Submitted:
28 May 2025
Posted:
29 May 2025
Read the latest preprint version here
Abstract
Objectives: This prospective case-control study aimed to compare the outcomes of aortic valve replacement using a Perceval sutureless bioprosthesis versus a conventional stented bioprosthesis in patients with hemodynamically significant aortic stenosis. Methods: A total of 233 elective patients who underwent aortic valve replacement at the University Clinical Center of Serbia between July 2017 and March 2021 were included in this study. Based on predefined criteria, 74 patients received a Perceval sutureless valve and 159 received a conventional stented valve. Results: The baseline characteristics were similar between the groups, with most patients being male (54.1% vs. 56.6%) and a mean age of approximately 72.6 years. Combined aortic valve replacement and coronary artery bypass grafting were performed in 19.3% of the patients. In the sutureless group, the most common valve size was 23–25 mm (41.8%). The mean aortic cross-clamp time was significantly shorter in the Perceval group (92.1 ± 29.3 min) than in the conventional group (104.5 ± 29.6 minutes, p < 0.05). Thirty-day mortality was comparable between the groups (5.9% vs. 6.3%). At 36 months, the survival rate was significantly higher in the Perceval group (88.3% vs. 76.8%, p = 0.048). Conclusions: Perceval sutureless bioprostheses appear to be a safe and effective option, particularly for elderly high-risk patients, although their long-term durability remains to be confirmed.
Keywords:
Aortic valve stenosis
; Surgery
; Aortic valve replacement
; Heart valve prosthesis
; Bioprosthesis
; Sutureless bioprosthesis
; Perceval valve
; Conventional stented valve
; Survival Rate
; Prospective Case-Control Study
1. Introduction
In developed countries, aortic valve stenosis (AS) is the most prevalent valvular heart disease [1]. Patients with severe AS and decompensated heart failure may experience transient improvement with vasodilator therapy as a bridge to aortic valve replacement (AVR) [2,3]; however, there is no effective long-term medical therapy for AS.
Surgical AVR is the gold-standard treatment for severe symptomatic AS [4]. Surgery is also indicated in asymptomatic patients with severe AS if they have high-risk features, such as left ventricular ejection fraction (LVEF) < 50%, peak aortic jet velocity ≥ 4.0 m/s, mean pressure gradient ≥ 40 mmHg, severely calcified valve with reduced systolic opening, need for other cardiac surgeries, low predicted surgical risk, or significantly decreased exercise tolerance on stress testing [2].
AVR has been performed since the 1950s [5]. Over time, increasing patient age and comorbidities have prompted refinements in surgical techniques and valve design to reduce procedure-related complications. One key goal is to minimize the operative time, as prolonged cardiopulmonary bypass (CPB) and aortic cross-clamp durations are associated with higher morbidity and mortality [6,7].
As the population ages, the prevalence of degenerative AS that requires surgery continues to increase. However, advanced age and cumulative comorbidities place approximately 25% of patients in the high-risk category for conventional AVR with sutured prostheses (mechanical or stented biological valves). This is especially true in patients with heavily calcified or small aortic roots, impaired left ventricular function, or those requiring concomitant procedures.
Sutureless aortic bioprostheses have been developed to simplify technically difficult and time-consuming AVR procedures in high-risk patients with the aim of reducing operative times, morbidity, and mortality. These valves allow rapid deployment under direct vision and provide a larger effective orifice area for a given annulus size, combining the advantages of conventional surgical AVR (complete excision of the diseased valve under direct visualization) with those of transcatheter AVR (elimination of sutures and shorter implantation time) [8]. Sutureless AVR (SU-AVR) has demonstrated favorable early outcomes in high-risk and combined-procedure patients [8].
The Perceval sutureless aortic valve (Corcym, Italy) is a collapsible, self-expanding bioprosthesis implanted in more than 22,000 patients worldwide over the last decade [9]. In appropriately selected patients with severe AS (including those with combined stenosis and regurgitation or a failing aortic prosthesis), Perceval has proven to be a safe and effective alternative to standard AVR via either full sternotomy or minimally invasive approaches in appropriately selected patients with severe AS, including those with combined stenosis and regurgitation or a failing aortic prosthesis. The valve is constructed from bovine pericardium, with tissue treated with glutaraldehyde and homocysteic acid to mitigate calcification and fixed within an expandable nitinol stent frame that secures the bioprosthesis at the native annulus. Intra- and supra-annular sealing collars help minimize paravalvular leaks. Perceval is available in four sizes (small, medium, large, and extra-large) to accommodate annular diameters ranging from 19 mm to 27 mm.
2. Materials and Methods
Between July 2017 and March 2021, 512 patients underwent surgical AVR using bioprosthetic valves at our institution. After applying the study inclusion and exclusion criteria, 233 consecutive patients were identified for analysis, including 74 who received a Perceval sutureless valve (Group I) and 159 who received a conventional stented biological valve (Group II). This study was approved by the Ethics Committees of the UC Clinical Centre of Serbia (protocol code: 111/8, date of approval: April 6, 2021) and of the Medical Faculty, University of Belgrade (protocol code: 17/I-19, date of approval: January 12, 2023). Written informed consent was obtained from all the patients.
Inclusion criteria:
- Indication for elective AVR with a bioprosthesis (via full sternotomy, mini-sternotomy, or right anterior mini-thoracotomy)
- Age > 65 years
- Severe AS with New York Heart Association (NYHA) class ≥ II symptoms
- Critical aortic stenosis on preoperative echocardiography: aortic valve area ≤ 1.0 cm² (or indexed area < 0.6 cm²/m²), mean gradient > 40 mmHg, peak velocity > 4 m/s, or Doppler velocity index < 0.25
- Sinotubular junction to annulus diameter ratio < 1.3
- Aortic root dimensions suitable for a Perceval valve (annulus 19–27 mm)
- Signed informed consent.
Exclusion criteria:
- Indication for elective AVR with a bioprosthesis (via full sternotomy, mini-sternotomy, or right anterior mini-thoracotomy)
- Age > 65 years
- Severe AS with NYHA class ≥ II symptoms
- Critical aortic stenosis on preoperative echocardiography: aortic valve area ≤ 1.0 cm² (or indexed area < 0.6 cm²/m²), mean gradient > 40 mmHg, peak velocity > 4 m/s, or Doppler velocity index < 0.25
- Sinotubular junction to annulus diameter ratio < 1.3
- Aortic root dimensions suitable for a Perceval valve (annulus 19–27 mm)
- Signed informed consent.
The baseline preoperative characteristics (Table 1) were recorded, including the patients’ clinical profiles and standard laboratory values. All patients underwent preoperative transthoracic echocardiography (TTE), and intraoperative transesophageal echocardiography (TEE) was performed in each case. In patients who underwent minimally invasive approaches (39 patients for upper mini-sternotomy and six for right anterior mini-thoracotomy), a preoperative multi-detector computed tomography (MDCT) scan was performed to assess anatomical suitability (aortic root position, distance from the sternum, and aortic angulation).
