
Submitted:
06 May 2025
Posted:
07 May 2025
You are already at the latest version
Abstract
Background/Objectives: High-flux online hemodiafiltration (OL-HDF) appears to be associated with better survival than hemodialysis (HD). In Brazil, OL-HDF is only affordable for patients with private health insurance. Although observational studies have shown a survival advantage with OL-HDF, even in Brazil, it is unclear whether this benefit applies to patients without private health insurance. We compared overall and cardiovascular mortality between OL-HDF and HD in patients treated exclusively through the Public Health Care system. We hypothesize that patients on OL-HDF will have a higher survival rate than those on HD.
Methods: This is an observational cohort study. Adult patients on maintenance hemodialysis or OL-HDF for at least one month during the period between September 1, 2022, and December 1, 2024. The primary outcome was all-cause mortality. The secondary outcome was cardiovascular mortality. Fine-Gray sub-distribution hazard models were used to evaluate survival in the presence of competing events (kidney transplant and recovery of renal function).
Results: Patients on HD (N=321) and OL-HDF (N=48) were similar in age, race, sex, and vascular access. Patients on HD were more likely to have diabetes (54.0% vs. 29.2%, p=0.001) and spent more hours per week on dialysis (11.2 ± 1.8 vs. 10.5 ± 1.6 hours, p=0.006). In an adjusted Fine-Gray model, the hazard of death for patients on OL-HDF was 68% lower than that for patients on HD, and the risk of death for patients with an arteriovenous fistula was 55% lower compared to those with a catheter. Cardiovascular mortality did not differ between the groups.
Conclusions: These findings suggest that OL-HDF is associated with higher overall survival compared to HD, even for patients without private health insurance.
Keywords:
arteriovenous fistula
; chronic kidney disease
; dialysis
; mortality
Introduction
Hemodialysis (HD) is the most often performed modality of renal replacement therapy in Brazil [1] and around the world [2]. However, the mortality rate among patients on maintenance HD remains unacceptably high. Following the need for innovations, several studies have shown that hemodiafiltration (HDF), a therapy that combines diffusion and convection, which has provided better survival outcomes compared to HD. Among these studies, the Turkish study [3], the ESHOL [4] and the CONVINCE [5] have demonstrate improvement in survival, although some criticism still exist regarding some discrepancies between groups.
In Brazil, 80.3% of patients on hemodialysis are covered by the Public System Care [6], and the access to HDF is restricted to patients without private health insurance. When attempting to replicate survival comparison between HD and HDF, the bias is inevitable, as patients on HDF generally have better healthcare access and a higher overall socioeconomic status. Therefore, in Brazil, such a comparison is not fair, as it involves more than just a comparison of dialysis modalities. To date, only one study in Brazil has shown a survival advantage for HDF over HD, with a hazard ratio of 0.29 (0.11-0.77), in a propensity score analysis [7]. However, since the comparison was between patients with and without private health insurance, doubt remains regarding non-measured factors that might have influenced the results.
In the present study, we aimed to compare mortality between HD and online HDF patients without private health insurance. We hypothesize that patients on OL-HDF will have a higher survival rate than those on HD.
Materials and Methods
This is a retrospective cohort study comparing overall and cardiovascular mortality among patients receiving HD and online HDF (OL-HDF) in the absence of private health insurance.
Study Population
Patients on OL-HDF were recruited from the dialysis center of the Fundação Lia Maria Aguiar, a philanthropic dialysis center that provides HDF for all patients. Those on HD were recruited from a regional Hospital in the Public Health System. In both sites patients had no private health insurance.
Inclusion criteria were adult patients on maintenance dialysis for at least 1 month in the period between September 1st, 2022, and December 1st, 2024. Exclusion criteria were adult patients with acute kidney injury or those hospitalized in the last 3 months.
Sample size was obtained by convenience and all patients in both centers were screened. Patients were follow-up to the study entry until end of follow-up by reaching an endpoint or end of study.
Demographic, clinical, laboratory and dialysis data were obtained from electronic charts and manually checked in each center. Data evaluated included age, sex, presence of diabetes, and type of vascular access (arteriovenous fistula or catheter) at the study entry. Data on dialysis prescription were also evaluated and included frequency and number of dialysis hours per week).
