
Submitted:
11 June 2025
Posted:
12 June 2025
You are already at the latest version
Abstract
Survey researchers increasingly seek to enhance their data by linking respondents' answers to external records such as health records or pension databases. This practice requires informed consent, which can vary widely across contexts. Using data from the Survey of Health, Ageing and Retirement in Europe (SHARE), we examined cross-national variation in consent to data linkage among individuals aged 50 and over. We analysed real-life consent rates from 10 countries (N = 44,446) and hypothetical consent preferences from a pilot study in 28 countries (N = 1,963). Real-life consent rates at the first ask were highest in the Netherlands, Luxembourg, and Denmark (91% to 97.5%), and lowest in Girona and Italy. Repeated requests for consent had minimal impact. Hypothetical consent questions used standardised wording for all countries and covered four data domains: employment, pensions and social security contributions, income and taxes, and health. Hypothetical consent varied considerably, with the highest rates in Belgium, Denmark and Estonia (75%, 72%, and 71%) and the lowest in Italy, Hungary and Poland (11%, 14% and 18%). Some multilingual countries showed marked differences between language groups. Preferences for linking different types of administrative data varied across countries , although linkage to income and tax information was almost universally least popular. Multilevel regression found real-life consent was significantly associated with medium or high education levels, age, and being a minority language speaker, while gender had no effect. In contrast, male gender was the only significant predictor of hypothetical consent. Intriguingly, real-life consent rates were generally higher than hypothetical ones, suggesting that stated preferences may underestimate actual willingness. Our findings highlight the value of hypothetical consent questions as a predictive tool, and the need for a larger studies to better understand language group effects and country differences.
Keywords:
SHARE
; administrative data linkage
; older adults
; survey methodology
; privacy preference
1. Introduction
In many European countries, the availability of administrative data for research - such as pension, health, tax or employment records - has grown rapidly in recent decades. While considered highly accurate for their intended purposes, these data often lack additional information of interest to social researchers, such as household contexts and personal attitudes. Surveys, on the other hand, can be tailored to researchers’ specific topics of interest and collect data directly from respondents. However, they face challenges like non-response, recall error, and social desirability effects. Ideally, administrative and other process-generated data would be used to supplement survey data wherever available and improve data quality. Maximising the potential of these datasets requires strategic approaches to data linkage and respondent engagement.
The number of projects aimed at linking survey and administrative data has increased significantly in recent years. A critical aspect of this process is obtaining informed consent, particularly when linking survey data to these sensitive sources. This is not only an ethical imperative, but also a legal requirement under the General Data Protection Regulation (GDPR) in Europe.
A growing body of literature in survey methodology addresses the challenge of achieving high consent rates (Kreuter et al. 2016,Sakshaug et al. 2021), which vary based on survey design, national context, respondent demographics, and the type of administrative data involved. Findings on respondent characteristics, especially age, have been inconsistent across countries and studies (Bohensky et al. 2010,da Silva et al. 2012,Knies and Burton 2014). Some studies have found that older respondents are less likely to consent (Huang et al. 2007), more likely to consent (Dunn et al. 2004), or have found no effect of age at all (Baghal et al. 2014). Further variation in consent rates has been observed depending on the domain for which consent was sought (Jäckle et al. 2021,Peycheva et al. 2021), and across different age groups (Baghal et al. 2014). One takeaway from comparing consent rates across domains is their apparent ranking, with some perceived as more sensitive than others. Linkage to financial or tax data tends to yield lower consent rates than to other domains (Beuthner et al. 2022,Mostafa 2014,Walzenbach et al. 2023).
Despite this progress, cross-national, comparable data on consent behaviour remains scarce. Such research is essential for studies aiming to use linked data sources in comparative research, as it can promote culturally sensitive approaches and improve the representativeness of linked data across diverse populations. In addition, most research conducted to date has focused on the US, UK, or Germany. Reliable information on linkage consent in other countries is still lacking (Bohensky et al. 2010,Brand and Türkyılmaz 2024).
Spanning 27 European countries and Israel, the Survey of Health, Ageing and Retirement in Europe (SHARE) is ideally positioned to investigate cross-national consent rates. SHARE has been running for 20 years and focuses on individuals aged 50 and above - a demographic that has not been widely examined in consent research. Most studies consider the entire adult population, and people aged 50 and above might be summarised in just one or two categories (e.g. Baghal et al. 2014; da Silva et al. 2012; Sakshaug and Kreuter 2012), which limits insights into age-related differences in consent behaviour. Some of the countries within SHARE’s remit are multilingual, and some share a common language, allowing some scope for disentangling country-specific and language-related factors influencing consent behaviour. Additionally, SHARE’s harmonised protocols allow for more straightforward and consistent cross-national comparisons than would be possible with individual, non-standardised studies.
In this study, we investigate respondents’ consent behaviour across diverse data types and cultural contexts. Starting in Germany in 2009, SHARE has asked for consent to link data in ten countries, offering valuable insights into real-life consent behaviour. However, these linkages have covered different institutional contexts and data domains and therefore lack cross-national standardisation.
To extend our analysis, we also explore respondents’ hypothetical preferences using hypothetical consent questions, which are well-established in the literature (e.g. Bacher 2023). These consent questions are further broken down into sub-questions addressing different data domains, ranging from those generally considered as typically less sensitive to those considered as more sensitive. This approach allows us to investigate how respondents’ consent varies based on data domain sensitivity and provides a framework for more standardised cross-national comparisons.
We address the following research questions: Which demographic factors influence real-life consent behaviour, and how do real-life consent rates vary across countries? How does hypothetical willingness to consent differ by country, language group, and administrative data domain? To what extent are real-life and hypothetical consent rates comparable? To our knowledge, this is the first study to use a single, ex-ante harmonised survey to compare consent data across multiple countries, languages, and domains. It also provides the first cross-national evidence on real-life versus hypothetical consent for administrative data linkages, filling an important research gap.
2. Analysis
2.1. Data Source
We use data from SHARE, which is a longitudinal, cross-national European survey providing comprehensive data on health, socioeconomic status, and social and family networks of a representative sample of individuals (and spouses) aged 50 and above (Bergmann et al. 2019, 2022, 2021; Börsch-Supan et al. 2013). Face-to-face, computer-assisted interviews are conducted every two years. Data collection started in 2004, with 12 countries included in the first wave. The most recent, ninth wave was conducted in 2021/2022 and includes data from 27 European countries and Israel.
SHARE uses ex-ante harmonisation to standardise questions between countries: the SHARE questionnaire is designed as a generic version in English that is translated into the national languages using an internet-based translation tool in collaboration with the country teams. The national questionnaire versions are processed automatically in a software used by the interviewers of the survey agencies to administer the interview.
2.2. Real-Life Consenting Behaviours
We started by investigating real-life consent behaviours, for which we used SHARE data from Waves 5 to 9 (SHARE-ERIC 2025b) . These waves include consent questions for linking survey data with administrative databases in countries with linkage projects: Austria, Denmark, Estonia, Netherlands, Belgium, Germany, Italy, Luxembourg, and Finland. In addition, a linkage project was conducted in the province of Girona in the autonomous community of Catalonia, Spain (later referred to as Girona). For respondents first interviewed before Wave 5, demographic information is retrieved from earlier waves (SHARE-ERIC 2024a,b,c,d,e,f,g,h,i).
SHARE provides each participating country with the opportunity to introduce a national record linkage project. Due to differences in the national legal and institutional contexts, the wording of consent questions cannot be fully ex-ante harmonised across countries. Nevertheless, these questions are implemented within a standardised framework for the main procedures to maximise consistency across countries (Herold et al. 2021). As respondents’ consent to participate in the SHARE interview serves as the legal basis for data collection, additional informed consent has to be obtained for each national linkage. The SHARE questionnaire includes a separate module (approximately in the middle of the interview) with variations of consent requests tailored to each national context. Consent may be obtained in written or verbal form, depending on GDPR standards, national laws, the data domain, and data provider requirements. Regardless of the format, the interview records the respondent’s verbal reaction in the questionnaire software. Respondents always receive an information sheet explaining the linkage procedures, data sources, data exchange, and their rights in compliance with GDPR.
Inclusion criteria required participants to have been asked to consent to data linkage at least once from Wave 5 and to be at least 50 years old at the time of the first request. All analyses were conducted using R 4.4.2.
During the SHARE interview, respondents in their respective countries were asked about consent to link their interview responses with administrative data: “Do you consent to the linkage of data with the [national institute] as described in the form?", e.g. the German Pension Fund (Deutsche Rentenversicherung). Prior to Wave 8, consent approaches were more idiosyncratic as they only had to comply with national laws, resulting in country-specific adaptations. From Wave 8 onwards, the approach was standardised in line with the GDPR, with eligible participants being provided with a form outlining the linkage procedure, data handling, and the voluntary nature of participation. In addition, interviewers were trained to answer respondents’ questions and assist them with completing the consent form. As each of these national linkage projects was designed individually, there are some key differences in how and when consent was obtained, both between countries and between waves (Table A1).
Our dependent variable "consent" was operationalised as a dichotomous variable (yes/no), with positive consent marked for anyone who verbally agreed to data linkage at the first ask. Some countries require written consent in the form of a completed consent form; to make consent responses comparable to countries that only required verbal consent, we used participants’ spontaneous verbal responses ("yes", "no", or "unsure", which were also recorded) prior to signing the form. "Unsure" responses were regarded as a “no" in the analysis. It should be noted that verbal “unsure" responses could still be changed to final “yes" responses by sending in the consent form. This constellation was not considered in the analysis. In countries requiring verbal consent, the only possible answering options were “yes" and “no" and these were analysed as is.
