
Submitted:
26 May 2025
Posted:
28 May 2025
You are already at the latest version
Abstract
Purpose: To investigate the etiology of metachronous focal liver lesions (FLL) detected in patients with solid primary tumors (PT) and to evaluate the factors influencing the nature of these lesions.
Materials and Methods: This retrospective study analyzed 202 patients with a history of solid PT who developed metachronous FLL, defined as lesions detected at least 3 months after the initial PT diagnosis. Latency period (LP) was defined as the time interval, in months, between the initial diagnosis of PT and the detection of the FLL. All patients underwent hepatic ultrasound (US) at our tertiary university hospital between June 2016 and December 2023. Data were retrieved from a prospectively maintained registry. Diagnosis of malignant FLL (mFLL) was histologically confirmed and subclassified as metastases from the known primary tumor (M-PT) or de novo primary tumors (DNPT), which were further divided into metastases from a de novo primary tumor (M-DNPT) and hepatobiliary de novo primary tumors (HB-DNPT). Benign FLL (bFLL) were diagnosed either histologically or based on characteristic features on contrast-enhanced imaging and clinical follow-up, following current diagnostic guidelines. The prevalence, clinical parameters, and sonographic characteristics of the different lesion groups were analyzed and compared. Multinominal and binary regression analyses were used to examine the association between different variables and FLL types. The PT-FLL concordance rate (PT-FLLCR) for each PT was defined as the proportion of FLLs identified as metastases from the corresponding PT.
Results: The study cohort included 202 patients, including 98 males and 104 females, with a mean age of 64 ± 13 years. The average LP was 62.4 ± 72.6 months. Of all detected FLLs, 144 (71.3%) were malignant (mFLL) and 58 (28.7%) were benign (bFLL). M-PT was the most frequent etiology, accounting for 117 lesions (57.9%). Among DNPT, 19 (9.4%) were M-DNPT, and 8 (4.0%) were HB-DNPT. The most common benign lesions were hemangiomas (23; 11.4%), followed by fat deposition/sparing (10; 5.0%) and simple hepatic cysts (9; 4.5%). The final etiology of FLLs varied according to lesion’s echogenicity (p = 0.01), size (p = 0.009), multiple FLL (p = 0.002), and presence of extrahepatic metastases (p = 0.004). The highest PT-FLL-CRs were noted in pancreatobiliary (76.2%) and breast tumors (72.1%), while the lowest rates were seen in prostate carcinoma (20%) and malignant melanoma (6/16; 37.5%). However, there was no statistically significant association between PT-FLL-CR and either the anatomical site or histological subtype of the primary tumor (p > 0.05). Among the 144 mFLL cases, the likelihood of an FLL being a DNPT rather than an M-PT increased with longer LP; specifically, for each additional month of latency, the odds of the lesion being an M-DNPT (vs. M-PT) rose by 0.6% (OR 1.006, p = 0.036).
Conclusion: M-PT represents the most common etiology of metachronous FLL in patients with solid tumors. While lesion characteristics—such as size, echogenicity, multiplicity, and presence of extrahepatic metastases—differed significantly between FLL groups, neither PT origin nor PT histology independently predicted lesion type. Both benign lesions and de novo malignant FLLs can occur. Notably, among mFLLs, a longer LP was associated with a higher probability of DNPT. These findings underscore the importance of histological confirmation of FLLs in patients with a history of solid tumors.
Keywords:
metachronous liver lesions
; de novo tumors
; metachronous cancer
; late metastasis
1. Introduction
Metastases in patients with solid primary tumors (PT) are chronologically classified into synchronous, referring to lesions found at or prior to the diagnosis of the primary tumor, and metachronous, denoting lesions detected later after a latency period (LP) following the initial PT diagnosis. The precise time cutoff for distinguishing metachronous metastases remains a subject of debate, with reported thresholds varying between 3 to 6 months [1].
During the follow-up of malignant tumors, two key challenges arise in the evaluation of metachronous focal liver lesions (FLL). On one hand, benign liver lesions (bFLL) are found in up to 15% of the normal population [2]. These benign lesions may not be detected at the initial diagnosis of the PT due to factors such as small lesion size, limitations of baseline imaging modalities, overlooked or underreported findings, or subsequent parenchymal changes affecting lesion visibility [3-6]. Additionally, certain benign FLL may arise after PT diagnosis. Inflammatory lesions such as abscesses or pseudotumors, regenerative nodules, and hyperplastic lesions like focal nodular hyperplasia (FNH) may develop over time secondary to infections, systemic inflammation, vascular alterations, or as sequelae of chemotherapy-induced hepatic changes, including steatosis or sinusoidal obstruction [7-10]. On the other hand, metastatic spread is a hallmark of malignant diseases and a major determinant of patient prognosis. The liver has been identified as the most common site of distant metastases in solid tumors [11].
When a patient with a known malignant PT is found to have a new FLL after an LP, a comprehensive diagnostic work-up is necessary to differentiate between benign and malignant FLL (mFLL). B-mode ultrasound (B-US) and contrast-enhanced ultrasound (CEUS) remain the primary imaging modalities of choice in this setting [12-18]. Among contrast-enhanced techniques, CEUS, computed tomography (CT), and magnetic resonance imaging (MRI) demonstrate comparable diagnostic accuracy [12]. However, owing to its high sensitivity, specificity, broad availability, cost-effectiveness, and absence of radiation exposure, CEUS is recommended in international ultrasound guidelines for the evaluation of FLL [12,13,15,19,20].
Apart from colorectal cancer, where metachronous liver metastases are well-documented [1,21], data on the prevalence and etiology of metachronous FLL, both benign and malignant, in patients with other solid PT remain scarce. This study aimed to evaluate the etiology and distribution of metachronous benign and malignant FLLs, primarily detected on ultrasound, in patients with solid malignant tumors of various origins.
2. Patients and Methods
This study was conducted at a tertiary healthcare center (University Hospital of Marburg) and included 231 consecutive patients with solid (non-hematological) PT who developed newly detected metachronous FLL, defined as liver lesions identified at least 3 months after the initial PT diagnosis [1]. Lesions were either detected on ultrasound (US) or referred for US-guided biopsy evaluation after identification on other imaging modalities, during the period from June 2016 to December 2023. All data were recorded prospectively in a dedicated registry. Diagnosis validation of FLL was achieved through histological confirmation for all malignant FLL (mFLL) or based on a consensus of characteristic imaging patterns on contrast-enhanced studies, or both, for benign FLLs (bFLL) [19,22,23]. Clinical, imaging, and pathological data were retrospectively retrieved and analyzed. The study was approved by the local ethics committee (protocol code: RS 22/27) and conducted per the amended Declaration of Helsinki. An informed consent was obtained from all patients for the ultrasound examination. Twenty-nine of the initial 231 patients (12.6%) were excluded due to insufficient diagnostic validation, leaving 202 patients included in the final analysis. The exclusion process is illustrated in Figure 1.
2.1. Demographic Data of the Study Patients
Of the 202 study patients 98 (48.5%) were males and 104 (51.5%) females. The mean age was 64 ± 13 years (range 24-86 years).
2.2. Underlying Primary Tumors in the Study Cohort
Table 1 provides an overview of the anatomical sites and histological subtypes of the primary tumors (PT) in all 202 patients included in the study. The most common anatomical sites were the breast (44 patients; 21.8%) and the large intestine (35 patients; 17.3%). Adenocarcinoma was the predominant histological subtype, accounting for 129 cases (63.9%).