For OL-HDF (Fresenius 5008 machine) ultrapure dialysate and high-flux polysulfone membrane (Fresenius Cordiax Fx1000, FX 800, and FX 600) were used. Except in some cases with high risk of coagulation, post dilution OL-HDF is prescribed to achieve a substitution volume of at least 23 L per session. For HD (Fresenius 4008 machine), blood flow was set between 300-400ml/min. Dialysate flow rate was 500 ml/min in both sites. Ultrafiltration was prescribed according to dry weight and physicians were free to adjust upon clinical evaluation. Potassium dialysate concentration was 2 mEq/L and calcium 2.5 or 3 mEq/L, with bicarbonate individualized around 30-32 mEq/L.
The study was conducted according to the Declaration of Helsinki. Local Ethic committee has approved the protocol (#84252424.0.0000.5511), and all patients provided written consent form. Clinical data was anonymized for safety and privacy.
Study Outcomes
The primary outcome was all-cause mortality. All deaths and cause of deaths observed during the study period were recorded. Secondary outcome was cardiovascular mortality, defined as stroke, myocardial infarction or heart failure as primary cause of death.
All patients were followed until death, kidney transplant, recovery of renal function, loss of follow-up or end of study period.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation or median (25, 75 percentile) according to data distribution, checked using Shapiro-wilk test. Categorical data was presented as number and percentage. Comparison between OL-HDF and HD groups was performed using t-test or Mann-Whitney U test for normally and not-normally distributed data, respectively. For categorical data we used chi-square or Fisher, as appropriate.
Fine-gray sub-distribution hazard models were used to evaluate survival in the presence of a competing event (kidney transplant and recovery of renal failure). In the initial multivariate model, all predictor variables were considered. Then, the non-significant variables were excluded one by one in order of significance (backward method). Interactions between the predictor variables and time were included in the final model – the non-significance of these variables suggests no violation of this assumption. For all statistical tests, a significance level of 5% was used. The analyses were performed using the statistical package STATA 17.
Results
Baseline characteristics were illustrated in Table 1. Age, race and sex were similar between HD (N=321) and OL-HDF groups (N=58). Diabetes was more prevalent in patients on HD. More frequent dialysis (4 or more times a week) was performed mostly among patients on OL-HDF, although this group had a lower number of hours on dialysis per week.
During a median follow-up time of 27.4 months, there were 92 deaths (87 on HD and 5 on OL-HDF). Recovery renal function (10 and 4 patients on HD and OL-HDF, respectively) and kidney transplantation (16 and 1 patients on HD and OL-HDF, respectively), were treated as competitive risk. Non-adjusted Kaplan Meier survival analysis (Figure 1) showed an advantage of mortality in patients on OL-HDF (log rank test p=0.011).
As shown in Table 1, modality of dialysis (p=0.015) and the presence of an arteriovenous fistula (p<0.001) were significantly associated with a better overall survival in univariate model. In the final adjusted model, the hazard of death for patients on OL-HDF was 68% lower than that for patients on HD. Additionally, the risk of death in patients with an AVF was 55% lower compared to patients with a catheter. Figure 2 illustrates the cumulative number of events according to dialysis modality and vascular access.
For cardiovascular mortality, we identified only 7 events, and OL-HDF was not associated with better survival [HR: 2.59 (0.51-13.27), p=0.254] in a model adjusted for age, diabetes, vascular access and time on dialysis per week.

Table 2.