As participants can be asked for consent to data linkage multiple times across different waves, there is a difference between participant consent at the first ask and at a later stage (if asked again). We only analyse participant consent at the first ask. This is because longer-term SHARE participants have more opportunities to be asked, while participants who join in later waves as refreshment samples have fewer opportunities to be re-asked for consent, and others leave through attrition. By focusing only on the first ask, we capture a more uniform point of comparison for all participants, regardless of when they joined or how many times they were asked.
Table 1 presents demographics for the sample, tabulated by country and consenters/non-consenters at the first ask. In total, 44,446 individuals have ever been asked about linking their data. The proportion of women was slightly higher in all countries. Most respondents were in the 50-65 and 66-80 age groups when first asked for consent, with a smaller proportion aged 81+. Minority language speakers were present in Girona, Finland, and Estonia (39% Catalan, 5% Russian, and 4% Russian respectively). We did not define a minority language for Belgium and Luxembourg because these countries do not have minority languages in the same way as other countries in the sample due to their official multilingual status.
Figure 1 presents real-life consent rates at the first ask, derived from raw point estimates, along with any net increase in consent for people who consented when later re-asked. As a sensitivity analysis in the absence of longitudinal weights, we also used a logistic regression model with covariates (age, gender, education level) to estimate consent rates for each country. Country-level estimates were obtained by averaging predicted probabilities for each country subgroup in the sample. The model-obtained rates closely aligned with the sample means (Table A2), with minimal and non-significant differences of less than 0.01 percentage points.
Consent rates were particularly high in the Netherlands, Luxembourg, and Denmark (ranging from 91% to 97.5%), while southern European regions (Girona and Italy) exhibited lower consent rates overall.
Asking participants multiple times for consent increased the likelihood of obtaining consent in Germany and Estonia, with consent rate increases of 6.3 percentage points and 4.8 percentage points respectively. In other countries, (e.g. the Netherlands, Belgium), initial non-consenters rarely changed their decision. One caveat is that as above, the rates do not account for individual variations in the number of consent re-asks. Consequently, the net excess increase is likely lower than what might be seen if every participant were asked the same number of times.
A multi-level logistic regression model was used to predict consent at the first time a respondent was asked (Table 2). The model included education level, minority linguistic group membership, age category, gender, and year asked as fixed effects, while country was treated as a random effect. Individuals with a high or medium level of education were significantly more likely to consent than those with a low level of education. Minority language speakers were significantly more likely to consent than speakers of the majority language. Age also influenced consent behaviour: individuals aged between 66 and 80 were more likely to consent than those in the 50 to 65 group. Individuals older than 80 were significantly less likely to consent. Gender had no effect on consent likelihood.
Table 2 presents results from a multi-level regression model predicting real-life consent to data linkage among 44,174 respondents with complete data , in which respondent country was treated as a random effect.
2.3. Hypothetical Willingness to Consent to Data Linkage
While we only have real-life consent data for 9 countries and one region - which further also varies by year, format, and linked institution - asking standardised hypothetical questions to all countries facilitates clearer insights into consenting behaviour. For our analysis of hypothetical consent, we use data from the SHARE Wave 10 pilot phase (March-April 2024) (SHARE-ERIC 2025a). SHARE pilots test questions in advance of the main fieldwork, aiming for approximately 100 respondents per country.
The country teams are advised to use the same sampling procedure as for the main study to also pilot test the sampling procedures, but since this is not feasible in all cases, SHARE’s central coordination allows deviation from this procedure if necessary. Countries are still asked to draw a stratified random sample covering different genders, the relevant age groups, working status and survey languages (Bethmann and Bergmann 2023). In this pilot, we introduced a special module with hypothetical questions on respondents’ willingness to consent to record linkage, ensuring comparable data across all 28 countries. The hypothetical nature of the consent questions was clearly explained to participants, emphasising that responses would not affect confidentiality of their current data, and that the data would not actually be linked.
"Given the conditions of absolute confidentiality, anonymity and academic use only, in the case that SHARE would invite you to link your interview responses to administrative information on [data domain] in the future, would you be willing to give your consent? (Yes / No)"
The question was looped four times, each covering a different administrative data domain and in the following order: (1) employment, (2) pensions and social security, (3) income and taxes, and (4) health. These domains were chosen with respect to SHARE’s older target population and the existing data linkages in place.
Although hypothetical consent questions were asked across all 28 SHARE countries, operational constraints limited them to respondents who had used the internet in the past 12 months. As a result, the hypothetical consent questions were only asked to 1,963 (68%) of the Wave 10 pilot sample (N = 2,859).
Table A3 presents the demographic characteristics of the survey participants, stratified by their hypothetical consent to link their responses to each specific data domain. Women formed the slight majority. Most adults in the sample were aged 66 to 80. Those aged 81+ formed the smallest group. Most adults fell into the medium education level. Only 4.4% of the sample were interviewed in a minority language.
Figure 2 maps hypothetical consent rates to data linkage across Europe and Israel - these have been averaged across the four data domains. There was considerable variation in consent rates across Europe. Respondents from Belgium, Denmark and Estonia (75%, 72%, and 71%) were most likely to consent. Respondents from Italy, Hungary and Poland were least likely (11%, 14% and 18%). Apart from in the Nordic countries, there was limited spatial patterning to consent behaviour - for example, Italy and Greece to the South show markedly different consent rates to data linkage.
We used a weighted mean to calculate average consent rates across countries. Each country’s rate was multiplied by the count of its 50+ population (the weight), and the total was divided by the sum of the weights across all countries. The weighted mean accounts for differences in older populations between countries, ensuring that countries with larger populations have a greater influence on the overall average while preventing countries with smaller populations from having an outsized impact on the mean. Overall, this yields an estimated average representing the total 50+ population across all SHARE countries.
Domain-wise, respondents were more likely to consent to data linkage for employment history and health than for income and taxes: weighted average hypothetical consent rates across Europe were 43.7% for pensions and social security information, 43.5% for health, 43.5% for employment history, and 35.3% for income and tax information. Figure A1 presents a country-level breakdown of consenting patterns. Despite the small sample size, the consent rates of the countries in the upper part statistically differ from those of the countries in the lower part of Figure A1 for each of the four domains.
Interestingly, the relative sensitivity of each domain varied across countries in two ways (Figure 3):
- In some countries consent was more dependent on data domain than in others, where individuals show a greater tendency towards a blanket yes/no to data linkage consent regardless of domain
- Ranking of domain consent likelihood was not consistent across countries. While the average country respondent is almost always least likely to consent to linking income and tax information, the other domains switch ranks between countries.
As SHARE covers 28 countries and conducts interviews in 39 country-specific languages, it is important to consider not only country-level differences in consent willingness, but also differences between language groups as an indicator of linguistic and cultural differences. We examined this in two ways: a) In the seven countries that are multilingual, we compared consent willingness across language groups within the same country, b) For the six languages that are spoken in more than one SHARE country, we analysed both within-language and between-country differences.
Figure 4 illustrates the first case - variation in consent willingness across language differences within the same country. Some countries, such as Switzerland (French, German, Italian), Estonia (Estonian, Russian) and Israel (Arabic, Hebrew, Russian), show noticeable differences. However, only the difference between Hebrew and Arabic speakers in Israel is statistically significant. In Luxembourg and Belgium, the language groups exhibit more similar consent rates, suggesting that linguistic or cultural differences here might have less impact.
Figure A2 depicts the second case - variation in consent willingness among speakers of the same language across different countries. We observe similar rates for German, Swedish, and Russian speakers in different countries, but different patterns across data domains. While consent willingness for German speakers in four different countries varies the most for the employment histories domain, Russian speakers differ the least for employment. For other language groups (e.g. Greek, Italian, or French), we find less similarity, both in the consent willingness per domain and the willingness hierarchy across domains. These findings highlight the complexity of consent dynamics in multilingual, multicultural contexts, however we caution that the low sample sizes here undermine finding robustness.
Table A3 shows univariate associations between gender, birth year, years of education, and entry wave, with consent (true/false) for each data domain. Male participants were significantly more likely to consent to data linkage of all types. Birth year and SHARE wave of entry had no significant effect on consent likelihood.
We ran separate multilevel logistic regression models predicting consent (yes or no) for each data domain. These models accounted for the nested structure of our data, where respondents are grouped within countries, allowing us to isolate individual-level and country-level effects on consent behaviour. Demographic variables at the individual level (age (categorical), gender (categorical), minority language speaker (categorical), and education level (categorical)) were included as fixed effects. Country was treated as a random effect. Respondents with missing data for education level or age category were removed from regression analysis (N = 103, 5.2%).
Male gender was the only significant positive predictor of consent to data linkage across all four data domains (p < 0.01, Table 3). Other demographic factors, including age, minority language status, and education level, were not significant. This contrasts strongly with the results from our earlier model using a larger sample of real-life consent data, where male gender was not significantly associated with consent, but age and education level were. The pilot study’s smaller sample size likely limited its ability to detect broader effects, particularly given the diverse contexts of the 28 countries involved.
2.4. Comparing Real-Life and Hypothetical Consent Rates
Implementing record linkage consent questions in surveys requires a considerable investment of time and money, with results that are difficult to predict. As a result, survey researchers may want to assess the likelihood of success in advance. It is therefore important to assess whether hypothetical questions provide a realistic indicator of real-life consent likelihood.
We find that in countries with both real-life and hypothetical consent data, the former were nearly always higher than the latter, with the exception of Germany (Figure 5). In Luxembourg and the Netherlands, real-life rates were considerably higher. Higher rates for real-life consent might be due to a more specific question set-up and the provision of more information to respondents about linkage procedures.
