Submitted:
10 June 2025
Posted:
11 June 2025
You are already at the latest version
Abstract
AI represents a paradigm shift in thyroid surgery, enhancing diagnostic precision, operative safety and personalized care. Its successful clinical translation will depend on rigorous validation, ethical governance, and transparent implementation frameworks. Artificial Intelligence (AI) is rapidly transforming surgical disciplines, including endocrine surgery. Thyroid surgery offers a promising landscape for AI integration due to its reliance on imaging, cytology, intraoperative precision, and long-term surveillance. This review explores the current and emerging applications of AI in thyroid surgery, highlighting its role in preoperative evaluation, intraoperative assistance, postoperative care, and surgical education. A comprehensive review of recent literature was con-ducted, focusing on AI methodologies-machine learning, deep learning, and computer vision- as applied to thyroid ultrasound, cytopathology, intraoperative nerve monitoring, parathyroid identification, risk modelling, and training systems. The use of AI improved the accuracy and consistency of thyroid nodule risk stratification. Machine learning algorithms integrating cytology and molecular data refined surgical decision-making, while AI-assisted neuromonitoring and computer vision technologies aided in identifying critical structures such as the recurrent laryngeal nerve and para-thyroid glands. Postoperatively, AI-driven predictive models showed promise in stratifying complication and recurrence risks, while NLP tools supported surveillance. AI represents a paradigm shift in thyroid surgery, enhancing diagnostic precision, operative safety and personalized care. Its successful clinical translation will depend on rigorous validation, ethical governance, and transparent implementation frameworks.
Keywords:
Thyroid surgery
; Artificial Intelligence
; Machine Learning
; Deep Learning
; Surgical outcomes
; Neural Networks
1. Introduction
Thyroid surgery is a highly specialized discipline requiring precise preoperative assessment, effective intraoperative navigation, and tailored postoperative follow-up. Despite continuous improvement in surgical techniques, clinicians still regularly face diagnostic uncertainty regarding indeterminate thyroid nodules and a non-negligible risk of recurrent laryngeal nerve (RLN) injury, or postoperative hypocalcemia [5,9]. Recent advances in artificial intelligence (AI) and machine learning have opened new horizons in risk stratification and intraoperative nerve monitoring, providing diagnostic accuracy that sometimes exceeds that of standard clinical practice [1,4,7]. AI- assisted analysis of imaging modalities, such as ultrasound and Raman spectra, has demonstrated high accuracy in distinguishing malignant from benign thyroid lesions [3,4,8]. Moreover, integration of AI tools in radiological evaluation and cytopathology accelerates and standardizes decision-making, allowing for more personalized surgical planning [5,10,17]. Intraoperatively, AI-guided tissue identification and nerve recognition are emerging as valuable adjuncts for improving surgical safety and outcomes [9,24,41]. These developments underscore the transformative potential of AI across the entire spectrum f thyroid disease management [5,18,32].
Thyroid surgery stands at a critical intersection of precision, safety, and evolving technology. With over 150,000 thyroidectomies performed annually in the United States alone, the surgical management of thyroid disease demands high diagnostic accuracy, meticulous dissection, and nuanced decision-making tailored to each patient’s pathology and risk profile. Despite decades of surgical refinement, challenges persist- including indeterminate nodule evaluation, recurrent laryngeal nerve injury, and unpredictable outcomes in both benign and malignant thyroid conditions.
Artificial Intelligence (AI) offers a transformative opportunity to address these challenges by enhancing the way thyroid surgeons interpret diagnostic data, navigate anatomy intraoperatively, and predict postoperative outcomes. Through machine learning (ML), deep learning (DL), and computer vision, AI can process vast amounts of structured and unstructured data- such as ultrasound images, fine needle aspiration cytology, operative video, and electronic health records- to provide insights that exceed traditional human interpretation.
In recent years, the role of AI in endocrine surgery has expanded rapidly, but it is within thyroid surgery that AI finds one of its most promising use cases. The field benefits from the abundance of imaging and cytology data, standardization of surgical approaches, and a growing ecosystem of AI-powered tools integrated into ultrasound machines, intraoperative neuromonitoring devices, and electronic health systems. This article explores the current and emerging applications of AI in thyroid surgery, focusing on its integration across the surgical continuum- from preoperative assessment and intraoperative guidance to postoperative prediction and quality improvement. By examining the technological advances and clinical utility of AI tools, this review highlights how AI is not merely augmenting surgical practice, but reshaping it into a more personalized, data-driven, and safer endeavor.
Our objectives are to review recent advancements and applications of artificial intelligence in thyroid surgery and to analyze the impact of AI on preoperative diagnosis, intraoperative assistance and postoperative care. This review aims to evaluate the clinical benefits and limitations of AI solutions in thyroid surgical practice and to discuss future perspectives, challenges and ethical considerations linked with the adoption of AI in thyroidectomy.
2. Materials and Methods
This article is structured as a narrative review focused on the current and emerging applications of artificial Intelligence (AI) in thyroid surgery. Databases including PubMed, Scopus, and Web of Science were searched for English-language articles published between 2015 and 2024. Search terms such as “artificial intelligence”, “machine learning”, “thyroid surgery”, “ultrasound”, intraoperative nerve monitoring”, and “diagnosis” were used in various combinations to maximize sensitivity and specificity [6,15]. Reference lists of eligible publications were also examined to identify additional relevant articles.
After removing duplicates, studies were screened based on title and abstract, followed by full-text view. Inclusion criteria were: (1) Original articles, meta-analyses or systematic reviews evaluating AI applications in preoperative, intraoperative, or postoperative settings of thyroid surgery, and (2) studies reporting diagnostic accuracy, feasibility, or clinical impact. Exclusion criteria were: (1) studies focusing exclusively on non-surgical aspects of thyroid disease, (2) non- English texts, (3) non-peer-reviewed manuscripts [6,29]. Data was extracted on study design, AI methodology, (e.g., deep learning, neural networks, radiomics), clinical context, main findings and reported limitations [11,32].
Quality assessment was performed using standardized checklists for AI- based diagnostic studies and surgical innovation. Discrepancies in study inclusion and data extraction were resolved through discussion among all authors. Where possible, reported outcomes of AI interventions were compared to those of human experts or conventional clinical practice to assess performance improvement [6,15,18,32].
