
Submitted:
26 August 2025
Posted:
28 August 2025
You are already at the latest version
Abstract
Introduction: The impact of loco-regional treatment (LRT) on survival in de novo bone-only metastatic breast cancer (dnBOMBC) is controversial. The aim of this study is to assess the effect of LRT on survival utilizing international, prospectively acquired data in this cohort of patients. Materials and Methods: Patients with dnBOMBC were divided into two groups: those receiving systemic therapy only (ST) and those undergoing LRT. Further, patients who received LRT were divided into two subgroups: those who received ST after LRT (LRT+ST group) and those who received ST prior to LRT (ST+LRT group). Factors associated with disease progression including solitary or multiple bone metastases were analyzed. Results: There was a total of 744 patients with dnBOMBC treated at each of the participating institutions between 2014 and 2022, with 372 (50%) participants in each arm. Median follow-up was 48 months (32-66, 25-75%). Patients in the LRT group were significantly younger than the ST group [50 (42, 60) vs. 55 (44, 66), p=0.0001]. There were no significant differences in grade, HER2 status, triple-negative status, receipt of hormonal therapy, or intervention to metastatic sites. During follow-up, 58% (n=217) of patients in ST group and 32% (n=120) of patients in LRT group died (p<0.001). Local progression was observed in 20% of the patients in the ST group, whereas 9% progressed in the LRT group (p=0.0001). Systemic progression occurred more in the ST group; 66% (n=244) compared to 41% (n=152) of patients in the LRT group (p<0.001). The Hazard of death was 64% lower in LRT group than in ST group (HR: 0.36, 95% CI: 0.29-0.45, p<0.0001). The burden of metastatic disease differed significantly between the two groups with a higher rate of solitary bone metastases in the LRT group compared to the ST group (50% vs. 24%, p<0.001). However, the LRT group had better overall survival (OS) for both solitary (HR: 0.38, 95% Cl: 0.26-0.55) and multiple (HR: 0.38, 95% Cl: 0.29-0.51) bone metastases patients. Within the LRT group, survival rates were similar whether the breast surgery was performed before or after ST. Multivariate Cox analysis showed that LRT and ER/PR positivity significantly decrease the hazard of death (p<0.05). Conclusion: Analysis of this large multi-institutional patient cohort provides further evidence that LRT improves OS and lowers loco-regional recurrence in patients with dnBOMBC. In breast cancer patients with bone-only metastases at presentation, the decision for LRT should be made through a multidisciplinary approach with consideration of surgical therapy at the primary tumor.
Keywords:
metastatic breast cancer
; bone
; primary tumor surgery
1. Introduction
Breast cancer (BC) is the most common cancer diagnosed among women and the second leading cancer-related mortality reason worldwide [1]. Approximately 6–10% of newly diagnosed BCs in the United States are categorized as de novo metastatic breast cancer (dnMBC), characterized by the presence of distant metastases at initial diagnosis [2]. The median survival time of patients with metastatic BC was 2 to 3 years, but this has significantly improved in selected group of patients, up to 13 % of dnMBC patients can survive beyond 10 years [3,4]. With the advent of targeted therapies, cyclin-dependent kinase (CDK) 4/6 inhibitors, human epidermal growth factor receptor 2 (HER2)-directed agents, and multidisciplinary management, survival outcomes have nearly doubled, particularly in patients with bone-only metastases, hormone receptor (HR)-positive, and/or HER2-positive tumors.
Systemic therapies (ST) remain the mainstay of dnMBC treatment, especially in controlling disease progression and prolonging survival. However, in patients with favorable biology and indolent disease the prolonged ST treatment duration can result in cumulative toxicity, resistance, locoregional progression (LP) which reduce the quality of life [5]. The role of locoregional treatment (LRT), which includes surgical resection and/or radiotherapy (RT) directed at the primary breast tumor has gained increasing importance as a potential strategy to improve outcomes in select dnMBC patients [6]. International current practice guidelines have different recommendations. The National Comprehensive Cancer Network (NCCN) states that LRT in stage IV disease may be considered only after a favorable response to ST, highlighting that the survival benefit of upfront surgery remains unclear [7]. Meanwhile, the European Society for Medical Oncology (ESMO) suggests that the true value of LRT is still unknown but supports its selective use in carefully chosen patients, particularly those with limited disease burden and good performance status [8].
LRT improves local disease control and reduces the progression of the breast tumor. However, its impact on overall survival (OS) remains controversial. Multiple retrospective studies have provided mixed results; while some show no significant benefit, others reported improved survival in patients undergoing LRT, especially those with bone-only disease and low metastatic burden [9,10]. Meta-analyses suggest that certain subgroups, such as HR-positive and bone-only metastases, may have a survival benefit [11]. While randomized controlled trials (RCTs) are controversial on OS benefit from LRT, regardless of surgical timing, negative studies criticized often due to limitations such as small sample sizes, treatment imbalances, low rates of HER2-targeted therapy, and selection bias [12,13,14]. However, it is important to note that LRT is associated with better locoregional control and longer progression-free survival compared to ST alone in these RCTs.
Bone is the most frequent site of distant metastasis in BC, with up to 75% of distant metastasis being bone metastasis and among patients presenting with dnMBC, approximately 30–40% have bone-only metastases at diagnosis [15]. This subgroup often demonstrates a more indolent clinical course and favorable prognosis particularly when associated with HR-positive or HER2-positive disease. Given the relatively better prognosis and unique disease dynamics of de novo bone only metastatic breast cancer (dnBOMBC), this population presents a compelling opportunity to explore treatment strategies beyond ST alone. In our previous prospective, multicenter BOMET study (MF14-01), we demonstrated that LRT was associated with improved OS and reduced LP compared to ST alone [2]. To further explore this, we present the BOMETIN (MF14-1a) study, a larger, prospective, international and multi-institutional registry study. By analyzing real-world data, this study aims to clarify whether LRT confers a survival benefit in this uniquely prognostic and clinically relevant patient population.
2. Materials and Methods
Analyses were conducted considering two groups: those receiving ST only (ST group) and those receiving LRT (LRT group), even though the treating physicians determined on the treatment sequence. The patients who received LRT were subsequently divided into two groups: ST before LRT (ST+LRT group) and ST after LRT (LRT+ST group).
The diagnosis was made utilizing bone scintigraphy, magnetic resonance imaging (MRI), and Positron Emission Tomography–Computerized Tomography (PET/CT). Although it was not required, bone metastases were preferable confirmed by bone biopsy. If bone biopsy was not performed, at least two imaging modalities were required for single bone metastases. Bone biopsies to confirm the metastases were performed on only 15% of the patients (115/744). The absence of any metastases other than bone metastases was confirmed by PET/CT, computed tomography (CT), MRI, ultrasonography, or chest X-rays. While the treating physicians retained discretion over all treatment options and choices for primary tumors and metastases, patients with HER2-positive tumors received anti-HER2 therapy, and patients with HR-positive tumors received endocrine therapy. Until they died or the statistical analysis completed, patients were monitored every three to six months. OS, LP, and systemic progression (SP) were recorded and analyzed.
