Submitted:
15 May 2025
Posted:
16 May 2025
You are already at the latest version
Abstract
(1) Background: Gallbladder carcinoma (GBC) represents a tumor with an unfavorable prognosis because of late discovery and a 5-year survival of 5-10%; the diagnosis is based on CT scan or MRI, but half of the cases are accidentally discovered after cholecystectomy (occult cases). Transabdominal ultrasound (TUS) lacks sufficient accuracy for the diagnosis, however, high-resolution examination and the introduction of contrast-enhanced ultrasound (CEUS) has increased the performance in gallbladder carcinoma detection and characterization (2) Methods: We performed an observational, retrospective study that included all patients with gallbladder carcinoma admitted to the Craiova County Emergency Clinic Hospital between January 1, 2017, and December 31, 2024; patients with no pathological confirmation, and those with insufficient data were excluded. (3) Results: 40 cases of gallbladder carcinoma were diagnosed; TUS sensitivity was lower, but specificity was similar to that of the CT scan. CEUS was suggestive of GBC in 5 cases and was false positive in another case. The survival for gallbladder tumors was poor, with 32.5% 1-year and 10.5% 5-year survival. CDX2 immunostaining was positive in 50% of the 10 tested stage III carcinomas and was associated with a higher median survival. (4) Conclusions: Gallbladder carcinomas are rarely encountered (50% being occult cases) and harbor a dismal prognosis.
Keywords:
gallbladder carcinoma
; contrast-enhanced ultrasound
; adenosquamous carcinoma
; CDX2 immunohistochemistry
1. Introduction
Gallbladder carcinoma (GBC) represents the most frequent form of biliary tree cholangiocarcinoma [1,2,3], with 115000 new worldwide cases according to the GLOBOCAN 2020 [3]; the prevalence in mass screening ultrasonography in Japan was 0.011% [4]. The prognosis is poor, with 5-year survival of up to 5-10% [1,2,3,5,6], although recent data have shown a progressive increase in 5-year survival of up to 7-20% [1]. The main risk factors are gallbladder lithiasis (more often large stones > 3 cm), chronic inflammation, porcelain cholecystitis, and primary sclerosing cholangitis; environmental (obesity, metabolic syndrome, diabetes) and genetic factors are also involved [1,2,4,5]. Most malignant gallbladder tumors are adenocarcinoma, although rare cases of squamous and adenosquamous carcinoma, and neuroendocrine tumors have been described [1,2,5,7,8].
The diagnosis of gallbladder carcinoma is made by imaging techniques such as transabdominal ultrasound, CT scan, and Magnetic Resonance Imaging (MRI); several recent methods such as PET-CT, contrast-enhanced transabdominal ultrasound (CE-US), or endoscopic ultrasound can aid in the diagnosis [1]. CEUS represents a recently introduced imaging method for the diagnosis of liver, breast, thyroid, and kidney benign and malignant lesions [9], and especially for focal liver lesion diagnosis [10,11,12]. CEUS uses contrast enhancer injected into the blood circulation, which enhances the discrepancies between the blood flow and surrounding tissue [9], making it possible to detect tumoral blood flow [9]; lack of adverse events and significant contraindications make CEUS useful in case of CT or MRI contraindications [13]. Despite advancing imaging methods, the tumor is discovered from the cholecystectomy specimen in approximately half of the cases, being misdiagnosed as acute or chronic cholecystitis [1,5]. Incidental (occult) gallbladder carcinomas are found in 0.2-3% of cholecystectomies, and up to 3.4% of patients with gallbladder lithiasis have concomitant carcinoma at autopsy [5].
Caudal homeodomain transcription factor 2 (CDX2) represents a regulatory molecule involved in intestinal differentiation during embryogenesis and after birth; normal expression in adults is confined to the small and large bowel epithelium [14,15,16,17] and pathological expression was noted in Barrett epithelium, gastric intestinal metaplasia and gastric carcinoma, and also in cholangiocarcinoma and intrahepatic papillary neoplasia [14,15,16,17]. The CDX2 expression was absent in normal gallbladder, but gallbladder intestinal metaplasia and gallbladder carcinoma were associated with aberrant expression of both CDX2 and MUC2 [15,16,17].
Several studies and case reports of gallbladder carcinoma were published in Romania [18,19,20,21,22]; available cohort studies included patients diagnosed before 2011 [18,19], and data regarding new diagnostic methods such as helical CT scan and CEUS are limited to case reports. Because recent data regarding the prevalence, occult carcinoma frequency, diagnosis, and therapeutic particularities are lacking, a study assessing gallbladder carcinoma prevalence, diagnosis, prognosis, and treatment in Romania may be useful.
The purpose of our study was: (1) to evaluate the prevalence of gallbladder carcinoma, pathological types, and occult cases reported to the total number of cholecystectomies in an 8th-year study period; (2) to evaluate the predictive value of CT scan, transabdominal US and CEUS for gallbladder carcinoma diagnosis; (3) to assess CDX2 expression in patients with gallbladder tumors; (4) to evaluate the survival and prognostic factors for gallbladder carcinoma.
2. Materials and Methods
2.1. Patient Selection
We performed an observational, retrospective cohort study that included patients with malignant gallbladder tumors admitted to the Emergency Clinic Hospital (SCJUC) between January 1, 2017, and November 30, 2024. The data were collected from the analysis of the patient's discharge documents from the Hippocrates computer system of the hospital (Version 4, Romanian Software Solutions, Bucharest, Romania)), with diagnostic codes of malignant gallbladder tumors (C23) and also digestive tumors with unpredictable and unknown evolution (D37.7, D37.9). Because of the risk of occult gallbladder tumors, the investigation was completed by analyzing all cholecystectomies and gallbladder biopsies performed during the 2017-2024 period in Emergency Clinic Hospital Craiova (procedure code J101), and all pathological reports were scanned for malignant gallbladder tumors.
The diagnosis of malignant gallbladder tumors was based on clinical data, imaging (transabdominal ultrasound, contrast-enhanced transabdominal ultrasound, CT scan, MR imaging), and intraoperative aspects, and confirmed by pathology examination of the surgically resected gallbladder. The symptoms and the presence of complications were recorded. The CT scan and MR imaging noted the dimensions of the lesion (if the lesion was seen), the parietal thickening, the liver invasion, the presence or absence of invaded lymph nodes, and distant metastases.
CEUS was performed using Hitachi-Aloka Preirus Arietta 70 (Tokyo, Japan) between 2017 and 2019. We used a low-mechanical-index cadence contrast pulse sequencing technology, and an ultrasound contrast agent, SonoVue (Bracco, Geneva, Switzerland), was employed. Two phases of CEUS were analyzed for the gallbladder (the arterial phase, beginning 10-20 seconds after the injection and ending 30 seconds, and the venous phase, which lasts until 2 minutes after injection) [23]; in the late phase, liver parenchyma abnormalities were scanned.
We selected patients with cholecystectomies performed for benign diseases in our hospital as a control group. We analyzed the pathological type of malignant gallbladder tumors, and we estimated the sensitivity, specificity, accuracy, and positive and negative predictive value of CT scan and transabdominal ultrasound for the diagnosis. We used the data from the National Oncology Registry and the National Database for Population Registration for death records, and we analyzed survival by estimating the Kaplan-Meier curve and by performing statistical analysis of predictive parameters for survival.
The study was approved by the Clinical County Emergency Hospital of Craiova Ethics Committee (no. 14090/27.03.2024) on the following information: (1) data was collected within a retrospective, observational study; (2) the study did not interfere with current medical care; (3) data was collected and analyzed anonymously so that the patient data confidentiality would not be breached. The tumor stage was evaluated by using the 8th edition of the “TNM Malign Tumor Classification” from the International Cancer Control Union [24] – Table 1 and Table 2.
2.2. Statistical analysis
The extracted data were computed in an Excel spreadsheet. We used Microsoft Excel 2019 MSO (version 2304 Build 16.0.16327.20200) to build a database in which we included all the variables, and XLSTAT with Addinsoft 2016 version for statistical analysis. The frequencies were presented as absolute numbers of cases and percentages. Chi-squared tests were used to compare ordinal or nominal variables. Survival analysis was performed using R software (version 4.3) with the survival and survminer packages. Survival analysis was performed using the Kaplan-Meier method to estimate survival probabilities, and differences between groups were assessed with the log-rank test.
3. Results
Main Characteristics of Patients
4110 cholecystectomies were performed during the 2017-2024, 40 primitive carcinomas were diagnosed during the analyzed period, and 7 cases of gallbladder invasion were also recorded (three each from gastric or pancreatic carcinoma, and one from a transverse colon tumor). The rate of gallbladder carcinomas from total cholecystectomies was 0.97%; in 19 and 9 gallbladder carcinomas, the preoperatively and postoperatively diagnosed conditions were acute or chronic cholecystitis. The rate of occult gallbladder carcinomas (tumors discovered only by pathology) was 0.22%. Most patients were females (62.5%); the mean age was 68.8±9 years. Most tumors had an advanced stage at the moment of the diagnosis (45% in III stage and 47.5% in IV stage TNM). The flowchart of selected patients is presented in Figure 1.
The main characteristics of the patients with primitive gallbladder carcinoma are noted in Table 3.
In almost half of the cases, the preoperative diagnosis was acute or chronic cholecystitis; CT scan was available in 23 cases, with a suggestive examination for gallbladder tumor in 60.9% (Figure 2, Figure 3, Figure 4 and Figure 5). Transabdominal ultrasound was available in 17 cases, with a suggestive aspect for tumor in only 35.3%; contrast-enhanced ultrasound was used in 5 cases and showed focal thickening with moderate heterogeneous hyperenhancement in 3 cases or a large ill-defined mass in the gallbladder fossa (Figure 6, Figure 7, Figure 8, Figure 9, Figure 10, Figure 11, Figure 12 and Figure 13). The intraoperative aspect was suggestive of gallbladder tumors in 72.2% (Figure 14 and Figure 15) and of inflammation in 9 cases (25%). Lymphadenectomy was performed in only 2 cases (one with positive lymph nodes) and not performed in 23 cases with cholecystectomy (10 cases with intraoperative diagnosis of acute or chronic cholecystitis, 3 cases of incomplete resection because of local extension, 3 cases with liver or peritoneal metastases, 2 cases with severe jaundice, 3 cases with severe comorbidities-liver cirrhosis, diabetes-or advanced age, and in 2 cases no reason was specified).
We estimated the sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for transabdominal ultrasound, CT scan, and preoperative and intraoperative diagnosis (Table 4).
For transabdominal ultrasound, the sensitivity and positive predictive value were lower than for the CT scan, whereas specificity and negative predictive value were similar. It is important to point out that CT scan and MRI represent the most important imaging methods for the diagnosis of gallbladder tumors, but were rarely used in a presumed acute or chronic cholecystitis; for that reason, in occult cases, only transabdominal ultrasound is generally performed. It is also important to emphasize that the intraoperative aspect had a moderate sensitivity of 74.3%.
The pathology examination has shown 33 cases of adenocarcinoma and 4 adenosquamous gallbladder tumors (in another 3 cases, poorly differentiated carcinoma was diagnosed); CDX2 immunostaining was performed in 8 cases with stage III and 2 cases of stage IVA gallbladder carcinomas (Figure 16, Figure 17, Figure 18, Figure 19, Figure 20, Figure 21, Figure 22, Figure 23, Figure 24 and Figure 25). CDX2 positivity was noted in one of two adenosquamous carcinomas and 4 of 8 adenocarcinomas (50% positivity rate for CDX2). The median survival of patients with CDX2 positivity was 3.4 months (95% CI 1.4-5.3), and for CDX2 negative patients was 9.4 months (0.1-18.3, log-rank 0.20). Two cases were mucinous carcinomas.
Surgical exploration was performed in 36 of 40 cases (90%), and cholecystectomy was performed in 26 of 36 patients (72.2%); radical R0 resection was noted in 12 cases (46.2%). No neoadjuvant chemotherapy was indicated; however, postoperative chemotherapy was introduced in 15 of 36 patients who survived after surgery; the most used protocol was Gemcitabine with Oxaliplatin and 5-Fluorouracil with Oxaliplatin.
The survival of GBC in our patient group was poor, with 1-year, 3-year, and 5-year rates of 32.5% (95% CI, 20.8-50.8%), 13.6% (95% CI, 6.1-30.4%), and 10.2% (95% CI, 3.8-27.3%), respectively (2 patients were diagnosed in 2023-2024 and had not yet attained 3-year survival). Median survival was 3.8 months for all GBC (95% CI 2.2-14.1 months).
The KM survival curve (Figure 26) has shown an early survival drop, with the steep initial decline in survival probability (from 100% to ~50%) within the first 24 months, suggesting aggressive disease progression, typical of gallbladder carcinoma, which often presents at advanced stages. A small subset of patients (~7.5%, 3/40) survived beyond 60 months, indicating potential tumor biology or treatment response heterogeneity.
The Kaplan-Meier analysis shown no difference regarding survival stratified by age, gender, grading, R0 versus R1 resection type (median 11.2 months, 6.5-15.8, versus 9.5 months, 2.2-16.8, log-rank p-value 0.836), or adenocarcinoma versus adenosquamous carcinoma (median 7.4, 3.7-11.1, versus 1.9 months, 0.6-3.3, log-rank p-value 0.170). We noted significant differences regarding surgery (cholecystectomy versus laparotomy or no surgery), staging (especially in case of metastasis presence at the time of the diagnosis), and postoperative chemotherapy.
Patients performing cholecystectomy had a greater median survival than those with laparotomy with biopsy or without surgery (10.6 months, 95% CI, 2.9-20.6 versus 2 months, 95% CI, 1-NA for laparotomy, and 2.5 months, 95% CI, 1.7-NA for patients with no surgery performed, log-rank p-value 0.029) as in Figure 27. Patients who underwent no surgery (n=4) had universally poor outcomes, with all succumbing to the disease shortly after diagnosis; this aligns with the known aggressiveness of unresected gallbladder carcinoma. Both surgical groups (cholecystectomy versus laparotomy) showed overlapping survival curves, though the laparotomy cohort (n=10) had higher attrition early on (only 1 patient remaining at risk after 12 months). In GBC patients performing cholecystectomy, the 1-year, 3-year, and 5-year survival rates were 46.2% (95% CI, 30.5-69.9%), 16.9% (95% CI, 7-40.9%), and 11.3% (95% CI, 3.4-37.1%), respectively. For GBC patients without curative surgery, the survival rates were the same in all cut points (7.1%, 95% CI, 1.1%-47.2%). In patients with cholecystectomy, no survival differences were found regarding the presence of vascular, lymphatic, or perineural invasion (log-rank p-values 0.294, 0.327, and 0.736, respectively).
5-year survival rate for M0 disease ranges from 10–30%, while M1 disease has a <5% 1-year survival rate (Figure 28). For patients with no metastases, the median survival was 10.6 months (95% CI, 4.4-20.6), whereas in the M1 stage, the median survival was 2 months (95% CI, 1-4.1). For patients in the III stage, the median survival was 9.7 months (95% CI, 3-20.9) versus 2.2 months (95% CI, 1.9-9.5) for IV stage (log-rank p-value 0.0033). In patients with stage I and II, the survival curve does not drop below 1/2 during the observational period, thus, the median survival was undefined.
In patients with postoperative chemotherapy, median survival was 11.6 months (95% CI, 4.1-NA); the survival rates were 46.67% (95% CI, 27.17-80.16%) at 1-year, 20% (95% CI, 7.27-55.03%) at 3-years and 10% (95% CI, 1.80-55.63%) at 5-years. In patients without postoperative chemotherapy, the median survival was 2.7 months (95% CI, 1.8-6.3), and the 1-year, 3-year, and 5-year survival rates were 24% (95% CI, 11.95-48.21%), 9.6% (95% CI, 2.67-34.54%), and 9.6% (95% CI, 2.67-34.54%), respectively (log-rank p-value 0.14), as shown in Figure 29. However, the trend may still warrant clinical consideration: the curves show a numerical trend favoring chemotherapy early in follow-up (e.g., higher survival probability at earlier time points). This could imply a potential short-term benefit that was not sustained or detectable, given the small sample size.
4. Discussion
In our study, the rate of gallbladder carcinoma from total cholecystectomies was 0.79%, similar to literature data; in a study comparing US and pathology of cholecystectomy patients over 2631 cases, polyps were diagnosed by pathology in 2.6%, and the incidence of carcinoma was 0.38% [25]. The rate of occult carcinoma from total cholecystectomies was 0.3%; the diagnosis of malignancy was missed preoperatively in 60% of cases and intraoperatively in 25%. The presence of occult carcinoma may pose significant problems related to oncological management, especially when patients do not return for pathological results or they do not want a second (radical) surgery to complete the R0 resection and concurrent lymphadenectomy.
Most tumors were diagnosed in advanced stages (70% were T3 or T4, and 35% had distant metastases); lympho-vascular invasion was noted in 12 of 28 cases, and perineural invasion in 10 cases (42.9% and 37.5%, respectively). In a study of 127 pts, 34 were T1 or T2, and 63% were M(+) [26]. In another study, ten (16%), 11 (18%), eight (13%), 16 (25%), nine (15%), and eight patients (13%) were diagnosed with stages I, II, IIIA, IIIB, IVA, and IVB disease, respectively [27]. In another study of 78 resected gallbladder carcinomas, 56 were T3/T4, 37 were N(+), and 6 were M(+) [28]. In a multicentric study of 255 patients with re-resection with curative intent after cholecystectomy, 71.6% were T1 or T2, with perineural and/or lympho-vascular invasion in 37.6%, only 75 were N(+), and 7 were M(+) [29]. In another study, 29.4% were pTis or pT1, and 10.8% showed lymphatic invasion [30].
Transabdominal ultrasonography (TUS) and computed tomography (CT scan) represent the most used imaging methods for initial diagnosis of gallbladder tumors [31,32,33,34,35,36,37]; recent improvements in US imaging technologies (harmonics, compounding methods, speckle reduction imaging, microflow imaging, high-resolution US) has increased the accuracy of US examination and may even surpass CT scan for high-resolution US [36,38,39]. Asymmetric/focal wall thickening, discontinuity of wall layers, high mean flow velocity, and high shear wave velocity are associated with wall thickening-type of gallbladder carcinoma [31], while size over 10 mm, focal thickening of the gallbladder wall and incomplete wall beneath the lesion are associated with the polypoid-type [32]; however, 30% of gallbladder carcinomas have a size below 10 mm [35]. CT performed better than the US for intracholecystic papillary neoplasm [40]. In two systematic reviews of gallbladder polyps, the sensitivity and specificity for malignant polyps were 83.1% and 96.3% [33] and 79% and 89% [34]. The main problem for TUS is related to the accessibility of high-performance TUS in emergency settings (especially in suspected acute cholecystitis) when an accurate examination is not always available; in these situations, when a CT scan is not mandatory for the diagnosis of acute cholecystitis, some gallbladder carcinomas that mimic an acute inflammation may be missed.
CT and MRI remain the main imaging methods for the characterization of gallbladder neoplasms, with some studies showing that MRI may be preferred over CT scan, because of a higher soft tissue contrast resolution, with high-resolution T2W and arterial enhanced phase images helping to differentiate from chronic inflammation [41,42,43]. The differentiation between chronic xanthogranulomatous cholecystitis and gallbladder carcinoma may be challenging, regardless of the imaging method [42].
