
Submitted:
14 May 2025
Posted:
15 May 2025
You are already at the latest version
Abstract
Background/Objectives: Urinary tract infections (UTIs) can predispose women to preeclampsia and prematurity, which are common causes of maternal and neonatal morbidity and mortality. In low-middle-income countries (LMICs), the capacity for screening and treating UTIs is limited. In sub-Saharan Africa, AMR surveillance data are scarce, especially in vulnerable populations such as pregnant women. The aim of this study was to determine the prevalence and antimicrobial resistance patterns of community-acquired urinary tract infections among pregnant women attending the antenatal clinics of three hospitals in Gambia.
Methods: This was a hospital-based, cross-sectional, multicenter study conducted between November 2022 and January 2023. Patient information was obtained via a pre-tested questionnaire. The urine samples were analyzed via Gram staining and biochemical tests to determine the causative organisms. We also used antibiotic sensitivity testing to identify resistance patterns. The data collected were analyzed via SPSS version 20 and tested for associations at a significance level of p ≤ 0.05.
Results: The prevalence of significant bacteriuria was 5% (n=100). Escherichia coli (40%) and Staphylococcus aureus (40%) were the most common uropathogens. The prevalence of resistance was found for trimethoprim/sulfamethoxazole and ampicillin, and multi-drug resistance was detected in only one isolate (Citrobacter freundii).
Conclusion: This study revealed bacterial isolates with prevalent resistance to commonly prescribed drugs for community-acquired UTIs in pregnant women and suggested alternatives such as ceftriaxone, nitrofurantoin, erythromycin, and nalidixic acid as empirical treatment options. We recommend consistent health to combat drug resistance caused by inappropriate antibiotic use.
Keywords:
Antimicrobial resistance
; multicenter study
; Gambia
; urinary tract infections
; pregnant women
; bacterial uropathogens
1. Introduction
Urinary tract infections (UTIs) are among the most severe and frequent human infections that can be acquired in both communities and hospitals [1]. High recurrence of infection occurs, and treatment with antimicrobials increases the risk of selection for resistance. Using 27 studies and a total population of 30,641 individuals, a systematic review and meta-analysis of the incidence of UTIs during pregnancy worldwide was performed, and the prevalence rate of UTIs during pregnancy was 23.9% [2]. The emergence and global spread of multidrug resistance is also a growing concern due to the shortage of alternative antibiotics, especially in sub-Saharan Africa, where 27.3 deaths per 100,000 people occurred in 2019 [3]. The increased global increase in resistance warrants local surveillance. It results in more than 150 million cases each year worldwide, and up to 6 billion dollars are spent annually to mitigate the effects of the disease worldwide [1,4].
Approximately half of all women will experience a UTI at least once in their life, whereas a quarter will experience it more than once [5]. It is even more common in pregnant women because of pregnancy-related changes such as decreased immunity, difficulty with hygiene from a gravid abdomen, increased glucose levels in the urine and increased urine stasis in the tract [6]. Poor socioeconomic status and diabetes mellitus are additional risk factors [7,8].
There are natural, semisynthetic, and synthetic agents with unique mechanisms that can significantly alter metabolic and physiological levels. These agents include β-lactams and glycopeptides, which modify the synthesis of cell walls; macrolides and tetracyclines, which inhibit protein synthesis; sulfonamides, which inhibit metabolic pathways; and fluoroquinolones, which interfere with DNA replication and translation [9].
The majority of community-acquired UTIs during pregnancy are asymptomatic, but studies have shown that they can lead to low birth weight, preterm labor and prematurity, preeclampsia and abortion [10,11]. UTIs are diagnosed on the basis of clinical features and diagnostic tests such as urinalysis (to look for bacteria in the urine) and a urine dipstick (to check for nitrites and leukocyte esterase). A urine culture is used to look for the growth of a pathogenic organism and is combined with antibiotic sensitivity testing to determine the antibiotics used for that specific organism [12]. Sixty to eighty percent of all UTIs in pregnancy are caused by Escherichia coli, while the remainder are caused by Proteus mirabilis, Klebsiella pneumoniae, coagulase-negative staphylococci and others [1]. It has also been shown that gram-negative bacteria are the primary causes of UTIs in Gambia [13,14]. It is estimated that bacterial resistance to antimicrobials (AMRs) will lead to a total global GDP loss of 100.2 trillion USD and almost 10 million deaths per year by 2050 [3,15]. Therefore, local knowledge of the burdens of disease, etiology and AMR is important for informing therapeutic decisions.
There is a paucity of community-based antimicrobial surveillance data, especially in sub-Saharan Africa, including Gambia. The prevalence of UTIs in pregnant women in Gambia has not been studied before, as routine antimicrobial susceptibility testing is rarely performed in Gambia. Therefore, the data derived from this study add to the knowledge on AMR in Gambia. Such information would be highly relevant to healthcare providers when making decisions on the treatment of urinary infections with the right antibiotics in the absence of patient-specific antimicrobial susceptibility testing [16]. It is also important to understand the trends in Gambia since AMR varies regionally. Therefore, the aim of this study was to determine the prevalence and antimicrobial resistance patterns of community-acquired urinary tract infections in pregnant women attending the antenatal clinics of three hospitals in Gambia.
2. Materials and Methods
2.1. Study Design
The study was a hospital-based cross-sectional multicenter study carried out at the outpatient antenatal clinics and microbiology laboratories of three major hospitals in the western part of Gambia. Gambia is the smallest country on the African mainland and is situated on its western coast. It has a total area of 10,689 sq km and a population of 2,785,000 (2022 est.) [17]. The hospitals include tertiary-level referral facilities, Edward Francis Small Teaching Hospital (EFSTH), Kanifing General Hospital (KGH) and Bundung Maternal and Child Health Hospital (BMCHH). All these hospitals have Obstetrics and Gynecology and Microbiology departments and run antenatal care services, with EFSTH being the nation’s only teaching hospital. It was conducted from November 2022 to January 2023.
2.2. Sample Selection
Study Population and Sampling
The study population consisted of all pregnant women attending the antenatal clinics of all three hospitals. Study participants were selected via the convenience sampling technique.
Sample Size
A single population formula [18] was used to calculate the sample size via the following parameter: a 15.8% prevalence rate of UTIs in pregnant women from a study performed in Nigeria [19].
, where d=5%, the Z score for the 95% confidence interval=1.96 and p=15.8%
A sample size of 204 was achieved. With a calculated dropout rate of 30%, the minimum number of participants required was 143.
Inclusion Criteria
All pregnant women who attended the antenatal clinics of the hospitals provided consent and were recruited.
Exclusion Criteria
Pregnant women who did not consent to participate in the study and those who took antibiotics two weeks prior to the study were excluded.
2.3. Data Collection Tools
All pregnant women were interviewed via a semi structured questionnaire from Derese et al. [20] was adopted and modified on the basis of the study objectives to collect sociodemographic factors and clinical data. After the interview, each participant was taught how to obtain a midstream urine sample. The samples were then sent to the Bacteriology Department for microscopy, culture and antimicrobial susceptibility testing.
2.4. Data Analysis
Microbiological Studies
The color and consistency of the freshly collected urine samples were recorded. A Combi 10 dipstick (URIT Medical Electronic Co-LTD) was used for urinalysis.
Cysteine lactose electrolyte-deficient (CLED) agar and MacConkey (MAC) agar (Oxoid Ltd., England) were used for the inoculation of urine samples via a standard calibrated loop (0.001 ml) according to the manufacturer’s instructions. Streaked culture plates were incubated at 37°C for 24 hours and inspected for bacterial growth the next day, and colonies were counted manually on CLED. Urine cultures that grew ≥105 (CFUs)/ml of urine sample consisting of one type of colony morphology were considered significant bacteriuria.
The bacteria were identified by colony morphology, Gram staining, and other indicators on their respective media and confirmed by the pattern of biochemical reactions via a standard procedure [21,22].