Statistical Analysis
LRT and ST groups were analyzed using t-tests, Chi-square tests Shapiro-Wilk test, and the Kruskal-Walli’s test were appropriate. Kaplan-Meier log-rank tests used for survival analyses. Univariate and multivariate Cox models with baseline, clinical, tumor, and metastasis characteristics were run to estimate hazard ratio (HR) and 95% confidence interval (CI) for survival. The proportional hazards assumption was tested to analyze OS and survival of each group. For all comparisons and analyses, the proportional hazards assumption was met (P > 0.20). To account for the effect of confounding covariates on survival, in addition to multivariable Cox models, ST and LRT groups were matched based on significantly different clinicopathological factors including age, tumor size, number of metastases, treatment type, LP and SP using a propensity score matching method. Full matching gave the best matching and adequate balance (Figure 1). The propensity score was estimated using probit regression of the treatment on the covariates. Full matching (Hansen 2004; Stuart and Green 2008) used all treated and all control units, so no units were discarded by the matching. Kaplan–Meier survival curves in ST and LRT groups were estimated in the matched sample. Stratified log-rank tests (stratifying on matched sets) were used to compare survival curves (Austin 2014). Cox regression models weighted by the matching weights and including subclasses as a cluster (Austin and Stuart 2015) were run to estimate marginal HR and 95% CI. P-values of less than 0.05 were considered statistically significant. Statistical analyses were conducted with R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria, https://www.r-project.org) software packages. ‘MatchIt’ package (https://cran.rproject.org/web/packages/MatchIt/MatchIt.pdf; Version 4.2.0, May 26, 2021.) was used to implement propensity score matching [16,17,18,19].
Results
There was a total of 744 patients with dnBOMBC treated at each of the participating institutions between 2014 and 2022, with 372 (50%) participants in each arm. One hundred and fifty-one (40.6%) patients in the LRT group had received ST prior to primary breast surgery (ST+LRT group) and 221 (59.4%) patients underwent breast surgery prior to ST (LRT+ST group) (Table 1 and Table 2). Median follow-up was 48 months (IQR 25-75%: 32-66,) and it was 39 months and 58 months in ST and LRT groups, respectively (p<0.001). Patients in the LRT group were younger than the ST group (median age 50 vs. 55 years, p=0.0001) with no body mass index (BMI) differences (median 27 kg/m2 vs. 28 kg/m2, p=0.39). Solitary bone metastasis was significantly more common in the LRT group (50% vs. 24%, p<0.001). The ST group had more multiple metastases (76% vs. 50%), and higher T stage tumors (T3: 23% vs. 13%, p=0.009) (Table 1).
Invasive ductal carcinoma (IDC) predominated in both groups but was more common in the LRT cohort (84% vs. 77%, p=0.0005).
There were no significant differences in HER-2 positive (28% vs. 25%, p=0.36) and triple negative BCs (7% vs. 5%, p=0.28). Estrogen/Progesterone receptor (ER/PR) positive tumor was lower in the LRT group (84% vs. 89%, p=0.04), although hormonal therapy was administered equally (85% in both groups, p=0.99). Chemotherapy administration was higher in the LRT group (95% vs. 87%, p=0.0005), and bisphosphonate treatment was lower in the LRT group (62% vs. 70%, p=0.02). Ovarian suppression therapy use was similar (24% in LRT vs. 19% in ST; p=0.13). Intervention to metastatic sites was comparable between groups (53% LRT vs. 51% ST; p=0.46).
In subgroup analysis, solitary metastasis was more common in the LRT+ST group (57%) than in ST+LRT group (40%) (p<0.001). Chemotherapy use was slightly higher in the ST+LRT group (98%) compared to LRT+ST (93%) and ST group (87%) (p=0.0002). Bisphosphonate treatment was significantly less frequent in ST+LRT (54%) compared to LRT+ST (67%) and ST (70%) (p=0.003). Ovarian suppression therapy rates were similar between subgroups (Table 2).
During follow-up, 58% (n=217) of patients in the ST group and 32% (n=120) of patients in the LRT group died (p<0.001). LP was observed in 20% (n=76) of patients in the ST group, compared to 9% (n=32) in the LRT group (p=0.0001). When stratifying within the LRT cohort, mortality was lower in both LRT+ST (34%) and ST+LRT (29%) groups compared to ST group (58%) (p<0.001).
In the overall cohort (N=744), median OS was 49 months for the ST group, and 92 months (HR, 0.37; 95% CI, 0.29–0.48; p<0.0001) for the ST+LRT and it was 99 months (HR, 0.34; 95% CI, 0.24–0.47; p<0.0001) for the LRT+ST (Figure 2). Overall LRT group was associated with significantly improved OS compared to ST group (HR, 0.36; 95% CI, 0.29–0.45; p<0.0001). LRT improved OS in both solitary bone metastasis patients (HR, 0.38; 95% CI, 0.26–0.55; p<0.0001) and those with multiple bone metastases (HR, 0.38; 95% CI, 0.29–0.51; p<0.0001).
Propensity score matching is used to reduce the bias due to confounding variables might affect the LRT estimation in this registry study. Comparison of OS between propensity score matched ST and LRT groups further confirmed better survival for the LRT group (HR: 0.57, 95% Cl: 0.42-0.78) (Figure 2 and Figure 3).
SP occurred more frequently in the ST group, affecting 66% (n=244) of patients, compared to 41% (n=152) in the LRT group and it was 39% (n=87) in LRT+ST and 43% (n=65) in ST+LRT; p<0.001). LP was significantly less in the LRT group of patients (10% (n=23) in LRT+ST, 6% (n=9) in ST+LRT vs. 20% (n=76) in ST; p=0.0001).
In univariate analysis, LRT was associated with a significantly improved OS (HR 0.35; 95% CI 0.29-0.45; p<0.0001). Better OS was observed in patients younger than 52 years (HR 1.30; 95% CI 1.05-1.62; P=0.02), patients with no LP (HR 1.92; 95% CI 1.48-2.49; p<0.0001), no SP (HR 5.89; 95% CI 4.38-7.93; p<0.0001), lower number of metastasis (HR 1.59; 95% CI 1.26-1.99; p<0.0001) and ER/PR(+) (HR 0.74; 95% CI 0.56-0.98; p=0.04). In a multivariate Cox proportional model with a significant baseline and clinical characteristics, yielded consistent results with those from the univariable Cox analysis. OS was independently associated with LRT (HR 0.49; 95% CI 0.38-0.63; p<0.0001), age younger than 52 years (HR 1.29; 95% CI 1.02-1.61; p=0.03), SP (HR 4.84; 95% CI 3.55-6.63; p<0.0001) and ER/PR (+) (HR 0.62; 95% CI 0.46-0.84; p=0.002) (Table 3). However, LP and solitary metastasis lost their significance. Other factors such as tumor size, tumor type, histologic grade, chemotherapy and bisphosphonate treatment were not independent predictors of OS (p>0.05).