In our study, contrast-enhanced ultrasound (CEUS) was used for gallbladder carcinoma diagnosis in 5 cases; another case of presumed gallbladder carcinoma was not confirmed by surgery with pathological examination. CEUS was introduced in our hospital in the last 5 years; given that half of the cases of gallbladder carcinoma were not diagnosed preoperatively, and in other cases the diagnosis was established by CT scan or MRI, a large number of CEUS examinations in patients with gallbladder carcinoma are difficult to find. The main signs detected by CEUS in gallbladder carcinomas were irregular thickness of the gallbladder wall (3 patients) with heterogenous enhancement (2 patients), and surrounding tissue invasion (2 patients). The application of CEUS in the diagnosis of gallbladder carcinoma is still debatable [9]; the last guidelines of the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) and of Italian Society of Ultrasound in Medicine and Biology (SIUMB) stated that CEUS may be helpful for the differentiation between chronic cholecystitis and gallbladder carcinoma [9,44], and for the diagnosis of malignant polyps in delicate cases [45,46]. Several studies have analyzed the role of CEUS in the differential diagnosis of benign and malignant gallbladder lesions [10,13,23,43,47,48,49,50,51,52]. Irregular thickness of the gallbladder wall with heterogeneous enhancement and quick washout (fast in-fast out pattern), destroyed intactness of the gallbladder wall or surrounding tissue invasion, and a diffuse/branched type of contrast enhancement pattern were suggestive of malignancy; a quantitative analysis of CEUS parameters can help to the differentiation [53]. CEUS can make the contour of gallbladder lesions much clearer [10], with 94.1% sensitivity, 95.5% specificity, 80% PPV, and 98.8% NPV [10]. An accuracy of 92.2% was reported for malignant polypod lesions above 1 cm [47]; however, in small lesions below 1 cm, no advantage of CEUS compared to standard US was noted [47]. Moreover, hypo-enhancement or homogeneous enhancement was also recorded in malignant gallbladder lesions [47,54]. Several cutoff values between 35 and 60 seconds for washout time in malignant gallbladder lesions were proposed [47,55,56,57]. In two meta-analyses that analyzed the importance of CEUS for the detection and differentiation of gallbladder carcinoma [9,57], the pooled sensitivity, specificity, and AUC were 92%, 91%, 0.9689 [57], and 81%, 81%, and 0.9371, respectively [9]. Some lesions, such as xanthogranulomatous cholecystitis, adenomyomatosis, and adenoma, can mimic gallbladder carcinoma at imaging procedures [54]. In several studies, CEUS and CT scan accuracy were similar [58,59].
50% of our patients with gallbladder carcinomas were CDX2 positive; in a study published in 2005, 36.8% of gallbladder carcinomas have expressed CDX2 (with a higher expression in highly differentiated versus moderate or poorly differentiated adenocarcinoma) [15], whereas in other 2 studies, 45.4% and 29.3% of gallbladder carcinomas have expressed CDX2 [16,17]. The CDX2 expression was independently associated with better prognosis in several studies [16,17], and with lower T stage and smaller size in extrahepatic cholangiocarcinoma [14], while other studies did not show a correlation with clinicopathological factors such as papillary or tubular type, gallbladder, hepatic bed or vascular invasion, and lymph nodes positivity [15]. In our study, median survival was higher in patients negative for CDX2 (9.4 versus 3.4), although the statistical significance was not attained, possibly because of the small number of cases.
Surgery remains the only therapy associated with a definitive cure, although only a subset of gallbladder carcinoma may benefit from radical resection [60,61,62]. In our study, 27 of 40 patients (67.5%) had cholecystectomy, whereas in 11 cases only laparoscopy with biopsy was employed instead, and in 4 cases no surgery was performed. In two large studies in the USA, 40.6% had surgery nationwide between 2004 and 2016 [62], and in a single surgical center, 60.4% performed surgical exploration between 1992 and 2015, with 39.7% complete resection and 95.1% lymphadenectomies in patients with R0 resection [61]. The median survival in patients with surgical exploration was 19.6 months, and 5-year OS was 26%, and for patients with R0 resection, the median OS was 41.2 months, with 5-year OS of 43% [61]. The R0 resection (HR 0.25), incidental diagnosis (HR 0.51) had a lower risk of death, while those with jaundice at admission (HR 2.60) and positive lymph nodes (HR 2.47) had a higher risk of death [61]. In older studies, curative resection was possible in 1/3 of cases, with a 20% 5-year survival rate [26]. No patient had performed re-resection after index cholecystectomy in our study, but R0 resection was noted in 7 of 10 patients with occult carcinomas and 4 of 15 patients with cholecystectomy for pre- or intraoperative gallbladder carcinoma. The re-resection is particularly important in occult cases to remove any residual local tumor and adjacent lymph nodes [29]. A very low rate of lymphadenectomy was also recorded in our study ( 2 of 15 cases with pre- or intraoperative gallbladder carcinoma), but advanced disease or significant comorbidities preclude lymphadenectomy in most cases. Radical lymph node dissection and a significant number of harvested lymph nodes are associated with better survival rates [28].
Vascular, lymphatic, and perineural invasion is rarely encountered in early gallbladder carcinoma but is found in 71-97% of pT3 and pT4 tumors [30]. In our study, we noted lower rates compared to the literature data (42.9% for vascular, 25% for lymphatic, and 35.7% for perineural invasion). No prognostic role was found in the statistical analysis.
In our study, 4 cases of adenosquamous gallbladder carcinoma were found (10% of the total cases). Squamous gallbladder carcinoma represents rare tumors (3-5% of total gallbladder carcinoma in two large database studies) [7,8], with dismal prognostic as compared to gallbladder adenocarcinoma; the 1-year, 3-year, and 5-year overall survival were 43%, 23%, and 18% compared to 63%, 35%, and 25% [8], and the median overall survival 10.3 versus 20.5 months in one study [8] and 13 versus 29 months in another study [7]. In our study, all 4 adenosquamous carcinomas were discovered in III and IV stages and died within 3 months after diagnosis; no chemotherapy was administered. One of the two cases in which CDX2 immunostaining was performed was positive.
We noted several limitations to our study. The small size of the patient group, explained by the monocentric nature, can limit the generalizability of our findings; only a few cases have undergone CEUS. During the study, several ultrasound and CT scan devices were used for the diagnosis, and several physicians performed examinations, which can add heterogeneity to the interpretation. The retrospective nature of our study further limited the accuracy of the obtained findings because of the missing information. CDX2 immunostaining was limited to 10 cases, which limited the statistical analysis regarding the prognostic role. Low rates for lymphadenectomy may also impact survival. However, given that limited data regarding gallbladder carcinoma are currently available in our region, our study may add significant information about the main characteristics, diagnostic possibilities, and prognosis in this type of tumor.
5. Conclusions
We diagnosed 40 gallbladder carcinomas during the 8-year study period; 19 cases were diagnosed preoperatively as acute or chronic cholecystitis, and in 10 cases, the diagnosis at discharge was the same. The accuracy of transabdominal ultrasound and CT scan was similar; contrast-enhanced ultrasound was used in 4 cases and helped to differentiate between GBC and acute or chronic inflammation. The CDX2 can represent a prognostic marker in gallbladder carcinoma. Despite technical progress regarding diagnosis by videocapsule endoscopy, CT scan, and MRI, an early diagnosis and treatment of gallbladder tumors is hard to accomplish, especially in cases with late diagnosis, and because of the low rates of radical cholecystectomy.
Author Contributions
Conceptualization, SM.C, DN.F, and LD.S.; methodology, SM.C, S.R, and L.S.; software, A.TS, SM.C, and AA.R.; validation, CV.O, A.TS, and LD.S.; formal analysis, MM.F, CV.O, and L.S.; investigation, MM.F, AA.R, CV.O, and A.D.; resources, MM.F, LD.S, S.R.; data curation, A.TS, LD.S, and DN.F.; writing—original draft preparation, SM.C, MM.F, LD.S, and DN.F.; writing—review and editing, SM.C, LD.S, and DN.F.; visualization, SM.C, A.D, and DN.F.; supervision, LD.S, S.R, and MM.F.; project administration, SM.C, LD.S, and DN.F. All authors have read and agreed to the published version of the manuscript.
Funding
The article processing charges were funded by the University of Medicine and Pharmacy of Craiova, Romania.
Institutional Review Board Statement
This study was approved on 19 April 2023 by the Institutional Review Board (IRB) at the Clinical County Emergency Hospital of Craiova (Comisia de Etica a Spitalului Clinic Judetean de Urgentă Craiova) (approval No. 14090/27.03.2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pavlidis, E.T.; Galanis, I.N.; Pavlidis, T.E. New trends in diagnosis and management of gallbladder carcinoma. World J Gastrointest Oncol. 2024, 16, 13–29. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.N.; Jain, S.; Dixit, R. Gallbladder carcinoma: Aggressive malignancy with protean loco-regional and distant spread. World J Clin Cases. 2015, 3, 231–44. [Google Scholar] [CrossRef] [PubMed]
- Miao, W.; Liu, F.; Guo, Y.; Zhang, R.; Wang, Y.; Xu, J. Research progress on prognostic factors of gallbladder carcinoma. J Cancer Res Clin Oncol. 2024, 150, 447. [Google Scholar] [CrossRef] [PubMed]
- Inui, K.; Yoshino, J.; Miyoshi, H. Diagnosis of gallbladder tumors. Intern Med. 2011, 50, 1133–6. [Google Scholar] [CrossRef]
- Goetze, T.O. Gallbladder carcinoma: Prognostic factors and therapeutic options. World J Gastroenterol. 2015, 21, 12211–7. [Google Scholar] [CrossRef]
- Lv, T.R.; Wang, J.K.; Li, F.Y.; Hu, H.J. Prognostic factors for resected cases with gallbladder carcinoma: a systematic review and meta-analysis. Int J Surg. 2024, 110, 4342–4355. [Google Scholar] [CrossRef]
- Ayabe, R.I.; Wach, M.M.; Ruff, S.M.; Diggs, L.P.; Martin, S.P.; Wiemken, T.; Hinyard, L.; Davis, J.L.; Luu, C.; Hernandez, J.M. Gallbladder squamous cell carcinoma: An analysis of 1084 cases from the National Cancer Database. J Surg Oncol. 2020, 122, 716–722. [Google Scholar] [CrossRef]
- Murimwa G, Hester C, Mansour JC, Polanco PM, Porembka MR, Wang SC, Zeh HJ Jr, Yopp AC. Comparative Outcomes of Adenosquamous Carcinoma of the Gallbladder: an Analysis of the National Cancer Database. J Gastrointest Surg. 2021, 25, 1815–1827. [CrossRef]
- Cheng, Y.; Wang, M.; Ma, B.; Ma, X. Potential role of contrast-enhanced ultrasound for the differentiation of malignant and benign gallbladder lesions in East Asia: A meta-analysis and systematic review. Medicine (Baltimore). 2018, 97, e11808. [Google Scholar] [CrossRef]
- Zhang, H.P.; Bai, M.; Gu, J.Y.; He, Y.Q.; Qiao, X.H.; Du, L.F. Value of contrast-enhanced ultrasound in the differential diagnosis of gallbladder lesions. World J Gastroenterol. 2018, 24, 744–751. [Google Scholar] [CrossRef]
- Ciocalteu, A.; Iordache, S.; Cazacu, S.M.; Urhut, C.M.; Sandulescu, S.M.; Ciurea, A.M.; Saftoiu, A.; Sandulescu, L.D. Role of Contrast-Enhanced Ultrasonography in Hepatocellular Carcinoma by Using LI-RADS and Ancillary Features: A Single Tertiary Centre Experience. Diagnostics (Basel). 2021, 11, 2232. [Google Scholar] [CrossRef] [PubMed]
- Urhuț, M.C.; Săndulescu, L.D.; Streba, C.T.; Mămuleanu, M.; Ciocâlteu, A.; Cazacu, S.M.; Dănoiu, S. Diagnostic Performance of an Artificial Intelligence Model Based on Contrast-Enhanced Ultrasound in Patients with Liver Lesions: A Comparative Study with Clinicians. Diagnostics (Basel). 2023, 13, 3387. [Google Scholar] [CrossRef]
- Gerstenmaier, J.F.; Hoang, K.N.; Gibson, R.N. Contrast-enhanced ultrasound in gallbladder disease: a pictorial review. Abdom Radiol (NY). 2016, 41, 1640–52. [Google Scholar] [CrossRef] [PubMed]
- Jinawath, A.; Akiyama, Y.; Yuasa, Y.; Pairojkul, C. Expression of phosphorylated ERK1/2 and homeodomain protein CDX2 in cholangiocarcinoma. J Cancer Res Clin Oncol. 2006, 132, 805–10. [Google Scholar] [CrossRef]
- Wu, X.S.; Akiyama, Y.; Igari, T.; Kawamura, T.; Hiranuma, S.; Shibata, T.; Tsuruta, K.; Koike, M.; Arii, S.; Yuasa, Y. Expression of homeodomain protein CDX2 in gallbladder carcinomas. J Cancer Res Clin Oncol. 2005, 131, 271–8. [Google Scholar] [CrossRef]
- Li, Q.L.; Yang, Z.L.; Liu, J.Q.; Miao, X.Y. Expression of CDX2 and hepatocyte antigen in benign and malignant lesions of gallbladder and its correlation with histopathologic type and clinical outcome. Pathol Oncol Res. 2011, 17, 561–8. [Google Scholar] [CrossRef]
- Chang, Y.T.; Hsu, C.; Jeng, Y.M.; Chang, M.C.; Wei, S.C.; Wong, J.M. Expression of the caudal-type homeodomain transcription factor CDX2 is related to clinical outcome in biliary tract carcinoma. J Gastroenterol Hepatol. 2007, 22, 389–94. [Google Scholar] [CrossRef]
- Graur, F.; Mois, E.; Margarit, S.; Hagiu, C.; Al Hajjar, N. Gallbladder carcinoma. Surgical management of gallbladder carcinoma. An analysis of 37 cases. Ann Ital Chir. 2018, 89, 501–506. [Google Scholar]
- Vlad, L.; Osian, G.; Iancu, C.; Munteanu, D.; Mirică, A.; Furcea, L. Gallbladder carcinoma. A clinical study of a series of 38 cases. Rom J Gastroenterol. 2003, 12, 199–202 PMID: 14502320. [Google Scholar] [PubMed]
- Neculoiu, D.; Neculoiu, L.C.; Popa, R.M.; Manea, R.M. The Many Hidden Faces of Gallbladder Carcinoma on CT and MRI Imaging-From A to Z. Diagnostics (Basel). 2024, 14, 475. [Google Scholar] [CrossRef]
- Constantin, A.; Achim, F.; Turcu, T.; Birceanu, A.; Evsei, A.; Socea, B.; Predescu, D. Giant Gallbladder Tumor, Unusual Cancer-Case Report and Short Review of Literature. Diagnostics (Basel). 2023, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Chiorean, L.; Bartos, A.; Pelau, D.; Iancu, D.; Ciuleanu, T.; Buiga, R.; Oancea, I.; Mangrau, A.; Iancu, C.; Badea, R. Neuroendocrine tumor of gallbladder with liver and retroperitoneal metastases and a good response to the chemotherapeutical treatment. J Med Ultrason (2001). 2015, 42, 271–6. [Google Scholar] [CrossRef]
- Zhu, L.; Li, N.; Zhu, Y.; Han, P.; Jiang, B.; Li, M.; Luo, Y.; Clevert, D.A.; Fei, X. Value of high frame rate contrast enhanced ultrasound in gallbladder wall thickening in non-acute setting. Cancer Imaging. 2024, 24, 7. [Google Scholar] [CrossRef]
- Weerakkody, Y.; Yap, J.; Luong, D.; Knipe, H.; Mukherjee, A. Gallbladder cancer (staging - AJCC 8th edition). Reference article, Radiopaedia.org (Accessed on 16 Apr 2025). [CrossRef]
- Spaziani, E.; Di Cristofano, C.; Di Filippo, A.R.; Caruso, G.; Orelli, S.; Spaziani, M.; Fiori, E.; Picchio, M.; De Cesare, A. Polypoid lesions of the gallbladder in a consecutive series of 2631 patients. A single-center experience. Ann Ital Chir. 2019, 90, 305–310. [Google Scholar]
- Schauer, R.J.; Meyer, G.; Baretton, G.; Schildberg, F.W.; Rau, H.G. Prognostic factors and long-term results after surgery for gallbladder carcinoma: a retrospective study of 127 patients. Langenbecks Arch Surg. 2001, 386, 110–7. [Google Scholar] [CrossRef]
- Murakami, Y.; Uemura, K.; Sudo, T.; Hashimoto, Y.; Nakashima, A.; Kondo, N.; Sakabe, R.; Kobayashi, H.; Sueda, T. Prognostic factors of patients with advanced gallbladder carcinoma following aggressive surgical resection. J Gastrointest Surg. 2011, 15, 1007–16. [Google Scholar] [CrossRef]
- Liu, G.J.; Li, X.H.; Chen, Y.X.; Sun, H.D.; Zhao, G.M.; Hu, S.Y. Radical lymph node dissection and assessment: Impact on gallbladder cancer prognosis. World J Gastroenterol. 2013, 19, 5150–8. [Google Scholar] [CrossRef]
- Vega EA, De Aretxabala X, Qiao W, Newhook TE, Okuno M, Castillo F, Sanhueza M, Diaz C, Cavada G, Jarufe N, et al. Comparison of oncological outcomes after open and laparoscopic re-resection of incidental gallbladder cancer. Br J Surg. 2020, 107, 289–300. [CrossRef]
- Kijima, H.; Wu, Y.; Yosizawa, T.; Suzuki, T.; Tsugeno, Y.; Haga, T.; Seino, H.; Morohashi, S.; Hakamada, K. Pathological characteristics of early to advanced gallbladder carcinoma and extrahepatic cholangiocarcinoma. J Hepatobiliary Pancreat Sci. 2014, 21, 453–8. [Google Scholar] [CrossRef]
- Gupta, P.; Marodia, Y.; Bansal, A.; Kalra, N. ; Kumar-MP; Sharma, V. ; Dutta, U.; Sandhu, M.S. Imaging-based algorithmic approach to gallbladder wall thickening. World J Gastroenterol. 2020, 26, 6163–6181. [Google Scholar] [CrossRef]
- Wu, C.H.; Luo, Y.; Fei, X.; Chou, Y.H.; Chiou, H.J.; Wang, H.K.; Lai, Y.C.; Lin, Y.H.; Tiu, C.M.; Wang, J. Algorithmic approaches to the diagnosis of gallbladder intraluminal lesions on ultrasonography. J Chin Med Assoc. 2018, 81, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Martin, E.; Gill, R.; Debru, E. Diagnostic accuracy of transabdominal ultrasonography for gallbladder polyps: systematic review. Can J Surg. 2018, 61, 200–207. [Google Scholar] [CrossRef]
- Wennmacker, S.Z.; Lamberts, M.P.; Di Martino, M.; Drenth, J.P.; Gurusamy, K.S.; van Laarhoven, C.J. Transabdominal ultrasound and endoscopic ultrasound for diagnosis of gallbladder polyps. Cochrane Database Syst Rev. 2018, 8, CD012233. [Google Scholar] [CrossRef]
- Okaniwa, S. How Can We Manage Gallbladder Lesions by Transabdominal Ultrasound? Diagnostics (Basel). 2021, 11, 784. [Google Scholar] [CrossRef]
- Bang, S.H.; Lee, J.Y.; Woo, H.; Joo, I.; Lee, E.S.; Han, J.K.; Choi, B.I. Differentiating between adenomyomatosis and gallbladder cancer: revisiting a comparative study of high-resolution ultrasound, multidetector CT, and MR imaging. Korean J Radiol. 2014, 15, 226–34. [Google Scholar] [CrossRef]
- Tao, J.; Zhang, Y.; Chen, H.; Wang, S.; Sun, Q.; Zhang, W.; Liu, Q.; Mai, X.; Yu, D. Triphasic dynamic contrast-enhanced computed tomography predictive model of benign and malignant risk of gallbladder occupying lesions. Medicine (Baltimore). 2020, 99, e19539. [Google Scholar] [CrossRef]
- Jang, J.Y.; Kim, S.W.; Lee, S.E.; Hwang, D.W.; Kim, E.J.; Lee, J.Y.; Kim, S.J.; Ryu, J.K.; Kim, Y.T. Differential diagnostic and staging accuracies of high resolution ultrasonography, endoscopic ultrasonography, and multidetector computed tomography for gallbladder polypoid lesions and gallbladder cancer. Ann Surg. 2009, 250, 943–9. [Google Scholar] [CrossRef]
- Zhu L, Han P, Jiang B, Li N, Fei X. [Differential diagnosis of gallbladder polypoid lesions by micro-flow imaging]. Nan Fang Yi Ke Da Xue Xue Bao. 2022, 42, 922–928 Chinese. [CrossRef]
- Kim, J.H.; Kim, J.H.; Kang, H.J.; Bae, J.S. Contrast-Enhanced CT and Ultrasonography Features of Intracholecystic Papillary Neoplasm with or without associated Invasive Carcinoma. Korean J Radiol. 2023, 24, 39–50. [Google Scholar] [CrossRef]
- Kalage, D.; Gupta, P.; Gulati, A.; Reddy, K.P.; Sharma, K.; Thakur, A.; Yadav, T.D.; Gupta, V.; Kaman, L.; Nada, R.; Singh, H.; Irrinki, S.; Gupta, P.; Das, C.K.; Dutta, U.; Sandhu, M. Contrast Enhanced CT Versus MRI for Accurate Diagnosis of Wall-thickening Type Gallbladder Cancer. J Clin Exp Hepatol. 2024, 14, 101397. [Google Scholar] [CrossRef]
- Kalra, N.; Gupta, P.; Singhal, M.; Gupta, R.; Gupta, V.; Srinivasan, R.; Mittal, B.R.; Dhiman, R.K.; Khandelwal, N. Cross-sectional Imaging of Gallbladder Carcinoma: An Update. J Clin Exp Hepatol. 2019, 9, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Liu LN, Xu HX, Lu MD, Xie XY, Wang WP, Hu B, Yan K, Ding H, Tang SS, Qian LX, et al. Contrast-enhanced ultrasound in the diagnosis of gallbladder diseases: a multi-center experience. PLoS One. 2012, 7, e48371. [CrossRef]
- de Sio I, D'Onofrio M, Mirk P, Bertolotto M, Priadko K, Schiavone C, Cantisani V, Iannetti G, Vallone G, Vidili G; SIUMB experts committee. SIUMB recommendations on the use of ultrasound in neoplastic lesions of the gallbladder and extrahepatic biliary tract. J Ultrasound. 2023, 26, 725–731. [CrossRef]
- Foley, K.G.; Lahaye, M.J.; Thoeni, R.F.; Soltes, M.; Dewhurst, C.; Barbu, S.T.; Vashist, Y.K.; Rafaelsen, S.R.; Arvanitakis, M.; Perinel, J.; et al. Management follow-up of gallbladder polyps: updated joint guidelines between the, E. S.G.A.R.; EAES; EFISDS; ESGE Eur Radiol. 2022, 32, 3358–3368. [Google Scholar] [CrossRef]
- Sparchez, Z.; Radu, P. Role of CEUS in the diagnosis of gallbladder disease. Med Ultrason. 2012, 14, 326–30 PMID: 23243646. [Google Scholar] [PubMed]
- Zhang, X.; Tang, S.; Huang, L.; Jin, H.; Wang, Y.; Wang, Y.; Liu, Z.; Lu, C. Value of contrast-enhanced ultrasound in diagnosis and differential diagnosis of polypoid lesions of gallbladder ≥ 1 cm. BMC Gastroenterol. 2022, 22, 354. [Google Scholar] [CrossRef]
- Hattori M, Inui K, Yoshino J, Miyoshi H, Okushima K, Nakamura Y, Naito T, Imaeda Y, Horibe Y, Hattori T, et al. [Usefulness of contrast-enhanced ultrasonography in the differential diagnosis of polypoid gallbladder lesions]. Nihon Shokakibyo Gakkai Zasshi. 2007, 104, 790–8 Japanese (Abstract).