2.1. Operative Technique
All surgeries were performed under general anesthesia with standard monitoring. In 188 cases (80.4%), full median sternotomy was the surgical approach, whereas the remaining patients underwent upper mini-sternotomy or right anterior mini-thoracotomy, as determined by MDCT screening. Standard cardiopulmonary bypass was established with central aortic and right atrial (or femoral) cannulation, and myocardial arrest was achieved using cold crystalloid St. Thomas Cardioplegia. A transverse aortotomy was performed approximately 5 mm above the sinotubular junction (near the Rindfleisch’s ridge) to excise the native aortic valve and thoroughly debride the annulus. Three guiding 4-0 polypropylene sutures were placed at the nadir of the aortic sinuses (120° apart) to aid prosthesis alignment. The appropriate Perceval valve size was selected using the manufacturer’s sizers, and the prosthesis was collapsed and mounted on a delivery holder (Figure 1).
A sutureless valve was implanted using three guiding sutures that were passed through the annular eyelets of the prosthesis to position it in the annulus. The inflow and outflow frames of the stent were released, allowing the valve to expand and sit in place. Proper positioning and seating were visually confirmed and the valves were secured. Post-implantation modeling was performed by inflating a balloon inside the valve into four atmospheres for two cycles of 30 s each, with warm saline infused into the aortic root during inflation. The guiding sutures were removed and the aortotomy was closed in a standard fashion (Figure 2). After weaning from CPB, TEE was repeated to verify the correct prosthesis position and check for any paravalvular leak.
Minimally invasive aortic valve replacement (MI-AVR) with a Perceval prosthesis (Figure 3), in selected cases, is usually performed via an upper mini-sternotomy or right anterior thoracotomy (5–7 cm incision).
Postoperative management was performed according to standard protocols. Patients were monitored in the intensive care unit and then in the surgical ward. Clinical and echocardiographic follow-up examinations were scheduled at hospital discharge and 1, 3, 12, 24, 36, 48, and 58 months after surgery. At each follow-up visit, TTE was performed to evaluate prosthetic valve function (peak and mean transvalvular gradients) and to detect any complications, such as paravalvular leak, valve migration, structural degeneration, or thrombosis. The mean follow-up duration was 42 months (range: 36–58 months), and 100% of the patients completed the scheduled follow-up.
2.2. Statistical Analysis
Data were analyzed using SPSS Statistics v22.0 (IBM Corp.). Continuous variables are presented as mean ± standard deviation, and categorical variables as absolute counts and percentages. Group comparisons were conducted using Student’s t-test for normally distributed continuous variables and Mann–Whitney U test or Kruskal–Wallis test for non-parametric variables, as appropriate. Survival was analyzed using the Kaplan–Meier method and compared between the groups using the log-rank test. A Cox proportional hazards regression model was used to evaluate the effects of the covariates on survival. Multivariate analysis was performed to identify independent predictors of survival in both groups.
3. Results
Preoperative patient characteristics (Table 1) shoes that groups were similar in age (72.6 ± 7.2 vs 72.7 ± 7.1 years, p > 0.05), sex distribution (54.1% vs 56.6% male, p > 0.05), and body mass index. The mean preoperative transvalvular gradient was 52 ± 17 mmHg in both groups. The aortic valve area was significantly smaller in the Perceval group (0.61 ± 0.15 cm²) than in the stented valve group (0.90 ± 0.24 cm², p < 0.05), reflecting more severe baseline stenosis in the sutureless cohort. The prevalence of most comorbid conditions was comparable between the groups, except for hypertension and dyslipidemia, which were more frequent in the Perceval group (94% vs. 76% for hypertension and 66% vs. 40% for dyslipidemia; both p < 0.05).
The intraoperative and early postoperative outcomes are shown in Table 2. In the Perceval group, most implanted valves were of size L (23–25 mm; 41.8%), followed by size M (26.9%), S (17.9%), and XL (13.4%). Among patients undergoing combined AVR + CABG, the CPB time was longer in the sutureless group (120.3 ± 38.2 min) than in the stented group (101.4 ± 36.5 min, p < 0.05), whereas for isolated AVR, the CPB times were similar between the groups. The aortic cross-clamp time for the combined procedures was significantly shorter in the Perceval group (92.1 ± 29.3 min vs 104.5 ± 29.6 min, p < 0.05). The surgical approach (full sternotomy vs. mini-sternotomy) did not significantly affect the CPB or cross-clamp times in either group. No significant intergroup differences were observed in postoperative complications (Table 2). Notably, the rates of stroke (0% in both groups) and permanent pacemaker implantation (5.4% vs. 3.1%, p > 0.05) were low and similar. Early postoperative blood loss, intensive care unit (ICU) stay, and total hospital length of stay were also comparable. Thirty-day (hospital) mortality rates were 5.9% (4 patients) in the sutureless group and 6.3% (10 patients) in the stented group (p > 0.05).
Late postoperative and mid-term follow-up findings are shown in Table 3. During a mean follow-up period of 42 months, there were no differences between the groups in NYHA functional class or prosthetic valve hemodynamics. Most surviving patients in both groups had NYHA class I or II at the last follow-up, with no significant intergroup differences (p > 0.05). Echocardiography at follow-up showed low transvalvular gradients in both groups (mean gradient: 9 ± 2 mmHg in the sutureless group vs. 10 ± 2.2 mmHg in the stented group, p > 0.05). The incidence of late complications was generally low. No stroke occurred in either group during follow-up. There were 0 cases of endocarditis in the Perceval group and three cases (1.9%) in the stented valve group (p > 0.05). The only significant difference was the higher rate of late thrombocytopenia in the Perceval group (20.3% vs. 10.7%, p < 0.05), although this did not translate to adverse clinical outcomes.
Kaplan–Meier survival analysis revealed a trend toward better mid-term survival in the sutureless group. At 36 months postoperatively, survival was 88.3% in the Perceval group and 76.8% in the Stented Valve group (log-rank p = 0.048; Table 4 and Figure 4). After 36 months, survival in the Perceval group remained at 88.3% at 58 months of follow-up, whereas no further follow-up data were available for the Stented group after 36 months. The overall 3-year survival rate of the entire cohort (both groups combined) was approximately 84%.
4. Discussion
For high-risk surgical patients, particularly those for whom prolonged operative times are expected, sutureless aortic valve implantation offers potential advantages. In our experience, the Perceval valve was beneficial in patients requiring complex or combined procedures (such as AVR with CABG) by simplifying implantation and potentially reducing cross-clamp time. Similarly, Shrestha et al. reported that SU-AVR is safe and effective in patients undergoing combined cardiac procedures [10]. The need for concomitant coronary revascularization in patients with AS has increased from approximately 5% to 25% over the last 20 years, underscoring the importance of techniques that streamline AVR.
Unlike conventional stented bioprostheses, the Perceval valve has no sewing ring, which allows for a larger effective orifice area for any given annulus size. This is especially beneficial for patients with small aortic roots who are at high risk of patient–prosthesis mismatch. In our study, although the Perceval group had smaller annuli on average (as evidenced by a lower preoperative valve area), the postoperative gradients were low and comparable to those in the stented valve group, suggesting that the sutureless valve provided excellent hemodynamics, even in small roots.
SU-AVR is also advantageous in minimally invasive surgeries, where a limited operative field can make suture placement and tying challenging. A sutureless prosthesis can be deployed more easily through a small incision, potentially expanding the applicability of less-invasive approaches. In our cohort, we found that using the Perceval valve in minimally invasive cases (upper mini-sternotomy or anterior thoracotomy) was feasible without prolonging the CPB or cross-clamp times.