Antimicrobial susceptibility testing was performed via the disk diffusion method as described by Kirby-Bauer [23] on Mueller‒Hinton agar (MHA) (Oxoid Ltd., England) [24] via the use of commonly prescribed antibiotics from the Clinical and Laboratory Standards Institute 2019 guidelines. Different antibiotics, including ciprofloxacin, gentamicin, ceftriaxone, nitrofurantoin, ceftazidime, cefuroxime, methicillin, trimethoprim/sulfamethoxazole, ampicillin, amoxicillin/clavulanate, nalidixic acid, tetracycline and erythromycin, are available and recommended in the 2019 CLSI guidelines. Loopful pure cultures were taken from colonies suspended in 5 ml of sterile saline (0.85% NaCl). The turbidity of the suspension was then adjusted to an optical density of 0.5 McFarland standard. A sterile cotton swab was used to inoculate the suspension on MHA, and the plates were incubated at 37°C for 24 hours. The diameters of the zones of bacterial growth inhibition around the discs were subsequently measured to the nearest millimeter via a metallic caliper and interpreted as sensitive or resistant according to the standardized table provided by CLSI, 2019.
2.5. Statistical Analysis
The data collected were entered into Microsoft Excel 2019, and the analysis was performed with the Statistical Package for the Social Sciences (SPSS) version 20 (Chicago, IL, USA). Quantitative analysis was performed using coded categorical variables. The data were cleaned to ensure accuracy validity. The data are presented via graphs and tables. The mode, means and frequencies of continuous data were checked via descriptive statistics. The chi-square test was used to determine the statistical significance of the associated risk factors (p≤0.05).
3. Results
3.1. Description of the Participants
Overall, 112 pregnant women were recruited for this study, of which 100 samples were analyzed. The women were between the ages of 15 and 45 years, with a mean age of 28 years. Half of them (49%) had attained secondary education, and 48% were housewives. A third (31%) of them were nulligravida, while 44% of them had more than one child. The majority (67%) were in their third trimester, and only 37% of them previously had a UTI. Seven of the 100 participants were symptomatic, with dysuria present in all of them (see Table 1).
3.2. Prevalence of UTIs Among Pregnant Women: Sociodemographic, Obstetric, and Clinical Factors
Five of the 100 cultured urine samples contained a significant number of bacteria, with an overall prevalence of 5%, two of which were detected in the 30–34-year-old age group (40%). Only 20% of them had tertiary educations, whereas 80% had more than one child. None of the infected patients were in their first trimester, and 80% of them were asymptomatic (see Figure 2). Furthermore, 40% of them had previously had a UTI, whereas 60% of them had not used antibiotics without a prescription before this study (see Table 2).
3.3. Risk Factors for UTIs During Pregnancy
A higher prevalence was found among women aged 30--34 years, those with no formal education, those with multiple gravidas, and women in their second and third trimesters. Logistic regression analysis revealed no statistically significant associations between the presence of bacteriuria and age (p=0.363), level of education (p=0.716), gravidity (p=0.687), parity or gestational age. This was also observed with a history of UTI or antibiotic use without prescription (Table 2).
3.4. Bacterial Pathogens Isolated from Urine Cultures
In this study, a total of 5 bacteria were isolated from 3 different species. Only 1 out of the 5 bacteria isolated was from a symptomatic patient. There were more gram-negative bacteria (3/5, 60%), which included Escherichia coli and Citrobacter freundii, and the other two were Staphylococcus aureus, the only gram-positive bacteria (see Figure 1 and Table 3).
3.5. Prevalence of AMR and Its Patterns
Among the 5 patients with significant bacteriuria, one (1) of the culture plates was susceptible to all the drugs, one (1) was resistant to more than one class of antimicrobial used in this study, and the remaining three cultured organisms were resistant to just one drug class. All the isolates were 100% susceptible to ciprofloxacin, ceftriaxone, nitrofurantoin, tetracycline and erythromycin. High resistance to cefuroxime (100%) and trimethoprim/sulfamethoxazole (50%) was detected. None of the isolates were resistant to co-amoxiclav. The E. coli isolates were resistant to ampicillin and cefuroxime, whereas S. aureus was methicillin sensitive. Among the total isolates (n=5), only 1, Citrobacter freundii, presented multidrug resistance (resistance to three or more classes of antimicrobials) but was sensitive to nitrofurantoin and ceftriaxone (Table 4 and Figure 3).
4. Discussion
The aim of this study was to determine the prevalence and antimicrobial resistance patterns of urinary tract infections in pregnant women attending the antenatal clinics of three hospitals in Gambia. We found that the prevalence of significant bacteriuria in 100 pregnant women from the three hospitals was 5%. It was mostly observed in the 30–34 year age group, and 4 of the 5 infected pregnant women were asymptomatic. Escherichia coli and Staphylococcus aureus were the most prevalent organisms isolated, and antibiotic sensitivity was highest for ceftriaxone, nitrofurantoin, tetracycline and nalidixic acid. Only Citrobacter freundii was found to harbor MDR strains to various antibiotic classes.
The overall prevalence of UTIs was 5% in this study, which was lower than that reported in data published from community-acquired UTIs from the same setting [14], and the global prevalence ranged from 13--33% [25]. This percentage was higher than that reported in some studies in India (3.3%) [26] and Uganda (3.75%). This number was lower than those reported in many studies conducted in African countries, such as Ethiopia (7.8%) [27], Iran (13.1%) [28], South Africa (16.8%) [29], Somalia (21%) [30], Egypt (29%) [31] and Nigeria (49%) [32]. These variations in prevalence can be attributed to these studies using larger sample sizes and inpatient data. There is a greater likelihood of being identified and treated for any infection if pregnant women attend ANC as necessary, which may also be related to the rate of adherence to ANC visits throughout pregnancy in various nations [33]. These differences could be because the studies were conducted in different locations with different populations. Another factor may also be differences in socioeconomic status, social habits and hygiene practices [30].
Like Negussie et al. [34] and Rejali et al. [28], there was no statistically significant association between maternal obstetric risk factors and UTIs in this study. In contrast, other studies have shown that age, gravidity, parity, level of education, gestational age and a history of UTI are significantly associated with UTI during pregnancy [35,36,37,38]. These variations may be due to population differences and differences in sample size. One of the studies that found significance with low education attributed this finding to the limited knowledge about health practices and diseases in the illiterate population [37]. No evidence of an association was found between gestational age and UTIs, which is different from the findings of Obeng-Forson et al. [39]. Another study revealed that age was significant and that most of the infected patients were younger than 30 years of age. This could be attributed to the higher rate of sexual intercourse in that age group and the increased incidence of UTIs [36,40].
Data on microbial trends and antibiotic resistance are needed for empirical therapy guidelines. The isolated organisms included S. aureus (40%), E. coli (40%) and C. freundii (20%). The results of this study revealed that Escherichia coli and Staphylococcus aureus were the most common bacteria involved in urinary tract infection among pregnant women, which is in line with the findings of other studies in other African countries [19,30,41,42,43], and the popularity of gram-negative bacteria has been reported in two studies in Gambia [13,14]. E. coli was also the most commonly isolated bacterial species in pregnant women in Latin America, at 70%, according to a systematic review and meta-analysis De Souza [44]. Even though steps are taken to prevent skin contamination, it is challenging to determine whether S. aureus is a skin contaminant or a real uropathogen. It was the most common isolate (55.9%) in a small study by Younis et al. in Libya [45]. The risk of contracting a UTI caused by E. coli during pregnancy may increase due to anatomical and functional changes such as urinary stasis, as well as difficulties maintaining personal hygiene or the use of poor hygiene practices such as wiping from back to front after using the toilet. E. coli is commonly found in the perineal area, and its virulence factors promote attachment to the uroepithelium, making it easier to colonize the urinary tract [46]. The observed similarities and differences in the type and distribution of uropathogens may be due to a variety of factors, including the environment, medical practices, patient factors, number of patients examined, and laboratory techniques employed for urine examination [47].