2.3. Diagnostic Workup for Focal Liver Lesions (FLL)
Ultrasound examinations were conducted using an ACUSON SEQUOIA 512 ultrasound system (Siemens, Erlangen, Germany) equipped with a 4C1 curved array transducer. For B-mode ultrasound (B-US), a frequency of 4 MHz was applied. Contrast-enhanced ultrasound (CEUS) examinations were performed using the same probe in contrast-specific mode at 1.5 MHz. CEUS examinations were performed and interpreted according to European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) guidelines [12]. All B-US, CEUS assessments, and ultrasound-guided liver biopsies were conducted by a DEGUM Level III-certified investigator (C.G., specialist in internal medicine) with more than 40 years of experience in diagnostic ultrasound [24]. Cross-sectional imaging was performed in 193/202 (95.5%). Histological diagnosis of FLL was available in 159/202 (78.7%) including All 144 mFLL and 15/58 (25.9%) bFLL. The diagnosis of the remaining bFLL was based on characteristic morphology on CEUS and cross-sectional imaging and clinical follow-up (FU). The mean FU was 22.9 ± 22.9 months. All tissue specimens were examined by two experienced pathologists in gastrointestinal diseases at a tertiary university hospital.
2.4. Statistical Analysis
Continuous variables were reported as mean ± SD. Categorical data were analyzed using the Chi-square or Fisher’s exact test, and continuous variables using the Mann–Whitney U or Kruskal–Wallis test. Multinominal and binary regression analyses were used to examine the independent effect of different variables on FLL final diagnosis. A p-value < 0.05 was considered statistically significant. Analyses were conducted using Excel and SPSS v26.0 (Microsoft Excel (Microsoft 365 MSO; Microsoft Corporation, Redmond, WA, USA) and IBM SPSS Statistics, Version 26.0 (IBM Corp., Armonk, NY, USA).
3. Results
3.1. Final FLL Etiology
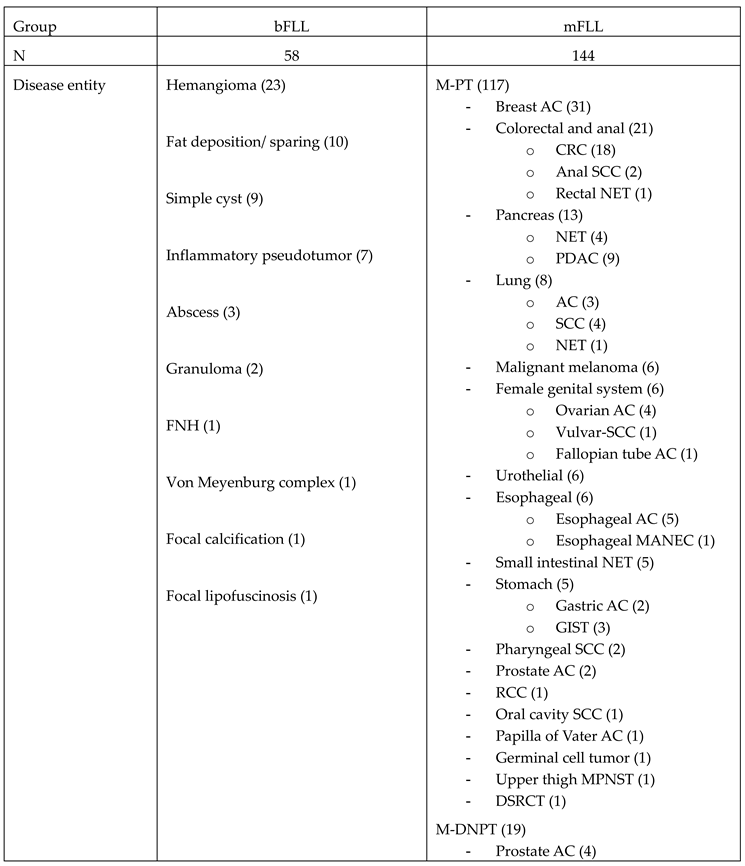
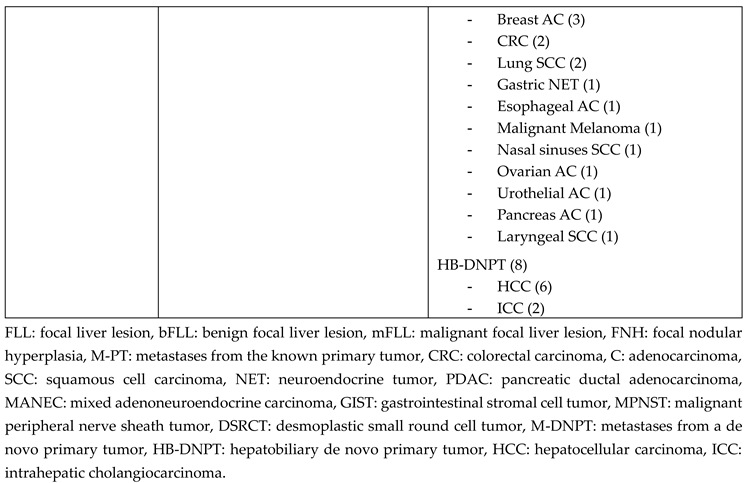
Among the 202 patients, 58 (28.7%) had bFLL, while 144 (71.3%) had mFLL. Hemangioma was the most common bFLL, observed in 23 patients (11.4%). Within the mFLL group, metastases from the known primary tumor (M-PT) represented the most frequent etiology (117 cases; 57.9%), followed by metastases from a de novo extrahepatic primary tumor (M-DNPT) in 19 cases (9.4%), and hepatobiliary de novo primary tumors (HB-DNPT) in 8 cases (4.0%). The final etiologies in all FLLs are shown in Table 2. There were no significant differences in the frequency of FLL etiology based on the anatomical site (p > 0.05) or histological subtype (p > 0.05) of the PT.
3.2. Clinical Features
There were no statistically significant associations between age or gender and FLL category (p > 0.05). Likewise, latency period (LP) did show significant influence on the FLL category (p = 0.16) in our study sample. Figure 2. Extrahepatic metastases (EHM) were more frequently present in the M-PT and M-DNPT groups (62.4% and 63.2%, respectively), compared to the bFLL and HB-DNPT groups (31.0% and 25.0%, respectively; p = 0.004). However, there were no significant differences in FLL distribution between patients with pre-existing EHM (diagnosed >3 months prior to FLL detection) and those with concurrent EHM (p > 0.05). Table 3.
3.3. Sonographic Features
The largest mean lesion sizes were observed in HB-DNPT (4.8± 1.7 cm), followed by M-PT (3.2 ± 2.8 cm) and M-DNPT (3.2 ± 1.4 cm). In contrast, bFLLs had significantly smaller mean sizes (1.9 ± 2.1 cm; p = 0.009). Hypoechogenicity was more frequently observed in M-PT and M-DNPT groups (78.6% and 78.9%, respectively) compared to bFLL and HB-DNPT groups (48.3% and 50.0%, respectively; p = 0.01). Additionally, multiple lesions (>3 FLLs) were more commonly found in the M-PT and M-DNPT groups (55.6% and 78.9%, respectively), while they were significantly less common in the bFLL and HB-DNPT groups (17.2% and 12.5%, respectively; p = 0.002). Table 3. However, in pair comparison using Bonferroni correction there were no significant differences in FLL size or echogenicity within the mFLL group (M-PT vs. DNPT; p > 0.05).

Table 3.
Distribution of different metachronic focal liver lesions (FLL) groups in relation to different clinical and sonographic features in 202 study patients.
Table 3.