Another important consideration is the operative time during combined and complex procedures. A prolonged CPB duration is known to increase morbidity, particularly in older patients and those with multiple comorbidities (reflected by high EuroSCORE-II and STS risk profiles). Utilizing a sutureless valve in such combined procedures can help reduce aortic cross-clamp and overall operative times. [11,12] In our study, the cross-clamp time was shorter with Perceval in the combined AVR+CABG cases, although the total CPB time was somewhat longer (likely due to other procedural factors). In the largest reported series of combined procedures to date, Shrestha et al. documented mean CPB and cross-clamp times of 79 ± 32 and 51 ± 23 min, respectively, using the Perceval valve in combined surgeries [10].
A potential drawback of Perceval prosthesis is its long-term durability. Englberger et al. reported the 5-year outcomes of an earlier-generation sutureless valve, suggesting that these prostheses may not be suitable for all patients who are candidates for bioprosthetic AVR [13]. Further research and longer follow-up periods are needed to determine the durability and performance of Perceval over time.
Limited data are available on the use of sutureless valves in patients with bicuspid aortic valves. Initially, bicuspid anatomy (especially Sievers type 0) was considered a contraindication for SU-AVR because of its elliptical annular shape. However, subsequent reports have described successful percutaneous implantations in patients with bicuspid AS without increased complication rates. For example, one series of 25 bicuspid patients reported no instances of paravalvular leakage, valve migration, or embolization during intraoperative TEE. In our cohort, only two patients (2.7%) had a bicuspid aortic valve (Sievers type 1), and both were treated successfully with Perceval, with no device-related issues [14].
We also compared our perioperative and early postoperative results with those of the other SU-AVR studies. The hospital- and 30-day mortality rates in our study were 5.9%, while the 1-year mortality rate was 8.4%, respectively. These results do not differ significantly from those reported by centers with similar experience [15,16,17,18].
The incidence of a significant paravalvular leak requiring reoperation in our series was 4.0%, which is slightly higher than that reported in most published reports on sutureless valves. Previous studies have reported rates of severe PVL of the order of 1–2% [19,20,21,22,23,24,25,26], although one multicenter study reported a rate of 4.6% [27]. Thus, the observed PVL rate was at the upper end of the published range, possibly reflecting a learning curve or a difference in patient anatomy.
Conduction disturbances leading to a complete heart block and permanent pacemaker implantation are known complications of surgical AVR [28]. In our study, 5.4% of the patients required a new pacemaker postoperatively, which is within the range reported in the literature for sutureless valves. Most series have reported pacemaker rates between 3% and 8% for the Perceval valve [15,29]. For example, Glauber et al. observed a 3.3% pacemaker rate in a prospective study of minimally invasive SU-AVR [30], while a recent meta-analysis reported an incidence of approximately 7.9%.[31] However, some studies have documented pacemaker rates as high as 10–15% and up to 23% in isolated cases. This variability is a concern, given the significant morbidity associated with pacemaker implantation. Previous analyses have identified factors such as older age, pre-existing conduction disturbances, thickened septum, bicuspid aortic valve, and concomitant mitral or tricuspid valve procedures as predictors of pacemaker requirement after AVR [32,33,34,35].
The main limitations of this study are its single-center design and relatively small sample size. In addition, the study was not randomized and lacked a contemporaneous control group aside from the comparison between the two bioprosthesis types. We have presented only early and mid-term outcomes; there remains a need to collect long-term data to fully evaluate the performance of the Perceval valve, which we plan to monitor over the next five years.
5. Conclusions
Our experience indicates that Perceval sutureless bioprostheses are safe and effective options for AVR in elderly patients with severe AS. SU-AVR can be performed with excellent results and may become the preferred surgical approach in high-risk patients, owing to the reduced operative time. Continuous follow-up and further studies are required to assess the long-term durability and outcomes of the bioprostheses.
Author Contributions
Conceptualization, D.M.L. and M.J.K.; methodology, D.M.L., G.M., F.V., M.K.K., M.G. and I.Đ.; validation, M.K., S.P. and D.C.; formal analysis, G.M.; investigation, D.M.L., G.M., F.V., M.K.K., M.G. and I.Đ; data curation, B.M.; writing—original draft preparation, D.M.L.; writing—review and editing, D.M.L., and M.J.K.; visualization, D.M.L.; supervision, M.J.K., S.P. and D.C. All authors have read and agreed to the published version of the manuscript.
Funding
This study did not receive external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committees of the UC Clinical Centre of Serbia (protocol code: 111/8, date of approval: April 6, 2021) and of the Medical Faculty, University of Belgrade (protocol code: 17/I-19, date of approval: January 12, 2023).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
Raw data supporting the conclusions of this study will be made available by the authors upon request.
Acknowledgments
We dedicate this work to our colleague and friend Filip Vučićević, whose intelligence, dedication, and kindness are deeply woven into this research and publication, as well as into our lives. He left us too soon but would remain with us forever.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACC | Aortic Cross-Clamp |
| AS | Aortic Stenosis |
| AVR | Aortic Valve Replacement |
| AVR + CABG | Aortic Valve Replacement plus Coronary Artery Bypass Grafting |
| BMI | Body Mass Index |
| BSA | Body Surface Area |
| CABG | Coronary Artery Bypass Grafting |
| CPB | Cardiopulmonary Bypass |
| CT or MDCT | (Multi-Detector) Computed Tomography |
| DVI | Doppler Velocity Index |
| EF / LVEF | Ejection Fraction / Left Ventricular Ejection Fraction |
| ICU | Intensive Care Unit |
| LVEF | Left Ventricular Ejection Fraction |
| NYHA | New York Heart Association |
| SD | Standard Deviation |
| STS | Society of Thoracic Surgeons |
| SU-AVR | Sutureless Aortic Valve Replacement |
| TEE | Transesophageal Echocardiography |
| TTE | Transthoracic Echocardiography |
| Vmax | Peak Aortic Jet Velocity |
| ACC | Aortic Cross-Clamp |
References
- Carabello, B.A.; Paulus, W.J. Aortic stenosis. Lancet 2009, 373, 956-966.
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., 3rd; Guyton, R.A.; O'Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014, 63, e57-185. [CrossRef]
- Khot, U.N.; Novaro, G.M.; Popović, Z.B.; Mills, R.M.; Thomas, J.D.; Tuzcu, E.M.; Hammer, D.; Nissen, S.E.; Francis, G.S. Nitroprusside in critically ill patients with left ventricular dysfunction and aortic stenosis. N Engl J Med 2003, 348, 1756-1763. [CrossRef]
- Vahanian, A.; Alfieri, O.; Andreotti, F.; Antunes, M.J.; Barón-Esquivias, G.; Baumgartner, H.; Borger, M.A.; Carrel, T.P.; De Bonis, M.; Evangelista, A.; et al. Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur J Cardiothorac Surg 2012, 42, S1-44. [CrossRef]
- Edwards, W.S.; Smith, L. Aortic valve replacement with a subcoronary ball valve. Surg Forum 1958, 9, 309-313.
