
Submitted:
16 August 2024
Posted:
19 August 2024
You are already at the latest version
Abstract
Despite the lack of evidence that suggests hemodiafiltration (HDF) offers a better survival outcome than standard hemodialysis (HD), the number of patients initiating HDF in Japan continues to rise. This study examined the temporal change in the number of HDF incidents, evaluated factors associated with all-cause mortality, and compared the mortality risk and survival time of patient on HDF with patients receiving standard HD in three sets of 2-year cohorts. The primary analyses included the insurance claims data of 460 HDF patients and propensity score-matched 903 standard HD patients who initiated dialysis therapy between April 1, 2012 and March 31, 2018. Patient follow-up was censored at the time of death or the end of the 2-year study period. The influence of comorbidities on all-cause mortality was investigated, and the survival outcomes between HDF and standard HD patient groups throughout cohorts were compared. The number of HDF patients was increasing throughout cohorts, but the proportions of mortality cases across cohorts slowly decreased. Dementia status increases the mortality risk of patients regardless of dialysis modality. The mortality risk among HDF patients with dementia was more significant than HD patients. Adjusting for all covariates, we observed that HDF patients had a reduced mortality risk and longer survival time than patients on standard HD. This study supports the notion that HDF reduces all-cause mortality compared with standard HD in an incident dialysis population in Fukuoka Prefecture, Japan.
Keywords:
hemodiafiltration
; hemodialysis
; all-cause mortality
; survival outcome
; insurance
; Japan
1. Introduction
In Japan, hemodiafiltration (HDF) and hemodialysis (HD) are the two most commonly used treatment modalities for end-stage renal disease (ESRD). Recent statistics showed that 55.1% of the dialysis population in Japan received HDF as the primary treatment, while 41.5% of the dialysis population in Japan received HD on a regular basis.[1] Although HD care has been available to the public as a treatment for ESRD through public insurance scheme since the 1960s, HDF was only officially recognized to be used for treating ESRD patients and was reimbursed by the Japanese health insurance system in April 2012.[2,3] Since then, the number of HDF patients has increased considerably.
Notable Randomized Clinical Trials (RCTs), which compared the outcomes of HDF with conventional HD, had been conducted in several European countries. However, the RCT results were inconclusive, and only two studies showed a survival benefit of HDF over conventional HD.[4,5] In the ESHOL trial examining the effectiveness of online HDF, the data revealed that HDF patients experienced a 30% lower risk of all-cause mortality, a 33% lower risk of cardiovascular mortality, and a 55% lower risk of infection-related mortality compared to those receiving standard HD care.4 These encouraging findings were further supported by the more recent CONVINCE trial, where the HDF patient group had a significantly lower all-cause mortality rate than the high-flux HD patient group.[5]
Nonetheless, all published RCTs contain a potential risk of bias, leading to overestimation or underestimation of the actual effect.[6] On the other hand, results from retrospective cohort studies showed favorable results for HDF, with statistically significant reductions in all-cause mortality or/and cardiovascular mortality.[7,8,9]
Notwithstanding, the results of studies which were conducted in European countries could not be generalized to the Japanese population due to significant practice variations.[10] Unlike the HD treatment for patients who treated in European countries, the use of low-flux HD in Japan is uncommon as most patients are treated with high or super-high dialyzers.[1,2,3] Studies also showed that the average blood flow for Japanese patients was between 200 and 220 ml/min.[3] With such low average blood flow, a predilution treatment for HDF is commonly used due to the difficulty of substituting an adequate volume during treatment time (average of 4 hours). Additionally, the volume of substitution fluid is also different between Europe and Japan. For on-line HDF patients in Japan, the mean volumes were 9.2 and 40.6 liters for the post-and-predilution treatment respectively.[3,11] The mean volume of 9.2 liters for post-dilution on-line HDF is lower than that of European countries and that reported level is necessary to provide a better outcome for on-line HDF patients. Likewise, favourable findings for on-line HDF reported in the ESHOL and CONVINCE trials were based on post-dilution mode. Due to low average of blood flow, such a dilution mode is uncommon in Japan, as it was estimated less than 10% of HDF patients were treated with post-dilution on-line HDF.[11]
There are not many comparative studies of HD and HDF survival among Asian populations that use population data over an extended period. A study that compares the secular trend in mortality between HD and HDF is currently unavailable. Therefore, this study was conducted to investigate the temporal change in mortality of patients in 3 sets of 2-year cohorts (April 1, 2012 – March 31, 2014, April 1, 2014 – March 31, 2016, and April 1, 2016 – March 31, 2018). The researchers measured the hazard ratio and mean restricted survival time for patients who were treated with HD and HDF for mortality within 2 years of follow-ups and compared the trend between these three cohorts. The survival differences between HD and HDF treatments over time were also compared.
2. Methods
2.1. Study Design
This study was designed as a retrospective cohort study. By using the electronic database, all ESRD patients that began on-line HDF or HD treatment between April 1, 2012 and March 31, 2017 were identified. Based on the treatment initiation date, the patients were divided into three cohorts: Cohort 1 (April 1, 2012 – March 31, 2014), Cohort 2 (April 1, 2014 – March 31, 2016), and Cohort 3 (April 1, 2016 – April 1, 2018). Patients in each cohort were followed for two years, starting from the day they received treatment until the day they died, emigrated to other prefectures, or by the end of 2 years of follow-up or whichever comes first. The primary endpoint of the analysis was death.
2.2. Study Location
This research was carried out in Fukuoka Prefecture, which is located on Kyushu Island in the southwestern region of Japan. Dialysis care is provided by a total of 199 institutions that are located all over the prefecture.1 These establishments are operated as ambulatory hemodialysis units which are attached to a hospital or as stand-alone hemodialysis centers or clinics.