- Zheng SG, Xu HX, Liu LN, Lu MD, Xie XY, Wang WP, Hu B, Yan K, Ding H, Tang SS, et al. Contrast-enhanced ultrasound versus conventional ultrasound in the diagnosis of polypoid lesion of gallbladder: a multi-center study of dynamic microvascularization. Clin Hemorheol Microcirc. 2013, 55, 359–74. [CrossRef]
- Miwa H, Numata K, Sugimori K, Sanga K, Hirotani A, Tezuka S, Goda Y, Irie K, Ishii T, Kaneko T, et al. Differential diagnosis of gallbladder polypoid lesions using contrast-enhanced ultrasound. Abdom Radiol (NY). 2019, 44, 1367–1378. [CrossRef]
- Liu, X.S.; Gu, L.H.; Du, J.; Li, F.H.; Wang, J.; Chen, T.; Zhang, Y.H. Differential diagnosis of polypoid lesions of the gallbladder using contrast-enhanced sonography. J Ultrasound Med. 2015, 34, 1061–9. [Google Scholar] [CrossRef]
- Xu JM, Guo LH, Xu HX, Zheng SG, Liu LN, Sun LP, Lu MD, Wang WP, Hu B, Yan K, et al. Differential diagnosis of gallbladder wall thickening: the usefulness of contrast-enhanced ultrasound. Ultrasound Med Biol. 2014, 40, 2794–804. [CrossRef]
- Bae JS, Kim SH, Kang HJ, Kim H, Ryu JK, Jang JY, Lee SH, Paik WH, Kwon W, Lee JY, et al. Quantitative contrast-enhanced US helps differentiating neoplastic vs non-neoplastic gallbladder polyps. Eur Radiol. 2019, 29, 3772–3781. [CrossRef]
- Kong, W.T.; Shen, H.Y.; Qiu, Y.D.; Han, H.; Wen, B.J.; Wu, M. Application of contrast enhanced ultrasound in gallbladder lesion: is it helpful to improve the diagnostic capabilities? Med Ultrason. 2018, 20, 420–426. [Google Scholar] [CrossRef]
- Xie XH, Xu HX, Xie XY, Lu MD, Kuang M, Xu ZF, Liu GJ, Wang Z, Liang JY, Chen LD, et al. Differential diagnosis between benign and malignant gallbladder diseases with real-time contrast-enhanced ultrasound. Eur Radiol. 2010, 20, 239–48. [CrossRef]
- Serra C, Felicani C, Mazzotta E, Gabusi V, Grasso V, De Cinque A, Giannitrapani L, Soresi M. CEUS in the differential diagnosis between biliary sludge, benign lesions and malignant lesions. J Ultrasound. 2018, 21, 119–126. [CrossRef]
- Wang, W.; Fei, Y.; Wang, F. Meta-analysis of contrast-enhanced ultrasonography for the detection of gallbladder carcinoma. Med Ultrason. 2016, 18, 281–28. [Google Scholar] [CrossRef]
- Yuan, Z.; Liu, X.; Li, Q.; Zhang, Y.; Zhao, L.; Li, F.; Chen, T. Is Contrast-Enhanced Ultrasound Superior to Computed Tomography for Differential Diagnosis of Gallbladder Polyps? A Cross-Sectional Study. Front Oncol. 2021, 11, 657223. [Google Scholar] [CrossRef]
- Inoue, T.; Kitano, M.; Kudo, M.; Sakamoto, H.; Kawasaki, T.; Yasuda, C.; Maekawa, K. Diagnosis of gallbladder diseases by contrast-enhanced phase-inversion harmonic ultrasonography. Ultrasound Med Biol. 2007, 33, 353–61. [Google Scholar] [CrossRef]
- Sun, J.; Xie, T.G.; Ma, Z.Y.; Wu, X.; Li, B.L. Current status and progress in laparoscopic surgery for gallbladder carcinoma. World J Gastroenterol. 2023, 29, 2369–2379. [Google Scholar] [CrossRef]
- Creasy JM, Goldman DA, Gonen M, Dudeja V, O'Reilly EM, Abou-Alfa GK, Cercek A, Harding JJ, Balachandran VP, Drebin JA, et al. Evolution of surgical management of gallbladder carcinoma and impact on outcome: results from two decades at a single institution. HPB (Oxford). 2019, 21, 1541–1551. [CrossRef]
- Maegawa, F.B.; Ashouri, Y.; Hamidi, M.; Hsu, C.H.; Riall, T.S. Gallbladder Cancer Surgery in the United States: Lymphadenectomy Trends and Impact on Survival. J Surg Res. 2021, 258, 54–63. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The flow chart shows the inclusion of gallbladder carcinoma.
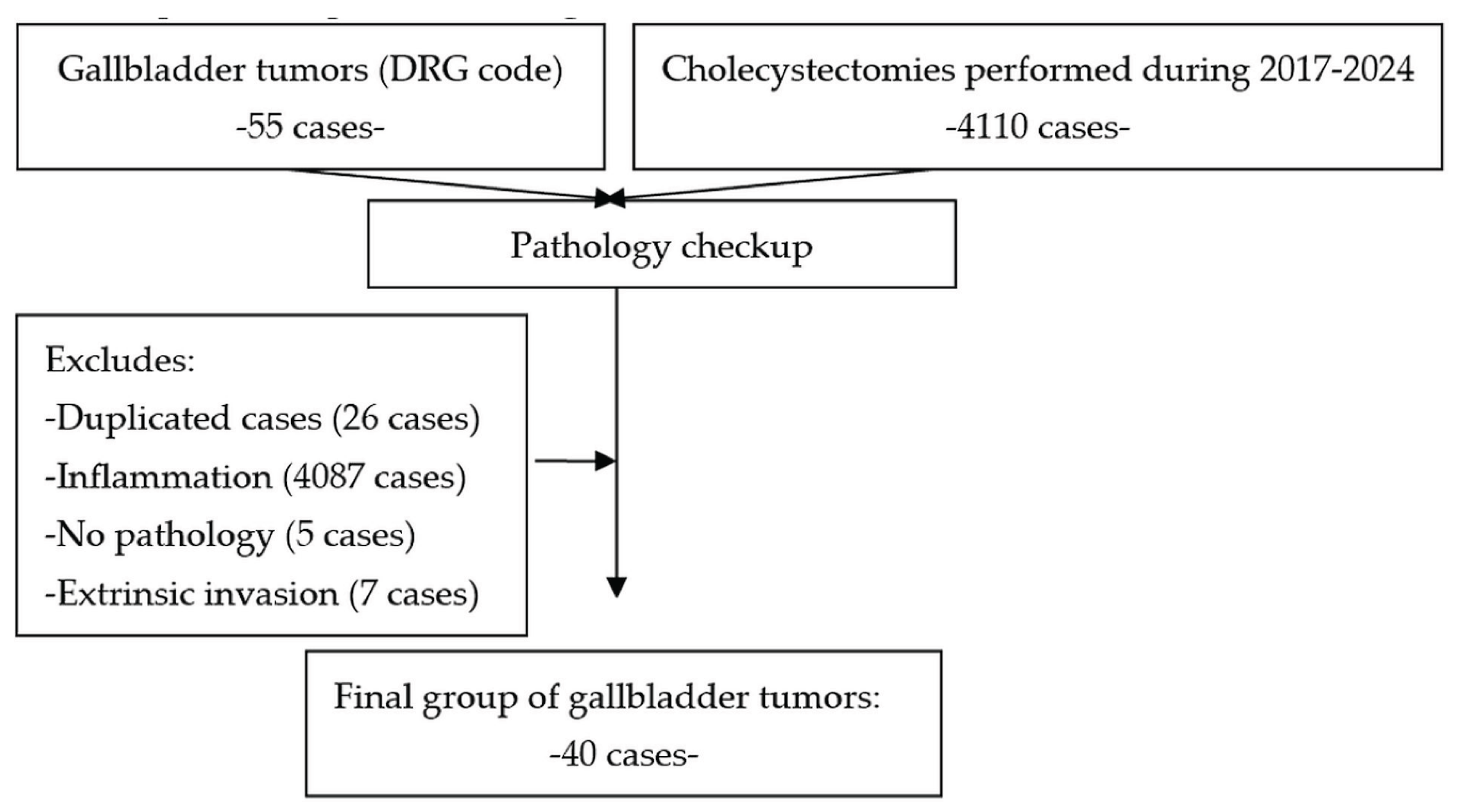
Figure 2.
Native CT scan showing a 4 cm gallbladder mass (white arrow). Cholecystectomy with pathology exam confirmed the diagnosis of T1N0 gallbladder carcinoma (case 1).
Figure 2.
Native CT scan showing a 4 cm gallbladder mass (white arrow). Cholecystectomy with pathology exam confirmed the diagnosis of T1N0 gallbladder carcinoma (case 1).
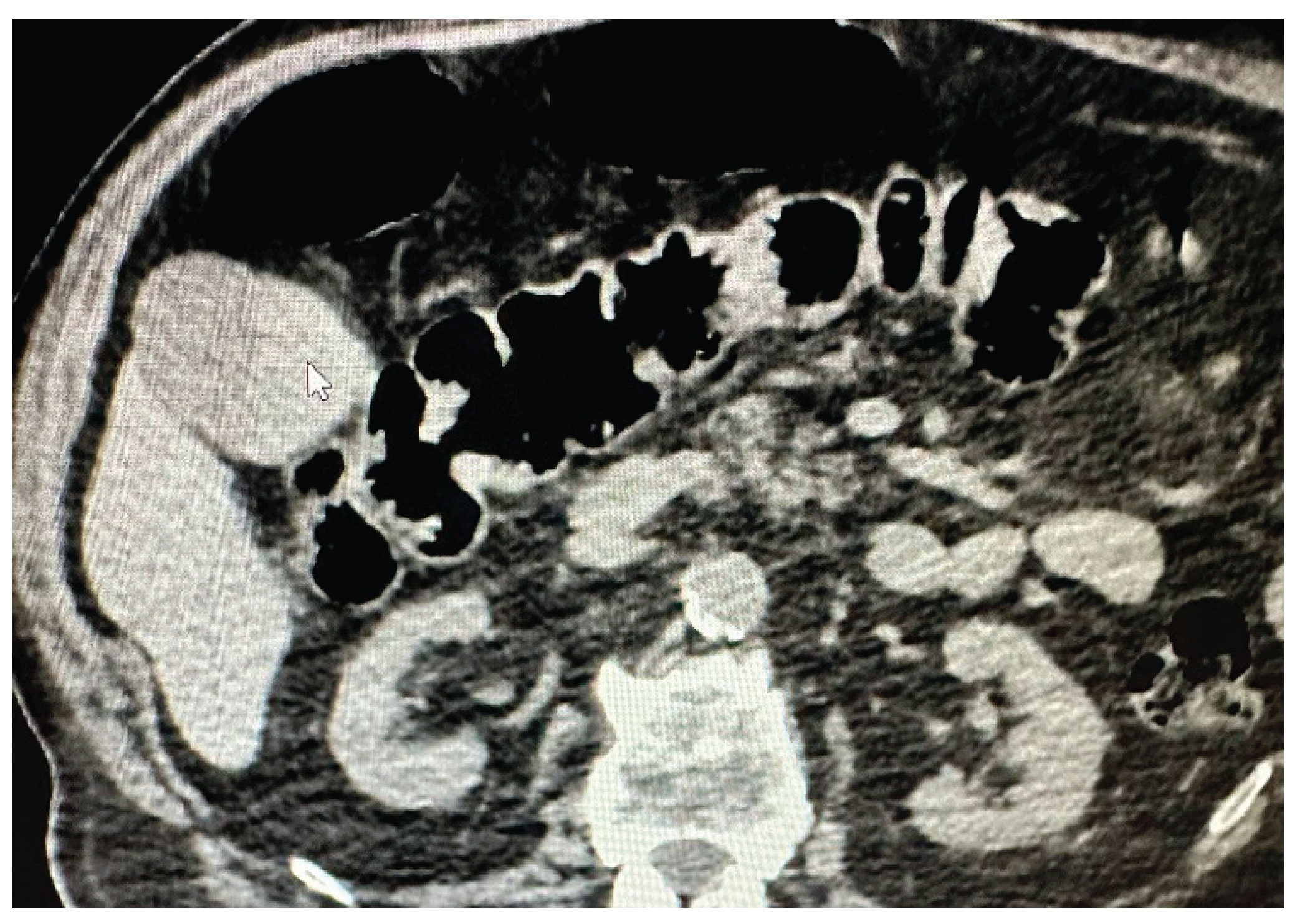
Figure 3.
Postcontrast CT scan (case 1): moderate enhancement of gallbladder mass (black arrows).
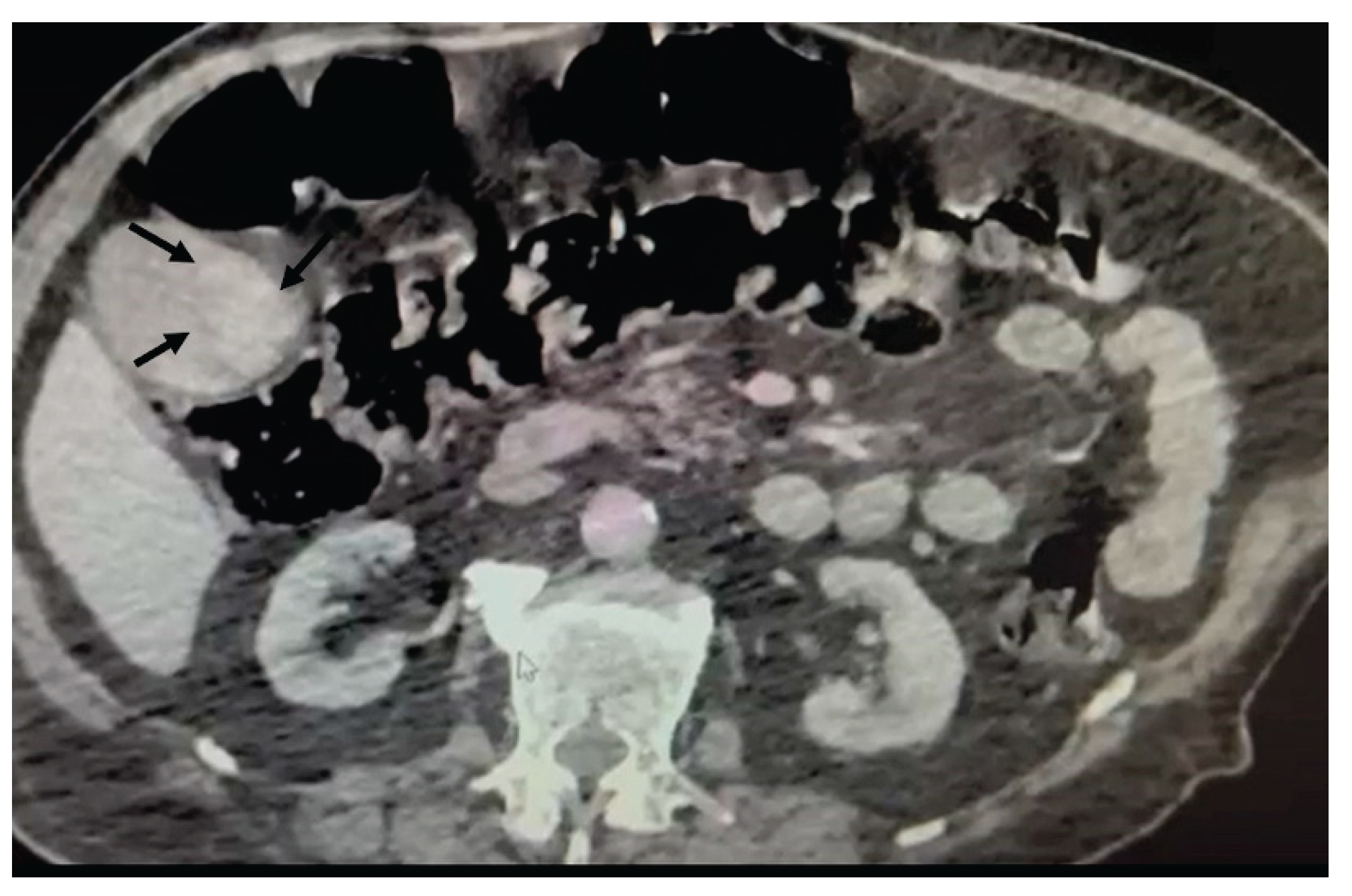
Figure 4.