The isolates were assessed for susceptibility to commonly used antibiotics. AMR in bacterial pathogens is becoming a serious threat because of the limited choice of antibiotics to use in pregnancy and their wide availability and usage [48]. The present study revealed that most of the pathogens were sensitive to Ceftriaxone, nitrofurantoin, tetracycline, erythromycin, nalidixic acid and co-Amoxiclav and resistant to ampicillin and cefuroxime trimethoprim/sulfamethoxazole. This susceptibility to these agents suggests their use as an empirical treatment for UTIs during pregnancy. The resistance to these latter agents could stem from the large amount of these drugs being prescribed to pregnant women and the lack of data on resistance trends limiting their choices [49]. The high sensitivity to ceftriaxone and nitrofurantoin is in accordance with data reported in this setting and other studies, such as those of Johnson et al. in Uganda, involving 400 pregnant women with symptomatic UTIs [6]; in Gambia [13,14]; and in Ethiopia, by Ejerssa et al., who reported the highest sensitivity to amikacin, an antibiotic not tested in our study [46]. The high sensitivity to nitrofurantoin is encouraging since it is listed as the first-line treatment in most international guidelines [50]. Our high level of ampicillin resistance is similar to the findings of Orji et al. from South Africa [29]. A meta-analysis also revealed that resistance to ampicillin was at least 75% across various studies performed in low- and middle-income countries where owing to limited resources, clinicians may prescribe antibiotics without performing a urine culture and sensitivity test [51]. None of our isolates were resistant to co-amoxiclav, similar to studies performed in Ethiopia [49,52] but contrary to other studies in Uganda and Ethiopia [6,46,53]. The 50% resistance to TMP/SMX we observed was similar to the findings of Ali et al. from Somalia [54]. This study revealed a low rate of resistance to erythromycin and tetracycline, which was different from the findings of a multicenter study involving 400 pregnant women with asymptomatic bacteriuria from Ghana [55]. The observed high prevalence of antimicrobial resistance to commonly used antibiotics may be attributed to the easy availability of commonly prescribed antimicrobials over-the-counter combined with the misuse of antibiotics by both patients and clinicians and a lack of trained personnel for urine culture [52]. This could also be due to a la [56]ck of regulation of the prescription of these drugs and their sale by local pharmacies [13,30].
E. coli, the predominant gram-negative isolate, was sensitive to ceftriaxone, nitrofurantoin and nalidixic acid (all 100%) but resistant to ampicillin and cefuroxime. The 100% sensitivity of E. coli to Ceftriaxone is similar to what Derese et al. reported in a small study in Ethiopia [20] but disagrees with the findings of Ngong et al. [57] and Asmat and colleagues [58]. Abu et al. [52] reported high resistance to tetracycline, which was different from the findings of the present study and those of Agarwal et al. This study revealed high resistance to ampicillin in E. coli, which is in line with the findings of Derese et al. [20] and two Gambian studies [13,14]. This finding is worrying considering that ampicillin is the most commonly prescribed antibiotic for UTIs during pregnancy in Gambia. This implies that changes may be needed in the treatment protocols used. With the exception of gentamicin, S. aureus was sensitive to all the drugs tested in this study. There was no methicillin resistance in S. aureus, as shown previously in this setting by Darboe et al. [59] and was also reported in a study of asymptomatic pregnant women by Onanuga and colleagues in Nigeria [60]. These differences could be due to variations in antibiotic prescription patterns across various countries, different costs of the drugs and their availability.
Limitations of the Study
There are several limitations to this study worth noting. This was a short-term study involving only pregnant women who attended the participating hospitals in urban areas; hence, this might limit inference of the results to the general population of the country. Information such as sexual activity, which is considered a risk factor, could not be assessed because the women in the study area did not feel comfortable giving out such details. However, this did not affect the study, as its purpose was still to be carried out. Few drugs were tested due to the limited availability of funds, hence limiting us to the drug discs available to the hospital at every given point. This study also involved a small number of participants. To relate the results to the entire country, another has to be done with a larger sample size and longer time period to include women from rural areas. However, the results of this study add to the body of knowledge concerning the prevalence of AMR among pregnant women at antenatal clinics and their knowledge of UTIs in low-income countries such as Gambia.
5. Conclusions
We detected a low prevalence of community-acquired UTIs, possibly because this study was performed over a short period and in urban centers where patients have a high literacy rate and easy access to medical care. Escherichia coli, as expected, was the most common causative organism, and except for ampicillin and trimethoprim/sulfamethoxazole, susceptibility to commonly used drugs was high. These findings also show that ceftriaxone, nitrofurantoin, erythromycin and nalidixic acid can be used as empiric treatments when culture-specific sensitivities are not available. We recommend that routine surveillance and monitoring studies be conducted to update clinicians on prevalent pathogens and the rational and empirical treatment of UTIs. The choice of antimicrobial therapy during pregnancy should be determined according to sensitivity and resistance for foeto-maternal safety.
Author Contributions
Conceptualization, Mustapha Sowe, Abdoulie Keita and Abdoulie Badjan; Data curation, Mustapha Sowe; Formal analysis, Mustapha Sowe, Abdoulie Keita and Abdoulie Badjan; Investigation, Mustapha Sowe, Kalifa Sanneh, Kelefa Secka and Abdoulie Badjan; Methodology, Mustapha Sowe, Abdoulie Keita, Saffiatou Darboe and Abdoulie Badjan; Project administration, Mustapha Sowe; Resources, Mustapha Sowe, Kalifa Sanneh, Kelefa Secka and Abdoulie Badjan; Software, Mustapha Sowe; Supervision, Abdoulie Keita and Abdoulie Badjan; Validation, Mustapha Sowe, Abdoulie Keita and Abdoulie Badjan; Visualization, Mustapha Sowe, Abdoulie Keita and Abdoulie Badjan; Writing—original draft, Mustapha Sowe, Abdoulie Keita, Saffiatou Darboe, Ousman Bajinka and Abdoulie Badjan; Writing—review & editing, Mustapha Sowe, Abdoulie Keita, Saffiatou Darboe, Ousman Bajinka and Abdoulie Badjan.
Funding
No funding was received for this research.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Ethics approval was obtained from the ethics committee of the University of the Gambia School of Medicine and Allied Health Sciences, Edward Francis Small Teaching Hospital (reference number EFSTH_REC_2022_111), and permission was obtained from all the hospitals involved in the study (Edward Francis Small Teaching Hospital (EFSTH), Kanifing General Hospital (KGH) and Bundung Maternal and Child Health Hospital (BMCHH)) before the commencement of the study. Confidentiality and privacy were strictly observed, and the participants were informed of their personal rights and benefits. In addition, pregnant women were informed of the rationale of the study via a patient information sheet and signed a written consent form before being chosen as participants.
