
Submitted:
06 May 2025
Posted:
07 May 2025
You are already at the latest version
Abstract
Introduction: De novo metastatic breast cancer (dnMBC) accounts for 3–10% of newly diagnosed cases, with 20–40% presenting as a bone-only metastatic disease (dnBOMBC), which can achieve survival outcomes exceeding 10 years with multimodal therapy. However, the role of multimodal therapy remains controversial in the guidelines. Objective: This study aims to identify dnBOMBC subgroups to develop a pragmatic staging system for guiding locoregional therapy decisions. Materials and Methods: Data from the MF07-01 phase III randomized trial (2021, median follow-up time (mFT): 40 months (range 1-131)), and the BOMET prospective multi-institutional registry trial (2021, mFT: 34 months (range 25-45)), were combined for analysis, including only patients who presented with bone-only metastases. Exclusion criteria were patients under 18 and those with a history of prior cancer or cancer metastases. Patients with missing data and positive surgical margins were excluded. Out of 770 patients, 589 were included. Survival analyses were first conducted according to molecular subgroups, after which patients were further stratified by hormone receptor status, HER2 status, tumor grade, and clinical T (cT) stage. Group A (GrA) included HR-positive, low- or intermediate-grade tumors at any cT; HR-positive, high-grade tumors with cT0–3; or any HER2-positive tumors. Group B (GrB) included HR-positive, high-grade tumors with cT4 disease or any triple-negative tumors. Results: The hazard of death (HoD) was 43% lower in GrA than in GrB. Median overall survival (OS) was 65 months (39-104) for GrA patients and 44 months (28-72) for GrB patients (HR 0.57, 95% CI 0.41-0.78, p = 0.0003). Primary tumor surgery (PTS) significantly improved OS in GrA patients, regardless of the number of metastases (solitary: HR, 0.375, 95% CI 0.259-0.543, p<0.001; multiple: HR 0.435, 95% CI 0.334-0.615, p <0.001). Conversely, GrB patients did not experience a significant benefit from PTS. Conclusions: This study demonstrates that GrA patients have better OS than GrB patients, and PTS reduces the HoD in GrA patients compared to systemic therapy alone. These findings support using a modified staging system in dnBOBMC to identify patients who may benefit multimodal therapy including PTS.
Keywords:
Stage IV breast cancer
; novel staging system
; multimodal therapy
; primary tumor surgery
; bone-only metastases
; locoregional treatment
; de novo metastatic breast cancer
Introduction
De novo metastatic breast cancer (dnMBC) is approximately 3–10% of new BCs, with bone being the most common metastatic site. With multimodal therapy, these patients often achieve relatively more prolonged survival, with some studies showing an excess of 10 years [1,2]. Despite longer overall survival (OS) in dnBOMBC, current guidelines do not indicate which subgroups benefit most from systemic therapy (ST) and loco-regional therapy, such as primary tumor surgery (PTS) and radiotherapy (RT). Traditional staging classifies all metastatic BCs as Stage IV, obscuring the substantial heterogeneity in prognosis for patients with different biological tumor subtypes and metastatic distributions. This highlights the need for a refined or “pragmatic” staging system for dnBOMBC.
In other malignancies like colon, lung, ovarian, and thyroid cancers, the American Joint Committee on Cancer (AJCC) has introduced metastatic subcategories to enhance prognostic accuracy [3,4,5,6]. Tamirisa et al. showed that reclassifying BC patients with supraclavicular metastases (cN3c) from Stage IV to IIIc improved survival, with multimodal therapy achieving a 5-year OS of 59%, compared to 28% in other groups [7]. Similarly, Plichta et al. compared the AJCC 7th and 8th editions and found that 36.6% of patients were restaged, with 29.7% down staged, including 94.1% of Stage IB and 82.5% of Stage IIIC cases. These findings highlight the potential impact of refined staging systems in improving outcomes for dnMBC patients [8].
A new staging system for dnMBC was recently proposed, along with an online calculator, using data from the National Cancer Database (NCDB) and Surveillance, Epidemiology, and End Results (SEER). This proposed staging integrates clinical and pathological variables, including T category, tumor grade, ER/PR/HER2 status, histology, metastatic sites (bone-only vs. others), and the number of affected organ systems. Patients were stratified into stages IV A–D based on 3-year OS rates (>70%, 50–70%, 25–50%, and <25%), with bone-only metastases identified as a favorable subgroup. While this model demonstrated the importance of stratifying dnMBC patients, the AJCC system still lacks classifications specific to dnMBC [9,10,11]. In this study we aim to introduce subgroups for dnBOMBC patients based on immunohistochemical and anatomical features and test the hypothesis that some may be appropriately classified as Stage IIID.
Materials and Methods
Data were collected from the previously published MF07-01 (phase III, prospective randomized trial) and MF14-01, BOMET (prospective multi-institutional registry study) cohorts [1,12]. The current study included only patients with bone metastases. Exclusion criteria were patients under 18 and those with a history of prior cancer or cancer metastases. Patients with missing clinical T or N stage, tumor grade, hormone receptor (HR) status, human epidermal growth factor receptor 2 (HER2) status, or metastatic disease site were excluded. All patients who underwent surgery had negative surgical margins.
Initial analyses were conducted across four main groups based on HR and HER2 status. The first group was subdivided into subgroups 1a, 1b, and 1c according to cT stage and grade (G) status (Table 1). HR positivity was defined as either estrogen or progesterone receptor positivity. HER2 status was classified as HER2(-) for HER2 “0” and “1”, and as HER2(+) for HER2 “2+” if the FISH test was positive. HER2 “3+” was directly classified as HER2(+).
The multimodal therapy in this study incorporated PTS, RT, and ST, providing a comprehensive approach to patient management. The OS of patients who had loco-regional therapy (LRT) was compared to those who received ST only.
Statistical Analysis
Student t-tests were used to compare continuous variables with normal distribution between the groups. Violations of normal distribution were tested using the Shapiro-Wilk test, and the Wilcoxon rank-sum test was used for variables without normal distribution. Chi-square tests were used to compare the distribution of categorical variables. Survival rates were estimated using Kaplan-Meier log-rank tests. Univariate Cox models were run to estimate hazard ratio (HR) and 95% confidence interval (CI) for survival rate estimates. P-values of less than 0.05 were considered statistically significant. Statistical analyses were conducted with R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria, https://www.r-project.org) software packages and IBM SPSS Statistics (IBM Corp., Armonk, NY, ABD), IBM SPSS Statistics for Windows, version 22.0.