2.3. Data Source
The data were mainly based on claims that were submitted to the Fukuoka Prefecture's Insurance Association for the Elderly. In Japan, citizens aged ≥ 75 are entitled to medical coverage under the Latter-stage Health Insurance Scheme. Insurance coverage extends to patients aged 65 to 74 with a particular disability such as ESRD who require ongoing dialysis care. Insurance claim records were stored electronically. The data were extracted from the insurance database using SQL Server 2014 (Microsoft Corporation, Redmond, WA).
2.4. Participant Identification
The population of this study was ESRD patients with active insurance status who began on-line HDF or HD treatment from April 1, 2012 - March 31, 2018. The International Classification of Disease, 10th revision, code N18.0 was used to identify chronic kidney disease diagnosis and specific insurance codes were utilized to confirm patients' HD or HDF maintenance status. This inclusion was limited to patients who received on-line HDF or HD exclusively as the primary treatment for ESRD. Thus, patients who primarily received peritoneal dialysis but also needed intermittent on-line HDF or HD care were excluded. Besides that, patients who changed treatment modality during the study period were excluded as well.
2.5. Matching
In this study, the baseline characteristics of HDF and HD patients were analyzed and the propensity scores for each patient were calculated based on sex, age and Charlson's comorbidity index score. Then, each HDF patient was matched with two patients on HD by applying a greedy matching algorithm with a caliper set at 0.2.[12,13]
2.6. Final Sample
460 HDF patients were identified and found to meet the inclusion criteria. These consisted of patients who began HDF treatment between April 1, 2012 and March 31, 2014 (cohort 1, n = 48), April 1, 2014 – March 31, 2016 (cohort 2, n = 110), and April 1, 2016 – March 31, 2018 (cohort 3, n = 303). For a comparative analysis, 907 propensity score-matched patients who began HD treatment between April 1, 2012 – March 31, 2014 (cohort 1, n = 96), April 1, 2014 – March 31, 2016 (cohort 2, n = 220), and April 1, 2016 – March 31, 2018 (cohort 3, n = 587) were identified. For cohort 3, only one propensity score-matched HD case was found for 19 HDF cases. The claim data of all patients (N =1367) were retrospectively reviewed and the reported all-cause mortality cases were analyzed. Figure 1 shows the participant selection process.
2.7. Definition of Variables
The patients were categorized by sex and two age categories: 65–74 years old and ≥ 75 years old. The International Classification of Disease, 10th revision (ICD-10) codes were used to identify the status of heart failure (I11.0; I13.0; I42.0 – I43; I50.0–I50.9), diabetes (E10, E11, E13, E14), cerebral stroke (I60.0–I66.9), malignancy (C00.0–C43.9; C45.0–C75.9; C76.0–D03.9; D05.00–D09.9), and dementia (F00, F01, F02, F03). By using unique patient identification, the data from the Long-term Care Insurance database were linked to identify the status of elderly care needs. In Japan, long-term care services are provided to the insured when people aged ≥ 65 and above require long-term care or support for daily activities. Available statuses include Support Level 1 (SL1) to Support Level 2 (SL2), and Care Level 1 (CL1) to Care Level 5 (CL5).[14] A higher care level indicates a higher degree of physical disability and the need for support. In this study, the status was categorized into three groups: low support (SL1 – SL2 and CL1), moderate support (CL2 – CL3), and high support (CL4 – CL5).
The Charlson Comorbidity Index (CCI) was adapted and used to assess the presence and severity of comorbid conditions.[15,16] This validated instrument assigned weights (1, 3, or 6) to each of 19 major comorbid conditions that would likely influence treatment prognosis and survival outcomes. This study modified the weight (m-CCI) to exclude chronic kidney disease. Subsequently, three categories were created based on the calculated weights to represent the degree of severity: mild (m-CCI ≤ 1), moderate (m-CCI = 2 – 6), and severe (m-CCI ≥ 7). The use of CCI to measure the severity of comorbid conditions based on the insurance claims data in Japan has been widely documented.[17,18]
2.8. Definition of Outcome
The primary outcome was all-cause mortality during the follow-up period. The insurance claim code 202 was used to determine mortality status. In the insurance data, such a code signifies loss of insurance eligibility due to death. Several epidemiological studies in Japan have used a claim-based definition of death. Past studies that validated such mortality status indicated high specificity and positive predictive values, suggesting a low likelihood of outcome misclassification.[19,20]
2.9. Data Analysis
In this study, data were analyzed by cohort (cohort 1, cohort 2, cohort 3). Data in each cohort were also combined and analyzed separately. The descriptive statistics for categorical variables were expressed in numerical values and percentages. The possible trend of HDF enrollment and all-cause mortality cases across cohorts were evaluated using Cochran-Armitage chi-squared for trend and the Jonckheere-Terpstra test.[21,22,23]
Cox regression analyses were performed to compare the mortality risks between HD and HDF patients, and restricted mean survival time (RMST) was calculated to measure the average survival time over the follow-up period. All reported P-values were 2-tailed and the significance level was set at P < .05. Stata Statistical Software: Release 17 (StataCorp LP, College Station, TX) was used to analyze the data.
2.10. Ethical Considerations
This This study used anonymized claim insurance data. Thus, the requirement to obtain informed consent was waived in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan. This study was also approved by the Institutional Review Board of Kyushu University (Clinical Bioethics Committee of the Graduate School of Medical Sciences, Kyushu University). Approval Code: 2020-9
3. Results
3.1. Baseline Characteristics of HDF Patients
Baseline characteristics of HDF patients were analyzed by cohorts. The number of patients that began HDF had increased dramatically across cohorts. The proportion of patients which were grouped by age and sex was almost balanced in all cohorts. Among patients who initiated HDF in cohort 1, a significant number of them had a history of heart failure and cerebral stroke. A similar trend was also observed among those who started HDF in cohort 2, where patients with heart failure and a history of cerebral stroke was prevalent. A high number of HDF patients with a history of heart failure was also observed in cohort 3, but the proportion of patients with a history of cerebral stroke was slightly reduced when compared with those without such status. In all cohorts, most HDF patients had no records of support care needs. This indicated that these patients were most likely physically independent and did not require daily living assistance. We failed to observe a significant trend in the proportion of HDF patients when they were analyzed against baseline characteristics except for diabetes status.