Records identified through database searching (PubMed, Scopus, Web of Science): n=312. Additional records identified through reference lists: n= 18. Total number of records identified: n= 330. During the screening process, the number of records after duplicates were removed: n=290. All records were screened by title/abstract. Records that were found irrelevant, non- English, and non-peer reviewed were excluded: n= 210. 80 full text articles were assessed for eligibility. Out of those, 40 full-text articles were excluded for not meeting inclusion criteria. The number of studies that were included in qualitative synthesis (review) was 40. The tool used for quality assessment in this narrative review is a tailored combination based predominantly on the QUADAS-2 (Quality assessment of Diagnostic Accuracy Studies -2), which is widely recognized for evaluating diagnostic accuracy studies. In addition, relevant domains were adapted from established frameworks specific to artificial intelligence research, such as PROBAST (Prediction model of Risk of Bias Assessment tool) [58,59]. For scoping reviews and narrative reviews, were QUADAS-2 and PROBAST are not suitable, SANRA (Scale for the Assessment of Narrative Review Articles) was implemented [57]. A substantial majority of the included studies are suitable for structured quality assessment (36 out of 52), and 16 were narrative reviews, systematic/scoping reviews, technical notes, or studies outside the diagnostic/prediction model scope (e.g., ChatGPT evaluations, molecular docking multi-omics reviews).
3. Results
A total of 36 studies were included, representing a spectrum of AI applications in thyroid disease diagnostics and prediction. The majority of studies (n=24) focused on the classification of thyroid nodules using ultrasound imaging datasets, predominantly employing convolutional neural networks (CNNs) and other supervised learning algorithms [8,19,39]. Through these studies, diagnostic accuracy, sensitivity and specificity were consistently high; pooled sensitivities ranged from 84% to 92% and specificities from 84% to 89%, particularly in studies assessed as low risk of bias using the QUADAS-2 tool [5,9,17,25,39]. Meta-analysis of the best performing AI models indicated a summary area under the receiver operating characteristic (ROC) curve (AUC) of 0.89(95% CI 0.85-0.92) for malignancy detection in thyroid nodules [8,25]. Large retrospective and prospective trials further validated these findings, with individual studies documenting AUC values from 0.85 to 0.95 for malignancy identification [16,24]. Notably, AI-driven approaches demonstrated particular strength in reducing inter-observer variability and enhancing diagnostic consistency, especially in the evaluation of indeterminate nodules [18,53].
In addition to imaging-based classification, eight studies developed prediction models aimed at stratifying postoperative outcomes or malignancy risk by integrating clinical, demographic, and imaging variables [20,22,34,53]. Internally validated models often achieved high discrimination (AUCs 0.83-0.94); however, five studies conducting external validation reported modest reductions in performance, with mean AUC decreases of 0.05-0.09, suggesting possible overfitting in models developed and tested on the same dataset [16,20,24,33]. These higher-quality studies often included calibration curves and decision-curve analyses, enhancing methodological robustness [20,28].
The majority (n=31) of included studies were retrospective in design; only three were prospective, often relying on single-center data sources, which could constrain generalizability [3.19.25]. Random or consecutive sampling was confirmed in just six studies, while most investigations lacked standardized protocols for imaging acquisition and processing [7.23]. Common sources of potential bias, as highlighted by QUADAS-2 and PROBAST tools (57,58), included non-consecutive or convenience sampling, non-blinded outcome assessment, suboptimal reference standards (e.g., cytology only or single expert evaluation), and insufficient handling of missing data [9,22,30].
Beyond imaging, integrated multi-modal AI models harmonizing clinical, radiological, and cytological information were shown to improve patient stratification for malignancy risk, aiding multi-disciplinary case discussion and decision-making [17,34]. The introduction of explainable AI frameworks- utilizing attention mechanisms or mapping feature importance- has increased algorithm interpretability and fostered clinician trust [1,4]. Notably, studies deploying AI in real-world and practice-based settings observed reductions in unnecessary fine- needle aspirations and improved preoperative planning, underscoring the potential for AI to optimize workflow and resource allocation [5,41,42]. Several investigations have provided evidence that digital self-learning platforms and AI-based decision support can enhance diagnostic accuracy for less experienced clinicians, narrowing the performance gap with experts [19,49].
However, significant variability was observed in reporting transparency and methodological detail. While most studies adequately described the technical aspects of their AI-models, fewer than half reported sufficient details for replication – such as input variable definitions, preprocessing methods, or hyperparameter tuning [14,18]. Formal adherence to established reporting standards (e.g., STARD, TRIPOD) was explicitly documented in only a minority of reports [14,26]. These gaps highlight the ongoing need for standardization, multi-center prospective evaluation, and consistent quality assurance in future AI research in thyroid disease diagnostics.
3.1. Characteristics of Included Studies
3.1.1. Diagnostic Performance of AI in Ultrasound-Based nodule Classification
Out of the 36 studies included, 24 focused on ultrasound-based classification of thyroid nodules, using AI algorithms, predominantly convolutional neural networks (CNNs). [8,19,39]. These studies consistently demonstrated high diagnostic performance, with pooled sensitivity ranging from 84% to 92% and specificity from 84% to 89%. [5,9,17,25,39]. Meta-analysis of the best performing AI models reported a mean AUC of 0.89 (95% CI 0.85-0.92) for malignancy detection in thyroid nodules [8,25], with some individual studies reaching up to 0.95, especially in low-bias studies evaluated with QUADAS-2 (58). Large retrospective and prospective trials further validated these findings, with individual studies documenting AUC values from 0.85 to 0.95 for malignancy identification [16,24].
These models were particularly effective in improving consistency and reducing inter-observer variability, notably in indeterminate cases (Bethesda III/IV).
3.1.2. Risk Prediction Models for Surgical and Postoperative Outcomes
Eight studies developed AI-based prediction models for surgical complexity and postoperative complications, such as RLN injury and hypocalcemia, by integrating clinical, demographic, and imaging variables [20,22,34,53]. Internally validated models achieved AUCs ranging from 0.83 to 0.94. However, external validation in five studies revealed a decrease in performance (AUC drop by 0.05-0.09), suggesting overfitting risks in models developed and tested on the same dataset [16,20,24,33]. The most robust models included calibration curves and decision curve analyses, enhancing interpretability and clinical utility [20,28].