Distribution of different metachronic focal liver lesions (FLL) groups in relation to different clinical and sonographic features in 202 study patients.
| Group | bFLL | M-PT | M-DNPT | HB-DPT |
p-value |
| N (%) | 58 (28.7) | 117 (57.9) | 19 (9.4) | 8 (4.0) | |
| Age (years) | 61±14 | 64±13 | 70±8 | 75±8 | 0.12 |
| Males (%) | 30 (51.7) | 51 (43.6) | 13 (68.4) | 4 (50.0) | 0.79 |
| Latency period (months) |
60.3 ± 81.4 | 57.3 ± 65.1 | 80.1 ± 59.8 | 110.6 ± 117.4 | 0.16 |
| Presence of EHM (%) | 18 (31.0) | 73 (62.4%) | 12 (63.2%) | 2 (25.0%) | 0.004 |
| Time of diagnosis of EHM: concurrent/ preexisting | 6/12 | 40/33 | 8/4 | 1/1 | 0.29 |
| Ascites | 2 (3.4) | 15 (12.8) | 3 (15.8) | 1 (12.5) | 0.20 |
| FLL size (cm) | 1.9±2.1 | 3.2±2.8 | 3.2±1.4 | 4.8±1.7 | 0.009 |
| Hypoechoic echotexture (%) | 28 (48.3) | 92 (78.6) | 15 (78.9) | 4 (50.0) | 0.01 |
| Multiple lesions (%) | 10 (17.2) | 65 (55.6) | 15 (78.9) | 1 (12.5) | 0.002 |
bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor, EHM: extrahepatic metastases. P-values based on multinominal regression test using M-PT as the reference category.
3.4. PT–FLL Concordance Rate
The primary tumor–focal liver lesion concordance rate (PT–FLL-CR) was defined as the percentage of patients in whom the FLL was histologically confirmed to be a metastasis from the known primary tumor (M-PT/PT). Among primary tumors with n >10, the highest PT–FLL-CRs were seen in pancreatobiliary tumors (16/21; 76.2%), breast cancer (31/43; 72.1%), and colorectal tumors (19/35; 54.3%). In contrast, tumors with n >10 and low PT–FLL-CRs included prostate cancer (2/10; 20.0%) and malignant melanoma (6/16; 37.5%). However, the observed variations in FLL concordance and discordance across different anatomical sites of the primary tumors were not statistically significant (p > 0.05). Similarly, the PT–FLL-CR did not significantly differ among patients with various histological subtypes of the primary tumor, including adenocarcinoma (76/129; 58.9%), neuroendocrine tumors (NET) (12/21; 57.1%), squamous cell carcinoma (SCC) (10/19; 52.6%), and malignant melanoma (6/16; 37.5%) (p > 0.05). Figure 3 and Figure 4.
3.5. Latency Period (LP) in Malignant FLL (mFLL)
We performed a binary logistic regression analysis on 144 mFLL cases to assess the impact of LP on the likelihood of an FLL being a DNPT rather than an M-PT. The model was statistically significant (p = 0.036), with LP emerging as a significant predictor (OR = 1.006). This indicates that with each additional month of latency, the odds of the FLL being due to a DNPT (vs. M-PT) increase by 0.6% (Figure 5).
4. Discussion
Upon detection of a new FLL, it is crucial to review the patient's clinical history for any earlier malignancies. Both synchronous and metachronous metastases are possible across various PT, with the etiology of FLL varying depending on clinical factors such as the presence or absence of a malignancy history, underlying liver cirrhosis, and the nature of the PT [17,18,25,26] (Table 4). In addition, two key aspects must be considered when evaluating new FLLs in oncology patients. First, benign FLLs are relatively common [2] , and may either be initially overlooked [3-6] or develop metachronously after the diagnosis of the primary tumor [7-10]. Second, hepatic metastases can also emerge after prolonged periods of disease remission [27]. These findings highlight the dynamic nature of liver imaging in oncology and the importance of thorough longitudinal follow-up to differentiate benign from malignant lesions.
Table 4.
Prevalence of malignant focal liver lesions in different diagnostic contexts: a stratified overview for risk assessment.
Table 4.
Prevalence of malignant focal liver lesions in different diagnostic contexts: a stratified overview for risk assessment.
|
Clinical background |
Prevalence of malignant FLL (%) |
N |
Year |
Author |
| Incidental finding in asymptomatic patients | 0.6 | 542 | 2016 | Choi et al. [28] |
| Patients with synchronous hematological malignancy | 33.0 | 61 | 2013 | Heller et al. [26] |
| Patients with a synchronous non-hematological malignancy | 59.4 | 434 | 2021 | Safai Zadeh et al. [17] |
| Patients with liver cirrhosis | 68.4 | 228 | 2022 | Alhyari et al. [18] |
| Patients with metachronous non-hematological malignancy | 71.3 | 202 | 2025 | Present study |
FLL: focal liver lesion.
In this standardized study, we analyzed the frequency of different FLLs in patients with a history of solid primary tumors. Benign lesions accounted for nearly one-third (28.7%) of all FLLs. The most frequent were hemangiomas (23; 11.4%), followed by fat deposition/sparing (10; 5.0%) and simple hepatic cysts (9; 4.5%) (Table 2). As expected, malignant FLLs (71.3%) were more common than benign lesions. The prevalence of mFLL in our cohort exceeded that reported in patients with synchronous hematologic malignancies (33.0%) as described by Heller et al. [26], and surpassed the frequency seen in synchronous solid malignancies (59.4%) reported by Safai Zadeh et al. [17]. Notably, the frequency of metachronous mFLL in our study was comparable to that seen in patients with liver cirrhosis, where rates between 68% and 84% have been reported [18,29].
M-PT represented the most frequent etiology among all FLL, accounting for 57.9% of cases. There were observable variations in the frequency of M-PT across different PT types. The highest primary tumor–FLL concordance rates (PT–FLL-CR) were seen in pancreatobiliary tumors (76.2%), breast cancer (72.1%), and colorectal cancer (54.3%). In contrast, tumors such as prostate cancer (20.0%) and malignant melanoma (37.5%) exhibited lower concordance rates. However, these differences in PT–FLL-CR based on anatomical site were not statistically significant. Similarly, no significant differences were noted in PT–FLL-CR across histological subtypes, including adenocarcinoma (58.9%), neuroendocrine tumors (57.1%), squamous cell carcinoma (52.6%), and malignant melanoma (37.5%).
The cumulative incidence of metachronous liver metastases from colorectal cancer (CRC) has been reported to range between 1% at one year and 15% at five years post-diagnosis [30]. Risk factors associated with metachronous CRC metastases include advanced age, higher N and T stage, specific anatomic locations of the tumor, elevated postoperative carcinoembryonic antigen (CEA) levels, and the presence of mutations such as EGFR and HER2 overexpression [30-40]. In contrast, data on the incidence and risk factors of metachronous liver metastases in non-CRC solid tumors are still limited. For instance, in patients with stage III pancreatic cancer, one study reported cumulative incidences of metachronous liver metastases at 7.2% after 3 months, 18.8% after 6 months, and 37.8% after 12 months following the initial diagnosis, although no specific predictive factors were identified [41].
On the other hand, patients with prior PT have a higher risk of developing a second synchronous or metachronous tumor. Differentiating between de novo tumor from PT metastasis (M-PT) is critical for guiding treatment and prognosis. Although a long LP (typically >5 years), solitary presentation, and an atypical site of metastasis favor a de novo tumor, whereas a short LP and multifocal involvement suggest M-PT, these features are indicative but not definitive—histological evaluation remains essential for accurate diagnosis [42].
In our cohort, metastases from a de novo extrahepatic primary tumor (M-DNPT) were seen in 9.4% of patients, while hepatobiliary de novo primary tumors (HB-DNPT) accounted for 4.0%. No significant associations were found between patient age or gender and the frequency of certain FLL categories. Differences were observed in the mean LP among FLL categories—bFLL (60.3 ± 81.4 months), M-PT (57.3 ± 65.1 months), M-DNPT (80.1 ± 59.8 months), and HB-DNPT (110.6 ± 117.4 months). However, the LP did not significantly influence the FLL category in our study (P > 0.05).