Analyses of mortality cases showed a decreasing proportion of HDF patients who died across the cohort, despite the number of reported cases in each cohort continuing to rise. A high number of cases were reported among older patients as well as those with heart failure, malignancy, and dementia. In terms of the status of care level, a high number of mortality cases observed among patients who began HDF in cohort 1 and cohort 2 were those who did not require daily living assistance or support. However, in cohort 3, those who require a moderate level of care showed the highest proportion of mortality cases. Table 1 summarizes the results of descriptive statistics of patients on HDF and the survival outcome within 2 years of follow-up according to the HDF initiation cohort.
3.2. Evaluation of Treatment Modality
The hazard ratios for patients on HDF were calculated by using patients on standard HD as a reference group. The analyses indicated a lower mortality risk among HDF patients than HD patients. However, the results were only statistically significant among patients who began HDF care in cohort 2 and cohort 3. By combining all propensity score-matched samples from three different cohorts, the reduction in mortality risk was also statistically evident. The calculated RMSTs for both groups also showed that patients with HDF treatment had longer survival time compared to those with HD treatment. There were also some improvements in terms of survival time based on cohorts. Although both modalities showed an improved survival outcome over time, HDF is still superior in terms of survival benefit as it offers a longer survival time. Table 2 summarizes the results of the analyses.
Kaplan-Meir plots were constructed to compare the survival function by plotting the cumulative incidence proportion (1 - survival). Log-rank chi-squared tests indicated a statistically significant difference in cumulative incidence proportion between HDF and HD groups for cohorts 2 and 3. Figure 2 presents the Kaplan-Meir plots of cumulative incidence proportion (1 - survival) for HDF and HD patients by cohorts.
4. Discussion
In this epidemiological cohort study, the researchers examined the incidence of ESRD patients on on-line HDF and evaluated the performance of HDF and standard HD in reducing all-cause mortality.
By evaluating patients' survival on HDF and conventional HD, the findings suggested that HDF may confer a survival advantage compared to conventional HD among Japanese patients. The analysis results for propensity score matched model (HR 0.32, 95% CI 0.26 - 0.40, p <.001) showed statistically significant reductions in mortality risk among HDF patients compared to patients with standard HD. Evaluation of survival estimates based on cohort also showed that the survival of HDF patients improved over time. These findings were not surprising, given that several studies had previously documented a superior performance of HDF over standard HD. A propensity score-matched cohort study that was conducted in Spain observed a significant 24% of reduction in all-cause mortality among HDF patients (HR 0.76, 95% CI 0.62 - 0.94) compared with standard HD patients.24 Likewise, a cohort study that used the Australian and New Zealand data also found that HDF patients were associated with a significantly lower risk of all-cause mortality (Australia: HR 0.79, 95% CI 0.72 - 0.87; New Zealand: HR 0.88, 95% CI 0.78 - 1.00).25 Comparatively, estimates of hazard ratios of this study were smaller, implying a more significant reduction in all-cause mortality. These results might be related to HDF practice variations such as the prevalent use of predilution mode among on-line HDF. A previous study that was conducted in Japan also found the superiority of the predilution mode of on-line HDF compared to the post-dilution mode in reducing all-cause mortality.26 Improving clinical practice in HDF care might also explain the improving survival risk across cohorts.[27]
The estimates of survival benefits were based on the Cox regression hazard ratio. However, several researchers who examined the utility of such estimates posited that they are not intuitive to interpret, have restrictive proportional hazards assumption, and statistical power depends heavily on the number of events.[28,29,30] Although the median survival time difference provides an intuitive interpretation, the researchers also argued that such an estimate is insensitive to outliers and is often less precise.[31] In this study, the event rate was low (< 50%); therefore, the median survival time and the difference could not be estimated. By considering data and methodological limitations, the analyses were supplemented with the calculation of RMST. As the statistical power depends on the exposed follow-up time, the RMST could provide a more precise estimate in case of a low event rate. The applicability of RMST in evaluating the treatment effects has also been documented in many medical studies. Nonetheless, analyses based on RMST also indicated that patients with HDF treatment had longer survival time in propensity score-matched analyses. Like Cox regression results, survival benefits of HDF increased over time across all cohorts. With that, additional statistical evidence was provided to the notion that HDF provides superior patient survival.