- Berretta, P.; Andreas, M.; Meuris, B.; Langenaeken, T.; Solinas, M.; Concistrè, G.; Kappert, U.; Arzt, S.; Santarpino, G.; Nicoletti, A.; et al. Sutureless and rapid deployment versus sutured aortic valve replacement: a propensity-matched comparison from the Sutureless and Rapid Deployment International Registry. Eur J Cardiothorac Surg 2022, 62. [CrossRef]
- Sá, M.P.; Jabagi, H.; Dokollari, A.; Awad, A.K.; Van den Eynde, J.; Malin, J.H.; Sicouri, S.; Torregrossa, G.; Ruhparwar, A.; Weymann, A.; et al. Early and late outcomes of surgical aortic valve replacement with sutureless and rapid-deployment valves versus transcatheter aortic valve implantation: Meta-analysis with reconstructed time-to-event data of matched studies. Catheter Cardiovasc Interv 2022, 99, 1886-1896. [CrossRef]
- Powell, R.; Pelletier, M.P.; Chu, M.W.A.; Bouchard, D.; Melvin, K.N.; Adams, C. The Perceval Sutureless Aortic Valve: Review of Outcomes, Complications, and Future Direction. Innovations (Phila) 2017, 12, 155-173. [CrossRef]
- Phan, K.; Tsai, Y.C.; Niranjan, N.; Bouchard, D.; Carrel, T.P.; Dapunt, O.E.; Eichstaedt, H.C.; Fischlein, T.; Gersak, B.; Glauber, M.; et al. Sutureless aortic valve replacement: a systematic review and meta-analysis. Ann Cardiothorac Surg 2015, 4, 100-111. [CrossRef]
- Shrestha, M.; Folliguet, T.; Meuris, B.; Dibie, A.; Bara, C.; Herregods, M.C.; Khaladj, N.; Hagl, C.; Flameng, W.; Laborde, F.; et al. Sutureless Perceval S aortic valve replacement: a multicenter, prospective pilot trial. J Heart Valve Dis 2009, 18, 698-702.
- Müller, H.; Szalkiewicz, P.; Benedikt, P.; Ratschiller, T.; Schachner, B.; Schröckenstein, S.; Zierer, A. Single-center real-world data and technical considerations from 100 consecutive patients treated with the Perceval aortic bioprosthesis. Frontiers in Cardiovascular Medicine 2024, Volume 11 - 2024. [CrossRef]
- Lamberigts, M.; Szecel, D.; Rega, F.; Verbrugghe, P.; Dubois, C.; Meuris, B. Sutureless aortic valves in isolated and combined procedures: Thirteen years of experience in 784 patients. The Journal of Thoracic and Cardiovascular Surgery 2024, 167, 1724-1732.e1721. [CrossRef]
- Englberger, L.; Carrel, T.P.; Doss, M.; Sadowski, J.; Bartus, K.; Eckstein, F.F.; Asch, F.M.; Martens, S. Clinical performance of a sutureless aortic bioprosthesis: five-year results of the 3f Enable long-term follow-up study. J Thorac Cardiovasc Surg 2014, 148, 1681-1687. [CrossRef]
- Nguyen, A.; Fortin, W.; Mazine, A.; Bouchard, D.; Carrier, M.; El Hamamsy, I.; Lamarche, Y.; Demers, P. Sutureless aortic valve replacement in patients who have bicuspid aortic valve. The Journal of Thoracic and Cardiovascular Surgery 2015, 150, 851-857.
- Flameng, W.; Herregods, M.C.; Hermans, H.; Van der Mieren, G.; Vercalsteren, M.; Poortmans, G.; Van Hemelrijck, J.; Meuris, B. Effect of sutureless implantation of the Perceval S aortic valve bioprosthesis on intraoperative and early postoperative outcomes. J Thorac Cardiovasc Surg 2011, 142, 1453-1457. [CrossRef]
- Sian, K.; Li, S.; Selvakumar, D.; Mejia, R. Early results of the Sorin® Perceval S sutureless valve: systematic review and meta-analysis. Journal of Thoracic Disease 2017, 9, 711-724.
- Niinami, H.; Sawa, Y.; Shimokawa, T.; Domoto, S.; Nakamura, Y.; Sakaguchi, T.; Ito, T.; Toda, K.; Amano, A.; Gersak, B. 1-year outcomes of patients implanted with the Perceval sutureless valve: the Japanese post-marketing surveillance study. Heart Vessels 2023, 38, 949-956. [CrossRef]
- Schizas, N.; Samiotis, I.; Nazou, G.; Iliopoulos, D.C.; Anagnostopoulos, I.; Kousta, M.; Papaioannou, N.; Argiriou, M.; Dedeilias, P. Perceval-S over time. Clinical outcomes after ten years of usage. Journal of Cardiothoracic Surgery 2024, 19, 192. [CrossRef]
- Concistrè, G.; Santarpino, G.; Pfeiffer, S.; Farneti, P.; Miceli, A.; Chiaramonti, F.; Solinas, M.; Glauber, M.; Fischlein, T. Two alternative sutureless strategies for aortic valve replacement: a two-center experience. Innovations (Phila) 2013, 8, 253-257. [CrossRef]
- Martens, S.; Sadowski, J.; Eckstein, F.S.; Bartus, K.; Kapelak, B.; Sievers, H.H.; Schlensak, C.; Carrel, T. Clinical experience with the ATS 3f Enable® Sutureless Bioprosthesis. Eur J Cardiothorac Surg 2011, 40, 749-755. [CrossRef]
- Miceli, A.; Gilmanov, D.; Murzi, M.; Marchi, F.; Ferrarini, M.; Cerillo, A.G.; Quaini, E.; Solinas, M.; Berti, S.; Glauber, M. Minimally invasive aortic valve replacement with a sutureless valve through a right anterior mini-thoracotomy versus transcatheter aortic valve implantation in high-risk patients. Eur J Cardiothorac Surg 2016, 49, 960-965. [CrossRef]