Given the high diagnostic accuracy of modern US, CEUS, and other imaging modalities in reliably identifying benign lesions and suggesting malignancy [12,15,19,20,22], bFLL can typically be diagnosed with a high degree of confidence, often without the need for histological confirmation. Therefore, it is methodologically sound to focus comparative analyses on malignant FLLs, where diagnostic uncertainty tends to be greater and histological diagnosis is often required. In this context, we analyzed the influence of LP on the likelihood of an FLL being a DNPT rather than M-PT. The logistic regression model demonstrated statistical significance (p = 0.036), with LP emerging as a significant predictor (OR = 1.006). This finding indicates that for each additional month of latency, the odds of the lesion being a DNPT (as opposed to an M-PT) increase by 0.6% (Figure 5).
The prevalence of de novo metastatic cancer varies widely, with reports of 5–10% in developed countries to over 20% in certain African nations [43]. This is partly due to comprehensive cancer screening programs and greater public health awareness in high-income countries which enable earlier cancer detection, thereby reducing the likelihood of cancers presenting with de novo metastases [43].
Extrahepatic metastases (EHM) were significantly more frequent in the M-PT and M-DNPT groups (62.4% and 63.2%, respectively) compared to the bFLL and HB-DNPT groups (31.0% and 25.0%, respectively). However, the timing of EHM—whether pre-existing or detected concurrently with the FLL—did not significantly influence the etiology of the liver lesion.
Regarding sonographic characteristics, mFLLs groups were significantly larger than bFLLs. M-PT and M-DNPT lesions were more often hypoechoic than bFLL and HB-DNPT (48.3% and 50.0%, respectively). Furthermore, multifocal FLL were more often found in M-PT and M-DNPT (55.6% and 78.9%, respectively) as compared to bFLL and HB-DNPT (17.2% and 12.5%, respectively).
This study had several limitations. It was retrospective in design and conducted at a single tertiary university center, which may limit generalizability. Moreover, not all focal liver lesions were histologically confirmed; however, all diagnoses were made either through histology or in accordance with established radiologic consensus criteria.
5. Conclusions
In patients with solid malignancies, metachronous FLL are predominantly malignant, with metastases from the known primary tumor being the leading cause. This study underscores tumor-specific differences in metastatic behavior, which may aid in clinical risk stratification. Although statistical significance was not achieved, the observed high concordance rates in pancreatic and breast cancers suggest potential utility for tailored imaging and follow-up strategies. Notably, approximately one-third of FLLs were benign and nearly one-sixth represented de novo malignancies, emphasizing the critical importance of histological confirmation. Larger prospective studies are warranted to enhance predictive models for FLL etiology in this patient population.
References
- Kow, A.W.C. Hepatic metastasis from colorectal cancer. Journal of Gastrointestinal Oncology 2019, 10, 1274–1298. [Google Scholar] [CrossRef] [PubMed]
- Kaltenbach, T.E.; Engler, P.; Kratzer, W.; Oeztuerk, S.; Seufferlein, T.; Haenle, M.M.; Graeter, T. Prevalence of benign focal liver lesions: ultrasound investigation of 45,319 hospital patients. Abdom Radiol (NY) 2016, 41, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Sawatzki, M.; Husarik, D.B.; Semela, D. Assessment of focal liver lesions in non-cirrhotic liver – expert opinion statement by the Swiss Association for the Study of the Liver and the Swiss Society of Gastroenterology. Swiss Medical Weekly 2023, 153, 40099. [Google Scholar] [CrossRef]
- Hasan, H.Y.; Hinshaw, J.L.; Borman, E.J.; Gegios, A.; Leverson, G.; Winslow, E.R. Assessing Normal Growth of Hepatic Hemangiomas During Long-term Follow-up. JAMA Surgery 2014, 149, 1266–1271. [Google Scholar] [CrossRef]
- Reguram, R.; Ghonge, A.; Tse, J.; Dhanasekaran, R. Practical approach to diagnose and manage benign liver masses. Hepatol Commun 2024, 8. [Google Scholar] [CrossRef]
- Ramanathan, S.; Raghu, V.; Virmani, V.; Sheikh, A.; Al Heidous, M.; Tirumani, S. Unveiling the unreal: Comprehensive imaging review of hepatic pseudolesions. Clinical Imaging 2021, 80, 439–453. [Google Scholar] [CrossRef]
- Patnana, M.; Sevrukov, A.B.; Elsayes, K.M.; Viswanathan, C.; Lubner, M.; Menias, C.O. Inflammatory Pseudotumor: The Great Mimicker. American Journal of Roentgenology 2012, 198, W217–W227. [Google Scholar] [CrossRef]
- Balabaud, C.; Al-Rabih, W.R.; Chen, P.J.; Evason, K.; Ferrell, L.; Hernandez-Prera, J.C.; Huang, S.F.; Longerich, T.; Park, Y.N.; Quaglia, A.; et al. Focal Nodular Hyperplasia and Hepatocellular Adenoma around the World Viewed through the Scope of the Immunopathological Classification. Int J Hepatol 2013, 2013, 268625. [Google Scholar] [CrossRef]
- Pope, M.C.; Olson, M.C.; Flicek, K.T.; Patel, N.J.; Bolan, C.W.; Menias, C.O.; Wang, Z.; Venkatesh, S.K. Chemotherapy-associated liver morphological changes in hepatic metastases (CALMCHeM). Diagn Interv Radiol 2023, 29, 571–578. [Google Scholar] [CrossRef]
- Robinson, P.J.A. The effects of cancer chemotherapy on liver imaging. European Radiology 2009, 19, 1752–1762. [Google Scholar] [CrossRef]
- Obenauf, A.C.; Massagué, J. Surviving at a Distance: Organ-Specific Metastasis. Trends Cancer 2015, 1, 76–91. [Google Scholar] [CrossRef] [PubMed]
- Claudon, M.; Dietrich, C.F.; Choi, B.I.; Cosgrove, D.O.; Kudo, M.; Nolsøe, C.P.; Piscaglia, F.; Wilson, S.R.; Barr, R.G.; Chammas, M.C.; et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med 2013, 34, 11–29. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.F.; Sharma, M.; Gibson, R.N.; Schreiber-Dietrich, D.; Jenssen, C. Fortuitously discovered liver lesions. World J Gastroenterol 2013, 19, 3173–3188. [Google Scholar] [CrossRef]
- Dong, Y.; Wang, W.P.; Mao, F.; Zhang, Q.; Yang, D.; Tannapfel, A.; Meloni, M.F.; Neye, H.; Clevert, D.A.; Dietrich, C.F. Imaging Features of Fibrolamellar Hepatocellular Carcinoma with Contrast-Enhanced Ultrasound. Ultraschall Med 2021, 42, 306–313. [Google Scholar] [CrossRef]
- Friedrich-Rust, M.; Klopffleisch, T.; Nierhoff, J.; Herrmann, E.; Vermehren, J.; Schneider, M.D.; Zeuzem, S.; Bojunga, J. Contrast-Enhanced Ultrasound for the differentiation of benign and malignant focal liver lesions: a meta-analysis. Liver Int 2013, 33, 739–755. [Google Scholar] [CrossRef]
- Lantinga, M.A.; Gevers, T.J.; Drenth, J.P. Evaluation of hepatic cystic lesions. World J Gastroenterol 2013, 19, 3543–3554. [Google Scholar] [CrossRef]
- Safai Zadeh, E.; Baumgarten, M.A.; Dietrich, C.F.; Görg, C.; Neesse, A.; Trenker, C.; Alhyari, A. Frequency of synchronous malignant liver lesions initially detected by ultrasound in patients with newly diagnosed underlying non-hematologic malignant disease: a retrospective study in 434 patients. Z Gastroenterol 2022, 60, 586–592. [Google Scholar] [CrossRef]
- Alhyari, A.; Görg, C.; Alakhras, R.; Dietrich, C.F.; Trenker, C.; Safai Zadeh, E. HCC or Something Else? Frequency of Various Benign and Malignant Etiologies in Cirrhotic Patients with Newly Detected Focal Liver Lesions in Relation to Different Clinical and Sonographic Parameters. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Dietrich, C.F.; Nolsøe, C.P.; Barr, R.G.; Berzigotti, A.; Burns, P.N.; Cantisani, V.; Chammas, M.C.; Chaubal, N.; Choi, B.I.; Clevert, D.A.; et al. Guidelines and Good Clinical Practice Recommendations for Contrast-Enhanced Ultrasound (CEUS) in the Liver-Update 2020 WFUMB in Cooperation with EFSUMB, AFSUMB, AIUM, and FLAUS. Ultrasound Med Biol 2020, 46, 2579–2604. [Google Scholar] [CrossRef]