The survival improvement attributed to on-line HDF might also be linked to the high convection volumes, as indicated by previous studies. In CONTRAST trial, no significant differences in overall mortality were found between the HD and on-line HDF groups.[32] However, further analysis revealed that on-line HDF patients with high convection volume (>21.85 litres) experienced better survival outcomes.[32] In the ESHOL trial, which focused on high-efficiency post-dilution HDF patients with median convection volumes ranging from 22.9 to 23.9 litres, a 30% decrease in overall mortality rate was reported compared to HD patients.[4] A similar positive outcome was also seen in the CONVINCE trial that restricted patients who received high-dose on-line HDF with a convection volume ≥ 23 litres in post-dilution mode per session.[5] In this trial, a lower all-cause mortality risk among patients with HDF than conventional high-flux HD was observed. While the results of these studies strongly imply that high convection volume is needed for improved survival outcomes among post-dilution HDF patients, the positive effect of high-volume HDF could also be seen in pre-dilution HDF as evidenced in a Japanese study that analyzed the survival outcomes between conventional HD and pre-dilution HDF patient groups with a substitution volume of ≥ 40 litres/session, where an optimal substitution volume of 50.5 litres was determined to improve survival outcome.[33] Perhaps, with this preponderance of evidence, it is safe to say that the most critical factor is not performing HDF, but supplying enough convection volume during HDF is what matters.[34]
This study has several limitations. This study has several limitations. As it was an observational design, HDF treatment was not assigned randomly. Therefore, causality could not be assessed. The absence of random assignment also increases the risk of selection and confounding biases, potentially leading to skewed inferences and erroneous conclusions. Despite the bias was statistically controlled using propensity score matching (PSM), it is essential to note that no method can completely eliminate selection bias, as the success of PSM is contingent upon the availability and accurate measurement of all relevant confounders. While PSM significantly reduces selection bias and improves the reliability of inferences in observational studies, it cannot fully account for all confounding variables, particularly unmeasured ones. Additionally, such a technique could not be used as a substitute for randomization because residual confounding or reverse causality phenomena could not be ruled out. In our study, the issue is further complicated as the data used in the analyses were primarily obtained from the claim records provided by the insurance association (company). As the records were purposely submitted by the health care providers for reimbursement, they rarely contain crucial clinical information such as patients’ prescriptions, type of vascular access, dialysis vintage, blood flow rate, serum albumin level, blood flow rate, and fluid volume replacement. Additionally, the mode of on-line HDF, whether pre-dilution or post-dilution, could not be determined from the claims record. Nonetheless, the available data suggest that over 90% of on-line HDF in Japan is pre-dilution HDF.[11] The standard characteristics of pre-dilution HDF are as follows: Blood flow rate: 200-250 mL/min; Substitution fluid volume: 40-60L/session; Dialysate flow: 500-600 mL/min; Dialysis time: 4-5 hours; Hemodiafilter: protein leakage membrane, Central dialysate delivery system, and Target removal rate of αMG 35-40% and βMG 80%.[11]
Despite its limitation, to the best of our knowledge, this study is the first to analyze the all-cause mortality of incident Hemodiafiltration (HDF) patients in Japan. While there are several dialysis-related studies focusing on the older population in Japan, there is currently a lack of population-based studies evaluating HDF performance. Therefore, the results of this study may still have clinical relevance and can assist clinicians in selecting dialysis modalities for patients, especially older ones. Additionally, patients who changed their dialysis modality during the analysis were excluded, which helped eliminate any bias that may have been introduced by modality crossovers.
Analyzing healthcare insurance data is pivotal in identifying trends and patterns in healthcare utilization, offering insights that can drive policy decisions, improve patient outcomes, and enhance the efficiency of healthcare systems. In Japan, the number of patients with ESRD requiring dialysis care continues to increase as the country recorded 347,474 ESRD cases at the end of 2022, with a prevalence rate of 2,781 cases per million population.[1] A significant change in the trend for dialysis modality selection was also observed in recent years, where the number of ESRD patients treated with HDF has far surpassed the number of patients treated with HD and other modalities. As the number of ESRD patients initiated or switched treatment modality to HDF is expected to increase further, the findings underscore the importance of HDF studies in Japan, not only in providing information regarding improved patient survival but also in advancing the scientific understanding of dialysis treatment, expanding therapeutic applications, and assisting policymakers in making evidence-based decision.
In conclusion, this study supported the notion that HDF reduces all-cause mortality compared with conventional HD among dialysis population. Therefore, this study adds to the observational evidence which suggests the superiority of HDF among dialysis population of Fukuoka prefecture in Japan.
Author Contributions
AJ: conceptualization (lead); investigation (lead); writing the original draft (lead); formal analysis (lead). AB: review and editing (lead); supervision (lead); software (supporting); formal analysis (supporting). NL: review and editing (supporting); software (supporting). TF: review and editing (equal); software (supporting). SK: review and editing (supporting). YL: software (lead); conceptualization (equal); formal analysis (supporting).
Funding
No funding was received for this article.
Acknowledgments
The authors would like to express their gratitude to the Wide-area Association of Latter Stage Elderly Healthcare of Fukuoka Prefecture for providing a healthcare claims database.
Conflicts of Interest
The authors declare that they have no conflict of interest. This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Hanafusa N, Abe M, Tsuneyoshi N, Hoshino J, et al. Current Status of Chronic Dialysis Therapy in Japan (as of December 31, 2022). Article in Japanese. Nihon Toseki Igakkai Zasshi. 2023, 56, 473–536. [Google Scholar]