CT scan (arterial phase): an advanced gallbladder carcinoma (black arrows) with central enhancement (white spot). Laparoscopy with biopsy was performed (case 2).
Figure 4.
CT scan (arterial phase): an advanced gallbladder carcinoma (black arrows) with central enhancement (white spot). Laparoscopy with biopsy was performed (case 2).
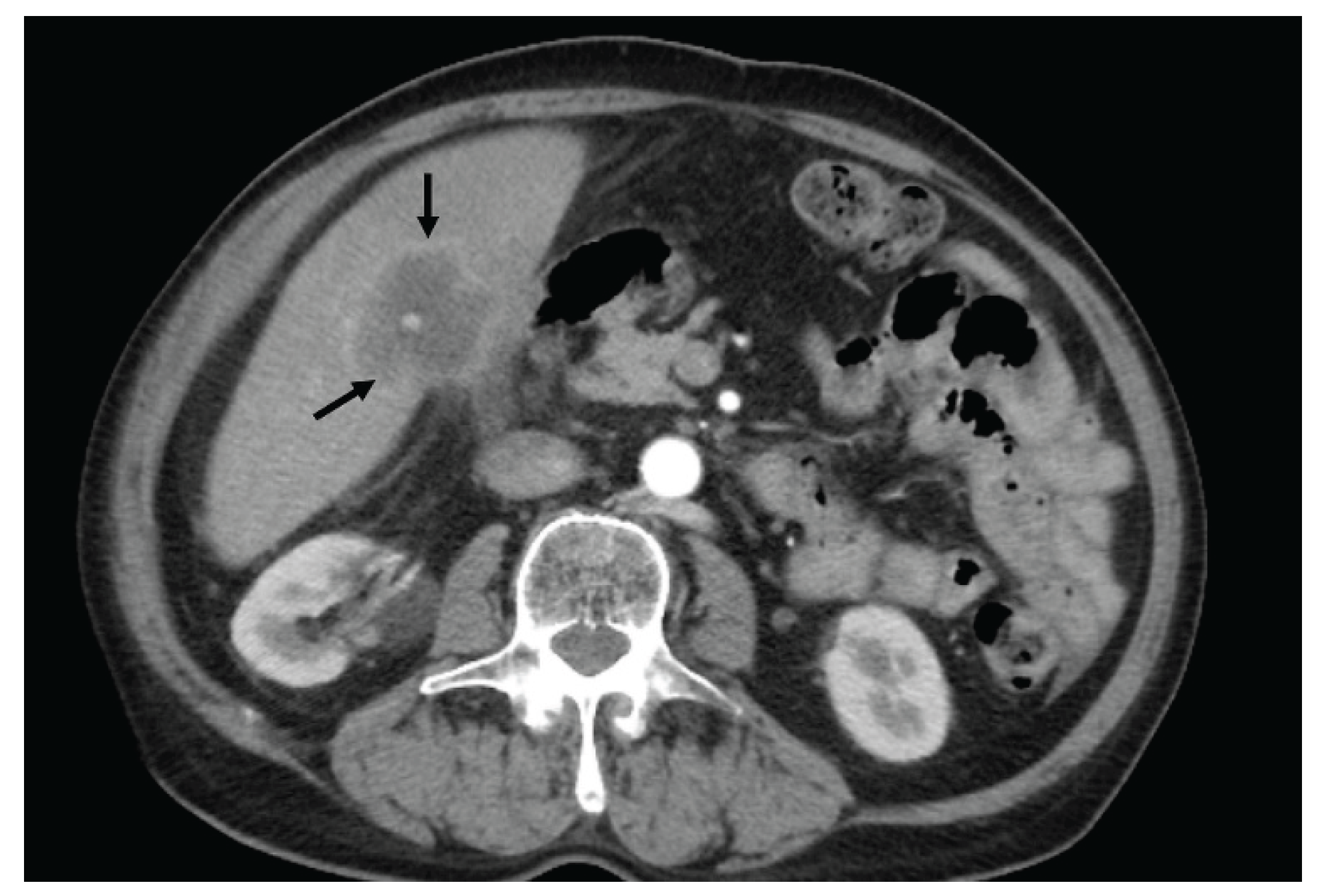
Figure 5.
CT scan: no washout during venous phase in gallbladder mass (case 2).

Figure 6.
TUS: gray-scale examination (case 2). An ill-defined mass in the gallbladder fossa, isoechoic to the liver, heterogeneous, with intralesional hyperechoic foci (gallstones). The anterior wall is ill-defined, due to the invasion of the adjacent hepatic parenchyma. The gallbladder is completely replaced by the malignant mass.
Figure 6.
TUS: gray-scale examination (case 2). An ill-defined mass in the gallbladder fossa, isoechoic to the liver, heterogeneous, with intralesional hyperechoic foci (gallstones). The anterior wall is ill-defined, due to the invasion of the adjacent hepatic parenchyma. The gallbladder is completely replaced by the malignant mass.
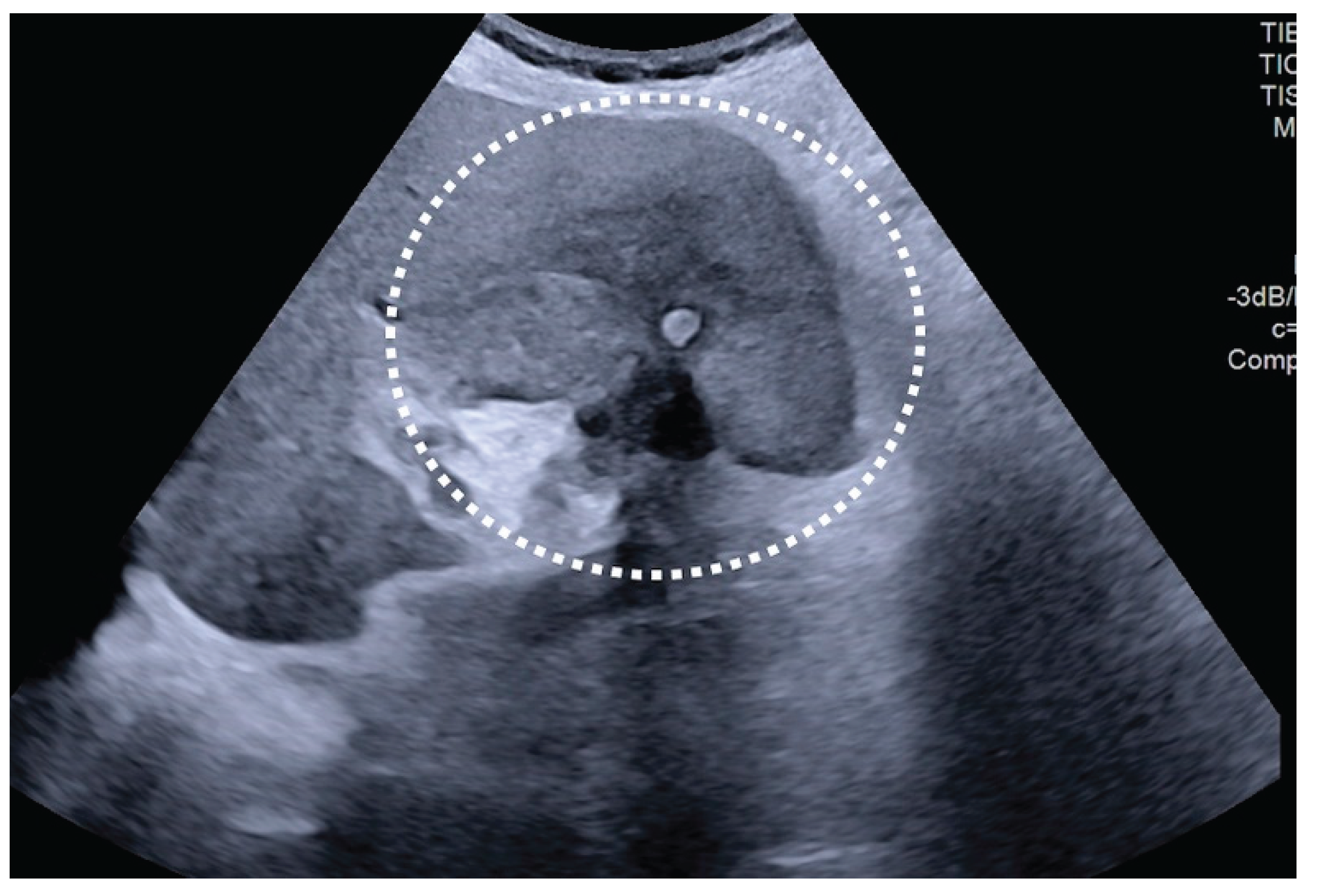
Figure 7.
TUS and CEUS examination: arterial phase (case 2). Moderate and heterogeneous enhancement of the gallbladder mass, with a small central non-enhancing zone (arrow).
Figure 7.
TUS and CEUS examination: arterial phase (case 2). Moderate and heterogeneous enhancement of the gallbladder mass, with a small central non-enhancing zone (arrow).
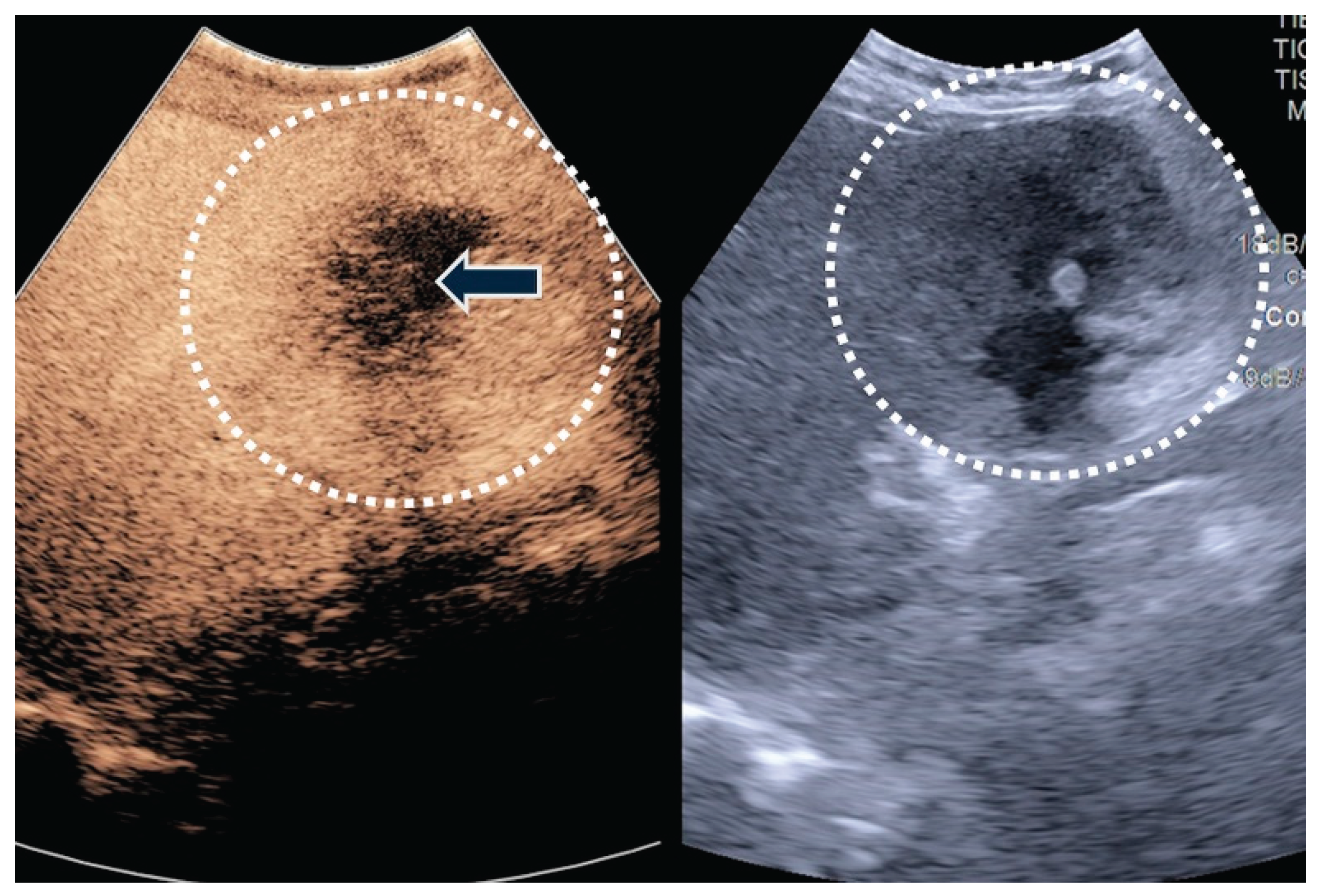
Figure 8.
TUS and CEUS examination (case 2): In the late phase, complete and rapid washout of the gallbladder mass is noted.
Figure 8.
TUS and CEUS examination (case 2): In the late phase, complete and rapid washout of the gallbladder mass is noted.
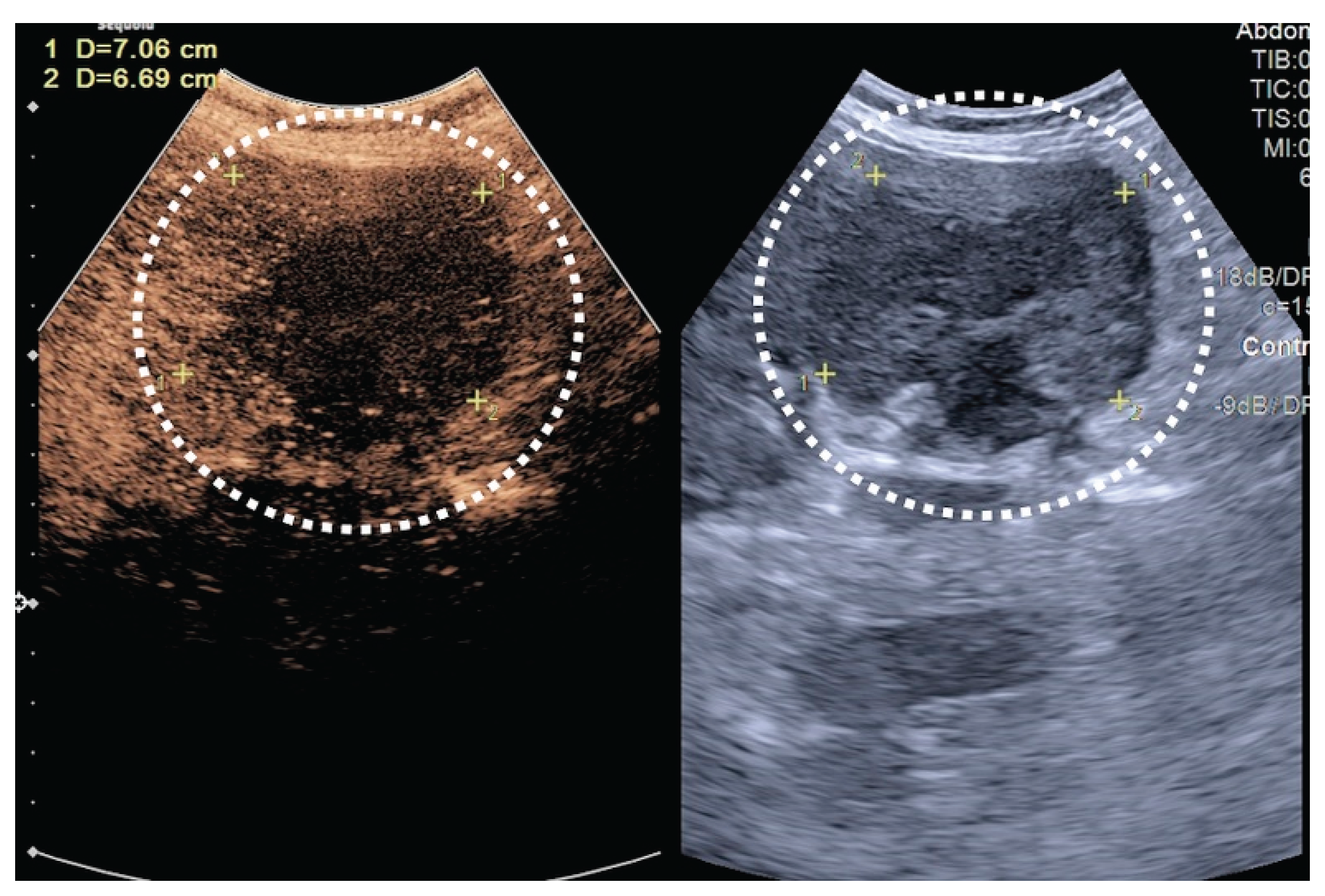
Figure 9.
TUS: gray-scale examination (case 3). A heterogeneous gallbladder mass adherent to the posterior wall, with invasion of the adjacent hilum (arrows).
Figure 9.
TUS: gray-scale examination (case 3). A heterogeneous gallbladder mass adherent to the posterior wall, with invasion of the adjacent hilum (arrows).