Results
The study included 589 patients, average age 53 years (range: 19-90). No statistically significant survival difference was observed among patients in groups 1a, 1b, 2, and 3, with median OS of 64, 72, 63, and 68 months, respectively (p = 0.67), so they were classified as Group A. In contrast, the median OS for patients in Group 1c and Group 4 were 41 months (range: 14.7-67.3) and 48 months (range 32.1-63.9), with no significant difference (p = 0.34), forming Group B (Figure 1).
Of the 589 patients in the study, 530 (89%) were in Group A and 59 (10%) in Group B. The median follow-up was 55 months (range: 37-71.5). PTS was performed in 315 patients (53.48%), including 54.34% of patients in Group A and 45.76% in Group B.
The median OS was 65 months (range: 39–104) in Group A versus 44 months (range: 28–72) in Group B, with a 43% lower hazard of death (HoD) (HR 0.57, 95% CI 0.41–0.78, p = 0.0003). (Figure 2).
LRT significantly improved OS in Group A. Among patients with solitary bone metastases, median OS was 93 months (95% CI: 79.14–106.86) in the LRT group, vs. 53 months (95% CI: 41.44–64.56) in the ST-only group (HR 0.375, 95% CI: 0.259–0.543, p < 0.001). In Group A subgroup with multiple bone metastases, the median OS was 82 months (95% CI: 68.74–95.26) in LRT group vs. 49 months in ST-only group (HR 0.453, 95% CI: 0.334–0.615, p < 0.001) (Figure 3).
Conversely, Group B patients showed no OS benefit from LRT, regardless of bone metastase count (solitary metastasis p = 0.07; multiple metastasis p = 0.12) (Figure 4).
Discussion
dnMBC is defined as the presence of metastasis at initial BC diagnosis. The dnMBC rate among all MBC patients has risen from 20% to 30-40% [13]. The AJCC 8th edition classifies MBC as a single stage. Notably, nearly half of these patients present with oligometastatic disease, benefiting from a multimodal treatment, including ST, PTS, and RT. However, evidence is largely based on non-randomized studies. Careful selection of dnMBC patients is crucial to avoid overtreatment.
The term oligometastatic disease was first introduced in 1995, referring to patients with limited metastases and a better prognosis [14]. Although the definition remains debated, the most commonly accepted criterion is the presence of five or fewer metastatic lesions, regardless of the number of involved organs [15]. Oligometastatic disease is also characterized by the feasibility of definitive treatment for all metastatic sites [16]. Bone (41.1%) is the most frequent site, followed by lung (22.4%), liver (7.3%), and brain (7.3%) [17].
Bone metastases play a crucial role in prognosis and treatment. The phase III MF07-01 trial found that after 10 years, 19% (95% CI: 13–28%) of patients undergoing surgery were alive versus 5% (95% CI: 2–12%) receiving ST alone (p < 0.0003), with the most significant benefit in ER/PR+, HER2+, and solitary bone metastases [1]. In patients with solitary bone metastases, LRT showed a 14-month median survival benefit more than ST only, with an HR of 0.55 (95% CI 0.36-0.86, p = 0.009). LRT and ST combination decreased mortality by 29% at 10 years in HR-positive subgroups (HR 0.71, 95% CI 0.59-0.86, p = 0.0003). No survival benefit was seen in TN, visceral metastases or multiple bone metastases.
The BOMET MF14-01 study underscores the efficacy of multimodal treatment, showing 5-year OS of 33% for ST-only vs. 72% for LRT+ST (HR, 0.40; 95% CI: 0.30–0.54, p < 0.0001). In solitary metastases, the 5-year OS was 45% in the ST-only and 75% in the LRT (p = 0.0005), while oligometastatic patients demonstrated 42% and 72% in the ST-only and LRT groups, respectively (p = 0.002). In multi-metastatic disease, the 5-year OS rates were 31% in the ST-only group and 69% in the LRT (p < 0.0001). For patients with more than five metastases, the survival rates dropped to 14% and 49% in the ST-only and LRT groups, respectively (p = 0.005). Additionally, in HR-positive dnBOMBC, the HoD was reduced by 72% in the multimodal treatment group. However, no statistically significant difference in HoD was observed in TN patients receiving multimodal therapy compared to those treated with ST only (HR 0.51, 95% CI: 0.24–1.10) [12]. Similarly, our study demonstrated the survival benefits of LRT, particularly for Group A patients, who had a median OS of 65 months (range: 39–104) compared to 44 months (range: 28–72) in Group B (HR: 0.57; 95% CI: 0.41–0.78; p = 0.0003). Notably, among Group A patients with solitary bone metastases, the median OS in the LRT group was 93 months (95% CI: 79.14–106.86), compared to 53 months (95% CI: 41.44–64.56) in the ST-only group (HR: 0.375; 95% CI: 0.259–0.543; p < 0.001).
Several retrospective studies confirm multimodal treatment benefits, particularly in younger patients, ≤3 metastases, and HR+/HER2− or HER2+ tumors. Thomas et al., using SEER data from 21,372 patients, found that surgery improved median OS in BOM patients (19 vs. 28 months; p < 0.001) and enhanced 10-year survival (OR 3.61, 95% CI 2.89–4.50). Similar trends were found in studies by Lane (53 vs. 38 months; p < 0.001), Pons-Tostivint (62 vs. 46 months; p < 0.001), Lopez-Tarruella (40 vs. 22 months; p < 0.0001), Cady (35 vs. 24 months; p = 0.021), and Shien (27 vs. 22 months, p = 0.049), confirming the impact of LRT, especially in limited bone metastases. Xiong et al. reported marked OS benefits in patients with ≤3 metastases (78 vs. 37 months; p = 0.002), while Kwong and Co observed improved 5-year OS rates with surgery after ST (43.9% vs. 33.9%; p = 0.0026) [18,19,20,21,22,23,24,25]. In our study, Group A patients benefited significantly from LRT regardless of the number of metastases. For solitary metastatic patients, the HR was 0.37 (95% CI 0.25-0.54; p < 0.001), while for patients with multiple metastases, the HR was 0.45 (95% CI 0.33-0.61; p < 0.001).