- Hanafusa N, Fukagawa M. Global Dialysis Perspective: Japan. Kidney360 May 2020, 1, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Akizawa T, Koiwa F. Clinical expectation of on-line hemodiafiltration: A Japanese Perspective. Blood Purif 2015, 40 (suppl 1), 12–16. [Google Scholar] [CrossRef]
- Maduell F, Moreso F, Pons M, et al. High-efficiency postdilution on-line hemodiafiltration reduces all-cause mortality in hemodialysis patients [published correction appears in J Am Soc Nephrol 2014, 25, 1130]. J Am Soc Nephrol 2013, 24, 487–497. [Google Scholar] [CrossRef]
- Blankestijn PJ, Vernooij RWM, Hockham C, et al. Effect of Hemodiafiltration or Hemodialysis on Mortality in Kidney Failure. N Engl J Med. 2023, 389, 700–709. [Google Scholar] [CrossRef] [PubMed]
- Schiffl, H. Online hemodiafiltration and mortality risk in end-stage renal disease patients: A critical appraisal of current evidence. Kidney Res Clin Pract 2019, 38, 159–168. [Google Scholar] [CrossRef]
- See EJ, Hedley J, Agar JWM, et al. Patient survival on haemodiafiltration and haemodialysis: a cohort study using the Australia and New Zealand Dialysis and Transplant Registry. Nephrol Dial Transplant 2019, 34, 326–338. [Google Scholar] [CrossRef]
- Canaud B, Bragg-Gresham JL, Marshall MR, et al. Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS. Kidney Int. 2006, 69, 2087–2093. [Google Scholar] [CrossRef] [PubMed]
- Maduell F, Varas J, Ramos R, et al. Hemodiafiltration Reduces All-Cause and Cardiovascular Mortality in Incident Hemodialysis Patients: A Propensity-Matched Cohort Study. Am J Nephrol 2017, 46, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Tomo T, Larkina M, Shintani A. et al. Changes in practice patterns in Japan from before to after JSDT 2013 guidelines on hemodialysis prescriptions: results from the JDOPPS. BMC Nephrol 2021, 22, 1–9. [Google Scholar] [CrossRef]
- Kawanishi, H. Development of on-line hemodiafiltration in Japan. Ren Replace Ther. 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Dyer M, Frieze A, Pittel B. (1993). The Average Performance of the Greedy Matching Algorithm. Ann Appl Probab. 1993, 3, 526–552. [Google Scholar]
- Wang Y, Cai H, Li C, Jiang Z, Wang L, Song J, et al. Optimal Caliper Width for Propensity Score Matching of Three Treatment Groups: A Monte Carlo Study. PLoS ONE. 2013, 8, e81045. [Google Scholar] [CrossRef]
- Yamada M, Arai H. Long-Term Care System in Japan. Ann Geriatr Med Res. 2020, 24, 174–180. [Google Scholar] [CrossRef]
- Sundararajan V, Henderson T, Perry C, Muggivan A, Quan H, Ghali WA. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef]
- Kim SW, Akiyama T, Morishita A. PNS73 Retrospective Study for Comorbidities in ACTIVE Population Using Japanese Health Insurance Claims Database. Value Health Reg Issues. 2022, 22 (Suppl), S94. [Google Scholar] [CrossRef]
- Kimura, T. , Sugitani, T., Nishimura, T., & Ito, M.. Validation and Recalibration of Charlson and Elixhauser Comorbidity Indices Based on Data From a Japanese Insurance Claims Database. Jpn J Pharmacoepidemiol/Yakuzai ekigaku. 2019, 25, 1–4. [Google Scholar]
- Ooba N, Setoguchi S, Ando T, et al. Claims-based definition of death in Japanese claims database: validity and implications. PLoS One. 2013, 8, e66116. [Google Scholar] [CrossRef]
- Sakai M, Ohtera S, Iwao T, et al. Validation of claims data to identify death among aged persons utilizing enrollment data from health insurance unions. Environ Health Prev Med. 2019, 24, 63. [Google Scholar] [CrossRef]
- Cochran, W. G. Some Methods for Strengthening the Common χ2 Tests. Biometrics. 1954, 10, 417–451. [Google Scholar] [CrossRef]
- Armitage, P. Tests for Linear Trends in Proportions and Frequencies. Biometrics. 1955, 11, 375–386. [Google Scholar] [CrossRef]
- Jonckheere, AR. A Distribution-Free k-Sample Test Against Ordered Alternatives. Biometrika. 1954, 41, 133–145. [Google Scholar] [CrossRef]
- Maduell F, Varas J, Ramos R, et al. Hemodiafiltration Reduces All-Cause and Cardiovascular Mortality in Incident Hemodialysis Patients: A Propensity-Matched Cohort Study. Am J Nephrol. 2017, 46, 288–297. [Google Scholar] [CrossRef] [PubMed]
- See EJ, Hedley J, Agar JWM, et al. Patient survival on haemodiafiltration and haemodialysis: a cohort study using the Australia and New Zealand Dialysis and Transplant Registry. Nephrol Dial Transplant. 2019, 34, 326–338. [Google Scholar] [CrossRef] [PubMed]
- Masakane I, Kikuchi K, Kawanishi H. Evidence for the clinical advantages of predilution on-line hemodiafiltration. Contib Nephrol. 2017, 189, 17–23. [Google Scholar]
- Masakane I, Sakurai K. Current approaches to middle molecule removal: room for innovation. Nephrol Dial Transplant. 2018, 33 (Suppl 3), iii12–iii21. [Google Scholar] [CrossRef] [PubMed]
- Royston P, Parmar MK. Restricted mean survival time: an alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med Res Methodol. 2013, 13, 152. [Google Scholar] [CrossRef]
- Perego C, Sbolli M, Specchia C, et al. Utility of Restricted Mean Survival Time Analysis for Heart Failure Clinical Trial Evaluation and Interpretation. JACC Heart Fail. 2020, 8, 973–983. [Google Scholar] [CrossRef] [PubMed]
- Kim DH, Li X, Bian S, Wei LJ, Sun R. Utility of Restricted Mean Survival Time for Analyzing Time to Nursing Home Placement Among Patients With Dementia [published correction appears in JAMA Netw Open. 2021 Mar 1;4, e213081]. JAMA Netw Open. 2021, 4, e2034745. [Google Scholar] [CrossRef]
- Ben-Aharon O, Magnezi R, Leshno M, Goldstein DA. Median Survival or Mean Survival: Which Measure Is the Most Appropriate for Patients, Physicians, and Policymakers? Oncologist. 2019, 24, 1469–1478. [Google Scholar] [CrossRef] [PubMed]
- Penne EL, Blankestijn PJ, Bots ML, et al. Effect of increased convective clearance by on-line hemodiafiltration on all cause and cardiovascular mortality in chronic hemodialysis patients - the Dutch CONvective TRAnsport STudy (CONTRAST): rationale and design of a randomised controlled trial [ISRCTN38365125]. Curr Control Trials Cardiovasc Med. 2005, 6, 8. [Google Scholar] [CrossRef]
- Kikuchi K, Hamano T, Wada A, Nakai S, Masakane I. Predilution online hemodiafiltration is associated with improved survival compared with hemodialysis. Kidney Int. 2019, 95, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Shin SK, Jo YI. Why should we focus on high-volume hemodiafiltration? Kidney Res Clin Pract. 2022, 41, 670–681. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of study participant selection.