Data Availability Statement
The data supporting the findings of the article are available upon request from the authors. They include:
Acknowledgments
This work would not have been possible without the immense support and guidance of my supervisors Dr Abdoulie Badjan and Dr Abdoulie Keita. They not only enlighten me with academic knowledge but also motivated and inspired me throughout this work. Special thanks to PhD candidates Saffiatou Darboe and Dr Ousman Bajinka for their immense support and contribution to manuscript writing. I want to especially thank the amazing nurses at the antenatal clinics and the microbiology laboratory staff of Edward Francis Small Teaching Hospital, Kanifing General Hospital and Bundung Maternal and Child Health Hospital for taking time off their busy schedules to assist me in this work. I also want to say big thank you to Mr. Kelefa Secka and Mr. Kalifa Sanneh for their work on this.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
List of Abbreviations
List of Abbreviations
| AMR | Antimicrobial resistance |
| E. coli | Escherichia coli |
| S. aureus | Staphylococcus aureus |
| C. freundii | Citrobacter freundii |
| GDP | Gross Domestic Product |
| USD | United States Dollars |
| WHO | World Health Organization |
| UTI | Urinary tract infection |
| EUA | European Urology Association |
| ASB | Asymptomatic bacteriuria |
| MDR | Multidrug resistant |
| ANC | Antenatal clinic |
| EFSTH | Edward Francis Small Teaching Hospital |
| KGH | Kanifing General Hospital |
| BMCHH | Bundung Maternal and Child Health Hospital |
| CFU | Colony forming units |
| GMD | Gambian Dalasi |
| LMICs | Low- to middle-income countries |
| DNA | Deoxyribonucleic acid |
| CLED | Cysteine lactose electrolyte-deficient agar |
| MAC | MacConkey agar |
| MHA | Mueller‒Hinton agar |
| CLSI | Clinical and Laboratory Standards Institute |
References
- Chelkeba, L.; Fanta, K.; Mulugeta, T.; Melaku, T. Bacterial profile and antimicrobial resistance patterns of common bacteria among pregnant women with bacteriuria in Ethiopia: a systematic review and meta-analysis. Arch. Gynecol. Obstet. 2022, 306, 663–686. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Khoshbakht, Y.; Hemmati, M.; Khodayari, Y.; Khaleghi, A.; Jafari, F.; Shohaimi, S.; Mohammadi, M. Global prevalence of urinary tract infection in pregnant mothers: a systematic review and meta-analysis. Public Heal. 2023, 224, 58–65. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis,” Lancet, vol. 399, pp. 629–55, 2022.
- B. M. A and S. M, “A Systematic Review on Drug Resistant Urinary Tract Infection Among Pregnant Women in Developing Countries in Africa and Asia; 2005–2016,” Infect. Drug Resist., vol. 13, pp. 1465–77, 2020.
- J. Marcon, C. G. Stief, and G. Magistro, “Harnwegsinfektionen: Was ist gesichert in der Therapie?,” Internist, vol. Dec;58(12):1242–9, 2017.
- Johnson, B.; Stephen, B.M.; Joseph, N.; Asiphas, O.; Musa, K.; Taseera, K. Prevalence and bacteriology of culture-positive urinary tract infection among pregnant women with suspected urinary tract infection at Mbarara regional referral hospital, South-Western Uganda. BMC Pregnancy Childbirth 2021, 21, 159. [Google Scholar] [CrossRef] [PubMed]
- Azami, M.; Jaafari, Z.; Masoumi, M.; Shohani, M.; Badfar, G.; Mahmudi, L.; Abbasalizadeh, S. The etiology and prevalence of urinary tract infection and asymptomatic bacteriuria in pregnant women in Iran: a systematic review and Meta-analysis. BMC Urol. 2019, 19, 43. [Google Scholar] [CrossRef] [PubMed]
- S. Aydoğmuş and E. Kaya Kiliç, “Determination of antibiotic resistance rates of Escherichia coli and Klebsiella pneumoniae isolates, which are the causative agents of urinary tract infection in pregnant women,” Anatol. Curr Med JACMJacmj, vol. 27;5(2):97–101, Mar. 2023.
- Abushaheen, M.A.; Fatani, A.J.; Alosaimi, M.; Mansy, W.; George, M.; Acharya, S.; Rathod, S.; Divakar, D.D.; Jhugroo, C.; et al. Antimicrobial resistance, mechanisms and its clinical significance. Dis. Mon. 2020, 66, 100971. [Google Scholar] [CrossRef]
- Ndmason, L.M.; Marbou, W.J.; Kuete, V. Urinary tract infections, bacterial resistance and immunological status: a cross sectional study in pregnant and non-pregnant women at Mbouda Ad-Lucem Hospital. Afr. Heal. Sci. 2019, 19, 1525–1535. [Google Scholar] [CrossRef]
- Adedze-Kpodo, R.K.; Feglo, P.K.; Agboli, E.; Asmah, R.H.; Kwadzokpui, P.K. Genotypic characterization of extended-spectrum β-lactamase producing urinary isolates among pregnant women in Ho municipality, Ghana. Heliyon 2022, 8, e12513. [Google Scholar] [CrossRef]
- Al Lawati, H.; Blair, B.M.; Larnard, J. Urinary Tract Infections: Core Curriculum 2024. Am. J. Kidney Dis. 2024, 83, 90–100. [Google Scholar] [CrossRef]
- Darboe, S.; Mirasol, R.; Adejuyigbe, B.; Muhammad, A.K.; Nadjm, B.; Maurice, A.D.S.; Dogan, T.L.; Ceesay, B.; Umukoro, S.; Okomo, U.; et al. Using an Antibiogram Profile to Improve Infection Control and Rational Antimicrobial Therapy in an Urban Hospital in The Gambia, Strategies and Lessons for Low- and Middle-Income Countries. Antibiotics 2023, 12, 790. [Google Scholar] [CrossRef]
- Kebbeh, A.; Dsane-Aidoo, P.; Sanyang, K.; Darboe, S.M.K.; Fofana, N.; Ameme, D.; Sanyang, A.M.; Darboe, K.S.; Darboe, S.; Sanneh, B.; et al. Antibiotics susceptibility patterns of uropathogenic bacteria: a cross-sectional analytic study at Kanifing General Hospital, The Gambia. BMC Infect. Dis. 2023, 23, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sifri, Z.; Chokshi, A.; Cennimo, D.; Horng, H. Global contributors to antibiotic resistance. J. Glob. Infect. Dis. 2019, 11, 36–42. [Google Scholar] [CrossRef] [PubMed]
- A.J. A, N. M, and A. A. N, “The threat of antimicrobial resistance in developing countries: causes and control strategies,” Antimicrob. Resist. Infect. Control, vol. 6, no. 47, 2017.
- E. Britannica, “The Gambia summary” [Internet] [Internet.” 2020. [Online]. Available: https://www.britannica.com/summary/The-Gambia.
- C. C. Serdar, M. Cihan, D. Yücel, and M. A. Serdar, “Sample size, power and effect size revisited: simplified and practical approaches in preclinical, clinical and laboratory studies,” Biochem Med Zagreb, vol. 15;31(1):010502, Feb. 2021.
- M. Ali and A. M.S, “Prevalence of Urinary Tract Infection among Pregnant Women in Kano, Nothern Nigeria,” Arch. Reprod. Med. Sex. Health, vol. 2, no. Issue 1, pp. 23–9, 2019.
- Balakrishnan, S.; Derese, B.; Kedir, H.; Teklemariam, Z.; Weldegebreal, F. Bacterial profile of urinary tract infection and antimicrobial susceptibility pattern among pregnant women attending at Antenatal Clinic in Dil Chora Referral Hospital, Dire Dawa, Eastern Ethiopia. Ther. Clin. Risk Manag. 2016, 12, 251–260. [Google Scholar] [CrossRef]
- M. Cheesbrough, District Laboratory Practice in Tropical Countries, 2nd ed. London, UK: Cambridge University Press, 2006.
- P. M. Tille, Bailey & Scott’s diagnostic microbiology, Fifteenth Edition. St. Louis, Missouri: Elsevier, 2022.
- B. A. W, K. W. M, S. J. C, and T. M, “Antibiotic susceptibility testing by a standardized single disk method,” Am. J. Clin. Pathol., vol. 45, no. 4, pp. 493–6, 1966.
- C.L.S.I., Performance Standards for Antimicrobial Susceptibility Testing, 27th ed., vol. 37. Wayne, PA: Clinical and Laboratory Standards Institute, 2019.