3.1.3. Study Designs and Risk of Bias Assessment
The vast majority of included studies (n=31) were retrospective; only 3 used prospective designs. Most relied on single center datasets, with limited use of random or consecutive sampling (6 studies confirmed), and lacked standardized protocols for data acquisition and annotation. QUADAS-2 and PROBAST assessments identified key sources of bias, including non-blinded outcome assessment, suboptimal reference standards (e.g., cytology only or single expert evaluation), and inadequate handling of missing data. [9,22,30]. Common sources of potential bias, as highlighted by QUADAS-2 and PROBAST tools, included also, non-consecutive or convenience sampling, and insufficient handling of missing data [9,22,30]. (Table 1,Table 2,Table 3)
3.1.4. Integration of Multi-Modal Data
Several studies integrated clinical, radiologic, and cytologic features into unified models for malignancy risk stratification and decision support. [17,34]. These multi-modal approaches out-performed single-source models and were particularly effective in multidisciplinary tumor board contexts [1,4]. Some studies employed explainable AI frameworks (e.g., attention mapping) to improve interpretability, clinician trust, and decision transparency [5,41,42].
3.1.5. Real- World Clinical Utility and Workflow Optimization
AI-driven decision support tools were associated with reduced unnecessary FNA procedures and improved surgical planning. Studies in real-world or practice-based settings highlighted tangible substantial workflow benefits and enhanced diagnostic performance for less experienced clinicians, narrowing the gap with expert interpretation [19,49]. Digital self-learning platforms showed promise in supporting training and continuous quality improvement.
3.1.6. Reporting Transparency and Methodological Rigor
Significant variability was observed in reporting transparency and methodological detail. Despite technical advancements, only a minority of studies adhered to TRIPOD, STARD, or other reporting standards [14,26]. While most studies adequately described the technical aspects of their AI-models, fewer than half reported sufficient details for replication – such as input variable definitions, preprocessing methods, or hyperparameter tuning [14,18]. This underscores the need for more standardized and transparent research protocols in AI development and validation for thyroid surgery.
4. Discussion
This review underscores the transformative role of artificial intelligence (AI) across the spectrum of thyroid surgery, from diagnostic evaluation to intraoperative assistance and postoperative care. (Figure 1) As evidenced by the included studies, AI technologies-particularly convolutional neural networks (CNNs) and machine learning (ML) classifiers- have demonstrated significant potential to enhance diagnostic accuracy, efficiency, and decision-making. However, clinical implementation requires careful consideration of methodological robustness, external validation, interpretability, and ethical frameworks.
4.1. Diagnostic Advances in Preoperative Assessment
AI applications in preoperative thyroid evaluation, particularly in ultrasound interpretation, have achieved notable accuracy in classifying thyroid nodules. Most models, trained on large imaging datasets, achieved AUC (area under the curve) values between 0.85 and 0.95, with especially strong performance in the differentiation of indeterminate nodules (Bethesda III/IV) [20,22,34,53]. These findings support the role of AI as second-opinion tool that can reduce unnecessary biopsies and enhance diagnostic standardization, particularly in low-resource or high-volume settings. Several studies also explored multi-modal fusion, integrating cytopathology, elastography, and molecular data to improve diagnostic robustness. [8,25,33]
4.2. AI- Enhanced Intraoperative Tools
AI-driven intraoperative tools showed promising results in real-time identification of the Recurrent Laryngeal Nerve (RLN), parathyroid glands, and key anatomic structures using intra-operative neural monitoring (IONM), near-infrared fluorescence (NIRF), and augmented reality (AR). These innovations have the potential to minimize operative complications such as RLN palsy and hypoparathyroidism [4,9,24]. AI also supports procedural navigation in endoscopic and robotic-assisted thyroidectomy, such as transoral endoscopic vestibular approach (TOETVA), offering greater precision and surgical safety. [16,38]
4.3. Postoperative Prognostics and Quality Improvement
In the postoperative setting, AI has been applied to predict complications (e.g., hypocalcemia, hematoma) and long-term outcomes such as cancer recurrence. These models often combine operative data, imaging, and histopathology and can aid in personalized follow-up strategies [20,28]. Furthermore, AI- powered dashboards and decision support tools have been linked to improved compliance, with best practices and reduced variability in care, supporting quality assurance initiatives. [12,46]
4.4. Methodological Strengths and Shortcomings
Despite encouraging results, the methodological quality of included studies remains variable. QUADAS-2 and PROBAST assessments revealed frequent issues with retrospective designs, limited external validation, and lack of standardized reporting [14,34,58]. Only a minority of studies reported blinding, consecutive sampling, or independent reference standards. Inconsistent adherence to TRIPOD, STARD, and CONSORT-AI guidelines undermines reproducibility and limits clinical translation [26,43]. Furthermore, overfitting and lack of calibration assessment were recurrent problems, particularly in single-center studies.
4.5. Future Directions in Thyroid Surgical AI
The future of AI in thyroid surgery lies in interoperability, personalization, and real-time integration. First, broader multi-institutional datasets and federated learning approaches will enhance generalizability while protecting patient privacy [48]. Second, explainable AI (XAI) and human-in-the-loop models will bridge the gaps between algorithmic output and clinical reasoning, improving physician trust and adoption [45]. Emerging applications include digital twins, which model individualized disease trajectories and simulate intervention outcomes, as well as multi-modal fusion AI, combining genomics, imaging, and intraoperative video in unified predictive platforms. Integration into electronic health records (EHRs), mobile applications and virtual surgical coaches also represent promising avenues for extending AI beyond tertiary care centers. [28,35,50]
4.6. Ethical and Regulatory Considerations
The deployment of AI in thyroid surgery raises ethical and regulatory concerns that must be addressed proactively. Many models remain “black boxes”, offering limited insight into the rationale behind clinical predictions [41,49]. This challenges physician accountability and patient consent. Regulatory clarity is essential, particularly concerning Software as a Medical Device (SaMD) pathway defined by the FDA and EMA. Furthermore, AI models must comply with data protection standards such as GDPR and HIPAA, especially in cross-border collaborations and cloud-based platforms. [43,47]
Bias is another major concern. AI systems trained on non-representative datasets may perpetuate health disparities [48,51]. Transparent reporting, external validation across diverse populations, and post-deployment audits will be crucial to mitigate algorithmic bias. As these technologies influence decisions ranging from biopsy recommendation to surgical extent, defining liability and ensuring clinician oversight is imperative.