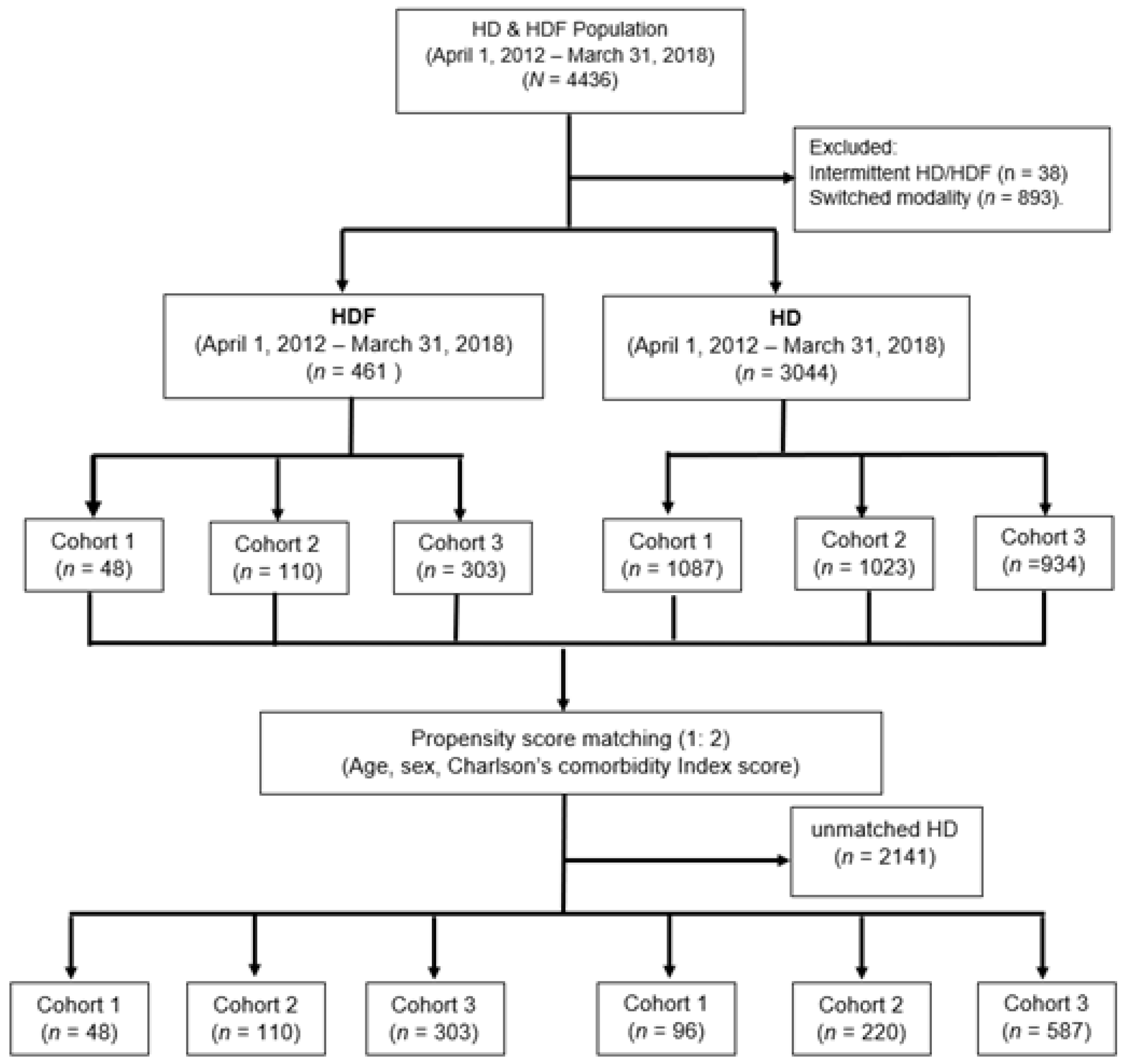
Figure 2.
Kaplan-Meir plots of cumulative incidence proportion (1-survival) comparing dialysis modality by cohorts. Cohort 1 (A): April 1, 2012 - March 31, 2014; Cohort 2 (B): April 1, 2014 – March 31, 2016; Cohort 3 (C): April 1, 2016 – March 31, 2018; All cohorts (D): April 1, 2012 – March 31, 2018. Statistically significant difference in cumulative incidence proportions was observed in cohort 2 and cohort 3, but not in cohort 1.
Figure 2.
Kaplan-Meir plots of cumulative incidence proportion (1-survival) comparing dialysis modality by cohorts. Cohort 1 (A): April 1, 2012 - March 31, 2014; Cohort 2 (B): April 1, 2014 – March 31, 2016; Cohort 3 (C): April 1, 2016 – March 31, 2018; All cohorts (D): April 1, 2012 – March 31, 2018. Statistically significant difference in cumulative incidence proportions was observed in cohort 2 and cohort 3, but not in cohort 1.