It is important to note that these rates are not directly comparable. Real-life consent data are derived from Waves 5 to 9 of the main SHARE survey, while hypothetical consent data are available only from the Wave 10 pilot study. The pilot sample in which the hypothetical questions were asked is also different from that of the main sample. Further, the domains for data linkage vary by country, reflecting the specific institutions included in each context. Hypothetical consent rates for each country are calculated based on the corresponding domains asked in the pilot study and are averaged across those domains. The domains included for each country are as follows: Denmark (DK): Employment, Health; Luxembourg (LU): Pensions; Netherlands (NL): Employment, Health, Income; Estonia (EE): Employment, Health, Pensions; Belgium (BE): Employment, Health; Finland (FI): Health, Pensions; Austria (AT): Income, Employment; Germany (DE): Pensions, Employment; Italy (IT): Pensions.
Looking at the consent rates at the country level, the Spearman correlation coefficient ( = 0.47, p = 0.23) suggests a weakly positive relationship, although it is not statistically significant.
3. Discussion
This paper investigates consent rates to record linkage with administrative data in different contexts using SHARE data, and it is the first study to analyse consent rates across multiple countries in a single survey. First, we analysed real-life consent rates across ten different countries. Second, we analysed hypothetical consent rates across 28 different countries, considering different language groups and domains of administrative data. In a third step, we compared findings from the real-life consent analysis with results from the hypothetical analysis for those countries from which we have both data types available.
We find significant cross-European variation in consent rates for both real-life and hypothetical consent requests. This adds another dimension of inconsistency regarding consent to those already identified by previous literature. In the following, we discuss some of our key findings in detail.
3.1. Individual Differences in Consent Behaviour
We found strong cross-national variation in consent likelihood for both real-life and hypothetical scenarios, although there were some notable dissimilarities between the two. In the real-life context, higher education and being middle-aged were associated with a greater likelihood of consent. In contrast, for the hypothetical questions, age showed no effect, and male gender emerged as the only positive predictor.
Strikingly, we found that repeatedly asking for consent over multiple waves had minimal effect on the likelihood of obtaining consent. In most cases, respondents who initially refused to provide consent remained firm in their decision. The strongest increases in consent rates were found in Germany (6.3%) and Estonia (4.8%). These findings are not in line with results from previous studies, noting that the effort of re-asking increases consent notably and that respondents are likely not to be consistent with their decision over waves (e.g. Jäckle et al. 2021). This may be due to details of the consent process, data domain, question wording, and country-specific differences, though.
As for hypothetical consent, our study highlights important individual and geographic differences in consent behaviour across different countries and data domains. On average across all countries examined, there were higher hypothetical consent rates for health and employment history compared to income and tax information. These findings align with existing literature underlining that individuals may perceive financial data as more sensitive or private compared to other types of information.
3.2. Cross-National Variations and the Role of Macro-Level Factors
Our study also revealed substantial cross-national differences in consent behaviour, both in terms of overall consent rates and the ranking of data domains in terms of the likelihood of obtaining consent. Even though the real-life consent questions are not standardised across countries regarding question wording, consent type (verbal/written) or data domain, they still align in terms of survey topic, target group and position of the question in the questionnaire. The lack of comparability cannot alone explain the differences between our outliers Denmark (97%) and Italy (20%).
We find similar results in country differences for the hypothetical consent rates. In our hypothetical scenario, Belgium at 75% and Italy at 11% represent notable extremes under the condition of full harmonisation. These findings suggest that differences might stem from varying macro-level factors that need to be further investigated. According to anecdotal evidence, factors influencing consent behaviour might be trust in public institutions, the familiarity of citizens with data linkage practices, and the general cultural attitudes toward privacy and government authority. It is possible that citizens from countries with higher trust in public institutions may exhibit higher overall consent rates, while those with lower institutional trust or less experience with data linkage systems may show greater resistance. Previous research from single country settings suggests that trust in institutions’ data confidentiality and/or trust in the administrative data providing institution themselves can lead to a higher consent willingness (Fobia et al. 2019; Herold, Bergmann, and Bethmann Herold et al.; Herold et al. 2023; Jäckle et al. 2023). The SHARE dataset, with its cross-European scope and standardised hypothetical consent questions, provides a unique opportunity to explore these variations across diverse cultural and institutional contexts.
3.3. Language Group Differences
Language groups within countries were considered as an indicator for cultural differences and defined as majority and minority languages accordingly. We had only three multilingual countries with real-life consent data. Surprisingly, we found that minority language speakers were significantly more likely to consent. In the hypothetical scenario, we looked at both within-country between-language differences and within-language between-country differences, but no distinct conclusion emerged. Contrary to the real-life scenario, minority language speakers consented less often in Finland and Estonia, but more often in Israel.
Variability in hypothetical consent rates across language groups highlights potential cultural and linguistic differences. This might again indicate varying trust levels in government institutions by ethnic or linguistic identity, but disentangling linguistic from cultural effects is challenging due to the small sample sizes here.
Additionally, exploring how nuances in question translation affect participation can inform culturally tailored approaches in cross-national studies. The language in which survey questions are presented can impact both comprehension and perception, and even subtle differences in translation may lead to differences in how respondents interpret questions about consent. However, disentangling these effects would likely require an experimental, randomised design.
3.4. Temporal Discrepancies and Familiarity Effects
Real-life consent rates were nearly always higher than hypothetical consent rates. Real-life consent data were drawn from Waves 5 to 9 of the main survey, while hypothetical consent data were collected exclusively during the Wave 10 pilot study. This temporal discrepancy raises the possibility of year effects, as societal attitudes, policy environments, or other external factors may have shifted over time. Moreover, some countries provided respondents with multiple opportunities to consent over several waves, who would then potentially benefit from increased familiarity with the survey. In contrast, hypothetical consent questions have only been asked once so far in SHARE. The correlated ranking between each country’s real-life and hypothetical consent rates suggests that hypothetical consent questions can serve as fairly reliable predictors of real-life consent behaviour, providing a valuable tool for planning and decision-making in data collection efforts. In this context, hypothetical consent rates may provide a lower bound for the consent rates a country can expect to observe in practice.
3.5. Limitations and Implications for Future Research
Besides novel insights into linkage consent behaviour across countries, this study also has some limitations. For the real-life consent questions, comparability across countries is hindered by factors such as non-standardised question wording, different (re-)asking strategies, and differences in the institutions providing administrative data. The analysis of hypothetical consent is mainly limited by the small sample size, which is particularly relevant to analyses of linguistic group differences. Regarding the comparison of real-life and hypothetical consent, it is important to note that the analysis is based on two distinct samples, and the questions were asked at different points in time.
Weights are essential in survey samples to correct for selection bias and ensure representativeness. However, constructing longitudinal weights is particularly challenging, as it requires accounting for changes in both the sample and the population over time, along with non-response and attrition. Although we were unable to apply these weights in our analysis of the real-life consent, we mitigated some of these concerns by including relevant demographic variables - those typically used to generate weights - directly in our regression models, helping to adjust for potential biases.
Our findings emphasise the need for a multilevel approach to understanding consent behaviour, one that considers both individual differences and broader societal influences. Future research should focus on country-level influences to better understand how systemic trust and institutional familiarity shape consent behaviour alongside individual characteristics. More research is needed to understand why countries differ in the data domains and institutions they potentially consider to be most sensitive to link to.
Additionally, our study highlights the need for culturally sensitive approaches to improving consent rates. Language group differences in consent behaviour suggest that a "one-size-fits-all" approach may not be effective in multilingual or multicultural settings. Future research should explore how the wording of consent questions and the cultural context in which they are asked may influence respondents’ decisions to consent. The same applies to interviewer effects, which need to be thoroughly explored in multilingual and multicultural settings, especially as they may be difficult to disentangle from language differences.
Taken together, our findings highlight the importance of considering country-specific contexts when designing consent questions. They also demonstrate that hypothetical consent questions can be a fruitful tool for researchers to assess where they might be more likely to gain consent to data linkage. By examining the interplay between personal and contextual factors, future research can help develop strategies to meet respondents’ needs when considering consent, improve consent rates, and ensure the ethical and effective use of linked data in research.
Acknowledgments
Imke Herold, Yuri Pettinicchi, and Arne Bethmann gratefully acknowledge the pilot project funding received from the NIA-funded Network for Innovative Methods in Longitudinal Aging Studies, or NIMLAS. Research reported in this publication was supported by the National Institute On Aging of the National Institutes of Health under Award Number U24 AG077012-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. We thank the SHARE central coordination unit for their support: especially, the questionnaire development team for their assistance in designing questions and the database management team for providing us with the internal release data. We further thank participants at the NIMLAS Plenary sessions and CSDI conference, for their helpful discussions and comments. SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA No211909, SHARE-LEAP: GA No227822, SHARE M4: GA No261982, DASISH: GA No283646) and Horizon 2020 (SHARE-DEV3: GA No676536, SHARE-COHESION: GA No870628, SERISS: GA No654221, SSHOC: GA No823782, SHARE-COVID19: GA No101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, VS 2020/0313, SHARE-EUCOV: GA No101052589 and EUCOVII: GA No101102412. Additional funding from the German Federal Ministry of Education and Research (01UW1301, 01UW1801, 01UW2202), the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, BSR12-04, R01_AG052527-02, R01_AG056329-02, R01_AG063944, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see www.share-eric.eu).
Appendix A

Table A1.