Conversely, the TATA and ECOG-ACRIN 2108 trials found no OS benefit from LRT. TATA trial reported improved locoregional progression-free survival (LPFS) but worse distant progression-free survival (PFS), while ECOG-ACRIN found no significant OS or PFS improvement. However, both had patient selection limitations [26,27]. A prospective trial by Abo-Touk showed higher 2-year OS (LRT 46% vs. ST-only 22%) but was not statistically significant (HR 0.346, 95% CI 0.031–3.817; p = 0.085). Although not statistically significant, they suggest LRT may be beneficial for patients based on bone metastases, the extent and location of metastases, and clinical T and N stages [28]. A Japanese trial at ASCO 2023 found LRT + ST improved LPFS (63 vs. 20 months, p < 0.0001), particularly in ER+, premenopausal, single-organ metastases, especially BOM [29]. Similarly, our study found that ER positivity, BOM, and single-organ metastases were common variables that positively affect survival, although disease-free survival data were unavailable.
In contrast, our study demonstrated clear survival advantages with LRT, particularly for Group A patients with solitary metastases, where the median OS was 93 months (95% CI: 79.14–106.86) compared to 53 months (95% CI: 41.44–64.56) in the ST-only group (HR 0.375, 95% CI: 0.259–0.543, p < 0.001).
Meta-analyses also confirm LRT’s impact. Chongxi Ren et al. found no OS benefit (HR 0.87; 95% CI 0.68–1.11; p = 0.265) but notable LPFS improvement (HR 0.27, 95% CI 0.19–0.38, p < 0.001) [30]. Similarly, another meta-analysis found an improvement in LPFS, particularly in patients with BOM (HR 0.18; p = 0.017) [31]. Weikai Xiao et al. showed better distant PFS (HR 0.42, p < 0.001), particularly in solitary metastases, bone-only disease, and negative surgical margins [32].
Our study corroborates the survival advantages of LRT, especially in selected BOM patients, particularly Group A patients as the most likely to benefit from LRT and provides a pragmatic framework for refining patient selection and optimizing treatment outcomes.
Targeted therapies further improve dnMBC survival. The CLEOPATRA trial demonstrated pertuzumab + trastuzumab + docetaxel extended OS (HR 0.60, CI 0.50–0.72), while PALOMA-2 (27.9 vs. 22 months; HR 0.61) and MONALEESA-3 trial (59.9 vs. 50.9 months; HR 0.62) confirmed CDK 4/6 inhibitors’ efficacy. KEYNOTE-355 trial demonstrated pembrolizumab improved PFS in metastatic TNBC (7.6 vs. 5.6 months; HR 0.74, p = 0.0014) [33,34,35,36]. While our study did not include immunotherapy or CDK 4/6 inhibitors, our results align with findings in low tumor burden and HR+ patients benefiting from multimodality treatment.
There is an unmet need for research to evaluate the integration of new therapy regimens for enhanced survival for specific patient subgroups.
Patients with dnMBC are a diverse group in terms of prognosis and necessitating personalized treatment approaches. The AJCC 8th edition Staging System incorporates immunohistochemical characteristics and anatomical factors for BC staging but does not provide specific adjustments for dnMBC. Patients with lower tumor burden, limited metastases, and HR-positive status experience more prolonged survival [37,38,39]. New staging systems are crucial in more accurately assessing the prognosis of dnMBC patients, allowing for more effective planning of ST and LRT. In response, several studies have proposed novel staging systems and nomograms to predict outcomes in dnMBC patients better. Lin et al. identified M1a (solitary bone metastases or a single non-liver/brain site) as experiencing the most significant benefit from LRT (HR 0.57; 95% CI 0.48-0.67) [40]. Wang et al. proposed a nomogram showing significantly longer OS in surgery vs. non-surgery groups (53 vs. 33 months; HR 0.64; p < 0.001), factors affecting the benefit of LRT included histological grade, T stage, molecular subtype, the location of metastases, with BOM identified as a strong positive factor [9]. Yoo et al. used a survival prediction model, where surgery showed significantly better median OS (53 vs. 31 months; p < 0.001), identifying younger, HR-positive, with smaller tumors, low metastatic burden, and BOM patients as ideal candidates for LRT, including PTS, RT, and metastatic resection [41]. Kommalapati et al.’s prognostic model demonstrated BOM, ER positivity, and low tumor grade associated with better OS, while high tumor burden and aggressive histology were negative factors [42]. Our study aligns with these findings, showing LRT significantly improved OS in BOM patients, particularly solitary metastasis (93 vs. 53 months; p < 0.001) and multiple bone metastases (82 vs. 49 months; p < 0.001).
Plichta et al. (2023) proposed a novel staging system for dnMBC based on metastatic site, ER and HER2 status, clinical T stage, and tumor grade. The categorized metastatic stage IV for these stages was 73.2% for IVA, 61.9% for IVB, 40.1% for IVC, and 17% for IVD (p < 0.001). In the paper, the authors proposed a new staging system using a web-based calculator that can be used to restage such patients. This nomogram is for all dnMBC patients using data pulled from SEER and NCDB datasets. In their paper, S1-4 was defined as the number of organ systems involved, such that a patient with BOM would be assigned “S2” regardless of the number of bone metastases and liver metastases. Patients who have one organ metastasis and ER(+)/PR(+)/T0-3/HER2(-) and grade 1-2/ ductal histology/ BOM are staged as Stage IVB, and median 3-year OS was 58.4% and 64.2% in validation one and validation two cohort samples, respectively [43]. In our proposed model of dnBOMBC data, this patient would fit into Group 1a. For solitary bone metastasis, the median OS was 93 months in the LRT group compared to 53 months in the ST-only group (p < 0.001), with a median follow-up of 55 months. The same patient characteristics with multiple bone metastases, the median OS was 82 months in the LRT group, 33 months longer than in the ST-only group (p < 0.001) in our proposed model. While restaging dnMBC, we think it’d be more accurate to separate bone metastasis from non-bone metastasis.
While existing models focus on histology and molecular subtypes, future refinements should incorporate additional factors such as genomics and circulating tumor cell/DNA burden [44,45]. Our analysis of the MF07-01 and MF14-01 BOMET studies indicated that isolated bone metastasis is a key prognostic factor, and thus, we focused our study on this patient group. Meta-analyses and prospective studies consistently identify HR status, HER2 status, tumor grade, and cT stage as prognostic factors [46]. We utilized a pragmatic algorithm similar to that proposed by Plichta et al. to define subgroups based on these prognostic factors. Our findings revealed that higher tumor grade and cT stage were associated with poorer outcomes in HR-positive patients, while TN was a significantly poor prognostic factor. Notably, LRT in Group B did not provide a survival benefit.