- Bernatik, T.; Schuler, A.; Kunze, G.; Mauch, M.; Dietrich, C.F.; Dirks, K.; Pachmann, C.; Börner, N.; Fellermann, K.; Menzel, J.; et al. Benefit of Contrast-Enhanced Ultrasound (CEUS) in the Follow-Up Care of Patients with Colon Cancer: A Prospective Multicenter Study. Ultraschall Med 2015, 36, 590–593. [Google Scholar] [CrossRef]
- Garajova, I.; Balsano, R.; Tommasi, C.; Dalla Valle, R.; Pedrazzi, G.; Ravaioli, M.; Spallanzani, A.; Leonardi, F.; Santini, C.; Caputo, F.; et al. Synchronous and metachronous colorectal liver metastases: impact of primary tumor location on patterns of recurrence and survival after hepatic resection. Acta Biomed 2020, 92, e2021061. [Google Scholar] [CrossRef]
- Safai Zadeh, E.; Prosch, H.; Ba-Ssalamah, A.; Findeisen, H.; Alhyari, A.; Raab, N.; Görg, C. Contrast-enhanced ultrasound of the liver: basics and interpretation of common focal lesions. Rofo 2024, 196, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Șirli, R.; Popescu, A.; Jenssen, C.; Möller, K.; Lim, A.; Dong, Y.; Sporea, I.; Nürnberg, D.; Petry, M.; Dietrich, C.F. WFUMB Review Paper. Incidental Findings in Otherwise Healthy Subjects, How to Manage: Liver. Cancers (Basel) 2024, 16. [Google Scholar] [CrossRef]
- Heese, F.; Görg, C. [The value of highest quality ultrasound as a reference for ultrasound diagnosis]. Ultraschall Med 2006, 27, 220–224. [Google Scholar] [CrossRef]
- Choi, S.H.; Byun, J.H.; Kim, S.Y.; Lee, S.J.; Won, H.J.; Shin, Y.M.; Kim, P.N. Liver Imaging Reporting and Data System v2014 With Gadoxetate Disodium-Enhanced Magnetic Resonance Imaging: Validation of LI-RADS Category 4 and 5 Criteria. Invest Radiol 2016, 51, 483–490. [Google Scholar] [CrossRef]
- Heller, E.; Görg, C. [Focal liver lesions in patients with malignant haematological disease: value of B-mode ultrasound in comparison to contrast-enhanced ultrasound--a retrospective study with N = 61 patients]. Z Gastroenterol 2013, 51, 558–567. [Google Scholar] [CrossRef]
- Hamada, Y.; Tameda, M.; Nakagawa, H. Metachronous Liver Metastasis during Long-term Follow-up after Endoscopic Submucosal Dissection of a Small Rectal Neuroendocrine Neoplasm. Intern Med 2025. [Google Scholar] [CrossRef]
- Choi, S.H.; Kwon, H.J.; Lee, S.Y.; Park, H.J.; Kim, M.S.; Sohn, J.H.; Chung, E.C.; Park, H.W. Focal hepatic solid lesions incidentally detected on initial ultrasonography in 542 asymptomatic patients. Abdom Radiol (NY) 2016, 41, 265–272. [Google Scholar] [CrossRef]
- Seitz, K.; Greis, C.; Schuler, A.; Bernatik, T.; Blank, W.; Dietrich, C.F.; Strobel, D. Frequency of tumor entities among liver tumors of unclear etiology initially detected by sonography in the noncirrhotic or cirrhotic livers of 1349 patients. Results of the DEGUM multicenter study. Ultraschall Med 2011, 32, 598–603. [Google Scholar] [CrossRef]
- Hao, M.; Wang, K.; Ding, Y.; Li, H.; Liu, Y.; Ding, L. Which patients are prone to suffer liver metastasis? A review of risk factors of metachronous liver metastasis of colorectal cancer. European Journal of Medical Research 2022, 27, 130. [Google Scholar] [CrossRef]
- Chuang, S.C.; Su, Y.C.; Lu, C.Y.; Hsu, H.T.; Sun, L.C.; Shih, Y.L.; Ker, C.G.; Hsieh, J.S.; Lee, K.T.; Wang, J.Y. Risk factors for the development of metachronous liver metastasis in colorectal cancer patients after curative resection. World J Surg 2011, 35, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Liang, L.; Ren, L.; Chen, J.; Wei, Y.; Chang, W.; Zhu, D.; Lin, Q.; Zheng, P.; Xu, J. A specific KRAS codon 13 mutation is an independent predictor for colorectal cancer metachronous distant metastases. Am J Cancer Res 2015, 5, 674–688. [Google Scholar] [PubMed]
- Huang, C.W.; Tsai, H.L.; Chen, Y.T.; Huang, C.M.; Ma, C.J.; Lu, C.Y.; Kuo, C.H.; Wu, D.C.; Chai, C.Y.; Wang, J.Y. The prognostic values of EGFR expression and KRAS mutation in patients with synchronous or metachronous metastatic colorectal cancer. BMC Cancer 2013, 13, 599. [Google Scholar] [CrossRef]
- Khan, M.S.; Bakar, M.A.; Saba, A.; Khan, M.A.; Akbar, S.A.; Islam Nasir, I.U. Risk factors effecting development of metachronous liver metastasis in rectal cancer patients after curative surgical resection. Shaukat Khanum Memorial Cancer Hospital and Research Centre, Lahore experience. J Pak Med Assoc 2019, 69, 201–204. [Google Scholar]
- Laubert, T.; Bente, V.; Freitag-Wolf, S.; Voulgaris, H.; Oberländer, M.; Schillo, K.; Kleemann, M.; Bürk, C.; Bruch, H.P.; Roblick, U.J.; et al. Aneuploidy and elevated CEA indicate an increased risk for metachronous metastasis in colorectal cancer. Int J Colorectal Dis 2013, 28, 767–775. [Google Scholar] [CrossRef]
- Margonis, G.A.; Buettner, S.; Andreatos, N.; Kim, Y.; Wagner, D.; Sasaki, K.; Beer, A.; Schwarz, C.; Løes, I.M.; Smolle, M.; et al. Association of BRAF Mutations With Survival and Recurrence in Surgically Treated Patients With Metastatic Colorectal Liver Cancer. JAMA Surg 2018, 153, e180996. [Google Scholar] [CrossRef]
- Pan, H.D.; Peng, Y.F.; Xiao, G.; Gu, J. High levels of serum platelet-derived growth factor-AA and human epidermal growth factor receptor-2 are predictors of colorectal cancer liver metastasis. World J Gastroenterol 2017, 23, 1233–1240. [Google Scholar] [CrossRef]
- Pantaleo, M.A.; Astolfi, A.; Nannini, M.; Paterini, P.; Piazzi, G.; Ercolani, G.; Brandi, G.; Martinelli, G.; Pession, A.; Pinna, A.D.; et al. Gene expression profiling of liver metastases from colorectal cancer as potential basis for treatment choice. Br J Cancer 2008, 99, 1729–1734. [Google Scholar] [CrossRef]
- Styczen, H.; Nagelmeier, I.; Beissbarth, T.; Nietert, M.; Homayounfar, K.; Sprenger, T.; Boczek, U.; Stanek, K.; Kitz, J.; Wolff, H.A.; et al. HER-2 and HER-3 expression in liver metastases of patients with colorectal cancer. Oncotarget 2015, 6, 15065–15076. [Google Scholar] [CrossRef]
- Zheng, P.; Ren, L.; Feng, Q.; Zhu, D.; Chang, W.; He, G.; Ji, M.; Jian, M.; Lin, Q.; Yi, T.; et al. Differences in clinical characteristics and mutational pattern between synchronous and metachronous colorectal liver metastases. Cancer Manag Res 2018, 10, 2871–2881. [Google Scholar] [CrossRef]
- S, D.; L, W.; B, G.Y.; F, Y.H.; H, S.X.; Q, M.Z.; Hao, C.; W, C.Q.; S, L.Z. Risk factors of liver metastasis from advanced pancreatic adenocarcinoma: a large multicenter cohort study. World J Surg Oncol 2017, 15, 120. [Google Scholar] [CrossRef] [PubMed]
- Rolston, R.; Sasatomi, E.; Hunt, J.; Swalsky, P.A.; Finkelstein, S.D. Distinguishing de novo second cancer formation from tumor recurrence: mutational fingerprinting by microdissection genotyping. J Mol Diagn 2001, 3, 129–132. [Google Scholar] [CrossRef]
- Daniels, J.; Amunyela, O.I.; Nyantakyi, A.Y.; Ayabilah, E.A.; Tackie, J.N.O.; Kyei, K.A. Prevalence and clinicopathological characteristics of de novo metastatic cancer at a major radiotherapy centre in West Africa: a cross-sectional study. Ecancermedicalscience 2024, 18, 1805. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Exclusion and diagnosis validation diagram. PT: primary tumor, FLL: focal liver lesion, mFLL: malignant focal liver lesion, bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, DNPT: de novo primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor, FU: follow-up.