Discussion
Distant metastasis is the most important factor shortening survival in BC patients. The St. Gallen International Consensus and ESMO guidelines have increasingly supported curative-intent approaches in carefully selected cases of oligometastatic BC(20-23). In 2021 at the St. Gallen International Consensus, patients with low-volume or oligometastatic disease who respond to ST were considered candidates for multimodal treatment with curative intent. This trend continued in subsequent years, with 85–86% of experts supporting the addition of LRT in isolated bone metastases, particularly in HER2-positive or HR-positive patients [20,21]. These evolving recommendations reflect a growing international consensus toward expanding the role of potentially curative strategies in selected dnMBC patients.
Bone is the most frequent site of distant metastatic site in BC, and patients with bone-only metastases generally have a more favorable prognosis than those with visceral or brain involvement [24]. Although Marie et al. retrospectively reviewed 242 bone only MBC patients, stratifying them by age (< 50 vs ≥ 50 years), and found no significant differences in 5-year OS (44.9% vs 39.2%; p = 0.21) or 5-year progression-free survival (both 22.7%; p = 0.55) [25]. The MF07-01 randomized trial by Soran et al. demonstrated a 29% reduction in the hazard of death (HoD) in the LRT group (HR: 0.71; 95% CI: 0.59–0.86; p = 0.0003), particularly in HR-positive, HER2-negative, bone-only patients under 55 years [14,26]. Patients with solitary bone-only metastases patient had 45% less HoD (HR 0.55; 95% CI 0.36-086; p= 0.009) at the 10 year follow-up [26]. In addition, a prospective registry showed a 60% reduction in mortality risk in the LRT group [2]. The current BOMETIN registry study substantially expands upon this with a larger cohort, longer follow-up, and consistent findings, reinforcing the survival benefit of LRT in dnBOMBC. In this current analysis, LRT was associated with a 64% reduction in HoD (HR 0.36; 95% CI 0.29–0.45; p < 0.0001). In multivariable Cox regression analysis, age younger than 52 years was identified as an independent predictor of improved OS (HR 1.29 95% CI 1.02–1.61; p = 0.03). This large-scale, prospective, multi-national and multi-institutional registry study provides strong real-world evidence supporting the use of LRT in dnBOMBC. Among 744 patients treated between 2014 and 2022, those receiving LRT had significantly lower mortality (32% vs. 58%, p < 0.001), fewer LP (9% vs. 20%, p = 0.0001) and SP (41% vs. 66%, p < 0.001). This benefit remained consistent across patients with solitary (HR = 0.38; 95% CI: 0.26–0.55) and multiple bone metastases (HR = 0.38; 95% CI: 0.29–0.51), suggesting independence from disease burden. Notably, outcomes did not differ based on the timing of surgery in relation to ST.
Metastatic BC represents a heterogeneous disease spectrum. Our subgroup analysis revealed better outcomes in ER/PR-positive patients (HR = 0.62; p = 0.002), while SP was the most significant negative prognostic factor (HR = 4.84; p < 0.0001). Similarly, Lane et al. reported that surgery was independently associated with improved OS in ER-positive patients [27]. Several retrospective and prospective studies have evaluated the extent of metastatic burden. Lopez-Tarruella et al. found improved OS with LRT in a large cohort of dnMBC patients, particularly in those with bone or oligometastatic disease [28]. Wang et al. demonstrated that LRT improved survival even in patients with multiple bone lesions and even some limited visceral metastases [29]. In our study, patients with solitary bone metastasis were more likely to receive LRT (50% vs. 24%; p < 0.001). However, survival benefit from LRT persisted in both solitary and multiple metastasis subgroups.
While many observational studies with a large sample size support the survival benefit of surgery, some RCTs have not demonstrated a significant OS advantage in unselected dnMBC populations [9,10,30,31]. These RCTs had some limitations, such as patients not receiving standard care of ST agents, early termination of the study with a very limited patient enrollment, heterogeneous patient characteristics, or suboptimal surgical techniques. A pooled meta-analysis of 7 RCTs including 1,018 patients found no OS benefit (HR: 0.87; 95% CI: 0.68–1.11; p = 0.265), though LP free survival was significantly improved (HR: 0.27; 95% CI: 0.19–0.38; p < 0.001) [32]. Although elimination of dissemination of disease from the primary tumor, control of metastatic disease prompted by removal of the primary tumor, and eliminating the possibility of the primary tumor producing factors that promote the growth of distant disease are proposed reasons that might improve survival, biological hypotheses suggest that surgical removal of the primary tumor may disrupt dormancy signals or promote circulating tumor cell dissemination [33,34,35]. The Cochrane review by Tosello et al. concluded that while LRT improved local control (HR: 0.22; 95% CI: 0.08–0.57), it was associated with worse distant progression (HR: 1.42; 95% CI: 1.08–1.86), possibly due to delays or interruptions in ST [36]. The ECOG-ACRIN trial reported improved local control with LRT, no benefit in OS, but was criticized for inadequate margins and a high percentage of patients with advanced local disease [30]. Similarly, Reinhorn et al.'s pooled analysis of four RCTs showed no OS benefit regardless of subtype or metastatic pattern [37]. By contrast, in our study with anthracycline-taxane-based chemotherapy, anti-HER2 therapy, endocrine therapy (aromatase inhibitors or tamoxifen/ovarian suppression), and bone-modifying agents, LRT reduced mortality from 58% to 32% (p<0.001), extended median OS from 49 months to 92 months (ST+LRT) and 99 months (LRT+ST), decreased LP from 20% to 9% (p=0.0001), and decreased SP from 66% to 41% (p<0.001), underscoring the value of optimal patient selection and integration of LRT with modern ST in this population.
To better define candidates for LRT, predictive models and nomograms have been proposed. Kommalapati et al., analyzed 67,978 dnMBC patients to create a prognostic scoring system and they found that the patients who received LRT had significantly improved median OS (45 months) as compared to those who did not (24 months) (p<0.0001) [38]. Although it awaits validation, a SEER-based model has shown promise for a new prognostic staging system for de novo MBC [39]. A study comparing MD Anderson and Jeanny nomograms in 72 dnBOMBC patients found better predictive performance in surgically treated patients [40]. Goktepe et al. published a study of a combination of data from a phase 3 randomized trial and a prospective multi-institutional registry trial and in this study, LRT significantly improved OS in patients with Her 2-positive, HR-positive and low grade tumor and less than 5 cm tumors (solitary: HR, 0.375, 95% CI 0.259-0.543, p<0.001; multiple: HR 0.435, 95% CI 0.334-0.615, p <0.001) [41]. Conversely, in the group of patients who had high grades, T4 and triple-negative tumors, there was no significant benefit of OS from LRT. These results underline the need for individualized, surgery-specific prognostic tools.