In our study, Group A OS was comparable to Stage IIIC, with a median OS of 62 months. Qiu et al. reported a median OS of approximately 54 months, while Ai et al. noted 76 months, with variations depending on molecular subtypes and clinical characteristics in Stage IIIC. İn our study at 5 years, the median OS for Group B was 44 months, while for Group A, this could not be determined due to a substantial proportion of patients still alive (95% CI: 32.4–55.6 months; p = 0.001). Ai et al. showed a 5-year OS of 61.7%, while Qiu et al. reported 51.72%, with variations observed across N3 subgroups in Stage III. In our study at 10 years, OS declined to 18% overall, with 19% for Group A and 12% for Group B, and median OS was 65 months for Group A (95% CI: 59.5–70.5 months) and 44 months for Group B (95% CI: 32.4–55.6 months; p = 0.0003). Although a limited 10-year OS data for Stage IIIC are available in the literature, indicating poor outcomes, particularly for N3c disease, our study shows similar OS comparing Stage IIIC [47,48].
This study has certain limitations. First limitation was combining two trials: MF07-01 was a phase III prospective randomized trial, and MF14-01 was a BOMET (prospective multi-institutional registry study) cohort. Although all patients in the MF14-01 BOMET study had bone-only metastasis at the time of BC diagnosis, only 46% of patients in the MF07-01 study had bone-only metastasis when the staging analysis was performed. The second limitation was that both studies did not require a metastatic site biopsy, but two different imaging modalities were used to confirm the bone metastases. A further limitation was that metastatic site intervention was left to the institution’s choice.
Over time, ST has evolved, and various modalities have been applied in different studies, including ours, which may influence outcomes. Additionally, the limited survival rates of metastatic patients often result in relatively short follow-up periods in many studies. To more accurately identify the patient groups that will derive the greatest benefit, it is essential to conduct studies with longer follow-up durations. Therefore, increasing the number of studies with extended follow-up is crucial for refining treatment strategies and improving patient outcomes.
Conclusions
LRT is a standard part of multimodal therapy for Stage III BC, but its role in Stage IV BC remains controversial. When a subgroup of dnBOMBC patients demonstrates OS similar to Stage III BC and receives multimodal therapy, they might be reclassified as Stage III D and prioritized for LRT. Our study presents a practical grouping model that distinguishes patients most likely to benefit from LRT, providing a more applicable framework than current nomograms. Further large-scale studies are essential to validate these findings and refine the proposed staging system, providing clear guidance for integrating LRT into dnBOMBC treatment.
Acknowledgments
We would like to express our gratitude to each multidisciplinary member of the Breast Health Working Group International (BHWGI), who work under the motto “Everyone plays a vital role in defeating BREAST cancer,” for their valuable contributions.
References
- Soran, A.; Ozmen, V.; Ozbas, S.; et al. Primary Surgery with Systemic Therapy in Patients with de Novo Stage IV Breast Cancer: 10-year Follow-up; Protocol MF07-01 Randomized Clinical Trial. J Am Coll Surg 2021, 233, 742–751.e5. [Google Scholar] [CrossRef] [PubMed]
- Iwase, T.; Shrimanker, T.V.; Rodriguez-Bautista, R.; et al. Changes in Overall Survival over Time for Patients with de novo Metastatic Breast Cancer. Cancers 2021, 13, 2650. [Google Scholar] [CrossRef]
- Weiser, M.R. AJCC 8th Edition: Colorectal Cancer. Ann Surg Oncol 2018, 25, 1454–1455. [Google Scholar] [CrossRef] [PubMed]
- Lababede, O.; Meziane, M.A. The Eighth Edition of TNM Staging of Lung Cancer: Reference Chart and Diagrams. Oncologis 2018, 23, 844–848. [Google Scholar] [CrossRef]
- Berek, J.S.; Renz, M.; Kehoe, S.; Kumar, L.; Friedlander, M. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update. Int J Gynaecol Obstet 2021, 155 (Suppl. 1), 61–85. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Grani, G.; Arvat, E.; et al. 8th edition of the AJCC/TNM staging system of thyroid cancer: what to expect (ITCO#2). Endocr Relat Cancer 2018, 25, L7–L11. [Google Scholar] [CrossRef]
- Tamirisa, N.P.; Ren, Y.; Campbell, B.M.; et al. Treatment Patterns and Outcomes of Women with Breast Cancer and Supraclavicular Nodal Metastases. Ann Surg Oncol 2021, 28, 2146–2154. [Google Scholar] [CrossRef]