Figure 1.
Exclusion and diagnosis validation diagram. PT: primary tumor, FLL: focal liver lesion, mFLL: malignant focal liver lesion, bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, DNPT: de novo primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor, FU: follow-up.
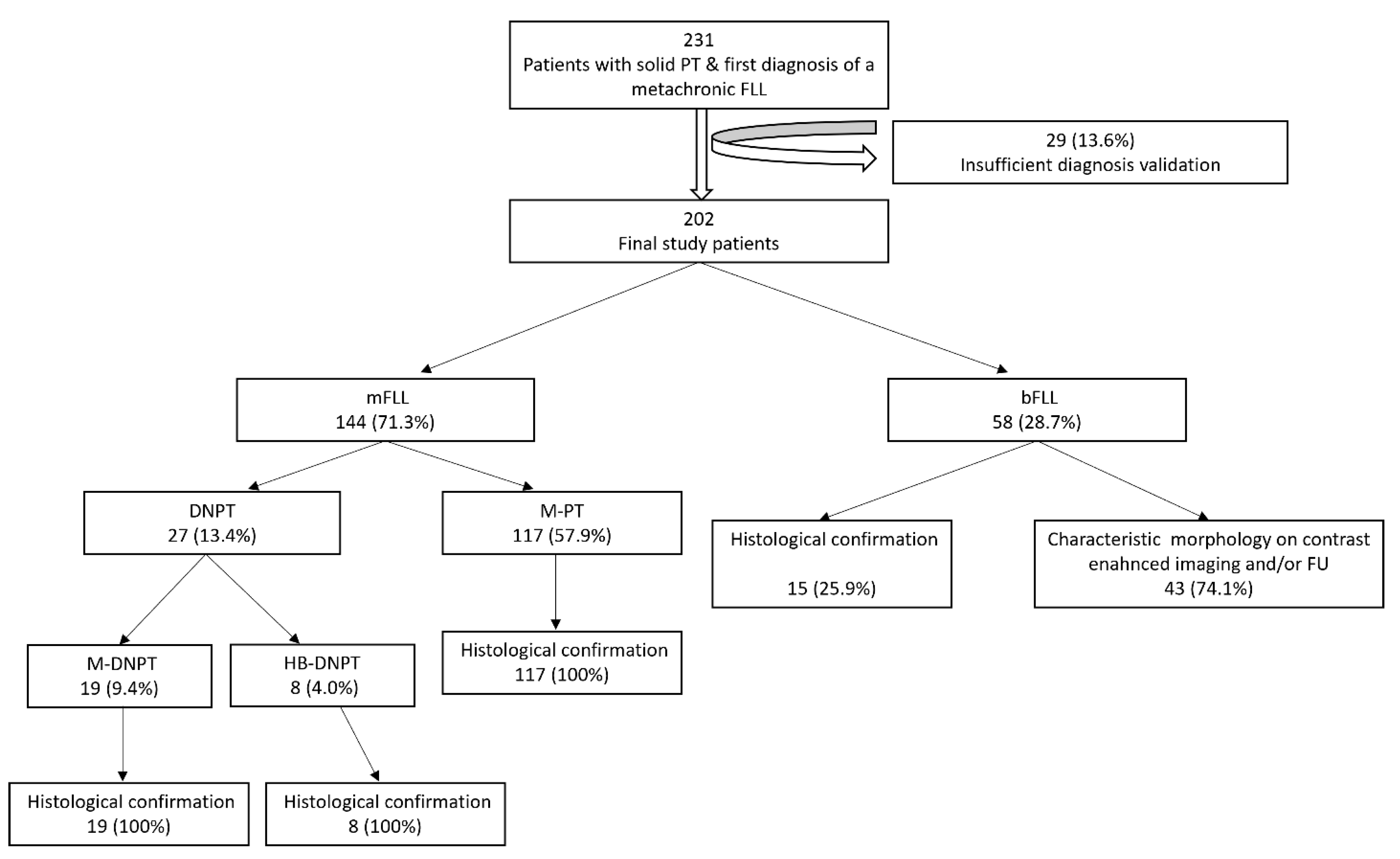
Figure 2.
Differences in the latency period (LP) between the time of initial diagnosis of the primary tumor (PT) and the first diagnosis of metachronous focal liver lesions (FLL) across different FLL categories. bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor.
Figure 2.
Differences in the latency period (LP) between the time of initial diagnosis of the primary tumor (PT) and the first diagnosis of metachronous focal liver lesions (FLL) across different FLL categories. bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor.