Record linkage consent procedures by country
| Country | Consent procedure |
|---|---|
| Austria | Respondents have been asked verbally for consent to link their interview responses to the Austrian Social Security Institution and the Public Employment Service Austria since Wave 5 (except Wave 6 and Wave 7). All respondents have only been asked once for their consent. |
| Belgium | Asked for the first time in Wave 7 for consent. With the implementation of the GDPR guidelines in 2018, adaptations needed to be made to the consent documents and all respondents had to be asked again in Wave 9. Written consent was obtained for a linkage with the Belgian Statistical Office (Statbel). As interviews are conducted in French and Dutch, consent documents were provided in both languages. |
| Spain (Girona) | In the region of Girona, respondents were asked within a special project to consent to the linkage of SHARE data with some of their official medical records. The consent was obtained in written form and only in Wave 6. |
| Denmark | Has conducted linkage since Wave 5. Before GDPR (Wave 5 to Wave 7), consent was not required under Danish law. From Wave 8 onwards, consent was obtained in written form for a linkage with Statistics Denmark and the Danish Health Data Authority. In Wave 8, all respondents were asked; in Wave 9, only those who had not consented in Wave 8 were asked. |
| Estonia | Has been asking for consent since Wave 5 for linkage with Statistics Estonia and several health data registries. In Wave 5, all respondents were asked; in Waves 6 and 7, only those who had not consented before. In Wave 8, all respondents had to be asked again due to GDPR; in Wave 9, only those who had not consented in Wave 8 were asked. The consent question and material were provided in Russian and Estonian. |
| Finland | Introduced a record linkage project in Wave 7 and asked verbally for consent. With GDPR, the consent request changed to written consent in Wave 8 and all respondents were asked again. The consent covers linkage with Statistics Finland, Finnish Center for Pensions (ETK), and Finnish Social Insurance Institution (Kela). In Wave 9, only those who had not consented before were asked. Consent material was provided in Finnish and Swedish. |
| Germany | Started a linkage project in Wave 3, but only consent data from Wave 5 onwards is used. Written consent was asked for linkage from Wave 3 to Wave 9 (except Wave 7) with data from the German Pension Insurance. Respondents were re-asked if they had not consented or if data could not be linked. From Wave 8 onwards, the consent request was restricted to those who had not refused twice already and changed from passive to active request. |
| Italy | Respondents were asked for consent to linkage with the Italian Social Security Institution (INPS) for the first time in Wave 8. Written consent was obtained from all respondents. The request was repeated in Wave 9 for those not asked before. |
| Luxembourg | Introduced a verbal consent question for linkage with the General Inspectorate of Social Security (IGSS) in Wave 5. All respondents received the question in Waves 5 and 6. Consent material was provided in German and French. |
| Netherlands | Verbal consent obtained in Waves 5 and 9 for linkage with Statistics Netherlands. In Wave 9, an additional information sheet was provided, and only those who had not been asked before received the consent request. |
Figure A1.
Consent rates to hypothetical data linkage show significant variation across Europe and Israel. Each bar is shown with Wilson’s confidence intervals. The dashed line shows the mean consent rate for all countries, weighted by the 50+ population count.
Figure A1.
Consent rates to hypothetical data linkage show significant variation across Europe and Israel. Each bar is shown with Wilson’s confidence intervals. The dashed line shows the mean consent rate for all countries, weighted by the 50+ population count.
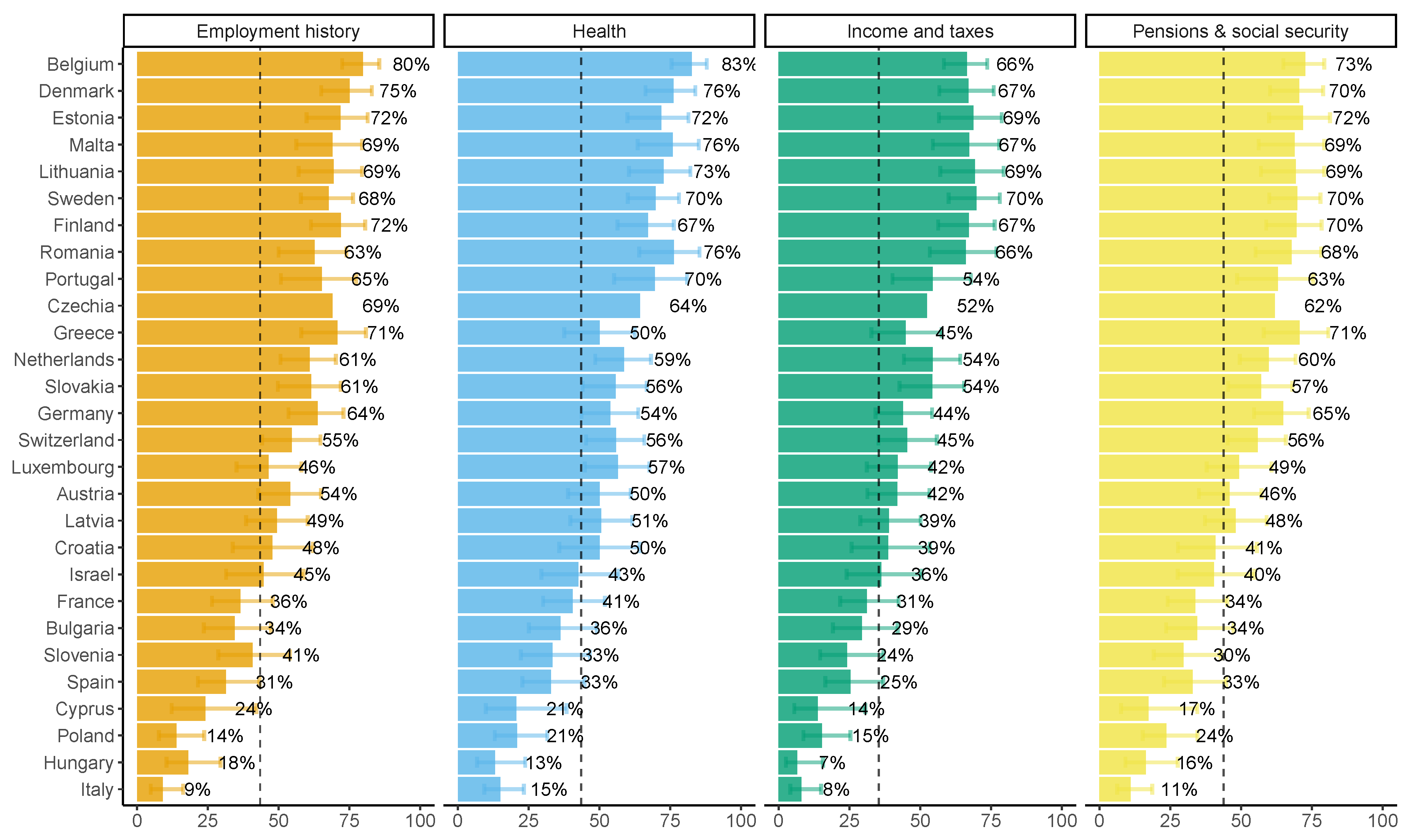
Figure A2.
Within-language, between-country variability. Bars shown with Wilson’s confidence intervals.
Figure A2.
Within-language, between-country variability. Bars shown with Wilson’s confidence intervals.
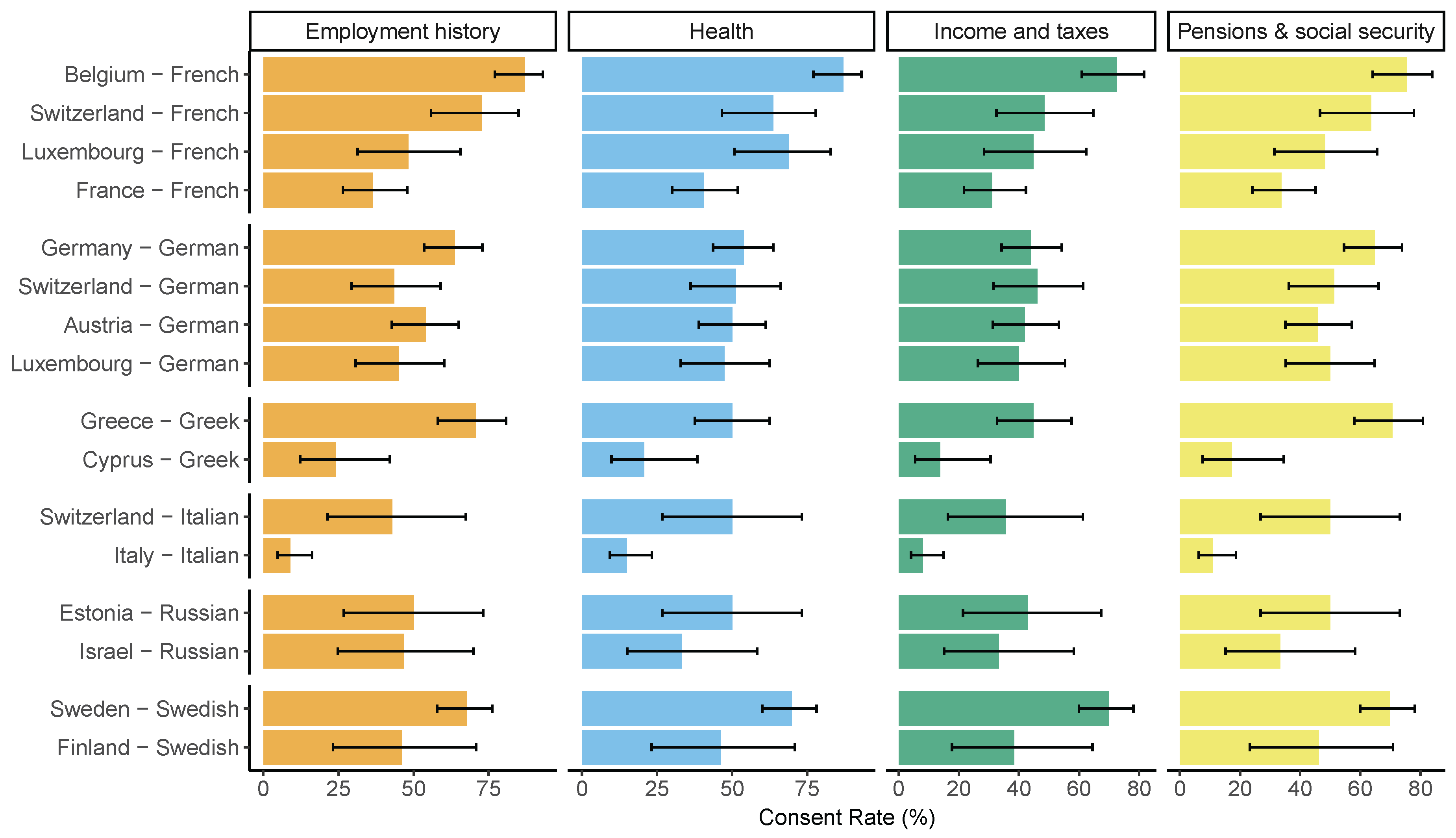
Table A2.