- Plichta, J.K.; Ren, Y.; Thomas, S.M.; et al. Implications for Breast Cancer Restaging Based on the 8th Edition AJCC Staging Manual. Ann Surg 2020, 271, 169–176. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, B.; Chen, J.; et al. A Novel Nomogram Model to Identify Candidates and Predict the Possibility of Benefit From Primary Tumor Resection Among Female Patients With Metastatic Infiltrating Duct Carcinoma of the Breast: A Large Cohort Study. Front Oncol 2022, 12, 798016. [Google Scholar] [CrossRef]
- Kommalapati, A.; Tella, S.H.; Goyal, G.; Ganti, A.K.; Krishnamurthy, J.; Tandra, P.K. A prognostic scoring model for survival after locoregional therapy in de novo stage IV breast cancer. Breast Cancer Res Treat 2018, 170, 677–685. [Google Scholar] [CrossRef]
- Plichta, J.K.; Thomas, S.M.; Sergesketter, A.R.; et al. A Novel Staging System for De Novo Metastatic Breast Cancer Refines Prognostic Estimates. Ann Surg 2022, 275, 784–792. [Google Scholar] [CrossRef]
- Soran, A.; Dogan, L.; Isik, A.; et al. The Effect of Primary Surgery in Patients with De Novo Stage IV Breast Cancer with Bone Metastasis Only (Protocol BOMET MF 14-01): A Multi-Center, Prospective Registry Study. Ann Surg Oncol 2021, 28, 5048–5057. [Google Scholar] [CrossRef]
- Daily, K.; Douglas, E.; Romitti, P.A.; Thomas, A. Epidemiology of De Novo Metastatic Breast Cancer. Clin Breast Cancer 2021, 21, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Weichselbaum, R.R.; Hellman, S. Oligometastases revisited. Nat Rev Clin Oncol 2011, 8, 378–382. [Google Scholar] [CrossRef]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Lievens, Y.; Guckenberger, M.; Gomez, D.; et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother Oncol 2020, 148, 157–166. [Google Scholar] [CrossRef]
- Berman, A.T.; Thukral, A.D.; Hwang, W.T.; Solin, L.J.; Vapiwala, N. Incidence and patterns of distant metastases for patients with early-stage breast cancer after breast conservation treatment. Clin Breast Cancer 2013, 13, 88–94. [Google Scholar] [CrossRef]
- Thomas, A.; Khan, S.A.; Chrischilles, E.A.; Schroeder, M.C. Initial Surgery and Survival in Stage IV Breast Cancer in the United States, 1988-2011. JAMA Surg 2016, 151, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Lane, W.O.; Thomas, S.M.; Blitzblau, R.C.; et al. Surgical Resection of the Primary Tumor in Women With De Novo Stage IV Breast Cancer: Contemporary Practice Patterns and Survival Analysis. Ann Surg 2019, 269, 537–544. [Google Scholar] [CrossRef]
- Pons-Tostivint, E.; Kirova, Y.; Lusque, A.; et al. Survival Impact of Locoregional Treatment of the Primary Tumor in De Novo Metastatic Breast Cancers in a Large Multicentric Cohort Study: A Propensity Score-Matched Analysis. Ann Surg Oncol 2019, 26, 356–365. [Google Scholar] [CrossRef]
- Lopez-Tarruella, S.; Escudero, M.J.; Pollan, M.; et al. Survival impact of primary tumor resection in de novo metastatic breast cancer patients (GEICAM/El Alamo Registry). Sci Rep 2019, 9, 20081. [Google Scholar] [CrossRef]
- Cady, B.; Nathan, N.R.; Michaelson, J.S.; Golshan, M.; Smith, B.L. Matched pair analyses of stage IV breast cancer with or without resection of primary breast site. Ann Surg Oncol 2008, 15, 3384–3395. [Google Scholar] [CrossRef] [PubMed]
- Shien, T.; Kinoshita, T.; Shimizu, C.; et al. Primary tumor resection improves the survival of younger patients with metastatic breast cancer. Oncol Rep 2009, 21, 827–832. [Google Scholar] [CrossRef]
- Xiong, Z.; Deng, G.; Wang, J.; et al. Could local surgery improve survival in de novo stage IV breast cancer? BMC Cancer 2018, 18, 885. [Google Scholar] [CrossRef] [PubMed]
- Co, T.H.M.; Ng, J.; Kwong, A. Long term survival study of de-novo metastatic breast cancers with or without primary tumour resection. Cancer Treat Res Commun 2019, 20, 100148. [Google Scholar] [CrossRef]
- Abo-Touk, N.A.; Fikry, A.; Fouda, E.Y. The benefit of locoregional surgical intervention in metastatic breast cancer at initial presentation. Cancer Research Journal 2016, 4, 32–36. [Google Scholar] [CrossRef]
- Badwe, R.; Hawaldar, R.; Nair, N.; et al. Locoregional treatment versus no treatment of the primary tumour in metastatic breast cancer: an open-label randomised controlled trial. Lancet Oncol 2015, 16, 1380–1388. [Google Scholar] [CrossRef]
- Khan, S.A.; Zhao, F.; Goldstein, L.J.; et al. Early Local Therapy for the Primary Site in De Novo Stage IV Breast Cancer: Results of a Randomized Clinical Trial (EA2108). J Clin Onco 2022, 40, 978–987, [published correction appears in J Clin Oncol 2022, 40, 1392. https://doi.org/10.1200/JCO.22.00666]. [Google Scholar] [CrossRef]