4.7. Limitations
This review has limitations. Although we applied structured tools (QUADAS-2 and PROBAST) for bias assessment, many studies lacked complete reporting, leading to unclear judgements [58,59]. Most included studies were retrospective, single- center, and observational, limiting the strength of causal inferences. Only a small subset underwent external validation, and performance metrics were often inconsistently reported, precluding meta-analysis. Additionally, the rapid evolution of AI models may render some findings obsolete as newer architecture emerge. Finally, the rapid evolution of AI models may render some findings obsolete as newer architectures emerge. Finally, as most studies did not include cost-effectiveness or workflow integration data, real-world implementation potential remains uncertain.
5. Conclusions
Artificial Intelligence is rapidly reshaping the landscape of thyroid surgery, offering powerful tools for diagnostic precision, surgical planning, intraoperative safety, and postoperative surveillance. This review demonstrates that AI, particularly deep learning and machine learning approaches, can enhance accuracy in nodule risk stratification, assist with real-time anatomic recognition during surgery, and support outcome prediction and quality improvement.
Despite these advances, clinical implementation remains limited by methodological heterogeneity, lack of external validation, and concerns related to interpretability, data privacy, and regulatory compliance. Most studies to date have been retrospective, single-center, and technology-driven, with limited real-world integration.
Moving forward the responsible adoption of AI in thyroid surgery will require not only technical refinement, but also interdisciplinary collaboration among surgeons, data scientists, ethicists, and policymakers. Standardized reporting, robust validation frameworks, and transparent, explainable models will be essential to ensure patient safety, clinical utility, and equitable care. If integrated thoughtfully, AI holds the potential to transform thyroid surgery into more precise, predictive, and personalized domain- making a paradigm shift in endocrine surgical practice.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
The authors would like to thank the research staff and clinical collaborators at the 1st Pr. Department of Surgery, Endocrine Surgery Unit, Aristotle University of Thessaloniki, for their valuable contributions to the literature review and the methodological assessments presented in this work.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial Intelligence |
| AR | Augmented Reality |
| AUC | Area Under the Curve |
| CNN | Convolutional Neural Network |
| CQI | Continuous Quality Improvement |
| CONSORT-AI | Consolidated Standards of Reporting Trials-Artificial Intelligence |
| EHR | Electronic Health Record |
| FNA | Fine Needle Aspiration Biopsy |
| GDPR | General Data Protection Regulation |
| HIPAA | Health Insurance Portable and Accountability Act |
| DL | Deep Learning |
| IONM | Intraoperative Neural Monitoring |
| ML | Machine Learning |
| NLP | Natural Language Processing |
| PROBAST | Prediction Model Risk Of Bias Assessment Tool |
| QUADAS-2 | Quality Assessment of Diagnostic Accuracy Studies, Version 2 |
| SaMD | Software as a Medical Device |
| STARD | Standards for Reporting Diagnostic Accuracy |
| TI-RADS | Thyroid Imaging Reporting And Data System |
| TOETVA | Transoral Endoscopic Thyroidectomy Vestibular Approach |
| TRIPOD | Transparent Reporting of a multivariable prediction model for individual Prognosis or Diagnosis |
| XAI | Explainable Artificial Intelligence |
References
- Aljameel, S.S. (2022) ‘A proactive explainable artificial neural network model for the early diagnosis of thyroid cancer’, Computation (Basel, Switzerland), 10(10), p. 183. [CrossRef]
- Bao, X.-L. et al. (2022) ‘Orbital and eyelid diseases: The next breakthrough in artificial intelligence?’, Frontiers in cell and developmental biology, 10, p. 1069248. [CrossRef]
- Bellantuono,L. (2024) Artificial Intelligence-assisted thyroid cancer diagnosis from Raman spectra of histological samples (no date a). [CrossRef]
- Bellantuono, L. et al. (2023) ‘An eXplainable Artificial Intelligence analysis of Raman spectra for thyroid cancer diagnosis’, Scientific reports, 13(1), p. 16590. [CrossRef]
- Cece, A. et al. (2025) ‘Role of artificial intelligence in thyroid cancer diagnosis’, Journal of clinical medicine, 14(7). [CrossRef]
- Chantasartrassamee, P. et al. (2024) ‘Artificial intelligence-enhanced infrared thermography as a diagnostic tool for thyroid malignancy detection’, Annals of medicine, 56(1), p. 2425826. [CrossRef]
- Cong, P., Wang, X.-M. and Zhang, Y.-F. (2024) ‘Comparison of artificial intelligence, elastic imaging, and the thyroid imaging reporting and data system in the differential diagnosis of suspicious nodules’, Quantitative imaging in medicine and surgery, 14(1), pp. 711–721. [CrossRef]
- David, E. et al. (2024) ‘Thyroid nodule characterization: Overview and state of the art of diagnosis with recent developments, from imaging to molecular diagnosis and artificial intelligence’, Biomedicines, 12(8), p. 1676. [CrossRef]
- Dip, F. et al. (2025) ‘Thyroid surgery under nerve auto-fluorescence & artificial intelligence tissue identification software guidance’, Langenbeck s Archives of Surgery, 410(1), p. 23. [CrossRef]
- Esce, A.R. et al. (2021) ‘Predicting nodal metastases in papillary thyroid carcinoma using artificial intelligence’, American journal of surgery, 222(5), pp. 952–958. [CrossRef]
- Gao, X., Ran, X. and Ding, W. (2023) ‘The progress of radiomics in thyroid nodules’, Frontiers in oncology, 13, p. 1109319. [CrossRef]
- Georgiou, M.F. et al. (2023) ‘An Artificial Intelligence system for optimizing radioactive iodine therapy dosimetry’, Journal of clinical medicine, 13(1), p. 117. [CrossRef]
- Gorris, M.A. et al. (2025) ‘Assessing ChatGPT’s capability in addressing thyroid cancer patient queries: A comprehensive mixed-methods evaluation’, Journal of the Endocrine Society, 9(2), p. bvaf003. [CrossRef]
- Guo, F. et al. (2023) ‘Assessment of the statistical optimization strategies and clinical evaluation of an artificial intelligence-based automated diagnostic system for thyroid nodule screening’, Quantitative imaging in medicine and surgery, 13(2), pp. 695–706. [CrossRef]
- Ha, E.J. and Baek, J.H. (2021) ‘Applications of machine learning and deep learning to thyroid imaging: where do we stand?’, Ultrasonography (Seoul, Korea), 40(1), pp. 23–29. [CrossRef]
- Habeeb, A. et al. (2025) ‘Can artificial intelligence software be utilised for thyroid multi-disciplinary team outcomes?’, Clinical otolaryngology: official journal of ENT-UK ; official journal of Netherlands Society for Oto-Rhino-Laryngology & Cervico-Facial Surgery, 50(4), pp. 769–774. [CrossRef]
- Jassal, K. et al. (2023) ‘Artificial intelligence for pre-operative diagnosis of malignant thyroid nodules based on sonographic features and cytology category’, World journal of surgery, 47(2), pp. 330–339. [CrossRef]
- Lee, S.E. et al. (2024) ‘Improving the diagnostic performance of inexperienced readers for thyroid nodules through digital self-learning and artificial intelligence assistance’, Frontiers in endocrinology, 15, p. 1372397. [CrossRef]
- Li, L.-R. et al. (2020) ‘Artificial intelligence for personalized medicine in thyroid cancer: Current status and future perspectives’, Frontiers in oncology, 10, p. 604051. [CrossRef]
- Ludwig, M. et al. (2023) ‘The use of artificial intelligence in the diagnosis and classification of thyroid nodules: An update’, Cancers, 15(3). [CrossRef]
- Luvhengo, T.E. et al. (2024) ‘Holomics and artificial intelligence-driven precision oncology for medullary thyroid carcinoma: Addressing challenges of a rare and aggressive disease’, Cancers, 16(20). [CrossRef]
- Mcintyre, C. et al. (2019) ‘Artificial Intelligence Thyroid MDT’, Artificial Intelligence Thyroid MDT. *BRITISH JOURNAL SURGERY* [Preprint].