Model-estimated prevalence of consent at first ask and excess increase in consent rate upon further asks (where relevant), by country (adjusted for age and gender)
Table A2.
Model-estimated prevalence of consent at first ask and excess increase in consent rate upon further asks (where relevant), by country (adjusted for age and gender)
| Country | At first ask (%) | Excess (%) |
|---|---|---|
| Austria | 70.67 | 0.00 |
| Germany | 58.64 | 7.92 |
| Netherlands | 91.00 | 0.00 |
| Spain (Girona) | 45.15 | 0.00 |
| Italy | 20.08 | 0.00 |
| Denmark | 96.50 | 1.00 |
| Belgium | 86.66 | 4.49 |
| Luxembourg | 91.15 | 4.08 |
| Estonia | 82.86 | 8.19 |
| Finland | 82.31 | 2.74 |
Table A3.
Demographic characteristics for recipients of hypothetical consent questions
| Characteristic | Employment History | Health | Income and Taxes | Pensions and Social Security | ||||
|---|---|---|---|---|---|---|---|---|
| TRUE (N=1053) | FALSE (N=910) | TRUE (N=1057) | FALSE (N=906) | TRUE (N=902) | FALSE (N=1061) | TRUE (N=1025) | FALSE (N=938) | |
| Gender | ||||||||
| Female | 575 (54.6%) | 550 (60.4%) | 580 (54.9%) | 545 (60.2%) | 490 (54.3%) | 635 (59.8%) | 558 (54.4%) | 567 (60.4%) |
| Male | 478 (45.4%) | 360 (39.6%) | 477 (45.1%) | 361 (39.8%) | 412 (45.7%) | 426 (40.2%) | 467 (45.6%) | 371 (39.6%) |
| Age Category | ||||||||
| 50–65 | 468 (44.4%) | 387 (42.5%) | 465 (44.0%) | 390 (43.0%) | 395 (43.8%) | 460 (43.4%) | 455 (44.4%) | 400 (42.6%) |
| 66–80 | 511 (48.5%) | 462 (50.8%) | 513 (48.5%) | 460 (50.8%) | 434 (48.1%) | 539 (50.8%) | 494 (48.2%) | 479 (51.1%) |
| 81+ | 72 (6.8%) | 56 (6.2%) | 77 (7.3%) | 51 (5.6%) | 71 (7.9%) | 57 (5.4%) | 74 (7.2%) | 54 (5.8%) |
| Missing | 2 (0.2%) | 5 (0.5%) | 2 (0.2%) | 5 (0.6%) | 2 (0.2%) | 5 (0.5%) | 2 (0.2%) | 5 (0.5%) |
| Education Level | ||||||||
| Low | 167 (15.9%) | 151 (16.6%) | 172 (16.3%) | 146 (16.1%) | 151 (16.7%) | 167 (15.7%) | 163 (15.9%) | 155 (16.5%) |
| High | 421 (40.0%) | 259 (28.5%) | 404 (38.2%) | 276 (30.5%) | 346 (38.4%) | 334 (31.5%) | 397 (38.7%) | 283 (30.2%) |
| Medium | 430 (40.8%) | 439 (48.2%) | 439 (41.5%) | 430 (47.5%) | 373 (41.4%) | 496 (46.7%) | 427 (41.7%) | 442 (47.1%) |
| Missing | 35 (3.3%) | 61 (6.7%) | 42 (4.0%) | 54 (6.0%) | 32 (3.5%) | 64 (6.0%) | 38 (3.7%) | 58 (6.2%) |
| Minority Language | ||||||||
| Yes | 48 (4.6%) | 38 (4.2%) | 50 (4.7%) | 36 (4.0%) | 42 (4.7%) | 44 (4.1%) | 45 (4.4%) | 41 (4.4%) |
| No | 1005 (95.4%) | 872 (95.8%) | 1007 (95.3%) | 870 (96.0%) | 860 (95.3%) | 1017 (95.9%) | 980 (95.6%) | 897 (95.6%) |
References
- Bacher, Johann. 2023. Willingness to consent to data linkage in austria - results of a pilot study on hypothetical willingness for different domains. Survey Methods: Insights from the Field. [CrossRef]
- Baghal, Tarek Al, Gundi Knies, and Jonathan Burton. 2014, 12. Linking administrative records to surveys: Differences in the correlates to consent decisions. Understanding Society Working Paper Series. [CrossRef]
- Bergmann, Michael, Thorsten Kneip, Giuseppe De Luca, and Annette Scherpenzeel. 2019. Survey participation in the Survey of Health, Ageing and Retirement in Europe (SHARE). SHARE Working Paper Series, 1–7. [CrossRef]
- Bergmann, Michael, Thorsten Kneip, Giuseppe De Luca, and Annette Scherpenzeel. 2022. Survey participation in the eighth wave of the Survey of Health, Ageing and Retirement in Europe (SHARE). SHARE Working Paper Series. [CrossRef]
- Bergmann, Michael, Melanie Wagner, and Axel Börsch-Supan. 2021. Share wave 8 methodology: Collecting cross-national survey data in times of covid-19. Munich: MEA, Max Planck Institute for Social Law and Social Policy.
- Bethmann, Arne and Michael Bergmann. 2023. Share sampling guide 10. SHARE Working Paper Series. [CrossRef]
- Beuthner, Christoph, Florian Keusch, Henning Silber, Bernd Weiß, and Jette Schröder. 2022, 1. Consent to data linkage for different data domains – the role of question order, question wording, and incentives. SocArXiv. [CrossRef]
- Bohensky, Megan A., Damien Jolley, Vijaya Sundararajan, Sue Evans, David V. Pilcher, Ian Scott, and Caroline A. Brand. 2010. Data linkage: A powerful research tool with potential problems. BMC Health Services Research 10. [CrossRef]
- Brand, Türknur and Ahmet Sinan Türkyılmaz. 2024, 5. Investigating the determinants that influence consent behavior for linking survey data with administrative records. Fiscaoeconomia 8, 495–516. [CrossRef]
- Börsch-Supan, Axel, Martina Brandt, Christian Hunkler, Thorsten Kneip, Julie Korbmacher, Frederic Malter, Barbara Schaan, Stephanie Stuck, and Sabrina Zuber. 2013, August. Data resource profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). International Journal of Epidemiology 42(4), 992–1001. [CrossRef]
- da Silva, Márcia Elizabeth Marinho, Cláudia Medina Coeli, Miriam Ventura, Marisa Palacios, Mônica Maria Ferreira Magnanini, Thais Medina Coeli Rochel Camargo, and Kenneth Rochel Camargo. 2012. Informed consent for record linkage: A systematic review. Journal of Medical Ethics 38. [CrossRef]
- Dunn, Kate M., Kelvin Jordan, Rosie J. Lacey, Mark Shapley, and Clare Jinks. 2004, 6. Patterns of consent in epidemiologic research: Evidence from over 25,000 responders. American Journal of Epidemiology 159, 1087–1094. [CrossRef]
- Fobia, Aleia Clark, Jessica Holzberg, Casey Eggleston, Jennifer Hunter Childs, Jenny Marlar, and Gerson Morales. 2019. Attitudes towards data linkage for evidence-based policymaking. Public Opinion Quarterly 83, 264–279. [CrossRef]
- Herold, Imke, Michael Bergmann, and Arne Bethmann. Trust, concerns and attitudes: Examples for respondent (non-)cooperation in SHARE. Survey Research Methods.
- Herold, Imke, Michael Bergmann, and Arne Bethmann. 2023, 1. Trust in surveys, income non-response and linkage consent - the SHARE perspective. Discussion Paper. [CrossRef]
- Herold, Imke, Yuri Pettinicchi, and Daniel Schmidutz. 2021. Harmonising record linkage procedures in share. In M. Bergmann, M. Wagner, and A. Börsch-Supan (Eds.), SHARE Wave 8 Methodology: Collecting cross-national survey data in times of COVID-19. MEA, Max Planck Institute for Social Law and Social Policy.