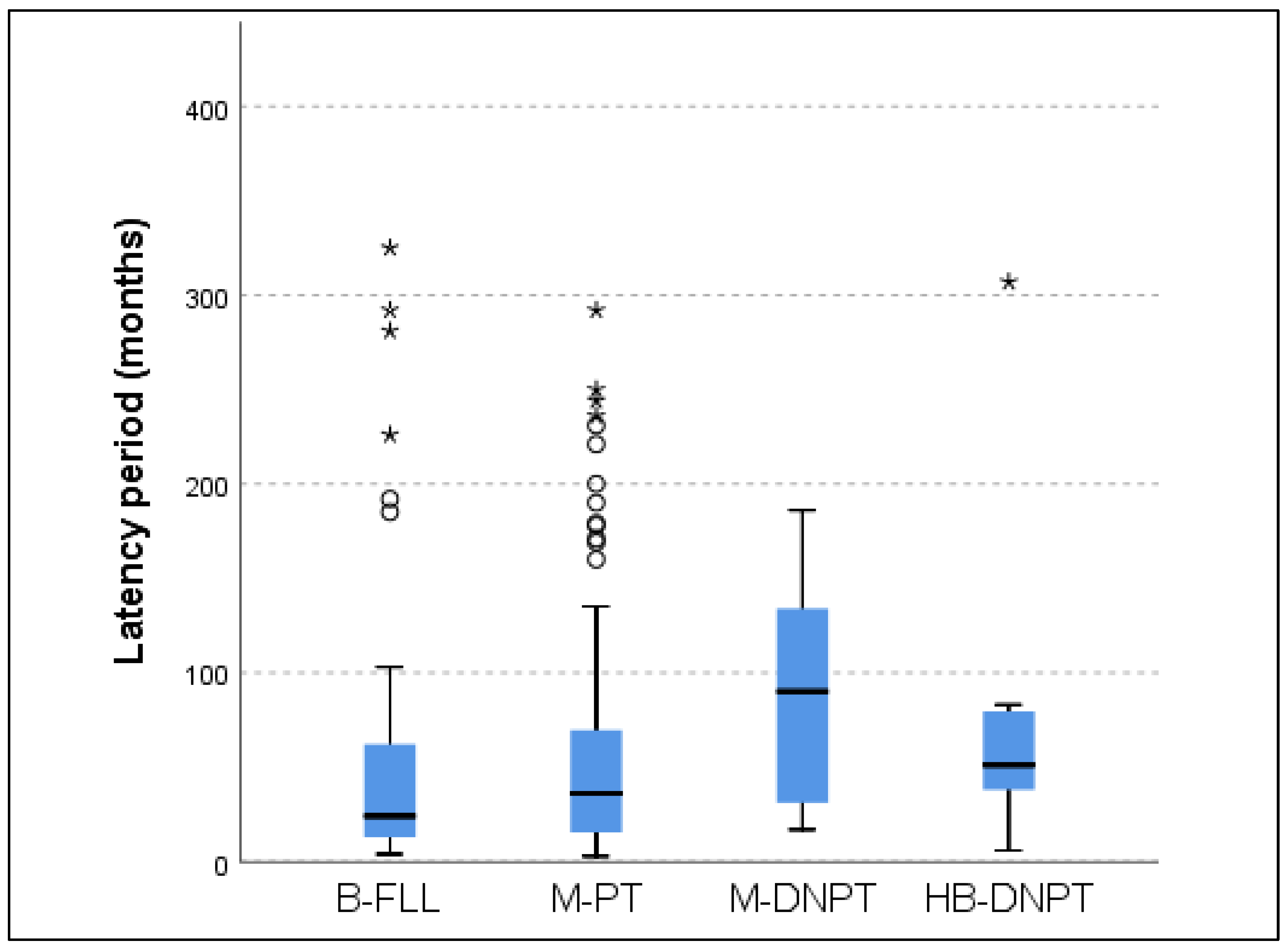
Figure 3.
Distribution of various categories of focal liver lesions depending on the anatomical site of the underlying primary tumor (where n >10). FLL: focal liver lesion, bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor.
Figure 3.
Distribution of various categories of focal liver lesions depending on the anatomical site of the underlying primary tumor (where n >10). FLL: focal liver lesion, bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor.
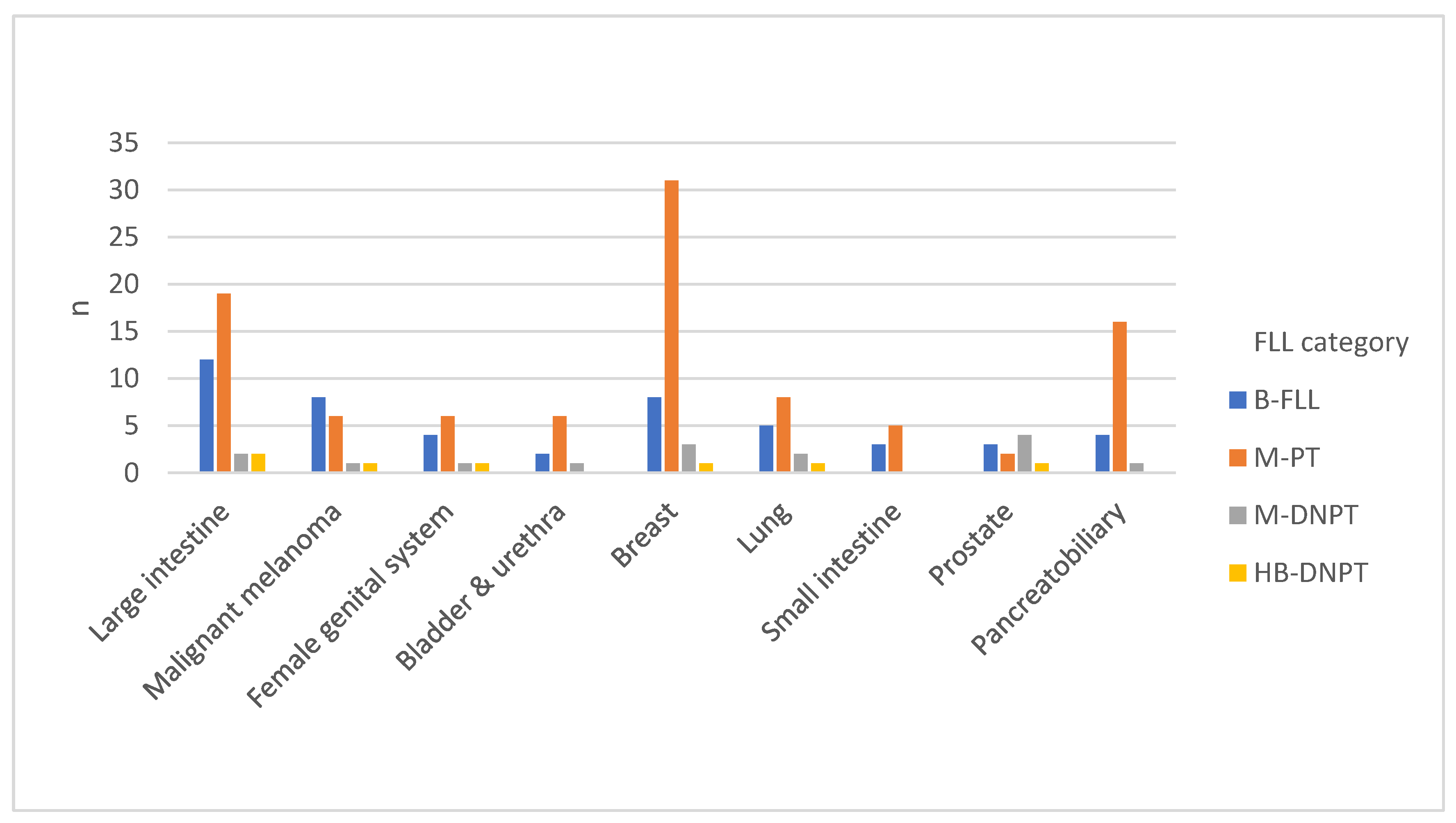
Figure 4.
Distribution of various categories of focal liver lesions depending on the histological type of the primary tumor (where n >10). SCC: squamous cell carcinoma, NET: neuroendocrine tumor, FLL: focal liver lesion, bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor.
Figure 4.
Distribution of various categories of focal liver lesions depending on the histological type of the primary tumor (where n >10). SCC: squamous cell carcinoma, NET: neuroendocrine tumor, FLL: focal liver lesion, bFLL: benign focal liver lesion, M-PT: metastases from the known primary tumor, M-DNPT: metastases from a de novo primary tumor, HB-DNPT: hepatobiliary de novo primary tumor.