- Shrestha, M.; Maeding, I.; Höffler, K.; Koigeldiyev, N.; Marsch, G.; Siemeni, T.; Fleissner, F.; Haverich, A. Aortic valve replacement in geriatric patients with small aortic roots: are sutureless valves the future? Interact Cardiovasc Thorac Surg 2013, 17, 778-782; discussion 782. [CrossRef]
- Cerillo, A.G.; Amoretti, F.; Mariani, M.; Cigala, E.; Murzi, M.; Gasbarri, T.; Solinas, M.; Chiappino, D. Increased Gradients After Aortic Valve Replacement With the Perceval Valve: The Role of Oversizing. Ann Thorac Surg 2018, 106, 121-128. [CrossRef]
- Laborde, F.; Fischlein, T.; Hakim-Meibodi, K.; Misfeld, M.; Carrel, T.; Zembala, M.; Madonna, F.; Meuris, B.; Haverich, A.; Shrestha, M. Clinical and haemodynamic outcomes in 658 patients receiving the Perceval sutureless aortic valve: early results from a prospective European multicentre study (the Cavalier Trial)†. Eur J Cardiothorac Surg 2016, 49, 978-986. [CrossRef]
- Erfe, J.M.; Malaisrie, S.C.; Andrei, A.C.; Pham, D.T.; Churyla, A.; Kruse, J.; Piotter, C.; Xu, Y.; McCarthy, P.M. Outcomes of Sutureless/Rapid Deployment Valves Compared to Traditional Bioprosthetic Aortic Valves. Ann Thorac Surg 2021, 111, 1884-1891. [CrossRef]
- Berretta, P.; Andreas, M.; Carrel, T.P.; Solinas, M.; Teoh, K.; Fischlein, T.; Santarpino, G.; Folliguet, T.; Villa, E.; Meuris, B.; et al. Minimally invasive aortic valve replacement with sutureless and rapid deployment valves: a report from an international registry (Sutureless and Rapid Deployment International Registry)†. Eur J Cardiothorac Surg 2019, 56, 793-799. [CrossRef]
- Folliguet, T.A.; Laborde, F.; Zannis, K.; Ghorayeb, G.; Haverich, A.; Shrestha, M. Sutureless perceval aortic valve replacement: results of two European centers. Ann Thorac Surg 2012, 93, 1483-1488. [CrossRef]
- Santarpino, G.; Pfeiffer, S.; Concistrè, G.; Fischlein, T. A supra-annular malposition of the Perceval S sutureless aortic valve: the 'χ-movement' removal technique and subsequent reimplantation. Interact Cardiovasc Thorac Surg 2012, 15, 280-281. [CrossRef]
- Gilmanov, D.; Miceli, A.; Ferrarini, M.; Farneti, P.; Murzi, M.; Solinas, M.; Glauber, M. Aortic valve replacement through right anterior minithoracotomy: can sutureless technology improve clinical outcomes? Ann Thorac Surg 2014, 98, 1585-1592. [CrossRef]
- Glauber, M.; Di Bacco, L.; Cuenca, J.; Di Bartolomeo, R.; Baghai, M.; Zakova, D.; Fischlein, T.; Troise, G.; Viganò, G.; Solinas, M. Minimally Invasive Aortic Valve Replacement with Sutureless Valves: Results From an International Prospective Registry. Innovations (Phila) 2020, 15, 120-130. [CrossRef]
- Moscarelli, M.; Santarpino, G.; Athanasiou, T.; Mastroroberto, P.; Fattouch, K.; Nasso, G.; Speziale, G. A pooled analysis of pacemaker implantation after Perceval sutureless aortic valve replacement. Interact Cardiovasc Thorac Surg 2021, 33, 501-509. [CrossRef]
- Fischlein, T.; Folliguet, T.; Meuris, B.; Shrestha, M.L.; Roselli, E.E.; McGlothlin, A.; Kappert, U.; Pfeiffer, S.; Corbi, P.; Lorusso, R. Sutureless versus conventional bioprostheses for aortic valve replacement in severe symptomatic aortic valve stenosis. J Thorac Cardiovasc Surg 2021, 161, 920-932. [CrossRef]
- Lorusso, R.; Folliguet, T.; Shrestha, M.; Meuris, B.; Kappetein, A.P.; Roselli, E.; Klersy, C.; Nozza, M.; Verhees, L.; Larracas, C.; et al. Sutureless versus Stented Bioprostheses for Aortic Valve Replacement: The Randomized PERSIST-AVR Study Design. Thorac Cardiovasc Surg 2020, 68, 114-123. [CrossRef]
- Szecel, D.; Eurlings, R.; Rega, F.; Verbrugghe, P.; Meuris, B. Perceval Sutureless Aortic Valve Implantation: Midterm Outcomes. Ann Thorac Surg 2021, 111, 1331-1337. [CrossRef]
- Sievers, H.H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J Thorac Cardiovasc Surg 2007, 133, 1226-1233. [CrossRef]
Figure 1.
Sterile preparation of the Perceval sutureless valve on the side table. (A) Valve unpacking; (B) collapsing the prosthesis onto the holder; (C) collapsed prosthesis mounted on the holder, ready for implantation; (D) key components of the Perceval device. (Source: Clinic for Cardiac Surgery, University Clinical Center of Serbia).
Figure 1.
Sterile preparation of the Perceval sutureless valve on the side table. (A) Valve unpacking; (B) collapsing the prosthesis onto the holder; (C) collapsed prosthesis mounted on the holder, ready for implantation; (D) key components of the Perceval device. (Source: Clinic for Cardiac Surgery, University Clinical Center of Serbia).
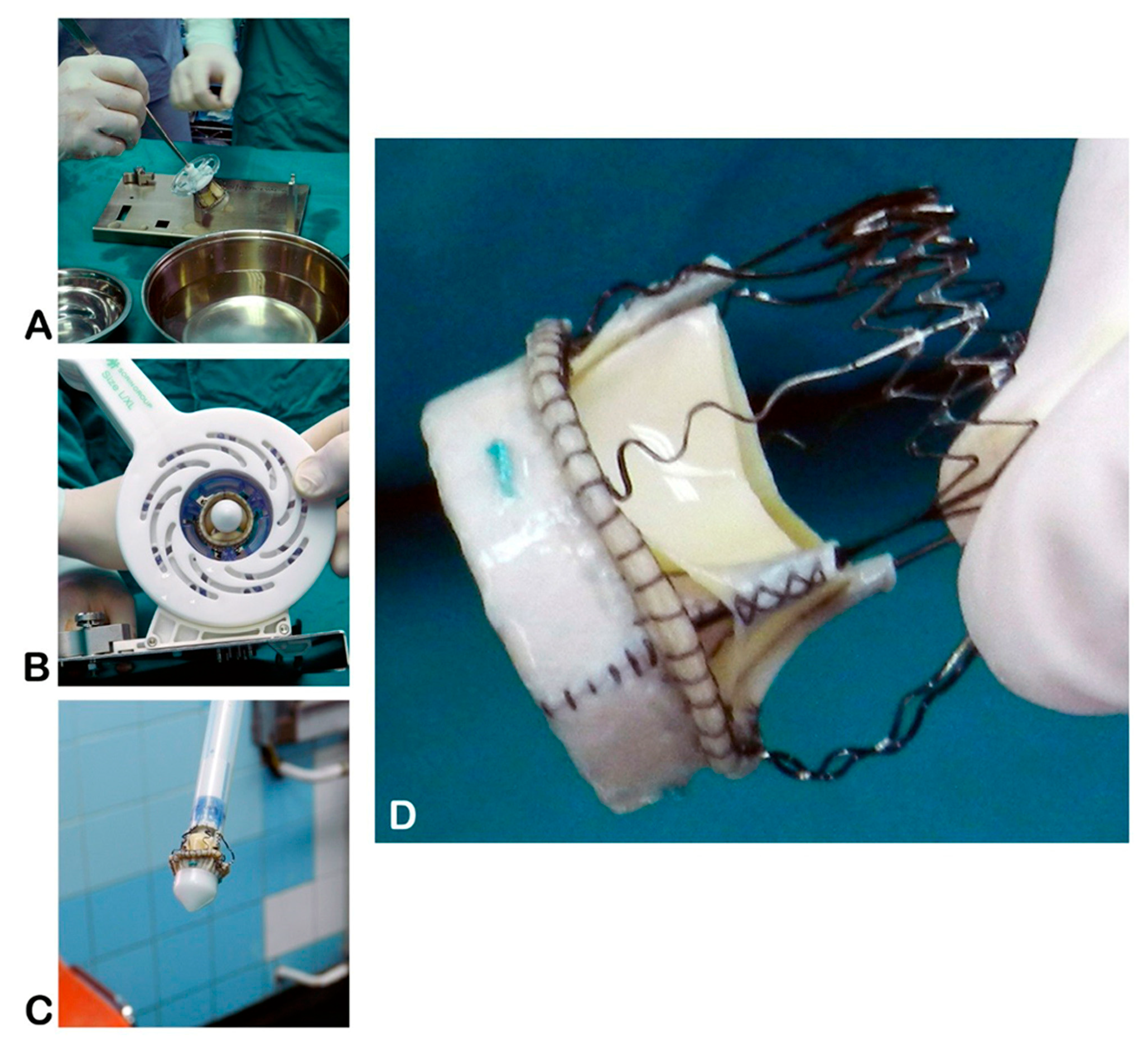
Figure 2.