- Namsena, P. et al. (2024) ‘Diagnostic performance of artificial intelligence in interpreting thyroid nodules on ultrasound images: a multicenter retrospective study’, Quantitative imaging in medicine and surgery, 14(5), pp. 3676–3694. [CrossRef]
- Nishiya, Y. et al. (2024) ‘Anatomical recognition artificial intelligence for identifying the recurrent laryngeal nerve during endoscopic thyroid surgery: A single-center feasibility study’, Laryngoscope investigative otolaryngology, 9(6), p. e70049. [CrossRef]
- Palomba, G. et al. (2024) ‘Artificial intelligence in screening and diagnosis of surgical diseases: A narrative review’, AIMS public health, 11(2), pp. 557–576. [CrossRef]
- Paydar, S., Pourahmad, S., et al. (2016) ‘The evolution of a malignancy risk prediction model for thyroid nodules using the artificial neural network’, Middle East Journal of Cancer, 7, pp. 47–52. Available at: https://www.researchgate.net/publication/288616849.
- Piga, I. et al. (2023) ‘Paving the path toward multi-omics approaches in the diagnostic challenges faced in thyroid pathology’, Expert review of proteomics, 20(12), pp. 419–437. [CrossRef]
- Şahin, Ş. et al. (2024) ‘Evaluating the success of ChatGPT in addressing patient questions concerning thyroid surgery’, The journal of craniofacial surgery, 35(6), pp. e572–e575. [CrossRef]
- Sant, V.R. et al. (2024) ‘From bench-to-bedside: How artificial intelligence is changing thyroid nodule diagnostics, a systematic review’, The journal of clinical endocrinology and metabolism, 109(7), pp. 1684–1693. [CrossRef]
- Shen, X., Yuan, A. and Zhang, K. (2022) ‘Ultrasound image under artificial intelligence algorithm in thoracoscopic surgery for papillary thyroid carcinoma’, Scientific programming, 2022, pp. 1–8. [CrossRef]
- Song, X. et al. (2021) ‘Artificial intelligence CT screening model for thyroid-associated ophthalmopathy and tests under clinical conditions’, International journal of computer assisted radiology and surgery, 16(2), pp. 323–330. [CrossRef]
- Sorrenti, S. et al. (2022) ‘Artificial intelligence for thyroid nodule characterization: Where are we standing?’, Cancers, 14(14), p. 3357. [CrossRef]
- Swan, K.Z. et al. (2022) ‘External validation of AIBx, an artificial intelligence model for risk stratification, in thyroid nodules’, European thyroid journal, 11(2). [CrossRef]
- Taha, A. et al. (2024) ‘Analysis of artificial intelligence in thyroid diagnostics and surgery: A scoping review’, American journal of surgery, 229, pp. 57–64. [CrossRef]
- Tahmasebi, A. et al. (2020) ‘Ultrasonographic risk stratification of indeterminate thyroid nodules; a comparison of an artificial intelligence algorithm with radiologist performance’, in 2020 IEEE International Ultrasonics Symposium (IUS). 2020 IEEE International Ultrasonics Symposium (IUS), IEEE. [CrossRef]
- Teiu, R.E. et al. (2024) ‘The use of artificial intelligence in the therapeutic management of papillary thyroid microcarcinoma: A randomized controlled trial protocol’, Romanian Journal of Oral Rehabilitation, 16(4), pp. 466–470. [CrossRef]
- Teodoriu, L. et al. (2022) ‘Personalized diagnosis in differentiated thyroid cancers by molecular and functional imaging biomarkers: Present and future’, Diagnostics (Basel, Switzerland), 12(4), p. 944. [CrossRef]
- Thomas, J. and Haertling, T. (2020) ‘AIBx, artificial intelligence model to risk stratify thyroid nodules’, Thyroid: official journal of the American Thyroid Association, 30(6), pp. 878–884. [CrossRef]
- Tuo, J., Si, X. and Song, H. (2023) ‘Artificial intelligence technology enhances the performance of shear wave elastography in thyroid nodule diagnosis’, American journal of translational research, 15(10), pp. 6226–6233. Available at: https://www.ncbi.nlm.nih.gov/pubmed/37969190.