- Rosana, Y.; Ocviyanti, D.; Halim, M.; Harlinda, F.Y.; Amran, R.; Akbar, W.; Billy, M.; Akhmad, S.R.P. Urinary Tract Infections among Indonesian Pregnant Women and Its Susceptibility Pattern. Infect. Dis. Obstet. Gynecol. 2020, 2020, 9681632–7. [Google Scholar] [CrossRef]
- Kant, S.; Lohiya, A.; Kapil, A.; Gupta, S. Urinary tract infection among pregnant women at a secondary level hospital in Northern India. Indian J. Public Heal. 2017, 61, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Tula, A.; Mikru, A.; Alemayehu, T.; Dobo, B. Bacterial Profile and Antibiotic Susceptibility Pattern of Urinary Tract Infection among Pregnant Women Attending Antenatal Care at a Tertiary Care Hospital in Southern Ethiopia. Can. J. Infect. Dis. Med Microbiol. 2020, 2020, 1–9. [Google Scholar] [CrossRef]
- Rejali, M.; Ahmadi, S.S. Prevalence and Risk Factors of Urinary Tract Infection among Pregnant Women in Shahrekord, Iran. Int. J. epidemiologic Res. 2019, 6, 55–59. [Google Scholar] [CrossRef]
- Orji, O.; Dlamini, Z.; Wise, A.J. Urinary bacterial profile and antibiotic susceptibility pattern among pregnant women in Rahima Moosa Mother and Child Hospital, Johannesburg. South. Afr. J. Infect. Dis. 2022, 37, 8. [Google Scholar] [CrossRef]
- Nteziyaremye, J.; Iramiot, S.J.; Nekaka, R.; Musaba, M.W.; Wandabwa, J.; Kisegerwa, E.; Kiondo, P. Asymptomatic bacteriuria among pregnant women attending antenatal care at Mbale Hospital, Eastern Uganda. PLOS ONE 2020, 15, e0230523. [Google Scholar] [CrossRef]
- Mohamed, N.R.; Omar, H.H.H.; Abd-Allah, I.M. Prevalence and Risk Factors of Urinary Tract Infection among Pregnant Women in Ismailia City, Egypt. IOSR J. Nurs. Heal. Sci. 2017, 6, 62–72. [Google Scholar] [CrossRef]
- B. R. Oyedeji, G. O. Daramola, H. A. Edogun, O. O. Ogunfolakan, H. A. Egbebi, and A. O. Ojerinde, “Polybacteria in Urinary Tract Infection among Antenatal Patients.” Attending University Teaching Hospital Ado-Ekiti, Ekiti State, Nigeria.
- H. ohamoud, S. Tadesse, and A. Derbie, “Antimicrobial resistance and ESBL profile of Uropathogens among pregnant women at Edna Adan Hospital, Hargeisa, Somaliland,” Ethiop J Health Sci, vol. May;31(3):645–52, 2021.
- Negussie, G.A. Worku, and E. Beyene, “Bacterial identification and drug susceptibility pattern of urinary tract infection in pregnant Women at Karamara Hospital Jigjiga, Eastern Ethiopia,” Afr. J. Bacteriol. Res., vol. 10, no. 2, pp. 15–22, Jul. 2018.
- T. N. C, O. E. C, N. C. C, E. E. C, N. N. T, and M. E, “Clinical presentation, risk factors and pathogens involved in bacteriuria of pregnant women attending antenatal clinic of 3 hospitals in a developing country: a cross sectional analytic study,” BMC Pregnancy Childbirth, vol. Dec;19(1):143, 2019.
- Fosu, K.; Quansah, E.; Dadzie, I. Antimicrobial Profile and Asymptomatic Urinary Tract Infections among Pregnant Women Attending Antenatal Clinic in Bolgatanga Regional Hospital, Ghana. Microbiol. Res. J. Int. 2019, 1–8. [Google Scholar] [CrossRef]
- Matalka, A.; Al-Husban, N.; Alkuran, O.; Almuhaisen, L.; Basha, A.; Eid, M.; Elmuhtaseb, M.S.; Al Oweidat, K. Spectrum of uropathogens and their susceptibility to antimicrobials in pregnant women: a retrospective analysis of 5-year hospital data. J. Int. Med Res. 2021, 49. [Google Scholar] [CrossRef] [PubMed]
- L. A.-K. MM, “Urinary Tract Infection among Pregnant Women and its Associated Risk Factors: A Cross-Sectional Study,” Biomed Pharmacol J, vol. 31;12(04):2003–10, Dec. 2019.
- A.O. Forson, W. B. Tsidi, D. Nana-Adjei, M. N. Quarchie, and N. Obeng-Nkrumah, “Escherichia coli bacteriuria in pregnant women in Ghana: antibiotic resistance patterns and virulence factors,” BMC Res Notes, vol. Dec;11(1):901, 2018.
- Karikari, A.B.; Saba, C.K.S.; Yamik, D.Y. Assessment of asymptomatic bacteriuria and sterile pyuria among antenatal attendants in hospitals in northern Ghana. BMC Pregnancy Childbirth 2020, 20, 1–7. [Google Scholar] [CrossRef]
- E. Nwachukwu, “Prevalence of urinary tract infections in pregnant women in Onitsha.” Nigeria. [Online]. Available: https://medcraveonline.com/JBMOA/prevalence-of-urinary-tract-infections-in-pregnant-women-in-onitsha-nigeria.
- Oli, A.N.; Akabueze, V.B.; Ezeudu, C.E.; Eleje, G.U.; Ejiofor, O.S.; Ezebialu, I.U.; Oguejiofor, C.B.; Ekejindu, I.M.; Emechebe, G.O.; Okeke, K.N. Bacteriology and Antibiogram of Urinary Tract Infection Among Female Patients in a Tertiary Health Facility in South Eastern Nigeria. Open Microbiol. J. 2017, 11, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Wabe, Y.A.; Reda, D.Y.; Abreham, E.T.; Gobene, D.B.; Ali, M.M. Prevalence of Asymptomatic Bacteriuria, Associated Factors and Antimicrobial Susceptibility Profile of Bacteria Among Pregnant Women Attending Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia. Ther. Clin. Risk Manag. 2020, ume 16, 923–932. [Google Scholar] [CrossRef]
- de Souza, H.D.; Diório, G.R.M.; Peres, S.V.; Francisco, R.P.V.; Galletta, M.A.K. Bacterial profile and prevalence of urinary tract infections in pregnant women in Latin America: a systematic review and meta-analysis. BMC Pregnancy Childbirth 2023, 23, 1–15. [Google Scholar] [CrossRef]
- M. Younis, S. Ajroud, E. L. H. A, U. A. S, and E. R. A, “Prevalence of Urinary Tract Infection among Pregnant Women and Its Risk Factor in Derna City,” Sch. Int. J. Obstet. Gynecol., vol. Aug;2(8):219–23, 2019.
- Ejerssa, A.W.; Gadisa, D.A.; Orjino, T.A. Prevalence of bacterial uropathogens and their antimicrobial susceptibility patterns among pregnant women in Eastern Ethiopia: hospital-based cross-sectional study. BMC Women's Heal. 2021, 21, 1–15. [Google Scholar] [CrossRef]
- Yeta, K.I.; Michelo, C.; Jacobs, C. Antimicrobial Resistance among Pregnant Women with Urinary Tract Infections Attending Antenatal Clinic at Levy Mwanawasa University Teaching Hospital (LMUTH), Lusaka, Zambia. Int. J. Microbiol. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Koffi, K.A.; Aka, E.K.; Apollinaire, H.; Britoh, A.M.; Konan, J.M.P. Epidemiological, bacteriological profile and bacterial resistance of urinary tract infections at pregnant woman in prenatal consultation in African setting. Int. J. Reprod. Contraception, Obstet. Gynecol. 2020, 9, 461–467. [Google Scholar] [CrossRef]
- Taye, S.; Getachew, M.; Desalegn, Z.; Biratu, A.; Mubashir, K. Bacterial profile, antibiotic susceptibility pattern and associated factors among pregnant women with Urinary Tract Infection in Goba and Sinana Woredas, Bale Zone, Southeast Ethiopia. BMC Res. Notes 2018, 11, 799. [Google Scholar] [CrossRef]
- Corrales, M.; Corrales-Acosta, E.; Corrales-Riveros, J.G. Which Antibiotic for Urinary Tract Infections in Pregnancy? A Literature Review of International Guidelines. J. Clin. Med. 2022, 11, 7226. [Google Scholar] [CrossRef] [PubMed]
- Al Kadri, H.M.; El-Metwally, A.A.; Al Sudairy, A.A.; Al-Dahash, R.A.; Al Khateeb, B.F.; Al Johani, S.M. Antimicrobial resistance among pregnant women with urinary tract infections is on rise: Findings from meta-analysis of observational studies. J. Infect. Public Heal. 2024, 17, 102467. [Google Scholar] [CrossRef] [PubMed]
- Abu, D.; Abula, T.; Zewdu, T.; Berhanu, M.; Sahilu, T. Asymptomatic Bacteriuria, antimicrobial susceptibility pattern and associated risk factors among pregnant women attending antenatal care in Assosa General Hospital, Western Ethiopia. BMC Microbiol. 2021, 21, 348. [Google Scholar] [CrossRef]
- K. Bizuwork, H. K. Bizuwork, H. Alemayehu, G. Medhin, W. Amogne, and T. Eguale, “Asymptomatic Bacteriuria among Pregnant Women in Addis Ababa, Ethiopia: Prevalence, Causal Agents, and Their Antimicrobial Susceptibility,” Int. J. Microbiol., vol. 2021, pp. 1–8, Jul. 2021.