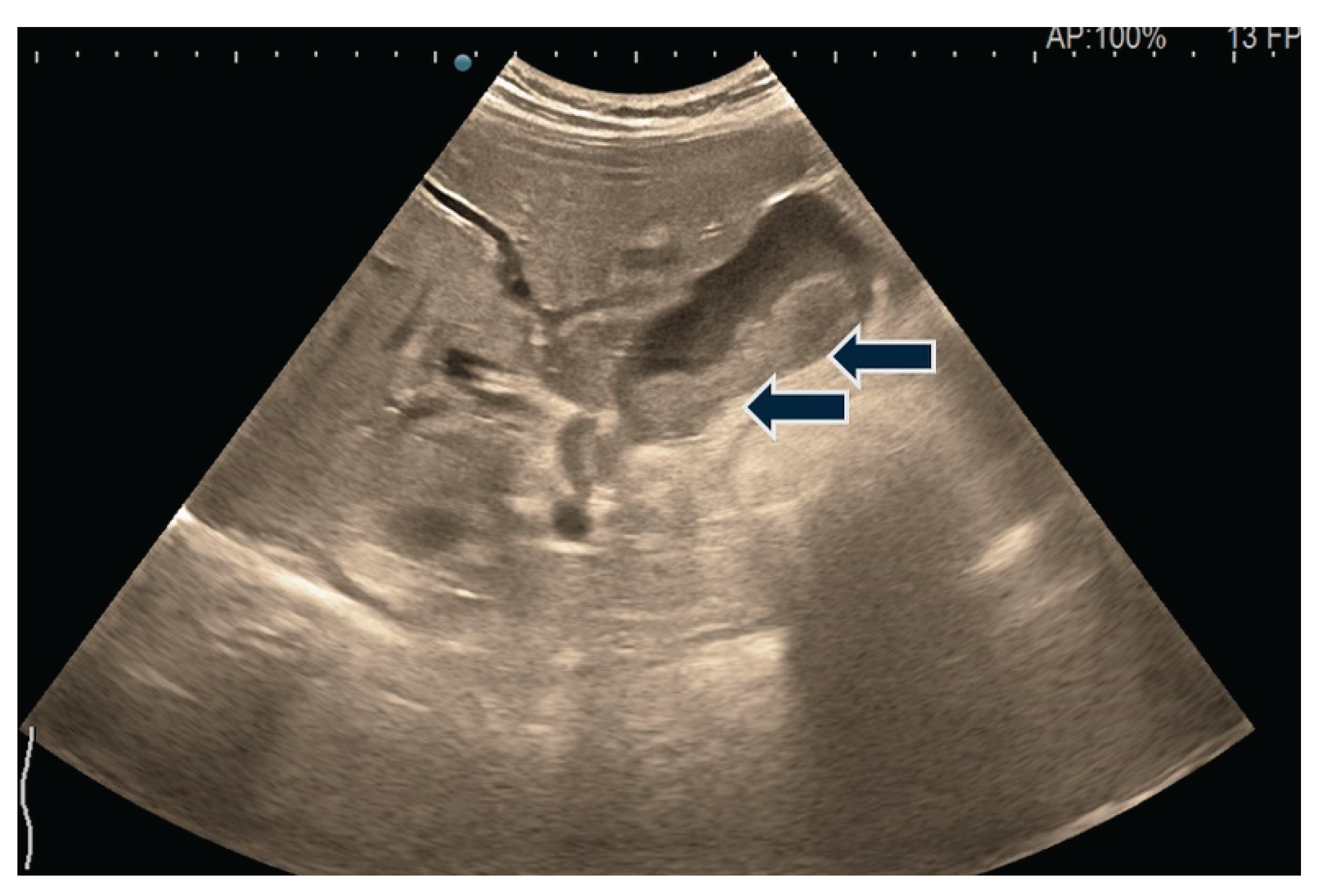
Figure 10.
After the injection of 2.4 ml SonoVue, in the arterial phase, the posterior gallbladder wall is hyperenhanced and thickened (the tumoral component of the gallbladder mass) while the image of the biliary sludge shows no contrast uptake.
Figure 10.
After the injection of 2.4 ml SonoVue, in the arterial phase, the posterior gallbladder wall is hyperenhanced and thickened (the tumoral component of the gallbladder mass) while the image of the biliary sludge shows no contrast uptake.
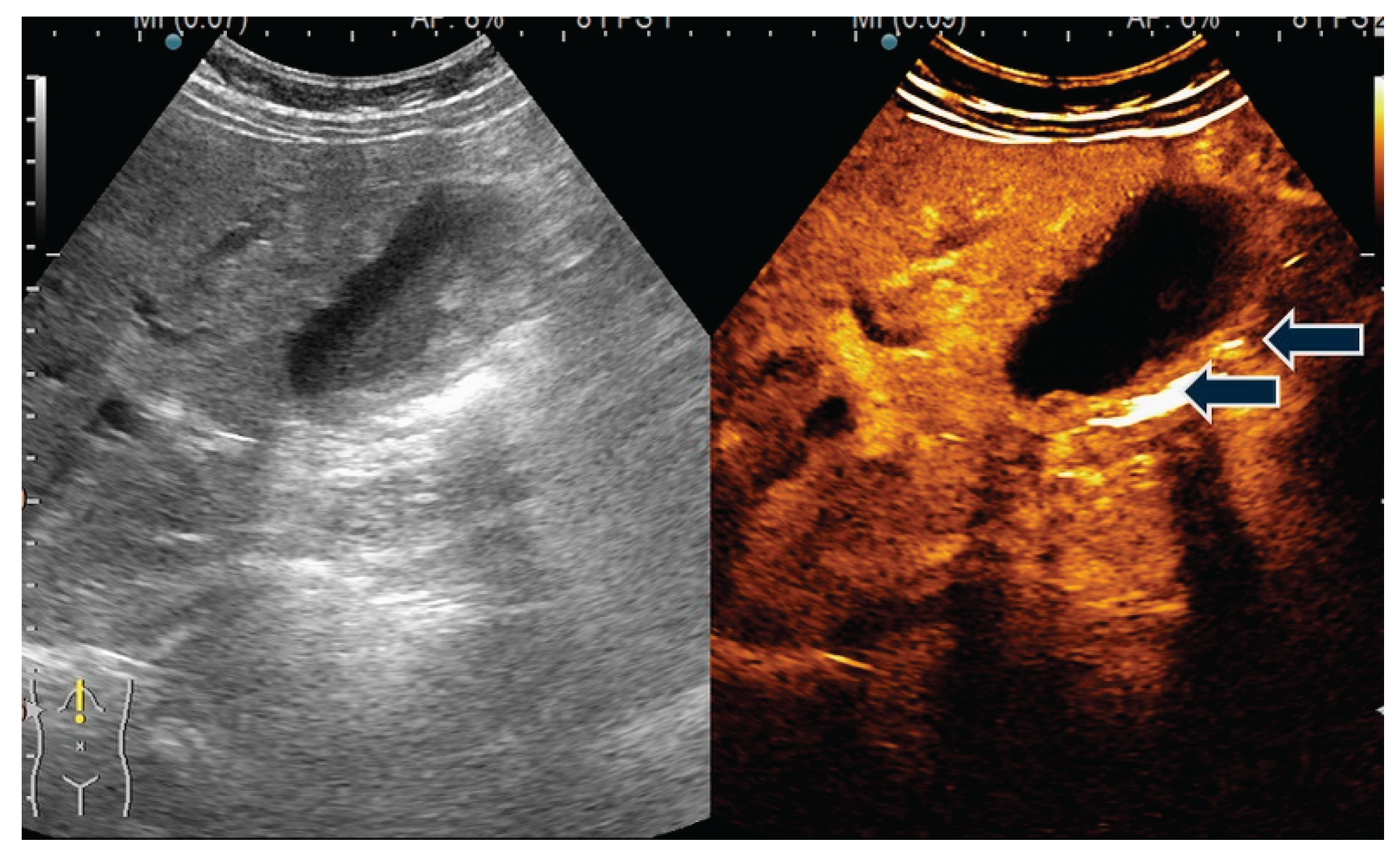
Figure 11.
In the late phase, the wash-out of the tumoral component of the gallbladder mass is observed, suggestive of malignancy.
Figure 11.
In the late phase, the wash-out of the tumoral component of the gallbladder mass is observed, suggestive of malignancy.
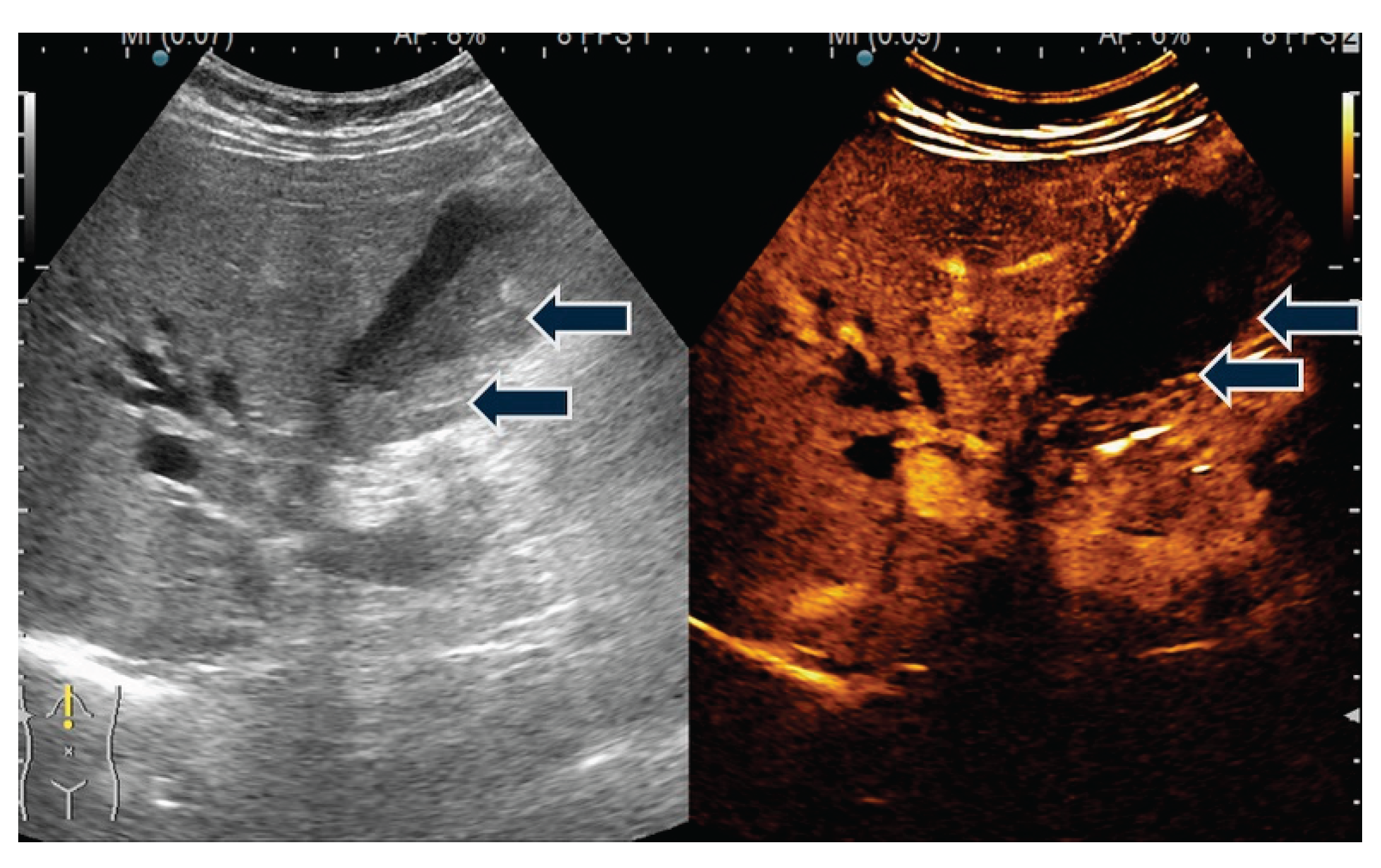
Figure 12.
Near the gallbladder, in hepatic segment 4, two tissue formations are visualized. They appear iso-echoic on 2D ultrasound and show hyperenhancement in the arterial phase following contrast agent injection.
Figure 12.
Near the gallbladder, in hepatic segment 4, two tissue formations are visualized. They appear iso-echoic on 2D ultrasound and show hyperenhancement in the arterial phase following contrast agent injection.
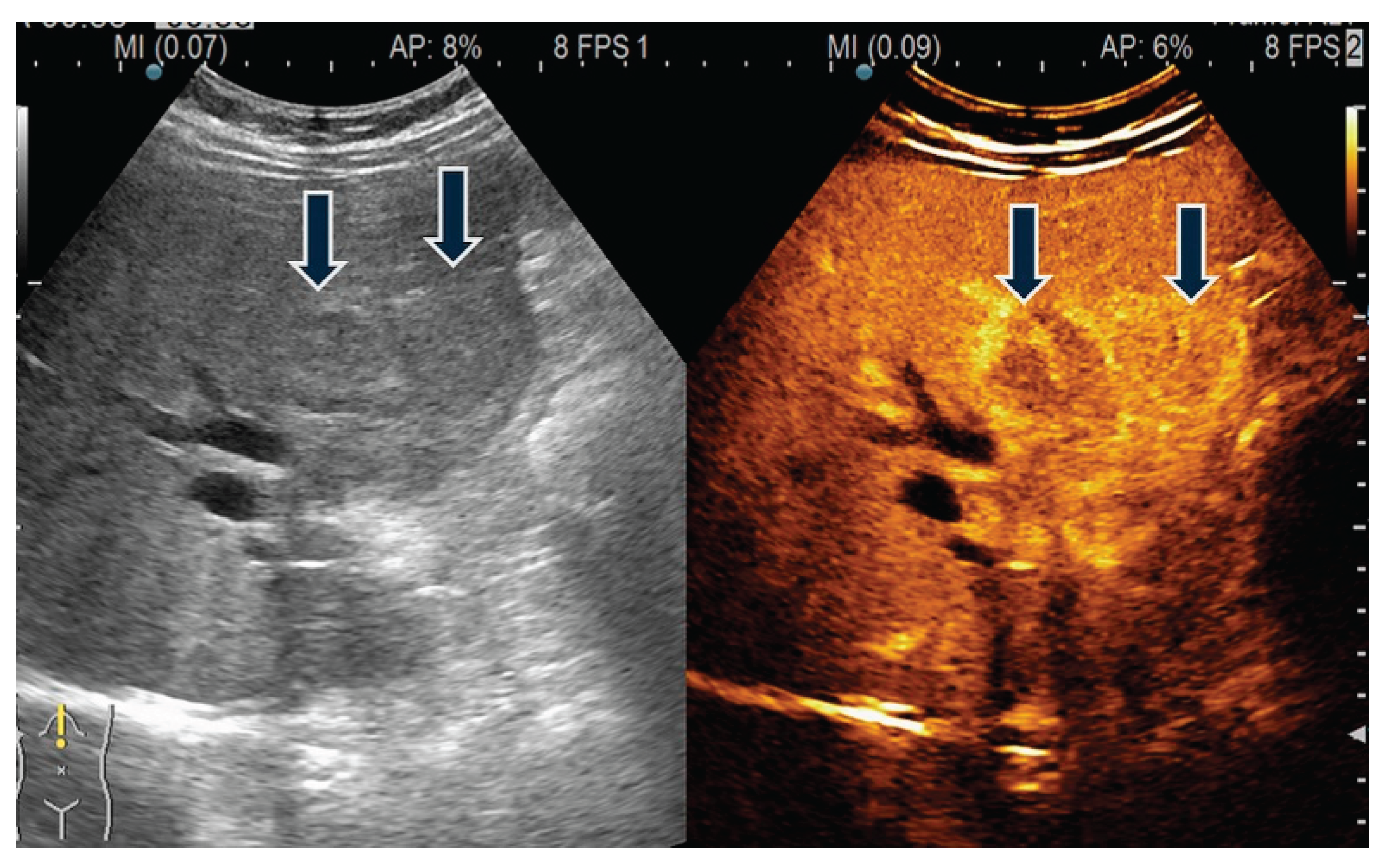
Figure 13.
TUS and CEUS (case 4). Heterogeneous encasement during the arterial phase.
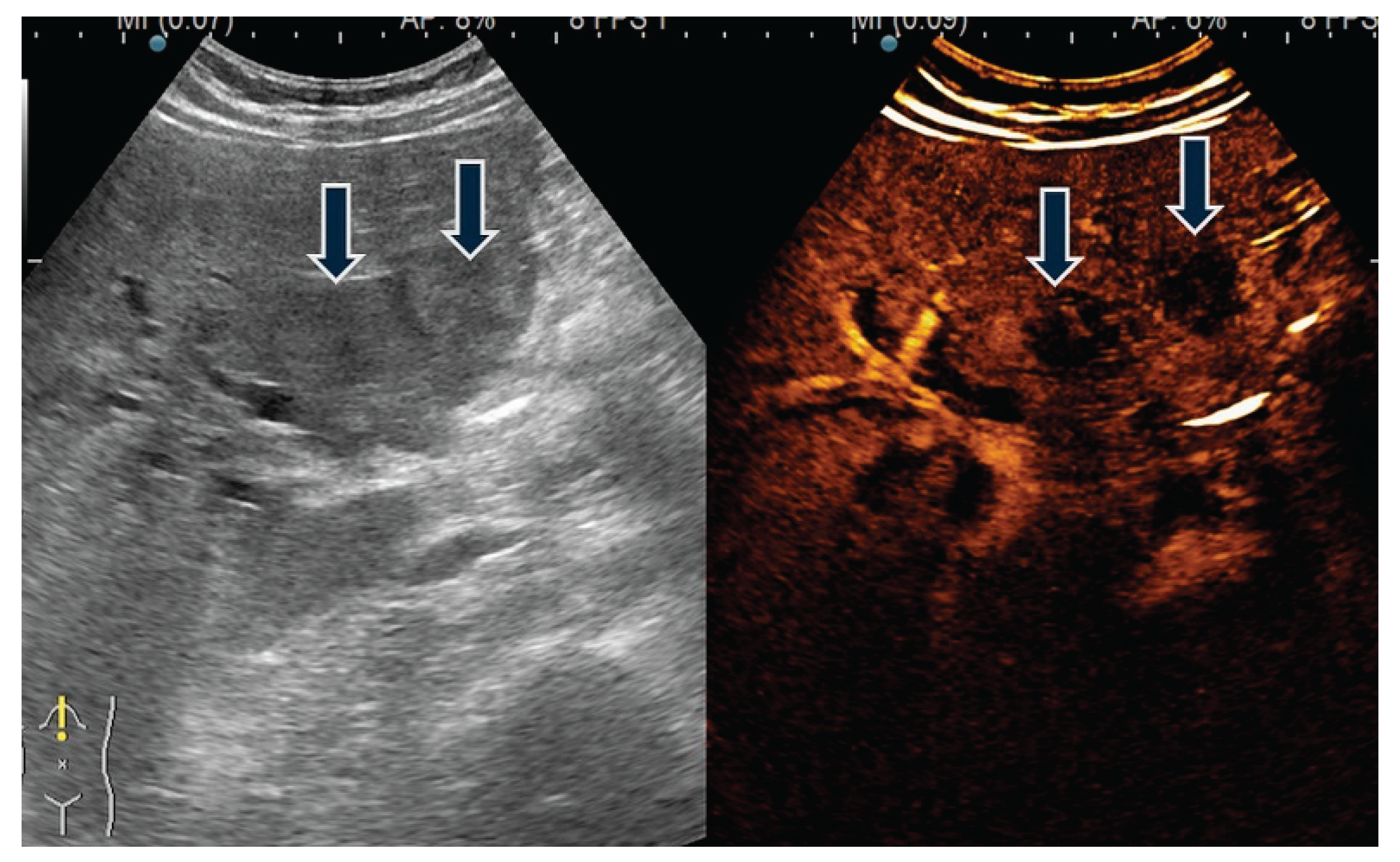
Figure 14.
Intraoperative aspect of a resected gallbladder. Visible tumor inside the open gallbladder.
Figure 14.
Intraoperative aspect of a resected gallbladder. Visible tumor inside the open gallbladder.

Figure 15.
Intraoperative aspect of gallbladder carcinoma. (white arrow). Liver metastasis (black arrow).
Figure 15.
Intraoperative aspect of gallbladder carcinoma. (white arrow). Liver metastasis (black arrow).
