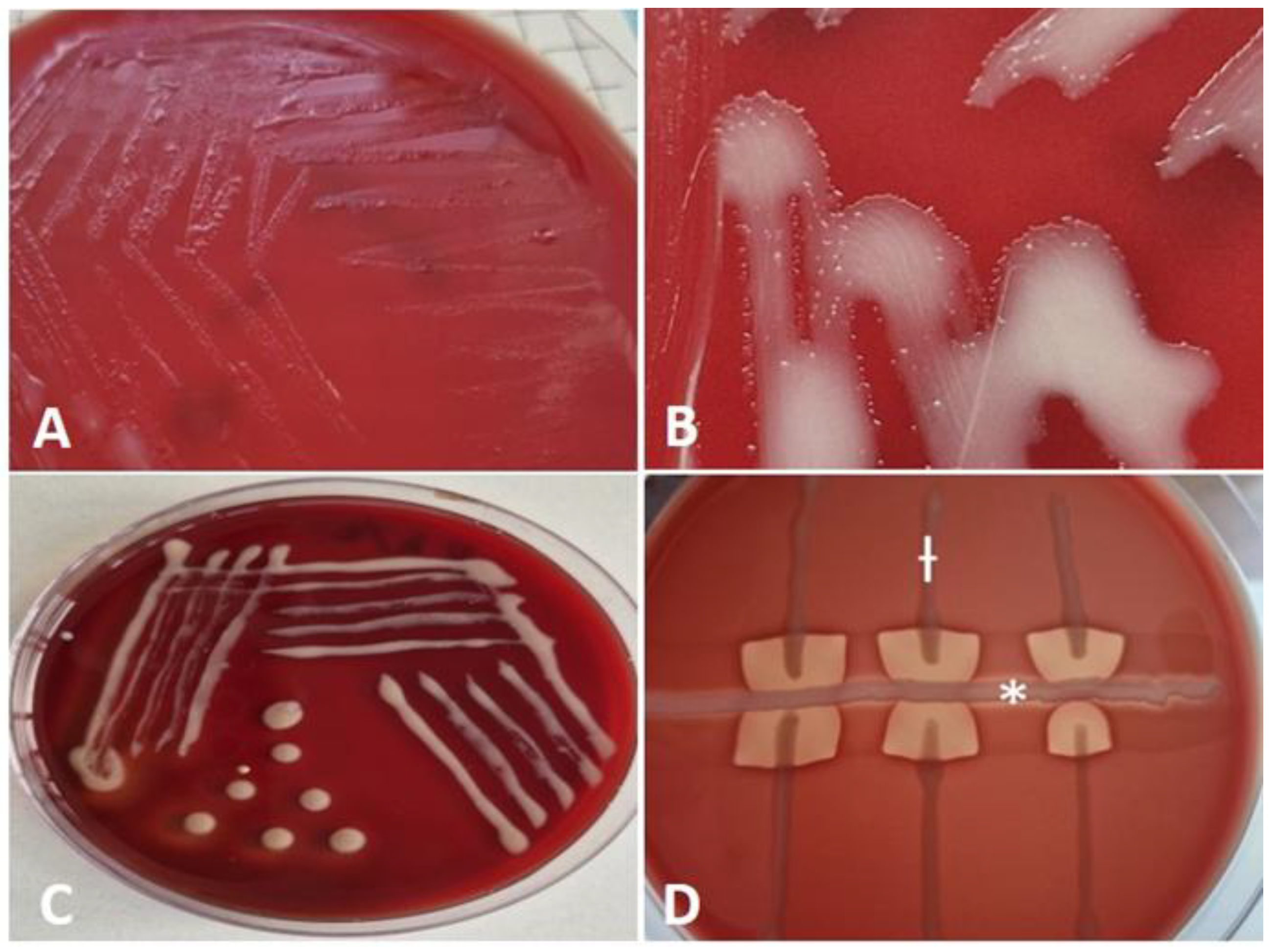
Figure 3.
Microscopic images illustrating the differential cell morphology of the isolate observed in the exponential (A) and stationary (B) growth phases.
Figure 3.
Microscopic images illustrating the differential cell morphology of the isolate observed in the exponential (A) and stationary (B) growth phases.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