- Ali, A.H.; Reda, D.Y.; Ormago, M.D. Prevalence and antimicrobial susceptibility pattern of urinary tract infection among pregnant women attending Hargeisa Group Hospital, Hargeisa, Somaliland. Sci. Rep. 2022, 12, 1419. [Google Scholar] [CrossRef]
- Karikari, A.B.; Saba, C.K.S.; Yamik, D.Y. Assessment of asymptomatic bacteriuria and sterile pyuria among antenatal attendants in hospitals in northern Ghana. BMC Pregnancy Childbirth 2020, 20, 239. [Google Scholar] [CrossRef]
- Agarwal, A.; Pandey, S.; Maheshwari, U.; Singh, M.; Srivastava, J.; Bose, S. Prevalence of asymptomatic bacteriuria and antimicrobial resistance profile among pregnant females in a Tertiary Care Hospital. Indian J. Community Med. 2021, 46, 469–473. [Google Scholar] [CrossRef]
- Ngong, I.N.; Fru-Cho, J.; Yung, M.A.; Akoachere, J.-F.K.T. Prevalence, antimicrobial susceptibility pattern and associated risk factors for urinary tract infections in pregnant women attending ANC in some integrated health centers in the Buea Health District. BMC Pregnancy Childbirth 2021, 21, 673. [Google Scholar] [CrossRef]
- Asmat, U.; Mumtaz, M.Z.; Malik, A. Rising prevalence of multidrug-resistant uropathogenic bacteria from urinary tract infections in pregnant women. J. Taibah Univ. Med Sci. 2021, 16, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Darboe, S.; Dobreniecki, S.; Jarju, S.; Jallow, M.; Mohammed, N.I.; Wathuo, M.; Ceesay, B.; Tweed, S.; Roy, R.B.; Okomo, U.; et al. Prevalence of Panton-Valentine Leukocidin (PVL) and Antimicrobial Resistance in Community-Acquired Clinical Staphylococcus aureus in an Urban Gambian Hospital: A 11-Year Period Retrospective Pilot Study. Front. Cell. Infect. Microbiol. 2019, 9, 170. [Google Scholar] [CrossRef]
- Onanuga, A.; Omeje, M.C.; Eboh, D.D. Carriage of multi-drug resistant urobacteria by asymptomatic pregnant women in yenagoa, bayelsa state, nigeria. Afr. J. Infect. Dis. 2018, 12, 14–20. [Google Scholar] [CrossRef]
Figure 1.
Isolated bacterial uropathogens from pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
Figure 1.
Isolated bacterial uropathogens from pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
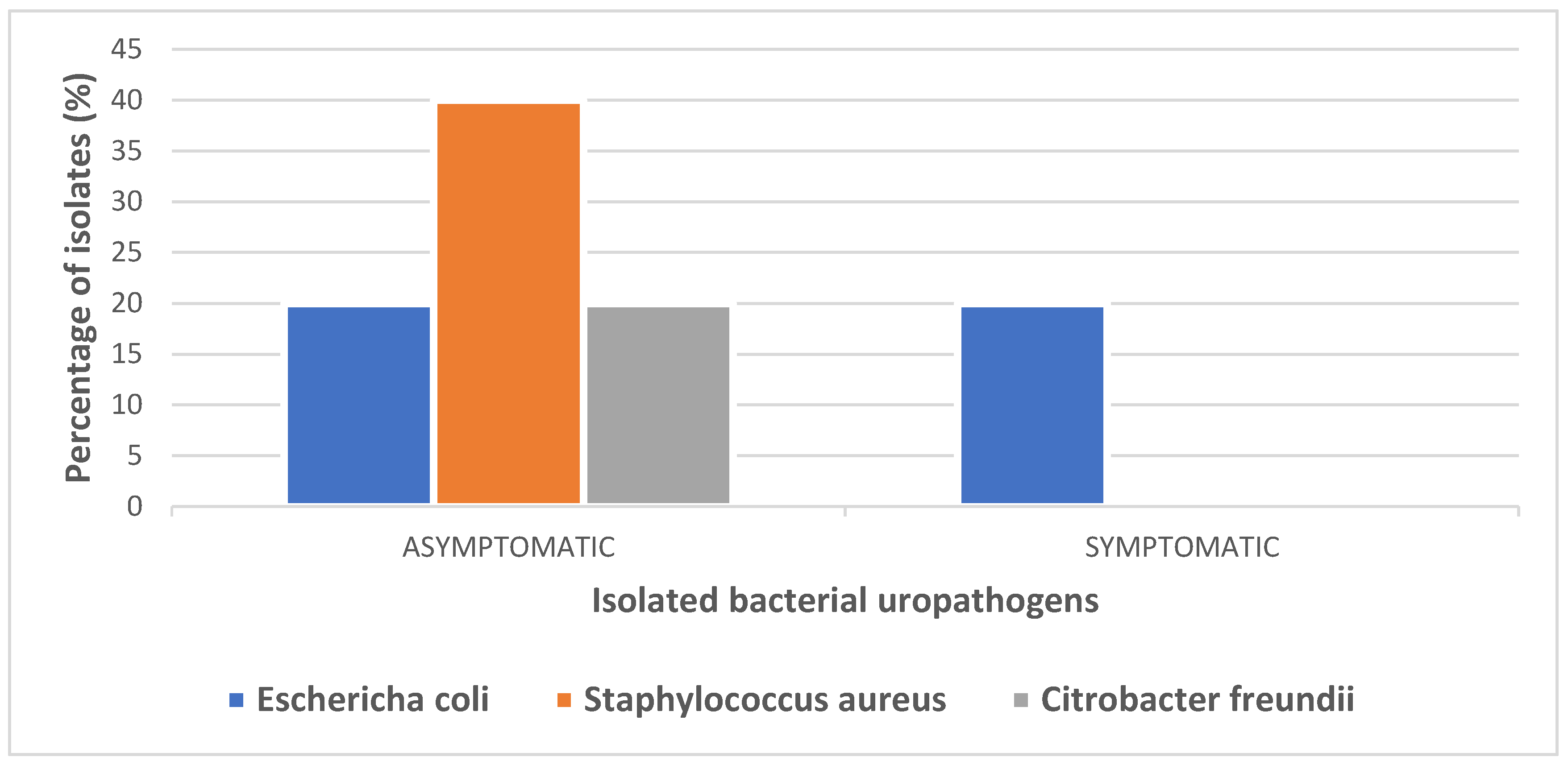
Figure 2.
Symptomatic and asymptomatic UTIs among pregnant women at the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
Figure 2.