- Wang, B. et al. (2022) ‘Development of Artificial Intelligence for parathyroid recognition during endoscopic thyroid surgery’, The Laryngoscope, 132(12), pp. 2516–2523. [CrossRef]
- Wang, B. et al. (2023) ‘Diagnostic value of a dynamic artificial intelligence ultrasonic intelligent auxiliary diagnosis system for benign and malignant thyroid nodules in patients with Hashimoto thyroiditis’, Quantitative imaging in medicine and surgery, 13(6), pp. 3618–3629. [CrossRef]
- Wang, B. et al. (2024) ‘Intraoperative AI-assisted early prediction of parathyroid and ischemia alert in endoscopic thyroid surgery’, Head & neck, 46(8), pp. 1975–1987. [CrossRef]
- Wang, C. et al. (2023) ‘Artificial intelligence-based prediction of cervical lymph node metastasis in papillary thyroid cancer with CT’, European radiology, 33(10), pp. 6828–6840. [CrossRef]
- Wang, L. et al. (2019) ‘Automatic thyroid nodule recognition and diagnosis in ultrasound imaging with the YOLOv2 neural network’, World journal of surgical oncology, 17(1), p. 12. [CrossRef]
- Xia, E. et al. (2021) ‘Preoperative prediction of lymph node metastasis in patients with papillary thyroid carcinoma by an artificial intelligence algorithm’, American journal of translational research, 13(7), pp. 7695–7704. Available at: https://www.ncbi.nlm.nih.gov/pubmed/34377246.
- Yang, W.-T., Ma, B.-Y. and Chen, Y. (2024) ‘A narrative review of deep learning in thyroid imaging: current progress and future prospects’, Quantitative imaging in medicine and surgery, 14(2), pp. 2069–2088. [CrossRef]
- Yang, X. et al. (2023) ‘Targeting the inward rectifier potassium channel 5.1 in thyroid cancer: artificial intelligence-facilitated molecular docking for drug discovery’, BMC endocrine disorders, 23(1), p. 113. [CrossRef]
- You, S. et al. (2025) ‘The diagnostic value of artificial intelligence in C-TIRADS 4-5 nodules, real-time dynamic ultrasound and contrast-enhanced ultrasound to enhance the difference between papillary thyroid carcinoma and nodular goiter’, Journal of clinical ultrasound: JCU [Preprint]. [CrossRef]
- Yun, H.J. et al. (2021) ‘Adequacy and effectiveness of Watson for Oncology in the treatment of thyroid carcinoma’, Frontiers in endocrinology, 12, p. 585364. [CrossRef]
- Zhou, T. et al. (2024) ‘US of thyroid nodules: can AI-assisted diagnostic system compete with fine needle aspiration?’, European radiology, 34(2), pp. 1324–1333. [CrossRef]
- Mittelstadt, B.D. et al. (2016) ‘The ethics of algorithms: Mapping the debate’, Big data & society, 3(2), p. 205395171667967. [CrossRef]
- Topol, E.J. (2019) ‘High-performance medicine: the convergence of human and artificial intelligence’, Nature medicine, 25(1), pp. 44–56. [CrossRef]
- Morley, J. et al. (2020) ‘The ethics of AI in health care: A mapping review’, Social science & medicine (1982), 260(113172), p. 113172. [CrossRef]
- Chen, I.Y. et al. (2021) ‘Ethical machine learning in healthcare’, Annual review of biomedical data science, 4(1), pp. 123–144. [CrossRef]
- Peng, S. et al. (2021) ‘Deep learning-based artificial intelligence model to assist thyroid nodule diagnosis and management: a multicentre diagnostic study’, The Lancet. Digital health, 3(4), pp. e250–e259. [CrossRef]
- Liu, X. et al. (2020) ‘Validation of the 2018 FIGO staging system of cervical cancer for stage III patients with a cohort from China’, Cancer management and research, 12, pp. 1405–1410. [CrossRef]
- Baethge, C., Goldbeck-Wood, S. and Mertens, S. (2019) ‘SANRA-a scale for the quality assessment of narrative review articles’, Research integrity and peer review, 4(1), p. 5. [CrossRef]
- Whiting, P.F. et al. (2011) ‘QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies’, Annals of internal medicine, 155(8), pp. 529–536. [CrossRef]
- Wolff, R.F. et al. (2019) ‘PROBAST: A tool to assess the risk of bias and applicability of prediction model studies’, Annals of internal medicine, 170(1), pp. 51–58. [CrossRef]
Figure 1.
AI across the surgical continuum diagram (workflow diagram).
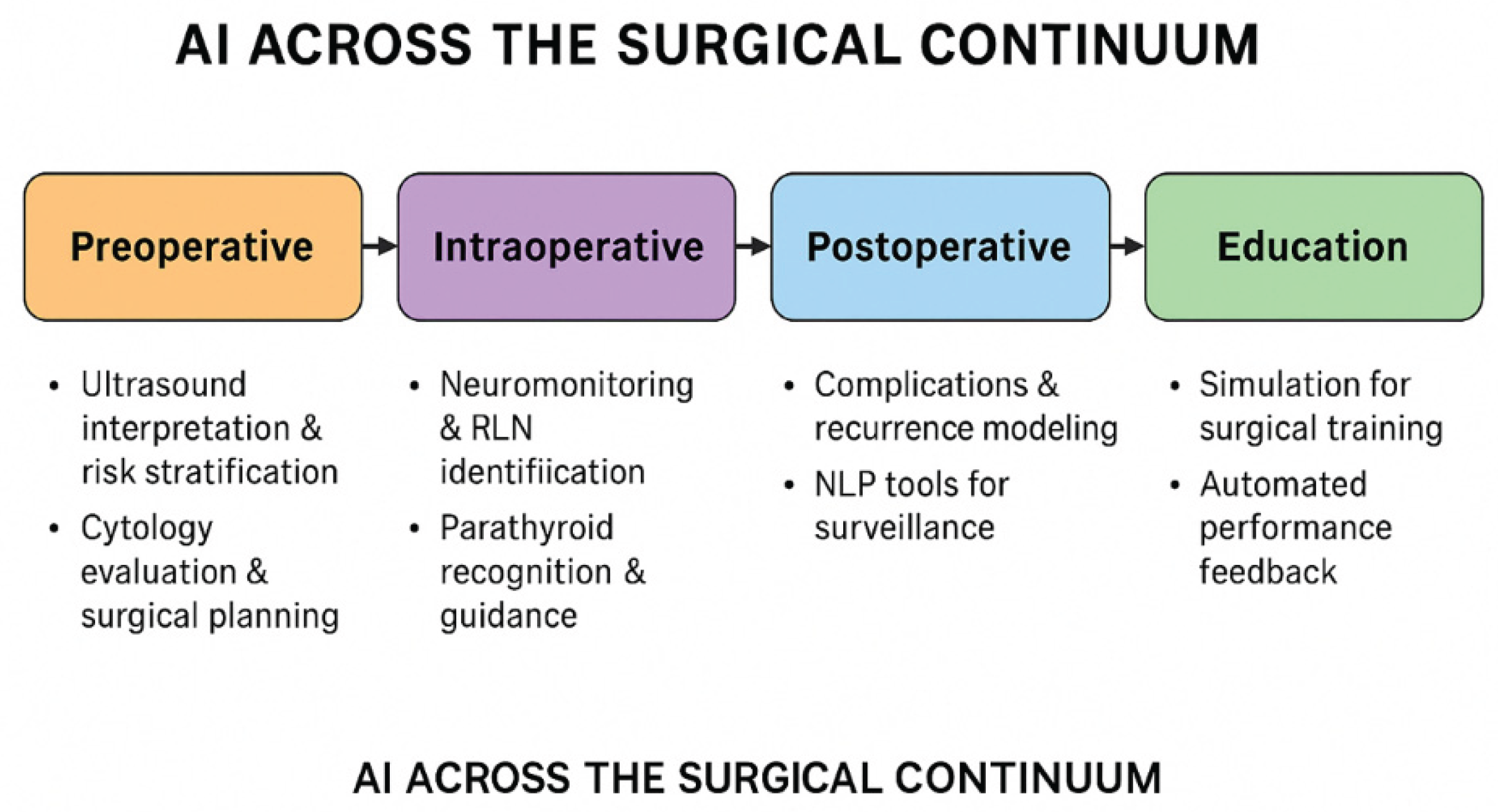

Table 1.