The strengths of our study include its large prospective registry design, long follow-up (median 48 months), and multi-institutional collaboration. LRT remained an independent predictor of improved OS in both surgical subgroups in univariate and multivariable Cox regression models. Although this study has a greater sample size, there are some limitations; patients in the LRT group were younger (median age 50 vs. 55 years; p = 0.0001), had more solitary bone lesions (50% vs. 24%; p < 0.001), and more frequently received chemotherapy (95% vs. 87%; p = 0.0005), suggesting possible selection bias. Limitations also include a lack of quality-of-life data, detailed radiotherapy fields, surgical techniques, and use of newer ST agents such as CDK4/6 inhibitors or immunotherapy. On the other hand, to reduce the bias due to confounding variables might affect the LRT estimation in this registry study propensity score matching is used. Comparison of OS between propensity score matched ST and LRT groups further confirmed better survival for the LRT group (HR: 0.57, 95% Cl: 0.42-0.78) (Figure 2 and Figure 3).
In conclusion, this large prospective registry study focused exclusively on dnBOMBC provides the most recent high-level real-world evidence that LRT significantly improves survival and disease control. Future prospective trials should further refine patient selection and incorporate quality-of-life outcomes to inform personalized, multidisciplinary treatment strategies.
Contributions:
- Atilla Soran: study design, data collection, statistical analysis, data interpretation and editing of the manuscript.
- Berk Goktepe: study design, statistical analysis, writing of the manuscript.
- Berkay Demirors: study design, statistical analysis, writing of the manuscript.
- Ozgur Aytac: study design, statistical analysis, writing of the manuscript.
- Serdar Ozbas: study design, statistical analysis, writing of the manuscript.
- Lutfi Dogan: study design, statistical analysis, writing of the manuscript.
- Didem Can Trablus: study design, statistical analysis, writing of the manuscript.
- Jamila Al-Azhri: study design, statistical analysis, writing of the manuscript.
- Kazım Senol: study design, data interpretation, editing of the manuscript
- Shruti Zaveri: study design, data interpretation, editing of the manuscript
- Salyna Meas: study design, data interpretation, editing of the manuscript
- Umut Demirci: study design, data interpretation, editing of the manuscript
- Hasan Karanlik: study design, data interpretation, editing of the manuscript
- Aykut Soyder: data interpretation, editing of the manuscript
- Ahmet Dag: data interpretation, editing of the manuscript
- Ahmet Bilici: data interpretation, editing of the manuscript
- Mutlu Dogan: data interpretation, editing of the manuscript
- Mehmet Ali Nahit Sendur: data interpretation, editing of the manuscript
- Hande Koksal: data interpretation, editing of the manuscript
- Mehmet Ali Gulcelik: data interpretation, editing of the manuscript
- Neslihan Cabioglu: data interpretation, editing of the manuscript
- Levent Yeniay: data interpretation, editing of the manuscript
- Zafer Utkan: data interpretation, editing of the manuscript
- Nuri Karadurmus: data interpretation, editing of the manuscript
- Gul Daglar: data interpretation, editing of the manuscript
- Turgay Simsek: data interpretation, editing of the manuscript
- Birol Yildiz: data interpretation, editing of the manuscript
- Cihan Uras: data interpretation, editing of the manuscript
- Mustafa Tukenmez: data interpretation, editing of the manuscript
- Cihangir Ozaslan: data interpretation, editing of the manuscript
- Niyazi Karaman: data interpretation, editing of the manuscript
- Arda Isik: data interpretation, editing of the manuscript
- Efe Sezgin: study design, statistical analysis, writing of the manuscript
- Vahit Ozmen: study design, statistical analysis, writing of the manuscript
- Anthony Lucci: study design, statistical analysis, writing of the manuscript
Funding
This study was conducted without external funding.
Conflicts of Interest
All the authors of this study have no conflict of interest to disclose.
Abbreviations
| LRT | Loco-regional treatment |
| ST | Systemic therapy |
| OS | Overall survival |
| dnBOMBC | De novo bone-only metastatic breast cancer |
| dnMBC | De novo metastatic breast cancer |
| HR | Hormone receptor |
| HER2 | Human epidermal growth factor receptor 2 |
| ER | Estrogen receptor |
| PR | Progesterone receptor |
| LP | locoregional progression |
| LRT | locoregional treatment |
| SP | Systemic progression |
| CDK | cyclin-dependent kinase |
| RCT | Randomized controlled trial |
| HR | Hazard ratio |
| CI | Confidence interval |
| OS | Overall survival |
| NCCN | National Comprehensive Cancer Network |
References
- Wagle NS, Nogueira L, Devasia TP, Mariotto AB, Yabroff KR, Islami F, et al. Cancer treatment and survivorship statistics, 2025. CA: A Cancer Journal for Clinicians. 2025. [CrossRef]
- Soran A, Dogan L, Isik A, Ozbas S, Trabulus DC, Demirci U, et al. The Effect of Primary Surgery in Patients with De Novo Stage IV Breast Cancer with Bone Metastasis Only (Protocol BOMET MF 14-01): A Multi-Center, Prospective Registry Study: A. Soran et al. Annals of Surgical Oncology. 2021;28(9):5048-57. [CrossRef]
- Iwase T, Shrimanker TV, Rodriguez-Bautista R, Sahin O, James A, Wu J, et al. Changes in overall survival over time for patients with de novo metastatic breast cancer. Cancers. 2021;13(11):2650. [CrossRef]
- Eng LG, Dawood S, Sopik V, Haaland B, Tan PS, Bhoo-Pathy N, et al. Ten-year survival in women with primary stage IV breast cancer. Breast cancer research and treatment. 2016;160(1):145-52. [CrossRef]
- Gupta RK, Roy AM, Gupta A, Takabe K, Dhakal A, Opyrchal M, et al. Systemic therapy de-escalation in early-stage triple-negative breast cancer: dawn of a new era? Cancers. 2022;14(8):1856. [CrossRef]
- Liu B, Liu H, Liu M. Aggressive local therapy for de novo metastatic breast cancer: Challenges and updates. Oncology Reports. 2023;50(3):163.
- Gradishar WJ, Moran MS, Abraham J, Abramson V, Aft R, Agnese D, et al. Breast cancer, version 3.2024, NCCN clinical practice guidelines in oncology. Journal of the National Comprehensive Cancer Network. 2024;22(5):331-57. [CrossRef]
- Gennari A, André F, Barrios C, Cortes J, de Azambuja E, DeMichele A, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer☆. Annals of oncology. 2021;32(12):1475-95. [CrossRef]
- Gera R, Chehade HEH, Wazir U, Tayeh S, Kasem A, Mokbel K. Locoregional therapy of the primary tumour in de novo stage IV breast cancer in 216 066 patients: A meta-analysis. Scientific reports. 2020;10(1):2952. [CrossRef]
- Vohra NA, Brinkley J, Kachare S, Muzaffar M. Primary tumor resection in metastatic breast cancer: A propensity-matched analysis, 1988-2011 SEER data base. The breast journal. 2018;24(4):549-54.