- Huang, Nicole, Shu Fang Shih, Hsing Yi Chang, and Yiing Jenq Chou. 2007. Record linkage research and informed consent: Who consents? BMC Health Services Research 7. [CrossRef]
- Jäckle, Annette, Kelsey Beninger, Jonathan Burton, and Mick P. Couper. 2021, 1. Understanding Data Linkage Consent in Longitudinal Surveys, pp. 122–150. wiley. [CrossRef]
- Jäckle, Annette, Jonathan Burton, Mick P Couper, Thomas F Crossley, and Sandra Walzenbach. 2023, 11. Survey consent to administrative data linkage: Five experiments on wording and format. Journal of Survey Statistics and Methodology. [CrossRef]
- Knies, Gundi and Jonathan Burton. 2014. Analysis of four studies in a comparative framework reveals: Health linkage consent rates on british cohort studies higher than on uk household panel surveys. [CrossRef]
- Kreuter, Frauke, Joseph W. Sakshaug, and Roger Tourangeau. 2016, 3. The framing of the record linkage consent question. [CrossRef]
- Mostafa, Tarek. 2014, 11. Variation within households in consent to link survey data to administrative records: Evidence from the uk millennium cohort study. Technical report, Institute of Education, University of London.
- Peycheva, Darina, George Ploubidis, and Lisa Calderwood. 2021, 1. Determinants of Consent to Administrative Records Linkage in Longitudinal Surveys: Evidence from Next Steps, pp. 151–180. wiley. [CrossRef]
- Sakshaug, Joseph W and Frauke Kreuter. 2012. Assessing the magnitude of non-consent biases in linked survey and administrative data. Survey Research Methods 6, 113–122.
- Sakshaug, J W, A Schmucker, F Kreuter, M P Couper, and L Holtmann. 2021. Respondent understanding of data linkage consent survey methods: Insights from the field. Survey Methods: Insights from the Field. [CrossRef]
- SHARE-ERIC. 2024a. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 1. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024b. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 2. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024c. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 3 – SHARELIFE. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024d. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 4. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024e. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 5. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024f. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 6. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024g. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 7. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024h. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 8. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2024i. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 9. Release version: 9.0.0. SHARE-ERIC. Data set. [CrossRef]
- SHARE-ERIC. 2025a. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 4-10. Field Rehearsal & Pretest Data. Release version: 1. Internal data set. SHARE-ERIC, Munich.
- SHARE-ERIC. 2025b. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 5-9. Linkage Data. Release version: 1. Internal data set. SHARE-ERIC, Munich.
- Walzenbach, Sandra, Jonathan Burton, Mick P. Couper, Thomas F. Crossley, and Annette Jäckle. 2023, 6. Experiments on multiple requests for consent to data linkage in surveys. Journal of Survey Statistics and Methodology 11, 518–540. [CrossRef]
Figure 1.
Real-life consent rates in SHARE countries. Consent request policies fell into three categories: (A) re-asking all participants in at least one wave (Belgium, Denmark, Estonia, Finland, Luxembourg), (B) re-asking only non-consenters (Germany), and (C) never re-asking (Austria, Girona, Italy, Netherlands). Consent rates are presented neutral to the year in which consent was obtained or the type of Institution (e.g. health, financial, employment).
Figure 1.
Real-life consent rates in SHARE countries. Consent request policies fell into three categories: (A) re-asking all participants in at least one wave (Belgium, Denmark, Estonia, Finland, Luxembourg), (B) re-asking only non-consenters (Germany), and (C) never re-asking (Austria, Girona, Italy, Netherlands). Consent rates are presented neutral to the year in which consent was obtained or the type of Institution (e.g. health, financial, employment).
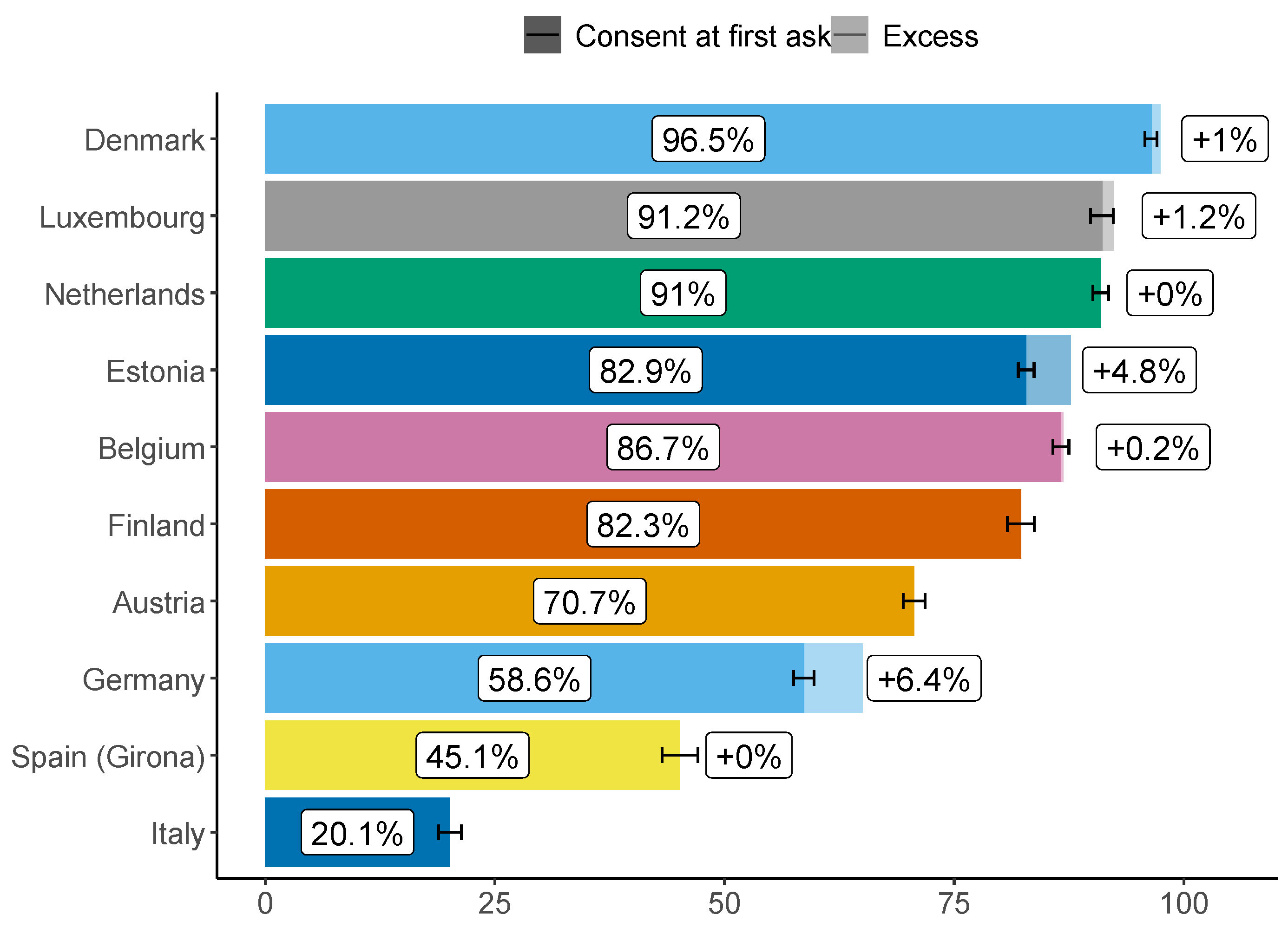
Figure 2.
Mapped consent rates to hypothetical linkage across 27 European countries and Israel (averaged across the four data domains). Apart from in the Nordic countries, there is limited spatial patterning to consent behaviour.
Figure 2.
Mapped consent rates to hypothetical linkage across 27 European countries and Israel (averaged across the four data domains). Apart from in the Nordic countries, there is limited spatial patterning to consent behaviour.