Key steps of Perceval valve implantation. (A) Aortotomy, native valve excision, and placement of guiding sutures; (B) connecting the guiding sutures to the collapsed prosthesis; (C) positioning the prosthesis in the annulus; (D) expanded Perceval valve in situ; (E) closure of the aortotomy. (Source: Clinic for Cardiac Surgery, University Clinical Center of Serbia)
Figure 2.
Key steps of Perceval valve implantation. (A) Aortotomy, native valve excision, and placement of guiding sutures; (B) connecting the guiding sutures to the collapsed prosthesis; (C) positioning the prosthesis in the annulus; (D) expanded Perceval valve in situ; (E) closure of the aortotomy. (Source: Clinic for Cardiac Surgery, University Clinical Center of Serbia)
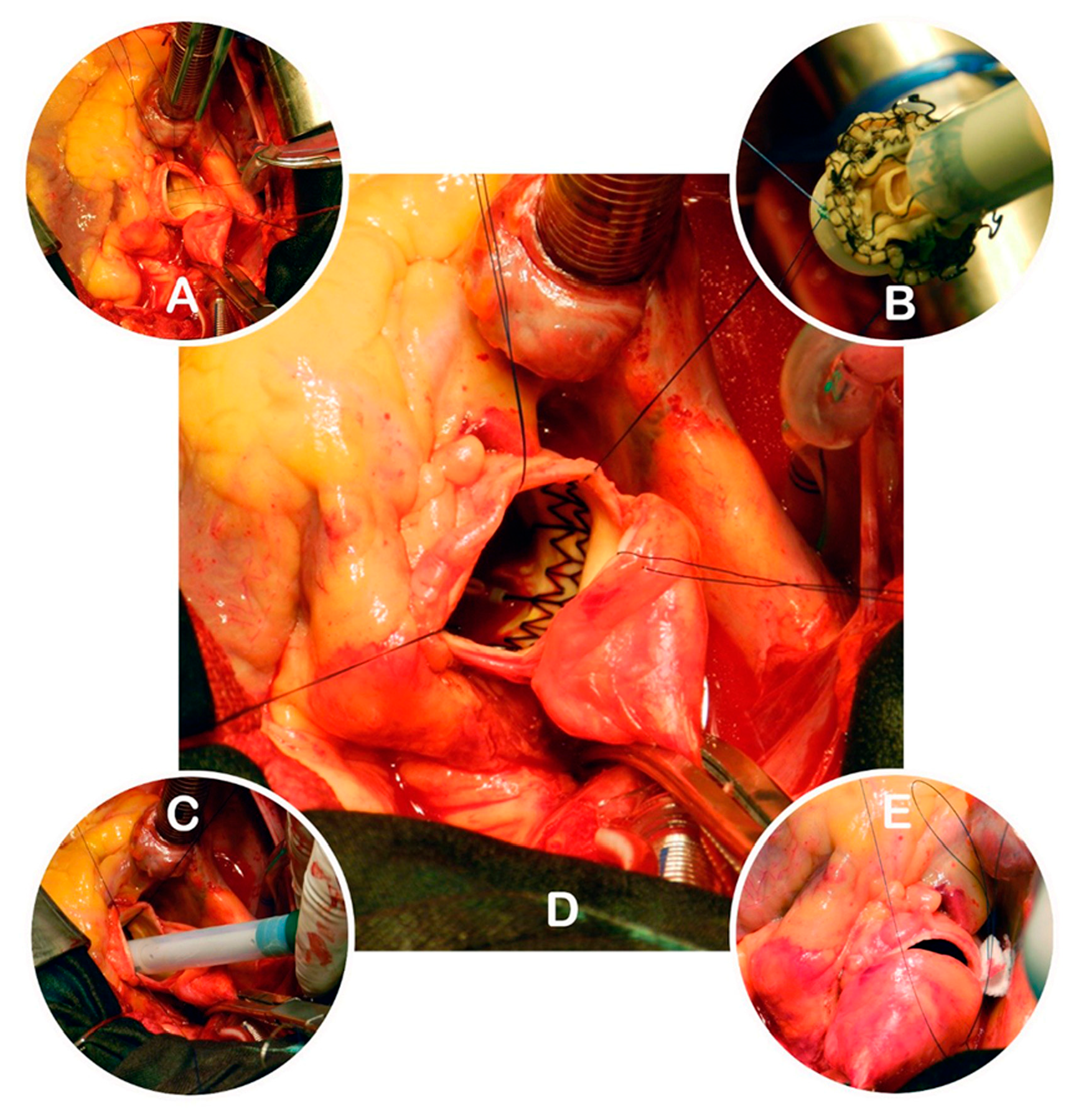
Figure 3.
Operative field view during MI-AVR: A- central cannulation ascending aorta, B- superior vena cava cannulation, C- conventional transverse aortotomy, D- balloon dilation Perceval valve (source: Clinic for Cardiac surgery, University Clinical Center of Serbia)
Figure 3.
Operative field view during MI-AVR: A- central cannulation ascending aorta, B- superior vena cava cannulation, C- conventional transverse aortotomy, D- balloon dilation Perceval valve (source: Clinic for Cardiac surgery, University Clinical Center of Serbia)
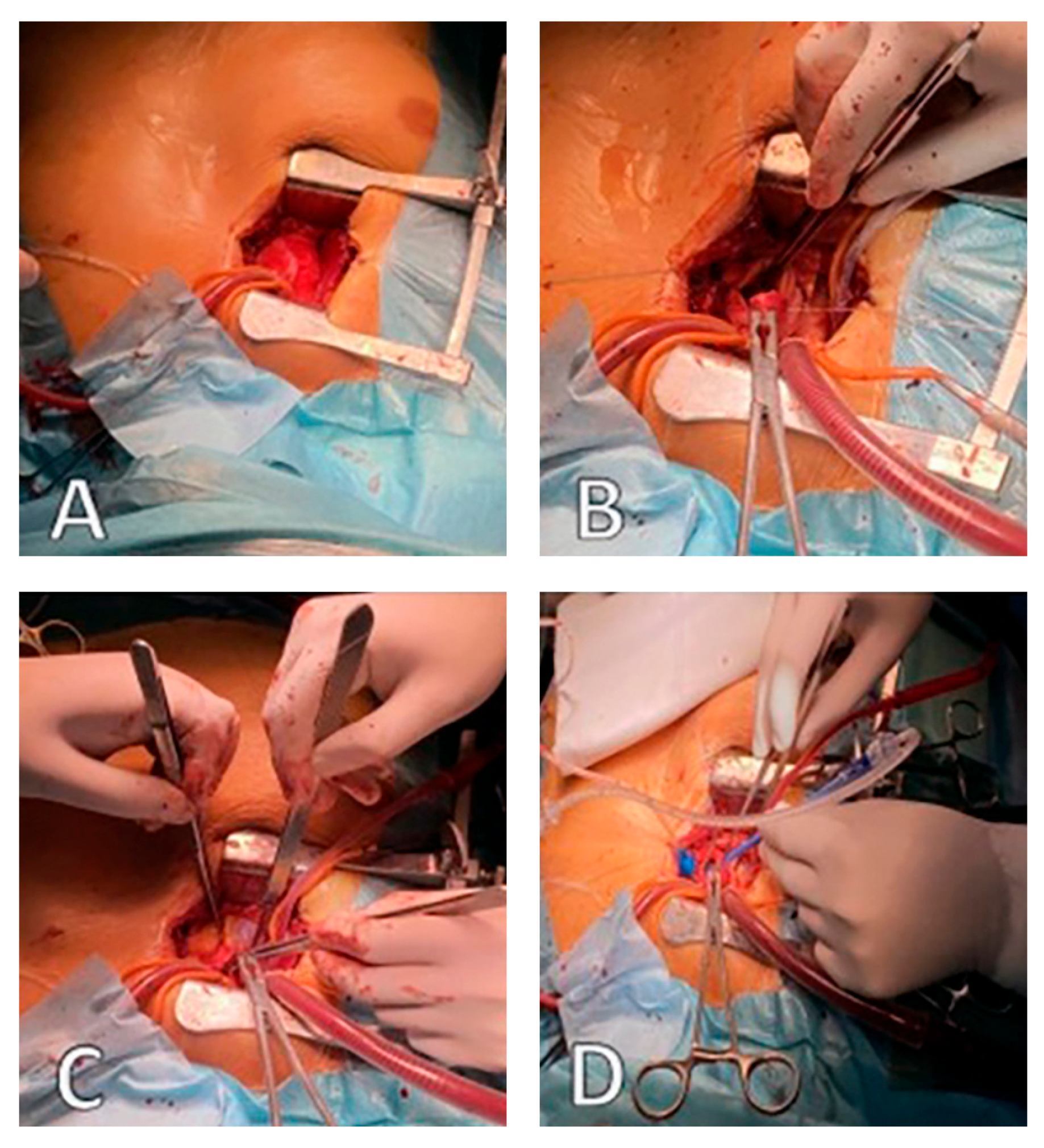
Figure 4.