- Xiao W, Zou Y, Zheng S, Hu X, Liu P, Xie X, et al. Primary tumor resection in stage IV breast cancer: A systematic review and meta-analysis. European Journal of Surgical Oncology. 2018;44(10):1504-12. [CrossRef]
- Badwe R, Hawaldar R, Nair N, Kaushik R, Parmar V, Siddique S, et al. Locoregional treatment versus no treatment of the primary tumour in metastatic breast cancer: an open-label randomised controlled trial. The lancet oncology. 2015;16(13):1380-8. [CrossRef]
- Abo-Touk N, Fikry A, Fouda E. The benefit of locoregional surgical intervention in metastatic breast cancer at initial presentation. Cancer Research Journal. 2016;4(2):32-6. [CrossRef]
- Soran A, Ozmen V, Ozbas S, Karanlik H, Muslumanoglu M, Igci A, et al. Randomized trial comparing resection of primary tumor with no surgery in stage IV breast cancer at presentation: protocol MF07-01. Annals of surgical oncology. 2018;25(11):3141-9. [CrossRef]
- Pulido C, Vendrell I, Ferreira AR, Casimiro S, Mansinho A, Alho I, et al. Bone metastasis risk factors in breast cancer. Ecancermedicalscience. 2017;11:715. [CrossRef]
- Austin, PC. The use of propensity score methods with survival or time-to-event outcomes: reporting measures of effect similar to those used in randomized experiments. Statistics in medicine. 2014;33(7):1242-58. [CrossRef]
- Austin PC, Stuart EA. Optimal full matching for survival outcomes: a method that merits more widespread use. Statistics in medicine. 2015;34(30):3949-67. [CrossRef]
- Hansen BB. Full matching in an observational study of coaching for the SAT. Journal of the American Statistical Association. 2004;99(467):609-18. [CrossRef]
- Stuart EA, Green KM. Using full matching to estimate causal effects in nonexperimental studies: examining the relationship between adolescent marijuana use and adult outcomes. Developmental psychology. 2008;44(2):395. [CrossRef]
- Burstein H, Curigliano G, Thürlimann B, Weber W, Poortmans P, Regan M, et al. Customizing local and systemic therapies for women with early breast cancer: the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Annals of oncology. 2021;32(10):1216-35. [CrossRef]
- Curigliano G, Burstein H, Gnant M, Loibl S, Cameron D, Regan M, et al. Corrigendum to “Understanding breast cancer complexity to improve patient outcomes: The St Gallen International Consensus Conference for the Primary Therapy of Individuals with Early Breast Cancer 2023”:[Annals of Oncology 34 (2023) 970-986]. Annals of Oncology. 2025;36(3):351.
- Loibl S, André F, Bachelot T, Barrios C, Bergh J, Burstein H, et al. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up☆. Annals of Oncology. 2024;35(2):159-82. [CrossRef]
- Im S-A, Gennari A, Park Y, Kim J, Jiang Z-F, Gupta S, et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the diagnosis, staging and treatment of patients with metastatic breast cancer. ESMO open. 2023;8(3):101541. [CrossRef]
- Yao Y-B, Zheng X-E, Luo X-B, Wu A-M. Incidence, prognosis and nomograms of breast cancer with bone metastases at initial diagnosis: a large population-based study. American journal of translational research. 2021;13(9):10248.
- Marie L, Braik D, Abdel-Razeq N, Abu-Fares H, Al-Thunaibat A, Abdel-Razeq H. Clinical characteristics, prognostic factors and treatment outcomes of patients with bone-only metastatic breast cancer. Cancer Management and Research. 2022:2519-31. [CrossRef]
- Soran A, Ozmen V, Ozbas S, Karanlik H, Muslumanoglu M, Igci A, et al. Primary surgery with systemic therapy in patients with de novo stage IV breast cancer: 10-year follow-up; protocol MF07-01 randomized clinical trial. Journal of the American College of Surgeons. 2021;233(6):742-51. e5. [CrossRef]
- Lane WO, Thomas SM, Blitzblau RC, Plichta JK, Rosenberger LH, Fayanju OM, et al. Surgical resection of the primary tumor in women with de novo stage IV breast cancer: contemporary practice patterns and survival analysis. Annals of surgery. 2019;269(3):537-44.
- Lopez-Tarruella S, Escudero M, Pollan M, Martín M, Jara C, Bermejo B, et al. Survival impact of primary tumor resection in de novo metastatic breast cancer patients (GEICAM/El Alamo Registry). Scientific reports. 2019;9(1):20081. [CrossRef]
- Wang K, Shi Y, Li Z-Y, Xiao Y-L, Li J, Zhang X, et al. Metastatic pattern discriminates survival benefit of primary surgery for de novo stage IV breast cancer: A real-world observational study. European Journal of Surgical Oncology. 2019;45(8):1364-72. [CrossRef]
- Khan SA, Zhao F, Goldstein LJ, Cella D, Basik M, Golshan M, et al. Early local therapy for the primary site in de novo stage IV breast cancer: results of a randomized clinical trial (E2108). Journal of Clinical Oncology. 2022;40(9):978-87. [CrossRef]
- Shien T, Nakamura K, Shibata T, Kinoshita T, Aogi K, Fujisawa T, et al. A randomized controlled trial comparing primary tumour resection plus systemic therapy with systemic therapy alone in metastatic breast cancer (PRIM-BC): Japan Clinical Oncology Group Study JCOG1017. Japanese journal of clinical oncology. 2012;42(10):970-3. [CrossRef]
- Ren C, Sun J, Kong L, Wang H. Breast surgery for patients with de novo metastatic breast cancer: A meta-analysis of randomized controlled trials. European Journal of Surgical Oncology. 2024;50(1):107308. [CrossRef]
- Fitzal F, Bjelic-Radisic V, Knauer M, Steger G, Hubalek M, Balic M, et al. Impact of breast surgery in primary metastasized breast cancer: outcomes of the prospective randomized phase III ABCSG-28 POSYTIVE trial. Annals of surgery. 2019;269(6):1163-9.
- Tohme S, Simmons RL, Tsung A. Surgery for cancer: a trigger for metastases. Cancer research. 2017;77(7):1548-52. [CrossRef]
- Castano Z, San Juan BP, Spiegel A, Pant A, DeCristo MJ, Laszewski T, et al. IL-1β inflammatory response driven by primary breast cancer prevents metastasis-initiating cell colonization. Nature cell biology. 2018;20(9):1084-97. [CrossRef]
- Tosello G, Torloni MR, Mota BS, Neeman T, Riera R. Breast surgery for metastatic breast cancer. Cochrane Database of Systematic Reviews. 2018(3).