Fine and Gray model for all-cause mortality.
| Univariate model | Initial multivariate model | Final multivariate model | ||||
|
Crude HR (IC 95%) |
p |
Adjusted HR (IC 95%) |
p |
Adjusted HR (IC 95%) |
p | |
| HD - reference | 0.33 (0.13-0.81) | 0.015 | 0.32 (0.13-0.81) | 0.015 | 0.32 (0.13-0.77) | 0.011 |
| Age, years | 1.01 (1.00-1.03) | 0.104 | 1.01 (0.99-1.03) | 0.234 | - | - |
| Diabetes | 1.47 (0.97-2.23) | 0.068 | 1.36 (0.88-2.09) | 0.167 | - | - |
| Arteriovenous fistula | 0.46 (0.29-0.71) | <0.001 | 0.46 (0.29-0.72) | 0.001 | 0.45 (0.29-0.69) | <0.001 |
| Hours on dialysis/week | 0.95 (0.87-1.05) | 0.339 | 0.93 (0.85-1.03) | 0.177 | ||
HR, hazard ratio. N=92, 31 and 146 cases of death, competitive events and censored cases, respectively. Final model proportional risk test (p=0.992).
Discussion
In this study we found that OL-HDF was associated with higher survival rate over a 2-year follow-up period. Even adjusting for the mains factors influencing mortality in patients on maintenance dialysis, such as the presence of diabetes and the type of vascular access, OL-HDF showed a 68% lower incidence of all-cause mortality compared to patients on standard HD. Our study is unique because we included patients without private health insurance, which reduces the bias of selecting patients who have better overall access to healthcare.
The population included in this study shares some characteristics with the dialysis population in Brazil. Compared to data from the Census of the Brazilian Society of Nephrology,[1] patients in the HD group have a higher percentage of diabetes (54.5% vs. 32%), a similar percentage of patients undergoing dialysis 4 or more times per week (5.9% vs. 1.1%), and a lower percentage of patients with an arteriovenous fistula (47.4% vs. 70.8%). The age of our patients is also comparable to that of a large cohort of individuals starting hemodialysis in many regions in Brazil [8]. HDF was performed in 22% of patients with private health insurance in 2022 [1], a modality that has been increasing despite the lack of formal guidelines from the National Supplementary Health Agency. Recently, a suggestion for prescribing HDF was published in a Brazilian journal [9], following the initiative of implementation of the modality with the HDFit trial, a randomized study assessing the benefits of OL-HDF over HD, particularly in improving patients’ physical activity. [10]
The median follow-up in the current study was 27 months, which is similar to the follow-up period in the Turkish study [3] but shorter than the follow-up achieved in the CONVINCE study [5] (30 months) and the ESHOL study [4] (36 months). Nevertheless, despite the relatively short follow-up we observed 92 cases of death, which provided enough events to strengthen the statistical analysis. However, for the cardiovascular mortality, the number of events was too small to allow for meaningful analysis.
Comparing mortality between patients with and without private health insurance in Brazil is challenging. A previous study found no difference in 1-year mortality rates among adult patients starting HD from January 2011 to December 2021 [11]. In contrast, another study involving adults undergoing HD between 2012 and 2017 across 21 dialysis centers in Brazil showed an increased risk of death for patients whose treatment was funded by the public health system [12]. For incident patients, a population a higher mortality risk, it seems that patients with private insurance have an advantage in survival [13]. Discrepancy among results may be explained by differences in the populations included or in the statistical methods used, as Cox regression does not account for competing risks such as kidney transplant or recovery of renal function. Nonetheless, it is undeniable that patients who can afford private insurance are more likely to receive better overall care beyond just dialysis, including access to medical exams, treatment from other specialties, and hospitalization when needed.
Although Cox regression has been used long before the recognition of competing risks, it is now considered the most appropriate approach to assess survival in dialysis patients. In this population, follow-up for clinical events of interest is complicated by the possibility that a completely different event may occur first, such as recovery of kidney function or a kidney transplant—which could prevent the occurrence of the event of interest [14]. Indeed, a previous study in patients with chronic kidney disease (CKD) showed that traditional methods increasingly overestimated the risk of an event (such as kidney failure) as the follow-up time lengthened [15].
Recently, our group has compared patients on HD and HDF in Brazil in a propensity score matched study 2:1 (170 patients on public health HD : 85 patients on private insurance OL-HDF) [7]. The authors showed that HDF was associated with a reduced risk of mortality, after adjusting for age, type of access, Kt/V, hemoglobin, and phosphorus. Even with multiple adjustments, the question of whether HDF is superior remains influenced by the additional care that patients with private insurance receive. Moreover, private dialysis facilities in Brazil tend to offer more intensive multidisciplinary care, which includes physiotherapy, a factor that could impact the results beyond the dialysis modality itself. o that end, the current study is less likely to be biased, as the only difference among the dialysis centers was the dialysis modality. However, we cannot completely rule out the potential contribution of ultrapure water treatment, a condition that was only available to patients on HDF, and has been associated with lower inflammation [16] and mortality [17].