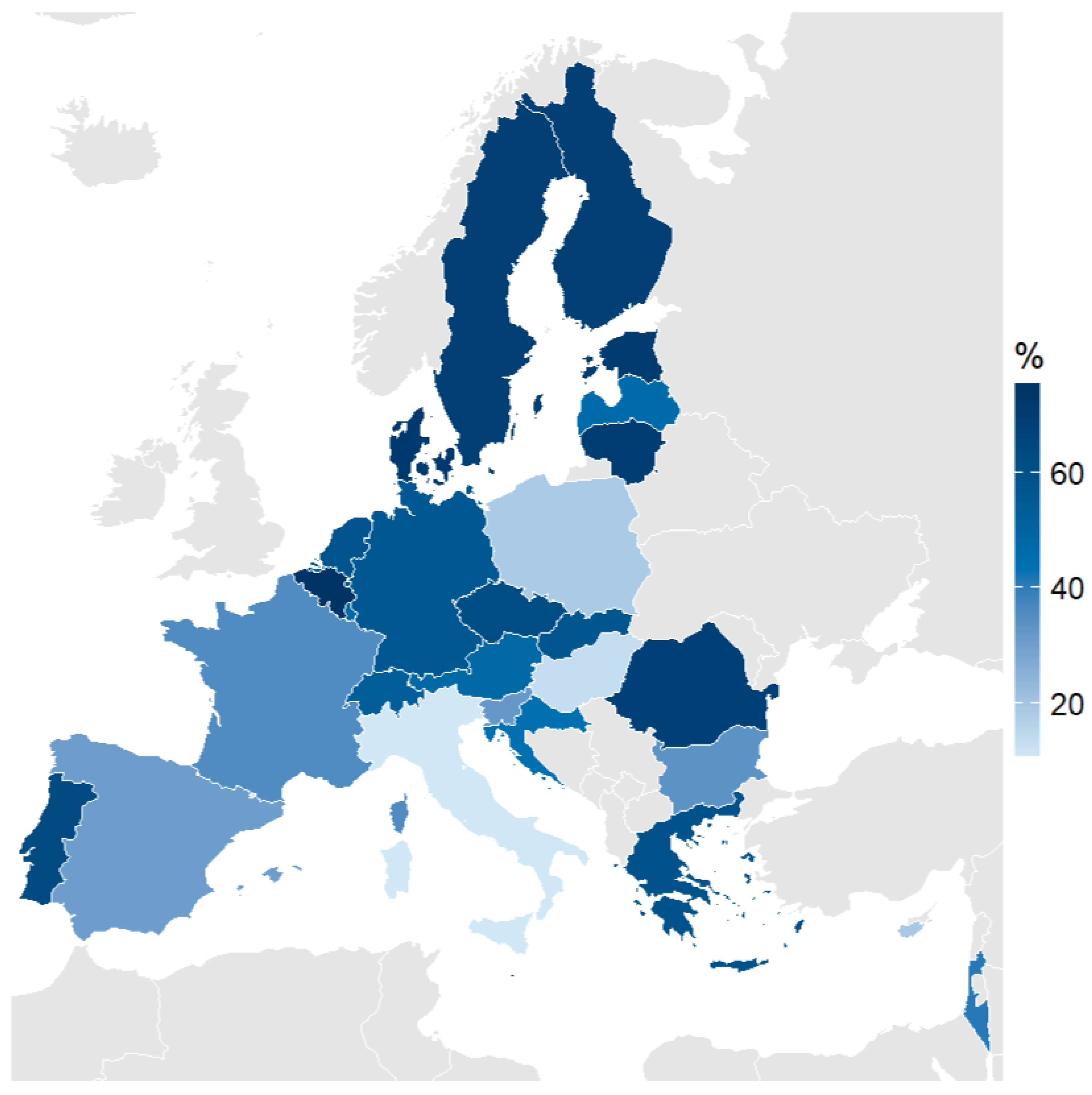
Figure 3.
Consent rate for each domain, by country. A larger gap between lines for a country indicates a greater effect of data domain on consent likelihood. The figure shows that the ranking of consent likelihood across domains was not uniform internationally. Linkage to income and tax information was almost universally least popular.
Figure 3.
Consent rate for each domain, by country. A larger gap between lines for a country indicates a greater effect of data domain on consent likelihood. The figure shows that the ranking of consent likelihood across domains was not uniform internationally. Linkage to income and tax information was almost universally least popular.
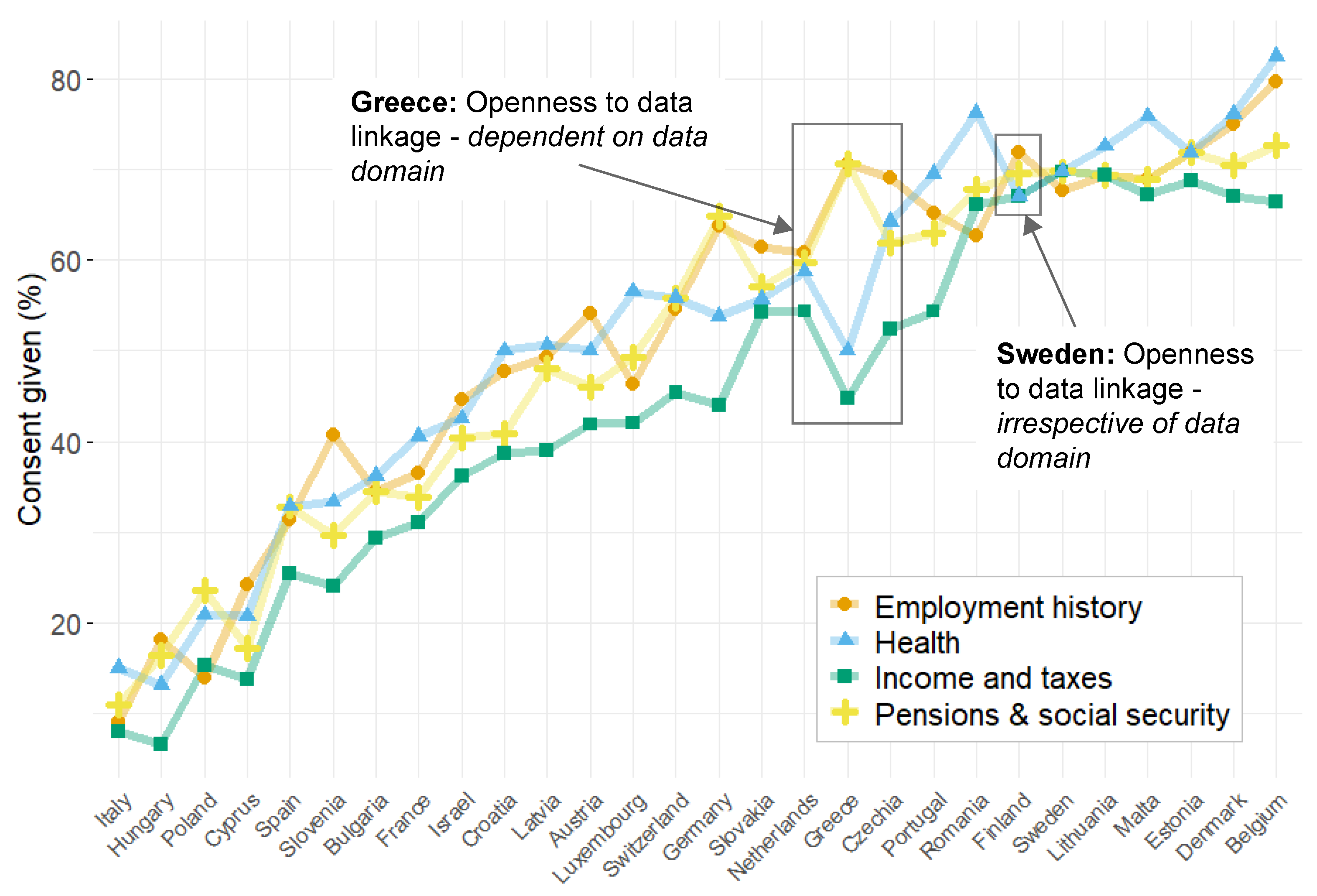
Figure 4.
Within-country, between-language variability. Bars shown with Wilson’s confidence intervals.
Figure 4.
Within-country, between-language variability. Bars shown with Wilson’s confidence intervals.
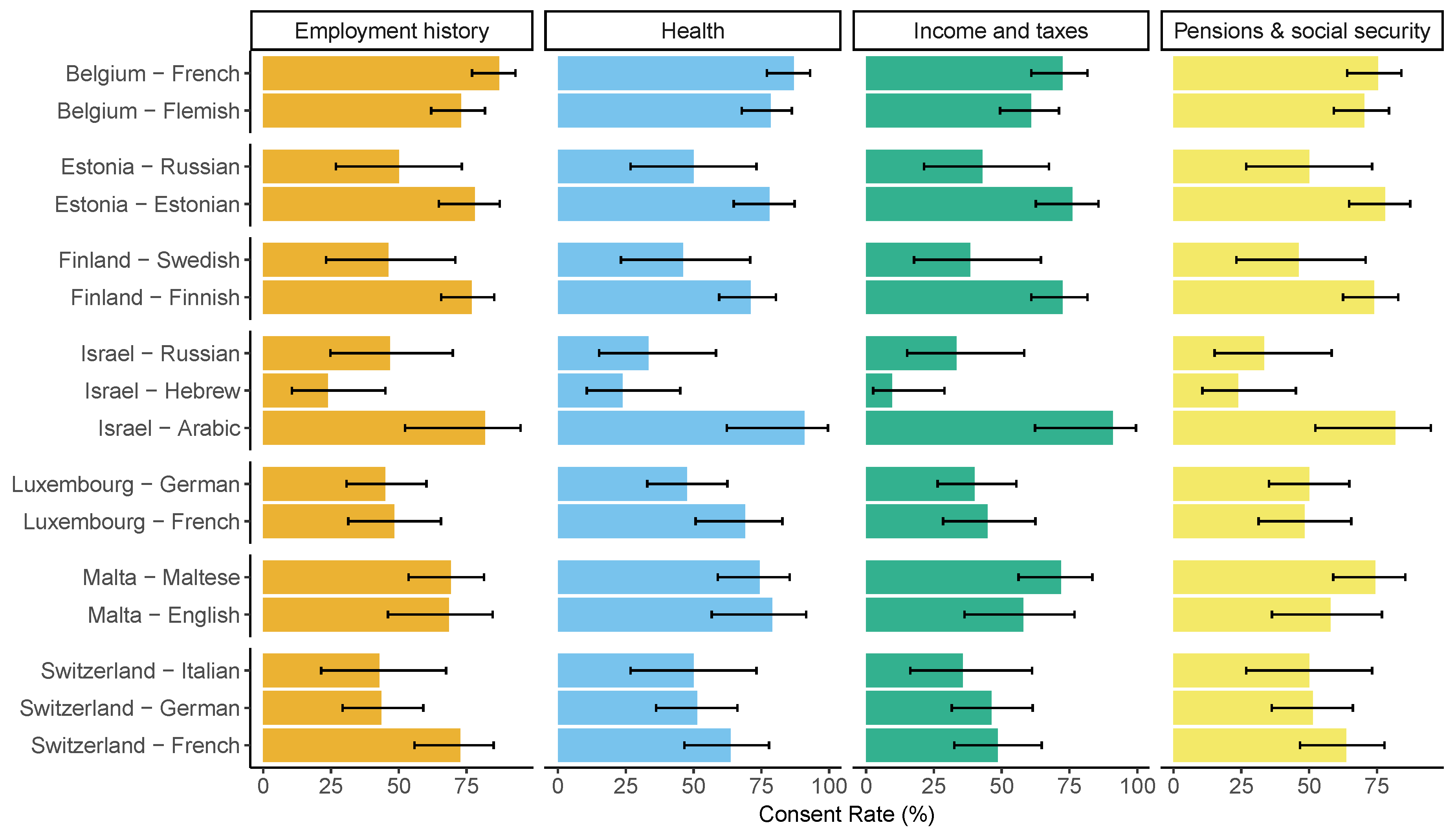
Figure 5.