- Reinhorn D, Mutai R, Yerushalmi R, Moore A, Amir E, Goldvaser H. Locoregional therapy in de novo metastatic breast cancer: systemic review and meta-analysis. The Breast. 2021;58:173-81. [CrossRef]
- Kommalapati A, Tella SH, Goyal G, Ganti AK, Krishnamurthy J, Tandra PK. A prognostic scoring model for survival after locoregional therapy in de novo stage IV breast cancer. Breast Cancer Research and Treatment. 2018;170(3):677-85. [CrossRef]
- Bai J, Li Z, Guo J, Gao F, Zhou H, Zhao W, et al. Development of a predictive model to identify patients most likely to benefit from surgery in metastatic breast cancer. Scientific Reports. 2023;13(1):3845. [CrossRef]
- Verghis N SC, Soran A, editor The applicability of two survival nomograms for surgery in bone-only de novo stage IV breast cancer. The 26th 2025 American Society of Breast Surgeons Annual Meeting; 2025; The Bellagio Las Vegas.
- Goktepe B, Demirors B, Senol K, Ozbas S, Sezgin E, Lucci A, et al. A Pragmatic Grouping Model for Bone-Only De Novo Metastatic Breast Cancer (MetS Protocol MF22-03). Cancers. 2025;17(12):2033. [CrossRef]
Figure 1.
Standardized mean differences of confounding covariates before and after propensity score matching.
Figure 1.
Standardized mean differences of confounding covariates before and after propensity score matching.
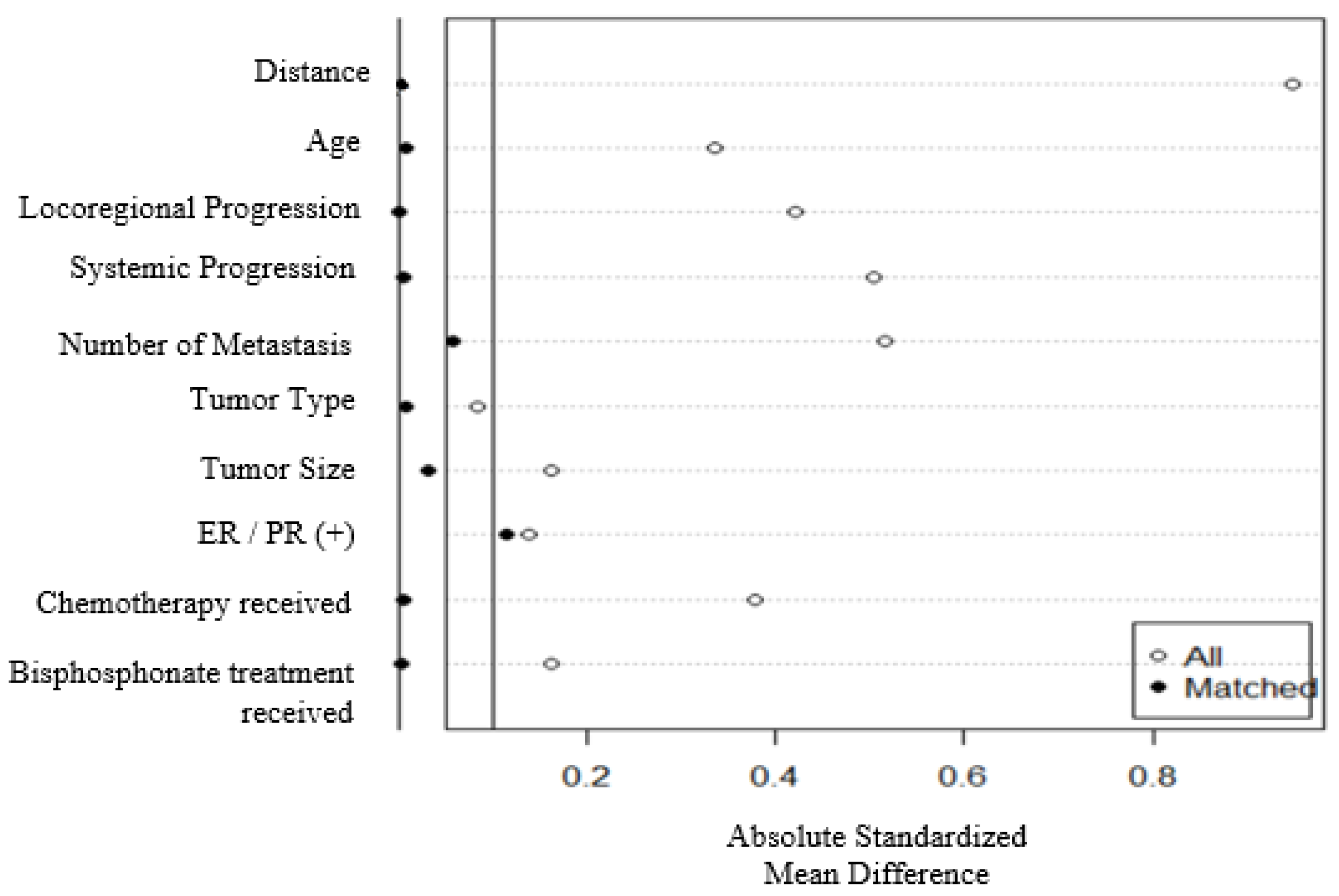
Figure 2.
Overall survival regarding systemic therapy (ST) and loco-regional therapy (LRT); subgroups defined as LRT+ST and ST+LRT groups.
Figure 2.
Overall survival regarding systemic therapy (ST) and loco-regional therapy (LRT); subgroups defined as LRT+ST and ST+LRT groups.