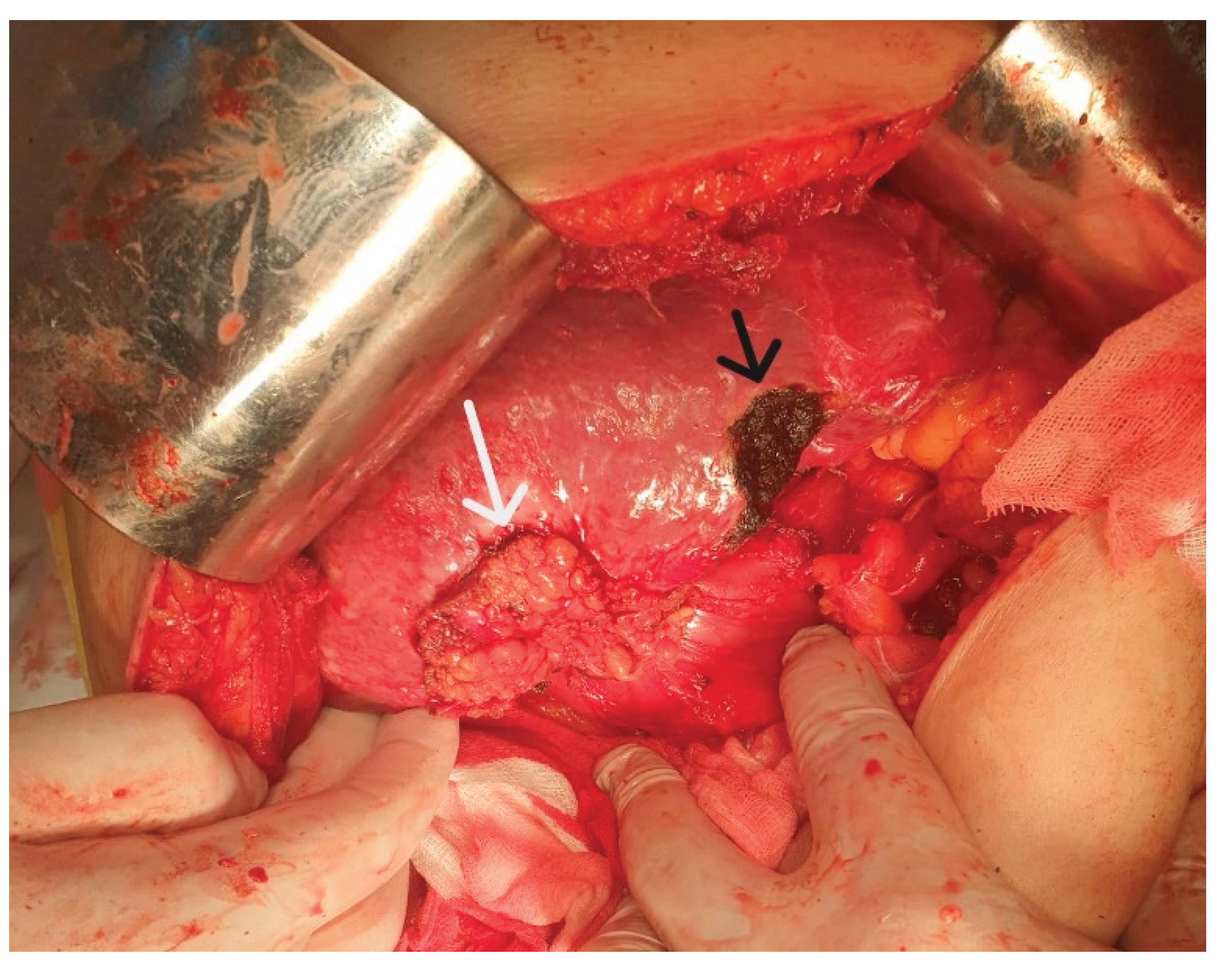
Figure 16.
Adenosquamous gallbladder carcinoma, HE staining. (ob.20x).
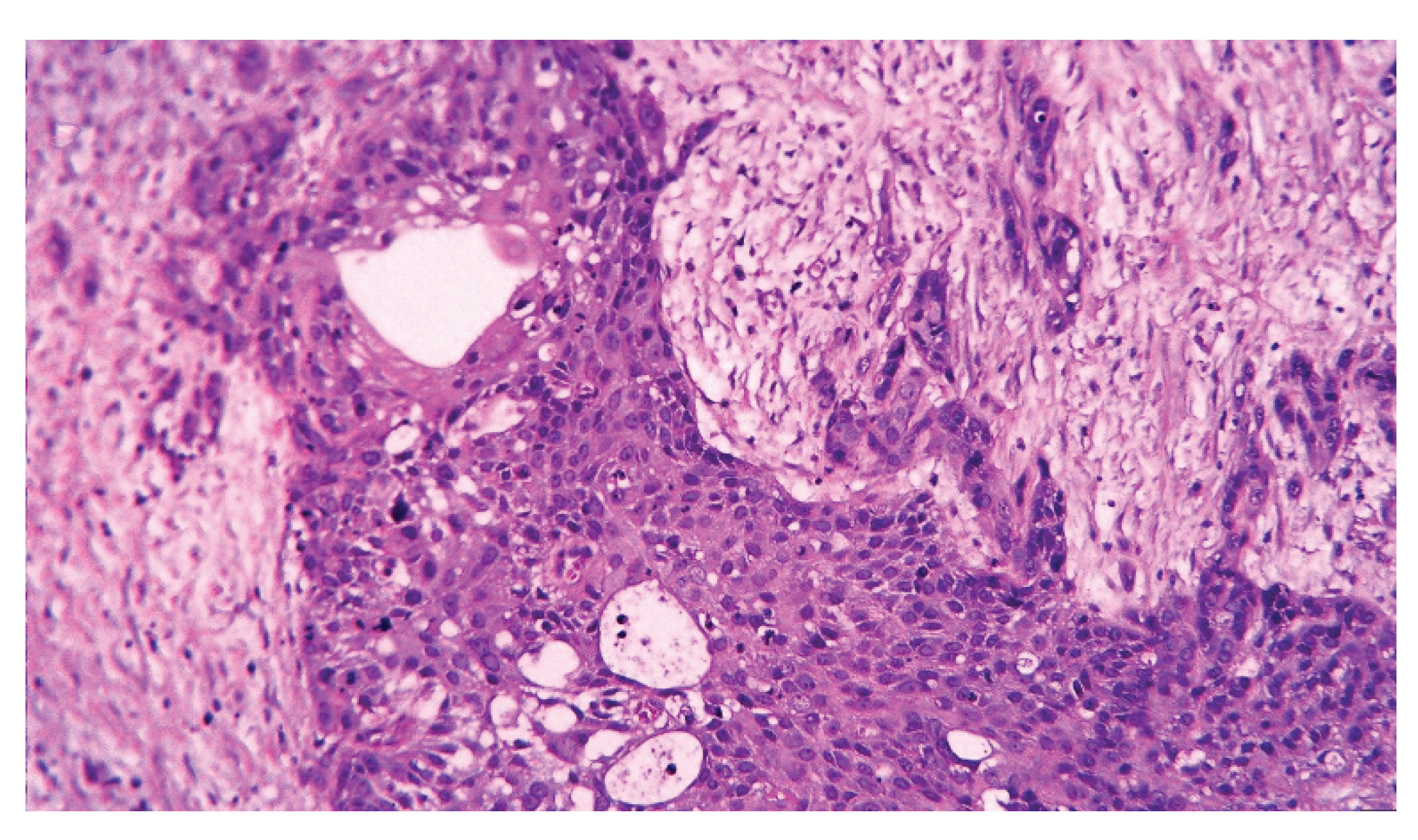
Figure 17.
Adenosquamous gallbladder carcinoma, negative immunostaining for CDX2 (ob.20x).
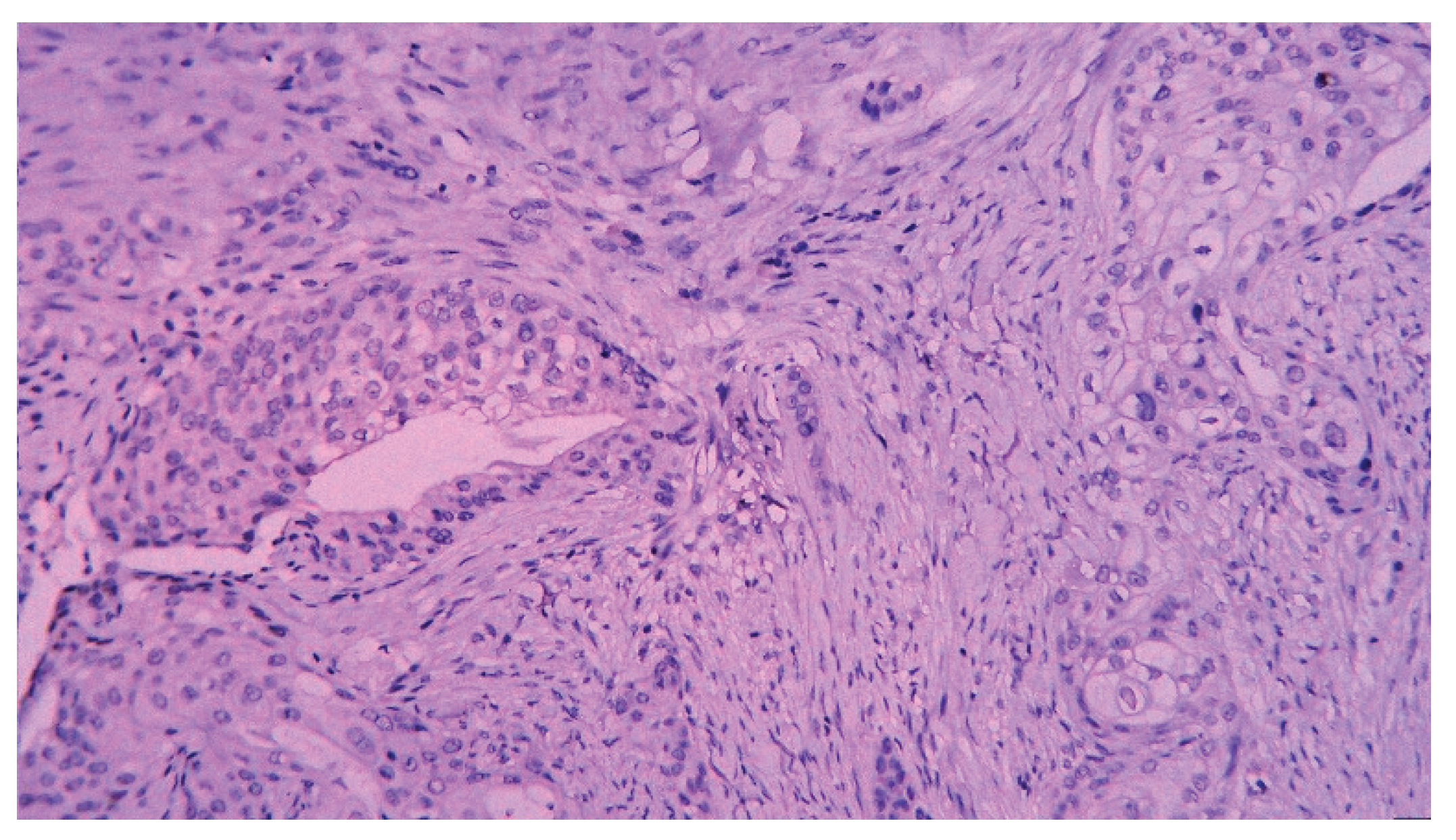
Figure 18.
Adenosquamous gallbladder carcinoma, positive immunostaining for CDX2 (ob.20x).
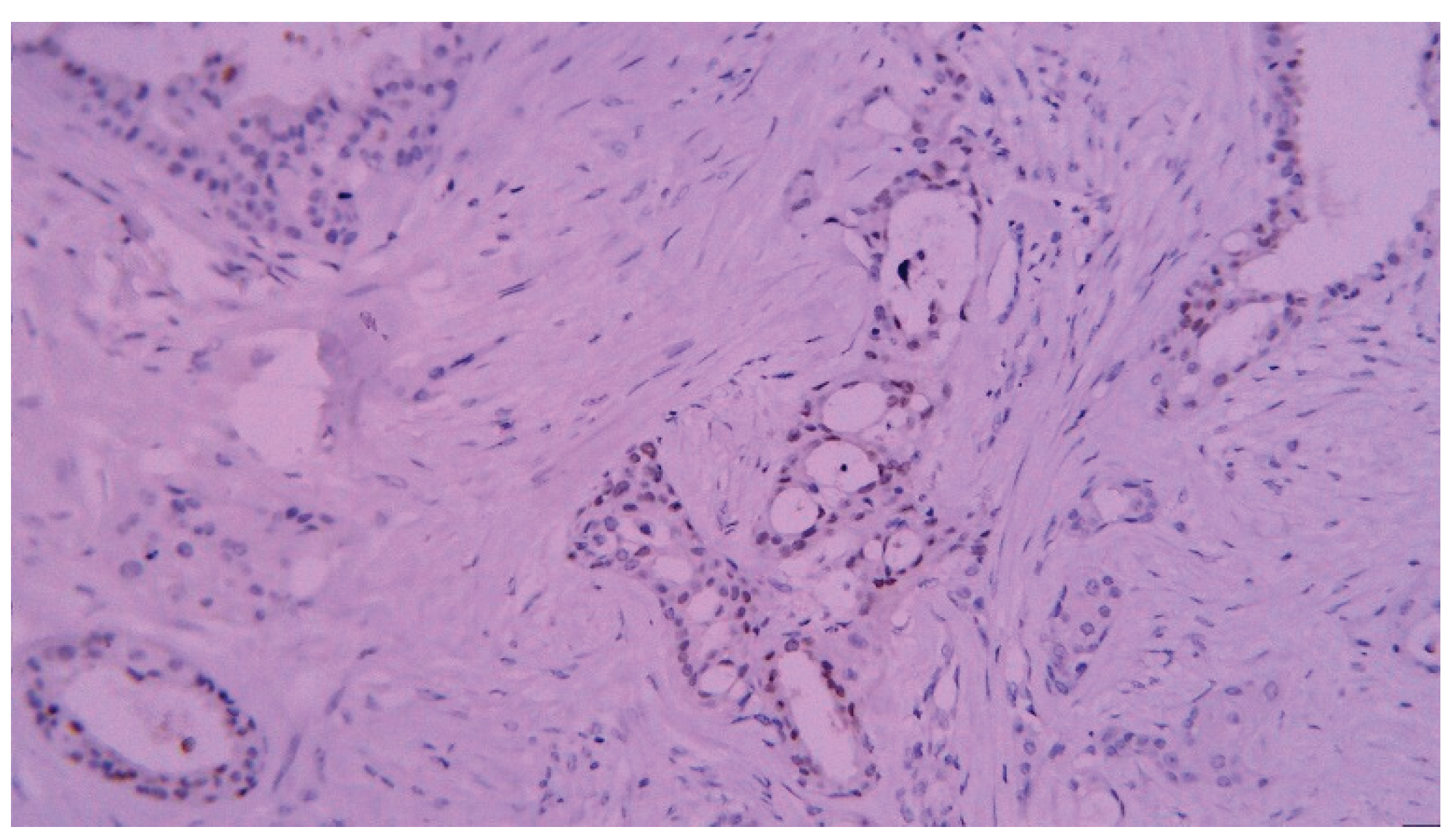
Figure 19.
Gallbladder carcinoma invasive into the adjacent fat tissue, HE staining (ob.10x).
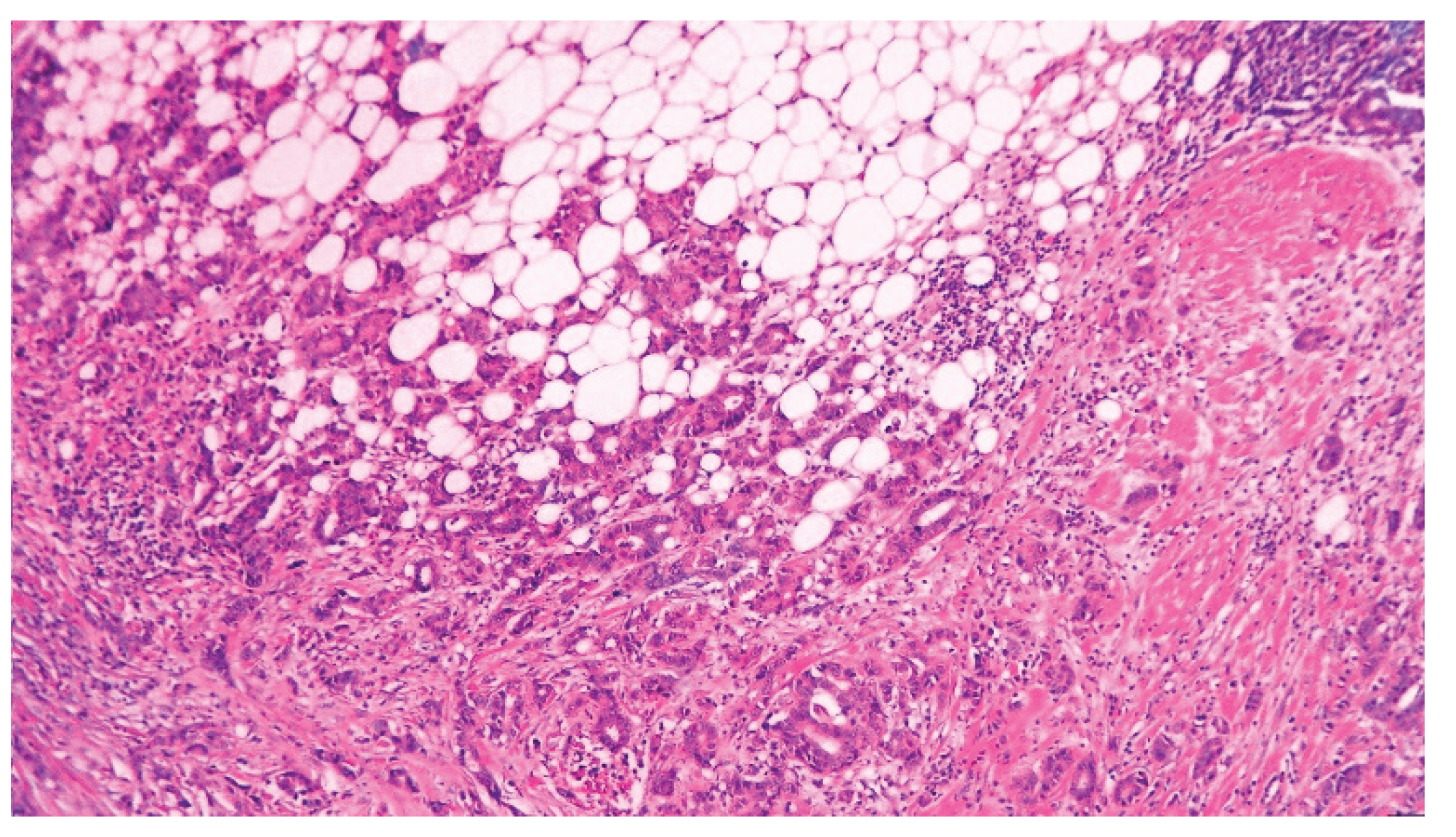
Figure 20.
Moderately differentiated gallbladder adenocarcinoma invasive into the serosa, He staining (ob.4x).
Figure 20.
Moderately differentiated gallbladder adenocarcinoma invasive into the serosa, He staining (ob.4x).