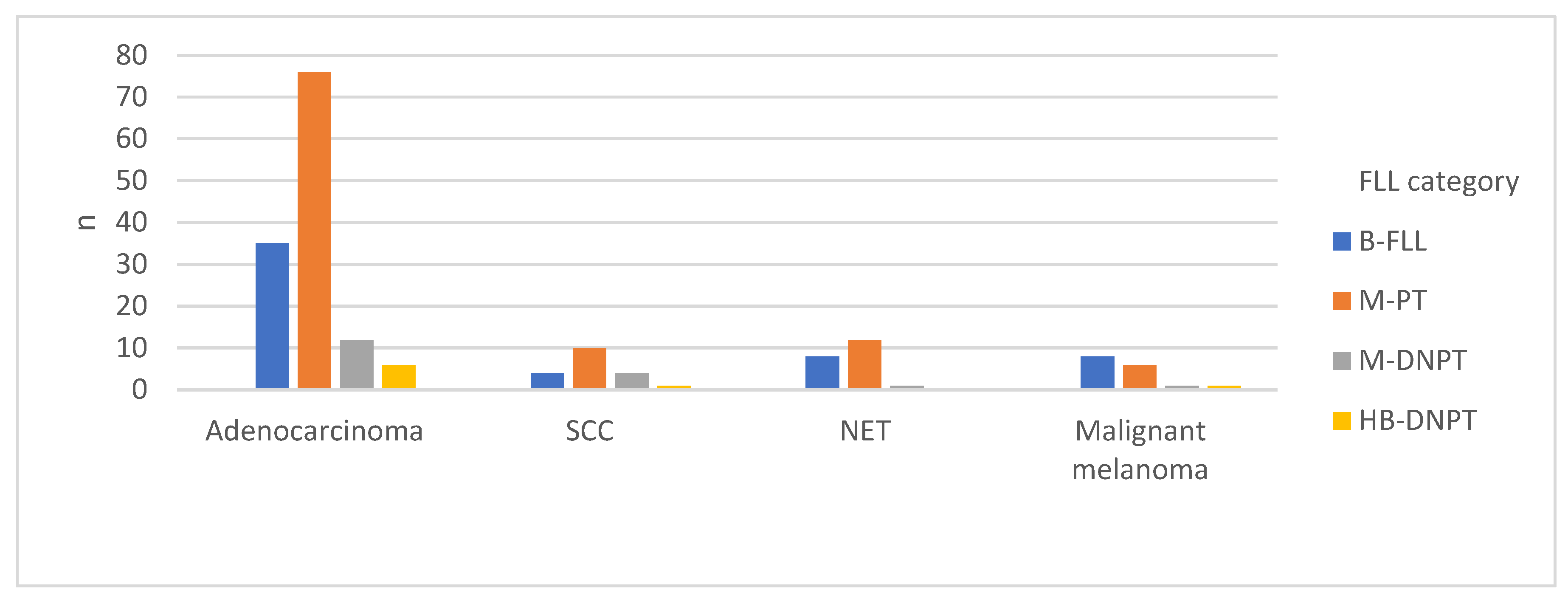
Figure 5.
Modeled probability of de novo primary tumor (DNPT) as a function of latency period in metachronous malignant focal liver lesions in n = 144 patients with a history of solid tumor.
Figure 5.
Modeled probability of de novo primary tumor (DNPT) as a function of latency period in metachronous malignant focal liver lesions in n = 144 patients with a history of solid tumor.
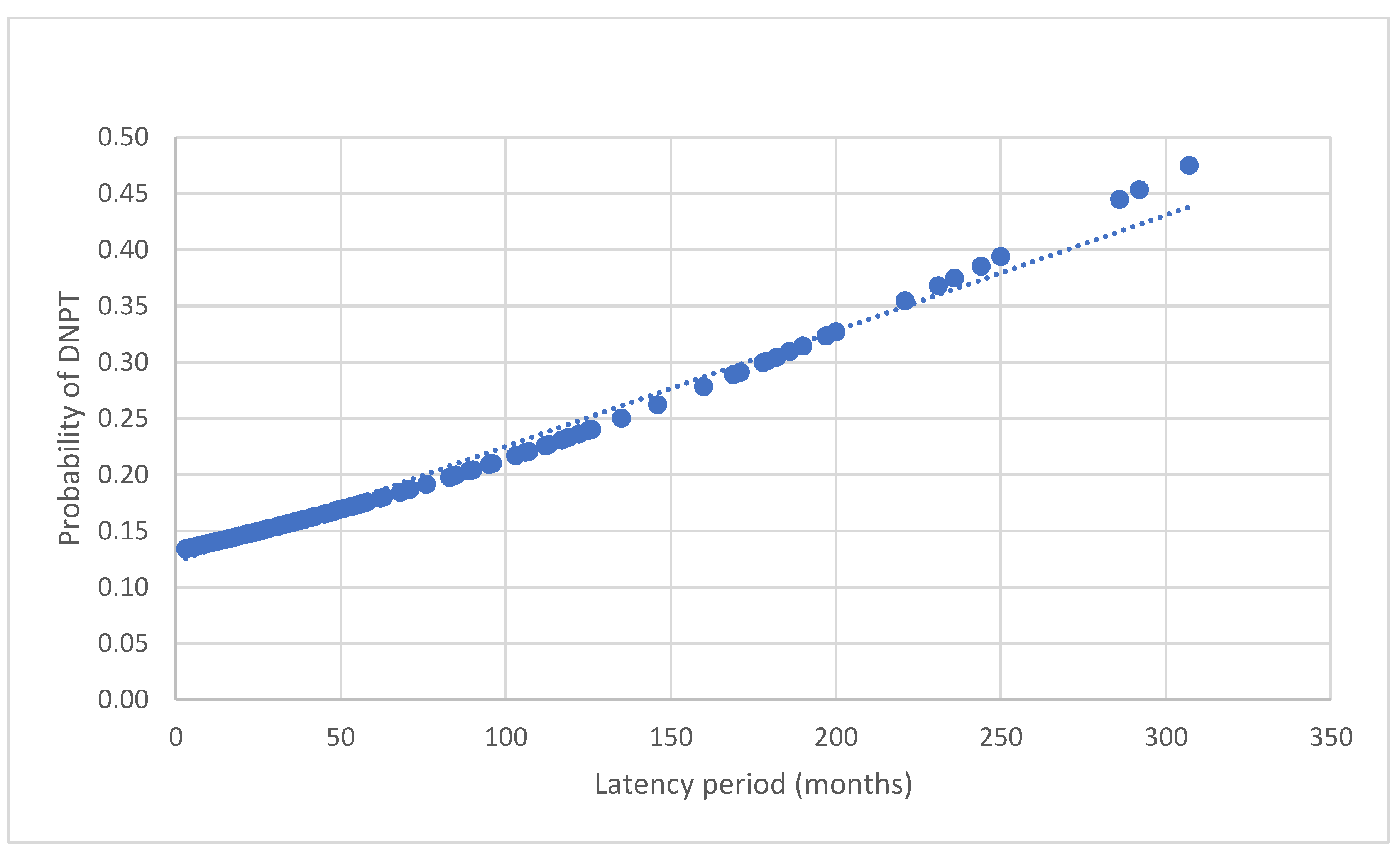
Table 1.
Anatomical site and histological subtypes of the primary tumor in all patients.
| Primary tumor anatomical site | N | Percentage (%) |
| Breast | 43 | 21.8 |
| Large intestine | 35 | 17.3 |
| Pancreatobiliary | 21 | 9.9 |
| Skin | 16 | 7.9 |
| Lung | 16 | 7.4 |
| Female reproductive organs | 12 | 5.4 |
| Prostate | 10 | 5.0 |
| Small intestine | 8 | 4.5 |
| Esophagus | 9 | 4.5 |
| Bladder & urethra | 9 | 4.5 |
| Head & neck | 7 | 4.0 |
| Stomach | 7 | 3.0 |
| Kidney | 5 | 2.5 |
| Others | 4 | 2.5 |
| Primary tumor histological subtype | N | Percentage (%) |
| Adenocarcinoma | 129 | 63.9 |
| NET | 21 | 10.4 |
| SCC | 19 | 9.4 |
| Malignant melanoma | 16 | 7.9 |
| TCC | 9 | 4.5 |
| Sarcoma | 6 | 3.0 |
| GCT | 1 | 0.5 |
| MANEC | 1 | 0.5 |
SCC: squamous cell carcinoma, NET: neuroendocrine tumor, TCC: transitional cell carcinoma, GCT: germinal cell tumor, MANEC: mixed adenoneuroendocrine carcinoma.
Table 2.
Final diagnoses of all 202 FLL.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