- Shien, T.; Nakamura, K.; Shibata, T.; et al. A randomized controlled trial comparing primary tumour resection plus systemic therapy with systemic therapy alone in metastatic breast cancer (PRIM-BC): Japan Clinical Oncology Group Study JCOG1017. Jpn J Clin Oncol 2012, 42, 970–973. [Google Scholar] [CrossRef]
- Ren, C.; Sun, J.; Kong, L.; Wang, H. Breast surgery for patients with de novo metastatic breast cancer: A meta-analysis of randomized controlled trials. Eur J Surg Oncol 2024, 50, 107308. [Google Scholar] [CrossRef]
- Yu, Y.; Hong, H.; Wang, Y.; et al. Clinical Evidence for Locoregional Surgery of the Primary Tumor in Patients with De Novo Stage IV Breast Cancer. Ann Surg Oncol 2021, 28, 5059–5070. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Zou, Y.; Zheng, S.; et al. Primary tumor resection in stage IV breast cancer: A systematic review and meta-analysis. Eur J Surg Oncol 2018, 44, 1504–1512. [Google Scholar] [CrossRef]
- Swain, S.M.; Miles, D.; Kim, S.B.; et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol 2020, 21, 519–530. [Google Scholar] [CrossRef]
- Slamon, D.J.; Diéras, V.; Rugo, H.S.; et al. Overall Survival With Palbociclib Plus Letrozole in Advanced Breast Cancer. J Clin Oncol 2024, 42, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.J.; Neven, P.; Chia, S.; et al. Ribociclib plus fulvestrant for postmenopausal women with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in the phase III randomized MONALEESA-3 trial: updated overall survival. Ann Oncol 2021, 32, 1015–1024, [published correction appears in Ann Oncol 2021, 32, 1307. https://doi.org/10.1016/j.annonc.2021.07.011]. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef]
- Leone, B.A.; Vallejo, C.T.; Romero, A.O.; et al. Prognostic impact of metastatic pattern in stage IV breast cancer at initial diagnosis. Breast Cancer Res Treat 2017, 161, 537–548. [Google Scholar] [CrossRef]
- Press, D.J.; Miller, M.E.; Liederbach, E.; Yao, K.; Huo, D. De novo metastasis in breast cancer: occurrence and overall survival stratified by molecular subtype. Clin Exp Metastasis 2017, 34, 457–465. [Google Scholar] [CrossRef]
- Lobbezoo, D.J.; van Kampen, R.J.; Voogd, A.C.; et al. Prognosis of metastatic breast cancer subtypes: the hormone receptor/HER2-positive subtype is associated with the most favorable outcome. Breast Cancer Res Treat 2013, 141, 507–514. [Google Scholar] [CrossRef]
- Lin, C.; Wu, J.; Ding, S.; et al. Subdivision of M1 Stage for De Novo Metastatic Breast Cancer to Better Predict Prognosis and Response to Primary Tumor Surgery. J Natl Compr Canc Netw 2019, 17, 1521–1528. [Google Scholar] [CrossRef]
- Yoo, T.K.; Chae, B.J.; Kim, S.J.; et al. Identifying long-term survivors among metastatic breast cancer patients undergoing primary tumor surgery. Breast Cancer Res Treat 2017, 165, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Kommalapati, A.; Tella, S.H.; Goyal, G.; Ganti, A.K.; Krishnamurthy, J.; Tandra, P.K. A prognostic scoring model for survival after locoregional therapy in de novo stage IV breast cancer. Breast Cancer Res Treat 2018, 170, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Plichta, J.K.; Thomas, S.M.; Hayes, D.F.; et al. Novel Prognostic Staging System for Patients With De Novo Metastatic Breast Cancer. J Clin Oncol 2023, 41, 2546–2560. [Google Scholar] [CrossRef]
- Cheng, J.; Holland-Letz, T.; Wallwiener, M.; et al. Circulating free DNA integrity and concentration as independent prognostic markers in metastatic breast cancer. Breast Cancer Res Treat 2018, 169, 69–82. [Google Scholar] [CrossRef]
- Pairawan, S.; Hess, K.R.; Janku, F.; et al. Cell-free Circulating Tumor DNA Variant Allele Frequency Associates with Survival in Metastatic Cancer. Clin Cancer Res 2020, 26, 1924–1931. [Google Scholar] [CrossRef]
- Li, X.; Zhang, X.; Liu, J.; Shen, Y. Prognostic factors and survival according to tumour subtype in women presenting with breast cancer bone metastases at initial diagnosis: a SEER-based study. BMC Cancer 2020, 20, 1102. [Google Scholar] [CrossRef] [PubMed]
- Ai, X.; Liao, X.; Li, J.; Tang, P.; Jiang, J. Clinical Outcomes of N3 Breast Cancer: A Real-World Study of a Single Institution and the US Surveillance, Epidemiology, and End Results (SEER) Database. Cancer Manag Res 2020, 12, 5331–5343. [Google Scholar] [CrossRef]
- Qiu, Y.; Chen, H.; Dai, Y.; Bao, B.; Tian, L.; Chen, Y. Nontherapeutic Risk Factors of Different Grouped Stage IIIC Breast Cancer Patients’ Mortality: A Study of the US Surveillance, Epidemiology, and End Results Database. Breast J 2022, 2022, 6705052. [Google Scholar] [CrossRef]
Figure 1.
Classification according to the characteristics of the cases.
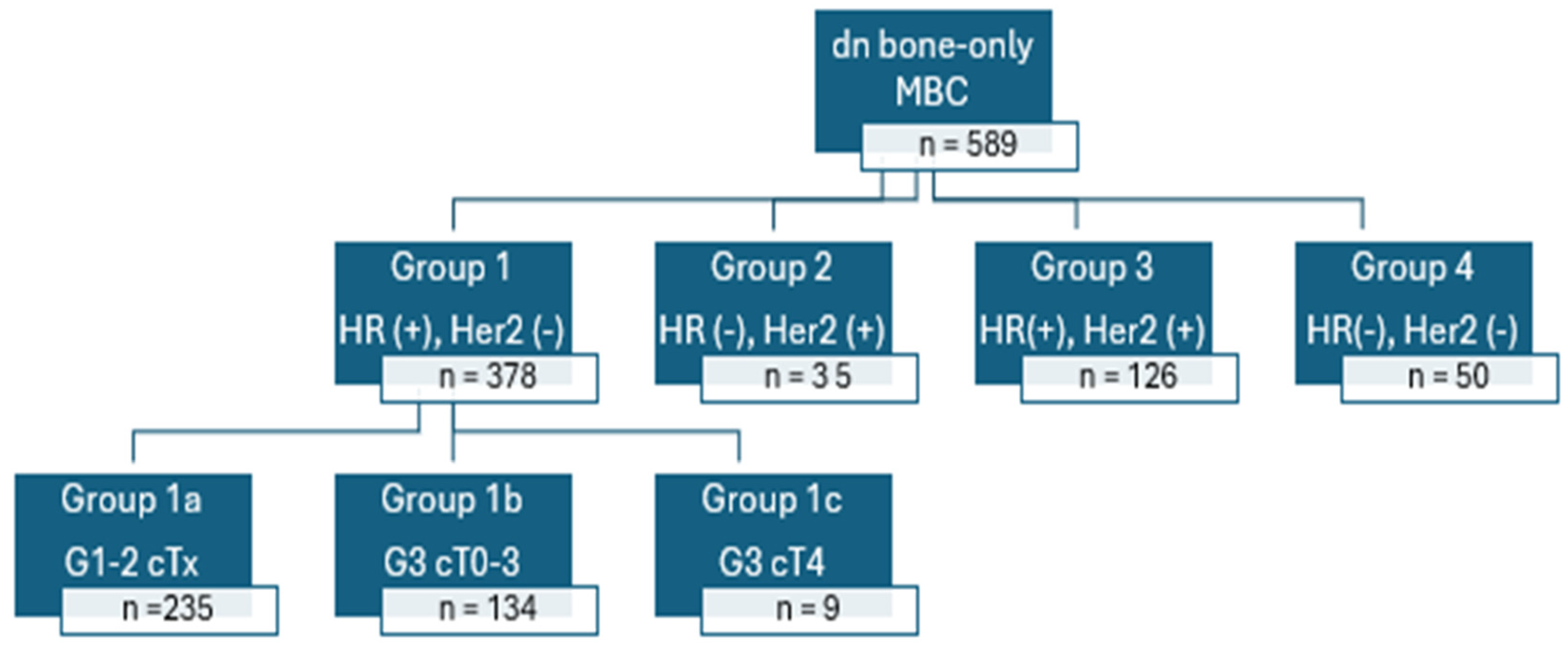
Figure 2.
Overall Survival group A vs group B.