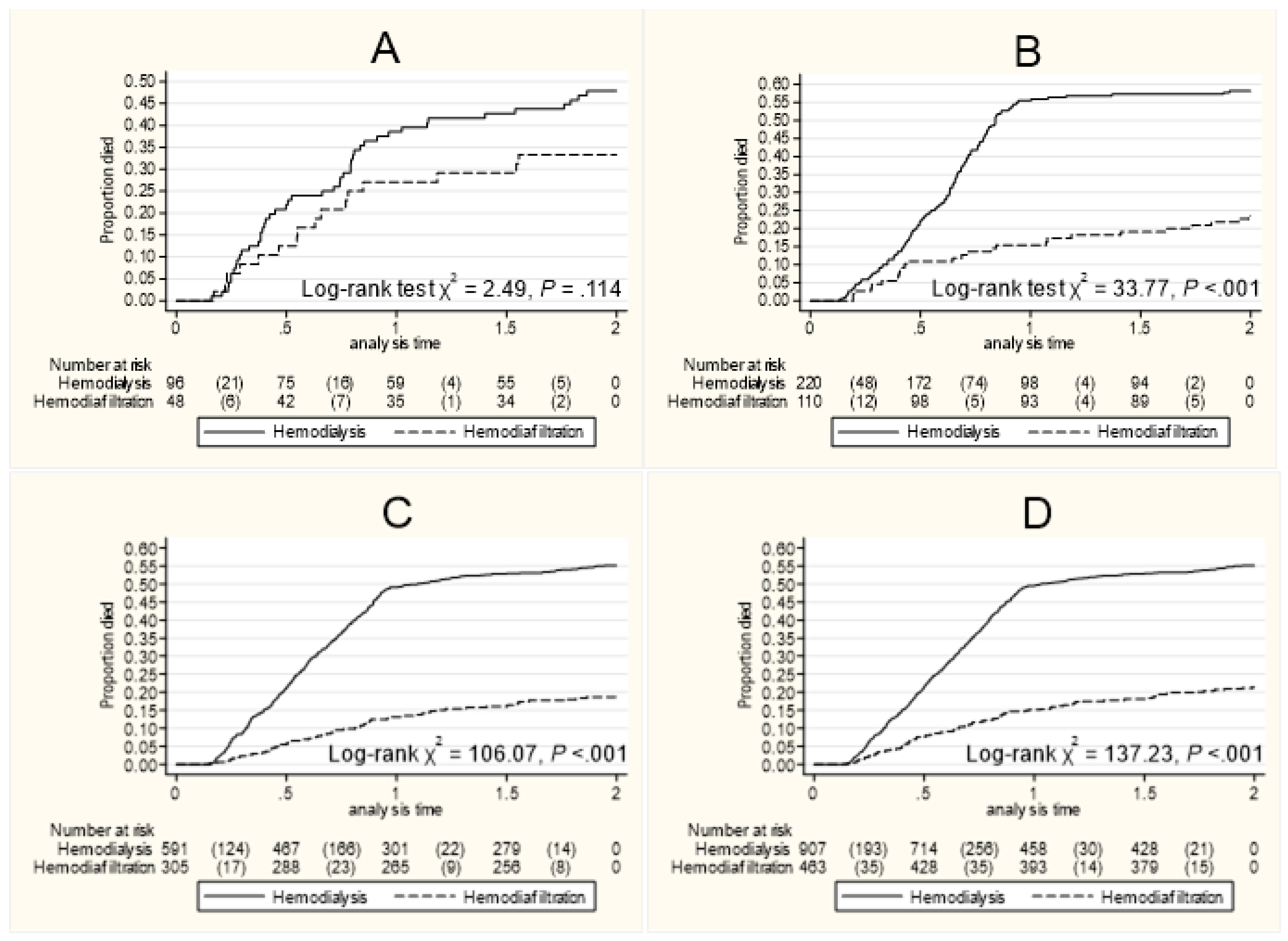

Table 1.
Descriptive statistics of HDF initiation and mortality cases within a 2-year follow-up.
| Cohort | Cohort 1 April 1, 2012 – March 31, 2014 |
Cohort 2 April 1, 2014 – March 31, 2016 |
Cohort 3 April 1, 2016 – March 31, 2018 |
All (April 1, 2012 – March 31, 2018) |
|||||||||||||||
| HDF (N = 48) | Died (N = 16, 33%) | HDF (N = 110) | Died (N = 26, 24%) | HDF (N = 305) | Died (N = 57, 19%) | HDF (N = 463) | Died (N = 99, 21%) | ||||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | *P | §P | ||
| Age | |||||||||||||||||||
| <75 | 24 | 50.0 | 8 | 33.3 | 58 | 52.7 | 7 | 12.1 | 151 | 49.5 | 14 | 9.27 | 233 | 50.3 | 29 | 12.5 | 0.74 | 0.34 | |
| ≥75 | 24 | 50.0 | 8 | 33.3 | 52 | 47.3 | 19 | 36.5 | 154 | 50.5 | 43 | 27.9 | 230 | 49.7 | 70 | 30.4 | |||
| Sex | |||||||||||||||||||
| Male | 24 | 50.0 | 8 | 33.3 | 50 | 45.5 | 12 | 24.0 | 169 | 55.4 | 37 | 21.9 | 243 | 52.5 | 57 | 23.5 | 0.16 | 0.34 | |
| Female | 24 | 50.0 | 8 | 33.3 | 60 | 54.6 | 14 | 23.3 | 136 | 44.6 | 20 | 14.7 | 220 | 47.5 | 42 | 19.1 | |||
| Heart Failure | |||||||||||||||||||
| No | 23 | 47.9 | 5 | 21.8 | 44 | 40.0 | 8 | 18.2 | 146 | 47.9 | 24 | 16.4 | 213 | 46.0 | 37 | 17.4 | 0.50 | 0.30 | |
| Yes | 25 | 52.1 | 11 | 44.0 | 66 | 60.0 | 18 | 27.2 | 159 | 52.1 | 33 | 20.8 | 250 | 54.0 | 62 | 24.8 | |||
| Diabetes | |||||||||||||||||||
| No | 39 | 81.3 | 15 | 38.5 | 79 | 71.8 | 20 | 25.3 | 204 | 66.9 | 36 | 17.7 | 322 | 69.6 | 71 | 22.1 | 0.03 | 0.88 | |
| Yes | 9 | 18.8 | 1 | 11.1 | 31 | 28.2 | 6 | 19.4 | 101 | 33.1 | 21 | 20.8 | 141 | 30.5 | 28 | 19.9 | |||
| Malignancy | |||||||||||||||||||
| No | 37 | 77.1 | 12 | 32.4 | 98 | 89.1 | 23 | 23.5 | 272 | 89.2 | 48 | 17.7 | 407 | 87.9 | 83 | 20.4 | 0.57 | 0.55 | |
| Yes | 11 | 22.9 | 4 | 36.4 | 12 | 10.9 | 3 | 25.0 | 33 | 10.8 | 9 | 27.3 | 56 | 12.1 | 16 | 28.6 | |||
| Stroke | |||||||||||||||||||
| No | 22 | 45.8 | 7 | 31.9 | 52 | 47.3 | 12 | 23.1 | 167 | 54.8 | 34 | 20.4 | 241 | 52.1 | 53 | 21.9 | 0.12 | 0.64 | |
| Yes | 26 | 54.2 | 9 | 34.6 | 58 | 52.7 | 14 | 24.1 | 138 | 45.3 | 23 | 16.7 | 222 | 47.9 | 46 | 20.7 | |||
| Dementia | |||||||||||||||||||
| No | 40 | 83.3 | 10 | 25.0 | 98 | 89.1 | 23 | 23.5 | 256 | 83.9 | 36 | 14.1 | 394 | 85.1 | 69 | 17.5 | 0.60 | 0.45 | |
| Yes | 8 | 16.7 | 6 | 75.0 | 12 | 10.9 | 3 | 25.0 | 49 | 16.1 | 21 | 42.9 | 69 | 14.9 | 30 | 43.5 | |||
| SCL | |||||||||||||||||||
| NA | 33 | 68.6 | 15 | 93.8 | 79 | 71.8 | 16 | 61.5 | 206 | 67.5 | 32 | 18.4 | 318 | 68.7 | 63 | 24.7 | 0.29 | 0.01 | |
| Low | 9 | 18.8 | 0 | 0.00 | 13 | 11.8 | 7 | 26.9 | 31 | 10.2 | 4 | 14.8 | 53 | 11.5 | 11 | 26.2 | |||