The presence of an arteriovenous fistula was associated with a lower risk of death in our study, which aligns with existing literature showing a significant impact on cardiovascular [18] and all-cause mortality [19]. It is still controversial this benefit in older patients [20]. Overall, fistula remains the preferred choice for vascular access in hemodialysis[21]. Longevity on dialysis is proportional to the quality of the treatment, which in turn depends on the access, ensuring and adequate flow rate to deliver the dialysis prescription. We demonstrated that the arteriovenous fistula was associated with a lower risk of death in patients on hemodialysis, a benefit that was further enhanced when OL-HDF was incorporated.
Our study should be evaluated considering some limitations: 1. We do not have data on nutritional markers, phosphorus and albumin. 2. The vascular access as a reference was the initial, in use at the time of study inclusion. 3. There is an imbalance between the groups, particularly in the prevalence of diabetes. However, we found that the hazard ratio for the modality did not change in the multivariate models, indicating that diabetes did not significantly influence our results. 4. We included prevalent dialysis patients, so mortality related to the initiation of dialysis could not be assessed. Our strengths include, first, the use of a competing risk analysis, which is more appropriate for the dialysis population. Second, we are the first in Brazil to compare HD and HDF in patients without private health insurance.
We concluded that OL-HDF was associated with a lower risk of death over a 2-year follow-up in a population without private health insurance in Brazil.
Data Availability Statement
Data supporting this research is available at https://data.mendeley.com/drafts/kmxhp4p5zr.
Funding
The author RME disclosure she received a research grant from the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ). The funder had no role in the design. data collection. data analysis. and reporting of this study.
Authors’ Contributions
Collect the data: EPL, AC and ECSA; Concept and design: EPL; Analyzed the data: RME; Written the manuscript: EPL and RME; Give significative contributions on reviewing the manuscript; EPL, JC, SFSR, DVA, WFR, AOM, CMB, and RME. All authors read and approved the final version of the manuscript.
Conflict Interest Statement
The author(s) declared no competing interest.
References
- Nerbass, F.B.; Lima, H.D.N.; Moura-Neto, J.A.; Lugon, J.R.; Sesso, R. Brazilian Dialysis Survey 2022. Jornal brasileiro de nefrologia : 'orgao oficial de Sociedades Brasileira e Latino-Americana de Nefrologia 2024, 46, e20230062. [CrossRef]
- Bello, A.K.; Okpechi, I.G.; Osman, M.A.; Cho, Y.; Htay, H.; Jha, V.; Wainstein, M.; Johnson, D.W. Epidemiology of haemodialysis outcomes. Nature reviews. Nephrology 2022, 18, 378-395. [CrossRef]
- Ok, E.; Asci, G.; Toz, H.; Ok, E.S.; Kircelli, F.; Yilmaz, M.; Hur, E.; Demirci, M.S.; Demirci, C.; Duman, S.; et al. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with high-flux dialysis: results from the Turkish OL-HDF Study. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association 2013, 28, 192-202. [CrossRef]
- Maduell, F.; Moreso, F.; Pons, M.; Ramos, R.; Mora-Macia, J.; Carreras, J.; Soler, J.; Torres, F.; Campistol, J.M.; Martinez-Castelao, A.; et al. High-efficiency postdilution online hemodiafiltration reduces all-cause mortality in hemodialysis patients. Journal of the American Society of Nephrology : JASN 2013, 24, 487-497. [CrossRef]
- Blankestijn, P.J.; Vernooij, R.W.M.; Hockham, C.; Strippoli, G.F.M.; Canaud, B.; Hegbrant, J.; Barth, C.; Covic, A.; Cromm, K.; Cucui, A.; et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. The New England journal of medicine 2023, 389, 700-709. [CrossRef]
- Nefrologia, S.B.d. Censo Brasileiro de Diálise. Available online: http://censo-sbn.org.br/inicio?_gl=1*xyuvlm*_ga*NjkxMDIwMTguMTczMDIxNzY5OA..*_ga_E1HJB87YJ7*MTczMDIxNzY5OC4xLjAuMTczMDIxNzY5OC42MC4wLjA. (accessed on.