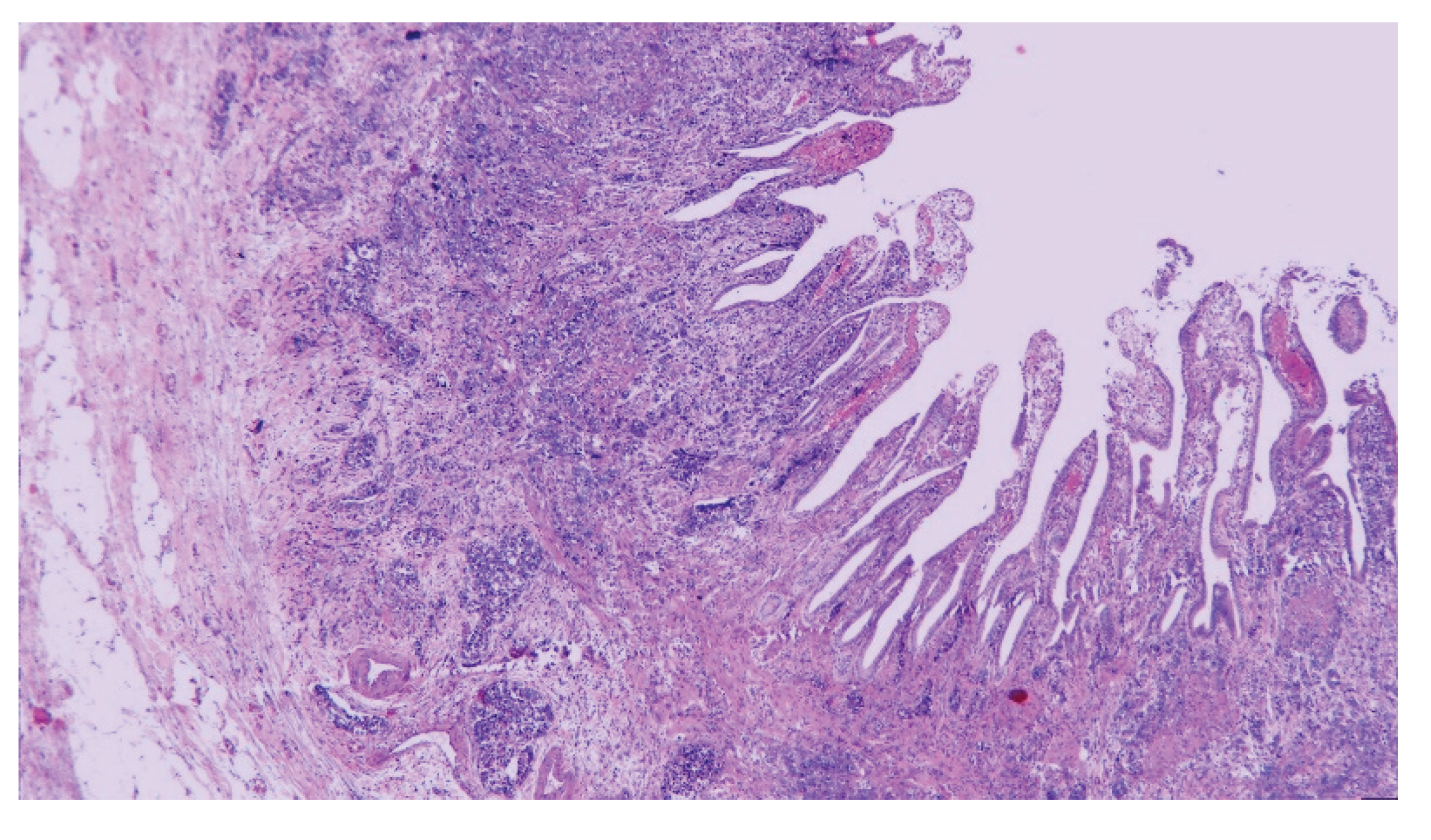
Figure 21.
Moderately differentiated gallbladder adenocarci-noma with diffuse positive CDX2 immunostaining (ob.10x).
Figure 21.
Moderately differentiated gallbladder adenocarci-noma with diffuse positive CDX2 immunostaining (ob.10x).
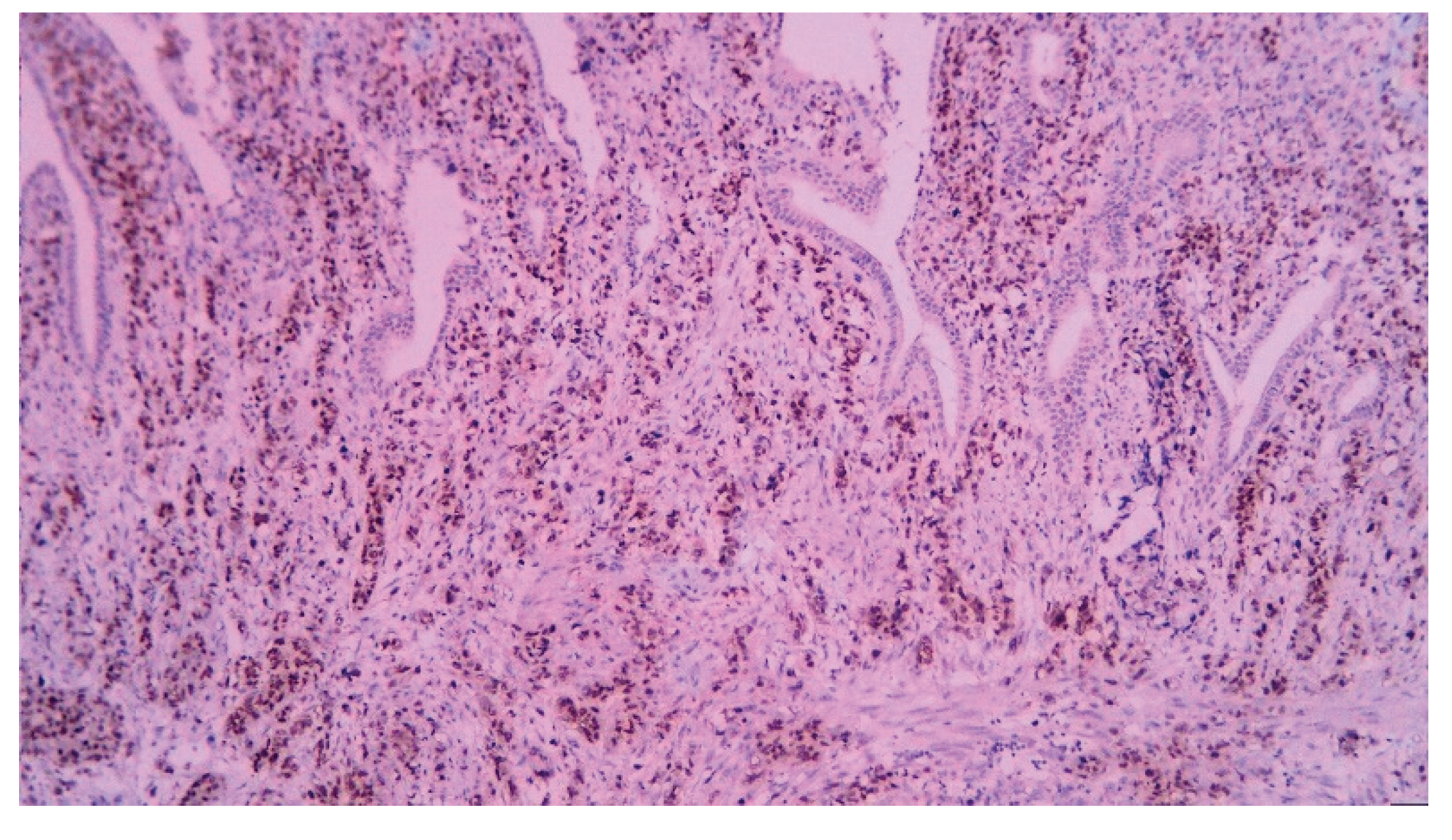
Figure 22.
Poorly differentiated gallbladder adenocarcinoma with perineural invasion, HE staining (ob.20x).
Figure 22.
Poorly differentiated gallbladder adenocarcinoma with perineural invasion, HE staining (ob.20x).

Figure 23.
Poorly differentiated gallbladder adenocarcinoma with positive CDX2 immunostaining (ob.20x).
Figure 23.
Poorly differentiated gallbladder adenocarcinoma with positive CDX2 immunostaining (ob.20x).
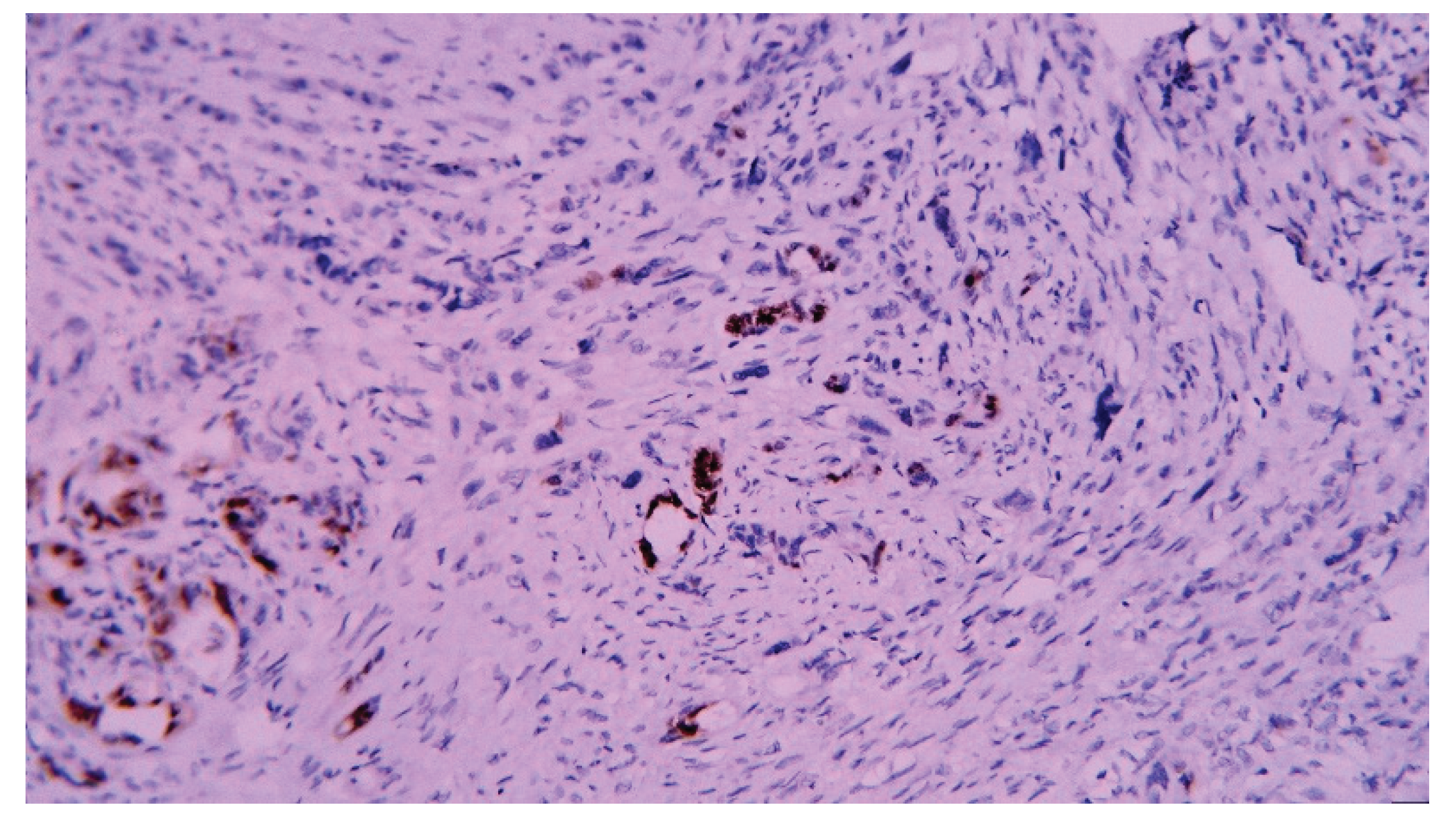
Figure 24.
Well-differentiated gallbladder adenocarcinoma, HE staining (ob.10x).
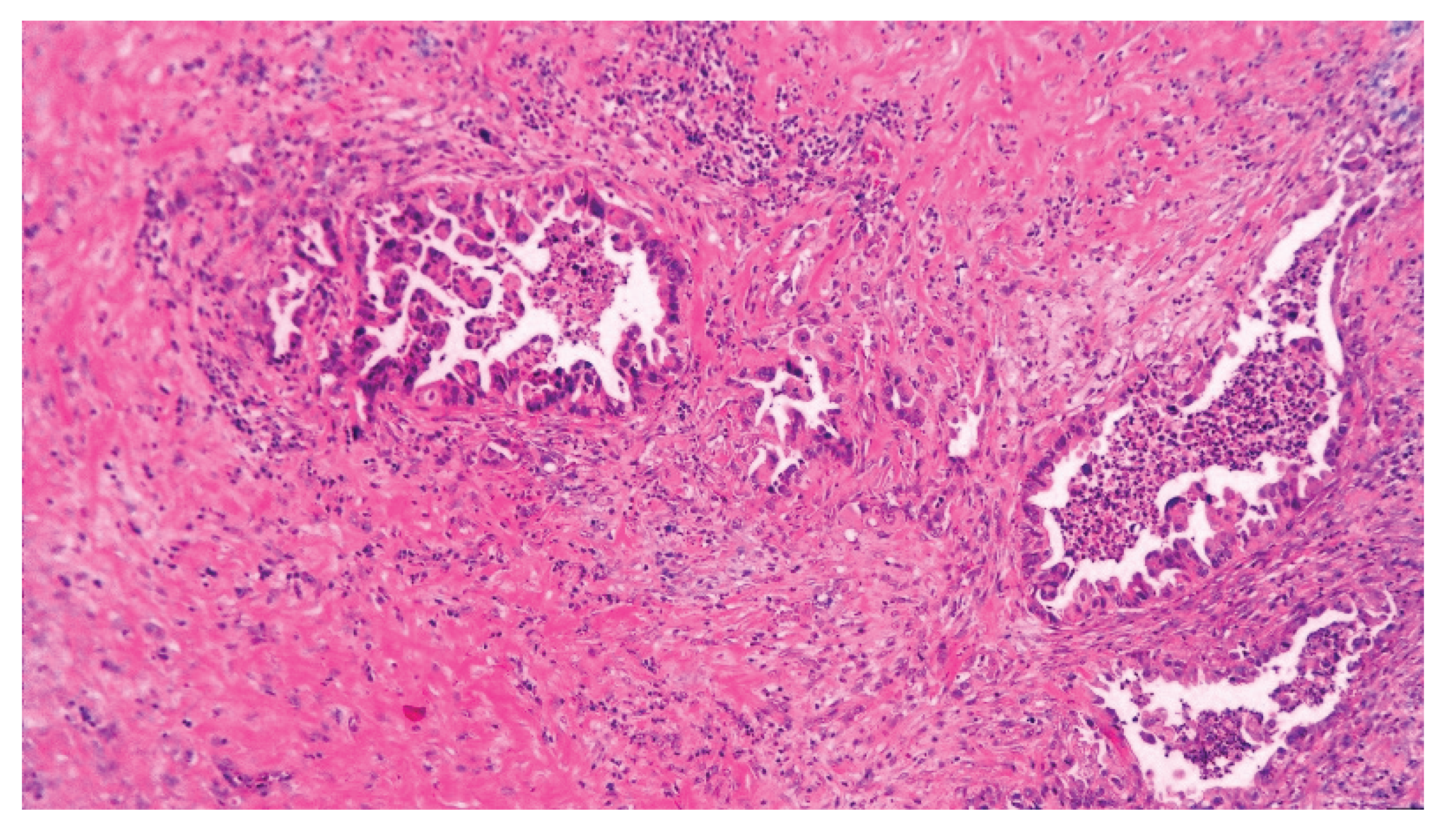
Figure 25.
Well-differentiated gallbladder adenocarcinoma with intense positive CDX2 immunostaining (ob.10x).
Figure 25.
Well-differentiated gallbladder adenocarcinoma with intense positive CDX2 immunostaining (ob.10x).
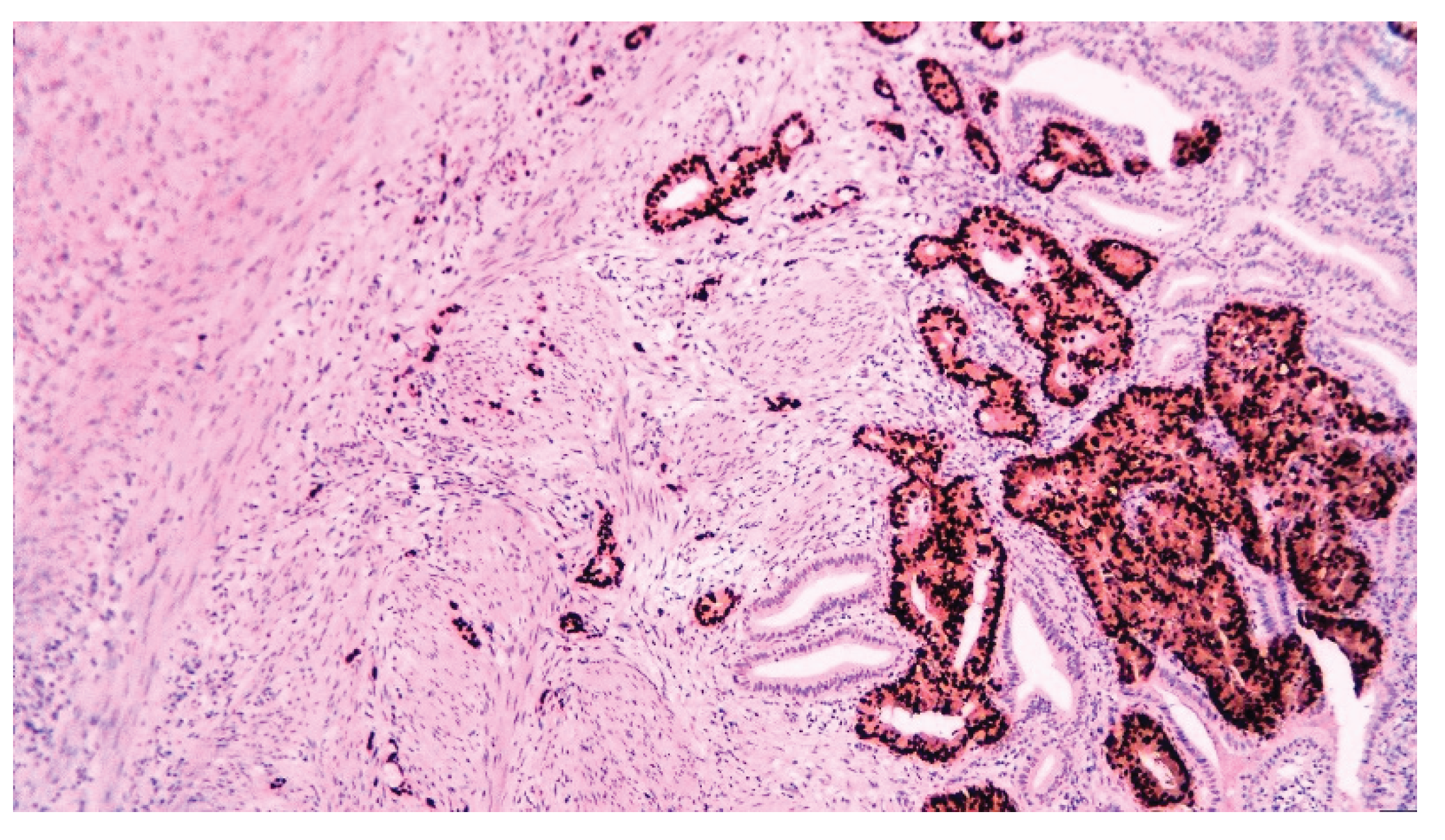
Figure 26.
The Kaplan-Meier curve for all GBC; the gray corridor represents the confidence interval.
Figure 26.
The Kaplan-Meier curve for all GBC; the gray corridor represents the confidence interval.