The Kaplan-Meier curve shows the survival of patients in both groups.
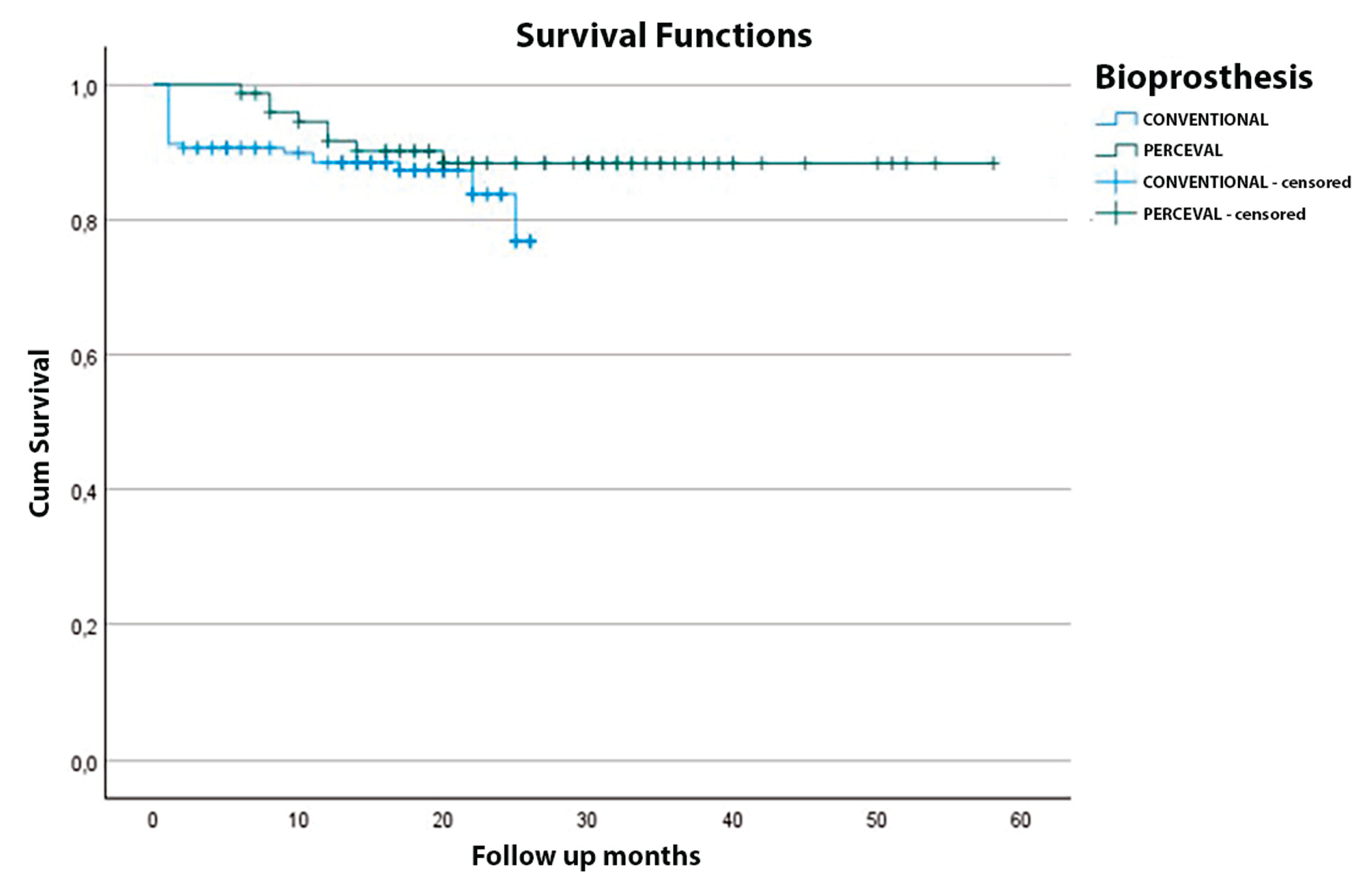

Table 1.
Preoperative patient characteristics.