- da Rocha, E.P.; Kojima, C.A.; Modelli de Andrade, L.G.; Costa, D.M.; Magalhaes, A.O.; Rocha, W.F.; de Vasconcelos Junior, L.N.; Rosa, M.G.; Wagner Martins, C.S. Comparing Survival Outcomes between Hemodialysis and Hemodiafiltration Using Real-World Data from Brazil. Journal of clinical medicine 2024, 13. [CrossRef]
- Barra, A.B.L.; Roque-da-Silva, A.P.; Canziani, M.E.F.; Lugon, J.R.; Strogoff-de-Matos, J.P. Characteristics and predictors of mortality on haemodialysis in Brazil: a cohort of 5,081 incident patients. BMC nephrology 2022, 23, 77. [CrossRef]
- Canziani, M.E.F.; Strogoff-de-Matos, J.P.; Guedes, M.; Barra, A.B.L.; Canhada, S.; Carvalho, L.; Gemente, D.; Poli-de-Figueiredo, C.E.; Pecoits-Filho, R. High volume online hemodiafiltration: a global perspective and the Brazilian experience. Jornal brasileiro de nefrologia : 'orgao oficial de Sociedades Brasileira e Latino-Americana de Nefrologia 2024, 46, e20230104. [CrossRef]
- Larkin, J.W.; Han, M.; Han, H.; Guedes, M.H.; Goncalves, P.B.; Poli-de-Figueiredo, C.E.; Cuvello-Neto, A.L.; Barra, A.B.L.; de Moraes, T.P.; Usvyat, L.A.; et al. Impact of hemodialysis and post-dialysis period on granular activity levels. BMC nephrology 2020, 21, 197. [CrossRef]
- do Nascimento Lima, H.; Monarrez-Espino, J.; Nerbass, F.B.; Moura-Neto, J.A.; Sesso, R.; Lugon, J.R.; Brazilian Dialysis Register, I. Comparison of 1-year survival between patients initiating chronic hemodialysis under public and private health insurance: register-based data analysis from Brazil. International urology and nephrology 2024, 56, 3013-3022. [CrossRef]
- Barra, A.B.L.; Silva, A.; Canziani, M.E.F.; Lugon, J.R.; Matos, J.P.S. Survival in hemodialysis in Brazil according to the source of payment for the treatment: Public Healthcare System (SUS) versus private insurance. Jornal brasileiro de nefrologia : 'orgao oficial de Sociedades Brasileira e Latino-Americana de Nefrologia 2023, 45, 302-309. [CrossRef]