| Moderate | 5 | 10.5 | 0 | 0.00 | 12 | 10.9 | 0 | 0.00 | 44 | 14.4 | 14 | 46.7 | 61 | 13.2 | 14 | 23.4 | |||
| High | 1 | 2.08 | 1 | 6.25 | 6 | 5.45 | 3 | 11.5 | 24 | 7.87 | 7 | 41.1 | 31 | 6.70 | 11 | 55.0 | |||
| m-CCI | |||||||||||||||||||
| Mild | 19 | 39.6 | 6 | 39.6 | 31 | 28.2 | 3 | 9.68 | 108 | 35.4 | 20 | 18.5 | 158 | 35.1 | 29 | 18.4 | 0.67 | 0.81 | |
| Moderate | 14 | 29.8 | 3 | 29.2 | 42 | 38.2 | 15 | 35.8 | 100 | 32.8 | 13 | 13.0 | 156 | 33.7 | 31 | 19.9 | |||
| Severe | 15 | 31.3 | 7 | 31.3 | 37 | 33.6 | 8 | 21.6 | 97 | 31.8 | 24 | 24.7 | 149 | 32.2 | 39 | 26.2 | |||
*P for trend for incident HDF proportions (variables SCL and m-CCI were tested using the Jonckheere-Terpstra test, and others were tested using Cochran-Armitage Test for trend). §P for trend for the proportion of HDF patients who died (variables SCL and m-CCI were tested using the Jonckheere-Terpstra test, and others were tested using the Cochran-Armitage Test for trend). Abbreviation: HDF = Hemodiafiltration; SCL = Support & care level; NA = Not applicable, m-CCI = modified Charlson Comorbidity Index.
Table 2.
The estimates of 2-year mortality risk and survival time of older patients according to treatment initiation cohorts, treatment modalities, and statistical models.
Table 2.
The estimates of 2-year mortality risk and survival time of older patients according to treatment initiation cohorts, treatment modalities, and statistical models.
| Cox Model | Restricted Mean Survival Time (RMST) | ||||||||||
| HR | 95% CI | P | M | 95% CI | Diff | 95% CI | P | Diffa | 95% CI | P | |
| Cohort 1 | |||||||||||
| HD | Ref. | 1.13 | 1.03–1.24 | ||||||||
| HDF | 0.62 | 0.34–1.13 | .117 | 1.26 | 1.12–1.40 | 0.13 | 0.30–0.15 | .154 | - | - | - |
| Cohort 2 | |||||||||||
| HD | Ref. | 1.15 | 1.06–1.24 | ||||||||
| HDF | 0.33 | 0.22–0.51 | <.000 | 1.65 | 1.55–1.75 | 0.50 | 0.37–0.63 | <.000 | 0.45 | 0.31–0.59 | <.000 |
| Cohort 3 | |||||||||||
| HD | Ref. | 1.19 | 1.14–1.28 | ||||||||
| HDF | 0.27 | 0.20–0.36 | <.000 | 1.67 | 1.62–1.72 | 0.48 | 0.40–0.55 | <.000 | 0.45 | 0.37–0.52 | <.000 |
| All | |||||||||||
| HD | Ref. | 1.23 | 1.18–1.27 | ||||||||
| HDF | 0.32 | 0.26–0.40 | <.001 | 1.70 | 1.65–1.75 | 0.47 | 0.41–0.54 | <.000 | 0.45 | 0.37–0.52 | <.000 |
HD = Hemodialysis, HDF = Hemodiafiltration, HR = Hazard Ratio, M = Mean for survival time, Diff = Difference. Sample was based on propensity score matching (1:2), using Greedy algorithm with a caliper set at 0.20, and the estimates were adjusted for all study covariates. aDifference was adjusted for all covariates
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