Comparison of real-life consent rates versus hypothetical consent rates across various European countries. The blue line indicates the best-fit regression line, and the dashed line represents a 1:1 relationship between hypothetical and real-life consent rates.
Figure 5.
Comparison of real-life consent rates versus hypothetical consent rates across various European countries. The blue line indicates the best-fit regression line, and the dashed line represents a 1:1 relationship between hypothetical and real-life consent rates.
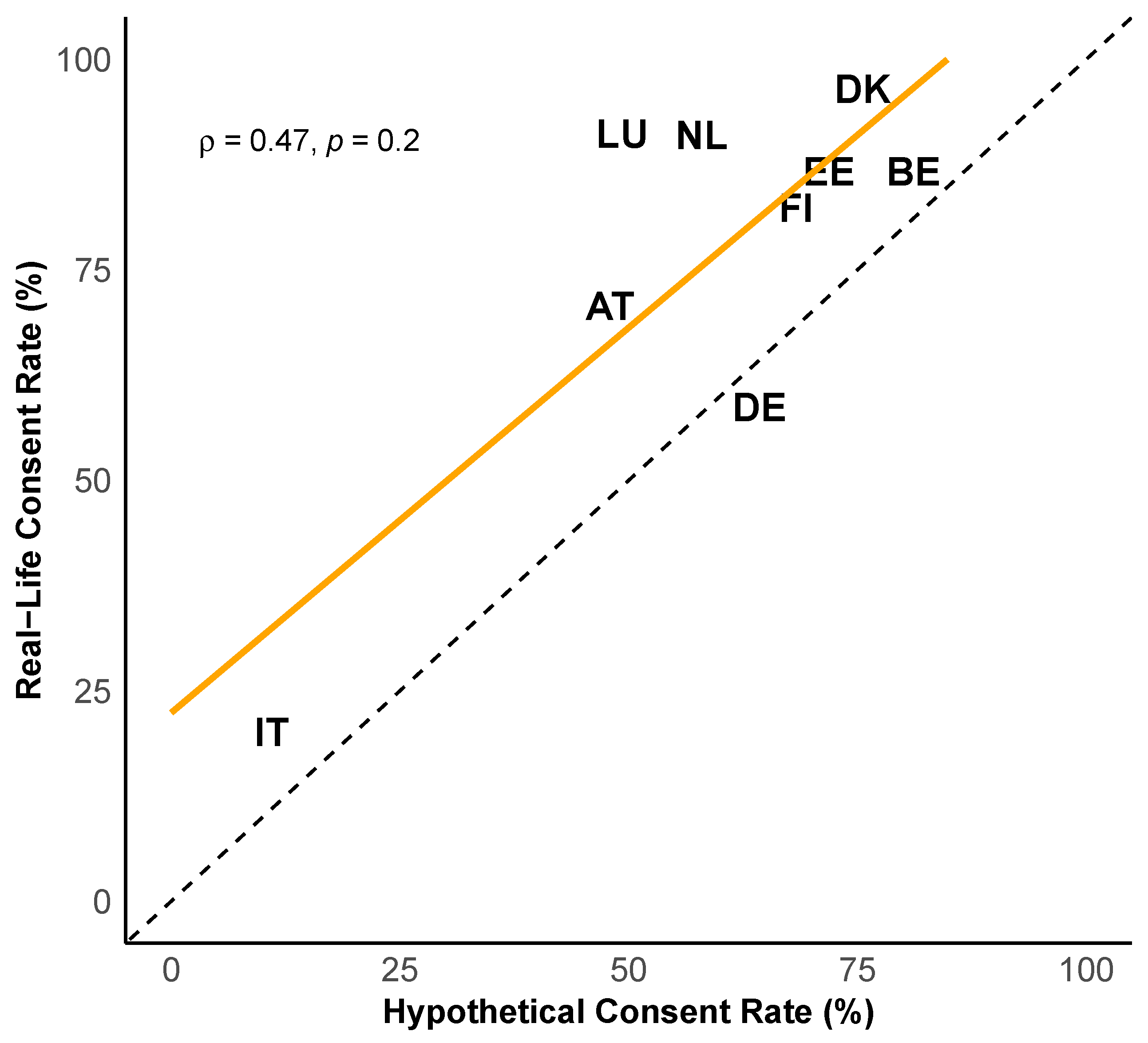
Table 1.
Descriptive statistics for countries with real-life data linkages.
| Age Category | Education Level | Minority | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | N | Female | 50–65 | 66–80 | 81+ | Low | Medium | High | Missing | Language | Consent |
| Austria | 5608 | 56.3% | 52.5% | 37.7% | 9.8% | 22.1% | 50.5% | 26.5% | 0.9% | 0.0% | 70.7% |
| Germany | 7302 | 51.5% | 59.5% | 33.1% | 7.3% | 11.5% | 56.4% | 32.0% | 0.2% | 0.0% | 58.7% |
| Netherlands | 4251 | 54.8% | 48.6% | 41.7% | 9.7% | 45.1% | 24.9% | 27.2% | 2.8% | 0.0% | 91.0% |
| Spain (Girona) | 4014 | 54.0% | 49.1% | 41.7% | 9.1% | 76.7% | 19.7% | 3.6% | 0.6% | 5.0% | 45.4% |
| Italy | 3923 | 56.1% | 52.0% | 43.9% | 4.0% | 66.7% | 23.8% | 9.4% | 0.2% | 0.0% | 20.1% |
| Denmark | 2941 | 53.8% | 44.2% | 44.6% | 11.3% | 14.8% | 37.5% | 47.5% | 0.2% | 0.0% | 96.5% |
| Belgium | 5923 | 55.2% | 50.3% | 36.8% | 12.8% | 34.0% | 28.3% | 37.0% | 0.7% | 0.0% | 86.3% |
| Luxembourg | 2024 | 53.3% | 59.5% | 31.9% | 8.6% | 45.7% | 34.7% | 19.6% | 0.0% | 0.0% | 91.2% |
| Estonia | 8396 | 59.4% | 51.3% | 38.0% | 10.7% | 24.6% | 52.2% | 23.2% | 0.1% | 18.9% | 82.7% |
| Finland | 2654 | 52.6% | 45.6% | 45.1% | 9.3% | 27.3% | 33.2% | 39.4% | 0.0% | 4.7% | 82.4% |
Table 2.
Multi-level regression model predicting real-life consenting behaviour, with country as a random effect.
Table 2.
Multi-level regression model predicting real-life consenting behaviour, with country as a random effect.
| Consent at first ask | ||
|---|---|---|
| Education level (Ref: Low) | ||
| High | 0. | (0.035) |
| Medium | 0. | (0.032) |
| Minority language speaker | 0. | (0.066) |
| Age group (Ref: 50 to 65) | ||
| 66 to 80 | 0. | (0.027) |
| 81+ | -0. | (0.041) |
| First consent (Ref: 2013) | ||
| 2015 | -0. | (0.087) |
| 2017 | -0.134 | (0.075) |
| 2019 | -0. | (0.048) |
| 2021 | -0. | (0.041) |
| Male gender | -0.004 | (0.025) |
| Constant | 1. | (0.406) |
| Observations | 44,174 | |
| Bayesian Inf. Crit. | 42,216.270 | |
*p<0.05; **p<0.01; ***p<0.001.
Table 3.
Summary of results from four multilevel logistic regression models predicting likelihood of consent for each data domain
Table 3.
Summary of results from four multilevel logistic regression models predicting likelihood of consent for each data domain
| Social security | Income | |||||||
|---|---|---|---|---|---|---|---|---|
| Health | Employment | and pensions | and taxes | |||||
| Consent | S.E. | S.E. | S.E. | S.E. | ||||
| Education level (Ref: Low) | ||||||||
| Medium | -0.077 | (0.156) | -0.120 | (0.158) | -0.081 | (0.156) | -0.200 | (0.156) |
| High | 0.175 | (0.162) | 0.272 | (0.164) | 0.180 | (0.161) | -0.011 | (0.161) |
| Minority Language Speaker | -0.126 | (0.275) | -0.289 | (0.274) | -0.402 | (0.271) | -0.316 | (0.272) |
| Age group (Ref: 50 to 65) | ||||||||
| 66 to 80 | -0.161 | (0.110) | -0.165 | (0.111) | -0.168 | (0.109) | -0.179 | (0.110) |
| 81+ | 0.044 | (0.223) | -0.145 | (0.221) | -0.004 | (0.220) | 0.185 | (0.220) |
| Male gender | 0. | (0.104) | 0. | (0.105) | 0. | (0.103) | 0. | (0.103) |
| sd(Country) | 0.873 | 0.945 | 0.898 | 0.928 | ||||
; Number of countries: 28; *p<0.05; **p<0.01; ***p<0.001
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