- Aquino, H.B.S.; Canziani, M.E.F.; Barra, A.B.L.; Roque-da-Silva, A.P.; Strogoff-de-Matos, J.P.; Dalboni, M.A.; Moyses, R.M.A.; Elias, R.M. PTH may predict early mortality in incident patients on hemodialysis: results from a large cohort. International urology and nephrology 2025, 57, 545-551. [CrossRef]
- Roetker, N.S.; Gilbertson, D.T.; Weinhandl, E.D. A Brief Introduction to Competing Risks in the Context of Kidney Disease Epidemiology. Kidney360 2022, 3, 740-743. [CrossRef]
- Al-Wahsh, H.; Tangri, N.; Quinn, R.; Liu, P.; Ferguson Ms, T.; Fiocco, M.; Lam Md, M.N.N.; Tonelli, M.; Ravani, P. Accounting for the Competing Risk of Death to Predict Kidney Failure in Adults With Stage 4 Chronic Kidney Disease. JAMA Netw Open 2021, 4, e219225. [CrossRef]
- Di Iorio, B.; Di Micco, L.; Bruzzese, D.; Nardone, L.; Russo, L.; Formisano, P.; D'Esposito, V.; Russo, D. Ultrapure dialysis water obtained with additional ultrafilter may reduce inflammation in patients on hemodialysis. Journal of nephrology 2017, 30, 795-801. [CrossRef]
- Hasegawa, T.; Nakai, S.; Masakane, I.; Watanabe, Y.; Iseki, K.; Tsubakihara, Y.; Akizawa, T. Dialysis fluid endotoxin level and mortality in maintenance hemodialysis: a nationwide cohort study. American journal of kidney diseases : the official journal of the National Kidney Foundation 2015, 65, 899-904. [CrossRef]
- Wasse, H.; Speckman, R.A.; McClellan, W.M. Arteriovenous fistula use is associated with lower cardiovascular mortality compared with catheter use among ESRD patients. Seminars in dialysis 2008, 21, 483-489. [CrossRef]
- Pisoni, R.L.; Arrington, C.J.; Albert, J.M.; Ethier, J.; Kimata, N.; Krishnan, M.; Rayner, H.C.; Saito, A.; Sands, J.J.; Saran, R.; et al. Facility hemodialysis vascular access use and mortality in countries participating in DOPPS: an instrumental variable analysis. American journal of kidney diseases : the official journal of the National Kidney Foundation 2009, 53, 475-491. [CrossRef]