Symptomatic and asymptomatic UTIs among pregnant women at the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
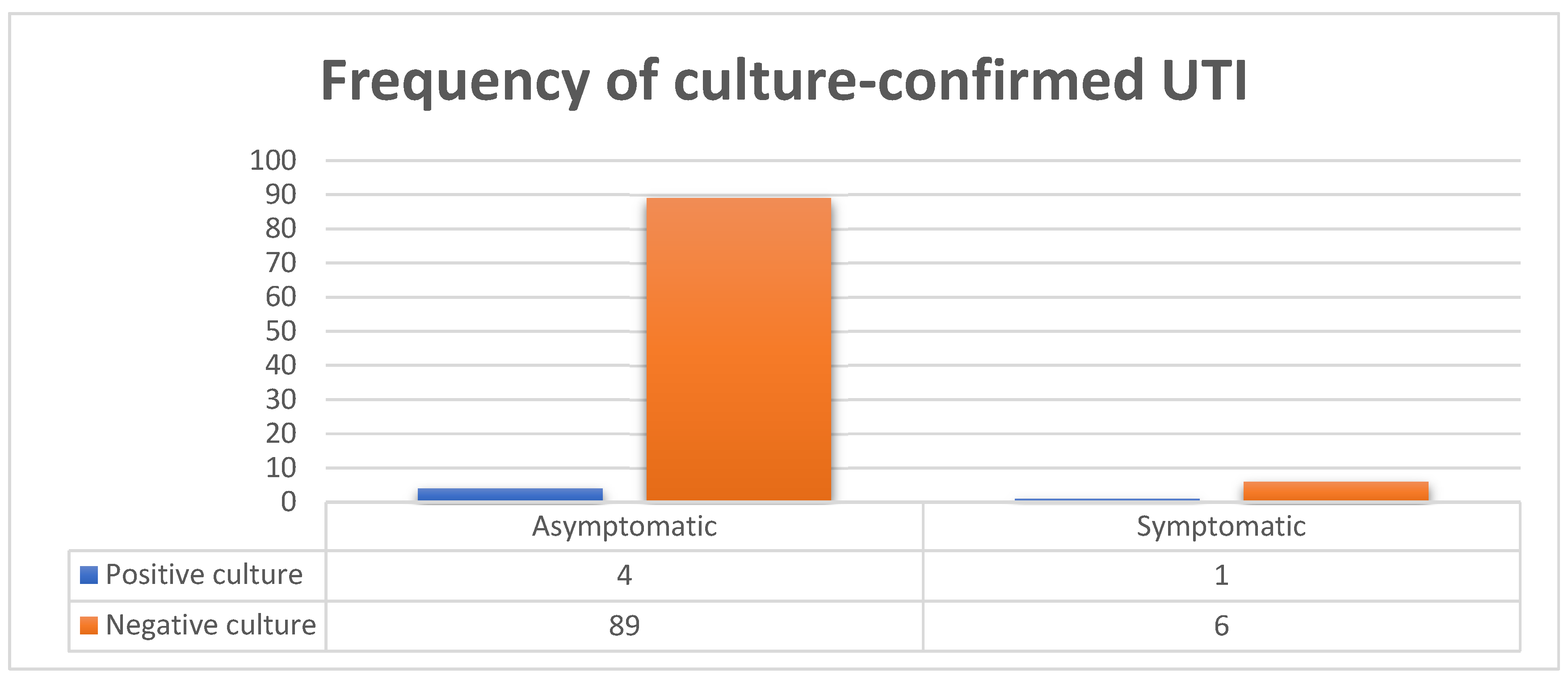
Figure 3.
Overall antimicrobial susceptibility patterns of bacterial pathogens isolated from the urine of pregnant women at the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023. Abbreviations: AMC: amoxicillin-clavulanate, AMP: ampicillin, CIP: ciprofloxacin, GEN: gentamicin, CEF: ceftriaxone, CTZ: ceftazidime, TSX: cotrimoxazole, NAL: nalidixic acid NIT: nitrofurantoin, MET: methicillin, CRX: cefuroxime, TET: tetracycline and ERY: erythromycin.
Figure 3.
Overall antimicrobial susceptibility patterns of bacterial pathogens isolated from the urine of pregnant women at the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023. Abbreviations: AMC: amoxicillin-clavulanate, AMP: ampicillin, CIP: ciprofloxacin, GEN: gentamicin, CEF: ceftriaxone, CTZ: ceftazidime, TSX: cotrimoxazole, NAL: nalidixic acid NIT: nitrofurantoin, MET: methicillin, CRX: cefuroxime, TET: tetracycline and ERY: erythromycin.
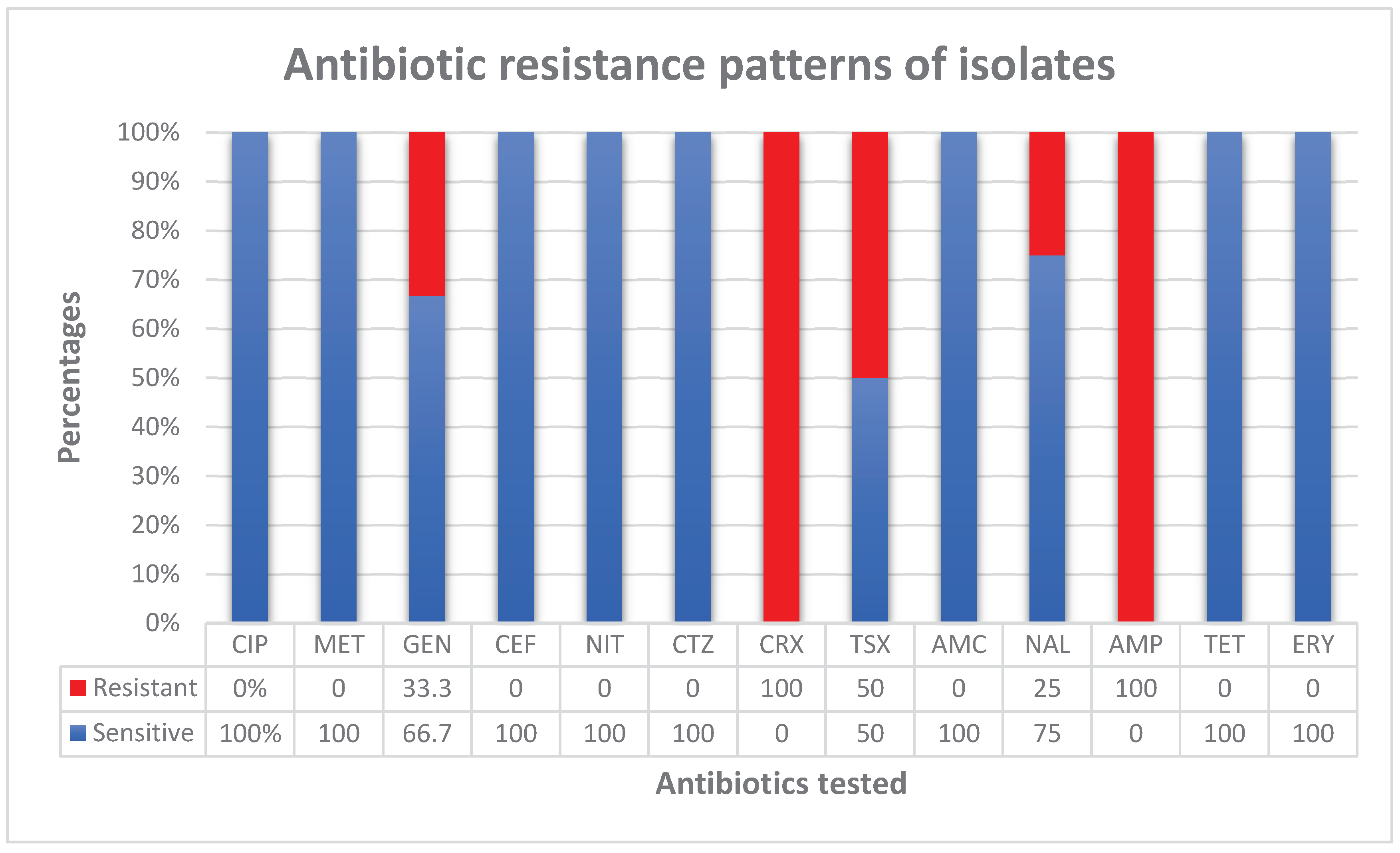

Table 1.