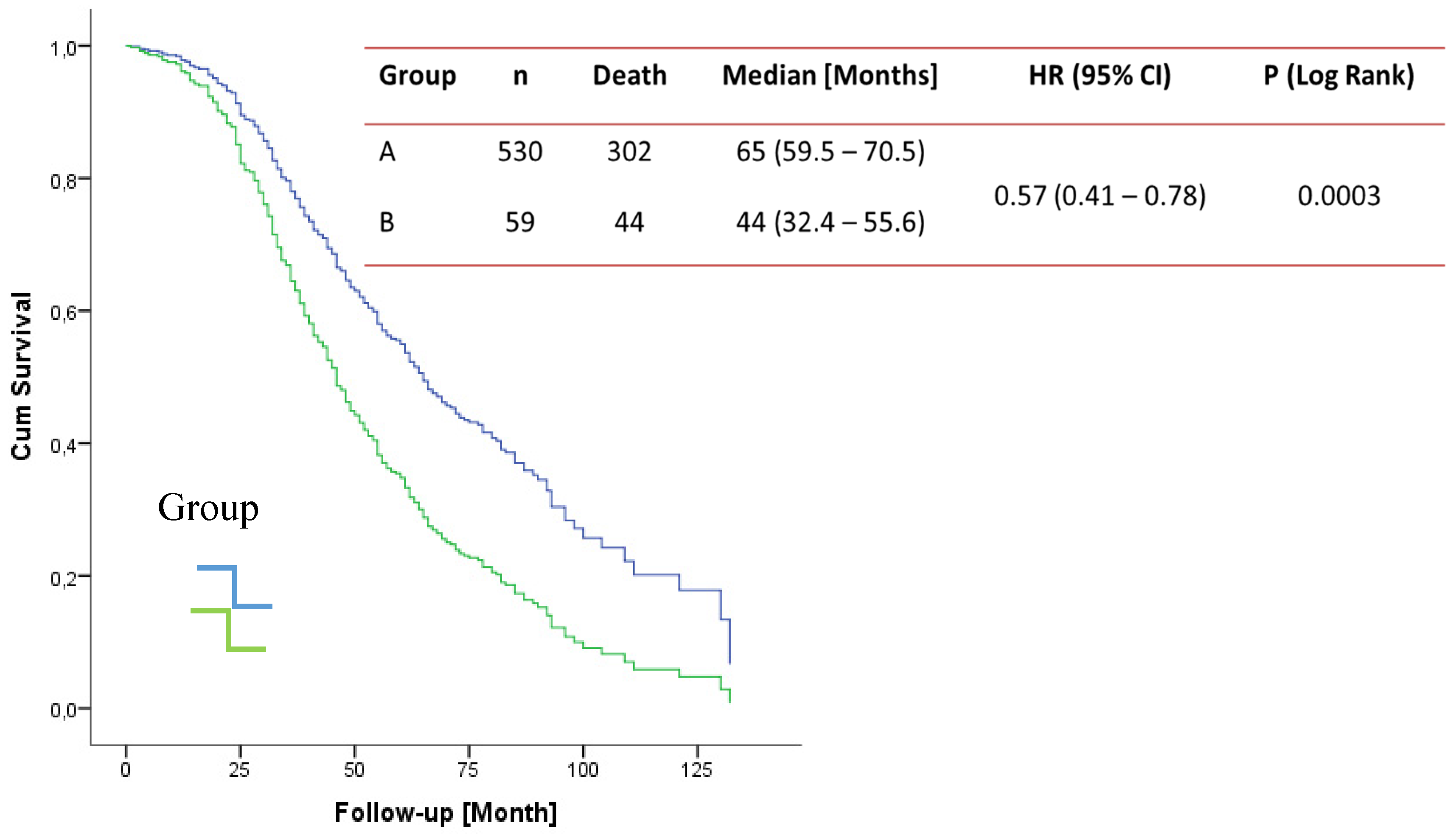
Figure 3.
Group A overall survival PTS vs ST a. solitary metastases b. multiple metastases. PTS: primary tumor surgery, ST: Sytemic therapy.
Figure 3.
Group A overall survival PTS vs ST a. solitary metastases b. multiple metastases. PTS: primary tumor surgery, ST: Sytemic therapy.
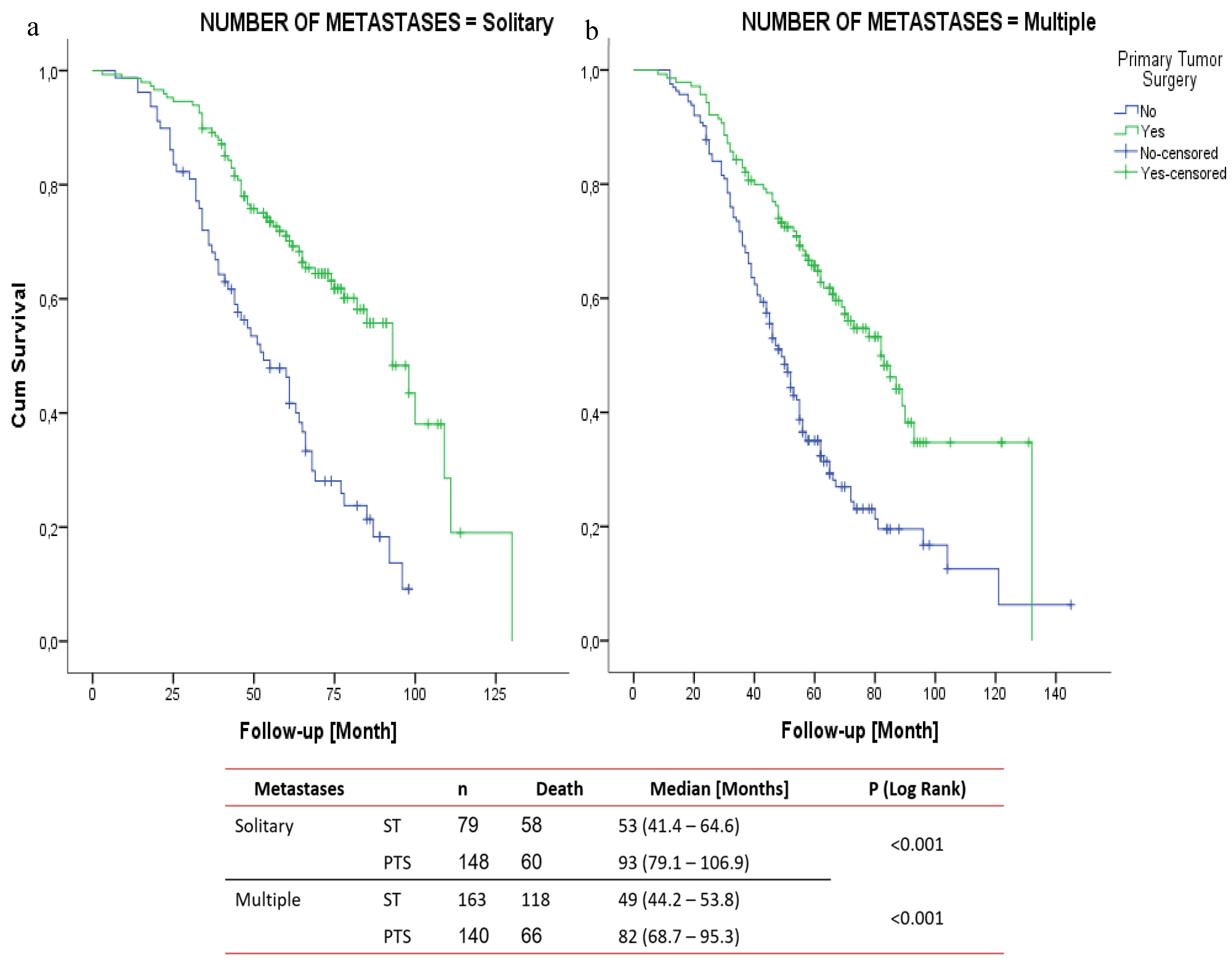
Figure 4.