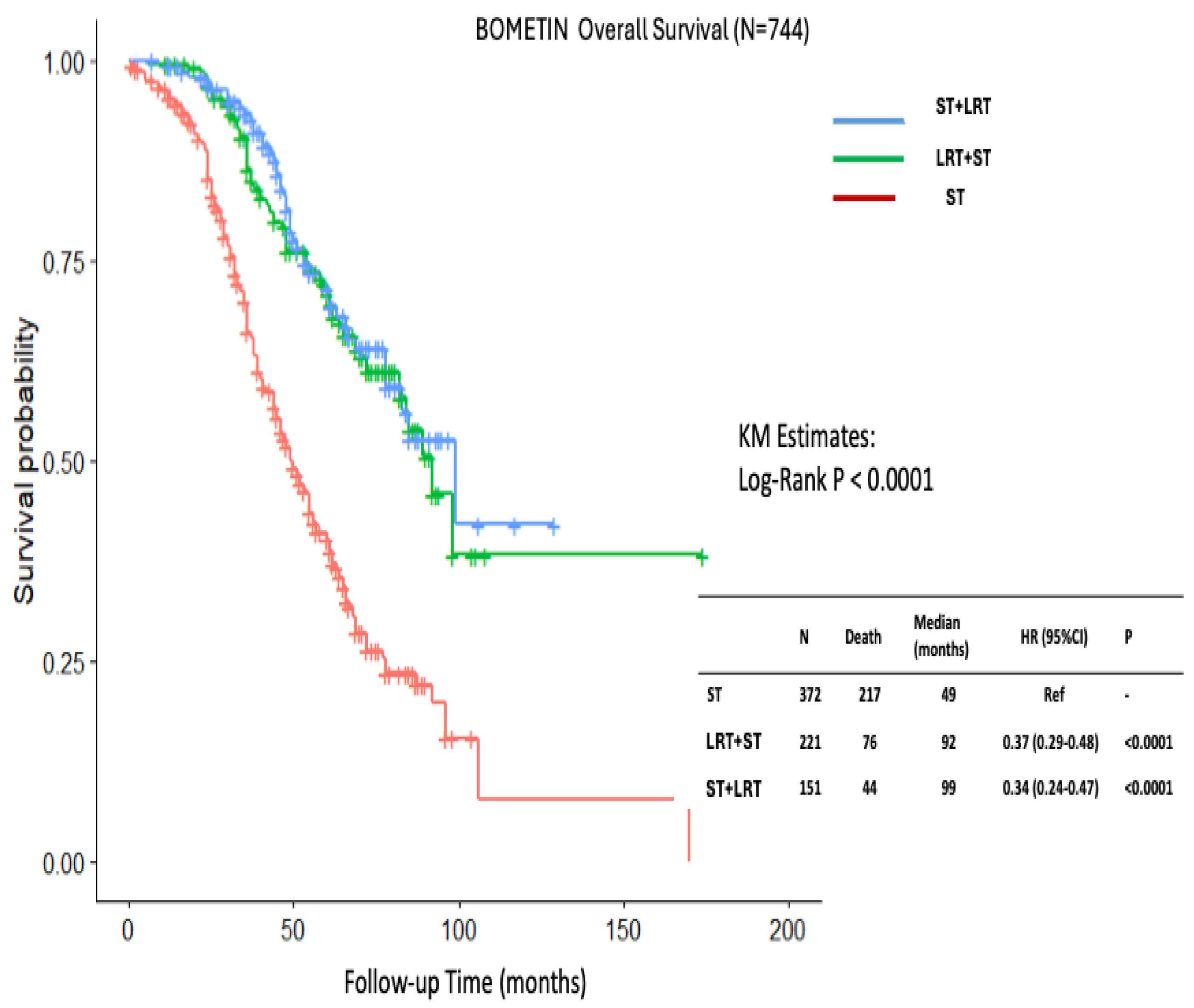
Figure 3.
Overall survival comparison between Systemic therapy (ST) and Loco-regional therapy (LRT) groups in patients’ propensity score matched.
Figure 3.
Overall survival comparison between Systemic therapy (ST) and Loco-regional therapy (LRT) groups in patients’ propensity score matched.
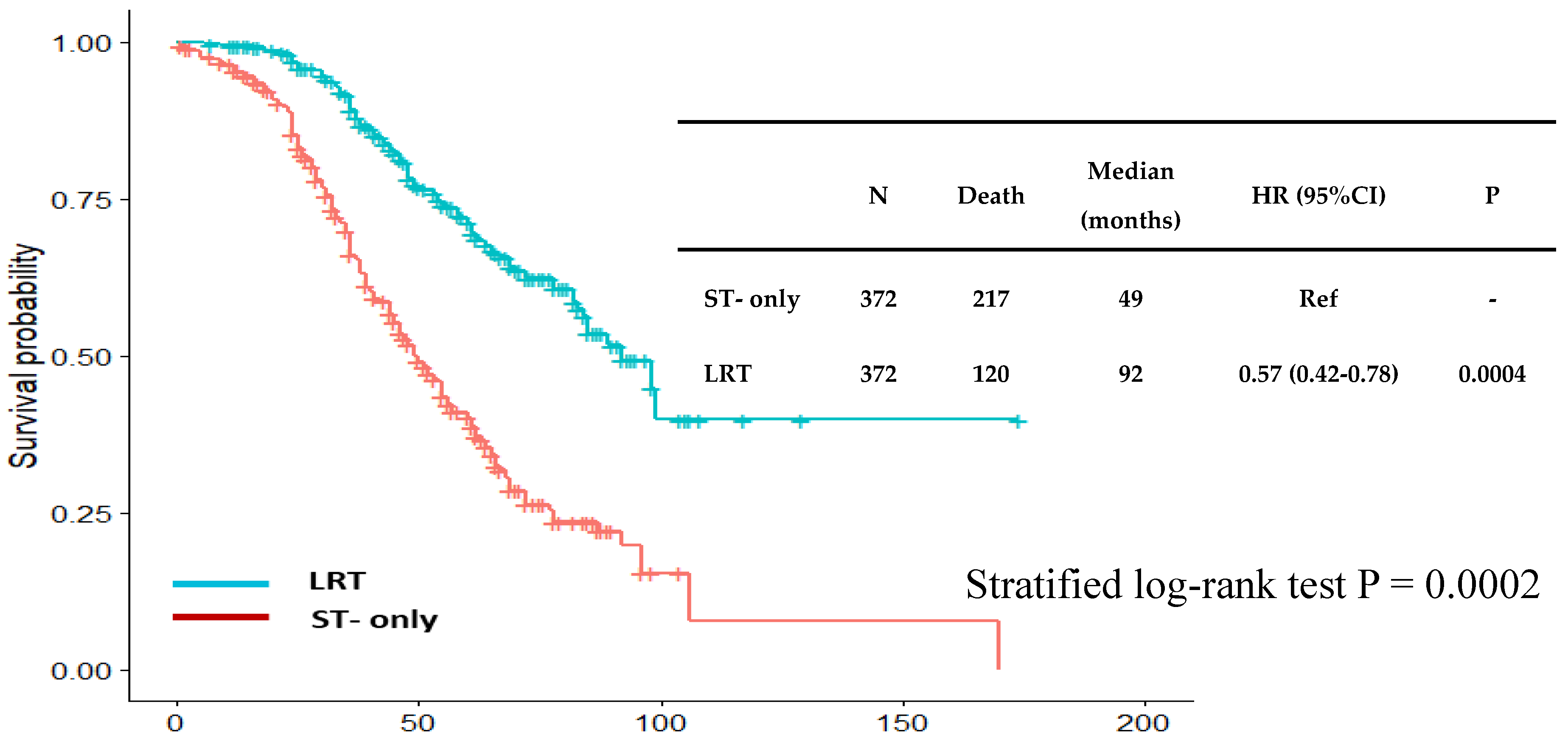

Table 1.
Baseline characteristics between Systemic therapy (ST) and Loco-regional therapy (LRT) groups.
Table 1.