- Lyu, B.; Chan, M.R.; Yevzlin, A.S.; Gardezi, A.; Astor, B.C. Arteriovenous Access Type and Risk of Mortality, Hospitalization, and Sepsis Among Elderly Hemodialysis Patients: A Target Trial Emulation Approach. American journal of kidney diseases : the official journal of the National Kidney Foundation 2022, 79, 69-78. [CrossRef]
- Lok, C.E.; Huber, T.S.; Lee, T.; Shenoy, S.; Yevzlin, A.S.; Abreo, K.; Allon, M.; Asif, A.; Astor, B.C.; Glickman, M.H.; et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. American journal of kidney diseases : the official journal of the National Kidney Foundation 2020, 75, S1-S164. [CrossRef]
Figure 1.
Kaplan Meier survival analysis according to dialysis modality, online hemodiafiltration (OL-HDF, green line) or hemodialysis (HD, blue line).
Figure 1.
Kaplan Meier survival analysis according to dialysis modality, online hemodiafiltration (OL-HDF, green line) or hemodialysis (HD, blue line).
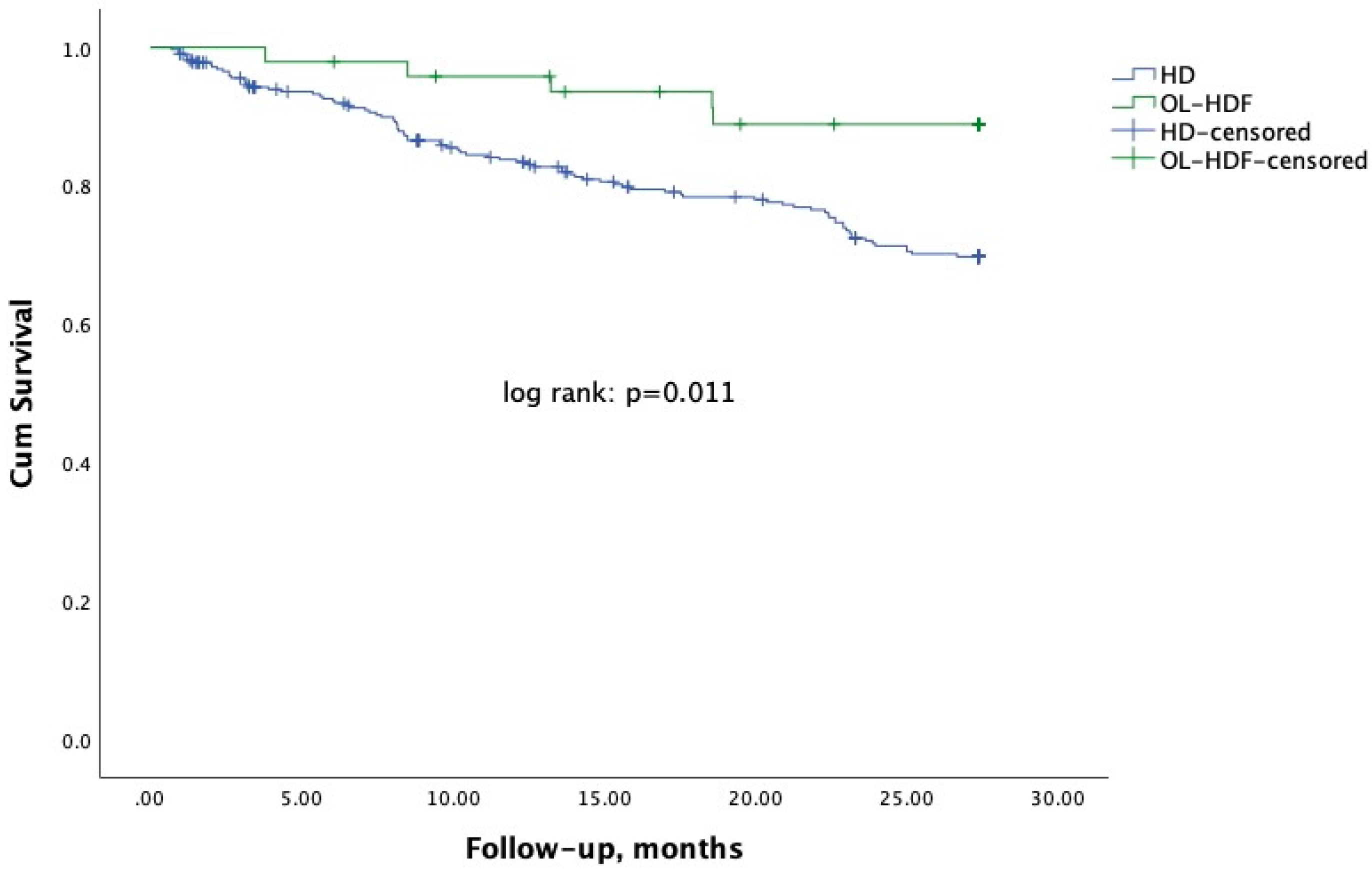
Figure 2.
Cumulative number of events according to dialysis modality (online hemodiafiltration – OL-HDF or hemodialysis – HD) and type of vascular access (catheter or arteriovenous fistula). From the top to the borrow lines represent patients on HD with a catheter (continuous blue line), patients on HD with arteriovenous fistula (dashed blue line), patients on OL-HDF with a catheter (continuous green line), and patients on OL-HDF with an arteriovenous fistula (dashed green line).
Figure 2.
Cumulative number of events according to dialysis modality (online hemodiafiltration – OL-HDF or hemodialysis – HD) and type of vascular access (catheter or arteriovenous fistula). From the top to the borrow lines represent patients on HD with a catheter (continuous blue line), patients on HD with arteriovenous fistula (dashed blue line), patients on OL-HDF with a catheter (continuous green line), and patients on OL-HDF with an arteriovenous fistula (dashed green line).