Group B overall survival PTS vs ST. a. solitary metastases b. multiple metastases. PTS: primary tumor surgery, ST: Sytemic therapy.
Figure 4.
Group B overall survival PTS vs ST. a. solitary metastases b. multiple metastases. PTS: primary tumor surgery, ST: Sytemic therapy.
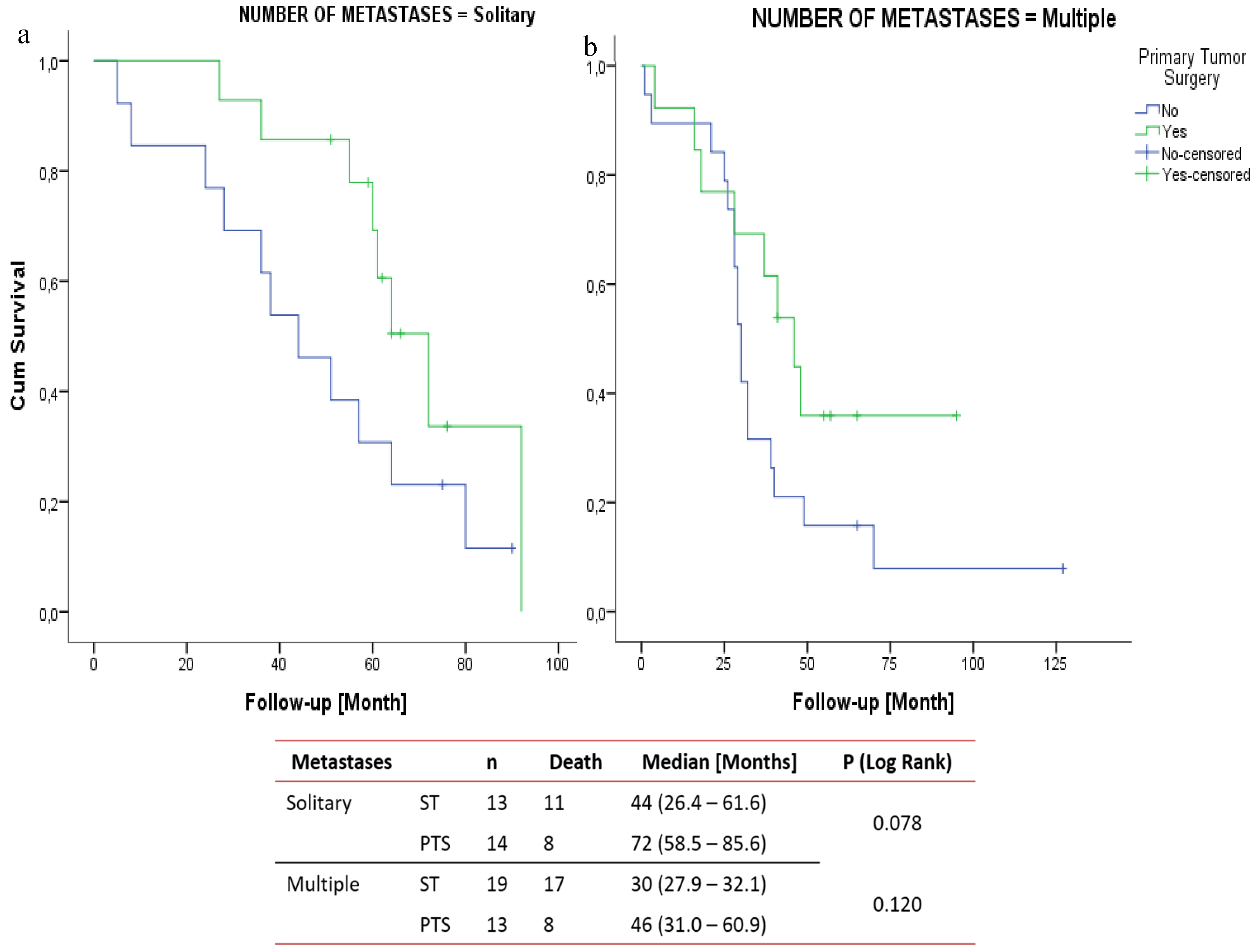

Table 1.
Grouping the patient based on HR and HER2 status, grade of the tumor and tumor size.
| Group 1: HR(+); HER2(-) |
| Group 1a: HR(+); HER2(-); Grade 1-2; cTany |
| Group 1b: HR(+); HER2(-); Grade 3; cT0-3 |
| Group 1c: HR(+); HER2(-); Grade 3; cT4 |
| Group 2: HR(-); HER2(+) |
| Group 3: HR(+); HER2(+) |
| Group 4: HR(-); HER2(-) |
| Group 1a, b and Group 2 and 3 were classified as Group A and group 1c and group 4 classified as Group B. HR: Hormone receptor, Her 2: Human epidermal growth factor receptor 2, T: tumor size |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