Baseline characteristics between Systemic therapy (ST) and Loco-regional therapy (LRT) groups.
| ST group N=372 (%) |
LRT group N=372 (%) |
P value | |
|---|---|---|---|
| Median follow-up (25%,75%) | 39 (26, 58) | 58 (38, 74) | < 0.001 |
| Median age (25%,75%) | 55 (44, 66) | 50 (42, 60) | 0.0001 |
| Median Body mass index (25%,75%) | 28 (25, 31) | 27 (25, 31) | 0.39 |
| Locoregional progression | 76 (20) | 32 (9) | 0.0001 |
| Systemic progression | 244 (66) | 152 (41) | < 0.001 |
| Mortality rate | 217 (58) | 120 (32) | < 0.001 |
| Number of metastases | < 0.001 | ||
| Solitary | 89 (24) | 185 (50) | |
| Multiple (>1) | 283 (76) | 187 (50) | |
| Tumor size | 0.009 | ||
| T1 | 66 (18) | 60 (16) | |
| T2 | 246 (66) | 219 (59) | |
| T3 | 47 (13) | 84 (23) | |
| T4 | 11 (3) | 9 (2) | |
| Tumor type | 0.0005 | ||
| Invasive Ductal Carcinoma | 286 (77) | 313 (84) | |
| Invasive Lobular Carcinoma | 58 (16) | 25 (7) | |
| Others | 27 (7) | 34 (9) | |
| Histologic grade | 0.02 | ||
| 1 | 52 (14) | 32 (9) | |
| 2 | 162 (45) | 188 (51) | |
| 3 | 129 (36) | 140 (38) | |
| Missing | 16 (4) | 8 (2) | |
| Her2 status | 0.36 | ||
| Negative | 279 (75) | 268 (72) | |
| Positive | 93 (25) | 104 (28) | |
| Estrogen/Progesterone receptors | 0.04 | ||
| Negative | 41 (11) | 60 (16) | |
| Positive | 331 (89) | 312 (84) | |
| Triple Negative | 0.28 | ||
| No | 353 (95) | 346 (93) | |
| Yes | 19 (5) | 26 (7) | |
| Hormonotherapy | 317 (85) | 317 (85) | 0.99 |
| Chemotherapy | 322 (87) | 353 (95) | 0.0005 |
| Bisphosphonate treatment | 260 (70) | 231 (62) | 0.02 |
| Ovarian suppression | 71 (19) | 88 (24) | 0.13 |
| Intervention to metastasis | 188 (51) | 198 (53) | 0.46 |
Table 2.
Baseline characteristics among Systemic therapy (ST) and Loco-regional therapy (LRT); subgroups defined as LRT+ST and ST+LRT groups.
Table 2.
Baseline characteristics among Systemic therapy (ST) and Loco-regional therapy (LRT); subgroups defined as LRT+ST and ST+LRT groups.
| ST group N=372 (%) |
LRT+ST group N=221 (%) |
ST+LRT group N=151 (%) |
P value | |
|---|---|---|---|---|
| Median follow-up (25%,75%) | 39 (26, 58) | 59 (40, 74) | 53 (38, 73) | < 0.001 |
| Median age (25%,75%) | 55 (44, 66) | 50 (43, 59) | 49 (40, 60) | 0.0001 |
| Median BMI (25%,75%) | 28 (25, 31) | 27 (24, 31) | 27 (25, 31) | 0.69 |
| Locoregional progression | 76 (20) | 23 (10) | 9 (6) | 0.0001 |
| Systemic progression | 244 (66) | 87 (39) | 65 (43) | < 0.001 |
| Mortality rate | 217 (58) | 76 (34) | 44 (29) | < 0.001 |
| Number of metastases | < 0.001 | |||
| Solitary | 89 (24) | 125 (57) | 60 (40) | |
| Multiple (>1) | 283 (76) | 96 (43) | 91 (60) | |
| Tumor size | 0.008 | |||
| T1 | 66 (18) | 42 (19) | 18 (12) | |
| T2 | 246 (66) | 132 (60) | 87 (58) | |
| T3 | 47 (13) | 44 (20) | 40 (26) | |
| T4 | 11 (3) | 3 (1) | 6 (4) | |
| Tumor type | 0.002 | |||
| Invasive Ductal Carcinoma | 286 (77) | 186 (84) | 127 (84) | |
| Invasive Lobular Carcinoma | 58 (16) | 12 (5) | 13 (9) | |
| Others | 27 (7) | 23 (10) | 11 (7) | |
| Histologic grade | 0.036 | |||
| 1 | 52 (14) | 18 (8) | 14 (10) | |
| 2 | 162 (45) | 111 (50) | 77 (52) | |
| 3 | 129 (36) | 84 (38) | 56 (38) | |
| Missing | 16 (4) | 8 (4) | 0 (0) | |
| Her2 status | 0.40 | |||
| Negative | 279 (75) | 155 (70) | 113 (75) | |
| Positive | 93 (25) | 66 (30) | 38 (25) | |
| Estrogen/Progesterone receptors | 0.05 | |||
| Negative | 41 (11) | 40 (18) | 20 (13) | |
| Positive | 331 (89) | 181 (82) | 131 (87) | |
| Triple negative | 0.07 | |||
| No | 353 (95) | 201 (91) | 145 (96) | |
| Yes | 19 (5) | 20 (9) | 6 (4) | |
| Hormonotherapy | 317 (85) | 182 (82) | 135 (89) | 0.17 |
| Chemotherapy | 322 (87) | 205 (93) | 148 (98) | 0.0002 |
| Bisphosphonate treatment | 260 (70) | 149 (67) | 82 (54) | 0.003 |
| Ovarian suppression | 71 (19) | 49 (22) | 39 (26) | 0.22 |
| Intervention to metastasis | 188 (51) | 99 (45) | 99 (66) | 0.0003 |
Table 3.
Univariate and Multivariable Cox models for overall survival.
| Parameter | HR (95%CI) | P | HRadj (95%CI) | Padj |
|---|---|---|---|---|
| Locoregional therapy | 0.35 (0.29-0.45) | <0.0001 | 0.49 (0.38-0.63) | <0.0001 |
| Age > 52 (median age) | 1.30 (1.05-1.62) | 0.02 | 1.29 (1.02-1.61) | 0.03 |
| Locoregional progression | 1.92 (1.48-2.49) | <0.0001 | 1.18 (0.89-1.55) | 0.25 |
| Systemic progression | 5.89 (4.38-7.93) | <0.0001 | 4.84 (3.55-6.63) | <0.0001 |
| Number of metastases | 1.59 (1.26-1.99) | <0.0001 | 1.21 (0.96-1.54) | 0.11 |
| Primary tumor size | 1.09 (0.93-1.28) | 0.28 | 1.06 (0.89-1.27) | 0.51 |
| Tumor type | 1.02 (0.85-1.22) | 0.85 | 0.93 (0.77-1.13) | 0.48 |
| Histologic grade | 1.01 (0.87-1.18) | 0.88 | 0.97 (0.83-1.14) | 0.71 |
| ER/PR (+) | 0.74 (0.56-0.98) | 0.04 | 0.62 (0.46-0.84) | 0.002 |
| Chemotherapy received | 0.83 (0.56-1.22) | 0.33 | 1.30 (0.81-2.09) | 0.27 |
| Bisphosphonate treatment received | 1.08 (0.85-1.37) | 0.54 | 1.00 (0.77-1.30) | 0.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