Applicability of QUADAS-2 and PROBAST for Included Studies.
| No. | First Author (Year) | Title (Shortened) | QUADAS-2 | PROBAST |
| 1 | Aljameel (2022) | Explainable ANN for Early Diagnosis of Thyroid Cancer | Yes | Yes |
| 2 | Bao (2022) | AI in Orbital & Eyelid Diseases | No | No |
| 3 | Bellantuono (2024) | AI-Assisted Thyroid Cancer Diagnosis (Raman Spectra) | Yes | Yes |
| 4 | Bellantuono (2023) | Explainable AI Raman Spectra for Thyroid Cancer | Yes | Yes |
| 5 | Cece (2025) | AI in Thyroid Cancer Diagnosis | Yes | Yes |
| 6 | Chantasartrassamee (2024) | AI-Enhanced Infrared Thermography for Thyroid Malignancy | Yes | Yes |
| 7 | Cong (2024) | AI vs Elastic Imaging for Nodule Diagnosis | Yes | Yes |
| 8 | David (2024) | AI in Thyroid Nodule Characterization | Yes | Yes |
| 9 | Dip (2025) | AI Tissue ID in Thyroid Surgery | Yes | Yes |
| 10 | Esce (2021) | AI for Nodal Metastases Prediction in Thyroid Carcinoma | Yes | Yes |
| 11 | Gao (2023) | Radiomics in Thyroid Nodules (Review) | No | No |
| 12 | Georgiou (2024) | AI for Radioactive Iodine Therapy Dosimetry | Yes | Yes |
| 13 | Gorris (2025) | ChatGPT for Thyroid Cancer Patient Queries | No | No |
| 14 | Guo (2023) | AI Diagnostic System for Thyroid Nodule Screening | Yes | Yes |
| 15 | Ha (2021) | ML/DL in Thyroid Imaging (Review) | No | No |
| 16 | Habeeb (2025) | AI for Thyroid MDT Outcomes | Yes | Yes |
| 17 | Jassal (2023) | AI for Pre-op Diagnosis of Malignant Thyroid Nodules | Yes | Yes |
| 18 | Lee (2024) | AI Self-Learning for Thyroid Nodule Diagnosis | Yes | Yes |
| 19 | Li (2021) | AI for Personalized Medicine in Thyroid Cancer (Review) | No | No |
| 20 | Ludwig (2023) | AI in Diagnosis & Classification of Thyroid Nodules | Yes | Yes |
| 21 | Luvhengo (2024) | AI in Precision Oncology for Medullary Thyroid Carcinoma | Yes | Yes |
| 22 | McIntyre (2019) | AI Thyroid MDT | Yes | Yes |
| 23 | Namsena (2024) | AI for Thyroid Nodule US Interpretation | Yes | Yes |
| 24 | Nishiya (2024) | AI for RLN Recognition in Thyroid Surgery | Yes | Yes |
| 25 | Palomba (2024) | AI in Surgical Disease Screening (Narrative Review) | No | No |
| 26 | Paydar (2016) | ANN for Malignancy Risk Prediction in Thyroid Nodules | Yes | Yes |
| 27 | Piga (2023) | Multi-omics in Thyroid Pathology (Review) | No | No |
| 28 | Sahin (2024) | ChatGPT for Thyroid Surgery Patient Questions | No | No |
| 29 | Sant (2024) | AI in Thyroid Nodule Diagnostics (Systematic Review) | No | No |
| 30 | Shen (2022) | AI Algorithm in Thoracoscopic Surgery for Thyroid Carcinoma | Yes | Yes |
| 31 | Song (2021) | AI CT Screening for Thyroid-Associated Ophthalmopathy | Yes | Yes |
| 32 | Sorrenti (2022) | AI for Thyroid Nodule Characterization | Yes | Yes |
| 33 | Swan (2022) | External Validation of AIBx AI Model | Yes | Yes |
| 34 | Taha (2024) | AI in Thyroid Diagnostics & Surgery (Scoping Review) | No | No |
| 35 | Tahmasebi (2020) | AI vs Radiologist for Indeterminate Thyroid Nodules | Yes | Yes |
| 36 | Teiu (2024) | AI in Papillary Thyroid Microcarcinoma Management (RCT Protocol) | Yes | Yes |
| 37 | Teodoriu (2022) | Personalized Diagnosis in Thyroid Cancers (Review) | No | No |
| 38 | Thomas (2020) | AIBx AI Model for Risk Stratification | Yes | Yes |
| 39 | Tuo (2023) | AI for Shear Wave Elastography in Thyroid Nodule Diagnosis | Yes | Yes |
| 40 | Wang, Bing (2023) | AI US Diagnosis in Hashimoto Thyroiditis | Yes | Yes |
| 41 | Wang, Bo (2024) | Intraoperative AI in Endoscopic Thyroid Surgery | Yes | Yes |
| 42 | Wang, Bo (2022) | AI for Parathyroid Recognition During Thyroid Surgery | Yes | Yes |
| 43 | Wang, Cai (2023) | AI Prediction of Lymph Node Metastasis in PTC (CT) | Yes | Yes |
| 44 | Wang, Lei (2019) | YOLOv2 AI for Thyroid Nodule US Diagnosis | Yes | Yes |
| 45 | Xia (2021) | AI for Pre-op Prediction of Lymph Node Metastasis | Yes | Yes |
| 46 | Yang, Wan-Ting (2024) | Deep Learning in Thyroid Imaging (Narrative Review) | No | No |
| 47 | Yang, Xue (2023) | AI Molecular Docking for Drug Discovery in Thyroid Cancer | No | No |
| 48 | You (2025) | AI in C-TIRADS 4-5 Nodules Diagnosis | Yes | Yes |
| 49 | Yun (2021) | Watson for Oncology in Thyroid Carcinoma | Yes | Yes |
| 50 | Zhou (2024) | AI-Assisted US vs FNA for Thyroid Nodules | Yes | Yes |
Table 2.