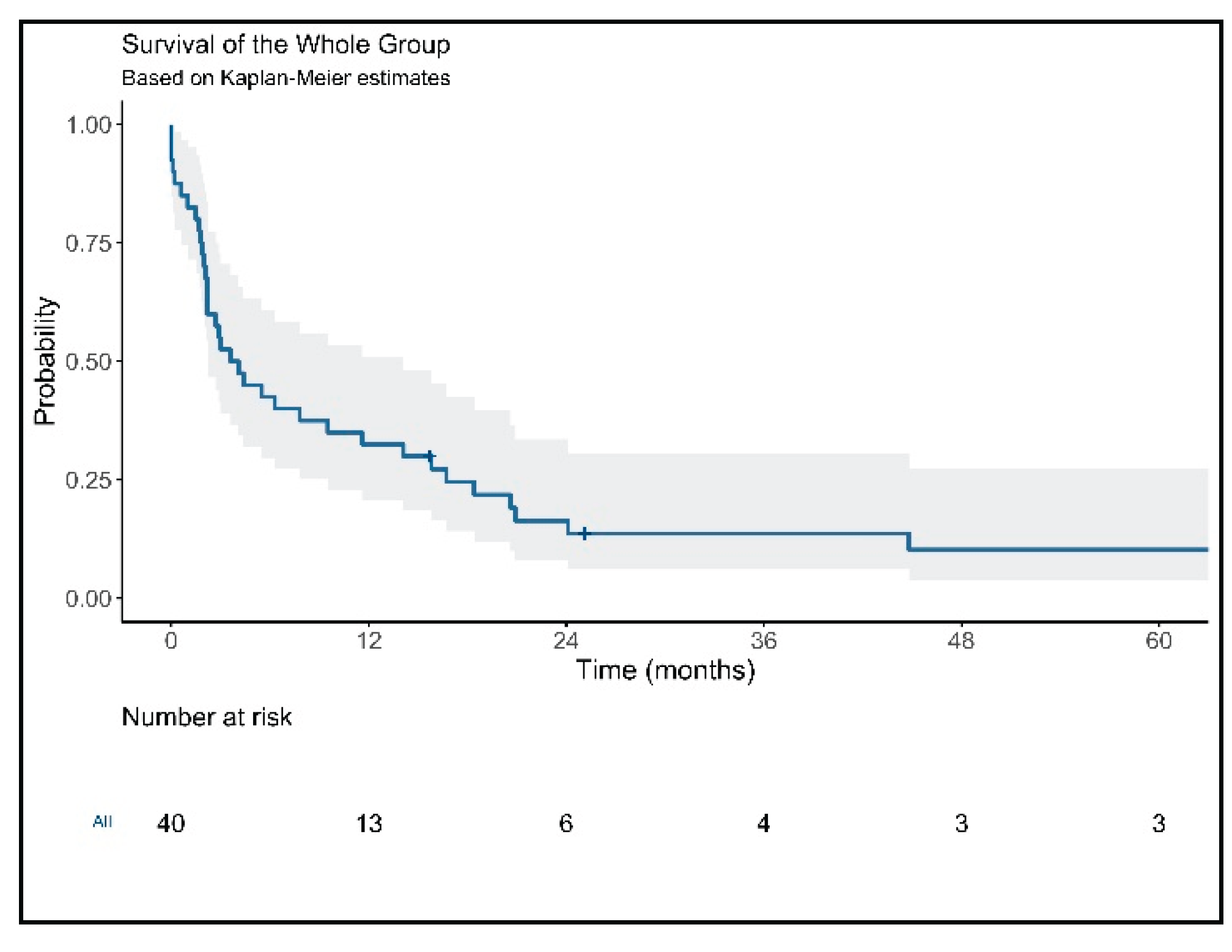
Figure 27.
The Kaplan-Meier curve for GBC stratified by surgery (cholecystectomy versus no curative surgery).
Figure 27.
The Kaplan-Meier curve for GBC stratified by surgery (cholecystectomy versus no curative surgery).
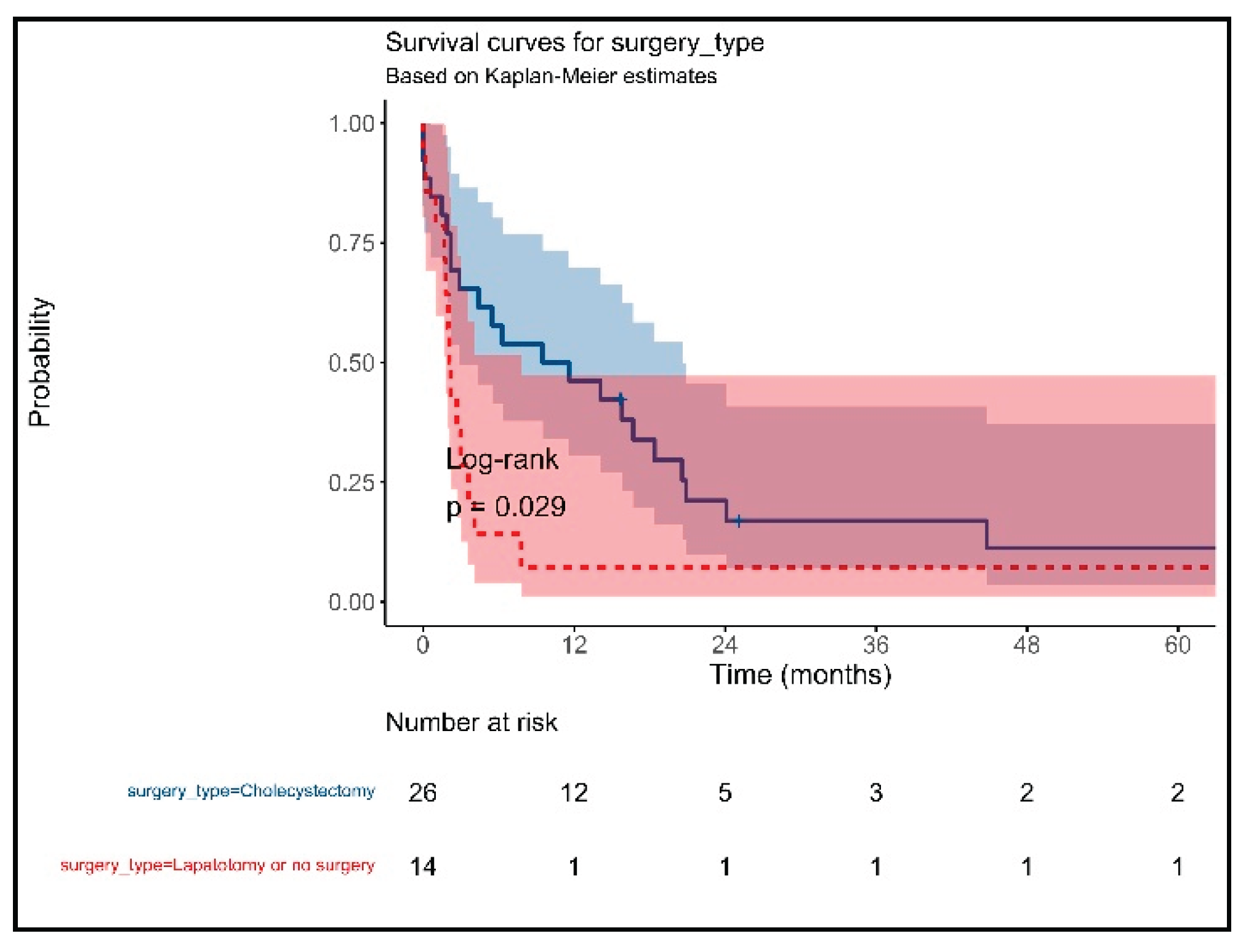
Figure 28.
The Kaplan-Meier curve for GBC stratified by the presence of metastasis.
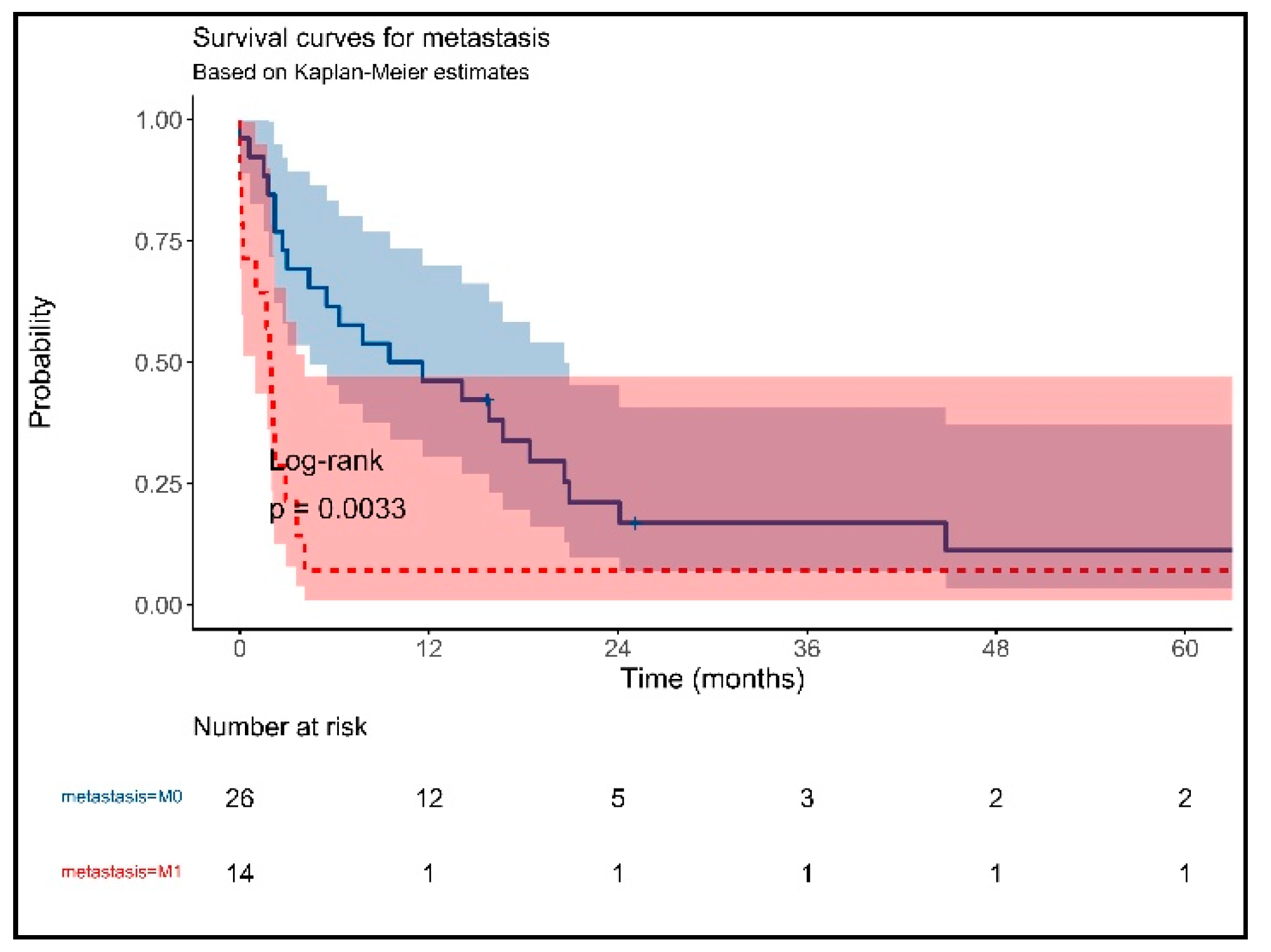
Figure 29.
The Kaplan-Meier curve for GBC stratified by postoperative chemotherapy.
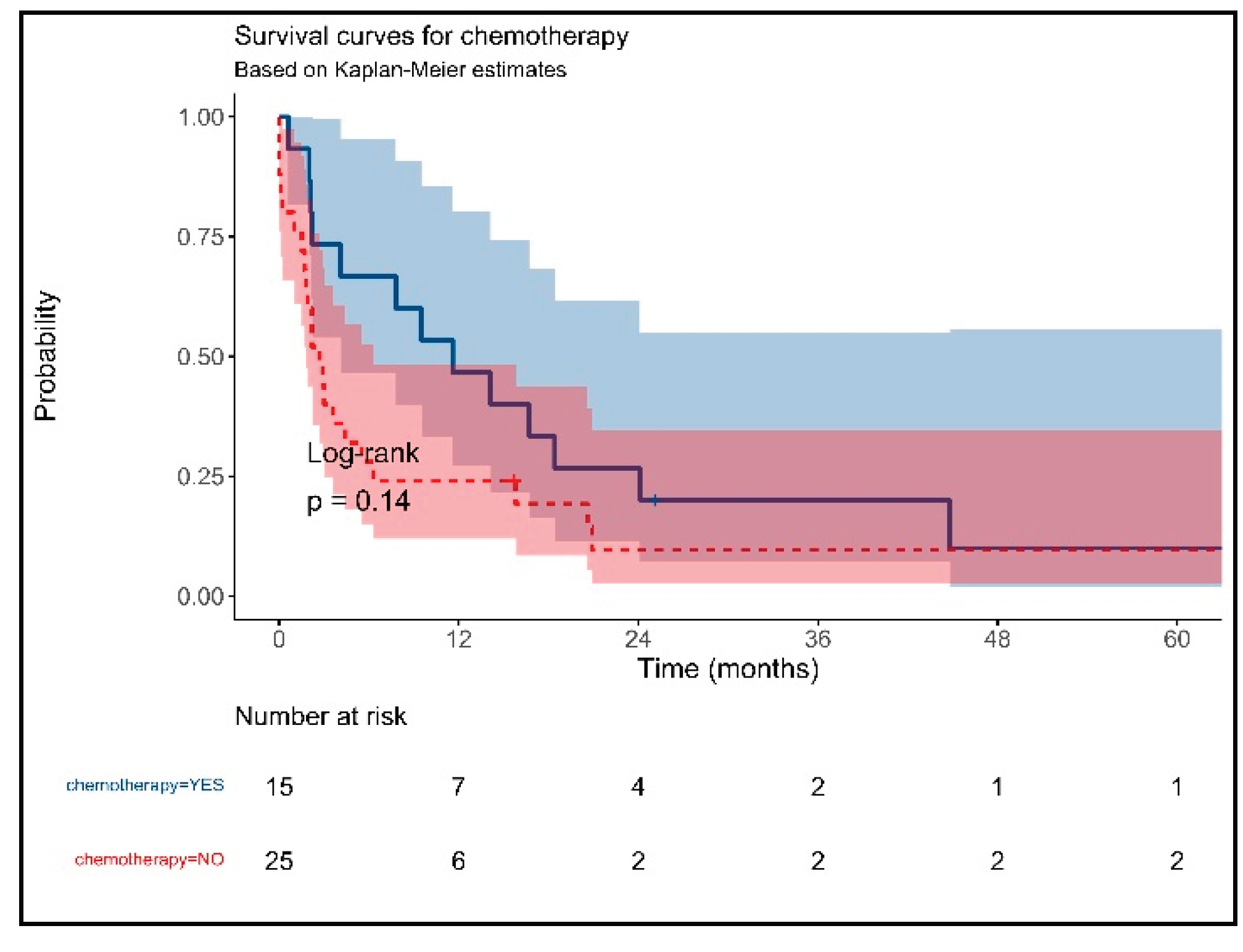

Table 1.
Definition of categories T, N, and M for gallbladder carcinoma [24].
Table 1.
Definition of categories T, N, and M for gallbladder carcinoma [24].
| T category | |
| Tis | Carcinoma in situ |
| T1 | |
| T1a* | The tumor invades the lamina propria. |
| T1b* | The tumor invades the muscular layer. |
| T2 | The tumor invades the peri-muscular connective tissue. |
| T3 | The tumor perforates the serosa/directly invades the liver/one adjacent organ/structure. |
| T4 | Tumor invades the main portal vein/hepatic artery/2 or more extrahepatic organs. |
| N category | |
| N0 | No regional lymph node metastasis. |
| N1 | Metastasis in lymph nodes along the cystic duct, common bile duct, hepatic artery, or portal vein. |
| N2 | Metastasis in the periaortic, pericaval, superior mesenteric artery, and celiac trunk. |
| M category | |
| M0 | No distant metastasis. |
| M1 | Distant metastasis. |
Table 2.
Stage categories for gallbladder carcinoma [24].
Table 2.
Stage categories for gallbladder carcinoma [24].
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| IIIA | T3 | N0 | M0 |
| IIIB | T1-3 | N1 | M0 |
| IVA | T4 | N0-1 | M0 |
| IVB | Any T | Any N | M1 |
Table 3.
Baseline characteristics of patients with primitive gallbladder carcinoma.
| No (%) | |
| Age mean±SD (min-max) | 68.8±9 (46-87) |
| M/F (%F) | 15/25 (62.5) |
| CT scan preoperatively (%) | 23 (57.5) |
| -tumor (%) | 14 (60.9) |
| -lymph nodes (% from preoperatively CT) | 3 (13) |
| -metastasis (% from preoperatively CT) | 6 (26) |
| Ultrasound | |
| YES | 17 (42.5) |
| -tumor | 1 (5.9) |
| -focal thickening | 5 (29.4) |
| -diffuse thickening | 10 (58.8) |
| -lithiasis | 11 (64.7) |
| -sludge | 4 (23.5) |
| Preoperative diagnosis | |
| -tumor | 15 (37.5) |
| -acute/chronic inflammation | 20 (50) |
| -Obstructive jaundice | 5 (12.5) |
| Intraoperative diagnosis | |
| -tumor | 25 (69.4) |
| -acute/chronic inflammation | 11 (30.6) |
| Surgery | |
| -Open cholecystectomy | 20 (50) |
| -Laparoscopic cholecystectomy | 6 (15) |
| -Laparoscopy with biopsy | 10 (25) |
| -No surgery | 4 (10) |
| Pathology | |
| -Adenocarcinoma | 34 (85) |
| -Adenosquamous | 4 (10) |
| -Undifferentiated carcinoma | 2 (5) |
| Lymphatic invasion | 7 (25) |
| Vascular invasion | 12 (42.9) |
| Perineural invasion | 10 (35.7) |
| Grading | 9 (47.4) |
| -G1 | 1 (3.3) |
| -G2 | 11 (36.7) |
| -G3 | 17 (56.7) |
| -G4 | 1 (3.3) |
| Staging | |
| -T1 | 1 (2.5) |
| -T2 | 5 (12.5) |
| -T3 | 20 (50) |
| -T4 | 13 (32.5) |
| -Tx | 1 (2.5) |
| -N0 | 21 (59.3) |
| -N+ | 15 (37.5) |
| -Nx | 4 (10) |
| -M0 | 26 (65) |
| -M1 | 14 (35) |
| -I | 1 (2.5) |
| -II | 2 (5) |
| -IIIA | 13 (37.5) |
| -IIIB | 6 (15) |
| -IVA | 4 (10) |
| -IVB | 14 (35) |
Table 4.
Sensitivity, specificity, positive and negative predictive value, and accuracy.
| Sensitivity | Specificity | PPV | NPV | Accuracy | |
| Transabdominal US | 35.3 | 98.4 | 27.3 | 98.9 | 97.3 |
| CT scan | 60.9 | 97.6 | 56.0 | 98.1 | 95.9 |
| Preoperative aspect | 51.3 | 99.0 | 45.5 | 99.2 | 98.3 |
| Intraoperative aspect | 74.3 | 99.8 | 83.9 | 99.6 | 99.4 |
PPV=positive predictive value, NPV=negative predictive value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