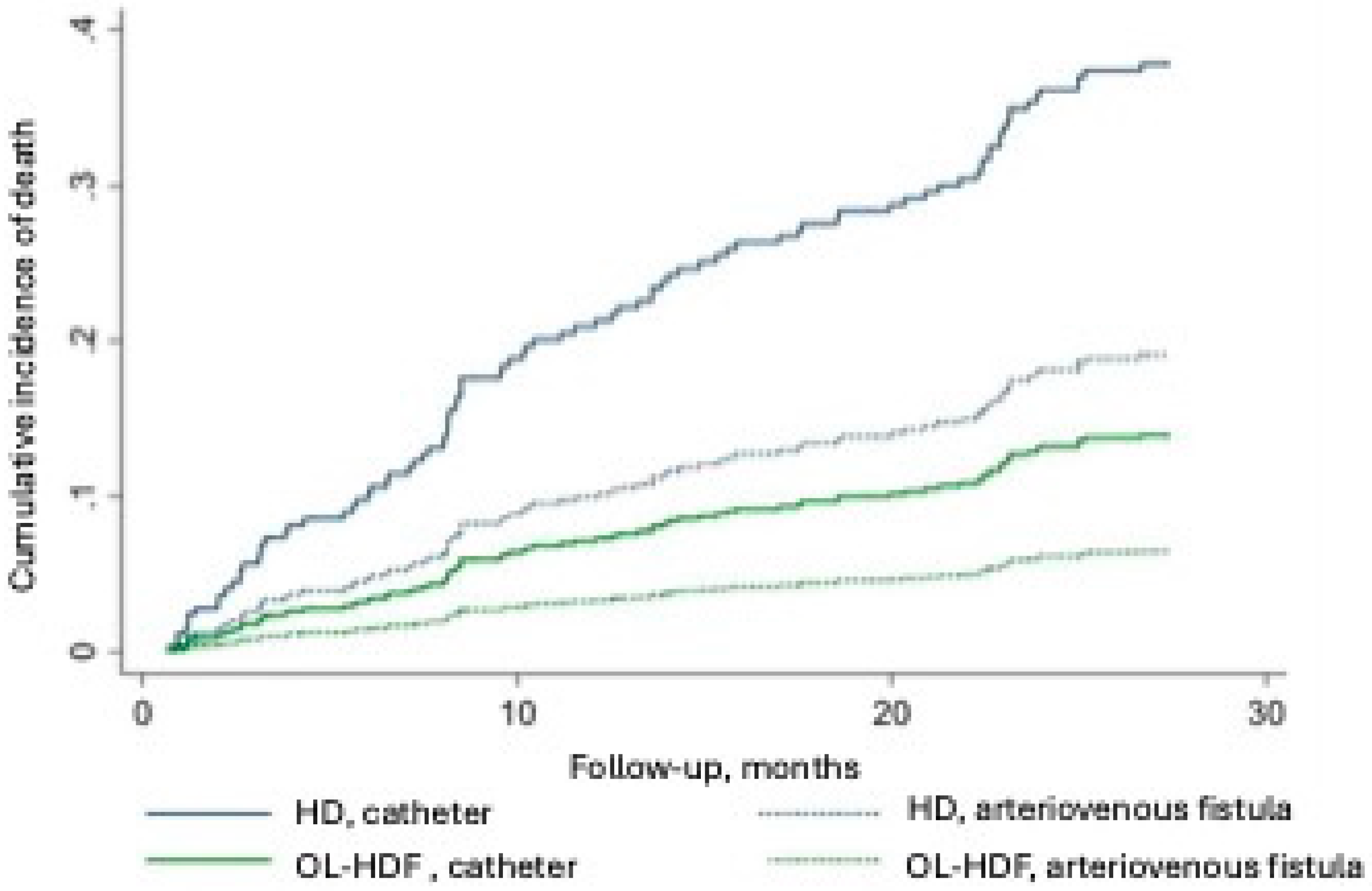
Table 1.
Characteristics of patients according to group hemodialysis (HD) or online hemodiafiltration (OL-HDF).
Table 1.
Characteristics of patients according to group hemodialysis (HD) or online hemodiafiltration (OL-HDF).
| Variable |
HD N=321 |
OL-HDF N=48 |
p |
| Age, years | 60 ± 14 | 61 ± 14 | 0.676 |
| White race, n (%) | 212 (66.0) | 32 (66.7) | 0.932 |
| Men, n (%) | 176 (54.8) | 30 (62.5) | 0.318 |
| Arteriovenous fistula, n (%) | 152 (47.4) | 21 (43.8) | 0.641 |
| Diabetes, n (%) | 175 (54.5) | 14 (29.2) | 0.001 |
| Dialysis frequency/week, % | <0.001 | ||
| 3 times | 94.1 | 66.7 | |
| 4 or more times | 5.9 | 33.3 | |
| Dialysis vintage, months | 75.1 (33.4. 156.0) | 35.3 (6.2. 68.2) | <0.001 |
| Week dialysis duration, h | 11.2 ± 1.8 | 10.5 ± 1.6 | 0.006 |
Unless otherwise specified. Data are expressed as mean ± SD or median (25, 75).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