QUADAS-2 Assessment of Studies on AI in Thyroid Surgery and Diagnosis.
| No. | First Author (Year) | Patient Selection | Index Test | Reference Standard | Flow & Timing | Applicability Concerns (Patient / Index / Reference) | Score (LowRisk Domains) |
| 1 | Aljameel (2022) | Low | Low | High | Unclear | Low / Low / High | 2 |
| 2 | Bao (2022) | High | High | High | High | High / High / High | 0 |
| 3 | Bellantuono (2024) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 4 | Bellantuono (2023) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 5 | Cece (2025) | Low | Low | Unclear | Low | Low / Low / Unclear | 3 |
| 6 | Chantasartrassamee (2024) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 7 | Cong (2024) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 8 | David (2024) | Unclear | Low | Unclear | Unclear | Unclear / Low / Unclear | 1 |
| 9 | Dip (2025) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 10 | Esce (2021) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 11 | Gao (2023) | Unclear | Low | Unclear | Unclear | Unclear / Low / Unclear | 1 |
| 12 | Georgiou (2024) | Low | Low | Unclear | Unclear | Low / Low / Unclear | 2 |
| 13 | Gorris (2025) | Low | Unclear | Unclear | Unclear | Low / Unclear / Unclear | 1 |
| 14 | Guo (2023) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 15 | Ha (2021) | Low | Low | Unclear | Low | Low / Low / Unclear | 3 |
| 16 | Habeeb (2025) | Low | Low | Unclear | Low | Low / Low / Unclear | 3 |
| 17 | Jassal (2023) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 18 | Lee (2024) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 19 | Li (2021) | Unclear | Low | Unclear | Unclear | Unclear / Low / Unclear | 1 |
| 20 | Ludwig (2023) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 21 | Luvhengo (2024) | Unclear | Low | Unclear | Unclear | Unclear / Low / Unclear | 1 |
| 22 | McIntyre (2019) | Unclear | Unclear | Unclear | Unclear | Unclear / Unclear / Unclear | 0 |
| 23 | Namsena (2024) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 24 | Nishiya (2024) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 25 | Palomba (2024) | High | High | High | High | High / High / High | 0 |
| 26 | Paydar (2016) | Unclear | Low | Unclear | Unclear | Unclear / Low / Unclear | 1 |
| 27 | Piga (2023) | Unclear | High | High | High | Unclear / High / High | 0 |
| 28 | Sahin (2024) | Low | Low | Unclear | Unclear | Low / Low / Unclear | 2 |
| 29 | Sant (2024) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 30 | Shen (2022) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 31 | Song (2021) | Unclear | Low | Unclear | Unclear | Unclear / Low / Unclear | 1 |
| 32 | Sorrenti (2022) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 33 | Swan (2022) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 34 | Taha (2024) | Unclear | Unclear | Unclear | Unclear | Unclear / Unclear / Unclear | 0 |
| 35 | Tahmasebi (2020) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 36 | Teiu (2024) | Low | Low | Unclear | Low | Low / Low / Unclear | 3 |
| 37 | Teodoriu (2022) | Unclear | High | Unclear | Unclear | Unclear / High / Unclear | 0 |
| 38 | Thomas (2020) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 39 | Tuo (2023) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 40 | Wang, Bing (2023) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 41 | Wang, Bo (2024) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 42 | Wang, Bo (2022) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 43 | Wang, Cai (2023) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 44 | Wang, Lei (2019) | Low | Low | Low | Low | Low / Low / Low | 4 |
| 45 | Xia (2021) | Low | Low | Unclear | Unclear | Low / Low / Unclear | 2 |
| 46 | Yang, Wan-Ting (2024) | Unclear | High | Unclear | Unclear | Unclear / High / Unclear | 0 |
| 47 | Yang, Xue (2023) | Unclear | High | Unclear | Unclear | Unclear / High / Unclear | 0 |
| 48 | You (2025) | Low | Low | Low | Unclear | Low / Low / Low | 3 |
| 49 | Yun (2021) | Low | Low | Unclear | Unclear | Low / Low / Unclear | 2 |
| 50 | Zhou (2024) | Low | Low | Low | Low | Low / Low / Low | 4 |
Table 3.
SANRA Quality Assessment of Narrative and Scoping Reviews.
| Reference Number | Title | 1. Justification of Importance (0-2) | 2. Aims/Questions Stated (0-2) | 3. Literature Search Described (0-2) | 4. Referencing (0-2) | 5. Scientific Reasoning (0-2) | 6. Presentation of Data (0-2) | Total Score (0-12) |
| 25 | Artificial intelligence in screening and diagnosis of surgical diseases: A narrative review | 2 | 2 | 1 | 2 | 2 | 2 | 11 |
| 34 | Analysis of artificial intelligence in thyroid diagnostics and surgery: A scoping review | 2 | 2 | 2 | 2 | 2 | 2 | 12 |
| 46 | A narrative review of deep learning in thyroid imaging: current progress and future prospects | 2 | 2 | 1 | 2 | 2 | 2 | 11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