| Characteristic | Sutureless (N = 74) | Stented (N = 159) | p-value |
|---|---|---|---|
| Age (years) | 72.61 ± 7.21 | 72.67 ± 7.19 | > 0.05 |
| Female, n (%) | 34 (45.9%) | 69 (43.4%) | > 0.05 |
| Male, n (%) | 40 (54.1%) | 90 (56.6%) | > 0.05 |
| Weight (kg) | 77.92 ± 8.40 | 75.82 ± 7.60 | > 0.05 |
| Height (cm) | 165.60 ± 14.50 | 166.86 ± 15.22 | > 0.05 |
| BMI (kg/m²) | 26.6 ± 4.67 | 28.3 ± 11.53 | > 0.05 |
| BSA (m²) | 1.81 ± 0.14 | 1.92 ± 0.19 | > 0.05 |
| Procedure: AVR (isolated) | 61 (82%) | 127 (80%) | > 0.05 |
| Procedure: AVR + CABG | 13 (18%) | 32 (20%) | > 0.05 |
| Peak transvalvular gradient (mmHg) | 76 ± 26 | 74 ± 23 | > 0.05 |
| Mean transvalvular gradient (mmHg) | 52 ± 17 | 52 ± 17 | > 0.05 |
| Aortic valve area (cm²) | 0.61 ± 0.15 | 0.90 ± 0.24 | < 0.05 |
| Bicuspid aortic valve, n (%) | 2 (2.7%) | 8 (5.0%) | > 0.05 |
| NYHA class II | 47 (63.5%) | 89 (56.0%) | > 0.05 |
| NYHA class III | 27 (36.5%) | 70 (44.0%) | > 0.05 |
| Coronary artery disease, n (%) | 16 (21.6%) | 33 (20.7%) | > 0.05 |
| Hypertension, n (%) | 70 (94%) | 122 (76%) | < 0.05 |
| Diabetes mellitus, n (%) | 33 (44%) | 64 (40%) | > 0.05 |
| Chronic lung disease, n (%) | 14 (19%) | 32 (20%) | > 0.05 |
| Neurological disease, n (%) | 9 (12%) | 20 (12.5%) | > 0.05 |
| Renal impairment, n (%) | 14 (19%) | 22 (14%) | > 0.05 |
| Peripheral vascular disease, n (%) | 11 (15%) | 16 (10%) | > 0.05 |
| Dyslipidemia, n (%) | 49 (66%) | 63 (40%) | < 0.05 |
| Current/previous smoking, n (%) | 50 (67.6%) | 102 (64.1%) | > 0.05 |
| LVEF < 30%, n (%) | 3 (4%) | 5 (3%) | > 0.05 |
| LVEF 30–50%, n (%) | 16 (22%) | 28 (18%) | > 0.05 |
| LVEF > 50%, n (%) | 55 (74%) | 126 (79%) | > 0.05 |
| Euro SCORE-II | 1.95 ± 0.84 | 1.76 ± 0.94 | > 0.05 |
| STS score | 1.80 ± 0.74 | 1.54 ± 0.64 | > 0.05 |
Legend: BMI - Body mass index; BSA - Body surface area; AVA - Aortic valve area; NYHA - New York Heart Association functional class; LVEF - Left ventricular ejection fraction; Euro-SCORE-II - European System for Cardiac Operative Risk Evaluation II; STS - Society of Thoracic Surgeons risk score.
Table 2.
Immediate postoperative and hospital outcome.
| Characteristic | Sutureless (N = 74) | Stented (N = 159) | p-value |
|---|---|---|---|
| CPB time (min) | |||
| AVR (isolated) | 83.8 ± 20.6 (n = 61) | 82.7 ± 21.8 (n = 127) | > 0.05 |
| AVR + CABG | 120.3 ± 38.2 (n = 13) | 101.4 ± 36.5 (n = 32) | < 0.05 |
| Full sternotomy | 96.4 ± 44.5 (n = 51) | 97.6 ± 42.8 (n = 137) | > 0.05 |
| Upper mini sternotomy | 88.4 ± 21.4 (n = 17) | 89.2 ± 43.6 (n = 22) | > 0.05 |
| Right anterior thoracotomy | 94.0 ± 9.2 (n = 6) | — (n = 0) | — |
| ACC time (min) | |||
| AVR (isolated) | 54.5 ± 14.6 (n = 61) | 56.8 ± 11.6 (n = 127) | > 0.05 |
| AVR + CABG | 92.1 ± 29.3 (n = 13) | 104.5 ± 29.6 (n = 32) | < 0.05 |
| Full sternotomy | 65.8 ± 27.6 (n = 51) | 67.6 ± 22.8 (n = 137) | > 0.05 |
| Upper mini sternotomy | 53.6 ± 15.8 (n = 17) | 55.4 ± 13.7 (n = 22) | > 0.05 |
| Right anterior thoracotomy | 64.7 ± 5.9 (n = 6) | — (n = 0) | — |
| Perceval prosthesis size | |||
| Small (19–21 mm) | 12 (17.9%) | N/A | — |
| Medium (21–23 mm) | 18 (26.9%) | N/A | — |
| Large (23–25 mm) | 28 (41.8%) | N/A | — |
| X-Large (25–27 mm) | 9 (13.4%) | N/A | — |
| Distal anastomoses (CABG) | |||
| 1 graft | 5 (6.8%) | 11 (6.9%) | > 0.05 |
| 2 grafts | 3 (4.0%) | 6 (3.8%) | > 0.05 |
| 3 grafts | 6 (8.1%) | 15 (9.4%) | > 0.05 |
| Complications | |||
| Paravalvular leak (significant) | 3 (4.0%) | 2 (1.3%) | > 0.05 |
| Neurological dysfunction | 2 (2.7%) | 2 (1.3%) | > 0.05 |
| Thrombocytopenia | 9 (12.2%) | 11 (6.9%) | > 0.05 |
| Re-exploration for bleeding | 4 (5.4%) | 11 (6.9%) | > 0.05 |
| Permanent pacemaker required | 4 (5.4%) | 5 (3.1%) | > 0.05 |
| 24-h chest tube output (mL) | 405 ± 93 | 494 ± 102 | > 0.05 |
| ICU stay (days) | 2.4 ± 1.9 | 2.7 ± 2.1 | > 0.05 |
| Hospital stays (days) | 7.6 ± 3.6 | 8.1 ± 2.3 | > 0.05 |
| 30-day (hospital) mortality | 4 (5.9%) | 10 (6.3%) | > 0.05 |
Legend: AVR – Aortic valve replacement; CABG – Coronary artery bypass grafting; ICU – Intensive care unit.
Table 3.
Late postoperative and follow-up outcomes.
| Characteristic | Sutureless (N = 74) |
Stented (N = 159) |
p-value |
|---|---|---|---|
| Stroke, n (%) | 0 (0%) | 0 (0%) | > 0.05 |
| Endocarditis, n (%) | 0 (0%) | 3 (1.9%) | > 0.05 |
| Neurological event, n (%) * | 3 (4.0%) | 6 (3.8%) | > 0.05 |
| Thrombocytopenia, n (%) | 15 (20.3%) | 17 (10.7%) | < 0.05 |
| Paravalvular leak (trivial), n (%) | 4 (5.4%) | 5 (3.1%) | > 0.05 |
| Peak transvalvular gradient (postop, mmHg) | 22.5 ± 8.1 | 24.5 ± 8.7 | > 0.05 |
| Mean transvalvular gradient (postop, mmHg) | 11.2 ± 4.3 | 12.6 ± 5.3 | > 0.05 |
| Peak transvalvular gradient (follow-up, mmHg) | 19 ± 2 | 20 ± 2.1 | > 0.05 |
| Mean transvalvular gradient (follow-up, mmHg) | 9 ± 2 | 10 ± 2.2 | > 0.05 |
| NYHA class I (latest) | 48 (64.8%) | 92 (57.8%) | > 0.05 |
| NYHA class II (latest) | 26 (35.2%) | 67 (42.2%) | > 0.05 |
Legend:* Includes transient ischemic attack or another neurologic dysfunction.
Table 4.
Postoperative survival during follow-up.
| Months after AVR | Overall survival (%) | Stented group (%) | Sutureless group (%) |
|---|---|---|---|
| 1 | 93.2 | 91.2 | 94.1 |
| 3 | 92.6 | 90.8 | 94.1 |
| 12 | 89.3 | 88.4 | 91.6 |
| 24 | 85.8 | 83.7 | 88.3 |
| 36 | 84.0 | 76.8 | 88.3 |
| 48 | 84.0 | — | 88.3 |
| 58 | 84.0 | — | 88.3 |
Legend: “—” indicates no patients at risk (no data) in the Stented Valve group after 36 months.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