Sociodemographic, obstetric, and clinical variables of pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023. (n=100).
Table 1.
Sociodemographic, obstetric, and clinical variables of pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023. (n=100).
| VARIABLE | PARTICIPANTS (n=100) | |
|---|---|---|
| Frequency | Percentage | |
|
Hospital KGH BMCHH EFSTH |
52 34 14 |
52 34 14 |
|
Age Less than 20 20–24 25–29 30–34 35–39 40 and above |
6 26 28 21 16 3 |
6 26 28 21 16 3 |
|
Residence Urban Rural |
100 0 |
100 0 |
|
Level of education No formal education Primary (1-6) Secondary (7-12) Tertiary |
23 11 49 17 |
23 11 49 17 |
|
Occupation Housewife Student Self employed Employee (Government or private) |
48 9 29 14 |
48 9 29 14 |
|
Marital status Single Married |
2 98 |
2 98 |
|
Gravidity Primigravida Multigravida |
31 69 |
31 69 |
|
Parity Nullipara Primipara Multipara |
33 23 44 |
33 23 44 |
|
Estimated Gestational Age 1st trimester 2nd trimester 3rd trimester |
7 30 63 |
7 30 63 |
|
History of UTI Yes No |
37 63 |
37 63 |
| History of catheterization | 0 | 0 |
|
History of antibiotic use without prescription Yes No |
29 71 |
29 71 |
|
Comorbidity present Diabetes mellitus HIV/AIDS Renal disease Others |
1 0 0 10 |
1 0 0 10 |
|
Symptomatic Yes No |
7 93 |
7 93 |
Table 2.
Sociodemographic, obstetric, and clinical variables and culture status of pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023. (n=100).
Table 2.
Sociodemographic, obstetric, and clinical variables and culture status of pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023. (n=100).
| VARIABLE | PARTICIPANTS (n=100) | CULTURE STATUS | |||
|---|---|---|---|---|---|
| Frequency | Percentage | POSITIVE no (%) (n=5) | NEGATIVE no (%) (n=95) | p value (X2) | |
|
Hospital KGH BMCHH EFSTH |
52 34 14 |
52 34 14 |
0 (0) 4 (80) 1 (20) |
52 (54.7) 30 (31.6) 13 (13.7) |
0.046 |
|
Age Less than 20 20–24 25–29 30–34 35–39 40 and above |
6 26 28 21 16 3 |
6 26 28 21 16 3 |
1 (20) 1 (20) 1 (20) 2 (40) 0 (0) 0 (0) |
5 (5.3) 25 (26.3) 27 (28.4) 19 (20) 16 (16.8) 3 (3.2) |
0.363 |
|
Residence Urban Rural |
97 3 |
97 3 |
5 (100) 0 (0) |
92 (96.8) 3 (3.2) |
0.687 |
|
Level of education No formal education Primary (1-6) Secondary (7-12) Tertiary |
23 11 49 17 |
23 11 49 17 |
2 (40) 0 (0) 2 (40) 1 (20) |
21 (22.1) 11 (11.6) 47 (49.5) 16 (16.8) |
0.716 |
|
Occupation Housewife Student Self employed Employee (Government or private) |
48 9 29 14 |
48 9 29 14 |
4 (80) 0 (0) 1 (10) 0 (0) |
44 (46.3) 9 (9.5) 28 (29.5) 14 (14.7) |
0.437 |
|
Marital status Single Married |
2 98 |
2 98 |
0 (0) 5 (100) |
2 (2.1) 93 (97.9) |
0.743 |
|
Gravidity Primigravida Multigravida |
31 69 |
31 69 |
1 (20) 4 (80) |
30 (31.6) 65 (68.4) |
0.687 |
|
Parity Nullipara Primipara Multipara |
33 23 44 |
33 23 44 |
1 (20) 3 (60) 1 (20) |
32 (33.7) 20 (21) 43 (45.3) |
0.129 |
|
Estimated Gestational Age 1st trimester 2nd trimester 3rd trimester |
7 30 63 |
7 30 63 |
0 (0) 3 (60) 2 (40) |
7 (7.4) 27 (28.4) 61 (64.2) |
0.303 |
|
History of UTI Yes No |
37 63 |
37 63 |
2 (40) 3 (60) |
35 (36.8) 60(63.2) |
0.887 |
| History of catheterization | 0 | 0 | 0 | 0 | |
|
History of antibiotic use without prescription Yes No |
29 71 |
29 71 |
2 (40) 3 (60) |
27 (28.4) 68 (71.6) |
0.841 |
|
History of diabetes mellitus Yes No |
1 99 |
1 99 |
0 (0) 5 (100) |
1 (1.1) 94 (98.9) |
0.818 |
|
Symptomatic Yes No |
7 93 |
7 93 |
1 (20) 4 (80) |
6 (6.3) 89 (93.7) |
0.242 |
Table 3.
Isolated bacterial pathogens from pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
Table 3.
Isolated bacterial pathogens from pregnant women who attended the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
| BACTERIAL ISOLATES | ASYMPTOMATIC | SYMPTOMATIC | TOTAL(n=100) |
|---|---|---|---|
| Escherichia coli | 1 | 1 | 2(40%) |
| Staphylococcus aureus | 2 | 0 | 2(40%) |
| Citrobacter freundii | 1 | 0 | 1(20%) |
| TOTAL | 4 | 1 | 5(100%) |
Table 4.
Antimicrobial susceptibility patterns of bacteria isolated from the urine of pregnant women at the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
Table 4.
Antimicrobial susceptibility patterns of bacteria isolated from the urine of pregnant women at the antenatal clinics of EFSTH, BMCHH and KGH from November 2022 to January 2023.
| BACTERIAL ISOLATES | Escherichia coli | Staphylococcus aureus | Citrobacter freundii | TOTAL | |||||
|---|---|---|---|---|---|---|---|---|---|
| Total | 2 | 2 | 1 | 5 | |||||
| SUSCEPTIBILITY | S | R | S | R | S | R | S | R | |
| ANTIBIOTICS TESTED/NO OF ISOLATES | CIP | - | - | 1 | - | - | - | 1 | - |
| MET | - | - | 1 | - | - | - | 1 | - | |
| GEN | 1 | - | - | 1 | 1 | 0 | 2 | 1 | |
| CEF | 2 | 0 | - | - | 1 | 0 | 3 | - | |
| NIT | 2 | 0 | 1 | - | 1 | 0 | 4 | - | |
| CTZ | 1 | - | - | - | - | - | 1 | - | |
| CRX | - | 1 | - | - | - | - | - | 1 | |
| TSX | 1 | - | - | - | 0 | 1 | 1 | 1 | |
| AMC | 1 | - | 1 | - | - | - | 2 | - | |
| NAL | 2 | 0 | 1 | - | 0 | 1 | 3 | 1 | |
| AMP | - | 1 | - | - | 0 | 1 | - | 2 | |
| TET | 1 | - | 2 | 0 | - | - | 3 | - | |
| ERY | - | - | 2 | 0 | - | - | 2 | - | |
Key: “- “= Not available or not tested for. S: Sensitive, R: Resistant, AMC: amoxicillin-clavulanate, AMP: ampicillin, CIP: ciprofloxacin, GEN: gentamicin, CEF: ceftriaxone, CTZ: ceftazidime, TSX: cotrimoxazole, NAL: nalidixic acid NIT: nitrofurantoin, MET: methicillin, CRX: cefuroxime, TET: tetracycline and ERY: erythromycin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



